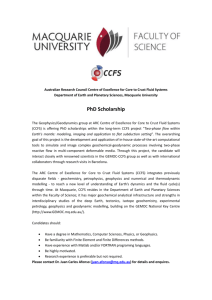
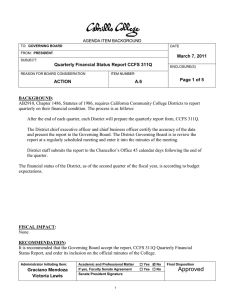
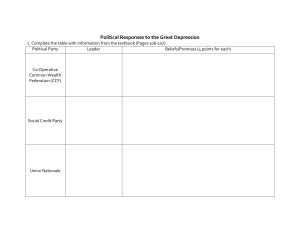
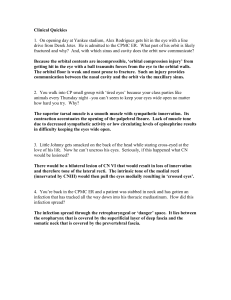
Original Article Carotid Cavernous Fistulas and Dural Arteriovenous Fistulas of the Cavernous Sinus: Validation of a New Classification According to Venous Drainage Giuseppe Leone1,2, Leonardo Renieri2, Alejandro Enriquez-Marulanda3, Adam A. Dmytriw4, Sergio Nappini2, Antonio Laiso2, Giuseppe Buono5, Mariano Marseglia5, Adriana Iuliano6, Mario Muto1, Francesco Briganti5, Salvatore Mangiafico2, Nicola Limbucci2 BACKGROUND: Multiple carotid cavernous fistula (CCF) classifications have been proposed. However, they lacked predictive factors for the clinical presentation, natural history, and hemorrhagic risk. Our aim was to externally validate a new classification according to venous drainage (i.e., the Thomas classification [TC]) to assess its relationship with symptoms, endovascular treatment, and outcomes. - METHODS: We performed a multicenter retrospective review of CCFs at 2 major academic institutions. The CCFs were classified using the Barrow classification (BC) and TC systems. - RESULTS: The data from 94 patients with a diagnosis of CCF were collected during a study period 23 years, 4 months. Of these 94 patients, 89 had undergone CCF treatment and 5 had experienced spontaneous occlusion. Complete occlusion was achieved in 89.9% of the treated patients. Complications occurred in 5.3% of the patients, including permanent deficits in 2.1%. TC type 4 was associated with cortical symptoms compared with type 2 (P [ 0.003) and type 3 (P < 0.001). The BC was not able to detect significant differences among the symptom types. Significant differences were found using the TC for the transarterial-only, transvenous anterior-only, and transvenous posterior-only approaches (P < 0.001, P [ 0.03, and P [ 0.001, respectively). The transvenous posterior and transvenous anterior approach were significantly associated with type 2 and 3 TC, respectively. Excluding direct CCFs, the BC was not related to the treatment approach. No significant differences in the outcomes were found. However, a trend toward a lower occlusion rate for TC type 4 compared with type 3 was observed. CONCLUSION: The TC provided useful information regarding the fistula anatomy and venous hemodynamics, which correlated with the clinical symptoms and treatment strategy. - - Key words - Carotid cavernous fistula - Classification - Venous drainage Abbreviations and Acronyms BC: Barrow classification CCF: Carotid cavernous fistula CS: Cavernous sinus DAVF: Dural arteriovenous fistula ECA: External carotid artery ICA: Internal carotid artery TC: Thomas classification From the 1Department of Neuroradiology, Antonio Cardarelli Azienda Ospedaliera di Rilievo Nazionale, Naples, Italy; 2Neurovascular Interventional Unit, Careggi University Hospital, WORLD NEUROSURGERY 128: e621-e631, AUGUST 2019 INTRODUCTION C arotid cavernous fistulas (CCFs) are acquired vascular lesions, representing an abnormal connection by direct shunt or dural branches of the internal carotid artery (ICA) and/or the external carotid artery (ECA) with the cavernous sinus (CS). Indirect connections include dural arteriovenous fistulas (DAVFs) of the CS. The CCFs types are disparate. Hemodynamic classifications have traditionally separated CCFs into highflow and low-flow fistulas. In contrast, etiological classifications have distinguished between spontaneous and traumatic lesions.1,2 Florence, Italy; 3Department of Neurosurgery, Boston Medical Center, Boston, Massachusetts, USA; 4Division of Diagnostic and Therapeutic Neuroradiology, Toronto Western Hospital, University Health Network, Toronto, Ontario, Canada; 5Unit of Interventional Neuroradiology, Department of Advanced Biomedical Sciences, Federico II University of Naples, Naples, Italy; and 6Ophthalmology Unit, Department of Neuroscience and Reproductive and Odontostomatological Sciences, Federico II University of Naples, Naples, Italy To whom correspondence should be addressed: Giuseppe Leone, M.D. [E-mail: g.leonemd@gmail.com] Citation: World Neurosurg. (2019) 128:e621-e631. https://doi.org/10.1016/j.wneu.2019.04.220 Journal homepage: www.journals.elsevier.com/world-neurosurgery Available online: www.sciencedirect.com 1878-8750/$ - see front matter ª 2019 Elsevier Inc. All rights reserved. www.journals.elsevier.com/world-neurosurgery e621 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION Figure 1. Thomas classification type 1 and Barrow classification type D fistula in a sexagenarian with severe diplopia, ptosis, and headache. (A) External and (B) internal right carotid angiograms in the lateral view showing a dural carotid cavernous fistula, fed by the external carotid artery and internal carotid artery dural