Pulmonary Hypertension
Pulmonary Hypertension is not a diagnosis. It is a hemodynamic observation.
Updated Hemodynamic Definition of PH
Definitions
Characteristics
Pre-Capillary PH
mPAP >20 mmHg
Pulmonary artery wedge pressure ≤15
mmHg
PVR ≥3 Wood units
Isolated Post-Capillary PH
mPAP >20 mmHg
Pulmonary artery wedge pressure >15
mmHg
PVR <3 Wood units
Combined Pre- and Post-Capillary mPAP >20 mmHg
PH
Pulmonary artery wedge pressure >15
mmHg
PVR ≥3 Wood units
The pulmonary vascular resistance in is one tenth that of the systemic
circulation.
The Right Ventricle can’t generate high pressure
The pulmonary vascular bed can increase its capacitance 4 folds with small
changes in pressure by:
So that the blood flow is directed to the well ventilated alveoli
Content
237
The most critical determinant of resistance is the Radius (r )
More than:
Viscosity (n )
Vessel length ( l )
R=8nl/∏.r4
Pressures in cardiac chambers
Updated classification of pulmonary hypertension (2020)
1.Pulmonary arterial hypertension (PAH).
➢ Idiopathic.
➢ Heritable.
➢ Drug-induced and toxin-induced
➢ Associated with the following:– Connective tissue disease.– Portal
hypertension.– Congenital heart disease.– Schistosomiasis.
➢ PAH long-term responders to calcium channel blockers
Content
238
➢ PAH with overt features of pulmonary veno-occlusive disease/or
pulmonary capillary hemangiomatosis
➢ Persistent PH of the newborn syndrome
2.Pulmonary hypertension due to left heart disease.
►PH due to heart failure with preserved left ventricular ejection fraction.
►PH due to heart failure with reduced left ventricular ejection fraction.
►Valvular heart disease.
►Congenital/acquired cardiovascular conditions leading to postcapillary PH.
3.Pulmonary hypertension due to lung disease and/or hypoxia.
►Obstructive pulmonary diseases.
►Restrictive pulmonary diseases.
►Other lung disease with mixed restrictive/obstructive pattern.
►Hypoxia without lung disease.
►Developmental lung disorders.
4. Pulmonary hypertension due to pulmonary artery obstruction.
►Chronic thromboembolic PH.
►Other pulmonary artery obstructions. – Sarcoma (high or intermediate
grade) or angiosarcoma.– Other malignant tumors (renal, uterine, germ cell
tumor of the testis, other tumors).– Non-malignant tumors (uterine
leiomyoma).– Arteritis without connective tissue disease.– Congenital
pulmonary arteries stenosis.– Parasites (hydatidosis)
5. Pulmonary hypertension with unclear and/or multifactorial mechanisms.
►Hematological disorders: chronic hemolytic anemia and myeloproliferative
disorders.
►Systemic and metabolic disorders: pulmonary Langerhans cell
histiocytosis, Gaucher disease, glycogen storage disease, neurofibromatosis
and sarcoidosis.
Content
239
►Others: fibrosing mediastinitis, chronic renal failure (with/without dialysis),
pulmonary tumorous thrombotic microangiopathy and HIV
Pulmonary arterial hypertension ( precapillary)
Pulmonary venous hypertension ( postcapillary)
Content
240
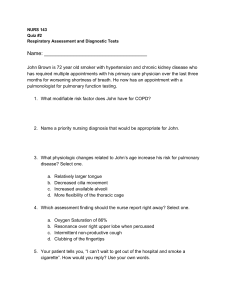
Pathogenesis
1. Pulmonary arterial hypertension
- Whatever the initial cause, it leads to vasoconstriction.
- Over time, the affected blood vessels become both stiffer and thicker,
(fibrosis).
