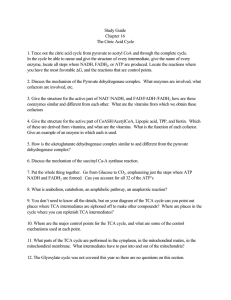
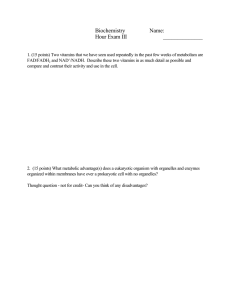
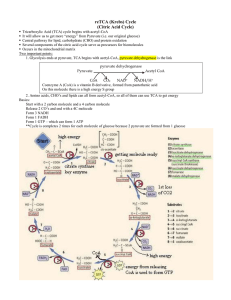
Biochemistry I (Week 14) Metabolism Cells carry out chemical reactions in organized steps called pathways, such as glycolysis. In these pathways, the product of one reaction becomes the starting material for the next. Pathways are grouped into two main types: catabolic pathways, which break down large molecules like proteins, fats, and carbohydrates into smaller ones such as carbon dioxide, water, and ammonia, and anabolic pathways, which build complex molecules like glycogen from smaller components such as glucose. These pathways often connect to form a network of chemical reactions that work together efficiently. The term metabolism refers to all the chemical changes happening in a cell, tissue, or the entire body, while metabolites are the intermediate products of these chemical reactions. The main focus is on the metabolic pathways that create and break down carbohydrates, fats, and proteins. Metabolism is easier to understand when we break it down into smaller pathways. Each pathway is made up of several enzymes, and each enzyme plays a key role in speeding up or controlling the process. This image shows a metabolic map of the main pathways involved in energy metabolism. This “big picture” helps us see how different pathways are connected, how molecules move through them and what happens if something blocks a pathway (like a drug or a missing enzyme due to a genetic disorder). Catabolic and Anabolic reactions Catabolic reactions break down energy-rich molecules to produce ATP, the cell's main energy source. Catabolic pathways are usually oxidative, meaning they need oxidized coenzymes like NAD⁺ to work. Catabolism also breaks down food or stored molecules into simpler parts, which the body can use to build more complex molecules. Catabolic reactions occur in three main stages. First, large molecules in food are broken down into smaller building blocks: proteins are degraded into amino acids, carbohydrates (polysaccharides) into simple sugars (monosaccharides), and fats into fatty acids and glycerol. Next, these smaller components are further broken down into simple molecules like acetyl coenzyme A (acetyl-CoA), generating a small amount of ATP. Finally, acetyl-CoA enters the TCA (Krebs) cycle, where it is oxidized, producing a large amount of ATP through oxidative phosphorylation as electrons from NADH and FADH₂ are transferred to oxygen. Process of building complex molecules from simpler ones. This process requires energy, typically from ATP. Breaking down large molecules into smaller ones to release energy, usually in the form of ATP. Anabolism is the opposite of catabolism. It is a process where a few simple molecules, like amino acids, are used to build a wide variety of complex molecules, like proteins. Anabolic reactions require energy (endergonic), which comes from breaking down ATP into ADP and inorganic phosphate (Pi). Unlike catabolism, which releases energy (exergonic), anabolism uses energy and involves chemical reductions. These reductions often rely on NADPH as the electron donor. Metabolic Map A metabolic map is a visual diagram showing how different chemical reactions and pathways in a cell are connected. It highlights how molecules are broken down (catabolism) to release energy and how they are built up (anabolism) to create essential compounds. The map typically includes key pathways like glycolysis, the citric acid cycle (TCA cycle), and oxidative phosphorylation, showing how energy and building blocks are produced and used. The tricarboxylic acid (TCA) cycle, also known as the citric acid or Krebs cycle, is a key part of metabolism. It is where the breakdown of carbohydrates, amino acids, and fatty acids meets. Their carbon atoms are turned into carbon dioxide (CO2), and this process helps produce most of the ATP in animals, including humans. The cycle happens in the mitochondria, close to the electron transport chain (ETC), which uses oxygen (O2) to help oxidize the molecules produced in the cycle (NADH and FADH2). Some reactions, like the breakdown of certain amino acids, add intermediates to the cycle (called anaplerotic reactions). The cycle also provides important molecules for building other substances, such as glucose, amino acids, and heme. Because of this, the TCA cycle is not a closed system but an open one, with compounds constantly entering and leaving as needed. Metabolic Map The major way all these metabolic pathways (glucose, amino acids, fatty acids, ketone bodies) are