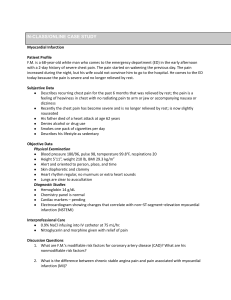
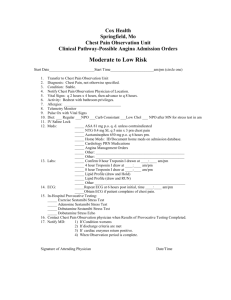
CONTINUED PROFESSIONAL DEVELOPMENT Dr Peter du Toit Travelling Fleet Supervisor – Medical Services Cell: +39 3490875696 Email: peter.dutoit@msccruisesonboard.com ACUTE CORONARY SYNDROME (ACS) - PART 1 Our first CPD topic is ACUTE CORONARY SYNDROME (ACS). Chest pain is a common presenting symptom. It is essential that our initial assessment and management is rapid but methodical and evidence based. Evaluation of emergency department patients with chest pain at low or intermediate risk for acute coronary syndrome (UPTODATE): • Chest pain accounts for approximately eight million annual visits to emergency departments (Ed’s) in the United States. • Acute coronary syndrome (ACS) evaluations account for approximately 10 to 20 percent of all these cases. • This group of patients is among the most challenging in acute care medicine, in part because of the frequency of the clinical problem. • Two primary goals of the early evaluation of patients with chest pain suggestive of myocardial ischemia are: • Rapidly confirm the diagnosis of an ACS, if possible (a "rule-in"), OR • Exclude the diagnosis. • Diagnosing ACS in a timely manner is a high priority, as early intervention in patients with ACS has been shown to lead to better outcomes. The management of ACUTE CORONARY SYNDROME is a complex topic, and we have divided the CPD into two parts. • ACS Part 1will focus on: o the initial evaluation and management of a patient presenting with chest pain. o how to determine risk and how to identify patients who can safely be discharged back to their cabin after presenting with chest pain. • ACS Part 2 will focus on: o the management of ST-Elevation Myocardial Infarction (STEMI) o the management of High-risk ACS patients including those diagnosed with a Non-STElevation Myocardial Infarction (NSTEMI) Certain passages and algorithms in the reference material will be highlighted in blue and author comments in gray. ** The attached UPTODATE articles are the main source of reference for this CPD** **Please allow your Team access to these articles** 1 The following are the main references for this CPD: 1. UPTODATE: Initial evaluation and management of suspected acute coronary syndrome (myocardial infarction, unstable angina) in the emergency department Available at: https://www.uptodate.com/contents/initial-evaluation-and-management-ofsuspected-acute-coronary-syndrome-myocardial-infarction-unstable-angina-in-the-emergencydepartment 2. UPTODATE: Evaluation of emergency department patients with chest pain at low or intermediate risk for acute coronary syndrome Available at: https://www.uptodate.com/contents/evaluation-of-emergency-departmentpatients-with-chest-pain-at-low-or-intermediate-risk-for-acute-coronary-syndrome 3. American Heart Association/American College of Cardiology (AHA/ACC): Guideline for the Evaluation and Diagnosis of Chest Pain. Available at https://www.ahajournals.org/doi/10.1161/CIR.0000000000001029 According to Life in the Fast Lane: Chest pain Differential Diagnosis: ( https://litfl.com/chest-pain-ddx/) The approach to non-traumatic chest pain requires the early recognition and exclusion of potential life threats, then further consideration of other causes. • Potentially life-threatening causes of chest pain o Cardiovascular: ▪ ▪ ▪ ▪ ▪ ▪ ▪ ▪ o Other: ▪ ▪ ▪ • Acute coronary syndromes (STE-ACS and NSTE-ACS) Aortic dissection Myocarditis (most common cause of sudden death in the young) Pericarditis Cardiac Tamponade Pulmonary embolism Cardiac valve disease e.g., aortic stenosis, mitral stenosis, mitral valve prolapses Stress Cardiomyopathies e.g., Takotsubo Tension pneumothorax Acute chest syndrome (in sickle cell disease) Boerhaave syndrome (perforated oesophagus) Common non-life-threatening causes of chest pain o Gastrointestinal: ▪ ▪ Biliary colic Gastroesophageal reflux, Peptic ulcer disease o Pulmonary o Chest wall syndromes ▪ ▪ ▪ ▪ ▪ ▪ o o Musculoskeletal pain Costochondritis Thoracic radiculopathy, Bornholm disease (Acute, transient viral myositis associated with Coxsackie B) Tietze syndrome (Idiopathic benign inflammation of one or more of the costal cartilages) Texidor twinge (precordial catch syndrome), Mondor disease ▪ Psychiatric: ▪ Anxiety ▪ o Pneumonia, Pleurisy Somatisation, Da Costa syndrome (Symptom-complex characterized by palpitation, dyspnea, precordial pain, fatigue, exaggerated emotional responses with increased cardiac awareness) Occult trauma: ▪ Rib fractures Infection: ▪ Shingles 2 COMMENT: • • • • • • • Chest pain is