- No category
Dengue Fever Clinical Guidelines: Diagnosis & Management
advertisement
Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ 1 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ DENGUE FEVER Sources: 1. Clinical Practice Guidelines on Dengue in Children, Pediatric Infectious Disease Society of the Philippines In 2009, the World Health Organization (WHO) set up criteria for classifying dengue into levels of severity based on clinical and/or laboratory parameters (WHO 2009). Dengue patients are classified as severe dengue or non-severe dengue, with the group of patients with non-severe dengue subdivided into those with warning signs and those without warning signs. Dengue infection is a systemic and dynamic disease. It has a wide clinical spectrum that includes both severe and non-severe clinical manifestations. After an incubation period of 3 to 14 days, the illness begins abruptly and is followed by the three phases: febrile, critical and recovery. The acute febrile phase of dengue usually lasts 2–7 days, often accompanied by generalized body ache, muscle and joint pains, headache, retro-orbital pain, facial flushing, sore throat, hyperemic pharynx, macular or maculopapular rash, petechiae and mild mucosal membrane bleeding. A positive tourniquet test and progressive decrease in total white cell count are early findings which could differentiate dengue from other acute febrile illnesses. These clinical features are indistinguishable between severe and non-severe dengue cases. During fever defervescence, usually on days 3–7 of illness, an increase in capillary permeability in parallel with increasing hematocrit levels may occur, marking the beginning of the critical phase. The period of clinically significant plasma leakage usually lasts 24–48 hours, followed by a convalescent phase with gradual improvement and stabilization of the hemodynamic status. Warning signs of progression to severe dengue occur in the late febrile phase and include persistent vomiting, severe abdominal pain, mucosal bleeding, difficulty breathing, and early signs of shock. Progressive leukopenia followed by a rapid decrease in platelet count usually precedes plasma leakage. At this point patients with non severe disease begin to improve, but people with clinically significant plasma leakage attributable to increased vascular permeability become worse and develop severe dengue disease with pleural effusion and/or ascites, hypovolemic shock, severe hemorrhage, or organ impairment. Shock occurs when a critical volume of plasma is lost through leakage and is often preceded by warning signs. With prolonged shock, the consequent organ hypoperfusion results in progressive organ impairment, metabolic acidosis and disseminated intravascular coagulation. This in turn leads to severe hemorrhage causing the hematocrit to decrease in severe shock. Severe organ impairment such as severe hepatitis, encephalitis or myocarditis and/or severe bleeding may also develop without obvious plasma leakage or shock. The group progressing from non-severe to severe disease is difficult 2 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ to define, but this is an important concern since appropriate treatment may prevent these patients from developing more severe clinical conditions. Therefore, monitoring for warning signs and other clinical parameters is crucial to recognizing progression to the critical phase. This will enable appropriate treatment with intravenous fluid therapy that may prevent these patients from developing more severe clinical conditions. Question 1: Among patients with confirmed or presumptive diagnosis of dengue in the outpatient setting, what clinical signs and symptoms warrant admission? Recommendation 1: Among patients with confirmed or presumptive diagnosis of dengue in the outpatient setting, patients with the following signs and symptoms should be admitted in a healthcare facility for closer monitoring and observation: • Shortness of breath • Irritability or drowsiness • Pleural effusion • Abdominal pain • Melena • Elevated hematocrit • Decreased or decreasing platelet count These signs and symptoms are strongly associated with more severe Dengue infection. Recommendation 2: Among patients with confirmed or presumptive diagnosis of dengue in the outpatient setting, there is insufficient evidence to say that vomiting is associated with more severe dengue. However, because patients with vomiting cannot tolerate oral rehydration fluids, consider admission. Consideration for recommendation: There is insufficient evidence to recommend which clinical or laboratory findings could accurately predict the development of severe disease and warrant admission. The studies evaluated different clinical and laboratory parameters and had different cut-off points for the laboratory parameters tested. In the draft recommendation presented to the stakeholders' panel, the recommendation for admission to a healthcare facility was platelet count <100,000/mm3. The Department of Health representatives commented that admitting patients with platelet counts <100,000/mm3 in an otherwise well child may result in unnecessary hospital admission of those who may be adequately managed on an outpatient basis. In the absence of published normal values for age of hematocrit among Filipino children, no absolute value for the Hematocrit can be recommended as a cut-off for admission. There is lack of data for hematocrit values for patients with iron deficiency anemia or hematologic disorders who subsequently develop dengue. 3 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ The criteria for admission should take into consideration the overall clinical condition of the child rather than focusing on platelet count or hematocrit values alone. It was emphasized that urine output should be one of the parameters to be evaluated in considering admission. However, there were no studies that evaluated this outcome. Question 2: Among patients with dengue, which risk factors are associated with mortality? Recommendation 1: Patients with dengue who present with any one of the following clinical findings may be at increased risk for mortality. Hypotension on admission Respiratory failure Narrow pulse pressure on admission Liver failure (AST elevation > 200 u and INR > 1.3) DHF stage 3 and 4 (severe dengue) Renal failure (BUN >20 mg% and serum Creatinine >1.0mg%) Significant bleeding including gastrointestinal bleeding Severe plasma leakage in multiple sites (pleural effusion, pericardial effusion and ascites) History of previous dengue Prolonged shock Recommendation 2: The presence of two or more of the following warning signs in patients with dengue may increase the risk for mortality: severe abdominal pain arterial hypotension neurologic manifestation painful hepatomegaly hypovolemic shock liver failure myocarditis Recommendation 3: Patients with dengue who present with one or more of the following laboratory findings may be at increased risk for mortality and warrant hospital admission for close monitoring: Decline in Hgb by ≥20% Thrombocytopenia, with APC < 50,000 Hemoconcentration, with Hct > 40 % or 20% increase in lowest and highest hematocrit Creatinine > 1 mg % AST > 1000 u Acidosis Recommendation 4: Prothrombin time (PT) and Partial Prothrombin Time (PTT) do not differentiate those who may be at increased risk for mortality and are not recommended as routine tests for patients with dengue. 4 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Question 3: Among patients admitted because of dengue, which clinical signs and/or laboratory findings indicate significant bleeding? Recommendation 1: Among patients admitted because of dengue, the presence of one or more of the following clinical or laboratory findings may increase the risk of bleeding: Hypotension Narrow pulse pressure Hepatomegaly Platelet count < 50,000/mm3 WBC count < 5000/mm3 Elevated ALT (> 3x the normal value) Recommendation 2: Among patients admitted because of dengue, there is some evidence to suggest that the following signs and symptoms may be associated with significant bleeding. Vomiting Abdominal pain Restlessness Pleural effusion or ascites Rash Recommendation 3: Prothrombin Time (PT) and Partial Thromboplastin Time (PTT) were not shown to be significantly associated with bleeding and should not be routinely done in patients with dengue. 5 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ FLUID THERAPY FOR DENGUE Maintenance intravenous fluids are commonly used in hospitalized children for maintaining fluid and electrolyte balance and homeostasis. Hypotonic fluids are the most commonly used type of fluids for children admitted in a hospital. Sick children are in a stressed state and secrete antidiuretic hormone (ADH) more than healthy children. This increased ADH secretion leads to water retention by the kidneys which in turn leads to hyponatremia defined as plasma sodium content (pNa < 136 mol/L). Early symptoms of hyponatremia include headache, nausea, and general malaise, progressing to seizures and coma, or even death without appropriate management. In the WHO 2009 guidelines, ambulatory patients are encouraged oral intake of oral rehydration solution, fruit juice and other fluids containing electrolytes and sugar to replace losses from fever and vomiting. Adequate oral fluid intake may reduce the number of hospitalizations. However, fluids containing high sugar or glucose should be avoided because they can exacerbate hyperglycemia of physiological stress from dengue. An ideal physiologic fluid is one that resembles the extracellular and intracellular fluids closely. If the patient develops warning signs but without shock, the recommendation is to give isotonic solutions such as 0.9% Saline or Ringer’s Lactate. Frequent reassessment of the clinical status and hematocrit should be done and fluid infusion rates should be reviewed accordingly. In patients with shock, the current recommendation of WHO is to start intravenous fluid resuscitation with isotonic crystalloid solution, then reassess the patients’ condition (vital signs, capillary refill time, hematocrit, urine output). The subsequent fluid management will depend on the patient’s hemodynamic status. An IVF is classified as isotonic if it approximates the effective osmolality of plasma and as hypotonic if its osmolality is lower than the effective plasma osmolality. The intravenous fluids closely resembling the osmolality of plasma; the most readily available and cheapest are 0.9 % NaCl and Ringer’s lactate solution, which are recommended by the WHO. In patients with dengue, the critical period lasts for 24-48 hours only, and during this time, patients should be frequently monitored until the danger period is over. In patients with hypotensive shock, colloids may be the preferred choice over crystalloids if the blood pressure needs to be restored urgently. However, crystalloids and colloids have their own limitations when used in large quantities. 