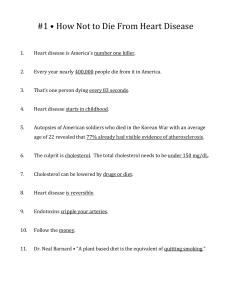
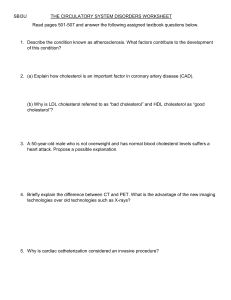
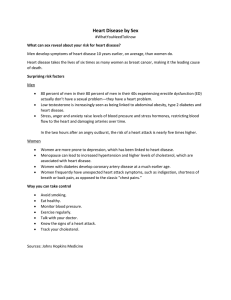
Cholesterol Production in Obesity By TATU A. MIETTINEN, M.D. SUMIMARY Sterol-balance studies were performed in 10 control subjects, 10 normolipidemic ol)ese patieints, and 10 hypertriglyceridemic (type IV, mostly obese) patients on a low-cholesterol solid-food diet. Fecal elimination of cholesterol was markedly elevated in the overweight patients and tended to be high in the hypertriglyceridemic subjects also. A signiificant correlation wx as found between body weight and fecal excretion of neutral, acidic, and total steroids, inidicating that the greater the body wveight the higher was the rate of cholesterol synthesis. Sterol-balance data in obese subjects showed that excess daily cholesterol production roughly amounted to 20 mg/kg of adipose tissue. The control subjects produced only 12 mg/kg of body weight daily. Thus, obesity is associated with an increased rate of cholesterol synthesis in man. However, the correlationi between serum cholesterol concentration and cholesterol production was low, suggesting that the overall rate of cholesterol synthesis was not the only factor determining the serum cholesterol level. That enhanced cholesterol production is not an irreversible phenomenon in obese subjects was indicated by the normalization of sterol-balance values in three overweight patients after their weights had been reduced by total fast folloved by a low-calorie diet. Additional Indexing Words: Hypercholesterolemia Hypertriglycerider Sterol balance Downloaded from http://ahajournals.org by on December 10, 2023 YPERCHOLESTEROLEMIA is frequently found in patients with obesity, so that the average serum cholesterol level is significantly higher in overweight subjects than in lean ones, and usually a significant correlation exists between serum cholesterol and obesity.1 2 It should be borne in mind, however, that a great many obese patients have normal serum lipid concentrations.3 Hypercholesterolemia4 5 and obesity6 are known to be associated with the development of ischemic heart disease, although the association is relatively weak in the case of obesity, according to recent studies.7 It therefore seemed worthwhile to study the Fecal steroids Bile acids cholesterol metabolism of obese patients in greater detail, the sterol-balance technique being used for determination of cholesterol synthesis. Kinetic analysis of serum cholesterol after administration of radioactive cholesterol has disclosed a positive correlation between cholesterol production and excess body weight.8 Results of the preliminary studies9' 10 and those reported here clearly demonstrate that obesity enhances cholesterol synthesis very potently and that reduction of weight effectively normalizes cholesterol production. Material and Methods Sterol balance was measured in three groups of patients, for whom clinical data are presented in table 1. The control group consisted partly of volunteers from among the laboratory personnel and partly of hospital patients with no detectable metabolic or other active disease. The obese group consisted of 10 markedly overweight patients, most of whom were hospitalized for reduction of weight. Although at the time of admission to the hospital some of the patients had From the Third Department of Medicine, University of Helsinki, Finland. This study has been carried out under contract with the Association of Finnish Life Assurance Companies. Address for reprints: Tatu A. Miettinen, M.D., Third Department of Medicine, University of Helsinki, Helsinki 29, Finland. Received November 18, 1970; revision accepted for publication July 19, 1971. 