- No category
Alzheimer's Disease Training for Healthcare Professionals
advertisement
CFTF: Consultants for the Future Continuing Education for Healthcare Professionals Alzheimer’s Disease and Related Disorders Information and Training 2 Contact Hours vega This course and Consultants for the Future have been approved by: The Florida Boards (Provider No. 50-435) Nursing, Clinical Social Work, Marriage & Family Therapy, and Mental Health Counseling, Occupational Therapy, Speech Therapy and Audiology, (clinical) Massage Therapy (Course No. 3344) Respiratory Therapy and Nursing Home Administrators The Florida Physical Therapy Association (FPTA) Course No. CE24-91509 (Accreditation of this course does not necessarily imply the FPTA supports the views of the presenter or the sponsors.) It is accepted through complementary board approval by the Board of Dietetics and Nutrition . Our DOEA training Provider No. is HH8. The curriculum approval number is HH 10306. (Approval expires and will be renewed by 11/7/2026) Council of Certified Nursing Assistants The Ohio Board of Speech and Language Pathology and Audiology (Provider No. 40-435) The District of Columbia Board of Nursing (Provider No. 50-435) The Alabama Board of Occupational Therapy (Provider NO. 50-435) The Georgia Board of Nursing (Provider No. 50-435) Accepted by the Iowa Boards of Nursing Behavioral Science Examiners for Mental Health Counselors and Marital & Family Therapists, Sponsor No. 1-05, Social Work Examiners, Sponsor No. 334; The California Board of Nursing, Provider No. 04422. The Course meets the requirements of the Minnesota, Ohio, Nevada, and Kentucky Boards of Nursing, and other states by reciprocity. Dr. Linda S. Greenfield No portion of this study may be reproduced without permission of the author and Consultants for the Future. Alzheimer’s Disease & Dementia Related Disorders Quality of life can be enhanced by quality care. This program emphasizes understanding and management approaches when caring for a client with impaired cognition. It has been designed to help those healthcare workers who directly care for persons with dementia. This course has been designed to meet the Florida requirements of F.S. 400.4785 and Rules 58A-8.001 and 58A-8.002 F.A.C. The curriculum is approved by the Department of Elder Affairs, #HHC02. Please read these IMPORTANT INSTRUCTIONS as they contain answers to many of the questions we are often asked regarding home study. You may save this PDF document on your computer and print all or any part of it. You may also return to your account on our website and find it on the course page. In this way the document is available to you as a resource for the future. Notice that there are questions placed throughout the reading material. At the end is an answer sheet. The answers cannot be submitted from this PDF.As you complete the study, you may record your answers on this answer sheet to help you when entering your answers on the website. Once you are ready to submit your answers and complete the course, you will need to sign in to your account at www.consultantsforthefuture.com using your username and password. Click on your name at top right of the home page to access your list of outstanding courses. Click on this course and then scroll down the page to see the list of test modules you need to complete. The questions from the course material you have just read are separated into test modules. Each module must be completed with a passing score of 75% in order to progress to the next module. Your answers are saved when you click on finish at the end of each module. The course is completed once you finish the last test module. If you need to leave the test module before you complete it, record your answers somewhere to enter when you begin that module again. You may refer to the material at any time and you may also study in groups, if you wish. Once you have successfully completed the entire course, you will have an opportunity to complete an evaluation of the course. You will be able to return to your account to view your certificate, which you can print at any time. You receive credit on the date you successfully pass the entire course. For those monitored by CE Broker, we will report the completion of your courses to CE Broker, with the actual date you completed the course. Hours are reported to CE Broker using only your license number, so please make sure you have listed it correctly in your account profile, with any letters followed by the numbers and, usually no spaces or dashes in between. The instructor’s name is Linda Greenfield. She is available to answer questions you may have about this material by phone from 9:00 am to 5:00 pm Monday through Friday. That number is 800-6542387. You can also email her at confut@aol.com and she will respond to your email within 24 hours. TABLE OF CONTENTS Course Instructions…………………………………….………… 1 Understanding ADRD………………………………………….. 2 Communicating with Clients with ADRD…………………………10 Behavior Management…………………………………………… 10 General Problem Solving…………………………………………..17 Promoting Independence Through Assistance with ADLs…… … 21 Developing Skills for Working with Families and Caregivers…… 27 Appendix I……………………………………………………… 31 Bibliography………………………………………………….. … 32 Current Revision: November 2023 1/06 1 Alzheimer’s Disease & Dementia Related Disorders “Mary has just pulled all of her clothes out of her drawers again,” her daughter said with a sigh of frustration. This was just the wrong time to have to deal with dresser drawers of clothes or Mary’s anger that will result when her care assistant tries to put the clothes away. They all knew Mary’s agenda. Mary was packing to “go home.” Yet Mary was home. She just didn’t recognize that fact. To her this wasn’t home and her caring family were mostly strangers. Mary’s situation is not uncommon and neither is anyone’s frustration. Providing assistance with the tasks of daily living can be quite a challenge on some occasions and the task certainly demands skill, patience and as much understanding as you can get when communication skills are so badly impaired by disease. This course offers guidance for those providing direct care. It is created to help those standing at the client’s side wondering how all of the required work can possibly be accomplished in time and still manage to be patient, caring and make the day for the client/client just a little brighter. Module 1: This covers Objectives No. 1 through No. 8. There are 8 questions to this module. Six correct answers are required to reach 75%. Understanding Alzheimer’s Disease and Related Disorders Objective No. 1: Define ADRD and “dementia.” Objective No. 2: Compare the function of the normal brain to how Alzheimer’s disease affects the brain. Objective No. 3: Differentiate how cognitive impairment from ADRD/Dementia differs from cognitive impairment in normal aging. Objective No. 4: Identify the stages of Alzheimer’s disease and how the disease progresses. Dementia, and particularly Alzheimer’s disease, is on the rise. “[Researchers] project the prevalence [of ADRD] will increase 178% among all Americans age 65 years or older by 2060, but Hispanic and other racial and ethnic groups will see the fastest growing rates.” (McNamara, 2018) “Among adult neurological disorders, dementia has the highest economic cost, and is only second to cerebrovascular disease as a cause of death. Alzheimer’s pathology and vascular disease, alone or in combination, account for the vast majority of dementia cases worldwide. (70-80%) The remainder are made up of Lewy body disease (5%) and a large number of pathologies with low prevalence.” (Salardini, 2019) These primary dementias will be explored in this course. First, there are several disease causes of dementia that are chronic and progress slowly, like Alzheimer’s disease, but they are not pathologically the same. These are called “related disorders.” ADRD stands for Alzheimer’s disease and Related Dementias. Appendix 1 at the end of the course has a list of other diseases that create dementia. Dementia is a clinical state characterized by a loss of function in multiple cognitive domains. Common symptoms include memory loss, aphasia (inability to use verbal communication), apraxia (inability to do things they used to be able to do, such as dress or eat, etc.), agnosia (inability to identify familiar objects like their fork or their bed, or even their children), and disturbances in executive functioning (inability to do tasks with multiple steps, like prepare a meal.) Alzheimer’s disease is characterized by a gradual and progressive decline in function. Once a skill is gone it rarely returns, unless the decline is due to some reversible situation, such as drug effect. Another cause of dementia symptoms is called “Lewy body dementia”. With this dementia there is more fluctuation in the symptoms. They may have “good” days when they can do some things, and “bad” days when they seem totally lost. These fluctuations can vary from day to day, hour to hour. This is not typical in Alzheimer’s. Another cause, called “vascular dementia” has more of a step-wise decline. Vascular dementia is most commonly associated with a series of small strokes, although this category is a syndrome of 2 Alzheimer’s Disease & Dementia Related Disorders differing vascular disorders. So, after a mini-stroke, people function much lower, but then they stabilize at that level or might even improve slightly. With the next “mini-stroke” they will be able to do less, but then will again stabilize at that newer, lower level. Vascular dementia has more motor systems, so they might have difficulty using one arm or have one-side weaker than the other. There are many other, more rare causes of dementia. In many elderly persons with dementia, there is a varying overlap of pathologies, so that an individual may have changes associated with Alzheimer’s, along with changes in vascular functioning, along with some characteristics of Lewy Bodies. Each person expresses this differently. In addition, many without noticeable dementia have pathology visible on autopsy indicating an underlying, hidden dementia process. “[A] variable but measurable amount of AD pathologic changes exist in most cognitively intact elderly individuals who undergo autopsy, indicating that AD is a chronic disease with latent and prodromal stages and suggesting that individuals may have varying abilities to compensate, either biologically or functionally, for the presence of AD.” (Montine, 2014) In addition, “Over 50% of all individuals who undergo autopsy and 40% of individuals without dementia have intermediate or high AD pathology.” (ibid) There are over-laps with other pathology. For example, Alzheimer’s has long been associated with neurofibrillary tangles and plaques. The fine filaments of the nerves in some parts of their brains where thinking and judgment are controlled, are tangled in clumps. But scientists can find some neurofibrillary tangles in normal, non-psychotic, aged clients. The plaques and tangles are much more numerous in Alzheimer's clients. Tangles are also present in Parkinson's disease and in Down's syndrome. We know that in dementias there are multiple imbalances in the chemicals that control nerve functioning in their brains, which disrupts other brain chemistry. Alzheimer's is a neurochemical disease. Intense reality orientation will not help. Getting angry and blaming them for mistakes only makes things worse. There are chemicals missing and nerve cells tangled. Their brains don’t function as they did before the diseases. Normal Brain vs. the Brain in Alzheimer’s Disease You can understand the behaviors and symptoms of dementia-creating diseases better if you know more about how the brain work normally. The central nervous system is composed of the cerebral cortex, cerebellum, medulla and brainstem that connect with the spinal cord. This study will focus on the cerebral cortex as this is the part of the brain most acutely affected by the Alzheimer's disease and most related disorders. The cerebral cortex, as a whole, is a vast information storage area. Here is where many memories are made and retrieved. Most of the senses and motor functions are at least interpreted in the cerebral cortex and operations from other parts of the brain are coordinated with the cerebral cortex to get a complete thought or action. The cerebral cortex is divided into lobes. The prefrontal/frontal lobe controls thought. An elderly person with normal prefrontal functioning can think clearly, make reasonable judgments, logical choices, (although a little slower sometimes and a little less so when stressed). His/her personality is much the same as when younger and s/he can recall memories in context with what’s happening. If the prefrontal area is damaged, as it is in Alzheimer’s, the client can still think, but since a lot of memory and some of the mechanisms for processing the information are gone, the thought process may not seem logical to others. Think for a moment about how important memories are. Memories allow us to recognize anything -- even the words on this page. Memories tell us what is good and bad, who we are and what our existence is. Our lives are our 3 Alzheimer’s Disease & Dementia Related Disorders memories. How we have learned to relate to other people are memories. In normal aging, these processes remain intact and functional. If a section of our brain that retrieves and uses memories is damaged and does not work well, the effects on our lives are devastating. The storage of memories is still poorly understood. Although there is drastic memory loss in advancing Alzheimer's disease, not all memory is lost. Memories for affection, friendships, likes and dislikes, etc. continue, although changed. Even throughout dementia a person's experience continues to influence the way s/he feels about him/herself relative to the social environment and this will affect his/her sense of worth, happiness and goals. A person with prefrontal loss is easily distracted and can't keep a thought for long. This part of the brain keeps mental functions directed toward a certain goal. Damage to this area causes the goal to be lost and attention span to be short. For example, it is difficult for a person with dementia to sit at the table long enough to finish a meal. But, on the other hand, it is easy to divert his/her attention when necessary. Another interesting facet to the loss of the prefrontal/frontal area is the loss of judgment; a very complex, abstract thought process. Judgment of right or wrong also arises through the formation and use of memories. Our parents, and then many others, teach us concepts or appropriate behavior or thoughts, with each experience. These conclusions are stored in our memories. A person with memory loss from prefrontal damage will not be embarrassed by sexual, personal, bowel/bladder, or social activities that may be inappropriate, or even labeled “wrong” by some. This person may also quickly change his mood from happy to depressed; from angry to docile. Our emotions and moods are affected by our memories and how we perceive our environment. We often hear, "Dad would never do that if he were himself". And that is true. His behavior was dictated by his life and the programming he received from childhood on. All of this programming was stored in his memory bank and the prefrontal area used these memories, with abstract thought and input from the emotional system, to control behavior patterns. Now, the prefrontal area is damaged and much of the memory is gone. Consequently, his behavior and emotions are different than in the past and not consistent from day to day. With more complicated diseases, such as Alzheimer's, there are few new memories being made to dictate behavior in the future. The parietal lobe largely deals with sensations and spatial organization. Persons who have normal parietal lobe functioning know where they are in a familiar environment and how to maneuver safely. When they feel pain, they can tell you where it hurts and maybe even why it hurts if they remember an injury. This person feels his/her body in space and recognizes that his foot might be asleep and needs to be moved. S/he can tell time and read a book correctly. A person with parietal damage may not know where his/her hand is. S/he can look at it, but may not recognize it as his/hers. S/he may feel an object is touching his/her skin, but s/he cannot distinguish the shape of the object or just where it is touching her/him. The damaged parietal lobe of the brain cannot interpret the sensation of touch correctly. Spatial relationships are not organized when there is parietal damage. If you ask a client with Alzheimer’s disease client to draw a clock, s/he may get all the numbers in the clock face, but cannot put the numbers in relationship to each other. Neither can s/he tell time. And these people will get lost easily. Imagine how frightening it must be to perceive the environment with little organization! Imagine what happens to their orientation when you turn them around in a wheelchair and pull them backwards into a bathroom for their baths. This “lost in space” feeling creates great anxiety. The temporal lobe and the occipital lobe also assist with the senses, particularly the interpretation of the information coming from the ears (temporal) and the eyes (occipital). In normal aging, the person can correctly interpret these senses. They know when they see a mirror that this is a mirror and how it functions. They know when they hear a familiar voice who this person is. Damage to this part of the brain causes errors in the interpretation of sight and sound. There are many behaviors that arise out of this misinterpretation, as the individuals with dementia (as well as those without dementia) tend to believe what their brains are telling them. With the deterioration of their memories, guesses are often wrong. 