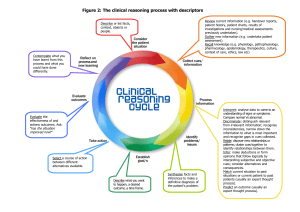
Kelley Durr, MSN, RN, CPNP-PC OBJECTIVES Discuss assessment findings for the endocrine system. Analyze laboratory and diagnostic tests specific to health problems affecting the endocrine system. Identify risk factors associated with health conditions of the endocrine system. Plan nursing therapies specific to the care of patients with endocrine disease. Discuss endocrine medications Discuss teaching plans for clients regarding endocrine health problems. DIABETES MELLITUS REVIEW Types Causes Diagnosis Treatment ACUTE COMPLICATIONS OF DIABETES HYPOGLYCEMIA VS HYPERGLYCEMIA Hypoglycemia Hyperglycemia Blood glucose _______ ____________ skin ___________ of fingers, toes, mouth Faintness, ____________ _________ speech ___________, coma _________ onset __________ blood glucose _______, _____ skin Increased _____________, _____________ Nausea and vomiting May progress to ___________ Mood swings __________onset PATHOPHYSIOLOGY OF HYPOGLYCEMIA Counter-regulatory _________ released Activation of ___________ nervous system Neuroglycopenia Hypoglycemic ____________ CAUSES OF HYPOGLYCEMIA Mismatch of food and _______ Oral _________ drugs _________ exercise Beta adrenergic blockers TAKE ACTION: HYPOGLYCEMIA ______________ _____________ selection IV _________ __________ Future prevention DIABETIC KETOACIDOSIS (DKA) Profound deficiency of ________ Most likely to occur with _______ diabetes Risk factors: Illness or __________ ___________insulin dosage _____________ type 1 diabetes Lack of education, understanding, or resources PATHOPHYSIOLOGY OF DKA Insufficient insulin glucose not used properly for _________ Fat broken down and used as fuel _________ _________ acidosis _____________ PATHOPHYSIOLOGY OF DKA Impaired protein synthesis _________ degradation _______ loss from tissues Production of glucose from amino acids increased ____________ __________________severe electrolyte depletion Hypovolemia shock renal failure coma death Blood glucose >____mg/dL Blood pH <_____ Bicarbonate <______ mEq/L Moderate to large ________ in urine or serum GOALS FOR DKA TREATMENT ______ resuscitation for volume ________ Reversal of __________ and ___________ ___________ of blood glucose Replenishment of ___________ Identify underlying cause EMERGENCY MANAGEMENT OF DKA ___________ management ____________ for fluids and electrolytes Continuous _________ drip ____________ replacement HYPEROSMOLAR HYPERGLYCEMIA SYNDROME (HHS) Life-threatening syndrome Risk factors Occurs with _______diabetes Enough _______ to prevent DKA but still have severe ____________ CAUSES OF HHS Acute illness Heart attack or stroke Sepsis Medications Newly diagnosed or poorly controlled ________ diabetes Impaired _______sensation/inability to replace fluids Poor ________ function ASSESSMENT CUES OF HHS _______________ in the early stages _________________ ___________ and _______________ Neurologic manifestations – DIAGNOSTICS OF HHS Blood glucose >______ mg/dL ___________ serum osmolality _________ absent or minimal Enough ________ to prevent ketoacidosis Arterial pH ________ Serum bicarbonate _______mEq/L TAKE ACTION: HHS Medical emergency with high ________ Management similar to ______ • IV _______ and IV _______ • ____________ monitoring and/or replacement Correct underlying cause COMPLICATIONS OF HHS ____________ Myocardial infarction _________ Coma _______ failure DKA vs HHS REVIEW ____________ gland is considered the master gland of the endocrine system. Anterior pituitary gland secretes ________ __________, __________, tropic hormones, ACTH or _____________ hormone, TSH or ________________ hormone, FSH or ________________ hormone, and LH or _____________ hormone. Parathyroid hormone regulates serum ________ and ___________ levels by stimulating bone resorption of _________, renal tubular reabsorption of ______, and activation of vitamin ____. DISORDERS OF ANTERIOR