6 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Question 4: Among Dengue patients without shock how effective are isotonic IVFs compared to hypotonic IVFs in reducing mortality? Recommendation: There is insufficient evidence that the tonicity of the intravenous fluid has an effect on mortality in dengue patients without shock. Isotonic fluids can be used as maintenance for dengue patients without shock. The use of hypotonic IVF is associated with hyponatremia among hospitalized pediatric patients. Question 5: Among Dengue patients with shock, how effective are colloidal IVFs compared to crystalloid IVFs in reducing mortality? Recommendation: In dengue patients with shock, either crystalloids or colloids may be used for fluid resuscitation. There is insufficient evidence to say that the use of colloid IVF compared to crystalloids will affect mortality. The use of colloids may be associated with more adverse reactions (e.g. bleeding, allergic reactions) compared to crystalloids. 7 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ ROLE OF BLOOD PRODUCT TRANSFUSION IN DENGUE Bleeding in dengue may be due to vasculopathy, thrombocytopenia, platelet dysfunction, and deranged coagulation). In some cases, bleeding may result from liver failure. When major bleeding occurs, it is almost always associated with profound shock since this, in combination with thrombocytopenia, hypoxia and acidosis, can lead to multiple organ failure and disseminated intravascular coagulation. Disseminated intravascular coagulation (DIC) leads to severe hemorrhage causing the hematocrit to decrease. A physician should always be on alert to the possibility of concealed bleeding if the patient continues to deteriorate with a serial decrease in the hematocrit in spite of the intravenous fluids. Massive bleeding may also occur without prolonged shock in instances when acetylsalicylic acid (aspirin), ibuprofen or corticosteroids have been taken. Blood products are not routinely used in dengue fever unless there is profuse bleeding or clinical deterioration refractory to vigorous fluid resuscitation. In such cases, blood transfusion is life saving and should be given as soon as severe bleeding is suspected or recognized. The use of red cell products such as fresh whole blood and packed red cells are the components of choice for those with massive bleeding especially those emanating from the gastrointestinal tract and/or vagina in adult females. The practice of platelet concentrate and plasma transfusion for severe bleeding remains controversial and may further exacerbate fluid overload. If hemorrhage persists despite red cell replacements with fresh whole blood or freshpacked cells or if DIC is suspected, some clinicians may consider giving plasma products such as fresh frozen plasma or cryoprecipitate. DIC should be suspected in cases of severe bleeding associated with low or rapid decline in platelet count, prolongation of clotting times, such as the prothrombin time (PT) and activated partial thromboplastin time (aPTT), presence of fibrin-degradation products in plasma, and low levels of fibrinogen and coagulation inhibitors such as antithrombin III. Inappropriate transfusion of platelet and fresh frozen plasma may cause fluid overload. Prophylactic transfusion of plasma products including platelet concentrate in those without signs of bleeding is unnecessary and is strongly discouraged due to the possibility of allergic reactions, transfusion-related acute lung injury, and transmission of other diseases. 8 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Blood Products in Dengue Fever 9 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Question 6: Among patients with thrombocytopenia because of dengue, how effective is prophylactic platelet transfusion in improving platelet count, preventing hemorrhage, and reducing mortality? Recommendation: There is insufficient evidence to say that prophylactic platelet transfusion in patients with minimal or no active bleeding will improve platelet counts, prevent hemorrhage and reduce mortality. Children with dengue who have platelet count <50,000/mm3 with minimal or no active bleeding should not be given prophylactic platelet transfusion. Question 7: Among Dengue patients with significant bleeding, how effective is plasma transfusion in controlling bleeding and reducing mortality? Recommendation: Among dengue patients with significant bleeding, there is insufficient evidence that plasma transfusion has an effect on controlling bleeding and reducing mortality. The effect of plasma transfusion on platelet count recovery is not significant in dengue patients with bleeding. In children exhibiting signs of disseminated intravascular coagulopathy (DIC), plasma transfusion may be considered. Question 8: Among populations at risk for Dengue transmission, how effective are citronella-based repellents compared to DEET-based repellents in reducing the incidence of Dengue? Recommendation: There is insufficient evidence to say that use of citronella-based repellents is more effective than DEET-based repellents in reducing dengue transmission. Recommendations for Fluid Therapy for Compensated Shock and Hypotensive Shock Based on the 2012 PPS Revised Guidelines on Fluid Management of Dengue Fever and Dengue Hemorrhagic Fever 10 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ A. Recommended Fluid Therapy for Compensated Shock 11 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ B. Recommended Fluid Therapy for Hypotensive Shock 12 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Hemodynamic Assessment: Continuum of Hemodynamic Changes 13 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ URINARY TRACT INFECTION Source: 1. Philippine Clinical Practice Guidelines on the Diagnosis and Management of Urinary Tract Infections in Adults 2015 Update ASYMPTOMATIC BACTERIURIA IN ADULTS Recommendations: 1. When is asymptomatic bacteriuria diagnosed? a. All diagnosis of asymptomatic bacteriuria (ASB) should be based on results of urine culture specimens that are collected aseptically and with no evidence of contamination. b. For asymptomatic women, bacteriuria is defined as two consecutive voided urine specimens with isolation of the same bacterial strain in quantitative counts ≥ 100,000 cfu/mL. c. In men, a single, clean-catch voided urine specimen with one bacterial species isolated in a quantitative count ≥ 100,000 cfu/mL identifies bacteriuria. d. In both men and women, a single catheterized urine specimen with one bacterial species isolated in a quantitative count ≥ 100 cfu/mL identifies bacteriuria. 2. What are the indications for screening and treatment of asymptomatic bacteriuria? a. Screening and treatment is recommended in the following to prevent bacteremia and sepsis: Patients who will undergo genitourinary manipulation or instrumentation All pregnant women b. The choice of antibiotic depends on culture results. A seven-day regimen is recommended. c. For specific antibiotic recommendations for ASB in pregnancy * May cause hemolytic anemia, anophthalmia, hypoplastic left heart syndrome, ASD, cleft lip and palate. May be given on the second trimester of pregnancy until 32 weeks AOG. Use in the first trimester of pregnancy is appropriate when no other suitable alternative antibiotics are available. 14 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ 3. Who should NOT be screened and treated for asymptomatic bacteriuria? a. Routine screening and treatment for asymptomatic bacteriuria is not recommended for healthy adults. b. Likewise, periodic screening and treatment for asymptomatic bacteriuria is not recommended in the following: Patients with diabetes mellitus Elderly patients Patients with indwelling catheters Solid organ transplant patients People living with human immunodeficiency virus (HIV) Spinal cord injury patients Patients with urologic abnormalities 4. What is the optimal screening test for asymptomatic bacteriuria? a. Screening by urine culture is recommended. b. In the absence of facilities for urine culture, significant pyuria (>10 wbc/hpf) or a positive gram stain of unspun urine (>2 microorganisms/oif) in two consecutive midstream urine samples can be used to screen for asymptomatic bacteriuria. c. Urine culture and sensitivity testing are not necessary when urinalysis is negative for pyuria or urine gram stain is negative for organisms. d. Pyuria accompanying asymptomatic bacteriuria is not an indication for antimicrobial treatment among patients for whom screening and treatment is not recommended. RECURRENT URINARY TRACT INFECTION IN WOMEN Reccomendations: 1. How is recurrent urinary tract infection (rUTI) diagnosed? a. Recurrent UTI is diagnosed when a healthy non-pregnant woman with no known urinary tract abnormalities has 3 or more episodes of acute uncomplicated cystitis documented by urine culture during a 12-month period OR 2 or more episodes in a 6- month period. b. Recurrent UTI may either be a relapse or a reinfection. Relapse occurs when the initial organism persists within the urinary tract and reemerges despite adequate treatment usually occurring 1-2 weeks after stopping treatment. Reinfection, on the other hand, occurs when recurrent UTI is caused by a different bacterial isolate, or by the previously isolated bacteria after a negative intervening culture or an adequate period (≥ 2 weeks) between infections. 