4 Alzheimer’s Disease & Dementia Related Disorders Mirrors, TVs, and radios all cause confusion because people with dementia can’t recognize what they are seeing or hearing. When the TV news program is displaying violence, this person often concludes that the violence is there in the room. S/he reacts with great anxiety, even though his/her frontal lobe cannot tell him or her that s/he is anxious, or even why. You can see the effects of this anxiety in increased pacing, increased nervousness and a decreased ability to focus. S/he can see, but s/he can't always interpret what s/he sees and may not recognize familiar objects. S/he might look intently at a shoe with total bewilderment and has no idea how to use the shoe. S/he may see a coat hanging on a rack and go up to it and talk to it as if it were a person. A nightlight behind the chair is thought to be a fire. The nursing assistant is thought to be the client’s daughter, but the real daughter is thought to be a stranger. A bundle of bed covers is thought to be a baby. I’m sure you can add your own list of ways things are misinterpreted. There is evidence that vision and hearing are quite distorted. Finally, the hippocampus, which sits deep in the middle of the cortex in the temporal lobe, is necessary for long-term memory. The hippocampus acts as a sorting station for memories -- retrieving those necessary for thought and storing others until needed later. Although that process is slowed in normal aging, it is still very much intact. With concentration, this person can remember that s/he ate breakfast and what food was eaten. They know the date, where they are, what and why they are doing things. They can remember things just read or repeat conversations accurately. In Alzheimer’s disease there is considerable damage to the hippocampus. Some long-term memories that existed before the damage might still be intact (although they often get jumbled), but short-term events cannot be transferred into long-term memory storage. This person cannot learn or learns very slowly. The hippocampus is an area of extensive research in Alzheimer's disease. The vast territory of the cerebral cortex requires extensive communication and networking between the various lobes. Communication happens, to a large extent, through the use of neurotransmitters, the chemicals of neuronal communication. For the cerebral cortex, a chemical that is very important to thinking and remembering is acetylcholine. All neurotransmitters, including acetylcholine, are enhanced or inhibited by a large range of things, including, drugs, food, diseases, moods, beliefs and more. As an example, aspartame (e.g., NutraSweet), a sugar substitute, is known to inhibit acetylcholine, which will make remembering slightly more difficult when intake is high. This is reversible. Alzheimer’s disease is characterized by a loss of acetylcholine which is irreversible and extensive. But imagine how brain function may deteriorate when a person with Alzheimer’s disease is given unlimited diet beverages. Cognitive Impairment of Dementia vs. Cognitive Impairment of Normal Aging You can see that, especially as the disease progresses, there is considerable difference between normal aging and dementia. However, in the early stages of the disease, it is not as easy to tell the difference and more than one elderly person has questioned his own cognitive functioning, wondering if he is normal or not. In normal aging one forgets, but the fact that something was forgotten kind of rumbles in the background until the person remembers. In dementia, the person forgets and soon forgets they have forgotten. The lost data is never retrieved. And normal aging stabilizes for years. It doesn’t keep getting obviously worse. The aging process is very slow. Normal aged people do not lose their ability to function independently. Dementia doesn’t stabilize. Gradually, these people do lose their ability to function independently. Alzheimer’s disease steadily declines over time, so even if there was doubt in the beginning, as time goes on, the doubt yields to the obvious. Normal aging doesn’t involve loss of the ability to use language or to recognize objects or family members, or to correctly use objects. Normal aging is not at all like dementia. People who are healthy and old can remember incredible details and think in very complex patterns. While they might process some things a little slower than they once did, when given that time, their judgment, logic, and ability to use language and do math, etc. is consistent with their total life span. While the adage is true, “if you don’t use it, you lose it”, it is true for all of us at any age. When non-diseased older people allow themselves to become “couch potatoes” with little mental stimulation, they will lose some of their skills. So will a younger person, although not as quickly. A healthy brain, like all organs, needs stimulation to stay healthy. But this is from lack of use, 5 Alzheimer’s Disease & Dementia Related Disorders kind of like muscle weakness arises from too little exercise. A disease process that destroys brain tissue is a totally different process. This course concerns caring for those who have the diseases of dementia. Stages of Alzheimer’s Disease The symptoms of Alzheimer's disease will be divided into four stages for study. This is considered broad staging and some sources teach seven stages. This curriculum teaches four stages, because with less division it is easier to learn and to respond immediately to situations involving different stages. We meet multiple clients in different stages. And often a specific person’s behaviors today are not consistent with the usual stage of behavior for that person. This could mean the client is in pain, or has an infection, or multiple other reasons. Caregivers need to be able to notice the difference and change the approach to match the client’s current stage. Keep in mind as you read, that any disease or change which alters brain functioning will cause similar symptoms. Not all dementia is from Alzheimer's disease. STAGES MILD: Alzheimer's disease usually begins with three cognitive impairments and then progresses to include others. The first three are evident in the beginning of the disease, but may not be alarming enough to cause the client to seek medical evaluation. These three are: difficulty forming new memories spatial difficulty, creating for example, an inability to follow a command despite having the strength to do so, or a tendency to get lost easily, or he is unable to draw maps or clocks, etc.; and an inability to remember names of things or people. He might describe something by function or history or relationship, but not by name. "Hand me the thingamajig you write with." Arising from these three cognitive impairments they might notice that logic and judgment become less acute. Many people can compensate to hide the symptoms, until the disease progresses and socially inappropriate behaviors, mood changes and severe memory loss begins to distress the caregiver. There are emotional responses to these losses, i.e., agitation, irritability, depression or apathy. These may be from the chemical deficiencies that the disease causes in the brain, or they may be the result of a lost body image and reaction to the changes the person perceives in himself. Using normal defense mechanisms, he may tend to blame others for his poor functioning or make-up forgotten facts. For example, he might say, "Why didn't you tell me I had a doctor's appointment today?" "Where did you put my glasses?" We all tend to defend our egos in this way, but with advancing memory loss, this tendency gets more noticeable. Many can still function independently. Some are seeking medical help at this time and some are hoping it will go away. This is sad, because first of all, it appears that our greatest chance for impacting the course of the disease is early, before significant damage is done. Newer research indicates that there is brain evidence of dementia-causing processes years before the diseases are diagnosed and perhaps there is a chance to prevent or slow the progression to dementia. A healthy lifestyle leads to a healthy brain. Many aspects of poor health are now considered risk factors to dementia. The Lancet Commission on Dementia Prevention, Intervention and Care (Hughes, 2020) has now listed twelve risk factors heavily linked to dementia in later life: not completing secondary education, hypertension, obesity, hearing loss, smoking, depression, physical inactivity, social isolation, diabetes, excessive alcohol intake, traumatic brain injury, and air pollution. Not listed in the Lancet paper, but very important, is good sleep throughout life. (Vega, 2018) It is during sleep that the hippocampus restores its capacity to hold short-term memories. Also important are atrial fibrillation (Frellick, 2023) and nonalcoholic fatty liver disease (Kim, 2022). Notice that many of these same risk factors are related to many other chronic diseases. For many reasons, recognizing early mental decline can perhaps motivate people to change their lifestyle and slow the dementia-causing processes. In this early stage, counseling will assist the client and his family to prepare for what is coming and cope with what is. One of the biggest problems in the mild stage is to convince the family and friends to accept the person as he is and not expect higher levels of functioning. Lecturing him to change his behavior only increases his anxiety, reduces his self-esteem and reduces his ability to think clearly. Trying to reason with him may no longer be effective. If the person can keep a personal diary of his feelings and share it, it will help the family understand. There are many things the family can do to help the client cope. Accepting him and loving him even with dementia, helps a great deal. 6 Alzheimer’s Disease & Dementia Related Disorders Planning for legal transfer of decisions is necessary within this stage time frame. Living wills and durable powers of attorney for health care and for control of finances can be signed. Estate planning is very important. Tools that will help in this first stage include many of the ideas we all use to support our own memory: notes, calendars, photos, phones, etc. Others include establishing strict routines that will be maintained as the disease progresses and will serve as memory enhancers. Included in the routine is keeping valuables in the same safe place. The client may falsely accuse the caregiver of stealing and the presence of this routine will offer security. The client will need encouragement to socialize, because it increases anxiety to have to remember all of the social graces and s/he fears embarrassment. Finding forgiving friends and continuing social activities will do much for mental stimulation, self-esteem and quality of life. Humor is much harder to understand, so use it as tolerated. MODERATE: After roughly two to four years, the symptoms of the moderate stage appear. There is more loss in a wider brain area and so more losses of memory, logic and judgment, and more communication problems. The memory loss progresses to the point that bathing, grooming, choosing clothing, dressing, toileting and eventually ambulating skills are affected, usually in that order. These inabilities usually result because the person cannot remember what to do or how to do it (apraxia and disturbances in executive functioning) and s/he becomes frightened or confused. During the course of this long stage, s/he may progressively forget friends, relatives and many personal details. The disease virtually disintegrates the personality. As more brain tissue becomes involved, the neurons in the sensory areas will become impaired, so the person cannot interpret the sensations. Thus, they can’t identify sounds or objects, or remember how these things operate (agnosia). Errors in verbal communication will become more obvious as aphasia develops. Nocturnal restlessness will increase as will daytime pacing. The movement seems to be a necessary stress relieving mechanism. When awake, s/he needs constant supervision. As the disease progresses, as many as 40% of the bedtime hours may be spent awake. This takes a tremendous toll on the caregiver. The person with dementia may burn caloric energy faster than s/he is eating, because s/he cannot concentrate on eating or sitting for long periods. Finger foods become necessary--food s/he can eat while moving. While the desire to be mobile increases, the ability to do so safely, decreases, not only because s/he may wander onto roads, or get lost, but also because a gait disorder frequently appears as the disease progresses. The gait is stooped, slow with no arm movement and mincing steps. Although this specific gate does not occur for all clients with dementia, it is important that you constantly be alert to the risk of falling with any client who has dementia. As the disease advances through the Moderate, Severe, and End Stages, there is an increasing need for monitoring and supervision. As more assistance will be required, it becomes difficult, but important, to maintain the client’s maximum level of functioning. Allow as much independence as possible, but with approaches which will not increase anxiety, i.e.; use yes/no questions, limit decisions, such as laying out two shirts for him to choose from, or buying several sets of the same outfit. Don't expect him to reason, or to remember what you want him to do. He will be in his own time and place and with patience, you may be able to relate to his reality. Fatigue is a major problem and a planned routine with frequent resting opportunities is vital. Delusional ideas, hallucinations (usually visual) and suspiciousness make it more difficult to establish a common "reality". S/he will not believe your reality, which is why reality orientation so often fails. Psychotic symptoms occur in about 50% of those with dementia. Extreme paranoia, wandering, flashes of anger, etc. all complicates the picture. SEVERE: This stage is characterized by severe impairment of cognitive functioning lasting 8 to 12 years with quality health care. This client needs continual supervision and total assistance with daily cares. It becomes very difficult for the family caregiver to provide this without significant help. Urinary incontinence may cause care problems. Incontinence in this client results from two deficiencies. One is not being able to recognize bathrooms, or remember how to remove clothing, etc. The other is due to damaged neurons in the brain that normally recognize the urination reflex and inhibit 7 Alzheimer’s Disease & Dementia Related Disorders it. With damage, the reflex is not recognized, and when not inhibited, urination occurs automatically when the bladder fills. Other behavioral characteristics occur in this stage. S/he may develop continuous, repetitive motions, like: lip licking, chewing, tapping, or walking. These are called “perseverations.” The client seems compelled to repeat the motion. One man would run his fingers along the wall even to the point of bleeding and still not stop the motion. For some, the motion changes. You might hand a client a washcloth with instructions to wash his/her face. S/he could wash one spot over and over until you physically move his/ her hand to another area. "Echolalia" is symptom defined as the continuous repetition of a phrase, word or syllable. Mary is one example. When you approach her, you might say, "Hello, Mary." She will say, "Mary, Mary, Mary, Mary...." for hours until you change the word for her. One woman reads everything: the walls, her chair, her dress, her napkin, etc. She has a monotone, reading voice and she "reads" continually. Sometimes people scream or cry “help me, when you have tried every action to help. Sometimes people make sounds that don’t convey any clear message. Your task is to listen carefully, trying to bring security, safety and comfort to the situation, as much as you are able. For some, there is a driving need for oral stimulation. Every object gets tasted and the appetite becomes insatiable. Sometimes the objects are not food, which creates a supervision problem. This desire to put everything in the mouth is sometimes combined with the compulsive desire to touch every object in sight and usually destroy it. Paper towels and napkins become dangerous as they shred them in tiny pieces, trying to eat some of them. The marked memory loss causes the client to forget who family members are, how to manipulate the environment and who they were. Not every client will exhibit all of the symptoms. Each is an individual with individual reactions to the disease. Some will be collectors; others will follow you closely and not let you out of their sight. Some will have paranoia; some will be depressed. Some will have dangerous flashes of anger and strike out. This course lists only the more common symptoms. END STAGE: The symptoms progress until the individual becomes mute and unresponsive. The ability to feed may diminish to the point that to preserve life a nasogastric (feeding) tube may have to be used. They simply forget how to chew and/or swallow. The most frequent cause of death is pneumonia. Other frequent causes of death include infections, malnutrition and dehydration. Alzheimer's does affect life expectancy and it is a fatal disease. A study reported in JAMA (Brooks, 2020) indicates that, “Dementia may be the underlying cause of nearly three times more deaths in the United States than official records show.” Question No. 1: Which is possible? a. A person, without dementia, was found to have significant Alzheimer’s disease pathological changes in the brain that were only discovered after death with autopsy. b. Patients who have a combination of Alzheimer’s disease, vascular dementia and Lewy bodies all contributing to their dementia symptoms. c. Two patients with Alzheimer’s disease, who have quite different symptoms. For example, one has major language problems and making essentially sounds, but he is happy; and the other can use real words, but is very paranoid. d. All of these possible. Question No. 2: Which of these describes a function of the parietal lobe of the brain? a. Being able to stay focused on a certain goal, or being able to pay attention. b. Creating a sense of morality. c. Interpreting what is seen – such as recognizing a coat hanging on a rack is not a person. d. Interpreting sensations and spacial organization, such as knowing how numbers are arranged in a clock. 