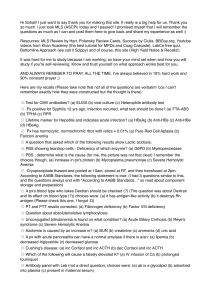
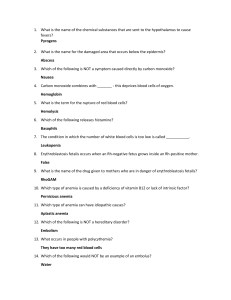
CIMS Weekly Quiz Week: 10 Question # 1 Question A 56‐year‐old # man is admitted to the hospital with exertional chest pain. Medical history is significant for hypertension and type 2 diabetes mellitus. Medications are lisinopril, atorvastatin, and metformin. On physical examination, temperature is 37.1 °C (98.8 °F), blood pressure is 126/67 mm Hg, pulse rate is 106/min, and respiration rate is 18/min. BMI is 27. The patient has pale conjunctivae and icteric sclerae. Cardiopulmonary examination reveals clear lungs and an S4. His abdomen is soft and nontender, with no organomegaly. Laboratory studies: Hemoglobin 7.6 g/dL (76 g/L) Leukocyte count 3900/µL (3.9 × 109/L) Platelet count 56,000/µL (56 × 109/L) Reticulocyte count 0.5% Alanine aminotransferase 29 units/L Aspartate aminotransferase 27 units/L Total bilirubin 4.9 mg/dL (84 µmol/L) Direct bilirubin 1.0 mg/dL (17 µmol/L) Lactate dehydrogenase 427 units/L Results of the direct Coombs (antiglobulin) test are negative. A peripheral blood smear is shown. An electrocardiogram is normal. Which of the following is the most likely diagnosis? A. Cobalamin deficiency B. Hereditary spherocytosis C. Paroxysmal cold hemoglobinuria D. Warm autoimmune hemolytic anemia See Image Answer : A ID: Utility:8 Difficulty: Low Pediatrics 2473 e19 Chapter: 128 Patients with cobalamin deficiency can have macroovalocytes and hypersegmented polymorphonuclear cells on the peripheral blood Answer : smear and hemolysis. The most likely diagnosis is cobalamin deficiency. This patient's peripheral blood smear shows macroovalocytes and hypersegmented polymorphonuclear cells consistent with cobalamin deficiency. Because cobalamin is necessary for erythrocyte maturation, cobalamin deficiency results in ineffective erythropoiesis that can present as hemolysis. Some patients with cobalamin deficiency may have glossitis, weight loss, and pale yellow skin caused by the combination of anemia and hemolysis, as well as possible neurologic manifestations, including loss of position or vibratory sense that can progress to spastic ataxia. Warm autoimmune hemolytic anemia is characterized by insidious symptoms and findings of anemia or jaundice and a peripheral blood smear showing spherocytes, which are erythrocytes that have lost their central pallor. In addition, the direct Coombs (antiglobulin) test is frequently strongly positive for IgG and negative or weakly positive for complement. Paroxysmal cold hemoglobinuria is a rare cause of hemolysis in adults and is caused by IgG antibodies that bind to the P‐antigen on erythrocytes in the cold, resulting in complement fixation and hemolysis upon warming. Macrocytosis and hypersegmented polymorphonuclear cells are not seen in paroxysmal cold hemoglobinuria, which may be associated with microspherocytes. Hereditary spherocytosis is an inherited disorder of the red cell membrane characterized by spherocytes on the peripheral blood smear and an increased likelihood of calcium bilirubinate gallstones. Splenomegaly is common in patients with this disorder. Bibliography Acharya U, Gau JT, Horvath W, Ventura P, Hsueh CT, Carlsen W. Hemolysis and hyperhomocysteinemia caused by cobalamin deficiency: three case reports and review of the literature. J Hematol Oncol. 2008;18:1‐26. PMID: 19094231 Question # 2 Question You are seeing # a patient in follow‐up in whom you have begun an evaluation for an elevated hematocrit. You suspect polycythemia vera based on a history of aquagenic pruritus and splenomegaly. Which set of laboratory tests are consistent with the diagnosis of polycythemia vera? A. Elevated red blood cell mass, high serum erythropoietin levels, normal oxygen saturation B. Elevated red blood cell mass, low serum erythropoietin levels, normal oxygen saturation C. Normal red blood cell mass, high serum erythropoietin levels, low arterial oxygen saturation D. Normal red blood cell mass, low serum erythropoietin levels, low arterial oxygen saturation Answer : B ID: Utility:6 Difficulty: Mod Pediatrics 1483 e19 Chapter: 131 The first step Answer : in diagnosing polycythemia vera is to document an elevated red blood cell (RBC) mass. A normal RBC mass suggests