2. Among those with recurrent UTI, who would benefit from further diagnostic evaluation? a. Routine screening for urologic abnormalities is not recommended for the general patient population. b. Screening for urologic abnormalities is recommended in the following situations: No response to appropriate antimicrobial therapy or rapid relapse after such therapy Gross hematuria during a UTI episode or persistent microscopic hematuria Obstructive symptoms Clinical impression of persistent infection 15 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Infection with urea-splitting bacteria (Proteus, Morganella, Providencia) History of pyelonephritis History of or symptoms suggestive of urolithiasis History of childhood UTI Elevated serum creatinine c. Patients with the above factors may benefit from further diagnostic evaluation as these risk factors have been identified to be associated with a higher incidence of urologic abnormalities. d. All women with recurrent UTI should undergo a complete history and physical examination to evaluate urogenital anatomy and estrogenization of vaginal tissues and to detect prolapse. Post-void residual urine should be measured. 3. What diagnostic work-ups are indicated in women with recurrent UTI? a. Radiologic or imaging studies and cystoscopy are not routinely indicated in patients with recurrent UTI. b. Renal ultrasound or CT scan/stonogram may be done to screen for urologic abnormalities. c. Patients with anatomical abnormalities should be referred to a specialist (nephrologist or urologist) for further evaluation 4. When is prophylaxis for recurrent UTI indicated? a. Prophylaxis is recommended in women whose frequency of recurrence is not acceptable to the patient in terms of level of discomfort or interference with activities of daily living. Prophylaxis may be withheld according to patient preference if the frequency of recurrence is tolerable to the patient. b. The following factors should guide the physician in determining the patient’s risk-benefit profile and in deciding which prophylactic strategies will be used: Frequency and pattern of recurrences Patient’s lifestyle, compliance and willingness to commit to a specific regimen Plans for a pregnancy Antimicrobial resistance and susceptibility pattern of the organisms causing the patient’s previous UTIs Risk of adverse events and drug allergies c. Prophylaxis should only be initiated after counseling and behavior modification have been attempted in order to minimize antibiotic exposure and possible adverse effects. d. Antibiotic prophylaxis should be limited to women with recurrent UTI in whom nonantimicrobial strategies have not been effective and who prefer prophylactic antimicrobial therapy. 5. How effective are non-antimicrobial strategies in preventing recurrent UTI? a. Behavioral changes i. Behavioral changes can be useful antimicrobial-sparing measures in the prevention of recurrent UTI. ii. These behavioral measures include the following: post-defecation and anal cleansing antero-posteriorly always in women to avoid contaminating the periurethral area with fecal flora post-coital douche or post coital urination 16 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ liberal fluid intake especially after intercourse avoidance of tight-fitting underwear use of alternative form of contraception for women using spermicide-containing contraceptives b. Biologic mediators Cranberry products: Cranberry juice and cranberry products are not recommended for the prevention of urinary tract infections in populations at risk because there is no consistent evidence as to Recurrent UTI in women the effective amount, concentration and duration of intake of cranberry products. The inconclusive evidence on the effect of cranberry products in the prevention of UTI maybe due to different PACS (proanthocyanidins) used. The recommended dose for UTI prevention is daily consumption of 300 mL of cranberry juice cocktail or 500 mg capsules containing 36 mg PACs) taken twice a day as the anti-adhesion activity decreases over time. Among patients wherein long-term antibiotic prophylaxis for recurrent UTI is deemed necessary, the use of cranberry 500 mg capsules containing 36 mg PAC taken twice a day can be an option to avoid emergence of resistance of fecal and urine isolates of E. coli to trimethoprim, amoxicillin and ciprofloxacin. c. Hormonal treatments in post-menopausal women Application of intravaginal estriol cream once each night for two weeks followed by twice-weekly applications for at least 8 months OR use of an estradiol releasing silicone vaginal ring for 3 months is recommended for the prevention of recurrent UTI in postmenopausal women Data is insufficient to recommend vaginal estrogens over antibiotics for the prevention of recurrent UTI. Low-dose oral estrogen is not recommended for the prevention of recurrent UTI. d. Immunoprophylaxis for recurrent UTI Immunoprophylaxis, using immune-active E. coli fractions, is recommended for the prevention of recurrent UTI. The dosing regimen is once daily per orem for 3 months. A longer/extended dosing regimen (once daily for 3 months, rest for 3 months, 10 days per month for 3 months, and rest for 3 months) may be associated with a better control of recurrence in the longer term. 6. How effective are antibiotic prophylactic regimens in preventing recurrent UTI? a. Prophylaxis is recommended in women whose frequency of recurrence is not acceptable to the patient in terms of level of discomfort or interference with activities of daily living. Prophylaxis may be withheld if the frequency of recurrence is tolerable to the patient. b. If a decision is made to give antibiotic prophylaxis, either of the following is recommended: Continuous prophylaxis, defined as the daily intake of a low-dose of antibiotic for 612 months OR Post-coital prophylaxis, defined as the intake of a single dose of antibiotic immediately after sexual intercourse OR 17 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Intermittent prophylaxis, defined as self-treatment with a single antibiotic dose based on patient’s perceived need. c. Any of the antibiotics in the Table given either continuously for 6 to 12 months or as postcoital prophylaxis can reduce the clinical and microbiologic recurrence of UTI episodes 7. How should individual episodes of UTI be treated in Antibiotics proven effective in reducing the number women with recurrent UTI? of recurrences of UTI a. Any of the antibiotics for acute uncomplicated cystitis (table below) may be used in the treatment of individual episodes of UTI in women with recurrent UTI. Antibiotics for acute uncomplicated cystitis b. Consider intermittent self-administered therapy in highly educated, well-informed, motivated patients, wherein the patients are able to recognize the characteristic signs and symptoms of UTI, are compliant with medical instructions and have a good relationship with a medical provider. 18 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ c. Breakthrough infections during prophylaxis should be treated empirically with any of the antibiotics recommended for uncomplicated cystitis other than the antibiotic being given for prophylaxis. Request for a urine culture and modify the treatment accordingly. 8. How effective are non-pharmacologic interventions treating urinary tract infections? a. Cranberry juice and cranberry products are not recommended for the treatment of urinary tract infection. b. There is evidence to recommend acupuncture for prevention of recurrent UTI among women when antibiotic prophylaxis is contraindicated. c. There is no available evidence to recommend coconut juice in the prevention or treatment of UTI. d. There is insufficient evidence to recommend oral water hydration (2 to 2.5 liters/day) in the prevention or treatment of UTI. e. There is insufficient evidence to recommend drinking more water and voiding before and after intercourse to prevent UTI. COMPLICATED URINARY TRACT INFECTIONS: GENERAL CONSIDERATIONS Reccomendations: 1. When is complicated urinary tract infection suspected or diagnosed? a. Complicated UTI (cUTI) is significant bacteriuria plus clinical symptoms, which occurs in the setting of (1) functional or anatomic abnormalities of the urinary tract or kidneys, or (2) the presence of an underlying disease that interferes with host defense mechanisms, (3) any condition that increases the risk of acquiring [persistent] infection and/or treatment failure. The cut-off for significant bacteriuria in complicated UTI has been set at 100,000 CFU/mL. However, in certain clinical situations, such as in catheterized patients, lowlevel bacteriuria or counts < 100,000 CFU/mL maybe significant. 2. In patients with suspected complicated UTI, what diagnostic tests should be done to assist the physician in managing the infection effectively? a. A urine sample for gram stain, and culture and sensitivity testing must always be obtained before the initiation of any treatment. b. Additional ancillary diagnostic tests will depend on the nature of the complicated UTI Imaging of the urinary tract is warranted whenever anatomic or structural abnormalities are suspected as contributing to a UTI. Such cases would include (a) pyelonephritis that is not responding to usual treatment, (b) severe pyelonephritis in certain high risk groups (e.g. DM), and (c) recurrent UTI in a man. c. CT-scan is generally preferred over KUB ultrasound as it can better identify and localize the presence of urinary tract abnormalities or multiple lesions such as abscesses; however, the imaging modality to be used may depend on local availability. 3. Do patients with complicated UTI need to be hospitalized? a. The following patients with complicated UTI require hospitalization: i. Patients with marked debility and signs of sepsis ii. Patients in whom there is uncertainty in diagnosis 19 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ iii. Patients in whom there is concern about adherence to treatment, iv. Patients who are unable to maintain oral hydration or take oral medications b. Patients with mild to moderate illness (symptoms of fever and lower or upper UTI without urosepsis, circulatory failure and/or organ dysfunction or failure), and who do not fall under the above categories may be treated on an outpatient basis. 4. What antibiotics are recommended for empiric therapy of complicated UTI? a. For mild to moderate illness, oral fluoroquinolones or amoxicillin/clavulanic acid may be used if there are no risk factors for infection with antibiotic resistant organisms and if the resistance rates to these antibiotics are < 20%. Due to the varying antibiotic sensitivity patterns of the most common uropathogens, it is recommended that local antibiotic sensitivity patterns be considered in the choice of empiric antibiotics for this set of patients. b. For severely ill patients, broad-spectrum parenteral antibiotics (see Table 3) should be used, choice of which would depend on the following: i. The expected pathogens ii. Results of the urine gram stain iii. The current susceptibility patterns of microorganisms in the area iv. Risk factors for the acquisition of drug-resistant organism c. Fluoroquinolones are not recommended as empiric antibiotics for severely-ill patients due to the high rates of resistance locally. d. Any underlying abnormalities or risk factors should be managed accordingly. 