PITUITARY GLAND Acromegaly Hypopituitarism ACROMEGALY ASSESSMENT CUES: ACROMEGALY ________ tumor ____________ and ______________ of bony and soft tissue _______ weakness and ______pain ______________of voice _______ changes Excessive _____________ ANALYZE CUES: ACROMEGALY _________ insulin-like growth factor-1 (IGF-1) Oral ________tolerance test Imaging TAKE ACTION: ACROMEGALY __________ _________ Drugs – Serial _____________ Support group HYPOPITUITARISM Selective hypopituitarism _____________________ Most commonly involves GH and gonadotropins Causes – ASSESSMENT CUES: HYPOPITUITARISM 1. 2. 3. 4. 5. 6. 7. DIAGNOSTICS H&P Imaging Labs TAKE ACTION HYPOPITUITARISM _________ Radiation ____________ REVIEW Antidiuretic hormone (ADH) or ______________ is produced in the ____________ and is _______ and __________ by the posterior pituitary gland. Osmolality is the ___________ of particles in a ________ _________. _______ ____________ is regulated by _______. SYNDROME OF INAPPROPRIATE ANTIDIURETIC HORMONE (SIADH) ______________ of ADH More common in older adults Causes • Surgery • ________ • ______disorders • ________ ASSESSMENT CUES OF SIADH ______________ Fluid ___________ Concentrated _______ Cramps __________ Headache ANALYZE CUES FOR SIADH Sodium ________ serum, _________ urine osmolality Urine specific gravity Imaging TAKE ACTION SIADH Fluid __________ ___________ fluid – 3% sodium chloride Positioning _______ diuretic Medications to inhibit _____ production Surgery DIABETES INSIPIDUS (DI) ___________of ADH Decreased _______response to ADH Not related to _____________ Fluid and electrolyte imbalance Acute or chronic TYPES OF DIABETES INSIPIDUS Central – ________ than normal ADH Nephrogenic – _______ not responding to ADH Primary (Dipsogenic) – __________ of ADH ASSESSMENT CUES OF DI __________ __________ _______ urine Hypotension _____________ Intracranial bleeding Dry ______________ ANALYZE CUES: DIABETES INSIPIDUS H&P Fluid __________ test __________ serum osmolality, _________ urine osmolality Urine specific gravity ______ Sodium ______ MRI TAKE ACTION DIABETES INSIPIDUS __________ saline, D5W Hormone therapy ______________ ________ I&O PITUITARY SURGERY Transsphenoidal hypophysectomy • Removal of a pituitary tumor through the nose via endoscope • Treatment option for acromegaly, hypopituitarism, SIADH, Cushing’s disease NURSING ACTIONS PITUITARY SURGERY PRE OP CONSIDERATIONS POST OP CARE POSSIBLE COMPLICATIONS HYPERPARATHYROIDISM ________ secretion of parathyroid hormone (PTH) Increased serum ________ Types • Primary – increased ______ secretion • Secondary – compensatory response to __________ • Tertiary – __________ of parathyroid glands ASSESSMENT CUES HYPERPARATHYROIDISM May be _____________ ____________ Cardiac ____________ __________bone density _________ weakness Loss of _________ Depression Complications • Osteoporosis • Renal _______ • Pancreatitis • ________changes • Long bone __________ DIAGNOSTICS HYPERPARATHYROIDISM Serum calcium ________ Phosphorus ________ Urinalysis _____ scan MRI, CT, ultrasound TAKE ACTION: HYPERPARATHYROIDISM Complete or partial removal of ____ glands IV fluids Medications – Post-op complication - _________ Monitor intake and output _________ precautions HYPOPARATHYROIDISM _______ PTH _____________ Pseudohypoparathyroism Cause - iatrogenic ASSESSMENT CUES HYPOPARATHYROIDISM Positive ___________ and _____________sign _________ Lethargy ____________ ____________ Muscle cramps TAKE ACTION HYPOPARATHYROIDISM Treat ______ complications IV ________ Rebreathing ___________ Diet PHEOCHROMOCYTOMA Very rare tumor in the adrenal medulla _________ ________ epinephrine and norepinephrine ASSESSMENT CUES PHEOCHROMOCYTOMA ____________ Palpitations ___________ Sweating Abdominal ______ ANALYZE CUES: PHEOCHROMOCYTOMA Physical exam Imaging Labs – 24 hour _______collection NURSING ACTIONS PHEOCHROMOCYTOMA ____________ Diet Medications -