branches, draining only toward the inferior The first notable CCF classification, proposed by Barrow et al.,3 was based on the arterial angioarchitecture. However, the main drawback of the Barrow classification (BC) has been the lack of predictive factors for the clinical presentation, natural history, and, importantly, the hemorrhagic risk. Other classifications, limited to CS DAVFs, have been proposed.4-8 The classifications by Borden et al.4 and Cognard et al.5 both focused on the drainage Figure 2. Thomas classification type 2 and Barrow classification type C fistula in a septuagenarian with mild chemosis, exophthalmos, and diplopia. (A) Angiogram after left external carotid artery injection showing a dural carotid cavernous fistula with low flow, e622 www.SCIENCEDIRECT.com petrosal sinus. (C) Because of the patency of the inferior petrosal sinus, retrograde transvenous catheterization was straightforward. (D) Common carotid angiogram after coiling of the cavernous sinus showing occlusion of the shunt. pattern of DAVFs. However, these classifications have not distinguished between anterior and posterior drainage in the CS region, which could be important for treatment planning and clinical correlation. These classifications, based on the venous pattern,4-8 albeit excluding direct CCFs, reflect that symptoms and hemorrhagic risk will be influenced more by the venous drainage than by the arterial supply.9 draining toward the superior ophthalmic vein and inferior petrosal sinus. (B) Because the symptoms were not severe, conservative management was attempted. The symptoms improved, and the 2-month follow-up angiogram showed occlusion of the fistula. WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2019.04.220 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. Figure 3. Thomas classification type 3 and Barrow classification type B fistula in a sexagenarian with history of progressive chemosis, ocular pain exophthalmos, ptosis, and diplopia. Right internal carotid artery angiogram in (A) lateral and (B) frontal views showing a high-flow dural carotid cavernous fistula with drainage into the superior ophthalmic vein (SOV). A tight stenosis was present at the junction between the cavernous sinus and the SOV. (C) Our aim was to validate a classification system for CCFs, recently proposed by Thomas et al.,10 which was based on the venous drainage pattern. We used data from a separate cohort of patients WORLD NEUROSURGERY 128: e621-e631, AUGUST 2019 VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION Catheterization of the fistula from the thrombosed inferior petrosal sinus was unsuccessful. The SOV was surgically exposed and catheterized. The fistulous compartment of the right cavernous sinus was embolized with coils and Onyx. (D) A compliant balloon was temporarily inflated in the carotid syphon to prevent arterial reflux. Angiogram after embolization of the right internal carotid artery in the (E) lateral and (F) frontal views showing occlusion of the shunt. with CCFs who had not been a part of the original study from 2 major academic institutions in Italy to assess its relationship with the symptoms, endovascular treatment approach, and outcomes. www.journals.elsevier.com/world-neurosurgery e623 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION Figure 4. Thomas classification type 4 and Barrow classification type D fistula in a septuagenarian complaining of severe headache, right ophthalmoplegia, ptosis, and bilateral chemosis. Right external carotid artery angiogram in (A) frontal and (B) lateral views showing right carotid cavernous fistula. The fistulous point was located in the medial METHODS Patient Characteristics We retrospectively reviewed the medical records and imaging studies of all patients who had been treated for CCFs at 2 major Italian academic institutions from October 1994 to February 2018. We enrolled 94 consecutive patients with CCFs. The population was stratified according to age, sex, CCF type using the BC and Thomas classification (TC),10 symptoms, treatment type, occlusion rate, morbidity, mortality, and clinical outcomes. The present study was conducted in accordance with institutional guidelines and institutional review board approval. All the patients had provided written informed consent before any invasive procedure and also for the eventual scientific publication of patient records and information anonymously. e624 www.SCIENCEDIRECT.com compartment of the cavernous sinus at level of the junction with the intercavernous sinus. The drainage was toward the superior ophthalmic vein and sphenoparietal sinus, with massive cortical reflux. Angiogram of right common carotid artery in (C) frontal and (D) lateral views showing occlusion of the fistula. CCF Classification Schemes According to the BC,3 a CCF was classified as