a common complaint amongst both our crew and guests. It is important that all patients presenting with chest pain are evaluated quickly and the initial assessment and management is methodical, and evidence based. The differential diagnosis for chest pain is wide-ranging, so focus on the life-threatening causes. Acute coronary syndrome is unfortunately becoming more common amongst both our crew and guests. The goals in the early evaluation of patients presenting with chest pain or symptoms suggestive of myocardial ischemia are: o Rapidly confirm the diagnosis of an ACS if possible (a "rule-in") ▪ This will require further investigations as history alone will not be able to exclude ACS. o Rapidly exclude (rule out) the diagnosis of ACS and manage the alternative diagnosis. ▪ Again, this could require further investigations to rule out ACS and to confirm alternate diagnoses. Diagnosing ACS in a timely manner is a high priority, as early intervention in patients with ACS has been shown to lead to better outcomes. Ensure your first responders are aware that crew or guests presenting with chest pain who either phone the medical line or present directly to the medical center are fast tracked into the medical center for a rapid evaluation. Initial evaluation and management of suspected Acute Coronary Syndrome (myocardial infarction, unstable angina) in the emergency department (UPTODATE) CLINICAL PRESENTATION • Ischemic chest pain: • Ischemic pain has several features that distinguish it from noncardiac pain. • These characteristics are described below using the OPQRST mnemonic. ✓ ✓ ✓ ✓ ✓ • • ✓ Symptoms associated with the highest relative risk of myocardial infarction include radiation to an upper extremity (particularly when there is radiation to both arms), pain associated with diaphoresis, or pain with nausea and vomiting. Historical features increasing likelihood of ACS: ✓ ✓ ✓ ✓ • Onset Provocation and palliation Quality Radiation Site Time course Patients with a prior history of ACS have a significantly increased risk of recurrent ischemic events. A prior history of other vascular disease is associated with a risk of cardiac ischemic events comparable to that seen with a prior history of ACS. Presence of Risk factors for ACS- advancing age, male, diabetes, hypertension, dyslipidemia, and cigarette smoking Recent use of cocaine or other sympathomimetic drugs (e.g., methamphetamine). Noncardiac chest pain ✓ ✓ ✓ ✓ ✓ ✓ ✓ Pleuritic pain, sharp or knife-like pain related to respiratory movements or cough. Primary or sole location in the mid or lower abdominal region. Any discomfort localized with one finger. Any discomfort reproduced by movement or palpation. Constant pain lasting for days. Fleeting pains lasting for a few seconds or less. Pain radiating into the lower extremities or above the mandible. 3 Guideline for the Evaluation and Diagnosis of Chest Pain (AHA/ACC) Table 3. Chest Pain Characteristics and Corresponding Causes • Nature ✓ ✓ • Onset and duration ✓ ✓ ✓ • • Physical exercise or emotional stress are common triggers of anginal symptoms. Occurrence at rest or with minimal exertion associated with anginal symptoms usually indicates ACS. ✓ Positional chest pain is usually nonischemic (e.g., musculoskeletal). Relieving factors ✓ • Ripping chest pain (“worse chest pain of my life”), especially when sudden in onset and occurring in a hypertensive patient, or with a known bicuspid aortic valve or aortic dilation, is suspicious of an acute aortic syndrome (e.g., aortic dissection). Precipitating factors ✓ ✓ • Anginal symptoms gradually build in intensity over a few minutes. Sudden onset of ripping chest pain (with radiation to the upper or lower back) is unlikely to be anginal and is suspicious of an acute aortic syndrome. Fleeting chest pain—of few seconds’ duration—is unlikely to be related to ischemic heart disease. Location and radiation ✓ Pain that can be localized to a very limited area and pain radiating to below the umbilicus or hip are unlikely related to myocardial ischemia. Severity ✓ • Anginal symptoms are perceived as retrosternal chest discomfort (e.g., pain, discomfort, heaviness, tightness, pressure, constriction, squeezing) Sharp chest pain that increases with inspiration and lying supine is unlikely related to ischemic heart disease (e.g., these symptoms usually occur with acute pericarditis). Relief with nitroglycerin is not necessarily diagnostic of myocardial ischemia and should not be used as a diagnostic criterion. Associated symptoms. ✓ ✓ Common symptoms associated with myocardial ischemia