linked to the TCA cycle is that they all contribute to providing acetyl-CoA (AcoA), which is the main starting component for the cycle. In addition to acetyl-CoA, some of these pathways also produce intermediates that can directly enter the TCA cycle. For example, succinyl-CoA can be produced from catabolism of valine, isoleucine, and odd-chain fatty acids. Other intermediates that directly enter the TCA cycle include oxaloacetate from transamination or deamination of aspartate, α-ketoglutarate from transamination or deamination of glutamate, fumarate from catabolism of phenylalanine and tyrosine, and malate, which can be synthesized from pyruvate via pyruvate carboxylation (an anaplerotic reaction). Pyruvate metabolism Pyruvate, the end product of glycolysis, can be metabolized through four distinct pathways depending on cellular conditions and energy demands: 1. Pyruvate is transaminated to alanine in a reaction catalyzed by the enzyme alanine aminotransferase (ALT). This reaction involves the transfer of an amino group from glutamate to pyruvate, producing alanine and αketoglutarate. This reaction is a key step in the alanine (Cahill) cycle, where alanine serves as a carrier of nitrogen and carbon between muscle and liver. During intense activity or fasting, muscle generates pyruvate from glycolysis and combines it with nitrogen from glutamate to form alanine, preventing nitrogen buildup and conserving energy. Alanine is transported to the liver, where it is converted back to pyruvate by ALT, transferring the amino group to α-ketoglutarate to form glutamate. Glutamate releases ammonia, which enters the urea cycle for excretion. The pyruvate in the liver is used for gluconeogenesis to produce glucose, which is released into the bloodstream and taken up by muscles as fuel, completing the cycle. Alanine cycle is crucial for maintaining energy balance and nitrogen homeostasis. Pyruvate metabolism 2. Pyruvate can be carboxylated to oxaloacetate by the enzyme pyruvate carboxylase in the mitochondria. This reaction requires ATP and biotin as cofactors and is crucial for gluconeogenesis and replenishing intermediates in the TCA cycle (anaplerosis). 3. In aerobic conditions, pyruvate is oxidatively decarboxylated to acetylCoA by pyruvate dehydrogenase complex (PDH). This reaction produces CO₂ and NADH and is an essential step for entry into the TCA cycle and fatty acid synthesis. 4. Under anaerobic conditions or during high-intensity exercise, pyruvate is reduced to lactate by the enzyme lactate dehydrogenase (LDH). This process regenerates NAD⁺ from NADH, which is necessary for continued glycolysis. Lactate is transported to the liver, where it is converted back to pyruvate and used for gluconeogenesis as part of the Cori cycle. Lactate buildup can lead to lactic acidosis. However, the Cori cycle helps prevent this by transporting lactate to the liver, where it can be converted back into pyruvate and used for gluconeogenesis, reducing the risk of acidosis. Pyruvate Dehydrogenase complex The major source of acetyl CoA for the TCA cycle is the oxidative decarboxylation of pyruvate by the multienzyme pyruvate dehydrogenase complex (PDH complex, or PDHC). However, the PDHC is not a component of the TCA cycle. Pyruvate, the end product of glycolysis, is transported from the cytosol into the mitochondrial matrix by the pyruvate mitochondrial carrier (MPC) of the inner mitochondrial membrane. In the matrix, the PDHC converts pyruvate to acetyl CoA. The pyruvate dehydrogenase complex (PDHC) is made up of three main enzymes: pyruvate decarboxylase (E1 or PDH), dihydrolipoyl transacetylase (E2), and dihydrolipoyl dehydrogenase (E3). Each enzyme handles a specific step in converting pyruvate to acetyl-CoA, and their close arrangement ensures the reactions occur in the correct order without releasing intermediates. The PDHC also includes two regulatory enzymes: PDH kinase, which inactivates the complex, and PDH phosphatase, which activates it. The pyruvate dehydrogenase complex (PDHC) requires five coenzymes to carry out its reactions: thiamine pyrophosphate (TPP) for E1 (pyruvate decarboxylase), lipoic acid and CoA (active form of vitamin B5) for E2 (dihydrolipoyl transacetylase), and FAD and NAD⁺ for E3 (dihydrolipoyl dehydrogenase). TPP, lipoic acid, and FAD are tightly bound to the enzymes and function as prosthetic groups. Pyruvate Dehydrogenase complex The different elements of the pyruvate dehydrogenase complex work together to convert pyruvate into acetyl-CoA. The first step involves the E1 subunit, which decarboxylates pyruvate, releasing