type A when a direct connection between the ICA and CS was seen; type B or C when the CCF was fed only by the dural branches of the ICA or ECA respectively; and type D when the CCF was fed by the dural branches of both the ICA and the ECA. Using the TC,10 the CCFs were classified as type 1 when fistula drainage was present only posteriorly and/or inferiorly through the inferior and/or superior petrosal sinuses, pterygoid and parapharyngeal plexus (Figure 1). The CCFs were classified as type 2 when the drainage was both anterior through the ophthalmic veins and posterior and/or inferior (Figure 2). The CCFs were classified as type 3 when the fistula drainage was occurring only anteriorly through the superior and/or inferior ophthalmic veins (Figure 3). The CCFs were classified as type 4 when cortical drainage was WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2019.04.220 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. Figure 5. Thomas classification type 5 and Barrow classification type A fistula in a septuagenarian with recent trauma resulting in skull base and right orbit fractures with development of a direct carotid cavernous fistula. She presented with a severe visual deficit, bilateral exophthalmos, and ophthalmoplegia. Right internal carotid artery angiogram in (A) frontal and (B) lateral views showing multiple direct shunting points, with drainage toward the bilateral inferior petrosal sinus, superior ophthalmic vein, and right identified as filling the superficial middle cerebral veins and perimesencephalic and cerebellar venous system (Figure 4). Finally, the CCFs were considered type 5 when a high-flow direct arteriovenous shunt was present between the ICA and CS (Figure 5). Two experienced interventional neuroradiologists reviewed the pretreatment angiograms and classified the CCFs using the BC and TC. The discrepant cases were resolved by consensus. After treatment, the follow-up imaging studies were reviewed, and the CCFs were classified as completely occluded, partially occluded (the shunt was still present but reduced), or inadequately occluded (minimal or no reduction). The clinical presentation, including WORLD NEUROSURGERY 128: e621-e631, AUGUST 2019 VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION sphenoparietal sinus with cortical reflux. After failure of the occlusion balloon test, selective embolization of the fistula was performed. Coils were simultaneously placed in the cavernous sinus through the retrograde transvenous and transarterial approaches. (C) A compliant balloon was temporary inflated in the carotid syphon to avoid migration of the coils through the fistula. (D) Internal carotid artery angiogram showing the outcome after 2 embolization sessions. ocular (i.e., loss of vision, ocular pain, glaucoma, chemosis, exophthalmos), cavernous (i.e., ophthalmoplegia, diplopia, ptosis, anisocoria), and cortical (i.e., intracranial hemorrhage, seizure, focal neurological deficits) involvement, was correlated with the TC and BC. Endovascular treatment was classified as conservative, transarterial, transvenous, or combined. The transvenous route was used for anterior CCFs via the ophthalmic veins or posterior/inferior CCFs via the petrosal sinuses and parapharyngeal plexus. The embolization methods included coiling, a combination of coiling and Onyx injection (Medtronic, Minneapolis, Minnesota, USA), and transarterial www.journals.elsevier.com/world-neurosurgery e625 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION Table 1. Patient Characteristics (n ¼ 94) Characteristic Value Age (years) Median 62.5 Interquartile range 54e73 Sex Female 58 (61.7) Male 36 (38.3) Symptoms Cavernous only 1 (1.1) Ocular/orbital 25 (26.6) Ocular/orbital plus cavernous symptoms 58 (61.7) Cortical 8 (8.5) Asymptomatic 2 (2.1) Data presented as n (%), unless otherwise noted. embolization (i.e., particles, coils, detachable balloons, or a combination). The occlusion grade, retreatment rate, morbidity, and mortality were recorded. The endovascular approach used and occlusion rate were correlated with the type of fistula according to the BC and TC. Statistical Analysis For statistical analysis, the observations were defined as patients, CCFs, or procedures, as applicable. The categorical variables are reported as proportions and continuous variables as the mean standard deviation or median and interquartile range, as appropriate, according to the distribution of the data. In each group, categorical variables were compared using the c2 test, and continuous variables were compared using the Kruskal-Wallis test. A pairwise multiple comparison adjustment was performed using the Bonferroni method and Dunn’s test. All statistical analyses were performed using the Stata, version 14, statistical software package (StataCorp., College