8 Alzheimer’s Disease & Dementia Related Disorders Question No. 3: Alzheimer’s disease creates all of these symptoms. Which symptom most closely reflects what we know about damage to the prefrontal lobe? a. An inability to correctly interpret what things are that he sees, (e.g. an inability to recognize a shoe.) b. A tendency to get lost and confused about location easily. c. Socially inappropriate behaviors such as taking off clothing. d. The inability to distinguish the sounds of language. Question No. 4: All of the following describes brain functioning in normal aging except one. Which is a symptom of dementia and is not characteristic of normal aging? a. A gradual inability to recognize family members. b. A very slow, slight change in cognitive functioning that stabilizes for years. c. Forgetting a few things, but in a short time the thing forgotten is usually remembered. d. The ability to remember details and make judgments in much the same way as when younger, although with slower processing time. Question No. 5: Which of these best describes a person in the first stage of Alzheimer’s disease? a. Daytime pacing or nocturnal restlessness with an increased risk of getting lost or falling. b. The ability to compensate for the symptoms so that others don’t easily recognize there is a problem. c. The compulsion to make continuous, repetitive movements or sounds. d. The client is mute and unresponsive. Communicating with Clients with Alzheimer’s Disease & Related Disorders And Behavior Management Objective No. 5: Understand how ADRD affects communication skills. Objective No. 6: Identify strategies and guidelines for verbal & nonverbal communication and for responding to clients who are noncommunicative or non-responsive. Objective No. 7: Recognize symptoms and behaviors associated with ADRD at each stage. How ADRD Affects Communication It is very difficult for the client with dementia to use language appropriately. Remember how you learned language. It was a process of collecting memories. One day you learned the word for “daddy” and another day you learned that saying “I want” would get you things. Alzheimer’s disease is a process of losing access to memories. They can’t find the words to express themselves. They can’t identify the meaning of words you use and they lose the ability to read. When you add that to the multiple other things they forget or can no longer identify and interpret, language becomes more and more dysfunctional. Their whole concept of reality changes and they merge memories from their past with stimuli currently happening. You, the caregiver, can no longer assume that you and the client are perceiving, interpreting, or defining the same reality as you share the same experiences. As the disease progresses, it becomes more and more difficult to use language as your primary form of communication. Yet, know that as the disease progresses, the client’s intuitions outlast his/her ability to use language. He will be able to “read” you very well, but it will be primarily a gut reaction without cognitive interpretation. He’ll know when you are upset, when you are calm, when you are sad or hurried. He just won’t understand as he could before and will simply react. Your anger or rushing will be reflected in his increasing anxiety. Your calm will communicate that “things are OK” and bring him a sense of security. Much more communication will occur nonverbally. 9 Alzheimer’s Disease & Dementia Related Disorders Symptoms and Behaviors Associated with ADRD at Each Stage Communication Strategies and Guidelines Years ago, Naomi Feil created a communication technique called “Validation Therapy” that is still very helpful today. These are differing approaches used with different stages of behaviors the client exhibits. These communication stages apply to those most commonly under our care. Remember that a client can worsen from his baseline stage in a day's time, when there are reversible attributes at play, such as infections, increased stress, pain, etc. Your approach will change as you recognize the change in stage. So first you will learn to recognize each stage and then you will learn which approach works best with each stage. STAGES MILD: A person in the latter part of this stage is basically oriented, but some facts seem distorted, as reason and judgment have been impaired. S/he is very threatened by his/her own disorientation. In fact, s/he can be very negative, even cruel to those around him/her who are less oriented. When the client makes eye contact, the eyes will be clear and bright, but sometimes suspicious. S/he tends to be tense, or anxious looking, moving in harsh, quick, direct manners. S/he can do his/her own personal care, although s/he may need reminders. S/he can read and write, s/he has some ability for humor, and s/he tries to obey the rules. Feelings are threatening to this client and s/he may deny them. Paranoia or persecutionary behaviors appear; e.g., the grandson is stealing the sweater, or there is a man under the bed, etc. This person will cling to personal possessions: a cane, a purse, a doll, a sweater. This is not an easy person to touch or hug. S/he doesn't want you to invade his/her personal space, unless s/he trusts you well. S/he confabulates, making up stories to fill in portions s/he doesn't remember. S/he may hoard, or collect things, such as available shoes, or hiding food in their rooms. Much of the memory may still be intact, but his/her speech may have lapses and repetitions. Those with Alzheimer's disease will have difficulty naming things, thus the sentences seem to ramble and have vague references. Reality orientation will work at times with a person in the mild stage. Reality orientation is given a brief trial, but if the client does not respond or becomes more anxious, then it is not used. Reality orientation will not work past the mild stage. There is no way that with constant reminders of "reality" you can bring back dead brain cells and the multiple memories lost. We all need indirect reminders of time and place, but don't push the point, or you will alienate the person. When a person with dementia asks you to call his spouse, who is dead, don’t say, “Don’t you remember that she died in 1962?” You might say, “Are you missing her now?” The person in the mild stage primarily needs guidance. S/he still has many capabilities to draw from. It seems harder to remember the steps or to remember what his/her goal or intent was. S/he might lose information given to him/her, so constant repeating of the day’s events, or what needs to happen now, etc. are necessary. Validation therapy teaches that in old-old age, a developmental task is resolution: resolving life's many conflicts. In order for resolution to occur, the person's feelings, derived from memories of these conflicts, must be validated. Feelings don't have to be based upon "reality". We can feel fear when there is nothing to be afraid of. We can feel happy over a happy memory. As we validate the clients’ feelings and memories, we restore their dignity and self-esteem. We can help them in resolution by putting their feelings into words they can't find on their own. As we empathize, we build trust. Trust brings security and reduces anxiety. To empathize and validate, we show we care. We do not scold, argue, or insist that the client should or must follow our reality. We become non-threatening, nonpunishing and non-patronizing. In this stage, you can gain insight into their behaviors, if they trust you. Although it is always helpful to be sensitive to your clients’ feelings, in the mild stage, talking directly about feelings might be threatening. This client is still quite sensitive to the pain of failure, or the risk of appearing confused. They might not want to talk about their losses, unless they know you well. Avoid feeling type questions, unless the client expresses them and wants this attention. Give as much positive feedback as you can to help them feel more secure in your presence. Be there with the assistance they need, but with the respect for those skills still remaining. 10 Alzheimer’s Disease & Dementia Related Disorders Touch is a very important communication tool in the later stages. In this stage, both eye contact and touch can communicate compassion and caring, but, again, you need to build trust first. Touch them when they trust you and not before. A cane can become a powerful weapon and you may become the target of confused aggression in a very painful way when trust does not exist. Protect yourself as well as others. Remain conscious of the cane, attend to the signs and symptoms of anxiety or distrust, and respect the client’s personal space, which includes the range of the cane. You build trust in this mild stage the same way you develop trust with most people. It comes from respect, being treated with dignity, being consistent in your moods and behaviors, not communicating judgments, and accepting the conditions and experiences as they arise without alarm or aggression. HOW TO USE STAGING TO HELP YOU CONNECT WITH THE CLIENT This section of the course is designed to help you recognize which stage your client is in and to use communication tools and approaches that are appropriate for that stage. Thus, when interacting with each client, you need to be able to access this information from your own memories. This course will share one method used to help you remember this information. As you read the descriptions of the common behaviors of each stage, try to recognize a client you have worked with, who is demented; who "fits" the description of that stage. This personal experience can act as your own personal “standard” for each stage. It will be easier to remember the behaviors of the stages, if you can compare them to your “standard” client. The first stage will use Mildred (my standard) to help you understand how to use your standard. If you can say, "this looks much like ‘your standard’", then the client is probably in the mild stage. Do this for each stage. Of course, at the professional level, there are assessment tools that can be more specific. The downside to this when providing direct care, is that a person’s stage can change as reversible conditions (i.e., increasing anxiety or infections) compound the problem and the disease process progressively declines. For the direct care worker, you need to know where the client fits into the staging process in this minute and respond to that on-the-spot assessment. It is easier with less stages. Mildred has behaviors and tendencies described in this section as the Mild stage. She is usually very pleasant, but if you challenge her elements of nonreality too much, she comes at you swinging. Then she remains very suspicious and uncooperative for a long time. She is always carrying something, her glasses, her sweater, etc. and if her hands are free, then someone has stolen whatever she is looking for. She can remember the day of the week for several hours, but she also has elements of nonreality. For example, she says there is a cat in her room (there isn’t), which is why she hides food from her dinner. She must feed the cat or it will die. Following is an example conversation with Mildred, using validation/language therapy Mildred: (The caregiver is assisting her with eating.) I can't eat. I'm choking. I'm choking. Caregiver: (Who observes no evidence of choking) What is causing you to choke? Mildred: I can't swallow. You're choking me. Caregiver: What's preventing you from swallowing? (Still offering food slowly, but without difficulty.) Mildred: I don't know. I always choke. Caregiver: Is there ever a time when you don't choke? Mildred: When Billie stays with me, I'm OK. Caregiver: If Billie (her son) were here, you wouldn't choke? Mildred: Not if Billie was here. Caregiver: Does Billie make you feel more secure? Mildred: Oh yes. Billie's my boy. Caregiver: Is there any way that I can help you feel more secure while Billie is not here? Take a moment to consider how this conversation would have gone without validation therapy. When Mildred said, "I'm choking", the classic response would be, "You're OK, Mildred, eat your lunch." When Mildred's sense of insecurity was ignored, she would have continued to say louder and louder, "I'm choking, I'm choking." This caregiver was acknowledging the insecurity and helping the client express 11 Alzheimer’s Disease & Dementia Related Disorders her needs. This is communicating respect, dignity, non-judgment and acceptance, while helping her feel more secure with the lunch process. There will be some differences in the way you use language with a person with mild dementia versus a cognitively intact person. Clients frequently have difficulty retrieving specific words. Guess at what s/he is trying to say, "Do you mean_____?" or supply the missing word. Sometimes it helps to describe the object or demonstrate the use of the object if the word doesn't seem to have meaning to the client. It will help if you minimize the use of pronouns. Instead, repeat the name or noun each time. Topics will be focused to situations in which the client is involved or are directly observable. Abstract conversations will be difficult to follow. Nonliteral terms are a part of our speech, but will be difficult for this person to follow. Don't say, "Let’s get you squared away." Say, "Let’s go to the bathroom.” Always establish friendly eye contact before initiating any conversation with any confused person. The more demented the person, the more important your nonverbal expressions become. Don't agree to things you don't understand. If the client is not making sense, repeat key words, try to connect with the feelings and search for important clues to understand their map of reality. Be patient. All the great communication techniques in the world will not unlock every conversation and make it meaningful MODERATE: Disorientation is more pronounced, so that clock time has very little meaning, as do facts, names or places. The time and place s/he is oriented to, wherever his or her memories lead and that becomes blurred. S/he can have mixtures of various pasts, so that s/he is caring for his/her son at age 7 and his/her son's son at age 10, in his/her memory. S/he can be interacting with you (present time) but you are part of his memory (1930s). S/he can still talk and use words, but what s/he says may not be rational, nor will s/he follow your line of thinking. Often his/her words are muddled and not understandable. S/he tends to use body motions, rhythms, and symbols to communicate more than before. S/he cannot fill in missing information to aid in understanding, which means others need to guess more often. Pronouns are helpful in this stage, as the vague reference can be used to validate feelings. There are other behavioral characteristics of this stage. Many clients are incontinent and some of them realize they are so. They usually require guidance and assistance with ADLs (activities of daily living), as memory loss is so extensive that the "how’s" of doing cares are lost. So are personal items, as he is continually losing things; slippers, canes, food, without concern. He moves much slower than in a mild stage. He can now sit for longer periods, more or less relaxed. He won't always sit, however, and his tendency to get lost will make escape from the home a problem. He can sing and laugh, but not always appropriately to the environment. When asked to do so, he can make eye contact, but most of the time he looks downward or inward. Feelings are freely expressed and he responds to your nurturing with smiles, hugs, etc. CONNECT WITH THE CLIENT IN THE MODERATE STAGE . Lucille is the standard this curriculum will use as an example of the Moderate stage. One of her difficult behaviors was her frequent desire to escape from the house and she tended to get lost. During those times when she was content to stay, she took paper, keys, silverware, or whatever objects she found and moved them to somewhere else, immediately forgetting where that was. Restoring order after Lucille had been on her own was difficult. A common agenda was to have to catch the bus to go to Georgia, which is why she tried to leave. Because of her tendency to create chaos, people reacted, usually as they would if she were a child: "Lucille, leave those papers alone." "Lucille, come back here." Or they might approach her as she is shredding the flowers and grab them from her hands. Although the caregivers knew better, they forgot that she was not in touch with reality. They reacted as though Lucille was aware that what she was holding were flowers and that she understood that she was shredding them and that this was wrong. In all probability, Lucille knew none of those things. The flowers might be green beans, which she was snapping in preparation of lunch, in some memory long past. Reality orientation in advancing dementia is very seldom effective. Yet, years of conditioning cause caregivers to continue to use it even at times when they think they aren't doing so. "Jane, don't pull all your clothes out of your drawers. There is no reason to pack. You are not going on a boat trip.” "Mary, leave your clothes on. People can see you." "Marge, don't eat Jim's food. Eat your own food." All of these are examples of reality orientation used to control disruptive behaviors. None of them worked. 