842 Circulation, Volume XLIV, November 1971 CHOLESTEROL PRODUCTION IN OBESITY 843 0 a) _ Lt 0 0 0 C: C2C 0 0 CC o tE r CC Cl C CC - -4 1- o :O n0 c cvC Ln cc ,0 C,] M C"] M - i - -4 -4 I- .c r-H 0 Cl CM o1 o 0 CC 0 oo 0 c 0 O I> 0 1C CD 0 c Cl Cl Cl l Cq -f A.,m e C' CC clt 0 0 0C * o S 0c o0 -C COcc Cl 1 CD W a; cl C cl] CM .z t. LC m cl Cl - LC ri rCl0 C' Cl m1 0 t- Cl oe .EC CC _41 00 C 0 X 0 CC X 0 XC 0 cCC CO Cl Cl Cl CC Cl CC Cl Cl C:5 Cl cc ~0C0C0 0 I c -C. Ul o m C1o cl "2 -41 CC 0 CO CO -H 6 Cc -rC s CO C Coo s Cl n - ~ CO0 Cl Cc 0o Cl 0 c _- 0o CCCC0x -sCl C-4 m C ClO c cc C~) Cl Cl CO G0 CID t. .- cc .' .- cc CO-Cl _-o 0 H 0 C-C. o o -H n X r--c, -I --I Downloaded from http://ahajournals.org by on December 10, 2023 c . ro 0o~ 0C ccO---CL-ifo 0 ° l0 4 QC M i 0 CCC mx SdqC nC .0 CC0CO0b-Z.- CC'-CC ICCO .2-.CCICC.CCLCC ICCCC ._ 0) +20 w12 . CO O O . ._ _ ._ ce 4 )0 d -. C.C 0 -. +. Q C.) C.) 0 C.) +. +2 . . .ZZ. ZI. C.) 0 . 0** w2 9-. "Z W *- --S . _ 02 0) .2 o bC. w2 ._ 02 M ~~~ -e2 0 SD> c3 ed - 3 X g S X X V ¢- V = V 1 V V I) - ClOC ClCl ClClClClClCl g ._ ._ C~) 0h O V: C) W = V 6 V 1-4 Cl CC S IC co t- Cc 000 - -C cl t-Cc O0 00 O CCCC Cl Circulation, Volume XLIV, November 1971 MIETTINEN (844 Downloaded from http://ahajournals.org by on December 10, 2023 slightly elevated serum clholesterol and/or triglycerides, the serum lipid values were within normal liimiits during the period of fecal collections. In this group excess body weight (calculated as the difference between the actual and ideal'1 weights) ranged from 15 to 80 kg and relative weight (absolute weight/ideal weight) from 1.21 to 2.42. Diabetes (controlled by diet) or diabetic glucose tolerance was found in six of the patients, twvo of whom had gallstones and two had clinical and electrocardiographic signs of coronary beart disease; one patient (no. 19) of the latter group had heart failure, which required relatively large doses of digitalis and diuretics for compensation. The third group contained 10 patients in whom hvpertriglyceridemia was conspicuous and whose lipoprotein pattern was consistent with type IV hyperlipoproteinemia according to the classification of Fredrickson et al.,12 although in some of them hypercholesterolemia and f3-lipoprotein bands in lipoprotein electrophoresis were also relatively marked. The excess body weight in this group ranged from -1 to 42 kg and the relative body weight from 0.98 to 1.60. Two of the patients had cutaneous xanthomatosis, six had clinical and electrocardiographic signs of ischemic heart disease but no heart failure, and seven exhibited diabetic glucose tolerance. All of the subjects were placed on a lowcholesterol solid-food diet, and chromic oxide (Cr203) and /3-sitosterol were given so that the respective corrections for fecal flow and degradation of cholesterol during intestinal transit13 could be made. From one to three 3-day stool collections were made for each subject after 5-10 days on the diet, Cr203, and /3-sitosterol. Analysis of the diet showed that the average cholesterol content was 120 mg/2400 kcal. In patients 12, 14, and 19 the study was repeated after the weights had fallen, in response to total fast followed by a low-calorie diet, by 38, 13, and 68 kg, respectively. In view of the times for which the new stable weights had been maintained (12, 1, and 6 months after weight reduction had been achieved), it was assumed that a new metabolic steady state had already been attained. Serum cholesterol was measured according to the method of Pearson and associates14 and triglycerides by the method of Carlson.15 Dietary sterols and fecal acidic and neutral steroids were measured by the thin-layer chromatographic gasliquid chromatographic method.16 17 In one case, recovery of administered and dietary /8-sitosterol in the feces was only 70%, and neutral steroid excretion was therefore corrected for the recovery of /3-sitosterol. In the others, the values for recovery ranged from 94 to 108%, suggesting that no sterol degradation had occurred.13 Therefore, in these cases the results were expressed in relation to