")
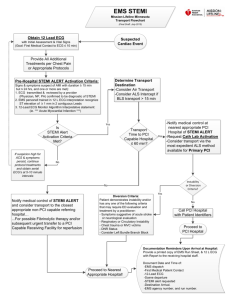
CONTINUED PROFESSIONAL DEVELOPMENT Dr Peter du Toit Travelling Fleet Supervisor – Medical Services Cell:: +39 3490875696 Email: peter.dutoit@msccruisesonboard.com ACUTE CORONARY SYNDROME(ACS) PART 3 In ACS Part 1, we focused on the early evaluation, management and risk assessment of a patient presenting with chest pain. The value of serial investigations including ECG’s and cardiac enzymes was highlighted. We reviewed the management of patients deemed to have a low risk for a major adverse cardiac event (MACE) using a clinical decision pathway (HEART score and pathway). In ACS Part 2, we focused on high-risk ACS patients, especially those that have been diagnosed with Non-ST-Elevation Myocardial Infarction (NSTEMI) or Unstable Angina. We also introduced new high risk ECG patterns and risk stratification using either the TIMI and GRACE scores. ACS Part 3 will focus on ST-Elevation Myocardial Infarction (STEMI) and other high risk ECG patterns. The concept of STEMI mimics and STEMI equivalents will be highlighted and a large portion of the CPD will focus on ECG pattern recognition. We will also look at reperfusion strategies and focus on the medical management and use of thrombolytics in a STEMI patient while at sea. ACUTE CORONARY SYNDROME ACUTE MYOCARDIAL INFARCTION UNSTABLE ANGINA ST-ELEVATION MYOCARDIAL INFARCTION NON ST-ELEVATION MYOCARDIAL INFARCTION Take time to review the articles and watch the educational videos. It is important that you have a good appreciation of the management and risk stratification of high-risk ACS cases. I have chosen the following references: 1. UPTODATE: Overview of the acute management of STEMI Overview of the acute management of ST-elevation myocardial infarction - UpToDate 2. UPTODATE: Acute ST-elevation myocardial infarction: The use of fibrinolytic therapy Acute ST-elevation myocardial infarction: The use of fibrinolytic therapy - UpToDate 3. Asatryan B, Vaisnora L, Manavifar N, et al. Electrocardiographic Diagnosis of Life-Threatening STEMI Equivalents. J Am Coll Cardiol Case Rep. 2019 Dec, Electrocardiographic Diagnosis of Life-Threatening STEMI Equivalents (jacc.org) 4. 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department https://www.sciencedirect.com/science/article/pii/S0735109722066189?via%3Dihub Certain passages and algorithms in the reference material will be highlighted in blue and author comments in gray. ** The attached UPTODATE articles are the main source of reference for this CPD** **Please allow your Team access to these articles** 1 OVERVIEW OF THE ACUTE MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION (UPTODATE) GOALS OF THERAPY • The primary goal of STEMI management is to reduce the risk of death and the extent of permanent cardiac injury associated with MI. • Therapy for patients with STEMI becomes less effective with each minute it's administration is delayed. The main goal of therapy is to rapidly treat STEMI patients while it remains effective. INITIAL ASSESSMENT • All patients with chest pain (acute coronary syndrome) should have an initial assessment with electrocardiogram, history, physical examination to rapidly confirm or exclude the diagnosis of STEMI, and to identify other conditions that may change management. • Rapid diagnosis of STEMI o The rapid diagnosis of STEMI only requires the presence of symptoms suspicious for an ACS (chest discomfort, dyspnea, cardiopulmonary arrest) and a confirmatory ECG; it does not require evidence of elevated cardiac bio-markers such as Troponin. o Patients with suspected ACS should undergo a focused history, physical, and ECG within ten minutes of hospital arrival to identify the key evidentiary features of STEMI • Characteristic symptoms and signs o The following signs and symptoms suggest the presence of STEMI: ▪ Chest pain or chest discomfort ▪ Dyspnea ▪ Ventricular arrhythmias, cardiac arrest, or syncope ▪ Atypical symptoms such as malaise, weakness, and back pain • ECG findings o ECGs should be reviewed for signs of severe myocardial ischemia, which include: ▪ ST-segment elevation with standard lead placement ▪ Newly identified left bundle branch block ▪ ST elevation with posterior or right-sided lead placement ▪ Other high-risk ECG findings (de Winter sign, transient ST-segment elevation) COMMENT: • “ECGs should be reviewed for signs of severe myocardial ischemia”. • This is a simple statement, but in practice can be one of the most difficult clinical decisions you face. • The interpretation of the patient’s presenting 12 lead ECG is a critical step in determining your initial diagnoses and subsequent treatment options. • It is important to be familiar with the following concepts: o Localization of Ischemia: determining the location of the infarction can influence further management options. o STEMI equivalents: several high-risk ECG patterns are associated with acute myocardial ischemia due to critical stenosis or occlusion of a coronary artery. o STEMI mimics: in certain cases, a patient's ECG can resemble a STEMI, yet the STsegment elevation is actually from a non-coronary-based syndrome We will focus on each of the above and highlight ECG patterns examples… 2 LOCALIZATION OF ISCHEMIA INITIAL EVALUATION AND MANAGEMENT OF SUSPECTED ACS IN THE ED (UPTODATE) LOCALIZATION OF ISCHEMIA • ECG leads are more helpful in localizing regions of transmural than subendocardial ischemia. • The anatomic location of a transmural infarct is determined by which ECG leads show ST elevation and/or increased T wave positivity: o Anterior wall ischemia ▪ Two or more of the precordial leads (V1 to V6) o Anteroseptal ischemia ▪ Leads V1 to V3 o Apical or lateral ischemia ▪ Leads aVL and I, and leads V4 to V6 o Inferior wall ischemia ▪ Leads II, III, and aVF o Right ventricular ischemia ▪ Right-sided precordial leads o Posterior wall ischemia ▪ Septal precordial leads (V1 to V2) and posterior precordial leads o The right-sided leads V4R, V5R, and V6R ▪ should be obtained if there is evidence of inferior wall ischemia demonstrated by ST elevation in leads II, III, and aVF. o The posterior leads V7, V8, and V9 ▪ may also be helpful if there is evidence of posterior wall ischemia as suggested by prominent R waves and ST depressions in leads V1 and V2. • You may find the following references useful. o UPTODATE: Electrocardiogram in the diagnosis of myocardial ischemia and infarction ▪ Available at: Electrocardiogram in the diagnosis of myocardial ischemia and infarction - UpToDate o REBEL EM ▪ Coronary Anatomy & ECG Leads - REBEL EM - Emergency Medicine Blog 3 LIFE IN THE FAST LANE: ECG LIBRARY https://litfl.com/ecg-library/ ECG Features of Anterior STEMI • ST segment elevation with subsequent Q wave formation in precordial leads (V1-6) +/- high lateral leads. • These changes are often preceded by hyperacute T waves • Reciprocal ST depression in inferior leads (mainly III and aVF) ECG Features of a Lateral STEMI • ST elevation in the lateral leads (I, aVL, V5-6). • Reciprocal ST depression in the inferior leads (III and aVF). • ST elevation primarily localised to leads I and aVL is referred to as a high lateral STEMI. 