spurious polycythemia. Next, serum erythropoietin (EPO) levels should be measured. If EPO levels are low, the diagnosis is polycythemia vera. Confirmatory tests include JAK‐2 mutation analysis, leukocytosis, and thrombocytosis. Elevated EPO levels are seen in the normal physiologic response to hypoxia as well as in autonomous production of EPO. Further steps in the workup include evaluation for hypoxia with an arterial blood gas, consideration of smoker's polycythemia (elevated carboxyhemoglobin levels) and disorders of increased hemoglobin affinity for oxygen. Low serum EPO levels with low oxygen saturation suggest inadequate renal production (renal failure). High RBC mass and high EPO levels with normal oxygen saturation may be seen with autonomous EPO production, such as in renal cell carcinoma. Question # 3 Question The triad of # portal vein thrombosis, hemolysis, and pancytopenia suggests which of the following diagnoses? A. Acute promyelocytic leukemia B. Hemolytic‐uremic syndrome (HUS) C. Leptospirosis D. Paroxysmal nocturnal hemoglobinuria (PNH) E. Thrombotic thrombocytopenia purpura (TTP) Answer : D ID: 1470 e19 Chapter: 129 Utility:7 Difficulty: Mod Pediatrics Each of the: listed diagnoses has a rather characteristic set of laboratory findings that are virtually diagnostic for the disease once the Answer disease has progressed to a severe stage. Both HUS and TTP cause hemolysis and thrombocytopenia, as well as fevers. Cerebrovascular events and mental status change occur more commonly in TTP, and renal failure is more common in HUS. Severe leptospirosis, or Weil's disease, is notable for fevers, hyperbilirubinemia, and renal failure. Conjunctival suffusion is another helpful clue. Acute promyelocytic leukemia is notable for anemia, thrombocytopenia, and either elevated or decreased white blood cell count, all in the presence of disseminated intravascular coagulation. PNH is a rare disorder characterized by hemolytic anemia (particularly at night), venous thrombosis, and deficient hematopoiesis. It is a stem cell–derived intracorpuscular defect. Anemia is usually moderate in severity, and there is often concomitant granulocytopenia and thrombocytopenia. Venous thrombosis occurs much more commonly than in the population at large. The intraabdominal veins are often involved, and patients may present with Budd‐Chiari syndrome. Cerebral sinus thrombosis is a common cause of death in patients with PNH. The presence of pancytopenia and hemolysis should raise suspicion for this diagnosis, even before the development of a venous thrombosis. In the past PNH was diagnosed by abnormalities on the Ham or sucrose lysis test; however, currently flow cytometry analysis of glycosylphosphatidylinositol (GPI) linked proteins (such as CD55 and CD59) on red blood cells and granulocytes is recommended. Question # 4 Question A 36‐year‐old # African woman with systemic lupus erythematosus presents with the acute onset of lethargy and jaundice. On initial evaluation, she is tachycardic, hypotensive, appears pale, is dyspneic, and is somewhat difficult to arouse. Physical examination reveals splenomegaly. Her initial hemoglobin is 6 g/dL, white blood cell count is 6300/L, and platelets are 294,000/L. Her total bilirubin is 4 g/dL, reticulocyte count is 18%, and haptoglobin is not detectable. Renal function is normal, as is urinalysis. What would you expect on her peripheral blood smear? A. Macrocytosis and PMN's with hypersegmented nuclei B. Microspherocytes C. Schistocytes D. Sickle cells E. Target cells Answer : B ID: 1444 e19 Chapter: 129 Utility:6 Difficulty: High Pediatrics This patient's lupus and her rapid development of truly life‐threatening hemolytic anemia are both very suggestive of autoimmune Answer : hemolytic anemia. Diagnosis is made by a positive Coomb's test documenting antibodies to the red cell membrane, but smear will often show microspherocytes, indicative of the damage incurred to the red cells in the spleen. Schistocytes are typical for microangiopathic hemolytic anemias such as hemolytic‐uremic syndrome (HUS) or thrombocytopenic thrombotic purpura (TTP). The lack of thrombocytopenia makes these diagnoses considerably less plausible. Macrocytosis and PMN's with hypersegmented nuclei