Uploaded by
sydney williams
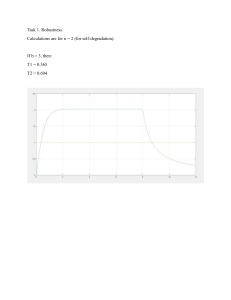
Medical-Surgical Nursing Review: Pancreatitis, Labs, Transfusions
advertisement

- Review s/s of hypocalcemia that demand immediate attention - MAINTAIN RESP FUNCTION - Labs - Glucose elevated because pancreas damage - Amylase elevated in blood - Infection causes WBC to increase Peritonitis - Fever, bloating, abd tenderness, rigid abd - Assess vitals for hypovolemic shock - Diaphoresis - Firm and in conjunction with severe abd pain Diverticulitis - n/v/d fever chills - Not contagious **REVIEW LAB INDICATORS - Low wbc- r/f - Decreased iron- iron deficitient anemia, chronic blood loss - Plt- know what to report in plt, low= report immediately - HGB- low is r/t anemia, skin pallor and nail beds - ALT and PT elevated in liver disease, cirrhosis, and hep B - PT INR increased with anticoagulants if pt is overdosed - Coumadin(warfarin) antidote = vitamin K - Heparin antidote =protamine sulfate - Review donor compatibility - Step to starting blood transfusion - Pt consent - Type and cross match - Check compatibility - Verify with nurse - For first 15 min be in the room with the pt - Look at post transfusion labs to compare results - Reaction steps - Stop infusion - Get rid of tubing - Infuse with NS - Monitor VS - Send blood bag AND tubing to the lab - Gauges - 18-23 - Blood infused over 2-4 hours, no more than 4 hours - Admin within 30 min of getting the bag - If pt comes 24 hours later with s/s of reaction, what med are you going to give? - Benadryl and NS - Watch pt for s/s of anaphylactic shock - Bronchospasm - HTN - Edema - Watch for circulatory overload - Crackles in the bilateral lower lobes - Tachycardia because the body is compensating - Decreased O2 - Altered mental status - Giving blood and the pt has hematuria and flank pain - s/s of hemolytic reaction - Blood products transfusion - When giving FFB needs to be thought out before because it is frozen so it needs to be thawed out - Infused over 15-30 min - Match ABO compatibility, if not the patient can have a reaction - WBC transfusion - Given to immunocompromised because of the risk for severe reaction - 400mL of plasma over 45-60min - Vitals every 15 min - Iron deficiency - adolescents(9th/10th grade), also in 70 y/o - Low HGB, low RBC - Cause: poor folic acid intake, bone marrow suppression, vegetarians - Pt will be getting iron - Black tarry stools - Stain teeth - s/s: cold extremities, pallor nail beds and mucous mem, orthostatic hypotension, SOB with exertion - Megaloblastic anemia - B12 and folic acid deficiency - Replace the supplements - Category of anemia, pernicious is a specific cause within this category - Pernicious anemia - Prevention of absorption of B12 - Requires B12 injections and can also be given Intranasal - Numbness in extremities, shiny beefy red tongue - Idiopathic aplastic anemia - Decreased in ALL blood cells - High risk for infection - Watch for s/s of infection - Cirrhosis - Life threatening complication of cirrhosis is hepatic encephalopathy - Inability to remove toxins which will damage brian - Do ammonia Lvl - Combative and confused if elevated and maybe GI bleed - LOC and neuromuscular changes - Asterixis (hand flapping) - DON'T talk slowly but communicate clearly, give time to respond. - You will also see ascites, measure the abd girth - You will be giving diuretic and low Na diet - Can develop esophageal varices - Propranolol to decrease the risk for bleeding - Effectiveness check: no blood in urine, negative stool test - Ascities - Paracenthesis as the diagnostic procedure - Need informed consent! - Assist pt to void to prevent r/f injury to the bladder - Cholecystitis - Inflammed gallbladder - Pain in RUQ - s/s: Pain in RUQ , +murphy sign(review this), fever - Keep pt NPO, provide good oral care - Monitor hydration status - Give pain medications - Can have rupture and sepsis - Avoid high fat intake foods - Promotion of venous return - Edema, problems with venous circulation (ascites): apply antiembolic stockings, elevate the legs, no pillow behind the knees, encourage ROM, frequent repositioning, don't massage a leg may release a clot. - GI (use the slides) - Gastric ulcers - Treated with PPI, cytoprotective drug - Cytoprotective drug: carafate (coats the stomach to protect it) - s/s: low BP - PUD: - Increased risk: NSAIDS, H pylori, smoke, stress - If vomiting blood that is a sign of massive bleeding and is major priority in the patient - How do they diagnose PUD? EGD - Treating H pylori: metronidazole - s/e: headache, nausea, dry mouth, metallic taste in mouth - Acute gastritis - Foods to avoid: citrus, alcohol, NSAIDS, caffeine, spicy foods - Give small frequent meals - Hepatitis - B and C - B risk factors: sharing needles, multiple sex partners, birth to infected mother, avoid sharing razors and toothbrushes, avoid activity with blood exposure, if married the partner needs to be told to discuss safe sex - Hepatitis is a reported disease to CDC, “ABCDE” - Renal - Monitor by BUN and creatinine - Pt with kidney disease what are some drugs that should alert - Nephrotoxic drugs - Gentamycin, NSAID, vancomycin - Hemodialysis - Pt in process of getting dialysis, what do you want to check first before anything else - BP because you are going to be pulling off fluid - If pt comes back with tachycardia, may be bleeding or too much volume was pulled off - n/v during the infusion is a sign that too much has been pulled off - Take BP then go from there - Watch potassium!!! - It will decrease after dialysis - Peritineal dialysis - Encourage pt to take showers and not baths to decrease infection - AB graft - Pain and coldness are NOT normal - Indication of decreased perfusion - Auscultate for bruit and feel for thrill - Erythropoietin - Synthesized in the kidneys - If pt has chronic renal failure anemia it is because there is inadequate erythropoietin - They gie epoietin alfa, and profate - AKI - It's a decrease in systemic circulation that decreased renal blood flow decreased glomerular perfusion - Severe dehydration, decreased CO, and HF - Not caused by nephrotoxic drugs - Causes: severe dehydration that reduces circulation - No obstruction so dont need foley or any procedure to get rid of stones - Review RIFLE stages, depending on the stage - Anuria: 12 hours = insert catheter , give Bicard for metabolic acidosis, strict I&O - Delegation - AP: Daily weights, VS, I&O, reconnect pt to ECG , NGT output - LVN: PO meds, stable diabetic pt post op, reinforce teaching, care for skin around peg tube, document NGT output - Read the question and not into the question - Participation shows in our exam reviews