4 ECG Features of Inferior STEMI • ST elevation in leads II, III, aVF • Hyperacute T waves may precede these changes • Reciprocal ST depression in aVL • Progressive development of Q waves in II, III, aVF ECG Features of a Posterior STEMI • Changes in V1-3: o Horizontal ST depression o Tall, broad R waves (>30ms) o Upright T waves o Dominant R wave (R/S ratio > 1) in V2 • Posterior infarction is confirmed by the presence of ST elevation and Q waves in the posterior leads (V7-9). 5 ECG Features of a Right Ventricular STEMI In patients with inferior STEMI, right ventricular infarction is suggested by: • ST elevation in V1 • ST elevation in V1 and ST depression in V2 (highly specific for RV infarction) • Isoelectric ST segment in V1 with marked ST depression in V2 • ST elevation in III > II Diagnosis is confirmed by the presence of ST elevation in the right-sided leads (V3R-V6R) COMMENT: • ECG interpretation remains an essential skill for a doctor working in a remote setting. • Decisions need to be timely and accurate as further management options are dependent on your initial ECG diagnoses. • When making an ECG diagnosis, consider using either an ECG textbook or online resources to compare your ECG with other examples. • For example, if you think you are dealing with an Inferior STEMI and the ECG doesn’t match any reference ECG’s, reconsider your ECG diagnoses. • Always consult with the rest of your Team regarding your diagnoses. 6 STEMI EQUIVALENTS ELECTROCARDIOGRAPHIC DIAGNOSIS OF LIFE-THREATENING STEMI EQUIVALENTS (J Am Coll Cardiol 201 • • • • • • • • • • • • Several high-risk ECG patterns have been reported in association with acute myocardial ischemia due to critical stenosis or occlusion of a coronary artery. These patterns include: o de Winter syndrome pattern o Isolated posterior STEMI, a challenge to diagnose with a 12-lead ECG but easy to recognize with additional posterior leads V7 to V9 o Wellens syndrome with often evolving T-wave abnormality (signs A and B) o Hyperacute T waves, usually preceding recognizable ST-segment elevation; and the “shark fin” sign. Furthermore, ECG criteria have been proposed to identify acute myocardial infarction with moderate-to-high probability in patients with pre-existing conditions that alter the QRS amplitude and width, as well as the J-point and/or ST-segment on resting ECG, such as: o left bundle branch block (LBBB), o right ventricular paced rhythm, o left ventricular hypertrophy. Integration of clinical evaluation along with serial ECGs, including assessment of previous ECGs recorded at an asymptomatic state, often assists in optimal decision making. As primary percutaneous intervention (PCI) has been rapidly adopted as the default reperfusion strategy for STEMI worldwide, clearly defined criteria are essential for accurate diagnosis and timely referral of patients. In current practice, ST-segment elevation at the J-point, ≥1 mm in ≥2 adjacent leads (other than leads V2 and V3, where elevation of ≥2 mm in men or ≥1.5 mm in women is considered significant) or a new LBBB is commonly used for STEMI diagnosis. However, these general ECG criteria fail to identify the STEMI equivalents. Therefore, patients with STEMI equivalents who do not present with these typical ECG changes despite having an acutely occluded coronary artery are more likely to undergo a delayed revascularization. Although clinicians caring for patients presenting with chest pain rely upon ECG findings as the essential non-invasive test for identifying those who might benefit from primary PCI, their awareness of these high-risk ECG patterns are pivotal in early recognition to provide adequate treatment. However, currently, the STEMI equivalents are neither adequately covered in teaching curricula nor properly addressed by the current guidelines. The authors certainly acknowledge that the ECG by itself is often insufficient to diagnose acute myocardial ischemia or infarction and that all ECG findings should be interpreted in the setting of clinical presentation. Fine-tuning our recognition of this wide range of ECG patterns, hinting for potentially lifethreatening coronary stenosis or occlusion, may allow faster diagnosis, resulting in proper treatment and improved patient outcomes. 7 8 COMMENT: • It is important to stress the above point: o STEMI equivalents are not yet adequately covered in teaching curricula or properly addressed by the current guidelines. • The literature is clear that there are several high-risk ECG patterns associated with acute myocardial ischemia due to critical stenosis or occlusion of a coronary artery. • These high-risk ECG patterns are known as STEMI equivalents and represent coronary occlusion without meeting the traditional ST-elevation criteria. • The literature is clear that patients diagnosed with these patterns need to be considered high risk similar to STEMI patients and require urgent referral to a cardiac unit for management via PCI or potentially, an early invasive strategy. • The literature is NOT clear as to which patterns are considered STEMI equivalents, and which are only considered high risk patterns. • The literature is clear they need a cardiac review and possible PCI, but the literature is not clear whether these ECG patterns fulfill ECG criteria for thrombolysis. • In 2022, the American College of Cardiology (ACC) published an Expert Consensus regarding Decision Pathways on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department. • For the purpose of the consensus document, the ACC classified ECG’s into the following groups and management options: 9 The following YOUTUBE lecture, STEMI Equivalents is an excellent resource that clearly explains some of the various STEMI equivalents to look out for. • • Available at: (299) STEMI Equivalents - YouTube Department of Emergency Medicine | Saint John QUICK TIPS on STEMI equivalents o QUICK TIPS on STEMI equivalents | Department of Emergency Medicine | Saint John (sjrhem.ca) 10 STEMI MIMICS COMMENT: STEMI MIMICS • Up until now, we have been focusing on the rapid