HEALTH SECTOR REFORMS IN UGANDA
advertisement

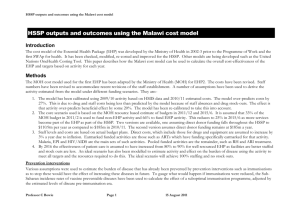
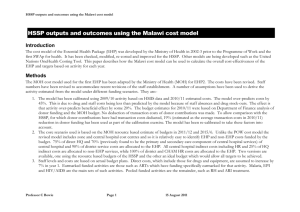
HEALTH SECTOR REFORMS IN UGANDA Reform Model in the Context of Post Conflict National Reconstruction A presentation to All Party Committee of Parliament, By Dr. Francis Omaswa, (formerly, DGHS, MOH, Uganda) Special Adviser, WHO, Geneva 9th May 2006, London. Outline of Presentation • Background & Context • Reforms – Across Government – Health Sector • Achievements • Challenges • Lessons Background & Context • Population 2006: 27m., Growth rate: 3.4% • Population Distribution: 80% Rural, 50%<15 yrs • GDP 2005 - $ 250 pc, Economic Growth 6%, Inflation 6%. • Proportion of people below the poverty line: 1992 1997 2000 2003 56% 44% 34% 38% BACKGROUND AND DEVELOPMENT MILESTONES • Political upheavals - Several coups 1966,1971,1979, 1985, still some unrest in parts of the country. • Prior to upheavals 1970s -1980s, country had best performing health sector in the region. • Period of decline resulted in reversal and total collapse of all sectors including health. • Opportunity of a new effort and new thinking with new leadership in mid 1980s. 250 200 150 100 50 00 20 95 19 91 19 88 19 80 19 69 19 59 19 48 0 19 infant deaths per 1000 live births Infant Mortality Rate in Uganda 1948 to 2000 (indirect estimates) Health Statistics – 1988 to 2002 Indices 1988 1995 2000 2002 UDHS UDHS UDHS Census IMR 122 97 88 83 Under 5 Mortality 203 147 152 MMR 550 506 504 Life expectancy 54 48 Fertility Rate 6.9 51 6.9 Reforms – across government 1. The Long term development vision – Vision 2025 2. New National Constitution 1992 - 1995 3. The Strategic Poverty Eradication Action Plan (PEAP/PRSP) 4. Public Sector Restructuring and Decentralisation of service delivery 5. New Public Sector Financial & Procurement Regulations 6. Other Governance Reforms: IGG, Human rights, Environment, Gender Reforms – across government PEAP Pillars 1. Framework for Economic Growth and Transformation 2. Ensuring Good Governance and Security 3. Directly increasing the ability of the poor to raise their incomes 4. Directly increasing the quality of Life of the Poor – – – – Improving the quality of education improving the quality of Health care Improving access to and equity of Water and Sanitation Reforms – Across Government PEAP Partnership Principles • Government of Uganda: – To seek donor support only for programs in PEAP – To develop comprehensive, costed, prioritized sector-wide programs covering the entire budget, so that government speaks with one voice. • Donors: – To ensure all support is fully integrated into sector-wide programs and is fully consistent with sector priorities – To end individual parallel country programs and stand alone projects – To increase level of delegation to country offices Reforms – Health Sector • 1986-1987: Sector Collapsed, donors came with free hand. Any help welcome. • 1986-1989: Health Policy Review Commission – consolidation of existing services and re-orientation to PHC • 3–year Rolling Plans and Donor Projects • 1996 – 2000: development of new National Health Policy (NHP) and Health Sector Strategic Plan (HSSP). Reforms – Health Sector SWAp Processes & Instruments • Government, NGOs, CSOs and DPs prepared the National Health Policy and Health Sector Strategic Plan facilitated by WHO Country Office. • HSSP1 was developed within the framework of the Poverty Eradication Action Plan (HSSP2 to revised PEAP and MDGs) Reforms – Health sector • SWAp structures – – – – – – – MoH and District Management Structures Health Policy Advisory Committee – and its technical Working Groups Joint Review Missions and National Health Assembly Health Development Partners Group Health Sector Working Group Interagency Coordination Committees Annual Meeting of District Directors & Hospital Managers • Tools for SWAp management – – – – – National Health Policy and Health Sector Strategic Plan Memorandum of Understanding Aide Memoirs of Joint Reviews Quarterly Performance Reports (Centre & Districts) Annual Health Sector Performance Report & Mid Term Review Report Other Reforms - Health Sector • Strengthened Regulatory Framework: – Professionals Councils – Health Services Act (Health Services Commission) – National Drug Authority & Medical Stores • Restructuring of the MoH & District Services • Improving Access and Quality of Care – Continuous quality improvement, service standards, equipment/infrastructure rehabilitation, health promotion and community mobilisation • Burden of Disease/Cost effective Study as basis for Minimum Health Care Package (1995) Achievements - Process • A