Manipulative Therapy in Rehabilitation Locomotor System 3rd Edition
advertisement

Copyrighted Material
Copyrighted Material
Copyrighted Material
Copyrighted Material
Copyrighted Material
Dedicated to my wife
Butterworth-Heincmann
L i n a c r e H o u s e , J o r d a n Hill, Oxford O X 2 8 D P
225 W i l d w o o d A v e n u e , W o b u r n , M A 0180-2041
A division of R e e d E d u c a t i o n a l and Professional Publishing Ltd
A m e m b e r of the R e e d Elsevier pic g r o u p
All rights r e s e r v e d . No p a r t of this publication m a y be r e p r o d u c e d in
any m a t e r i a l form (including p h o t o c o p y i n g or storing in any m e d i u m by
e l e c t r o n i c m e a n s a n d w h e t h e r o r n o t transiently o r incidentally t o s o m e
o t h e r use of this p u b l i c a t i o n ) without t h e written p e r m i s s i o n
of t h e copyright h o l d e r except in a c c o r d a n c e with the provisions of the Copyright,
D e s i g n s a n d P a t e n t s A c t 1988 or u n d e r the t e r m s of a licence issued by t h e
C o p y r i g h t Licensing A g e n c y L t d , 9 0 T o t t e n h a m C o u r t R o a d , L o n d o n ,
E n g l a n d W 1 P 9 H E . A p p l i c a t i o n s for t h e copyright h o l d e r ' s w r i t t e n
p e r m i s s i o n to r e p r o d u c e any part of this publication s h o u l d be a d d r e s s e d to t h e publishers
First published 1985
R e p r i n t e d 1987, 1988
Second edition 1991
R e p r i n t e d 1996, 1997
T h i r d edition 1999
© R e e d E d u c a t i o n a l and Professional Publishing Ltd 1999
Line drawings: © G e r d a Istler 1985
P h o t o g r a p h s : © Jaroslav Cmi'ral 1985
British Library Cataloguing in Publication Data
A catalogue record for this b o o k is available from t h e British Library
Library of Congress Cataloguing in Publication Data
A catalogue r e c o r d for this b o o k is available from the Library of Congress
ISBN 0 7506 2964 9
P r i n t e d and b o u n d in G r e a t Britain
Copyrighted Material
Copyrighted Material
Copyrighted Material
Copyrighted Material
Copyrighted Material
1
Introduction
Pain - especi al ly in the locomotor system - is
man k ind
suffered.
It
a
curse
been
control is
b ased
largely on reflex action, precise
the
information about wbere, how and w hy we should
commonest reason for his calls for hel p , answered
app ly one or the other method may be very useful
has always
of diverse treatments . To
and give us better insight into the various method s ,
the ortbodox the cure. it seems, can often be 'left to
as well as more reliable p ractica l results. As these
by a bewildering
m ul t itude
has
nature', sometimes assisted by rest in bed and the
methods are most
mixed blessing of pharmacotherapy, but there are
conditions, it may be useful to begin with the reflex
frequently applied in painful
many other methods (all si n cerely held by some to
response to nociceptive (painful) stimulation.
be singularly effe ctiv e ) that belong mainly, although
Any localized painful stimulation will act in the
not exclusively, to the realm of physical therapy.
segment to which the stimulated structure belongs.
These
In this segment there is usually a byperalgesic zone
include
local
anaesthesia
and
needling,
massage, electrotherapy, manipulation, local cold or
in the skin, muscle spasm (trigger point TrP), painf u l
hot applications, more recently the laser and the
periosteal points, movement restriction of the spinal
magnet, remedial exercise, hypnother a py, counter­
segment
irritative poultices and even leeches. All of these are
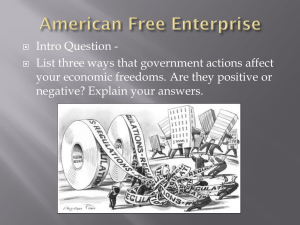
visceral organ (Figure
used for mor e or less the sa me type of disorder, and
both of recogni z i ng clinically which of these changes
and
(perhaps)
some
1.1).
dysfunction
of
a
Th.is provides a means
we may ask if any one of them should be prefe rred ,
is present and of using some of the methods avail­
especial ly since in practi ce we very often find that
able either upon the skin, the musc les (periosteal
the therapist uses the method he or she knows best.
points), the spinal segment or the visceral organ
The common feature of all these methods is that
involved. We may also try to find out which of these
they act reflexly, that is they act on sensory recep­
structures is the source of the painful stimulus, in
tors - usually in the region where the pain is felt or.
which structure the changes are more intense, and
even better, where it originates - to produce a reflex
so on.
re s p onse . They may thus be te rme d 'methods of
However, these reflex changes are not confined to
reflex therapy'. Assuming the reflex nature of the
a single segment. A vis ceral disturbance is accom­
action of this type of treatment, we may then ask
panied by viscerovisceral reflexes: for example, pain
which receptors are acted up on and w hic h structures
in the region of the gall bladder causes anorexia;
are
subserved
by
those
rec e p tors.
As
nervous
pain in the region of the h eart ,
viscus
t
I
I
I
I
I
skin
I
.- -------------------------
Figure 1.1 Reflex relalions within the segment
Copyrighted Material
a
sense of oppression,
Copyrighted Material
1l1froduclion
3
lively by post-isometric relaxation, by warmtll or by
atic fashion and, as we would do when making
infiltration. Periosteal points may be reached by soft
neurological examination, start at the peripheral
a
tissue techniques, deep massage, by needling, or, if
level and work up to the central, applying treatment
they are the insertion points of muscles, by post­
according to our findings,
isometric relaxation of the muscle. The most suitable
At times, however, the results fall far below what
treatment for joint or spinal segment movement
we might expect from our premises. One of the chief
restriction is manipulation: that for disturbed motor
reasons why this happens in this type of therapy is
patterns is remedial exercise.
the
presence
of a lesion
which
causes
intense
Furthermore, we must decide which of the affected
nociceptive stimulation and so dominates the clinical
structures is the most important and which less so;
picture without the patient being aware of it. The
which is likely to be primary and which secondary.
German literature uses the term
The severity of the change may be significant. Even
of disturbance. This is frequently an old scar after
Siorungsj(!ld,
focus
at the segmental level, however, there is a sort of
injury or operation, often a tonsillectomy scar. This
hierarchy: there may be a primary visceral disorder
focus-scar is usually tender on examination, with
and there may be blockage of a spinal segment.
pain spots, and surrounded by a hyperalgesic zone.
Changes in muscle can be secondary and in the skin
If the 'normal' therapy fails, the existence of such a
this is the rule. But in the locomotor system itself,
scar acting like a 'saboteur' must be considered;
and in the spinal column, there are regions of greater
treatment by local anaesthesia or simply by needling
and of lesser importance, regions in which
primary
the pain spots or stretching the scar tissue by soft­
lesion occurs more readily than in others. It is vital
tissue techniques can be most rewarding. Another
a
to recognize those faulty central motor patterns
reason for poor results in patients treated for pain
which, if significant, will cause relapses at the peri­
may be undiagnosed masked depression, which must
phery. In this connection psychological factors play
then be treated as such.
a major part, as motor patterns are to a certain
degree expressions of the state of mind: anxiety,
Disturbed
function of the
locomotor
system,
together with the reflex changes it produces, may
depression and an inability to relax will greatly
aptly be called the 'functional pathology of the loco­
influence motor patterns: no less important is the
motor system'. [n this connection the unfortunate
subject's psychological attitude to pain, as it is the
but frequent use of the term
most frequent symptom in our patients.
synonym or euphemism for 'psychological' is most
'functional'
as a
In addition to the importance of the changes
regrettable - it implies a grave underestimation of
diagnosed, there is also a practical or technical
the importance of function and changes of function
aspect to be considered, as not all of the methods
consequent on pathological changes. In rehabilita­
used are equally effective or 'economical'. Thus
tion we are primarily concerned with the restoration
needling of a periosteal pain spot (or infiltration) is
of impaired function even in those conditions where
usually more economical than periosteal massage
there is underlying structural pathology, This is
(deep friction), but wherever possible it is prefer­
understandable because structural lesions neces­
able to use post-isometric relaxation of the muscle
sarily produce disturbances of function. Indeed, so
(if the periosteal point is a point of muscle insertion)
fundamental is the distinction between morphological
soft tissue techniques because they are painless
lesions and function, that it can aptly be compared
or
and the patient can usually be taught to do it him­
to that between computer hard- and software.
self. The attractiveness of manipulation techniques
The greatest obstacle to the practical application
lies mainly in the fact that they are effective and not
of these apparently simple principles is a general
time consuming.
lack of clinical understanding of functional disorders
We can see from this that the choice of treatment
of the locomotor system or even of their reflex
is very broad. We can decide which to use by
manifestations, which are, in fact, the most typical
diagnosing each lesion in turn, and from this make
clinical manifestations of pain. The lesions that are
calls the palhogenelische
the most frequent, as well as being the object of
Alwwiiliilsdiagnose, the diagnosis of the lesion that
what
Gutmann
(1975)
manipulative therapy, are those affecting the spinal
is the most important link in the chain of pathology
column; the term vertebrogenic lesion is often used
at a given moment. We must do this, otherwise we
to describe them, but this is now believed to be not
may, for example, apply a method which acts on skin
quite
receptors when there are no signs of a hyperalgesic
include
zone, act on a muscle when there is no change in
spondylitis, osteoporosis, tumours, etc., while our
appropriate:
such
vertebrogenic
pathological
states
disorders
as
also
ankylosing
tension, manipulate a spinal segment with normal
main concern is with disturbed function. However,
mobility,
function is not confined to the spinal column but in­
or give
remedial
exercise
for
normal
movement patterns. Such very varied methods of
volves muscles, nervous control and very frequently
treatment should be applied only after full clinical
the extremities. It is therefore more appropriate to
examination and analysis, and with careful testing of
speak of disturbed function of the locomotor system,
the results of treatment. We must act in a system-
rather than of vertebrogenic disturbance.
Copyrighted Material
4
Manipulative
Therapy in Rehabilitation of the Locomotor System
What is the present place of reflex therapy? This
question is as difficult to answer as the question of
should be applied to all other methods of reflex
therapy.
the place of pharmacotherapy. Whereas pharmaco­
therapy has developed into an exact and sophisti­
cated science, methods of reflex (physical) therapy
History
have for the most part remained empirical, with
largely overlapping and even chaotic indications.
It might be as well to say something of the history
From what has already been said it is possible to
of manipulative therapy in order to explain the
formulate
anomalous position it holds in p resent-day medicine.
one
important principle:
we
do
not
prescribe treatment for a particular disease, but for
I will also consider its prospects and take the oppor­
those changes that are of pathogenic significance in
tunity to warn against some of the worst pitfalls.
the dis e a se. If, for example, headache is due to
It seems that some forms of manipulative therapy
muscular tension alone, then muscular relaxation by
are as old as the history of mankind, and it was, and
whatever may be the most effective method is the
is to this day, part of folk healing in Europe and
correct treatment. However, if this muscular tension
elsewhere. However, it is noteworthy that the father
is due to blockage of a motor segment of the cervi­
of European medicine, Hippocrates, saw 'rhachio­
cal spine, manipulation will be more suitable; if
therapy' as one of the cornerstones of medicine, on
faulty posture is the cause, remedial exercise may
a par with surgery and drug the r a py. According to
be the answer. However, the great advantages of
Waerland (1950), Hippocrates repeatedly pointed
this type of therapy over pharmacotherapy are that
out the imporlance of knowing all about tbe spinal
(I) the mainly physiological methods used cause a
(2)
column, since so many disorders are related to it.
minimum of side-effects if properly applied, and
Hippocrates is quoted as saying that manipulation
as most methods of reflex therapy act immediately,
of the spinal column was an old art, and that he
their effectiveness can be checked at once.
thought highly of those who first discovered its
It is worth saying a few words here about the role
importance and who would follow him in furthering
of pharmacotherapy in those lesions that mainly
the art of natural healing. Writing about articula­
affect the functioning of the locomotor system. It
tions, Hippocrates described 'pararthremata " similar
would be difficult to conceive of a drug that could
to slight dislocation or subluxation, in which the
restore a specific motor function, but drugs may alle­
vertebrae are only slightly shifted, and went on to
viate spasm, influence pain and damp down some of
say that the 'eyes and hands of the experienced
the reflex reactions involved, and thus facilitate the
physician should not miss anything which could be
restoration of function. Additionally, they are of
helpful in adjusting the shifted vertebra without
course necessary for the treatment of depression and
harming the patient .
anxiety symptoms.
. if treatment is performed
lege artis, the patient can come to no harm'.
.
There are numerous relief carvings and other
To sum up, neither the clinical diagnosis nor our
findings in themselves suffice as the basis for decid­
illustrations
ing the most appropriate therapy. O nly an analysis
traction as performed in classical antiquity (see
showing
manipulative
therapy
and
of pathogenesis enables us to determine the lesion
Frontispiece). The patient was usually prone on a
that is the most important at a given moment. After
specially constructed table while traction was applied
treatment the patient must be re-examined to gauge
to both the head and the feet. The physician then
any immediate effect, and from this we can see at
dealt with a specific vertebra. Galen, too, knew that
once whether our hypothesis about the pathology
nerves originated from the spinal column and could
was correct and can adjust treatment accordingly.
be
If treatment has been effective, then at the next
description of his treatment of the philosopher
examination
the
picture
should
have
changed
and again we have to determine which lesion has
damaged
Pausanius.
at
this site,
as we see
from
the
But while treatment with herbs dev­
eloped into modern pharmacotherapy, and surgery
become the most important. Thus therapy is never
became
a monotonous routine; at the same time it is always
manipulation remained unchanged throughout the
the
In
field
of
specialized
practitioners,
verifiable, which encourages the therapist to take an
centuries.
objective scientific approach.
manipulations was a 'bonesetter': in France he was
Manipulative th e ra p y which is one of the most
,
England
the
layman
performing
'Ie raboteur'.
effective and important of tbe various methods of
The first important school teaching manipulation
reflex therapy, is concerned with impaired function
on a professional basis in modern times was the
of the locomotor system. Because we can define its
osteopathic school founded by Andrew Sti ll
purpose (treatment of blockage) it serves to show
1828): he served as a surgeon in the American Civil
(born
that methods of reflex therapy are more effective it
War and then worked as a general practitioner. He
we know exactly on which type of lesion they act,
founded his school in Kirksville in 1897, and trained
and that they are improperly used if this is not
lay manipulators.
known. This is fundamental to our approach, and it
lasted for 2 year s
Copyrighted Material
Initially, courses at the school
,
but
later the curriculum was
IntroduClion
sCllools,
extended to 4 years,
and is now the same
study in
time
university faculties
osteopathic schools were private institutions,
in
recent years Colleges of Osteopathic Medicine have
been established at some American universities, the
less, for some
5
generation of
willlI1g to co-
chiropractors not
have been
operate with the
encouraged to refer patients to specialists when
advisable.
Chiropractic
colleges now
teach
and
undertake research on a modern scientific basis, are
first being that of the Michigan State University at
consistently overcoming their cherished ideology,
these colleges give full medical training and gradu­
ates are recognized in most of the states of the USA
system considering themselves specialists of the
istration; this entitles them to carry on medical
practice.
pharmacotherapy
East Lansing. In addition to osteopathic techniques,
as DO (doctor of osteopathy) by the state admin­
Soon after S till founded
grocer
(D. D.
practic'.
Palmer)
Born in
and limit their activities to problems of the locomotor
'neuro-musculo-skeletal system'.
The fact that chiropractors are taught neither
greater adherence
manipUlation is
nor
wrote that it was a
they also prescnbe
and use soft-tiSSUe
indeed - only a
chiropractors arc,
were trained. At first
being set up in
dollars! By 1911 courses lasted I year, and now
schools
also
give
students a 4-year course of training.
their
There are to this day some differences between
osteopaths and chiropractors. The former have full
medical training plus manipulation training, and are
entitled to work not only as general practitioners but
also as gynaecologists, surgeons, eye specialists, etc.
In this way they have become part of the medical
profession and the
little,
if at all, to manipulal
are
who remain faithful
something of an elite
physthrust
icians. They rely much
techniques
in
much
so that
than
certainly rely mOle
lI:ik"
chiropractic
results
by osteopaths.
College of Chiropraclic
American
surgery
day,
than
tech II iques,
preferring mobilization
active (,muscle energy')
sophisticated, they
form the most active and numerous body of manip­
ulating physicians.
The development of modern medicine in Europe,
in particular, has shown that an uncompromisingly
negative attitude to manipulation is not shared by
the whole of the medical profession. The discovery
of the mechanical role of disc prolapse in root
syndromes made doctors aware of the possibilities
of traction and even of other methods of mechanical
treatment, including
somewhat paradoxical
the osteopaths and
by the medical prolession
ing sophisticated
doctors began to
lation, even employing
It is no coincidence
a common
aim or denominator: to obtain myotascial release.
men who
devoted themselves La the an at malllpuiation were
profession has been crossed only gradually. To quote
Naegeli, who used very effective traction manipula­
The rift between chiropractic and the medical
a typical example: ' Chiropractic flourishes where
ignorance
prevails.
Chiropractic
will
Europeans. One of the first was a Swiss doctor,
tion on the cervical spine, which was particularly
disappear
effective in the treatment of headache. His book
and common sense. Testimonials are but hypnotic
lished 1954, 1979) makes good reading to this day.
because its time has come. Chiropractic defies logic
multiples of zero in an empty vacuum .. .' (Angrist,
1973).
Today chiropractors.
which he also
is in a way
nor surgery. In fact,
Cyriax, whose
American Medical
iated Medical Societies
IIh:mbcrs to
cooperate with
chiro-
'llIegal
practors took the rnatte I
conspiracy', and won their case
III
! 01::;:; the AMA is
now obliged by law to allow cooperation between
chiropractors.
The most important pioneer of medical manipula­
tion, however. was J. A. MennelJ (1952, 1964), an
outspoken protagolJlsl
curriculum enabling I
their students are
doctors and
Nervenleiden lind Nervenschmerzen (1903, repub­
It should be
noted,
however, that in the past the chiropractors themselves
showed little interest in such cooperation. Neverthe-
techniques
physloti1aapists. It
his
disciple
Medicine
(1977,1978) remains
assessment of molOl
decessor in
This gap was
also graduated in medicine and whose Manual of
Osteopathic Technique remains the classic in its field
(Stoddard, 1961). The London Coll ege of Osteo­
pathy (now the London Co.I.lege of Osteopathic
Medicine) was the first institution where osteopathic
Copyrighted Material
6
i?chohlill£iliol1 of
Manipulative
qualified
techniques
originally
the Locomotor System
doctors,
of this College
have plaYfil
obvious reasons a rift
Poland
medicine, or between
an
of manipulattve medicine throughout Europe and
school of thought, was
not likely to develop in all exclusively State-run
prominent. Working under De Seze he succeeded in
tbe interest of some members of his staff at the
medical practitioners (mainly specialists in physical
system, and in the potential of 'unconventional'
the development
particularly in France, where Maigne is the most
giving courses in manipulation at the Medical
Faculty of the University of Paris, attended by
medicine) but not by physiotherapists.
At the same time, i.e. shortly after 1945, a group of
German doctors became interested in manipulation,
mainly under
!\merican-trained
chiropractors
SCllldberg). Unlike
Maigne,
doctors in private
service.
Neurological.
broad field of
Professor
Henner
rehabilitation
of
encouraged
the locomotor
methods, among them manipulation. Svehla, Obrda,
Stary, Miratsky, Jirout and the present author, and
later Janda and Vele, worked on these lines. Here
the
of the most prominent
country, and it is in
the Czech Republic
were
team-work in research in
manipulation
doctors): the MWE
economy of manipu­
Extremitalcntherllpie]
bv Sell and the FAC
practice;
groups
medical
III
mg and teaching
formed wl1h
[(Gesellscilal!)
(Forschungs
Wlrbelsaulen-
und
und Arbcitsgemeinschaft fOr Chiro­
therapie) with Biedermann, Cramer, Gutmann and
H.-D. Wolff.
Unlike
France and Great Britain,
where courses for doctors lasted months or even a
year. in Germany doctors were given weekly courses
at intervals, arranged in a series of at first 4 and later
8 separate weeks. With this system it has been
progress.
Ministry
curriculurn ot the lll�tllutes of Postgraduate Train­
ning which run refresher courses tor specialists in all
fields of medicine. Doctors are thus trained in each
of the fields, the 'teachers' receiving additional
preparation. Teaching began in Czechoslovakia in
1961, and on the same lines in East Germany in
1965 (three courses of 2 weeks each, at 6-month
possible to teach manipulation techniques to far
intervals).
Austria, Holland
ment of
more doctors in Germany, and also in Switzerland,
into hundreds.
united to
Medicine,
heir numbers run
German groups
There is another striking feature of the develop-
with rehabilitation of
particular with techniques
developed
on high-velocity thrusts
gentler osteopathic
aroused a
being overCClmc,
mcdicine in Czechoslovakia -
As';(xlation of Manual
simpler chiropractic
have been formed
outside the
predominant
the Czechoslova k
incorporate it in the
which is only slowly
1113ny counlries of Western
improved
muscular
were in turn greatly
addition of neuro-
Europe important groups of medical men have
inhibition techniques, it
became obvious that team-work by qualified doctors
performed by
cal necessity for maximum effectiveness. Therefore.
promoted the idea that manipulation should be
exception of
qualified doctors only.
Maigne in France they
With
the
bave not,
however, succeeded in adding manipulative tech­
niques to the medical curriculum at universities and
teaching hospitals. They thus belong to what we may
call 'unofficial' trends in medicine;
remains rather
support of
(NonnenbruclL
Schuler and 01
of the univt:r'dl
outside
some of the
manipulation
'outsider's' method, despite the
German professors
together with trained physiotherapists was a practi­
with the exception of high-velocity thrusts, manipu­
lative techniques are now being taught ever more
widely to physiotherapists who work with doctors.
During the 1980s great interest in mal1!pulative
therapy also appeared in the former Soviet Union.
ZUCk,c!lwc:rdt, Junghanns,
Collea:'l1es frol11 Czechos!mJkia. the GDR and
Bulgall<'l
ilild systematic training
has belen
cities under the aegis
qualify in courses
held there in 1986 and
reluctant attitude
remunerated
companies.
institutions. Symposia on
for
medicine in
coulltries has followed
different lines. The first country where manipulation
was Llsed and taught on a large scale was Czecho­
slovakia, where the model that was created has since
been adopted by former East Germany, Bulgaria,
1991.
ne, doctors in differ­
began
interested in manipulation
first international meet­
ing took place in Switzerland in 1958. At the next
meeting, in Nice in 1962, it was decided to form an
international body; this came about in 1965. when
the I nternational Federation of Manual Medicine
Copyrighted Material
Copyrighted Material
2
Theoretical· considerations
Morphological aspects
It is, however. the very abundance of what are
called 'degenerative changes' that makes it difficult
Chapter 1 showed clearly that manipulation and
to
most of the methods of reflex therapy are used in a
changes
vast number of cases of pain in the locomotor
particular, occurs most often between the fourth and
define
their
relation
increase
with
to
age,
pain.
but
Degenerative
back
pain,
in
system, including back pain, even though the cause
sixth decade, to become less common in old age. Not
and therefore the therapy remain controversial. For
only do we find subjects
a long time these pains were generally considered to
showing considerable degenerative changes: a person
in perfect health but
be of inflammatory origin, for the simple reason that
with these changes and severe pain may recover
this aetiology could best explain the main symptom,
completely from the latter, whereas his degenerative
the pain itself.
For the same reason they were
changes continue to increase with advancing age. On
sometimes called 'rheumatic pains'. The many terms
the other hand, there can be severe pain symptoms
ending in '-itis' bear witness to this attitude (spondy­
in young patients with no degenerative changes at
litis, arthritis, radiculitis. neuritis, fibrositis, myositis,
all. Even more important, the significance of what
panniculitis, etc.) as does 'soft-tissue rheumatism'.
are known as degenerative changes appears to be
However, as inflammation is a well-defined patho­
very ill defined. On the one hand there are destruct­
ive lesions in extremity joints, e.g. coxarthrosis and
logical condition, it has to be proved, or disproved,
by the objective methods of pathological anatomy,
gonarthrosis, the great clinical significance of which
and
the
nobody will doubt. On the other hand there are
inflammation theory: it had to be abandoned for lack
changes that probably correspond to what may
of evidence.
be called inevitable 'wear and tear'; then again
this
in
the
long
run
was
fatal
for
Pathological anatomy and 'pathology in vivo' (X­
there may be merely a compensatory process, or
rays) generously compensated clinicians for the loss
adaptation, as in scoliosis and hypermobility.
of this simple theory by demonstrating in abundance
spondylolisthesis
what are called 'degenerative changes'. Instead of
spinal column better stability than an orthopaedic
a
In
large osteophyte may give the
terms ending in '-itis' we were then offered spondy­
operation. Changes resulting from trauma can be
losis, arthrosis, 'discopathy' and the like. There were
very similar to what is otherwise termed degen­
apparently even theoretical reasons for degeneration,
erative. One should therefore ask specifically in each
in particular of the disc: its vascularization is reduced
case of degenerative change whether this change is
early
in
decreases
the ontogenesis and its water content
rather
rapidly
during
the
first
three
decades of life (from 90% to 70%). According to
relevant or not; it is ilJ advised to draw clinical
conclusions from the mere existence of degenerative
changes in a radiograph.
Schmorl and Junghanns (1953),60% of women and
80% of men show evidence of degenerative changes
There is,
however, some correlation between
degenerative change and disc prolapse which may
at 50 while by the age of 70 the figure is 95% for
be of clinical importance. for, with
both sexes. No wonder that under the dominating
prolapse occurs mainly in discs already showing
a
few exceptions.
influence of the pathological anatomist the term
some degenerative change. The discovery that disc
'degenerative disease' is frequently heard.
prolapse could cause root syndromes was undoubtedly
8
Copyrighted Material
Theoretical considerations
9
a landmark: it m ade the medical p ub l i c aware of the
impo rtance of the spina l c o l u m n and of t h e
wor k s wi l l give us s o m e c l u e s as to w hat cause s pai n
possi b i l ity o f m e c han ical d i s t u rbance the re. O n t h e
in the loco m otor system when there is no defin i te
o t h er hand, t h e s t r iking success of s urg ical treat m e n t
pat h o l ogy .
i n fe r that
unde rstand i n g of how manipUlation
an
for some t i m e d i s c le s i o n s a n d disc
The firs t, naive explanat i o n of manipulative therapy
prolap s e were h e l d respo n s i b l e for a l m ost e v ery
was 're positi oning', and t h erefo r e something l ike a
mea n t that
disturbance
rela ted
to
the
s p i nal
co l u m n .
The
dis l ocat i o n or 'su b l u xati on' had to be assumed. This
reasoning w a s straightforward: i f root compress i o n
'the ory' was l o n g h eld by c h i ro p rac t o rs; S t ill m ust
in the lower lumbar reg i o n was found t o b e d u e t o
have b e l ieved in it, a s did Hippocrates, and pro b a b l y
disc pro lapse, t hen l umbago t hat occurs be fore root
a l l l ay m an i p u l ators down the age s - j ust
compres sio n is like l y to have t h e sa m e c a u s e . If root
right s o m e t hing t h a t was o u t of p l ace'. In fact, if a
compression in the l umbar reg i o n i s due t o the d i s c
pat i e n t with an acute w ry n eck or l umb ago, unable
t h e s a m e sho u l d a p p l y to t h e cerv ical spine a nd, b y
t o stra i g h ten up, is s u ccessfu l l y m a n i p ulated so t h a t
a n a l ogy,
to n e c k pai n; and a s ne c k pain i s frequently
'
putt i ng
h e i m m ediate l y s tands erect , it is l i t t l e w o n der t h a t
ass ociated w i t h headache, root co m p re s s i on may
s o m e t h i n g l i k e 're p o s i t ion i ng'
even be the ca use of c e r v i cal headac he. 'Discopathy'
e x p lanatio n . The reas o n w h y t h i s t h e o r y has bee n
was the fash i o nable w o rd t h e n, not vertebroge n i c
nor spondyloge nic diseas e .
S u rgical p r ac t ice soo n corrected t his vie w, t ho u g h
seemed the
likely
abandoned by p h y s i c i ans , as we l l as by m o d e rn
o s t e o paths and e v e n chiropractors, i s that wit h few
exc e p tions ne i t h e r d i s l ocat ion (,malalig n m e nt', 'sub­
by d e fault. Although disc surgery became a r o u t ine
l u xation' )
procedure for l u mbar root syndromes, it remained
m a n i p u l a t i o n can be proved. O n e of t h e meri ts o f
l u m bago, as well a s in
ro u t ine radiogra p h y i s tha t t h e s u b l u x a t i o n t h e o r y
the e x c e p t i o n
in simple
ce rv i ca l root s yndro m es, and is prac t i ca l l y n e v e r
used in the trea t m ent of pai n i n t he n e c k o r other
nor
reposi tio n ing
('adj u s t m ent' )
after
h a s had t o b e abandoned fo r l ack o f evide n c e .
Rece n t l y i t h a s bee n s h o w n b y M . Be rge r (pe rsonal
non-radicular cerv ica l s y n d r o m es. No r can disc
prol a pse be the only cause o f root syndromes in
the l u mbar regi o n : in o p e ration sta t i s t ics no disc
herniat i o n is fo u nd in abo u t 10% of the cases; the
comm u n i cat i o n )
large maj o r i t y of root sy ndro mes resolve w i th o u t
Jirout
operat i o n , a n d this i s t r u e even of cas es w i t h typical
s yn k i n e sis in t he sagi t tal plane aft e r s i d e - b e n di ng, to
findings
at
r adiograph
the
m y e l og r a phy .
shown
has
the
sam e
2.1a,b).
e ffect
for
the effe ct that the rela t ive h e ight o f t h e spi n o u s
w i th
case s
(1979)
processes was n o t t he same be fore a n d after s ide­
made
s u ch
t o an extreme p o s i t i o n a n d b a c k , so t h a t i t n eed n o t
re t u rn to the same n e u tral positio n ( F i g u re
the
is
in
on cineradiography of t h e
i s repeated after cli n i cal recov e r y (an d
myelography
[f
tha t
c e r vical s p i n e t h e re i s h yste re sis i f t h e h ead m o v e s
non-resorbable
con tras t oi l) , it has repeated l y bee n fo u nd t ha t t h e
disc p r o l apse remai n s u n c hanged , j u s t a s i t was at
be ndi n g in
a
n e u t ral p o s ition. [n o t h e r w o rds, t h e re
is no absolute n e u tral positi o n .
T h e flaw in t h i s ' re p ositio n' the o ry i s that i t
t he t i m e of maxi m u m pai n . It was, howeve r, show n
implies
i n man y, but n o t in a l .
dis p l aced, i.e .
man i p u lat i o n
of
a
ve r tebra
which
is
i n a ce rtain d i rect i o n , w h ereas in
longer fo u nd at c o m p uted to m ography after t he
reality we o n l y
pa tient is free from pai n . On tbe other han d, if disc
verte brae , as is e x p l a ined late r. Tec h n i ca l l y, t h i s i s
p rolapse i s fo und, e s pecial l y in s u bjects with o u t root
q u i t e a d ifferent p r o p o s i tion. In fact, as there is no
syndromes, it can be c o n s i de red irrelevant.
absol ute n e u tral posi t i o n , we can ass u me t ha t v e r te­
Reviewing t h ose morph o l o g i c a l changes t h a t are
u s ua l l y related to back pai n and assoc i a ted c o n ­
restore m o v e m e n t b e t w e e n
two
brae always return t o t h e req u i red n e utral p os i t i o n
ditio ns, w e can readily see t h a t t h e y do not e x plai n
i f tbey c a n move freely .
Fascinat i o n w i t h t h e
the com plaints o f the vast majori ty o f our patients .
explanation fo r the effect of manip ulat i o n ( S toddard,
This is a l s o t h e reas o n w h y this ty p e of pa t i e n t is
some times
vague l y
'idio pathic back
des cribed
as
suffe r i n g
from
pai n ' o r j ust 'pain without any
disc
also
p r ov i ded
an
1961; Mai g n e , 1968; C y riax, 1977), a l t h o u gh it i s
d i ffic u lt t o s e e how man i p u l atio n c o u l d ac h i eve re­
p o s i t i oning of a p r o l apse the exact p o s i t i o n of w hich
patho logy' or eve n 'wi t h out a n y diagnosis' ('non­
can n o t
specific bac k pai n '; Jayso n, 1970); in view o f t h e
app roac h is that m an i p u lation is not ap p l i ed t o the
n u m e rica l impo r tance o f t h i s g ro u p of pat i e n ts this
spinal
is l i t t l e to the cred i t of clin i cal m edi c i n e .
t reat m e n t o f e x trem i ty jo i n ts, a n d p a r t i c u larly s o at
be
known .
colu mn
The
o n ly:
it
grea t
is
also
wea k n e s s
effect ive
of
in
this
the
the c ra n i ocervical junctio n, o n t h e r i b s a n d at t h e
sacro iliac joint, where t h e re i s n o q u e s t i o n o f d i s c s .
C l i nica l experie n ce also shows qu ite c l e ar l y t h a t
Theoretical implications of
manipulation
manip u l a t i o n i s most effective i n c o n d iti o n s wh ere
we do not expect
If manipu l ative t reatme n t is succes s f u l it u s ua l l y
produces immed i a te re l i e f o f pai n . W e may t h e refore
to
find disc l es ions , and l e ss
effect i v e in true disc prolapse.
The sophisticated d i ag n ost ic techniques deve l oped
Copyrighted Material
10
Manipu/o(ive Therapy il1 Rehaoili({ffiOI1
of (he Lucul1Io(or Sys(em
by the os te opath s have pro vided what we believe to
be rel e vant clinical evidence of how manipulation
really works: we apply m a nipu l ation where we find
s ign s of mo vem e nt restriction, whether in an
ex t re m i t y joint, a rib, or a ver t eb ra l movement
segment, and if mani p u l a ti o n is s u cce ssfu l , mobility
is always restored. In o t h er w ords . ma n i p u l ati o n
does not achieve a c h ange o f structure, a s Still
thought, but normalization of function. This is even
true i n cases of wry neck or acute lumbago: the
crooked position of the neck or the back in such
c as es is itself p hysiological, and it is only the fact
that the patient is fixed in this position ( head
rotation plus incl i nat i o n in wry neck) th at is p atho­
lo gica l . Manipul ation merely frees mo bil ity and th u s
enables the p a tie nt to r eturn to the n eutra l p os itio n .
In this, wry neck and lumbago are the ex ce pti o n to
the rule; in the vast maj ority of cases movement
rest r ictio n is fo und wh ere j oin ts are in the neutral
pos itio n and t here is d i rn culty in pro ceed i ng th rou g h
the whole range of move ment.
Functional aspects
(a)
The most important theoretical inference from
clinical experience with m a n ip u l a tio n can be formu­
l ated thus: if one a pp lies ma n i p u lat io n only after
a d eq uate clinical exa mina tion of mob i li t y and is
careful t o re -examine after treatment. then one
regular l y finds that successful m ani p ulation achieves
normalization of restricted motor fu n ctio n . and that
this goes hand in hand with relief of symptoms. Thi,
theoretical inference should then logically be valid
not only for pas sive m ob i l i t y , but also for a ctive
muscle function. We owe to Janda (1967) the proof
that this is true in particular for faul ty motor
patte rns ( motor ste r eoty p es) producing o v ers tra i n in
the motor system. This is in keeping with the sim p l e
observation that e xcessive st rai n causes sympto ms.
whatever the ca u se of the strain.
In addition to active motor patterns. there is
another imp orta n t function, disturbance of which
frequ ently ca u s es symptoms: this is body statics. In
fact . in modern s o ciet y static overstrain may be at
I.east as frequent as faulty mobility, and a g a i n we
find that co rr e c t i o n of f a ul ty sta tics frequently brings
relief. Thus, m anipu l at i o n pioneered our involvement
w i t h fau l ty functioning of the locomotor system and
with its normalizatio n, as we shall sec thr o ughout
this book. Indeed, faulty fu n ct io n alone is the ca use
of frequent symptoms; this c an be sh o wn in ch i l d re n .
Morphological change s. on the other hand. do not
e x c l u de c h a n ges in function. This is pa rticul a r l y
true f o r disc lesions and may explain spontaneous
recovery and reco very al"ter conservative treatment
(including man ipulation ) . This is of great im portance
for rehabi l it a tio n in traumatology, where our
primary aim is to improve fun ction d es p it e mo r pho
logical changes, in o rder to achieve compensation.
As will be shown later. function and its d i st u rb­
ance s a re rarel y confined to one site or structu re .
and therefore diagnosis must take in the locomotor
system as a wh ole. The term 'vert ebroge nic' or
'spondylogenic' is thus no l o nge r appropriate, a s
even in back pain w e must take into a ccou n t muscle
funct i o n and its n er v o u s control as well as the
fu n ct io n of the pe lvi s and the extremities. As
­
(b)
Figure 2.1
(0)
In this X-ray of the upper cervical spine in
C2 is slightly rotated to the left with the
spinous process deviating to the right. (0) [n the same
neutral position there is marked rotation with deviation
or the same spi nous process; the subject had held his
head in maximum left rotation before returning to the
neutral position.
neutral position (reverse or false 'reposition')
Copyrighted Material
The clinical
segmental
'vertebrogenic' disea,,"
deAned
pathologicil
spondylitis or osteopOlo,i;"
the application of mampulatlOn and other measures
aimed at restoring function is whether the patient's
complaint is due (mainly or exclusively) to changes
of function, or to changes of structure (patholog y).
This is
a
more difficult matter than it may seem:
it requires a systematic assessment and a technique
of examination that has not yet been formulated. It
is the great
weakness of
manipulative therilpy,
remedial exercise, etc. - methods concerned with
improving the function
they have been, anel tor 1
mainly concerned with
that
I are,
(Figure
2.2).
These consist of (1) hypermobility and
(2) movement restriction; obviously, manipulative
therapy is concerned only with the latter.
importance; they include changes in quantity as well
as in quality, of which the f o r m e r - taking the form
of restricted mohility - is certainly the more straight­
forward. It is
extremity joint,
much more
the spinal
of great
column. Change!;
to remedy. This is
increased
diagnostic value.
the paradox that in
well
recognized, whereas
function is panlmount, thiS ium.lamcl1tal aspect is
rarely considered. However, the functioning of the
locomotor system is extremely c o m plex, as we shall
see, and diagnosis of disturbed function is it highly
sophisticated p roceeding carried out, as it were, in
a c.linical no man's land. There is an additional
disadvantage in that it can be investigated only by
clinical methods, for the most part, and these are at
present regarded as 'subjective', whereas 'modern'
research puts its faith
y.
The
principal (clinical) characteristics are of the utmost
with
clinical diagnosis of till
importance of change-s
We may now turn back to the intervertebral
motor segment and disturbances in its functioning
'binding'):
resistance during
Ihe lack of
the most striking
springing in the
motor s egment ;
ed joint or
I!l
position is never
a normal joint the extreme
reached abruptly, and a slight
increase of pressure increases the range of movement.
There is no absolute limit. In a joint with restricted
mobility, this springing or giving way has been lost
and we abruptly encounter a barrier. This has given
rise to the term 'blocking', or blockage, and is,
rerhaps, the most easily diagnosed sign.
In the osteopathic literature the barrier concert
is further elucid;ilcd:
'anatomical barrier'
ligament. Activ('
range than passive,
elastic barrier.
reaches the
111
capsule
or
:,ollh'what smaller
I
l.imited by an
restriction we
the range of
e n c o unter a 're s l nel
movement; this
quality, being
abrupt, with no
harrier may
even change the neulral position or a Joint. In the
direction of the pathological barrier, 'binding' may
be found on motion palpation. It should be pointed
out that although the barrier concept is most
freC]uently applied to joints, it may also be used with
respect to soft tissues and muscles (Figure 2.3) . It
should always be borne in mind that the barrier has
a protective function.
Figure 2.2 The mobile
: 955)
Ph
A
Figure 2.3 The barrier phenomenon: the anatomical, physiological and pathological barriers
Copyrighted Material
Hanipullllive
Rehabilillllion
locomotor Syw:ril
The physi ological barr i er which i s most important
from the practical point of v i ew i s the most ill
defined. In the osteopathi c glossary (1997) it is the
of acti ve motion.
only is this definition
cannot be
for soft
passi ve exami nation of joints,
pl <.l y
According to the latest chiropractic publication
this barrier is reached at the very end of
passive
motion. This
definition,
again,
is
2.5),
these
2.6).
mobili!v
thus be clinic:iliv
It
normal joint
movement;
a
restoring nonncli
most cUcetive and gentle
normal
(1995)
as is well illus­
shifting movements as well as distraction are
inferred
.
(2),
use springing techniques; and
trated by MennelJ's d i agram (Figure
the prerequisite
Its dlslurbance can b..:
likened to a drawer that has stuck, and needs to be
eased out.
most
unfortunate, beGlUse both (thrust)
rnobili zati on
C<lrlled out atlt·,
( engaging') thi s
T h i s necessarily
restriction and reflex
however, i s
stretch reflex
With good relaxation and spontaneous re l ease . For
an optimu m gentle technique we have to reach the
Blockage III an articulation and particularly III a
vertebral motor segment goes hand in hand with
barri er by the patient relaxing, the resistance of a
reflex changes mainly in the same
joint in neutral range being practically n i l. This is
These affect the dermatome as well as the muscles,
where sprillgmg
IIy true for
ant for both
release
most
segment.
changes is
complex
(989)
and treatmenL Thne
the
very little springi ng at the
range of
The same
for
called
at
coined the term 'segmental facilitation'. In movement
the
barrier,
which,
agai n,
requires
maximum relaxation.
addition,
good
dysfunction' (Greenman,
is characteri zed by asymmelcy, ahnormal range of
motIOn
soft tissue
restriction,
This is quite as true for soft tissues as for joi nts.
In
etc.
spi na l
palpation
is
mandatory
muscular
Korr
tension
or spasm
is
(1
most
important because it may fix the joi nt and may be a
for
very significant factor callsing restri ction; this can
of
be seen from a pOSitive straight leg
goes for the
antalgesi c posture'
(1998) showed that mcreased pressure produced
bendllJg of the whole lumbar spme prevent allY
increased stiffness of the lumbar spine.
attempt by the patient to straighten up.
and for sensing release: the
is, however,
than very
used.
s,yntlromes,
whc:n antcl'icxi on and
For all these reasons the correct definition of the
To quote Korr (1975), who has devoted most of
physiological barrier is the point where the first
of
his work to the implicati ons of manipulativc me rapy :
as the motors of
thi nking of
'Whi le
a
to
is
is met. Thi s
of the examiner
hallmark of his
very probably
contractiun.
nroduci ng motion
to remember
force,
libo used to
therefore proposed that it i s
that a muscle may become a major and highly
Joint play and movement
restriction
variable
impediment
to mobility of a
lesioned
"joi nt"'. After giving a thorough explanation of the
ilre
are two types
PLlssive
by movement l es,nctlOn
the
IS functional moverm:nt', i.e. movement earned
out by thc subject; joint play is passive movement.
whi ch cannot be carried out by the subject and
role
Korr
lIluscle spindle and
gamma syslenl
'The h i gh
with,
s an explanllllOn
resistance [0 moti on ("b ind") in une direction ...
They [the muscles] would also be provoked into
stronger and stronger contraction by the exaggerated
comprises a translatory (sliding) movement of one
spindle discharges as motions that tend to lengthen
joi nt surface agai nst the other, or even rotati on. and
Thus we
d istraction
the affected muscles occur'
found cli n i cal
explained not
finger, whereas
the metacaqul
any
direction, rotated, or distracted by axial pull. These
movements are not only felt, but can be demonstrated
radiographically (induding distracti on, F igure
2.4).
Joi nt play is by no means of academic interest only:
practical clinical
blockage at
normal, winch
lies in
) it
r,.1sponsi ble for
joint, but by the organ
To put it brieny. the
mOl/llment restriction
struct ure thl,!
mobility, i.e,
active movement, the
muscle. That is why osteopaths do not use the term
'blockage' for movement restriction bu t in order not
,
to commit themsclves, speak of 'osteopathic lesi ons',
or more
1978)
The
Copyrighted Material
of ' somatic
unction' (Green m l l lL
of shortened
in movement
Theoretical considerations
13
restriction has been demonstrated by J a nda (1967) .
Muscle relaxation
order to mobilize
techniques are widely used in
j o ints
.
The question must there­
joint in
fore be put: what is the role of the
pa s s i v e
movement restriction?
Blockage as an articular
phenomenon
The
si m p l i s t i c
entirely
view
or mainly an
that
passive
a rt ic ul a r
movement
is
phenomenon should
be abandoned. In fact. as K or r has shown , most
by which we recognize movement
restriction in a j o int or vertebral motor segment
might be explained by muscle ac tivi t y induced by
cli n ical pheno me n a
the m u s c l e pro pri ocep tors and the gam m a syste m .
What evidence remains t o show that the j o i nt has a
r ol e
of any importance')
There is one
obvious weakness in the purely
'mu sc u l ar' theory: it does not e x p l a in what s timu ­
lates the receptors: in other words, if m u scle activ i t y
is
a
reflex response, which n obody doubts, where
does the s t i mulu s come from? The pu re l y e m pir i c al
techniques
of
manipulati o n
are
base d
on j o i nt
a n a tomy . It is surprising that osteo paths, who a re
the
(a)
(b)
(c)
Figure 2.4 (a.
originators
of
most of these
very carefully
worked out and exactly taught techniques, appear
(d)
b) Distraction of the metacarpophalangeal joint: (c. d) medial and lateral gapping of the knee Joint.
visualized by X-ray
Copyrighted Material
14
lv/anipulative Therapy in
Rehabilitation of the Locomotor System
ar t i cula r
p he n omenon .
But t here
is e v e n
direct
evidence:
J. T h ere are three joints lhat are not moved by
muscles, nor can t heir movement be opposed by
them:
these are
the sacroiliac,
the
acromio­
cl a vicula r and t he tibiofibular joints. Yet these
joints show typica l signs of blockage and their
tre atment by pa ssi v e mobilization is particularly
(b)
(a)
Figure 2.5 Importance of joint play. (a) Gliding
movement is ess e n tial for join t function: if gliding is
disturbed
(b)
forceful movement may injure the joint
(MenneJl. 1964)
therapy
effective.
2. I n order to prove (or dispro v e ) the rol e of the arti­
culation we undertoo k the followi n g experiment:
in 10 patients the cervic al spine was examined
before operat ion ( mainly abdominal surgery) and
re-examined under anae s the s i a with myorelaxants
and intubation with artificial respiration. Tn all
cases movement restriction remained uncha nge d
and was even more easi ly r ecog ni z ab le d ur ing
narcosis, as the patient was completely relaxed.
Possible mechanism of joint
blockage and manipulation
fixation
The importance of the experiment just referred to
mobilization
lies not only in proving that movement restriction,
too, is an artic u lar p henomenon, but also in that it
prove d that we have to deal with a mech ani cal
obstacle in the joint. It was Emminger
first
suggested
that
such an
(1967)
who
obstacl e migh t
be
attributed to the me n iscoid s previ ously described by
therapy
Figure 2.6 The direction of gliding
mobilization. showing
how
movement and joint
this depends on whether the
pro x im a l or d i st a l partner is
concave
or convex (After
Kaltenborn. 1976)
very little aware of their theoretical implications.
More indirect evidence lies in the importance of
joint play as a prerequisite of normal joint function:
there is no doubt that muscles have a far stronger ,
direct influence on functional movement, which is in
fact induced by muscles and can for the same reason
be inhibited by muscles, than on the m o v eme n ts of
joint play. If, therefore, the muscular factor was the
decisive one, functional movement would be affe cted
first, and not join t play. We know, however, that
Figure 2.7 Entrapment of a meniscoid at the edge of a
the reverse is the case. Further evidence comes
from analysis of the h igh - v elocity t hrus t t echni q ues
joint space, according to the joint blockage theory of
producing gapping of the joi n t surfaces, together
position (a) has m ov ed between the joint facets and its
wit h a po pp ing sound, or 'click'. There are distraction
high-velocity thrusts which cause hardly any dis­
tension of the muscles, the j oint remaining in the
n eut r a l pos ition , and the cl i ck itself is certainl y an
Wolf
(1975). Top. tbe meoiscoid nor m all y lying in
hard edge has impinged: (b) bollom, it has returned to
n orm al pos i tion after treatment. A groove (c-d) remains
for a s h o rt time, but b eing flat it offers only minor
resistance to slipping back
Copyrighted Material
1:;
Theoretical comiderallom
Tbndury (J 948) in intervertebral j oin t s , and later
found by Kos (1968) even in extremity joints: the
meniscoids may get caught between the moving joint
facets, Indeed,
most
joints have very incong ruou s
produces a cavity i n the cartilage Hnd is trapped in
it (Figure 2.7).
The implications for the theory of ma nip u l a ti o n
are clear: if we sepa r a te the joint facets by high­
facets and smooth mobility is possible only if some
velocity th rust techniq ues, the meniscoid can slip
additional tissue call fill the redundant space, To do
out. Figure 2.7 shows that the tr app e d edge of the
joint facets, and may meet with difficulties, Kos and
overcome, cons is ti ng of two very shallow grooves
this the meniscoid must move freely between
the
Wolf (1972) have further elaborated this theory,
showing why the mechanism is easily di s tu rbed : ( 1)
the me niscoid h a s a soft base and
a
hard edge, which
ca n no t easily be comp r e ssed and (2) joint c a rtil a g e
is hard and elastic only if the force that acts on it
does so rapid ly , If, however, we subj ect the ca r til a ge
to
pressure, it
that pr essu re as
constant
exerting
therefo r e ,
the
adapts to
the material
though it were Auid. If.
meniscoid is
caught
gliding surfaces of the joint f acets,
between the
the hard edge
me
n iscoid
has
only
a
very
slight
r esist a nce
to
that open smoothly into the wedge-shaped space
between the c a r tilage surfaces. I n repetitive mobil­
ization
meeting
back-and-Forth
a
greater
m ove m e
resistance
in
nt
the
takes
place,
direction
of
incarceration than in that of liberation. After the last
resistance has been g r ad u ally overcome, the meni­
scoid
s lips
back into its original position. Fig ure 2.8
a lso illustrates how resistance becomes less with
each movement that increases the space between the
dotted lines.