5. How long should antibiotics be given in complicated UTI? a. In general, at least 7-14 days of therapy is recommended. Treatment duration may be extended depending on the clinical situation. b. Antibiotics are modified according to the results of the urine culture and sensitivity tests. Patients started with parenteral regimen may be switched to oral therapy upon clinical improvement. c. When an oral regimen is not available or if continuation of an intravenouslyadministered antibiotic is necessary, outpatient parenteral antibiotic therapy (OPAT) can be an option. d. Criteria for OPAT include: i. An indication for parenteral antibiotic therapy (i.e. presence of an infection that warrants antibiotic use) in the absence of an oral or alternate routes of delivery ii. No other clinical indication for hospitalization iii. Consent of the patient and/or caregiver to participate (including an understanding of the benefits, risks, and economic considerations involved) iv. Outpatient environment safe and adequate to support care (including logistic concerns, rapid and reliable communications between the OPAT team) 6. After the completion of antibiotics, what tests or procedures are recommended to reduce the risk of recurrence of complicated UTI? a. Urine culture should be repeated one to two weeks after completion of antibiotics. b. If significant bacteriuria persists post-treatment, consider referral to specialists (infectious diseases, nephrology, urology, etc.) to identify and correct any underlying 20 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ problem (anatomical, functional, or metabolic) that predisposes the patient to complicated UTI. Conditions that define complicated UTI 21 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Pathogens in Complicated UTI 22 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Antibiotic that may be used as empiric therapy for complicated UTI Oral Regimen Ciprofloxacin 500 -750 mg BID or 1000 mg extended release tablet OD x 7-14d* Norfloxacin 400 mg BID x 7-14d* Ofloxacin 200 mg BID x 10-14d* Levofloxacin 500-750 mg OD x 7-14d* Amoxicillin/clavulanate 500 mg/125mg TID or 875 mg/125 mg BID x 7-14d Parenteral Regimen Amikacin 15mg/kg q24h+ Doripenem 500 mg q8h Ertapenem 1 gm. q24h Gentamicin 3-5 mg/kg/day q24h+ Imipenem-cilastin 250-500 mg q6-8h Meropenem 1g q8h Piperacillin-Tazobactam 2.25-4.5 gms q6-8h *Determine if patient has risk factors for drug-resistance prior to use. +Monitor kidney function especially for patients with impaired renal function at baseline SPECIFIC ISSUES OF CONCERN IN COMPLICATED URINARY TRACT INFECTION UTI IN DIABETIC PATIENTS Reccomendations: 1. How should UTI in diabetic patients be managed? a. Diabetic patients require pre-treatment urine gram stain and culture and a posttreatment urine culture. At least 7-14 days of oral or parenteral antibiotics b. Diabetic patients who present with signs of sepsis should be hospitalized. Blood culture, in addition to urine culture, is indicated for severely ill patients before starting therapy. Failure to respond to empiric therapy within 48 to 72 hours warrants a plain abdominal radiograph of the KUB, a renal ultrasound, or a CT-scan. 2. Should diabetic patients be screened and treated for asymptomatic bacteriuria? a. Screening and treatment for asymptomatic bacteriuria among diabetic patients are not recommended because they do not reduce the occurrence of subsequent infectious complications. CATHETER-ASSOCIATED URINARY TRACT INFECTION (UTI) Recommendations: 1. UTI in patients with an indwelling urethral or suprapubic catheter or in those undergoing intermittent catheterization is termed as CAUTI. CA-UTI is diagnosed when: Fever and/or other signs or symptoms compatible with UTI are present with no other identified source of infection At least 103 colony forming units (cfu)/mL of at least 1 bacterial species are present in a single catheter urine specimen or in a midstream voided urine specimen In a patient with an indwelling urethral, suprapubic or condom catheter, or which has been removed within the previous 48 hours. 23 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ 2. Should patients with indwelling urethral, indwelling suprapubic, or intermittent catheterization be screened and treated for asymptomatic bacteriuria? a. Screening and treatment of catheter-associated asymptomatic bacteriuria (CA-ASB) are not routinely recommended. b. Screening and treatment of CA-ASB are recommended only for pregnant patients and those who will undergo urologic procedures. c. Data is insufficient to make any recommendations regarding screening and treatment of CA-ASB among post-solid organ transplant and neutropenic patients. 3. In patients with suspected CA-UTI, what diagnostic tests should be done to assist the physician in managing the infection effectively? a. Similar with the general recommendations in complicated UTI (cUTI), it is necessary to obtain urine gram stain and cultures BEFORE starting empiric antibiotic coverage for CA-UTI. b. In catheterized patients, pyuria alone is NOT diagnostic of CA-UTI and should not be interpreted as an absolute indication for initiating empiric antibiotics. c. The presence or absence of odorous or cloudy urine alone in catheterized patients is also not an indication for antibiotic treatment. 4. How should urine for culture and sensitivity studies be collected from patients with suspected CA-UTI? a. For patients in whom catheterization is still indicated, the urine specimen should be obtained from the freshly placed catheter prior to the initiation of antimicrobial therapy. Urine sample should be aspirated from the catheter port, or if not present, by puncturing at the distal end of the catheter with a sterile needle and syringe after disinfecting the area WITHOUT disconnecting the junction of the catheter and drainage tube b. For individuals whose catheters can be or have been recently removed and requires no further catheterization, a mid-stream, clean catch urine should be obtained. Urine samples for culture should not be obtained from collection bags. c. Urine specimens for culture should be processed as soon as possible, preferably within one hour of obtaining the specimen. If this is not possible, the urine specimen should be refrigerated. Refrigerated specimens should be processed within 24 hours. 24 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ ACUTE INFECTIOUS DIARRHEA Sources: 1. ACG clinical guideline: diagnosis, treatment and prevention of acute diarrheal infections in adults. 2. WHO. Integrated management of childhoold illness: distance learning course. Module 4: Diarrhoea. 3. www.psmid.org/wp-content/uploads/2022/07/CPG-acute-infectious-diarrhea_pocket-guide_v2 DIAGNOSTIC I. II. III. When is the diagnosis of acute infectious diarrhea suspected? a. Definitions Acute infectious diarrhea is suspected if a patient present with passage of 3 or more loose, watery or bloody stools within 24 hours that may be accompanied by any of the following symptoms: nausea, vomiting, abdominal pain, and fever. b. Acute diarrhea is the passage of three or more loose, watery or bloody stools from an immunocompetent person’s normal baseline in a 24-hour period lasting less than 14 days. The patient should not have received any antibiotics within the last three months, has had no previous hospitalizations and/or has not developed diarrhea after more than 48 hours of hospital admission. In considering if a patient has diarrhea, the change from the previous consistency of stool is the more important parameter to observe compared to change in frequency. According to the WHO, a young infant has diarrhea if the stools have changed from the usual pattern. What pre-treatment clinical evaluations are recommended for immunocompetent patients presenting with acute infectious diarrhea? a. Extensive clinical history should include consumption of raw, ill-prepared, or rotten food and/or intake of contaminated food and/or water as this could provide clues to the possible etiologies. b. Complete physical examination should be done to assess the severity of the disease, degree of dehydration presence of complication and presence of comorbid condition. What is the clinical utility of diagnostic tests in children and adults with acute infectious diarrhea? a. Diagnostic tests should be based on the assessment of the patient’s clinical status. b. Routine stool examination should not be done in most cases of acute watery diarrhea except in cases where parasitism is suspected or in the presence of bloody diarrhea. c. Stool cultures are indicated only for: severe cases (significant dehydration, high fever, persistent vomiting or severe abdominal pain, dysenteric stool), high risk for transmission of enteric pathogens (food handlers), increased risk of complications, for epidemiologic purposes, where there is suspicion of an outbreak that is enteric in origin. The yield is highest when requested within 3 days of symptoms and before administration of antibiotics d. There is insufficient evidence to support the use of biomarkers (CRP, calprotectin, ESR, PCT, total serum WBC) in distinguishing the cause of acute infectious diarrhea. 25 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ e. Rapid diagnostic tests may be used during suspected outbreaks of diarrhea and shigella, but confirmation with stool culture is still recommended IV. What are the clinical parameters that would indicate presence of dehydration in children with acute infectious diarrhea? a. Physical examination findings indicative of hydration status include the following: vital signs (tachycardia, tachypnea), level of consciousness (depressed sensorium), presence of depressed fontanel, presence of sunken eyeballs, presence of tears, skin turgor, capillary refill time, abnormal respiratory pattern, and history of urine output. V. What are the clinical parameters that would indicate presence of dehydration in adults with acute infectious diarrhea? a. Clinical and laboratory parameters indicative of hydration status include the following: Clinical parameters: fatigue, thirst, sunken eyes, orthostatic hypotension, increased respiratory rate, cold, clammy sin, lethargy, dry oral mucosa, muscle weakness, decreased skin turgor (>2 seconds) Laboratory parameters: Increased urine specific gravity (≥1.010), increased urine osmolality (>800msom/kg), increased serum osmolality (≥ 295 msom/kg), increased BUN/creatinine ration (>20 mg/dL), metabolic acidosis (pH < 22). 