Scars unseen - Pennsylvania Homecare Association

Scars unseen
The Unique Needs of VETERANS
AT
END OF LIFE
Objectives
• Review Statistics of Veterans’ Illness and
Death in PA
• Describe the Differences between VA Model of Care and Community care
• Develop an Understanding of the “WE Honor
Veterans” Campaign
• Develop an Understanding of the “No Veteran
Dies alone” Mission
Pennsylvania Statistics
• Rank 5 th in the nation for Percent of Veteran
Population > 65 years
Pennsylvania Statistics
• Ranks 5 th in the nation for Veteran Deaths
Pennsylvania Statistics
Veterans Enrolled in VA
• Total Veterans = 1,014,884
– War Time = 708,200
– Gulf War = 183,500
– Vietnam = 320,400
– Korean Conflict = 117,700
– WWII = 109,800
– Peacetime = 255, 900
– OIF/OEF/OND = 51, 784
National Center for Veterans Analysis and Statistics, 2010
VISN 4 OIFOEF Dashboard, 2012
Demographic Imperative
Only 4% of Veterans die in VA
(~21,000)
~642,370 Veterans will die in 2012
MANY with advanced serious illness
PTF file and VetPop for 2012
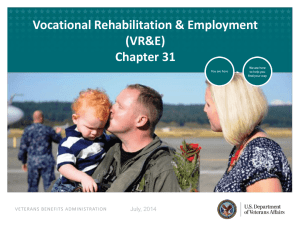
Selected Characteristics
30
25
20
15
10
5
0
Has a service connected disability
Uses VA
Health care
Use VA only No Health
Coverage
Below poverty
Male
Female
Source: U.S. Census Bureau, American Community Survey PUMS, 2009
Prepared by the National Center for Veterans Analysis and Statistics
Culture
Role
Funding
Location
VA Care vs. Community Care
Accountability
Veteran Affairs (VA)
Quasi- Military
Provider and Payer
Fixed appropriation and budget
Congress
Large Medical Centers
CBOC’s
Community
Nurse-led Movement
Provider
Entitlement-
Medicare/Medicaid hospice benefit: 3 rd party reimbursement
Governing body, CMS,
Fiscal Intermediaries, and
State
Private Homes
VA Hospice and Palliative Care
Film clip
VA Palliative Care
• Holistic
• Interdisciplinary Model
– Nursing
– Spiritual
– Psychosocial
– Symptom Management
– Medical Management
Palliative Care
• Even if a Veteran meets eligibility criteria for Hospice
Care, he might not be mentally ready for Hospice care.
• Palliative care (skilled nursing care symptom management) is offered until the Veterans symptoms are managed to an acceptable level set by the veteran.
Palliative Care continues until the skilled need or the goals of therapy are met or the veteran elects Hospice care.
Palliative care cont’
• Palliative care falls under the homecare umbrella of insurance coverage and can be offered through a home health and hospice agency. Not all homecare/hospice agencies have palliative care teams available.
• The Veteran must have a skilled need and be homebound in order for insurance to pay for it.
Veterans in Community Hospice /
Palliative Care
Home Hospice Care is provided wherever the Veteran calls Home
The VA purchases Community Hospice Service as a Comprehensive
Bundled per Diem Service for a Specific Period of Time.
If a Veteran has Medicare or Other Private insurance, he may elect to have the VA pay or his other insurance pay.
If a Veteran does not have insurance to pay for hospice care, the VA will pay through FEE basis, for the care the Veteran needs, through a community hospice agency.
Veterans in Community Hospice
The VA will pay for 3 levels of community hospice care
• Routine home care
• Continuous care
• Inpatient Care when indicated
For inpatient care, the hospice agency is to contact the VA for authorization prior to admission to an contracted facility.
Veterans in VA Health care
A VA Facility should be considered before a community facility
Reasons for Inpatient Admissions for Hospice and Palliative Care
• Uncontrolled Symptoms
• Inadequate Care or No Caregiver
• Caregiver Burden
What Influences Veteran Needs ?
• Cultural Impacts
• Fears
• Different War Eras
• Where They Served, How They Served
Cultural Impacts
• Military Service
– Military Values
– Stoicism
• Combat influences
– Heroic Measures
– Advance Directives
– Pets
Fears
65% Veterans :
• Have Poor Support Systems
• Have Psychological Stress
• Prefer the “Strength of many and the power and wisdom of the group”
• Oppose Institutionalization at End-of Life
• Desires Open Communication with Professionals
Different War Eras
• WWII
– Cold Injuries
– Mustard Gas Effects
– PTSD vs. Delirium
– Radiation Exposure
• Korean Conflict
– Cold sensitivity
– PTSD
– Minimizing of Experiences
War Eras Con’t
• Vietnam
– Alcohol/Substance abuse
– Agent Orange Exposure
– Homelessness
– Increased need for care
• Gulf war/OEF/OIF
– Exposure to Toxins
– Gulf war Syndrome
– TBI
– Chronic Fatigue Syndrome
PTSD- Post Traumatic Stress Disorder
• What is PTSD?
• 3 Major Symptoms
– Re-experiencing
– Avoidance
– Increased Arousal
• Management
• Spiritual and Emotional Distress
• Interdisciplinary Approach to Care
How can We IMPROVE Care to
Veterans?
• We Honor Veterans
• No Veteran Dies Alone
Designed to empower hospice professionals to meet the unique needs of dying Veterans :
• Military Check list
• Honoring Veteran Medical Needs
• PTSD & Psychosocial Needs
• Veteran Healthcare Benefits
How to Become Involved…
• Enroll
• Learn
• Complete Activity Reports
• Network
VA Provides Tiered Recognition
• Level 1- Commit to Program
• Level 2- Provide Education to Staff
Identify Veterans
• Level 3- Strengthen Relationships with VA
• Level 4- Increase Access and Quality Care to
•
Veterans
No Veteran Dies Alone
• “No one should die alone…. Each human
should die with the site of a loving face”
-Mother Teresa of Calcutta
• What is it?
• Who may help?
• How to help?
No Veteran Dies Alone
• National initiative
• The Department of Veterans Affairs says its mission is "to fulfill President Lincoln's promise ... 'To care for him who shall have borne the battle.' “
• VA hospitals around the country, provide the special care that Veterans desire when their final battle is coming to an end.
A Veteran’s Story
Jim Cooper
• Navy Frogman
• Korean War Veteran
• Advanced COPD
Home Care Agencies’ Best Friends
Federal Guide to Veteran & Dependent Benefits (on line & in print)
www.va.gov
(VA benefits, especially healthcare)
www.vba.va.gov
(general VA benefits)
VHA Handbook 1140.5 (Community Hospice Referral & Purchase
Procedures)
Your local VA facility Hospice/ Palliative Care POC, Community
Home Health Coordinator and Pre-registration staff
County Veteran Representatives – located usually in county courthouses
Summary
• Growing Numbers of Veterans
• Unique Needs
• How can WE honor Veterans?
– Collaboration
– Use of tools and Expertise
– Partnerships