Cr,O3, which was determined according to Bolin and associates.'8 Sterol balance, which in the steady state is equal to cholesterol synthesis, was obtained as the difference between fecal steroids derived from cholesterol and dietary cholesterol. Because weight reduction with a low-calorie diet was found to lead to decreased fecal steroid excretion in obese subjects,19 the amount of calories was rigidly adjusted to maintain the body weight constant. None of the subjects studied actually showed any significant change in weight during the experimental period of 14-19 days, at the end of which the fecal collections were performed. This indicates that a steady state with respect to calories had been achieved. Cholesterol intake varied little during the study, ranging, according to analyses, from 98 to 136 mg/2400 keal; serum cholesterol was constant during the experimental period; and fecal steroid analyses of 2-3 consecutive collections in each subject (for one control and one hypertriglyceridemic patient only a single collection was available) showed constant excretion. The latter was indicated by the finding that the difference between the total fecal steroids of the first and third (or second) collection did not differ significantly from zero (- 21 -+ 30 mg/day). The same was true of acidic and neutral steroids, indicating that cholesterol elimination from the body as bile acids and as cholesterol itself was stable. It is therefore reasonable to infer that the subjects of the three groups were in a comparable metabolic steady state.20 On the assumption that at their ideal body weights the obese and hypertriglyceridemic patients would synthesize cholesterol at the rate observed in the controls, their theoretical, ideal sterol balance was calculated by multiplying the ideal weight by the average sterol-balance value of the controls, expressed as milligrams per day per kilogram of body weight. Excess sterol balance, corresponding to excess cholesterol synthesis, was the difference between the actual and ideal values for sterol balance. Results Table 2 shows that in the obese patients fecal excretion of acidic, neutral, and total steroids (derived from cholesterol) is markedly higher than in the controls or even in the hypertriglyceridemic patients. The differences between the two latter groups were insignificant, although the actual (but not ideal) body weights were markedly higher in the hypertriglyceridemic group than in the controls. The sterol-balance values indicate that in the obese Circulation, Volume XLIV, November 1971 CHOLESTEROL PRODUCTION IN OBESITY 845 .00=00 0 t- 10 0 0 1- 10 0 00 10 0 t'- 0~ _- C td CD c;C I- P- o;C0i6P--H, P. -vt- 0 0 Cle C -H 4-- C -i -l - ;l6c9~cl Cd C7; n~ OCS i ---_4 -r------- 0o - ClI 1 I - I I I I I _ c0 I 6.0 0C* t-. 1- -14- ++ -1-- - - l - M o ' I II + r-l cl N 0 0 0 I 0j I 02 a) 0 .0 -1Ci) ~~~~~~--4 n C C9 s CS -~00 ;5 C'4z l 0c 0c 1- Cl l 00 10 >- cm 0 - 0 0Y_ C MO t- 14 N f-4 0H0 10 CO 10 -°00 r . -0 r-4 -- -- 0) Cr -4 00 t- 0 c0 00 C 0 00 000m 0 o =t- 0 c0 cc 0 cc cc 0 ntl -0m I- mr 1-4 Rt P- 00- -4 F4 10f0- o 10 m t- Io M -4 m t- 1- 1000 X 1 -HC I1 n 00000 - m CO cl Cl 10 I I_ cc 010 tr C) .3 10 Cl 0 -d X 0 In 0 C,l r-00 COm 0 - CO - O>10~ 'd cl 0O - 0 . - . P- cc0C00 0 c,l t- Cl 00 Cl --- Cq - - t>c C0 C_ _0 CO - - - ---I 0 .0 - 0 1- c0 LfO + C0 cl b t '- d; c; 0 - -4_1"~". _~ - m C9 - CO Cl i0 r.. -- >. _ _0 cc z._ 0 bD It 0001 o 0 zCO z CO 0000 r-CO mCl_q c <CD m -)m n _1i 10s 00 t- - 0: Cl 10 d n n ce X n I> CS dt 1] 11 dd1 0D 4 1: 0 - Cl 10 - .. O> Cl - d - t- t-~'' 6 lld CO :le ce~O= = Ci.