are very suggestive of vitamin B12 deficiency, which causes a more chronic, non‐life‐threatening anemia. Target cells are seen in liver disease and thalassemias. Sickle cell anemia is associated with aplastic crises, but she has no known diagnosis of sickle cell disease and is showing evidence of erythropoietin response based on the presence of elevated reticulocyte count. Question # 5 Question A 62‐year‐old # man undergoes a routine examination. He notes increasing fatigue of 8 months' duration but states he can perform his usual daily activities. He has no fever, night sweats, anorexia, or weight loss. The medical history is noncontributory, and he takes no medications. On physical examination, vital signs are normal. The spleen is palpable three finger breadths below the left midcostal margin. There is no lymphadenopathy or hepatomegaly. Laboratory studies indicate a hemoglobin level of 12.5 g/dL (125 g/L), a leukocyte count of 14,400/µL (14.4 × 109/L), and a platelet count of 148,000/µL (148 × 109/L). A peripheral blood smear is shown. The bone marrow cannot be aspirated, but the bone marrow biopsy reveals a hypercellular marrow with extensive fibrosis and abnormal‐appearing megakaryocytes. Results of conventional cytogenetic testing are normal. The JAK2 mutation assay is positive. Fluorescence in situ hybridization of the bone marrow for the (9;22) translocation is negative. Which of the following is the most appropriate management of this patient now? A. Allogeneic hematopoietic stem cell transplantation B. Danazol C. Hydroxyurea D. Imatinib E. Observation See Image Answer : E ID: Utility:8 Difficulty: Mod Pediatrics 2429 e19 Chapter: 131 Close observation, with palliative care as needed, is appropriate for patients with low‐risk primary myelofibrosis. The most appropriate Answer : management of this patient now is observation. This patient has primary myelofibrosis, which is a chronic myeloproliferative disorder characterized by overproduction of megakaryocytes and bone marrow stromal cell‐mediated collagen deposition. The peripheral blood smear shows marked leukoerythroblastic findings with tear drop‐shaped erythrocytes and megathrombocytes. The bone marrow aspirate is often “dry” (unsuccessful aspirate), and bone marrow biopsy shows marked fibrosis. This patient has low‐risk primary myelofibrosis (PMF) given the absence of high‐risk features such as age older than 65 years; fever, night sweats, and a weight loss of 10% or more; a hemoglobin concentration of less than 10 g/dL (100 g/L); a leukocyte count greater than 25,000/µL (25 × 109/L); and circulating blasts of 1% or more. As such, his median overall survival is 135 months or approximately 11 years. Given his favorable prognosis, he requires only observation for now. Allogeneic hematopoietic stem cell transplantation is potentially curative in patients with PMF but is associated with significant morbidity and mortality and would not be a good choice for a patient with low‐risk disease, but it could be considered if the disease progresses. Transplantation is the preferred treatment for younger patients with two or more adverse prognostic features. Danazol is used to treat PMF‐related anemia and leads to responses in 37% of patients with transfusion‐dependent anemia or a hemoglobin level less than 10 g/dL (100 g/L). This treatment is not indicated in this patient considering his hemoglobin level of 12.5 g/dL (125 g/L). Hydroxyurea would be a reasonable therapy if the patient had constitutional symptoms such as fever, weight loss, night sweats, symptomatic splenomegaly, or problematic thrombocytosis; however, this treatment is not required now. Imatinib is appropriate therapy in patients with chronic myeloid leukemia, but it is not effective in treating PMF. Bibliography Cervantes F, Dupriez B, Pereira A, et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for Myelofibrosis Research and Treatment. Blood. 