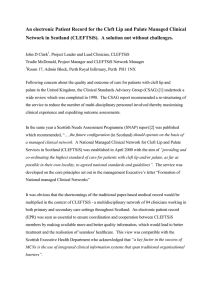
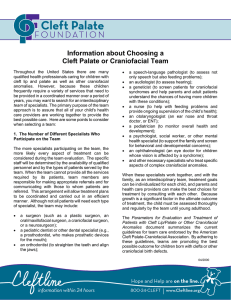
PERSPECTIVES SIG 5 Review Article The Effect of Dental and Occlusal Anomalies on Articulation in Individuals With Cleft Lip and/or Cleft Palate Kazlin N. Masona Purpose: Dental and occlusal anomalies are common in individuals with cleft lip and palate, placing them at risk for speech sound distortions. Speech-language pathologists and dental practitioners frequently interact when presented with clinical problems secondary to dental and occlusal anomalies. This is especially true when treating a child with a cleft lip and palate. The speech sound error types must be identified and their etiologies evaluated to develop appropriate management plans. The purpose of this review article is to describe the types of dental and occlusal anomalies that are common in individuals with cleft lip and/or palate and discuss the impact these anomalies have on articulation. Method: A review of the literature was completed with a focus on prevalence, definitions, and descriptions of dental and occlusal anomalies in individuals with cleft lip and palate. The impact of dental/occlusal anomalies on speech production is described. Results and Conclusions: There is sufficient evidence that dental and occlusal anomalies have an impact on articulation, but the relationship of dental or occlusal status is not always a direct one. The phonemes most affected by aberrant oral conditions are sibilants, though other phonemes may be impacted as well. These speech errors are considered to be obligatory oral distortions in that they are made in response to an oral structural defect. These speech errors are not typically amenable to speech therapy, but rather require orthodontic and/or surgical correction. Such treatment can be effective in improving these errors, often spontaneously, however, speech therapy may be necessary (and most effective) following correction of the dental and/or occlusal anomalies if errors persist. C with isolated cleft lip. In patients presenting with both cleft lip and palate, Akcam et al. (2010) found that 96.7% of patients demonstrated at least one dental anomaly. Consequently, structural anomalies found in the anterior oral cavity and skeletal malocclusion may present added complications for speech development in patients with cleft lip and palate, which can exacerbate speech production difficulties (Courtney et al., 1996; Hardin-Jones & Jones, 2005; Leavy et al., 2016; Molsted & Dahl, 1990; Satoh et al., 2004). Speech disorders associated with cleft lip and palate have been well documented in the literature (Hardin-Jones & Jones, 2005; Kuehn & Moller, 2000; Kummer, 2014; Marshs, 2009; Peterson, 1975; Sell, 2005; Trost, 1981). Speech production errors in children with cleft lip and palate are often grouped into categories of error types. Zajac and Vallino (2017) presented a framework for classification of articulation errors seen in individuals with cleft lip and palate. Within this context, compensatory errors are considered to be active articulatory substitutions that individuals raniofacial anomalies, such as cleft lip and palate, often result in anatomic differences that impact both structure and function in the craniofacial and dentofacial complex. Furthermore, anomalies that impact the relationship between the maxilla and mandible, such as cleft lip and/or palate, can alter speech production. Due to this, children with cleft lip and palate are often at risk for speech/articulation disorders. A high prevalence of dental and occlusal anomalies have been reported in individuals with cleft and craniofacial differences and these occur with greater frequency than that which occurs in the noncleft population. Vallino et al. (2008) documented dental and occlusal anomalies in 62% of patients a Department of Human Services, University of Virginia, Charlottesville Correspondence to Kazlin N. Mason: kazlin.mason@virginia.edu Editor-in-Chief: Brenda L. Beverly Editor: Brenda Louw Received March 1, 2020 Revision received May 19, 2020 Accepted September 3, 2020 https://doi.org/10.1044/2020_PERSP-20-00056 Publisher Note: This article is part of the Forum: Consideration of Structural Anomalies Related to Cleft and Craniofacial Conditions. 1492 Disclosures Financial: Kazlin N. Mason has no relevant financial interests to disclose. Nonfinancial: Kazlin N. Mason is the Continuing Education Content Manager for ASHA Special Interest Group 5: Craniofacial and Velopharyngeal Disorders and a member of the Professional Development Committee. Perspectives of the ASHA Special Interest Groups • Vol. 5 • 1492–1504 • December 2020 • Copyright © 2020 American Speech-Language-Hearing Association Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions SIG 5 Craniofacial and Velopharyngeal Disorders Table 1. Differences between compensatory and obligatory speech errors. Compensatory speech errors Placement is abnormal Learned behaviors that are amenable to therapy Errors typically persist after surgery to correct velopharyngeal insufficiency Treatment: Speech therapy addressing accurate placement Example: Glottal stop sound substitution for /p/ Pharyngeal stops and pharyngeal fricatives with velopharyngeal dysfunction may produce to bypass the anatomical or velopharyngeal deficit (Vallino et al., 2019). In contrast, obligatory errors have been defined as unavoidable errors that occur as a consequence of structural conditions such as dental and occlusal anomalies or velopharyngeal dysfunction (Vallino et al., 2019). Thus, obligatory errors are structurally based, whereas compensatory errors are thought to be learned. Obligatory errors and compensatory errors are also categorized as passive or active speech errors (Harding & Grunwell, 1998; Hutters & Brøndsted, 1987) with obligatory errors classified as passive and compensatory errors active (Harding & Grunwell, 1996). Table 1 illustrates key differences between compensatory speech errors and obligatory oral distortions. In passive or obligatory speech errors, the manner of the articulatory target is typically maintained, but the place of articulation is altered resulting in a distortion of the target sound. These errors or distortions occur within the oral cavity (Vallino et al., 2019). In contrast, active speech errors are produced posterior to the velopharyngeal valve and used in substitution of individual sounds or sound classes (Vallino et al., 2019). Obligatory errors arise secondary to oral structural deviations (e.g., dental/occlusal deviations and/or palatal fistulae) or physically based oral–nasal balance/resonance disorders (Harding & Grunwell, 1996; D. L. Jones, 2000; Riski, 1979; Riski & DeLong, 1984; Trost, 1981). Obligatory errors related to velopharyngeal dysfunction include hypernasality, nasal air emission, and weak oral pressure consonants. Obligatory errors secondary to dental and occlusal anomalies are termed obligatory oral distortions. Unlike compensatory speech errors, obligatory errors are not readily amenable to speech therapy. Therefore, management of cleft lip and palate requires multidisciplinary care across specialties, typically within the context of a cleft/craniofacial team. When patients with cleft lip and/or palate present with obligatory oral distortions, it requires an interdisciplinary partnership between the speech-language pathologist (SLP) and dental practitioner. Depending on the errors present and etiologies of errors, collaboration with differing dental practitioners (e.g., dentists, orthodontists, and/or oral-maxillofacial surgeons) may be warranted. The purpose of this review article is to provide an introduction to craniofacial development in children with cleft lip and/or palate, describe the types of dental and occlusal anomalies Obligatory oral distortions Placement is typically preserved Not amenable to correction with therapy Speech distortion errors due to abnormal structure, typically correct following orthodontics or surgery Treatment: Correct structure Example: Lateral lisp as consequence of anterior crossbitte Distortion of sibilant targets due to airflow interference from dental/skeletal anomalies that are commonly seen, and discuss the impact these anomalies have on articulation. Collaboration between the dental practitioner and SLP will be emphasized. Orofacial Development in Patients With Cleft Lip and Palate In a typically developing population, the growth of the mandible follows Scammon’s curve for general body structures and studies have reported that the mandible has an accelerated prepubertal and pubertal growth spurt (Bateman & Mason, 1984; Bloomer, 1971; R. Mason & Proffit, 1974). The tongue is reported to reach adult size by age 8 years, mirroring the growth of Scammon’s neural tissues (R. Mason & Proffit, 1974). Similarly, the growth of the maxilla closely mirrors the neural growth curve and is reported to complete its growth between 8 and 12 years of age (R. Mason & Proffit, 1974). In individuals with nonsyndromic cleft lip and palate, mandibular and lingual growth appear to follow similar trends (R. Mason & Proffit, 1974). However, maxillary growth is frequently restricted secondary to surgical interventions for cleft lip and palate (Jolleys, 1954; Liao & Mars, 2005; Meazzini et al., 2008, 2011). These interventions can alter both the bony and muscular structures of the craniofacial complex. Due to this, the craniofacial complex undergoes many changes following surgical interventions for cleft lip and palate as well as changes relating