~ = t- - C)i 6 tIl cO . - Cl M N m 00 n -0 CO0 _~ Od CZ 1H CO. 0 - -- O *C*C*C*C*C*C n dq < CO 0~ CO -(Cl , 0- CO CO CO 0: Cl C0 ---1 Cl d OO - ~ - eD zo-C- C'; Cl 0.. l0 *<=0 c0 02 02C~_ C3 od 0 Downloaded from http://ahajournals.org by on December 10, 2023 dS 0 H- 0t cl C- C7t -t- rf c - C5>i ,d4C't Cl'000 Ict~C'mC ~ :1C ~~~'-Cl m-0 00 = C C 0 -H ii ~- ' 00 0 - 0 to- 00 10 Cl 0D 0 CO n 0n 0-00 m t- to- - - (oo 00 00 0. O M Q0 X to r- cc) t- C< 00 0 CX C COO L0 000 -~ 0. -0 cc 0000 C- C- _ P-4 __4 P..) 0 0 C-- a) 00 Cl 0 10Cl C- 00 Cl C- - 10 10 CO 0 ~~ z 40 CO 00 < 00v0 S 00 d O- 00 004 C-H t- c cc0000 00 0" 0 Co 0C c CO -o000 -n 0o C-l 000 c0 C- CO CO 00 X 0 0 Co Xs CS100 LO m z c- X X C: " 0 c m l:t me m --4 ---4 --P-41.Cn c 002* *02 ._ -4-- -4-- ++ 0n 1- X 0 - - 0,02 02 m1 _ O 00 Cl c0c- c "400 02.b 00 -4. 00 -f- 0 Cl Cl 000 02 .0 ¢0 0 .~~~~~~~~ 0 CO - CO CO z 0 - CO 00 Cl 0 -_C_ Cl > Cl CO o~~~~~~~~~0-C C- < C- 10 COC - c= CO _ N 01 0 Oce d4 0010 X m CS "4 CO C ClCO c0 mO - d 0-0 X 4CCO -0 m: -0000 C C l 00 0 0 0 CD C - - cl C- cl cc - C) Cl 0_- Im Tt -O CS ]C Cl~0 O 10 Ci l ;0 CII 0 --- CS 0 0 0 1.- 0. _a 00 CO 02 0 c3) m -H) cs c3) c3 CO CDaH c3e cc 0~53 0n - c3 CO Cl CO CO3 OO- 202021 U2 -I l Cl Id 0z C- 0) z Circulation, Volume XLIV, Novefraber 1971 - Cl g1 WO 1 CD p; e3 ,p _ 1 ~ ~ clq c 00 " rW CX cq N N cs cq N N m COCO r-i MIETTINEN 846 - 10 r=0.68 x * 1.3 0 0 o * de 0.8 2- xo X o X @ NEUTRAL 0.3 e22 0.9 o X -J U.) r=0.64 0.5 X cD d' X . Jdx0 0. x Ld Lii o ACIDIC x x 0.1 o Q2 X 0 2.0 r-0.80 -~~~~~~~~ 2.0 * x~( x o 1.2 1. - x x 0' o o xx TOTAL 0.42 2 40 , 60 , 80 100 120 140 kg BODY WEIGHT Downloaded from http://ahajournals.org by on December 10, 2023 Figure 1 Relationship of body weight to fecc I1 neutral steroids (upper panel), bile acids (middle panel), and total steroids (sum of neutral and acidifc steroids; lower panel) in control subjects and in patjients with obesity and hypertriglyceridemia. 9 = feim ile controls; 8 male controls; x hypertriglycerideimic patients; a obese female patients; o = obese nuaile patients. cholesterol synthesis was twice as high, and in the hypertriglyceridemiic subjects 1.3 times as high, as in the cont rols. Since the average relative weights of th e three groups were 1.69, 1.27, and 0.96, and s ince their ideal weights were the same, it can be concluded that obesity, particularly witlhout hyperlipidemia, effectively stimulates ctolesterol synthesis in man. Figure 1 shows the positiive correlations between body weight and the fecal excretion of neutral, acidic, and total steroids. The controls exhibited a significant correlation for all parameters, the lighter females having lower acidic- and total-steroid XTalues, and lessgroup negative sterol-balance values than the heavier males. However, the sex difference, which was not seen in the obese patients because of the similar weight of the two sexes, disappeared when fecal-steroid values were expressed per kilogram of body weight, although even then the bile acid output was slightly lower in the women than in the men (table 2). The association between fecal steroids and body weight tended to be less significant in the hypertriglyceridemic than in the obese subjects, because, particularly in one markedly obese and hypertriglyceridemic patient, cholesterol elimination, both as bile acids and as neutral steroids, happened to be relatively low. Sterol balance, when expressed per kilogram of body weight, was no longer significantly higher in the obese (- 14.9 ± 0.8 mg) than in the hypertriglyceridemic (13.0 + 1.1 mg) or control subjects (-12.4 + 1.0 mg). The positive correlation (r - 0.64) between excess body weight and excess sterol balance (fig. 2) indicates that cholesterol synthesis is enhanced over a wide range of obesity. The average increment of cholesterol synthesis per kilogram of adipose tissue was calculated for the obese subjects by dividing the excess sterol balance by the excess body weight. It was found to be 20 + 2 mg/kg/day, which again demonstrates the effectiveness of adipose tissue in enhancing cholesterol production in man, cholesterol synthesis in the control subjects being only 12 mg/kg/day. However, the correlation between serum cholesterol and sterol balance