2009;113(13):2895‐2901. PMID: 18988864 Question # 6 Question # girl presents to the emergency department with pallor and jaundice. Her mother states A 5‐year‐old that the girl was in her usual state of health until 3 days ago, when she began to have fever, cough, and decreased activity. On physical examination, her oral temperature is 37.5°C, pulse rate is 120 beats/min, respiratory rate is 24 breaths/min, and blood pressure is 100/60 mm Hg. The child is pale with icteric sclerae. Her breath sounds are normal, and there is no hepatosplenomegaly or lymphadenopathy. The remainder of the examination is normal. Laboratory test results reveal: ⦁ White blood cell count, 13,500/µL (13.5 × 109/L), with 40% polymorphonuclear leukocytes, 53% lymphocytes, 5% monocytes, and 2% eosinophils ⦁ Hemoglobin, 4.0 g/dL (40 g/L) ⦁ Mean corpuscular volume, 85/µm3 (85 fL) ⦁ Platelet count, 402 × 103/µL (402 × 109/L) ⦁ Reticulocyte count, 12% (0.12) Of the following, the MOST likely cause of this child’s anemia is: A. autoimmune hemolytic anemia B. congenital erythrocyte hypoplasia (Blackfan‐Diamond anemia) C. glucose‐6‐phosphate dehydrogenase deficiency D. parvovirus B19 infection E. transient erythroblastopenia of childhood Answer : A ID: Utility:7 Difficulty: Mod Pediatrics 2490 e19 Chapter: 129 Hemolysis:can be divided into intrinsic and extrinsic hemolytic anemias. Intrinsic hemolytic anemias are due to defects within the Answer erythrocyte that affect the red blood cell membrane, hemoglobin, or cytosolic components (enzymes). These defects include gene mutations and nutritional deficiencies, which can lead to abnormal production of heme, globin chains, membrane proteins, or intracellular enzymes. Examples of intrinsic hemolytic anemias are sickle cell disease (globin chain), thalassemia (globin chain), hereditary spherocytosis (membrane defect), and glucose‐6‐phosphate dehydrogenase deficiency (enzyme). Extrinsic hemolytic anemias are due to immunologic, chemical, or physical factors that damage the erythrocyte. Examples of extrinsic hemolytic anemias include autoimmune hemolytic anemia, hypersplenism, toxins, heat, disseminated intravascular coagulation (DIC), hemolytic‐uremic syndrome, and thrombotic thrombocytopenic purpura. In some cases, both intrinsic and extrinsic mechanisms may be involved. Pallor, jaundice, and reticulocytosis are typical features of hemolytic anemia. Reticulocytes are young erythrocytes released from the bone marrow. The reticulocyte count is useful in distinguishing between anemias of decreased production vs those of increased destruction. Normally, reticulocytes account for 1% to 2% of all circulating red blood cells. When erythrocytes have a shortened lifespan (eg, from hemolysis), the erythropoietin level increases, which stimulates the bone marrow to increase its production of erythrocyte precursors. The percentage of reticulocytes can increase significantly above the steady state of 1% to 2%, as seen in this vignette, where the child is found to have a reticulocyte count of 12%. The girl in the vignette most likely has autoimmune hemolytic anemia (AIHA). In infants and young children, AIHA usually occurs after an infection, whereas in adolescents it is more likely to be associated with an underlying systemic disease. A positive direct antiglobulin test result (also known as the direct Coombs test), indicating the presence of antibodies to the red blood cells, would also support the diagnosis of AIHA. Glucose‐6‐phosphate dehydrogenase deficiency is another cause of hemolytic anemia, but its X‐linked recessive inheritance pattern makes it unlikely in girls. In contrast to the anemias of increased destruction, the anemias of decreased production will typically present with a low or normal reticulocyte count. Iron deficiency is the most common cause of anemia in the world and is due to decreased formation of the heme component of hemoglobin. A low reticulocyte count and low mean corpuscular volume are seen in iron deficiency anemia, both of which are not found in the patient in this vignette. Low reticulocyte count would be seen in congenital erythroid hypoplastic anemia (Blackfan‐Diamond anemia), which usually presents in the first year of life, and transient erythroblastopenia of childhood, which usually presents between 6 months and 4 years of life. Parvovirus B19 preferentially infects the red blood cell precursors in the bone marrow, which can lead to a transient red blood cell aplasia. This condition does not cause a significant anemia in individuals with a normal erythrocyte life span. However, in