12 Alzheimer’s Disease & Dementia Related Disorders Jane, Mary, and Marge were simply not aware of present reality, nor could they respond. The only thing really communicated with these words was the emotional overtone of reprimand and failure. Communicating with a client assessed to be in the moderate stage will still use the principles of validation therapy, but usually modifications will need to be made. Before you can enter his/her time and place, you need his/her attention. Touch will not only get his/her attention, it can be a communication of caring, increasing security. Touch of any type needs to be professional and appropriate. Steps need to be taken to ensure that touch will not spread infectious organisms. It is usually safe to touch the arm softly. As you become safer to the client, a gentle hug can be a valuable experience. An arm around the shoulder can offer careful guidance. Except for personal care, it is rare that touch needs to be more extensive. Touch is well received and should be done caringly, often. Then get eye contact. Use words sparingly until these two steps are accomplished. If you do not touch and use eye contact, you will probably waste your words, but increase anxiety producing stimuli, in your environment. As Lucille is heading for the door, the caregiver may yell, "Lucille, don't go out that door!" Lucille's pace would only increase. There really is no indication that she comprehends that she is being addressed, or that the message is of any importance. As much extra work as it seems (but it isn't because you'll be chasing her out the door, anyway), the correct approach is to catch up to her, touch her, match her pace in walking, and either divert her attention, or cause her to stop and look at you, or enter into a conversation with you. At any rate, your expression and tone of voice should be pleasant, caring and inviting. You want her to come with you, not run from you. The ability to focus is limited, so conversations won't be long. You may only learn a clue to the behaviors at times. Feelings about missing loved ones and life experiences are more easily understood. In your approach to those in the moderate stage, repeat key words and validate their feelings. Repeating familiar prayers, or singing simple songs might promote a connection. Music used as therapy can engage and connect people. You often obtain a smile or recognition as you dance a few steps or sing a few lines, encouraging the person to join you. Following are several brief examples communicating with those who are assessed to be moderate. It's 8:00 P.M. Harriett is sitting in her chair, waiting for bed. Harriett: I'm so tired! Oh, I'm so tired. I want to go to bed. (She has been repeating these words off and on over the last half-hour.) Caregiver: (Making eye contact and knowing that Harriett is seldom oriented, and ignoring the desire to interject pieces from her own reality into Harriett's) Are you very tired? What causes you to be tired? (Notice the caregiver didn't say, "We’ll be putting you to bed, soon. Be patient. Harriett: I've been sewing all day. I made a thousand dresses. I'm so tired. Caregiver: You must feel exhausted. Were you a good seamstress? Harriett: Yes, I was. Caregiver: You have much to be proud of in your life, don't you, Harriett. Harriett no longer repeated "I'm so tired", but instead continued to talk, mostly to herself, about sewing. It's 1:00 a.m. and a client has been yelling "help me" from his bed for some time. The family has been in his room frequently to try to assist, but within minutes after they leave, he continues to cry, "help me." This is not a client who will usually enters into a conversation. Neither does he usually cry out. The caregiver was aware of the client’s previous religious perceptions. Dan: "Oh, God, help me. Help me.......Help me.... God, help me" Caregiver: What is wrong, Dan? What kind of help do you need? Dan: You must have heard my prayer. Caregiver: Were you praying? What were you praying? Dan: I asked God to forgive me. I've been so bad. Caregiver: Are you feeling guilty? God tells us He will forgive us. He is very loving. Dan: Yes, I know. Caregiver: I will pray that God will send you peace. Can you sleep knowing God loves you? Dan: Yes, I think so. (He was able to sleep). 13 Alzheimer’s Disease & Dementia Related Disorders It is 2:00 in the afternoon and the client is sitting without anxiety in her wheelchair. Caregiver: Here is your medicine, Tillie. (A pill) Tillie: Oh, I can drink it. It's so sour. Some people put sugar in it, but I don't. I like it just as it is. It's just delicious. Caregiver: (Putting the pill and water into the client's hands and making eye contact. Her tone of voice is slow and kind.) Take this medicine.....Take this. (Gently guiding Tillie's hand toward her mouth.) Thank you. What is just delicious? Tillie: That drink. That pralink. You drink. It's delicious, but it's sour. My yes, it's sour. Caregiver: It's sour, but you like it. Did you drink it often? Tillie: Oh yes, whenever there were lemons--just a little lemon, but no sugar. Caregiver: Are you talking about lemon water? Tillie: (Eyes brighter) Yes. Caregiver: I like lemon water, too. Did you used to raise citrus trees? How many did you have? SEVERE: This stage was described by Feil as “perpetual motion". The name fits the behaviors well at the beginning of this final stage. By the end, the person lies motionless. It is becoming much more difficult for this client to process incoming sensory stimuli, and in his/her attempts to sort through the many sights, sounds, and touches s/he can no longer interpret, his/her anxiety levels rise sharply. In this stage there are more catastrophic reactions to rising anxiety (such as striking out or becoming combative) and more situationally inappropriate behaviors (such as using a flower pot for a toilet). At the front of this stage, s/he may be restless, pacing, and unable to sit still. Even if restrained to a chair, s/he is in constant motion, leaning over to pick up seen and unseen things, moving hands and feet, constantly. (Restraints should be avoided, if at all possible). Incontinence is now constant and s/he is unaware of it. S/he may also be unaware of the need to go to the bathroom, but his/her behaviors show an increased anxiety as the bladder fills. His/her face lacks expressions, although s/he may laugh outright without apparent reason. Eye contact is rare, but possible for brief seconds. Any sexual feelings will be uninhibited, as will most other behaviors. This is the stage of “total care” as the client need someone to provide for all of the activities of daily living. Language skills become severely affected. The tone of your voice and the speed of your speech will communicate many attitudes, but the words themselves will not be understood. S/e is very much in his/her own time and place, but will use symbols and motions to communicate memories s/he may be having. Words will be single, perhaps two or three at a time, on occasion. S/h doesn't talk or listen to others, except for very brief reactions to your concentrated efforts. Many clients in this stage develop echolalia, repeating the same word over and over. In this stage, verbal language skills will be used less and more emphasis will be placed on imitative movements, touch, music, and control of environmental stimuli. Repeating key words will help. CONNECT WITH THE CLIENT IN THE SEVERE STAGE The example "standard" used by this curriculum for the severe stage, by which you can compare other clients to learn which stage is involved, is Eileen. Eileen paces almost constantly. Seldom is she still for more than 5 minutes. Fatigue is a major problem and the caregivers work hard to create an environment that allows her frequent rest. Although she makes rather constant, low level, non-annoying sounds, a word or two that is understandable is sometimes said. In fact, on very rare occasions she says an entire sentence, which surprises the caregivers so much that they spend the day asking each other, "Did you hear what Eileen said?" Possible problems are assessed by her increases in pacing, reduced napping, louder constant verbalizing, etc. Her reality, as is true of others in this stage, is very fragmented now. Memories are pieces coming and going without order. We'll watch her pick up many objects and look at them without recognition, only to lay them down again. Touch is vital in this stage and will be your primary communication tool. Professional touch takes into consideration the person’s personal, cultural and religious preferences. Eileen is hugged repeatedly, almost every time anyone approaches her. She readily returns the hugs and the hugs are comforting to both parties. She loves to hold your hand and walk with you, and if you try to leave, there is a brief 14 Alzheimer’s Disease & Dementia Related Disorders moment of separation anxiety. Much like an infant who does not understand language, people in this stage, like Eileen, are very sensitive to emotional clues. They will perceive if you are afraid of them. They will feel if you want to be with them. They will intuit if you are angry with them. They will recognize if you are anxious, even if they are not the cause. But they will not be able to analyze or understand these feelings. They won’t be able to differentiate which feelings are yours and which are theirs. They will just feel it without any recognition of the process. You are no longer a worker in a home. You are the mother/father figure. That is, the client can find comfort in you, or greater anxiety. Mimicking motions will be another vital communication tool. Mirror what the client is doing, with the same emotional level and the same intensity. You are communicating empathy. As you mirror the movement, keep trying to guess the right feelings. The client will let you know when you guess right. He will notice you, or stress will decrease, or the movement will stop, or sometimes the client will speak. If you are wrong in your guessing, the client will continue to ignore you. As another example of validation/language therapy in the severe stage, consider Hazel, an 87-yearold Alzheimer client. Unlike Eileen who was passive and easily followed the guidance of the caregiver, Hazel was a challenge. With the standard approaches of the past, she was very combative on many occasions. She would not let many of the caregivers touch her, unless she trusted them and she did not trust readily. As she would escape from the house periodically, it was difficult to bring her back in, because she would ignore the caregiver’s presence and conversation, and if anyone touched to get her attention, she would swing. Typically, her return to the building was a forced, unpleasant situation. She did respond very positively to validation/language therapy. The more she could be validated, the greater the trust. When she trusted the caregivers, they could work easily, because they had her cooperation. With trust and validation, many heath workers could smile, sing, and walk hand in hand with her. However, in a flash, she would revert to striking out, when any one person approached her too quickly, or in any way reprimanding, anxious or afraid. The following example is of validation therapy. Hazel is found at 10 p.m. walking in the hall, appearing very fatigued and holding a blanket from her bed wrapped tight like a baby bundle. She is in her nightgown without slippers, because she was in bed only a few moments ago, but failed to sleep. She is talking quietly to herself, but the words can't be understood. The caregiver approached her and walked beside her without touching her. She concentrated on mirroring Hazel's rate of walking, head position, arm position and attitude. After a few moments of walking the caregiver said, "Hello, Hazel. Is this a baby (indicating the bundle)?" Hazel stopped and made eye contact with the caregiver. And then she continued walking. The caregiver, walking with her, said, "Is the baby not sleeping? Hazel stopped again to look at the caregiver with an expression of understanding. The caregiver said, “You must be exhausted with all of this walking. Can I hold your hand and help you? She slowly approached Hazel's hand with her own and Hazel held it tight. They continue to walk, but now they were close and Hazel allowed the caregiver to lead. As they walked toward Hazel's room, the caregiver said, "You must have been a very good mother." She starts to softly sing a lullaby and Hazel's pace slowed and she smiled. In the room, the caregiver said, "Let me help you lie down. You are so tired." She does not remove the blanket bundle. Once lying down, the caregiver begins to lightly massage Hazel's temples, forehead and neck, slowly repeating, "You are so tired. Close your eyes. Close your eyes. Go to sleep." Within five minutes, Hazel is asleep. COMMUNICATING WITH THE NONRESPONSIVE CLIENT End stage: At the end of life, this person may be called "vegetative", although that term is dehumanizing. This person may not show any recognition of visitors, family, time or place. Movements are flaccid, with little attempt to control them. S/he doesn't speak. Usually his/her eyes are closed, or when open briefly there is no eye contact. If there are emotions, they are not exhibited through behaviors. However, s/he might respond to touch, tone of voice, music, etc. Massaging hands, feet, backs, etc. with lotion seems enjoyable, physically beneficial, and offers a time of connection. There is testimony that these behaviors are capable of eliciting a response—a movement, a sound, a noticeable relaxation. We must treat this person experiencing brain failure with physical and sensual comfort and dignity. Soft, caring touch is the most obvious way to do this, although the sounds of your voice can be 15 Alzheimer’s Disease & Dementia Related Disorders soothing, even when words are meaningless. Acknowledge with the touch of your hand and the sound of your voice that you are there and that you recognize that they are there, too, still among the living. Consider a sample client named Gertie. She lies still in bed until she is moved. When positioned in her chair, she lies in the same position. Eating seems to be a reflex. She will not open her eyes to her name, or to most touch, however, the touch of the spoon to her lips may give a brief peek to blank eyes. Out of love for Gertie, the health workers and family are encouraged to offer frequent loving touch and stroking, and to tell her stories of the family, or just talk to her. They know her favorite music and can play it softly at times. The words don’t matter, but this communicates their presence with her. Visualize this nonresponsive client as someone who can sense, even though s/he can’t respond. It is no longer possible for the client to interpret those sensations, yet the skin is still feeling, the ears are still hearing, the eyes are still seeing, etc. There is some evidence that on some level there is awareness. One body of evidence that supports this is the rise in the death rate when people are moved from room to room in long term care. There is some sense of security that comes from familiar surroundings. Question No. 6: When your client doesn’t respond to a caregiver’s verbal message, which of these would be the least desired reaction of a caregiver? a. Find a way for gentle touch and make eye contact and then repeat key words. b. Give up and ignore the client’s scenario. c. Guess what the client might be feeling and put that into words, “Maybe you are sad right now. Can I sit with you?” d. Mimic what the client is doing (e.g., pacing), with empathy and a desire for connection. Question No. 7: Which of the following communication problems is NOT typical of ADRD? a. A loss of memories creates a loss of words and their meanings. b. Dementia causes a muscular weakness so that the person cannot move his mouth correctly to form sounds. c. Memories from past and present events become jumbled so the client’s concepts of reality change, and so does any communication describing that jumbled reality. d. Words become sounds that their brains cannot interpret. Question No. 8: If a client is assessed at communication-stage two or beyond, which would be the most effective strategy to enhance communication? a. Continually remind the client of the time and date and where they are. b. From a distance, give the client verbal instructions of what to do. c. Get eye contact and touch to allow the client to attend to your message. d. Just ignore this client because beyond stage two he won’t understand anyway. Module 2: This module covers the information in the second part of Objectives 5 through 12. It contains twelve questions. Nine correct questions are required to reach 75%. Objective No. 8: Develop a general problem-solving approach to challenge behaviors. Objective No. 9: Consider specific strategies and techniques for dealing with challenging behaviors. General Problem-Solving Approach There is no “one-size fits all” approach to the client with dementia. Using an approach that usually works in the mild stage can totally fail in the severe stage. Treating clients within the mild category in the 16 Alzheimer’s Disease & Dementia Related Disorders same