(8)
Figure 2.8 The effect of therapy. (a) Gapping of the joint by high-velocity thrust, making it possible for the meniscoid
to slip back. (b) Repetitive mobilization enabling the meniscoid to move back into its original position, first by small
degrees and then more rapidly
Copyrighted Material
of
(01
Copyrighted Material
17
Theoretical considerations
�'j
�
4
6
E
E
��
�.
5
/.
c
�I
� . �\�:
c
Q 4
ro
;;;
Q.
Q)
Ul
3
2
-.---- .
. -- .
r
/
./
Crack
L�-.--.-.I
2
,
4
,
6
10
8
12
Tension in kg
14
16
18
Tension in kg
Figure 2.11 The effect of the 'click' prod u ced by
distraction of a metacarpophalangeal joint, according to
Roston and Wheeler-Haines (1947)
Trauma
Figme 2.10 Distraction of a metacarpophalangeal joint;
below after a thrust ( i n to traction)
above before,
The second cause of disturbed locomotor function
is trauma. It is important to point out that there are
borderline cases between trauma and overstrain due
to a great variety of causes, because it is not always
important factor in spinal and locomotor function is
easy to say what is and what is not an injury for the
obviously the musculature and its nervous control.
spinal column.
Usually trauma is defined as an
This control is expressed by motor patterns and
exogenous force acting on the body for a short time
posture, formed in a highly characteristic way in
and capable of damaging structure or function. Even
every individual. As Janda (1967) has shown, there
uncler normal conditions the forces acting on the
is a certain balance between various muscle groups
(see p. 26) that move j o i nt s or vertebral motor
segments, and if this balance is disturbed the normal
spinal column arc considerable. If these forces are
suddenly increased because of sharp, ill-balanced
movement, the line between the two groups of
functioning of the joint suffers.
causes appears to be rather arbitrarily drawn.
Modern civilization brings with it very one-sided,
forced movements, causing muscular imbalance, and
this is no less true of posture - in fact, one of the
characteristic features of modern life is lack of
movement accompanying static or postural over­
Reflex action
Blockage may be of reflex origin due to changes in
a segment. As stated in Chapter 1, the spinal column
strain. Therefore the first and most fre q ue n t cause
is involved in disease wherever it occurs in the
of blockage is a faulty movement pattern due to
organism. Visceral disease causing nociceptive stimuli
muscular imbalance, ancl postural overstrain.
is followed by reflex spasm in the relevant segment
Copyrighted Material
18
Manipulative Therapy in Rehabiliwtion of the Locomotor Syslenl
Figure 2.12 Electromyogram showing an increase in muscle activity (force) in the triceps brachia during cervical
traction
(muscular defence) a n d in particular in th e deep
l a ye rs of the erect o r sp i n ae muscle. This is likely to
fix the vertebral motor segment as well as to
interfere with normal mobility of the trunk. If such
a spasm is of sufficiently long duration, blockage is
lik e l y to occur. H a nsen and Schliack (1962) d es c r i b e
characteristic sc ol iosi s in visceral d is ea s e . As is
shown in Chapter 7 (p. 282), we recognize a number
Figure 2.\3 Electromyogram t a k en from three leads in
a
of
characteristic ' spi n a l patterns' in visceral disease,
showing that there are certain p a thogen etic rules. A
st r i king feature of this type of blockage is its
recurrence if the internal disease relapses or
ex a cerbates . rn fact, we seem to k now m ore about
visceral influence upon the spi n a l column than about
the influence of the sp ina l column on visceral
di s eas e .
C8 root syndrome (a) before and (b) after cervical (thrust)
manipulation
Copyrighted Material
Copyrighted Material
20
Manipula tive Th erapy in Rehab ilita tion of {h e Locomotor System
heavy
head
on
the
fragile
cervical
spi n e .
P h ysiologica l l y , t h i s is t h e s i t e o f t h e t o n i c n e c k
r e A e x e s , a n d i n fl u e nces m u s c l e to n e t h ro u g h o u t
t h e p o s t u r a l t ru n k m u sc u l a t u re . I f fu n c t i o n h e re
is d i s t u r b e d . t h e re is m o s t fre q u e n t l y h y p e r t o n u s
of t h e pos t u r a l m u sc l e s , d i s t u r b a n c e s o f e q u i l i b ­
t h e o t h e r e n d o f t h e s p i n a l c o l u m n . o r ev e n i n t h e
e x t re m i t i e s . T o l e a v e s u ch a
l e s i o n u n tre a t e d
r i s k i n g t h e r a pe u t i c fai l u re a n d rc l a pse .
is
The impo rtan ce of nervous co ntrol
to be
The s p i n a l co l u m n c o u l d not a c t as a f u n c t i o n a l u n i t
i m p o r t a n t for r o ta t i o n . as o n l y t h e a t l a n to a x i a l
u n d e r n e r v e c o n t ro l . The r o l.e o f m o v e m e n t p a t te rn s
o f t h e c e rv i c a l s p i n e i s t h u s fo rced to t a k e o v e r a
t h i s i s the most s i g n i fi ca n t cause o f b l oc k a g e i n a
rium
and
l o c o m o t o r d e fi c i t w h i c h
has
c o m p e n s a te d b y t h e cervical s p i n e . T h i s i s m o s t
j o i n t i s i d e a l l y a d a p t e d for rota t i o n , a n d t h e r e s t
fu n c t i o n
fo r
w h ic h
it
is
poorl y
fi t t e d .
The
t e m p o ro m a n d i b u l a r j o i n t w i t h t h e m a s t i c a t o r y
m u sc l e s a n d t h e d ig a s t r i c u s a re c l os e l y r e l a te d t o
the cra n i o cerv i c a l j u nc t i o n .
2 . T h e l u m b o s a c ro i l i a c j u n c t i o n for m s t h e b a s e o f
t h e s p i n a l col u m n a n d t h e refore d e te r m i n es b o d y
s t a t i c s . A t t h e s a me t i m e i t t r a n s m its mov e m e n t
from t h e l e g s t o t h e s p i n a l c o l u m n a n d a c t s a s a
shock absorbe r.
3. The
c e r v i c o th o r a c i c j u n c t i o n
is
the
regi o n
u n l ess a l l i t s r e a c t i o n s w e re coord i n a ted b y m us c l e s
a n d t h e i r d i s t u r b a nce h a s al r e a d y b e e n st ressed . as
v e r t e b ra l m otor segm e n t . J a n d a
( 1 978)
has shown
t h a t t h e q u a l i t y o f m ov e m e n t p a t t e r n s v a ri e s from
one i n d i v i d u a l t o a n o t h e r , a n d t h i s goes h a n d in
h a n d w i t h v a r y i n g s u s ce p t i b i l i t y t o v e r t e b roge n i c
d is t u rb a n c e . O n t h e o t h e r h a n d , a n y d i s t u r b a n c e o f
f u n c t i o n i n a s i ngle m o t o r segm e n t w i l l h a v e i t s
r e p e r c u s s i o n s t h r o u g h o u t the b o d y a x i s a n d m u s t be
compe n s a te d . Here a ga i n , n e rv o u s c o n t rol p l a y s a
d e c i s i v e p a rt . T h i s is no l e ss t h e case w i t h pa i n . o n c e
t h e l e s i o n b e c o m e s p a i n fu l , fo r i t is the n e rv o u s
in
w h ich t h e m o s t m o bi l e s e c t i o n o f t h e sp i n a l
s y s t e m th a t d e t e r m i n e s h o w i n t e n se l y t h e s e g me n t
s p i n e a n d w h e re the p o w e rfu l
o t h e r w o r d s , i t i s t h e n e rv o u s s y s tem t h a t d e t e r m i n e s
co l u m n i s j o i n e d t o t h e re l a t i v e l y r i g i d t h o ra c i c
muscles o f t h e
wi l l react, and
w
he re
t h e t h re s h o l d o f p a i n l i es. I n
u p p e r e x t r e m i t i e s a n d s h o u l d e r girdle insert .
wheth e r
is well seen i n the transition ve rtebra T12 w h e r e
i n te n s e , d i s t u r b e d f u n c t i o n i n o n e m o t o r segm e n t
4. T h e g re a t s t ra i n on t h e t h o raco l u m b a r j u nc ti o n
t h e u p p e r a po p h ys e a l j o i n ts r e t a i n t h e t h o r a c i c
patte r n whereas the lower j o i nts have t h e l u m b a r
p a t t e r n , i . e . w h e r e o n e type o f fu n c t i o n c h a n ge s
a b r u p t l y to a n o t h e r . I f d u r i n g wa l k i n g t h e p e l v i s
c l i n i ca l l y .
d i s t u rb e d
fu n c t i o n
I f reaction
to
will
m a n i fe s t
nociceptive
i t se l f
s ti m u l us
is
wi l l prod uce a n a n ta l g e s i c response a n d a lt e r t h e
n o r m a l m o t o r p a t t e r n , h e nce p r o d u c i n g fi x a t i o n of
a
c h a nge in fu n c t i o n .
Co n trol
by
the
n e rv o u s s y s t e m
thus
has
two
t i lts from o n e s i d e t o t h e o t h e r , t h e l u m b a r s p i n e
a s p e c t s : i t s u b s e r v e s n o r m a l fu n c t i o n b y t h e m a i n ­
l ie s a t t h e leve l o f L3, t h e t h o raco l u m b a r j u nction
d i s t u r b e d fu n c t i o n . O n t h e o t h e r h a n d , a n i n t e n se
s i d e - be n d s s o th a t t h e vertex o f t h e s co l i o t i c c u r v e
r e m a i n i n g in l i n e with the s a c r u m ; t h i s t o o , c a n
t e n a n ce of correct motor p a t te rn s , a n d i t comp e n s a t e s
b e s e e n i f th e s u bj e c t m a r ks t i m e b e fo r e a n
and c h r o n i c p a i n fu l s t i m u l u s d is t u rbs n o r m a l motor
p a t t e rn s a n d m a y then cause alte red . p a t h ological
i n te n s e s p a s m n o t o n l y of b a c k m u s c l e s , b u t i n
the d i s e a s e process.
X - ra y screen .
D i s t u r b a nce
of function
p a r t i c u l a r of t h e psoas m u sc l e
causes
( K u b i s , 1 969),
the
m o t o r pa t t e r n s t o b e c o m e fi x e d , thus p e r p e t u a t i n g
It is,
t h e r e fo r e , n o c o i n c i d e nce
that d i s t u rb e d
q u a d ra t u s l u m b o ru m , t h e thoraco l u m b a r e re c t o r
fu n c t i o n o f the motor s y s t e m is m o re l i k e l y to be
t h i s t ra n s i t i o n a l r e g i o n u n l i k e t h e o t h e r th r e e ,
a re a s a rule psyc h o l ogica l l y l a b i l e a s we l l . In t h i s
s p i n a e and even the stra igh t a b d o m i n a Is, because
co n n e cts t w o v er y m o b i l e sec t i o n s o f t h e s p i n a l
c o l u m n . I m mob i l i za t i o n o f t h i s j u n c t i o n the refo re
m a kes s e v e r e m u s c u l a r s p a s m n e c e s s a r y .
5 . I n h u m a n s t h e fe e t a r e t h e b a s e o f b o d y s t a t i cs
a n d g a i t ; a t t h e s a m e t i m e t h e y a r e t h e s o u rce of
fo u n d in s u bj ects w i t h l a b i l e n e r v o u s regu l a t i o n . who
con n e c t i o n i t i s o f i n te re s t t h a t S t a ry
Figar
severe
( 1 970)
(1 970)
and
w e r e a b l e to s h ow t h a t p a t i e n ts w i t h
radicu l a r
s y n dromes
very
easi l y
fo rmed
co n d i ti o n e d rene x e s to a d d i t i o n a l pain s t i m u l i , and
tha t t b e s e reAexes w e re m o r e d i ffi c u l t to e x t i n g u i s h
t h e most powe rfu l p r o p r i oce p t i ve , e x t e roc e p t i v e
t h a n i n h e a l thy c o n t ro l s . F u r t h e rm o r e , K u n c el al.
s e n s ory orga n s .
p l a y s a m a j o r p a r t i n recove r y a fte r d i sc o p e r a t i o n .
and
n o c ice p t i v e
imputs,
comparable
to
o ur
( 1 955)
s h owed t h a t the m e n t a l con d i t i o n of p a t i e n ts
G u tzeit ( 1 95 1 )
In
view
of
their
i m po r t a n ce
and
t h e i r great
factor
is
fo u n d t h a t a pro m i n e n t psyc h o l og i c a l
c h a r a c t e r istic
fo r
v e r t e broge n i c
pain
v u l n e r a b i l i t y , t h e s e k e y r e g i o n s a re u s u a l l y t h e p l a ce
p a t i e n ts . S nl c e k a n d S k ra b a l ( 1 97 5 ) c o m p a red two
o b s e r v e d i n c h i l d re n . D i s t u rb a n c e of fu n c tion a t
s i g n s o f a nx i e ty a n d d e p ressio n . a n d 2 5 sch i zop h re n ics
col u m n ( a n d t h e motor syste m ) a s
c e rv i c a l
w h e re t h e s p i n a l c o l u m n s u ffers firs t , as c a n
b es t be
s u c h p o i n t s j e o p a r d i z e s t h e f u n c t i o n i n g o f the s p i n a l
seco n d a ry l e s i o n s . S u c h
a
a
whole, causing
d is t u r b a nce s h o u l d never
b e ov c r lo o k e d e v e n i f t h e s y m p toms a re m a n i fest a t
t y p e s of m e n t a l p a t i e n t s : 50 c a s e s o f n e u rosis w i t h
w i t h l o w e m o ti v i t y . B lo c k a g e . m o s t freq ue n t l y in t h e
spine, was
a bse n t
in only
fi ve n e u ro t i c
1 6 sch izop h renic
p a t i e n ts . The seg m e n t m o s t fre q u e n t l y a ffe ct e d w a s
p a t ie n t s , b u t w a s n o t fo u n d
Copyrighted Material
in
Th eoretical considerations
the a t l a n t o - occi p i ta l ; t h e d i ffe r e n ce w a s s i gn i fi c a n t
w e l l a pp l i e d , s h o u ld g i v e i m me d i a te
a t the P = O. O l level.
is
A ga i n , obse r v a t i o n s by J a n d a ( 1 978) a re o f g r e a t
relev a n ce :
inclined
fo u n d
p a r t i cu l a r l y
true
for
the
new
21
rel ief. This
n e u ro m u s c u l a r
tec h n i q u e s .
i n p a t i e n t s wi t h poor m o t o r p a t t e r n s ,
The m o s t n u m e r o u s c h i l d p a t i e n ts , p r e s e n t i n g a
t o i m b a l a nce o f t h e m u s c l e g ro u p s , h e
r e a l probl e m , a r e t h ose w h o s u ffer from h e a d ac h e ,
(1)
m i n o r n e u r o l o g i c a l d i s t u r b a nces w h i c h h e
t h e cerv ic a l spi n e b e i n g o n e o f the m o s t freq u e n t
te rmed ' m icrospa s t i c i ty ' , i n w h i c h move m e n ts w e r e
causative
n o t fu l l y coord i n a ted a n d a p pe a re d c l u m s y ; ( 2 ) s l i g h t
h e a d a c h e , i ncl u d i n g m igra i n e .
s e n s o r y i m p a i rm e n t , i n p a r t i c u l a r o f prop rioce p t i o n ;
c h i l d re n s u ffe r i ng from n o n - m ig r a i n o u s h e a d a c h e ,
( 3 ) worse a d a p t a t i o n to s t ress s i t u a t i o n s a s a re s u l t
m a n i p u l a t i o n g a v e e x ce l l e n t res u l ts , w i t h o n l y two
o f poo r l y coord i n a t e d b e h a v i o u r .
A l l t h i s corre­
sites. T h i s is t r u e o f v a rious types of
In
a g r o u p o f 30
fa i l u r e s , w h i l e in a group o f 27 c h i l d re n s u ffe r i n g
spo n d s t o a ( re l a t i v e l y ) n e w c l i n i c a l e n t i t y , m i n i m a l
from
bra i n dysfu n c t i o n , w h i c h i s fo u n d i n 1 0-1 5 % o f t h e
exce l l e n t resu l ts i n 24 c a s e s . T h e s e fi n d ings w e re
m i g ra i n e
t h e re
w e re
three
fa i l u re s ,
and
( 1 966) .
c h i l d pop u l a t i o n . J a n d a c o m p a re d t h e s o m a t i c a n d
co n fi rm e d by K a b a t n fk o v a a n d Kaba t n f k
psych o l ogica l fi n d i ngs i n
these c h i l d r e n w i t h t h e
p a r t i c u l a r l y i m p o r ta n t type o f h e a d a c h e i n c h i l d r e n ,
fi n d i ngs i n a d u l t pa t i e n t s w h o h a d v e ry u n fa v o u ra b l e
k n o w n a s ' sc h o o l h e a d a c h e ' , form e r l y b e l i e v e d t o b e
m o t o r pa t t e rn s t h a t produced re l a p s i n g v e r t e b ro­
o f p s y c h o l o g i c a l o r i g i n , w a s p ro v e d b y G u tm a n n
g e n i c d i sorders, a n d c o n c l u d e d t h a t s u c h c h i l d re n
( 1 968) t o b e d u e t o h e a d a nt e fl e x i o n d u r i n g s c h o o l
A
become those p a tie n ts w h o prese n t th e ms e l v e s i n
h o urs, w h e n
a d u l t l i fe
d e s k s . T h i s w a s c o n fi r m e d b y L e wi t a n d K u ncova
with
the
principal
symptom
of
pain,
p a t i e n t s were be n t
o v e r h o ri z o n t a l
beca use of s m a l l n e u ro l o g i c a l c h a nges w h i c h d o n o t
( 1 97 1 ) .
d isap p e a r d u ri n g a d o l esce n ce b u t i n s t e a d t a k e t h e
fu n c t i o n i n the l u m b o s a c r a l regi o n is dys m e n o r rh o e a
form o f d i s t u rbed f u n c t i o n o f t h e m o t o r syste m , w i t h
or a l go m e n o r r h o e a
resu l t i n g p a i n .
fi n d i n gs i n y o u n g g i r l s , freq u e n t l y s t a rti n g a t t h e
N e v e r th e l ess, however i m po r t a n t m o t o r i m b a l a n ce
may b e , it is n o t i d e n ti c a l to i m p a i re d j o i n t fu n c t i o n
or
b l ockage of
v e rt e b r a l mo t o r s e g me n t . S uc h
a
lesions d o a p p e a r e v e n
i n s u bj e c t s w i t h
perfect
m o to r p a t t e r n s , w h e re a s they may be m i ss i n g i n
One
c l i n ica l
m a n i fe s t a t i o n
with
negative
of
d i s t u rb e d
g y n a e co l ogi c a l
m e n a r c h e . Pa i n i s u s u a l ly fe l t i n the l o w b a c k a nd
i n the
abdome n .
Not o n l y
is
t h i s type
of p a i n
a m e n a b le t o ma n i p u l a tive t r e a t m e n t ; i t i s freq u e n tl y
t h e first s i g n o f d i s t u rb e d fu n c t i o n i n t h e l u m b o s a c r a l
reg i o n i n wo m e n .
p a t i e n ts w i t h seve re n e u ro l o g i c a l d i s e a s e . I n 1 420
True l u m b a g o i s m u c h l e s s fre q u e n t i n c h i ld h oo d ,
patie n ts with d i s se m i n a ted scle ros i s , Sc h a l te n b r a n d
b u t t h e r e e x i s t r a re c a s e s o f t r u e d i sc h e r n i a ti o n a s
( 1 938) fo u n d 22 . 3 % to be s u ffe r i n g from b a c k a c h e .
e a r l y a s p u be rt y . W i t h t h e exce p t i o n o f a c u t e w r y
I n o u r e x p e r i e n c e b a c k a c h e i s t h e r u l e i n P a r k i n so n ' s
n e c k , d i s t u rb a n ce of fu ncti o n i n t h e sp i n a l co l u m n
d is e a se ,
m a n i fe s t s
u nd e rs t a n d a b l y
in
view
of
the
m u sc l e
rigi d i ty i n t h i s co n d itio n . However, n o m a t t e r h o w
s e v e r e t h e n e u rologica l d i sord e r , i t is n o t t a n t a ­
m o u n t to p a i n
due
fu n c t i o n o f t h e
colu m n , s u c h
restricted
to d is t u r b a n ce o f a
m o t o r system a n d
as
i ncreased
m o b i l i ty
of
a
or
joint
t h e ve r t e b r a l
(more
or
s p ec i fi c
fre q u e n tly)
s p i n al
motor
i t s e l f i n d i re c t l y ,
for t h e m o s t
p a rt
as
h e a d a c h e , a n d i n you n g g i r l s a s a l go m e n o rr h o e a .
For
this
reason
I
was
i nt e rested
to
see
how
freq u e n t l y d i s t u r b a n c e s o f fu n c t i o n c o u l d be fo u n d
i n c h i ld r e n o f d i ffe r e n t a g e g r o u p s . T h e m o s t s t r i k i n g
p he n o m e n o n fo u n d espec i a l ly fre q u e n tl y i n c h i l d r e n
a nd a d o l esce n ts i s p e l v i c d i s t o r t i o n w h i c h i s d e a l t
w i t h i n l a t e r c h a pters. I fo u n d i t i n 1 1 o f 8 0 c h i l d r e n
segm e n t .
( 1 4--41
D isturbance of fu nction ( blockage)
in ch ildhood
m o nt h s o l d ) ex a m i n e d i n cre c h e s , i n 8 1 o u t
o f 1 8 1 c h i l d r e n ( a g e d 3-6 y e a rs ) i n n u rs e ry s c h o o l
and in
1 99
o u t of
ages o f 9 and
15.
459
s c h o o l c h i l d re n b e t w e e n the
S t a t is t i c a l e v a l u a t i o n s h o w e d no
s i g n i fi c a n t d i ffe r e n c e between t h e i n c i d e nc e i n boys
From w h a t h a s b e e n s a i d it fo l l ows t h a t d i st u r b a n c e s
of function m a y
(J )
and g i r l s . From n u rs e ry s c h o o l age o n w a rd s , p e l v i c
by t h e m s e l v e s c a u s e sym p t o m s
d i s t o r t i o n i s fo u n d i n a b o u t o n e - t h i rd t o o n e - h a l f o f
a n d (2) a p p e a r m uch s o o n e r t h a n struct u r a l ( m o r ­
t h e c h i l d re n . I n c o n t r a s t , I fo u n d m o ve m e n t restric­
p h o l ogica l ) c h a n g e s . Fo r t h i s r e a s o n I h a v e b e e n
t i o n in the cerv i c a l s p i n e ( m a i n l y a t the c r a n i o c e r v i c a l
p a r t i c u l a rl y i n t e re s t e d i n d i s t u rb a nces o f f u n c t i o n i n
j u n c t i o n ) i n n o n e o f t h e i n fa n ts i n c r e c h e s , i n o n l y
c h i l d h ood . Sch o n ( 1 95 6 ) a n d l a t e r G u t m a n n a n d
e i g h t o u t o f 1 8 1 n u rsery-sc h o o l c h i l d re n , a n d i n 7 3
W o l ff ( 1 95 9 ) h a v e s h ow n t h a t c l i n i c a l s y m p t o m s a s
out of
we l l as cha nges i n f u n c t i o n v i s i b l e i n c i n e r a d i o ­
459
schoolch i ldren o v e r t h e a g e of 9 years.
The s e i n v e s t i ga t i o n s d a t e fro m 30 y e a rs a g o , w h e n
gra phic s t u d i e s a p p e a r a b o u t 1 0 y e a r s e a r l i e r t h a n
t h e t e c h n i q u e o f exa m i n a t i o n fo r t h e u p p e r c e rv i c a l
d e ge n e ra t i v e c h a n ge s .
s p i n e was much less sophisticated than i t is today.
T h e m o s t t y p i c a l v e r t e b roge n i c l e si o n i n chi l d r e n
i s a c u te wry n e c k .
A l th o u g h i t i s a se l f- l i m i t i n g
co n d i t i o n , t r a c t i o n a n d m o b i l i z a t i o n tec h n i q u e s , i f
Our
c u rre n t
tec h n i q u e s ,
cli n ica l
has
shown
experience,
that
pelvic
using
s u b t ler
d i s torti o n
in
c h i l d re n goes h a n d i n h a n d w i t h b l oc k a g e , m a i n l y a t
Copyrighted Material
22
Manip uia live Therapy in Rehab iiilalioll of
Ih e Locotl1 o/Or Syslem
the a t l a n to-occ i p i t a l j o i n t , a n d a l so t h a t after m a n i ­
p u l a t i o n o f t h i s j o i n t , pelvic d is t o r t i o n d i s a p p e a rs. I n
1 98 2 I the refore exa m i n e d a g ro u p of 7 5 n u rsery­
school c h i l d r e n ( aged 3-6 years) a n d fou n d p e l v i c
d is t o r t i o n i n 24 , of w h o m 23 h a d m o v e m e n t
restri ction a t t h e a t l a n to-occ i pi t a l j o i n t ' I n 1. 2 o f
t h e se m a n i p u l a t i o n w a s c a rried out ( a t l as-occi p u t ) ;
t h e pe l v i c d i stortion d is a ppe a red s i m u l ta n e o u s l y .
T h e r e i s thus good r e a s o n to be l ieve t h a t m o s t of
the c h i l d re n in w h o m we fou n d pelvic d istortion 30
y e a rs ago also s u ffe red fro m b l ockage at t h e cra n i o ­
cerv i ca l j u n c t i o n . S o m e scoli otic deform i ty w a s
fo u n d i n 1 7 5 o f the 4 5 9 schoo l c h i l d re n t h e n e x a m i ned,
i n 1 5 out o f the 1 8 1 n u rse ry-school c hi ldre n . a n d in
o n l y one of the 80 c h i l d re n i n c rech es.
T h e pri m a ry i m portance o f t h e c r a n iocervica l
j u nction is i n keeping w i t h import a n t observ a t ions
by K u b i s , con fi rmed i n 1 093 new-born b a b i e s by
S e i fert ( 1 975 ) . Post u ra l n e c k reflexes ca n be e x a m i ned
i n the n e w b o r n : o n t u r n i n g the head to one s i d e , t h e
pe l v i s t u rns t o t h e opposite s i d e i f t h e c r a n i ocerv ical
j u nction fu nctions nor m a l l y . [ t was a b norma l in 298
o f t h e 1093 ex a m i ne d . In 5 8 per ce n t o f t h i s group,
using the normal tec h n i q u es , Se i fert d i a g n osed
b l ockage a t t h e cra n i ocervica l j un c t i o n , betwee n t h e
ages of 4 a n d 9 m o n t h s . A n o t h e r i m p o r ta n t gro u p
of c h i ld r e n of a l l ages w h o showed blockage m a i nly
of t h e a t l a n to-occ i p i t a l j o i n t a re t hose with re la psi ng
o r c h ro n i c t o n s i l l i t i s : i n a group o f 7 6 such
cases e xa m i ned and fo l l owed up by L e w i t a n d
pelvic d i s t o r s i o n
35
A b r a h a m o v i c ( 1 976 ) , 70 ( 92 p e r ce n t) h a d m o ve­
ment restrict i o n at the c ra n ioce rvical j u nctio n ,
m a i n ly at t h e CO-C 1 l e v e l .
I n o r d e r to esta b l i s h w h e t h e r these fi n d i ngs i n
c h i l d r e n a r e fort u i to u s or fa i r ly consta n t , a gro u p o f
chi l d re n w h o s t a rted sc hoo l a t te n d a nce i n 1 960 w e r e
systematica l l y fol l owed u p fo r 8 years ; h a l f the
n u m b e r s h owing some i m p a i re d function were
trea ted , a n d t h e o t h e r h a l f l e ft as con t ro l s . [ n
a d d i t i o n t o t h e s p i n a l col u m n , t h e extre m i t i es a n d
parti c u l a rly t h e m usc u l a t u re were t h o rough l y tested.
The res u l t s a re given in Figure 2 . 1 4 , t h e m ost
i m port a n t fi n d i ng b e i n g t h a t , w i t h few excepti o n s ,
Cha nges i n t h c function o f t h e p e l v i s a n d of t h e
c ra n i ocervi cal reg i o n re m a i ned const a n t i f not
t reated. O n the o t h e r h a n d , t he re were on l y a few
re l a ps e s afte r tre a t m e n t .
F r o m t h i s i t follows t h a t cha n ges i n t h e
functio n i ng o f t h e s p i n a l co l u mn a n d t he l o c o m o t o r
system cause s y m p t o m s far more fre q ue n t l y t ha n is
ge nera ll y a ss u m e d , even in c h i l d re n . M u c h more
freq u e n t l y , however. th ese lesions a re c l i n ic a l l y
l a te n t . Pelvic d i stortion p l u s u p p e r cervical lesions
a re fou n d in m o re t h a n a t h i rd of all s c h o o l c h i l d re n .
M u sc u l a r i m b a l a n ce is eve n m o re freq u e n t , a l t hough
less cons t a n t . I t can further be i n fe r red t h a t :
1.
Disturba nce o f fu n c t i o n a p pe a rs Ill uch e a r l i e r i n
t h e locomo t o r system t h a n do dege n e ra t i v e
m o rp h o l ogica l c h a nges.
scoliosis
�__________-J
A
�__________�
I
0;
.D
'"
-
30
.£
E
:l
c:
25
20
d i f f e re n c e
cervi c a l
i n leg l e n g t h
blockage
�
15
�
10
5
0
Fi g u re 2.14 Fol low- u p s t u d i e s ov e r 6 y e M s of 72 schoo l c h i l d re n of t h e s a m e age , cov e r i n g i n c i d e n ce of p e l v i c t o rsion ,
c e r v i c a l b l ockage
sco l i os i s , d i ffe r e n c e i n l e g l e n g t h a n d
Copyrighted Material
23
Theoretical consider(llions
2. T h i s d i stu rba n c e , a lo n e , c a n c a u s e s y m p t o m s
w i t h o u t s t r u c t u ra l c h a nge s .
t h e s e q u e l a e of t ra u m a are u s u a l l y more seve re in
s t r u c t u re s with dege n e ra t i v e c h a n ge s . I n d e e d , q u i te
freq u e n t l y w h a t a re c a l l ed dege n e ra t i v e c h a n ge s are
i n re a l i ty a n a t t e m p t to compe n s a t e d y s fu n ct i o n .
Th e y a r e t h e n tes t i m o n y t o p re v i o u s d a m a ge . O n e
Poss i b l e conseq u e n ces of
b l o c k a g e in t h e vertebra l m ot o r
seg ment
i m po r t a n t c o m p l i c a t i o n o f d eg e n e r a ti o n c a n b e disc
pro l a p s e ,
but h e re
again
we
find
a comp licated
r e l a t i o ns h i p betw e e n s t r u c t u r a l c h a nge a n d a l te r e d
fu n c t i o n : we k n o w t h a t e v e n d isc p r o l a pse m a y b e
I f b lockage occurs i n t h e s p i n a l col u m n o f a c h i J d o r
a n a d o l esce n t , a t fi rst s i g h t t h e c o n se q u e nces m a y
seem re l a t i v e l y i n s i g n i fi c a n t : t here m a y b e s o m e
tra n s i t o r y p a i n , as i n wry n e c k , b u t i n t h e s p i n e ,
u n l i ke
t h e e x t re m i ty j o i n t s , fu n c t i o n is re a d i l y
compe n sa te d b y n e i g h bou r i n g o r e v e n d i s t a n t m o t o r
segm e n t s . a n d t h e l e s i o n rem a i n s m a s k e d fo r a v e r y
l o n g t i m e . The re i s , howe v e r , a pri ce t o b e p a i d fo r
t h a t com p e n sa t i o n : i n c reased d e m a n d s on t h e
c o m p e n sa t i n g s tr u c t u r e s , w i t h possi b l e d ysfu n c t io n .
A good ex a m p l e is h e a d rota t i o n w b e n t h e re i s
c o m p a t i b l e w i t h a b sence o f s y m ptoms, a n d i t m a y
be a d is t u rbance of fu n c t i o n on top of th a t w h i c h
m a kes
the
lesion
m a n i fe s t .
On
re s to r i n g correct fu n c t i o n i n
a
the
oth e r h a n d ,
bloc k e d j o i n t , for
e x a m p l e , m a y p r o d u c e com pensa t i o n .
T h a t a l tered f u n c t i o n m a y be i m p o r t a n t i n n e rve
c o m p ressio n ( e n t r a p me n t s y n d ro m e s ) we have s e e n
in
the
c a rpa l
particularly
in
tunnel
the
syn d ro m e
initial
stages.
(see
On
p.
267 ) ,
thoro u g h
e x a m i n a t i o n we re g u l a rl y fi n d i n creased res i s t a n ce
to j o i n t p la y o f t h e carpa l b o n e s . W h e n j o i n t p l a y i s
block age b e t w e e n a t l a s a n d a x i s A l t h o u g h t h e j o i n ts
resto red , t h e s y mp to m s d i s a p p e a r a t t h i s s t a g e . I n
between t h e a t l a s a n d t h e a x i s are a d m i ra b l y s u i ted
to ro t a t i o n , t h e rest o f t h e ce r v i c a l s p i n e is not.
The refo re head rota t i o n ca r r i e d out w i t h a bJocked
a t las-a x i s mov e m e n t c a n be d e e me d a d y s fu n c t i o n ,
a n d e v e n m o r e so w h e n t h e restricted m o v e m e n t i s
n o t sym m e t rica l . Q u i te obv i o u s l y , m ov e m e n t restric­
tion in o n e se g m e n t p ro d u ces h y p e r mo bi l i ty in
a n o t h e r, and i n ge n e r a l , a s we h a v e see n , the
conseq u e n ce s of d y s f u n c t i o n w il l b e m os t m a r k e d if
fu n c t i o n i s d i s t ur be d in key r e g i on s .
O s teop h ytes a re t he typica l c o n se q u e nce of lo ng­
lasting ove rstra i n , nor i s b l ockage w i t h o u t co n s e ­
q u e nce s , fo r , a s we we l l k n o w , m u c h o f t h e l i t t l e ­
vascu l a r i ze d tissue o f c a r t i l age a n d d i scs d e p e n d s o n
move m e n t fo r i t s nu t r i t ion . R a d i o l o g y s u p p l i e s
a m p l e e v i d e n ce o f reg u l a r o s te o p h y te fo r m a t i o n i n
t h e m o t or seg m e n t adj a ce n t to a c o n ge n i t a l b l o c k .
Func t i o n a l b l o c k a ge i n a n te - a n d re t r o fl e x i o n , a s
s e e n rad i ogra p h i ca l l y , i s as a r u l e acco m p a n i ed by
o t h e r word s , o n l y i f t h e re i s free m o b i l i t y be tween
.
dege n e ra t i v e c h a n ge s - n a rro w i n g of t h e d i sc - i n
the restricted segme n t , a n d by o s t e o p h y tes i n t h e
neighbo u r i n g h ype r m o bi l e s e g m e n t ( J i ro u t, 1 956) .
M U li e r
seg m e n t
( 1 960)
has
eve n t u a l l y
shown
that
becomes
this
hypermobile
blocked,
a nd
the
process spreads t o n e i g h b o u r i n g seg m e n ts . T h i s i s
u n d ers t a n d a b l e , f o r osteo p h y t e s a re r i n g s h a pe d a n d
have a st a bi l i z i n g func t i o n , as c a n b e s t be s e e n i n
sta b i l ized s po n d y l o l i s t h e s i s .
Dege n e r a t i v e c h a n ge s i n t h e m se l ve s n e e d n o t
p r o d u c e m a n i fe s t c l i n i c a l s y m p t o m s . The y d o , h o w ­
e v e r , m a k e t h e s p i n a l co l u m n m o re s u sce p t i b l e t o
f u r t h e r d a m age. I t i s a g a i n d i s tu rbed fu n c t i o n t h a t
esta b l i s h e s i ts e l f more e a s i l y i n a structure a l re a d y
ma rked by dege n e ra t ive c h a nges; i n o t h e r w o r d s , i f
t h e bo n e s for mi n g the t u n n e l ca n t h e walls a d a p t
t h e mselves to t h e c o n t e nts o f t h e t u n n e l u n d e r
v a r y i n g co n d i t i on s of s t r a i n
should
not
fo rget
that
part
a n d movem e n t . W e
of t h e
wall
of the
i n te v e rtebral c a n a l w h e re r o o t c o m press i o n occu rs
is a l so the a po p h y s e a l j o i n t .
F i g u re 2 . 1 5 s u m m a rizes t h e m e c h a n i c a l fac t o r s i n
t h e p a th oge n e s i s o f bloc k a g e .
T h e s i g n ifica nce of d i stu rbed
m ovem ent patter n s (stereotypes)
T c o n si d e r d is t u r b e d m o v e m e n t p a t t e rn s a s t h e m o s t
i m porta n t s i n g l e c a u s e o f b l oc k a g e , a n d re m e d i a l
e x e rcise i s t h e n t h e t h e ra py o f c h o i c e . R e m e d i a l
exe rcise is w i d e l y reco m m e n d e d i n p a i n f u l v e r t e b ro­
genic c o n d i t i o n s , but w h a t is m e a n t by the t e r m i s
m u c h l e s s c l e a r , s i nce we a re n o t d e a l i n g h e re w i t h
o b v i o u s p a r e s i s , d efo r m i ty o r w e l l - d e fi n e d loco­
m o to r l e s i on ( w i t h t h e exce p t i o n of blockage, w he re
se l f- t r e a t m e n t exercises c a n be t a u g h t to t h e p a t i e n t ) .
W e h a ve J a n d a ( 1 97 5 ) t o t h a n k for s h e d d i ng l i g h t
o n t h i s p r o b l e m . T h e m a i n obj ect o f re m e d i a l e x e r ­
c i s e i n d i s t u r bed f u n c t i o n o f t h e l ocomotor s y s t e m
i s t h e corre c t i o n of fa u l t y p a t te r n i n g ( fa u l ty
l o c o m o t o r stereoty p e s ) , i . e . fa ulty coord i n a t i o n o f
m u s c l e f u n c t i o n d u e to d i s t u rbed c e n t r a l n e r v o u s
c o n t r o l . U n fo r t u n a t e l y fo r t h e sys t e m a tica l l y m i n d e d ,
m o v e m e n t pa tterns a r e h i g h l y i n d i vi d u a l m o t o r
progra m me s , fo r m e d by e a c h s u b j e c t i n t h e course
of h i s l i fe o n the basis of c h a i n s o f u n co n d i t i o n e d
a n d a c q u i re d (co n d i t i o n e d ) r e fl e x e s . T h e re is t h e re ­
function re m a i n s c o m p e n s a te d i n a s p i n a l col u m n
fo re gre a t v a r i a b i l i t y , a n d the l i m i ts of t he norm a r e
w i t h dege n e r a t i v e c h a n g e s , a s a r u l e n o s y m p t o m s
v e r y broa d . I n fac t , t h e w a y e a c h i n d i v i d u a l m o v e s
w i l l a r i s e . S u c h a s p i n a l col u mn , h o w e v e r , is m o r e
i s so c h a racte r i s t i c t h a t we c a n recogn i z e h i m b y h i s
l i a b l e t o d e co m pe n s a t i o n . T h a t i s w h y , fo r i n s ta nce ,
ga i t , h i s gestures, t h e way h e writes, a n d so o n .
Copyrighted Material
24
Manipula ti v e Therapy in Rehab ilitation of th e Locomotor System
F a u l ty m u sc l e
Visceral lesion
p a tt e r n
o f co rresp o n d i n g
segment
\
\
I
\
I
'"­
\
\
'-
/
B l ockage
I
I
/'
( i f p ri m a ry i n
\
k e y re g i o n )
\
\
\
/
I
I
I
t
I
I
I
I
I
S o ft t i s s u e a n d
C l i n i c a l d e c o m p e nsat i o n
degene rative
c h a n g es
( e . g . d i sc p r o l a p s e )
Figure 2.15 P a t h o g e n e s i s : p r o b a b l e c a u s e s a n d cons e q u e n c e s o f b l o c k age
Idea l l y , l o c o m o t o r p a t t e r n s s h o u l d a l low m o v e m e n t
of h i p e x t e n s i o n w i t h t h e a i d o f t h e h a m s t r i ngs a n d
t o b e a s e co n o m i c a l a s poss i b l e , i . e . t o c o n s u m e t h e
t h e e r e c t o r s p i n a e m a y re m a i n n o r m a L w h i l e t h e
s m a ll e s t possible q u a n ti ty o f e n e rgy.
p a t t e r n i s g re a t l y c h a n g e d , w i t h i m po r t a n t conse­
H e r e , a s i n m a n y o t h e r s i t u a t i o n s , i t is a b n o r m a lity
q u e nces for l o co m o t o r fu n c t i o n , as we s h a l l see l a te r .
that provides t h e rel e v a n t clues: e v e n a l a y m a n w i l l
Secondl y ,
recog n ize a n a w k w a rd p e r fo r m a n c e , w h i c h m o re
s u rp r i si n g l y
tes t i n g
o f t e n t h a n n o t is ta n t a m o u n t to a n u n e co n o m i c a l
m u s c l e s a lw a y s s h owed a te n d e n cy t o l e s s e r a c t i v i t y
o n e . T h e l a y m a n w i ll o fte n b e a b l e t o correct w h a t
( w e a k n es s ) a n d h y p o to n i a , w h e re a s o t h e rs t e n d e d t o
constan t
these
simple
pattern
m o v e m e n ts ,
e m e rged .
a
C e rt a i n
h e s e e s - fo r insta n c e , s p o r t s t r a i ners d o so d ur i n g
hypera c ti v i ty , i n creased te n s i o n a n d e v e n t a u t n es s ,
their work.
w h i c h ca used a t y p i c a l m o t o r i m b a l a n ce . T h i s i s so
I n p a t i e n ts w i t h c h r o n i c v e r te b r o ge n i c p a i n a n d
a w k w a rd move m e n t s , J a n d a
( 1 972)
a p p l ie d t h e c l a s s i c
c h a ra c te r i s t i c t h a t we can now d e te r m i n e s y n d romes
t h a t a re o f c l i n i c a l i m p o r t a n ce . T h e y a re c h a racter­
m us c l e test to i n d i v i d u a l m us c l e s . T h i s re v e a l e d t w o
istic for i n d i v i d u a l p a t i e n ts : i n s o m e cases t h e re is a
s i gn i fic a n t f a c t s . F i r s t , t h e s i m ple test m o v e m e n ts
pre p o n d e r a n c e of w e a k n es s , fl a b b i n es s g oing h a n d
b e l i e v e d to be c h a ra c t e r i s t i c fo r a s pe c i fic m u scle
i n h a n d w i t h hypermobili t y , w h e reas i n o t h e rs t a u t ness
g r o u p a re m o re often t h a n n o t p a t t e r n s in w h i c h
w i t h i n creased m u s c l e t e n s i o n prev a i l s . It is t h u s
a
is
p o s s i b l e to d r a w u p u s e fu l l i sts o f m uscles ( m uscl e
by
groups) t h a t s h o w a t e n d e ncy to h y p e r a c t i v i t y , a n d
gre a ter n u m be r of m u sc l e s take
co m m o n l y
thought.
Ex a m i n i n g
h ip
part than
extension
p o l y e l ec t r o m y ogra p h y , J a n d a s h owed that hip exte n ­
o f t h o s e t h a t t e n d to i n h i b i t i o n (Ta b l e
2.1).
This d i ffe r e n c e i n t h e be h a v i o u r o f m u s c l e s c a n
s i o n i s n o t o n l y a t e s t fo r t h e gl u t e u s m a xi m u s
m uscl e , b u t t h a t t h e p r i m e m o v e rs i n h i p e x t e n s i o n
be s e e n
are t h e h a m s t r i n gs , a n d t h a t i n a d d i t i o n to t h e s e t w o
p a rticu l a rl y c h a r acteristic i n c o m m o n p a i n f u l s t a tes:
u n d e r v a r i o u s c l i n i c a l co n d i t i o n s a n d i s
m uscle g r o u p s t h e l u m b a r ere c t o r s p i n a e a l s o t a k e s
in a p a i nf u l hip i t i s a lw a y s t h e fl e x o rs a n d a d d u c t o rs
p a r t . T h e characteristic d i s turba nce o f h i p exte n s i o n
t h a t a re tense a n d t h e g l u t e i w e a k ; i n s h o u ld e r p a i n
i s d e c r e a s e d a n d b e l a te d a c t i v i t y of t h e g l u t e u s
m a x i m u s ( Fi g u r e
recogn i ze
2.16).
c l i nically
We h a v e n o w l e a r n e d t o
which
m uscles
take
part
in
s i m ple test move m e n ts , t h u s u s i n g t h e test to assess
not
only
m u scle
tight band.
co n s i d e r a b l y
s a m e t y p e o f m u scle w i l l be i n h i bi te d a n d freq u e n t l y
s u p e rseded b y m u s c l e s w i t h a t e n d e n c y to h y p e r -
may
be
q u a li t y
a
a l tered w i t h o u t m u c h c h a nge i n fo rce ; t h e s t r e n g t h
q u a l i ty
also
we a k , t h e r e c t u s fe m o ris re m a i n i n g l i k e
Co n d i ti o n s a re v e ry s i m i l a r i n fa t i g u e : aga i n t h e
Th i s
but
c h r o n i c p a i n fu l c o n d i t i o n s o f t h e k nee t h e v a s t i a re
of
pe rfo rm a n c e .
weakness,
t h e p e c to r a l i s a n d s u b sc a p u l a r i s a re t a u t w h e r e a s t h e
s u p r a sp i n a ti , i n fra s p i n a t i a n d d e l t o i d s a r e w ea k ; i n
Copyrighted Material
Theoretical considerarions
I NduI
25
8W. .inl
obi ..... .
abel.
cIx
Figure 2. 16 E l e c t r o m y o g r a m o f r i g h t h i p e x t e n s i o n : the r i g h t g l u t e u s maximus i s b r o u g h t i n to a c t ion l a te a n d l i t t l e :
m a r k e d a c t i v i t y i n t h e h a m s t r i ngs o n t h e righ t a n d the e re ctores s p i n a e o n b o t h sides: i n h i b i t ion o f t h e r i g h t g l u t e u s
maximus ( From V . J a n d a . perso n a l co m m u n ic a t i o n )
a c t i v i t y a n d t a u t ness . O n c l o s e r sc r u t i n y w e fi n d t h a t
a n d t h era py a re d e a l t w i t h in t h e relev a n t c h a p t e r s .
m u scles w i t h a t e n d e n c y t o i n h i b i t i o n a re t h ose t h a t
I t is i m p o r t a n t to p o i n t o u t , h o w e v e r , t h a t t rigge r
a re a lso i n h i b i t e d ( fl a b b y ) i n u p p e r m o t o r n e u ro n
lesi o n s , w h i l e t h ose w i t h a t e n d e ncy to h y p e r a c t i v i t y
po i n ts m a y occ u r in b o t h t y p e s of m u s c l e , o n e type
being
painfully
tense,
the
other
p a i n fu l l y
flabby
become s p a s t i c . N e u ro logica l l y , the typica l i m b a l a n c e
( i n h i b i t e d ) . I n both, h o w e v e r , these trigger poi n ts
i n fa u l ty moveme n t p a t t e rn s , e n h a nced by p a i n a n d
a re effe c t i v e l y t r e a t e d by post- i s o m e t r i c rela x a t i on .
fa t i g u e , m a y b e i n t e rp reted a s ' m icrosp a s t i ci t y ' .
Ex a m i n a t i o n of s i m ple m o v e m e n ts by a p p ly i n g
Those m u scles w i t h a t e n d e n cy to i n h i b i t i o n a re
t h e m u scle t e s t i s o n ly o u r fi rst s t e p ; o u r h a b i t u a l
ca l l e d by J a n d a ' p redomi n a n t l y p h a s i c ' , w h i le h e
m o ve m e n t s a re i n d i v i d u a l ly a c q u i r e d
ca l l s
h y p e racti v i t y
s t e r e o t y p e s w i t h a degree of p l a s t i c i t y , so t h a t t h e y
' p red o m i n a n t l y pos t u r a l ' . T h e s e t e r m s , w h i c h a re
a re c a p a b l e of be i n g tra i n e d . H o w e v e r , t h i s t r a i n i n g
m u scl e s
with
a
tendency
to
patterns or
s t i l l p ro v i s i o n a l , i n d i c a t e t h a t t h e re a l p h y s i o logical
is v e r y t i r i n g , p a r t i c u l a rl y a t fi r s t , t h e fa t i g u e s e e m i n g
b a s i s for t h e d i ffe r e n c e ,
o u t o f a l l p r o p o r t i o n to t h e e n e rgy re q u i r e d fo r t h e
which
i s c l i n ic a l l y very
st r i k i ng , i s n o t yet known. W i t h o u t going too d e e p l y
move m e n t f o r w h i c h t h e s u b j ect i s b e i n g t ra i n e d .
i n to the q u e s t i o n h e r e , i t s h o u l d b e s t ressed t h a t
Th i s
t h e s e g ro u ps d o n o t c o r r e s p o n d to t h e t y p e s o f
t h e m o re s o for t h e s i c k ; i t i s s o m e t h i n g t h a t m u s t
is
true
even
fo r
h e a l th y
s u b j e cts,
and
all
muscle fi b re d i s t i n g u i s h e d by m o d e r n n e u ro p h y s i ­
n e v e r be forgo t t e n i n p l a n n i n g re m e d i a l e x e rc i s e
ology, h i s t o l ogy a n d b i oc h e m is t r y . Cl i n i c a l d i a g n os i s
( r e h a b i l i ta t i o n ) .