CO₂ and creating a 2-carbon intermediate called the hydroxyethyl group. Then E1 adds this intermediate to thiamine pyrophosphate (active form of vitamin B1), forming hydroxyethyl-TPP. Next, the E2 subunit transfers the hydroxyethyl group from TPP to lipoamide (the active form of lipoic acid), forming hydroxyethyllipoamide. The hydroxyethyl group is then oxidized by the E3 enzyme, using NAD⁺ and FAD⁺ as electron acceptors. During this oxidation process, two electrons are removed, converting the hydroxyethyl group into acetyl group. This process involves the reduction of lipoamide (the disulfide bond in lipoamide is reduced to form dihydrolipoamide) while the hydroxyethyl group is oxidized to form acetyl-dihydrolipoamide. After oxidation step, the acetyl group is transferred from dihydrolipoamide to the coenzyme A (CoA), catalyzed by E2, resulting in the formation of acetyl-CoA, which enters the citric acid cycle (TCA cycle) for energy production. Finally, the reduced dihydrolipoamide is regenerated back to its active form (lipoamide) by E3, which involves the oxidation of dihydrolipoamide back to lipoamide, using NAD⁺ as an electron acceptor. NADH and H⁺ are produced during this step. PDHC cofactors TPP is the active form of thiamine (vitamin B1). TPP is created by the phosphorylation of thiamine into thiamine monophosphate (TMP), and then TMP is further phosphorylated to form thiamine pyrophosphate (TPP). The enzyme which catalyzes these reaction steps is known as thiamine pyrophosphokinase, which uses ATP as the phosphate donor. FAD+ (flavin adenine dinucleotide) is synthesized from riboflavin (vitamin B2). During the synthesis process, riboflavin is first converted into FMN (flavin mononucleotide) by the action of riboflavin kinase. In the next step, the enzyme FMN adenylyltransferase adds AMP (from ATP) to FMN, creating FAD. FAD+ can accept 2 electrons and 2 protons (H+) to generate FADH2. This molecule serves as an electron carrier, which can donate electrons to the electron transport chain (ETC), ultimately contributing to the production of ATP. Lipoic acid is attached to a lysine residue on the E2 subunit via an amide bond, catalyzed by lipoate protein ligase (LplA). PDHC cofactors NAD⁺ (nicotinamide adenine dinucleotide) is synthesized from niacin (vitamin B3), also known as nicotinic acid. In addition to dietary intake, niacin can also be synthesized from tryptophan. Niacin is converted to nicotinamide mononucleotide (NMN) by the enzyme known as nicotinic acid phosphoribosyltransferase (NAPRT), using PRPP (phosphoribosyl pyrophosphate) as a donor. NMN is then converted to NAD⁺ by the enzyme NMN adenylyltransferase, which adds an AMP (from ATP) to NMN. NAD⁺ (nicotinamide adenine dinucleotide) can accept 2 electrons and 1 proton (H⁺) to generate NADH. This molecule serves as an electron carrier, which can donate electrons to the electron transport chain (ETC), ultimately contributing to the production of ATP. CoA (Coenzyme A) is synthesized from pantothenic acid (vitamin B₅), along with cysteine and ATP, through a multi-step enzymatic pathway. just like a FAD and NAD, CoA is also nucleotide coenzyme (is synthesised by the adding the vitamin to nucleotide). CoA primarily functions to facilitate the transfer and activation of acetyl (CH₃-C=O) or other acyl (R-C=O) groups in enzymatic reactions, playing a central role in metabolic pathways such as the citric acid cycle, fatty acid metabolism, and biosynthetic processes. PDHC regulation The PDH kinase is activated by high levels of ATP, acetyl-CoA, and NADH, which signals that the cell has enough energy, so it shuts down the PDHC. Pyruvate, on the other hand, inhibits PDH kinase, allowing E1 to stay active when pyruvate levels are high. Calcium (Ca²⁺) activates PDH phosphatase, which increases E1 activity. This is important in skeletal muscle, where Ca²⁺ release during muscle contraction stimulates the PDHC to produce more energy. Although the kinase and phosphatase regulation are key, PDHC activity can also be inhibited by high levels of its products, NADH and acetyl-CoA. When the NAD⁺/NADH ratio is increased, it indicates that the cell has a low amount of NADH available for the electron transport chain (ETC) and thus reduced capacity for ATP synthesis. Additionally, high levels of ADP suggest low ATP availability, signaling increased demand for energy, while elevated cytoplasmic calcium (Ca²⁺) levels in skeletal muscle cells indicate muscle contraction, a state requiring high energy production. Together, these signals reflect a high cellular energy demand, and as a