identification of a STEMI on a 12 lead ECG. • The quicker we make the diagnoses, the sooner we can consider a reperfusion strategy and potentially save a life! • Now we will introduce the concept of Mimics of ST Elevation Myocardial Infarction (STEMI) o In certain cases, a patient's ECG can resemble a STEMI, but the ST-segment elevation is caused by a non-coronary-based syndrome. o These circumstances are termed the STEMI mimics (other causes of ST elevation) and include benign early repolarization, acute pericarditis, and left ventricular aneurysm to name only a few. • Misdiagnosing a STEMI can potentially do harm from administering thrombolytics inappropriately and endangering the patient. • Remember the pitfalls of jumping to conclusions too early. o Beware confirmation bias, anchoring bias, and premature closure. • Always re-evaluate your diagnosis at critical decision-making points such as during admission and before thrombolysis. • LIFE IN THE FAST LANE (LITFL) is an excellent resource to review examples of ECG patterns • Below are some examples of ECG patterns that causes ST segment ELEVATION which can be mistaken for STEMI. • Please follow the above links to familiarize yourself with the above ECG patterns. o Causes of ST Segment Elevation (The ST Segment • LITFL • ECG Library Basics) ▪ ACUTE MYOCARDIAL INFARCTION ▪ CORONARY VASOSPASM (PRINTZMETAL’S ANGINA) ▪ PERICARDITIS ▪ BENIGN EARLY REPOLARIZATION ▪ LEFT BUNDLE BRANCH BLOCK ▪ LEFT VENTRICULAR HYPERTROPHY ▪ VENTRICULAR ANEURYSM ▪ BRUGADA SYNDROME ▪ VENTRICULAR PACED RHYTHM ▪ RAISED INTRACRANIAL PRESSURE ▪ TAKOTSUBO CARDIOMYOPATHY 11 • Morphology of the Elevated ST segment o Myocardial Infarction ▪ Acute STEMI may produce ST elevation with either concave, convex or obliquely straight morphology. o • ST Segment Morphology in Other Conditions Other refences to review: o STEMI Mimics You’ve Got to Know! By Amal Mattu, MD ▪ Available at: (164) STEMI Mimics You’ve Got to Know! | The Heart Course – YouTube o STEMI mimics (fabnhsstuff.net) 12 COMMENT: • We will now continue to review of the management of an ST-ELEVATION MYOCARDIAL INFARCTION OVERVIEW OF THE ACUTE MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION (UPTODATE) • Monitoring and testing: o For patients with STEMI, initial monitoring and testing typically include the following: o General measures ▪ Patients with STEMI require frequent blood pressure measurements, continuous heart rhythm monitoring, and continuous pulse oximetry. ▪ Laboratory studies • All patients with STEMI should have laboratory studies to evaluate for metabolic abnormalities, acute kidney injury, anemia, thrombocytopenia, and coagulopathy. Troponin levels should be obtained, but the acute management of STEMI does not require elevated troponin levels. BNP is a good indicator of the presence and degree of cardiac failure. ▪ Imaging studies • Patients with STEMI should have a chest x-ray to evaluate for other causes of chest discomfort and to assess the complications of MI (eg, pulmonary edema). • Evaluation for life-threatening conditions o The initial assessment of patients with STEMI includes a brief evaluation for conditions that require additional treatment or that alter the approach to STEMI therapy. These conditions include: ▪ Shock • Patients with STEMI should be assessed for evidence of shock and, if present, for signs or symptoms (eg, cool extremities, jugular venous distension) that help to characterize the type of shock (ie, cardiogenic, distributive). • Patients with shock require specific management of shock as well as appropriate and timely reperfusion. ▪ Heart failure • All patients with STEMI should be assessed for signs and symptoms of heart failure (orthopnea, jugular venous distension, pulmonary edema). ▪ Aortic dissection • Aortic dissection is a rare cause of STEMI but should be considered in all patients with STEMI. The signs and symptoms of aortic dissection include severe pain or tearing located in the chest or back, asymmetric upper extremity pulses or pulse deficits, new aortic valve murmurs, and widening of the mediastinum on chest x-ray. Patients with STEMI caused by aortic dissection require management that is different from the typical management of STEMI. ▪ Coagulopathy and/or thrombocytopenia • The management of patients with STEMI typically requires treatments that increase the risk of bleeding. All patients with STEMI should be assessed for chronic use of anticoagulant or antiplatelet medications, history of bleeding or coagulation disorders (uremia, heparin-induced thrombocytopenia), and the presence of abnormal coagulation studies or thrombocytopenia. 13 COMMENT: • Imaging studies o Do not delay thrombolysis for a CXR if the ECG is diagnostic. o Where there is diagnostic uncertainty, then serial ECG’s and further investigations including CXR’s are indicated. • OVERVIEW OF THE ACUTE MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION (UPTODATE) INITIAL MANAGEMENT • The initial management of patients with STEMI requires rapid selection and administration of reperfusion therapy. • Patients with STEMI should also receive treatments that prevent further coronary artery thrombosis, minimize myocardial injury, and treat the symptoms of MI. • Choosing and initiating reperfusion with PCI or fibrinolysis o For patients diagnosed with STEMI, the primary goal of acute management is to rapidly restore blood flow to the acutely occluded coronary artery (culprit artery) with a reperfusion therapy (percutaneous coronary intervention [PCI], fibrinolysis) o A reperfusion strategy should be chosen within minutes of arrival. 14 • Key factors that influence the choice of reperfusion strategy include: o Time delay between first medical contact and performance of PCI o Time from symptom onset to presentation o Presence of cardiogenic shock o Diagnostic uncertainty o Contraindications to PCI or fibrinolysis o High-risk factors that favor no reperfusion COMMENT: • It is obvious from the literature that Primary PCI is the reperfusion strategy of choice. • Primary PCI is only an option if the ship is in PORT; the port has access to a PCI facility, AND you are able to transfer your patient within 120minutes from first contact. • The use of local emergency services is critical and the urgency of the case needs to communicated to both the onboard and shoreside teams to ensure a speedy disembarkation. • Fibrinolytic therapy. o It is more likely that you will need to consider fibrinolysis in the cruise ship setting. o Fibrinolytic therapy MIGHT be a procedure you have not performed before, but it is an essential