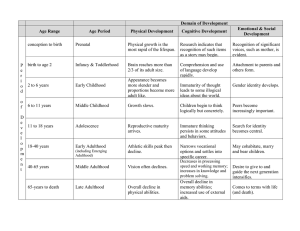
251 Unit 10.1 fa24 MEMORY DEVELOPMENT AND AGING Unit 10, Part 1: Behavioral Processes of Memory Development PSYC 251 Learning and Memory Fall 2024 Session 38 Wednesday, December 4 Copyright © 2024 Eric W. Gobel, PhD 251 Unit 10.1 fa24 Memory Development and Aging • Behavioral processes • The developing memory: Prenatal, infancy, and childhood • Sensitive periods for early learning • Adolescence: Crossing from childhood into adulthood • The aging memory: Adulthood through old age • Brain substrates • Clinical perspectives 251 Unit 10.1 fa24 Memory Development and Aging • Memory systems development parallels development of their underlying brain substrates • Understanding development of learning & memory systems: • Helps tailor school and teaching to place appropriate demands on students. • Helps us understand normal brain development and opens possibilities for extending/improving function across the life span. • One caveat: • Developmental trends represent averages across considerable variability. • Variability exists within a cohort (e.g., the huge diversity of ACT scores for high school seniors) and across developmental trajectories. 251 Unit 10.1A fa24 Memory Development and Aging • Behavioral processes • The developing memory: Prenatal, infancy, and childhood • Sensitive periods for early learning • Adolescence: Crossing from childhood into adulthood • The aging memory: Adulthood through old age • Brain substrates • Clinical perspectives 251 Unit 10.1A fa24 Memory Development: Infancy to Childhood • Incredibly, the ability to learn is intact even before birth. • By 34-36 weeks, auditory habituation: • A speaker is placed on the mother’s abdomen. • Sounds initially cause fetal movement. • Repeated sounds decrease responses. 251 Unit 10.1A fa24 Memory Development: Infancy to Childhood • Immediately after birth, human infants demonstrate incredible learning abilities: • Language • Motor control • Social skills • Some limitations are evident due to immature sensory and motor systems. • Formal experiments show excellent operant and classical conditioning… https://www.youtube.com/watch?v=ZgOu_Uc00ao (3:18) 251 Unit 10.1A fa24 Rovee-Collier Infant Mobile Studies 251 Unit 10.1A fa24 Memory Development: Infancy to Childhood • Infant operant conditioning: kick leg → move mobile • Quickly leads to vigorous leg kicking • Memory maintained for days (no reminders) to weeks (with reminders) • Discriminant stimuli: • Trained in crib with striped crib liner • Kicking in striped cribs • No kicking in plain cribs 251 Unit 10.1A fa24 Memory Development: Infancy to Childhood • Infants also show classical conditioning (remember baby Little Albert?) • Basics intact from birth, some aspects mature: • Eye-blink conditioning slower in infants than adults • Trace conditioning (gap between CS and US) not possible until age 4, and even then, still a bit slower than adults 251 Unit 10.1A fa24 Memory Development: Infancy to Childhood How about infant declarative memory systems? • Infants have semantic memory, which develops further over time. • The development of episodic memory is less clear. • Let’s look at each of these in turn… 251 Unit 10.1A fa24 Memory Development: Infancy to Childhood • Infants have semantic memory, which develops further over time. • Elicited imitation paradigm: • 10-month-old children shown a) how to operate a toy puppet or b) the puppet alone (no demonstration) • Four months later, presented with same puppet • Children who had seen the puppet demonstrated were later more interested in it and were better able to use it. • Shows intact recognition for puppet and how to operate it! • Episodic memory? 251 Unit 10.1A fa24 Memory Development: Infancy to Childhood • Episodic memory seems to develop more slowly. • Children hid stuffed toys around their homes and were later tested for the what, where, and when of these events. • 3-year-olds were worse than 4-year-olds at episodic memory retrieval 251 Unit 10.1A fa24 Memory Development: Infancy to Childhood • Episodic memory seems to develop more slowly. • Children hid stuffed toys around their homes and were later tested for the what, where, and when of these events. • 3-year-olds were worse than 4-year-olds at episodic memory retrieval • Do you remember your early childhood? Why not? • Possible causes of infantile amnesia: • Slow hippocampus development; needed to support episodic memory formation? • Developing sense of self? Infants don’t pass the “red mark” test until about 24 months. • Performance issue? Infants may have episodic memories, but it’s hard for them to express these memories. • The correct explanation is still unclear. 