include, but are not limited to, dyspnea, palpitations, diaphoresis, lightheadedness, presyncope or syncope, upper abdominal pain, or heartburn unrelated to meals and nausea or vomiting. Symptoms on the left or right side of the chest, stabbing, sharp pain, or discomfort in the throat or abdomen may occur in patients with diabetes, women, and elderly patients. Guideline for the Evaluation and Diagnosis of Chest Pain (AHA/ACC) • Angina pectoris is perceived as a retrosternal chest discomfort that builds gradually in intensity (over several minutes), is usually precipitated by stress (physical or emotional) or occurring at rest (as in the case of an ACS) with characteristic radiation (e.g., left arm, neck, jaw) and its associated symptoms (e.g., dyspnea, nausea, lightheadedness). • When actively treated or spontaneously resolving, it dissipates over a few minutes. • Relief with nitroglycerin is not necessarily diagnostic of myocardial ischemia and should not be used as a diagnostic criterion, especially because other entities demonstrate comparable response (e.g., esophageal spasm). • Associated symptoms such as shortness of breath, nausea or vomiting, lightheadedness, confusion, presyncope or syncope, or vague abdominal symptoms are more frequent among patients with diabetes, women, and the elderly. • A detailed assessment of cardiovascular risk factors, review of systems, past medical history, and family and social history should complement the assessment of presenting symptoms. 4 COMMENT: • History taking is a crucial part of the initial assessment of a patient presenting with chest pain. • While taking your history consider the potential differential diagnoses and enquire regarding the presence of both high-risk and low-risk symptoms. • It is important to not only take a good history, but also to thoroughly document your findings in SeaCare. History of Presenting Illness (HPI): • When taking a history from the patient consider using the OPQRST mnemonic to describe the chest pain characteristics. • Document whether your patients have any HIGH RISK or LOW RISK (noncardiac chest pain) symptoms. • Document positive AND negative findings. In the YouTube lecture by Dr Amal Mattu, he notes that missed ACS accounts for 20% of malpractice dollars paid out in the Emergency Room, with the majority due to the failure to recognize (or document) concerning features in the history. It is also important to be aware that that many missed ACS cases are misdiagnosed as reflux. Be wary of making a diagnosis of reflux without ensuring you have taken a very detailed history, considered risk factors, and at the very least, requested a 12 lead ECG. Dr Amal Mattu- “Acute Myocardial Infarction: A Big Piece of Medico-Legal Pie” • Available at: Acute Myocardial Infarction: A Big Piece of Medico-Legal Pie | The Heart Course - YouTube 5 Initial evaluation and management of suspected acute coronary syndrome (myocardial infarction, unstable angina) in the emergency department (UPTODATE) IMMEDIATE INTERVENTIONS: • During the initial assessment phase, the following steps should be accomplished for any patient at significant risk for ACS: ✓ Airway, breathing, and circulation assessed. ✓ Preliminary history and examination obtained. ✓ 12-lead electrocardiogram (ECG) interpreted. ✓ Resuscitation equipment brought to the bedside. ✓ Cardiac monitor attached to patient. ✓ Oxygen given as necessary. ✓ Intravenous (IV) access and blood work (troponin, if available) obtained. ✓ Aspirin 162 to 325 mg given. ✓ Nitrates given (contraindications to nitrates include severe aortic stenosis, hypertrophic cardiomyopathy, suspected right ventricular infarct, hypotension, marked bradycardia or tachycardia, and recent use of phosphodiesterase 5 inhibitor [e.g., Viagra]) COMMENT: • Ensure you are methodical when assessing a patient presenting with chest pain. • Delegate roles to the rest of the on-call team as many of the initially actions, including taking history and vitals, will be happening at the same time. • If the initial vitals are abnormal and the patient looks in distress, ensure you have as many of your Team available to help. Checklists/Aide de memoire • Pilots use a checklist before takeoff and landing to ensure they have not missed any critical steps. • A simple checklist that saves lives | News | Harvard T.H. Chan School of Public Health • It is such a simple concept that has finally gained traction within the medical community. • There are many examples of checklist in the literature including: • Rapid-sequence-induction-RSI-checklist-GD.pdf (litfl.com) • JBDS_02 _DKA_Guideline_amended_v2_June_2021.pdf (abcd.care) • Pre-Intubation-Checklist-V25Final.pdf (bwc.nhs.uk) • Safe Sedation Procedures in Adults - RCEMLearning • Quality Standards: Acute care equipment and drug lists | Resuscitation Council UK • As a ship’s doctor you will be dealing with many critical situations and some of them infrequently for example rapid sequence induction and conscious sedation. • UpToDate is an excellent resource, and you will find many checklists and algorithms that can help you in your daily practice. A reference sheet based on the current ACS CPD has been developed to act as an aide de memoire. It is intended as a support tool and is provided for information only. Clinical decision making remains the responsibility of all medical professionals and you will need to use your clinical judgement to make appropriate decisions, based on current best practice. 6 Initial evaluation and management of suspected acute coronary syndrome (myocardial infarction, unstable angina) in the emergency department (UPTODATE) TWELVE-LEAD ELECTROCARDIOGRAM: • A 12-lead ECG should be obtained within 10 minutes of arrival in all patients with possible coronary-related ischemia. • The 12-lead ECG provides an important basis for initial diagnosis and management and should immediately be shown to an emergency physician for interpretation. If the initial ECG reveals a STEMI, immediate intervention is required. • Remember that alternative lead placement can better detect certain types of acute MI. • Right-sided lead placement can highlight a ventricular infarct. • Posterior lead placement can highlight a posterior infarct. • The initial ECG is often not diagnostic in patients with ACS. Thus, the ECG should be repeated at 15- to 30-minute intervals if the initial study is not diagnostic, but the patient remains symptomatic and high clinical suspicion for ACS persists. DETERMINING WHO NEEDS AN ELECTROCARDIOGRAM: • Any patient over 30 with chest pain. • Any patient over 50 with any of the following: dyspnea, altered mental status, upper extremity pain, syncope, or weakness. • Any patient over 80 with abdominal pain, nausea, or vomiting. COMMENT: • It is important to keep in mind that managing chest pain is a time-critical event. • I cannot emphasize the point enough that the initial ECG is often not diagnostic and SERIAL ECG’s play an extremely important part in the early diagnoses of ACS. • The interpretation of a 12 lead ECG is a vital skill to have when you are working at sea. • It is always worth getting a second opinion from your colleagues onboard especially when you suspect a STEMI or want to rule out a STEMI. • It is good practice to keep your knowledge of ECG’s current and here are a couple Internet resources you can use: ▪ UPTODATE: • ECG tutorial: Basic principles of ECG analysis - UpToDate • Electrocardiogram in the diagnosis of myocardial ischemia and infarction UpToDate ▪ Life in the Fastlane • EKG Library • LITFL • ECG Library Basics • Killer ECG Patterns: Part 1 • LITFL • ECG Library • Killer ECG Patterns: Part 2 • LITFL • ECG Library ▪ Other: • Dr. Smith's ECG Blog (hqmeded-ecg.blogspot.com) • ECG Cases blog | Emergency Medicine Cases ▪ YouTube • Any lecture from Dr Amal Mattu • MedCram - Medical Lectures Explained CLEARLY - YouTube • ICU Advantage - YouTube • Ninja Nerd - YouTube ▪ ECG textbooks 7 AHA/ACC Guideline for the Evaluation and Diagnosis of Chest Pain. COMMENT: • Once you have completed your initial assessment including a focused history, a set of vitals, and the 1st ECG, you are left to choose from the following presumptive ECG diagnoses: o STEMI o Pericarditis o Ischemic changes (ST depression, new T-wave inversion) o Arrhythmia o Non-diagnostic or normal ECG • It is common to NOT be able to make a definitive diagnosis initially. • In the scenario where you have a non-diagnostic, or normal ECG, remember, you still haven’t RULED OUT ACS, but you also need to start looking at alternative diagnoses. • Therefore: o The patient needs to remain admitted to the medical center. o Observations: continuous cardiac monitoring and frequent vitals. o Consider supplemental O2 and additional medications where indicated. o Review the case, consider your differential diagnosis, and consider other probable causes of chest pain. o Further investigations are indicated to both identify other causes of chest pain and to rule in/out any myocardial damage. o Investigations could include: ▪ ECG’s: Serial ECG’s and consider other leads like posterior leads (V7-9) ▪ CXR: rule out other causes. ▪ Laboratory: Serial cardiac biomarkers (cardiac enzymes), basic electrolyte concentrations, kidney function studies, complete blood count, D-Dimer and BNP (when indicated and where available) 8 ACC: Figure 8. General Approach to Risk Stratification of Patients with Suspected ACS. COMMENT: • In the patient presenting with chest pain and a non-diagnostic or normal ECG, further observation and additional investigations should enable you to divide this group into: 1. Obvious Non-cardiac- discharge or manage with appropriate care. 2. Obvious Non-ischemic cause - discharge or manage with appropriate care. 3. Possible / Suspected ACS. • ACC Recommendations for Patients with Acute Chest Pain and Suspected ACS (Not Including STEMI) o In patients presenting with acute chest pain and suspected ACS, clinical decision pathways (CDPs) should categorize patients into low, intermediate, and high-risk strata to facilitate disposition (back to cabin, admit for further observations or consider disembarkation) and subsequent diagnostic evaluation. • There are a couple of clinical decision pathways (CDPs)to choose from. The most common and recommended by UpToDate is: o Heart Score o Heart Pathway. • Feel free to review the following YouTube lecture by Dr Amal Mattu regarding Chest Pain risk stratification. Available at: Chest Pain Risk Stratification | The Heart Course W/ Amal Mattu, MD - YouTube 9 Evaluation of emergency department patients with chest pain at low or intermediate risk for acute coronary syndrome (UPTODATE) The HEART score has been widely validated. • Validation studies have shown the need to add a three-hour troponin level to achieve acceptable sensitivity. • A score of 0 to 3 identifies a patient at low risk of major adverse cardiovascular events. • Patients with a score of 4 to 6 have intermediate risk of major adverse cardiovascular events. • Those with a score of 7 or greater are high risk of major adverse cardiovascular events. COMMENT: • Patients with Suspected ACS (non-cardiac causes ruled out) should remain admitted and continuously monitored in the medical center. • The patient should be managed using the HEART pathway. o On admission: ▪ 1st Cardiac enzyme (TropI) ▪ HEART SCORE o After 3 hours: ▪ 2nd Cardiac enzyme (TropI) ▪ HEART SCORE • There are various online resources where you can find medical calculators including MDCalc and UptoDate • Available at: HEART Pathway for Early Discharge in Acute Chest Pain - MDCalc • Available at: Calculators - UpToDate 10 Evaluation of emergency department patients with chest pain at low or intermediate risk for acute coronary syndrome (UPTODATE) The HEART Pathway consists of a modified HEART score which is estimated from clinical data, and two troponin values at zero and three hours. • Normal first troponin o For patients whose symptoms remain suspicious for an ACS or who have a low or intermediate risk of ACS (HEART Score ≥1), obtain a second troponin three hours after the first troponin and use the HEART Pathway approach. • Normal second troponin o If the second troponin value is also normal, use the HEART score to reestimate risk and the HEART Pathway to determine the next step in management: o If the HEART score is ≤3 points and two troponin measurements are negative (i.e., below the 99th percentile), and no new ischemic ECG changes are present, the risk of incident ischemic events is considered sufficiently low for discharge without further observation or diagnostic testing. o For HEART scores >3 points and two negative troponin measurements three hours apart, the patient is at intermediate or high risk and should be appropriately managed for ACS. • Available at: The HEART Pathway Randomized Trial | Circulation: Cardiovascular Quality and Outcomes (ahajournals.org) COMMENT: • Serial ECG’s and serial cardiac enzymes are important in the evaluation of ACS. • Shoreside laboratories machines are using high sensitive cardiac troponin (hs-cTn) as opposed to cardiac troponin (cTn). o The value of a high sensitive cardiac troponin (hs-cTn) assay, is the theoretical ability to rule out myocardial damage with a single negative reading (Rule Out Myocardial Infarction). o There are currently clinical decision pathways using a single high sensitive cardiac troponin (hs-cTn) to rule out myocardial damage to allow a patient to be discharged from hospital earlier. • Despite investing in newer laboratory equipment, it is still unclear whether you can safely RULE OUT a Myocardial infarction with a single hs-cTn assay onboard, especially for those patients presenting very early on (<1 hour). • Therefore, it is recommended to follow the HEART PATHWAY and do serial cardiac enzymes regardless of assay sensitivity. • Timing of cardiac enzymes if chest pain for > 3 hours prior to admission o Take 1st cardiac troponin (cTn) at hour 0 (on admission) o Take 2nd cardiac troponin (cTn) 3 hours later. • Consider delaying the second cardiac troponin (cTn) if chest pain < 3 hours from admission. 