way you would treat a client who is staged as severe, will insult them and cause them to stop trusting you. But there are some basic concepts that work for the majority. Become conscious of your attitudes and emotions. Even if you are upset at something in your personal life, the client with dementia will sense that and become anxious as a result. Do everything you can to be calm, peaceful, pleasant, and patient. Show respect at all times. Try to listen to the client’s underlying emotion, even when words or facts don’t make sense. The emotion is true. Respond to it. That is an act of caring and it will help increase security. Take time to carefully assess the current stage of function. Stress, anxiety, drugs, etc. can decrease his/her ability to function. You need to be able to adapt to the changes. Interact at the stage that works. One man would constantly get down on the floor and work with his hands in the air above him. It was a battle to get him off the floor that went on for months. Finally, the caregiver got down on the floor beside him and starting moving her hands in the same way for several minutes. Then the client looked at her and made eye contact. She responded, “What are we doing, Jim?” In a moment of unexpected clarity, Jim responded as if it was an obvious fact, “Changing the oil.” He would never have been able to reach that level of functioning without a sense of security and low stress. Now, it was easy to respond to his reality, instead of making him respond to theirs. Try to reduce the client’s anxiety. Interventions are those that might: 1. Provide less stimuli which is creating anxiety or is more than s/he can cope with; and/or 2. Increase his/her sensory input to include more cues for appropriate behavior; and/or 3. Provide items that increase his/her security;and/ or 4. Respond to him/he as a person with feelings. These will be the foundation for the suggested interventions. REDUCE STIMULI CREATING ANXIETY When you can determine what the offending stimulus is, you may be able to remove it. Does he become most upset and angry when trying to get dressed? Is it frustration that he can't remember how to work buttons? Obtain pull over shirts, or suggest several sets of the same clothing so that he is not frustrated trying to choose what to wear. Is a perceptual disturbance (an illusion) resulting from the TV, so that he thinks people are always talking about him? Turn off the TV Reduce environmental static as much as possible. The anxiety may be coming from the bombardment of sights and sounds, many of which are being misinterpreted or seem too fast to process. Frequently aggressive behaviors occur when there are loud noises, children squealing, loud talking, alarms, clapping during music, announcements on the TV, etc. Reduce the noise levels when possible. Keep colors soft and subdued and lighting intense enough for vision, but soft and indirect. Use soft, textured murals instead of pictures that are too stimulating or can be perceived as real. Does he play with his food, or throw it on the floor? Maybe the decisions are too many. Serve him only one food at a time. When increased sensory stimulation is desired, provide methods that are comforting; such as listening to soft music, watching the birds at the feeders, and pleasant tastes and smells of his past. Maintain stimulation at a slower pace. The client's routine is extremely important. Even small changes can drastically upset a confused person. As cheerful as many try to make holidays, the decorations, increased activities and visitors, etc. can be disastrous for a person who is forced to rethink everything. In general, create an environment that is very routine, stable and unchanging, with limited decisions to be made by the client. The more stable the environment, the more stable s/he will be, because s/he uses clues from the environment to tell him or her how to act. Fatigue certainly increases anxiety, making all stimuli more difficult to deal with. The client should be provided with frequent rest, or time out periods, at least once in the morning and once in the afternoon. These may be periods sitting in a reclining chair listening to music, or just napping. Without these quiet times, the day's demands compound, so that by afternoon, the client's coping mechanisms are overwhelmed and anxious pacing escalates. By nighttime, the stress threshold has been crossed and dysfunctional or catastrophic behaviors appear. The client, who by this time is excessively fatigued, is unable to sleep or even remain quiet, sometimes even with heavy medication. S/e needs short rest 17 Alzheimer’s Disease & Dementia Related Disorders periods throughout the day and many cues that night is approaching, so s/he can go through a "winding down" routine, which we all go through before we sleep. Diversion may work to reduce some stress. When using distraction, be very careful that you are not rewarding a bad behavior. This would be behavior modification in reverse. For example, a client is becoming upset and you want to distract him by offering some favorite food. If food is a reward for this person, you will have rewarded a "bad" behavior. Be sure he is doing something desirable before rewarding him, or use distracting methods that are not particularly rewarding. INCREASE SENSORY INPUT Many refer to increased sensory input as providing cues, or "cuing". For the client with impaired memory, we need to provide similar cues in multiple ways, repeatedly, using several senses simultaneously. At the same time, we should concentrate on reducing any cues that are irrelevant. For example, if we want our clients to know when it is bedtime, we can provide visual cues (dimmed lights), auditory cues (lowered noise level, or a tape with the quiet sounds of nature playing) and kinesthetic cues (the feel of bedding, and use of beds only for night and recliners for naps during the day). To use redundant cuing in an effort to help the client find his room, we might label his room with a color coding (his room is the blue room) and put his name in large letters on the door. The more cues, the greater the chance we may be successful. For people who can still read, cuing is easier. Instructions, sequences, appointments, daily schedules or tasks, etc., can be written down in key places and the client can read what s/he doesn't remember. Interventions for the 'sundown syndrome' will be included under this category of increasing sensory input. Sundowning is the tendency for some demented clients to become agitated and to wander to more extremes as night approaches. Some studies indicate that those most susceptible to nocturnal delirium are clients who obtain most of their sensory input visually. As the environment becomes darker, visual input decreases. One classic study reported by Beck et al (1999) involved placing clients with a history of sundowning into a darkened room, early in the day before fatigue became a factor. In every instance delirium appears within an hour. It disappeared in about an hour after the client was returned to the sunlit environment. If visual cues are important, then we need to help supply them, by turning on lights before it becomes too dark, making sure lighting is adequate and using nightlights. Nightlights can also serve to remind the client it is night. If the family can use nightlights to provide care, there is no need to turn on overhead lights, which may be an irrelevant cue indicating it is morning. Or, a sensory detected low-level light can be installed close to the floor. When the client’s feet approach the floor, the light automatically goes on. This allows more safety when going to the bathroom, but more darkness to promote sleep. There are other sources that can be misinterpreted. We have so many irrelevant cues in our environments, it is sometimes very difficult to see the client's world as s/he sees/hears it, especially when one considers the degree of mis-interpretation/ delusions, hallucinations, etc. INCREASE SECURITY Always seek to maintain the client's dignity. Use their reality and not yours. This person cannot decipher appropriate from inappropriate in the later stages, so don't judge behaviors as such. Security is hard to achieve in a confusional state. Music therapy can be very effective. Soft, slow music can be calming and relaxing, allowing good feelings to increase the sense of security. Nature is very healing and relaxing. Or ask the family to make recordings of the client's favorite people talking about the past, loved ones, family anecdotes and bestloved experiences. Then, play it when the primary caregiver is out and the client is depressed or overly agitated. The recording will sometimes calm him down, even though the same one is played over and over. If there is visual memory loss, he will not know the person is not there. Not only is this usually an effective intervention for problem behaviors, it also treats social isolation. Even when we cannot reduce anxieties, or provide enough cuing for them to understand us, we can still intervene by responding to their feelings. Emotions are communicated even in the last stages of aphasia. One lady named Sarah approached a nurse, apparently very upset. She spoke in "word salads", words that made very little sense. But as the nurse listened to her, she sensed her discomfort, 18 Alzheimer’s Disease & Dementia Related Disorders because Sarah’s eyes and nonverbal actions indicated she was upset. Also, ever so often a word or short phrase would come through the string of mixed-up words that had similar meaning to other phrases she used. "Terrible!"......"Just awful"......"Glad I wasn't there". Although the nurse had no idea what she was talking about, nor did she know if it was real or a delusion, she responded to the emotions. "Something has upset you, hasn't it?" That's when Sarah started crying. The nurse sat with the woman who was confused for a few minutes more, just listening and holding her hand. Typical of dementia, Sarah became distracted in a short time, was bored and probably couldn't remember what they were doing anyway. She walked away with a completely different mood. Had the nurse reacted with any other response except to consider Sarah’s feelings, or her need to communicate, the reactions could have been increased anxiety, anger or defensiveness, and certainly there was no gain in trust of the nurse. Your approach to a confused person is very important. Patience, understanding, tolerance, consistency, kindness and consideration are only a few of the qualities desired. THE ABCs of PROBLEM SOLVING When you are trying to determine what approach might work, remember the ABCs: A is for “Antecedent” which means you have to consider what happened immediately before the behavior. B is for “Behavior” which means you have to describe the behavior completely. “He got angry,” isn’t enough. That’s a conclusion. Describe how he moved. What he said. How he looked, etc. And C is for “Consequences”. How did the people in the room respond? Or what kind of reinforcement did the client receive? Try to find a pattern. Try to find the stimulus that led to the problem behavior. Get as much information as you can about the problem. This will help guide you as you increase security and provide redundant cuing. For example: Marge has no awareness of her need to urinate and she is incontinent. But she is aware of her physical discomfort when her pants are wet, so she removes her clothing. These are conclusions The problem-solving process began with evidence you found. This is (A). You often find her standing in the living room totally naked from the waist down, and when you find the clothing, it is wet with urine. (B) To elaborate on Marge’s behavior, you might write that when you take her to the toilet, she looks at the toilet without comprehension of what you want. Even if you help her remove clothing, she cannot comprehend how to urinate. But she does know how to take off her pants and she does so without regard to where she is. (C). There have been several embarrassing consequences, including the young grand-daughter encountering her half naked grandmother unexpectedly. With reactions of alarm, the client was immediately aware that something was amiss, but unable to process this information to know why. Her increased anxiety was noticeable after the granddaughter’s alarm, but not before. The family and home health workers talked over the idea of using adult diapers. They watched to see how behaviors changed. Again using the ABCs they could conclude that this remedy was effective. Specific Strategies and Techniques for dealing with Challenging Behaviors: Behaviors that indicate the client is having difficulty interacting with the environment include: repetitive behaviors, catastrophic behaviors, and situationally inappropriate behaviors. Repetitive behaviors include symptoms such as restless pacing, reduced eye contact, "shadowing" or closely following another person, or behaviors such as rubbing, clapping, etc. These types of behaviors may indicate the person cannot access enough sensory input and the client is searching for security. You might try to provide a fulfilling activity, which may mean you start a project and then let the client complete it easily. Success increases security. You might need to define the environment more by identifying where he is and what is happening, e.g. "Here is your room at the end of the hall. This is your chair that you always sit in. You can sit in it now, if you would like to." Catastrophic behaviors include aggressively striking out, or fighting, emotional outbursts, screaming, etc. These seem to indicate that the demands placed on the client exceed his/her capacity to cope. Catastrophic reactions frequently occur when something has interfered with the normal routine. Situationally inappropriate behaviors include eating nonfood, urinating in flowerpots, removing clothing, destroying paper napkins all over the room, etc. These behaviors suggest the client is 19 Alzheimer’s Disease & Dementia Related Disorders misinterpreting sensory input, maybe because there are not enough cues for him or her, or his/her sensory capacity has decreased. One very common expression of intolerable anxiety is aggression. Many studies have been done to learn the factors of aggression. The lower the cognitive status, the greater the risk of aggression, until the last, mute stage. The older the client, the higher the risk. Agitation, anxiety and insomnia account for most of the reasons for PRN drug administration. Most aggression does not just happen without warning. There are common signs to watch for which indicate anxieties are building. For example, most people with increasing stress and anxiety (confused and lucid) will raise their voice and talk faster. The body positions will be tight, with clenched fists, or a tightened jaw, increased fidgeting or pacing. If the client still uses language, s/he'll ask more questions when anxiety is building, e.g., "Where's my sweater?" "Who are you?" As emotions intensify, s/he'll refuse more, e.g. "I don't want that medicine." "I don't have to stay here, I'm going away". If anxiety continues unrelieved, the words will become intimidating and irrational just before s/he blows up, either verbally or physically. If language is not usable, the tone of their sounds and nonverbal behaviors communicates similar meaning. If you are aware of the warnings, you may be able to diffuse the anxiety and break the cycle, thus preventing an aggressive attack. Remain pleasant and calm. At all times avoid becoming defensive or acting superior. Never say things like, "Calm down." or "Get a hold of yourself." or "Stop yelling". Don't threaten by saying, "If you don't calm down, we'll have to take you to your room." That's making his or her room a punishment. There is a reason for the anxiety. Look for it. In the early stages of anxiety, personal attention, listening and offering diversions may help. If the anxiety has already been building for some time, s/he may not hear what you are saying. Your options become more limited, but one helpful intervention is to take the client to an area that has controlled low stimuli, such as his/her room. This is not done with a reprimanding or punishing attitude. It is done with concern and as a therapeutic intervention. Even demented clients can sense your attitude and believe me, there is a difference. Most incidences of abuse occur during high activity time and the highest times are when trying to give care, e.g., bathing and toileting. The most common type of abuse is hitting and scratching. It is not a matter of just wanting things done their way. If these clients knew what "doing things their way" was, they probably wouldn't be diagnosed as demented. People become aggressive in dementia because they are either fearful of having a basic need (safety, self-esteem, etc.) unmet, they have experienced too much failure, they are having delusions and/or they feel anxious from misinterpreting environmental stimuli. Any way we can assist in reducing fear/anxiety will be helpful. When the warning behaviors become dangerous, indicating that the client will try to hurt him/herself, you or others, back away. Leave the client in a safe environment and monitor from a distance. In time the memory loss will cause the client to forget whatever it was that was upsetting and you can begin again. Do not reprimand, yell, or try to shame him or her. There is nothing to judge in this situation. There is only a very confused person trying to do the best s/he can with the limited and distorted information his/her brain is providing. There is no need for you to take the client’s actions personally and there is no need for the client to have to come up to anyone’s standards of appropriate behaviors. There is only need for understanding and patience. Particularly help the families understand this, as they easily remember the client’s pre-disease personality and carry more expectations of what should be appropriate according to their memories. Question No. 9: Examples of external stimuli that may be increasing the client’s anxiety include: a. Changes in routines. b. Noises, such as the TV, alarms, loud talking, intense pictures, colors or music. c. Too many choices and decisions required, for example, what/how to eat, how to take a bath, how to get dressed. d. All of these are modifiable external sources of stress and anxiety. 