Copyrighted Material
26
Manipulative Therapy in Rehabilitation of the Locomotor System
Table 2.1 Musc l e groups t hat show a tend ency to
fac i l i t a t e s sto o p i n g , w h i l e l o o k i n g t o t h e s i d e faci l i ­
hyperacth'ity o r inhibition
t a tes rota t i o n o r i n h i b i ts m o v e m e n t i n t h e opposite
d i recti o n . Furth e r m or e , a s s t r a igh t e n i n g o f t h e b o d y
Hyperactivity
is c o n n ected w i th
Inhibition
i n h a l a ti o n ,
and
stooping w i t h
e x h a l a t i o n , i t i s e no u g h fo r t h e p a t i e n t t o l o o k u p to
fa c i l i ta t e i n h a l a t i o n a n d i n h i b i t e x h a l a t i o n , and v i ce
On the dorsal aspect of the body
Tr iceps su rae
G l u t e a l m uscles
H a ms t r i ngs
Tra pez i u s
L u m b a r s e c t i o n o f t h e e rector
Serratus l a teral i s
spinae
(lower
v e r s a . Th i s , as we s h a l l see, p l a y s a cruci a l pa rt i n
part)
t h e m o d e rn n e u ro m u s c u l a r tec h n i q ues most useful
fo r m o b i l i z a t i o n .
S u p r a - a n d i n fras p i n a t i
Q ua d ra t u s l u m b o r u m
D e l to i d
R e t u r n i n g t o t h e q u e s t i o n o f i mba l a nce o f muscle
groups,
M iddle and upper trapezius
with
the
p re d o m i n a n t l y
p ha s i c
m us c l e s
i n h i b i ted and t h e p r e d o m i n a n t l y post u ra l m u s c l es
Le v a t o r sca p u l a e
o v e r - a c t i v e , i t is e asy to s e e t h a t t h i s m u s t s e r i o u s l y
i n te r fe r e w i t h coord i n a te d l ocom o t o r p a t t e r n s . T h i s
On t h e ventral aspect of t h e body
i s p a r t i c u l a r l y so a s i n m a n y i n s t a nces t h e y a re
Ti b i a l i s a nterior
Th igh a d d uctors
a n tagon i s t s , t h e h y p e r a c t i v e m u scle t h e refore h a v i n g
E x t e n sors o f t h e toes
R e c t u s fe m o r i s
Te n s o r fas c i a e l a t a e
Pe ro n e i
a n i n h i b i to r y e ffect o n i t s w e a k a n t ago n i s t . Hyper­
I l i opsoas
Vast i
a c t i v e l u m b a r erectores s p i n a e w i l l u n fa v o u r a b l y
a ffec t w e a k a b d o m i n a l m us c l e s , a n d h y p e r a c t i ve h i p
Pectorales
Rect us a b d o m i n i s
S u bsca p u l a res
D e e p n e c k flexors
Scalenes
D i gastricus
fl e x o rs w i l l i n fl u ence w e a k g l u t e i .
S te r n o e l e i d o m a s t o i ds
The pathoge n ic mechanism of
d isturbed movement patterns
M a s t i c a t ory
On tile arms
F l e x o rs
E x t e n sors
H a v i n g e x p l a i n e d w h a t m o v e m e n t p a tterns a re a n d
h o w t h e y c a n b e d is t u r b e d by i m b a l a n ce o f spec i fi c
m u s c l e gro u p s , I n o w t race t h e m ec h a n i s m s b y w h ic h
T h e co n c e p t of p a t t e r n i n g is a v e r y importa n t o n e ,
d i s tu rb a nces o f t h e m o s t i m p o rta n t m u s c l e p a t t e r n s
a n d c a n c h a n ge o u r v i e w o f t h e d i ffe rence b e t w e e n
( s t e r e o types ) w i l l h a v e a d e l e t e r i o u s e ffect o n t h e
ago n i s ts a n d a ntago n i sts q u i t e decisively. For e x a m p l e ,
l o c o m o to r s y s te m .
t h e h a m s tr i ngs a n d t h e q u a d r i c e p s c a n be c o n s i d e re d
a s a n tago n i sts
i f we
a r e t h i n k i n g o f the s i m p l e
m o v e m e n t of k n e e fle x i o n . Howeve r , t h e m o v e m e n t
Wa l k i n g a n d sta n d i n g
o f w a l k i ng i s m u c h m o re com p l e x t h a n s i m p l e be n d i n g
H e re t h e m o s t i m po r t a n t i m b a l a nce is between w e a k
a n d s t r e tc h i n g o f t h e k n ee ; d u ri ng w a l k i ng b o t h
gl u t e a l m u scles w i t h h y p e ractive h i p A e x o r s , a n d
t h ese m us c l e s h a v e to c o n t r a c t a n d t o c o o rd i n a te a s
hyperactive
s t a bil i zers o f t h e k n e e . T h i s i s e q u a l l y t r u e o f t h e
a bd o m i n a l muscles. I n s t a n d i n g we see i n creased
a b d o m i n a l a n d b a c k m u s c l e s , a n d o f t h e fl e x o r s a n d
pelvic tilt and
e x te n s o r s o f t h e n e c k . I n fa c t , i n we l l - c o o rd i n a te d
lumbar
a
e rectores
spinae
with
weak
protruding a b d o m e n .
The p a t h o g e n i c m e c h a n i s m i s t h i s : s t a n d i n g p l aces
s t r a i g h t e n i n g u p fro m a s t oo p i n g pos i t i o n i t i s t h e
an i ncreased loa d o n the l u m b a r spi n e , a s even w h i l e
a b d o m i n a l m u sc l e s t h a t h a v e t h e d e c i s i v e rol e . I t i s ,
s ta n d i n g a t ease t h e re i s h y pe ractiv i ty o f t h e b a c k
t h e re fo r e , a g r a v e m i s t a ke i n re m e d i a l exercise t o
muscles;
t ra i n t h ese m u scles s i m p l y accord i n g to t h e res u l ts
p e r fo r m e d by t h e i n h i b i te d g l u t e i m a x i m i , b u t b y
o f t h e m u s c l e t e st, a n d n o t w i t h regard to t h e i r
t h e l u m b a r e rectores s p i n a e , c a u s i n g h y p e r l o rd o s i s
fu nct i o n i n t h e v i ta l s t e reotype c o n c e r n e d .
i ns t e a d of e x te n s i o n o f t h e
when
w a l k i ng,
hip
exte n s i o n
is
hip joint - t h a t
not
is,
is
t he r e is i nc r e a s e d s t ra i n o n t h e l u m b a r s p i n e , d u e to
i m p o r ta n t to re m e m b e r t h a t t h e y fu n c t i o n l i k e a
h y pe r m o b i l i ty in the s a g i t t a l p l a n e . T h i s i s gre a t l y
In
t ra i n i ng
correct
movement
pa tterns
it
' p rogra m m e ' t h a t c a n be read i l y fac i l i t a ted o r t r i g­
e n h a nced by t h e wea k g l u te i m e d i i ; w h e n t h e pa t i e n t
g er ed if t h e correct a ffe re n t i m p u l se s a re e m p l oye d .
s ta n d s o n o n e l e g these musc l es s ta b i l i ze t h e p e l v i s
F o r e x t r e m ity m o ve m e n ts , m o s t receptors a re o n t h e
i n t h e c o ro n a l p l. a n e ; i f t h e s e m u scles a re w e a k , t h e re
pe r i p h e ry , i . e . t h e fi n gers a n d toes. To fac i l i ta te
is i n c r e a s e d s w a y i n g of the pe l v i s , c a u s i n g l u m b a r
w a l k ing i t is i m p o r t a n t fo r t h e p a tie n t to t h i n k a b o u t
h y pe r m o b i l i ty i n t h e c o r o n a l p l a n e .
l i ft i n g h i s b i g t o e ; h e w i l l t b e n a u t o m a t i c a l l y d o r s i fl e x
t h e foot, a n d b e n d t h e k n ee a n d
h i p . S i m i l a rl y ,
fl e x i o n of t h e fi n ge r s w i l l trigge r fl e x i o n i n t h e e l b o w
a n d s h o u l de r . W h a t t h e fi n gers a n d t o e s a re fo r t h e
Stra i g hten i n g u p f r o m a stoop i n g
posit i o n (wei g ht lifti n g )
e x t re m i ti e s , t h e e y e s a re fo r t h e t r u n k : l o o k i n g u p
I f the tru n k i s i m a g i n e d a s a s t r a i g h t l e v e r d u ri n g
fa c i l i ta te s s t r a i g h t e n i ng of t h e b o d y , l o o k i n g d o w n
w e i g h t l i ft i n g a n d t h e LS-S l d i sc as t h e fulc r u m ,
Copyrighted Material
Theoretical considerations
fo rces act i n g on i t of up to a b o u t lOOO k Pa h a v e b e e n
c a l c ul a ted ( M a t t h i a s c h , 1 95 6 ; M o r r i s , 1 973 ) . S u c h a
force
would
crush
the
d i sc .
Nachemson
( 1 959)
27
The role of respiration in
locomoto r d isturbance
m e a s u red i n t r a d i sc a l pressu re in v a r i o u s posi t i o n s of
fo u n d t h a t t h e m a x i m u m p r e s s u r e
Th i n k i n g of b r e a t h i n g , o n e n a t u r a lly h a s in m i n d t h e
d u r i ng w e i g h t l i ft i n g was a b o u t 275 % o f t h a t i n t h e
res p i r a to r y s y s te m . Y e t i t i s t h e loco m o t o r s ys t e m
the body and
u p r i g h t posi t i o n , i . e . i t w a s 340 k P a .
that
Th e reason ( a ccord i n g to G racovets k y , 1 988) l i e s
makes
t h e l u ngs
work,
and
the
loco m o t o r
s y s t e m t h a t h a s to coord i n a te t h e specific r e s p i r a t o r y
to w h i c h
m o v e m e n t s w i t h t he rest o f t he b od y ' s locomotor
n o t o n l y t h e b a c k m u s c l e s a t t a c h b u t a l so t h e g l u t e i
a c t i v i t y . This t a s k i s s o c o m p l e x t h a t it would b e a
and
m i r a c l e i f d i s tu rb a n ces d i d n o t o cc u r .
in
t h e r o l e of t h e
i n d i re c t l y t h e
w h ich
l u m bodors a l
fasc i a
h a mstrings a s w e ll , a n d fro m
t h e s p i n a l co l u m n
is
' s uspended '
that
I t i s w i d e l y h e l d t h a t m u sc u l a r a c t i v i t y i s fac il i t a te d
fu r t h e r e n ­
d ur i n g i n h a l a ti o n a nd i n hibited d u r i n g e x h a l a t i o n ,
ha nced by t h e coo rd i n a ted a c t i v i ty o f t h e a b d om i n a l
b u t t h i s i s a n o v e rs i m p l i fi ca t i o n . T h e a b d o m i n al
leve rage i s e l i m i n a te d . T h i s m a y be
m u s c l e s w h ich h e l p t h e t h o r a x
so
to a p p ro a c h t h e
m u s c l e s m a y be a c t i v a t e d by ex h a l a t i o n , e s p e c i a l l y
e x h a l a t i o n a g a i n s t resis t a n c e . r h a ve a l re a d y m e n ­
s u p po r t i n g p e l v i s .
tio n e d t h e c l os e c o n n ec t i o n b e t w e e n l oo k i n g u p ,
i n h a l a ti o n
Lift i n g t h e a r m s
and
s t r a i g h ten i n g
of
the
body,
and
b e t w e e n loo k i n g d o w n , e x h a l a ti o n a n d s t o o p i n g .
H e r e t h e dec i s i v e fa c t o r i s c o r re c t fi x a t i o n o f t h e
Th i s , h o w e v e r , a p p l i e s on l y t o t h e c e rv i c a l
s ho u l d e r g i rd l e ; t h i s i s t h e fu n c t i o n o f t h e u p p e r p a rt
l u m b a r s p i n e ( w h ich a r e decisive i n v i ew o f t h e i r
and
of t h e t r a p ez i u s m u s c l e a n d t h e l e v a t o r sca p u l a e
g r e a t m o b i l i t y ) a n d l e s s to t h e t h o r a c i c s p i n e . H e re
from a bove , a n d o f t he l o w e r p a r t o f t h e t r a p e z i u s
it is m a x i m u m i n h a la t i o n t h a t fac i l i t a tes fl e x i o n i n a
m usc l e a nd t h e s err a t u s l a te r a l i s f r o m b e l o w . t h e fi r s t
k y p hotic posi t i o n
t w o m u scles being a t t a c h e d to t h e c e r v i c a l s p i n e a n d
faci l i t a tes e x te n s i o n in a l o r d o t i c p o s i t i o n , i . e . t h e
t h e l a s t t w o to t h e t h o r a c i c s p i n e .
t h o racic e x t e n s o r s p i n a e contracts, a n d th i s to s u c h
and
maximum
e x h a l a ti o n
that
The m u scu l a r i m b a l a nce fo u n d h e re i s w e a k n e s s
a n e x t e n t t h a t d e e p i n h a l a t i o n i s p ro b a b l y t h e m o s t
o f t h e l o w e r part o f t h e t ra p e zi u s a n d s e r r a t u s
effect i v e m e t h o d o f m o b i l i z i n g t h e t h o ra c i c s p i n e
l a t e ra l i s , w i t h h y p e r a c t i v i t y o f the u p per p a r t o f t h e
trapez i u s a n d of t h e l e v a t o r sca p u l a e , res u l t i n g i n
i n to fl e x i o n , a nd m a x i m u m e x h a l a t i o n m o s t effe c t i v e
fo r ex ten s i o n .
overstra i n of the c e r v i c a l s p i n e .
The
m o s t s u rp r i s i n g
e ffect
of
i n h a lation
and
e x h a l a ti o n , however, i s t h e a l te r n a t i n g fac i l i t a t i o n
a n d i n h i b i t i o n o f i n d ivid u a l segme n t s o f t h e sp i n a l
Wei g ht c a r ryi n g
co l u m n
d u ri n g
s i d e-bendi n g ,
d i sc o v e red
by
H e re t h e posi t i o n o f t h e s h o u l d e r j o i n t i s c r u c i a l : i f
G a y m a n s ( 1 980) . I t c a n b e regul a r l y s ho w n t h a t
t h e s h o u l d e r o f t h e w e igh t- b e a r i n g a r m i s be h i nd t h e
d uring
l i n e o f g r a v i ty o f the b o d y , t h e s h o u l d e r g i rd l e i s
c e r v i c a l as w e J l a s i n t h e t h o r a c i c s p i n e i n t h e e v e n
side-bending
resistance
increases
in
the
fixed i n s u c h a w a y t h a t very l i tt l e or n o w e i g h t i s
segm e n ts ( occi p u t-a t l a s , C 2 , e t c . , a n d a ga i n i n TI ,
b o rn e by t h e u p p e r fi x a t o rs o f t h e s h o u l d e r g i r d l e
T4 , e t c . ) d u ri n g i n h a l a t i o n ; d u r i n g e x h a l a t i o n we
( th e u p p e r p a rt of t h e t r a p e z i u s a n d t h e l e v a t o r
o bt a i n
sca p u l a e ) . I f t h e s h o u l d e r i s d ra w n fo rw a r d , o n t h e
Co n v e rse l y , r e s i s t a n c e i n c r e a s e s i n t h e o d d seg m e n t s
a
m o b i l iz i n g
effect
in
these
s e gm e n t s .
o t h e r h a n d . w e i g h t i s immed i a t e l y t r a n s m i t ted to t h e
( C l , C3 , T 3 , T5 , e t c . ) d u ri n g e x h a l a t i o n , w h i l e w e
upper fi x a to rs a n d t o t h e cervic a l s p i n e , which t h e n
o b t a i n m o b i l i z a t i o n d u r i n g i n h a l a t i o n . T h e re i s a
carries t h e bru n t . T h e m u s c u l a r i m b a la n ce c a u s i ng
' n e u t ra l ' zo n e b e t w e e n C7 a n d T2 . An i m p o r t a n t
this s i t u a t i o n is a h yp e r a c t i v e pectora l i s m us c l e , i n
pa rticu l a r i t s s u bc l a v ic u l a r p a rt a n d t h e pectora l i s
i n h a l a t i o n i nc r e a s e s r e s i s t a nce n o t o n l y a g a i n s t s i d e ­
fe a ture of t h e a t l a s-occ i p u t segm e n t i s t h a t h e re
m i n o r , a n d a w e a k l o w e r t r a pezi u s a nd p e r h a p s t h e
b e n d i n g b u t i n a l l d i re c ti o n s , w h e r e a s e x h a l a t i o n
r h o m bo i d s .
faci l i t a te s m o b i l i t y . Th i s e ffect i s m o s t m a r k e d a t t he
This same
i m ba l a nce
a ls o
c a uses
a
fo rward­
c r a n iocervica l j u n c t i o n a n d decreases in a c a u d a l
p a rt i c u l a r ,
d r a w n position o f t h e head, res u l t i n g n o t only in
d i re c t i o n ;
overs t r a i n o f t h e cervica l s p i n e a s a w h o l e , b u t
i n h a l a t i o n ( i n t h e o d d segme n ts ) d i mi n i s h e s i n t h e
even i n c o m p e n s a tory h y p e r l o rd o s i s a t t h e c r a n i o ­
l o w e r t h o ra c i c regi o n .
cervica l j u n c t i o n , pro d u c i n g re l a p s ing l e s i o n s i n t h a t
regi o n .
the
m o b i l izi n g e ffec t
of
A w e l l - k n o w n y e t n o l e s s s t r i k i ng p h e n o me n o n , i s
t h a t we b r e a t h e i n a n d h o l d o u r b r e a t h i n s i t u a t i o n s
These a re s o m e o f t h e m o s t o b v i o u s l y pa t h oge n i c
examples
in
of
fa u l ty
i n s t a nce when d e l i v e r i n g a b l o w , l i ft i n g a h e a v y
muscu l a r i m b a l a n c e . The most i m po rta n t locomoto r
weight, or sprinti ng; t h a t i s , w h e n oxygen consumption
stereotype
c a n b e e xpected to be v e ry high. If w e h a v e n o t t i m e
t h e re fo re
the
p a t te r n s
most
due
i n w h i c h m a x i m u m m uscle a c t i v i ty i s d e s i r e d , for
to
and
move m e n t
p a thoge n i c
d i s t u r b a n ce , h o w e v e r , i s fa u l t y b r e a th i n g .
to t a k e a brea t h , a s w h e n we a r e forced to bra ke
Copyrighted Material
Manipulative Therapy in Reha b ilitation of th e Locomotor System
28
s u d d e n l y w h i l e d ri v i n g we h o l d o u r b r e a t h w i th o u t
,
bre a t h i n g i n .
M o rr i s ef al. ( 1 96 1 ) showed t h a t t h e s pi n a l co l u m n
i s s u p p o r t ed b y t h e d i a p h ragm, t h e a b d o m i n a l c a v i ty
be i ng
a
A uid - fi l l e d
space
and
therefore
not
c o m p r e ss i b l e s o l o n g a s t h e a b d o m i n a l m u scles a n d
t h e m us c l e s o f t h e peri n e u m a re c o n t r a c te d ; i n fa ct
M o r r i s ( 1 97 3 ) s h owed e lec t r o m y o gra p h i c activity of
the abd o m i na l m u scles d ur i n g w e i g h t l i ft i n g ( Fi g u re
2.17).
S k l a d a l et al.
( 1 970)
made
the
important
o b s e r v a t i o n t h a t t h e d i a ph ra g m c o n t r a cts w h e n t h e
p a t i e n t s t a n d s o n h i s t o e s , a n d r i gh t l y i n te r p reted
t h i s a s a pos t u r a l reac t i o n . I n d e e d , we stand o n our
toes as a s t a r t reaction before r u n n i n g , j u mp i n g , etc.
H e t h e r e fore r ig h t l y d e s c r i b e d t h e d i a p h ra g m as a
' re s p i ra t o r y m us c l e w i th a p o s t u r a l fu n c t i o n ' a n d t h e
abdominal
m u sc l e s
as
' p o st u r a l
muscles
with
a
respira tory funct i o n ' . The s i g n i fi c a n ce of h o l d i n g t h e
bre a th d u r i n g m a x i m um m uscle a c t i v i t y ( the V a l s a l va
m a n oe u v r e) l i e s in t h e fact t h a t p o s tu r a l s t a bi l i ty i s
ach ieved
at
the
cost
of
the
vital
fu n c t i o n
of
re s p i ra t i o n , w h i c h is ( m o m e n t a r i l y ) s a c r i fi c e d to i t .
A s i g n ifi ca n t b u t freq u e n t l y n e g l e ct e d ro l e i s a l s o
p l a y e d by t h e p e l v i c d i a ph ra g m .
O b v i o u s l y , t h e po s t u ra l role o f resp i ra t i on is n o t
co n fi n e d to Va l s a l v a ' s m a n o e u vre , a n d pe rsist s i n a l l
phases o f resp i r a tion s o l o n g a s w e a re i n the v e r t i c a l
pos i t i o n . T h i s is m o s t o b v i o u s d u ring e x h a l a t i o n : a l l
respi r a t i o n aga i n s t res i s t a n ce a c t i v a tes t h e a b d o m i n a l
m uscl e s , a n d t h e s h outs o f j u d o w re s t l e rs a n d s k i
j u m p e rs a re e x a m p l e s .
The
s i t u a tion
is
m ore
co m p l ic a te d
during
i n h a l a t i o n ; t h e c l u e t o w h a t h a p p e n s m ust be s o u g h t
i n t h e fact t h a t the t h o ra x w i d e n s i n t h e h o ri zo n t a l
pl a n e as w e b r e a t h e i n . A n a t o m i s t s l i k e to e x p l a i n
t h i s phe n o m e n o n by t h e a c t i v i t y of t h e e x te r n a l
o b l i q u e i n tercosta l m u s c l e s , b u t
a more
s i gn i fi ca n t
fa ctor i s t h e c o n t r a c t i o n o f t h e m uscu l a r d i a p h r a g m ,
w h i c h l i fts t h e l ow e r r i b s as l o n g as t h e ce n t ra l
t e n d o n is s u p p o rted by co u n te rp r e s s u r e fro m t h e
Figure 2.17 Lo a d i n g o f t h e l u m bosacral j u n c t i o n w i t h o u t
(a) a n d w i t h (b) t h e support of t h e abd o m i n a l w a l l
( From Kapa ndj i , 1 974. R e p rod u ced by k i n d p e r m i ssion
of a u t h o r
and
publishers)
a b d o m i n a l m u sdes ( Ca m p b e l l e t at. 1 970; K a p a n dj i ,
1 974 ) . T h i s i s borne o u t b y
the
a c t i v i ty o f t h e
a bd o m i n a l m us c l e s d u ri n g i n h a l a t i o n i n t h e e rect
p os i t i o n ( C a mp b e l l et aI. , 1 970; B a s m aj i a n , 1 978) .
T h i s is t h e o n l y e x p l a n a t i o n of t h e w i de n i ng of t h e
thorax
from
b e l o w , a p h e n o me n o n w h i c h
is
an
i m po rt a n t c r i te r i o n o f c o r r e c t res p i r a t i o n ( Pa ro w ,
1 9 5 3 ; G a y m a n s , 1 980) .
I t c a n t h e r e fore be c o n c l u d e d t h a t res pi ra t i o n
g u a r a n tees po s t u ra l s ta b i l i t y in a l l i ts p h a s e s ; t h i s c a n
be co n s i d e ra b l y e n h a nced b y Va l s a l v a ' s m a n o e u v r e ,
b u t on l y i f t h e s t e re o type o f resp i r a t i o n i s t h a t
I f, however, th e s u bj e c t i s s u p i n e o r o n a l l fo u rs , no
post u ra l reac t i o n i s req u i re d ; p u re a b d o m i n a l
resp i ra t i o n is t h e n p h y s i o l ogica l , t h e a bd o m e n
b u lg i n g , i ts w a l l c o m p l e t e l y re l a x e d . U n d e r these
c o n d i t i o n s the t ho r a x need n o t widen a t a l l
( G a y m a n s type B ) .
The c l ose re l a t i o ns h i p b e t w e e n r es p i r a t i o n a n d
the m o t o r s y s t e m i s s h o w n i n w h a t m a y be c a l l e d
'
re s p i rato r y
synkinesis',
i.e.
a
ce r t a i n
type
of
move m e n t is l i n k e d e i th e r with i n ha l a t i o n o r w i t h
d e s c r i bed by Parow ( 1 953) a n d G ay m a n s ( 1 980) : t h e
e x h a l a t i o n . O n e s u c h e x a m ple is t h e G a y m a n s effect
t h o r a x w i d e n i n g from b e l o w , from t h e wa i s tl i n e ; i t
d ur i ng
m u s t n o t b e l i ft e d . T h e s h o u l d e rs a r e rel a x e d , t h e
e x a m ple is t he close l i n k betwe e n tr u n k a n d h e a d
s i d e - be n d i n g,
described
above.
A n ot h e r
c l a v i c l e s a n d upper r i b s are n o t l i fted b u t r o t a t e
e x t e n s i on a n d i n h a l a t i o n , a n d betwe e n fl e x i o n a n d
s l i g h t l y to a l low w i d e n i n g of t h e t ho r a x . I t i s t h i s
exh a l a t i o n . B e c a u s e , u n d e r p h y s i o l ogica l cond i t i o n s ,
t y p e o f resp i ra t i o n t h a t h a s a stro ng m o b i l i z i n g ef fec t
tru n k ( h e a d ) e x t e n s i o n g o e s h a n d i n
on
t h e sp i n a l co l u m n ( G ay m a ns resp i r a t i o n type A ) .
Copyrighted Material
h a n d wi t h
l oo ki n g u p , a n d fl e x i o n w i t h look i n g dow n , i n i t s e l f
Th eoretical considera tions
loo k i n g
up
fac i l i t a t e s
i n ha lation,
looking
down
29
i m porta n t t o be a w a re o f c e r t a i n li m i t a t i o n s (J a n d a ,
1 978) .
e x h a l a t i o n , a n d v i c e v e rsa . T r u n k r o t a t i o n i n t h e
uprigh t ( s i t t i n g ) p os i t i o n , from n e u t ra l p o s i t i o n to
the
side,
is
l i n ked
with
i n h a l a t io n
and
can
be
T h e s i g n ifica n c e of co n stitut i o n a l
hyperm o b i l ity
i n h i b i ted by e x h a l a t i o n . R e s i s t a nce a g a i n s t t r a c t i o n
of the n e c k i n creases d u ri ng i n h a l a t i o n a n d d i s ­
appears d u ri n g e x h a l a t i o n ; i n t h e l u m b a r s p i n e , o n
the o t h e r h a n d , r e s i s t a n c e ( p r o n e ) aga i n s t t r a c t i o n
The i m p o r t a nce of m o v e m e n t r e s t r i c t i o n ( b l o c k a g e )
d u ri n g
a n d o f s h o r t m u s c l e s restri cti ng m o b i l i ty h a s b e e n
i n h a l a t i o n . T h e re i s e v e n a l i n k b e t w e e n i n h a l a t i o n
d e a l t w i t h . The e x p e r i e nced c l i n ic i a n , h o w e ve r , i s
i ncreases
d u ring
e x h a l a ti o n
and
ceases
a n d ope n i n g t h e m o u t h , a n d be t we e n e x h a l a t i o n a n d
we l l a w a re t h a t h y pe r m ob i l i t y i s fre q u e n t l y an e v e n
c lo s i n g t h e m o u t h . I t i s e v i d e n t t h a t t h ese n a t u ra l
m o re d iffic u l t p r o b l e m , w i t h c o n s i d e r a b l e s i g n i ficance
rea c t i o n s
for
ca n
be
v e ry
usefull y
appl ied
for
mobilization . .
W h a t a re t h e r e l e v a n t m e c h a n i s m s o f d i s t u rb a n c e
o f t h e d i ap h r a g m .
p r i m a ry
or
seco n d a ry
thorax
vicinity
of
a
inhalation
and,
in
p a r t ic u l a r .
the
the
thorax
even
when
p ro n e ,
a l t hough
con c e r n s
( 1 96 9 ) .
we
He
( c o m p e n s a t ory,
restricted
joint) ;
the
in
the
latter
is
pa rti c u l a rly c h a racte r i s t i c of t h e s p i n a l c o l u mn .
pati e n t ' s i n a b i l i t y t o b r e a t h e i n to t h e pos t e r i o r w a ll
of
p ro b l e m
l o co m o t o r s y s t e m
L Loca l p a t h o l o g i c a l h y pe r m o b i l i t y , w h i c h m a y b e
The
seco nd mech a n ism is i n s u ffici e n t w i d e n i n g o f t h e
during
this
of the
d i s t i n g u i s h e s t h e fo l l o w i n g :
activ i t y i n t h e a b d o m i n a l m us c l e s , t h e spi n a l c o l u m n
t h e s u p port
W h e re
fu n c t i o n
owe a m aj o r c o n t r i b u t i o n t o S a c h s e
of res p i r a t i o n p a t te r n s ? The fi rs t i s i n s u ffi c i e n t o r n o
t h u s losi n g
p a t h o ge n e s i s .
disturbed
no
2. P a t h o l o g i c a l g e n e r a l iz e d h y p e r m o bi l ity, fre q u e n t
b l ockage h a s b e e n fo u n d i n t h e t h o ra c i c s p i n e . The
i n certa i n c o n g en i t a l a n d n e u r o l o g i c a l c o n d i t i o n s .
3 . Const i t u t i o n a l
thoracic spine s h ows n o re s p i ra tory wave. In s u c h
h y p e r m o b i l i ty ,
which
is
m ost
cases we fi n d r e l a p s i n g move m e n t restr i c t i o n o f t h e
i m p o rta n t from o u r p o i n t of v i e w . In i t se l f it i s a
t h o racic s p i n e olV i n g t o t h e a b s e n ce o f t h e m o b i l i z i n g
v a ri a n t of t h e n o r m , b u t u n d e r c o n d i t i o n s of
effect o f resp i ra t i o n .
m a i n l y sta t i c s t r a i n i ts p a t h og e n i c i m p o r t a nce
T h e m o s t i m p o r t a n t re s p i r a t i o n a l fa u l t i s l i ft i n g
b e c o m e s e v i d e n t . O v e r a l l mob i l i ty is g r e a t e s t i n
the t h o r a x w i t h a u x i l i a ry cerv i c al m u s c l e s i n s t e a d o f
c h i l d h oo d
w i d e n i n g i t i n t h e h o r i z o n t a l p l a n e . Not o n l y i s t h i s
ge n e ra l l y gre a t e r i n w o m e n t h a n i n m e n .
and
decreases
w i th
age ,
being
type o f brea t h i n g i n e ffe c t i v e from t h e p o i n t o f v i e w
of v e n t i l a t i o n , b u t i t a lso ove rstra i n s t h e c e r v i c a l
T h e re are co nd i t i o n s i n w h i c h h y p e r m o b i l i t y m a y
muscu l a t u re a n d t h e c e r v ic a l s p i n e ( see F i g u re 4 . 7 6 ) ,
e v e n be a n a d v a n t a g e , f o r i n s t a nce i n certa i n s p o rts.
causi ng rec u r re n t cervical s y n d r o m e s . W h e n t h i s
in
gy m n as t i c s ,
etc.
and
in
employment
w h e re
fa u l t i s s l ig h t . i t i s d e m o ns t r a b l e o n l y i f t h e p a t i e n t
m o b i l i t y is
i s a s k e d t o t a k e a d e e p b rea t h . W h e n i t i s s e v e r e ,
d e c r e a s e d s t a b i l i ty , h owever, a n d as i n m o s t occ u ­
a req u i re m e n t .
It
is acco m p a n i e d
by
t h e fau l t y p os i t i o n o f t h e t h o r a x d u r i ng i n h a .l a t i o n
pations
and
a re
i n d i v i d u a ls a re l e s s a bl e t o a d a p t to s t a t i c o v e r s t ra i n .
e v i d e n t even at rest i n t h e e re c t p os i t i o n ; i n v e r y
A s liga m e n tous l a x i ty i s u s u a l l y acco m p a n ied by
severe c a s e s i t c a n be s e e n i n
w e a k n ess of the p o s t u r a l m u s c l e s , t h e c o n se q u e n ce
the
a b sence
of
abd o m i n a l
a
resp i r a t i o n
supine patient. In
tod a y s t a tic postu re p r ed o m i n a te s , t h e s e
s o m e c a s e s t h e fa u l t i s a s y m m e t r i ca l , o n e s h o u l d e r
is
being raised higher than the other, causing u n i l a te r a l
p a r t i c u l a r l y u n s u i ta b l e fo r s u c h p a t i e n ts : t h e y s h o u l d
o v e rs t r a i n ,
re s u l t i n g
in
pain.
Some
j obs
a re
cerv i c a l l e s i o n s . I n e x t re m e cases t h e a bdomi n a l w a l l
n o t b e d e n t i s t s , f o r i n s t a n c e , o r t e l e p h o n is t s , o r h a v e
protrudes d u r i n g e x h a l a t i o n a n d i s d r a w n i n d u ri n g
t o spe n d l o n g p e r i o d s b e n t o v e r a d e s k o r
i n h a l a ti o n ( , p a r a d o x i c a l r e s p i ra t i o n ' ) .
I n s o m e very pron o u n ce d c a s e s t h ere i s a c o n d i t i o n
T h e i mm e n s e
patterns
fo r
i m p o r t a n ce o f fa u l ty
p a t hoge n e s i s
should
mov e m e n t
now be
clear.
Thi ngs a r e a l l t h e m o r e s e r i o u s b e c a u s e m o d e r n
a
m a ch i n e .
o f genera l i n s ta b i l i t y , a l a c k o f coord i n a t i o n w h i c h
can be
i n terpreted a s a t y p e of ' m i n i m a l b ra i n
d y s fu n c t i o n ' .
ind u s t r i a l ized c iv i l i z a t i o n e n c o u r a g e s t h is i m b a l a nce
I n t h i s c o n n ec ti o n J a n d a 's observ a t i o n s co n c e r n i n g
betwee n p r e d o mi n a n t l y p h a s ic a n d p r e d o m i n a n t l y
m i n i m a l bra i n d a m ag e s e e m re l e v a n t ( s e e p . 2 1 ) .
postu ra l m u scles i n fav o u r o f t h e l a t te r ; w h i l e m o b i l i ty
is i n creasingly l i m i t e d , t h e l o c o m o t o r s y s t e m
is
overb u rd e n e d by e v e r m o re s t a t i c p e rfo r m a n c e .
A ft e r r e v ie w i ng 1 00 c a s e s h e d i s t i n g u i s h e s t h ree
types. The fi r s t i s ' m icrospastic i t y ' , s h o w i n g m i l d
s i g n s o f fi r s t m o t o r n e u r o n l e s i on w h i c h c a n be
T h e p ra c t i c a l c o n se q u e n ces o f fa u l ty m o v e m e n t
a s y m me t r i c a l . T h e s e co n d i s c h a ra c t e r i z e d b y h y p o ­
patterns a re s h o w n i n t h e c h a p t e rs o n d i agn o s i s a n d
t o n i c i t y , a s y m m e tr i c a l t e n d o n r e fl e x e s a n d s i g n s of
t he r a p y , a n d
s uggeste d . T h e
h y p e r m o b i l i ty w i t h a t e n de n cy t o i n s t a b i l i ty a n d
patie n t c a n ofte n be t r a i n e d a d e q u a te l y to c o r re c t
res t l e s s n e s s , c o r r e s po n d i n g to s e v e r e h y pe rm o b i l i ty
t ra i n i n g
tec h n i q u e s
the pre d o m i n a t in g fa u l t i n a re l a ti v e l y s h or t t i m e ,
as d e s c r i b e d by S a c h s e . The t h i rd type is c h a racter­
resu l t i n g i n p e r m a n e n t re l ie f. H ow e v e r , i t i s a l s o
ized
by
c h a n ge s
Copyrighted Material
in
se n s i b i l i t y ,
in
particular
of
Manipulative
30
Rellilbtfitation of the Locomotor System
of awkward-
proprioception,
ness w h i c h
can
r e s t o r i n g m ob i l i t y o f the s o ft
fo r i ns t a nce c a n i ncrease
a ft e r j o i n t m a n i p u l a t i o n .
How can wc
The s i g n ifica nce of soft tissues
s u c h e ffe cts') I t w a s s a i d a t
t h e b e g i n n i ng t h a t a l l m o ve m e n t p e r fo r m e d b y t h e
m o t o r s y s t e m i m p l i e s s t re t c h a n cVo r s h i ft o f t h e soft
A n yo n c w h o t r e a t s d y s fu n ct i o n o f t h e m o tor s y s t e m
tissues s u rro u n d i n g it. Y e t soft t i s s u e s , a s the t e r m
a n d h a s l e a r n e d t h e t e c h n i q u e s o f j o i n t m a n i p u l a ti o n
i m p l i e s , a re n o t l i ke a s t r a i g h tj ac k e t a n d w o u l d n o t
sim p l y i m pa i r m o t i o n m e ch a n i c a l l y . I t i s certa i nl y a
s h o u l d b y n o w b e fu l l y a w a re o f t h e d e c i s i v e r o l e o f
m uscle
fu n c t i o n .
However,
t h e re
is
much
less
a w a reness o f the r o l e o f s o f t t i s s u e , i n p a r t i c u l a r o f
t h e co n n e c t i v e t i s s u e a n d o f fasci a . T h e p o ss i b l e r o l e
i IH' c o n n e c t i v e t i s s u e is
sca rs c a n p l a y
reflex e ffect d ue to te t h e ri n g , as is most c l e a r l y s h o w n
b y t h e effe c t o f ' act i v e ' s c a r s , t h a t i s scars w h i c h d o
n o t m o v e free ly , w h i c h s h o w ' a d hesio n s ' , i . e . i ncreased
a nd fold i n g ( p i n c h i n g ) .
to l ac k of sci e n t i fic
w i d e l y i g n o re d .
k no w l e d g e
e s p ec i a l l y i n t h e s k i n ,
p r o d u c i n g r e fl e x e ffec t s .
of l a c k o f c l i n ic a l
methods
o n palpation which
Cl i n ic a l
o f to n u s we a re
is
m o re
o ve r l y i n g
i n d i stu rbed
m u sc l e s , a l t h ou g h t he
l i s s u e may grea tly
m o d ify i t
11 0
n o r m s n o r s c i e n t i fic
d a t a a v a il a b l e .
I n the p reced i n g paragraphs I have t r i ed to show t h e
I t s e e m s o b v i o u s tha t t h e soft t i s s u e s s u r r o u n d i n g
t h e m o t o r s y s t e m m u s t a d a p t t o a ll i t s c h a nges o f
i m po r t a nce of d is t u rbed f u n c t i o n i n t h e l oc o m o t o r
s y s t e m a n d t h e s p i n a l co l u m n . Nevert h e l ess, d istu rbed
s h a pe d u ring movem e n t a n d p os t u ra l f u n c ti o n . A l l
fu n c t i o n in i tse l f i s n o t i d e n ti c a l w i t h c l i n ic a l d is e a s e .
i ts l a y e rs i nc l u d i n g t h e s k i n h ave t o s t r e t c h a n d
I n d e e d , t h e pati e n t d o e s n o t a s a r u l e s e e k m e d i c a l
s h o r te n a n d t o s hift o n e a ga i n s t t h e o t h e r , s o a s to
a d v i c e , n o r d o e s h e com p l a i n b e c a u s e of d is t u rbed
a d a p t s m o o t h l y t o every c h a n g e . This i s b y n o m e a n s
m o b il i ty , b u t because h e fee l s pa i n i n t h e back, o r
a n e asy t a s k o r f u n c t i o n a n d i t w o u l d b e a m i r a c l e
i n the h e a d , t h e e x t r e m i t i e s , o r c v e n p e r h a ps t h e
i f d i s t u r b n n c e w o u l fl n o t be comm o n 10 s o v e r y
complex
n o r m s of s t r e t c h
o r s h i ft o f
b e e n e s ta b l is h e d n o r
v i s ce r a . O n t h e o t h e r h a n d . t h e re a r e p e o p l e w i t h
These c a n b e
l o c o m o t o r system w h o
a re
o f pa i n a n d w h o d o
not
I n fac t , d i s t u r b a nce o f
a re a s o f s k i n
fol d i n g , s h i ft i n g s k i n
t h e n o c i c e p tive stim u l u s
against the
a l l t h e so ft t i s s u e s
a ga i n s t
W a rd )
n o w p l a ys t h e d e c i s ive
a r i se s is: i n w h a t w a y
i m po r t a n t c l i n ic a l
c o ns i d e r a b l e .
fo r e x a m p l e
c o m p J e x of
and i t is the reaction
part
prod uce
can
n oc i c e p t i v e
stimul ation and pain?
fac t s .
N u m e r o u s m e t h o d s o f massage d e a l w i t h soft
B e fo r e p r e s en ti ng a n e x p l a n a t i o n I s h o u l d s t ress
t i s s u e s ; i n d e e d , soft t i s s u e te c h n i q u e s a n d m a ss a g e
t h a t i t is n ot the p u rpose o f t h i s b o o k to d e a l w i t h
a re
t h e t h e o r e t i c a l aspects o f t h e p h y s i o l ogy o f p a i n ;
v e r y o f t e n refe r r e d
to
as
a lmost
identical.
H o w e v e r , t h e re is v e ry l it t l e precise d i ag n o s i s a t t h e
n e v e r t h e le s s , s o m e p e r t i n e n t t h e o re tica l concl u s i o n s
b a s i s o f t h e s e tec h n i q u e s a n d h e nce l i t t l e s p e c i fi c i t y .
s h o u l d be d ra w n f r o m c l i n i ca l obse r v a t i o n . A s I h a v e
The d e c i s i v e step i n
i s the consistent
a l re a d y p o i n te d o u t , observa t i o n b e fo re a n d a fter
m a n i p u l a t i o n h a s given u s i m po r t a n t c l ues, fo r n o t
W h e n e v e r we s tretch s k i n o r a n y o t h e r s t r u c t u re
( s t r e t c h or s h i ft )
o n l y fl o e s c l i n ic a l e x a m i n a ti o n s h ow t h a t m o b i l it y i s
u n ti l w e t a k e u p
:l f fc c t e d m u s c l e s , a n d e v e n
t h e s l ack
as in j o i n ts . H e r e ,
I n t e re s t i n g to n o t e t h a t t h e
too, t h e
grad u a l a n d w e l l
b e observed a fte r l o c a l
pathologica l. We
il b ru p l
p a t h o l og i c a l b a r r i e r , i . e . t h e
w h ic h s t r e t c h a n d,
the m us c u l a r t r i gger­
this
fi e l d
a p p l i c a t i o n o f t h e barrier phenomen o n .
t h e re is a
where l ittle
i n particular.
w e t h e n e ng a g e
i t revea l s t h a t te n s i on
etc., if pain has been
poinl
te n s i o n
c h a r a c t e rized b y i n c r e ased
pain.
t h e b a r r ie r , w e w a i t u n t i l w e o b t a i n r e l e a s e a n d t h u s
A p p a r e n t l y p a i n s u b s i d e s i f h a r m f u l fu n c t i o n i n g i s
n o r m a l con d i ti o n s . A s t h i s i s b a s e d o n e x a c t
d ia g n o s i s a n d t h e re s u l t i s p r e d i c t a b l e , t h i s could
aptJy be c a l le d ' soft t i s s u e m a n i p u l a t i o n ' . I t s c ffects
correct ed . I f w e a re forced t o m a i n ta i n a n u n co m ­
for t a b l e p o s i t i o n f o r l o n g , w e fee l d iscomfor t a t fi rs t , .
b u t a ft e r a t i m e we a re forced by p a i n to c h a nge t h a t
Copyrighted Material
31
pos i t i o n . The sa me is I
I ha t
e x c e e d s o u r s t re ng t h : t h e
pa i n
di mi nishes a nd w i l l soon
d e n o m i n a t o r i n al l t h i s i s t h e c l os e c o r re l a t i o n
b e t w e e n t e n s i o n a n d p a in i n t h e l oc o m o t o r s y s t e m .
T h I s i s pa rticularly eviden t i n p os t - is o m etr i c muscle
re l a x a t i o n w i t h i ts i m m ed i a te a n a l ge s i c e ffe c t n o t
o n ly i n th e muscle i tsel f , b u t a l s o i n i ts a t t a c h m e n ts
(see Chapter 6 ) .
A n y h a r m l u i or d isturbed f u n c t i on i n g i s bo u nd t o
cre a te t e n s i o n : b l o c k a g e , w h e n e v e r t h e p a t i e n t t r i e s
t o move i n the re s t r i c ted d i re c t i o n ; h y p e r m o b i l i ty
d u e to exce s s i v e m ov e men t",
l ilb l e
res u l t i n g i n s ta t i c overstr al ll
Ii
sense , and is in ke e p i ng
pa i n as a w a r n i ng s i g n
wa r nin g o f t h e onset o f I l ill
locomotor sy s te m is c o n i
t o d a mage as w e wish , and
i t s e l f o t h e r t h a n b y ca us i n g
t h e con s e q ll e n ce o f m o r p h o l og i c a l c h a ng e i t
not hav e t h is sig ni ficant ro le . I n t h i s w a y t h e
v o lu nt a ry a c t iv ity o f t he l o c o m o t o r sy stem i s k ep t
wi thin due bounds by pain . T h e l o c o m o t o r s y s t e m
is , t h u s , b y (ar the m o s t fre q u e n t sou rce o f p a i n i n
the h uman o r ga n is m , n o r i s i t m e r e coi n c i d e nce t h a t
refe rred p a i n from o t h e r or gans o r s y s t e m s i s , a s a
r u le , pe rce i v e d i n p a r t s of t h e l oc o m o t o r s y s t e m .
Th e c l ose c o n n e c t i o n b e t w e e n physical a n d
m e n ta l fa c t o rs c a n a l so b e
a p h y s i cal and a psycho log lc :1
s a m e i s t r u e o f re l a x a t i o n :
i ma g i n e psyc h o l o g i c a l
m uscle s . Th i s s h o u l d b e
w i t h pa t i e n ts s u ffe r i n g II
sy ste m .
to
W h a t is th e r e a c t io n t o
d i s t u r b e d fu n c t i o n ? first,
w h i c h we h a v e already men tioned .
m a y be o f l e s s e r or gre a t e r i n t e n s i t y , w h i c h is o f
gre a t c l i n ic a l s i g n I fi c a n c e : i t allows u s t o c o r r e la t e
the d eg r e e of c h a nged fu n c t i o n to t h e re flex changes ,
and i n t h i s w a y to e s t a b l i s h t h e pa t i e n t 's l a b il i t y
o r s t a b i l i t y . It is by n o m e a n s o nl y a m a t t e r o f
a u t o n o m i c fu n c t i o n s , a s i s fr e q u e n tly t h ou gh t , b u t
a l so conce rn s m uscle spas m or m u s c l e i n h ib i tio n , e t c .
between
The re m a y b e c o n s i d e r ;l b l ci nd iv id ua l pa t i e n ts , b u t
c o n s i d e ra b l y i n t h e s a m e
a c u t e v e rtebr o ge n ic pa i n
dr a ugh t , i t c a nn ot be d u e
in s uch p a t i e n ts w e li nd
o n e segm e n t , w i t h
b l oc k age i s c l i n i ca l l y l a te n t .
a lges i c zo ne i n t h e s e g men
s t r i k i ng t h i s hy per a l ges ic zone i s
s t i m u l us w h i c h in t ens i fi e s the p a t i e n t ' s re a c t i o n a nd
ca uses s e v e r e ll1 u s c l e s p a s m w h i c h m a k e s t h e l e s i o n
m an i fe s t .
Thus
t h e r e is
m e c h a n i c a l i r r i ta t i o n
p a i n by
ces, a s i s
I l ll e nc e o f
freq u e n t l y s u gge st ed ,
t h e root - c o m press i o n mod e l . I t w o u l d , m d e e d , b e a
pec u l i a r c o n c e p t o f t h e n e rv o u s system (a s yste m
d e a l i n g w i t h in f or mati on ) t h a t w o u l d h a v e i t
r ea c t i ng, a s a r u l e , n o t t o s t i m u l a t i o n of i t s r e c ep t o rs
but to m e c h a n i c a l d a m a g e t o i ts o w n s t r u c t u re s .
R e fe r r e d p a i n from the v iscera and Tr Ps c a n serve
as a n e x a mp l e , a s c a n t h e e x p e r i m e n t a l i n fi l tr a t i o n
o f hype r t o n i c s a l i n e sol u t io n i n to l ig a m e n t o u s
s t r u c t u re s o f t h e spina l c ol u m n , w h i c h was first
perfo r m e d by K e ll9. r e n ( .1
Hoc k a d a y and W h iny I
( 1 97 2 ) a n d F e i ns t e in
01. ( 1
J u s t a s i n t hese
d e e p s tru c t u res
rad i a te s i n t h e
c h a nges i n s k i n
sometimes with
' p tl Sm , e t c . ,
th us i m ita t i n g
p a m . B r ugge r 1,1 960, 1 962)
therefore ca lled it 'pseudoradic ular ' . A s m us cu l a r
s p a s m i s a p r o m i n e n t fe a t u re w i th c o n co m i t a n t p a i n
i n t e n d o n s a n d i ns e r t i o n s a s w e l l a s i n fasc i a e , t h e
t e r m ' my o fa s c i a l p a i n ' ( 't e nd o m y o s i s ' ) i s fre q u e n t l y
u s e d . I n t h e G e r m a n li t e r a tu re t h e t e r m ' re fl e x
s y n d ro m e ' is p r e f e rr e d a t p r e s e n t .