26 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ VI. What laboratory test should be done to assess for the presence of complications with acute infectious diarrhea? a. Complications such as acute kidney injury and electrolyte imbalances can occur in pediatric and adult patients with acute infectious diarrhea. For patients suspected to have complications of acute infectious diarrhea, the following laboratory tests may be requested: complete blood count, urinalysis, serum electrolytes (Na, K, Cl), BUN and creatinine, serum bicarbonate or total CO2 if available or ABG 27 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ TREATMENT: CHILDREN A. Who should be admitted among children presenting with acute infectious diarrhea? Children with acute infectious diarrhea with any of the following clinical history and physical findings should be admitted: o Based on clinical history: unable to tolerate fluids, suspected electrolyte abnormalities, conditions for a safe follow-up and home management are not met. o Based on physical findings: altered consciousness, abdominal distention, respiratory distress, hypothermia (temperature <36C) Pediatric patients with acute infectious diarrhea with the following co-existing medical conditions should be admitted: presence of co-existing infection/s (such as pneumonia, meningitis/encephalitis, sepsis), moderate to severe malnutrition, suspected surgical condition. B. What is the recommended management for dehydration among children with acute infectious gastroenteritis? For breastfed infants, breastfeeding should be continued in addition to hydration therapy. Sports, carbonated, caffeinated and sweetened drinks are not recommended. Frequency of monitoring: o Check the child from time to time during rehydration to ensure ORS is being taken satisfactorily and that signs of dehydration are not worsening. Evaluate status of hydration at least hourly C. What are the indications for empiric antibiotic treatment in children with acute infectious diarrhea? Primary management in acute infectious diarrhea in children is still rehydration therapy. Routine empiric antibiotic therapy is NOT recommended. Antimicrobials may be recommended for the following conditions: suspected cases of cholera, cases of bloody diarrhea and diarrhea associated with other acute infections (e.g. pneumonia, meningitis, etc.) 28 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ 29 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ 30 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ D. What are the recommended antimicrobials for the following etiologies of acute infectious diarrhea in children? E. What non-specific medications may be given in children with acute infectious gastroenteritis? Zinc supplementation (20mg/day for 10-14 days) should be given routinely as adjunctive therapy for acute infectious diarrhea in children more than 6 months old. Zinc supplementation is NOT routinely given as adjunctive therapy for acute infectious diarrhea in children less than 6 months old. Racecadotril (1.5 mg/kg/dose) 3 times a day during the first 3 days of watery diarrhea may be given to infants and children as adjunctive therapy to shorten duration of diarrhea. Loperamide is NOT recommended for children with acute infectious gastroenteritis due to serious adverse events. F. What is the role of anti-emetics in the management of vomiting in children with acute infectious diarrhea? Anti-emetics are NOT recommended in children presenting with vomiting with acute infectious diarrhea due to safety issues. G. What is the role of probiotics in the management of acute infectious diarrhea in children? Probiotics are recommended as an adjunct therapy in children throughout the duration of the diarrhea in children. Probiotics have been shown to reduce symptom severity and duration of diarrhea. Probiotics may be extended for 7 more days after completion of antibiotics. H. What is the recommended diet for children with acute infectious diarrhea? Breastfeeding should be continued in breastfed infants. 31 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ I. In general, feeding should be continued. However, if feeding is not tolerated, early refeeding may be started as soon as the child is able. Resumption of age-appropriate usual diet is recommended during or immediately after rehydration process is completed. If diarrhea persists for more than 7 days, or for patients being treated in the hospital due to severe diarrhea, lactose free diet may be given to children who are predominantly bottle-fed to reduce treatment failure and decrease the duration of diarrhea. No change in diet is recommended. Diluted lactose milk is NOT recommended. What is the recommended management for complications of acute infectious diarrhea in children? Acute kidney injury is a serious and potentially life-threatening complication therefore it is best to refer the patient immediately to a specialist at the first sign of AKI. ORS is safe and effective therapy for nearly all children with hyponatremia. Hospital treatment and close monitoring is recommended for patients suspected to have hyponatremia. Referral to specialist is advised. TREATMENT: ADULT Who should be admitted among adults presenting with acute infectious diarrhea? The following adult patients with the following clinical history and physical findings should be admitted: • Poor tolerance to oral rehydration •Moderate to severe dehydration • Acute kidney injury and/or electrolyte abnormalities • Unstable comorbid conditions (e.g. uncontrolled diabetes, congestive heart failure, unstable coronary artery disease, chronic kidney disease, chronic liver disease, immunocompromised conditions) • Frail, elderly (60 years old and above) and/or with poor nutritional status • Patients with unique social circumstances (living alone, with residence far from a hospital) What is the recommended management for dehydration in adults? 32 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Sports drinks and soda are not recommended to replace losses. The use of actual/estimated body weight for maintenance fluid rate calculations and ideal body weight for overweight or obese patients is suggested. Patients who are elderly and those at risk of fluid overload (patients with heart failure, kidney disease) should be referred to a specialist for a more individualized fluid management. Recommendations for type of fluid: − The use of Plain Lactated Ringer’s Solution (chloride – restrictive IVF) as fluid of choice in the hydration and fluid resuscitation of dehydrated patients caused by gastroenteritis isrecommended. However, if Plain Lactated Ringer’s Solution is not available, Plain Normal Saline Solution may still be used. During the initial resuscitation, hourly monitoring of the vital signs, mental status, peripheral perfusion, and urine output must be done. Subsequent frequency of monitoring will be based on the judgment of the clinician. The routine use of albumin, HES, or dextran and gelatins as fluids for resuscitation of dehydrated patients is not recommended. 33 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Algorithm for fluid resuscitation in adult patient Algorithm for maintenance and replacement therapy What are the indications for empiric antimicrobial treatment in adults with acute infectious diarrhea? Empiric antimicrobial treatment is NOT recommended for acute diarrhea with the following clinical features: mild to moderate dehydration only, non-bloody stools, symptoms less than 3 days. 34 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Empiric antimicrobial treatment is recommended for patients with acute diarrhea with moderate to severe dehydration plus any of the following clinical features: fever alone, fever and bloody stools, symptoms persisting for more than 3. The following antimicrobials are recommended for empiric treatment of acute infectious diarrhea: o Azithromycin 1g single dose OR o Ciprofloxacin 500 mg twice daily for 3-5 days o Once suspected organism is confirmed, antimicrobial therapy may be modified accordingly What are the recommended antimicrobials for the following etiologies of acute infectious diarrhea in adults? What non-specific medications may be given in adults with acute infectious diarrhea? Loperamide is NOT recommended in adults with acute infectious diarrhea. Racecadotril (100 mg three times a day) may be given to decrease the frequency and duration of diarrhea hat is the role of probiotics in the treatment of acute diarrhea among adults? There is insufficient evidence to recommend probiotics in adults. What is the recommended management for complications of acute infectious diarrhea in adults? Acute kidney injury is a serious and potentially life-threatening complication therefore it is best to refer the patient immediately to a specialist at the first sign of AKI. 35 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Hospital treatment and close monitoring is recommended for patients with severe hyponatremia/hypernatremia and/or symptomatic patients regardless of degree of sodium imbalance. Approach to therapy depends on the risk stratification. Referral to specialist is advised. Hospital treatment and close monitoring is recommended for patients with severe hypo/hypkalemia and/or symptomatic patients regardless of degree of potassium imbalance. Referral to specialist is advised. PREVENTION A. What interventions are effective in the prevention of acute infectious diarrhea? Hand hygiene o The promotion of hand hygiene in all settings, on all occasions is recommended to reduce transmission of causes of acute infectious diarrhea. o Handwashing with soap and water is the best method to reduce the number of microbes. o If soap and water are not available, alcohol based hand sanitizers (at least 60%) may be used. Hand sanitizers and moist hand wipes or towelletes are not recommended when hands are visible dirty or greasy. o All efforts should be made to provide access to clean water, soap and hand drying materials. Water safety Interventions o Drinking water should be clean and safe. Measures