Example:
Idiopathic P A H
Incidence: 1-2/million
Gender: 2.5/1 female/male
Age: median in 40’s
Familial: 6%
Up to 20% abnormal gene in isolated PAH
At least 50% abnormal gene in familial PAH
Vessels show:
Intimal thickening due to endothelial proliferation
Medial thickening and muscularization
Plexiform lesions
2. Pulmonary venous hypertension
There is no obstruction to blood flow in the lungs.
The left heart fails to pumps blood efficiently, leading to pooling of blood in
the lungs. This causes pulmonary edema.
3. Hypoxic pulmonary hypertension
The low levels of oxygen are thought to cause vasoconstriction. This leads to
a similar pathophysiology as pulmonary arterial hypertension.
Pulmonary vascular resistance increases due to :
a-Anatomic factors
• In situ thrombosis
• Destruction of pulmonary vascular beds (emphysema)
Content
241
b- -Functional factors
• Acute and chronic alveolar hypoxia +++
• Acidosis and hypercarbia
• Hypervolemia
• Hyperviscosity
4. Chronic thromboembolic pulmonary hypertension
The blood vessels are blocked or narrowed with blood clots. This leads to a
similar pathophysiology as pulmonary arterial hypertension.
Clinical picture
Symptoms: Because symptoms may develop very gradually, patients may
delay seeing a physician for years.
Common symptoms are shortness of breath, fatigue, non-productive cough,
angina pectoris, fainting or syncope, peripheral edema and rarely hemoptysis .
Pulmonary arterial hypertension (PAH) typically does not present with
orthopnea or paroxysmal nocturnal dyspnea, while pulmonary venous
hypertension typically does.
Signs:
1- Signs of Pulmonary Hypertension
Loud P2
parasternal heave,
RV lift
Systolic murmur (TR)
Diastolic murmur (PR)
RV S4
2- Signs of Right Ventricular Failure
JVD with V wave
RV S3
Hepatomegaly
Edema, ascites
Content
242
Investigations
1- Plain Xrays
2- ECG in Pulmonary Hypertension:
ECG signs are specific but not sensitive for the detection of right
ventricular disease.
Content
243
3- Pulmonary function tests:
Severe restrictive pattern with decreased:
-Mean vital capacity (VC)
-Mean total lung capacity (TLC).
4- Cardiopulmonary exercise test:
6MW distance is strongly predictive of survival:
< 332 meters: 20% 3-year survival
>332 meters: 92% 3-year survival
5- Echocardiography:
Normal or shows right side enlargement and pulmonary hypertension:
Simplified Bernoulli equation P=4V2
6- Right Heart Catheter:
Estimate pulmonary capillary wedge pressure
Content
244
7- Pulmonary angiography:
Shows filling defects in cases with thrombi.
Treatment
1. Pulmonary Arterial Hypertension
• Calcium channel blockers in responders by Swan-Ganz catheter (whose
mean pulmonary artery pressure falls by more than 10 mm Hg, or to less
than 40 mm Hg with an unchanged or increased cardiac output when
challenged with adenosine, epoprostenol, or nitric oxide)
• Prostacyclin derivatives
• Endothelin receptor antagonists
• Phosphodiesterase inhibitors Sildenafil
2. PH with Left Heart Disease
• Diuretics
3. PH with Lung Diseases/Hypoxemia
• Oxygen
• CPAP...
4. PH due to Chronic Thrombotic and/or Embolic Disease
• Pulmonary endarterectomy.
Treatment for hypoxic and miscellaneous varieties of pulmonary hypertension
have not been established.
Content
245
Many physicians will treat these diseases with the same medications as for
PAH.
Surgical
- Atrial septostomy communication between the right and left atria at the
cost of lower oxygen levels in blood
- Lung transplantation cures pulmonary arterial hypertension,
- Pulmonary thromboendarterectomy
Monitoring:
Patients are normally monitored through commonly available tests such as:
Pulse oximetry,
Arterial blood gas tests,
Chest X-rays,
Serial ECG tests,
Serial echocardiography, and
Spirometry or more advanced lung function studies.
Content
246
 0
0