251 Unit 10.1A fa24 Memory Development: Infancy to Childhood • Source memory seems to develop even more slowly. • Children learned factual question-answer pairs and were later tested for source memory. • Young children had poor source memory and could rarely recall having learned the pair within the experiment. • Why? 251 Unit 10.1B fa24 Memory Development and Aging • Behavioral processes • The developing memory: Prenatal, infancy, and childhood • Sensitive periods for early learning • Adolescence: Crossing from childhood into adulthood • The aging memory: Adulthood through old age • Brain substrates • Clinical perspectives 251 Unit 10.1B fa24 Sensitive Periods for Early Learning • Some learning abilities are only available early in life, a so- called sensitive period or critical period after which some forms of learning may become difficult/impossible. • Imprinting: forming a close bond with first individual seen after birth. • Common in birds, but also occurs in other species. • Bond forms best immediately after birth; after this critical period, harder to form. https://www.youtube.com/watch?v=eqZmW7uIPW4 251 Unit 10.1B fa24 Critical Period for Imprinting: Lorenz 251 Unit 10.1B fa24 Sensitive Periods for Early Learning • Some learning abilities are only available early in life, a so- called sensitive period or critical period after which some forms of learning may become difficult/impossible. • Sensitive/critical periods are also evident in other systems: • Visual development: impaired visual input early in development leads to permanent disruption of visual system. • Male sparrows raised in isolation don’t develop normal songs, unless played tape recordings during the exact right developmental time frame (30-100 days after birth). • Human language has also suggested to have a sensitive period. Let’s take a closer look… http://www.youtube.com/watch?v=QzkMo45pcUo 251 Unit 10.1B fa24 Sensitive Period for Visual Development 251 Unit 10.1B fa24 Sensitive Periods for Early Learning • Sensitive/critical periods for language learning? • Skill at phonetic discriminations for sound distinctions not used in exposed languages is lost during early development. 251 Unit 10.1B fa24 Sensitive Periods for Early Learning • Sensitive/critical periods for language learning? • Skill at phonetic discriminations for sound distinctions not used in exposed languages is lost during early development. • Some evidence suggests language must be learned before ~12 years of age to be fully mastered. • Despite extensive tutoring, “feral children” fail to develop normal language (e.g., Genie). • On the other hand… • Adults can learn a second language more quickly than young children, though they don’t usually end up with the same level of mastery. • Differences in mastery may be more related to time-on-task, which young children have lots of relative to most adults. 251 Unit 10.1C fa24 Memory Development and Aging • Behavioral processes • The developing memory: Prenatal, infancy, and childhood • Sensitive periods for early learning • Adolescence: Crossing from childhood into adulthood • The aging memory: Adulthood through old age • Brain substrates • Clinical perspectives 251 Unit 10.1C fa24 Adolescence: Childhood to Adulthood • Adolescence: the transitional stage between the onset of puberty and full adulthood. • Strong development of working memory and central executive function during adolescence. • Digit span increases through early teens. • Executive function develops throughout early adulthood. • Why? 251 Unit 10.1C fa24 Adolescence: Childhood to Adulthood • Adolescence: the transitional stage between the onset of puberty and full adulthood. • Strong development of working memory and central executive function during adolescence. • Ongoing development of frontal lobes • Increasing familiarity leading to better WM encoding (e.g., chunking) • Child chess experts can remember more locations of chess pieces than non- chess-playing adults, due to higher familiarity. 251 Unit 10.1C fa24 Adolescence: Childhood to Adulthood • Adolescence: the transitional stage between the onset of puberty and full adulthood. • Strong development of working memory and central executive function during adolescence. • Gender differences also emerge during this time: • Women perform slightly better (on average) on verbal memory and on spatial learning of landmark locations. • Men perform slightly better (on average) on spatial learning of routes. • Similar gender differences evident in many mammals, suggesting the differences aren’t purely cultural. • Gender differences may be due partly to different levels of sex hormones between males and females (more on this later). 