recommended in providing clean and safe water include boiling, chemical disinfection, ultraviolet and filtration. o Any drinking water should comply with the Philippine National Standards for Drinking water. Proper food handling o There is no specific recommended screening test for food handlers in the Philippines o No person shall be employed in any food establishment without a health certificate issued by the city/municipal health officer based on the “Implementing Rules and Regulations of Chapter III Food Establishments On The Code on Sanitation Of the Philippines (P.D. 856)”. o Food industry workers need to notify their employers if with any of the following: Hepatitis A, diarrhea, vomiting, fever, sore throat, skin rash and other skin lesions, discharge from ears, eyes or nose. Proper Excreta Disposal per Excreta Disposal Combination of safe stool disposal and hand hygiene are key behaviors to prevent infectious diarrhea. Per DOH recommendation, the following are the approved excreta disposal facilities : o Flush toilet connected to: community sewer, imhoff tank, septic tank, digester tank, chemical tank 36 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ o o Pit privy: VIP latrine, Pit type and “antipolo” toilet − Any disposal device approved by the Secretary of health or his duly authorized representative. Open defecation is not recommended. Vaccines o To prevent acute infectious diarrhea caused by cholera. o Universal immunization of infants against rotavirus is recommended. Rotavirus vaccines are effective in preventing rotavirus diarrhea and rotavirus diarrhea-associated hospitalization. Supplements o The following probiotics may be given to children and adult to prevent occurrence of acute infectious diarrhea: − Bifidocaterium lactis − Lactobacillus rhamnosus GG − Lactobacillus reuteri o Zinc supplementation is recommended to prevent acute infectious diarrhea for 6 months to 12 years old. o Vitamin A supplementation may be given to children (6 months and above) to prevent incidence of acute infectious diarrhea. The recommended doses are 100,000 IU every 4-6 months for infants 6-12 months − 200,000 IU every 4-6 months for children over 12 months old Breastfeeding o Exclusive breastfeeding is recommended during the first 6 months of life to prevent diarrhea. o All healthcare providers should promote breastfeeding OUTBREAK Outbreak detection and management A. Outbreak is suspected in the following scenarios: o “Cases of acute infectious diarrhea in excess of what would normally be expected in a defined community, geographical area or season lasting a few days or weeks or for several years”(World Health Organization) B. “A single case of communicable disease that has been absent from a population, or caused by an agent not previously recognized in the community, or the emergence of a previously known disease”(Center for Disease Control) C. Suspected cases of outbreaks should be reported immediately to disease reporting unit or disease surveillance coordinators. D. Collection of demographic data and specimen is mandatory. Stool samples via rectal swab or bulk stool should be sent to designated laboratories for analysis and confirmation. Water and food samples may also be collected, to determine the source of outbreak. E. Response to outbreak should involve epidemiologic investigation and formation of hypotheses, treatment of cases, implementation of control and prevention measures, and risk communication 37 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ HYPERTENSION Source: 1. www.philippinesocietyofhypertension.org.ph/ClinicalPracticeGuidelines RECOMMENDATIONS: DIAGNOSIS AND MANAGEMENT OF HYPERTENSION IN ADULT POPULATION Clinical Question 1. Among adult Filipinos, what is the definition of hypertension? A. Hypertension is defined as an office blood pressure (BP) of 140/90 mm Hg or above, typically at least twice taken on 2 separate days. B. It is recommended that office BP be classified as Normal, Borderline, Hypertension. C. Out of office BP measurements are recommended to confirm the diagnosis of hypertension, with ambulatory blood pressure monitoring (ABPM) as the preferred method, and home blood pressure monitoring (HBPM) as an acceptable alternative. Clinical Question 2. Among adult Filipinos, what device is recommended for accurate blood pressure determination and monitoring? A. A properly validated automated oscillometric sphygmomanometer (digital device) is recommended for in office or out of office use. B. The aneroid sphygmomanometer (manual device) may be used in office or out of office provided the examiner is efficient and well trained, and the device is periodically checked according to standard maintenance procedures. C. The aneroid sphygmomanometer is recommended for special cases like the presence of arrhythmias or extremes in BP levels 38 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Clinical Question 3. Among adult Filipinos, what are the blood pressure thresholds for treatment and BP targets for the prevention of cardiovascular disease? A. A therapeutic threshold of 140/90 mmHg to achieve a goal of less than 130/80 is recommended for most adults with hypertension. B. For the very elderly, defined as 80 years old and above, a therapeutic threshold of 150/90 mm Hg to achieve a goal BP of less than 140/90 mm Hg is recommended. Clinical Question 4. Among Filipinos with hypertension, what are the general treatment recommendations? Clinical Question 4.1. What non-pharmacologic approaches are recommended for persons with hypertension? A. Lifestyle modification remains the cornerstone for the management of hypertension. Robust clinical trial evidence has shown that it can prevent or delay the onset of high blood pressure and can reduce cardiovascular risk. Healthy lifestyle choices are the first line of antihypertensive treatment and of course are synergistic to the effects of antihypertensive medications. Lifestyle modifications should include the following: a. Sodium restriction to as low as 1500 mg/day. The American Heart Association recommends that sodium intake be limited to 2300 mg/d (about roughly half a teaspoon of table salt) in most healthy individuals and 1500 mg/d in people with prehypertension or hypertension. b. Dietary Approaches to Stop Hypertension (DASH) meal plan which is low in sodium and high in dietary potassium, can be recommended for all patients with hypertension without renal insufficiency. The DASH diet is rich in fruits, vegetables, low-fat dairy, fish, whole grains, fiber, potassium, and other minerals at recommended levels and low in red and processed meat, sugar sweetened foods and drinks, saturated fat, cholesterol, and sodium. c. Aerobic physical activity and (dynamic) resistance exercises. d. Abstinence from alcohol or moderate alcohol intake. e. Significant weight loss of > 5% of the baseline weight for those who are overweight or obese. f. Smoking cessation Clinical Question 4.2. What are the preferred drugs for the treatment of hypertension among adult Filipinos for prevention of cardiovascular diseases? A. Among persons with uncomplicated hypertension, angiotensin-converting enzyme (ACE) inhibitors or angiotensin-receptor blockers (ARBs), calcium channel blockers, thiazide/thiazide-like diuretics are all suitable first-line antihypertensive drugs, either as monotherapy or combination. B. Ideal combination therapy includes renin-angiotensin-system (RAS) blocker with calcium channel-blocker (CCB) or thiazide/thiazide-like diuretics. Other combinations of the five major classes may also be used in patients with compelling indications for the use of specific drug classes. C. ACE inhibitors & ARBs are not recommended to be used in combination. Likewise, combinations of ACE-I or ARBs with direct renin inhibitors should not be used. 39 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ D. The use of free combinations is recommended if single-pill combination therapy is not available or not affordable. E. Beta blockers are suitable as initial therapy in hypertensive patients with coronary artery disease, acute coronary syndrome, high sympathetic drive and pregnant women. Beta blockers for those with congestive heart failure was specified to be bisoprolol, carvedilol, metoprolol succinate or nebivolol. F. Among patients with BP >150/100 mm Hg (or >160/100 mm Hg in the elderly), a combination of 2 agents, preferably combination of a RAAS inhibitor (ARB/ACE-is) and CCB or diuretic, should be given initially since it is unlikely that any single agent would be sufficient to achieve the BP target. MANAGEMENT OF HYPERTENSION AMONG PERSONS WITH DIABETES 40 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Clinical Question 5. Among persons with diabetes, what is the threshold for treatment of elevated blood pressure? A. Among persons with diabetes and hypertension, it is recommended that drug therapy (along with lifestyle change) be initiated at a blood pressure of > 140/90 mm Hg. Clinical Question 6: Among persons with diabetes and hypertension, what nonpharmacologic therapy is recommended? A. The general advice for non-pharmacologic therapy for hypertension among persons with diabetes is similar to the general population. Additionally, screening for obstructive sleep apnea may be worthwhile as randomized studies of people with diabetes have shown that treatment of OSA (by Continuous Positive Airway Pressure or CPAP) reduces blood pressure. Clinical Question 7. Among persons with diabetes and hypertension, what are the blood pressure targets for prevention of cardiovascular diseases (mortality and morbidity)? A. A blood pressure target of <130/80 mm Hg is recommended for most persons with diabetes mellitus and hypertension; however, do not lower down the blood pressure below 120/70 due to an increased risk for adverse events. Clinical Question 8. Among persons with diabetes, what are the preferred drugs for the treatment of hypertension? A. It is recommended to initiate treatment with a low-dose combination of a RAAS blocker (ACEI or ARB) with a CCB or thiazide/thiazide-like diuretic, preferably using a single- pill combination (SPC). Free tablet combinations may also be given if SPCs are not available. B. The combination of ACE and ARB is not recommended due to a higher risk of hyperkalemia and renal failure. MANAGEMENT OF HYPERTENSION IN PERSONS WITH CHRONIC KIDNEY DISEASE Clinical Question 9. Among patients with CKD who are pre-dialysis, what is the level of blood