protocol that you need to be familiar with, much like resuscitation and rapid sequence induction. o o o Fibrinolytic therapy is a time-critical procedure. Any significant delay in fibrinolysis will result is increased morbidity or even mortality. Aim for a door-to-needle time of 30 minutes or less. ACUTE ST-ELEVATION MYOCARDIAL INFARCTION: THE USE OF FIBRINOLYTIC THERAPY (UPTODATE) BACKGROUND • Fibrinolytic (ie, thrombolytic) therapy, when administered within the first several hours after symptom onset, is capable of reestablishing antegrade coronary artery blood flow in nearly 75 percent of patients with STEMI. • The restoration of myocardial blood flow is key to improving cardiovascular outcomes. • The benefit of fibrinolytic therapy declines rapidly as the time from onset of symptoms to therapy increases beyond three hours. • After 12 hours, the risk may exceed the benefit. • All fibrinolytic agents, compared with placebo, reduce mortality in acute STEMI. The magnitude of reduction in risk of death in randomized trials is generally between 15 and 30 percent. 15 INDICATIONS FOR FIBRINOLYTIC THERAPY • All STEMI patients who cannot receive primary percutaneous coronary intervention (PCI) in a timely manner should be immediately considered for fibrinolytic therapy. • Fibrinolytic therapy should not await the availability of results of cardiac biomarkers if the diagnosis is reasonably certain. • Patients with chest pain suggestive of acute myocardial ischemia who present up to 12 (and possibly up to 24) hours after symptom onset are candidates for fibrinolytic therapy if the following electrocardiographic evidence is present: o New ST elevation at the J point in two anatomically contiguous leads using the following diagnostic thresholds: ▪ ≥0.1 mV (1 mm) in all leads other than V2 to V3, where the following diagnostic thresholds apply: • ≥0.2 mV (2 mm) in men ≥40 years • ≥0.25 mV (2.5 mm) in men <40 years • ≥0.15 mV (1.5 mm) in women o Patients with typical and persistent symptoms in the presence of a new or presumably new left bundle branch block or a true posterior MI are also considered eligible. CONTRAINDICATIONS FOR FIBRINOLYTIC THERAPY • Absolute contraindications to fibrinolytic therapy include: o Prior intracranial hemorrhage (ICH), o Known structural cerebral vascular lesion, o Known malignant intracranial neoplasm, o Ischemic stroke within three months, o Suspected aortic dissection, o Active bleeding or bleeding diathesis, o Significant closed-head or facial trauma within three months. • Important relative contraindications include: o Poorly controlled or chronic sustained hypertension (ie, systolic BP >180 mmHg). o Ischemic stroke more than three months previously. o Dementia or other intracranial pathology (except as above). o Traumatic or prolonged cardiopulmonary resuscitation (>10 mins) or major surgery (within <3 weeks). o Recent (within two to four weeks) internal bleeding. o Noncompressible vascular puncture. o For streptokinase, prior exposure (more than five days previously and up to one year) or prior allergic reaction to these agents. o Pregnancy. o Active peptic ulcer. o Current use of anticoagulants. 16 COMMENT: • STEMI: Indications for thrombolysis: o It is important to know the CURRENT standard criteria for STEMI and the indications for thrombolysis are based on the Fourth Universal Definition of Myocardial Infarction (2018) ACUTE ST-ELEVATION MYOCARDIAL INFARCTION: THE USE OF FIBRINOLYTIC THERAPY (UPTODATE) Patients with chest pain suggestive of acute myocardial ischemia who present up to 12 (and possibly up to 24) hours after symptom onset are candidates for fibrinolytic therapy if the following electrocardiographic evidence is present: • New ST elevation at the J point in two anatomically contiguous leads using the following diagnostic thresholds: o ≥0.1 mV (1 mm) in all leads other than V2 to V3, where the following diagnostic thresholds apply: o ≥0.2 mV (2 mm) in men ≥40 years o ≥0.25 mV (2.5 mm) in men <40 years o ≥0.15 mV (1.5 mm) in women • Patients with typical and persistent symptoms in the presence of a new or presumably new left bundle branch block or a true posterior MI are also considered eligible. o Where the ST-elevation is not that pronounced, ensure you correctly measure the ST elevation: ▪ Electrocardiogram example of ST-segment elevation. The initial onset of the Q wave shown by arrow 1 serves as the reference point and arrow 2 shows the onset of the ST-segment or J-point. The difference between the two identifies the magnitude of displacement. Measurements of both arrows should be made from the top of the electrocardiogram line tracing. Fourth universal definition of myocardial infarction (2018) | European Heart Journal | Oxford Academic (oup.com) 17 • Once you have determined ST-elevation is present you should: 1. Rule out STEMI mimics. 2. Determine location of ischemia 3. Determine whether you need additional leads to confirm your suspicion and it might also affect your further management. 4. Compare your STEMI diagnoses with other ECG examples for additional confirmation. 5. Review ST-elevation and whether the ECG pattern meets STEMI criteria for fibrinolysis. 6. If criteria for fibrinolysis is not met, treat as NSTEMI/High risk ACS o Continue to monitor for ECG changes as criteria might be met later if there are dynamic changes. 7. If criteria for fibrinolysis is met: o Review for contra-indications to fibrinolytic therapy o Discuss fibrinolysis with the patient and obtain a signed consent if the patient consents to the procedure. 8. Review all medical management including adjunctive therapy. COMMENT: • STEMI equivalents o This is where it becomes more complicated. o As the previous author noted, the current guidelines have not kept pace with the latest information we have gained regarding STEMI equivalents and other high risk ECG patterns. o According to the ACC consensus document: ▪ In the ED, the initial ECG should be examined for signs of ischemia, particularly for STEMI or a STEMI equivalent, as this identifies patients who should undergo immediate reperfusion therapy and be managed in accordance with the 2013 STEMI guideline. ▪ Emergent consultation for expert over-read should be obtained for ECGs concerning for ACS that lack clear diagnostic criteria. o Expert opinion is not always available, which is why you need to have good understanding of ECG’s. You can use UpToDate and LITFL as resources to guide you. o Some STEMI equivalents are eligible for thrombolysis and should be managed accordingly: ▪ Posterior STEMI ▪ Left bundle branch block or ventricular paced