Anesthesia Techniques for Carotid Endarterectomy: A Review
advertisement

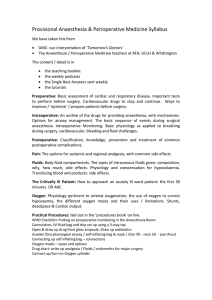
Anaesthesia 2025, 80, 109–111 doi:10.1111/anae.16456 Science Letter Safety of anaesthesia techniques in patients undergoing carotid endarterectomy: a systematic review with metaanalysis of randomised clinical trials Each year, approximately 3000–3500 patients undergo respiratory complications; quality of life one month after carotid endarterectomy in the UK, and over 150,000 surgery; and haemodynamic parameters. Screening and worldwide [1, 2]. It is thought that the selection of data collection were conducted in duplicate by independent anaesthetic method – whether cervical plexus block, reviewers. We assessed risk of bias in individual studies general anaesthesia or a mix of both – can impact using the Risk of Bias 2 tool and judged the certainty of haemodynamic parameters differently and the oxygenation evidence according to GRADE recommendations (online and perfusion of the brain and heart. This variability may Supporting Information Figure S1). have an impact on the risk of stroke, myocardial infarction We categorised the interventions into four groups for and mortality [3]. We conducted a systematic review to the Bayesian network meta-analyses: epidural; regional (i.e. compare the safety and clinical outcomes of different cervical plexus block and/or local infiltration); general; and anaesthetic techniques in patients undergoing carotid combined regional and general anaesthesia. We also endarterectomy. performed Bayesian pairwise meta-analyses comparing This analysis was based on data from a systematic regional with general anaesthesia. Overall, 24 studies review, the protocol of which was registered prospectively. encompassing 5341 patients were included in the analyses. We included randomised clinical trials that enrolled patients We did not find any significant differences between the aged ≥ 18 y undergoing carotid endarterectomy. The interventions for the primary outcomes of stroke and studies included comparisons between any two anaesthesia myocardial infarction within 30 days of surgery (Table 1 techniques (general, local/regional, combined regional and and Fig. 1). However, there was significantly less use of an general). Our primary outcomes were stroke and myocardial arterial shunt with regional compared with general infarction within 30 days of surgery. We also included anaesthesia (relative risk (95% credible interval) 0.33 studies reporting postoperative pain data on within death 24 h; within 30 days; (0.17–0.66), Table 1). No significant differences were found arteries shunted; for the remaining outcomes. postoperative haematoma; time course of arterial occlusion; Our study did not yield results to inform decision- patient satisfaction; surgeon satisfaction; postoperative making regarding choice of anaesthetic technique for cognitive dysfunction; duration of surgery, ICU stay and carotid endarterectomy. No significant differences were hospital stay; need for reintervention; cranial nerve injury; observed for most outcomes. However, readers should not Table 1 Results of the Bayesian pairwise meta-analyses comparing regional with general anaesthesia for four outcomes. Outcome Relative risk (95%CrI) Probability of improvement with regional anaesthesia I2 Certainty of evidence according to GRADE Stroke (seven studies; 4184 patients) 1.05 (0.64–1.90) 45.0% 0.0% Very low Due to risk of bias and relevant imprecision Myocardial infarction (six studies; 3891 patients) 1.08 (0.53–2.23) 41.4% 0.0% Very low Due to risk of bias and relevant imprecision Mortality (seven studies; 4188 patients) 0.76 (0.39–1.51) 81.1% 0.0% Very low Due to risk of bias and relevant imprecision Need for arterial shunt (11 studies; 4356 patients) 0.33 (0.17–0.66) 99.7% 78% Low Due to heterogeneity and imprecision 95% CrI, 95% credible interval. © 2024 Association of Anaesthetists. 