20 Alzheimer’s Disease & Dementia Related Disorders Question No. 10: Important to problem solving are all but one of these. Which is the least likely to be effective? a. Become conscious of how you are thinking and feeling and choose to be calm, patient and pleasant. b. Carefully assess the client’s current stage of functioning. c. Respond to the client as a person with valid feelings. d. Emotionally remain distant and in computer mode. Interact as little as possible. Question No. 11: If you assess warning signs of anxiety escalating to aggression, which of these is least likely to help prevent the aggression? a. Judge this as a seriously bad scenario, get stressed-out, and begin to tighten control with threats of punishments. b. Look for the reason for the anxiety and try to make the situation easier for the client to handle it. c. Make sure everyone is in a safe place and interact at a safe distance. d. Slow down, reduce as much stimuli as possible, change location to somewhere calming, and validate the client’s feelings. Question No. 12: When there are challenging repetitive or situationally inappropriate behaviors, which of these approaches has the least chance of being effective? a. “I see you found the napkins we use when we eat.” They are shredded. Provide a similar motion that is more desired. For example. “Can you help me snap these beans?” (Removing the napkins shreds after you assisted in starting the bean-snapping project by handing them beans and helping them snap them.) b. Say, “Can’t you see what you’re doing? Look at the mess you made here!” c. Try to create success at accomplishing anything, e.g. a show of delight when s/he could successfully snap two beans. d. Verbally identify something in the scenario that is a good thing. For example. “We don’t need these napkins right now. But you are sitting at the table in the kitchen because it is close to mealtime. If you want to snap the beans, thank you, but if you don’t, you can sit here and talk with us if you want. Promoting Independence through Assistance with Activities of Daily Living Objective No. 9: Recognize general strategies for promoting independence through assistance with ADLs in the beginning, middle and late stages. Objective No. 10: Consider examples illustrating care techniques for monitoring, assisting and providing total care in dressing, grooming, eating, bathing or toileting and incontinence. General Strategies for Activities of Daily Living (ADLs) in Stages In the beginning stages, the client remains mostly functional. Care involves mostly reminders of what needs to be done and guidance to assure safety. Remember that in this stage the client does not trust easily and becomes suspicious. A common agenda is that someone is stealing his/her things. Use consistent routines to keep personal items handy and then continually remind him/her of those things. “Did you look by your lamp, where we agree we would always store your glasses?” Introduce the client to other caregivers so that he becomes accustomed to more than one. Later it will be more difficult for the client to leave his/her primary caregiver. Having that foundation of trust in others will become vital for the health of the primary caregiver. This is a time of planning for the future. Teach families to learn about the disease so that they can begin creating the security that will be necessary in the future. Gradually 21 Alzheimer’s Disease & Dementia Related Disorders they will begin limiting the decisions the client will need to make. Slowly they will adjust the client’s environment with safety controls. Because family caregivers are more able to handle care at this stage, you will not be as involved as in later stages. In the middle stages, much more assistance with care will become necessary. Needs for care assistance continually increase. You can teach the family how to maintain the person’s dignity and independence by limiting the client’s decisions, rather than by deciding for him or her. Your focus of care here will be to promote safety. You will need to assess and monitor the environment continually, teaching ways in which an environmental change might promote safety. Special locks on doors or shut off switches on stoves might help as there are risks that s/he will get lost outside of the home, or injure him/herself inside the home when s/he forgets how appliances operate. In trying to help the client maintain independence, assess what s/he can do, so you can supply the necessary cues. Some clients have difficulty in sequencing the action. They don't remember what to do, but their body remembers how to do it. If we arrange the materials in the order they are needed, s/he may be able to carry on. This applies well to the steps of dressing. Sometimes they just need to get started. Always give simple instructions. Don't say, "Get dressed". Give one-step-at-a-time directions and remember s/he has forgotten how to get dressed. Other confused clients know what to do, but have forgotten how to do it. They can't follow through with the actions or respond to the instruction. For example, if you want to help them put on a sock, say, "Put on your sock now" and at the same time move to his or her foot with an open sock. Frustration enters into everything and can turn a simple procedure into a catastrophe. Be calm and unrushed. If you see signs this is going to cause a catastrophic reaction, then back off and come back later, or distract his/her attention. Don't reprimand the client, or indicate in your leaving that s/he has failed, so you will leave until s/he can learn to act "like a good boy/girl". The frustration did not arise from a conscious effort to be "bad" and in fact, in most cases, the client is coping in the best way s/he can manage. You might say, "This is becoming frustrating for both of us. I need a short time out. I will return in five minutes." S/he will probably forget the incident and you can start again with a different approach. It could be the inability to make decisions that frustrates him or her. Gradually, great assistance becomes total care in the later stages. Here, much of your focus will be to prevent complications from immobility, such as contractures or pressure ulcers, and weight loss. This level of physical care can be exhausting for a lone family member. Seek to increase access to assistance with care. Care Techniques Wandering: There are many things to monitor, but one of the more consistent to Alzheimer’s disease is the client’s tendency to wander. Simple wandering is not dangerous. Getting lost is. Issues of wandering can begin in late stage one and continue until the last stage when the person becomes immobile. We’ll begin with a review of wandering in general, then consider many principles of total care, and finally present some ideas about each category of care. There are various types of wandering behavior. Those restlessly pacing as a side effect of psychotropic drugs probably are the least focused and will respond least to environmental interventions. They need their drug dosage lowered or discontinued. “Exit seekers” are the most goal oriented. These clients often have an agenda and purpose to their wandering. They may be reenacting prior work roles, or seeking familiar routines. These people might be trying to recapture old satisfying situations that brought them safety and a sense of belonging. For example, George was usually seeking to escape, because he had to visit his son. Some wander because of their previous personality-ingrained behaviors that caused them to seek stimulation outside of themselves. Wanderers tend to have been people who were extroverted before their disease, whereas non-wanderers seem more capable of finding security and comfort through internal processes and inner feelings. It is helpful to remember that “exit seekers” and “external-stimulators” can remain focused for some time. These types of wanderers may benefit by being assigned a simple task. One example is to ask 22 Alzheimer’s Disease & Dementia Related Disorders the person to sweep, or fold washcloths as a therapy. Lucille likes to file papers away in drawers (creating unbelievable chaos) and she wanders in search of business. She feels best when she is busy, "helping" in her own way. She doesn't understand how her help creates so much more work. For her, to be given something that "needs to be done" is perfect. For a select few, they will be so busy sweeping an area; they will not remember to wander to other places. "Busy boxes" work well with some. These are highly individualized boxes, bags, etc. that attract the attention of a specific client. For example, one client had been a business executive for many years. His individual busy box was a briefcase that contained calling cards, calendars, papers, etc. When he seems unusually restless, the family might say, "This briefcase is just a mess. Would you please straighten it out for me?" He would be busy for a time sorting out the cards, looking at the papers, etc. If he left the busy box, it was just scooped back into the briefcase for the next time it was needed to be in "just a mess". In addition to diversion, this also stimulated comforting memories of his past and increased his self-esteem as he perceives himself to be helping in a way he feels comfortable. A particular woman's busy box might be a sewing box with quilt scraps, yarns, tapes, etc., or a basket of laundry that always "needs to be folded". There is no limit to the creative busy boxes that can be used effectively. Some wanderers are attracted to one stimulus after another and easily distracted. One stimulus that needs to be monitored carefully is an open door. Take a problem wanderer with you as you do some things. Many just need to walk and will placidly follow you wherever you go. The agitated wanderer is reducing stress, but the placid wanderer is often just bored and wants to explore. If you can identify a motivating need, that helps. Wandering is usually a stress relieving mechanism for most. There may be a need for increased motor activity. Structured physical exercise, accompanied walks, dances, etc., can be more appropriate outlets. In most cases, any intervention that will reduce this client's anxiety level and increase his/her security and self-esteem will decrease the need to wander. If there is ANY other way, do not restrain the client. S/he needs to move. It is true that there is danger in pacing, but there is also danger in using restraints. Restraints may cause: severe mental anguish, exacerbation of problems, depression, loss of ego, and more. These are risks worth considering. In a safe environment, wandering can stimulate circulation and oxygenation. It can promote exercise, decrease contractures, and decrease feelings of stress and anxiety. Problems arise when the client wanders into unsafe places or wanders out of the house or building. There are several routine safety precautions. A picture of the wanderer should be readily available. Provide the client with a med-alert bracelet with his/her address and a statement that s/he is memory impaired. In the early stages, the "safe-return" program is a good idea. This bracelet is engraved with a toll-free number and a 4-digit code that can be called in from anywhere in North America to identify the person and who to contact. You can register in this program through the Alzheimer's Association, or call 800-272-3900. You can provide suggestions for creating a safe environment. Think of the design of the house. Can divided doors, screens, or regular doors be used to set aside an area so the client could wander without causing problems? Put locks or alarms on the doors and perhaps modify appearance of the door so that it is not a stimulus for exit. In some home environments, the door can be wallpapered to look like a wall. Pictures or motifs (even a stop sign) can be added to the door, so that it is still clearly a door for those who are not confused, but the message is clouded for the demented. Place a chair beside the door facing back toward the room. As the client approaches the door, he may see the chair and choose to sit a few minutes. When he rises from the chair, he sees the room and the door is behind him. Wandering and restless motion are behaviors with meaning to the client. To thwart these behaviors only increases the feelings -- and the problems. All behaviors have meaning, even in confusion, so some thought should be given as to why this client is exhibiting his particular behavior, particularly if the pacing is increasing. Is he misinterpreting some environmental stimulus? Are there too many stimuli for her to sort through, creating more confusion and anxiety? Is the environment too non-stimulating, creating sensory deprivation? Has he developed an infection, or toothache, or does he have other discomfort? Is she tired? Is he hungry? Use the ABCs of problem solving. A behavioral log can provide ongoing assessment as you try to find the causes. This works particularly well for clients who are living at home. Focusing on one specific behavior, note when the behavior occurs, the events or stimuli preceding it (A), the behavior (B) and the 23 Alzheimer’s Disease & Dementia Related Disorders reactions of the client and the caregivers following it (C). If a daily log is kept for 1 to 2 weeks, you may be able to recognize a cause-effect relationship that will help you intervene. If the behavior is not dangerous, look for a safe place for this behavior to occur. If your client with dementia is pacing relentlessly and seems paranoid, or is trying to leave the building and you ignore his symptoms, or restrain him to a chair or his room, would your client be more secure, less frightened, or would the behavior stop? Of course not. In all probability, as soon as the client is confined, the client will become more upset, noisy and cry out in his anxiety. You have not only ignored his need for increased security, you have disrespected his adult status and some part of this client still remembers that he is not a child. At the very least, communicate respect. If you suspect the reason for the behavior is insecurity, seek ways to make him feel more secure. Sometimes, if he trusts you, just walking with your arms around him to a quiet space filled with familiar items, may help. Tell him that you know how to find him and that he is in the right place. Bathing: It is stressful if you can't remember the steps to take a bath, or recognize the sound of water running, or are bombarded by strangers invading your very personal space. The more memory loss there is, the more bathing become difficult. You can help by not offering decisions or presenting the whole concept of a "bath". Most lose all orientation if they are rolled into the shower chairs backward. The noise levels in tiled rooms are high and people talk loudly to be heard over the running water, etc. It is an environment and procedure to be feared. We can concentrate on providing instructions slowly, for one step at a time, with frequent reassurance and clues of orientation. We can minimize the amount of water in the tub. We can allow the client some control over simple tasks. We can smile and remain relaxed. It will also help to create as much routine as possible to the bathing procedure. Bathe at the same time of day, using the same caregiver, if possible. Pay special attention to privacy and keep the bathroom a comfortable temperature. Despite best efforts, the bath seems to be one of the more terrifying activities. It may require focused creativity and an ability to "think outside of the routines" in order to bathe some clients. For example, Mary refused to take her clothes off. Week after week of bath-induced trauma made the bath an awful experience for client, family and the aide. Finally, in desperation, the aide began running the shower over Mary as she sat in the shower chair fully clothed. Mary responded by taking off her clothes. Another bath option is a towel bath. In this case the client stays in bed and is covered with towels soaked in a warm, no-rinse solution. Using these towels, the person is massaged and cleaned at the same time. Soft, background music can enhance a very pleasant experience. Dressing and Grooming: Routine is so important, that even simple grooming activities should follow the same routine, daily. For example, a job list posted in the bathroom might read: 1. Wash face and hands. 2. Brush teeth. 3. Shave. 