Station, Texas, USA). RESULTS Patient Characteristics Overall, 94 patients were identified. The patient characteristics are summarized in Table 1. Most of the patients (61.7%) had combined ocular and cavernous symptoms. Cortical symptoms were reported in 8 patients (5 with type 4 TC and 3 with type 5 TC). Among the patients with cortical symptoms as their primary presentation, 4 also had had ocular symptoms and 3 had also had cavernous symptoms. The CCF type according to the BC and TC is reported in Table 2. Treatments and Outcomes Invasive treatment was performed in 89 patients (94.7%), and 5 patients (5.3%) had experienced spontaneous resolution. The e626 www.SCIENCEDIRECT.com proportion of patients with spontaneous occlusion resolution was 7.2% including only those with dural CCFs. All 5 patients with spontaneous resolution had small-size fistulas, without cortical venous drainage and had presented with few symptoms. Spontaneous occlusion had occurred within a mean period of 50 days after the diagnosis. In addition, 3 of the 5 patients experienced transient clinical worsening before spontaneous recovery. The treatment characteristics are summarized in Table 3. Complications (transient or permanent symptoms) occurred in 5 patients (5.3%). Treatment-related permanent complications occurred in 2 patients (2.1%); both were ischemic events. In 1 patient, CS thrombosis and intracerebral bleeding occurred 2 months after unsuccessful transvenous embolization, before a new treatment attempt but without permanent deficits. No deaths occurred. The mean follow-up time was 42 months (range, 24e60). The complete occlusion rate after the first embolization treatment was 69.7%. Of the 89 patients, 18 (20.2%) required retreatment. Excluding those patients with spontaneous resolution, after all the treatments, occlusion was complete in 80 patients (89.9%), partial in 6 (6.7%), and inadequate in 3 patients (3.4%). In addition, clinical complete resolution occurred in 81 patients (86.2%) and partial resolution in 7 (7.4%). However, the symptoms were unchanged in 3 patients (3.2%) and had worsened in 3 patients (3.2%). None of the CCFs recurred. Classification of CCFs and Association with Patient Characteristics Using the TC, we found a significant association with patient age (P ¼ 0.01; Table 2). After adjustment for multiple comparisons, we found a significantly lower patient age for those with type 5 compared with those with type 2 (P ¼ 0.002) and type 3 (P ¼ 0.004). The BC was also able to detect a significant difference according to patient age (P ¼ 0.005; Table 4). After adjustment for multiple comparisons, we found a significantly lower age among those with type A compared with those with type B (P ¼ 0.0007) and type D (P ¼ 0.007). The TC system was also able to detect significant differences in the symptoms (Table 2). After adjustment for multiple comparisons, we found type 4 CCFs had a greater association with cortical symptoms compared with type 2 (P ¼ 0.003) and type 3 (P < 0.001). Also, type 4 CCFs were significantly less associated with ocular and/or orbital symptoms with or without cavernous symptoms compared with type 2 (P ¼ 0.003) and type 3 (P < 0.001). Patients with type 1 CCFs had significantly more cavernous-only symptoms compared with those with type 3 (P ¼ 0.001) and type 5 (P ¼ 0.01). However, the low number of type 1 fistulas limited the clinical significance of these results. We found no significant differences among the patients’ symptoms using the BC (Table 4). Finally, we found no significant differences in sex, asymptomatic presentation, and spontaneous resolution of the CCF using either classification system. Classification of CCF and Association with Treatment Approach Significant differences according to the TC were detected for the transarterial-only, transvenous anterior-only, and transvenous posterior-only approaches (P < 0.001, P ¼ 0.03, and P ¼ 0.001, WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2019.04.220 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION Table 2. Carotid Cavernous Fistula Type According to Thomas Classification Thomas Classification Variable Type 1 (n [ 4) Type 2 (n [ 14) Type 3 (n [ 41) Type 4 (n [ 10) Type 5 (n [ 25) P Value Age (years) 75 (65e78) 69.5 (60e78) 67 (56e72) 62.5 (54e65) 55 (38e62) 0.01* Female sex 2 (50.0) 1 (7.1) 17 (41.5) 4 (40.0) 12 (48.0) 0.13 Cavernous only 1 (25.