pressure to start pharmacotherapy to prevent cardiovascular complications and renal progression? A. Patients with BP more than or equal to 140/90 mmHg should have prompt initiation and timely titration of pharmacotherapy to achieve blood pressure goals. Patients with BP more than or equal to 140/90 mmHg should have prompt initiation and timely titration of pharmacotherapy to achieve blood pressure goals. A. For routine office blood pressure measurement, maintain a BP target consistently less than 140 mmHg systolic and less than 90 mmHg diastolic in patients with low risk of cardiovascular disease and CKD grade 4 and 5, or if with adverse effect on intensive target of less than 130/80 41 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ mmHg. CKD patients with high cardiovascular risk or CKD grade 3 or earlier is recommended to have a blood pressure target of less than less than 130/80 mmHg. B. A systolic BP of less than 120 mmHg using a standardized office BP measurement is targeted, when tolerated, among adults with high BP and non-dialysis CKD (ND-CKD). An individualized treatment target is recommended for the following patient populations: a. Diabetic Kidney Disease patients b. CKD grade 4 and 5ND patients c. patients with proteinuria of more than 1 g/day d. individuals with baseline SBP of 120 to 129 mmHg e. those with very low diastolic BP of less than 50 mmHg with CAD f. those with white coat or severe hypertension g. stroke patients h. those with age less than 50 with low absolute risk for CV disease or those individuals above 90 years of age i. very frail patients j. those with limited life expectancy k. those with symptomatic postural hypotension. For these patient populations, a specialist referral is suggested. C. . If unable to obtain a standardized BP measure, maintain a blood pressure target consistently less than or equal to 130 mmHg systolic and less than or equal to 80 mmHg diastolic in patients with urine albumin excretion of more than 30 mg per 24 hours unless adverse event occurs with achievement of this target. Clinical Question 11. Among patients with CKD, what is the level of blood pressure to start initiation with two antihypertensive drugs to prevent cardiovascular complications and renal progression? A. Patients with confirmed office-based blood pressure or more than or equal to 160/100 mmHg should, in addition to lifestyle modification, have prompt initiation and timely titration of two drugs or a single-pill combination of drugs demonstrated to reduce cardiovascular events. A two-drug combination should consider these mechanisms in the choice of anti-hypertensives: calcium channel blockers and diuretics to address volume dependent type of hypertension, and ACE, ARB and beta blockers for the renin dependent type. Clinical Question 12. Among patients with CKD, what is the anti-hypertensive of choice to prevent cardiovascular complications and renal progression? A. Treatment for hypertension should include drug classes demonstrated to reduce cardiovascular events in patients with CKD such as ACE inhibitors, Angiotensin Receptor Blockers, Thiazide-like diuretics, and dihydropyridine calcium channel blockers. 42 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Clinical Question 13. Among patients with CKD with albuminuria/proteinuria, what is the antihypertensive of choice to prevent cardiovascular complications and renal progression? A. An ACE inhibitor or Angiotensin receptor blocker, at maximally tolerated dose is the recommended first-line treatment for hypertension in CKD patients with urinary albumin-to creatinine ratio more than or equal to 30 mg/g (or equivalent). If one class is not tolerated, the other is substituted. These medications should not be discontinued unless serum creatinine level rise above 30 % over baseline during the first two months of treatment or hyperkalemia (serum potassium level > or = 5.6 mmol/L). If the patient is intolerant to both ACE inhibitor and angiotensin receptor blocker, a non-dihydropyridine calcium channel blocker (verapamil or diltiazem) may be used as first line treatment in this setting. B. Combinations of ACE inhibitor and Angiotensin receptor blocker and of ACE inhibitors or angiotensin receptor blockers with direct renin inhibitors should not be used. Clinical Question 14. Among patients with CKD with resistant hypertension, is the addition of mineralocorticoid receptor antagonist beneficial in reducing albuminuria and cardiovascular events? A. CKD patients with resistant hypertension not meeting blood pressure targets on three classes of anti-hypertensive medications (including diuretic) should be considered for mineralocorticoid receptor antagonist therapy Clinical Question 15. Among patients with CKD, is giving anti-hypertensive at bedtime more beneficial in reducing cardiovascular event? A. Administer one or more antihypertensive medications at bedtime. BLOOD PRESSURE MANAGEMENT AMONG PERSONS WITH STROKE Clinical Question 16.1 For adults with acute ischemic stroke (AIS) who are eligible for intravenous (IV) thrombolysis but not for mechanical thrombectomy, what is the threshold for pharmacological treatment and the target blood pressure (BP)? A. For adults with AIS who are eligible for IV thrombolysis but not for mechanical thrombectomy, a referral to a neurologist or stroke specialist is advised. It is recommended that the BP be maintained < 185/110 mmHg prior to treatment and during infusion. For the next 24 hours after treatment is given, the BP is recommended to be maintained < 180/105 mmHg. Clinical Question 16.2 For adults with AIS who are eligible for IV thrombolysis but not for mechanical thrombectomy, what are the pharmacologic agents of choice to reach the target BP? A. It is recommended to use a titratable intravenous medication to allow dynamic adjustment of the drug depending on the current BP. For patients with acute ischemic stroke otherwise eligible for intravenous thrombolysis with BP >185/110 mmHg before or during infusion, or BP >180/105 mmHg after treatment, the recommended pharmacologic agent is Nicardipine 43 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ B. 1- 5mg/hr. IV, titrated up by 2.5mg/hr. every 5-15 minutes, with maximum of 15mg/hr. If available, labetalol 10 mg IV over 1-2 minutes followed by continuous IV infusion of 2-8 mg/min may also be used. Clinical Question 17.1 For adults with AIS who are not eligible for IV thrombolysis or mechanical thrombectomy, what is the target BP and threshold for pharmacological treatment? A. For adults with AIS who are not eligible for IV thrombolysis or mechanical thrombectomy, it is recommended to maintain a target mean arterial pressure (MAP) of 110 to 130 mmHg. For adults with AIS who are not eligible for IV thrombolysis or mechanical thrombectomy, the threshold for urgent antihypertensive treatment is with severe hypertension of Systolic BP >220 mmHg or Diastolic BP >120 mmHg. If with severe hypertension, it might be reasonable to reduce the BP by 15% during the first 24 hours after the onset of stroke. Clinical Question 17.2. For adults with AIS who are not eligible for IV thrombolysis or mechanical thrombectomy, what pharmacological agent may be used to achieve target BP, when needed? A. For adults with AIS who are not eligible for IV thrombolysis or mechanical thrombectomy, the use of IV nicardipine to achieve the target BP may be considered Clinical Question 18.1. For adult patients with acute hypertensive parenchymal intracerebral hemorrhage (ICH), what is the threshold for BP lowering in the first few hours upon presentation at the emergency room? A. For adult patients with acute ICH, the threshold for BP lowering is SBP ≥ 180 mmHg. Clinical Question 18.2 What would be the target BP when lowering the blood pressure in acute ICH? A. The target SBP is <180 mmHg. In patients with SBP ≥180 mmHg, careful BP lowering to 140 to 160 mmHg should be considered. The magnitude of BP reduction is dependent on the clinical context. It should be careful SBP lowering (avoiding reductions ≥60 mmHg in 1 hour). o It is recommended to keep the blood pressure stable and avoid variability. o It is also recommended not to lower the BP acutely to < 140 mmH Clinical Question 18.3 What are the pharmacologic agents of choice and manner of administration? A. It is recommended to use intravenous antihypertensive agents that can easily be titrated to lower the BP to the desired level. The 1st line drug of choice is IV Nicardipine. Alternative treatment choice would be labetalol, when available. Clinical Question 19. For adults who have a history of stroke, what is the target blood pressure level for secondary prevention? A. For adults with history of stroke, the target blood pressure level for secondary prevention is less than or equal to 130/80 mm Hg. RAS blockers, CCBs and thiazide diuretics remain to be the first-line pharmacologic agents in hypertension management for secondary stroke prevention. 