Pharmacology
Introduction
Definitions
› Pharmacology:
–
The science of drugs, their composition,
uses, and effects, the characteristics or
properties of a drug
*Nurses need to have knowledge about the
actions and effects of medications
*To safely and accurately administer
medications, nurses need to have an
understanding of pharmacologic principles
Drug Names
› Chemical name
– Describes the drug’s chemical composition and molecular
structure
› Generic name (nonproprietary name)
– Name given by the United States Adopted Name Council
› Trade name (proprietary name)
– The drug has a registered trademark; use of the name
restricted by the drug’s patent owner (usually the
manufacturer)
Drug Names
**Nurses need to know both names, but should use the generic
name (May be more than one trade name, NCLEX uses generic
name)
Example:
Pharmacological Concepts: Classification
› Classification- Nurses learn to categorize meds
with similar characteristics by their class by:
Usage – why the drug is used
Body system – where the drug works
Chemical or pharmacological class – what the drug
is made of
Pharmacological Concepts: Classification
› Medication classification indicates the effect of the
med on the body system, the symptom the med
relieves, or the med’s desired effect (e.g. oral
hypoglycemic, beta-blockers)
› A medication may also be part of more than one
classification system
Example:
Aspirin is an analgesic, antipyretic, anti-inflammatory, and
anti-platelet agent
Pharmacological Concepts: Classification
When in doubt, look it up!
As a nurse, you are professionally, ethically, legally,
and personally responsible for every dose of
medication you administer.
Pharmacokinetics
› The processes of drug absorption,
drug distribution, drug metabolism,
and drug excretion
–Absorption
–Distribution
–Metabolism
–Excretion
***It’s important to understand the
difference between:
Pharmacokinetics-drug movement
Pharmacodynamics-drug action
Routes of Medication Administration
› Drugs are manufactured for a specific route of
administration and are absorbed at different rates
depending on the route of administration.
› Routes of administration
Oral- the drug is swallowed and absorbed from the
stomach or small intestine
Enteral- drug is given directly to the stomach or intestine
Sublingual – the drug is held under the tongue and
absorbed through the mucosa
Buccal/Transmucosal – medication is held against the
mucous membrane of the cheek until it dissolves
Routes of Medication Administration cont’d
Topical (skin) – drug acts locally and is absorbed though the
skin
Topical (Instillations) - The drug is placed into a body cavity
(e.g., urinary bladder, rectum, vagina, ears, nose, eye)
Topical (Inhalation) - A device (e.g., nebulizer, face mask)
**Some drugs are intended for local effects in the
respiratory passages; others (e.g., anesthetic gases) are for
systemic effects, especially in the brain
Parenteral - drug taken into the body other than through
the digestive system
Intravenous – medication directly to the vein – circulatory system
Intramuscular
Subcutaneous
Forms of Medications
› Medications are available in
a variety of forms and
preparations
› The form of the med will
determine its route of
administration
› Composition of med is
designed to enhance its
absorption & metabolism
› Many meds are available in
several forms
› Tablet
› Capsule
› Elixir
› Enteric-coated
› Suppository
› Suspension
› Parenteral
› Transdermal patch
Oral Medications
Advantages
Convenient
Sterility is not needed
Economical
Noninvasive, low-risk
procedure
Easy to administer, good for
self-administration
Capsule can mask
unpleasant taste
Capsule can be time
released
Disadvantages
Unpleasant taste may cause
non-compliance
May irritate the stomach
Patient must be conscious
Digestive juices may destroy
drug
Cannot use if the patient
have difficulty swallowing
May be harmful to teeth
How are drugs metabolized in the body?
› Metabolism (or biotransformation)
–is the chemical inactivation of a drug through its
conversion into a more water-soluble compound or
into metabolites that can be excreted from the body
–Once a medication reaches its site of action, it is
metabolized (changed into the inactive form) in
preparation for excretion
**Metabolism takes place in the liver
Why is it important to know that?
How Are Drugs Excreted From the Body?