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) <0.001* Ocular/orbital with or without cavernous symptoms 3 (75.0) 14 (100.0) 40 (97.6) 5 (50.0) 21 (84.0) <0.001* Symptoms Cortical 0 (0.0) 0 (0.0) 0 (0.0) 5 (50.0) 3 (12.0) <0.001* Asymptomatic 0 (0.0) 0 (0.0) 1 (2.4) 0 (0.0) 1 (4.0) 0.9 Spontaneous resolution 1 (25.0) 1 (7.1) 3 (7.3) 0 (0.0) 0 (0.0) 0.24 Transarterial only 2 (50.0) 1 (7.1) 6 (14.6) 1 (10.0) 17 (68.0) <0.001* Transvenous anterior only 0 (0.0) 1 (7.1) 14 (34.1) 1 (10.0) 2 (8.0) 0.03* Transvenous posterior only 1 (25.0) 10 (71.4) 14 (34.1) 8 (80.0) 4 (16.0) 0.001* Combined transvenous 0 (0.0) 1 (7.1) 4 (9.8) 0 (0.0) 0 (0.0) 0.42 Open surgical 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (8.0) 0.23 0 (0.0) 1 (7.1) 0 (0.0) 1 (10.0) 3 (12.0) 0.26 Treatment approach Complications Occlusion after first embolization 0.61 Complete 2 (66.7) 10 (76.9) 26 (68.4) 5 (50.0) 19 (76.0) Partial or incomplete 1 (33.3) 3 (23.1) 12 (31.6) 5 (50.0) 6 (24.0) 0 (0.0) 3 (23.1) 8 (21.0) 3 (30.0) 4 (16.0) Retreatment Occlusion on follow-up after all treatment 0.79 0.012* Complete 1 (33.3) 12 (92.3) 36 (94.7) 8 (80.0) 23 (92.0) Partial or inadequate 2 (66.7) 1 (7.7) 2 (5.3) 2 (20.0) 2 (8.0) Clinical outcome 0.59 Resolution 4 (100.0) 12 (85.7) 38 (92.7) 8 (80.0) 19 (76.0) Partial resolution 0 (0.0) 1 (7.1) 2 (4.9) 0 (0.0) 4 (16.0) Unchanged 0 (0.0) 0 (0.0) 1 (2.4) 1 (10.0) 1 (4.0) Worse 0 (0.0) 1 (7.1) 0 (0.0) 1 (10.0) 1 (4.0) Data presented as median (interquartile range; P value calculated using Kruskal-Wallis test) or n (%; P value calculated using c test). *Statistically significant (P < 0.05). 2 respectively; Table 2). After adjustment for multiple comparisons, we found that type 5 CCFs were significantly more likely to be associated with a transarterial approach compared with type 2 (P < 0.001), type 3 (P < 0.001), and type 4 (P ¼ 0.002). Also, type 5 was significantly less associated with the transvenous posterior-only approach compared with type 2 (P ¼ 0.001) and type 4 (P < 0.001). Posterior transvenous treatment was more common for type 2 than type 3 fistulas (P ¼ 0.015) and for type 2 fistulas compared with the remaining population (P < 0.05; considering both all types of fistulas and dural fistulas only). The anterior transvenous approach was more common for type 3 WORLD NEUROSURGERY 128: e621-e631, AUGUST 2019 fistulas than for the remaining population (P < 0.001). A trend was found for using the anterior transvenous approach for type 3 fistulas compared with type 2 fistulas (P ¼ 0.05). The BC was able to detect differences for the transarterial-only and transvenous posterior-only approaches (Table 4). After multiple comparison adjustment, type A was associated with greater rates of the transarterial approach compared with types B and D (P < 0.001 for both comparisons). Additionally, type B was associated with greater rates of the transvenous posterioronly approach compared with type A (P < 0.001). No other significant differences were found when comparing the treatment www.journals.elsevier.com/world-neurosurgery e627 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION Table 3. Treatment Characteristics (n ¼ 94) Characteristic n (%) Spontaneous resolution 5 (5.3) n ¼ 89 Treatment Transarterial only 27 (28.7) Transvenous anterior only 18 (19.1) Transvenous posterior only 37 (39.4) Transvenous anterior plus posterior 5 (5.3) Combined arterial plus posterior Embolic material used 2 (2.1) n ¼ 89 compared with the other fistula types. A significant difference in the occlusion rate at follow-up (excluding spontaneous resolution) was detected using the TC (Table 2). After multiple comparison adjustment, type 1 was associated with lower complete occlusion rates compared with type 3 (P ¼ 0.001) and type 5 (P ¼ 0.005). However, the low number of type 1 fistulas limited the clinical impact of these results. Among the other types, type 4 had the lowest complete occlusion rate (80%), without significant differences compared with the other fistula types (P ¼ 0.36). Using the BC, no significant differences were noted for the occlusion rates at follow-up after all treatments (Table 4). The occlusion status after the first embolization and retreatment was not significantly different using either scale. The clinical outcome also was not significantly different using either scale. Coils 64 (73.6) Acrylic glue 2 (2.3) DISCUSSION Particles 4 (4.6) Coils plus Onyx 12 (13.8) Coils plus particles 1 (1.1) Onyx plus particles 1 (1.1) The BC and TC are the only classification systems that include both direct and dural fistulas.3,10 Other classifications, such as the Cognard classification, have included only dural fistulas.5 Classifying only indirect fistulas is understandable from a pathological viewpoint. Albeit direct and indirect fistulas are different diseases with different etiologies, an anatomy-based classification that includes both dural and direct fistulas, such as the BC and TC, could be useful because both types of CCFs can have overlapping symptoms, venous patterns, and therapy options. The mainstay of CCF treatment has been transvenous embolization, with transarterial embolization rarely performed and, in most cases, reserved for direct CCFs.11 Transarterial embolization of