or excess balance (fig. 3) did not reach a significant level in this small series, which indicates that the serum cholesterol concentration is not determined solely by the overall rate of cholesterol synthesis. Neither body weight, excess weight, nor relative weight of the obese group was correlated significantly with the serum cholesterol concentration. From table 3 it is seen that in three excessively obese subjects reduction of weight to near-normal values led to a marked decrease in the elimination of fecal cholesterol from the body. This indicates that the Circulation, Volume XLIV, November 1971 CHOLESTEROL PRODUCTION IN OBESITY 0 .+1.2 0 4 xN. 0 0 L z o 4.+0.8 0 0 4. m) U) 0 0 wnW.0 0 c)wO -1 0 0 0 ~~~~~~r=0.65 0 ~~.0~~ 0 _ni U., -5 0 +80 +4 0 +6 0 +2 0 EXCESS BODY WEIGHT, kg Figure 2 Relationship between excess body weight and excess sterol balance in patients with obesity (o) and hypertriglyceridemia (-). abnormally high cholesterol synthesis occurring in obese subjects can be normalized by effective weight reduction. Discussion Downloaded from http://ahajournals.org by on December 10, 2023 The results of the present study show that cholesterol synthesis is normally proportional to body size, obesity being especially potent in EXCESS BALANCE g/DAY E Body weight Collection period (days) 119.8 120.3 119.8 0-3 4-6 7-9 Mean 0-3 4-6 7-9 Mean (kg) 82.1 81.9 82.2 * r=0.60 CD C) Table 3 Effect of Weight Reduction on Fecal Steroid Excretion in Three Obese Subfects 111.7 112.2 0 r= 0.54 300 stimulating this process. Thus, the marked difference in cholesterol synthesis found between the male and female control subjects disappeared when the values were expressed per kilogram of body weight. No sex difference was seen in the obese patients, among whom the body weight happened to be similar in males and females (fig. 1). The fact that in our earlier series21 no difference (expressed in relation to total body weight) was found between men and women turned out, on retrospective study, to be due to the similar body weights in the two groups. Only a few sterol-balance studies made with accurate methods on human subjects have -1.2 -0.7I -0.2 847 250 99.4 98.9 99.2 * O * 0 E 152.0 152.5 151.9 @000 200p 00 0 0 0 150L 0 00 -2.0 -1.5 BALANCE,g /DAY Figure 3 Relationship of the serum cholesterol concentration to sterol balance (o) and excess sterol balance (-) in obese subjects. Correlation coefficients (r = 0.54 and 0.60) did not reach a statistically significant level. .0 -1. Cii.culation, Volume XLIV, November 1971 84.1 84.1 83.9 84.1 Fecal steroids (mg/day) Acidic Neutral Total* Patient no. 12 395 362 383 380 242 346 267 285 Patient no. 14 0-3 282 4-6 238 Mean 260 0-3 172 4-6 148 7-9 220 Mean 180 Patient no. 19 0-3 1045 4-6 892 931 7-9 Mean 9a6 0-3 452 422 4-6 7-9 429 10-12 497 Mean 475 1420 1.532 1369 1440 825 903 704 810 1815 1894 1752 1820 1067 1249 961 1095 1258 1398 1328 1162 1099 1281 1159 1540 1636 1588 1334 1247 1438 1339 802 918 863 861 578 664 1847 1810 1794 1817 1030 1086 984 1164 1090 555 663 615 *Three determinations of dietary cholesterol on each body weight showed that the average intake had fallen significantly between the two studies in cases 12 and 19 (31 and 49 mg/day, respectively) and insignificantly (14 mg/day) in case 14. 848 Downloaded from http://ahajournals.org by on December 10, 2023 been reported so far. Effects of dietary fats on fecal steroid excretion were studied by Connor and associates in six normocholesterolemic prisoners." The mean sterol-balance values for two control periods on a cholesterol-free liquid-formula diet (fat consisted of cocoa butter), one before and the other after a cornoil diet, were -783 and -682 mg/day (neutral steroids corrected for losses of ,B-sitosterol), respectively. Despite marked differences in the diet, the figures are in good agreement with the control value of the present study (777 mg/day). The