44 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ 45 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ 46 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ MANAGEMENT OF HYPERTENSION IN PREGNANCY Clinical Question 20. What are the different types of hypertensive disorders of pregnancy (HDP) and what are the criteria for each? A. Pre-eclampsia- Elevated blood pressure and proteinuria. a. Elevated blood pressure defined as: i. Systolic blood pressure of 140 mm Hg or more or diastolic blood pressure of 90 mm Hg or more on two occasions at least 4 hours apart after 20 weeks of gestation in a woman with a previously normal blood pressure. ii. Systolic blood pressure of 160 mm Hg or more diastolic blood pressure of 110 m Hg or more. (Severe hypertension can be confirmed within a short interval (minutes) to facilitate timely antihypertensive therapy). b. Proteinuria i. 300 mg or more per 24 hour urine collection (or this amount extrapolated from a timed collection), or ii. Protein/creatinine ratio of 0.3 mg/dl or more or iii. Dipstick reading of 2+ (used only if other quantitative methods not available) c. Or in the absence of proteinuria, new onset hypertension with the new onset of any of the following: i. Thrombocytopenia: Platelet count less than 100,000 x 109 /L ii. Renal insufficiency: Serum creatinine concentrations greater than 1.1 mg/dL or a doubling of the serum creatinine concentration in the absence of other renal disease iii. Impaired liver function: Elevated blood concentrations of liver transaminases to twice normal concentration iv. Pulmonary edema v. New-onset headache unresponsive to medication and not accounted for by alternative diagnoses or visual symptoms B. Eclampsia- New-onset tonic-clonic, focal, or multifocal seizures in the absence of other causative conditions such as epilepsy, cerebral arterial ischemia and infarction, intracranial hemorrhage, or drug use. C. Chronic Hypertension- Hypertension of any cause, that predates pregnancy. BP > 140/90 mm Hg before pregnancy or before 20 weeks gestation or both. D. Chronic Hypertension with Superimposed Pre-eclampsia- Chronic hypertension in association with preeclampsia. Others define it as worsening baseline hypertension accompanied by newonset proteinuria or other findings supportive of preeclampsia. a. For patients with chronic hypertension, It can be difficult to differentiate worsening of the hypertension from superimposed preeclampsia. Conditions that may indicate superimposed preeclampsia, that warrants a referral to a maternal fetal medicine specialist/perinatologist, include the following: i. Acute, severe, and persistent elevations in blood pressure. ii. Sudden increase in baseline hypertension. iii. New-onset proteinuria or sudden increase in proteinuria 47 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ E. Gestational Hypertension – a. Systolic blood pressure 140 mm Hg or more or a diastolic blood pressure of 90 mm Hg or more, or both, on two occasions at least 4 hours apart after 20 weeks of gestation, in a woman with a previously normal blood pressure. b. Hypertension without proteinuria or severe features develops after 20 weeks of gestation and blood pressure Clinical Question 21. What blood pressure threshold is used to define hypertension in pregnancy? A. Hypertension is diagnosed empirically when appropriately taken blood pressure is 140 mm Hg systolic or 90 mm Hg diastolic or above. Korotkoff phase V is used to define diastolic pressure. Clinical Question 22. What antihypertensive agents can be used for urgent blood pressure control in pregnancy? A. Acute-onset severe hypertension (systolic BP of 160 mm Hg or more or diastolic BP of 110 mm Hg or more, or both) can occur in the prenatal, intrapartum and postpartum period. It is accurately measured using standard techniques and is persistent for 15 minutes or more. The first line of treatment is intravenous (IV) hydralazine and labetalol; intravenous nicardipine is also an option. Extended release oral nifedipine also may be considered as a first line therapy, particularly when IV access is not available. Use of these drugs does not require cardiac monitoring. Clinical Question 23. When do we treat hypertension during pregnancy? A. Treatment of severe hypertension (blood pressure of >160/100mmHg) is always recommended as it prevents serious maternal and fetal complications to set in. It is also important to avoid hypotension because the degree by which placental blood flow is autoregulated is not established, and aggressive lowering may cause fetal distress. Clinical Question 24. What are the pharmacologic treatment options in the OPD management of hypertension in pregnancy? A. The choice of antihypertensive drug for initial therapy should be based on the characteristics of the patient, contraindications to a particular drug and physician and patient preferences. The first line drugs are methyldopa, calcium channel blockers or beta blockers, and ACEinhibitors and angiotensin-receptor blockers (ARBs) are generally not recommended. Antihypertensives may be used to keep systolic blood pressure at 130 to 155 mmHg and diastolic blood pressure at 80 to 105 mmHg. Clinical Question 25: How is hypertension managed during the immediate postpartum and breastfeeding periods? A. Blood pressure should be recorded shortly after birth and if normal again within 6 hours. B. All women should have BP recorded and discharge deferred for at least 24 hours or until vital signs are normal and/or treated or referred. Any woman with an obstetric complication and/or newborn with complications should stay in the hospital until both are stable. a. In hospital stay for at least 24 hours 48 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ b. Check up within 48-72 hours of the birth and again 7-14 days and at six weeks postpartum. c. All women should be reminded of the danger signs of preeclampsia following birth including headaches, visual disturbances, nausea, vomiting, epigastric or hypochondrial pain, feeling faint or convulsions BLOOD PRESSURE MANAGEMENT IN THE PEDIATRIC POPULATION Clinical Question 26. Among pediatric patients, what is the threshold for commencing pharmacologic treatment for Hypertension? A. Pharmacologic treatment for hypertension (HTN) should be started for children with the following conditions: a. Children who remain hypertensive even after six (6) months of lifestyle modification strategies* b. Symptomatic hypertension or Stage 2 hypertension c. Presence of co-morbidities like chronic kidney disease (CKD) or diabetes mellitus (DM), or any evidence of target organ involvement (e.g. left ventricular hypertrophy). B. The goal of pharmacologic therapy should be a reduction in systolic blood pressure (SBP) and diastolic blood pressure (DBP) to <90th percentile for age, sex and height and <120/80 mm Hg in adolescents ≥13 years of age. C. For children with CKD, BP targets should be less than or equal to 50th percentile for age, sex and height. D. The goal of treatment of hypertension in the pediatric population is not only to reduce BP to <90th percentile for age, sex and height and <130/80 mm Hg, but also to reduce cardiovascularrisk factors, and prevent target organ damage. E. Follow-up every 4-6 weeks is recommended for monitoring and evaluation of therapy 49 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ Clinical Question 27. What advice regarding nonpharmacologic treatment is recommended for pediatric patients? A. Non-pharmacologic therapy of lifestyle modification which include Dietary Approaches to Stop Hypertension (DASH) and engaging in 30-60 minutes of moderate to vigorous physical activity at least 3-5 days a week should be initiated in all pediatric patients consulting for the first time for hypertension. B. All children with hypertension should have their body mass index (BMI) measured during each visit C. Weight loss intervention is recommended for identified overweight and obese children until a normal BMI is attained through dietary counselling and exercise (weight loss of 1 to 2 kg per month). D. All children diagnosed to have hypertension or elevated BP should be advised to do the following: a. Decrease intake of high sodium content and calorie-dense food and beverages, and to increase intake of fruits and vegetable to 3-5 servings per day. b. Decrease intake of high sodium content and calorie-dense food and beverages, and to increase intake of fruits and vegetable to 3-5 servings per day. c. Avoid smoking including electronic cigarettes and exposure to tobacco smoke. d. Avoid alcohol intake and caffeinated energy drinks. Clinical Question 28. What are the BP targets for prevention of target organ complications? A. The target BP for children is <90th percentile for age, sex and height or <120/<80 mmHg whichever is lower B. For CKD patients, BP target is less than or equal to the 50th percentile for age, sex and height. Clinical Question 29. What are the preferred medications for children? A. Any of the following drugs may be used as initial treatment for children with hypertension: ACE inhibitors (Enalapril, Captopril), ARBs (Losartan, Valsartan), or calcium channel blockers (Amlodipine). B. For children with co-existing chronic kidney disease, proteinuria or diabetes mellitus, an ACEinhibitor or ARB is recommended as the initial antihypertensive drug unless with absolute contraindications. Referral to a specialist is highly recommended. C. Therapy should start with a single drug at the lowest possible dose and titrated up every 2 to 4 weeks until target BP is achieved, or the maximal dose reached or adverse effects occur. D. If BP is not controlled with a single agent (maximal dose is reached or adverse effects occur), a second agent can be added to the regimen and titrated as with the initial drug. Because the use of other anti-hypertensive agents can lead to compensatory salt and water retention, the addition of a thiazide diuretic to an initial drug for uncontrolled hypertension is prudent. In combining agents from different drug classes, it is preferable to give those with complementary modes of action. Ideally, no two drugs which act separately on the RAAS, 50 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ should be used in combination because of the risk of hyperkalemia, impaired kidney function and hypotension. Clinical Question 30: What is the recommended technique and BP device for accurate BP measurement in pediatric patients? A. The use of proper technique and appropriately-sized cuff is critical for the accurate measurement of BP in children. B. An auscultatory device using an aneroid non-mercury sphygmomanometer is recommended for children. C. An oscillometric device is a suitable alternative to auscultation for initial BP screening and monitoring in the pediatric population. D. Ambulatory BP monitoring (ABPM) is recommended in children (> 5 years old) and adolescents with the following conditions: a. Elevated office BP measurements for 1 or more years, or if with stage 1 hypertension over 3 clinic visits, for confirmation of hypertension. b. Those with high-risk conditions (e.g. obesity, CKD or structural renal abnormalities, diabetes mellitus, those who have undergone solid organ transplant, obstructive sleep apnea, repaired aortic coarctation) to document masked hypertension. c. Those with suspected white coat hypertension. E. Home BP monitoring should not be used to diagnose hypertension, MH, or WCH but may be a useful adjunct to office and ambulatory BP measurement if clinically validated oscillometric apparatus and appropriate-sized cuffs are used. 51 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ 52 Republic of the Philippines Province of Zamboanga Sibugay OLUTANGA MUNICIPAL HOSPITAL Bateria, Olutanga, Zamboanga Sibugay _____________________________________________________________ 53
 0
0
advertisement
Related documents


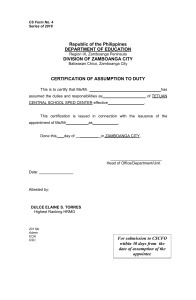
Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users