patients who have chronic hemolytic conditions and rely on reticulocytosis to compensate for their anemia (as in patients with sickle cell disease or hereditary spherocytosis), infection with parvovirus B19 can lead to a severe aplastic crisis. CLINICAL PEARLS: • In infants and young children, autoimmune hemolytic anemia usually occurs after an infection, whereas in adolescents it is more likely to be associated with an underlying systemic disease. • The reticulocyte count is useful in distinguishing between anemias of decreased production vs those of increased destruction. • Pallor, jaundice, and reticulocytosis are typical features of hemolytic anemia. Question # 7 Question A 65‐year‐old # man is evaluated for a 2‐year history of daytime somnolence, snoring, and apneic episodes during the night as witnessed by his wife. He does not have blurred vision, tinnitus, or headache. He has no cardiopulmonary symptoms and does not smoke cigarettes. The patient has hypertension for which he takes lisinopril and atenolol. On physical examination, temperature is normal, blood pressure is 170/98 mm Hg, pulse rate is 72/min, and respiration rate is 18/min. BMI is 44. Oxygen saturation is 95% with the patient breathing ambient air and does not decrease with modest exertion. The patient's face is erythematous, and his neck is thick. Hepatosplenomegaly is absent. Laboratory studies: Hemoglobin 17.5 g/dL (175 g/L) Leukocyte count 5000/µL (5.0 × 109/L) Platelet count 225,000/µL (225 × 109/L) Erythropoietin 35 mU/mL (35 units/L) Which of the following is the most appropriate management? A. Initiate hydroxyurea B. Order sleep study C. Perform bone marrow biopsy D. Perform phlebotomy Answer : B Answer : ID: 2453 e19 Chapter: 131 Utility:7 Difficulty: Low Pediatrics Question # 8 Question A 35‐year‐old # woman is evaluated in the emergency department for the sudden onset of substernal chest pain, dyspnea, and syncope. Medical history is noncontributory. On physical examination, temperature is normal, blood pressure is 80/45 mm Hg, pulse rate is 55/min, and respiration rate is 22/min. Cardiac examination reveals an S3. Lungs are clear to auscultation. Splenomegaly is present. Laboratory studies: Hematocrit 37% Hemoglobin 12.5 g/dL (125 g/L) Leukocyte count 10,000/µL (10 × 109/L) with a normal differential Mean corpuscular volume 80 fL Platelet count 1,095,000/µL (1095 × 109/L) Troponins Elevated An electrocardiogram shows an ST elevation in leads II, III, and aVF. The peripheral blood smear shows increased platelet numbers and circulating megathrombocytes but is otherwise normal. Which of the following is the most likely cause of this patient's thrombocytosis? A. Chronic myeloid leukemia B. Essential thrombocythemia C. Iron deficiency D. Polycythemia vera Answer : B ID: Utility:7 Difficulty: Low Pediatrics 2480 e19 Chapter: 131 Extreme thrombocytosis involving platelet counts greater than 1 million/µL (1000 × 109/L) strongly suggests essential thrombocythemia. Answer : The most likely cause of this patient's thrombocytosis is essential thrombocythemia. Essential thrombocythemia is a myeloproliferative disorder characterized by an elevated platelet count in the absence of conditions known to cause secondary thrombocytosis. Other blood counts are typically normal. Twenty percent of those affected are younger than 40 years, and complications including arterial or venous thrombosis can occur in 20% to 30% of patients. Extreme thrombocytosis involving platelet counts greater than 1 million/µL (1000 × 109/L), as demonstrated in this patient strongly suggests essential thrombocythemia. When the platelet count increases to more than 1.5 million/µL (1500 × 109/L), patients can develop a qualitative functional defect analogous to type 2 von Willebrand disease. The peripheral blood smear typically shows circulating megathrombocytes, and a mild leukocytosis may be present. Approximately 40% to 50% of patients have splenomegaly, and about 20% have hepatomegaly. Patients may also have basophilia. The diagnosis of essential thrombocythemia is one of exclusion. A reactive thrombocytosis (such as iron deficiency, an underlying inflammatory disorder, or cancer) must be excluded. To establish the diagnosis, the platelet count must