› Kidneys - are the primary site of excretion
› Liver and GI Tract - some drugs broken down by the
liver are excreted into the GI tract and eliminated in
the feces
› Lungs – drugs are removed through exhalation
› Exocrine Glands - excretion through the exocrine
(sweat and salivary) glands is limited
Definitions, Cont’d…
› Biological Half-Life:
– The time required for half the quantity of a drug or other
substance deposited in a living organism to be metabolized
or eliminated by normal biological processes
–the time required for something to fall to half its
original value
Example:
Tramadol a narcotic-like pain reliever, has a half-life of
approximately 6 hours. This means if you take a 50-mg
dose at 0800, by 1400 half of that dose (25 mg) will still be
left in your body. In 12 hours, one-fourth of the initial dose
(12.5 mg) will be left in your body
Onset, Peak, Duration
› Onset
– The time it takes for the drug to elicit a therapeutic
response
› Peak
– The time it takes for a drug to reach its maximum
therapeutic response
› Duration
– The time a drug concentration is sufficient to elicit a
therapeutic response
FIGURE 26-4
Pharmacodynamics:
The study of actions and/or effects of
the drug in living organisms
› Drug-induced alterations to normal
physiologic function
› Positive change:
– Therapeutic effect or goal of therapy
› Negative change:
– Side effects
– Adverse effects
Pharmacodynamics
› Mechanism of Action
› Therapeutic Effect
› Side Effects
› Adverse Effects
› Toxic Effect
› Idiosyncratic Reactions
› Allergic Reaction
› Medication Interactions
› Iatrogenic Response
Mechanism of Action
› In pharmacology, the term mechanism of action (MOA)
refers to the specific biochemical interaction through
which a drug substance produces its pharmacological
effect
› A mechanism of action usually includes mention of the
specific molecular targets to which the drug binds, such
as an enzyme or receptor
› Example: Furosemide MOA
– Furosemide works by blocking the absorption of sodium,
chloride, and water from the filtered fluid in the kidney
tubules, causing a profound increase in the output of urine
(diuresis)
Therapeutic Effect
› The expected or predictable physiological response a
medication causes
› A single med can have several therapeutic effects (Aspirin)
› It is important for the nurse to know why med is being
prescribed
– What do we want to happen?
– What do we expect to see?
– How will we know it worked?
› Not just recognizing the action but seeing evidence of the goal
› Furosemide will relieve symptoms of CHF through its action,
and we will see this therapeutic effect in decreased respiratory
difficulty (rate and effort) and reduction of pulmonary crackles
Side Effects
› Unintended secondary effects a medication predictably
will cause
› May be harmless or serious
› If side effects are serious enough to negate the
beneficial effect of meds therapeutic action, it may be
dicontinued
› People may stop taking medications because of the side
effects
› Furosemide SE: frequent urination, hypokalemia,
hypovolemia, hypotension
Adverse Effects
› Undesirable response of a medication
› Unexpected effects of drug not related to therapeutic
effect
› Should be reported to FDA – file an Adverse Drug
Reaction (ADR) report
› Can be a side effect or a harmful effect
› Can be categorized as pharmacologic, idiosyncratic,
hypersensitivity, or drug interaction
› Furosemide can lead to hearing loss, erythema
multiforme major (Steven Johnson Syndrome)
Steven-Johnson Syndrome
› Black Box Warning:
– A warning that appears in the
instructions for use surrounded
by a thick black box to alert
medical professionals to serious
life-threatening adverse effects
associated with the drug’s usage.
› Toxic effect may develop after prolonged intake or
when a med accumulates in the blood because of
impaired metabolism or excretion, or excessive
amount taken
– Toxic levels of opioids can cause respiratory depression
– Antidotes available to reverse effects
› Allergic reaction
– Unpredictable response to a medication
– Makes up greater than 10% of all medication reactions
– Client may become sensitized immunologically to the initial
dose, repeated administration causes an allergic response
to the med, chemical preservative or a metabolite
Allergic Reaction
› Medication acts as an
antigen triggering the
release of the body’s
antibodies
– May be mild or severe
› Among the different classes
of meds, antibiotics and
opiates cause the highest
incidence of allergic reaction
› Anaphylaxis
› Drug rash
› Etc.