to typical developmental stages and growth patterns that occur between infancy and adolescence (Bishara, 1973; da Silva Filho et al., 1993; Doucet et al., 2019; Jackson et al., 2020; Mars & Houston, 1990; Reddy et al., 2017; Ross, 1970; Shibasaki & Ross, 1969). Children with oral clefts are at a higher risk for disorders of speech production related to underlying oral and nasopharyngeal anomalies resulting from the cleft (Kuehn & Moller, 2000). Furthermore, tissue deficiencies and heterogeneous anomalies of the oral cavity are common in individuals with cleft lip and palate. For example, individuals with bilateral cleft lip and palate often demonstrate a protrusive premaxilla prior to surgical repair, which may result in more significant dental anomalies (Long et al., 2000). Specifically, individuals presenting with bilateral cleft lip and palate are more likely to demonstrate a greater degree Mason: Dental Anomalies and Obligatory Speech Errors Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions 1493 SIG 5 Craniofacial and Velopharyngeal Disorders of tissue deficiency and larger nasopharyngeal volume than individuals with unilateral cleft lip and palate (Long et al., 2000; K. Mason & Perry, 2016). Thus, individuals with cleft lip and palate can exhibit cleft-specific differences in craniofacial anatomy and physiology depending on the type and severity of the cleft (Reddy et al., 2017; Tome et al., 2016). This heterogeneity of the mechanism impacts maturation and growth of craniofacial and dentofacial structures (Honda et al., 2002; Ross, 1970; Subtelny & Subtelny, 1959; Tan et al., 2012). The maxilla is the primary bony structure involved in clefting, and a hypoplastic and/or retrusive maxilla is commonly observed. The degree of maxillary hypoplasia and/or retrusion is related to the cleft type as well as the timing and type of surgical management received. In unilateral cases, medial collapse of the maxillary arch can create misalignment of the bony maxillary segments (Peat, 1974). This problem frequently results in the development of dental and occlusal anomalies, such as an anterior crossbite on the side of the cleft. In contrast, the premaxilla is often protrusive prior to repair for patients with bilateral cleft lip and palate. Following repair, forward growth of the maxilla and alveolar segments may be reduced due to hypoplasia of the structures and the restrictive effects of surgical intervention (Reiser et al., 2011, 2010). The mandible is not directly impacted by clefting; however, positioning of the mandible can be altered by the horizontal and vertical alignment of the maxilla (Wolford & Stevao, 2002). Additionally, maxillary hypoplasia may give an appearance of a prognathic mandible in a child with a cleft (Molina & Figueroa, 1999; Ogasawara et al., 2002). Therefore, the SLP needs to re-evaluate a child with a cleft lip and palate at staged intervals with a focus on when changes are likely to occur and how surgical, dental, and other management procedures are likely to impact articulatory development and velopharyngeal function. Dental and Occlusal Anomalies Associated With Cleft Lip and Palate Dental deviations observed in individuals with cleft lip and/or palate can also be seen in individuals without cleft lip and/or palate. The differences, however, relate to the severity, frequency, and location of dental anomalies. Furthermore, this relationship is variable due to individual subject differences. Studies have reported relationships between severity of clefting and number of dental anomalies (Akcam et al., 2010; Qureshi et al., 2012; Tannure et al., 2012). Dental deviations can arise secondary to the cleft lip and/or palate or following surgical intervention for the cleft. Occlusal anomalies, related to the relationship between the maxillary and mandibular arches, can also occur in both cleft and noncleft populations (Akcam et al., 2010; Vallino & Tompson, 1993). For those with cleft lip and/or palate, severity is often related to the type and location of the cleft. These occlusal relationships may be related to dentition and/or skeletal anomalies of the dental arches. Occlusal defects and dental anomalies observed in individuals 1494 with cleft lip and/or palate will be defined and described below. Occlusal Defects Associated With Cleft Lip and Palate Occlusal defects are problems related to the relationship between the upper and lower jaws. Occlusal defects can be dental (related to the teeth alone) or skeletal (involving the relationship between the maxilla and/or mandible). A classification system to define occlusion and malocclusion was designed by Angle (1899), and, despite debate on how this system may best be applied and adapted in modern clinical practice (Katz, 1992a, 1992b), it continues to be referenced today. In normal occlusion, the maxillary arch is larger and fits over the mandibular arch. In the population of individuals with cleft lip and palate, this is not often the case due to maxillary hypoplasia from the cleft itself as well as consequences of surgical interventions (Vargervik, 1983). In Angle’s system, the maxillary and mandibular first molars serve as reference points to define the occlusal relationship. Furthermore, while Angle’s system references the occlusal relationship of the maxillary and mandibular molars, it is additionally important to take into account how the orientation of the skeletal maxillary and mandibular arches impact both dentition and the overall dentofacial complex. Accordingly, alignment/occlusion of the anterior and posterior dentition (as seen in crossbite and open bite relationships) is often directly related to alignment of the cranium, maxilla, and the mandible (Bloomer, 1971; Leavy et al., 2016). Class I. This occlusal pattern is often referred to as a “neutroclusion,” and the arch relationship is normal, but misalignment of the anterior teeth may still be present. In a Class I occlusal pattern, the mesial buccal cusp of the maxillary first molar is typically positioned to the buccal groove of the mandibular first molar (see Figure 1). When anterior dentition is misaligned, but occlusal relationship is appropriate, this pattern may be termed as “Class I malocclusion” (Christie, 1977; Katz, 1992b). Class II. A Class II occlusal pattern has the mesial buccal cusp of the maxillary first molar positioned anterior to the buccal groove of the mandibular first molar. This may be referred to as a “distoclusion.” This occlusal relationship is less common in individuals with cleft lip and palate; however, children with Stickler syndrome, Pierre Robin sequence, or mandibulofacial dysostosis (Treacher Collins syndrome) may demonstrate a Class II malocclusion (Kamioka et al., 2007; Suri et al., 2010; Vallino-Napoli, 2002). If misalignment of the maxillary and mandibular arches is present, a patient may be labeled as having a “retrognathic” mandible and/or “prognathic” maxilla, depending on the overall craniofacial profile. Class III. In a Class III occlusal pattern, or “mesioclusion,” the mesial buccal cusp of the maxillary first molar is positioned posterior to the buccal groove of the mandibular first molar. This can arise secondary to maxillary hypoplasia and/or a prognathic mandible (Ellis & McNamara, 1984; Guyer et al., 1986; Meyer-Marcotty et al., 2011). Class III Perspectives of the ASHA Special Interest Groups • Vol. 5 • 1492–1504 • December 2020 Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions SIG 5 Craniofacial and Velopharyngeal Disorders Figure 1. A normal Class I occlusal relationship. Arrows identify the relationship between the maxillary and mandibular molars. malocclusions may be observed in individuals with cleft lip and palate who demonstrate significant midface hypoplasia (Vargervik, 1983). Garrahy et al. (2005) noted a Class III occlusal relationship occurred in 31.3% of children with bilateral cleft lip and palate, compared to 9.1% of children with unilateral cleft lip. Crossbites. The overlap of the maxillary arch with the mandibular arch is reversed when a crossbite is present (Garrahy et al., 2005; Pruzansky & Aduss, 1964; Wangsrimongkol & Jansawang, 2010), resulting in a maxillary tooth or teeth that rest inside the mandibular arch. This arrangement is frequently seen in patients with Class III malocclusion. Maxillary hypoplasia and restricted maxillary width often contribute to this configuration (Figueroa & Polley, 2007). Anterior crossbites occur when the central incisors, lateral incisors, and/or canines rest inside the mandibular incisors. A posterior crossbite occurs when the teeth posterior to the canines rest inside the mandibular teeth. Crossbites can be right-sided, left-sided, or bilateral. A crossbite of one or more teeth on the side of the cleft often occurs in the primary dentition of patients with cleft lip and/or palate (Leavy et al., 2016). Figure 2 provides one example of a crossbite after alveolar bone grafting in an individual with unilateral cleft lip and palate. Open bite. Subtelny and Sakuda (1964) defined an open bite as an opening in the vertical dimension of the maxillary and mandibular teeth (i.e., these teeth do not make contact when in a centric occlusion). An open bite can occur in the anterior and/or posterior dentition and may be a result of dental etiologies (such as thumb sucking or poor dental eruption) and/or skeletal etiologies (such as poor facial growth). Class II and III occlusal anomalies can coexist with an open bite relationship. Open bites can have a significant