109 Science Letter Figure 1 Forest plots with the comparative network effect sizes of four interventions. Black squares, estimated network effect sizes; black bars, 95% credible intervals. Values are reported as relative risks. Note: some effect sizes fall outside the range of 0.1–10, with some black squares non-visible. Shunt, need for arterial shunt; regional, cervical plexus block and/or local infiltration; epidural, epidural anaesthesia; general, general anaesthesia; NA, not available. interpret these findings as evidence of equivalence as they inadequate sedation might lead to tachycardia and may reflect insufficient data. hypertension, increasing the risk of myocardial ischaemia in While our findings show reduced use of arterial shunt this high-risk cohort of patients. This adds complexity, as with the use of regional anaesthesia, there is a possibility different techniques may affect key outcomes like stroke that this result is due to chance, given the number of and myocardial infarction differently. Future research might analyses performed. Applying a Bonferroni correction consider evaluating composite or more critical outcomes, would render this significant difference non-significant. Our such as mortality. results also indicate that regional anaesthesia may reduce Although our findings do not provide strong mortality within 30 days of surgery (Table 1 and Fig. 1). evidence to inform clinical decision-making, they do However, it is important to emphasise that this was not suggest a potential difference between anaesthetic statistically significant, the certainty of evidence is very low, techniques in relation to important outcomes such as and this finding should not be used to inform clinical the need for arterial shunt and mortality. These findings practice. are consistent with observational data and may be Other researchers have summarised data from associated with the incidence of stroke and myocardial randomised trials and observational studies [3–5]. While infarction [3, 5]. As such, our results underscore the observational data suggest improved outcomes with need for further research to determine whether any regional anaesthesia [3, 5], including a reduced incidence of specific technique or combination of techniques may stroke, myocardial infarction and death, these results were improve patient outcomes. not confirmed by a previous summary of randomised studies [4], and not by our updated analysis. In conclusion, the current evidence does not provide robust support for the selection of any specific anaesthetic While regional anaesthesia may improve outcomes by technique for carotid endarterectomy. We did not observe blocking nociceptive pathways and increasing cerebral significant differences for most outcomes, and the one blood flow, it is also possible that uncovered nerve fibres or observed difference may be attributable to chance. 110 © 2024 Association of Anaesthetists. 13652044, 2025, 1, Downloaded from https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/anae.16456 by Test, Wiley Online Library on [17/12/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License Anaesthesia 2025, 80, 109–111 Acknowledgements This systematic review was prospectively registered with PROSPERO (CRD42024505658). Clıstenes C. de Carvalho Idrys H. L. Guedes Federal University of Campina Grande, Campina Grande, Brazil Email: clistenescristian@hotmail.com Anna L. S. Holanda Centro Universit ario Unifacisa, Campina Grande, Brazil Anaesthesia 2025, 80, 109–111 endarterectomy. Ann Vasc Surg 2023; 88: 9–17. https://doi. org/10.1016/j.avsg.2022.08.007. 3. Hajibandeh S, Hajibandeh S, As A, Torella F, Antoniou GA. Metaanalysis and trial sequential analysis of local vs. general anaesthesia for carotid endarterectomy. Anaesthesia 2018; 73: 1280–9. https://doi.org/10.1111/anae.14320. 4. Rerkasem A, Orrapin S, Howard DPJ, Nantakool S, Rerkasem K. Local versus general anaesthesia for carotid endarterectomy. Cochrane Database Syst Rev 2021; 10: CD000126. https://doi. org/10.1002/14651858.CD000126. 5. Harky A, Chan JSK, Kot TKM, et al. General anesthesia versus local anesthesia in carotid endarterectomy: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth 2020; 34: 219– 34. https://doi.org/10.1053/j.jvca.2019.03.029. doi:10.1111/anae.16456 Yuri S. C. Costa Hospital Santa Izabel/SCM-BA, Salvador, Brazil Supporting Information Additional supporting information may be found online via References 1. Watson S, Johal A, Li Q, et al. National Vascular Registry: 2023 State of the Nation Report. 2023. https://www.vsqip.org. uk/wp-content/uploads/2024/04/NVR-2023-State-of-the-NationReport.pdf (accessed 24/09/2024). 2. Brown CS, Osborne NH, Hider A, Kemp MT, Albright J, Scheidel C, Henke PK. Assessment of determinants of value in carotid © 2024 Association of Anaesthetists. the journal website. Figure S1. Risk of bias at outcome level according to Risk of Bias 2 tool: (a) stroke; (b) myocardial infarction; (c) mortality; (d) need for arterial shunt. 111 13652044, 2025, 1, Downloaded from https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/anae.16456 by Test, Wiley Online Library on [17/12/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License Science Letter