result, the PDHC must be activated to produce more acetyl-CoA for the TCA cycle, ultimately increasing ATP synthesis via the ETC. In contrast, when the NAD⁺/NADH ratio is decreased, it indicates a high NADH level, reflecting sufficient electron donors for the ETC and ATP synthesis. Additionally, high levels of ATP indicate that the cell already has sufficient energy, while elevated acetyl-CoA levels suggest an abundant supply of a key TCA cycle intermediate. These signals indicate that the cell has an adequate energy supply and does not require additional ATP synthesis, leading to the inhibition of PDHC activity. PDHC deficiency A deficiency in the α subunits of the E1 component of the pyruvate dehydrogenase complex (PDHC) is a rare cause of congenital lactic acidosis. This deficiency reduces the ability to convert pyruvate into acetyl-CoA, causing pyruvate to be turned into lactate instead, leading to lactic acid buildup. This is particularly harmful to the brain, which relies on the TCA cycle for energy and is sensitive to acidosis. Symptoms can vary and may include brain damage, muscle stiffness, and early death in infants. In addition to lactic acidosis, the situation is worsened because the reduction of acetyl-CoA formation inhibits TCA cycle activity, leading to decreased energy production. AcoA is also an essential activator of pyruvate carboxylase (PC), and without it, this enzyme cannot be activated, resulting in reduced formation of oxaloacetate. This further diminishes TCA cycle activity and also impairs gluconeogenesis, contributing to a further reduction in energy production, particularly in tissues like the brain. On the other hand, similar to lactic acid, the formation of alanine from accumulated pyruvate is also increased, leading to an elevation of alanine levels, which typically starts in infancy. Currently there is no proven cure, but limiting carbohydrates in the diet, increasing the intake of ketogenic nutrients (e.g. high-fat content or high lysine and leucine) as alternative sources for acetyl-CoA formation, and taking thiamine (a key cofactor for PDHC) may help alleviate symptoms in some patients. Alcoholics usually have thiamine deficiency for several reasons, including poor diet, impaired absorption due to damage to the gastrointestinal (GI) tract, liver damage (which reduces the liver's ability to store and activate thiamine into its active form, TPP), and increased excretion of thiamine through the urine (as alcohol increases thiamine excretion by the kidneys). This must be considered in clinical practice because administering glucose to alcoholics with thiamine deficiency can lead to severe lactic acidosis, a potentially fatal condition. Without sufficient thiamine, the PDHC cannot function properly, causing pyruvate to accumulate and be converted into lactate (lactic acid). Arsenic poisoning mainly affects enzymes that need lipoic acid as a coenzyme, including PDH, α-ketoglutarate dehydrogenase, and branched-chain α-keto acid dehydrogenase. Arsenite (the toxic form of arsenic) binds to the thiol (−SH) groups of lipoic acid, preventing it from working properly. This leads to the buildup of pyruvate and lactate, similar to PDHC deficiency. The brain is especially affected, causing neurological problems and even death. Patient may exhibit a garlic-like odor on their breath, which is caused by the oxidation of arsenic to arsenous oxide, responsible for the characteristic smell. Nonspecific symptoms of arsenic poisoning include vomiting, diarrhea. TCA cycle TCA cycle is a central pathway in cellular metabolism that generates high-energy molecules, such as NADH, FADH₂ (which are used in the electron transport chain for ATP synthesis) and GTP. TCA cycle takes place in the mitochondrial matrix. AcoA donates two carbon atoms to the TCA cycle. During the cycle, these carbons are removed as CO₂ (So, for each round of the TCA cycle, there is no net gain or loss of intermediates). As a result, the carbons from acetyl-CoA cannot be directly used for the synthesis of oxaloacetate (OAA), a precursor for gluconeogenesis. This means acetyl-CoA cannot be directly utilized for gluconeogenesis. However, acetyl-CoA plays a crucial role in triggering gluconeogenesis. The first step of the TCA cycle is the synthesis of citrate, a 6-carbon molecule, through the irreversible condensation of the 4-carbon molecule oxaloacetate (OAA) with the 2-carbon molecule acetyl-CoA (AcoA). This reaction is catalyzed by the enzyme citrate synthase, which is inhibited by high levels of ATP and citrate. When ATP is high, it indicates that the cell