X-Rays new - Rawalianresearch.org
advertisement

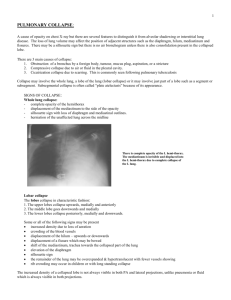
Tension hydropneumothorax • Air fluid level at right costophrenic angle • Deeper right costophrenic angle as compared to the left • Contralateral shift of mediastinum ARDS • Bilateral diffuse fluffy infiltrates • Normal cardiac size • Tracheostomy tube • Right subclavian central line going inside the right atrium • ECG wires Right lung collapse - PA view • Ipsilateral shift of mediastinum and trachea • Bronchial cut-off sign suggestive of endobronchial obstruction • Rib crowding • Loss of volume • Obscured right mediastinal and cardiac outline • Obscured right hemidiaphragm (silhouette sign) • Compensatory hyperinflation of left lung • Prominent left pulmonary artery (cardiac output passing through single artery) Right lung collapse – lateral view • Loss of gradually increasing transradiancy down the spine • Only one hemidiaphragm is visible (left) • Suspicion of mass in lower lobe with lymph node in mediastinum Left lung collapse • Ipsilateral shift of trachea, carina and mediastinum • Bronchial cut-off sign (left mainstem bronchus) • Rib crowding • Loss of volume • Compensatory hyperinflation of right lung Collapse with airbronchogram • Airbronchogram sign – Produced as a result of airspace opacification of the lung parenchyma – This results in visibility of the normally invisible black bronchi against a background of white opacification • Seen in consolidation and collapse with at least some patency of the bronchus Left upper lobe collapse – PA view • Loss of volume on left side • Ipsilateral shift of trachea and mediastinum • Compensatory hyperinflation of left lung • Raised left hemidiaphragm (compare with right) with tenting • Haziness over the aortic knuckle (silhouette sign) Left upper lobe collapse – Lateral view • Oblique fissure displaced anteriorly • Opacification anterior to the oblique fissure Right upper lobe collapse - PA view • Loss of volume on right side • Opacification of right upper lobe • Transverse fissure raised • Right hilum is also raised Right upper lobe collapse – lateral view • Oblique fissure displaced anteriorly • Transverse fissure pulled upwards • Opacification with loss of volume of right upper lobe Left lower lobe collapse – PA view • Loss of volume on left side • Ipsilateral shift of the heart • Both hila are at the same level (left hilum has come down) • Double opacity behind the heart • Outline of left hemidiaphragm is obscured (silhouette sign) • Left hemidiaphragm is raised (watch the gastric bubble) Left lower lobe collapse – Lateral view • Loss of gradually increasing transradiancy down the spine • One hemidiaphragm is clearly visible • Oblique fissure is displaced posteriorly Miliary shadowing • Multiple small millet sized nodules throughout both lung fields Mediastinal mass with left lower lobe collapse • Mediastinal widening in upper part mediastinum • Loss of volume on left side • Double opacity behind the heart • Left hemidiaphragm not visible • Heart shifted to the left side Aspergilloma • Fungus ball with surrounding rim of air Mesothelioma • Left sided pleural effusion • Associated lobulated pleural thickening • No shift of mediastinum due to encasement by mesothelioma Pleural based mass • Cat under the rug appearance indicative of pleural based origin • Angle between chest wall and opacity is obtuse (>90o) Sarcoidosis • Bilateral hilar lymphadenopathy • Right paratracheal strip enlargement • Bilateral infiltrates involving predominantly the mid zones Pneumothorax • Left sided apical pneumothorax • Visceral pleural line is clearly visible – There should be no lung markings distal to the visceral pleural line Effusion with collapse • Complete opacification of right hemithorax without significant contralateral shift of mediastinum • Absence of shift is indicative of concomitant collapse • Usually a sign of malignancy