data did not appear to be correlated with body weight. Grundy and Ahrens`0 23 reported sterol-balance data on formula diets varying in cholesterol, plant sterol, and fat composition, for 15 hypercholesterolemic (type II, types as described by Fredrickson and associates'2 ), one normocholesterolemic, and four hypertriglyceridemic (three type V and one type IV) subjects. The sterol balance ranged from -374 to -749 mg/day for hypercholesterolemic subjects and from -726 to -1833 mg/ day for hyperglyceridemic subjects on a formula diet containing saturated fat; the data appeared to bear some relationship to body weight. In 43 patients with familial hypercholesterolemia, sterol balance, fecal neutral steroids, and bile acids were found to be correlated with body weight.9 As in the present investigation, some but not all of the hyperglyceridemic patients exhibited a high bile acid production in the studies by Grundy and Ahrens20° 23 and by Kottke .24 In the latter series bile acid metabolism was measured isotopically, and a marked interindividual heterogeneity in bile acid production was observed. Monkey adipose tissue synthesizes cholesterol in vitro at a rate25 that would account for the increment revealed by sterol-balance data in the obese subjects studied here. However, more recent studies have indicated that human and rat adipocytes are not able to convert labeled glucose or acetate into cholesterol, and that adipose tissue is only a cholesterolstorage organ that receives its cholesterol from circulating lipoproteins or chylomicron.26 The MIETTINEN liver and intestinal mucosa,27 on the other hand, have been shown to be the sites where serum cholesterol is primarily synthesized, which suggests that these organs are responsible for the augmented production of cholesterol in obesity. Studies with a labeled acetate-mevalonate mixture also indicated that synthesis was markedly enhanced in obese patients and that this stimulation took place between acetate and mevalonate.10 Furthermore, the rapid appearance of newly synthesized radioactive cholesterol in the serum suggested that it originated from a rapidly equilibrating cholesterol pool ( s), supposedly situated primarily in the liver and intestinal wall.27 Hypertriglyceridemic (type IV) subjects, who are usually obese and whose cholesterol synthesis in the present study was only moderately increased, have been shown by Salen et al.28 to have a high rate of intestinal cholesterol synthesis. The latter was minimal in hypercholesterolemic (type II) patients, but it was markedly stimulated by interruption of the enterohepatic circulation of bile acids with cholestyramine; clofibrate inhibited synthesis in the cholestyramine-treated hypercholesterolemic patients and in a case with hypertriglyceridemia. The cholesterol ester turnover is also higher in obese subjects than in lean ones and is significantly correlated not only with body weight but also with serum cholesterol and triglyceride concentrations.29 3 Nestel et al.,8 using the two-pool model for calculation of cholesterol metabolism, showed that cholesterol production, which bears no correlation to serum cholesterol, is increased by 22 mg/day/kg of excess body weight. This is in good agreement with the value of 20 mg/day/kg obtained in the present study by drect measurement of the fecal end products of cholesterol metabolism. Primarily enhanced elimination of cholesterol from the body, resulting, for instance, from treatment with cholestyramine or from an ileal bypass operation,,3Y is almost always accompanied by a reduced level of serum cholesterol. The magnitude of the latter is not correlated with the increment of fecal Circulation, Volume XLIV, November 1971 CHOLESTEROL PRODUCTION IN OBESITY Downloaded from http://ahajournals.org by on December 10, 2023 elimination, owing to a compensatory increase in the synthesis and possibly in the mobilization of