be greater than 600,000/µL (600 × 109/L) on two different occasions separated by at least 1 month, and bone marrow examination must show hypercellular marrow and morphologically abnormal megakaryocytic hyperplasia with the megakaryocytes in clusters. Approximately 50% of patients have the JAK2 mutation, which may be present in all of the myeloproliferative disorders. In patients with chronic myeloid leukemia, the median leukocyte count is approximately 100,000/µL (100 × 109/L), and the differential includes cells in various stages of maturation from myeloblasts to mature neutrophils. This patient has none of these findings. Iron deficiency is unlikely in this patient with a normal hemoglobin level and mean corpuscular volume. Polycythemia vera is excluded if the hematocrit is normal as it is in this patient. Bibliography Beer PA, Green AR. Pathogenesis and management of essential thrombocythemia. Hematology Am Soc Hematol Educ Program. 2009:621‐628. PMID: 20008247 Question # 9 Question A 56‐year‐old # man is evaluated in the emergency department for a 4‐week history of progressive fatigue, increased sleepiness, dyspnea on exertion, and chest pain with moderate activity. He also notes an inability to perform all his duties as a construction worker. Family and medical history are noncontributory, and he takes no medications. On physical examination, temperature is 36.7 °C (98.2 °F), blood pressure is 123/69 mm Hg, pulse rate is 98/min, and respiration rate is 16/min. The patient has scleral icterus and no lymphadenopathy. Abdominal examination discloses splenomegaly. Laboratory studies: Hemoglobin 8.1 g/dL (81 g/L) Leukocyte count 4900/µL (4.9 × 109/L) with a normal differential Platelet count 159,000/µL (159 × 109/L) Reticulocyte count 5.4% Direct Coombs (antiglobulin) test ‐ IgG, strongly positive; C3, weakly positive The complete blood count from 1 year ago was normal. The peripheral blood smear is shown. Which of the following is the most likely diagnosis? A. Cold agglutinin disease B. Glucose‐6‐phosphate dehydrogenase deficiency C. Hereditary spherocytosis D. Thrombotic thrombocytopenic purpura E. Warm autoimmune hemolytic anemia See Image Answer : E ID: 2464 e19 Chapter: 129 Utility:6 Difficulty: Mod Pediatrics Warm autoimmune hemolytic anemia is characterized by insidious symptoms of anemia, jaundice, splenomegaly, spherocytes on the Answer : peripheral blood smear, and direct Coombs (antiglobulin) test results that are strongly positive for IgG and negative or weakly positive for complement. The most likely diagnosis is warm autoimmune hemolytic anemia. Warm autoimmune hemolytic anemia is characterized by insidious symptoms of anemia, jaundice, splenomegaly, and a peripheral blood smear showing spherocytes, which are erythrocytes that have lost their central pallor. In addition, the direct Coombs (antiglobulin) test is frequently strongly positive for IgG and negative or weakly positive for complement. In cold agglutinin disease, the direct Coombs test is negative for IgG and positive for complement, reflecting the properties of the pathogenic IgM antibody. Although patients with glucose‐6‐phosphate dehydrogenase (G6PD) deficiency may have episodic hemolysis, the peripheral blood smear is more likely to show “bite cells,” which are characterized by eccentrically located hemoglobin confined to one side of the cell, rather than spherocytes. A positive direct Coombs test is not consistent with G6PD deficiency. Hereditary spherocytosis is characterized by a personal or family history of anemia, jaundice, splenomegaly, or gallstones; spherocytes on the peripheral blood smear; and negative direct Coombs test. The positive direct Coombs test, noncontributory personal and family medical history, and the patient's prior normal complete blood count help to differentiate warm autoimmune hemolytic anemia from hereditary spherocytosis, although the peripheral blood smear may be similar in both conditions. Patients with thrombotic thrombocytopenic purpura (TTP) have microangiopathic hemolytic anemia (schistocytes on the peripheral smear and an increased lactate dehydrogenase level) and thrombocytopenia. TTP is unlikely in this patient given the normal platelet count, positive direct Coombs test, and