251 Unit 10.1D fa24 Memory Development and Aging • Behavioral processes • The developing memory: Prenatal, infancy, and childhood • Sensitive periods for early learning • Adolescence: Crossing from childhood into adulthood • The aging memory: Adulthood through old age • Brain substrates • Clinical perspectives 251 Unit 10.1D fa24 Aging Memory: Adulthood to Old Age • Adult abilities can remain stable for many years. • Unfortunately, though, the overall pattern in old age is decline in most basic learning, memory, and cognitive skills. 251 Unit 10.1D fa24 Aging Memory: Adulthood to Old Age • Adult abilities can remain stable for many years. • Unfortunately, though, the overall pattern in old age is decline in most basic learning, memory, and cognitive skills. • Working memory is one of the first to show age-related decline. • Proactive interference? Older adults have learned much more and may be less able to prevent this from interfering with the contents of working memory. • Similar trends for conditioning and skill learning: • Eyeblink conditioning starts declining at 40-50 years and can take twice as long in older adults relative to young adults. • Skill learning declines rapidly after 60 years (e.g., rotary pursuit). 251 Unit 10.1D fa24 Aging Memory: Adulthood to Old Age • Semantic and episodic memory show uneven decline: • Ability to retain and retrieve these memories shows little decline during healthy aging. • e.g., older adults who studied Spanish in high school still recalled many Spanish words learned, even with little practice over long spans of time. • Unfortunately, the ability to encode episodic and semantic memories (i.e., encoding) does decline with age. • Older adults show poor paired associate learning. • Deficits can be ameliorated with slower rates of presentation and/or meaningful stimuli. 251 Unit 10.1D fa24 Aging Memory: Adulthood to Old Age • Some good news: strong compensation • Although basic skills decline, older adults have more skills and experience to draw on. • This richer pool of experience can often help compensate for diminished skills and enable performance of complex skills at the same or better level than in young adults! • Example: older typists make slower movements but have better semantic memory and need to look at their manuscript less often, leading to excellent overall performance. • Warning: use it or lose it! • Overall performance is only preserved in skills that are practiced throughout aging. 251 Unit 10.1 fa24 Interim Summary: Behavioral Processes • Learning and memory ability varies over the life span. • In infancy: • Habituation, instrumental conditioning, and classical conditioning are intact (though developing) from birth or earlier. • Semantic memory seems intact (but developing) from an early age, but episodic memory may take more time to fully develop. • During adolescence, strong development of working memory and executive function, and the appearance of small gender differences. • Through adulthood, period of stability but overall decline in most basic memory and cognitive skills, especially working memory. • Storage & retrieval of declarative memories is strong throughout healthy aging, but formation of new declarative and skill memories declines. • Some learning exhibits sensitive periods (such as imprinting), but evidence for a sensitive period for language is unclear. 251 Unit 10.3B fa24 MEMORY DEVELOPMENT AND AGING Finish Part 1: Behavior Part 2: Alzheimer’s Disease PSYC 251 Learning and Memory Fall 2024 Session 39 Friday, December 6 Copyright © 2024 Eric W. Gobel, PhD 251 Unit 10.3B fa24 Memory Development and Aging • Behavioral processes • Brain substrates • Clinical perspectives • Down syndrome • Alzheimer’s disease • A connection between Down syndrome and Alzheimer’s disease 251 Unit 10.3B fa24 Alzheimer’s Disease • Alzheimer’s disease (AD) — a form of progressive cognitive decline from accumulating brain deterioration. • AD affects about 4.5 million people in the U.S. • As many as 50% of people over age 85 are afflicted. • Progression of memory loss in Alzheimer’s disease: • Earliest symptoms are episodic memory failures, such as forgetting recent visitors. 113 251 Unit 10.3B fa24 10 Words Recalled 8 Healthy Elderly 6 4 2 Early AD 0 1 2 3 Delay Trial Patients with AD show marked impairment in many forms of memory, including list learning. Over 3 trials with a 10-word list, AD patients recall fewer items than same-aged healthy controls; after a 10-minute delay, the patients recall almost none of the studied words. Adapted from Figure 1 of Moulin et al. (2004). 251 Unit 10.3B fa24 Alzheimer’s Disease • Alzheimer’s disease (AD) — a form of progressive cognitive decline from accumulating brain deterioration. • AD affects about 4.5 million people in the U.S. • As many as 50% of people over age 85 are afflicted. • Progression of memory loss in Alzheimer’s disease: • Earliest symptoms are episodic memory failures, such as forgetting recent visitors. • Later, there are declines in semantic memory (e.g., forgetting familiar names, locations). • Much later, conditioning and skill memory deteriorate. • In late-stage AD, there is often a lack of awareness and activities of daily living (ADL) skills. 