This b r in g s u s t o ' s o ft t i s s u e c h ang e s ' , w h i c h a re
t h e ob j ec t of ' s o ft t i s s u e t e c h n i q u es ' or e ven o f ' s oft
h a v c'
with these
t i s s ue m a n i p u l a t i o n '
s k i n or
c h a n g e s ( h y p e r a l geSIC
) I!l a i nly i n
connective tissue, and
a ru le ,
t e r m s of ' r e fl e x
i n t h e a c u t e s t a ge
because immedi ate
o f m us c l e s p a s m
a c h i e v e d a fte r j oi n l
l a t e r s t a g e s , c h a nges
t h e deep l aye r o f fa s c i a e a nd m uscle s , te nd to
become c h ro n i c; s h o r te n e d , t h e se t i s s u e s then cause
m o v e m e n t r e s t r i c t i o n . Thi s is w h a t R u ss i a n a u t h o rs
m e a n by t h e ' d ys t r o p h i c s tage ' ( V e s el o vs k i a n d
Pope l y a n s k i , 1 9 8 2 ; Pop e lya ns k i , 1 9 84 ) . A s i n j o i n t s ,
w e e nco u nt e r a res t r i c t iv e b a r r i e r w h e n s t re tc h i ng
or s h i fti n g these fa s c i a e , a nd c o n s e q u e n t ly h a ve to
o v e r c o m e i t in o r d e r t o o b ta i n re l e a s e . W h e n t h i s i s
a c h i e v e d , even a t
s i dered m orp h ol o g i c a I
i.e. functiona l . There
under t h e c o n trol 01
so t h a t d y s t r o p h y can
I have d w e l t m o s !
th i s can m o s t rea d i l y
e v e r , i t s h o u l d n o t be
reac t i o n , it is per c e l v c'cI
thresh o l d of p a i n pe r c e p t i o n w h ich
n e rv o u s c o n trol. On e xa m i n a t i o n , i n d e e d , we v e ry
f r e q u e n t ly fi nd c h a n ges i n m a n y s e g m e n ts , of w h i c h
pa ti e n ts a re e n t i re l y unaw a re .
Copyrighted Material
32
l\Ilanip u /alive Therapy in Rehabilitation of the L o c o m o t o r System
f u n c t i o n , a s we h a v e se e n , is c l osely
r o o t c o m p ress i o n s u c h a s d i sc p ro l a p s e ? F i r s t , i t
con n ected to t h e reflex c h a nges typica l for nociceptive
s h o u l d b e poi n ted o u t t h a t n e rv e com p ress i o n a l o ne
s t i m u l a t i o n . T h e y t h e refore con s t i t u t e an e n t i ty t h a t
causes p a re s i s and a n a es t h e s i a , b u t no p a i n . W h a t i s
I m p a ired
we p ro p o s e to t e r m 'fu n ct io n a l p a t h o l o gy o f t h e
then
m o t o r syste m ' .
e x a m p l e , d i s c p r o l a pse ca u s e s pa i n ? Q u i t e o b v i o u s l y ,
the
most
l i kely
mechanism
by
w h ich,
fo r
S u c h i s t h e d i s t r u s t a n d lack o f k n o w l e d g e o f t h e
d i sc p r o l a pse ca n n o t i m p i n ge o n t h e n e rve root
w a y t h e m o t o r s y s t e m fu n c t i o n s , t h a t ' fu n ct i o n a l
b e fore a c t i n g o n t h e d u ra a n d the d u r a l s h e a t h s . It
p a t h o l o g y ' i s v i e w e d a s a s o r t o f s u b t e r fu ge , o r a s
i s p recise l y these s t r u c t u re s t h a t a re r i c h l y s u p p l i e d
a n a t tem pt to ' e x p l a i n a w a y ' c l i n i ca l p h e n o m e n a ,
w i t h pa i n rece p t o r s , a n d we s h o u l d be a w a r e t h a t a t
w h i l e t h e ' tr u e p a t h o l og y ' i s n o t y e t k n o w n . Y e t w h a t
o t h e r e x p l a n a t i o n i s t h e re fo r t h e fact t h a t n o t o n l y
s h e a t h s a re
symptoms b u t a lso mobi l ity, m uscle tension and
s h o u ld n o t b e fo rgo t t e n t h a t Laseg u e ' s s ign i n d i c a t e s
a u to n o m i c p h e n o m e n a m a y b e restored to cli n ic a l
m e n i nge a l i nv o l v e m e n t . T h i s i s i n k e e p i n g w i t h t h e
normality
e ffec t o f e p i d u r a l a n a e s t h e s i a i n d i sc l e s i o n s .
i m m e d i a te l y
after
mobil ization
of
a
every mov e m e n t o f t h e l egs a n d t r u n k t h e d u ra l
be i n g
rubbed o v e r the
p ro l a ps e .
It
restr i c t e d j o i n t , after re l a x a t i o n o f a m u s c l e w i t h a
A n o t h e r c l i n i c a l o bs e rv a t i o n a l so i n d i c a t e s t h a t
t rigge r p o i n t , or a ft e r s t re tc h i n g of a s h o r t e n e d fasc i a ?
p a i n i s p r i m a r i l y d u e t o s t i m u l a tion o f p a i n receptors,
H o w c o u l d s u c h i m m e d i a t e e ffec t b e e x p l a i n e d i f
eve n i f t h e re a r e clear n e u rological s i g n s o f n e rve
ro o t i n v o l v e m e n t . Ce r n )1 ( 1 948) registered t h e rad­
t h e re w e r e , i n d e e d , m o r p h o l o g i c a l c h a nges? The
s i t u a t i o n c a n be compared t o t h e w o r k i n g o f a c a r :
iating pain
t h e e n g i n e m a y n o t w o r k bec a u s e o f
u s i n g a u to d e r m o g r a p h y o f t h e p a i n , a n d fo u n d t h a t
a
fa u l ty b a l l
in
p a t ie n ts w i t h ra d i c u l a r s y n d ro m e s ,
bea r i n g o r a b u rs t c y l i n d e r ( m o r p h o l og i c a l c h a n g e ) ,
t h i s w a s m o re exact a n d
b u t it m a y n o t w o r k b e c a u s e , a l t h o u g h t h e s t r u c t u r e
l o c a l i za t i o n t h a n the t y p i c a l n e u rological sign s , in
i s i n tact, t h e i g n i t i o n i s out o f order, o r the carbur­
p a r t ic u l a r
e t t o r n e e d s adj u s t i n g ; a fte r a s i m p l e a d j u s t m e n t , t h e
beca use a nerve root d oe s not conta i n fi b res from
c a r fu n c t i o n s n o r m a l l y a ga i n .
o n e segme n t o n l y , but t r a n s i tory fi b re s from n e i g h ­
more
so
than
reliable
i n d e r m a t ome
h y po a e s t h es i a .
Th is
is
O n e o f t h e r e a s o n s w h y t h e m e d i ca l profe s s i o n i s
b o u r i n g s e g m e n ts a re u s u a l ly a lso prese n t . T h i s i s
s o s l o w i n rea l i z i n g th a t d y s f u n ction i s t h e m o s t
n o t o n l y a f a c t we l l k n o w n to a n a to m i s ts: i t e x p l a i n s
freq u e n t c a u se o f p a i n i n t h e loco m o t o r s y s t e m i s
t h e over l a p t h a n k s to w h i c h r a d i cotomy i s n o t , a s
t h a t t h e e v i d e nce i s b a s e d o n c l i n i c a l fi n d in g s, a n d
r u l e , fo l lo w e d by h y po a e s t h e s i a i n t h e correspo n d i n g
a
t h is i s rej ec t e d a s ' s u bj e c t i v e ' . T h i s i s a l s o the r e a s o n
segme n ts . T h i s r u l e , h o w e v e r , i s o n l y p a r t i a l l y v a l i d :
w h y c l i n ic a l ex a m i n a t i o n a n d c l i n ic a l sc i e n cc a re
t h e re a re freq u e n t e x c e p t i o n s . H a n ra e t s ( l 95 9 ) e x ­
i n c r e a s i n g l y u n d e rra t e d . We h a v e a l re a d y s e e n t h a t
pla i n e d i t a s fo l l o w s . D u ri n g o p e r a tion h e freq u e n t l y
t h e ' puzzle o f pa i n ' i n t h e l o c o m o t o r s y s te m , i . e . t h e
fo u n d t h a t n e rv e r o o t s v a ry c o n s i d e ra b l y i n t h i c k n e s s :
fact t h a t p a i n i s c l o s e l y r e l ated to t e n s i o n , w h i l e
if a root i s v e ry t h i c k o n o n e s i d e i t s n e i g h b o u r i s
d ec r e a s e d te n si o n goes a l o n g w i t h re l i e f o f p a i n , i s
l i k e l y to be m u c h t h i n n e r , beca u s e t h e t r a nsitory
u n fo r t u n a te l y b a s e d m a i n l y o n c l i n i c a l e v i d e n c e ; t h e
fi bres be l o n g i n g to t h i s n e i g h bo u r i n g s eg m e n t ca n
a n sw e r t o t h e ' p uzzl e ' l ie s l i t e ra l l y i n o u r ( p a l pa t i n g )
be v e r y n u m e ro u s ; i n t h e t h i n ( ne ig h bo u r i n g segm e n t)
h a n d s . Pa i n rece p t o rs a r e fo u n d p r e c i se l y i n t h ose
root, t r a n s i t o ry fi b re s a re c o n se q u e n t ly v e ry fe w , or
s t r u e t u r e s w h e re te n s i o n i s prod u ce d : in a t t ac h m e n ts
m a y be a b se n t a l t og e t h e r . C o n d i t i o n s on the o t h e r
of t e n d o n s , l i ga m e n ts , i n j o i n t c a ps u le s , m u s c l e s a n d
s i d e m a y be q u i te d i ffere n t : fo r e x a m p l e , i f t h e
m e n i n ge a l s h e a t h s . I n re a l i ty , t h e m o s t fu n d a m e n t a l
root is t h i c k on t h e r i g h t , t h i s n e e d n o t be so on t h e
L5
d i s t i n c t i o n b e t w e e n d i ffe re n t p a i n fu l co n d i t i o n s o f
l e ft . I f
t h e l o c o m o t o r s y s te m i s t h a t between co n d i t i o n s
w i ll be v e r y l i t t l e or no s e n s o ry c h a n ge , b u t if a very
a t tr i b u t a b l e
th i c k
to
p a t h o m o r phological
c h a nges
and
t h o s e c a u s e d by d y s fu n c t i o n , a d i s t i n e t i o n a l re a d y
a
v e ry t h i n root i s c o m p ressed o r c u t , t h e re
root is
i nvolved
t h e re w i l l
be
h a rd l y a n y
t r a n s i t o ry fi b re s i n t h e n e i g h bo u r i n g root o r roots;
d e s c r i b e d a s c o m p a r a b l e to t h a t betwe e n h a rd w a re
hence, t h e re w i l l be m a r k e d h y po a e s t h e s i a a n d some
a n d s oftw are ; h e re d iffe ren t i a l d i a g n o s i s is esse n t i a l .
dysaest hesia
Yet
to
w hi c h w i l l a ffect n e i g h b o u r i n g derma tomes a s we l l
m o rp h o l og i c a l c h a nges, i m prove m e n t ( a n d t h u s a l so
a n d p r o d u ce s o m e c h a n ge s o f s e n s i t i v i ty i n t h e m .
even
in
pain
a nd
disease
a t t ri b u t a b l e
o r i gi n a t i n g
in
the
t ra n s i to ry
fi b res,
d i a g n o s i s ) o f d i s t u rbed f u n c t i o n may be o f great
W h e n H a n r a e t s ( 1 959) s t i m u l a ted s u c h a t h i c k root
c l i n ica l i m po r t a n c e to t h e p a t i e n t a n d i s , i n d e e d , t h e
d u ri n g ope r a t i o n , his p a t i e n ts a lso fe l t dysaesthesia
t y p i c a l o bj e c t of r e h a b i l i t a t i o n m e d i c i n e .
in t h e n e i g h b o u r i n g derma tomes. Hence , a n e rve
root is not necess a r i l y m o n o-seg m e n t a l I S t a r y a n d I
fo u n d s o m e t h i n g v e r y s i m i l a r ( S t a r )1 a n d
Rad icular pa in
Lew i t ,
1 95 8 ) a fte r r a d i c o t o m y i n p a t i e n t s o p e r a ted o n fo r
root s y n d r o m e , i n w h o m no d i s c p r o l a pse w a s fo u n d
A ft e r s h o w i n g t h a t p a i n i n t h e m o t o r s y s te m is d u e
( t h e re w a s a t i m e w h e n r a d i c o t o m y w a s c a r r i e d o u t
to nocice p t i v e s t i m u l a t i o n o f p a i n rece p t o r s , w h a t i s
i n s u c h cases ) . M o s t o f t hese p a t i e n ts h a d few
c o m p l a i n ts , if a n y , b u t t h e re were s o m e i n w h o m
o u r explanation of p a i n i n cases of true mechanical
Copyrighted Material
Th eoretical considerations
33
perma n e n t h y p o a e s t h e s i a fo ll o we d , a n d w a s resen t e d .
t a ke n i n t o accou n t i n d i ffere n t i a l d i agnos i s . If t h is i s
H e r e , a p p a re n t l y , a t h ic k root w i t h m os t
c l e a r , t h e t h e r a p e u t i c con s e q u e n c e s s h o u l d n o t c a u s e
of t h e
t r a n s i to ry fi b re s o f t h e n e i g h b o u r i n g s eg m e n ts h a d
much controversy.
been cut.
Y e t , a s w i l l b e s e e n i n f u r t h e r c h a p te rs , v e r t e b ro­
R e fe rr e d pa i n com i n g from rece p t o r s , h o w e v e r
v i sc e r a l r e l a t i o n s a re m o re com p l e x , and fo r t h i s
( i . e . from d u r a l s h e a t h s ) , is fe l t in o ne s e g m e n t o n l y
re a s o n s o m e ci rc u m s pe c t i o n i s d e s ira b l e w h e n u s i n g
and
t h e t e rm ' v e r t e b ro ge n i c ' . Th e re a re ma n y d i sorders
t h e re fore
r a d i a tes
only
in
the
d e r m a to m e
corresp o n d i n g e x a c t l y t o t h e c o m p re s s e d roo t . I n
that a re c a u se d b y m o r e t h a n one fa c t o r , and t h e
o t h e r w o r d s , w h a t w e c a l l a r a d i c u l 8 r sy n d ro m e i s a
s p i n a l c o l u m n m a y be o n l y o n e o f s e v e r a l factors
co m b i n a t i o n o f p a i n o r i g i n a t i n g from pa i n re c e p t o r s
causing
w i t h i r ra d i a t i o n i n t h e seg m e n t , a n d o f n e u ro l o gi c a l
s i g n s of root co m p ress i o n ( h y po a e s t h e s i a , d ys a e s ­
t h es i a a n d p8res i s ) .
The re i s y e t a n o t h e r v e ry i n teres t i n g fe a t u r e t h a t
s h o w s t h e role o f t h e fu n c t i o n a l c o m p o n e n t : t h i s
i s t h e freq u e n t i m m e d i a te i m prove m e n t o f m us c l e
s t re n g t h i n w e a k m u s c l e s a n d even o f t e n d o n
r e fl e x e s ( s e e F i g u re s 2 . .1 2 a n d 2 . 1 3 ) a ft e r m a n i p u ­
l a t i o n . This agrees w i th t h e e le c t rom yogra p h i c a l
co u l d b e b e t te r t o s p e a k o f d is e a s e w i t h a v e rt e b ro ­
s p i n a l c o l u m n ( t h e l o c o m o t o r syste m ) is t h e s o l e o r
fi n d i n gs of D rech s l e r ( 1 970) a n d H a n a k
d is e a s e process, b u t o n c e t h i s h a s s t a rted i t m a y
s h ow i n g
that,
in
true
radicu l a r
el
a l . ( 1 97 0 ) ,
synd romes
with
a
p a t h o l ogica l c o n d i t i o n . In s u c h a case i t
g e n i c fa c t o r , r a t h e r t h a n v e r t e b r o g e n i c d is e a s e . A
t y p i c a l i n s ta n c e is m i g r a i n e : we s h o u l d r e s e r v e t h e
t e r m v e r t e b roge n i c fo r t h o s e c o n d i t io n s i n w h i c h t h e
d e c i s ive fa c t o r , a s i n t h e c e r v i cocra n i a l sy n d r o m e .
Howe v e r . a s J u n g h a n n s ( 1 957) h a s p o i n t e d o u t ,
t h e role o f t h e v e r t e b roge n i c fa c t o r m a y c h a n g e i n
t h e c o u rse o f
a
s i n g l e d i s o rd e r . I t m a y t r igge r t h e
d e v e l o p i n d e p e n d e n t l y . G u t ze i t ( 1 95 3 ) v e r y a p t l y
c l i n i ca l s i g n s o f m u sc l e wea k n e s s , n e rv e c o n d u c t i o n
c h a racte rized
v e l oc i ty m a y be n o rm a l . T h i s m a y be i n t e r p r e t e d a s
v a r i o u s roles i n t h e p a t h og e n e s i s o f s o m e d i se a s e s ,
m e re re fl e x i n h i b i t i o n . D rec h s l e r i n s i s t e d t h a t t h e
a s ' i n i t i a t o r , p r o v o k e r , m u l t i p l i e r , l oc a l ize r ' .
c l i n ical
prognosis
was
worse
in
t h os e
t h e s p i n a l co l u m n accord i n g to i ts
ra d i c u l a r
s y n d r o m e s i n w h i c h h e fo u n d d ec r e a sed c o n d u c t i o n
v e l oc i t y .
Conclusi ons
1.
The term 'vertebro gen ic'
M orp h o l og i c a l c h a nges c a n n o t e x p l a i n the gre a t
m aj o r i t y o f p a i n s a r i s i n g from
the locomotor
syste m . T h e s e c h a nges m a y , h o we v e r , p l a y t h e
A f t e r t e r m s s u c h a s ' d e ge n e r a t i v e d i se a s e ' a n d ' d i s ­
copa t h y ' h a d b e e n a b a n d o n e d , t h e n o n -co m m i tta l
p a r t o f a 10ClIS minoris res islen liae.
2.
By
fa r
the
t e r m ' v e r t e b roge n ic ' s e e m e d use fu l a n d h a s b e e n
d i s t u r be d
wi d e l y
mobi lity
adopted .
I
have
a l ready touched
on
i ts
m os t
freq u e n t
cause
of
pain
is
function . This m a y concern passive
U o i n ts ) , m u sc l e
activity (TrPs a nd move­
s h o r t co m i n gs : i t i n c l u d e s s t r u c t u ra l d is e a s e of t h e
m e n t p a t te rn s ) , o r
spi n a l co l u m n b u t d oe s n o t c o v e r c h a n ge s i n t h e
t r e a t m e n t i s d i re c t e d t o m o v e m e n t r e s t r i c t i o n o f
fu ncti o n i n g o f t h e l o co m o t o r syste m o u t s i d e t h e
j o i n ts o r m o t o r s e g m e n ts o f t h e s p i n a l co l u m n -
spi n a l co l u m n . H o w e v e r , i n t h e s e n se t h a t t h e s p i n a l
col u m n i s u s e d a s
a
pars pro 10/0 , t h e t e r m i s
acce p t a b l e . S o l o n g a s i t i s u s e d fo r b a c k pai n a n d
body sta tics.
Manipulative
b l oc k a g e .
3 . The
most
i m portant
ca u s e
of
b l o c k a ge
is
o v e r s t r a i n c a u s e d b y fa u l t y m o v e m e n t p a t t e rn s or
(closely) re l a t e d d i sorde rs, i t i s h a rd l y c o n t r o v e rs i a l ;
body s t a t i c s , t r a u m a o r v i sce ra l d is e a s e .
i t beca m e , a n d s t i l l i s , c o n trovers i a l w h e n a p p l ied to
fre q u e n t l y fo u n d even in e a r l y chil d hood .
I t is
d i sorders, m a i n l y pai n , us u a l l y a s c r i b e d to i n te r n a l
4. I t s con s e q u e n c e s a r e d i s t u rb e d fu n c ti o n , h y per­
o rga n s . Th i s c o n t roversy beca m e p a r t i c u l a r l y h e a ted
m o b i l i t y and a ga i n b l o c k age i n the n e i g h b o u r i n g ,
beca use o f s o m e of t h e t h e r a pe u t i c c o n se q u e n c e s o f
or e v e n i n m ore d i s t a n t , pa rts o f t h e loco m o t o r
m a ni p u l a t i o n .
syst e m .
T h e re is .l i t t l e room
for
c o n t roversy i f o u r p r e s e n t
k n o w l edge a b o u t re fe r r e d a n d ra d i a t i n g p a i n is
t a k e n i n to acco u n t . M e l z a c k and W a l l ( 1 96 5 ) a n d
M i l n e e l al. ( 1 98 1 ) h a v e show n t h a t n o c i c e p t i v e
s t i m u l i fro m a l l s t r u ctu res i n a s e g m e n t c o n v e rge t o
c e U s i n t h e l a m i n a V o f t h e b a s a l s p in a l n u c l e u s .
Th i s , o f c o u rse , a l s o a p p l i e s t o p a i n c o m i n g from
rece ptors
in
the
joint
capsules
of
a po p h y s e a l
U l ti m a t e l y ,
by
d istu rbed
fu n c t i o n
or
c o m p e n s a tory h y p e r m o bil i t y, they c a u s e d e ge n e r­
a tive c h a nges.
5 . The locomotor system a n d the s p i n a l col u m n act
a s a f u n c t i o n a l u n i t w h i c h a d a p t s i ts e l f to a n d
c o m p e n s a tes
fo r
distu rbed
functio n ,
so
that
e q u i l i b r i u m i s a l w a y s m a i n ta i n e d .
6 . C h a n g e s o f m e c h a n i c a l fu n c t i o n a l o n e d o n o t
cause c l i n ical symptoms (pa i n ) . They const i t u t e ,
i n t e rverte b r a l j o i n ts as w e l l as from i n t e r n a l orga n s .
h owev e r , t h e n o c i c e p t i v e stim u l u s w h i c h prod u c e s
I t i s , t h e re fore , e a s y t o s e e t h a t t h e l o c o m o t o r s y s te m
c a n read i l y s i m u l a te v i s ce r a l p a i n , a n d v i ce v e r s a ,
a n d t h a t t h i s co n s t i t u t es a n i m po rta n t a s p e c t t o b e
r e fl e x c h a n ge s i n t h e s e g m e n t ( m u s c l e s p a s m ,
h y p e ra l gesic z o n e s , e t c . ) . I f t h ese a re o f s u ffic i e n t
i n t e n s i t y t o p a s s t h e p a i n t h resh o l d , p a i n i s fe l t .
Copyrighted Material
34
Manip,,!ui" !.·
Neflil!n!ilation of the LocomolOr System
s i n n u l us i s i n cr e a s e d
f u n c t i o n t h a t i s t h e most
i s t h e r e fo r e a
the most freq u e n t t y p e
w a r n i n g :>ign of h a r m f u l f u n ct i o n i n g w h i c h s h o u l d
o f pa i n w i t h o u t a s pe c i fi c d ia g n osis, a n d t re a t -
T h e m os t
t e n s io n .
7 . Pa i n i n
i m p a i r m e n t of m o tor
I
b e c o r r e c t e d i n t i m e b e fore i t c a u ses p e rm a n e n t
m e n t o f t h e p a i n a s s u c h , w i t h ou t a t h o ro u g h
d a m a g e . I t i s p r o b a b l y t h e m o s t freq u e n t t y p e o f
c l i n i c a l u n d e rs t a n d in g o f t h e f u n c t i o n i n g o f t h e
locomotor s y s t e m , i s c o u r t i n g fa i l ur e .
p a i n t h ro u g h o u t t h e orga n i s m .
S . I f t h e p a t i e n t i s a b l e to d e s c r i b e a n d l o c a l iz e t he
p a i n , a n d we fi nd some
c h a n ge s
in
a
9 . T h e complex o f c h a n ge s i n f u n c t i o n o f t he l oco­
of t h e t y p i c a l reflex
c orrespo n d i n g
are a
and
h a ve
e x c l u d e d gross p a t h o l o g y , t h e n i t is o u r t a s k t o
Copyrighted Material
motor s y s t e m a n d t h e res u l ti n g r e fl e x c h a nges
c o n s t i t ute w h a t may be ca l l e d the ' fu n c t i o n a l
p a t h o l ogy of t h e m o t o r syst c m ' .
3
Functional anatomy and radiography of
the spinal column
Without a good un dersta nding of fu nctional anatomy
as p rese n ted by X-rays, i t is almost impossi ble to
u n d e rstand i m p a i red function and t h erefore to
i n terpret correctly w hat we have fe lt with our h a n d s
d uring examinat i o n . I t is, o f course, not t h e pu rpose
of this chapter to dea l with a n a tomy in detai l , but
to present those featu res that a re essentia l for a n
und e rsta nding bot h o f t he w a y i n w h ich function
may be imp a i red, a n d of the mech a n isms involved.
Basically X-ray d i agnosis o f the s p i n a l col u m n
serves t h ree pu rposes: (1) d i agnosis o f c h a nges i n
structure, (2) assessme nt o f locomotor function
(ki nema tics) a n d (3) assesme n t of static function
(spina l c u rvature, position o f i n d i v i d u a l vertebrae ) .
Diagnosis o f structural changes
Classic X-ray d i agnosis is concerned mainly with
cha nges in structu re, and this type of d i agnosis is
essentia l in ord e r to avoid serious e rror; methods
aimed a t correcti n g fu nction are out of p l ace in
cases where the u nder l y i n g condition is structura l
pathology . Our specia l i n te rest i n t h i s fie ld, however,
l i es i n such cha nges of st ruct u re as ma y have a d i rect
influence o n fu nction, such as various a n omal ies, i n
particular in the shape of j o i n ts, asymme try o f t h e
vertebrae, spinal c u rva t u re, etc. Not o n l y is the
shape or deformity o f some vertebrae t h e ca use
o f asym metrica l function ( e .g. in sco l iosis), but it
can itself bc the result of asymme t r ica l function
(e.g. rota t i o n of the lower cerv i c a l spine ow ing to
dom i n a nce of one h e m isphere a n d asymmetrical
loading of the upper extremities, as Jirout (1980) has
shown). Diagnosis of structur a l c h an ge can be fou n d
i n the classic tex tbooks both o f a n a to m y a n d of
radiology, and t h e refore need not be dea l t w i t h i n
detail here.
Diagnosis of disturbed function
(mobility studies)
The X-ray examination of d i sturbed fu nction i n v o l ves
exa m i n a tion o f the s p i n al col u m n in vario u s, usu ally
extreme, positions such as a n te- and retroflexion
(exte n s i o n), side-bend i n g or even rotation. This type
of examina t i o n und o u b t e d l y p rovides some d i rect
information about mobility; as a routine examination,
howeve r, it i s very time consu ming and uneconomica l
a nd i ts practical v a l u e is t h u s limited to complicated
cases w h e re specia l information is required, o r to
cases invol v i n g l i tiga tion. It is advisable to use X-ray
exa m ination in cli nica lly re l e v a n t positions, e . g. i n
retroflexion in cases o f ve rtigo ca used by ben d i ng
the head back. Doctors familia r with manu a l
diagnosis of d i s t u rbed funct i o n a re accustomed to
assessi ng mobi lity by cli nica l examination; neve r­
theless X-ray exa m i nati on of mobi l i ty is extre m e l y
i mporta n t for res e a rch p u rposes, as i t gives insight
into the mechan i s m s u nderlyi ng mobility and i ts
d i s turbance, an ins i g h t no othe r m ethod can provide.
Diagnosis of disturbed static
function (spinal curvature and
'malalignment')
Mobi l i ty is what is usua l l y m e a n t by 'spi n al function',
yet static function is no less importa nt, a n d X-rays
of the s p i n a l co l u m n with the p a t i ent standing or
s i t t i n g (ta ken und e r standard conditio ns) ca n, a n d
should, be eva l u a ted f o r static function. As is s h own
in more d e t a i l below, spi n a l curva tu re sho uld be
such as not to upset b a l a nce. Thi s goes not only for
t h e sagittal b u t also for t h e coronal plane, in which
every obliq u i t y (e.g. i n w a lki ng) p roduces a scoliotic
35
Copyrighted Material
Manipulative Therapy in Rehabilitation
36
of the Locomotor Systan
c u rva t ure with the correspo n d i ng rotatio n . Curva­
posture. To d etermine the p os i tio n of the ce rvical
ture may be smo o t h, or less so; in
segments
spine, the base o f the skull mus t be v i s i b l e , as we l l
kyp h o tic ,
a s the whole o f t h e cervical .
t h e re
may
b e a s harp bend
ce r t ain
(scolio tic ,
l ord otic) or even som e rotatio n or shift ('offset' ) .
The imp orta nce of the se s ig ns of m al a l ignm e n t is
highly controversial, es pe cial l y in v i ew of t h e dis ­
c r ed ite d sublu x at i o n tb e ory. The controversy is
f u e ll e d by t he d oub t fu l impor ta n ce of asy m m e try,
as, in fact, asy mmetry i s t h e rule rat her t h an the
exce ptio n . Yet Jir o u t (1978) has shown that alt h oug h
to assess the shape of the l umbar sp i n e we need to
se e at le a s t the t h oracolu m b a r j u n ctio n , the ilia, the
p u bic sy m physi s and both hip joints on a sin gl e AP
picture. This gives a suf fi c i ent n u m ber of l a n dmarks
by which to assess correct focusing and t o com p are
successive p ictu r e s if a stan dard te c h n iq u e is used .
Th e id e al method f o r X-ray exami n a t io n o f t h e
asymmetry of the positi o n of the atlas in rela t i o n to
sp i n a l column i s t o s h ow the whole column o n a
t h e axis is the rule, i ts i n cidence incre ases with age.
s i n g l e pi cture. An AP a n d
This is e qua lly true for t he a sym m etrical shape of
patie n t st a n ding are required: the on ly condition to
a
l a t e ra l vie w with the
the sp i nous p r o cesses. He conc l u de d that t his is
be obse rved for the AP vi e w is t h a t both feet must
pro b a bly the r e s ult of a s y m m e tr ica l pull due to the
be place d sy m m e t r ic ally in relation to the X-ray
d ominance o f o n e c e r eb ral h e mi sp h e re .
scre e n , and t h at the patie nt be re qu este d to d istri b ute
F r o m this it appears reas o n a b l e to deduce tha t
his weight e q u all y be t w een his t w o feet, keep ing his
asymmetry and irregu l a rity of ' alig n m ent ", while not
legs straig h t . In the lat e ral view, the feet s h o u l d be
in themselves p at h o l og i cal , can be the exp ress i on of
place d so that the ankles are about a fing er' s breadth
example,
. behind the v e r ti ca l to the flo or. from the mid-po i nt
the axis is rotat ed in n eutral posi tion , not only will
of the horizontal edge of the cass ette; the head
s h o u ld be n eith e r bent Lo the side no r rotated, the
p a tien t fixing s o m e o bj ec t at eye -le v e l in ord er to
asym metry or a n om a l y in fu n c tion.
If, for
it ro tate asym m e t rically d u ring side-bending, b u t the
rest of the cervical spine will follow suit (see p.
65).
retroflexion
Without j u m ping to c o n cl u sio n s , marked asymmetry
avoid a n te tlex i o n or
or 'm alalig nment' in the X-ray pic ture sho uld be
p atie n t holds his arms crossed ove r t h e chest and his
c orrel ated to the c l inical find ings. Marked irregularity
h a n d s on his shoulders.
of t h e head; the
of the r ela t ive p osi tion of vertebrae in the X-ray can
be regard ed as a warning signal that there may al.so
be some fu n c tio n al anomal y or at least su s cept i b i l i ty
to dis t urbe d fun c tio n.
X-ray of the lumbar spine and the
pelvis
One obvious ad v a n tage of t h e exam ination of
static fun c tion is its e c o n omy: on ly t w o X - rays are
Th e pat i e n t mus t be standi n g if X-ray p i c ture s that
re q ui r e d , t h e anteroposterior (AP) view and the side
can
view. Sta n d a rd c o n d itions must be adh e red to. As
obtained. He is therefore p l ac ed before the X-ray
individual posture is highly characteristic, i.e. constant,
s c re e n as when pictures are take n of the who l e spinal
co m pa r a b l e pi c tures can be e x pe c ted on rep e tition .
column. To acquire in f or m a t i o n about the sta t ics of
be
e v alua t e d
Gutman n a n d Vele (1978) h ave ve ry a ptly s u mmed
the spinal column
up the i m p o r ta n ce of static function: 'The d o minat i ng
Gutman n
fo r sta t ic function are
as
a whole,
a
to be
dev i ce described by
(1970) is used , in which a plumb-line
p rincip le of the sp i nal colu m n is body s t a t i cs '. All
indicates the vertical line from the head. A lin e
ot h e r func tions are subordinate to the requirements
which c o rr es po n d s to the centre of the scre e n is
the fl oo r: for the AP vie w the patie n t
of u p right posture on two le gs . Loss of m ob i lity and
draw n on
p a i n ful i m pi nge m e nt of nerve roots is pr e ferred to
places o n e f o o t symmetrically o n each sid e of the
sacrifice of the e re c t p o sture .
line. A movable pl u m b - li n e of m etal wire is attached
to the scre e n . The s c re e n is fi r st raise d to t h e l evel
of the p a t i e n t ' s oc ci p u t and the metal wire m ove d
Techn i c a l require m e nts
The
be
take n
to
in
a
posit i o n
a
point
c o r resp o n di n g
to the
o u t er occ ipit a l
that
protuberance. In this way the plumb-line sh ows the
c o rresp o n ds to t h e pa t ie n t ' s natural posture, either
head position. The screen is the n adj ust e d to the
X-ray sh ould
standing or sit ti ng (with the e x c e p t i o n of the AP
he i gh t re quir e d to t ake a picture of the lum bar spine
view o f the cer vical spi n e , which is taken with t h e
and the p e lvis (with the cen tral b eam and the cent r e
p a t ie n t su pi n e ) .
There s h ould ,
therefore, be
no
artificial correction of the patient's p os ture. Distortion
must be avoided and f ocusing m ust be s cru pu l ous t o
obtain clear pi c tures t ha t can be used s u c cess i v e l y
of the screen roughly at the h e igh t of the n avel ) . The
wire should n ow be taped to the lower edge of t h e
screen a n d th e patie nt l eans aga i n st t h e screen s o as
n o t to bl ur the p ict u re (Figure 3.1 ) .
fo r com par i s o n . To ac h i e ve this, some corre c tion is
For t h e lat e ral vie w t h e patie n t p u ts his feet as
u n avoid ab l e , for insta n c e to prevent d i s t o r tion or
desc ribed for t h e X-ray of t h e whole spi ne: the
tilt, b u t t h e nat ural posture must be r e gis t e r ed. It is
scree n with the p l um b -l i ne is raised to the
also esse n t ial to v i sual i z e
suflkiently lo n g section
the h ead in o rder to place the p l u m b - l in e at a point
of the spinal column t o make it p ossible t o assess
correspon ding to the outer meat us acousticus, and
a
Copyrighted Material
l evel
of
Functional analOmy and
radiography of {he spinal co/ul11n
Figure 3.1 X-ray technique of the lumbar spine with the patient standing. (a) Positioning of the moveable plumb-line:
the device prepared For X-ray, AP view: (c) positioning of plumb-line: (d) the device prepared for X-ray, lateral
view (After Gutmann, 1970)
(b)
Copyrighted Material
37
38
Manipulative Therapy
in
Rehabiliratioll of rhe Locomoror
Sysrern
(Figure
3.2).
lumbar
sp ine is o v er-exposed or the lumbosacral
With
the normal t echniq ue , either the
j unc tion is
t ube to
under-exposed. The dis ta n c e of the X-ray
the fi l m should be as great as possible,
depending on t he power of the apparatus a n d the
corpulenc e of
the
patie nt , the ideal dista n ce b ein g
2 m.
X-ray evaluation of lumbar spinal
statics
As
we
h a ve al rea d y seen, X-ray examination of t h e
p a t ie n t st a n di n g serves mainly for d ia gnosis o f static
fu n c tion and i ts disturbance. It should be borne i n
mind tha t clinical examination alone can ascertain
the position of the outer occipital prot ub e rance , t h e
spinous processes, the intergluteal line and
the
mid­
point be tween t he heels in rela ti on to a p lumb-line.
In the sagittal plan e , clinic al examination can show
the position of the sh oulders, the great troc hante rs
and the heels in relation to a plum b -l ine from t h e
external aud itory meatus. Clinical exa min a t ion,
ever,
how­
cannot provide information about the position
of the sacrum
and L5, i.e. the true base of the s pinal
column, information which is essential for the under­
s tan ding and evalua tio n of spinal statics.
This e xplai n s why clinicians in t e r e ste d in body
s t a tics have d e v o t e d t h e i r a t ten tion mainly to the
question of bo d y equilibrium as a whole, studyin g
d eviation of the head and dev iation from the line of
g r a vit y by means of sta tove ctography. Rash an d
Burke (1971) p oin te d out that 'in s tationary
the
c e n tre of
g rav i t y
be ver tically above the area of
preferably n e ar
Figure 3.2 Lateral view of the lumbar spine using the
technique illL:strated in Figure 3.1: perfect visualization
of the innominate and the femoral heads, and of the
lumbosacral j u nc ti o n. The rest of the lumbar spine is
neither over-exposed not distorted
its
posture
of eac h bod y segment sbould
centre.
If
the
supporting base,
persistent gravitation a l
torques are bei ng borne by ligamen ts . or if ex c e s s i ve
m uscular c o n traction is r e qui red to m a intai n balance,
this p r i nci p l e is being viola ted'. X-ray exa m ina t i o n
u n der sta t i c
conditions prov ides pertinent informatio n
on this type of s t a tic disturbance .
The me ch a n is m of balance differs
a nd the sagitt al p la n es .
This
is
in
readily
the coro nal
un d erst ood
if the effe ct of a heel-pad is consid ere d. An arti­
with the p lumb-lin e in place the screen is t h en
the
ficial difference of m o re t h an 1 cm in leg length
this
the coronal plane ; it is
felt and resented by the subject,
wh ere as ra isin g (or lowerin g ) both h e els is hardly
noticed. T his is because in the coronal plan e the lin e
of gra v ity lies between the two hip joints and the
heels, guaran t eein g ( r ela t i v ely ) stable equili bri um .
Purely mechanical sta t i c chan ges a re t h e re for e much
more readi l y felt in the coro n al than in th e sagittal
plane . In the l a tter the tru n k is in a state of labile
equilibrium above th e two perfectl y round sur faces
tec h nique is that it giv e s an u n disrort e d view of the
of the hip joi n ts. Ba l a n ce in this pla n e canno t be
pelvis and the hip j oin ts and correct exposure of
maintained by static forces alone ; dyna m i c m uscul ar
bo t h t h e lumbar s pin e and the l umb osa cra l junc tio n,
forces mus t be brought i n t o pla y , but should be kept
and yet there is no disto r t ion of the lumbar spine
at
lowered to
level requ i red for t h e latera l v i e w of
the lumbar spine (the centre of the screen at the
level of the
navel
or slight ly above ) . The p l umb- line
must a g ain be ta ped to
the lower edge
of
the screen
and the p a t i e n t must le a n aga inst the screen to avoid
blurring. In the la t e ral view it is an adva n tage not
to focus t h e central beam o n th e mid dle of the
pic tur e but eccentric ally mi d way between the i l i a c
cre s t a nd th e greater t ro chan te r , i. e.
level of
the sa cral
roughly
a t t he
promontory. The advantage of
changes t he balanc e in
i m med iat ely
Copyrighted Material
a
minimum.
FunClionai analomy and radiography of the
Lumbar spinal statics i n the coronal
pla ne
Under 'ideal' cond i tions the pelvis a n d sacrum in
the AP view a re s t r a ight and a l l vertebrae a re
symmetrical: the outer occi pi ta l protru berance is i n
the mid-line a n d s o are all the spinous processes
down to the sacrum, as well as the coccyx and the
p u b ic s ym ph ysi s. Not only is such a s p i n a l colu m n
the exception but it is o f l ittle i n te rest. N o bod y ever
sta nds n atu ra l l y sy m metrica l l y o n both feet. a n d
du r i ng move m e n t the p e l vi s con s t a n t ly s w i n g s f r o m
one side t o the oth e r. The pro b l e m is thus not
obliquity in i tse l f b ut correct or fa u l ty reactio n to
obliquity, and the crite ria by which this reaction c a n
b e j udged.
This can be stud ied physiologically i f one creates
obliquity of the base i n a he a lt h y s u bject b y
lengthe n i ng one le g (Figure 3.3). The pe lv is shifts to
the h igh e r side while the lumbar s pi n e bends to the
same s i d e , if bo t h l egs are stra ig ht and the p a t i e n t
re l a x e s.
Tn X-rays the same shift to the side. sco li o si s a n d
rotation to t h e lower s i d e can b e observed. The
summit of th e scoliotic curve i s us ua l ly at the mi d ­
lumbar reg i o n , so that the tho racol u m b a r junctio n
comes to stand above the sacrum. The d egree o f
rotation i n l u m b a r scoliosis d e p e n d s on lordosis: if
this is prese nt, rotation is norma l l y fo und. If th e r e
is no lordosis - as in acute l u m bago or sci a tica, for
example - there is a l so no rotation; if t here is
kyphosis there may even be rotation to the o p po s i t e
side.
The c rit e r ion of norma l stat i c function of the
lumbar spine mllst therefore be its reactio n to
obliquity at the base - this base not necessari l y being
only the sacrum but also the l ower l umbar vertebrae
up to U. If the ob liq u ity is not due to a sho rt l e g
(pelvic i n cl i n a t i o n ) but o n l y to inclinati o n of the
base of the s pi n e . i t will persist w h e n the p a tie nt
is seated, and therefore correction of the sitting
pos it i on should be cons i d e red .
Reaction to o b l iquity at the base is normal if (1)
t h e r e is s co l io s is to t h e lower s id e; (2) there is
rotation to the same s i de , p rov ided th at lordosis is
present; (3) t he th oracol umbar junction stands
vertically above the sacrum; and (4) the pelv i s shifts
to t h e higher side . Tho racic scoliosis is always in the
opposite d i r e c t io n to l u m b a r scol i osis (Figu re 3.4).
These facts reflect the physiology of bala nce a n d
Figure 3.3 Body statics with the subject standing:
with his weight equally on both feet. the body axis
corresponds to the plumb-line between the heels:
(b) with a heel-pad, the weight again equally on both
feet. the pelvis shifts to the higher side; (c) w i t h the
weight on the right foot the whole body deviates to the
right. the head deviating furthest
(a)
Copyrighted Material
spinal
column
39
40
Manipulative Therapy
in
Rehabilitation of the
Locomotor System
Figure 3.4 Normal reaction of the lumbar spine and pelvis to a short right leg (pelvic obliquity): static dextroscoliosis
with dextrorotation of the lumbar spine, deviation of the pelvis to the left from the mid-line (arrow)
affect the whole question of difference in leg length.
that while clinically we determine pelvic tilt,
This in itself is of no significance if it does not cause
cannot determine the position of tbe
sacrum
we
nor that
obliquity of the base of the spinal column. There­
of the lumbar vertebrae that constitute the base of
fore, the age-old dispute over how to measure this
the spinal column, as the pelvis may be straight while
difference is beside the point. What is important is
the sacrum is tilted, and vice versa. Only by X-ray
Copyrighted Material
Functionrd anatomy
and radiography of the spina! column
41
Figure 3.5 Pelvic obliquity. (a) Pelvis lower on the right (short right leg) with a horizontal sacrum, the lumbar spine
with a right heel-pad the pelvis is horizontal, but sacral obliquity appears, with deviation or the lumbar
spine to the left and slight dextroscoliosis
straight: (b)
examination can the true b a s e of the s pinal col umn
and the reaction of the s p i n a l col u mn to incl i n ati on
b e determined (Figure 3.5).
The principa l pathological fi nd i n g s a r e :
1. Obliquity
without scol iosis or w ith insu ffic i e n t
scoliosis, so that the thoracolumbar j uncti o n is
n o t above the lumbosacral.
2. No pelvic shift to t h e hi g he r side.
3. No rotation whe n there is sco l iosis and lordosis
or ro t a t i o n i n the opposite d irectio n from t h e
scoliosis, or even sco l i osis to t h e h igh er s ide .
Co rre ct i n g disturbance of st a t ics by me a n s of a
heel - p ad is the pra c t i ca l a pplica tion of these cr ite r i a .
This is, of cou rse, always a c l i n i cal q uestion whi c h
can ne v er be decided b y X-ray alone. Neve rtheless,
it is X -ra y examination that prov id e s the m ost
i m p or t a n t information.
What do we expect to a ch ieve by usi ng a hee l-pad
to reduce obliqu ity?
1. If
scol iosi s is
sufficient to bring t h e
above the lumbosacral,
or if sc o li o s i s is abse n t , the th oracolumbar
j unc tion will be b ro ugh t to stand above the
lu mb o sac r a l , or to a ppro a c h t h is p os i t i o n .
2. If the pelvis is shifted, usually to t h e h i g he r side,
it wil l return to the mid-line.
not
thoracolumbar j unct i o n
3.
Even if the scoliosis (scoliotic c urv e ) has been
b a l a nced, it will decrease a fter o n e h e e l h a s b e en
r a is e d .
All this m u s t be c h ec k e d again b y X-ray. With
each of these p ossi bi l i ti es we obse rve a p os i t i v e or
a negative r e a c t i on , t h e spi nal column e i ther ' a cce pt ­
ing' or ' rej e c t ing' the c o rrection . In cases of 'rejection'
i t would b e wro n g t o 'force' c o rrec t i o n upon the
patient, be c a us e t h is wo uld only in cre ase the s t r a i n
a t t h e b a s e (F i g ure s 3.6 and 3.7).
D e v i a ti on fr om t he p l u m b - li ne c a n us u a l l y be
i n te rpr e t ed as a s i gn t h a t the p a t i e n t p u t s m o re
weight on the leg towards w h ic h the plumb-line i s
s h i fted .
The tra d i t i o n a l reacti o n t o o b l iqu i t y has been
studied by Ill i (1954) a nd Biederma n n and Edi n ge r
(1957), w i th t h e s ubj ect ma r ki ng time i n fro n t of a n
X -r a y screen . A t every step ob l iqu i ty appeared a t
t he b a s e and with i t sco l iosis to th e lower side; the
s u mmi t of the scol i o tic cu rv e ap p e a r ed at L3 a nd the
thoracolumbar junction was b ro u g ht above the
s acrum. A bove T12 the thoracic s p i ne made a (co m­
pe nsatory) scoliosis to the opp o site side, but it was
le ss marked, like a d a m ped w a v e . A cc o rding to
Biedermann and E di ng e r (1957), the thoracolumbar
jun ct i o n forms a k i nd of fixed p o i nt which s h o u l d
n o t swing more than 4 c m fr o m o ne s id e to t h e
o t h e r.
Copyrighted Material
42
Manipulalive Therapy
in
Rehabililation of the Locomotor
System
Figure 3.6 Pelvic aDd sacral obliquity due to a short left leg. (a) Left scoliosis with eleviation of the thoracolumbar
the right; (b) normal l um ba r statics after application of a left heel-pael
junction to
Figure 3.7 Pelvic and sacral obliquity elue to a short left leg. (a) Left scoliosis with deviation of the thoracolumbilr
(b) l e s s pelvic obliquity after application of a left heel-pad, but 110 improvement in lumbar statics
jun ction to the le ft :
Copyrighted Material
rudiographr
FllncJjoJloi [!i1alorny
The relation of scoliosis to rotation under the
influence of lordosis has been studied by Lovett
;!ccording
whom the
spine'
ares
is lordosis, but
direction oC scoliosis if
lhe opposite side in kyphosis. This call be
43
'iff! spinal
there is an increased difference between L5 and T 12,
the latter being more than 4 cm dorsal to L5 (Figure
1
is
l'labby'
llnualance
the
lypical
to
reaction
the rnuscles conlrolling poslure of the
explained by the relative mobility of the vertebral
lumbar spine and pelvis; it may be the result of weak
bodies and the arches during side-bending. If there
abdominal and gluteal muscles, but equally well of
is
the
in
sagittal
proeesse" which an,
?lre locked
therefore rccsist
side-bending; the vertebral bodies, however, arc lice
4).
hack
hip
muscles
Lumbar splltal curvature
J�
(see
clearly dependent
to bend sideways. Hence, there will be more lateral
on pelvic tilt which, in turn, varies according to
flexion of the vertebral bodies than of the arches,
the 'type' of pelvis, as is shown in the following
"Ide of scoil()slS will resuit, the
and ro(;ltion to
spinolls processes rnnaining
in mid-line
IO!1.
can, therefore\ be concluded that
spinal
On the other hand, if there IS kyphosis the joints
curvature is adequate if in the sagitta! plane the
are much freer to move, as the joint facets are in
thoracolumbar junction is behind the lumbosacral
loose apposition. The vertebral bodies, however, are
junction and there is no excessive anteposition of
pre,;scd against
antt:nor edge, and
as
other, pcnticularly
therefore
as free
tbeir
bend
lordosis. Side-bending of the arches will tllus
sdcral promolltory, and
L5 (not
T12 is
far
the most important
coronal
average). In
100
which is double the
than
be the same as, or even exceed, lateral flexion of
criterion is also that the thoracolumbar junction
the vertebral bodies. The result will be either no
rotation at all, or rotation in
opposite direction
from
scoliosIs.
can be
in X-ray
should be vertically above the lumbosacral. If there
of
(Figure
3.8).
with acute lumbago, taken slandll1g
obliquity
base
normal redetion is
scoliOSIS and rotal!on
shift of
pelvis to
lordosis
present)
higher side.
