EHCP Parent Partnership
advertisement

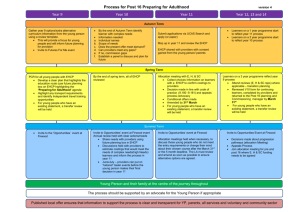
LONDON BOROUGH OF CROYDON Education, Health and Care Plan 23rd April 2014 Seven primary changes: 1. Assessment to involve parents, CYP; a different way of communicating 2. All duties apply to all LA funded schools including academies and free schools 3. Co-ordinated assessment process for 0-25’s 4. LA, Health and Care services to commission services for children jointly 5. A clear, transparent local offer of services to be published for all CYP with SEND 6. Statutory protection for 16-25’s; focus on preparing for adulthood; there will be a national framework for colleges 7. Families to be offered a personal budget; more choice and control for families to develop a personalised programme Bill amendments: • Children with disability added • LA’s have a duty to provide core information for, and to, children • Added a requirement to publish responses to comments linked to the Local Offer • Health and Social Care in a plan classed as ‘education’ • Social care duty in EHCP’s included – linked to the Chronically sick and Disabled Act 1970 (S2) • LA’s to have regard to age (requires additional time to complete their education • Young offenders included – new rights under new CoP • Mediation extended to cover health and care – tribunal extended? • LA’s to assist parents in making suitable arrangements A Family Centred System: • Need to involve children, parents and young people in decision making • Statutory right to contribute to the decision making process • More streamlined assessment process, co-ordinated across education, health and care, and involves children and young people and their families throughout. • New 0-25 Education, Health and Care Plan, replacing the current system of Statements and Learning Difficulty Assessments, which reflects the child or young person’s aspirations for the future, as well as their current needs. • Children have the right to be involved in making decisions and exercising choices. • Person centred planning Issues identified by Pathfinders • Health engagement/Joint Commissioning ~ new duty on health commissioning, to deliver the health element of EHC Plans • EHC plans from 0-25: thresholds, timing, panels, commissioning and outcomes • Phasing out SEN Statements & phasing in new EHC plans with parents at the centre of assessment process • Personal Budget implementation • Links with Education Funding Reforms/wider funding issues • Multi-agency keyworking support to assessment • IT and data • Children and young people below threshold for EHC Plan • Implementing new systems in difficult financial times • Statutory protections for young people 16-25 in full time education EHCP • Outcomes – including for adult life and arrangements for setting shorter term targets • Must consider the views, wishes and feelings of the child • Must consult with the child’s parent • A ‘tell us once approach’ • 20 week timescale; 6 weeks, 6 weeks, 2 weeks,15 days, 15 days Process: • Focus on CYP as individual – not label • Must outline the CYP’s views, interests and aspirations • What they have done, what they are interested in and outcomes • Drawing up a one page profile of the CYP • Including the CYP/family Overarching considerations: • We know the Early Years TAC model not appropriate for entire SEN cohort • Need to implement staged approach – based on level of need or/and funding model (process requires the same approach, planning/review requires differentiated approach) • Ability to change/adapt the model over 3 year implementation phase Key Worker vs. Co-ordination role KEY WORKER EHCP CO-ORDINATOR Direct 1:1 family contact high commitment Contact limited to key areas of process Time required to deliver contact 1:1 – time consuming Sufficient time provided to undertake family facing elements of the process Greater ability to ensure holistic approach Adoption of proportional approach based on children’s individual need Creation of ‘champions’ for age groups or agencies Administration burden removed from key workers/agencies Specialised input to EHCP ensuring high quality Specialism in co-ordinating Plan and Plan process; consistency in approach and content Reduces dependency culture from families on agencies Ability to complete plans in the absence of sufficient agency engagement Increased family satisfaction Increased family satisfaction – reduction in appeals Prior to request for EHCP + request Prior to requests: • Lead agency/person drawing up a one page profile of the CYP – key agency/worker (statutory) • Multi-agency meeting led by key agency/worker leading to collation • Collation of documentation – Key agency/worker – request made Following request: • LA receive request and 6 week statutory timeline initiated • To panel – EHCP Co-ordinator • Multi-agency EHCP Panel – agree/refuse application, confirm further documentation required Process – Stage 2: 10 weeks • Requested statutory evidence gathered – EHCP Co-ordinator • Meeting with parent to draft EHCP – EHCP Co-ordinator Objectives and targets set through reports Professional reports required to be outcome focused Process – Stage 3: 2 weeks • Document amended following parental meeting – EHCP Co-ordinator • Provision commissioned – Commissioning team Overview and sign off to be determined Process – Stage 4: 2 weeks Amendments made – document finalised Tribunal alerts provided/given at this point. No exception to timescales for late evidence! NB: clear advice only given on 16 weeks – clarification on ‘missing’ 4 weeks awaited Review • Annual • Review process/timeline identified by EHCP Coordinator • Entire plan to be amended, if necessary, every year. Model of good practice, negates ‘separate’ process • TAC approach too resource heavy for all cases; requires staged approach Disputes • New joint agency decision making process required for disputes between agencies • Needs independent group and chair - would require high level chair to ensure transparency and equity of decision making. • Needs to be (i) equitable between agencies or (ii) independent of all agencies Mediation • Parents have to discuss mediation option before they can go to appeal; parents are required to pro-actively consider mediation • LA’s have to agree to mediate with 30 day timeframe • LA’s may have to pay parents reasonable expenses to attend mediation (this does not include legal fees) but could include travel etc. There is a maximum cap on this. • LA’s will have to develop dispute resolution service for non-tribunal related disputes • Health and social care have to attend mediation in relation to their services in an EHCP (SENDIST likely to follow) • Mediation speculated to take longer