115 251 Unit 10.3B fa24 Plaques and Tangles in the Brain • Amyloid plaques = deposits of beta-amyloid (abnormal byproduct of amyloid precursor protein, or APP; kills adjacent neurons). • Plaques are fairly evenly distributed across cerebral cortex. • Neurofibrillary tangles = collapsed tau protein, which normally functions as scaffolding within neurons. • Early in AD, accumulate in hippocampus and MTL, relating to declarative memory deficits (episodic and semantic). • Hippocampal shrinkage = early AD warning sign • Verification of presence of plaques and tangles (to confirm AD diagnosis) can only happen at autopsy. • 10% to 20% of “probable AD” diagnoses (based on MRI, PET, lumbar puncture, etc.) are incorrect. • Many other conditions (some treatable) mimic AD (e.g., vitamin B deficiency, hypothyroidism, depression) • So better diagnostic tests needed (e.g., PiB imaging on next slide) 119 251 Unit 10.3B fa24 Plaques and Tangles — Hallmarks of Alzheimer’s Disease a) Amyloid plaque (dark center spot) surrounded by residue of degenerating cells. b) Neurofibrillary tangles (seen as darkened areas). (a) Cecil Fox/Science Source/ Photo Researchers. (b) Adapted from Figure 3 of Hardy & Gwinn-Hardy, 1998. 251 Unit 10.3B fa24 251 Unit 10.3B fa24 251 Unit 10.3B fa24 Genetic Basis of Alzheimer’s Disease • Several genes are implicated in AD. • Most progress is in understanding genetic cause of early- onset Alzheimer’s disease (begins at 35–50 years). • Early-onset = less than 1% of AD cases • Caused by genetic mutations that are autosomal dominant (just one mutated gene from either parent will likely trigger early-onset AD). 122 251 Unit 10.3B fa24 Possible Causes of Alzheimer’s Disease • Early-onset Alzheimer’s disease (onset < 60 years; rare = less than 1% of cases) has significant genetic component • Autosomal dominant mutations found in genes coding for proteins involved in amyloid processing are linked to early-onset AD • Amyloid precursor protein (APP), presenilin (PS1, PS2) mutations • Late-onset Alzheimer’s disease (onset > 60 years; 99% of cases) is more influenced by environmental factors • But also linked to ApoE4 mutation of gene for apolipoprotein E • Neurobiological research approach: Study AD-linked mutations to learn about mechanisms of neuropathology • These mutations cause β-amyloid protein to accumulate and cluster into plaques 251 Unit 10.3B fa24 Treatment and Prevention of Alzheimer’s • Cholinergic agonists • ACh has widespread cortical and hippocampal projections • AChE inhibitors (e.g., Aricept) • Methods to decrease β-amyloid accumulation • Aβ1-42 vaccine Leqembi (new AD drug) • Antioxidants • Prevention: remain active cognitively, socially, physically • Promotes neuronal survival and hippocampal neurogenesis • Slows cognitive aging in both healthy and disease states 251 Unit 10.3B fa24 Interim Summary: Clinical Perspectives In Alzheimer’s disease, plaques and tangles accumulate in the brain. • Memory symptoms are prominent early in the disease. • Consistent with finding that hippocampus and nearby MTL areas suffer pathology early in the disease. • Several genes may contribute to an individual’s risk for the common, late-onset form of the disease. 125 251 Unit 10.3B fa24 The brain-changing benefits of exercise (Wendy Suzuki, NYU) https://www.ted.com/talks/wendy_suzuki_the_brain_changing_benefits_of_exercise On YouTube: https://www.youtube.com/watch?v=BHY0FxzoKZE Longer talk: https://www.youtube.com/watch?v=Y0cI6uxSnuc 251 Unit 10 fa24 Interested in Memory Development & AD? If you are interested in learning more about the behavioral and neural aspects of memory development: • PSYC 273 Developmental Psychology (multiple sections every semester) • PSYC 350 Developmental Cognitive Neuroscience (taught in spring by Dr. Guy) If you are interested in learning more the clinical implications of memory development and aging such as Alzheimer's Disease: • BIOL 357 Neural Disease, Degeneration, and Regeneration covers neurodegenerative diseases (including Alzheimer’s and Parkinson’s) in even more depth (taught in fall/spring by Dr. Yu) • Pre-requisites: BIOL 251, BIOL 282, NEUR 101 251 Unit 10 fa24 In-Class Reflection Question: Metacognitive Self-Reflection After self-reflection, answer some or all of these question prompts on Top Hat: • What did you learn in this course? It may help to identify the three most important skills/concepts that you learned and/or experiences that you had in the course. • How have your ideas, perspectives, attitudes, and skills changed as a result of this course? • How will you apply the concepts and skills learned in this course in the future?