impact on articulation. An anterior open bite may be present in patients with Treacher Collins syndrome. Within this syndrome, the mandible is hypoplastic with a downward curvature of the lower border of the mandible. As a consequence, these individuals typically develop a Class II skeletal open bite malocclusion (da Silva Dalben et al., 2006; Martelli-Junior et al., 2009). Figure 3 demonstrates an example of a skeletal Class III malocclusion with an open bite. The malocclusion is termed a “skeletal” Class III malocclusion since the discrepancy between the upper and lower dentition is related to either an overdevelopment of the mandible or a retrusive position of the maxilla. In this Figure 2. (A) The left lateral incisor has erupted in an anterior crossbite and the canine is erupting in crossbite as well. (B) Left sided view of the dental arch. Note the maxillary posterior and canine crossbite. Image and caption courtesy of Robert Mason, DMD, PhD. Mason: Dental Anomalies and Obligatory Speech Errors Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions 1495 SIG 5 Craniofacial and Velopharyngeal Disorders Figure 3. A skeletal Class III malocclusion (arrows) with an open bite. Note the horizontal relationship of upper and lower canines and first molars as well. Image and caption courtesy of Robert Mason, PhD, DMD. example, the mandible is overdeveloped, and thus, the open bite and malocclusion involved is a product of the jaw disparity. Dental Anomalies Associated With Cleft Lip and Palate Dental anomalies refer to abnormalities in a tooth or several teeth that have deviated in form, number, or position. Specific anomalies related to dentition play a role in the potential for speech production difficulties for individuals with cleft lip and palate. The severity of clefting and number of dental anomalies present are typically correlated. Dental anomalies were found to be 7 times more prevalent among patients with cleft lip and palate than the general population (Lopes et al., 1991). More than 93% of patients with unilateral cleft lip and palate and 96% of patients with bilateral cleft lip and palate present with at least one dental anomaly (Akcam et al., 2010; Qureshi et al., 2012; Tannure et al., 2012). The congenital absence of the cleft-sided lateral incisor has been observed in 40%–50% of patients with both unilateral and bilateral cleft lip and palate (Lourenço Ribeiro et al., 2003; Rullo et al., 2015). In a cohort of 201 patients with unilateral cleft lip and palate and unilateral cleft lip and alveolus, Jamilian et al. (2016) identified the upper left lateral incisor as the most frequently missing tooth and this corresponded with the location of the cleft. In a study of patients with isolated cleft palate, Margareta, Rune, and Olafur (1998) identified a higher frequency of agenesis of the mandibular second premolar, followed by the maxillary lateral incisor, and the upper second premolar. Consequently, dental anomalies are specific to the type and location of the cleft or may arise as a result of surgical intervention. Cleftspecific relationships of the central and lateral incisors, as well as missing, malpositioned, or malformed teeth have additionally been reported (Akcam et al., 2010; Camporesi et al., 2010). Anomalies of dentition frequently seen in individuals with cleft lip and palate include missing teeth 1496 (hypodontia), supernumerary teeth, natal teeth, ectopic teeth, malpositioned teeth, crossbites, and open bites (Shprintzen et al., 1985). Fistulae in the anterior oral cavity may be present as well and must be assessed as these also demonstrate the potential to impact speech production depending on the severity and location. Missing teeth (hypodontia). Hypoodontia, or congenitally missing teeth, are common in the primary dentition of patients with cleft lip and palate (Lopes et al., 1991). Missing teeth have been reported to be directly related to severity and location of the cleft, with a higher likelihood of hypodontia occurring in more severe forms of clefting (Lopes et al., 1991). Most often, the lateral incisor neighboring the cleft is affected (Bishara et al., 1985). Supernumerary teeth. Supernumerary teeth, or additional teeth that are present beyond the typical deciduous or permanent dentition, have been reported to occur in approximately 16%–22% of patients with cleft lip and palate (Lopes et al., 1991; Vichi & Franchi, 1995). Lourenço et al. (2003) report this as the second most common anomaly found in patients with cleft lip and palate. These teeth are frequently located near the site of the cleft, but can also be found posteriorly along the maxillary and mandibular arches. Most commonly, these can be present in the maxilla, distal to the cleft in the premaxillary area. Natal teeth. Natal teeth occur in approximately 2% of infants with unilateral cleft lip and palate and 10% of infants with bilateral cleft lip and palate (Leung & Robson, 2006). Natal teeth represent the early eruption of primary deciduous teeth and are reported to occur along the maxillary incisal area of individuals with cleft lip and palate. These teeth are present when the child is born, often demonstrate hypoplastic enamel, and are mobile in nature (Leung & Robson, 2006). Presence of natal teeth may impact successful use of presurgical orthodontics, such as nasal alveolar molding, and require careful extraction (Ziai et al., 2005). Ectopic teeth. Ectopic teeth are those that erupt in an abnormal location. In individuals with cleft lip and palate, eruption adjacent to or within the cleft site is common. Ectopic eruption has been reported to range between 2% and 6% for the maxillary first molars and between 1% and 2% for the permanent canines (Barberia-Leache et al., 2005; Fox et al., 1995). For individuals with cleft palate only, ectopic eruption occurs more frequently in the premolar region (Margareta et al., 1998). Malpositioned teeth. Rotated eruption of the permanent central and lateral maxillary incisors typically occur adjacent to the cleft as a result of altered development (i.e., clefting) along embryological suture lines (Braumann et al., 2002; Letra et al., 2007). Malpositioned teeth are very common in children with cleft lip and palate. Approximately 16% of children with cleft lip and palate and 7% of children with cleft palate only demonstrate malpositioned maxillary teeth (Filho et al., 2015). Positive or negative overjet. These terms are used to describe the horizontal relationship between the anterior dentition. An overjet can be related to the positioning of the teeth alone (dental defect) or associated with occlusal Perspectives of the ASHA Special Interest Groups • Vol. 5 • 1492–1504 • December 2020 Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions SIG 5 Craniofacial and Velopharyngeal Disorders misalignment. When associated with malocclusion, a positive overjet is commonly present with a Class II malocclusion. A negative overjet (or underjet) is commonly correlated with a Class III malocclusion and an anterior crossbite. Overbites and underbites. An overbite or underbite is used to describe the vertical relationship between the anterior dentition. When the maxillary incisors overlap more than 25% of the mandibular incisors, an overbite is present. An underbite is present when the mandibular incisors overlap the maxillary incisors. Underbites may be observed with a Class III malocclusion while overbites may be seen with a Class II malocclusion. Other Contributors to Articulatory Distortions in Cleft Lip and Palate Appliances. Palatal expanders are often placed during the mixed dentition stage (between 6 and 9 years of age) to facilitate maxillary expansion in children with cleft lip and palate. The quad helix device may impact articulatory placement for tongue tip alveolar consonants. However, a rapid palatal expander (see Figure 4) does not typically interfere with articulation given where it is positioned in the oral cavity. Any speech distortion that arises from dental appliances typically resolves once the appliance is removed. Palatal fistulae. Palatal fistulae can occur along embryological fusion lines or surgical suture sites post–palate repair due to a breakdown or dehiscence of tissue (Cohen et al., 1991; Parwaz et al., 2009; Stein et al., 2019). A palatal fistula may also occur as a result of palatal expansion. The impact of a fistula on speech production is highly variable and dependent on size and location (Karling et al., 1993). For example, a fistula located at the junction of the hard and soft palate will result in more significant speech production difficulties than a small pinhole fistula along the alveolar ridge. These small fistulae in the alveolar ridge may have absent or minimal impact on speech in individuals with cleft lip and palate (Karling et al., 1993). Figure 4. Image of a palatal expander. Importance of Identifying Dental and Occlusal Status for SLPs Identification and documentation of the dental and occlusal status is important for SLPs to assess as it guides recommendations and treatment (i.e., “Are the articulation errors I’m detecting able to be remediated with therapeutic measures or is their etiology related to a structural anomaly? Is a referral for an alternate orthodontic, prosthetic, or surgical management route needed?”). Assessment of dental and occlusal status can be completed during the oral exam. To assess dentition, ask the child to “bite/close your teeth and smile.” To visualize the occlusal relationship, clinicians can use a