This can also be ascertained clinically
If curvature of the spinal column subserves these
if a subject with a marked lumbar kyphosis when
rules, i,e. the rules of body statics, then it is physio-
sitting relaxed is told to side-bend: while in lordosis
his
in
spinous processe:;
Ime, in
the,
remain airnost
form a
; I am not 8ware of any other criteria of spinal
be infern:cI that the
curvature. Furthermore, it
column
scoliotic arch.
only helps
maintain equilibrium
the whole body but also determines the relation­
ship between the various parts of the body under
Lumbar spinal statics in
plane
the influence of gravity. Wc
sagittal
therefore speak of
equilihnum' subservcd
accordance
38).
the spimil column
the criteria of Rash
Burke
In the sagittal plane we are concerned with what are
(1971) (see p.
called 'normal' curvatures, generally held to comprise
cervical lordosis, thor8cic kyphosis, lumbar lordosis
recumbent or if the position of the pelvis and the
and sacral kyphosIs.
(1961
have the
Sollmann and Breitenbach
for clisproving this
Curvature cannot be evaluated if the patient is
spine
to at
cannot
seen on
the thoracolumbar
single radIOgraph.
accepted view, on the basis of 1000 X-rays of the
entire spinal column. They came to the conclusion
'flat' spine) goes hand in hand with hypermobility
that there is only an 'individual norm': they do not,
anrllack of stahilitv, while greater curvature (in both
however lay down
thai
is a con,llInt
correlation between the ti It of L5 and that of T12,
and more important still, that the T12 vertebra lies
4 cm behind L5 (150 measurements were taken). I
in 200
mysI'lf ccmfirmecl
,ewit,l
lind
also showed that
plumb-Ililc from the external
acoustic meatus passes exactly through the scaphOlds
at its base. The sacral promontory lies 4 mm behind
and the axis of the hip joints 12 mm in front of this
changed in distllrb­
plumb-11IIe. These cI1I1ditions
anct'
dynamics,
of muscular function.
IS
wrote
most eVident in muscle spasm due to acute sCl3tica
It is important to realize that a slight curvature (a
sagittal and
and
coronal
corrcsponds to
rnobility.
The pelvis
pelvis
the spinal column constitute a
functIOnal entity, the pelVIS being the base of the
column and the point of connection with the lower
extremities. The pelvis transfers motion from the
extremitit"
[he ilia,
and acts
a shock absorber.
muscles dnd Iigarllcills attach
themselves to the spine as though to a mast. The
or lumbago in disc lesions, when there is a forward
sacroiliac joints and the pubic symphysis allow
thrust posture (Figure
for some mobility (springing) while guaranteeing
whieh
3.9)
or in flabby posture in
he sacral promontory
forwa
and
Copyrighted Material
44
Manipulalive Therapy in Rehabiliralion of lhe LocomOlOr System
Figure 3.8 Typical posture in acute disc lesions with deviation of the plumb-line and the (straight!) pelvis 10 the side:
'paradoxical' scoliosis vith slight rotation to the opposite side: lumbar kyphosis can be deduced from the shape of the
pelvis
Pelvic types
There are frequent anomalies of the lumbosacral
The function of the pelvis and its influence on body
region: the last lumbar vertebra is a 'transitional'
statics depend largely on its type. We owe this
vertebra and shows by definition that there is harclly
concept to Erdmann (1956) and Gutmann (1965).
any 'norm' and that variation is the rule. ff the
Copyrighted Material
Functional anatomy
and radiography
of Ihe spillal column
45
forward thrust posture, in an acute radicular syndrome
Figure 3.10 Lateral view of the lumbar spine in 'flabby'
posture - a fo rw a rd shift of tbe pelvic promontory - in
this case due to a shortened iliopsoas muscle
variations are asymmetrical, the result may be obli­
pe l v ic gird l e, the sacroiliac j oin ts having the d ec isi v e
quity of the sacrum, c a us in g the c hanges in statics
role.
Figure 3.9 Lateral view of the lumbar spine with
a
d ist ing u is h
The sacr u m is wedge shaped in two directions: (1)
the w h ole structure tapers like a p y ra m id in the
caudal direction; and (2) the upper part (S1-S2)
t apers in a d orsa l d i r e c ti o n ( accord ing to Solonen,
1957), while the lower p art may taper in either
three p elvic types with far-reaching d ifferences in
direct i o n . There is a tuberosity on the i nn om inate
already dealt with. If, h oweve r , there is symm etric a l
variation,
the
most important
con s eq uence is a
change in the length of the sa cru m , a ffec t ing the
postion of the sacral promontory.
Gutmann (1965) and E r d m a n n
(1956)
fun c t i on and possible pathology. The first pr es ents a
bone
long s a crum and high sacral p romon tor y , the second
su r fa c e,
the average or intermediate ty p e , and the third
a
low
p elvic inclination,
a pp r ox i m ately
in
t he
mid d le
of the joint
fitting into an impression on the joint
surface of the sacrum at the lev e l of S2, but there is
For greater cl arity the d iffe re nt criteria are s h ow n
grea t variability and this is not the only t u be r os i t y .
In the AP X-ray there is a d o u bl e contour owing to
the wedge sha p e described above, but this varies
from case to case and is frequently asymmetrical. It
in Tabl e 3.1 and F i gure 3.11.
is of some i m p or tance that the greater the distance
promontory
and
considerable
which the authors call Hohes Assimiliationsbecken,
Normal Becken and Uberlastungsbecken, respectively .
when
between the two contou rs of the j o i nt , the greater
evaluating X-ray findings: the type of pel vis will
the d iv erg ence (or convergence) a n d the na rr ower
All
of
this
sh o ul d
be
b or n e
in
mind
determine the d egre e of lordosis to be expe cte d ,
the joint space appears. C o n ve rsel y , if th e r e is no
while the height of the last intervertebral disc will
con verge n ce and we see only o ne contour, the j oint
de termin e the mobility of the se g men t.
space appears to be wide.
Greater c o nv ergence
(wedge sh ap e) g i v es more stabi li t y , whereas little
convergence accom p a ni e s hypermobility.
The sacroiliac joints
It is
impor ta n t to poin t out that, d espite its
Thanks to the s acroilia c joints an d the p u bi c sym­
unusual shape and the fact that t h e r e are no muscles
phy s is there is some m obili t y of the otherwise firm
moving
the
Copyrighted Material
sacrum against
the innominate,
t he
46
Manipllimnc
Rehllhiillalion of Ihe Locomotor Syslem
vertical from
the promontory
the outer
and to the
(b)
vertical from
(a)
Figure 3.11 Pelvic types. (a) High promontory:
(b) average type: (c) increased pelvic (sacral) inclination
(After Gutmann, 1965)
Copyrighted Material
(c)
vertical from
the outer meatus
Fun Clional
analOmy
radiography of the
and
spinal column
47
Table 3.1 Pelvic ty pes
Crilerion
Typ e
High
I n c l i n a t i o n of s acr u m
Interm ediate
Low
50-70
35-50
1 5-35
\ 5 -30
3 0- 50
50-70
p rom ontory
prom o n t o ry
( degrees)
I nc l i n a t i o n of u p p e r
s u r fa ce of S l (degrees)
Pos i t i o n o f L4 disc
Above t h e l i n e of t h e i l iac
cres t s
At the
h e i g h t o f the
l i n e o f the i l i a c d iscs
Posi t i o n of the .
At
Ecce n t ric ( d orsa l )
pro m o n t o r y i n t h e pe l v i c
t h e c e n tre
At t h e ce n t re o r eve n
r i ng
Rec t a n g u l a r
Wedge s h a pe d
S h a p e of L5 d i sc
R e c t a n g u l a r a n d h ig h e r t h a n L4
Wedge shaped a n d
l owe r t h a n
W e d ge s h a p e d
L4
LS-S I
L4-- L 5
L i t t l e fi x a t i o n of L5
G ood fi x a t i o n of
m o b i li t y
R o l e of i l i o l u m b a r
Wed ge s h a pe d a n d
lower than
L4
L4-- L S
L5
l i ga m e n t
W e i g h t - b e a r i n g s t ru c t u re
l i n e of t h e
v e n t ra l
S h a p e of L5 v e r te b r a
Level o f m a x i m u m
B e l ow the
i l iac c r e s t s
G oo d
fi x a t i o n o f LS
a n d e v e n o f L4
End p l at e of L5
E n d p l a te of L5
A poph ysea l j oi n t
s u r face of
SI , s a c ro i l i a c
j oi n t
Spi n a l c u r v a t u re
Flat
Average
I nc r e a s e d
X-ray statics
H i p j o i n ts in fro n t o f p r o m o n t o ry : t h e
p l u m b - l i ne from t h e o u te r acoustic
m e a t u s coi ncides w i th the ve r t i c a l
A s fo r h ig h ­
The p l u m b - l i n e from
p ro mo n t or y t y pe
f r o m the os n a v icu l a r e a n d l i e s b e h i n d
t h e h ip j o i n t , sl i gh t l y b e h i n d
the
lies
i n fro n t o f t h e h i p
j o int
H y p e r m ob i l i t y , d e ge n e ra t i o n o r
pro l a p s e o f
fro n t o f
the pro m o n t o ry , w h i c h
p romo n tory
Clinical c o n s e q u e n c e s
the o u t e r aco u stic
mea t us l ies i n
B lo c k a g e , d i s c l e s i o n
LS d isc: l i g a m e n t p a i n
sacroi l i ac joint is a true dia rthrosis w ith its own
mobility ( M e n neIJ, 1 952; Weisl, 1 954; Co lachis el al.,
1 96 3 ; Duckworth, 1 970) . A ccord i n g to Duckworth,
' the normal movemen t that occurs is rota tion of
the sacrum a ro u n d the s h ortest and strongest part
of the i n terosseus sacro i liac l i game nts, w h i ch run
from t he i l iac tube rosities to the transverse tu bercles
of the second sacra l vertebra ' . Th is move m e n t can
be described as nutation, a n d the weight o f the spinal
col umn d u r i n g walki ng w i l l le nd to rotate the sacr u m
forward w i t h each step, t h e sacroi l i a c j o i n ts p l a y i n g
t h e part of spri nging shock-absorbers. This rotational
move ment o f the sacrum against the ilium ca n be
palpated and is fa m i l i a r to gy naecologists i n the
manageme n t of labour. However important i t i s that
there should be some mobi l i t y o f the sacro i l i a c j o i n t ,
it should b e very lim ited a n d l ax i ty is u n d esirable.
A t t h e e n d of t h i s section on t h e function a l
anatomy o f the p e l v i s some re m a r k s a re re q u i red
o f L 4 disc
A rt h ro s i s : l u m b o s a c r a l,
s a cro i l ia c and
o f the h i p
about a cli n ically very stri king p h e n o m e n o n w h ich
m a y be called ' pelvic d istorti o n ' . I f the most promi­
nent points of t h e bony pelvis are palpate d , a
peculi a r a pparent d iscrepa ncy e merges: whereas the
posterior spi n a il iaca superior (PSIS) i s higher on
one side, us u a l ly t h e right, the reve rse is fou n d on
palpating the a n terior s p i n a i l i aca superior ( A S I S ) .
T h e i l i a c crest may be l a tera l l y a t t h e same level, o r
t h e r e may be a slight d iffe re nce. O n p a l p a t i o n o f t h e
posterior part o f the i l iac crest a s i m i l a r d i ffe rence
will be fel t to t h a t observed o n the posterior spinae
i l i a cae, confirm ing the fi n d i ngs. This might give the
i m pressio n t h a t one i nn o m i n a te was rota ting against
the oth e r o n a horizo n t a l axis. This cannot be so
beca use we should then find a considera b l e s h i ft of
the pubic bones a t the symphysis.
These c l i n ica l facts may best be i ll u strated a n a ­
tomically by Cra m e r 's d i agram (Figure 3 . 1 2 ) . This
s h ows a one-sided n u tation a n d there fore a l so sl ight
Copyrighted Material
48
Manip u lative Therapy ill Rehab ilitation
of the
Locomotor System
has been foun d t h a t p a l p a t i o n fi n d ings of a
in the l e v e l of the p u b i c b o n e s a t t h e
s y m p h y s i s a n d a t t h e ischia l tube ros i ties do not
co r r e s p o n d to X-ray fi n d i ngs (see Chapter 4 ,
p a l p a tory i l l u s i on , p . 1 00 ) .
It
d i ffe r e n c e
The lumbar spine
A l t h o u g h o n l y a l i t t l e s h orter t h a n t h e t h o ra c i c
spine, t h e l u m b a r sp i n e i s u s u a l l y fo r m e d o f fi ve
vertebrae. H ow e ve r , m o b i l i t y i n a n t e - a n d retro­
fle x i o n as well a s i n l a te r a l be n d ing e ns u r e s most
o f the m o bi l i t y of the t r u n k . In a d d i t i on t o t h i s
i m po rt a n t
a spect, the lumbar s p i n e h a s t o c a r r y m o s t
t h e trunk. The vertebral bod ies as
w e l l a s the a r ch e s a re t h ere fore m o re r o b u s t .
The a p o p h y s e a l j oi n t s give b o t h m o b i l i t y a n d
s t a b i l i t y . They a re v e r t i c a l , t h e ( l a r g e r ) l a te r a l p a r t
of
FiglJfe
3.12 The
mechan ism
of pelvic distortion ( A fte r
Cra m e r , ( 965)
the
w e i g h t of
i n the s a g i ttal pla ne a n d t h e ( s m a l le r ) m edia l p a r t i n
the
coro n a l p l a n e . T h e two p a rt s m a y t h u s t y p i ca l l y
form a n a n g l e : howe v e r ,
t h e sacrum between the i Ji a , p ro d uc i n g
r o t a t i o n o f o n e i n no m i n a t e rou n d a horizo n t a l a x is
a n d o f t h e ot h e r roun d t h e ve r t ic a l .
A l t h o u g h m a n y a t t e m p ts h a v e b e e n m a d e to
v i s u a l i z e by X - r a y so m e of the a s y m m e tr ica l ch a n g es
to be ex p e c t e d . X - r a y d i a g nos i s of t h i s co n d i tion
rema i ns unsat isfactory . T h e re is one c h a n ge , however.
that do es a p pe a r in the X - ra y p i c t u r e , and that i s a
ch a ng e in the statics of t h e l u m b a r spi n e , co n si s t i n g
c l i n i ca l l y i n a s h i f t of t h e p e l v i s to t h e s i d e o f t h e
h i g h e r pos te r i o r i l iac s p i n e , w h i c h m a y p rod u ce
static decompe nsa t i o n of the l um b a r s p i n e , v is i b l e i n
t h e X - r a y p i ct u re t a k e n s t a n d i n g ( F i g u re 3 . 1 3 ) .
ro t a t i o n of
( a)
a n a rc h ,
the
freq u e n t ly
t h e y o n l y form
l a te r a l part po i n t i n g i n to ( h e s ag i t t a l a n d
i n t o t h e c o ro n a l p l a n e . I f there is
the joi n t is e a s i l y v i s u a l ized by X - r a y , b u t
t h i s is not t h e c a s e i f i t is a rch e d . The l u m b o sa c ral
j o i n t , h o w e v e r . i s m a i n l y i n t h e coro n a l p l a n e . As
t h e fi n a l s h a p e of the j o i n t is formed d u r i n g o n to­
g e n e s i s , a nom a lies a n d a s y m m e t ry a r e v e ry fre q u e n t .
T h e s h a pe o f the a r t i c u l a t i o n determ i n es t h e
f u n c tion o f the lum b a r s p i n e ; i t a l l o w s f o r m uch a n t e ­
a n d r e t ro fl e x i o n a n d p r a c t i c a l l y e xc l u d e s a n y a x i a l
rota t i o n as l o n g a s t h e l u m b a r s p i n e is e re c t . I t l i m i t s
.l a tera l fl e x i o n as l o n g a s l o r d os i s i s p rese n t , a s
h as a l re a d y b e e n e x p l a i ne d (see p p . 42 a n d 43). It
the
medial
a n g u la rity
( b)
( c)
Figure 3.13 D i s t u r bed sta t ics i n p e l v i c d i s t o r t i o n . (a) Pelvis s t r a i g h t . o b l i q u i t y at L4 w i t h d e v i a t i o n of t h e l u m b a r s p i n e
t o t h e l e f t a n d s l i g h t s i n i s t rosco l i o s i s . ( b ) N o i m p ro v e m e n t a ft e r a p p l y i ng a l e ft h e e l - p a d . ( c ) A ft e r trea t m e n t o f a
b l oc k e d a t l a n t o - o c c i p i t a l ( ! ) j o i n t . n o r m a l s t a t i c s a o d no p e l v ic d i s t o r t i on
Copyrighted Material
( ollimn
Functional ana /amy and
shou l d , however, be
v e r t e b r a e . A l t h o lJ {' h
caps u l es a re v e r y w i d e
i n t e rv e r t e b r a l fora m e n
a p p o s i t i o n o n l y i n l or d o s i s
the rest o f t h e l u m b a r
i n n e u t r a l a n d k y p h o t i c pos i t i o n s .
im p or t a n t
T h e i n te rv e r t e b r a l d i scs a re t h ic k e s t i n t h e l u m bil r
to bear
49
t h ick, tbe
n a rrower t h a n
fo r a m i n a . I t i s
in
m i nd
that
the
i liolumbar
m ob i l i ty . T h e i r t h i c k n e ss
l ig a m e n t i s a t t a c h e d t o t h e t r a n s v e rs e p ro c e s s o f L5
s o t h a t the fift h l um b a r v e r te b r a t r a n s m i ts i m p u l s e s
i nc r e a s e s from Ll down t o L4; h e n c e , m a x i m u m
t o t h e l u m b a r s p i n e b o t h f r o m t h e s a c r u m a n d from
mob i l i t y i s u s u a l l y fou n d a t t h e L4/5 s e g m e n t . O n l y
the i l i a , p l ay i n g the r o l. e of a s h oc k - a b s o r b e r as w e l l .
;\ s t h e u p p e r s u r f a c e o f t h e s a c r u m i s u s u a l l y con­
spine
a n d a l l ow g r e a t
i n t h e p e l v i c t y p e w i t h a h i g h s a c r a l p r o m o n to r y i s
m a x i m u m t h i c k n e s s a n d m o b i l i t y fo u n d b e t w e e n L5
s i d e r a b l y i n c l i n e d , t he p os i t i o n o f the l u m bo s a c r a l
and S 1 .
a p o p h y s e a l j o i n ts i n a m a i n l y c o ro n a l p l a n e m a y a c t
fo rw a r d g l i d in g
as a preven t i o n
Some of the
X-ray a nato m y
T h e w h o l e o f t h e v e rt e b r a l
h a v e a l re a d y b e e n
cases o f transi t i o n a l
in Figure
d i ffi c u l t t o dete r m lll c
3. I 4 ;
the oval
e n c o u nt e r e d
types. I n
i t may be
vertebra
( r a d i x a rc u s ) a re m o s t
p r oj ects o n t o t h e u p p e r
i s a l u m ba r i z e d
t h e fi ft h v e r t e b r a a n d
i liac crests: i f an
most p r o b ab l y a t t r i b u t a b l e [ 0 l
t h e vertebra beJo\\
of t h e v e rt e b r a l c a n a l i n t h e l o w e s t p a r t
l i n e passes t h rough t h e m i d d l e o f a verte bral body,
I
The m o s t
r e l i a b l e r e fe r e n c e
l u m b a r s p i n e From the p e d i c l e w e may fo l l o w t h e
b r o a d s h a d o w o f t h e l a m i n a i n t h e d i re c t i on o f t h e
.
the two
t h a t l i ne
,
however, t h i s
i t m a y b e i m poss i b l e t o d e t e r m i n e t h e t ra n s i t i o n a l
s p i n o u s p r o c e s s . La t e r a l t o a n d a b o v e t h e p e d i c l e
v e r t e b r a , i n p a r t i c u l a r i f t h e re a p p e a r to be s i x
l u m b a r v e r t e b r a e , w i t h o u t t a k i n g a n X - r a y of t h e
we c a n fi n d t h e u p p e r a r t i c u l a r p ro c e s s ; f r o m t h e
t h orac i c s p i n e . I n s t e a d o f a t r a n sv e r s e p ro c e s s , a
l a m i n a downwards and below the ped icl e , t h e l o w e r
t r a n s i ti o n a l l u m b o s a c r a l v e r t e b r a m a y h a v e a m a s s a
a r t ic u l a r p rocess c a n be t r a c e d i n a c a u d a l a n d l a t e r a l
l a te ra l i s w h i c h ( o nu s a
d i rectio n towards t h e p e d i c l e ( a n d t h e u p p e r a rt i c u l a r
m a s s a l a t e r a l i s o f t h e s a c ru m , a n d m a y e v e n c a u s e
process) o f t h e n e x t ( c a u d a l ) v e r t e b r a . B e t w e e n t h e
s y m p to m s
a rc h for m e d b y b o t h l o w e r
and
.
T h e m ost i m por t a n t
t h e s p i n o u s process 01
a b l y a n a rr o w s p i n a l
v e r t e b r a it i s poss i b l e t o
n a rrowe r a s a res u l t
i . e . t h e c a n a l i s n o t coveTed
e a s i l y recog n ized
i n d i c a to r o f t h e e ffe c t i v e
p ro p o r t i o n b e twe c: 11
s h o r t t h i c k p e d ick"
i n t h e A P proj e c t i o n . W h e re
m i n a a n d the s t e e p
m e e t ( c l os e a bo v e t h e
space ( i f p a r t o f t h e
pse u d o a rt h ro s i s w i t h t h e
, i s probbecome e v e n
r e l a t i ve l y
t h e d i s­
body a n d
I m e rv e r t ebra l
fo r a -
A P v i e w , a l th o u g h
IS
I n t he s a g i t t a l p l a n e ) .
th i s co n d i t i o n s h o u l d n e v e r b e a s s e s s e d a c c o r d i ng
T h e re i s s l igh t d i v e rgence o f t h e a p o p h ys e a l j o i n t i n
to t h e i n te rpe d ic u l a r d i sta n c e , b u t by t h e d i s t a n c e
a c ra n i a l d i rect i o n .
b e t w e e n t h e t w o l o w e r a rt i c u l a r proces s e s , i . e . t h e
T h e l a t e r a l v i c w (Figure 3 . 1 5 ) a ls o s h o w s t h e t h i c k
w i d t h of t h e t ra ns l u c e n c y corres po n d i n g t o t h e s p i n a l
p e d i cl e s , from w h i c h t h e a r t i c u l a r p r o c e s s e s a ri s e .
c a n a l . I n s u c h c a s e s t h e a rt i c u l a r processes p rese n t a
H e r e , t o o , we m a y s e e t h e j o i n t s p a c e i f p a r t o f t h e
j o i nt i s i n t h e coro n a l p l a n e . B e t w e e n t h e u pp e r a n d
s w a l l o w - t a i l s h a p e on X-ray T h e a r t i c u l a r processes
l o w e r a r t i c u l a r p r o c e s s e s l ie s t h e p a rs i s t h m i c a , t h e
s i te w h e re s po n d y l o l y s i s m a y b e s o u g h t . B e l o w t h e
p i ct u r e i s s e e n i n b o t h v i e w s we m a y in fe r t h a t t he
s p i n a l ca n a l i s trefoi l i n h o r i z o n ta l section. ( Ho w e v e r
ped i c l e s w e s e e t h e i O lc n e rt e h r a l
l ie a l m o s t e x a c t l y i n t h e
sca n n i n g v i s u a lizes
\\ h i c h
.
a r e v e ry t h ic k and the j o i nts c l e a r l y v i s i b l e . If a t y p i c a l
r a d i o l o gy CT
s i g n i fi c a n t t he s e
It
is,
,
of course.
zon t a l d i a m e t e r a l m o s t
post e r i o r w i d t h o f t h e
criteria for a s s e ss i n g
c ov e re d b y t h e a r t ic u l a r
d i s c ; i t s h o u l d be b o r n e
t h e se p rocesses o n ly t h e
h y po p l a s i a i s a c o m n l O l 1
p rocess ca n be see n . T h e I
w i t h d is c d e ge n e r: 1 1
sound
I
on to t h e a r t i c u l a r p rocess
fou n d p a r t i c u l a rl y
sm a l l t h i c k s h a d o w .
( w h e r e a n o m a l ie s m o s t o fl e n occ u r ) . T h e r e fo r e i f
T h e l a s t l u m b a r v e r t e b r a d i ffers fro m t h e r e s t i n
many ways: i n t h e side view i t i s wedge shaped a n d
t h e l a s t v e r t e bra s h o w s m a r k e d s i g n s o f be i ng a
t ra ns i t i o n a l v e r t e b r a a n d t h e r e are n o s i g n s o f
w i t h powerfu ll y d e v e l oped t r a n sv e r s e processes i t
m a rg i n a l s cl e ro s i s , b o n e s p u rs o r i nc r e a s e d l a x i ty
s ho w s a t r a n s i t i o n a l s h a pe i n r e l a t i o n t o t h e s a c r a l
( s h i ft ) a d i a g n o s i s of d e ge n e ra t i o n i s u nfo u n d e d . A
,
Copyrighted Material
50
Manip u lative Therapy in
Rehabilitation of the Locomotor System
10
2
11
12
3
4
5
6
7
13
8
9
14
(a)
(b)
( i)
( ii )
�
1
(e )
( iii )
0
o
/
(d )
Figure 3.14 Com p a r i s o n of t h e a n a to m i c a l s t r u c t u r e s i n t h e d o rs a l a s p e c t of t h e l u m b a r s p i n e a nd t h e s a c r u m (a) w i t h
t h e a n t e ro poste r i o r X - r a y ( b ) a n d t h e v e n t r a l a s p e c t ( e ) . 1 , S p i n o u s process; 2 , u p p e r a r t i c u l a r process; J , l a m i n a ;
4 , p a r s i n t e r a r t i c u l a r i s ; 5 , j o i n t s p a c e ; 6 . low e r a r t i cu l a r process; 7 . s p i n a l ca n a l ; 8 , posterior s p i n a i l iaca supe rior: 9 ,
dorsal p a r t o f t h e s a c ro i l i a c j o i n t; 1 0 , disc: 1 L t r a n s v e rse p rocess: 1 2 , v e r t e b r a l bod y ; 1 3 , p e d i c l e ; 1 4 , v e n t r a l p a r t o f t h e
s a c ro i l i a c j o i n t . ( d ) D e Seze ' s d i a g r a m v i s u a l i z i n g t h e A P X - r a y o f l u m b a r ve rtebrae: ( i ) t h e v e r te b r a l bod y , (Ii) t h e
v e r t e b ra l a r c h , ( iii) t h e p e d i c l e s , ( i v ) t h e e n t i re v e r t e b r a
Copyrighted Material
Functio l / a l a l / atomy a n d radiography of th e sp inal
column
51
7
6
5
Ij.
7
2
3
Figure 3.15 Co m pa ri s o n of t h e a n a tomical s t ru c t u re s in the l a te r a l v i e w of t h e l u m b a r spine (model) a n d t h e X-ray.
1. Ped icle: 2, p a rs i n t e ra r l i cu l a r i s ; 3 , lowe r a rt i cu l a r p rocess; 4 , up p er a r t i c u l a r p roce s s : 5 , joint space ; 6 , i n te rverte b r a l
fora m e n : 7 , t ra n s verse p r ocess
v a l u a b l e s ig n of d i sc h y p o p l a s i a i s r e d u c e d wi d t h o f
bot h v e r te b r a l margins a dj a c en t to th e h y p o p l a s t i c
disc . A l t h o ug h w e u s u a l l y r e l y o n la teral v i e ws fo r
t i o n s h o u l d be p rop o r t i on a t e to scoli o s i s a n d c a n be
modi fi e d by t he degree of lordosis ; if rota tion is d is­
proportiona te, o r l i m i ted to one or two i n terverte b r a l
t h e assess m e n t of d i sc s , marke d asy m metry in t h e
segmen ts o n l y , i t c a n be a s ign o f d istu rbed fun c t i o n .
AP v i e w m a y be o f s o m e i m por t a n c e , p a rti c u l a rl y at
the LS-S 1 i n ters p ac e , as here assess m en t may be
d i ffi c u l t in view o f t h e fre q uen c y of a n oma l i es . A
process a n d the ped i c l es i n t h e d ir e c t i o n opp o s i t e to
marked nar rowing on one s i de m a y t h e n poin t t o
becomes w i d e r a n d t h e ar t i c u l a t ion is better vis u a l ­
d isc d e gen e ra t ion ( Fig u r e
ize d ; t he t r a n s v e rse p rocess i s sh o r t er ( F i g u re 3 . 1 7 ) .
3 . 1 6) .
R o t a t i o n is recognized
by
a
s h i f t of th e s p in o us
t h a t of rot a t ion . On t h e sid e of ro tation t h e p e d i c l e
Rotati on sho u l d never b e eval u a t e d o n t h e basis o f
o n e s i n g l e sign
E v a l ua t i o n o f fu nct i o n
F o r eval uation o f fu n c tion and
(such
a s devia tion o f t h e s p i n ou s
p roces s ) . T h e a s s ess m e n t of lateral fl e x i o n ( scolios i s )
its
possible d i s ­
t u r b a n c e s , p ictures m u s t b e ta k e n u n d e r standa rd
cond itions (see pp. 36-3 8 ) .
A ssessment of r o t a t i o n is of value, because rota-
i s ca r r i e d out a c cord in g t o the p rin c i p l e s o f bod y
sta tics .
In the lat e ral v iew we assess lord osis or k y p h o sis
a forwa rd or bac kward s h i ft . A l oca l
a s wel l as
Copyrighted Material
52
Manip uia live Therapy in
RehaiJililGlion of Ihe LocomOlor System
Figure 3.16 The a n t e rior lower edge o f the verte b r a l b o d y o f L5 i s lower on the l e ft s i d e (artTow) in re l a t i o n t o t h e
s a cr u m , h e n ce t h e L 5 d i s c is n a rrowe r on t h e l e ft : com p e n s a t o ry l u m b a r sco l i osis w i t h l e ft ro t a t i o n
i n te r r u p t i o n o f t h e l o rd o t i c l i n e
or of kyphosis,
b e t w e e n t w o v e r t e b ra e , c a n be a s i g n
of
d i s c l e s ion .
A s h i ft ( f o r w a r d s or b a c k w a r d s ) m a y be a s i g n o f
i n c r e a s e d m o b i l it y - l a x i t y . T h i s m a y be p a r t i c u l a r l y
c o n s p i c u o u s d u ring a n t e - o r r etr o fl e x i o n . V e ry s l i g h t
p r op o r t i o n a l s h i fts in a n te- o r r etr o fl e x i o n i n youn g
p a t i e n t s , see n a t X - ray e x a m in a t i o n , c a n be rega rded
a s n o rm a l . Tw o d i a g n o s t i c p itfa lls must b e s t r e s s e d .
The fi r s t i s t h e i n c o n gru o u s s u rfa ces o f two a dj a ce n t
v e r te b r a e , o cc u r ri n g m o s t fr e q u e n t l y betwe e n L5
a n d t h e sacru m ; th e u p per s u r f a ce of S l in such c a s e s
i s u s u a l l y s l i g h t l y l o nger t h a n the l o w e r s u rface o f
L 5 , a n d look i n g
at the
edge of t h e adj a c e n t
o f a n a n t e r i o r s h i ft
the a n t e r i o r e d ge) of a posterior
pos terio r
ve r t e b ra e o n e gets t h e i m pre s sion
o f L 5 , or ( l oo k i n g at
s h i ft of L5 . The second p i t f a l l i s s l ig h t rota ti o n : h e re
the p os t e r i o r a n d a n t e r i o r m a rg i n s of the v e r t e b ra e
fo rm a d o u b l e co n t o u r w h i ch c a n be m i s t a k e n for a
s h i ft .
to h y p e r m o b i l i ty m u s t , o f c o urs e ,
from true spo n d y l o l isthe s i s ( w i t h
s p o n d y l o l ys i s ) a n d fro m degenerative spon d y l o l i s ­
t h e s is ( t he p s e ud o s p o ndy l o l i s t h e s i s o f J u ngha n n s ,
1 930) d u e to d e fo r m i ty . t h e b e n d i n g fo rwa rd o f a n
These s h i fts
due
be d i s ti n g u i s h ed
Copyrighted Material
Func/ional a n a /amy
and ra diography of (he sp inal co/limn
53
Figure 3.17 R o t a t i o n o f l u m b a r v e r t e b r a e
with l a t e r a l s h i ft o f t h e s p i n o u s processes
a n d p e d i c l e s i n re l a ti o n t o the v e rte b r a l
bodies
u p p e r a r t ic u l a r p rocess ( m ost freq u e n t l y
w h i c h t h e v e rt ebra a b o v e gl i d es fo r w a rd
L5 )
over
m a y be d e s c r i b e d a s a s o r t of l e v e r a ge (J i r o u t , 1 95 6 ) .
N a r rowing o f a n i n te rv e r t e b r a l d i sc, c a u s e d b y
.
d egeneration , m a y some t i m e s be v i s i b l e o n l y i n a n t e ­
or re trofle x i o n . I n s u c h c a s e s we see exagge ra ted
X - ray studies of move m e n t
X - r a y p i c t u re s
in
the
upright
posi t i o n
a n te r i o r n a rrow i n g of the d i s c ( w i t h o u t compe n s a t o r y
may
not
p os t e r i o r w i d e n i ng) i n a n t e fl e x i o n a n d e x a gge r a t e d
provide a n y c l u e s t o d i s t u rbed f u n c ti o n ; t h ose t a k e n
poste r i o r n a r r o w i n g ( wi t h o u t c o m pe n s a t o r y a n te r i o r
i n a n te- o r retrofle x i o n o r l a t e r a l fl e x i o n m a y t h e n
w i d e n i ng ) i n retrofle x i o n .
reve a l s o m e i r re g u l a ri t y . W e m a y d i s t i n g u i s h seg­
M o b i l i ty s t u d i e s a r e u s u a l l y m a d e w h e re t h e re i s
m e n t s o f i n c re a s e d o r l ow e r e d m o b i l i t y . In a n te - a n d
a c l i n i c a l rea s o n f o r d o i n g s o , i . e . i f move m e n t i n
retrofle x i o n i ncreased m o b i l i t y m a y t a k e t h e fo r m o f
some speci fic d i recti o n c a uses s y m p t o m s . A cond i t i o n
v e n t r a l o r d o rs a l s h i ft , respect i ve l y ( ' d isc r o l l i n g ' ) .
i n w h ic h t h is t y p e o f e x a mi n a t i o n i s p a r ti c u l a rly
A s has a l re a d y b e e n p o i n te d o u t , v e r y s l ig h t pro­
i m po r t a n t i s s p o n d y l o l is t h e s i s , beca u s e i t i s a d v i s a b l e
port i o n a l s h i ft i n g m o v e m e n t s in all se g m e n ts may b e
to asce r t a i n w h e t h e r t h e s p o n d y l o l i s t h e s i s is fi x e d o r
cons i d e red n o r m a l , p a r t i c u l a r l y i n y o u n g s u bj e c t s
m o b i l e ; i t i s t h e l a t t e r t h a t c a uses s y m p t o m s a n d h a s
(J i r o u t , 1 95 6 ) . The re is o n e i n te r e s t i n g exce p t io n : i n
a te n d e n cy to d e t e r i o r a t e .
t h e l u m b osacra l segm e n t t h e re s o m e t i m e s o c c u r s
a
I n l a t e r a l fl e x i o n i t i s m o s t i m p o r t a n t to corre l a t e
' p a ra d o x i c a l ' s h i ft , i . e . a d o r s a l s h i ft d u r i n g a n te ­
t h e d e g re e o f fl e x i o n a n d rota t i o n w i t h rega rd t o t h e
fl e x i o n a n d a v e n t r a l s h i ft d u r i n g r e t r ofl e x i o n . w h i c h
degree o f lordosis (see p.
Copyrighted Material
43 ) .
54
Manip uialive Therapy in Rehab ililOlioll of !he Locomo!or Syslem
The thoracic spine
coro na I p l a n e as if o n the p e r i p h e r y of a cylinder
w hose cen tre is i n front of t he ve rtebral b o d y T h i s
s h ape would a l low for considera b le r o ta t i on w e re it
n o t fo r the r i bs and the i n terve rtebral d iscs. S i d e ­
a n d fo rward-bendi ng, too, a re l i m i te d m a i n l y by rh e
ribs, a l t h oug h t h e l a tter movem e n t is a l s o h e l d i n
check b y t h e i n te r- a n d s u p r a s p i n a l l iga m e n ts. B ack­
bending i s l i m i ted m a i nly by a p p o s i t i o n locking of
the articular a n d t h e s p i nous processes. Because of
t his relativel y l i m i ted m o b i lity, t ru n k r o t a ti o n was
,
.
Fun ctional a n atomy
The thoracic s p i n e (Fig u re s 3 . 1 9 a n d 3 . 20) is the long­
est part of the s p i n a l col u m n a n d that which e n j o ys
the least m o b i l i t y The main reason for th i s i s i ts c l ose
re l a t i on s h i p to the thorax but i t is a lso related to t h e
t h i n ness o f th e i n te rve rtebra l d iscs. Th e apophyse a l
j o i n ts a re a l m ost ve rtical a n d s h o w a s l i g h t t i l t i n the
.
Figure 3.18 The t h o ra co l u m b a r
( sJde �exion) begi nning a t LS
spi n e d uri n g t r u n k ro t a t i o n with the pe l v i s fixe d : t h e re is both rot a t i o n a n d s c o l iosis
Copyrighted Material
FlinCl iulla! anatumy and
be l i eved
to take
p l a ce m a i n l y i n t h e l o w e s t t h or a c i c
55
the
l o west p a rt o f t h e t h o r a ci c spi n e ( l h e t h o ra co l u m b a r
j u n c t i o n ) w a s refu t e d by S i n g e r a n d G i l e s ( 1 9 90 ) .
Fu n c t i o n a n d i ts d i st u r ba nces a re of p a r t i c u l a r
thoraco l u m b a r j u n c t i o n . T h is m a y
b e b e c a u s e i n t h i s re g i o n moveme n t c h a nges fro m
o n e l y p e 1 0 a n ot h e r w i t h i n a s ing l e s e gm e n t . as c a n
b e d e d u c e d fro m t h e s h a pe o f t h e a p o p h ys e a l j o i n ts :
on a s i n g l e vertebra t h e u p p e r a r t i c u l a r pr oc e s s e s
m a y be i n t h e co r o n a l p l a n e a n d t h e l o w e r m os t l y
i n t h e s a g i t t a l p l a n e ( Fi g u re 3 . 1 9 ) . As we h a v e
a l re a d y s e e n (see p . 4 3 ) , w i t h t h e p a t i e n t m a r k i n g
t i m e t h e t h o ra co l u m b a r j u n c t i o n fo rms a re l a t i ve l y
f ix e d poi n t w h e re l u m ba r sco l iosis to o n e s i d e cba nges
to thoracic s c o l i os i s to t h e o p p o s i t e s i d e . T h e
t h o raco l u m ba r j u n c t i o n i s a l s o t h e o n l y tra n s i t i o n a l
regi o n w here t w o v e ry m o b i l e s e c t i o n s of t h e s p i n a l
c o l u m n m e e t : d y s f u n c t i o n i n t h i s r e g i o n t h e refore
re s u l t s in w i d e s p r e a d s p a s m .
coil l m n
T h a t t r u n k ro t a t i o n ta k e s p l a c e m a i n l y i n
segm e n t s , t h o s e l e a s t fixed b y t h e r i b s .
s i g n i fi c a nce a t t h e
radiog raphy oj Ihe spinal
Th e y de m o nstra t e d
by
s o m e ro t a t i o n o f
fe w d e g r e e s t a k e s p l a ce
a
CT d u r i n g t r u n k r o t a t i o n t h a t
both i n
thro u g h o u t a l l t h e seg m e n ts
To e x p l a i n the poss i b l e m e c h ­
t h e l ower t h o r a c i c a n d
of t h e l u m b a r sp i n e .
a n i s m , I e x a m i n e d t ru n k r o ta t i o n by X - r a y ( L e w i t ,
1996) a n d d e m o n s t ra t e d th a t s i d e fl e x i o n d o e s
i n deed t a k e p l a c e d u r i n g t r u n k r o t a t i o n , i . e . t h ere i s
a c o u p l e d m o v e m e n t w h i c h i s v e ry s i m i l a r to w h a t
w e see d u ri ng s i d e - b e n d i ng ( Figure 3 . 1 8 ) .
A n o t h e r re g i o n o f t ra n s i t i o n a n d i n c r e a s e d v u l ­
n e ra b i l i t y is t h e c e r v i c o th o r a c i c j u n ct i o n d o w n to
T3-4 , b e c a u s e i t is h e re t h a t m o v e m e n t s of t h e h e a d
a n d n e c k e n d , a s a r e m o s t c l e a r l y s e e n i n ma x i m u m
a n t e - a n d re t r o fl e x i o n . T h e s a m e i s t r u e fo r s i d e ­
be n d i n g a n d r o t a t i o n i f t h e c e rv i c o t h o r a ci c j un c t i o n
Figure 3.19 C o m p a r i s o n of t he a n a t o l1l i c a l s t ru c t u res in t h e d o rs a l v i e w of t h e t h o r a c i c s p i n e ( s k e l e t o n ) w i t h t h e
a n l c ropos t e r i o r X - r a y . I , S p i n o u s p rocess: 2, p c cl i c l e s : 3 , r i b s ; 4 , t ra n sve rse process: S , t r a n s v e rsocos t a l j o i n t
Copyrighted Material
Manipulative Therapy
56
is held
upright
.
ill
Rehabili llltion of the
Function is partic u l a r l y
Locom otor System
v u l n e ra b l e
h e r e , beca u s e t h e v e ry m o b i l e c e r v i ca l s p i n e m e e t s
the m uc h less
with i ts
g i rd l e
,
mob
ile
t h oracic s p i n e . T h e s h o u l d e r
p o w e r fu l m u sc l e s , i s
a lso
a ttached
to
t h is j u n c t i o n .
A l l t r a n s i ti o n a l
r e g i o n s a re r i c h i n a n o m a l i e s .
m a y be a r u d i m e n t a r y t w e l ft h r i b or a
( r u d i m e n tary) l u m ba r L 1 ; r e ma r k a b l y , a c e rv i c a l r i b
(C7) i s q u i t e com m o n , w h e r e a s w e r a re l y fi n d a
r u d i m e n ta ry fi r s t r i b .
T h e re
The ribs
r i b s a re attached t o t h e vertebrae a t t h e
tra nsversocost a l a n d costoverte b r a l j o i n t s . The h e a d
of the r i b a r t i c u l a te s w i t h t h e u p p e r m a rgin o f t h e
b o d y of t h e corresp o n d i n g v e r t e b ra a n d w i t h t h e
The
l ower m a rg i n o f
t h e n e x t v e r t e b ra l boel y a b o v e . T h e
of t he h e a d o f t h e ri b (crista capitu l i ) i s
a t t a c h e d to the i n te rverte b ra l el i s e b y l iga m e n ts. The
firs t rib is a n exce p t i o n in t h a t i t a r t ic u l a t e s
e x c l u s i v e l y w i t h t h e b o d y o f t h e fi rs t thoracic
verteb r a . The n e c k o f the r i b fi xeel b e t w e e n the
costove r t e b r a l and costotra n s v e rs a l a rticu lation fo r m s
a n a x i s f o r r i b m o v e m e n t . Th i s a x i s i s h o r i z o n t a l i n
t h e t ru e ( v e r t e b roste r n a l ) r i bs and p rod uces a
m o v e m e n t by w h i c h t h e s t e r n u m is l i fteel a n d at the
same ti me t h e thorax broa d e n s . In the fa lse ( v e r t e ­
b roc h o n d ra l ) r i b s the a x i s is o b l i q u e , l a terodo rso­
ca u d a l , a nd p ro d u c e s a w i n g- l i k e move m e n t . T h e
l a st two r i bs ( free r i b s ) a re a t t a c h e d t o r u d i m e n ta ry
c e n tre
t r a n s v e rse processes by c o n n e c t i v e t i s s u e o n l y ( s y n ­
d e s m os i s ) .
Co n se q u e n t l y ,
t h e re
n o j o i n t move m e n t re s t r ic t i o n
is no j o i n t a nd
can a r ise h e r e .
h e nce
Figure 3.20 C o m p a rison o f t h e a n a t o m ica l s t ructu res i n t h e l a t e r a l v i e w o f t h e s k e l e t o n o f t h e t h o r a c i c s p i n e w i t h t he
X - ra y . I , L o w e r a r t i c u la r p rocess; 2, j o i n t space; 3. u p p e r a rt i c u l a r p rocess: 4. i n t e rverte bral fo r a m e n : 5, pe d i c l c s : 6. ri b :
7 , t ra n sve rse process
Copyrighted Material
Fl lnctional anatomy alld
d e fo r m i t y ,
The X-ray picture
coillmn
w hi c h
I
the
the
1 11
osteo-
t ho r a c i c spine a s
I n t h e A P v i e w , v i s u a l izm l () o
57
v e r t e b r a l a rc h is m u c h l ess d e t a i l e d t h a n i n t h e
c h o n d ro s i s .
In a s y m m e t r i c a l move m e n t r e s tr i c t i o n of the ribs
l u m b a r s p i n e . I n a d d i t i o n t o t h e v e r t e b ra l bod i e s a n d
t h e re may b e a s y m m e t ry of the d i s ta n c e be tw e e n the
i n t e r v e r t e b r a l d i sc s , w e s e e t h e s p i n o u s processes
a rc h e s o f the r i b s .
a n d t h e p e d i c l e s (see F i g u re
3. 19).
It s h o u l d be b o r n e
i n m i n d t h a t fro m a b o u t T 4 t o T l O t h e t i p o f t h e
s p i n o u s p rocess i s s e e n a t t h e l e v e l o f t h e b o d y o f
The cerv i c a l sp i n e
t h e n e x t v e r t e b ra b e l o w . T h e c h a ra c te r i s t i c fe a t u re
is the c o s t o v e r t e b r a l j u nc t i o n , the h e a d of t h e r i b
agaJ llst t he i n te rv e rt e b ra l d is c a n d t h e o v e rl a p p i ng
s h a d o w o f t h e costa l
cess. A s t h e facets o f t h c
I
pro­
t i l t e d from d o rsoe r a n i ,l l
T h e c e r v i c a l s p i n e i s th e m o s t m o b i l e s ec t i o n o f t h e
w h o l e s p i n a l c o l u m n . T h e c r a n i oc e r v i c a l j u n c t i o n i n
pa rticu l a r is the
their repercussi o n s
t h e vertica l p l ane) t h e
m u s c u l a t u r e ; d i st
a re , t h e refore,
ized i n t h e A P v i e w
a d e q u a te t re a t m e n t
rc ll e x e s w i t h
1f1
pos t u ra l
t h i s region
and
t he i r
t h oracic r i b s , i f t h i s t i l l
I n t h e l a te r a l v i e w
v c rte b r a l
a r c h e s a re p a r t l y o ve r l a p pe. d
X -ray tech n i q u e
I n o r d e r to o b ta i n p i c t u re s t h a t c a n b e e v a l u a t e d fo r
t h e p i c t u res a re c l e a r , w e g e t a g o o d v i e w o f t h e
i n t e rv e r t e b r a l fo r a m e n a n d e v e n o f t h e j o i n t f a c e t s
f u n c t i o n , a d e q u a t e s ta n d a rd
( a r t i c u l a r process e s ) . T h e t h o r a c i c s p i n e a bo v e T 3
a d h e re d to. The u s u a l t e c h n i q u e , w h i c h v i s u a l izes
i s u n fo r t u n a t e l y h i d d e n b y t h e s t r u c t u re s o f t h e
s h o u l d e r g i r d l e a n d m us t be v i s u a l i z e d e i t h e r b y
o b l i q u e v i ews o r b y t o mogra p h y .
I t m a y b e d i ft1 c u l t t o n u m be r t h e v e r t e b r a e i n t h e
t e c h ni q u e s m us t
be
the cra n i o ce r v i c a l j un c t i o n p oo r l y in t h e s i d e v i e w
a n d n o t a l a l l i n t h e A P v i e w , i s n o t e v e n a d e q u a te
to s h o w t h e a n a to m i c a l d e t a i l s p ro p e rl y a n d i s
c o m p l e tely u s e l e s s for t h e e v a l u a t i o n o f fu n c t io n .
l a te r a l v i e w , a s T l c a n n o t b e s e e n a n d i t i s h a rd t o
I n t h e A P v i ew t h e e n ti re c e rv i c a l s p i n e s h o u l d b e
re cog n i ze T 1 2 . I t i s t h e refore usefu l t o r e m e m b e r
v i s i b l e , from t h e c ra n i oc e rv i c a l j u n c t i o n ( fora m e n
t h a t t h e lowe r a n g l e o f
m a g n u m w i th t r h '
u s u a l ly
at t h e h e i g h t o f T7 , t h e
the
t h o ra c i c v e r te b r a e .
fo r k o f t h e t r a c h e a
the
s u ffic i e n t , b u t 1 5
d i a p h ra g m a t T91 1 0 .