already has sufficient energy, so the TCA cycle is downregulated to prevent the production of more ATP. Citrate itself is an important indicator of the cell’s energy status. High levels of citrate inhibit glycolysis (as no additional energy is needed) and activate fatty acid synthesis (to store excess energy). TCA cycle At the next step of the TCA cycle, aconitase catalyzes the conversion of citrate to cis-aconitate, and then the conversion of cis-aconitate to isocitrate (an isomer of citrate). This step is reversible. Aconitase can be inhibited by a rat poison called fluoroacetate. When this poison enters the body, it is converted into fluoroacetyl-CoA, which then reacts with oxaloacetate (OAA) to form fluorocitrate. Fluorocitrate is a potent inhibitor of aconitase, blocking its activity in the TCA cycle. In the next step of the TCA cycle, the six-carbon molecule isocitrate undergoes oxidative decarboxylation to form the five-carbon molecule α-ketoglutarate. During this reaction, a carbon atom is removed from isocitrate in the form of CO₂. This irreversible step is catalyzed by isocitrate dehydrogenase, an enzyme that utilizes NAD⁺ to facilitate the oxidative step, resulting in the production of NADH. The NADH generated can then enter the electron transport chain (ETC) to drive ATP synthesis. This reaction represents one of the key rate-limiting steps of the TCA cycle. Isocitrate dehydrogenase is inhibited by high levels of ATP and NADH, indicating that the cell is in high-energy state and doesn’t require additional ATP production. Conversely, When ADP levels are high, it means the cell is low on energy. This activates the enzyme, helping it produce more ATP, the cell's main energy source. Additionally, elevated cytoplasmic Ca²⁺ levels, particularly in skeletal muscle cells during contraction (a state demanding high energy production) also activate isocitrate dehydrogenase. TCA cycle The next irreversible step in the TCA cycle involves the synthesis of the fourcarbon molecule succinyl-CoA through the oxidative decarboxylation of the fivecarbon molecule α-ketoglutarate. This reaction is catalyzed by the α-ketoglutarate dehydrogenase complex, which consists of multiple copies of three different enzymes and operates in a manner similar to the PDHC. The reaction requires five coenzymes: TPP, lipoic acid, FAD, NAD⁺, and CoA, each of which plays a specific role in the reaction mechanism. During this reaction, one carbon atom from α-ketoglutarate is released in the form of CO₂, and the remaining four-carbon structure is attached to CoA to form succinyl-CoA. This process also generates a second molecule of NADH, which can enter ETC to drive ATP synthesis. This step can be inhibited by succinyl-CoA through feedback inhibition, as well as by elevated levels of NADH. In skeletal muscle cells, increased Ca²⁺ levels in the cytoplasm can activate the enzyme's activity. TCA cycle The next reversible step in the TCA cycle is catalyzed by succinate thiokinase (also known as succinyl-CoA synthetase), which breaks the high-energy thioester bond of succinyl-CoA. This process removes CoA from succinyl-CoA, resulting in the production of succinate. The reaction is coupled with the phosphorylation of GDP to form GTP, which can be used for energy. It should be mentioned that GTP and ATP can be converted into each other through a reaction catalyzed by nucleoside diphosphate kinase (GTP + ADP ⇄ GDP + ATP). succinyl-CoA is is very important substrate for the synthesis of heme molecule and hemoglobin. Additionally, succinyl-CoA can be derived from propionyl-CoA, a product of the metabolism of fatty acids with an odd number of carbon atoms and certain amino acids. Succinyl-CoA can also be converted into pyruvate for gluconeogenesis. In the next step, succinate is oxidized to form fumarate. This reaction is catalyzed by succinate dehydrogenase (also known as Complex II in ETC), which uses FAD as the electron acceptor. During this process, FAD is reduced to FADH2, which can be used in the electron transport chain for ATP synthesis. Succinate dehydrogenase is the only enzyme in the TCA cycle located in the inner mitochondrial membrane. Because of this, it also functions as Complex II in the ETC, serving as the enzyme for both the TCA cycle and the ETC. Fumarate can also be synthesized in the urea cycle, during purine synthesis (specifically in IMP synthesis), and during the breakdown of amino acids such as tyrosine and phenylalanine. As a result, all of these reactions can contribute fumarate to the TCA cycle. TCA cycle In the next step, fumarate is hydrated