tongue blade to retract the cheek and visualize the posterior molar relationships. Figure 5 presents an example of the multiple dental and occlusal anomalies that could occur in a single patient. As will be discussed below, when speech errors are obligatory to underlying dental or occlusal defects, speech therapy is not typically warranted. Relationship Between Speech Production and Dental/ Occlusal Anomalies in Cleft Lip and Palate According to Kummer (2020), “…when there is normal dental and occlusal relationships, the lips come together easily at rest, the lower lips are able to approximate the maxillary teeth for labiodental sounds, and the jaws (both the maxilla and mandible) are appropriately aligned so that the tongue tip rests under the alveolar ridge and behind the maxillary incisors.” For individuals with cleft lip and palate, these ideal relationships are not always achieved, resulting in articulatory distortions, adaptations, and compensations. Articulation of consonants is determined therefore, in part, by the relationships of the dentition, maxillary and mandibular arches, and hard palate. The majority of speech sounds are produced in the anterior oral cavity and the dental arch Figure 5. Dental and occlusal anomalies in patient with repaired unilateral complete cleft lip and palate demonstrating an anterior and posterior crossbite, collapsed maxillary arch, rotated and malpositioned incisors, congenitally absent lateral incisor on the right, absent premolars, and suspected ectopic eruption of the left lateral incisor along the cleft suture in the alveolar ridge. Mason: Dental Anomalies and Obligatory Speech Errors Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions 1497 SIG 5 Craniofacial and Velopharyngeal Disorders relationship is an important factor in articulatory placement and intelligibility (Johnson & Sandy, 1999; Subtelny & Subtelny, 1959; Vallino & Tompson, 1993). Consequently, due to anatomical differences in the oral cavity arising from a cleft, children with cleft lip and palate typically demonstrate poorer articulation skills than children without cleft palate or with cleft lip only (Chanchareonsook et al., 2006; Kuehn & Moller, 2000; Kummer, 2014; Riski & DeLong, 1984). For example, a cleft that includes the alveolus may alter articulatory contacts for the tongue tip. In cases of bilateral cleft lip and palate, the premaxilla may be significantly protrusive and the ability to achieve a bilabial seal can be impacted for /p, b, m/. Maxillary collapse associated with both unilateral and bilateral cleft lip and palate may contribute to these difficulties as well as occlusal misalignment, missing or malpositioned teeth, ectopic eruption, and the presence of supernumerary teeth in the palatal region. Impact of Dental and Occlusal Anomalies on Speech Production Dental anomalies. Anomalies of the dentition, in the absence of occlusal, velopharyngeal, or other craniofacial differences are less likely to result in significant articulatory deficits. However, when dental variations occur in conjunction with the craniofacial differences commonly seen in individuals with cleft lip and palate, such as arch malformations or velopharyngeal insufficiency, the potential impact on speech production is increased (Subtelny, 1964; Laine et al., 1988). The likelihood of dental anomalies being present during critical periods of speech development is increased for children with cleft lip and palate (Harding & Grunwell, 1996; Vallino et al., 2008). Ectopic eruption and supernumerary teeth can pose difficulties for speech production depending on their location and severity. It is common for the incisors of individuals with cleft lip and palate to be displaced posteriorly or erupt in the palate, which may impact the production of lingua-palatal phonemes (Gable et al., 1995; Leavy et al., 2016). An anterior crossbite can also impact placement of the tongue tip, secondary to interference from the maxillary incisors, which results in an obligatory lateral distortion or frontal distortion. Rotated and misaligned teeth can also impact production of centralized oral airflow resulting in obligatory speech errors. The severity of speech production difficulty has been reported to increase when multiple dental anomalies occur simultaneously (Akcam et al., 2010; Peterson-Falzone, 1988, 1995). Occlusal anomalies. Malocclusion of the maxillary and mandibular arches have the potential to impact articulation. However, the true influence on speech production is often multifactorial, and many occlusal, dental, and/or velopharyngeal anomalies may co-occur to alter the overall function of the articulatory system and severity of the speech deficit (Kummer, 2016; Vallino et al., 2008). Maxillary arch width has been reported to contribute to errors in speech production (Laitinen et al., 1998; Zajac et al., 2012). Poorer articulatory accuracy has been documented in children with 1498 a narrower maxillary arch in comparison to the mandibular arch (Vallino & Tompson, 1993). Severe maxillary protrusion, seen in Class II malocclusions, can impact bilabial closure needed to produce /p/, /b/, and /m/ phonemes, resulting in a labiodental production for these targets. Mandibular protrusion or maxillary retrusion, seen in Class III malocclusions, demonstrates similar speech consequences. The palatal vault is often narrow in Class III malocclusions associated with both unilateral and bilateral cleft lip and palate, and the restricted arch width may impact tongue placement for sibilant and affricate phonemes (R. Mason & Proffit, 1974). Articulatory distortions related to dental open bites and crossbites can be exacerbated by skeletal malocclusion as well. Anterior open bites, resulting from significant arch anomalies, can result in interdental distortions of sibilant targets. Posterior open bites may result in lateral or retroflex distortions (Yamashita & Michi, 1991). Furthermore, both a Class II and Class III malocclusion can reduce the vertical dimension of the anterior oral cavity causing lingual crowding and the potential for obligatory lateral distortion of sibilant phonemes (Kummer, 2020). See Table 2 for a summary of dental and occlusal anomalies and the potential resulting articulation error(s). Phonemes Frequently in Error Fletcher (1978) examined the speech sound production skills of a group of children with cleft lip and palate through the use of factor analysis. In these individuals, it was reported that children with cleft palate produced sibilants (/s, z, ʃ, ʒ/) in error 47% of the time. Nonsibilant fricatives (/θ, ð, f, v/) were produced in error 24% of the time, and plosive targets (/p, b, t, d, k, g/) were produced in error 17% of the time. The speech sound /s/ was the most frequently misarticulated target (Fletcher, 1978). Additional studies have reported similar results related to articulation abilities in children with cleft lip and palate (C. Jones et al., 2003; Morris & Ozanne, 2003; Subtelny & Subtelny, 1959; Whitehill & Chau, 2004). Vallino and Tompson (1993) identified consonant errors across four occlusal patterns. Individuals demonstrating a Class II malocclusion, with and without open bite, produced /s, z/ in error at a rate of 90% and /ʃ, ʒ, tʃ, dʒ/ in error at a rate of 46%–48%, and /p, b, m/ in error at a rate of 9%–11%. Consequently, phonemes commonly impacted by malocclusion and dental anomalies are those produced in the anterior area of the oral cavity and typically include /t, d, f, v, s, z, ʃ, ʒ, tʃ, dʒ/ (C. Jones et al., 2003; Lohmander & Olsson, 2004; Subtelny & Subtelny, 1959; Vallino & Tompson, 1993). Obligatory Articulation Errors Secondary to Dental Anomalies and Malocclusion Obligatory articulation errors result in perceptual distortions of speech sounds secondary to lateral direction of airflow and interdental, retroflex, or lingual placement (Yamashita & Michi, 1991). For example, production of sibilant targets /s/ and /z/ may be produced with what appears as an anteriorly displaced tongue position (lingual protrusion); however, the Class III malocclusal relationship Perspectives of the ASHA Special Interest Groups • Vol. 5 • 1492–1504 • December 2020 Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions SIG 5 Craniofacial and Velopharyngeal Disorders Table 2. Impact of dental and occlusal anomalies on speech. Dental or occlusal anomaly Missing teeth Phonemes impacted Resulting obligatory speech error(s) /s, z/ Depending on location, lateralization, or interdentalization (frontal lisp) of sibilants targets may occur (/s, z/). Distortion of sibilants, lingual–alveolar, and lingual–palatal consonants may occur when teeth are rotated. This can interfere with airflow and tongue placement for alveolar targets (/s, z, ʃ, ʒ , t, d/). If located in the premaxilla or anterior palate, may alter tongue placement of lingual– alveolar consonant targets (/t, d, s, z, n, l/). Malpositioned or rotated teeth /s, z, ʃ, ʒ, t, d/ Ectopic and supernumerary teeth Crossbite (anterior and/or posterior) Open bite /t, d, s, z, n, l/ /f, v, s, z, ʃ, ʒ, tʃ, dʒ/ /m, p, b, t, d, s, z, n, l/ Overbite or Underbite /s, z, ʃ, ʒ/ Class II malocclusion /p, b, m/ Class III malocclusion /p, b, m, f, v, s, z, ʃ, ʒ, tʃ, dʒ/ Lateralization of sibilant and affricate targets (/s, z, ʃ, ʒ, tʃ, dʒ/) may occur. If severe, labiodental phonemes (/f, v/) may be produced as a reverse labiodental. Difficulty approximating lips for bilabial targets in severe Class II and Class III malocclusion. May result in labiodental production