Other Drug Reactions: Definitions
› Teratogenic-Structural effect in unborn fetus
(thalidomide)
› Carcinogenic-Causes cancer
› Drug interactions-occurs when one med modifies the
action of another
– Common in people taking several medications at once
– One med may potentiate or diminish the action of another
or alter the way it is absorbed, metabolized or eliminated
– Warfarin and Amiodarone
Other Drug Reactions: Definitions
› Idiosyncratic Reactions - is an unexpected, abnormal,
or peculiar response to a medication. It may take the
form of the following responses to a drug:
Extreme sensitivity
Lack of response
A paradoxical (opposite of expected) response, such as
agitation in response to a sedative
› Iatrogenic-unintentional adverse effects that occur
during therapy
– Treatment-Induced Dermatologic-rash, hives, acne
– Renal Damage-Aminoglycoside antibiotics, NSAIDS, contrast
medium
– Blood Dyscrasias- Destruction of blood cells (Chemotherapy)
– Hepatic Toxicity-Elevated liver enzymes (hepatitis-like
symptoms)
› Synergistic-Effect of 2 meds combined is greater than
the meds given separately
– Alcohol & Antihistamines, antidepressants, barbiturates,
narcotics
– Not always undesirable, physician may combine meds to
create an interaction that will have beneficial effects
(Vasodilators & diuretics to control high BP)
› Incompatibility:
› Undesirable interaction between drugs not
suited to be administered together
› Drug Tolerance:
–Requirement of larger doses to be consumed in
order to obtain desired effects; decreased drug
effect occurring after repeated drug administration
› Drug Resistance:
– Lack of responsiveness to administered medication
› Drug Tolerance:
–Ability of the body to alter its
response (adapt) to drug effects so
that effects are minimized over time
more drugs are needed to achieve
the same therapeutic level
› Drug Resistance:
– Lack of responsiveness to
administered medication
› Incompatibility:
– Undesirable interaction between
drugs not suited to be administered
together
Definitions, Cont’d…
› Loading Dose:
– Initial drug dose administered to
achieve rapid therapeutic drug
concentrations
› Maintenance Dose:
– dose needed to maintain
therapeutic blood levels;
maintain blood levels in the
therapeutic range
› Polypharmacy:
– situation where patients are
taking multiple medications for
the same condition
› Often prescribed by different
specialist
› Common in the elderly
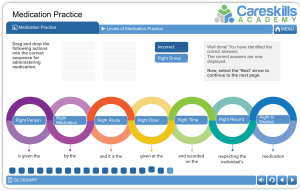
Rights of Medication Administration
1. Right Patient
2. Right Medication
3. Right Dose
4. Right Route
5. Right Time
6. Right Documentation
Medication Rights
Right patient
– Check the name on the order and the patient. Use 2
identifiers. Ask patient to identify himself/herself
– When available, use technology (for example, bar-code
system)
Right medication
– Check the medication label. Check the order
Right dose
– Confirm the appropriateness of the dose using a current drug
reference
– If necessary, calculate the dose and have another nurse
calculate the dose as well
Medication Rights
Right route
– Again, check the order and appropriateness of the route
ordered
– Confirm that the patient can take or receive the medication by
the ordered route
Right time
– Check the frequency of the ordered medication
– Double-check that you are giving the ordered dose at the
correct time
– Confirm when the last dose was given
Medication Rights
Right documentation
– Document administration AFTER giving the ordered
medication
– Chart the time, route, and any other specific information as
necessary. For example, the site of an injection or any
laboratory value or vital sign that needed to be checked
before giving the drug.
Other “Rights”
Right reason
– Confirm the rationale for the ordered medication. What is
the patient’s history? Why is he/she taking this medication?
– Revisit the reasons for long-term medication use
Right response
– Make sure that the drug leads to the desired effect. If an
antihypertensive was given, has his/her blood pressure
improved? Does the patient verbalize improvement in
depression while on an antidepressant?
– Be sure to document your monitoring of the patient and
any other nursing interventions that are applicable
Other “Rights”
› System Analysis
– The entire system of medication management needs a
constant “double-check”
– Ordering, dispensing, preparing, administering,
documenting
– Involves the physician, nurse, nursing unit, pharmacy
department, and patient education
› Close consideration of special situations
› Prevention and reporting of medication errors
› Refusal of medication
› Patient teaching
Patient Safety
Preventing Medication Errors
› Minimize verbal or telephone orders
– Readback and verify
› Avoid medical shorthand, including abbreviations and
acronyms
– Abbreviation – “Do not use list”
Preventing Medication Errors
› Never assume anything about items not specified in a
drug order (i.e., route)
› NEVER use “trailing zeros” with medication orders
– Do not use 1.0 mg; use 1 mg. 1.0 mg could be misread as 10
mg, resulting in a tenfold dose increase
› ALWAYS use a “leading zero” for decimal dosages
› Do not use .25 mg; use 0.25 mg
– .25 mg may be misread as 25 mg. “.25” is sometimes called
a “naked decimal”
 0
0