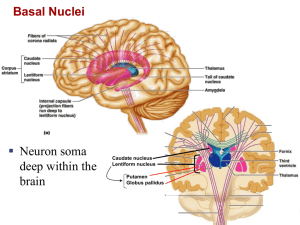
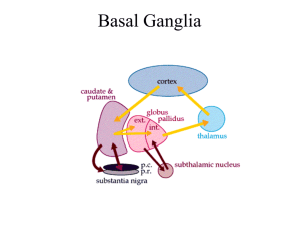
Neuroanatomy Basal Nuclei Dr. Moira Jenkins can't let go? hypo (parkinsons) stops the thalamus from pulling "files" letting thalamus go = "unlocking" cant keep control? hyper (huntingtons chorea) Basal Nuclei Functions • Controls the assembly of overall motor plans • Scaling the intensity of execution of motor patterns in the context of the task requirements • Enable automatic performance of practiced motor acts • Sets the body position and muscle tone for movement and at rest • “Initiation” of motor patterns like walking, chewing • Involved in cognition • Implementation of motor plans that are reliant on motivation and emotion • Some function in memory • Some function in motivation • Extrapyramidal System (as opposed to the pyramids of the corticospinal tract) • Start, Stop, Modulate Movements NOT weakness Basal Nuclei • Often called Basal Ganglia • Identified by LOCATION in cerebral hemispheres Basal Nuclei – Dorsal • Corpus Striatum – associated with movement regulation *Named for striped appearance Subparts -Putamen -Globus Pallidus (internal & external) -Caudate Nucleus Lentiform nucleus = putamen + globus p. • Amygdala – part of limbic system FEAR • Claustrum – sensory input biggest boy The CAUDATE NUCLEUS has a massive head, body, and curving tail that follows the curve of the lateral ventricle Follows path of lateral ventricle, head forms the lateral wall of the anterior horn Basal Nuclei –capsular divisions • Internal capsule separates caudate from lentiform - corticospinal tract - corticobulbar tract - sensory fibers from the anterolateral and medial lemniscus projection fibers • External capsule separates putamen from claustrum association fibers • Extreme capsule separates insula from claustrum association fibers 7 Basal Nuclei- Ventral • Lie ventral to the anterior commissure and are linked to bio rewards and motivation • Subthalamic nucleus- in diencephalon involved in movement and limbic • Substantia Nigra – in midbrain, movement and limbic source of dopaminergic neuronsimplicated in Parkinson’s disease • Nucleus accumbens – dopaminergic, biorewards reward nucleus, has relationship Part of the limbic system • Olfactory tubercle – also part of limbic syste with basal nuclei - disorders like parkinsons can have an affect on this areas Substantia Nigra • Named because of the black appearance from melanin pigment • Pars compacta • Neurons contains pigment melanin and release neurotransmitter dopamine • Pars reticularis • Neurons release neurotransmitter GABA • Located in the midbrain –ventral to red nucleus • Plays a role in movement, motivation, and reward Basal Nuclei Incoming Connections • *There is no direct path to or from the spinal cord or the brainstem • The striatum (putamen and caudate nucleus) receives input from several areas of the cortex Corticostriatal Pathway from cortex to nuclei And from the Substantia Nigra (receives input from cortex) Nigrostriatal Pathway from substantia nigra to nuclei Basal Nuclei Outgoing Connection → Thalamus Then thalamus projects to the motor cortex motor thalamus • *The only output is to other areas within the basal nuclei or to thalamus “motor thalamus” • From thalamus projections go to motor cortex and “unlock”, or disinhibit preprogrammed movement patterns, sequenced patterns • Normally, only the movement desired will be unlocked, or disinhibited • This is the thalamocortical pathway Connections within the Basal Nuclei 1. unlock thalamus for desired movement (DIRECT PATH EXCITES the thalamus) 2. inhibit thalamus to stop undersired movement (INDIRECT PATH - INHIBITS the thalamus) • Several interconnections of nuclei • Results in a “direct” and a “indirect” pathway • The direct and indirect pathways counterbalance each other • Direct path excites cortex • Indirect path inhibits cortex • The basal ganglia have a dual function -enable desired movements (release inhibition) -inhibit undesired movements • Disturbances in different portions of the pathway can result in either production of involuntary movement or cessation of movement indirect path Striatum I-I D-E indirect path fine tunes both paths Inputs to the Basal Ganglia are Processed Through 3 Pathways 1. Direct Pathway- Start movements 2. Indirect Pathway- Stop unwanted movements 3. Nigrostriatal Pathway- modulate the direct and indirect pathways All 3 pathways influence Globus Pallidus Internus Pallidothalamic pathway is inhibitory to Thalamus Striatum thalamocortical I-I D-E pallidothalamic Thalamus VA and VL nuclei Thalamicocortical fibers are excitatory to cortex RELEASES DOPAMINE How the Basal Nuclei Functions Direct Route → activates thalamus → movement occurs Indirect Route → inhibits thalamus → suppress unwanted movements Both pathways activated when a specific movement occurs Dopamine enhances the direct path, allows movement to occur Basal Ganglia Disorders • Negative signs – patient wants to perform actions but cannot • Akinesia (hesitancy), bradykinesia (slow movement), abnormal postural adjustments (inability to make adjustments when falling or tilting) • Positive signs – manifestations of loss of pallidal movements they dont want inhibition of the thalamus • Alteration in muscle tone (hypertonicity/rigidity) and forms of dyskinesias (occur at rest; cannot be prevented or stopped): tremors, chorea, athetosis, ballismus, tics Basal Nuclei Dysfunction • Dyskinesia- abnormal or impaired motor activity, not paralysis With the cortex or cord there is paralysis – spastic muscle weakness With the cerebellum there is ataxia – lack of muscle coordination, awkward with intentional movements • Basal Nuclei-usually some movement at rest “resting tremor” • See a combination of -positive signs – abnormal movements patient does not want to have -negative signs – patient cannot perform actions that they want • Hypokinesia – reduced motor activity similar to parkinsons but more emotional Ex: Parkinson’s disease, Lewy Body component • Hyperkinesia – loss of movement inhibition, increased motor activity Ex: Huntington’s Chorea, Hemiballism, Tourette’s Syndrome Parkinson’s Disease • Parkinson’s Disease (paralysis agitans) • Parkinson’s disease, first described by James Parkinson in 1817 is caused by the destruction of pigmented cells in the substantia nigra. These pigmented cells release dopamine and their degeneration results in a depletion of dopamine to the striatum, less excitation to cortex Symptoms of Parkinson’s Disease 1. An expressionless, mask-like face that conveys no emotion. 2. Akinesia (difficulty in initiating movement) 3. Bradykinesia (slowness in execution of movement) 4. Shuffling gait. Walking is reduced to a shuffle, with the patient frequently losing his balance Walking turns into a rapid, stiff shuffle as the patient chases his center of gravity, festinating gait (Latin, festinare, to hasten) 5. Rhythmic tremor at rest ("pill rolling") ends when voluntary movement begins. 6. Cogwheel rigidity - is felt when the examiner moves a limb 7. Rigidity of muscles due to effect on tone 8. Intellectual decline 9. Micrographia – progressively small handwriting TREATMENT L-DOPA Hyperkinesia Chorea is the name given to certain convulsive movements of a forcible, jerking, and rapid nature that resemble a sort of dance (Chorea means dance in Greek) It is caused by the degeneration of neurons in the caudate nucleus and putamen causing a release phenomenon Huntington's disease Hereditary, appears 35-45 years old autosomal dominant, if one parent has, 50% chance child will Often leads to death 15 - 20 years after onset Woodie Guthrie – folk song writer, musician, and artist famous person had it and died at age 55 Trey Gray – drummer with Brooks and Dunn country band Huntington’s Chorea Signs and symptoms dance • Chorea movements • Facial grimacing • Dementia • Lack of restraint, fidgeting • Delusions • Hypertonia and hypotonia • Difficulty thinking clearly – may be first sign • In Huntington's disease, the output of the basal ganglia is decreased • In Parkinson's disease, the output of the basal ganglia is increased • Since the effects of the basal ganglia on the thalamus are inhibitory, the motor loop is facilitated in Huntington's and inhibited in Parkinson's Hyperkinesia – Syndenham’s Chorea Syndenham’s chorea (also called Saint Vitus’ dance, rheumatic chorea, chorea minor) The disease is apparently caused by the same streptococcal bacillus that causes rheumatic fever, in which case it follows the infection by several months after all other symptoms have disappeared Usually 5-15 years old Loss of neurons in striatum Rarely fatal, usually recover Hyperkinesia – Hemiballism Hemiballism (Greek – a half throwing) Violent flinging of a limb on one side of the body (opposite the lesion) The disease is caused by a lesion to the subthalamic nucleus, usually vascular infarction Usually recover Other Hyperkinetic Disorders Perservation = the repetition of a particular response despite lack of a stimulus • Athetosis – dyskinesia movements are continuous, slow, writhing and snake-like damage to corpus striatum • Tourette’s Syndrome- facial tics, phonic tics, first appears in childhood PANDAS - post infection - weird behavior, tic, coughing - paranoia, anxiety, night terros - SUDDEN ONSET - treatment: reduce inflam in basal nuclei involves basal nuclei and connection to frontal lobe • Obsessive Compulsive Disorder – now thought to have some involvement with basal nuclei, endlessly repeating movement circuits