tissue cholesterol.31 32 On the other hand, primarily enhanced synthesis, such as obviously occurs in obesity, can be assumed to increase the serum cholesterol level in almost every case, although the magnitude of the increase is not necessarily correlated with the enhancement of synthesis, because simultaneous stimulation of cholesterol elimination prevents this augmentation to an extent which differs from one subject to another. This compensatory increase of elimination is enough to keep the serum cholesterol level low in some obese patients, while in others elimination may be more or less defective, so that hypercholesterolemia results. Thus, the latter may accompany both reduced and enhanced synthesis; in familial hypercholesterolemia the primary disorder appears to be defective elimination of cholesterol, this being secondarily associated with a compensatory decrease in cholesterol synthesis;9' 10, 21 in obesity it is synthesis that is primarily enhanced, but in some cases augmentation of elimination is not proportionate and hypercholesterolemia results. The variable response of elimination to enhanced cholesterol synthesis in obesity may explain why the serum cholesterol level usually shows only a weak correlation with body weight or body fatness.1' 2 However, since obesity is frequent in modern society, it may, as a potent factor enhancing cholesterol synthesis, be a very important etiologic factor in hypercholesterolemia and hence in ischemic heart disease, even though, according to the more-recent epidemiologic studies,7 the association between the latter and obesity is relatively weak. Weight reduction was accompanied with a marked decrease in cholesterol synthesis in -the limited number of subjects studied. This therapeutic measure, so commonly recommended for prevention and treatment of hypercholesterolemia and ischemic heart disease, seems to be a very effective procedure as far as reduction of cholesterol synthesis is concerned. Weight reduction has actually been reported to Circulation, Volume XLIV, Novemnber 1971 849 decrease the serum choiesterol level in obese subjects,34 although in the new steady state initial values may be resumed.35 References 1. TANNER JM: The relation between serum cholesterol and physique in healthy young men. J Physiol 115: 371, 1951 2. MONTOYE HJ, EPSTEIN FH, KJELsBERG MO: Relationship between serum cholesterol and body fatness. Amer J Clin Nutr 18: 397, 1966 3. LEwis LA, OLMSTED F, PAGE IH, LAWRY EY, MANN GV, STARE FJ, HANIG M, LAUFFER MA, GORDON T, MOORE FE: Serum lipid levels in normal persons: Findings of a cooperative study of lipoproteins and atherosclerosis. Circulation 16: 227, 1957 4. KANNEL WB, KAGAN A, DAWBER TR, REVOTSKIE N: Epidemiology of coronary heart disease: Implications for the practicing physician. Geriatrics 17: 675, 1962 5. EPSTEIN FH, FRANCIs T JR, HAYNER NS, JOHNSON BC, KJELSBERG MO, NAPIER JA, OSTRANDER LD JR, PAYNE NW, DODGE HJ: 6. 7. 8. 9. 10. Prevalence of chronic diseases and distribution of selected physiologic variables in a total community, Tecumseh, Michigan. Amer J Epidem 81: 307, 1965 KANNEL WB, LEBAUER EJ, DAWBER TR, McNAMARA PM: Relation of body weight to development of coronary heart disease. Circulation 35: 734, 1967 KEYS A, editor: Coronary heart disease in seven countries. Circulation 41 (suppl I): 1970 NESTEL PJ, WHYTE HM, GOODMAN DEWS: Distribution and turnover of cholesterol in humans. J Clin Invest 48- 982, 1969 MIETTINEN TA: Sterol balance in hypercholesterolemia (abstr). Scand J Clin Lab Invest 24 (suppl 110): 48, 1969 MIETTINEN TA: Enhanced cholesterol metabolism in obesity (abstr). Scand J Clin Lab Invest 25 (suppl 113): 28, 1970 11. Metropolitan Life Insurance Company Statistical Bulletin 40: Nov-Dec, 1959 12. FREDRICKSON DS, LEVY RI, LEES RS: Fat transport in lipoproteins-An integrated approach to mechanisms and disorders. New Eng J Med 276: 34, 94, 148, 