11 Point-of-care testing (POCT) • POCT is a form of testing in which the analysis is performed where healthcare is provided close to or near the patient. • On our vessels, all our laboratory equipment is basically POCT. • This allows for a smaller footprint but will never be able to match the accuracy of larger shoreside equipment. • This is especially true when dealing with lower concentrations of a specific enzymes or electrolytes. Cardiac capabilities onboard: • Medical Facilities is currently working on ensuring each vessel in the Fleet has the capability of measuring Quantitative Troponin I with either (or both) Quidel Triage® MeterPro or iStat. • Lateral Flow tests are still available but should only be used when a quantitative test is not available. Quidel Triage® MeterPro • Medical Facilities has purchased the Quidel Triage® MeterPro for fleetwide implementation and is currently working on shipping them to each vessel. • • • The Quidel Triage® MeterPro is a portable fluorescence instrument used to measure the results of tests (TropI, BNP and D-Dimer) manufactured by Alere San Diego, Inc. Cardiac Enzymes: Troponin I (TnI) o Troponin I (TnI) is a regulatory subunit of the troponin complex and plays an integral role in the regulation of muscle contraction. o Clinical studies have demonstrated the release of cardiac TnI (cTnI) into the blood stream within hours following myocardial infarction (MI) or ischaemic damage. o Elevated levels of cTnI (above the values established for non-MI specimens) are detectable in serum within 2 hours after the onset of chest pain, reach peak concentrations in approximately 8-28 hours, and remain elevated for 3-10 days following MI. o https://www.nwlpathology.nhs.uk/tests-database/troponin-high-sensitivity/ o Once set up, use the Quidel Triage® MeterPro as the primary method to measure TnI. Brain Natriuretic Peptide (BNP) o BNP is a hormone released by the heart when the ventricles are stretched e.g. by fluid overload. o The hormone then causes fluid and sodium loss in the urine and mild vasodilation. o In heart failure, BNP levels are raised, directly proportionate to heart failure severity according to New York Heart Association classification. If BNP is normal, it generally rules out heart failure. (Negative Predictive Value 97%) o • https://www.nbt.nhs.uk/sites/default/files/BNP%20Fact%20Sheet.pdf D-Dimer o D-dimer results are often used in conjunction with the Well's score (an index of clinical suspicion of venous thromboembolism (VTE)) in determining the diagnostic probability of a VTE. o A negative d-dimer result is indicative of a low probability of VTE, but a raised d-dimer result may be due to many other factors, eg. infection, inflammation, or pregnancy, and so should not be used to confirm a VTE diagnosis in the absence of any other supporting evidence. o https://www.nwlpathology.nhs.uk/tests-database/d-dimer/ 12 • Once you have received the Quidel Triage® MeterPro, ensure you read the set-up manual and watch the instructional videos sent by Medical Facilities 13 Evaluation of emergency department patients with chest pain at low or intermediate risk for acute coronary syndrome (UPTODATE) COMMENT: • The above algorithm is a useful tool in your management of ACS. • Consider using this algorithm when you are dealing with a patient who presents with chest pain but has a non-diagnostic ECG. • Follow the steps in the algorithm to determine disposition. o Step1: ▪ Eligibility: all patients with a probability of ACS o Step 2: ▪ Laboratory: take blood for cardiac enzymes: Troponin I ▪ Consider also doing other investigations including hematology, renal and electrolytes, BNP, and D-Dimer. 