1 t o t h e fi r s t
the upper thoracic
p a ti e n t i s p l a ce d a s ro l
1 95 6 ) : fi r s t he i s
t h e e x t e n d e d l eg :,
Eva l uating X - r a ys
As i n a l l pa r t s o f t h e
li re i s
i m p orta n t h e re from t h e p o m ! o f v i e w o f fU li c t i o n ,
the
m o s t s i g n i fi c a n t c h a n g e s b e i n g sco l i os i s a n d
i n c re a s e d k y p h o s i s . H e re a ga i n i t m u s t b e p o i n t e d
o u t t h a t i t i s esse n t i a l for u s t o k n ow w h e th e r t h e
each side of the
one on
a s ke d t o
l i e d o w n , w i t h o u t u s i n g h is a rm s , i n t h e p os i t i o n t h a t
i s m o s t n a t u r a l t o h i m ( t h e pos i t io n m a y b e c h e c k e d
b y r e pe a t i n g t h e p ro ce d u r e ) . I f t h e h e a d r eg u l a r l y
yet
d e v i a te s f r o m t h e m i d - l i n e t h i s m us t n o t be c o r ­
r e c t e d , b e c a u s e t o d o s o w o u l d e i t h e r correct o r
a n o t h e r I m p o r t a n t a s p e c t o f c u r v a t u r e : t h e m o re
p ro d u c e c e r v i c a l sco l i o s i s a nd a t t h e s a me t i m e
m a r k e d it i s , t b e l e s s m o b i l e t h a t s e c t i o n of t h e s p i n a l
i n d uce a x i s r o t a t i o n a n d l a tera l d e v i a t i o n of t h e a t l a s .
c u rv a t u re
is
in
s t a t i c e q u i l i b ri u m .
T h e re
is
co l u m n w i l l b e , a n d c o n v e rs e l y , a fl a t t h o r a c i c s p i n e
I t i s t h e r e fo r e n e c e s s a ry to s h i ft t h e fi l m a n d t he
i s accom p a n i e d b y h y p e r m ob i l i ty , w h i c h i s o f c o n ­
s i d e r a b l e c l i n ic a l s i g n i fi c a n c e
X - r a y t u b e a c c o rd i n g l y . The p a ti e n t n o w o p e n s h i s
mout h as wide
is placed
1 0 u n ti l t h e
between his teet h ,
seen i n t h e u p p e r t h or a C i C
g l a be l l a a nd t h e 1 1
C h a nges i n f u nc t i o n
h o r i zo n t a l
h e a d i s o ft e n
s i g n s of s u d d e n r o t a t i o n
plane. For this a
or w i t h a s u d d e n d e v i a t i o n
n e ce ss a r y .
toge t h e r w i t h s i g n s o f
d i a g n ose d b y a s h i ft o f
W e a re n o w
ce n t r a l r a y m us t
o n e fi n ge r
a nd t h e p e d i c l e s i n t h e
b e l o w t h e upp e r
a b ove t h e
o f rota t i o n .
poster i o r m a rg i n o f t h t: oCCi p i t a l lor a m t: n ( F i g u re
S h i fts a re h a r d l y e v e r s e e n i n t h e l a te r a l v i e w o f
the t h o r a c i c s p i n e , n o r i s k y p h o t i c a ng u l a t i o n b e t w e e n
3.21 ) .
tube. The
I f t he pa t i e n t h a s no t e e t h t h e c e n t ra l r a y
p a s s e s t h ro u g h a p o i n t o n e fi n g e r b e l o w t he u p p e r
t w o v e r t e b r a e t h a t i s s i mp l y a tt r i b u t a b l e t o c h a n ge s
g u m s to t h e pos t e r i o r ma rgi n o f the foram e n m a g n u m .
i n fu n c t i o n . A n g u l a t i o n m a y , h o w e v e r , b e d u e t o
T h e d is t a n c e fro m foc u s t o fi l m s h o u l d b e 1 m .
Copyrighted Material
58
Manipulative Therapy in
Rehabilitation of the Loconwlor
Syslem
Figure 3.21 X-ray tech n i q u e of the ce rvica l spine accord i n g to S a nd b e rg ( 1 955). (a) F oc u s i n g the ce n t r a l r a y in t h e
a n t e ropos t e r i o r v i e w w i t h t h e aid of a s t r i n g , the h e a d in a horizon ta l p o s i t i o n ; (b) foc u s i n g t h e X - r a y t u be i n the
l a t e r a l v i e w a t t h e m a s to i d process
F i n a l l y , we correct a n y rotatio n o f the pati e n t ' s
e y e s o n s o m e obj e c t at eye- l e v e l , to kee p the h e a d
h ead , b eari n g in m i n d t h e possib i lity o f as y m m e try
in a
(th e u p p e r tee t h are a u s e f u l l a n d m ark) .
fl e xion m us t be c o r r e c te d .
I t is poss.ib l.e to proceed in an a nal ogo u s m a n n e r
s ta n d ard
position; h ead
rotation
o r l a te ra l
T h e ce n tra l ray i s foc used not a t t h e m i d - cervical
(c e n tre
of
t he
fil m )
but
at
wit h t h e patie n t s e a te d , w h i c h is m ore di fficu l t b u t
region
has t h e a d v a n tage of being perfor m e d u n d e r t h e
proc e s s . Th is yields an u n d is t orted view o f th e base
the
mastoid
i n fl u e nce o f bod y s tatics . N e v e rt h e l ess, t h e re can b e
o f the sku l l a n d y e t ca uses no d i s t o r t i o n of the l o wer
diag n o s tic advan tage if t h e sid e view, which m ust
cervica l spine ( b ecause the base o f the skull is w ide,
a l ways be take n w i t h the patie n t seate d , reve a l s
w hi l e t h e cervical v e r te b r a e are n a rrow) . In additi o n
d i screp a n cies w h e n c o m p ared with t h e
AP
v i ew
take n w i t h the patie n t s u pin e . In s u c h cases t h e
AP
we ac h ie v e correct e x posure of b o t h t h e base o f t h e
sku l l a n d t h e cranioce rvical j u nctio n a n d
of the
v i ew c a n a l w a y s be repe a t e d in t h e si t ting pos i t i o n .
c e rv ic a l v e rte brae . The distance from foc u s to fi l m
S o m e a ut h ors d is l i k e t h e o p e n - m o u t h t ec h n i q u e
s h o u l d b e .1 5 0 c m o r more . W i t h t his tech n i q u e
because t h e man d i b l e overlaps t h e mid-cerv i cal s pin e ,
pict ures o f t h e cra n i o cervical j u n c t i on are so cl ear
a n d prefer to t a k e t h e picture w h i l e t h e patie n t
th a t tomogra p h y is s e l d o m n e ce ssary.
r h y t h m ic a l ly o p e n s a n d s h u t s h i s m o u t h ; i n t h is w a y
t h e shadow o f t h e m a ndib l e is bl u rred. The tec hniq u e ,
h owever, pres e n ts t h e danger of a s l i g h t s haki n g o f
t h e h ead , w h i c h w i l l cau s e bl urrin g o f t h e image o f
t h e a p o p hyseal j oi n t s o f t h e cranioce rvical j u n c t io n .
I n t h e l atera l view t h e patient i s s eated re l ax e d i n
Asses s m e n t of the q u a l ity of X - r a y
p i ctu res
B e fore e v a l u a t i n g an X -ray o f t h e c e rvica l spin e ,
partic u l a r l y w h e re fun ctio n i s co n c e r n e d , we m us t
cm or
3.22 ) . I n t h e
A P v i e w we fi r s t m a k e sure that we c a n s e e b o th
2 4 x 30 c m , a n d m u s t be p lace d s o t h at t h e X -ray
occipital c o n d y l e s , t h e a t las a n d t h e ax i s with both
fro n t o f a vertic a l X -ray casse t te ; n o Potte r - B u c k y
d iaph r a g m i s n e e d e d . T h e fi l m may be
1 8 x 24
assess i t s q u a lity a s a p i c t u r e (Fig u re
s h ows t h e base of the sku l l wit h t h e s e l l a turcica , t h e
tra n s versocostal fo ramina (fora m i n a o f the verte bra l
h a r d p a l a te a n d t h e cervical s p i n e d own to C7 , if
artery) , a n d at t h e c a u d a l e n d , t h e (irst t h o r a c i c
possib l e with t h e first two th ora cic v e r t e b ra e . T h is ,
v ertebra. I f t h e v i e w i s co rrec t we see t h e c l e f t
howev e r , i s poss i b l e o n l y i n s u bj ects ( u s u a l l y w o m e n )
b e tw e e n t h e u p p e r and l o w e r fro n t te eth in mid - l ine ,
with v e r y tapering s h o u l d e rs . The patie n t nxes h i s
toge t h e r w i th t h e ce n tre of t h e o d o n toid p rocess and
Copyrighted Material
Functional anatomy
and
radiography of the
59
spinal colLlmn
Figure 3.22 A n a t o m i c a l s t r uctures o f the c r a n i o c e r v i c a l j u n c t i o n , a n t e ropos t e r i o r v i e w . 1, L o w e r edge o f the c l i v u s ;
2, fo ra m e n m a g n u m ; 3 , occi p i t a l co n d y l e : 4 , l o w e r e d g e o f t h e a n t e r i o r a r c h of t h e a t l a s ; 5 , l a t e r a l t r i a n g l e ; 6 , fo r a m e n
t r 3 1l s v e rsa r i u m of t h e a x is: 7 . l o w e r con t o u r o f t h e s q u a m a occipi t a l i s ; 8 , m e d i a l t ra n s l u ce ncy o f t h e a t l a s ; 9 , t r a n s v e rse
p rocess o f t h e a t l a s : 1 0 , l o w e r e d ge o f the p o s t e r i o r a rc h o f the a t l a s : 1 1 , ped i c l e of the axis: 1 2 , l a m i n a of the a x i s
o f t h e ch in. T h e cervica l spi n e as a w h o l e must lie
be t w e e n the two halves of th e
man d ibu l a . E v e n i f each of these structures is asym­
metrical there a re suffi cient la ndm a r ks by w h ich to
recogni ze dis tor tion. A pict ure without the cra nio­
ce rvical j u ncti on and the fi rst thoracic verte b r a with
the thoracic outlet is insuffici ent fo r o u r purpose .
s y m metr ica l l y
T n the l ate r a l view w e need t o see the base of
t h e s k ull w i th the sella turcica , the c l i vus d o w n to
the ba si on , t h e
p o st e rio r
margin of the
fora men
magnum, the hard p a l ate , the odontoid process and
If po s s i b l e even the
fi rst thoracic verteb ra s hou ld be see n, but in heavily
the cervical spin e down to
C7 .
bui l t pati ents it m a y be impossible
to
vi suali ze
C7
in the l a teral vie w . It is imp o rta nt tha t the hard
palate
should be
lordos i s
horizontal
or kyphosis)
(fo r
assess m e n t
and tha t the two halves
of
of
the
m a ndibula should be e x actly ove rlaid, showing tha t
( Figure
there is neither side -be nding nor rot a tion
3 .23 ) .
Fine m a n et al.
of only
( 1 963 )
show ed that
10 degrees in incli na tion
of
a
d i fference
the
head
is
su fficien t to c h ange lordotic to linear posture, and
vice versa.
T h e o b l iqu e view serves m a i nly to show
the
intervertebral fora min a , wh i ch in the ce rvical s p i ne
a re not visualize d at al l in the side vie w a nd
Copyrighted Material
poorly
60
Manipulative Therapy in Rehabilitation of the Locomotor System
Figure 3.23 La t e ra ] X-ray o f t h e e e l'viea l
p l a n e of t h e fora m e n
magnum. t h e a t l a s a n d the a x i s
i n d ica ted : t h e c l i v u s a n d t h e pos t e ri o r
e d g e o f t h e v e r t e b r a l c a n a l a r e a ls o
shown
s p i n e with t h e
i n the A P view. I t should be t a ken with the p a t i e n t
s i t ti ng o n a c h a ir t u r n e d a t 45 degrees to the casse tte ;
the p a t i e n t u s u a l l y sits with h i s back to i t , b u t l i ke
G u t m a n n I p r e fer t h e p a t i e n t to face the cassette
a n d t o h o l d the h e a d in retrofle x i o n , because if t h e
patie n t faces t h e cassette i t i s t h e fo r a m e n n e a r e r t o
i t t h a t is visualize d , a n d na rrowing o f t h e fora men
is o fte n v i s i b l e o n l y i n re t ro fl e x i o n ( Figure 3 .24) .
O b l i que views a re p a r t i c u l a r l y i m po r t a n t i n
cervical radic u l a r synd romes a n d i n cases of the
v e rtebra l artery syndrome. because of the close
re l a t i o n s h i p betwee n the i n terve rtebra l fo rame n , the
n e rve roots and the verte b r a l artery.
F u n ct i o n a l a n atomy of t h e cervi ca l spi n e
The cervical s p i n e h a s two very disti n ct sect ions: the
cra n i ocervica l j u nction between the occi p u t and C2.
and the section from C2 to C7. Most of the move ­
m e n t s i t pe rforms start a t t h e cra niocervica l j unction,
and the mov e m e n ts of the head a n d neck a re u s u a l ly
i n i tiated by eye moveme n ts . I therefo re b e g i n w i t h
a s h o r t a na t o m i c a l descri ption i n w h i c h t h e t w o pa rts
a re t re a te d separa t e l y , w h i le t h e fu nction of t h e
ce rvical s p i ne is dea l t w i t h a s a w h o l e .
F u n ct i o n a l a n ato m y
C2-C7
As in o t h e r pa rts o f the spi n a l co l u m n , the cl egree
o f move m e m t i n the cervic a l s p i n e is d e t e r m i n e d
m a i n l y by t h e th ick ness o f the i n terverte b r a l d isc;
t h i s is usua l l y greatest in the segme n ts C4/5 a n d
C5/6 , w h e re mobi l i t y i s a lso greatest. T h e c h a r­
acteristic fe a t u r e o f t h e ce rv ica l verte b r a l bodies is
a latera l ridge the u n ci fo r m process . Its sign i ficance
fo r cervica l fu nctio n is t h a t the s h a pe of the vertebral
body l i mits l a te r a l fl e x i o n while encouraging a n t e ­
a nd la tera l fl e x i o n .
T h e a po ph y se a l j o i n ts a re al most p a ra l l e l o n
b o t h sid es and a re t i lted f r o m v e n t rocra n ia l to
Copyrighted Material
,
Fun Cliona/ aJ1a lOmy and radiography of
Ihe sp inal co/u /1 / 11
ol
a d u l t s , a r e l e s s m a r k e d i n h i g h e r a g e g ro u ps . I t i s
i m p orta n t to r e a l i ze t h a t t h e y a r e p h y s i o l o g i c a l i f
th e y a re p roportion a te . a n d t h a t t h e sh i ft i s grea test
a t t b e C2/3 s e g m e n t ( s e e F i g u re 3 . 30)
It m u s t be a l so b o r n e in m i n d t h a t d u ri n g a n te ­
fl e x i o n t b e ce r v i c a l v e r t e b ra l ca n a l l e n g t h e n s c o n s i d ­
er a b l y . shorte n i n g d u r i ng retrofl e x i o n . T h i s p rod uces
a s i g n i fi ca n t m o v e m e n t of t h e m e n i nges w i t h t h e i r
root s l e e v e s , a n d a l s o o f t h e s p i n a l cord , wh i c h c a n
be s e e n i n p n e u m o m y e lographs to g e t l o n g e r a n d
t h i n n e r i n a n t e fl e x i o n a n d s h o r t e r a n d t h ic k e r i n
re t r o fl e x i o n .
A n o t h e r h i g h l y s i g n i fi c a n t fe a t ure i s the cou rse o f
t h e v e r te b r a l a rtery, w h i c h e n te rs t h e b o n y c a n a l
a t t h e tra n sv e rsoco s t a l fora m e n of
C6
a nd r u n s
u pw a rd s , cro s s i n g t h e i n te rv e r t e b ral c a n a l s i n c l ose
c o n t a c t w i t h the a r t i c u l a r p rocesses a l m o s t at ri g h t
a n g l e s to t h e cou rse o f t h e n e r v e r o o t s . T h e r e fo re ,
a s the i n te rv e r t e b r a l fo ra m e n ( c a n a l ) n a rrows i n
retrofl e x i o n , t h i s m a y a ffec t the n e rv e r o o t a n d t h e
ve rte bra l a r tery.
F u n cti o n a l a n atomy of the cra n i ocervica l
j u n ction
S t u d y o f t h i s m o s t i m porta n t j u n c t i o n i s co n ce r n e d
w i t h t h e m o b i l ity o f e ac h o f i ts j o i n ts a nd t h e b o n y
s t r u c t u res a n d l i g a m e n t s t h a t l i m i t i t . T h e r e a re n o
i n te rv e r t e b r a l d i scs.
T h e upper a rt i c u l ar fa cets o f t h e a t l a s are o v a l
wi t h t h e l o n g a x i s r u n n i n g o b l i q u e l y , c o n v e rg i n g
p o s t e r i o r l y a n d m e d i a l l y l i k e a sect i o n o f t h e s u rface
Figure 3.24 O b l i q u e v i e w
of
of a sphere w i t h t h e c e n tre loc a t e d above
lhe cerv i c a l s p i n e i n
both
a r t ic u l a r s u rfaces . The m a i n m o b i l i ty i n t h e a t l a n to ­
ret ro A e x i o n s h ow i ng a n a r ro w e d i n t e rv e r t e b r a l fo r a m e n
occi p i t a l
of C213 on t h e r i g h t
j o i n ts
d e g re e s ( Fi g u r e
i s a n t e - a n d r e t r o fl e x i o n , a b o u t 15
3.25).
There is poste r i o r gli d i n g o f
t h e occ i p i t a l c o n d y l e s d u r i n g a n te fl e x i o n a n d a n te r i o r
d o rsoca u d a l . Th i s t i l t v a r i e s co n s i d e r a b l y ( a b o u t 4 5
gl id i ng d u r i n g retro fle x i o n . S l i g h t rota t i o n i s poss i b le .
d egrees ) . b e i n g g r e a t e s t a t C2/3 a s a r u l e . A t t h i s
w h ich J i r o u t ( 1 98 1 a ) h a s s h o w n to be a v e r y l i m ited
l e v e l t h e j o i n ts a re freq u e n t l y n o t p a ra l l e l b u t a s i f
l a t e ra l fl e x i o n , rota t i o n b e i n g c o u p l e d w i t h s i d e ­
o n t h e s u rface o f a cy l i n d e r w i t h i ts c e n tre b e h i n d
be n d i n g to t h e o p p o s i t e s i d e .
the s p i n a l c o l u m n ; i t i s t h e refore n o t p a t h o l o gical i f
t h e a r t i c u l a t i o n C213 i s n o t we l l v i s u a l i zed i n t h e s i d e
v i ew ( u n l i ke t h e o t h e r cerv i c a l a po p h y se a l j o i n ts) .
The s h a p e o f t h e cerv ica l a p o p h y s e a l j o i n ts is best
s u i t e d t o a n te - and re t r o fl e x i o n . O n l a t e r a l flex i o n
t h e t i l t o f t h e j o i n ts produces rota t i o n t o t h e s i d e o f
in c l i n a ti o n a n d d u r i n g h e a d ro t a t i o n i n c l i n a ti o n
The
a t l a n toax i a l
j oi n ts
com p r i s e
the
a t l anto­
o d o n to i d a s w e ll a s the j o i n ts b e t w e e n t h e m as s a e
l a t e r a l e s a n d t h e a x i s , a n d th e i r m a i n f u n c t i o n i s a x i a l
r o ta t i o n . T h e j o i n t fa cets r u n a n te roposte r i o r l y a n d
a re concave on t h e m a ss a l a tera l i s of t h e a t l a s a n d
convex o n t h e a x i s . I n a d d i t i o n , t h e re i s t h e a t l a n t o -
re s u l ts fo r t h e s a m e reaso n .
D u ri ng a n te fl e x i o n t h e re is freq u e n t l y a s l i g h t s h i ft
of t h e c ra n i a l v e r t e b r a , a n d i n r e t r o fl exi o n a sl i g h t
b a c k w a rd s h i ft w h ich is a lso i n a c c o r d a n c e w i th t h e
t i l t o f t h e a r t i cu l a r face t s . Accord i n g to Pe n n i ng
( 1 968)
cra n i a l
t h i s fo rward a n d b a c k w a r d move m e n t of t h e
vertebra
i s l i k e a rota t i o n
of the upper
vertebra i n t h e s a g i t t a l p l a n e r o u n d a n a x i s s i t u a ted
at the d o rs a l part of the l ow e r verte b r a l bod y . It
s h o u l d be po i n te d o u t t h a t t h e se s h i ft i n g m o v e ­
Figure 3.25 A n t e - and retrofle x i o n bet w e e n occi p u t a n d
m e n t s . w h i c h a re t h e r u l e i n c h i l d r e n a n d yo u n g
atlas
Copyrighted Material
62
Manip uialive Therapy in
RchabililaliOI1 of the
Locomotor
o d o n t o id j o i n t between t h e a n terior a rc h of t h e a tl.a s
a n d t h e odon toid process a n t e r i o r l y . w h i l e t h e
p o s t e r i o r s u rface of t h e od o n t oi d p rocess is l i n e d by
c a r ti l a g e and in c o n t a c t w i t h t h e t r a n sv e r s e l i g a m e n t .
T he p ossi b l e movements a re a n te- and retro­
flexion and r ot a t i o n . D u r i n g a n te - and r e t r o fl e x ion
t h e a n terior arch of t h e a t l a s g l i d e s u p a n d down o n
t h e odon toid a n d i f t h e t r a n s v e rs e l i ga m e n t i s fi r m
t h e space between t h e s e t w o structures d o e s n o t
w i d e n . The range o f m ovm e n t h ere is a g a i n a bo u t
1 5 degrees.
The m ost i m p o rta n t m o v e m e n t , h o w e v e r , i s
r o t a t i o n , i n w h i c h a l l j o i n ts t a ke p a r t ; w h i l e t h e re i s
rota tion rou n d t h e o d o n t o i d , the m assa l a t e r a l i s of
t h e a t l a s g l i d es on t h e axis p os te ri o r l y o n the side
of rota t i on a n d a n t e ri o r l y o n t h e o pp o s i t e s i d e .
Rotation i s l i m i te d b y th e j o i n t c a p s u l e a n d the
p o w e r f u l alar l iga m e n ts w hi c h are a t tached t o t h e
m a rgins o f t h e forame n m a gn u m a n d t o t h e atlas.
R o t a t i on a m o u nts o n ave rage to 2 5 d e g rees to e a c h
side, the m a x i m u m b e i n g 40 d e g r e es ( F i g u re s 3.26
and 3 .27) . D v o r a k ( 1 988) h a s sh o w n b y a xi a l
c o m p u t e d tomo gr a p h y that the ra nge o f mo v e m e n t
between a t l a s a n d a x i s m a y b e e v e n gre a t e r : h e
fo u n d ave rages o f 4 1 . 5 d e g r e e s t o t h e r i g h t and
44 d e g r e es to t h e l e ft w i t h a m ax i m u m o f 50 d e g re e s
( ' ) to o n e s i d e , a nd i n a d d i t i o n a n a v e r a g e of 4 . 5
d e g r e e s be t w e e n o c c i pu t a nd a t l a s to t h e r i g h t , a n d
4 . 1 d e g r e e s to t h e l e ft . H ug u e n in a n d H o p f ( 1 993 )
u s i n g m a g n e t i c reson a n ce, on t h e o t h e r h a n d , fo u n d
t h a t t h e ra nge o f motion c o r r e s p o n d s m u c h m o r e to
o u r e a r l i e r fi n d i n g s .
K i n e s i o l o g y of t h e cerv i c a l spi n e as a
whole
Rota tion
D u ri n g ro t a t i o n , m ov e m e n t sta rts b e tw e e n the a tlas
a n d the axis a n d t a k es p l ace m a i n l y t h e re until the
range of motion is e x h a u s te d , i . e . to about 25 d e g rees
to e ac h side, o n a ve r a ge . U p to t h i s p o i n t the re i s
pure a x i a l rotat ion i n t h e hor i zon t a l p l a n e . From this
p o i n t o n w a rd s rotation t a kes place fro m C3 to C7
in s u cc e s s i o n j f there i s fl e x i o n a t t h e c e r v i c o t h o r a c i c
j u n ct i o n , a n d as fa r as T3 if t h e cervicothoracic
j u n c t i o n i s s t r a i g h t e n e d up. Th ere i s sti I I s o m e a d d i ­
t i o n a l pa s s i v e r o t a tion be t w e e n t he o c c i p u t a n d t h e
at l a s . T h e m o m e n t rotation t a k e s p lace i n t h e c e rv i c a l
s p i n e b e low t h e a x i s ; s i d e - b e n d i n g a u t om a t i c a l l y
occurs a t t h e s a m e t i m e , u n less d e l i be r a t e l y a v o i d e d .
Side-bending
System
u p p e r cervica l a rea (Figu re 3 .28). T h i s shows t h a t
l a t e r a l fl e x i o n sta rts w i t h rota t i o n of t h e a x i s i n t h e
d i re c t i o n o f s i d e - b e n d i n g a n d a t t h e s a m e t i me t h e re
is sy n k i n e s i s o f t h e a t las, s h i ft i n g re lative to the
o cc i p i t a l c o n d y l es and to t h e a x i s , i n the d i rection o f
s id e - b e n d i n g .
O n l a t e r a l flexion of t h e w h o l e of t h e c e rv i ca l s p i n e
we see s i d e - b en d i n g a n d r o t a t i o n i n t h e d i r e c t i o n o f
l a te r a l flex i o n , b e i n g g r e a t e s t a t t h e a x i s . As J i rout
( 1 968) h a s s h ow n , t h i s rota t i o n usua l l y e nd s i n t h e
l ow e r c e r v ica l s p i n e d u r i n g s i d e - b e n d i n g to the r i g h t .
b u t d u r i n g l a te ra l !kx ion to t h e l e ft ca n be fo l lowed
d o w n i n t o t h e u pper t h o r ac i c re g i o n . (This he
e x p l a i ns as t h e result of s t ro nger p u l l o f the m u s c l e s
o f the shou l d e r g i rd l e a t t a c h e d t o t h e s p i n ou s
processes on t h e r i g h t s i d e . ) T h i s co m b i n a ti o n o f
s i d e - be n d i n g a n d rotati on is, o f cours e . i n ac c o rd a n c e
wi t h the t i l t o f t h e c e r v i c a l a po p h y s e a l j oi n ts b u t n o t
a d i rect c o n s e q u e n c e o f the t i l t , as i s u s u a l l y t h o u g h t ,
as t h e movem e n t sta rts a t t h e c r a n i o c e r v i ca l j u nction
a n d rot a t ion o f t h e a x is c o m e s fi rs t , fol lowed by
r o t a tio n of t h e l o w e r c e r v i c a l v e rte b r a e in success ion .
A s i s s h ow n i n d e ta i l l a te r , i f ro t a t io n o f t h e a x i s
does not t a k e p l a c e , t h e re i s n o ro t a t i o n o f t h e rest
o f t h e c e r v i c a l s p i ne . J i rollt ( 1 97 1 ) h a s d e p i c t e d t h e
force c a u s i n g rot a ti o n d u r i n g s i d e - b e n d i n g (Figure
3 .29) . I t c a n eas i ly be seen t h a t s o m e a n te fl e x i o n
m i g h t t a k e p l a ce w i th r o t a t i o n d u r i n g s i d e - be n d i n g ,
and these s y n k i n es e s in the sagi t t a l p l a n e h a v e , i n
fa c t , been co n fi r m e d b y J i ro u t ; t h e y const i t u t e j o i n t
p l a y i n t h e c e rv i c a l s p i n e ( see F i g u re 3 . 4 6 ) . H o w e v e r ,
the exact m e c h a n i s m t h a t fo rces t h e a x i s to rotate ,
t h e moment t h a t l a t e r a l fl e x i o n s t a rts ( w h i c h c a n
e a s i l y b e p a l pa te d ) , re m a i n s u n k now n .
A n te flexion a n d retro flexion
A n te fl e x i o n can be carried out i n d i ffe re n t ways: w e
can e i t h e r draw the c h i n i n , or l e t t h e h e a d d ro p
fo r w a r d , o r b r i n g t h e c h i n to t h e chest. which is a
c o m b i n a t i o n of t h e fi rst two m ov e m e n t s . In
r e t rofl e x i on t h ere a re no s u c h d i ffere nces. T h e two
m e c h a n i s m s o f a n t e fl e x i o n a re s o m e w h a t ;r. com­
pe t i t i o n : u n l ess there i s h y p e r m o b i l i t y , if w e d r a w
t h e ch i n i n w e c a n not d ro p t h e h e ad fa r f o rw a r d a n d
if we d r o p i t fo rw a rd , we c a n not d raw t h e ch i n i n .
Th e e xp l a n a t i o n l i e s i n t h e m e c h a n i s m o f a t l as ti l t ,
w h ich must b e u n d e rs tood i n order to assess c e r v i c a l
a n te- and retro fl e x i o n .
T h e fo l l ow i n g c h a n g e s c a n b e o bs e rved i n X - r a y
s t u d i e s i n t h e s a g i t t a l p l a n e ( s e e F i g u r e s 3 . 30 a n d
3.3 1 ).
1.
S i d e - b e n d i n g can be studied o n l y by X-ray, a n d
t h e re fore i s d e a l t w i t h u n d e r X-ray m o b i l i t y s t u d ies.
Like rota t i o n , i t b e g i n s a t the cra n i ocervical j u n c t i o n .
T h i s c a n b e s t be s t u d i e d d uring p a ssiv e s i d e - t i l t i n g
m o v e m e n t l o ca l i zi n g l a t e ra l fl e x i o n m a i n l y i n t h e
Wi t h t h e p a t i e n t i n t h e e r e c t p o si t i o n t h e p l a n e s
of t h e fora m e n m a g n u m and the a x i s r u n a l m o s t
p a r a l l e l . t h e atlas b e i ng t i l t e d b a c k w a rd s a t a n
a v e r a g e a ngle of about 6 degrees.
2 . W h e n t h e p a t i e n t draws i n t h e c h i n , a n t e fl exi on
b e t w e e n occi p u t a n d atlas i n c rease s o n l y s l i g h t l y :
Copyrighted Material
FI /llction al ana lOmy and
b
f
Figure 3.26 A n te ropos t e ri o r X · rays of an i s o l a t e d a x i s :
t h e p i c t ure s a re use fu l f or grad i ng rota t i o n
mdiogmphy of the
spinal column
63
c
h
9
(a)
i n n e u t r a l pos i t i o n a nd ( b-h ) in ro t a t i o n from 5 to 40 d e g r e e s :
Figure 3.27 R o t a t i o n o f the a x i s i n
rela t ion t o t h e a t l a s ( h e a d ) : t h e h e a d i s
fi x e d i n n e u t r a l pos i t i o n , th e b o d y i n
m a x i m u m rota tion ( h e re a t 4 0 degrees
axis r o t a t i o n : cf. Figure 3 . 26 (h))
t h e m a i n m o v e m e n t i s a n t e fle x i o n b e t we e n a t las
and a x i s , t h e fo r m e r b e i n g now t i l t e d fo r w a rd
w h i l e t h e rest of t h e c e r v i c a l s p i n e re m a i n s a l m o s t
s t ra i g h t .
3 . In m a x i m u m a n le ll e x i o n t h e c e r v ic a l s p i n e i s
a l m o s t h o r i zo n t a l : t h e re i s p ro p o r t i o n a te v e n t r a l
s h ift of the ce rvical v e r t e b r a e u p t o C2/3; there is
m a x i m u m a n tefle x i o n between Cl/2 b u t , c o n t r a ry
to pos i t i o n s ( I ) a n d (2) ,
a n t e fl e x i o n
of t h e o cc i p u t
a g a i n s t t h e a t l a s h a s now d isappe a r e d , i . e . t h e re
is
r e t ro fle x i o n
of the h e a d a g a i n s t t h e a t l a s o r
for w a rd t i l t o f t h e a t l a s . Conseq u e n tl y , the a n gl e
Copyrighted Material
64
i'vl a l f ip u lati ve Th erapy
il7
Rehab ilitOlion of the Locomotor
S )'stem
Figure 3.28 A n te r o p o s t e r i o r X - r a y of t h e c e r v i c a l spine
of a h e a l t h y s u bj e c t . i n n e u t r a l posi t ion . d u r i n g a c t i ve
l a t e r a l fl e x i o n . and p a s s i v e l a t e r a l Ikx i o n l i m i t e d to the
upper c e r v ica l re g i o n . ( a ) In n e u t ra l pos i t i o n the a t l a s is
t o the r igh t i n r e la t i o n to the co n d y l e s. a n d t h e p l a n e of
the c o n d y l e s a n d the axis c o n v e rge o n t h e righ t . t h e a x is
be i n g ro t a te d a b o u t 5 d e grees to t h e l e f t . (b) At a c t i v e
l a t e ra l fl e x i o n t o t h e l e ft t h e a t l a s i s s t i l l t o t h e r i g h t o f
t h e c o n d y l e s a n d the p l a n e o f t h e cond y l e s a n d t h e a x i s
con verge a l i t t l e t o t h e r i g h t . t h e a x i s n o w b e i n g ro t a te d
about l O degr e e s to t h e l eft . (c) Passive l a t e ra l fl e x ion o f
t h e upper c e r v i c a l s p i n e t o t h e l e f t : t h e a t l a s i s n o w
c l e a r l y t o t h e le ft o f t h e c o n d y l e s il n d the p l a n e o f t h e
co n d y l es i s para l l e l t o t h e a x i s w h i c h is ro t a t e d a b o u t
1 0 d e g rees
Copyrighted Material
Fl Il1clional anatom v and
radiogmphy of the spinal cO/limn
fo r a m c n m a g n u ln Th e c o n d y l e s
u( u l a te
65
the
l a te r a l m a s s o f t h e a t l a s , t h e a t l a n lo occ i p i l a l j o i n t s
b e i n g v i s i b l e o n b o t h s i d e s , t h e i r p l a n e s m e e t i ng a t
an
o f Cl b o u t
co n d v l e s we
1 25 -110
on
degrees . B e n e a t h the
bot h sides
t h e ocl o n to i d
process t h e l a te r a l m a s s e s o f t h e a t l a s , w h i c h a rc
w e d ge s h a p e d , t a pe r i n g t o w a rd s t h e m e d i a l b o rd e r .
Cl ose
t h e h o rd e r we o ft e n
translucency
be t a l.. e ll for o s te o l y s i s . L a t e ra l l y
which should
t h e re a re t h e t r a n s v e rse proces s e s . F r o m o n e t r a n s ­
v e rse p rocess t o t h e o t h e r , o n e c a n fo l l o w t h e c o u rse
of t h e poste r i o r a re h w h i c h i s l i ke
a t its c e n t re .
spindle, broader
l a t e r a : l r i a n g l t: s o f t h e m d s s a e
l a t e r a l e s p roj ect b elow t h e s h a d o w of the p o s te r i o r
arch.
Someti mes
the
cros s i n g t h e t i p
a n te r i o r a rc h
can
he
see n
t h e o d o n to i d .
B e low t h e m a s s a e l a t e r a l e s o f t h e a t l a s w e s e e t h e
Figure 3.29 M e c h a n ism or l a t e ra l rl e x i o n o f the cerv i c 8 1
s p i n e ll Ccord i n g
J i r o u t ( I (7 1 ) . D u r i n g s i d e - b e n d i n g the
h e a d tO ta tes
a sag"
a xi s ( x ') s i l uated
a n t e r i o r c r a n i a l fos s a . The diagram s h o w s h o w the base
of the s k u l l . w i t h t h e c o n d y l e s , s h i ft s in the o p p o s i t e
d i re c ' l o TI o f l a r c r 2 1 fl e x i o n " c a i n s t t h e 2 t l a 5 . a n d h o w t h e
axis w i t h t h e
ce rv i c a l v e r t e b r D e
b r o u g h l mto
rO l a t i o n a n d t h e ,pi n o Ll s process o f the a x i s i s l i l t e d
for w a rd by c r a n i a l p u l l
b e t w e e n t h " c l i v u c; a n d t h e o d o n t o i d ,
l.G.
th"
m e a s u re o f k y p h o s i s b e t w e e n t h e h e a d a n d t h e
odon toid.
re m a i n s [ h (� s a m (' 8 S w i t h t h e h e a d
erect , a n d
g re a t e s t w h e n t h e c h i n is J w w n i n .
rhe re is s o m e degree of fo rward s h i fr o f t h e
b a s i o n agai n s t t h e t i p o f t h e od o n t o i d .
4.
r e t ro f\: x i o n w i t ' l
nEI ,( l m u m
(not
t h e occi r u t
proportionate
v\'1 l e bra('
p a t i e n t s i t t i n g . l il e re i "
r o fl e x n J f1 o f t h e
against
a ga i n s t I he a x i s
the a t l a s l ) ; we s e e a
b a c k w a r d s s h i ft
o f the hll s i o n
of t h e c e r v i c a l
the
I
of the
a t l a n toa x i a l j o i n ts a n d t h e j o i n t face t s
M e d i fi l
of
the axis.
t h e se fa c e t s e n d i n a n o t c h borde r i n g t h e
o d o n tuid
p rocess
s i t u a te d
b e t w c e ll
the
l a te r a l
m a s s e s o f t h e a t l a s a n d we l l b e l o w t h e b o r d e r o f t h e
fo r a m e n m a g n u m . C l o s e b e n e a t h t h e l a t e r a l t i p o f
the
we
joint
t h e fo ra m e n costl! t ra ns-
fo r a m e n
llxis. Medial to
see
t h e p e d i c l e s . w h i l e b e t w e e n t h e p e d i c l c s we s e e t h e
v e rs a n u m o f
a r ch of t h e a x i s w i t h t h e s p i n o lI s p rocess i n m i d - l i n e .
to
the
H t h ere I S m a r k e d l o rd O S I S i t i s
t r a n s l uccncy o f t he s p i m l l c a n al at t ll .! t l e ve l .
B e l ow C2 t h e ce rvical v e r te b r a e a re c h a ra c t e rized
by the u n c i fo r m p roces<; o n b o t h <; i d e s ; t h e i n t e r­
v e r t e b r a l d isc
t h e r e fore m u ch h ig h e r m e d i a l l y
t h a n l a t e ra l l y . T h e n a r r o w s h a d o w o f t h e p e d i c l e s
l i es b e t we e n t h e u n c i form process, a n d t h e s p i n o u s
processes a re
m i d - l i n c . Lateral
t h e u n c i fo r m
p roC,ISS t h e i n te rv e rt e b r a l fo r a m e n C;1Il be
The
l a te r a l c o n t o u r i s for m e d b y t h e t r a n sve rsocos t a l
process, a n d s o m e t i m e s t h e i n t e r v e r t e b ra l j o i n t c a n
be see n .
odon to i d .
5 . I n r e t ro fl e x i o n w h i l e l y i n g o n t h e s i d e t h e re i s
n o w m a x i m u m re t ro fl t: x i o n of the occi p u t il ga i n s i'
atlas
atlas
much
re t r o fle x i o n o f
a g a Jl1 s t t h e Cl x i s . T h e re is no s h i ft of t h e b a s i o n
b a c k w a r d s ( t h e s u bj e c t m u s t n o t fo rce h i s h e a d
(sec Figure 3 . .\ 1 ) .
Side vie w (Figure 3. 34)
In the; s i d e v i e w a n u n d l s t o r t e d
re of
base
o f t h e � k u l l w i t h I ls r e l a t l O n � h i p to t h e u p p e r c e r vi c a l
spi n e i s o b ta i n e d . I n p a r t i c u l a r , t h e c l i v u s c a n b e
fo l l o w e d d o w n
where
for m s t h e: a n te r i or m a rg i n
o f t h e fora m e n m a gn u rn ( b a s i o n ) w h i c h is u s u a l l y
Th e m e c h a n i s m u n d e r l y i n g t h e s e p h e n o m e n a , i n
p a r t i c u l a r m o ve m e n t o f the a t l a s , i s i l l u s t r a t e d i n
F i p ll f C 3 . 3 1
which
h mv
atlas
t i l te d
s i t u a te d s t r a i g h t a b o v e
ti p of the
odontoid
for a m e n m a g n u m ( o p i'il i o n ) i s so m e t i m e s c i c: a r l y
forwmd d u r i n g a n te fl e x i o n a n d b;l c k w a r d s d u ri n g
seen
retroflex i o n , w i t h t h e s u bj e c t s e a t e d , by t h e w e i g h t
t h e base
the sq
of
occl p i l a l i s i s fo l lo w e d d o w n t o
t h e s k u l l . I f n o t , t h e p o s t e r i o r m a rg i n of
t h e c � r v i ca l s p i n (l l c a n a l i s fo l lo w e d a n d w h e r e i ts
of the occ i p i ta l c o n d y l e s
p r o l o n ga t i o n m e e t s t h e
o f t h e s k u U t h e pOS i t i o n
o f t h e o p i s t i o n i s u e t e rm lllcd ( s e e Fig u r e
X-ray a n atomy of the cervical spi n e
AP
the
process. T h e p os i t i o n o f t h e poste r i o r m a r g i n o f t h e
3.23).
T h e m a s t o i d p r o c e s s freq u e n t l y o v e rs h a d o w s p a r t
o f t h e m a ss a l a te r a l i s o f t h e a t l a s
vie w (Fig ures 3.32 and 3. 33)
a t l a ll t o occi p i t a l j o i n t i ,
I n t h e AP v i e w we s e e t h e a r c h to r m e d by b o t h
in the SIde view;
occi p i t a l c o n d y l e s a n d t b e a n te r i o r m a r g i n o f t h e
seen v e r y w e l l (Figure
Copyrighted Material
111
t h e r e fo r e t h e
a l wHYs w e l l v i s lI ;i l i z e d
some c a s e s , h o w e v e r , i t c a n be
3.35).
116
Manipulalive Therapy
in
Rehabilillllion of the LOCOmOI()r
System
Figure 3.30 Mobil i ty of the c e r v i c a l s p i n e d u ri n g a n t e - a n d r e t ro fl e x i o n . ( a ) N e u t r a l pos i t i o n w i t h the p a t i e n t e re c t : the
atlas is i n r e t r o fle x i o n with r e l a tion t o t h e axis a n d t h e h e a d in a n t e fl e x i o n in r e l a t i o n to t h e a t l a s . (b) With the c h i n
d r a w n i n , a n t e fl e x i o n o f t h e occi p u t with relation t o t h e a t l a s i n cr e a s e s o n l y v e r y l i t t l e , w h e r e a s t h e re i s n o w m a r k e d
a n t e fl e x i o n o f t h e a t l a s i n r e l a t i o n t o t h e a x i s . ( e ) A n teflex i o n : w h i l e a n t dl e x i o n o f t h e a t las i s n o w a t m a x i m u m
( a n te ri o r t i l t of t h e a t l a s ) t h e h e a d h a s m o v e d i n t o re t ro fl e x i o n s o t h a t t h e pl a n e o f t h e fora m e n m agn u m a n d of t h e
a t l a s n o w l i e a l m o s t p a ra l le l . (d) R e t r o fl e x i o n s i tting : t h e r e is b o t h r e t r o fl e x i o n of t h e h e a d a g a i n s t the a t l a s a n d o f t h e
a t l a s aga i n s t the axis, t h e fo rm e r b e i n g l e s s o w i n g t o t h e t i l t i n g o f t h e a t l a s : a s i n a n t e fl e x i o n , t h e plane o f the fo r a m e n
m a g n u m l i es p a r a l l e l t o t h e p l a n e o f the a t l a s . ( e ) R e t r o fl e x i o n w i t h t h e p a t i e n t o n h e r s i d e : as t h e w e i g h t o f t h e h e a d
n o l o nger plays a p a r t , t h ere i s n o back w a r d t i l t o f t h e a t la s a n d t h e re i s m a x i m u m retrofle x i o n o f the h e a d a ga i n s t t h e
a t l as a n d fa r l e s s r e t r o fl e x i o n o f t h e a t l a s a g a i n s t t h e a x is . N o t e a l so t h e s h i ft o f t h e b a s i o n fo rward d u ring h e a d
a n t e fl e x i o n a n d b a c k w a r d s d u r i n g re t ro fl e x i o n ( s i tt i n g )
Copyrighted Material
Funclional
Figure 3.30
of Ih e spinal CDllimn
67
(con t i n u e d )
Figure 3.31 T h e m e c h a n i s m o f a t l a s t i l t
T o d e t e rm i n e the p l ane of t h e fo r a m e n m a g n u m
l i n e i s d rawn from the b a s i o n t o t he posterior
m a r g i n of t h e fora m e n magn u m . The p l a n c of t he
a tl a s corresponds to a l i n e co n n e c t i n g the ce n t re o f
the an terior a n d the posterior a rches: the p l a n e of
the axis corresponds to a l i n e from t h e lowest poi n t
o f t h e transve rsocos t a l p rocess t o t h e lower margin
o f the arch o f t h e axis. This a l lows rel a t i v e a n te - o r
retrofl exion t o be assessed (see Figure 3 .23 ) .
The sha dow o f the o d o n to i d process i s j ust b e h i n d
t h e a n t e r i o r a rch o f l h e a t l as, the t i p o f the odontoid
a
analOmy lint! radiography
being usually about the s a m e level as the upper
m a rg i n of t h e a n t e rior a rch . I t s h o u l d n o t be m u c h
a bove t h e pala to-occi pital line; t h i s i s t h e c a s e i n
basi l a r i m p ressio n .
U n l i k e t h e res t o f t h e s p i n a l col u m n , t h e tra ns­
ve rsocostal p rocesses w i t h the pedicles project on to
the vert e b r a l bod ies i n the si de view. Th e u p p e r
m a rg i n of t h e t r a n sversocost a l process is e v e n slightly
a bove t h e upper m a rgi n of t he verte b r a l bod ies,
somew h a t bl urri n g t h e l ow e r contour of t h e i n ter­
ve rtebra l d iscs.
The s hadows o f t h e articu l a r p rocesses and the
tra n s l ucency of t h e j o i n ts p rojecting into t h e spi n a l
ca n a l ca n b e s e e n be h i n d t h e v ertebra l bodies. I f t h e
s i d e v i e w has b e e n t a k e n correctly, o n l y o n e l i ne can
be see n , showing t h a t the j o i nts a re p a ra l l e l . The
posterior m a rg i n o f the spin a l ca n a l is i n d icated b y
a s h adow a t the b a s e of the s p i n o u s processes w h e re
t h e l a m i n a e m e e t . The shadow is u s u a l ly also clearly
v is i b l e a t t h e l e v e l o f the atlas; i ts absence i s a clear
sign of spina b i fi d a , a fre q u e n t a n o m a ly o f t he a t l as
a rc h .
X-ray eva l u at i o n o f fu n ct i o n
The most c h a racteristic d isturbance of s t a t ics i n the
cervica l reg i o n i s the fo rward drawn position (Figure
3 . 3 6 ) . Th is is so because even when sta tics a re n o r m a l
the centre o f gra v i ty of the head is slightly i n fron t o f
its s u pport a nd the refore there i s a lways some m us­
c u l a r activ i ty in the neck m u sc u l a t u re in the e rect
Copyrighted Material
68
Manipulative Therapy in Rehab ilita tion
of th e
Locomotor System
7
3
1/. --_.:;:
6 -----"=-...:'
7
-L-----,.
_
_
_
Figure 3.32 S k e l e t o n of the ce rvical s p i ne ( v e n t r a l aspect) compared w i t h t h e a n t e ro p os t e r i o r X - ra y . I . A n t e r i o r e d g e
t h e fo ra m e n m a g n u m : 2 , l ow e r edge o f t h e a n t erior a r c h o f the atlas: 3 . fo ramen cos l o t ra n s v e rs a r i u m o f t h e a x i s :
4 . fo ra m e n i n te rv e r t e b r a l e : 5 . c o u rse o f t h e v e r te b r a l a r t e r y ; 6 . u nc i fo r m process: 7 . ped i c le
of
Figure 3.33 S k e l e to n of t he c e rv i c a l s p i n e ( d o r s a l a s p e c t ) c o m pa re d w i t h the a n t e ro p os t e r i o r X - r a y . I . Fo r a m e n
2 . l o w e r e d g e o f t h e poste r i o r a rc h o f t h e a t la s : 3 . r n a s s a l a t e r a l i s o f t h e a t b s w i t h
4 . t h e l a te r a l t ri a n g l e : 5 . j o i n t s p a c e : 6 . s p i n o u s p r o c e ss
cos t o t r a n s v e r s a r i u m o f t h e a x i s ;
Copyrighted Material
Flln Cliot/ n l analOIllY and
radiography of rh e
spinal column
1
6
Figure 3.34 S k e l e t o n o r t h e c e rv i c a l s p i n e ( l a t e r a l a s p e c t ) c o m p a red w i t h the l a tera l X - ra y . 1 . Transve rse process:
2 , w i d t h or t h e s p i n a l c a n a l : 3 , j o i n t space: 4. lower a r t i c u l a r p roce s s : 5 , ro ra m e n i n t e r v e r t e b r a l e : 6 . u p p e r a r t i c u l a l­
process
Figure 3.35 A t l a n to-occi p i t a l j o i n t . l a t e r a l view
Copyrighted Material
69
70
Manip l l iative Therapy in Rehabiliwlion of the Locomotor Sys/al1
Figure 3.36 Fo rwa r d - d r a w n posi t i o n of the head : t h e
e x t e rn a l a u d i t ory c a n a l a n d t h e o d o n toid p rocess l i e fa r
a n t e r i or to t h e u p p e r a n d a n t e r i o r e d ge of C2: t h e
c r a n iocerv i c a l j u n c t i o n i s i n a pos i t i o n o f c o m p e n s a t o r y
h y p e r l o rdosis
Figure 3.37
view of the c e r v i c a l s p i n e w i t h t h e
e re c t : t h e e x t e rn a l a u d i t o ry c a n a l ( ce n t re
of g r a v i t y of t h e h e a d ) a n d t h e o cl o n t o i d process l i e
above t h e a n t e ri o r a n d u p per e d ge o f t h e v e r t e b r a l b o d y
of C 7 . I n t h i s c a s e k y p h o s i s o f t h e m i d -cerv i c a l s p i n e i s
i n k e e p i n g w i t h a n o rm a l s t a t i c f u n c t i o n , ow i n g t o a fl a t
bac k , C 7 be i n g a l m os t h o r i z o n t a l
L a te r a l
pat i e n t si tting
Copyrighted Material
FIII1C1ion({/ anowmy
({nd radiography
of (h e spi/l11/ column
71
Figllre 3.38 Late ral view of t h e c e rv i ca l s p i n e w i t h
t h e a t l a s i n a n t elk x i o n ( rela tive t o t h e axis)
posi t i o n . O b v i o u s l y . i n t h e forw a rd d r a wn p os i t i o n
t h i s i m b a l a n c e is gre a t l y e n h a n ce d . p ro d u c i n g i n ­
creased
aci ti v i t y
i n the neck
m u sc l e s
and
( b y co u n ­
kyphosis.
m a y be i n
A s G a i z l e r ( 1 974 ) h a s s h ow n , i n ord e r t o ge t a
t r u e p i c t ure it is v e r y i m p o rt a n t to t a k e the l a t e r a l
v i e w i n a re l a x e d p o s i t i o n . t h e s u bj e c t s i t ti n g w i t h o u t
s u pport. or fa u l t y p os t u re m a y be o v e r l oo k e d . It i s
ne c e ssa r y . how e v e r . t o i n s is t o n t h e p a t i e n t r e l a x i n g
a
the o u t e r
lordosis
or
p o s i t i o n o f a n te - o r r e t ro fl e x i o n
in
' at l a s
i n fe r i o r '
used
by
c h i ro p ra c t or s
a re
most
confus ing a nd s h ould b e avoid ed ) . Because of t h e
tilting
mech a n ism
a
gro u p
of
the
atlas
as d es c r i b e d
in
U iI U
o f S O p a t i e n ts I c o m pa r e d la te ral v i e ws w i t h t h e
e r e c t , s t a n d i n g a n d s i t t i n g re l a x e d .