indirect low-flow CCFs will generally be cumbersome owing to the small size, complex anatomy, and multiplicity of arterial feeders. Therefore, transarterial embolization has been typically used only to reduce arterial inflow before transvenous occlusion for high-flow indirect CCFs and as a viable alternative after failure of transvenous attempts. Although coils and particulate agents have been used, these agents, used alone, cannot provide permanent occlusion of the fistula. Transvenous access to the CS can be from the posterior approach (usually from the inferior petrosal sinus) or anterior approach (usually from the superior ophthalmic vein), or combined. Because the main difference between the BC and TC is that former was based on the arterial anatomy and the latter on the venous drainage pattern, we believe the TC system might be more useful during therapeutic planning. In contrast to a classification system based on the arterial angioarchitecture, such as the BC,3 we found that the TC types significantly correlated with the patients’ symptoms. The pattern of symptoms is dependent on the functional and anatomical features, such as the shunt velocity, direction of the venous drainage, and pressure within the venous structures.10 Therefore, because the symptoms are strictly related to the venous drainage pattern,11 a classification using the venous drainage pattern could be of greater importance for the management CCFs. Also, any novel classification should not disregard this anatomical aspect. Concerning the patient characteristics, type 5 and type A CCFs were significantly associated with a younger patient age. Our Detachable balloon 3 (3.4) Complications 5 (5.3) Occlusion after first embolization n ¼ 89 Complete 62 (69.7) Partial 18 (20.2) Inadequate 9 (10.1) Retreatment 18 (20.2) Treatment number n ¼ 89 1 71 (79.8) 2 17 (19.1) 3 1 (1.1) Occlusion after all treatments Complete n ¼ 89 80 (89.9) Partial 6 (6.7) Inadequate 3 (3.4) Clinical outcome n ¼ 94 Complete resolution 81 (86.2) Partial resolution 7 (7.4) Unchanged 3 (3.2) Worse 3 (3.2) approach between the other types of fistulas using the BC. We found no significant differences for the combined transvenous or open surgical approach using either scale. Classification of the CCF and Association with Outcomes Complications occurred in 5.3% of the patients (12% of direct fistulas). However, no significant differences were observed e628 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2019.04.220 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION Table 4. Carotid Cavernous Fistula Type According to Barrow Classification Barrow Classification Variable Type A (n [ 25) Type B (n [ 10) Type C (n [ 6) Type D (n [ 53) P Value Age (years) 55 (38e62) 73.5 (65e76) 70.5 (56e80) 64 (56e73) 0.005* Female sex 12 (48.0) 3 (30.0) 3 (50.0) 18 (34.0) 0.56 Cavernous only 0 (0.0) 0 (0.0) 0 (0.0) 1 (1.9) 0.85 Ocular/orbital with or without cavernous symptoms 21 (84.0) 9 (90.0) 5 (83.3) 48 (90.6) 0.83 Cortical 3 (12.0) 1 (10.0) 0 (0.0) 4 (7.5) 0.79 Asymptomatic 1 (4.0) 0 (0.0) 1 (16.7) 0 (0.0) 0.05 0 (0.0) 2 (20.0) 0 (0.0) 3 (5.7) 0.11 Symptoms Spontaneous resolution Treatment approach Transarterial only 17 (68.0) 0 (0.0) 3 (50.0) 7 (13.2) <0.001* Transvenous anterior only 2 (8.0) 0 (0.0) 1 (16.7) 15 (28.3) 0.06 Transvenous posterior only 4 (16.0) 8 (80.0) 2 (33.3) 23 (43.4) 0.004* Combined transvenous 0 (0.0) 0 (0.0) 0 (0.0) 5 (9.4) 0.25 Open surgical 2 (8.0) 0 (0.0) 0 (0.0) 0 (0.0) 0.13 3 (12.0) 1 (10.0) 0 (0.0) 1 (1.9) 0.24 Complications Occlusion after first embolization Complete Partial/inadequate Retreatment 0.48 19 (76.0) 7 (87.5) 4 (66.7) 32 (64.0) 6 (24.0) 1 (12.5) 2 (33.3) 18 (36.0) 4 (16.0) 0 (0.0) 0 (0.0) 14 (28.0) Occlusion on follow-up after all treatment 0.13 0.26 Complete 23 (92.0) 7 (87.5) 4 (66.7) 46 (92.0) Partial 2 (8.0) 1 (12.5) 2 (33.3) 4 (8.0) Resolution 19 (76.0) 8 (80.0) 5 (83.3) 49 (92.4) Partial resolution 4 (16.0) 0 (0.0) 0 (0.0) 3 (5.7) Unchanged 1 (4.0) 1 (10.0) 1 (16.7) 0 (0.0) Worse 1 (4.0) 1 (10.0) 0 (0.0) 1 (1.9) Clinical outcome 0.16 Data presented as median (interquartile range; P value calculated using Kruskal-Wallis test) or n (%; P value calculated using c2 test). *Statistically significant (P < 0.05). findings are similar to those reported by Grumann et al.,12 likely because direct CCFs are often the consequence of trauma, which frequently occur in younger persons. We did not detect any differences when stratified by sex, asymptomatic presentation, or spontaneous resolution using the TC or BC. In our series, type 1 CCFs were significantly associated with the presence of cavernous symptoms only compared with types 3 and 5. Hemodynamically, it can be envisaged that posterior-only venous drainage will increase the pressure in the CS, such that vascular steal could result in cranial