Changing incentives for health workers through a
advertisement

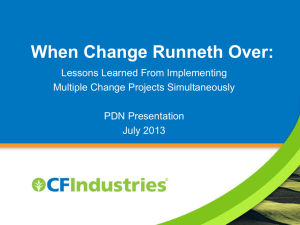
Changing incentives for health workers through a voucher scheme for maternal health services Ekirapa- Kiracho E1, Kiwanuka SN 1, Ruairi B 2, Sengooba F 1, Thomas S 3 • • • • • • Chraic Scholarship Program Irish Aid DFID and Future Health Systems Consortium Maker ere University School of Public health Trinity College Dublin Royal College of Surgeons Outline • • • • • Introduction Methods Results Discussion Policy implications Introduction and background • MMR- 435 per 100,000 live births • Utilization of MCH services has been low Health facility deliveries (42%) (UDHS 2006) 4th ANC (47%) and PNC within 1st 2 days (23%) • Constraints on the demand side and supply side • Demand and supply side interventions to increase access to MCH services Intervention Maternal child health services Vouchers for MCH services Vouchers for transport Pregnant women in control Training Supervision Supplies, drugs and equipment Maternal child health services Pregnant women in Intervention Aims • The intention of this study was to explore changes in the incentives for providers and their influence on the behaviour of providers Methods • Study design - case study design • Study site – Kamuli and Pallisa districts • The study population - health workers, community leaders and women of reproductive age • Data was collected using key informant interviews (health workers – 25 and community leaders- 13) and 16 focus group discussions (women of reproductive age) prospectively • Coding and Analysis – assisted by Nvivo Incentives for health workers -Increased allowances, top ups -Increased income for facilities “Am very happy one Hundred times. The money that is the reality I would even have gone away” Improved working conditions -Resources( supplies, equipment, infrastructure) “Like this money that we recently got I bought some scrubing brush, liquid soap, Jik and then moppers. I saw that it was encouraging the staff because we used to use hand brooms, compound brooms for scrabing the ward. At least when you have this one it encourages the staff.” Increased job enrichment - acquisition of new skills- diversity of patients - patients to work on “If you are a mid wife and mothers come to deliver you just enjoy to work you will just know that you are working but when you just sit there Idle you even forget some complications of labour and then you mess up and because you take time to deliver and when they come you get the chance to know other complications” Incentives for health workers Increased team spirit and cooperation among staff We help on the side of antenatal because there is a time when women may come to deliver like three or two a day. And then you find she can’t be here and there in antenatal .so for us we help her there. Opened doors for other opportunities for “because if it was not you people our deliveries funding would be really down and we were not going to score anything so I believe it is you who have made us score so that our graph is high” Training Interviewer: According to you what new things would you say that you have learnt? Interviewee: New born care including the mothers. Interviewer: Where did you learn that from? Interviewee: In the workshop Perspective of clients about health workers Health workers were more available “ These days nurses attend to mothers even at night ....... Sometime ago ....nurses would remain indoors without coming out to help the mothers” Health workers are more responsive “Ever since the project started they respond very fast and keep on checking on you” Attitudes of health workers have improved “The coming of the project helped us so much to improve on the health workers’ attitudes towards the patients; they no longer shout at us and they give us good care” Improved client community relationships “We had no love for a hospital because of the nurses; we used to change from hospital to hospital, but ever since Results EXPENDITURE OF FUNDS RECEIVED BY THE HEALTH FACILITIES INFRASTRUCTURE 23% DRUGS/SUNDRIES PERSONNEL 13% 61% EQUIPMENT 3% Financial incentives • Financial incentives very important when salary is very low • Conflicts were minimized by Discussing procedures with district management Asking facilities to meet and agree on how to spend the money Getting feedback and reviewing procedures and amounts for payment Inclusion of all health workers in facility Challenges • One of the challenges reported was a high workload especially in understaffed facilities • Lack of basic infrastructure such as wards for admission, ambulances, facilities for record keeping • Sustainability of such positive initiatives “When the project was still going on, the nurse was ever available but these days, she first digs; she doesn’t mind at all, so we request the project to come back and we get good services” Discussion • Financial and non financial incentives together with their internal drive to serve patients had a positive influence on the behaviour of the health workers Health workers not inherently rude but working in difficult circumstances Absenteeism linked to need to supplement salary, redundancy, poor working conditions Use of existing systems / structures for reporting imp for reducing burden on health workers Limited use of non financial incentives at facility level Policy implications • Governments need to have comprehensive plans for providing resources for the delivery of MCH services. • Negotiation with donors to promote planned targeted use of resources rather than a project approach but results and accountability must be strengthened! Human resources development - hands on workshops, facility level supervision and mentoring, problem solving techniques Human resources numbers – intergration and team work, recruitment , training of middle level providers Increased remuneration - Salary with additional amounts linked to performance ( incentives for improving efficiency and quality ) Basic Infrastructure -wards, ambulances, lighting Governments must invest in their human resources for health for sustained improvements in the performance of health workers 16