Insulin
Diabetes Outreach
(June 2011)
Insulin
Learning outcomes
> Understand the difference between insulin
therapy in type 1 diabetes as compared to
type 2 diabetes.
> State what is meant by basal and bolus
insulin.
> Understand the main groups of insulins.
> Understand the basic principles regarding
insulin administration.
2
Insulin action
The action of insulin is to:
> Help the movement of glucose into the cells.
> Stimulate cells to take up glucose from the
blood.
> Facilitate the storage of glucose, amino acids
and fatty acids.
> Facilitate glycogen formation and storage in
the liver.
3
Aim of insulin therapy
> Exogenous insulin therapy aims to mimic the
actions of endogenous insulin production so that
blood glucose levels can be maintained as near
to normal as possible
– Type 1 diabetes: total insulin replacement for
survival
– Type 2 diabetes: insulin supplementation to
improve glycaemic control when OHAs are no
longer effective.
4
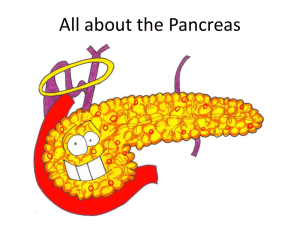
Blood insulin level
Natural insulin pattern
bolus
basal
5
Insulin in type 1 diabetes
> Insulin in type 1 diabetes is needed for survival.
> No insulin is produced and so insulin must be
administered to cover meal times (bolus) and
between meals and overnight (basal).
> Most people with type 1 diabetes are on an
intensive regimen ie basal bolus or insulin pump
therapy.
6
Insulin in type 2 diabetes
> Over time people with type 2 diabetes start to
produce less and less insulin and eventually
require insulin therapy to reach target BGLs.
> It is common for the person to start on one basal
injection in combination with oral hypoglycaemic
agents.
> Over time their treatment will intensify as insulin
secretion drops further.
7
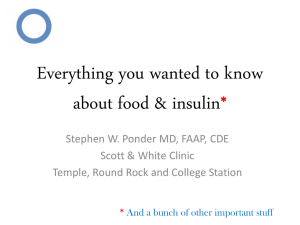
Types of insulin's available
Rapid (bolus)
Plasma Insulin Levels
Short (bolus)
Detemir (basal)
NPH (basal)
Glargine (basal)
0
2
4
6
8
10
12
14
16
18
20
22
24
Hours
8
Timing of insulin
Bolus (meal time)
Basal (background)
Timing
Timing
Rapid
immediately
Glargine
anytime (same
time each day)
Short
30mins prior
Detemir
Breakfast
Bed time (2130
or ask person)
NPH
Breakfast
Bed time
Pre-mix
- Rapid
- Short
immediately
30mins prior
9
Rapid insulins (bolus insulins)
Human analogue: Humalog/ Novo Rapid/ Apidra
> onset 0.25 - 0.5 hrs
> peak 1 - 3 hrs
> lasts 3 - 5 hrs
10
Short acting insulins (bolus)
> onset 0.5 - 1 hr
> peak 2 - 4 hrs
> lasts 5 - 8 hrs
11
NPH insulins (basal)
Isophane: Protaphane/ Humulin NPH (cloudy)
> onset
1 - 2 hrs
> peak
4 - 12 hrs
> lasts
16 - 24 hrs
12
Long acting analogue insulins
(basal)
Human analogue:
> Glargine
– onset
– peak
– lasts
2 - 4 hrs
nil
24 hrs
> Detemir
– onset
– peak
1 - 2 hrs
6 - 12 hrs
– lasts
20 - 24 hrs
13
Premixed insulin - human
Neutral plus Isophane mix:
Mixtard 30/70, 50/50, Humulin 30/70
> human (cloudy)
> mixture of intermediate and short
Mixtard 50/50
Mixtard 30/70
Humulin 30/70
14
Premixed insulin - analogue
Biphasic insulin aspart plus protamine mix:
NovoMix 30, Humalog Mix 25, Humalog Mix 50
> analogue (cloudy)
> mixture of intermediate and rapid
NovoMix 30
Humalog
Mix 25
15
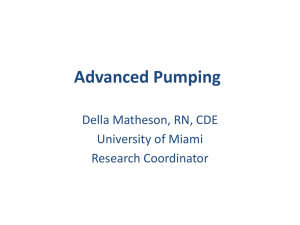
Self administration of insulin
What are the important factors to consider when
giving an insulin injection eg storage, sites for
injection, preparing the injection, side effects,
timing.
window indicating
dose
replaceable
needle to deliver
the dose
plunger
depressed to
deliver dose
dial rotated to
deliver dose
16
Insulin therapy in hospital
What are the nurses responsibilities in the area
of insulin administration whilst the person is in
hospital?
17
Syringe disposal
>
>
>
>
>
Take care at all times
Store supplies in their original box
Use a sharps container
Do not recap needles/ pen needles/ lancets
For local arrangements about safe disposal of
containers check council, public hospital or
community health centre.
18
References
> Diabetes Outreach (2009) Diabetes Manual,
Section 10: Medication
> MIMS product information sheet
19
20
 0
0