Whereas with the
inc rea sed
cra n i o c e r v i c a l j u n c t i o n t h e a t l a s
k e e p i n g h i s gaze on a n o bj e c t
at e y e l e v e l . to a v o i d h e a d a n t e[-l e x i on . In
p a t i e n ts s i t t i n g
l oca l l y
a nd/or
A t the
re l a t i o n to t h e a x i s ( t h e te r m s ' a t l a s s u p e r i o r ' or
t e r p r e s s u re ) i n c re a sed s t ra i n on t h e c e r v i c a l s p i n e .
w h i l e c o ns t a n t l y
position)
subject
s i t t i n g e r e c t ( Fi gu re
3.37)
a u d i to r y m e a t u s w a s a l m o s t e x a c t l y a b o v e
t h e a n te r i o r u p p e r e d g e o f t h e C7 v e r te b ra ( o n
m m be h i n d ) , i n s t a n d i n g p a t i e n t s i t w a s
7 m m i n fro n t o r t h i s e d ge . a n d i n t h e re l a x e d s i t t i ng
pos i t i on ( i . e . i n t h e h a b i t u a l w o r k i n g pos t u re ) i t was
1 6 mm in fro n t. I n i n d i v i d u a l c a ses t h ere w e r e
d i ffe rences of u p to 5 cm ' Th i s is p a r t i c u l a r l y s o if
t h e re i s m a r k e d l u m b a r k y p h o s i s i n s i t t i n g , ca u s e d
average 1 . 9
by
l umbar
h y per mobil i t y .
c h a n ge s i n s ta t ics co n c e r n i n g t h e
w h o l e c e rv ic a l spine. t h e re ca n be re l a t i v e fo rwa rd
In addition
or
b a c k w a rd
to
s h i ft
(even
in
the
n e u t ra l .
erect
Figure 3.39 A s y m m e t r i c a l posi t i on of t h e a t las re l a t i v e to
the co n d y l e s a n d the axis ( t h e dotted l i n e s represe n t t h e
p l a n e s o f t h e co n d y l es a n d t h e a x i s . conve rg i n g to t h e
s i d e of t h e re l a t iv e a t l a s s h i ft )
Copyrighted Material
72
Man ipulative Th erapy
in Rehab ili/ation of th e Loco/n %
/ System
(8)
Figure 3.41 D e x t r o r o t a t i o n of t h e a t l a s . ( a ) A n te ro ­
X - ra y . ( b ) D i a g r a m
poste r i o r
I n a d d i t i o n to r o ta t i o n i n i n d i v i d ua l segme n t s
t he re is fre q u e n t a s y m m e t ry o f t h e a t l as i n re l a t i o n
t o t h e a x i s , a s though t h e a t l a s w e re s h i ft e d to one
s i d e . A t t h e same t i m e the c o n d y l e s a re s h i f te d
re l a t i v e to t h e a t l a s i n the o pp o si t e d i recti o n . T h i s
i s fre q u e n t l y descri bed a s a s h i f t o f t h e a t l a s re l a tive
to t h e a x i s and the condyles i n t h e s a m e d i re c t i o n ,
b u t t h i s i s n o t q u ite cons iste n t . a s m o v e m e n t i n t h e
s p i n a l colu m n s h o u l d a l w a y s be d e s c r i b e d in re l a t i o n
to t h e l ow e r ele m e n t (Figu res 3 . 3 9 a n d 3 . 40) .
I s o l a t ed r o t a t i o n o f t h e a t l a s in r e l a t i o n to both t h e
a x i s a n d t h e occi p u t i s u n c o m m o n . O n t h e s i d e o f
ro t a t i o n there i s a n a rrow a rtic u l a r c l eft b e t we e n
a t las a n d a x i s a n d a l a rge r l a t e r a l t r i a n g l e o f the
a tl as , t h e cen tre o f the poste r i o r a t las a rc h b e i n g
s h i ft e d i n t h e o p p o s i t e d i re c t i o n a n d t h e m a s s a
l a t e r a l i s b e i n g l a rg e r o n t he s i d e o p p o s i t e t o ro t a t i o n
( F i g u r e 3 .4 1 ) .
M u c h more fre q u e n t l y t h a n rota t i o n o f t h e a t l a s
i s a x i s r o t a t i o n i n t h e n e u t r a l p os i t i o n o f t h e h e a d
a n d n e c k ( s e e F i g u r e s 3 . 2 6 a n d 3 . 2 7 ) . In fact, r o t a t i o n
of t h e order of 5 d e g re e s is q u i t e common a n d eve n
of t h e order of t o degrees i s n o t u n u s u a l . I n t e rest­
i n g l y , ro t a t i o n ( a n d eq u a l ly a sy m m e t ry of the sp i n o u s
process) of t h e a x i s is acco m p a n i e d by rota t i o n of
the ce rvica l verte b rae be l o w the a x i s , q u i te fr e ,
Ib)
Figure 3.40 ( a ) A n t e ro p o s t e r i o r X - r a y s h o w i ng
the a t l a s a ga i n s t the occi p i t a l
c o n d y l e s t o t h e l e ft . ( b ) A ft e r t r e a t m e n t t h e pos i t i o n i s
a s y m m e t r i c a l pos i t io n of
s y m m e t rica l
a n teAex io n a n d re tro A e x i o n s i t t i n g (see Figure 3 . 30 ) ,
t h e a t l a s is u s u a l l y i n a s l i g h t l y retroAexed p o s i t i o n
if t h e r e is c e rv ica l l o r d os i s , the h e a d b e i n g conse­
q u e n t l y i n a n teAe x i o n ; c o n v e r s e l y i n a k y ph o ti c
forw a rd - d r a w n p o s i ti on the a t l a s t e n d s to b e i n
a n te Aexion a n d t h e h e a d i n r e t r o A e x i o n i n re l a t i o n
to t h e a t l a s (Fig u re 3 . 3 8 ) .
,
,
Copyrighted Material
Fu n crional
ana/om v a n d
ra diography of rile sp inal column
73
Figure 3.42 Rot a t i o n of t h e cerv i c a l sp i n e i n t h e
l a t e r a l v i e w : t h e t r a n s ve r s e a n d a rt i c u l a r
p rocesses a s w e l l a s t h e j o i n t s p a ces a re
v i s u a l ized s e p a r a t e l y , o w i n g to r o t a tory d istortion
que n t l y down to C7 , p a r ticula r l y when r o t a t i o n is to
h y p e r mobi lit y ; rota tion t e l l s u s m u c h l e s s because it
t h e l e ft. The mecha n i sm is p roba b l y that d es c ribe d
i s di f A c u l t to a s se s s .
duri n g sid e-bending ( see Mob i l i ty s t u dies , below) .
T h e c h a racte r i s t i c fe a t u r es of a x is rota t i o n i n t h e
A P v i e w a re a s fo l l o w s : t h e s p i nous process a n d t h e
ped icles s h i ft t o t h e oppos i te dire c t ion to tha t of
The physiologi c a l
rota t i on . the transve rse fo ra men opens on the s i d e
d u ring
o f rot a t i on a n d the a t l a s/a xis joint s pace na r rows on
functiona l
t h e opp o s ite s i d e . In t h e r e s t of
the re is d is tort i on of t h e
the
u n ciform
L a tera l flexion
rea ction of t h e cerv ical s pine
side-bending
anato m y .
has
been
La teral
d escribe d
flexion
under
i s e x a mine d
ce rvic a l s pi n e
m a in l y in order to d etect movement restrictio n . One
p rocesses in
of t h e most i n te re s t i n g obse rvations is that if the re
addition to t h e s h i ft of the s pinou s processes a n d
is no rot a t i on in the u p p e r ce rvic a l s p i n e d u r i n g side­
ped icles. I n t h e s i d e v i ew o f rot a t i o n o f t h e cerv i c a l
b e n d i ng, t h e re wil l be n o n e i n the lowe r cervic a l
s p i n e , t h e s t r u ctures t h a t u sual l y overla p a re separ­
s p i n e (Figure 3 . 43 ) . O n the ot h e r hand , l a c k of
ately vis u a l ized : joint spaces, a r t i c u l a r proce sses a n d
ro t a t i o n i n t h e lower c e r v ic a l s p i n e w i l l not have a n y
t r a n sverse p rocesses . I n fa c t , t h e t r ansve rse p roce s s
e ffec t o n rota tion i n t h e u p p e r c e rv ic a l spi ne. This
o f t h e a x i s i s proj ected i n fro n t o f t h e bod y of t h e
is yet f u r t h e r proof th a t rota tion of t h e ce r v ic a l s p i ne
a x i s (Figu re
during sid e - be n d in g origin a te s a t t h e a x i s . J i rout
An
3 .42).
i m port a n t
sign
of
s t a tic
d i s t u r b a nce
is
( 1 97 1 ) ha s s h o w n t h a t rot a t ion is tran s m i tted to the
d i scre p a n c y b e tw e e n t h e A P view t a k e n w i th t h e
l owe r cerv i c a l ve rtebrae by m eans of t h e s pinous
pa t i e n t sup i n e a n d t h e l a te r a l v i e w in s i tt i n g , i n
proces s e s . I f, for ex a m pl e . the s pinous p rocess of C2
pa r ticul a r i f t h e re i s m a r k e d rotation in s i t t i n g a n d
or
non e a t a l l i n t h e supi n e posi tion; thi s i s usua l l y d u e
r o t a ted , e.g. pointing to the r i g h t
t o o b l iqu i t y b e l o w the c e r v ic a l s p i n e .
b e n di n g to the right t hi s s p i nous p rocess w i l l not
C3 i s a s y m m e t ri c a l wi thout tha t ve rtebra being
,
then on sid e­
d e viate to the left, but m a y re ach only t he mid- line.
In such a case the rest of t h e c e r v i c a l s pi ne bel ow
M o b i l ity stu d i e s
this v e r te b ra wi l l not rota te , just as t h ough rota tion
X - r a y s o f l a te ra l , a n te - a n d ret ro fl e x i o n c a n b e u s e f u l
had
i n the d i ag n os i s of movem e n t res t r i c t i o n
( Fi g u r e 3 .44) .
and
of
been
rest ricted
Copyrighted Material
in
t h e upper ce rvic a l
s p i ne
74
{V/(fl1ip u lalive
Therapy in RehabililOliol1 of th e
Locomotor Sys/e/11
(b)
(a)
Figure 3.44 T h e e ffe ct o f a sy m m e t ri c a l po s i t i o n o f a
process on r o t a t i o n of t h e ca u d a l cerv i c a l
ve rte b r a e a t s i d e - b e n d i n g . ( a ) A t n e u t r a l p o s i t i o n t h e
s p i n o u s p r oc ess o f C 2 d e v i a t e s t o t h e r i g h t . ( b ) S i d e ­
be n d i n g t o t h e r i g h t c a ll s e s d e x t roro t a t i o n of t h e a x i s .
t h e s p i n o u s process o f t h e a x i s rOUl t i n g o n l y i n t o m i d ­
l i n e , however: t h e ca u d a l c e rv i c a l v e re t e b r a e re m a i n
unrotated ( A fter J i ro u t . 1 970)
s p i n o ll s
h a n d . if th e axis d o e s n o t r o t a t e t h e re i s n o s i d e ­
b e nd i n g a t t h e c ra n i oc e r v i c a l j u n ct i o n ( F i g u re
This i s i n k e e p i n g w i t h t h e fa c t t h a t i n
3 .45 ) .
cases o f
a t l a s a ss i m i l a t i o n to t h e occ i p u t , s i d e - b e n d i n g a t t h e
j u nc t i o n
may be n o rm a l .
T h e q u e s t i o n n o w a rises w h e t h e r m o v e m e n t re­
s t ri c t i o n b e t w e e n a t l as a n d occi p u t o n s i d e -b e n d i ng
c a n be v i s u a l i z e d by X - r a y . We h a v e s h o w n t h i s to
b e po s s i b l e
( Le w i t and K r a u s o v <l . 1 967 ) , but o n l.y
i . e . w i t h a t l as/a x i s l o c ke d . This
i s o f great i m p o rt a n c e for c l i n i ca l d i a g n os i s .
w i t h the h e a d r o t a t e d .
Figllre 3.43
(a)
B l o c ked rot a t i o n o f t h e
a x i s il t
t h e r i g h t : n o ro ta t i o n o f t h e ce rv i c a l
s p i n e be l ow C 2 . ( b ) A ft e r t r e a t m e n t : norm a l
d e x t ro ro t a t i o n from t h e a x i s d o w n t o C.'i . l a t e r a l flex ion
o f the e n t i re sp i n e i n creased c o m p a red w i th (a)
l a t e ro fl e x i o n t o
A l t h o u g h s i de -s h i ft i ng o f t h e a t l a s i s the r u l e i n
l a t e r a l fl e x i o n . a t t i m e s i t d o e s n o t t a k e p l a c e w i t h o u t
m o ve me n t r e s t r i c t i o n . i n p a r t i c u l a r i f t h e re i s m a r k e d
a s y m m e t ry : e v e n m ore i m porta n t . e v e n i n c a se s o f
cl i n i c a l l y s e v e re m o v e m e n t re s tr i c t i o n b e t w e e n a t l a s
a n d occ i p u t , t h i s s i d e - s h i ft m a y be see n . On t h e o t h e r
It is u s u al l y e a s y to s e e m o v e m e n t re s t ri c t i o n
between t h e a t l as a n d a x i s o n side-be n d i ng: the a x i s
d o e s n o t r o t a t e ( Fi g u re 3 . 45 ) . I n t h e r e s t o f t h e
c e r v i c a l s p i n e t h i s i s m uc h l e s s e a s y t o v i s u a l i ze
by X - r a y , e v e n w h e r e it c a n be c l e a rl y d i a g n os e d
c l i n i c a l l y . A cco r d i n g to J i ro u t ( 1 970) s m a l l t i l t i n g
m o v e m e n ts i n t h e s a g i t t a l p l a n e t a ke p l ace on s i d e ­
b e n d i n g a n cl c a n be r e c o g n i z e d b y a c h a n ge i n t h e
p o s i t i o n o f t h e s p i n o u s p ro c e s s . T h e s e sy n k i n e s e s i n
t h e s a gi t t a l p l a n e c o r r e s p o n d t o j o i n t p l a y o f t h e
ce r v i c a l s p i n e a n d a re m o re p r o n e to m ov e m e n t
r e s t r i c t i o n th a n i s l a t e r a l b e n d i n g ( a s c a n be s e e n
from c o m p a r i s o n o f X - ra y s taken b e fore a n d a fte r
m a n i p u l a t i o n ) . Mo r e o ve r . t h e c h a n g e d posi t i o n o f
t h e s p i n o us process, i . e . t h e t i l t i n t h e sagi t t a l p l a n e ,
d o e s n o t n eces s a r i l y d i s a p p e a r a ft e r t h e ce rv ic a l
s p i n e re t u r n s to n e u t ra l po s i t i o n : i t m a y n o t r e a c h
t h e s a m e po s i t i o n , b u t m a y e v e n o v e r r e ac h i t .
Copyrighted Material
Fun clional analOm v
lind radiography of Ihe
spi n a l
column
75
Figure 3.45 B l o c k e d pass i v e l a t e ra l fl e x i o n a t t h e
I n t h e n e u t r a l p os i t i o n t h e
c r a n ioce r v i c a l j u n ct i o n . ( a )
a t l a s i s s l i gh t ly a s y m m e t r i ca l , to t h e r i g h t o f t h e c o n d y l e s
a n d t h e a x i s . ( b ) A t t e m p t e d p a s s i v e l e ft l a te r a l fl e x i o n a t
fa i l e d ; t h e re i s n o a x i s
rota t i o n , y e t t h e a t l a s h a s m o v e d t o t h e I d t ( I ) . ( c ) A ft e r
t rea t m en t , n o rm a l l a terai ll e xi o n o f t h e u p p er cervica l
s p i ne is r e s t o re cl , wi t h n o rm a l ( sl i g h t ) ro t a t i o n of t h e a x i s
a n d s h i fr o f t h e a t l a s t o t h e l e ft
t h e u p p e r ce r v i ca l s p i ne h a s
Copyrighted Material
76
Manipulative Th erapy in Rehabilitation of rhe Locomotor System
Figure 3.46 AP p i c t u res of the c e r v ica l s p i n e : l e l t in n e u t r a l pos i t i o n , right s i d e be n t to the l e ft . Co m p a r e t he pos i t i o n
o r t h e s p i n o u s process i n r e l a t i o n to t h e v e r t e b r a l b o d y a t C 7 a n d C 6 ( r e p r o d u c e d b y k i n d p e r m i s s i o n o f Pro fessor
-
J i ro u t)
s h ow i n g
( F ig u re
t he
v a r i a b il i t y
of
the
n e u t ra l
po s i t i o n
3 . 46) .
We m u s t t h e re fore c o n c l u d e t h a t l a te ra l A e x i o n o f
t h e h e a d a ga i n s t t h e c e r v i c a l s p i n e i n t h e c o ro n a l
p l a n e is m a i n l y t h e res ult o f a x i s rota t i o n ; c o n ­
v e rs e l y , i f we res to re blo c k e d s i d e - be n d i n g a t t h e
c ra n i o c erv i c a l
e v e n II) a s i n gle segm e n t .
j u nct i o n
j u n c t i o n we
re s t o r e ro t a t i o n b e t w e e n
t h ere
may
be
At
the
t he c ra n i ocerv i c a l
fo llow i n g
s i n gs
of
h y p e nn o b i l i ty :
I . La x i ty o f t h e tra n s v e rse l ig a m e n t b e t w e e n a t l a s
a n d a x i s , w i t h a n i nc r e a s e d d i s ta n ce betwee n t h e
a n t e ri o r arch o f t h e a t l a s a n d t h e o d o n t o i d . As a
the atlas a n d axis.
co nseq u e n ce
L a t e r a l A e x i o n b e t w e e n occ i p u t a n d a t l a s c a n b e
(Figure
3 .47) .
the
At
b a s io n
the
a l so
s h i fts
t i me
same
fo r w a rd
the
a ngle
e s t a b l i s h e d c l i n i c all y a n d b y X - r a y o n ly i f t h e a t l a s
b e t w e e n t h e cl i v u s a n d t h e o d o n t o i d de cre ases
a n d a x i s a re l o c k e d , i . e . i f t h e h e a d is r o ta t e d
Move m e n t restr i c t i o n of t h e o c c i p u t on t h e a t l a s
a n te A e x i o n of t h e whole of t h e c e r v i c a l sp i n e
not o n l y when t h e chin i s h e l d i n , but a l so d u r i n g
.
( F i g u r e 3 .47) .
d o e s n o t i n t e r fe re w i t h s i d e - bend i n g i n t h e c o r o n a l
pl ane, nor
with
a s h ift i n g sy n k i n es is o f t h e a t las
a g a i ns t the occiput d uri n g ro ta t i o n
2.
.
T il ere i s h y p e r m o b i l i t y be twee n t h e o cc i p u t a n d
t h e a t l a s , w i t h i n creased s h i ft o f t h e b a s i o n a n d
o p i st h i o n i n re l a t i o n to t h e a t l a s , w i t h o u t l a x i ty
of t h e t r a n s v e rse l i game n t ( F i g u r e
A n teflexion
A n te - a nd retro A e x i o n are
the
m ov e m e n ts m o s t
p e r fo r me d by t h e ce r v i c a l s p i n e ; h e n c e
r e s t r i c t i o n w i l l s h o w o n ly i n re l a t i vely s e v e r e
c a s e s ( e x c ept b e t w e e n occi p u t a n d a t l a s ) . O n
e a s i ly
3.48) .
S o m e m o r p h o l o g i c a l aspects
It is, o f c o u rs e , i m poss i b l e to cl o j u sti ce to the v a s t
fi e l d o f m o r p h ology i n t h i s b o o k : fo rtu n a t e l y , i t i s
t h e o t h e r h a n d , a n t e - a n d retro A exion w ill revea l
a de q uately dealt w i t h i n t h e tra d i t i o n a l l i te ra t u r e ,
a n y hyperm obil i t y :
shift i n g m o v e m e n ts
a n cl
l ordosis or k y p h osis
i m p o r t a nt fo r u s a re to u c h e d o n h e r e
between C2
and
i n c re a se d
C7 , i n c r e a s e d
Copyrighted Material
o n ly
some
aspects
w h ich
a re
.
p a r t icu l a r l y
Fl ln ctional anatomy and
radiograph y of tite
sp illal collll11n
Figure 3.47 H y p e r m o b i l i t y at head a n te fl e x i o n w i t h l a x i t y o f t he t r a n s v e rse l i ga m e n ts o f t h e a t l a s . (a) In the n e u t r a l
pos i t i o n the a n t e r i o r fa c e t of the a n t e ri o r a rc h of the a t l a s is p a r a l l e l to t h e o d o n t o i d p rocess. ( b ) L i g h t a n d
(e) m a x i m u m a n tefl e x i o n : t h e re is i n cre a s i n g a n gu l a t i o n b e t w e e n t h e a r t i c u l a r fa c e t s o f t h e a n t e ri o r a rch o f t h e a t l a s
a n d t he o d o n t o i d ; n o t e t h e c h a n g e i n t h e a n g l e b e t ween t h e c li v u s a n d t h e a x i s a n d t h e a n t e r i o r s h i ft of the b a s i o n
Copyrighted Material
77
7i3
Mllnipu/a/ive Therap .l' in Rehab ilita tion o( /he Locomo/Or Sys/ci l /
h e a d il n t e - a n d re t ro fl e x i o n b e t w e e n o cc i p u t a n d a t l a s . ( 0 ) A t a n t e fle x i o n ( a u t o t o m o g r il m
b a s i o n l i e s a b ove t h e a n t e r i o r a rc h o f t h e a t l a s and the o p i s t h i o n il h ove t h e pos t e r i o r " rc h :
t h e a rc h e d c o u rse o f t h e fo r a m e n m a g n u m M a ge n d i h a s b e e n d r a w n i n . ( b ) At re t ro rl e x i o n t h e occ i p u t h a s s h i ft e d
2 . 5 e m ( ' ) b a c k (compa re t h e re l a t i ve p o s i t i o n s o f t h e b a s i o n a n d t h e odon t o i d p rocess a n d t h e o p i s t h i o l l a n d t h e
p o s t e r i or a rc h o f t h e a t l a s). F o r e a s i e r c o m p a ri s o n ( a ) h a s b e e n t u rn e d 90 d e g r e e s c l o c k w i s e
Figure 3 . 48 H y p e r m ob i l i ty
at
d ur i n g p n e um ograp h y ) t h e
Figure 3.49 I n c o m p l e t e c o n g e n i t a l c o a le s e n ce o f C5 a n d
C6 w i t h a h y p o p l a s t i c i nt e l've r t e b r a l d i sc a n d a s h o rt
a n t e ro poste r i o r d i a m e t e r of bot h a d j a c e n t verte b r a l
Figure 3 . 5 0 The
bodies
Copyrighted Material
n a rrow
sp i lw l c a n n l
Fl lnClioll (f1 alll/lOmy lind radiography of the spin a l colul1m
79
Figure 3.51 B a s i l M i m p r e ss i o n . (iI ) Late ra l v i e w w i t h s h o r t c l i v u s . ( b ) P os i t ion of t h e o d o n t o i d h i g h a b ove t h e c o n d y l e s
Figure 3.52 Os o d o n t o i d e s , side
view ( a r r o w s ) ( R e prod u c e d by
k i n d p e r m i s s i o n o f D r E . G.
Metz)
Copyrighted Material
tlO
Mal1 ip l lialive Therapy
il1
RehaiJ ilil[{/iOI1 of Ihe Locom otor System
( a)
Figure 3.53 Spo n d y l a rth ros i s w i t h a h orizo n t a l C O llrse of t h e i n tervertebral apophyseal
j o i nts. (a) In the A P ; ( b ) ( opposite) i n the s i d e view
A n o m a l i es
A n o m a l ies m a y be i m p o r ta n t b e c a u s e tbey
fre q uently imply some degree of c h a n ge i n funct i o n .
T h i s is pa rticu l a r l y o b v i o u s i n coa l esce nce o f
vertebra l bod i es a n d/or a r c h e s . These m a y be o n l y
parti a l . a n d i n s u c h c a s e s w e s e e a hypop l astic
i n te rverte b r a l d i sc, the verte b r a l bodies adjace n t to
tha t d isc being n a rrower (Figure 3.49). The a n o m a l y
i m p l i e s red u c e d or n o m o b i l i ty i n a segm e n t a n d
prod uces (compensa t ory) hypermobili ty i n t h e neigh­
bouring segm e n t ( u s u a l l y cran i a l ) res u l ting u l t i mately
i n degenerative cha nges. A fre q u e n t anoma l y is a
transitio n a l cerv i cot horacic ve r t e b r a C7 w i t h l a r ge
tra n sverse p rocesses a nd/or cervical ribs and w i thou t
unciform processes; it is often asymmetrical.
Cl i n ic a l l y the most i m porta n t anomaly is a na rrow
s p i n a l ca n a l , because it m a y cause cervica l myelo­
p a t h y . A more usefu l method t h a n measuring the
w i d t h o f t h e a n te r i o r-posterior d i a m e t e r is t o ob­
serve t h e a l t e red proport ions visible a t firs t glance:
n o r m a l l y the s p i n a l c a n a l is wider t h a n the vertebra l
body i n the cerv i c a l spine; i n t he n a rrow s p i n a l ca na l
it is na rrowe r a n d t h e s h a d ow of the a r ticu l a r
Copyrighted Material
FI I I I Uiol7 (1 /
(JIl(l l O m V
(I n r i
radiography of fhe spinal
cO/limn
8l
( b)
Figure 3.53
(co n t i n ued )
processes cover m o s t of t h e b r e a d t h o f t h e s p i n a l
a b o v e t h e b i m a s t o i d a n d b i d i ga s t r i c a l l i n e s ( Fi g u re
ca n a l
3.5 1). At the
( Figu re 3 . 50 ) .
The
c ra n i oc e r v i c a l
j u n ct i o n .
as
a
region
of
t r a n s i t i o n . i s the s i t e o f freq u e n t a n o m a l i e s . The
most i m p o r t a n t o f t h e s e is b a s i l a r i m press i o n d u e t o
hypop l a s i a o f t h e b a s e o f t h e occ i p i t a l b o n e . I n t h i s
co n d i t i o n t h e o c c i p i ta l p a r t o f t h e cl i v u s i s s h o r t e n e d
a n d t h e r e f o re t h e o d o n t o i d process i s d r a w n u p i n to
t h e fo ra m e n m a g n u m a n d is s i t u a te d c o n s i d e ra b l y
above t h e p a l a t o -occ i p i ta l l i n e i n t h e l a t e r a l v i e w ; i n
t h e A P v i e w i t c a n r e a c h t ile u p p e r b o r d e r o f t h e
fora m e n m a g n u m betwe e n t h e c o n d y l e s , a n d b e h igh
s a m e t i m e t h e fo ra m e n m a g n u m m a y
be n a rrow e r t h a n us u a l , u n l e ss t he r e i s a l so a n
A rno l d -Ch i ari d e form i t y . T h e c h a n g e s m a y c a u se
c o m p re s s i o n of t h e nervo u s tiss u e n o t u n l i k e t h a t
w h i c h oc c urs w i t h a n a rrow s p i n a l ca n a l f u r t h e r
d o w n ( F i g u re 3 . 5 1 ) .
I n a d d i t i o n t h e re i s o f t e n h y p o p l as i a o r a s s i m i ­
l a t i o n of t h e a t l a s to t h e occ i p i t a l c o n d y l e s . Less
i s c o a l e s c e n c e o f t h e m a s s a l a t e ra l i s
o n e - s i d e d ) w i t h t h e a x i s . A ll t h e a n o m a l i e s
m o re oft e n
th a n n o t a s y m m e t r i ca l : t h is
common
(u s u a l ly
are
Copyrighted Material
82
lv/an ip l l iative Therapy in Rehabilitation of the
Locomotor System
O n e i m porta n t a n o m a l y ( m a lfo r m a t i o n ) is hypo­
plasia of the odontoid and the os odo n t o ides, which
i m p l i e s p a t h o logica l hypermob i l i ty (Figure 3 . 5 2 ) .
A n o t h e r s i g n i fi ca n t a n o m a l y o f t h e odontoid is i n ­
creased rec l i n a tion ( G u t m a n n , 1 98 1 ) , wh ich forces
the atlas i n t o a position of retroflexion a n d the refore
p l aces i ncreased s tra i n on t h e transverse liga m e n t of
t h e a t l a s d u ring head a n teflex i o n , a n d m a y cause
l a x i ty of that ligame n t .
D e g e n erative c h a n g e s
Degenerative c h a nges in t h e cerv ica l sp i ne a re o f
speci a l c l i n i c a l i n terest w h e n t h e y i mpi nge on t h e
i n te rve rte bral fora m i n a a n d m a y therefore i n terfe re
w i t h b o t h t h e sp i n a l roo t a n d the vertebral artery.
For t h is reason oblique views are useful (see Figu re
3.24). These cha nges m a i n l y conce r n the u n c i form
processes ( n e u rocent ral j o i n t s ) i n pa rticular t h e i r
poster i o r parts . They a re close l y corre l a ted to d isc
dege n eratio n , as n a rrowi n g of the d isc b r i ngs t h e
u n ciform p rocess o f t h e lower vertebra into close
c o n tact with the lower la tera l m a rgin of the vertebra
a bove.
S i m i larly, deform i t y o f t h e articu l a r processes m a y
i m p i nge o n t h e i n te rve rtebral fora m e n . This i s fou n d
i n a rth rosis o f the apophyse a l j o i nts, w h i c h u s u a l l y
goes h a n d i n h a n d w i t h a h o r i z o n t a l posi tion ; i n such
cases t h e a pophyse a l j o i n ts beco m e the weight­
bearing structures (Figure 3 . 5 3 ) . They a r e the refore
seen very w e l l in the A P v i e w .
Fi n a l l y , I m ust poi n t o u t t h e great sign i ficance o f
a c h a nge i n the p a ra l l e l course of both apophyse a l
j oi n ts i n o n e segm e n t , seen i n a n und isto rted l a t e ra l
v iew
T h is i m p l ies fo rced rotation o f the ce rvica l
spi n e d u ri n g retro fl e x ion , p rod ucing na rrow i n g o f
t h e i n tervertebra l foramen o n one s i d e ( Fi g u r e 3.54).
,
Figure 3.54 D i ffe rence in the o b l i q ue co u rse of t h e
C3 a n d C 4 i n t h e l a t e r a l v i e w
a p o p h y s e a l j o i n ts b e t we e n
( a rrow)
asy m me t ry concerns t h e w h o l e of the cra n iocervical
j u nction a n d m a y p rod uce side-s h i ft of the atlas and
e v e n m a r ked rotation of the axis in n e u t r a l posi t i o n ,
w h i c h n ecessa rily prod uces asymmetrica l mechanisms
of s i d e - b e n d i n g a n d rotati o n .
Copyrighted Material
.
4
Examination of locomotor function and
its disturbance
Case history
heart, or in
times and
As in oth er fields of medicine, examination sta rts
with the anamnesis. B ec a u se v erte b ro genic disorders
represent the m ost im portant grou p, they will serve
as the pr in cipa l e x a m pl e. I t i s i m p ort a nt to stre ss
from the outset that diagnosis of disturbed f u nctio n
as the cause of d is ease should not be ma de per
exclusion em - i.e . o n ly if other ( organ ic) causes are
ru led out - but principa lly on po siti v e evidence, of
which a cha ra ct e ri stic history is sig n ifi c a nt. We owe
the main c r ite r ia t o G u tze i t (1956).
Chronic i ntermittent course
Unless we see a n acute condition in a young patien t ,
we can us u a l ly ascertain by q u es tion ing that t h e re
have been p reviou s a ttacks, perh aps going a s fa r
back as ad o l e sce nce (e.g. low - b ac k pain d urin g
menstrua tion i n y o u ng girls). There are pe ri od s o f
com p l e t e recovery i n b etwe en, a n d w e sho u l d try t o
ascert ai n the frequency a nd d u ration of the a t tacks
( and the free inte r v a l s ) , and the t i me of onset of t h e
l a test attack, providing ev i d ence for the ge neral
tre nd of the p at i en t ' s condi tion.
Involve ment of the locom otor system
function o f t h e l ocomo to r system a n d its
d ist u rbance can never be l im i ted only to one
structure, and therefore sym p toms occur in various
more d istant parts of the system in t h e co urse
of time, the vari o u s l y l ocated c om p laints ha ving,
perh aps, a comm o n denominator - the vertebral
colu mn. This, too, has t o be elicited by c a re ful
questioning; the patient will pr ob a bly be una wa re of
the pos si ble connection between, for exa m pl e,
h eada c he , sh o u l der pa in , pain in the reg io n of the
The
the
hip or knee, ex p e r ie nced
at
different
pe rh a ps after considerable intervals.
S u sceptibi l ity to strain a n d sustained
posture
Fun ction and
its
disturba nces i n the locomotor
syste m are ob v i ou s ly
influe n ced by stra in imp ose d
by e n fo rced movement or sustained posture. O ne of
the most important poin ts in recording the case
h is to ry is to det ermine u n der wha t condi tions the
a t ta c ks occur; this is n ot on l y of d ia gnostic va l u e, bu t
a l so im po r tan t for t h e ra p y a nd pre v en t ion . This is
the m ost crucial but also the most diffic u l t inform­
a t i on to extract from the p a tient. It does little good
to a sk him after what his sy m ptoms started, for he
is likely to provi d e all the theories he has h e ard or
formed for himself. Wha t we need to know a re the
imm edia t e circumstances i n which p a i n was fe l t . Thi s
pa t i e nt s are often rel uc t a n t t o tell, either beca use
they cannot reme m be r or bec a u se t h e y find it i rrele­
vant o r unim p o rt a nt ; such s ta t e ment s a s 'I was s itt i n g,
a n d w h e n I got u p from my ch ai r ... ', 'I was shaving
a nd when I looked in to the mirror . .. ', ' . . . when
wak i n g up i n the m orning o r turn ing round in bed
. ..', 'when 1 st oo p ed to p ick up this bit of pa per
from the floor . . . ', a re sign ifican t details. It is also
important to learn which po sition or movement
giv es rel i e f. I t is i mportant to .k
provo k ed b y a si ng l e br u sq ue movement, by stre n ­
uous effort of so m e d u ra t ion, or by an e n for ced l),
rigid pos i ti on . S l ight d etails m a y be i m p ort a n t : the
u nderlying calise of p a in may be very differe nt if
it occurs d u ri ng fo r w a r d b e nding, while stooping
(e.g. o ver a work bench ) , in maximum flexion ( e.g.
s t oo ping to wipe a floor ), or while straightening u p
from a sto oping posi tion. Also pain m a y occur o n
co u g hin g , sneezing, even la u gh i ng.
83
Copyrighted Material
H4
Manipu/otil'I.."
/?ciluhrlirarion of rhe Locomotor S),SI"lIl
Even if the patient
or
Trauma
further questioning
desCi
Trauma is
of
causes of disturbed
paroxysmally.
revea
function alltl pnlvldllS e'lgnifICi\f11 corroboration, even
ii' structural damage is also present. We must insist
on the fact that any external force applied to the
body affects the locomotor system and the spinal
column. This is particularly the case in head injury.
Asymmetrical localization
Vertebrogenic pain is rarely sYlllmetricaL and IS often
one-sided. This holds for radicular and pseudo­
Unfortunately the patient often forgets a minor
radicular syndromes of the extremitics as well as for
trauma (such as an awkwardly performed somer­
headache, shoulder pain and pain in the chest.
saUlt) and it is therefore advisable to ask what sports
he indulges in. To give a typical example
Cl
patient
who 'never suffered am' trilumil' silid that hiS hobbies
The role of age
For
were boxing
tlecolCiing to the age of the
the
patienl
We
In vertebrog,"rJlc
t is important to bear in
pathological conditions
osteochonclrosis in adol-
mechanical factor
in young patients and
rCJC!ions of the nervous
middle-aged adults; after
II bll
account. These include undue susceptibility to changes in the weathcr,
particularly to cold and to high humidity; infectiOUs
(osteoporosis) may occur,
the ilGt
especially in women; progressive (destructive) osteo­
arthrosis, especially of the hip and knee JOJlll. can
is not the
system mthl
Olle'.
diseases causing high temperatures; hormonal diS'
be found in older men and women and so, too, can
turbances (more apparent in women because of the
malignant disease. For this reason a history of pain
menstrual cycle); pain of locomotor origin which is
in the locomotor system that b eg ins after the age of
heightened during menstruation; even allergy may
about 50 and takes a progressive course mLlst be
be involved.
treated with great circumspection.
The
Exa
As the
instrument of our
!.lent symptom of
expected I
present
in
it is only to be
by clinical examination.
of medicine in which
!llctor is frequently
decisive a role, and is so
The
Psychological
of locomotor function.
excludes, but rather
moment the patient enters
I
clr:;lUrbed function of
the motor system. It must be stressed that adequate
down, undresses, etc. The patient must always un­
treatment of the locomotor disturbance usually deals
dress for the first examination (to bra and briefs);
involvemellt
corroboral
he or she moves, sits
most effectively with the pain, giving the phYSician
natural movement is essential. Whatever the site of
a much better chance to deal with the psychological
the trouble, important if not vital information may
problems, having understood the patient's main
be missed if the patient remains fully dressed.
trouble. The course of treatment reveals the import­
ance of the psychological factor as such and finally
shows whether the patient recovers psychologically
when relieved of pain. or whether the psychological
relapse through
conditions
muscular
masked
Examination of posture
(inspection)
for example, in
with the rear view; the
pain is not
the heels. This is
is capabJe of
observing the patient
I. without frequent
fronl
of tIle'
final.ly by examination
be followed by examin-
atiol!
We
Paroxysmal
looking at the shape
(roundness) of the heel and its deviation; the shape
Those complaints in which autonomic nervous symp­
toms are prominent follow a typical paroxysmal
course, e.g. vertebrogenic headache, vertIgo, cardiac
and thickness of the Achilles tendon and the calves;
the lateral deviation of the knees; the shape and
thickness of the thighs; the height of the gluteal lines;
Copyrighted Material
Examination of /ocorl1otOf
t he posi tio n a n d symme t r y of t he h ips; t h e c o u rse of
the i n te r glu tea l l i n e a n d t he sh ape of t he b u ttoc k s;
the wa ist bet wee n t h e pe nd a n t arms forming t r i ­
angles whi c h may o r m a y n o t b e symm e t r i ca l ; the
rhom boid of Michae l i s between the d i mples si t u a ted
at the p o ste r i o r iliac spines and t h e upper en d of the
i n terglute a l l i n e and the culm i n a t i n g p o i n t of l u m bar
lordosis and i ts t ra nsi t i o n i n t o t h orac i c kyp h osis. The
t h i c k ness and prom i n e n ce o f t h e erector spi n a e
muscles are compared o n each sid e , as is the groove
between these muscles w here t h e sp i n ous processes
are s i t u a te d , and a sco l i o tic c u rve m a y b e detected .
Above the wa i st the posi t i o n of t h e s h o u l d e r b l ades
is c ompa red , toge t h e r w i t h t h e i r rel a ti v e he ig h t and
dist a n ce from t he m i d -line: then the h ei ght and
course o f the shou l d e rs is compa red . The l a t e r a l
contour o f t h e b a c k i s fo rmed by t h e qu a d r a tus
lumborum muscle at the w a i s t a n d the l a tissimus
dorsi above, u p to t h e a x i l l a . The upper margi n of
the shoul ders is fo rmed by t h e m uscu l us trape z i u s
l atera l l y , a n d b y t h e leva tor scapu lae m o r e med i a l ly .
The neck s h o u l d be in mid-line, b u t may devia t e t o
one s i d e o r t h e oth e r; fi n a l l y , t h e h e ad may be in
m i d - l i n e . or i n c l i n e d i n line w i t h t he neck , or form i n g
a n ang l e w i t h the nec k . T h e n eck c a n be s l im o r
thick, and the h a i r l i n e may b e h i g her o r lowe r o n
t h e n ape o f t h e n ec k .
J n t h e side v i e w i t is advisa b l e t o consid e r the
pos t u re as a w h ole: n o r m a l l y , t h e h e a d s h o u l d be
vert i c a l above the s h o u l d e rs w h i c h a re vertical a b ove
the hips a n d the f e e t , so t h a t t h e o u t e r me a t us
acous t i cus is vertica l l y above t h e clavi c u l a r b o n e
a n d slightly i n f ront o f t h e a n k les. I t is extreme l y
important to regi s te r a fo rw a rd - d ra w n pos i t i o n
w h e r e the head a n d n eck a re i n fro n t of t h e s h oulder
g i r d l e and t h i s is i n f ront of the hips , so t h at the
buttocks stick out b e h i n d t h e a rms, w h i c h h a n g
l oo s e l y o n e i t h e r sid e .
Ag a i n t h e e x a m i n e r looks from t h e feet up w a r d s ,
no ting t he sh ape of the fee t, t he cou rse of t h e l e gs,
in pa r tic u l a r wheth e r the knees a re bent bac k w a rds
or eve n slightly fo rward, and the convexi ty of the
buttocks. Then he fol l o ws t h e ( us u al l y lordotic)
curve of t h e l umba r spi ne; i t is importa n t to note
whether lordosis is m ost accentua ted a t the l um b o­
sacra l or i n t h e m i d o r upper l u mbar region. In cases
of i n c re ase d l o rdosis (Aa b b y posture) the a bdomen
pr o tr u de s (even if the pati e n t is s l i m ) a n d aga i n this
protrusion may be acce n t u ated at the l e v e l of the
na v e l o r above t h e pe lvis, accord i n g to w here t he
muscu l a t u re is wea kest .
In the thoracic regio n ( w h i c h is u s u a l ly k yp h o t i c )
it is i mportant to note w h e t h e r t he back is Aat or
not, w h e t h e r k yphosis is exagge rated a n d also if
kyphosis is mainly in t h e uppe r or lower t h o racic
regio n . A Aa t back freque n tly accompa n ies i ncreased
kyp hosis at the cervicothoracic j u n c ti o n . In a d dition
to kyph osi s it is i mpo rtant to n o t e w h e t h er t h e
shoulders a re d rawn fo r w a rd . Ce rvic a l lo r d osi s
d e pe nd s on
junctioll
and ils disturbance
85
the s hape of t h e t h o raci c spine, a n d in
fla t backs (frequen t ly in a thl etic y o u n g s te rs ) t h ere is
no lo rdos i s . If t h ere is i n creased l or d o s i s, typical in
Aabby posture , the t rache a a n d t h e t h yr o i d c a rt i l a g e
may p r o t r u d e , at first g l a nce giv i n g t h e impression
of an e nl a rg e d t h y r o i d gland w h ic h , however, dis­
a pp e a rs in the supine pos i t i o n . Fi n a lly , in a forw a rd ­
drawn position t h e re is fre que n t ly h ype rl o r d o s i s a t
t h e cran.iocervical junc ti o n .
I n t h e f r o n t v i e w, the e x a m i n e r may begin w i th
t h e posi t i o n of the toes a n d the a rc h o f t h e fee t .
followed b y the legs; a t t h e knee we note v a lg osi t y
o r v arosity and poss ible l a te ra l d evia tion of t he
p a t e l l a . We then foHow the con t o u rs of the t h ighs
a n d o f t h e lowe r a b d o m e n between t h e i l i a and t h e
nave l , wh ich m a y be s h i fted t o t h e s i d e , m a y b e o n
t h e su r f a c e , or m a y be e n gu l fed. The Aa n ks ma y be
d ra w n in at the w a i s tl i n e , or m a y bul g e . I f muscles
are wea k, the abdomen p rot rude s w i th the n avel on
i ts s u r face and the tlanks are bulg i n g. The lower e d g e
of t h e t h or a x m a y be p r o m i n e n t, o r m a y be h i d d e n
b y a p rot r u d i n g a b d omen; t h e e pi gastric a ngle may
be obtuse o r a cute .
It is only po ss i b l e to assess the sternum and its
p os i t ion relative to the p ect o r a l m usc l e s in men. The
l a ter a l portion of t he p ector a l i s fo rms t he anteri o r
bord er of t h e axilla: the subclavic u l a r porti o n o f the
p e cto r a lis can be a ssessed even i n w ome n who a re
not obese, a n d the upper r i b s may be visi ble . Above
the in frac l avic u l a r f os sa a re the col l ar bo n e s on both
s i d es, and it is part i cula rly impo rtant to note to wha t
e x te n t they m ove d ur i n g r espi r a tio n . The d e pt h of
t h e s upr acl avicu l a r fossa m a y be i m p o r ta n t ( t h e
i nsp i ra t o ry p osit i on of t h e t h ora x ); above th is there
is t h e contour of t h e trapezius a n d the le v a t o r
sca p u l a e, w h i c h i s n o r m a l l y concave p ro v i d e d that
there is no h yperton u s . The s h o u l d ers are late r a l l y
a b ove t h e a x i l l a, often unequal i n h e i ght.
The m o s t pro m i n e n t feature of t h e n e c k is the
j ug u l a r fossa and t h e two ste roocleid o m astoi d s; the
a t ta c h m e n t po i n t at the sternum is m ore n o t iceable
than o n the cla v i cle . B e tw e en the steroomastoids
a n d t h e tr a p e z ius some b un d l e s of t h e scaleni may
be v isib l e . In mid-line a b o v e the fossa j ugu laris t h e re
is t he p romin e n ce of t h e thyroid carti lage; it is very
i m po rt a n t to n o te wheth er it is e x ac tl y in mi d - lin e .
or p e r h a ps is slig h t l y shifted to o n e side (diffe re nce
in te nsion in the d i gastric musc les). If this is the case,
there m a y be noticeable asy m m e try of t h e subma n­
d i b u l a r reg i o n , a s far as to the angl e o f the man dible.
Hype rton us a n d h y peractivity of the mast i c a tory
musc l es is ofte n seen, a n d w e sho u l d note h o w far
the patient opens h is mouth d u r i ng spee c h . Facial
asymme t ry is very frequent a n d can be comb i n e d
w i t h a symmetry o f both the tee t h and t he skull as
we l l as w it h sco l i osis.
From both t h e r e a r and front view it is possible
to d i a gnose rel a tive weakness of o n e sid e ( h e m i h ypo­
ge ne sis); d o m inance of o n e cere b r a l hem isp here can
Copyrighted Material
86
Manipulative Therapy in Rehabilitation of the Locomotor System
freque n t l y be recognized by the d iffere nce i n
m uscula t u re o f the upper e xtremi ties . In the lower
l i mbs, the s u pporti n g leg is u su a l l y the l eft ( n o n­
d om i n a n t), w h i c h is t h e r e fore m ore powe rfu l .
Inspecti o n d u ri n g a n te flexion o f t h e trunk IS
i m p o r t a n t; rotation of t h e v e r t e b r a l co l u m n i n
sco l i os i s pat i e n ts t h u s becomes m o re a pp ar ent in
bot h t h e lu m b a r a n d t h e t h o racic region, w i t h t h e
r i b s beco m i n g even m o re prominent o n the con­
vexi ty. There is often l i t tle or no kyphosis in t h e
l owes t t h o ra c i c are a, o r i n t h e l ow l u m bar re g i o n ,
whereas k y ph os i s m a y be exaggerated in the upper
thoracic region .
I nspection from above may reveal rot a t i o n o f the
s h o uld er gird le i n relatio n to the pel v i c girdle a n d
t h e hee l s .
Inspec ti on o f t h e seated patient when relaxed may
s h o w m a r k e d c h a n ges i n posture, p a r t i cul a r l y i n
h y p e r m o b i l e s ubjects, i n w h o m m arked l u m b a r l or­
dosis s ta n d i n g becomes sign ifica n t l u m bar kyphosis
w h e n seate d . T h i s resul ts i n a n i m p O t1a nt c h a nge in
h e a d positi on, which m a y be norm a l w h e n t h e
patient s t a n d s but dra w n forward w h e n h e s i t s i n a
re l a xe d posi t i on. T h i s i s p a r t i c u l a rl y i m po r t a n t In
s u bj ects whose profe s s i o n is mainly s e d e nta ry
.
Pa l pati o n (soft tiss u e l e s i o n s)
P a l p a tion is e ssen t ial, both for d i a g n o si s of p ainful
c han g e s in t h e tis s ues in general and in the
loco m o t o r system in p a r t icular, and also for a ll
m a n i p u l a tive tec h n iques. 1t is t hus l ogical to proce ed
to palpation and soft tissue d i ag n osis a t t h is point.