of bilabial targets (/p, b/) and interdental distortion of lingual–alveolar targets (/t, d, s, z, n, l/). A shortened vertical dimension may result in lingual crowding or lateral distortion of sibilant targets (/s, z, ʃ, ʒ). May impact bilabial closure of /p, b/ due to inability of upper lip to approximate lower lip. Approximation of these consonants may be obtained by approximating the lower lip with the maxillary central and lateral incisors with a mild auditory and visual distortion. May demonstrate difficulty approximating lips for bilabial targets. May result in labiodental production of bilabial targets (/p, b/), interdental production of sibilants (/s, z/), and reverse labiodental production of fricatives /f, v/. Affricates /ʃ, ʒ, tʃ, dʒ/ may be impacted by lateralized and retroflex distortions from the maxillary dentition. is the cause of the anterior tongue position. This results in an obligatory interdental distortion. Given that the position of the tongue is directly influenced by the oral cavity, this obligatory error is unavoidable and a Class III malocclusion causes the interdental positioning of the tongue for alveolar targets. Obligatory distortions of affricate phonemes may demonstrate similar interdental productions, as a result of a Class III malocclusion, with lingual protrusion resulting in lateralized productions of /tʃ, dʒ/. Class II malocclusions with or without skeletal open bites can also result in interdentalized sibilants, and, in extreme cases, bilabial stops may be produced labiodentally. Daniloff et al. (1980) found interdental productions such as this resulted in less acoustic energy distributed across a broader frequency range, which would explain perceptual differences heard in these obligatory productions. An anterior crossbite can impact sibilants and lingual–alveolar targets as well, resulting in obligatory lateral distortions. In this case, the dorsum of the tongue may articulate with the maxillary incisors causing lateralization of airflow for sibilant and lingual–alveolar targets. Vallino et al. (2019) also make an argument for classifying palatalized tongue tip alveolar stops (/t, d/), when produced with the dorsum of the tongue and tongue tip down, as an obligatory oral distortion, particularly when other tongue tip alveolar targets are impacted (e.g., /l, n/). The authors cite reduced maxillary arch width commonly associated with a Class III malocclusion, eruption of teeth in the anterior palate, and/or oronasal fistulae as potential structural causes for this distortion. This error is often difficult to identify accurately, and SLPs should carefully inspect the articulatory contacts for these targets. Visual distortions have been described by Vallino and Tompson (1993). Visual distortions may also arise as a result of dental and occlusal anomalies. When a visual distortion is present, despite the abnormal appearance of the obligatory articulatory production, the target generally maintains many of the perceptual and acoustic features. For example, an anterior crossbite with Class III malocclusion may obligate an individual to produce a bilabial fricative or a reverse labiodental production for /f/ and /v/ phonemes (Harding & Grunwell, 1995). The lower lips may also articulate with the upper teeth for bilabial stops and nasals (/p, b, m/; Valling, 1990; Vallino & Tompson, 1993). Children with cleft lip and palate may additionally demonstrate a lateral shift of the mandible when attempting sibilant productions (/s, ʃ, tʃ, dʒ/), as a result of anterior dental and occlusal anomalies (Harding & Grunwell, 1996; Vallino & Tompson, 1993). Visual errors of this nature do not typically result in distortions of the acoustic signal. These visual distortions are the result of attempting to produce appropriate oral speech sounds while meeting the demands of rapid, conversational articulation, despite the structural deficits presented by a skeletal or dental malocclusion related to the cleft lip and palate. In a discussion of Vallino and Tompson’s study, Warren (1993) elaborated on how the nature of visual distortions highlights the “highly regulated and precise process of coordination and integration” of the speech structures. He speculated that, in the presence of malocclusion, the speech subsystem is required to adapt to the structural deficit to maintain oral pressure at an appropriate level. He argued that “visual distortions may in fact be successful adaptations in placement.” Others Mason: Dental Anomalies and Obligatory Speech Errors Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions 1499 SIG 5 Craniofacial and Velopharyngeal Disorders have referred to these visual errors as adaptive compensations (LeBlanc & Cisneros, 1995; Leblanc & Golding-Kushner, 1992; Peterson-Falzone et al., 2001). Golding-Kushner (1995) noted that these errors are the “closest possible approximation of a sound in the presence of an anatomic deviation.” In many cases, however, these visual distortions are passive and not active articulatory changes. These errors also differ from compensatory/maladaptive errors, given that they remain in the oral cavity and perceptual/ acoustic characteristics are generally preserved. Obligatory errors of this nature may or may not resolve once the anatomic relationship between oral structures is corrected. Additional research is needed for this unique class of errors to more fully understand the articulatory response to these anatomic differences. Clinical Implications: To Treat or Not to Treat? Generally, when structural deficits are the cause of a speech error, the error will not respond to speech therapy. Production of these targets are likely to improve with dental and/or orthognathic management. For example, orthognathic surgery to improve a Class III malocclusion can result in improved articulation of sibilants without the need for speech intervention. Palatal expansion by the orthodontist may cause a temporary increase in sibilant distortions, but once the child adapts to the expander, speech generally returns to baseline without direct intervention. However, Peterson-Falzone et al. (2001) note that some individuals “may benefit from traditional placement therapy techniques to eliminate mild distortion errors despite the dental or occlusal anomalies that are present.” Generally, the majority of patients will be unable to eliminate these errors until orthodontic or orthognathic management is completed. It remains difficult to predict when this will be the case. Therefore, a thorough assessment and/or diagnostic therapy may be beneficial to facilitate this determination and make referrals as needed. Successful management relies heavily on the contributions of many professions. For obligatory oral distortions, coordination between dental, orthodontic, and speechlanguage practitioners is necessary. Delineation of treatment goals, coordination and timing of treatment across specialties, and maintenance of coordinated follow-up is enhanced through this multidisciplinary process. For patients who may be candidates for orthognathic surgery, pre- and postoperative speech evaluations are necessary (American Cleft Palate-Craniofacial Association, 2018). When articulation deficits are present in children with cleft lip and/or palate, part of the SLP’s role is to identify if what is being perceived during speech production tasks is truly an obligatory distortion or another type of speech error (compensatory or developmental) and to determine appropriate intervention plans (e.g., surgical, dental, speech-language therapy). The oral exam and speech sample are key to making this determination. Trost-Cardamone (2013) has developed a guide specifically related to obtaining speech samples in children with cleft lip and palate. The American 1500 Speech-Language-Hearing Association’s (ASHA) Practice Portal provides an in-depth hierarchy for evaluating speech and resonance in children with cleft lip and palate (ASHA, n.d.). Vallino-Napoli (2004) has additionally developed a process model and flow chart that outlines assessment tasks for this population. The most recent edition of Kummer’s textbook further provides a video library of resources and speech samples to reference for self-study (Kummer, 2020). These resources, in combination with informational sessions presented annually by ASHA’s Special Interest Group (SIG) 5: Craniofacial and Velopharyngeal Disorders, provide a framework to facilitate these clinical decisions. Conclusions The majority of speech sounds in English are produced in the anterior area of the oral cavity. Therefore, the presence of a cleft lip and palate has the potential to significantly alter the anatomic relationships of structures within the oral cavity, resulting in articulatory distortions secondary to dental and occlusal anomalies. There is sufficient evidence that dental and occlusal anomalies have an impact on articulation, but the relationship of dental or occlusal status is not always a direct one (Leavy et al., 2016; PetersonFalzone & Graham, 1990; Vallino & Tompson, 1993). The phonemes most affected by aberrant oral conditions are sibilants, though other phonemes may be impacted as well. These speech errors are considered to be obligatory oral distortions in that they are made in response to an oral structural defect. These speech errors are not typically amenable to speech therapy, but rather require orthodontic and/or surgical correction. Such treatment can be effective in improving these errors, often spontaneously (Golding-Kushner, 