215, 273, 1967 13. GRUNDY SM, AHRENS EH JR, SALEN G: Dietary ,B-sitosterol as an internal standard to correct for cholesterol losses in sterol balance studies. J Lipid Res 9: 374, 1968 14. PEARSON S, STERN S, MCGAWACK TH: A rapid, accurate method for the determination of total cholesterol in serum. Anal Chem 25: 813, 1953 850 Downloaded from http://ahajournals.org by on December 10, 2023 15. CARLSON LA: Determination of serum triglycerides. J Atheroscler Res 3: 334, 1963 16. GRUNDY SM, AHRENS EH JR, MIETTINEN TA: Quantitative isolation and gas-liquid chromatographic analysis of fecal bile acids. J Lipid Res 6: 397, 1965 17. MIETTINEN TA, AHRENS EH JR, GRUNDY SM: Quantitative isolation and gas-liquid chromatographic analysis of dietary and fecal neutral steroids. J Lipid Res 6: 411, 1965 18. BOLIN DW, KING RP, KLOSTERMAN EW: A simplified method for the determination of chromic oxide (Cr203) when used as an index substance. Science 116: 634, 1952 19. MIETTINEN TA: Fecal steroid excretion during weight reduction in obese patients with hyperlipidemia. Clin Chim Acta 19: 341, 1968 20. GRUNDY SM, AHRENS EH JR: Measurements of cholesterol turnover, synthesis, and absorption in man, carried out by isotope kinetic and sterol balance methods. J Lipid Res 10: 91, 1969 21. MIETrINEN TA, PELKONEN R, NIKKILX EA, HEINONEN 0: Low excretion of fecal bile acids in a family with hypercholesterolemia. Acta Med Scand 182: 645, 1967 22. CONNOR WE, WITIAK DT, STONE DB, ARMSTRONG ML: Cholesterol balance and fecal neutral steroid and bile acid excretion in normal men fed dietary fats of different fatty acid composition. J Clin Invest 48: 1363, 1969 23. GRUNDY SM, AHRENS EH JR: The effects of unsaturated dietary fats on absorption, excretion, synthesis and distribution of cholesterol in man. J Clin Invest 49: 1135, 1970 24. KOTTKE BA: Differences in bile acid excretion: Primary hypercholesterolemia compared to combined hypercholesterolemia and hypertriglyceridemia. Circulation 40: 13, 1969 25. DIETSCHY JM, WILSON JD: Cholesterol synthesis in the squirrel monkey: Relative rates of synthesis in various tissues and mechanisms of control. J Clin Invest 47: 166, 1968 MIETTINEN 26. ANGEL A, FARKAS J: Cholesterol storage in white adipose tissue (abstr). Circulation 42 (suppl III): III-1, 1970 27. DIErsCHY JM, WILSON JD: Regulation of cholesterol metabolism. New Eng J Med 282: 1128, 1179, 1241, 1970 28. SALEN G, AHRENS EH JR, GRUNDY SM: Regulation of intestinal synthesis of cholesterol in patients with hyperlipidemia (abstr). J Clin Invest 49: 84a, 1970 29. NESTEL PJ, MONGER EA: Turnover of plasma esterified cholesterol in normocholesterolemic and hypercholesterolemic subjects and its relation to body build. J Clin Invest 46: 967, 1967 30. NESTEL PJ: Turnover of plasma esterified cholesterol: Influence of dietary fat and carbohydrate and relation to plasma lipids and body weight. Clin Sci 38: 593, 1970 31. MIETTINEN TA: Effect of cholestyramine on fecal steroid excretion and cholesterol synthesis in patients with hypercholesterolemia. In Proceedings of the Second International Symposium on Atherosclerosis, edited by R Jones. Heidelberg, Springer-Verlag, 1970, p 558 32. MIETTINEN TA: Drugs affecting bile acid and cholesterol excretion. In Proceedings of the Second International Symposium on Atherosclerosis, edited by R Jones. Heidelberg, SpringerVerlag, 1970, p 508 33. MOORE RB, FRANTZ ID, BUCHWALD H: Changes in cholesterol pool size, turnover rate and fecal bile acid and sterol excretion after partial ileal bypass in hypercholesterolemic patients. Surgery 65: 98, 1969 34. GALBRAITH WB, CONNOR WE, STONE DB: Serum lipid changes in obese subjects given reducing diets of varied cholesterol content. Clin Res 12: 352, 1964 35. DRENICK EJ: Starvation in the management of obesity. In Obesity, edited by NL Wilson. Philadelphia, F. A. Davis Co., 1969, p 191 Circulation, Volume XLIV, November 1971