to malate in a freely reversible reaction catalyzed by the enzyme fumarase. In the final reversible step of the TCA cycle, malate is oxidized to oxaloacetate (OAA) by the enzyme malate dehydrogenase. This enzyme uses NAD⁺ as the electron acceptor, producing the third and final NADH of the cycle, which can be ETC for ATP synthesis. Malate can be used in the malate-aspartate shuttle. OAA can also be produced from the amino acid aspartic acid through a process called transamination, or it can be generated from pyruvate by the enzyme pyruvate carboxylase. Each turn of the TCA cycle generates 3 NADH, 1 FADH₂, and 1 GTP. Each NADH produces 2.5 ATP when oxidized by the electron transport chain (ETC), and each FADH₂ produces 1.5 ATP. Therefore, the ATP yield from oxidizing one acetyl-CoA is 10 ATP. (Note: The previous calculation estimated 12 ATP). Malate-Aspartate shuttle. The reversible conversion of malate to oxaloacetate (OAA) can be used to shuttle molecules from the cytosol into the mitochondria, a process known as the malate shuttle. To understand the malate shuttle, two key points must be considered. First, malate can cross the mitochondrial membrane, while NADH and OAA cannot. As a result, this shuttle is used to transport electrons from NADH (which is generated in the cytoplasm), into the mitochondria to enter the electron transport chain (ETC). Second, It also facilitates the transport of OAA, synthesized in the mitochondria, into the cytoplasm for gluconeogenesis. NADH, which is synthesized in the cytoplasm, cannot directly enter the mitochondria to participate in the ETC for ATP synthesis. To transport electrons from NADH into the mitochondria, cells use the malate shuttle. In the first step, OAA in the cytoplasm is reduced to malate, a reaction that uses NADH and generates NAD+ in the process (NADH donates electrons to malate). Malate can then cross the mitochondrial membrane through specific transporters and enter the mitochondria, bringing the electrons inside. Once inside, malate is oxidized back to OAA, a reaction that uses NAD+ (malate donates electrons to NAD+ to generate NADH, which can enter the ETC). OAA in the mitochondria can also be converted into aspartate, which can be transported back to the cytoplasm, where it is converted back into OAA, thus regenerating OAA in the cytoplasm. OAA synthesized in the mitochondria cannot directly enter the cytoplasm to participate in gluconeogenesis. First, OAA must be converted into malate, which can then leave the mitochondria through specific transporters. Once in the cytosol, malate is converted back into OAA, which can then participate in gluconeogenesis. Fumarase deficiency Fumarase deficiency is a rare genetic disorder caused by mutations in the FUM1 gene, which encodes the enzyme fumarase. This enzyme is crucial for the TCA cycle, catalyzing the reversible hydration of fumarate to malate. This condition disrupts the TCA cycle, leading to an accumulation of fumarate, which impairs cellular energy production and can cause toxicity, particularly affecting the nervous system. When fumarase is deficient, TCA cycle is disrupted, and fumarate accumulates in the cells. This accumulation leads to several metabolic imbalances, including impaired ATP production, as the TCA cycle cannot efficiently generate the highenergy molecules NADH, FADH₂, and GTP, which are essential for ATP synthesis through the electron transport chain (ETC). The buildup of fumarate also causes oxidative stress, which damages cellular structures such as proteins, lipids, and DNA. Moreover, fumarate can interfere with cellular signaling pathways, particularly in the regulation of histone demethylases and the hypoxia-inducible factor (HIF) pathway, leading to Fumarase abnormal gene expression and further disruption of normal cellular functions. The most significant impact of fumarase deficiency occurs in the nervous system, particularly the brain. Neurons, which require high amounts of ATP for normal function, are severely affected due to the energy shortage and the toxic effects of fumarate accumulation. This results in neurodegeneration, developmental delay, intellectual disabilities, seizures, and hypotonia (low muscle tone). The accumulation of toxic metabolites leads to brain cell death and impaired neural development, which is the hallmark of the disease. Other energy-demanding tissues, such as muscles, are also affected, leading to muscle weakness and movement disorders. Overall, fumarase deficiency leads to severe neurological and metabolic consequences, with the brain being the most impacted organ.