lack of schistocytes on the peripheral blood smear. Bibliography Packman CH. Hemolytic anemia due to warm autoantibodies. Blood Rev. 2008;22(1):17‐31. PMID: 17904259 Question # 10 Question # You are seeing a 2‐week‐old newborn in your office following discharge from the neonatal intensive care unit after treatment for indirect hyperbilirubinemia. The newborn was born at term after an unremarkable pregnancy, with prenatal screening notable for maternal blood type O positive and antibody negative. The newborn was jaundiced at less than 24 hours after birth. Evaluation at that time included blood type B positive and direct antiglobulin test positive. Intense phototherapy and intravenous immunoglobulin therapy was required, with the total bilirubin peaking at 18.2 mg/dL (311.3 µmol/L). At the time of hospital discharge, the hemoglobin was 12 g/dL (120 g/L), the total bilirubin was 10.2 mg/dL (174.5 µmol/L), and the direct bilirubin was 0.9 mg/dL (15.4 µmol/L). The mother asks if there are complications related to the jaundice that she needs to worry about. Of the following, the most likely complication to be seen in this infant is: A. Cholestatic liver disease B. Hearing loss C. Kernicterus D. Late anemia of infancy E. Malignant melanoma Answer : D ID: Utility:6 Difficulty: High Pediatrics 2492 e19 Chapter: 129 The newborn Answer : in this vignette has hemolytic disease of the fetus and newborn (HDFN) due to ABO incompatibility and is at increased risk of late anemia of infancy. Mothers with blood type O naturally have antibodies against A and B red blood cell (RBC) surface antigens. These antibodies are immunoglobulin G type and cross the placenta. Although 15% of pregnancies are at risk for ABO incompatibility, it occurs in only 4% of at risk newborns. Affected newborns commonly present with hyperbilirubinemia within the first 24 hours after birth that may progress to levels causing kernicterus if treatment is not initiated. Intensive phototherapy is the initial treatment for hyperbilirubinemia caused by HDFN. Affected newborns whose bilirubin values continue to rise in spite of optimized phototherapy or whose values are close to the exchange transfusion threshold may be treated with intravenous immunoglobulin (IVIG). Although the efficacy of IVIG has not been proven, IVIG is felt to block antibody receptors on RBCs and inhibit hemolysis. Double volume exchange transfusion is reserved for those newborns whose total serum bilirubin values reach the established threshold. Kernicterus and late anemia of infancy are the 2 major complications of HDFN. Early and effective management of hyperbilirubinemia can prevent the development of kernicterus. Late anemia of infancy is seen in the first month after birth and is attributed to continued destruction of the newborn’s RBCs by the circulating maternal immunoglobulin. Intrauterine or exchange transfusion may further exacerbate the anemia by suppressing erythropoiesis. At risk newborns should be monitored by serial hematocrit and reticulocyte counts after discharge from the hospital. Multiple dose treatment with IVIG has been suggested to decrease the ongoing hemolysis, decreasing the need for transfusion for late anemia of infancy. The newborn in this vignette is unlikely to have kernicterus, as the majority of cases in term newborns occur when the serum bilirubin values exceed 20 mg/dL (342.1 μmol/L). Infants with high bilirubin values have brainstem auditory evoked response abnormalities, but these adverse effects appear to reverse with treatment of the hyperbilirubinemia. Limited studies have not demonstrated any increased risk of skin cancer, including melanoma following treatment with phototherapy. Although up to 13% of infants with HDFN may develop cholestatic liver disease, it is independently associated with intrauterine RBC transfusion or Rhesus D alloimmunization. CLINICAL PEARLS: • Kernicterus and late anemia of infancy are the 2 major complications of hemolytic disease of the fetus and newborn. • The late anemia of infancy associated with hemolytic disease of the fetus and newborn is seen in the first month after birth and is attributed to continued destruction of the newborn’s red blood cells by the circulating maternal immunoglobulin.