14 o o o o Step 3 ▪ 1st Troponin • Elevated: o Admit and treat for ACS. • Normal: o Calculate HEART SCORE Step4 ▪ HEART SCORE: 0 • If symptoms best explained by non-cardiac diagnosis, review and manage for other non-ACS condition. • If symptoms or history still suspicious: o Admit and continue with HEART Pathway ▪ HEART SCORE: ≥ 1 o Admit and continue with HEART Pathway Step 5 ▪ 2nd Troponin 3 hours later • Elevated: o Admit and treat for ACS. • Normal: o Calculate HEART SCORE Step 6 ▪ HEART SCORE > 3 • These patients are considered intermediate or higher risk patients. • Further observations and monitoring will be required. ▪ HEART SCORE: 0 to 3: • Look for other causes of chest pain. • If they are asymptomatic, you could consider discharging them back to their cabin and ensure frequent follow ups. • In the DISPOSITION section of SeaCare, document that you have advised the patient of the following: o Diagnosis: ▪ Ensure they are aware of the diagnosis and implications. o Emergency: ▪ How to contact the Medical Center in an emergency. o Follow up onboard: ▪ When to return for a follow up visit. • I would suggest frequent reviews until disembarkation. • At least daily reviews focusing on high-risk symptoms. o Medication: ▪ How to take any newly prescribed medications. ▪ Discuss any warnings/ side-effects or interaction of the new medications. o Medical notes and ECG’s: ▪ Ensure all ECGs are uploaded into SeaCare. ▪ Ensure the patient has a copy of their ECG’s and clinical notes to take to their doctor. o Follow up at home: ▪ Ensure you have advised them to immediately follow up with their doctor at home for a further review and possible further investigations. 15 LESSONS LEARNED AND PITFALLS • In each CPD module we will discuss LESSONS LEARNED and highlight potential PITFALLS LESSONS LEARNED • There are examples where an initial diagnosis of ACS was made without consideration being given to differential diagnoses or ruling out other critical life-threatening causes. This can inevitably cause potential harm to the patient, especially when subsequent investigations cast doubt on the initial diagnoses. Be mindful to reconsider your diagnosis when additional clinical evidence or investigation results become available. • This is an example of confirmation bias, anchoring bias, and premature closure. Confirmation bias involves selectively gathering and interpretating evidence to conform with one’s beliefs, as well as neglecting evidence that contradicts them. ▪ Since it occurs early in the treatment pathway, confirmation bias can lead to mistaken diagnoses being passed on to and accepted by other clinicians without their validity being questioned, a process referred to as diagnostic momentum. o Anchoring bias is much like confirmation bias and refers to the practice of prioritizing information and data that support one’s initial impressions of evidence, even when those impressions are incorrect. o Premature closure is the failure to consider alternative diagnoses after the initial impression is formed (often based on pattern recognition alone). ▪ Premature closure is exacerbated by anchoring, the tendency for clinicians to stick with the initial impression even as new information becomes available. Become aware of the common tendency to jump to a conclusion too early in the evaluation. Consider the first impression as one, but not the only, diagnostic explanation. Gather sufficient supporting information and avoid jumping to conclusions. Re-evaluate the diagnosis at critical decision-making points such as admission or discharge. There are many refences in the literature and internet discussing cognitive bias, here are a couple of links: o • • • • • o o https://www.emra.org/emresident/article/weighed-down-by-words-how-to-recognize-and-avoid-anchoringbias https://psnet.ahrq.gov/web-mm/anchoring-bias-critical-implications PITFALLS: Identifying Emergency Department Patients with Chest Pain Who Are at Low Risk for Acute Coronary Syndromes Available at: https://www.ebmedicine.net/topics/cardiovascular/chest-pain-risk-stratification Risk Management Pitfalls in Managing Patients at Low Risk for Acute Coronary Syndromes 1. “My patient was young and healthy, so I didn’t suspect ACS.” o Younger patients are at lower risk of ACS, but 4% to 8% of myocardial infarctions still occur in patients < 40 years old. While traditional cardiac risk factors are generally not useful in the management of undifferentiated chest pain, a high risk-factor burden is more predictive of ACS in younger patients. Validated clinical risk scores can identify very-low-risk patients in this age group with excellent accuracy. 