rhythm with Sgarbossa Criteria ▪ Left bundle branch block or ventricular paced rhythm with Smith-modified Sgarbossa Criteria o However, De Winter pattern and Hyperacute T waves are not included in the current fibrinolysis criteria. o There are case reports of patients with chest pain and the de Winter ECG pattern who have received thrombolysis, but this has not yet become part of the mainstream criteria. • • • Thrombolytic therapy in a patient with chest pain with de Winter ECG pattern occurred after ST-segment elevation: A case report - PubMed (nih.gov) Thrombolysis in the de winter electrocardiography pattern: A therapeutic dilemma Kumar A, Chetiwal R, Tanwar S, Gupta S, Kumar R - J Pract Cardiovasc Sci (j-pcs.org) Thrombolytic therapy to the patients with de Winter electrocardiographic pattern, is it right? | QJM: An International Journal of Medicine | Oxford Academic (oup.com) 18 So, how do we manage patients presenting with STEMI equivalents and High Risk ECG patterns onboard a cruise ship? • There is no simple answer, and each case will need to be managed according to the clinical picture, serial ECG pattern, access to local facilities, possible use of expert opinion, referring to current guidelines, and utilizing online resources like UpToDate. • The ACC (American College of Cardiology) recommends that STEMI equivalents are treated as high-risk ECG patterns and need immediate referral for a cardiac opinion and transfer to a PCI lab. • If you are in port: o patients diagnosed with STEMI equivalents and High-Risk ECG patterns should be immediately disembarked to a local hospital for a cardiac opinion and possible referral to a PCI lab • If you are at sea o Patients diagnosed with STEMI equivalents and High-Risk ECG patterns need to be managed as a High-risk ACS patient until you have managed to medically disembark them. o Consider thrombolysis if they fulfill the criteria for: ▪ Posterior STEMI ▪ Left bundle branch block or ventricular paced rhythm with Sgarbossa Criteria ▪ Left bundle branch block or ventricular paced rhythm with Smith-modified Sgarbossa Criteria o If they do not fulfill the current STEMI criteria or eligibility for thrombolysis then consider managing these patients initially as a NSTEMI and seek expert help. o ▪ DeWinter pattern ▪ Hyperacute T-waves ▪ aVR ST-segment elevation ▪ ST-segment depression ▪ Wellen’s syndrome ▪ Inverted T waves It is important to continually repeat the ECG and monitor for dynamic ST-segment changes. o There is a chance that the dynamic ECG changes result in an patient meeting the STEMI criteria. o Discuss the case with the Medical Operations Team as the patient may be considered for a medical disembarkation and referral ashore for primary PCI strategy. 19 ACUTE ST-ELEVATION MYOCARDIAL INFARCTION: THE USE OF FIBRINOLYTIC THERAPY (UPTODATE) INITIATION OF THERAPY • For patients with STEMI in whom fibrinolysis is chosen as the reperfusion strategy (when primary percutaneous coronary intervention is not available), treatment should be given as soon as possible after the diagnosis. • Timing o Door-to-needle time - the time time from first medical contact (whether it be in an ambulance capable of delivering fibrinolytic therapy or a hospital emergency department) to drug administration should be less than 30 minutes. Ideally, fibrinolytic therapy should be delivered within 10 minutes of STEMI confirmation on the electrocardiogram. o As a patient's door-to-needle time increases, the benefit from therapy decreases. o The survival benefit is greatest when fibrinolytic agents are administered within the first four hours after onset of symptoms, but particularly within the first 70 minutes. o Early therapy also has the greatest impact on infarct size and left ventricular ejection fraction o A mortality benefit is less likely with fibrinolytic therapy at 13 to 18 hours. o However, there may be a benefit in patients presenting 12 hours after symptom onset and possibly up to 24 hours if the patient has ongoing or stuttering chest pain. • Choice of agent o We prefer fibrin-specific agents over streptokinase, and third-generation agents (tenecteplase and reteplase) over alteplase based on their generally favorable benefit-to-risk profile and ease of use. • Concomitant Therapies. o All STEMI patients receiving fibrinolytic therapy should receive the following therapies as soon as possible after the diagnosis is made: o Anticoagulant therapy ▪ We treat all STEMI patients receiving fibrinolytic therapy with an anticoagulant. ▪ It should be started as soon as a decision to treat with fibrinolytic therapy is made. ▪ We choose either unfractionated heparin or enoxaparin for patients, including those who may receive PCI after fibrinolysis. o Antiplatelet therapy ▪ We give nonenteric-coated aspirin (loading dose of 162 to 325 mg) as soon as possible after the diagnosis has been made. ▪ Once fibrinolysis is chosen as the reperfusion strategy, we give clopidogrel as a 300 mg loading dose in those ≤75 years of age and a 75 mg loading dose in those >75 years. o Statins ▪ For all patients with an acute coronary syndrome not on treatment with a statin, we initiate high-intensity statin therapy (80 mg of atorvastatin or 20 to 40 mg of rosuvastatin daily) regardless of the baseline low density lipoproteincholesterol level. We start therapy as soon as possible after the diagnosis. o Beta blocker ▪ For all patients with acute MI, we recommend initiation of oral beta blockers within the first 24 hours, as long as no contraindications are present. However, early initiation of intravenous beta blocker in the emergency department should be avoided in most patients and in particular those with cardiogenic shock. 20 COMMENT: • Ensure you have discussed both the benefits and risks with your patient. • Use a translator if needed. • The patient should sign a consent form agreeing to the procedure. • Here is an example of the verbiage you could use: Consent for Thrombolysis: ‘It is likely that you have suffered a heart attack, and the best treatment is a clot dissolving drug called xxx. The quicker you receive this drug, the lower the risk from the heart attack – which is why doctors recommend the treatment is started as soon as possible. These drugs can cause serious side effects in a small minority of patients which I can explain to you in more detail if you so wish, but the risks attached to this treatment are very much less than the likely benefit. Would you like me to give you the injection or would you prefer to have more details?’ In the unlikely event that patients do want more information they should be given the following information:‘Treatment at this stage saves the lives of about 4 patients for every 100 we treat. But it can sometimes cause serious bleeding. The biggest risk is stroke which affects about 1 patient in every 200. Some patients also have allergic and other effects that do not usually cause any major problem. https://www.jrcalc.org.uk/jrcalc-suggested-consent-for-thrombolysis/ 21 UPTODATE: OVERVIEW OF THE ACUTE MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION • • • After the fibrinolytic agent and its associated treatments have been given, the patient should be monitored for their response to fibrinolysis. Patients with evidence of failed fibrinolysis or hemodynamic instability may benefit from urgent PCI. Patients with STEMI who were initially treated with fibrinolysis may benefit from routine PCI (pharmacoinvasive strategy) in the hours or days following successful fibrinolysis. Post Fibrinolysis complications • Bleeding o Bleeding is the primary complication of fibrinolytic therapy, and hemorrhagic stroke is the greatest concern. The most common site for spontaneous bleeding is the gastrointestinal tract • Stroke o The risks of stroke and intracranial hemorrhage (ICH) are 1.2 and 0.7 percent. Strokes associated with fibrinolysis are also associated with very high rates of mortality and morbidity. • Primary failure of fibrinolysis: o Often clinically suspected by persistent or worsening chest pain (particularly if associated with other symptoms such as dyspnea and diaphoresis), persistent or worsening ST-segment elevation on the ECG, hemodynamic instability, and/or heart failure. o Repeat fibrinolysis for failed primary fibrinolysis is usually considered when access to PCI is not available. • Re-occlusion o Re-occlusion of an infarct-related artery after reperfusion therapy is associated with a significant increase in mortality. • • • • Heart failure o In addition to appropriate reperfusion, patients with STEMI and HF may require therapy for volume overload (eg, diuretics) and respiratory distress (eg, supplemental oxygen, positive pressure ventilation) Arrhythmias o In patients with STEMI, the management of arrhythmias is focused on advanced cardiac life support (ACLS) for unstable patients, rapid reperfusion, and additional therapies that reduce the risk of arrhythmias. Prophylactic use of antiarrhythmics. o During the early phases of acute MI, ventricular arrhythmias (eg, premature depolarizations, nonsustained ventricular tachycardia) are common. o However, antiarrhythmic agents (other than beta blockers) are not typically used to prevent ventricular arrhythmias in acute MI. Right ventricular infarction o Patients with right ventricular infarction may require additional management of complications such as bradyarrhythmias, hypotension, and shock. Cardiogenic shock o In addition to specific therapies for shock, patients with shock typically benefit from rapid reperfusion. 22 COMMENT: • Once you have administered your fibrinolytic agent and adjuncts, it is important to closely monitor the patient for any reperfusion arrhythmias, hemodynamic or neurological changes. • Take serial 12 lead ECG’s so you can monitor any ST segment changes. o If the ST segments do not show evidence of resolution at 90 minutes, and the patient has on-going symptoms, then you will need to discuss with the MedOps team as matter of urgency. o Failure of fibrinolysis is often suspected by ongoing or worsening chest pain, persistent or worsening ST-segment elevation on ECG, hemodynamic instability, and/or heart failure. o Needless to say, these are critical patients and immediate referral ashore should be considered. • Patients with successful fibrinolysis need to remain admitted to the medical centre and medically disembarked at the next available port. • Monitor continuously for any signs of bleeding for the first few hours after tenecteplase. o Should serious bleeding (not controlled by local pressure) occur, any concomitant anticoagulant or antiplatelet agents should be discontinued immediately • Perform the following observations for at least 4 hours: o Monitor continuously for signs of internal bleeding (tachycardia, hypotension, pallor, restlessness, lower back pain, new muscle weakness/numbness in lower extremities). o Assess for external bleeding (e.g. IV sites, gums) hourly o Urine full ward test each void or 1/24 post dose for indwelling catheter. o Faecal occult blood test if bowels opened. o Blood pressure (with manual blood pressure cuffs to avoid bruising from over-inflation from automatic blood pressure machines), HR, RR, Sa02, temp and GCS at baseline, then every 15 minutes for the first hour post tenecteplase, followed by half hourly. o A change in GCS should be reported • Many hospitals have admission proformas that also include nursing care plans. • There are various nursing plans available online. • One of the most comprehensive is Nurseslabs.com and is worth using as a reference site. o 8 Myocardial Infarction (Heart Attack) Nursing Care Plans - Nurseslabs o Nursing Interventions and Actions o Therapeutic interventions and nursing actions for patients with myocardial infarction may include: 1. Initiating Pain Relief and Ischemia & Improving Respiratory Function 2. Monitor Laboratory and Diagnostic Tests 3. Administering Medication and Pharmacologic Support 4. Improving Cardiac Output & Monitoring Potential Complications 5. Improving Tissue Perfusion & Initiating Cardiac Rehabilitation 6. Reducing Anxiety and Fear 7. Improving Tolerance to Activity 8. Initiating Health Education & Teaching • In ACS part 2 we discussed the use of Doctor’s admission orders using the ADC VANDALISM mnemonic. • We will again look at doctor’s orders, now focusing on STEMI patients. • It is especially the post-thrombolysis period where close monitoring and one-to-one nursing is essential. • Although these are standard orders for nurses, it would be recommended that the duty doctor also stay with the patient for at least 4 hours post successful reperfusion to monitor for any arrhythmias and complications. • Below is a suggested DOCTOR’S ORDERS for a post-thrombolytic STEMI patient 23 Doctor’s Orders for STEMI/Thrombolysis patients should include: ADMIT to ICU DIAGNOSIS: STEMI CONDITION: Critical VITALS: Monitored and recorded pre-thrombolytic therapy; then post thrombolytic therapy every 15 minutes for the first 2 hours, then ½ hourly for 2 hours, hourly for 4 hours, then 4 hourly if stable. Use manual blood pressure cuffs to avoid bruising from over-inflation from automatic blood pressure machines. Neuro Vital