lecture_5
advertisement

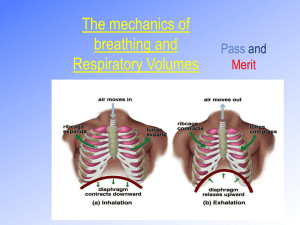
Man at High Altitudes • Atmosphere controls ability to live at high altitudes – Cold temperature – Low humidity – Low oxygen Physiological Responses to Cold Environments • Homeostasis- Warm-blooded mammals maintain a relatively constant body temperature regardless of ambient conditions- humans 37oC • Homeostasis achieved by control mechanisms that regulate heat production and loss • Core body temperature drop of a few degrees reduces enzymatic activity, coma, death • Core body temperature increases of a few degrees may irreversibly damage the central nervous system • C Van Wie (1974) Physiological response to cold environments. Arctic & Alpine Enviornments Adaptation to Cold Environments • To maintain temperature: – Increase insulation – Increase heat production – Lower core temperature (hypothermia) Thermoregulation • Heat produced by metabolic processes and muscular exertion – Inactive • Brain 16% • Chest and abdomen 56% • Skin and muscles 18% – Active • Brain 3% • Chest and abdomen 22% • Skin and muscles 73% Thermoregulation • Heat lost from body core to muscle and skin by conduction and convection • Blood circulating through body carries heat from core to outer body – Some lost to air – Much of the heat transferred to cooler veinous blood returning from extremities – Enables body to maintain extremities at lower temperature Thermoregulation Skin layer heat losses • As air flow increases, convective heat loss from skin increases- windchill • Evaporation • Predominant heat loss from skin in cold environments is radiation – Nude, with skin temp 31C, radiates 116 Watts to room with walls of 21C – At rest, total heat production is 84 Watts – Better put some clothes on Wind Chill Science • http://windchill.ec.gc.ca/workshop/index_e.html? • http://windchill.ec.gc.ca/workshop/papers/html/ses sion_2_paper_1_e.html • Bluestein, Maurice, Jack Zecher, 1999: A New Approach to an Accurate Wind Chill Factor. Bulletin of the American Meteorological Society: Vol. 80, No. 9, pp. 1893–1900. Pathologic Effects of Excessive Heat Loss • If skin temperature < freezing for extended period: – Chilblains- red, swollen itching lesions between joints of fingers – Trench foot- similar to chilblains except on foot • If skin freezes – Frostbite- local burning and stinging followed by numbness • Exposure- condition when body is not able to maintain a normal temperature – Core temp < 30C lose consciousness – Core temp < 27C heart ceases Physiological Response to Cold Stress • Autonomic control measures respond to cold by: – Increasing heat production – Increasing insulation layers – Permit moderate hypothermia (lower core body temperature) Heat Generation • At rest, muscles provide 18% of total heat • Voluntary exercise- heat production increased 10 times • Involuntary exercise- shivering – heat production increased 4-5 times – but 90% of heat produced by shivering lost by convection because of body movements • Non-shivering thermogenesis – Metabolism/hormones of body adjust and increase heat production Insulation • Initial reaction to cold – Blood vessels in extremities contract rapidly – Increases insulation of body • Long term- more fat Physiological Factors of Altitude: Oxygen Deficiency • • • • • • Proportion of Oxygen in atmosphere- 21% Partial pressure of Oxygen decreases with height in proportion to other gases Lungs saturated with water vapor; reduces available oxygen Oxygen in lungs: (ambient pressure – saturation water vapor pressure at body temp (37C) (63 mb)) * .21 Sea level (1013 – 63 ) * .21 = 200 mb; 5000 m (540 – 63 ) * .21 = 100 mb Hypoxia- intolerance to oxygen deficiency – Humans can tolerate half sea level value indefinitely – Symptoms significant above 3000 m (133 mb of Oxygen) • Standard Atmosphere varies with latitude (4000 m roughly 630 mb equatorward of 30o; 593 mb (winter)-616 mb (summer) at 60o • Cyclone could drop pressure 10-20 mb; equivalent to several hundred meters in elevation • Grover (1974); Man living at high altitudes. Arctic and Alpine Environments. Inspired Oxygen as a Function of Elevation 200mb 100mb Supplemental Oxygen • Mt. Everest (8848 m/29,028 ft) – Mean pressure near 314 mb – Most climbers use bottled oxygen above 7300 m (24,000 ft) • Pilots required to use supplemental oxygen above 3810 m (12,500 ft) for flights lasting more than 30 minutes Oxygen in the body • PIO2- inspired oxygen- oxygen available in the lungs • O2 transported in body by respiratory pigment haemoglobin in red blood cells – Lungs oxygenate blood – Heart pumps blood through body – High pressure of O2 in capillaries causes diffusion into tissue • Sea-level- 100 ml of blood contains 20 ml of O2 Physiological Adaptions to Hypoxia • Reduced PIO2 reduces pressure of O2 in blood: PaO2 • Brain triggers respiratory muscles to bring greater volume of air into lungs with each breath • Hyperventilation- increase volume of air inspired per minute offsets decrease in air density • # O2 molecules taken into lungs per minute is nearly same as at sea level • However, while quantity of O2 available in lungs remains unchanged, PaO2 reduced as elevation increases • Reduced PaO2 haemoglobin binds less O2; less saturation of O2 in blood; reduces O2 in blood Oxygen Saturation 70 116 mb Haemoconcentration Other physiological changes • Decrease in Oxygen in blood causes heart rate to increase initially in order to maintain Oxygen transport • Amount of water in blood plasma decreases after about a week – Decreases plasma volume without changing volume of red blood cells – Blood can carry greater quantity of Oxygen – Prolonged hypoxia stimulates bone marrow to produce more red blood cells • After a week, heart rate normalizes but stroke volume (volume pumped by left ventricle) decreases, leading to net drop in cardiac oxygen output VO2 • Highest pressure in O2 transport system determines efficiency of system • VO2- aerobic working capacity- maximum amount of O2 that can be consumed per minute • 10% decrease in VO2 per 1000m increase in altitude above 1500 m • Humans can’t work as hard at high elevation as at lower ones VO2 Problems at High Altitude • Humans can adapt to altitudes of 3-4 km and remain healthy indefinitely • Acute mountain sickness- initial response to rapid ascent to high elevation – Poor sleep; headaches; nausea; vomiting; apathetic; irritable; little appetite • Chronic mountain sickness- develops in people who have lived at high elevation for years; lose adaptation to hypoxia • Pulmonary Oedema – Accumulation of fluids in the lungs interrupts transfer of oxygen from air to blood Athletic Use of Hypoxia http://www.sltrib.com/2001/aug/08262001/sports/126267.htm