2004; Harding & Grunwell, 1995, 1998; Valling, 1990; Vallino et al., 2008). However, speech therapy may be necessary (and most effective) following correction of the oral defects if errors persist (Zajac & Vallino, 2017). Given that obligatory oral distortions frequently co-occur with other articulation errors (e.g., compensatory speech errors, developmental articulation disorders), as well as resonance disorders, SLPs should carefully identify and assess these errors. Collaboration with the craniofacial team and dental professionals is necessary to coordinate care and provide appropriate intervention for these patients. Acknowledgments The author would like to acknowledge Bob Mason for his contributions to this review article. References Akcam, M. O., Evirgen, S., Uslu, O., & Memikoğlu, U. T. (2010). Dental anomalies in individuals with cleft lip and/or palate. The European Journal of Orthodontics, 32(2), 207–213. https:// doi.org/10.1093/ejo/cjp156 American Cleft Palate-Craniofacial Association. (2018). Parameters for evaluation and treatment of patients with cleft lip/palate Perspectives of the ASHA Special Interest Groups • Vol. 5 • 1492–1504 • December 2020 Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions SIG 5 Craniofacial and Velopharyngeal Disorders or other craniofacial differences. The Cleft Palate–Craniofacial Journal, 55(1), 137–156. https://doi.org/10.1177/1055665617739564 American Speech-Language-Hearing Association. (n.d.). Cleft lip and palate [Practice Portal]. https://www.asha.org/practiceportal/clinical-topics/cleft-lip-and-palate/ Angle, E. (1899). Classification of malocclusion. Dental Cosmos, 41, 350–375. Barberia-Leache, E., Suarez-Clúa, M. C., & Saavedra-Ontiveros, D. (2005). Ectopic eruption of the maxillary first permanent molar: Characteristics and occurrence in growing children. The Angle Orthodontist, 75(4), 610–615. Bateman, H., & Mason, R. (1984). Applied anatomy and physiology of the speech and hearing mechanism. Charles C. Thomas Publisher Limited. Bishara, S. E. (1973). Cephalometric evaluation of facial growth in operated and non-operated individuals with isolated clefts of the palate. The Cleft Palate Journal, 10(3), 239–246. Bishara, S. E., de Arrendondo, R., Vales, H., & Jakobsen, J. (1985). Dentofacial relationships in persons with unoperated clefts: Comparisons between three cleft types. American Journal of Orthodontics, 87(6), 481–507. https://doi.org/10.1016/0002-9416 (85)90086-7 Bloomer, H. H. (1971). Speech defects associated with dental malocclusions and related abnormalities. In L. E. Travis (Ed.), Handbook of Speech Pathology and Audiology (pp. 715–766). Prentice-Hall. Braumann, B., Keilig, L., Bourauel, C., & Jäger, A. (2002). Threedimensional analysis of morphological changes in the maxilla of patients with cleft lip and palate. The Cleft Palate–Craniofacial Journal, 39(1), 1–11. https://doi.org/10.1597/1545-1569(2002) 039<0001:TDAOMC>2.0.CO;2 Camporesi, M., Baccetti, T., Marinelli, A., Defraia, E., & Franchi, L. (2010). Maxillary dental anomalies in children with cleft lip and palate: A controlled study. International Journal of Paediatric Dentistry, 20(6), 442–450. https://doi.org/10.1111/j.1365-263X. 2010.01063.x Chanchareonsook, N., Samman, N., & Whitehill, T. L. (2006). The effect of cranio-maxillofacial osteotomies and distraction osteogenesis on speech and velopharyngeal status: A critical review. The Cleft Palate–Craniofacial Journal, 43(4), 477–487. https:// doi.org/10.1597/05-001R1.1. https://doi.org/10.1597/05-0011.1 Christie, T. (1977). Cephalometric patterns of adults with normal occlusion. The Angle Orthodontist, 47(2), 128–135. Cohen, S., Kalinowski, J., LaRossa, D., & Randall, P. (1991). Cleft palate fistulas: A multivariate statistical analysis of prevalence, etiology, and surgical management. Plastic and Reconstructive Surgery, 87(6), 1041–1047. https://doi.org/ 10.1097/00006534-199106000-00005 Courtney, M., Harkness, M., & Herbison, P. (1996). Maxillary and cranial base changes during treatment with functional appliances. American Journal of Orthodontics and Dentofacial Orthopedics, 109(6), 616–624. https://doi.org/10.1016/S08895406(96)70073-2 Daniloff, R. G., Wilcox, K., & Stephens, M. I. (1980). An acousticarticulatory description of children’s defective /s/ productions. Journal of Communication Disorders, 13(5), 347–363. https:// doi.org/10.1016/0021-9924(80)90004-0 da Silva Dalben, G., Costa, B., & Gomide, M. R. (2006). Prevalence of dental anomalies, ectopic eruption and associated oral malformations in subjects with Treacher Collins syndrome. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, 101(5), 588–592. https://doi.org/10.1016/j.tripleo.2005.07.016 da Silva Filho, O. G., Normando, A. D. C., & Capelozza Filho, L. (1993). Mandibular growth in patients with cleft lip and/or cleft palate—The influence of cleft type. American Journal of Orthodontics and Dentofacial Orthopedics, 104(3), 269–275. https://doi.org/10.1016/S0889-5406(05)81729-9 Doucet, J.-C., Russell, K. A., Daskalogiannakis, J., Mercado, A. M., Emanuele, N., James, L., Hathaway, R. R., & Long, R. E., Jr. (2019). Facial growth of patients with complete unilateral cleft lip and palate treated with alveolar bone grafting at 6 years. The Cleft Palate–Craniofacial Journal, 56(5), 619–627. https:// doi.org/10.1177/1055665618792791 Ellis, E., & McNamara, J. A. (1984). Components of adult class III malocclusion. Journal of Oral and Maxillofacial Surgery, 42(5), 295–305. https://doi.org/10.1016/0278-2391(84)90109-5 Figueroa, A. A., & Polley, J. W. (2007). Management of the severe cleft and syndromic midface hypoplasia. Orthodontics & Craniofacial Research, 10(3), 167–179. https://doi.org/10.1111/j.16016343.2007.00392.x Filho, M. R. M., Dias, V. O., Martelli, D. R., Paranaíba, L. R., Swerts, M. S. O., de Barros, L. M., & Júnior, H. M. (2015). Tooth malposition in patients with cleft lip and/or palate in a Brazilian population. Dentistry 3000, 3(1), 32–37. https://doi. org/10.5195/D3000.2015.38 Fletcher, S. G. (1978). Diagnosing speech disorders from cleft palate. Grune & Statton. Fox, N., Fletcher, G., & Horner, K. (1995). Localising maxillary canines using dental panoramic tomography. British Dental Journal, 179(11), 416–420. https://doi.org/10.1038/sj.bdj.4808945 Gable, T. O., Kummer, A. W., Lee, L., Creaghead, N. A., & Moore, L. J. (1995). Premature loss of the maxillary primary incisors: Effect on speech production. ASDC Journal of Dentistry for Children, 62(3), 173–179. Garrahy, A., Millett, D. T., & Ayoub, A. F. (2005). Early assessment of dental arch development in repaired unilateral cleft lip and unilateral cleft lip and palate versus controls. The Cleft Palate–Craniofacial Journal, 42(4), 385–391. https://doi.org/ 10.1597/03-159.1 Golding-Kushner, K. (1995). Treatment of articulation and resonance disorders associated with cleft palate and VPI. In R. J. Shprintzen & J. Bardach (Eds.), Cleft Palate speech management: A multidisciplinary approach (pp. 327–351). Mosby. Golding-Kushner, K. (2004). Treatment of sound system disorders associated with cleft palate speech. SIG 5 Perspectives on Speech Science and Orofacial Disorders, 14(2), 16–20. https://doi.org/ 10.1044/ssod14.2.16 Guyer, E. C., Ellis, E. E., McNamara, J. A., & Behrents, R. G. (1986). Components of class III malocclusion in juveniles and adolescents. The Angle Orthodontist, 56(1), 7–30. Harding, A., & Grunwell, P. (1995). Active versus passive cleft-type speech characteristics: Implications for surgery and therapy. International Journal of Language & Communication Disorders, 30(S1), 242–247. https://doi.org/10.1111/j.1460-6984.1995. tb01679.x Harding, A., & Grunwell, P. (1996). Characteristics of cleft palate speech. International Journal of Language & Communication Disorders, 31(4), 331–357. https://doi.org/10.3109/13682829609031326 Harding, A., & Grunwell, P. (1998). Active versus passive clefttype speech characteristics. International Journal of Language & Communication Disorders, 33(3), 329–352. https://doi.org/ 10.1080/136828298247776 Hardin-Jones, M. A., & Jones, D. L. (2005). Speech production of preschoolers with cleft palate. The Cleft Palate–Craniofacial Journal, 42(1), 7–13. https://doi.org/10.1597/03-134.1 Honda, Y., Suzuki, A., Nakamura, N., & Ohishi, M. (2002). Relationship between primary palatal form and maxillofacial growth in Japanese children with unilateral cleft lip and palate: Infancy Mason: Dental Anomalies and Obligatory Speech Errors Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions 1501 SIG 5 Craniofacial and Velopharyngeal Disorders to adolescence. The Cleft Palate–Craniofacial Journal, 39(5), 527–534. https://doi.org/10.1597/1545-1569_2002_039_0527_ rbppfa_2.0.co_2 Hutters, B., & Brøndsted, K. (1987). Strategies in cleft palate speech with special reference to Danish. The Cleft Palate Journal, 24(2), 126–136. Jackson, O. A., Kaye, A. E., Lee, A., Minugh-Purvis, N., Cohen, M. A., Solot, C. B., McDonald-McGinn, D., Jawad, A. F., Zackai, E. H., & Kirschner, R. E. (2020). Orofacial manifestations of stickler syndrome: An analysis of speech outcome and facial growth after cleft palate repair. Annals of Plastic Surgery, 84(6), 665–671. https://doi.org/10.1097/SAP.0000000000002114 Jamilian, A., Lucchese, A., Darnahal, A., Kamali, Z., & Perillo, L. (2016). Cleft sidedness and congenitally missing teeth in patients with cleft lip and palate patients. Progress in Orthodontics, 17(1), Article 14. https://doi.org/10.1186/s40510-016-0127-z Johnson, N. C., & Sandy, J. R. (1999). Tooth position and speechIs there a relationship? The Angle Orthodontist, 69(4), 306–310. Jolleys, A. (1954). A review of the results of operations on cleft palates with reference to maxillary growth and speech function. British Journal of Plastic Surgery, 7, 229–241. https://doi. org/10.1016/S0007-1226(54)80027-0 Jones, D. L. (2000). The relationship between temporal aspects of oral-nasal balance and classification of velopharyngeal status in speakers with cleft palate. The Cleft Palate–Craniofacial Journal, 37(4), 363–369. https://doi.org/10.1597/1545-1569_2000_037_ 0363_trbtao_2.3.co_2 Jones, C., Chapman, K., & Hardin-Jones, M. (2003). Speech development of children with cleft palate before and after palatal surgery. The Cleft Palate–Craniofacial Journal, 40(1), 19–31. https:// doi.org/10.1597/1545-1569(2003)040<0019:SDOCWC>2.0. CO;2 Kamioka, H., Ishihara, Y., Sawada, D., & Takano-Yamamoto, T. (2007). A case of Stickler syndrome with orthodontic treatment. Orthodontic Waves, 66(2), 52–59. https://doi.org/10.1016/j.odw. 2007.03.002 Karling, J., Larson, O., & Henningsson, G. (1993). Oronasal fistulas in cleft palate patients and their influence on speech. Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery, 27(3), 193–201. https://doi.org/10.3109/02844319309078111 Katz, M. I. (1992a). Angle classification revisited 1: Is current use reliable? American Journal of Orthodontics and Dentofacial Orthopedics, 102(2), 173–179. https://doi.org/10.1016/0889-5406 (92)70030-E Katz, M. I. (1992b). Angle classification revisited 2: A modified Angle classification. American Journal of Orthodontics and Dentofacial Orthopedics, 102(3), 277–284. https://doi.org/ 10.1016/S0889-5406(05)81064-9 Kuehn, D. P., & Moller, K. T. (2000). Speech and language issues in the cleft palate population: The state of the art. The Cleft Palate-Craniofacial Journal, 37(4), 348–348. https://doi.org/ 10.1597/1545-1569(2000)037<0348:SALIIT>2.3.CO;2 Kummer, A. W. (2014). Speech and resonance disorders related to cleft palate and velopharyngeal dysfunction: A guide to evaluation and treatment. SIG 16 Perspectives on School-Based Issues, 15(2), 57–74. https://doi.org/10.1044/sbi15.2.57 Kummer, A. W. (2016). Evaluation of speech and resonance for children with craniofacial anomalies. Facial Plastic Surgery Clinics, 24(4), 445–451. https://doi.org/10.1016/j.fsc.2016.06.003 Kummer, A. W. (2020). Dental anomalies. In A. W. Kummer (Ed.), Cleft palate and craniofacial conditions: A comprehensive guide to clinical management (pp. 149–189). Jones & Bartlett Learning. Laine, T., Warren, D. W., Dalston, R. M., Hairfield, W. M., & Morr, K. E. (1988). Intraoral pressure, nasal pressure and 1502 airflow rate in cleft palate speech. Journal of Speech and Hearing Research, 31(3), 432–437. https://doi.org/10.1044/jshr.3103.432 Laitinen, J., Ranta, R., Pulkkinen, J., & Haapanen, M.-L. (1998). The association between dental arch dimensions and occurrence of Finnish dental consonant misarticulations in cleft lip/palate children. Acta Odontologica Scandinavica, 56(5), 308–312. https:// doi.org/10.1080/000163598428509 Leavy, K. M., Cisneros, G. J., & LeBlanc, E. M. (2016). Malocclusion and its relationship to speech sound production: Redefining the effect of malocclusal traits on sound production. American Journal of Orthodontics and Dentofacial Orthopedics, 150(1), 116–123. https://doi.org/10.1016/j.ajodo.2015. 12.015 LeBlanc, S., & Cisneros, G. (1995). The dynamics of speech and orthodontic management in cleft lip and palate. In M. Sasser & K. F. White (Eds.), Cleft Palate Speech Management (pp. 352–363). Mosby. Leblanc, S. M., & Golding-Kushner, K. J. (1992). Effect of glossopexy on speech sound production in Robin sequence. The Cleft Palate–Craniofacial Journal, 29(3), 239–245. https://doi.org/ 10.1597/1545-1569_1992_029_0239_eogoss_2.3.co_2 Letra, A., Menezes, R., Granjeiro, J., & Vieira, A. (2007). Defining subphenotypes for oral clefts based on dental development. Journal of Dental Research, 86(10), 986–991. https://doi.org/ 10.1177/154405910708601013 Leung, A. K., & Robson, W. L. (2006). Natal teeth: A review. Journal of the National Medical Association, 98(2), 226–228. Liao, Y.-F., & Mars, M. (2005). Long-term effects of clefts on craniofacial morphology in patients with unilateral cleft lip and palate. The Cleft Palate–Craniofacial Journal, 42(6), 601–609. https://doi.org/10.1597/04-163r.1 Lohmander, A., & Olsson, M. (2004). Methodology for perceptual assessment of speech in patients with cleft palate: A critical review of the literature. The Cleft Palate–Craniofacial Journal, 41(1), 64–70. https://doi.org/10.1597/02-136 Long, R. E., Jr, Semb, G., & Shaw, W. C. (2000). Orthodontic treatment of the patient with complete clefts of lip, alveolus, and palate: Lessons of the past 60 years. The Cleft Palate–Craniofacial Journal, 37(6), 1–13. https://doi.org/10.1597/1545-1569_2000_ 037_0533_ototpw_2.0.co_2 Lopes, L. D., Mattos, B., & Andre, M. (1991). Anomalies in number of teeth in patients with lip and/or palate clefts. Brazilian Dental Journal, 2(1), 9–17. Lourenço Ribeiro, L., Teixeira das Neves, L., Costa, B., & Ribeiro Gomide, M. (2003). Dental anomalies of the permanent lateral incisors and prevalence of hypodontia outside the cleft area in complete unilateral cleft lip and palate. The Cleft Palate– Craniofacial Journal, 40(2), 172–175. https://doi.org/10.1597/ 1545-1569_2003_040_0172_daotpl_2.0.co_2 Margareta, L., Rune, H., & Olafur, P. J. (1998). Dental abnormalities and ectopic eruption in patients with isolated cleft palate. Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery, 32(2), 203–212. https://doi.org/ 10.1080/02844319850158831 Mars, M., & Houston, W. J. (1990). A preliminary study of facial growth and morphology in unoperated male unilateral cleft lip and palate subjects over 13 years of age. Cleft Palate Journal, 27(1), 7–10. https://doi.org/10.1597/1545-1569_1990_027_0007_ apsofg_2.3.co_2 Marshs, J. L. (2009). Velo-pharyngeal dysfunction: Evaluation and management. Indian Journal of Plastic Surgery, 42, S129–S136. https://doi.org/10.4103/0970-0358.57201 Martelli-Junior, H., Coletta, R. D., Miranda, R.-T., de Barros, L.-M., Swerts, M.-S., & Bonan, P.-R. (2009). Orofacial features Perspectives of the ASHA Special Interest Groups • Vol. 5 • 1492–1504 • December 2020 Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions SIG 5 Craniofacial and Velopharyngeal Disorders of Treacher Collins syndrome. Medicina Oral Patologia Oral y Cirugia Bucal, 14(7), E344–E348. Mason, K., & Perry, J. (2016). Relationship between age and diagnosis on volumetric and linear velopharyngeal measures in the cleft and noncleft populations. Journal of Craniofacial Surgery, 27(5), 1340–1345. https://doi.org/10.1097/SCS.0000000000002744 Mason, R., & Proffit, W. (1974). The tongue thrust controversy: Background and recommendations. Journal of Speech and Hearing Disorders, 39(2), 115–132. https://doi.org/10.1044/ jshd.3902.115 Meazzini, M. C., Donati, V., Garattini, G., & Brusati, R. (2008). Maxillary growth impairment in cleft lip and palate patients: A simplified approach in the search for a cause. Journal of Craniofacial Surgery, 19(5), 1302–1307. https://doi.org/10.1097/ SCS.0b013e31814fb711 Meazzini, M. C., Tortora, C., Morabito, A., Garattini, G., & Brusati, R. (2011). Factors that affect variability in impairment of maxillary growth in patients with cleft lip and palate treated using the same surgical protocol. Journal of Plastic Surgery and Hand Surgery, 45(4–5), 188–193. https://doi.org/ 10.3109/2000656X.2011.583493 Meyer-Marcotty, P., Kochel, J., Boehm, H., Linz, C., Klammert, U., & Stellzig-Eisenhauer, A. (2011). Face perception in patients with unilateral cleft lip and palate and patients with severe Class III malocclusion compared to controls. Journal of CranioMaxillofacial Surgery, 39(3), 158–163. https://doi.org/10.1016/ j.jcms.2010.05.001 Molina, F., & Figueroa, A. A. (1999). Distraction of the maxilla. In J. G. McCarthy (Ed.), Distraction of the craniofacial skeleton (pp. 308–320). Springer. https://doi.org/10.1007/978-1-46122140-1_11 Molsted, K., & Dahl, E. (1990). Asymmetry of the maxilla in children with complete unilateral cleft lip and palate. The Cleft Palate Journal, 27(2), 184–190. discussion 190–192. https:// doi.org/10.1597/1545-1569(1990)027<0184:AOTMIC>2.3.CO;2 Morris, H., & Ozanne, A. (2003). Phonetic, phonological, and language skills of children with a cleft palate. The Cleft PalateCraniofacial Journal, 40(5), 460–470. https://doi.org/10.1597/ 1545-1569_2003_040_0460_ppalso_2.0.co_2 Ogasawara, T., Kitagawa, Y., Ogawa, T., Yamada, T., Nakamura, M., & Sano, K. (2002). Treatment of severe mandibular prognathism in combination with maxillary hypoplasia: Case report. Journal of Cranio-Maxillofacial Surgery, 30(4), 226–229. https:// doi.org/10.1054/jcms.2002.0316 Parwaz, M. A., Sharma, R. K., Parashar, A., Nanda, V., Biswas, G., & Makkar, S. (2009). Width of cleft palate and postoperative palatal fistula—Do they correlate? Journal of Plastic, Reconstructive & Aesthetic Surgery, 62(12), 1559–1563. https://doi. org/10.1016/j.bjps.2008.05.048 Peat, J. H. (1974). Early orthodontic treatment for complete clefts. American Journal of Orthodontics, 65(1), 28–38. https://doi.org/ 10.1016/0002-9416(74)90155-9 Peterson, S. J. (1975). Nasal emission as a component of the misarticulation of sibilants and affricates. Journal of Speech and Hearing Disorders, 40(1), 106–114. https://doi.org/10.1044/ jshd.4001.106 Peterson-Falzone, S. J. (1988). Speech