clear vision for the sector: Minimum Health Care Package technically sound • Trust built between GoU, DPs, NGOs based on openness, mutual respect and patience. • Mechanisms for dialogue, monitoring and managing threats, weakness and strengths • Improved ownership, commitment & capacity of districts • Planning and Budgeting Process – transparent and consultative, – Result-oriented, Integrated Annual, Central and District Work plans; – Bottom up - from lower levels upwards given decentralisation. Achievements - Process Strengthened sector supervision, monitoring and evaluation: • The strategic plan with indicators for monitoring health sector performance • Annual Joint Review Mission : GoU – Central & Local, donor, private, civil society – replaced multiple donor missions • Institutionalised Support Supervision from the centre to the districts and lower levels • An Annual Health Sector Performance Report discussed at the JRM. Annual District League Table Resources Available to fund the HSSP I to II (2003/04 prices) 700.00 Billions Uganda Shillings 600.00 500.00 400.00 300.00 200.00 100.00 0.00 97/98 Govt Total NGOs 98/99 99/00 00/01 01/02 02/03 Donor Project Resource Envelope 03/04 04/05 05/06 User Fees 06/07 Government of Uganda Budget Expenditure for District Primary Health Care Activities 1997/98 to 2006/07 Proportion of GOU Health Sector Budget spent at the different levels 1999/00 to 2006/07 60% 50% 40% 30% 20% 10% 0% Central services District Health Services Central hospitals Regional referral Hospitals 120 100 80 60 40 20 0 19 97 /98 19 98 /99 19 99 /00 20 00 /01 20 01 /02 20 02 /03 20 03 /04 20 04 /05 20 05 /06 20 06 /07 19 99 /0 0 20 00 /0 1 20 01 /0 2 20 02 /0 3 20 03 /0 4 20 04 /0 5 20 05 /0 6 20 06 /0 7 billion Ug. Shs 140 Achievements - Inputs • Human Resources for Health – Recruited over 3,200 primary health care workers resulting in improved staffing levels of trained health workers – from 33% in 2000 to 68% in 2005. • Health Infrastructure – Constructed over 400 PHC units and upgraded others resulting in increased access to basic health services from 49% in 2000 to 72% by end of 2004, by 2005 to 84%. • Essential Medicines and Health Supplies – Increased per capita essential medicine funding from $0.8 in 2000 to $1.8 per capita in 2005 . per capita new OPD attendance New OPD attendance at public and PNFP health facilities during the HSSP I 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 0.9 Abolition of User Fees 0.72 0.79 0.7 0.6 0.4 0.43 1999/00 2000/01 2001/02 2002/03 2003/04 2004/05 HSSP I Target . pentavalent 3 infant coverage Pentavalent Vaccine 3rd dose Coverage in infants during the HSSP I 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 84% 83% 2002/03 2003/04 89% 85% 63% 48% 41% 1999/00 2000/01 2201/02 2004/05 HSSP I Target proportion mothers delivering in health facilities Proportion of expected mothers delivering in public and PNFP health facilities for the HSSP I 40% 35% 35% 30% 25% 20% 25% 24.40% 22.60% 19% 25% 20.30% 15% 10% 5% 0% 1999/00 2000/01 2001/02 2002/03 2003/04 2004/05 HSSP I Target Prevalence (%) 35 30 Nsambya Rubaga Mbarara Jinja Tororo Mbale 25 20 15 10 5 0 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 Year Challenges • Leadership and Management capacity for Health Services (centre and districts) – Human resources – recruitment, retention and deployment – Capacity of autonomous bodies still weak • Intersectoral collaboration • Sustaining partnership and trust – High turn-over of Development Partner staff – Sustaining level of commitment and mutual respect • Global Initiatives – Resurgence of vertical programmes • Low and stagnating (recent past) health sector public resource envelope – Macro-economics and Health Resources Available to fund the HSSP I to II (2003/04 prices) 700.00 Billions Uganda Shillings 600.00 500.00 400.00 300.00 200.00 100.00 0.00 97/98 Govt Total NGOs 98/99 99/00 00/01 01/02 02/03 Donor Project Resource Envelope 03/04 04/05 05/06 User Fees 06/07 Lessons • Government Leadership (Stewardship and Accountability) is critical determinant. • Reforms across government provide a positive enabling environment. • Comprehensive health sector planning with instruments for managing implementation essential. • All elements of the health systems are interlinked and synergistic and need simultaneous development. Lessons • Need for critical mass of committed individuals to trigger and champion the reform process. • Trust, Openness and mutual respect between government officials and DPs need to be nurtured. • WHO as a credible member state body can effectively facilitate health sector development at country level