4. Comb hair. If the client fails to complete the list, you can reinforce the sequencing, by reviewing with him what he has accomplished. "First you washed your face and hands. Then, you combed your hair. Then, what was next? If necessary, complete the sentence for him, while you hand him his shaver. As the disease progresses, he will not be able to read or remember. You can still encourage him to help as he is able. Hand him the wash cloth, but when he continually washes the same area over and over, move his hands to some other area, while you continue to wash other areas. Dressing and grooming take a great deal of time and patience, and for some families the energy is lacking to do this daily. Encourage the families to change the client’s attire. Encourage the family caregiver to dress as well. It helps with self-esteem. It sets up the cues to day-time behavior versus night-time behavior. Help the families find ways to make dressing easier, such as elastic-wasted pants or pull over shirts. Find shoes that can be slipped on and off easily yet still provide sure footing and protection from falls. Short hair styles are easier than long hair. Short fingernails stay cleaner. Feeding: Using the multiple principles you are learning, you can summarize some aspects of daily care. For example, when feeding a confused client, increase the number of cues and decrease interfering stimuli. 24 Alzheimer’s Disease & Dementia Related Disorders Everything you do that reduces anxiety will make it easier for this client to sit still long enough to eat. Make sure the environment is low noise and confusion. Reduce the number of choices for food. Serve one or two foods at a time and interchange them when his attention span weakens. Serve food in a way that takes the least amount of work to eat. Best is finger-foods. Worst is any dish that requires altering (e.g., adding milk or condiments), utensils, or is the wrong temperature. Provide verbal cuing whenever they appear to need it. “Here is your spoon, Mary. Let me help.” Seek to reduce anxiety by preserving dignity. Don’t reprimand or raise your voice. Show the family how to just quietly supply the client with what he needs, in the least insulting manner. “John, this is your food. It is macaroni and cheese. Can I help serve you?” That’s much more pleasant than. “John, stay out of my food. This is your food. Here eat.” Remember that the more you work to keep stress levels low, the easier it will be for you to provide care in all areas. Monitor how much food the client actually swallows (versus goes on the floor or stays on the plate.) If it appears the client is not getting enough food, communicate your concerns so that specific steps can be taken to supply supplemental feedings. If the normal supplements aren’t working, communicate this as well and keep thinking of ways that might work. There is room for creative solutions in your position. As the disease progresses, there will be more need to feed the client. Teach the family the principles of feeding, including how to do the Heimlich maneuver and how to support a sitting position to help insure a safe swallow. Toileting and Incontinence: As the disease approaches the middle stages, people with dementia forget where the bathroom is or how to use it. Mark the bathroom with a realistic picture of a toilet, or leave the door open. Remove or camouflage all mirrors. The client may see himself in the mirror and think someone else is already using the bathroom. Some people will need help remembering how to start, i.e.: working zippers, buttons, etc. Some need cuing to help them remember the right sequence to the task. Others will need consistent bladder retraining. Toileting in advance of need (TIAN) prevents incontinence and reduces the amount of internal stimuli coming from the sensations of bladder filling, which this client cannot usually interpret. If all attempts fail, try adult briefs. They are much preferred over catheters. Catheters will get pulled out and it is dangerous to restrain this person so he will leave the catheter alone. The rate of infections is huge. The risks of catheters are very great. Briefs will allow mobility. Frequently, at least in the later stages, this is the person doesn't care if he's incontinent or not and he's not going to care if he's in briefs or not. When the client is confused and forgetful, it may become harder to keep him continent. As memory continues to fail, the maintenance of skin integrity sometimes becomes more important than maintaining continence. If it is suspected that urinary or fecal incontinence may contribute to skin breakdown, preventative measures must be taken. If the client is incontinent of feces also, the problem is magnified, because feces converts urea from urine into ammonia. The shift in pH reactivates the digestive enzymes (which had been inactivated as they passed through the GI tract) and these erode the skin. As the client becomes more immobile the risk of pressure ulcers rises. Clients in this position are constantly slipping down in their bed or chair and causing shearing and tearing. Friction on the surface of the skin (particularly wet skin) probably leads to superficial skin tears. Lift your client, don't slide him and teach the family to do the same. This means you'll need help, but dual time used in prevention may save countless hours of ulcer care later. The use of a turning sheet to lift offers less shearing than sliding the client across the sheets. Use proper lifting techniques and/or help to protect your own back. Remember the pressure points whenever you evaluate the position of a bedfast client. The turning frequency is determined by how long it takes before a reddened area doesn’t resolve. Although for most 25 Alzheimer’s Disease & Dementia Related Disorders clients, every two-hour turning works, in some you will find a red spot that remains. If that is the case, two hours is too long. Damage has already happened to this skin area and the skin will break down if you put more pressure on it. Try 1½ hours. The red spots should disappear before the next turn. In some very fragile clients, even one hour to a side is a concern. Preventing Falls: Monitor for difficulties walking and general muscular weakness. Physical & occupational therapies may help the client improve muscle strength and balance. Put the client who will get up even without help in a safe position. Mattresses on the floor, beanbag chairs, chairs designed with walking devices, etc. all help prevent injury from falls, but you need to assess family’s ability to help the client stand from the floor. Be observant for safety hazards that might trip a client who is confused, such as loose rugs, chairs in the way, etc. Clear the path whenever you can. Ask to be kept informed of drug administration that might increase the client’s confusion or delirium. The drugs most associated with falls are tranquilizers such as Ativan or Xanex. Extra monitoring is required when these drugs are given. But even cold medicine can increase the risk for falls. Question No. 13: Which of the following is NOT a general strategy for promoting independence and will most likely reduce independence? a. Break large tasks into steps that the client can accomplish, e.g., instead of “take a bath”, hand him/her a washcloth and start him/her washing the face. b. Limit the number of things to choose from according to his/her stage of function, but continue to allow him to make a choice. c. Try to keep the home environment unchanged, and encourage the client to learn how to negotiate it safely. d. Use consistent routines to keep personal items handy, e.g. store glasses next to the lamp. Question No. 14: All of the following are true, except one. Which answer is wrong? a. ‘Exit-seekers’ usually have a goal or agenda that they try to fulfill in their wandering, for example, Betsy ‘has to go home.’ b. Excessive pacing may be a stress relieving strategy. These people need physical activity. c. Restraining a client alone in his room when his wandering becomes too restless is probably the best strategy to increase his sense of security. d. Those who wander as a side effect of psychotropic drugs respond the least to environmental interventions. Question No. 15: Keeping a behavior record of a new or isolated problem for a short time helps to identify cause/effect relationships. Which of these is NOT a necessary part of a behavior log and not helpful? a. (Antecedent--Events preceding.) Lunch was normal and we talked about not seeing his son for a while. The TV was on, but low and in the next room. b. (Behavior) Just after lunch on Tuesday he started to pace around the house, trying all the doors. c. (Consequences).) The wife tried to get him to sit down and relax and his anxiety worsened. We couldn’t learn why he wanted to leave and couldn’t make him understand how hot it was. He just kept pacing door to door for several hours. The wife looked anxious herself. d. (Judgment.) It is so hard because he causes so much disruption in the family. This is so much work. NO one can do anything but monitor him. 26 Alzheimer’s Disease & Dementia Related Disorders Question No. 16: Which of the following decreases the client’s risk of falling? a. Decorating with rugs and furniture placed in the middle of the room. b. Encouraging sitting or lying, as conditioning the client’s muscles with exercise is no longer necessary. c. The use of devices that keep the client safely positioned, such as chairs with walking devices. d. The use of tranquilizing drugs. Question No. 17: How can you help prevent falls? a. Ask to be kept informed of drug changes and become aware of drug side effects that increase falls, such as from tranquilizers, cold medicines, and even blood pressure medicines. b. Constantly check for hazards, such loose rugs, electric cords, lack of hand railings, etc. c. Keep the client physically strong with exercise, or consultation with physical therapy or occupational therapy when necessary. d. All of these. Question No. 18: Which is the best example of “low-stimulus” at meal time? a. The client is offered a sandwich and allowed to roam as desired. Other finger foods are given with each opportunity. b. The client sits at the table and the food is self-served from common dishes in the center. His place is filled with some of each food option. c. The dog is begging for food and the grand-child is visiting and being fed. d. While the client is in the kitchen during food preparation, the pans clatter, the dish washer is loud, the garbage disposal is used and there is a radio going. Developing Skills for Working with Families and Caregivers OBJECTIVE NO. 11: Recognize issues and concerns of family members of clients and participants with ADRD in early, middle and late stages. OBJECTIVE NO. 12: Understand and recognize the grief process and how it relates to the multiple, ongoing losses associated with ADRD. Many families are willingly and quietly caring for their demented member in addition to caring for their immediate household. This usually involves sacrifice of time and money. Imagine how your life would be changed if you brought your mother or father into your home to care for them. Imagine also that this person needs twenty-four-hour supervision and daily care in maintaining personal hygiene, feeding and activities. Imagine the doctor bills, the bills for medication, tests, the extra burden on the food and clothing budget, and perhaps special equipment (much of which third party payers will not pay). Imagine this situation is not just for a few months, but for years. Include in your visual picture, your feelings of love for this person and a sense of responsibility to them. Include also the heartbreak as you watch them fail progressively and you know there is currently minimal help available. Don't forget to add the frustration when they won't eat because they "can't pay", or won't sleep because they need to "feed the baby". Imagine the battles when you want this person to take a bath, or when she accuses you of stealing her possessions. Deal with incontinence on your furniture. What kind of emotional and mental condition will you be in? Please don't be judgmental of families. You only need to walk in their shoes a few steps to know they deserve praise and recognition instead of criticism and avoidance. Katie Courtice writes, "Expect to experience fear of the unknown course of the illness, sadness as you remember and mourn a relationship that will never be the same; anger that you have been singled 27 Alzheimer’s Disease & Dementia Related Disorders out for this trial; despair when you doubt your ability to cope; guilt when you worry that you haven't done everything for the impaired person, or when you feel love slipping away under the stress of daily frustrations; resentment when this person fails to respond to you in loving ways that you have grown accustomed to expect." In many ways, the life of the family member changes as drastically as it does for the client. Sometimes the caregiver is like a second patient. “The caregiver responsibility translates into an enormous burden. In a survey cited by the report, almost 60% of respondents reported high or very high emotional stress and more than a third reported physical stress linked to caregiving. More than half (54%) had to take time off work to accommodate their caregiving role.” (Barclay, 4/24/2014) Mild Stage Time is precious to these family caregivers, because they are frequently pulled several ways; their own family, their own interests, jobs, etc. You have to become knowledgeable about the ways to approach a confused person so you can teach the family. Then you have to be able to show them that what you can teach them will save grief and time. In the early stages much of your teaching and care will be informing them of what to expect as the disease progresses. Support groups for families can be a valuable communication tool. There is a national association of The Alzheimer's Disease and Related Disorders Association (ADRDA) located at: 919 North Michigan Avenue, Suite 1000, Chicago, Il. 60611. They can offer information and references to family members and/or health professionals. A 24-hour free national hotline is available. Call (800) 621-0379 (nationwide) or (800)572-6037 (Illinois). They can offer a newsletter and books for the caregiver, such as: Understanding Alzheimer's Disease by Aronson, and Care of Alzheimer's Clients: A Manual for the Nursing Home Staff by Gwyther (also good for home care), and The 36-Hour Day by Mace. States have an ADRDA association and there are usually many local support groups. They can help each other and you. Families will help other families locate home health services, or guide them through the grief of nursing home placement, or they can lend a hand in relieving a caregiver for a few hours at home. Support groups can be an ear to listen and, more importantly, understand. You can communicate information through the support group, as a resource person. Families need us and we certainly need them. Planning for the future should begin when the client can still give input and knowing what to expect and why will increase the family's tolerance of annoying behaviors. Often families feel the client's behaviors are purposeful or stubborn. It is difficult to work through the denial and relate to the behaviors as "his best". Families also need to be aware of his baseline activity so they are able to recognize those times when unusual negative behaviors mean pain, infection or other changes. Early in the disease it is helpful to establish as broad a base to caregiving as is possible, either through multiple family members or respite care. The family may argue they are doing fine and do not need these resources. Emphasize that as the disease progresses, the client will cling to familiar surroundings and people. The client will resist having others come into his home and will resist even more going out. Caregiver fatigue becomes very real. If s/he can find comfort with alternate caregivers and locations early, this will make it much easier to utilize these resources later, when it will be needed. Moderate and early Severe Stage The physical, emotional, financial, and mental burdens of providing care to a family member are great and the resources for respite or relief are very limited. This becomes more and more of a reality as the disease progresses. The needs of the family caregiver are a serious health concern for our nation. Non-paid caregivers account for 8.4 billion hours of care in Alzheimer’s disease and dementias. Approximately 60% of the caregivers are women, ranging from very young to very old (average age is 48). Fifty-seven percent of the family caregivers hold full or part-time jobs in addition to the care given. For 32% of these caregivers, they have been providing care for 5 years or longer. (Statistics from Alzheimer’s Association Facts and Figures www.Alz.org/alzheimers_disease_facts_figures.asp) This tremendous health care resource needs our attention, our assistance and our teaching support. In these years, more and more care will become a physical need. Families will have to overcome the idea of “giving Mom a bath” or “cleaning up after my wife.” Those levels of intimacy are difficult for family members. As the need for safety escalates the physical structure of the house will have to change. Furniture will have to be protected or moved to create a safer, freer environment. Beds might be moved 28 Alzheimer’s Disease & Dementia Related Disorders downstairs or dining rooms used as bedrooms. These are great adjustments for families. It is difficult to maintain some sense of “normal life” and incorporate the needs of the client at the same time. The ability for the family to maintain a life outside of the home becomes more and more difficult. This is all very stressful and as the disease progresses for years, relief is difficult to find. Sleep becomes fragmented as you sleep with one ear tuned in to the client, who may well be up and about. Often, the health of the caregiver begins to decline and frequently the stimulus that caused the client to enter a nursing home was a health crisis of the primary caregiver. We need to monitor and support the caregiver at the same time we help the client. Encourage the caregiver to seek respite care. Families need us to listen more to them. For many, it's important to talk about their