nerve deficits, manifesting as ophthalmoplegia, ptosis, or anisocoria.10 Type 2 and 3 CCFs were significantly associated with ocular symptoms because their WORLD NEUROSURGERY 128: e621-e631, AUGUST 2019 drainage mainly occurs through the ophthalmic veins with resultant ophthalmic venous hypertension, explaining the development of orbital congestion, secondary glaucoma, and optic neuropathy. Reversal of flow from the CCF into the anterior aspect of the CS and the ophthalmic vein was present in all our patients with orbital congestion. As expected, type 4 TC CCFs were associated with cortical symptoms. The importance of the presence of cortical drainage is related to its association with a severe presentation and a greater hemorrhagic risk, which has also been stressed in various classifications of DAVFs4,5 and dural CCFs6-8 but was not considered in the BC.3 www.journals.elsevier.com/world-neurosurgery e629 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION In our series, treatment was indicated for patients with severe progressive symptoms and those with cortical venous drainage. The reported rates of spontaneous dural CCF regression have ranged from 3.7% to 90%.13-16 In our series, spontaneous resolution occurred in 5.3% of patients (7.2% including only dural CCFs). This event occurred within a mean period of 50 days after the diagnosis. Of the 5 patients, 3 experienced transient clinical worsening before spontaneous recovery. Spontaneous closure can occur when the shunt elevates the venous pressure within the sinus to a critical point at which stasis occurs and thrombosis is facilitated.16,17 No spontaneous resolution occurred in patients with TC type 4 or 5. A likely confounder was that type 4 CCFs were promptly treated because of the significant hemorrhagic risk. In addition, type 5 CCFs almost never spontaneously thrombose owing to the high-flow shunt. In its original description, the TC system was significantly associated with the endovascular treatment approach used. Both TC type 5 and BC type A, corresponding to direct fistulas, were associated with the transarterial approach. However, TC types 1 and 2 were significantly associated with the transvenous posterior approach, and type 3 was significantly associated with the transvenous anterior approach. In contrast, the BC system was not associated with the different transvenous approaches.10 Also, in our study, the BC and TC systems were associated with the transarterial treatment approach for direct CCFs. Transarterial embolization should be preferred because the large direct shunt provides easy access to the CS to occlude the fistulous point.18 The transvenous posterior approach was associated with TC type 2 and the transvenous anterior approach with TC type 3 CCFs. Also, in the study by Thomas et al.,10 the preference was to treat type 3 CCFs with a transvenous anterior approach only, in contrast to our series in which both anterior-only and posterioronly transvenous approaches were used equally for the treatment of this type of CCF. In types 2 and 3 CCFs, either approach can be successful, because catheterization of the inferior petrosal sinus will be feasible even if it is occluded.19 Therefore, we believe that REFERENCES 1. Ellis JA, Goldstein H, Connolly ES, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012; 32:E9. 2. Henderson AD, Miller NR. Carotid-cavernous fistula: current concepts in aetiology, investigation, and management. Eye Lond Engl. 2018;32: 164-172. 3. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985;62:248-256. 4. Borden JA, Wu JK, Shucart WA. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg. 1995;82:166-179. 5. Cognard C, Gobin YP, Pierot L, et al. Cerebral dural arteriovenous fistulas: clinical and e630 www.SCIENCEDIRECT.com the treatment choice for categories is mainly dependent on the neurointerventionalist’s preference. We found an occlusion rate of 89.9% after all treatments, with complete clinical resolution in 86.2%. These results are similar to those reported in recent series.12,20-22 We found that TC type 1 CCFs were associated with a lower complete occlusion rate compared with that for type 3 and type 5, although the symptoms had resolved in all patients with type 1 CCF. It is possible that in a type 1 fistula, a minimal pressure decrease in the CS might improve the cavernous symptoms, such as ophthalmoplegia, ptosis, and anisocoria. However, this class of fistula is rare, and the small proportion of patients (4.2% in our series) weakened the statistical power of this assertion. Study Limitations The present study was limited by its retrospective nature with all the inherent bias of such a study design. The sample size was relatively small, which could have limited our ability to detect differences between the groups, mainly when performing