signs include: Assessment of conscious level (GCS), Limb assessments and Pupil size and reaction to light. Monitored and recorded pre-thrombolytic therapy; then post thrombolytic therapy every 15 minutes for the first 2 hours, then ½ hourly for 2 hours, hourly for 4 hours, then 4 hourly if stable Parameters for notifying duty doctor if: □ T >38°C, SBP >190 mmHg or SBP <90 mmHg, HR >120 bpm or HR <50 bpm, RR >30 or RR <10 or drop in GCS, perceived weakness or pupillary changes. O2 saturation: Supplemental oxygen should be administered if arterial saturation less than 90%, respiratory □ distress, or other high-risk features for hypoxemia. If required, supplemental oxygen must be administered via a mask as nasal prongs can cause nasal mucosa damage. ACTIVITY: Strict rest in bed is required for 24 hours, but longer if unstable. Falls prevention NURSING INSTRUCTIONS: Bleeding: Monitor continuously for any signs of bleeding for the first few hours after thrombolysis. □ Should serious bleeding (not controlled by local pressure) occur, any concomitant anticoagulant or antiplatelet agents should be discontinued immediately. □ Pressure dressings should be applied to puncture sites to reduce risk of haematoma formation. Risk: □ During, and for 48 hours after thrombolysis due to the increased risk of bleeding, unnecessary invasive procedures should be avoided, as should IM injections, wet-shaving, use of rigid catheters, vigorous brushing of teeth and nonessential handling of the patient. □ Venepuncture must only be undertaken with care. SeaCare: □ Place in Inpatient module and complete assessments DIET: Low salt and cholesterol ALLERGIES (to food & Meds): review LABS AND INVESTIGATIONS: □ 12 lead ECG: ECG’s should be recorded pre-thrombolysis and then at 60 minutes and 90 minutes post-thrombolysis. Repeat if any changes in ECG morphology, arrythmias, new onset chest pain and every 8 hours. □ Cardiac enzymes: at 6 hr and 12 hr post thrombolysis. Then 8 hourly □ Electrolytes, haematolgy, random blood glucose and LFT's: at 6 hr and 12 hr post thrombolysis. Then 8 hourly □ Stat: BNP (monitor for heart failure), random cholesterol and possibly D-dimer if indicated. □ Guaiac fecal occult blood test (FOB) with every stool □ CXR if not already completed 24 IV FLUIDS: As charted SPECIALISTS OR CONSULTS: Disembarkation details MEDICATIONS: □ Analgesia. If ongoing ischemic discomfort consider sublingual Glyceryl Trinitrate (GTN) 0.4 mg every 5 min for a total of 3 doses, after which assessment should be made about the need for IV GTN, if not contraindicated. □ Review: Antiplatelet therapy, Anticoagulation, Statins, B-blockers and PPI's. □ Review patient’s own medications. □ As needed meds: Review need for: Night sedation, Paracetamol for headaches and constipation relief MONITORING: □ Continuous ECG and O2 sats monitoring to monitor closely for arrhythmias for a minimum of 48 hours, and defib/pacing pads in-situ for the first 24 hours. □ Monitor fluid input and output. COMMENT: • STEMI/ post thrombolysis patients are critical patients and need urgent referral ashore. • Even those that underwent successful thrombolysis could still be eligible for PCI o In Port: ▪ Patients should be disembarked to a local medical facility, preferably with cardiac catheter lab capabilities. ▪ If you are in a port without cardiac facilities, discuss the possibility of a medevac to a cardiac unit in an alternative location with MEDICAL OPERATIONS o At Sea: ▪ While at sea, we can only offer thrombolysis as a reperfusion strategy. ▪ Even with successful thrombolysis, these patients remain critical and at risk of serious complications. ▪ Early communication with MEDICAL OPERATIONS is essential to determine medical evacuation options. ▪ According to: UptoDate: Risk stratification after acute ST-elevation myocardial infarction • In general, risk stratification does not influence the acute management of patients with STEMI. • Patients with STEMI can undergo risk assessment with either the TIMI risk score or the GRACE risk model. • These tools include predictors of poor outcomes identified in large databases of patients with STEMI. • A report published in 1998 from the National Registry of Myocardial Infarction (NRMI) evaluated data on 170,143 patients admitted with an acute MI (with or without ST-segment elevation) in an attempt to identify patients at high risk • Significant risk factors included age over 70 years, prior MI, Killip class at admission anterior MI, and the combination of hypotension and tachycardia. ▪ Although ALL STEMI patients are considered high risk patients, it is worth doing a risk assessment as it could influence the medical evacuation options. ▪ Patients with high-risk features, especially failed thrombolysis, would warrant the possibility of a more urgent medical evacuation. 25 o Communication Clear and concise communication with the Medical Operations Team is important to ensure both parties’ expectations are met. ▪ Below is a STEMI AND POST THROMBOLYSIS COMMUNICATION CHECKLIST that you should refer to prior to contacting MEDICAL OPERATIONS. ▪ Timing: • Thrombolysis is a time critical procedure. • Do not delay thrombolysis to speak to MedsOps about your patient. ▪ Preparation • It is important to be prepared BEFORE you make this call • In a STEMI scenario uploading the ECG’s into SeaCare is essential ▪ Advise • Clinical advice can always be sought when you have diagnostic or therapeutic uncertainties. • However, ensure you have already referred to UptoDate, other clinical reference sites including LITFL and discussed the case with your colleagues before reaching out to MedOps. Communicate using the SBAR tool: ▪ Situation (WWW.Y) ▪ o ▪ ▪ ▪ • Who you are. • Where you are calling from. • Who you are speaking about. • WhY you are calling. Background • Age, Gender • Presenting Complaint • Brief summary of relevant background history Assessment • Vitals/Scores and key clinical findings • Relevant tests & treatments carried out so far • (Differential) Diagnosis • Any specific major concern Recommendation • “My plan for this patient is….” • “I think this patient requires disembarkation for the following reasons..” • “Can we discuss / review…” • “Is there anything I need to do in the meantime?” 