2. “Her symptoms didn’t sound like angina, so ACS wasn’t even in my differential diagnosis.” o A patient's history cannot reliably exclude ACS. Atypical symptoms are often present and are more common in women, the elderly, and diabetics. Additional testing, especially in these population groups, should be considered to reliably rule out ACS. 16 3. “The ECG was normal, so I didn’t think further testing was indicated.” o A normal ECG lowers the risk of ACS but does not adequately exclude it, and nearly 8% of patients with myocardial infarction have a normal ECG. Misinterpretation of the ECG is also a factor associated with missed diagnosis of ACS. Accuracy is increased by obtaining serial ECGs. 4. "His chest pain began 6 hours prior, so I thought 1 troponin would be sufficient.” o Troponin will be detectable within 6 hours in nearly all patients with myocardial infarction. However, if the history is inexact, if the patient has a moderate to high pretest probability of ACS, or if the troponin assay is older or less-sensitive, additional testing will be required. 5. “The pain was reproducible on palpation, so I ruled out ACS.” o Pain that is reproducible on palpation lowers the risk of ACS but does not exclude it. 6. “The patient had negative serial troponins, so I thought that ruled out ACS.” o Currently, unstable angina is a purely clinical diagnosis, and biomarkers will be negative in this condition. Negative biomarkers should be used in conjunction with validated clinical risk scores for optimal risk stratification. 7. “He had chest pain and an elevated troponin, so I diagnosed him as having a myocardial infarction.” o The specificity of troponin for myocardial infarction is less than its sensitivity, and troponin can be elevated in many other conditions that cause nonischemic myocardial injury (e.g., heart failure, pulmonary embolism, chronic kidney disease, sepsis). 8. “My patient had a TIMI score of 0, so I excluded ACS and discharged him without further testing.” o A TIMI score of 0 confers a 1.8% risk of 30-day MACE, which may be unacceptably high. Using TIMI in conjunction with serial biomarkers improves its prognostic ability. 9. “My patient had normal serial ECGs and negative serial troponins, so I told him that ACS was ruled out and he didn't need any further testing.” o There is strong evidence to suggest that confirmatory testing does not add any incremental benefit in low-risk patients. However, this approach has not been tested in randomized trials, and is not yet endorsed by consensus guidelines. Furthermore, patients who are at intermediate or high risk of ACS or MACE as determined by a validated clinical risk score should undergo further testing, even with normal ECGs and negative troponins. 10. “She had a negative stress test 6 months prior, and the ECG was normal, so I thought it was safe to send her home without any further testing.” o The annual event rate (myocardial infarction or cardiac death) is about 1% after any stress test. Any patient presenting to the ED with chest pain should be evaluated with ECG and biomarkers, and risk stratified using a validated clinical risk score, despite the recent negative stress test. 17 FINAL COMMENT: • Chest pain is a frequent complaint amongst guests and crew. • A poorly managed case can cause significant injury to your patient and can result in legal action against you and the company. • Have a systematic approach to managing chest pain: o Use checklists to remind yourself of important steps to take. • Beware of atypical presentations, especially amongst diabetics, women, and elderly patients • Time is critical: o Ensure the Team is aware that an early ECG is imperative! o Document critical timings. • Documentation is important: o The characteristic of the chest pain can either reassure you, or prompt to be more cautious. o Past medical history is also an important aspect of determining risk. • Diagnosis: o Don’t be too quick to make a diagnosis. There is a wide ranging of conditions that cause chest discomfort that aren’t ACS, some of them life-threatening. o Always keep an open mind and be willing to be challenged regarding your presumptive diagnosis. o You are not always going to be able to make a definitive diagnosis after your first ECG. o Always keep the patient admitted and fully monitored patient until you have made a final diagnosis. o Serial testing including ECG’s and cardiac enzymes play an important part in making the correct diagnosis. • Risk: o Use the HEART score and HEART Pathway to determine risk and outcome. • Follow up: o Even those patients who are considered LOW RISK, are still at risk of a complication. o Ensure you follow them up frequently. o Ensure they have a copy of their ECG’s and laboratory results to give their doctors when they return home. o ALWAYS advise guests who have been assessed for ACS to seek a review by their own doctors when they return home. o Always document the advice you have given the patient. WHEN IN DOUBT, ERR ON THE SIDE OF CAUTION 18