subgroup analyses. Another limitation was the long temporal paradigm, which included a patient cohort treated during a study period of >20 years, during which the preferred endovascular methods changed. CONCLUSION Knowledge of the CCF drainage pattern is crucial for informed decision making for endovascular treatment. The TC system provided useful information on fistula anatomy and hemodynamics, which will correlate with the clinical symptoms in a large cohort of patients. Our findings suggest that a classification system based on the venous drainage is applicable in clinical practice and demonstrates a correlation with the symptoms. This could further aid in planning fistula access during endovascular embolization. A comparison with other available classification systems could be useful to further validate the TC. angiographic correlation with a revised classification of venous drainage. Radiology. 1995;194: 671-680. 6. Wenderoth J. Proposal for an improved classification system for cavernous sinus dural arteriovenous fistula (CS-DAVF). J Neurointerventional Surg. 2017;9:220-224. 7. Suh DC, Lee JH, Kim SJ, et al. New concept in cavernous sinus dural arteriovenous fistula: correlation with presenting symptom and venous drainage patterns. Stroke. 2005;36:1134-1139. 8. Satomi J, Satoh K, Matsubara S, Nakajima N, Nagahiro S. Angiographic changes in venous drainage of cavernous sinus dural arteriovenous fistulae after palliative transarterial embolization or observational management: a proposed stage classification. Neurosurgery. 2005;56:494-502 [discussion: 494-502]. 9. Stiebel-Kalish H, Setton A, Nimii Y, et al. Cavernous sinus dural arteriovenous malformations: patterns of venous drainage are related to clinical signs and symptoms. Ophthalmology. 2002; 109:1685-1691. 10. Thomas AJ, Chua M, Fusco M, et al. Proposal of venous drainage-based classification system for carotid cavernous fistulae with validity assessment in a multicenter cohort. Neurosurgery. 2015;77: 380-385 [discussion: 385]. 11. Ducruet AF, Albuquerque FC, Crowley RW, McDougall CG. The evolution of endovascular treatment of carotid cavernous fistulas: a singlecenter experience. World Neurosurg. 2013;80: 538-548. 12. Grumann AJ, Boivin-Faure L, Chapot R, Adenis JP, Robert PY. Ophthalmologic outcome of direct and indirect carotid cavernous fistulas. Int Ophthalmol. 2012;32:153-159. 13. Shields CB, Tutt HP. Spontaneous obliteration of carotid-cavernous fistulas. South Med J. 1981;74: 617-620. WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2019.04.220 ORIGINAL ARTICLE GIUSEPPE LEONE ET AL. 14. Briganti F, Caranci F, Leone G, et al. Endovascular occlusion of dural cavernous fistulas through a superior ophthalmic vein approach. Neuroradiol J. 2013;26:565-572. 15. Sasaki H, Nukui H, Kaneko M, et al. Long-term observations in cases with spontaneous carotidcavernous fistulas. Acta Neurochir (Wien). 1988;90: 117-120. VALIDATION OF NOVEL CCF AND DAVF CLASSIFICATION direct carotid cavernous fistula. Interv Neuroradiol. 2013;19:344-352. cavernous sinus dural arteriovenous fistula. Neuroradiology. 2011;53:983-992. 19. Jia ZY, Song YS, Sheen JJ, Kim JG, Lee DH, Suh DC. Cannulation of occluded inferior petrosal sinuses for the transvenous embolization of cavernous sinus dural arteriovenous fistulas: usefulness of a Frontier-wire probing technique. AJNR Am J Neuroradiol. 2018;39:2301-2306. Conflict of interest statement: The authors declare that the article content was composed in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. Received 30 January 2019; accepted 24 April 2019 20. Meyers PM, Halbach VV, Dowd CF, et al. Dural carotid cavernous fistula: definitive endovascular management and long-term follow-up. Am J Ophthalmol. 2002;134:85-92. Citation: World Neurosurg. (2019) 128:e621-e631. https://doi.org/10.1016/j.wneu.2019.04.220 21. Kirsch M, Henkes H, Liebig T, et al. Endovascular management of dural carotid-cavernous sinus fistulas in 141 patients. Neuroradiology. 2006;48: 486-490. Available online: www.sciencedirect.com 17. Seeger JF, Gabrielsen TO, Giannotta SL, Lotz PR. Carotid-cavernous sinus fistulas and venous thrombosis. AJNR Am J Neuroradiol. 1980;1:141-148. 18. De Renzis A, Nappini S, Consoli A, et al. Balloonassisted coiling of the cavernous sinus to treat 22. Jung KH, Kwon BJ, Chu K, et al. Clinical and angiographic factors related to the prognosis of 16. Luciani A, Houdart E, Mounayer C, Maurice J-PS, Merland J-J. Spontaneous closure of dural arteriovenous fistulas: report of three cases and review of the literature. AJNR Am J Neuroradiol. 2001;22: 992-996. WORLD NEUROSURGERY 128: e621-e631, AUGUST 2019 Journal homepage: www.journals.elsevier.com/worldneurosurgery 1878-8750/$ - see front matter ª 2019 Elsevier Inc. All rights reserved. www.journals.elsevier.com/world-neurosurgery e631