guilt and frustration. They need our emotional support. Families need help planning and they definitely want to be included in the planning process. Most of all, families want us to care for those they love with skill and patience, with care and understanding, so they can be assured they are somehow providing the best life possible for this person who continues to be a meaningful part of their lives. End Stage: Care in the end stages is almost totally physical and, as such, is physically demanding. Teach families how to protect their own backs as they strive to turn or lift this person to a new position. All aspects of total care will need to be supported, including providing adequate nutrition, good skin care, range of motion, etc. In this stage the person ceases to respond, which can be very difficult for family members. Gone are the concerns for elopement. Gone are worries that he’ll be up in the night breaking things. Gone are the arguments over which pajamas to wear or that he needs to sit down and eat. Gone, also is the person who they love. Grief begins long before the funeral. Much of the grief and fear that surrounds dementia is there because we all feel so helpless. The problems are certainly large enough to require the efforts of all of us. Working together, client, families and healthcare workers, we can provide support that is been needed. The Grief Process: The grief process is characterized by stages of shock and disbelief, anxiety, anger and bargaining, and acceptance. It is easy to identify the grief response when there has been a single, identifiable loss. However, in ADRD there are continual losses. The loved person slips away in stages, each stage creates more losses grief. First the person cannot carry his share of the responsibility and the family loses that assistance. Then the client’s personality begins to erode and features that the caregiver cherished, begin to disappear. The good times become harder to find. As care needs escalate, the caregiver’s freedom is lost. As the disease continues, it seems to the caregiver that his life is kidnapped by the ever-increasing needs of the client. Loss after loss, not the least of which is the life of the client. Thus, family caregivers find that they are in all the stages of grief at once. Today they can be in denial about the course of the future and angry that their savings are going to doctor bills. They can be anxious about the shift in responsibility they face and bargaining with other family members over the need to get away for a while. They spend years reaching acceptance and peace only for brief periods and usually in some stage of grief. The timing of the stages is variable and grieving is individualized for everyone. There is incredible stress to grief. It, alone, is work. More work, added to the endless work of caring for another adult in every respect. More work, when energy seems to be declining. More work, when there are fewer people available to listen, care, support and help carry the load. People are very good about showing up in an acute crisis. They tend to fade away when the crisis continues year after year. As the years go on, many caregivers begin to feel very isolated and alone. If you are there as a healthcare worker, every smile, every word of encouragement, every human connection becomes a source of strength. Your ability to be fully present, even in those times when the caregiver hasn’t got it all together, without judgment, is a priceless gift. It is true that your responsibility is to the client, but don’t forget that the health of the caregiver is vital to the health of the client. Every minute you can spare to talk, teach, or just listen while they cry a few tears, is part of your therapy. And when the tears are over, find something to laugh about. Life can get so ridiculous on some days, it shouldn’t be difficult. 29 Alzheimer’s Disease & Dementia Related Disorders That’s really what life is about, whether we are in touch with reality or not. It’s about caring and sharing, laughing and loving. It’s about connecting with each other. Needing and feeling needed. It’s about being real – not perfect, not superhuman, not saintly. Just real. And recognizing that real is OK. Always there is something we could have done better. Always there is something we could do that is worse. But we all do what we can do with the energy we have and the beliefs, priorities, and values that each of us hold dear. Sometimes we could just use a little recognition that we are doing what we can, especially when that never seems to be enough. The care of the client and family of those with Alzheimer’s disease and related disorders is complex, challenging and creative. There are many opportunities here for you to tackle problems and find solutions that do make things better. There are multiple ways that your contributions can make life worth living. Thank you for taking this complex challenge to create a better place for those who face this struggle, and for wanting to make a difference. Question No. 19: All of these are true about grief in cases of dementia, except one. Which is NOT valid or true? a. Caregivers experience anger, denial and anxiety just as do others experiencing grief. b. The family’s grief is usually resolved by the time the client enters the middle stages of ADRD. c. Supportive friends and family tend to become more limited as the crises continue year after year. d. There are multiple on-going losses to integrate and resolve over years of ongoing grief. Question No. 20: Which of the following is a concern of family members and the client that is most specific to the early stages of ADRD? a. The need for deep sleep. b. The need for physical support. c. The need to give intimate physical care. d. The need to plan for the future. 30 Alzheimer’s Disease & Dementia Related Disorders APPENDIX 1: CONDITIONS CAUSING DEMENTIAS AND DELIRIUMS DEMENTIAS DELIRIUM EITHER Alzheimer.................................. Yes Lewy Body Dementia………… Yes Yes Yes Multi-Infarct/Vascular....................................................................... Yes Transient Ischemic Attacks........................................ Yes Huntington's Chorea....................... Yes Picks.............................................. Yes Parkinson's....................................................................................... Yes Korsakoff's Psychosis.................... Yes Creutzfeldt-Jakob.......................... Yes Neurosyphilis................................. Yes Drug Toxicities................................................................................ Yes Depression....................................................................................... Yes Renal failure..................................................................................... Yes Fluid & Electrolyte Disorders.................................... Yes Acid/Base Disturbance....................................... ...... Yes Hypo/Hyperglycemia................................................. Yes Hepatic Failure................................................................................. Yes Hypo/Hyperthyroidism...................................................................... Yes Metabolic Diseases (B12 deficiency).................................................Yes Cushing's Syndrome....................... Yes Infections......................................................................................... Yes Cardiovascular disorders................................................................... Yes Brain Trauma............................................................ Yes Brain Tumors................................................................................... Yes Normal Pressure Hydrocephalus..... Yes Fecal Impaction......................................................... Yes Urinary Retention...................................................... Yes Fracture.................................................................... Yes Surgery..................................................................... Yes Blindness or Deafness....................................................................... Yes Hospitalization........................................................... Yes 31 Alzheimer’s Disease & Dementia Related Disorders BIBLIOGRAPHY Alagiakrishnan, Kannayiram, “Vascular Dementia,” http://emedicine.medscape.com/article/292105, Aug. 14, 2017. Anderson, P., “Exercise Top Lifestyle Factor for Alzheimer’s Prevention?” http://www.medscape.com/viewarticle/883781, August 4, 2017. Anderson, P., “Three-Minute Test for Lewy Body Dementia,” http://www.medscape.com/viewarticle/854577, November 16, 2015. Ault, Alicia, “Warnings About Benzodiazepine Use in the Elderly Go Unheeded,” https://www.medscape.com/viewarticle/901169, August 24, 2018. Barclay, Laurie, “Women Much More Vulnerable to Alzheimer’s Disease,” http://www.medscape.org/viewarticle/823171, 4/24/2014 Beck, C. Bogelpohl, T., “Problematic Vocalizations in Institutionalized Individuals with Dementia,” Journal of Gerontological Nursing, September 1999. Brauser, Deborah, “Nondrug Therapy Useful in Managing Agitation in Dementia,” http://www.medscape.com/viewarticle/836114, December 8, 2014. Bredesen, Dale, “Reversal of Cognitive Decline: A New Therapeutic Program,” http://www.impactaging.com/papers/v6/n9/full/100690.html, 9/26/2014. Brooks, Megan, “Antihypertensive Therapy Reduces Alzheimer’s, Dementia Risk,” https://www.medscape.com/viewarticle/900131, August 2, 2018. Brooks, Megan, “Depression at Any Stage of Life Tied to Increased Dementia Risk,” https://www.medscape.com/viewarticle/995094, August 2, 2023. Brooks, Megan, “US Dementia Deaths Vastly Underestimated,” https://www.medscape.com/viewarticle/936418, August 27, 2020. Carroll,Linda, “Happiness Training May Ease Dementia Caregivers's Anxiety,” https://www.medscape.com/viewarticle/912546, May 3, 2019. Caselli, R, et al, Personality Changes During the Transition From Cognitive Health to Mild Cognitive Impairment,” Journal of the American Geriatric Society, 66(4), https://www.medscape.com/viewarticle/895583, 2018 Chawla, Jasvinder, “Neurological Manifestations of Vascular Dementia,” http://emedicine.medscape.com/article/1135408, April 11, 2016. Crystal, Howard, “Dementia With Lewy Bodies,” http://emedicine.medscape.com/article/1135041, April 11, 2016. Doyle, Kathryn, “Singing Familiar Songs May Help Prompt Alzheimer’s Patients to Speak,” http://www.medscape.com/viewarticle/828172, July 14, 2014. Feil,Naomi, "Validation Therapy", Geriatric Nursing, May/June 1992, pg. 129-133. Frellick, Marcia, Atrial Cardiopathy Linked to 35% Higher Dementia Risk,” https://www.medscape.com.viewarticle/979511, August 19, 2022. Frellick, Marcia, “Women With Atrial Fibrillation More Likely to Develop Dementia,” https://Medscape.com/s/viewarticle/993707, June 26, 2023. Gomes-Osman,J., et al, “Exercise for Cognitive Brain Health in Aging,” Neurology in Clinical Practice, 8,2018. Goodwill, A., Szooke, C., “A Systematic Review and Meta-Analysis of the Effect of Low Vitamin D on Cognition,” Journal of the American Geriatric Society, 65(10), https://www.medscape.com/viewarticle/888700, 2017. Hackethal, Veronica, ‘Severity of Diabetes Complications Linked to Dementia,” http://www.medscape.com/viewarticle/848051, July 15, 2015. Harding, Anne, “Intervention for Caregivers of Dementia Patients Has Lasting Effects,” https://www.medscape.com/viewarticle/916045, July 26, 2019. Hirschler, Ben, “Nobel Discovery Opens Window On to Alzheimer’s Disease, http://www.medscape.com/viewarticle/832857, October 7, 2014 Hughes, Sue, “Heavy Drinking ‘Strongest’ Modifiable Risk Factor for Dementia,” https://www.medscape.com/viewarticle/892918, February 20, 2018. Hughes, Sue, “Hypertension in 40s Linked to Later Dementia, but Only in Women,” https://www.medscape.com/viewarticle/886936, October 12, 2017 Hughes, Sue, “Twelve Risk Factors Linked to 40% of World’s Dementia Cases,” https://www.medscape.com/viewarticle/935013, August 2, 2020. Isaacson, Richard, “How Much Exercise is Too Much for the Brain?’ https://www.medscape.com/viewarticle/904179, November 9, 2018. Jacobs, Aland, “What Precedes the Onset of Alzheimer Disease?” http://www.medscape.com/viewarticle/843457, May 5, 2015. Jhung, Lisa, “Scientists Frind Brain Mechanism Behind Age-Related Memory Loss,” https://www.medscape.com/s/viewarticle/976566, July 5, 2022. 32 Alzheimer’s Disease & Dementia Related Disorders Kim, G., et al. “Association Between Non-Alcoholic Fatty Liver Disease and the Risk of Dementia,” Liver International, 42(5), https://Medscape.com/s/viewarticle/973671, 2022. Kolanko, M., Malhotra, P., “Exploring Alzheimer’s DiseaseSubtypes in the Prodromal Stage,” Brain, 141(12), https://www.medscape.com/viewarticle/906239, 2018. Lamb, etal, “Dementia AND Physical Activity (DAPA) trial of moderate to high intensity exercise training for people with Dementia,” British Medical Journal, 36(1):k1675, 2018. Ling, S., et al, “Addressing Neuropsychiatric Symptoms in Patients with Dementia,” http://www.medscape.org/viewarticle/863602, June 9, 2016. McNamara, D.,, “Alzheimer’s Related Dementias Predicted to Double by 2060,” https://www.medscape.com/viewarticle/902323, September21, 2018. Montine, Thomas, “Dementia Pathology,” http://emedicine.medscape.com/article/2003174, December 29, 2014. Muche, Julie, “Geriatric Rehabilitation,” http://emedicine.medscape.con/article/318521, Feb. 25, 2015. Osterweil, N., ‘Scripts for Drug Tied to Cognitive Decline ‘Alarmingly High’”, https://www.medscape.com/viewarticle/877848, March28, 2017. Paaauw, Douglas, “How Can I Keep From Losing My Mind?, https://www.medscape.com/s/viewarticle/983497, November 9, 2022. Reuben, David, “Caregiving in Dementia: Directing Families to Resources,” http://www.medscape.com/viewarticle/859714, March 7, 2016. Sabbagh, M., et al, “Advances in the Early Identification and Management of Alzheimer’s Disease,” http://www.medscape.org/viewarticle/867868, September 14, 2016. Salardini, A., “An Overview of Primary Dementias as Clinicopathological Entities,” Seminars in Neurology,30(2), https://www.medscape.com/viewarticle/911244, 2019. Shafi, M., et al, “Advancing the Neurophysiological Understanding of Dementia,” Journal of the American Geriatric Society, 65(6), https://www.medscape.com/viewarticle/882383, 2017. “SSRI Improves Cognition, Major Depression in Early Dementia,” https://www.medscape.com/viewarticle/993414, June 20, 2023. Syrek, Ryan, “Trending Clinical Topic: Blood Pressure Drugs and Dementia Risk,” https://www.medscape.com/viewarticle/986958, January 20, 2023. Vega, C., “Can Physical Fitness Fight Dementia?” https://www.medscape.com/viewarticle/894682, April 13, 2018. Vega, C., “Could Better Sleep Prevent Dementia?” https://www.medscape.com/viewarticle/895313, April 25, 2018. Vergne, D. et al, “Agitated Patients? They May be Taking Their Cue From You,” http://www.medscape.com/viewarticle/867680, August 24, 2016. Wajngarten, Mauricio, “Does Evidence Support Pharmacologic Treatment for Dementia?” https://www.medscape.com/viewarticle/987375, January 30, 2023. Walter, C., et al, “Differentiating Alzheimer Disease, Lewy Body, and Parkinson Dementia Using DSM-5,” Journal for Nurse Practitioners, http://www.medscape.com/viewarticle/823809, 10(4), 2014. Whitlock Burton, Kelli, “Higher Dementia Risk in Women Explained,” https://www.medscape.com/viewarticle/988728, February 24, 2023. Yasgur, B., “Depression More Severe, Persistent in the Elderly,” https://www.medscape.com/viewarticle/898385, June 21, 2018. Yasgur, B., “Late-Life Low BP, Weight Loss, High Blood Sugar PrecedeDementia,” https://www.medscape.com/viewarticle/899994, July 30, 2018. Yasgur, B., “Midlife Anxiety Tied to Late-Life Dementia,” https://www.medscape.com/viewarticle/895997, 5/1/2018. Yasgur, B., “Music Therapy Improves Mood, Quality of Life in Dementia,” https://www.medscape.com/viewarticle/900955, August 20, 2018. Yasgur, B., “Underpinnings of Air Pollution and Dementia Risk Explained,” https://www.medscape.com/viewarticle/994844, July 26, 2023. 33 Alzheimer’s Disease & Dementia Related Disorders STATE LICENSE NO. (or Certificate No.) NAME____________________________________________________ ADDRESS_________________________________________________ 1:_____ _____________ 2:_____ _____________ 3:_____ _____________ ________________________________________________ OCCUPATION _____________________ Use this answer sheet as a guide when you submit your answers on the website. Once you are ready to submit your answers and complete the course, you will need to sign in to your record at www.consultantsforthefuture.com, using your username and password. Click on your name at the upper right of the home page to find your list of outstanding courses. Select this course, and scroll down to find the list of modules for the test. The questions should be the same as in the course material you just read. Select your answers and then press “Finish” Online submission is immediate. After successful completion, you have an opportunity to complete the evaluation. Return to your account to find your certificate, which you can print. There is only one correct answer for each question. 1. (a) (b) (c) (d) 11. (a) (b) (c) (d) 2. (a) (b) (c) (d) 12. (a) (b) (c) (d) 3. (a) (b) (c) (d) 13. (a) (b) (c) (d) 4. (a) (b) (c) (d) 14. (a) (b) (c) (d) 5. (a) (b) (c) (d) 15. (a) (b) (c) (d) 6. (a) (b) (c) (d) 16. (a) (b) (c) (d) 7. (a) (b) (c) (d) 17. (a) (b) (c) (d) 8. (a) (b) (c) (d) 18. (a) (b) (c) (d) 9. (a) (b) (c) (d) 19. (a) (b) (c) (d) 10. (a) (b) (c) (d) 20. (a) (b) (c) (d) 11/23 CE Broker Tracking No. 20-91509 34
 0
0
advertisement



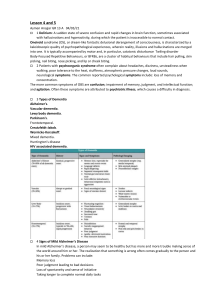
Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users