disorders related to craniofacial structural defects: Part 2. In N. J. Lass, L. V. McReynolds, J. L. Northern, & D. E. Yoder (Eds.), Handbook of SpeechLanguage Pathology and Audiology (pp. 477–547). Decker. Peterson-Falzone, S. J. (1995). Speech outcomes in adolescents with cleft lip and palate. The Cleft Palate–Craniofacial Journal, 32(2), 125–128. https://doi.org/10.1597/1545-1569_1995_ 032_0125_soiawc_2.3.co_2 Peterson-Falzone, S. J., & Graham, M. S. (1990). Phoneme-specific nasal emission in children with and without physical anomalies of the velopharyngeal mechanism. Journal of Speech and Hearing Disorders, 55(1), 132–139. https://doi.org/10.1044/jshd. 5501.132 Peterson-Falzone, S. J., Hardin-Jones, M., Karnell, M., & McWilliams, B. (2001). Cleft palate speech. Mosby. Pruzansky, S., & Aduss, H. (1964). Arch form and the deciduous occlusion in complete unilateral clefts. The Cleft Palate Journal, 1(4), 411–418. Qureshi, W. A., Beiraghi, S., & Leon-Salazar, V. (2012). Dental anomalies associated with unilateral and bilateral cleft lip and palate. Journal of Dentistry for Children, 79(2), 69–73. Reddy, R. R., Reddy, S. G., Vaidhyanathan, A., Bergé, S. J., & Kuijpers-Jagtman, A. M. (2017). Maxillofacial growth and speech outcome after one-stage or two-stage palatoplasty in unilateral cleft lip and palate. A systematic review. Journal of Cranio-Maxillofacial Surgery, 45(6), 995–1003. https://doi.org/ 10.1016/j.jcms.2017.03.006 Reiser, E., Andlin-Sobocki, A., Mani, M., & Holmström, M. (2011). Initial size of cleft does not correlate with size and function of nasal airway in adults with unilateral cleft lip and palate. Journal of Plastic Surgery and Hand Surgery, 45(3), 129–135. https://doi. org/10.3109/2000656X.2011.576839 Reiser, E., Skoog, V., Gerdin, B., & Andlin-Sobocki, A. (2010). Association between cleft size and crossbite in children with cleft palate and unilateral cleft lip and palate. The Cleft Palate– Craniofacial Journal, 47(2), 175–181. https://doi.org/10.1597/ 08-219_1 Riski, J. (1979). Articulation skills and oral-nasal resonance in children with pharyngeal flaps. The Cleft Palate Journal, 16(4), 421–428. Riski, J., & DeLong, E. (1984). Articulation development in children with cleft lip/palate. The Cleft Palate Journal, 21(1), 57–64. Ross, R. (1970). The clinical implications of facial growth in cleft lip and palate. The Cleft Palate Journal, 7(1), 37–47. Rullo, R., Festa, V. M., Rullo, R., Addabbo, F., Chiodini, P., Vitale, M., & Perillo, L. (2015). Prevalence of dental anomalies in children with cleft lip and unilateral and bilateral cleft lip and palate. European Journal of Paediatric Dentistry, 16(3), 229–232. Satoh, K., Nagata, J., Shomura, K., Wada, T., Tachimura, T., Fukuda, J., & Shiba, R. (2004). Morphological evaluation of changes in velopharyngeal function following maxillary distraction in patients with repaired cleft palate during mixed dentition. The Cleft Palate–Craniofacial Journal, 41(4), 355–363. https:// doi.org/10.1597/02-153.1 Sell, D. (2005). Issues in perceptual speech analysis in cleft palate and related disorders: A review. International Journal of Language & Communication Disorders, 40(2), 103–121. https://doi. org/10.1080/13682820400016522 Shibasaki, Y., & Ross, R. (1969). Facial growth in children with isolated cleft palate. Cleft Palate J, 6(290–302), 49–62. Shprintzen, R. J., Siegel-Sadewitz, V. L., Amato, J., Goldberg, R. B., Opitz, J. M., & Reynolds, J. F. (1985). Anomalies associated with cleft lip, cleft palate, or both. American Journal of Medical Genetics, 20(4), 585–595. https://doi.org/10.1002/ajmg. 1320200404 Stein, M. J., Zhang, Z., Fell, M., Mercer, N., & Malic, C. (2019). Determining postoperative outcomes after cleft palate repair: A systematic review and meta-analysis. Journal of Plastic, Reconstructive & Aesthetic Surgery, 72(1), 85–91. https://doi.org/ 10.1016/j.bjps.2018.08.019 Subtelny, J. D. (1964). Physio-acoustic considerations in the radiographic study of speech. The Cleft Palate Journal, 1(4), 402–410. Mason: Dental Anomalies and Obligatory Speech Errors Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions 1503 SIG 5 Craniofacial and Velopharyngeal Disorders Subtelny, J. D., & Sakuda, M. (1964). Open-bite: Diagnosis and treatment. American Journal of Orthodontics, 50(5), 337–358. https://doi.org/10.1016/0002-9416(64)90175-7 Subtelny, J. D., & Subtelny, J. D. (1959). Intelligibility and associated physiological factors of cleft palate speakers. Journal of Speech and Hearing Research, 2(4), 353–360. https://doi.org/ 10.1044/jshr.0204.353 Suri, S., Ross, R. B., & Tompson, B. D. (2010). Craniofacial morphology and adolescent facial growth in Pierre Robin sequence. American Journal of Orthodontics and Dentofacial Orthopedics, 137(6), 763–774. https://doi.org/10.1016/j.ajodo.2008. 07.020 Tan, E. L., Yow, M., Kuek, M. C., & Wong, H. C. (2012). Dental maturation of unilateral cleft lip and palate. Annals of Maxillofacial Surgery, 2(2), 158–162. https://doi.org/10.4103/22310746.101345 Tannure, P. N., Oliveira, C. A. G., Maia, L. C., Vieira, A. R., Granjeiro, J. M., & de Castro Costa, M. (2012). Prevalence of dental anomalies in nonsyndromic individuals with cleft lip and palate: A systematic review and meta-analysis. The Cleft Palate–Craniofacial Journal, 49(2), 194–200. https://doi.org/ 10.1597/10-043 Tome, W., Yashiro, K., Otsuki, K., Kogo, M., & Yamashiro, T. (2016). Influence of different palatoplasties on the facial morphology of early mix dentition stage children with unilateral cleft lip and palate. The Cleft Palate–Craniofacial Journal, 53(2), 28–33. https://doi.org/10.1597/14-191 Trost, J. E. (1981). Articulatory additions to the classical description of the speech of persons with cleft palate. The Cleft Palate Journal, 18(3), 193–203. Trost-Cardamone, J. (2013). Cleft palate speech: A comprehensive two-part set. American Speech-Language-Hearing Association. Valling, L. D. (1990). Speech, velopharyngeal function, and hearing before and after orthognathic surgery. Journal of Oral and Maxillofacial Surgery, 48(12), 1274–1281. https://doi.org/10.1016/ 0278-2391(90)90481-G Vallino, L. D., Ruscello, D. M., & Zajac, D. J. (2019). Ceft palate speech and resonance: An audio and video resource. Plural. Vallino, L. D., & Tompson, B. (1993). Perceptual characteristics of consonant errors associated with malocclusion. Journal of Oral and Maxillofacial Surgery, 51(8), 850–856. https://doi.org/ 10.1016/S0278-2391(10)80101-6 Vallino, L. D., Zuker, R., & Napoli, J. A. (2008). A study of speech, language, hearing, and dentition in children with cleft lip only. The Cleft Palate–Craniofacial Journal, 45(5), 485–494. https:// doi.org/10.1597/06-207.1 1504 Vallino-Napoli, L. D. (2002). A profile of the features and speech in patients with mandibulofacial dysostosis. The Cleft Palate– Craniofacial Journal, 39(6), 623–634. https://doi.org/10.1597/ 1545-1569_2002_039_0623_apotfa_2.0.co_2 Vallino-Napoli, L. D. (2004). Assessing communication in cleft and craniofacial disorders: A process model for the practitioner. SIG 5 Perspectives on Speech Science and Orofacial Disorders, 14(2), 9–16. https://doi.org/10.1044/ssod14.2.9 Vargervik, K. (1983). Growth characteristics of the premaxilla and orthodontic treatment principles in bilateral cleft lip and palate. The Cleft Palate Journal, 20(4), 289–302. Vichi, M., & Franchi, L. (1995). Abnormalities of the maxillary incisors in children with cleft lip and palate. ASDC Journal of Dentistry for Children, 62(6), 412–417. Wangsrimongkol, T., & Jansawang, W. (2010). The assessment of treatment outcome by evaluation of dental arch relationships in cleft lip/palate. Journal of the Medical Association of Thailand, 93(4), 7. Warren, D. W. (1993). Perceptual characteristics of consonant errors associated with malocclusion. Journal of Oral and Maxillofacial Surgery, 51(8), 856. https://doi.org/10.1016/S0278-2391 (10)80102-8 Whitehill, T. L., & Chau, C. H.-F. (2004). Single-word intelligibility in speakers with repaired cleft palate. Clinical Linguistics & Phonetics, 18(4–5), 341–355. https://doi.org/10.1080/ 02699200410001663344 Wolford, L. M., & Stevao, E. L. (2002). Correction of jaw deformities in patients with cleft lip and palate. Baylor University Medical Center Proceedings, 15(3s), 250–254. https://doi.org/ 10.1080/08998280.2002.11927848 Yamashita, Y., & Michi, K.-I. (1991). Misarticulation caused by abnormal lingual-palatal contact in patients with cleft palate with adequate velopharyngeal function. The Cleft Palate–Craniofacial Journal, 28(4), 360–368. https://doi.org/10.1597/1545-1569_ 1991_028_0360_mcbalp_2.3.co_2 Zajac, D. J., Cevidanes, L., Shah, S., & Haley, K. (2012). Maxillary arch dimensions and spectral characteristics of children with cleft lip and palate who produce middorsum palatal stops. Journal of Speech, Language, and Hearing Research, 55(6), 1876–1886. https://doi.org/10.1044/1092-4388(2012/11-0340) Zajac, D. J., & Vallino, L. D. (2017). Evaluation and management of cleft lip and palate: A developmental perspective. Plural. Ziai, M., Bock, D., Da Silveira, A., & Daw, J. (2005). Natal teeth: A potential impediment to nasoalveolar molding in infants with cleft lip and palate. Journal of Craniofacial Surgery, 16(2), 262–266. https://doi.org/10.1097/00001665-200503000-sss2 Perspectives of the ASHA Special Interest Groups • Vol. 5 • 1492–1504 • December 2020 Downloaded from: https://pubs.asha.org Sarah Vetter on 12/26/2020, Terms of Use: https://pubs.asha.org/pubs/rights_and_permissions