26 MEDICAL OPERATIONS (URGENT 24/7 MOBILE: +44 (0) 7770451054) STEMI AND POST THROMBOLYSIS COMMUNICATION CHECKLIST □ PREPARE □ Ensure you have all the details you need at hand before starting the call. □ SEACARE □ Time permitting, complete the notes as best you can. Focus on history, serial vitals and medications administered □ Upload ECG’s and laboratory results if possible before contacting Medical Operations □ SITUATION: □ Identify yourself □ Identify the vessel □ State current location (use either the departing port or the next port as reference) □ State your concern: □ BACKGROUND: □ Patient identifiers and other relevant data: □ Patient name: □ DOB: □ Age □ Male/Female □ Nationality: □ Weight: □ Cabin no: □ NOK: □ Other relevant data: □ History of presenting illness (add times if relevant) □ Relevant medical history □ ASSESSMENT: □ Current vitals with trend □ Current clinical assessment □ 12 lead ECG findings (also note serial changes) □ Laboratory results, especially cardiac enzymes, BNP (also note serial changes) □ Risk: TIMI/GRACE SCORE: HIGH-RISK CHARACTERISTICS: □ Working diagnosis: STEMI □ Brief synopsis of the treatment to date including: □ Thrombolysis administered? □ Yes: What time? Door to needle time: □ No: Reason for not administering: Course of the admission: Course of the admission: □ Concern: □ RECOMMENDATION □ Explain what you need – be specific about request and time frame. □ Make suggestions. □ Clarify expectations. 27 LESSONS LEARNED AND PITFALLS • In each CPD module we will discuss LESSONS LEARNED and highlight potential PITFALLS LESSONS LEARNED • Bias leading to potential harm. o An incident was noted where ST-elevation was noted and an immediate but incorrect diagnois of STEMI was made, resulting in possible harm to the patient. o Beware confirmation bias, anchoring bias, and premature closure. o During your initial assessment of the ECG, you should always review your differential diagnoses of other causes of ST elevation (STEMI mimics) o Compare the ECG with other reference ECG’s. o Re-evaluate the diagnosis at critical decision-making points during admission and again before administration of thrombolytics. • Failure to provide thrombolysis. o An incident was noted where thrombolysis was initially withheld due to the treating doctor’s reluctance to perform the procedure. o The unwillingness stemmed from the doctor’s concern that they had not performed this procedure before. o We know that the survival benefit is greatest when fibrinolytic agents are administered within the first four hours after onset of symptoms, and particularly within the first 70 minutes. o This is a case where doing nothing causes more harm to your patient. o Doctors working in remote settings need to be skilled in emergency medicine as they are at times the only treating physician available. o If you are called upon to perform a procedure for the first time, then always weigh up the risks and benefits of the procedure to your patient. o Thrombolysis does carry a risk of intracerebral bleeding but administered within the first several hours after symptom onset, is capable of reestablishing antegrade coronary artery blood flow in nearly 75 percent of patients with STEMI, thereby greatly reducing the chance of morbidity and mortality thereby greatly benefiting your patient. o Not performing thrombolysis when indicated can lead to significant malpractice lawsuits that are ultimately indefensible. • Delayed thrombolysis o An incident was noted where thrombolysis was delayed. o Although the onboard Team successfully administered thrombolysis, it took them more than 40 minutes from the time the crew member presented with chest pain. o There was no diagnostic uncertainty and delay was simply due to the Team not realizing that time is muscle. o Managing a STEMI is complicated and requires multiple interventions. Ensure your whole Team is available and delegate tasks to ensure you can perform thrombolysis and quickly and safely as possible. o HOWEVER, when there is diagnostic uncertainty, it is good practice to HOLD OFF thrombolysis until you are sure you are dealing with a STEMI. Time is still critical, so consider serial ECG’s (every 15 minutes), perform other investigations where needed and consult with a colleague where possible. If the patient ultimately does have a STEMI, comment in your notes the reason for the delay. 28 PITFALLS: • Benign Early Repolarization (BER) o BER is a relatively common ECG pattern found amongst our crew and an ECG pattern you need to be familiar with. o Crewmembers presenting with chest pain need to be taken seriously and evaluated for possible ACS. o Although many will ultimately be diagnosed with musculoskeletal pain or dyspepsia, it is always prudent to consider ACS. o BER is usually a benign ECG pattern, however it looks very similar to pericarditis or acute MI. o Benign Early Repolarisation • LITFL • ECG Library Diagnosis ▪ Benign Early Repolarization (BER) is a usually benign ECG pattern producing widespread ST segment elevation that is commonly seen in young, healthy patients < 50 years of age. ▪ Also known as “high take-off” or “J-point elevation”, ▪ It may mimic pericarditis or acute MI. o ECG Features ▪ Widespread concave ST elevation, most prominent in the mid-to-left precordial leads (V2-5) ▪ Notching or slurring at the J point ▪ Prominent, slightly asymmetrical T waves that are concordant with the QRS complex ▪ ST elevation: T wave height ratio in V6 < 0.25 (see below) ▪ No reciprocal ST depression to suggest Occlusion MI J-point morphology • One characteristic feature of BER is the presence of a notched or irregular J point: the so-called “fish hook” pattern. This is often best seen in lead V4. • ECG Fish-hook pattern BER If you are unsure whether you are dealing with a BER, simply follow the SUSPECTED ACS PATHWAY which will includes doing serial ECGs, looking for dynamic changes in the ECG. ▪ o 29 FINAL COMMENT: • Although ACS is a time critical event, never rush your decisions. Repeating an ECG, discussing the case with a colleague or simply consulting a reference article might help you make the correct diagnosis and stop you doing harm. • The management of ACS includes multiple medications including GTN and B-Blockers. When these medications are indicated, use them with caution. Titrate to response. There is no point doing everything right and then managing a severe hypotension because you were too aggressive with either drug. • Managing a STEMI on a cruise ship, while you are at sea, will be one of the most stressful clinical cases you will be expected to manage. • • Ensure you are prepared: o Know where all your ACS drugs are. o Ensure they are in date, and you have sufficient supplies. o Consult checklists to remind you what steps to take or what medications to prescribe. When managed well, these are some of your most rewarding cases that you will manage during your time at sea. WHEN IN DOUBT, ERR ON THE SIDE OF CAUTION 30