T h e first step in p a l p a t io n, afte r to u ch i n g the
surface of the pa tie n t s body, is to c o n cen trate on
o u r goal: tes t i n g resistance, m o b i l i ty, shape, te m per
a t u re, moisture and roug h n e ss, or provoki ng pa in.
As palpation is related to touch, a n d to uch receptors
to press ure it is freq u entJ y a ss u m ed that pa l patio n
is pr i m a r i l y t h e registr a t i o n of pressure, and t h a t a
pressu re-registeri n g d e v ice could make p a l pa t i o n
m o r e objecti v e. Un fo r t u n a tely, t h i s i s r a re l y t h e
c a s e , fo r d u r ing palpation our fingers ( hands) d o
n o t exert static pressure, bu t pe rform s u b t l e a n d
j u d i c i o u s move m e n ts. Therefore we engage n o t o n l y
tacti l e but a lso p r o pri oce p ti v e receptors a n d
in t e gra te i n fo rma tio n from b o t h .
T h e b a r ri e r p h e n ome n o n common to mos t soft
t issu e s h a s already bee n discussed (Cha pter 2, p. II);
whether soft t i s s u e is stretched, or s o ft tissue layers
a re sh i fted, we fi rst meet very l i tt l e res ista n ce u nti l
we re a c h a n e a s i l y spru n g b a r r i e r . In h ype ra l ge s i c
zon e s (HAZ) s t r e t c h or mobility i s l i m i ted; t h e
b a rr ie r i s sti f f a n d d oe s no t g i ve .
T h e b a r r i e r p h e n o m e n on ena b l e s us e v e n t o
differen tiate the s u p erficia l from the u n d e r l y ing
tissue l a y e rs by s h ifting one a g a i nst the oth er:
shifting t h e m o s t supe rficia l l a y e r by m i n i m a l force
'
­
,
,
we a t first meet n o resistance until t h e ba rri e r is
reached. At t h i s moment the next underlying t is s ue
layer s t a rts m o v i ng and so on. T h i s is particularly
i m p o r ta n t in movement p a lp a ti on of bon y structures
co v e red by soft tissues: th e soft tissues move first
and bone will not move until we have reached the
b ar ri er (e.g. in sacroili a c m otio n pa l p a ti on )
T h e s i m p l e st w a y to tind a hyperalgesic skin zone
(HAZ) is to r un one's ri ngers very ligh t ly over the
surface of the skin: increased skin drag re ve al s
he i gh tene d fri cti o n due to moister s k in a t the s ite of
an HAZ. This is m o re re a di l y recognized, the lighter
the touch.
For further ex a m i n a t i on of t he superlkial layer of
the s kin it is best to stretch the a re a of increase d
ski n d rag, if s m all between the tinger tips, a larger
area between the thumb a n d the thenar, while a
c onsi d erable patch of skin is b e st ex a m i ne d between
the crossed hands. T h e barrier is reached w it h a
s l i g h t pull ( ta k i n g up the s l ack ), w h ile another slight
tug (witho u t moving a wa y from the barrier) should
s p r i n g it. A symmetrical skin patch on the other s i de
of the body must be stretched in t h e same direction
for compa rison (see F igure 6.72). This technique is
pa rt i cularl y valuable a t the skin fo l d between t oes
and fi ng e rs which is the s i t e of cl inica l l y i m po r t a n t
HAZs in root sy n d r o mes . A n ot he r ( for the patient
more p a i n ful) t e c h ni q ue is to create a skin fold : it is
t h icke r at the s i te of t he HAZ in comparison w ith a
s y mm e tri ca l ly localized normal area.
To examine connective tissue ( i e subcutaneous
tissue, s c a r tissue, muscles w i t h th ei r fas c i a ) it is best
t o fo r m a fo l d (see Fi gure 6.74) and to stretch (not
s q uee ze) i t u nt i l a bar r ie r is reached; t h i s should
spring, but will be stiff if there is an HAZ. If soft
tissue cann o t be fol d e d, m o derate pressure may be
a p plie d ; t h e pressing finger s i n k s into the tissue until
the barrier is engaged. The diagnosis of a n o rma l or
a pa t h o l o gi c al ba r r i e r c a n t h us be made (see Figur e
.
.
.
6.75.).
In d ia gn os in g c h a nge s in the fascia, i t is useful to
tissue r e l ati v e to b o n y
structures: sh i ft i ng the lumbodorsal fasc ia towards
the b uttocks or the shoulders. with the pa t ient
prone; moving the bu ttocks up or down; shifting
( a nd s tre tch i n g) the deep tissue layers on both s i des
of t h e trunk, with t h e patient seated (see Figu re s
6.77-6.79). The sca l p can re ad ily be s h i fted in all
directions a gai n s t t h e skul l , and restrict i v e 'ad h e ­
si ons' noted. The mobility o f soft tissues against bone
can be ex a m in e d at the hee l, by ro t a t o ry moveme n t
a t the n ec k and the extremities, and resistance can
be felt. At pe r i os t a l p ain po ints we regularly tind
shift deep l a y er s of soft
('adhesions') of subperiostal
tissue in one direction, unl ike the other si de fOLlnd
pathological barriers
,
ty pically at spi n o us pro ce sse s e pico nd y les iliac
spines etc.
T h e re are specific disturbances o f mobility where
movement of a d j a c en t bones depe n ds on soft tissue
Copyrighted Material
,
.
Examina/ion
Taut (palpable) bands in muscle
of locom%
r IttnClion
and
ils disflIrbance
87
Local twitch response
Taut
bands
Relaxed
Local
muscle
t==:::=:::==�� of
twitch
fibres
band
A
A
Figure 4.1 Snapping palpation according to Travell and Simons (l983)
resistance; this is particularly the case between the
pointing to the affected root. At the same time we
metacarpal and metatarsal bones. This resistance is
also usually find an HAZ b e twe e n the fingers or toes.
often
increased
in
root
radiates to the toes, and is
syndromes
a
where
A very characteristic soft tissue lesion presents as
pain
valuable diagnostic sign
a
myofascial
Copyrighted Material
trigger
poin t
(TrP);
this
widely
88
Manipulative Therapy in Rehabilitation of the Locomotor Systern
Table 4.1 Important muscular trigger points
Muscle
Clinical significance
Soleus
Pain at the Achilles tendon
Quadriceps femoris, tensor fasciae latae
Pain at the upper edge of
Thigh adductors
Lesion of the hip joint
the patella
Iliacus
Lesion of segment
LS/SI (coccy x)
Piriformis
Lesion of segment
LAI5 (coccyx)
L3/4
Rectus femoris
Lesion of segment
Hamstrings
Lesion of segments LS-Sl. pain at the tuberosity of the ischium
Levator ani (per rectum)
Coccyx
M. coccygeus (Jig. sacrotuberale)
'S'-reflex - pe lvic dysfunction (Silverstolpe) pelvic diaphragm
and fibular
(hip)
head
Psoas and quadratus lumborum
Lesion of thoracolumbar junction (TIO-Ll)
Erector spinae
Lesion of segment at the corresponding level
Rectus abdominis
Tenderness of xiphoid,
Pectoralis major
a bd o m in al viscera
Thoracic viscera, upper ribs
symphysis,
low-back pain at back-
bending,
t he upper thoracic ouLiet
of upper extremity
Pectoralis minor
Tender proc. coracoideus, syndrome of
Middle part of trapezius
Cervicobrachial and radicular syndromes
Subscapularis
Frozen shoulder. scapular pain
Supinator, finger extensors. biceps, brachioradialis
Radial epicondylalgia
Finger flexors
Ulnar epicondylalgia
Triceps brachii
Pain at the dorsal aspect of the axilla
Upper part of trapezius
Any
Sternocleidomastoid
Lesion of segment
Short extensors of the occiput (overlying the
Lesion of the atlanto-occipital. segment
cervical lesion
COil and e2/3, pain referred to skull and face
posterior arch of the atlas)
Masticatory muscles
Digastricus
Temporomandibular Joint, h eadache, facial pain
Pain at the h yoid dys p h agi a
.
acce pted term has been d efined best by Travell and
Simons (1983): A h y per-irritable spot, usually within
a ta u t band of s k e l e t a l muscle or in the m u scle's
fascia, tha t is pa i nful on com pression and can give
rise to ch aracte ristic referred pain, t e n derness a n d
auton o mic phenome n a'. If such a m uscu lar ba nd i s
rolled under the fingers, a l oca l twi tch ca n be felt
a n d can be registe red by EMG, whi l e the patient
fee l s a sha r p pain (Figure 4.1),
The trigger p oint appears to be a band of m u scul ar
tissue which is in a state of contraction while the rest
of the m u scle is quiesce n t; com p l ete relief ca n be
obtained by d econ traction (e,g. by the spray and
st retch method, or by post-isome tric relaxatio n); i.e.
what we have h ere is a reversible cha nge of fu nction,
s i m i l a r to reversible jo i n t moveme nt restriction. In
1993 Hubbard showed that spontaneous EMG
activi t y can be registered in TrPs with the a i d of
monopo l ar e lectrod es.
Myo fascia l TrPs are not the onl y tend er points
(TePs); these ca n be fo u n d a t perioste a l poi nts, on
joints (j oin t ca p s u l e s ) , and at attachment poi nts of
m uscles. I n deed. a muscle with a TrP p rod ucing
te nsio n is u sua l l y con nected with a TeP at the m uscle
a ttachment. Eve n in m uscles there may be tender
poi n ts which a re not taut bands, e.g. in 'tibromyalgia'
w here we can p a l pate a painfu l 'pasty (i,e, dough'
like) hypo tonus'. Such TePs may even prod uce
re ferred pain, but no twitch sign can be elicited nor
does re lax atio n prod uce any re sults .
Eliciting the twitch sign i n a TrP i l l ustrates
another very important fea ture of palpa tion: it
provokes a reaction of the patie n t's tissues, add itional
d i agn ostic informa tio n esta blis h i n g a u n ique feed­
back relationship between two highly com plex se l f­
regula ting systems, examiner and patie nt. which can
be matched by no other instrument. This would
satisfy any criteria of mod ern inform atio n t heory,
if it were reprod ucible and scie ntificaJly verifiable.
We are thus faced with a parad oxical situation: the
clinical method that p rovides the richest and most
diffe re n tiated i n form ation is stigm atized as 'sub­
j ective' a n d the refore n o n-scientific. compared with
sophisticated apparatus which at best is but a poor
copy of the nervous system. w h ereas pal pation uses
the h um a n bra i n itself. and the sensing hands.
Tab le 4.1 lists some importa n t muscle trigger
points.
Reflex c h a nges on the perioste u m - p a i n
p o i nts
There a re n u m erous pain points on the periosteum
in patie nts with disturbed fu nction of the loco motor
Copyrighted Material
Examinalion of 10comOIOr J�lnclion and ilS dislurbance
89
Table 4.2 Important periosteal points
Peri os leal poilll
Clinical significance
Calcaneal spur
Tension in pla n t ar a po n e u rosis
Pes anserinus (tubercle of tibia)
fibular head
Tension in long adductors. hip l es ion
Tension in biceps femoris, block a ge
Upper margin of pa te ll a
Tension in quadriceps or tensor fasciae latae
P oste r ior su p erior iliac spine
Frequent but not speci fi c
Tuberosity of the ischium
Tension in hamstrings
Lateral aspe ct of the p u bi c symphysis
Tension in the adductors. s ac roi liac b l o ck age hip l es i o n
Uppe r margin of the sy m p h y sis
Tension in the rectus abdomi n is
Coccy x
Tension in the gluteus maxim us, levator ani, pi riformis
Iliac crest
Lesion of thoracolumbar junction. tension in q uadra tus and gluteus
medius
Greater trochanter
.
Tension in abductors. hip lesi on
Spinous process (most frequently LS)
Spinous process Th5, 6 (Maigne's 'dorsalgie')
Tension in deep paraspinal muscles
Spinous process of C2
Lesion of segments Cl/2 C2/3. t e nsi o n in levator sca p u Jae
Xiphoid process
Tension in rectus abdominis
On rib s in the mammary and axillary line
At sternocostal ju n ct io n of upper ribs
Tension in pectoralis and serratus atta c h ed here. visceral pain
Angulus costae
Sternum just
be low clavicle
Low cervical lesion, th or acolumbar le sion
Tension in the scaJenus
Movement restrict ion of ribs
Lesion of fi rst rib
Medial end of clavicle
Tension in sternocleidomastoid
Erb's point
Transverse p ro cess of atlas
Lesion of atlas/occiput segment, tension in sternocleidomastoid and
On the oc ci put (Iinae nuchae)
Styloid proc ess of radius
Epicondyles
Upper limb root syndromes. te nsion in the scaJenes
recti capit is lat er aJe s
Referred from the pos t e r ior arch of the a t la s and l a te ral aspect of
spi no us process C2
Lesion at the elbow joint
Lesion of the elbow joints. tension of mus cles attached at
epi con dyJe s
.
Attachment of deltoid
Lesion of scapulohumeral j oin t
Condyle of mandible
Lesion of t empor o ma ndi bu lar joint. tension in mas t i ca tory muscles
Cornua of hyoid bone
Tension of the digastricus. dysphagia
system. Frequently. like trigger points in muscles,
joint which is palpated in the groin, of the acromio­
pain points are highly characteristic of certain lesions
clavicular and sternoclavicular j oints palpated at the
and therefore have high diagnostic value (Table 4.2).
lateral and medial end of the clavicle, and of the
Their disappearance (improvement) also serves as a
temporomandibular joint palpated before the tragus.
valuable test of the efficacy of treatment. Frequently
the tender periosteum is changed on palpation,
offering increased resistance to shift. Many periosteal
Root syndromes
pain points are sites of attachment of tendons or
ligaments
(enthesopathy). and the
tenderness is
I have repeatedly stressed that mere reflex changes
apparently related to increased muscular tension,
in a single segment, including radiating pain, hyper­
e.g. the greater trochanter, fibular head. Achilles
algesia and even dysaesthesia, do not constitute
tendon and attachments. If spinous processes are
sufficient grounds for a diagnosis of root syndrome.
tender on one side. this correlates with the side of
Conclusive evidence of a root lesion is provided
muscle spasm and with restricted rotation to that
by neurological deficit: hypoaesthesia. hypoalgesia.
side.
muscular weakness with hypotonia and/or atrophy,
Where joints can be palpated directly they are
increased idiomuscular excitability and decreased
tender on palpation if there is any lesion. This is true
tendon reflexes. Unless these signs are present we
for the intervertebral joints. which can be particu­
may suspect root lesion but require further proof.
larly well palpated in the cervical region with the
There are two signs. however, which strongly suggest
patient supine; for the rest of the spinal column deep
a root syndrome: pain and/or dysaesthesia radiating
paraspinous palpation is required, with the patient
as far as the toes or fingers. the impression that the
prone. All extremity joints are accessible to palpation.
entire leg is painful and that the bone hurts; and the
and this is very important in affections of the hip
straight leg raising test below 4S degrees.
Copyrighted Material
90
Manipulative Therapy in Rehabilitation of the Locomotor System
(a)
Figure 4.2 The dermatome chart given by Hansen and Schliack
(f):
(1962)
the leg and foot; (f) on the outer aspect
of
the leg;
(g)
at the
perineum
Copyrighted Material
by Keegan (1944)
(d) on the inner and (e) outer
(a-e and g) and
dermatomes on the (a) ventral. (b) dorsal, (c) lateral aspects of the trunk;
aspect of
Examination
Figure 4.2
of 10COnW!iH
(continued)
Copyrighted Material
di.l!urbance
91
92
Manipulative Therapy
in Rehabilitation of the LocanlOtor System
(e)
(e)
(d)
(f)
Figure 4.2 (con li n ued)
Copyrighted Material
Examination oj locomotor junction and its disturbance
93
E xa m i nati o n of m o b i l ity
Only certain g e n e r a l p r i nciples a re d e a l t with here.
should examine a c t i v e m o b i l i t y , p a ssiv e mob i l i t y
a n d move m e n t a gai n s t resis t a n c e . A c t i v e m o b il it y
shows bot h muscula r activ i t y a n d j o i n t m o b i l i ty
u n i n fl u ence d by t h e exa m i ne r . Any force a p p l i e d by
t h e exa m i n e r may be less tha n , equal to or gre a t e r
t h a n t h a t used by t h e p a t i e n t ; we t h e n h a ve c o n ­
We
centric ( resisted) m o v e m e n t , isometr i c resista nce,
or ecc e n t r ic m o v e m e n t . Each t e c h n i q ue e x a m i n es
m u scul a r function ( t h e s t r e n gth of m u scle, reaction
to p a i n provoked i n t h e muscles, e v e n coord i n a tion ) .
Pass i ve move m e n t shows the d egree o f m o b i l i ty
of j o ints a n d m a y at the s a m e t i m e reveal musc u lar
t e n s i o n or s p a s m . E x a m i nation o f a p a r t i c u l a r j o i n t
m a y d i sclose norma l , i nc reased, o r restricted m o b i l ­
i t y . T h i s m a y affect functio n a l m o v e m e nt as wel l a s
j o i n t play (see Chapter 2) . Th e fol l ow i n g c h a nges
s h o u l d be looked fo r d u ring exami nat ion:
Fi g ure 4.2 (con t i n u e d )
The i n d i v i d u a l root s y n d romes are dealt with i n
Chapter 7 . T h e dermatome c h a r t o f H a n s e n a n d
Sch l i ack ( 1 962 ) is rep rod uced here ( Figure 4.2a-e
and g) toget her w i th t h a t of Keegan ( 1 944 ) (F i g u r e
4.2f) for the l eg. I t s h o u l d be poi n t e d o u t t h a t to t h is
day there is no g e n e r a l l y a cce p t e d d e rma to m e chart,
w h ich m a y per h a ps be e x p l ai n ed by the fact t h a t
d e r m at o m e s v a ry from o n e s u bj e c t t o the n e x t . A n
i m po r ta n t poi n t i n t h e H a n se n a n d S c h l i a c k ( 1 9 6 2 )
cha rt is the i r 'cerv icothoracic a nd lum bosacra l h ia t u s ' :
segm e n ts C5-T I a n d L2-S2 d o n o t a p pear o n t h e
tr u n k , b u t o n l y o n t h e extrem ities. O n t h e s c a p u l a r
line on the ba c k t h e re is a 'step' which these a u th o rs
consider to be t h e r e g i o n w h e re the dors a l a n d
v e n t r a l rami m e e t .
I n conclusion, i t can be s a i d that t h e re is a w e a l t h
o f de tecta b l e s i g n s o f re fl e x c h a nges d u e t o p a i nfu l
( n ociceptive) s t i m u l a t ion i n t he s k i n a n d u n d e r l y i n g
t i ss u e s , i n m u s c l e s , pe r i o st e u m , te n d o n s a n d
l igame n ts , a l l o f w hic h ca n be d i agnosed c l i n i ca l l y
and some of which c a n be regi stered ( s k i n
tempe ra t u re . ele ctrical resistance, e tc . ) . These signs
enable us t o m a k e a c l i n ica l d i agnosis a n d to locate
those changes t h a t can be the o b j ec t of s pec ific and
a d e q u a t e t h e ra py .
7,?00
1.
Limi ted range o f movement com pared with the
sym m e t r ical joint o r a neighbo u ri n g s p i n a l motor
segme n t , the ' p a t h o l ogical b a r r i e r ' of A m e r i c a n
os t e o p a t h s ; this h a s been regi s t e re d r e m a r k a b l y
s u cc e s s fu l l y by a de v i c e constructed by Berger
( 1 982 ) , wh i c h i s l i ke l y to prove very i m p o r t a n t
fo r acc u r a t e a n a lysis o f i m pa i red mob i l i t y (see
Fi g u r e 4.32b, c , p. 1 1 2 ) .
2 . R e s i s t a n ce d u r i n g m o t i o n , particu l a r l y d u ring t h e
exa m i n a tion of joint p l a y .
3 . R e s i s t a n ce or s p ri n gi n g i n t h e e n d - posi t i o n . T h e
p a t h o l o gi c a l barr i e r , i f e n ga g e d , d o e s n o t s p r i n g .
H e re i t is e s sent i a l to t a k e up the s l ack of both
functi o n a l move m e n t and j o i n t p l a y . This resist­
a nce in e n d-position has been r e g i s t e red by F i gar
and Kra usova ( 1 975) u s i ng a re s i s t a n c e transducer,
i n a b l ocked ce rvical seg m e n t before tre a t m e n t ,
d u r i n g a h i g h - v e l o c i t y thrust a n d a Eter treatm e n t
( Fi g u re 4 . 3 ) .
A d i agnosis o f move m e n t res tricti on ( b l o c k a g e ) i s
u s u a l l y fol l owed by e x a m i n at i o n for the directi o n o f
Kraft in N (9)
77,3 (7730)
7c,3 (7230)
12,00
O ��AL------���--�-�-(a)
(b)
(c)
Fi g ure 4.3 Record i n g re s is t a n c e i n t h e e n d - po s i t i o n by t h e m e t hod o f Figa r a n d K ra u sova (1 9 7 5 ) . (a) I n c r e a s e d
in t h e block e d seg m e n t . ( b ) The fo rce req u i red fo r thrust m a n i p u l a t i o n i n t h e blocked se g m e n t . (c) E q u a l
res i s t a n c e i n all seg m e n t s a ft e r m a n i p u l a t i o n . A w e i g h t o f 4 0 0 g w a s u s e d a s a g a u ge
re s i sta n c e
Copyrighted Material
94
Manipuiariv(! Therapy in Relwb ilira riol7
Figure 4.4 The
m e c h a n i s m o f l a t e ra l fl e x i o n
of rhe
Lacamaror Sysrem
in t h e
Figure 4.5 Co m p a rison o f t h e l e v e l
o t h e r s y m m e t ri c a l s t r u c t u re s . usi n g
the i l i a c c r e s t s o r
spirit level
of
a
l u m ba r s p i n e
rest r i c t i on ; t h e ra pe u tic tec h n i q ues a re concerned
m a i n l y w i t h m o b i l izati o n i n a specific d i rect i o n . W i t h
move m e n t res t r i c t i o n i n t h e s p i n a l co l u m n , howev e r ,
it is someti m e s o f i n terest to n o te n o t o n ly t h e
d i re c t i o n of restriction but a l so w h i c h o f t h e two
i n te rv e r te b r a l apophyse a l j o i n ts is i n v o l ve d . H o w­
e v e r , t h i s is not a lways easy to d e te r m i n e a n d , i n
f act , m o s t tech n i q u e s a re e ffecti v e i f a p p l i e d i n t h e
correct d i re c t i o n , w h i c h e v e r j o i n t i s a ffected .
The q ue s t i o n o f w h ich s i d e is a ffected is most
r e a d i J y solved in t h e lumbar region by s i m p l e c l i n i cal
e x a m i n a t i o n , beca use h ere axial rota tion is not
po s s i b l e and t h e refore a c o m b i n a t i o n o f restri c t i o n
in t h e sagi t t a l a n d coro n a l p l a n e s s h ows c l e a r l y
w h ich s i d e i s i n volved . It can b e e a s i l y u n d e rstood
that o n a n te fl e x i o n t h e a r t icu l a r s u r faces a re i n e n d ­
to-end position , w h e r e a s i n retrofl e x i o n t h e y a r e
i n fu l l c o n t a c t . D u r i n g s id e - b e n d i ng, h owever, t h e
artic u l a tion o n t h e c o n v e x s i d e i s i n a n e n d - t o - e n d
pos ition as d u r i ng a n te fl e x i o n , w h e re a s t h a t on the
c o n c a ve side i s in fu l l c o n t a c t as d ur i n g re tro fl e x i o n
( F i g u re 4 . 4 ) . T h e re fore, rest ricted retroflex i o n a n d
s i d e - b e nd i n g to o n e s i d e s h o w s t h a t the j oi n t o n t h e
s i d e o f restricted l a te rofl e xion i s a t fa u l t , w h e re a s
restricted a n te fl e x i o n a n d s i d e - b en d i n g i n d icates
t h a t t h e j o i n t o n the s i d e o p p o s i t e to restricted
l a terofl e x i o n i s l es i o n e d .
I n t h e r e s t o f t h e s p i n a l col u m n , i n p a r t i c u l a r i n
t h e cerv ica l region, a comb i n a tion o f la t e r o fl ex i on
a n d a n te - or r e t ro fl e x i o n m a y be h e l p f u l : if l a tero­
fle x i o n i s restricted ( m a i n ly ) in re troflexion i t is t h e
j o i n t o n t h e s i d e to w h i c h we s i d e - b e n d t h a t i s
a ffec t e d ; i f i t i s m o re rest ricted i n a n t e fl e x i o n t h e
j o i n t o n t h e o p p o s i te s i d e is b l ocked .
E x a m i n ati o n of t h e l ower
extrem ities a n d t h e pelvis
is n o n e e d to repeat h e re w h a t f h a v e a l re a d y
s a i d a b o u t t h e gene ra l e x a m i n a t i o n o f p os t u re . f t is
T h e re
i m portant t o a ssess t h e a rch o f t h e fo o t i n both
p l a n e s . To c o m p a re t h e fee t it is useful to pla ce one
fi n ge r under t h e a rc h of each, from the medial
a s p e c t : w h e re t here i s a fl a t foo t , t h e fi n ge r m e e ts
resist a n c e . [t m a y be even m ore revea l i n g to exa m i n e
t h e arch as i t fu n c t i o n s ( i n w a l k i n g ) : from t he m ed i a l
aspec t we c a n s e e w he t h e r t h e a rc h sags (decom pen­
sation of fl a t foo t ) . F o r the fu n c t i o n o f t h e whole
l i m b i t i s v e ry i m p o r t a n t t o note va lgosity o f t he heel
a n d t h e d egree of e x te r n a l rola t i o n o f the foot ( i . e .
of t h e h i p ) .
Exa m i n i ng t h e k n e e , we a r e interested b o t h i n
va rosi t y a nd i n v algosity, a n d i n t h e ge n u rec u rv a t u m .
Flexion i n the h ip j o i n t w h i l e s ta n d i n g i s c h a ract e r­
i s t i c of h i p j o i n t i n v o l v e me n t : i t prese n ts itself,
h o w e v e r , by i n c rea s e d l o rd os i s ( u n l i k e l u m b a g o )
a n d by k n e e fl ex i o n .
For more d e t a i l ed e x a m i n a t i o n o f t h e pe l v i s ,
p a l p a t i o n is n e e d e d . Fi rst t h e i l i ac cres t s s h o u l d
be p a l p a t e d . T h i s i s m o r e d i fficu l t t h a n i s us u a l ly
t ho u g h t : i t m u s t be done from above, fro m t h e r i bs
d o w n - t h e crests ca n be m uch h i g h e r t h a n one
w o u l d e x pect from the s h ape o f t h e b u t toc k s , i . e .
close b e l o w t h e lowest r i b . I f t h e h i p s d ev i a te to o n e
s i d e t h e i l iac crests a l s o dev i a t e , a n d t h e r e fore i t i s
n o t d i ffi c u l t to p a l p a t e t h e crest on t h e s i d e to which
t h e p e lv i s d e v i a t e s , b u t g r e a t e r p r ess ur e is need e d
t o g e t o n t o p o f t h e i l iac crest o n t h e o t h e r s i d e . T h e
i l i a c cre s t t h u s a p pea rs h i g h e r on t he s i d e to w h i c h
t h e p e l v i s s h i fts, u n l e s s g r e a t ca re i s exercised .
To be s u re th a t the i l i a c cre s t s a re at t h e s a m e
h e i g h t i t i s w i s e to c h e c k w i t h a s pi r i t leve l (Figu r e
4 . 5) .
The i l i a c crests s h o u l d be p a l p a ted l a t e r a l l y ( a t t h e
h ighest poi n t ) a n d fo l lowed towa rds b o t h posterior
s u pe r i o r i l i a c s p i n e s , and note t a k e n w h e t h e r the two
p a l p a t i n g h a n d s c o n v e rge. Both t h e p o s t e r i o r a n d
t h e a n t e ri o r i l i a c s p i n e s po i n t d o w n w a rd s a n d s i d e ­
w a y s a n d h a v e therefore t o be p a l pated f ro m be l ow
a n d from t h e s i d e in order to fi n d the correspo n d i n g
poi n ts .
Copyrighted Material
EXl1minarion of /ocomoror /ill1c1ion anri irs disturbance
95
At t h e s a m e tim e w ei g h t dis tri b u t ion c a n be
e x a m ined on t wo sca les ( F i g u r e 4 . 6 ) , w i t h a nd w i t h ­
o u t a heel - p a d o n t h e lower s i d e , t o see w h e t h e r the
p a t i e n t i s b e tter a b le to a s s e s s e q u i l i b r i u m w i t h or
w i t h o u t the p a d . The s u bj e cti v e react ion i s test e d by
as k i n g t h e p a ti e n t w h e t h e r he fee l s h a pp i e r w i t h a
h e e l - p a d , or w he t h e r it m a kes no d i fference. ( J n view
o f static c o r rec t i o n an X- ray c heck is nec e s s a ry : see
pp. 39-43 . )
If w e co nclude t h a t t here i s a d i ffe r e nce i n l e g
le n g t h we a g a i n c h ec k w hether t h i s i s d ue to a s y m ­
m e t ri c a l d e f o r m i ty a t t h e k n e e (va lgosity o r varos i ty )
or to a one-sided fl a t foot, i n w h ich case a n a rc h
s uppo r t is more app r o p r i a te th a n a he e l -p Cl d .
Bes ides o b l i q u i t y , t he p e l v i s m ay be r o ta t e d a s a
w h o le in rela t i o n to the s h o u l d e r g i rdle a nd the fe e t .
I ncl i na t ion (rec l i n a t ion) of the pe l v i s is assessed by
c o m p a r i n g the h e i g h t of the a n te r i o r a n d p o s t e r i o r
u ppe r iliac s p i n e s .
Pe lvic distortio n
Fig u re 4.6 Ex a m i n a t ion of s y m m e t r i c a l s t a nce
scales in fro n t 0 1 a p l u m b - l i n e
a ll
two
I f both i l i a c c r e s t s a re a t t h e s a me h e i g h t - a n d
t h is is a lso t r u e o f t h e a n t e ri o r a n d p o st e r i o r i l i a c
spines - t h e p e l v i s i s h o r i z o n t a l and t h e legs a r e
p ro b a b l y o f e q u a l l e n gt h : i f t h e i l i ac cr e s t i s h ig h e r
on o n e s i d e - a n d the s a m e is t r u e o f both a n terior
a n d pos t e r i o r s u perior i l i ac s p i n e s - and if the A n g e rs
pa l p a t i ng t h e crests t o w a r d s t h e pos ter io r spines
meet, t h e re i s pe l v i c o b l i q u i t y and t h e m o s t p r o b a b l e
re ason i s d i ffe rence i n l eg l e n g t h .
Pelvic o b l i q u ity
Me a s ur e m e n t of leg l e n g t h i s m o re d i fAcu l t th a n
might be t h o u g h t , beca u se t h e fe m o r a l h e a d s a n d
n ec k s a re h i d d e n . Pe l v i c o b l i q u i ty i s t h us t h e m o s t
re l i a b l e c l i n i c a l s i g n of d i f fe r c nce in le g l e n gt h ,
u n l ess t h i s i s c a u s e d by a d i tle re n ce in the l e n g t h
of the le g s below t h e k n e e , a c o n d i t i o n w h i c h ca n
be rea d i l y H ss e s se d , e . g. w i t h t h e pHtient s u p i n e ,
w i t h k n ees fl e xe d . T h e e x a m i nat i o n o f a p a t i e n t
s t a n d i ng, w i t h b o t h l e g s s t r a i g h t , u s u a l l y d e tects
d e v i a t i o n o f the p e l v i s towa rds the h i gher side; in
t y p ica l cases the s h ou l d e r i s l o w e r on t h e side w h e re
the p e l v i s is h i g h e r . The (cl i nica l ) e ffect of a h e e l ­
p a d shou l d t h e n b e t e s ted : i f t h e pe l v i s i s leve l a fter
the heel has been ra ised on t h e l ow e r side, t h e re
s h o u l d be n o s i d e-s h i ft a n d t h e s h o u l ders s h o u l d
h a v e l e v e l l e d o u t . Howe ver, t h i s te s t i s usefu l only
i f there is n o maj or move m e n t r e s t r i c t i o n a nyw h e r e
i n the spine.
T h is is a curious p he n o m e n o n w h i c h m us t be
d i s t i n gu i s he d fro m p e l v ic o b l i q u i t y a nd i s a lways
s e c ond a ry to some othe r lesion which s h ou l d be
fo u n d a nd t re a ted. In the r e a r view t h e pelvi s
devi a tes s l i ghtly to one s i d e ( u s u a l l y to t h e r i g h t )
a n d is s l i gh t ly rot a ted ( u s u a l l y to t h e l e ft) . P a l p a t i n g
of t h e i l i ac c r e s ts s h ows that t h e y a re more or less
o n the s a me leve l l a t e r a l l y , but as the A n g e r s p a l pate
towa rds t h e posterior s u p e r i o r s p i n e s t h e y do not
meet: o n e s u p e r i o r p o s t e r i o r s p i n e (usu a l ly t h e righ t )
l i e s h i g her t h a n t h e o t h e r . T h i s c a n be confi rmed by
d i rect p a l p a t i o n of t he spi ne s . In the fro n t view the
converse i s fou nd : here the r i g h t a n t e r i o r su p e r io r
i l i a c s p i n e is usu a l l y lower a nd t he l e ft h i g h e r . The
two i l i a seem to be d istorted one a g a i ns t t h e o t he r .
Thus t h ere is a l ways a d i sc r ep a n cy i f t h e i l i ac c r e s t s ,
a nd t h e a nt e rior a nd p os te r i o r superior i l i a c sp i n e s ,
are c o m pa re d , b u t re l a t i o n s vary s o m u c h here th a t
t h e differ e nce a t t h e a n terior o r pos terior sp i n es m a y
b e g re a te r o r sm a l le r , a n d t h e crests a cc o rd i ng l y level
o r no t ; confus ion w i t h pelvic o b l iqu i ty c a n e a s i ly
occur ( Figure 4 .7 ) .
F o r t h i s reaso n, i f e x a m i na t io n s h o w s s i g ns o f
p e l v ic ob l i q u i ty w ith some d i s c re p a ncy o n p a l p a t i o n
of t h e most i m port a n t p oin t s on t h e pe l v i s , t h e best
a p p roach is to t r e a t the pe l v ic d i stortion il rst, a n d
t he n to re -exa m i n e fo r pe l v i c o b l i q u i ty ,
A n o t he r fe a t u re of pelvic d i s to rt i o n is i m po r t a n t
because i t po i n ts to d i s t urbance of fu n c t i o n : th e
' o v e r t a k e ' p h e n o m e n on , in whi c h on s ta n d i n g or
s i t tin g t h e l e ft su per i o r poste rior i l i a c s p i n e i s Ll s u a l l y
t h e lower, b u t ov e rt a k es t he r i g h t on s to o p i n g ,
b e c o m i n g t h e more cra n i a l of t h e two fo r a s h o r t
t i m e (less th a n 20 s ) , a fter which t h e t w o spi ne s a re
leve l a nd re t u r n t o a s y m m et r ic a l posi t i o n . If t h er e
is n o overta ke p h e n om e n o n o n s t a n d i ng we s h o u ld
ex a m i n e it w i t h the p a t i e n t s e a t e d o r w i t h both
Copyrighted Material
96
M a n ip u la t i v e Therapy
ill Rehab ilitalion or Ihe LocomolOl" Syslem
figure 4.7 Pe l v i c d i s t o r t i o n i n a c h i l d . N o t e t h e typica l p e l v i c a sy m m e t ry
knees s l i g h l ty b e n t so as to e x c l u d e t h e p u l l o f t h e
h a m stri ngs.
F i g u r e 3 . 1 2 ( see p . 48 ) s hows t h a t the s a c r u m m u s t
l i e a sy m m e t ri c a l l y b e tw e e n t h e i l i a i n s u c h a w a y a s
to c r e a t e m o re t e n s i o n o n t h e s i d e o f t h e l o w e r
p o s t e ri o r s u pe ri o r i li a c spine; as a r e s u l t i t fol lows
the s a c r u m mo re p ro m p t l y in stoopi n g . ca u s i n g t h e
' o v e r ta k e ' . T h e fi g u re s h ow s clea rly t h a t i n t h e
s u p i n e posi t i o n t h e r e i s grea t e r e x t e r n a l r o t a t i o n o f
t h e le g o n t h e s i d e o f t h e l o w e r p o s t e r i o r spin e , a n d
t h ere m a y be w h a t D e r b o l o w s k i ( 1 956) h a s ca l l e d a
' v a ri a b l e d iffe ren c e ' i n l e g l e n g t h - i . e . o n e l e g m a y
be a p p a r e ntly s h o r t e r i n t h e s u p i n e p o s i t i on . whe re ­
as on s i t t i n g t h i s is r e v e rsed .
M ore s i gnific a n tl y , i n t h i s co n d i t i o n th ere i s
u s u a l l y musc u l a r i m b a l a n ce i n t h e p e l v i c re g i o n :
s p a s m of t h e i l i a c u s is freq u e n t on t h e s i d e o f
t h e l o w e r p o s t e r i o r s p i n e a n d t h e fu n c t i o n o f t h e
g l u te a l m u sc u l a t u re is f re q ue n t l y a s y m m etrical.
but m u c h d e p e n ds o n the ca use of the p e l v i c
d i s t o r t i o n , w h i c h , as I h a v e s t resse d , is always
sec o n d a ry .
Copyrighted Material
Exam ination of /ocomolOr function and its disturbance
97
t e m p o r ari l y pos i t i v e o n the s i d e o f the l o w e r PS I S ,
Sacroi l i ac blockage
b u t a ft e r 1 0-20 s t h e d i s t a nce i n c r e a s e s to n o r m a l .
A l t h o u gh t h e re i s n o a c t i v e
m o ve m e n t b e t w e e n
T h e a d v a n tage o f t h is s i g n o v e r t h a t o f t h e ove r t a k e
t h e sacrum a n d the i l i u m , passive m o b i l i t y c a n be
p h e n o m e n o n i s t h a t i t i s p o s i t i v e e v e n if t h e r e i s
ex a m i n e d , as well
s p r i n g i ng. ( G y n a ec o l ogists a r e
b l o c k a ge o n b o t h s i d e s . W e p re fe r t o p a l p a t e t h e
fa mi l i a r w i t h t h e n u ta t i o n m o v e m e n t o f t h e s a c r u m
s p i n o u s p r o c e s s o f LS t o l a n d ma r k s o n t h e s a c r u m
d u r i ng l a b o u r . )
b e c a use i t i s e a s i e r t o fee l .
as
I n a d d i t i o n to the o v e r t a k e p h e n o me n o n , a s i m p l e
sc ree n i n g m e t h o d of d i a g n o s i n g sa croi l i a c b l oc k a ge
d u r i n g s t a n d i n g is by d i re c t p a lp a t i o n w i th t h e
t h u m bs be low a nd m e d i a l to t h e p o s t e r i o r s u p e r i o r
P r o b a b l y t h e si m p l e st scree n i n g m e t h od w i t h t h e
p a ti e n t sta n d i n g h a s rece n t l y been
described
by
R o s i n a ( p e rs on a l co m m u n icati o n , 1 99 6 ) : t h e e xa m i n e r
p l a ces b o t h h a n d s o n t o p of t h e i l ia c c r e s t s a nd t e l l s
i l i a c spi nes ( PS I S ) w h i l e t h e p a t i e n t m a r ks time . I t
t h e p a t i e n t t o r o t a te h i s h e a d a s fa r a s h e c a n t o o n e
is m ore e x a c t , h o w e v e r , t o e x a m i n e t h e ' s p i n e s i g n '
s i d e a n d ( h e n t o the o t h e r . A fter a few seco n d s
(Figure
4 . 8 ) . The e x a m i n e r s i ts be h i nd the s t a n d i n g
l a te n c y the e x a m i n e r fee ls t h a t t h e i l i a c c r e s t i s
patient
p l a c i n g o n e t h u m b on t h e p o s te r i o r i l i a c
.
s p i n e a n d t h e o t h e r o n t h e s p i n o u s p rocess o f S 1 o r
b e t t e r of L S f r o m t h e s i d e o f t h e
joint
we i n t e n d t o
higher
On
t h e s i d e t o w h i c h t h e h e a d r o t a t e s . I f t h e re
is s a c ro i l i a c b l ockl age the i l i ac cres t d o e s n o t mo v e .
Th i s i s n o t o n l y a re l i a b l e t e s t . i t i s v e ry e a s y t o
ex a m i n e . The p a t i e n t i s t h e n t o l d e i t h e r t o r a i s e t h e
p e r fo r m i n cases where p a l pa t i o n o f t h e P S I S a n d
leg o n t h e s i d e w h ere t h e P S I S i s b e i n g p a l p a t e d . o r
even
t o b e n d h e r k n e e a n d l e t t h e h i p d ro p . I n e i t h e r case
i n a c c u r a te . I t i s . however. use less i f h e a d rota t i o n i s
t h e d i sta nce
res t r i c te d . T h e PSIS a n d ASIS a l s o move .
betwee n t h e
PSIS and t h e s p i n o us
of t h e s p i n o u s p rocess c a n
be
d i ffi c u l t o r
movement
A n o t h e r scree n i n g m e thod is to e xa m i n e r e s t r icted
rest r i c t i o n . I n p e l v i c d i s t o r t i o n t h i s s i g n m a y b e
a d d u c t i o n o f t h e t h i g h w i t h t h e h i p flexed to a b o u t
process
i n c re a s e s .
u n less
t h ere
is
,
9 0 degrees. T h e p a t i e n t i s s u p i n e . T h e e x a m i n e r
s t a n d s by t h e t a b l e a n d g r a s ps t h e p a t i e n t ' s f u r t h e r ­
m o s t k n e e , w h i ch is be n t , a n d fl e x e s t h e h i p ; w i t h h i s
other h a n d h e fi x e s t h e a n te r i o r s u p e r i o r i l i a c s p i n e
to
t h e ta b l e ,
fro m a b o v e .
He
then
a d d u c ts
the
p a t i e n t ' s t h igh a c ross t h e p e l v i s a n d c o m p a re s t h e
a n gl e o f a d d u c t i o n o n t h e two s i d e s . I f t h e re i s
n o rm a l m o b i l i t y o f t h e h i p j o i n t , a d d u c t i o n res t r i c t i o n
i s d u e t o a b l oc k ed sacro i l i a c j o i n t . A t t h e s a m e t i me
t h e e xa m i n e r c a n s e n se t h e abse n ce of s p r i n g i n g
w h e n h e r e a c h e s e n d - p o s i ti o n .
T h e s a c ro i l i a c j o i n t c a n be s p r u n g s i m i l a rl y : t h e
patient
i s aga i n s u p i n e
a n d t h e e x a m i n e r aga i n
grasps t h e k n e e a n d a d d u c ts t h e th igh a c r oss t h e
p a ti e n t ' s p e l v i s , b u t w i t h o u t fi x i n g i t wi t h t h e o t h e r
h a n d . I n s t e a d h e conti o u e s a d d uc t i o n u n t i l t h e p e l v i s
begi n s t o rotate , i . e . t h e poste r i o r s p i n e b e g i n s to l i ft
fro m the ta b l e . A t t h i s p o i n t t h e s l a ck is t a k e n u p at
the sacro i l i a c j o i n t a n d the ex a m i ne r pl aces a fi n ge r
o f h i s free h a n d betwe e n t h e poste r i o r s u p e r i o r s p i n e
a n d t h e s a c r u m , s o a s to p a l p a te move m e n t ( s p r i ng­
i n g ) . W i t h o u t i n c reasing a d d u c t i o n he n o w e x e rts
s l i g h t pressure a ga i n s t the p a t i e n t ' s k n ee in t h e
d i rection o f t h e a x is o f t h e t h i g h ( t a k i n g u p t h e s l a c k )
a n d f r o m t h i s p o s i t i o n s p r i n gs t h e j o i n t b y a g e n t l e
p ush i n t h e s a m e d i re c t i o n ( Fig u re 4 . 9 ) . The force
w i t h which t h e sacr o i l i a c j o i n t is s p r u n g i n t h i s
tech n i q u e p r o d u c e s a dorsa l s h i ft o f t h e i l i u m aga i n s t
t h e sacr u m , i . e . a m o v e m e n t m a i n l y i n t h e sagi t t a l
p l a n e . T h i s t e c h n i q u e i s very p o p u l a r b u t d i ffi c u l t
beca use w e h a v e t o e n gage t h e barri e r twice : fi rs t
Figure 4 . 8 T h e ' s p i n e sign ' : c o m p a ri s o n o f t h e d i s t a n c e
between t h e t w o t h u mbs pl aced o n t h e s p i n o u s process
of LS a n d t h e PS I S , r e s pe c t i ve l y . when the p a t i e n t s t a n d s
w i t h b o t h l e gs s t ra i g h t . t h e n w i t h o n e leg b e n t a n d t h e
h i p d ro p p e d
w h e n we t u rn t h e p a ti e n t t o t h e po i n t w h e n t h e PSIS
begi n s t o be l i ft e d . a n d t h e n when a p p l y i ng a x i a l
press u r e o n t h e p a t i e n t ' s k n e e .
T h e re i s a n o t h e r v e r y usefu l m e t h o d fo r s p r i n g i n g
t h e s a c ro i l i a c j o i n t . The p a ti e n t l i es o n h e r s i d e , a n d
Copyrighted Material
98
Manipulative Therapy in Rehabilitation of the L ocomotor System
Figure 4.9
S p r i n g i n g the sacro i l i ac j o i n t : w i t h t h e p a t i e n t
s u p i n e , o n e leg flexed a t the h i p a n d k n e e
a n d add ucted
on the
across t h e p e l v i s , t h e t h e r a p i s t e x e r t s press u re
pat i e n t ' s k n e e
t o stabil ize the pelvis it is best i f t h e lower leg is
extended a n d the upper fl exed, with t h e knee on the
ta ble. The operat or p u ts his forearm (soft muscles)
o b l i q u e l y over the patient's i l i ac crest, so as to
p rod uce gapping between t h e poste rior superior
iliac spine a n d t h e sacr u m . This is achieved by slight
pressure i n a ventromediocran i a l d i recti o n , b u t great
ca re m ust be taken not to rotate t h e pelvis. Gapping
is fe lt with t h e thumb o f t h e other hand, between
the posterior su perior i l iac s p i n e and t h e sacrum
( Figure 4 . 1 0 ) . This techn i q u e t h u s prod uces a
movement o f the i l i u m against the sacrum io the
horizo n t a l p l a ne , and i t is importa n t to point o u t
t h a t i t ca n revea l bl ockage even i f the tech n i q ues
d escribed a bove show normal mobility. R hythmic
repe tition of this m a n oe u vre evokes excell e n t mobil­
ization, a n d i t ca n be used as a high-velocity t h rust
a fter ta k i n g u p t h e s l ack (see p . 179) .
S p r i nging of the sacroiliac j o i n t c a n o n l y be
examined a t the upper or lower end; fre q u e n tl y o n l y
Figure 4. 11
P a l p a t i o n o f m o b i l i t y a t t h e uppe r p a r t o f
the
s a c ro i l i a c j o i n t w i t h t h e p a t i e n t p ro n e
one part o f the j o i n t is blocke d . I f restriction is fou n d
at t h e u pper end t he exa miner p laces his t h u m b o r
fi n g e r on t h e upper end of the s a c r u m , w h i l e the
other hand grasps the a n terior s p i n a ( A S IS) from
below, t h e patient ly i n g pro n e , and l i fts i t
rhythmically i n a vertical d i recti o n . I f t h e re is no
restriction t h i s l i fting move m e n t should ha rdly be
fel t a t all a t t he base of the sacru m . I n blockage,
however, i t is clearly fel t by the p a l pating t h u m b
(Figure 4 . 1 1 ) . A t t he lower e n d o f t h e sacrum t h e
exa m i n e r d i rectly springs the end of the s a c r u m o n
the r i g h t a n d on t h e l eft w i t h h i s t h u m b , from above,
and com p a res the degree of resistance o n e i th e r s i d e .
T h e m ob i l ization tec h n iques shown i n C h a p t e r 6
can be used for d i agn osis.
The re are typica l pain points a t t he upper and
lower e d ge of the sacroi l iac joint on the sacrum
where increased resista nce to spri nging may be fe l t,
a n d a tender a t t achment p o i n t of the add uctors a t
the symphysis. We fi n d a s l ightly posi tive Patrick's
sign w i t h the straight leg raisi n g test, but n o pain is
felt i f the patie n t is s itting u p w i th l egs o u ts tretched '
There is some back-be n d i ng a n d/or stooping restric­
t i o n , and p a i n rad i a tes in the SI dermatome.
Sym p hysea l s h ift
Figure 4.10 Wit h t he p a t ient lying o n h e r si d e the therapist
i l i u m in an o b l i q u e ventromed iocra n i a l
d i rect i o n , w i t h h i s fore a r m , to produce ga p p i n g between
spr ings the
t he pos t e r i o r sacro i l i a c spine a n d the sacru m , w h i c h h e
pa l pa t e s w i t h t h e
t h u m b of t h e o t h e r h a n d
A n o t h e r c l i n ic a l l y importa n t lesion ca n be described
as 'symphysea l s h ift ' , the n a t u re o f w h ich is d i scus­
sed below. O n palpa tion with the patient supine we
fi n d t h a t t he pubic bones close to the sym physis are
not leve l ; i n most cases (83 o u t of 92 examined) the
right was lower than the left. I n a l l these cases there
was also a s h i ft at the isch i a l tuberosity i n the prone
pos i t i o n . In 3 9 cases the t u b e rosity was lower on the
side where the pubic bone was lower; in 53 cases it
was lower on the opposite s i d e . The symp hysis a n d
a djacent parts o f t h e p u b i c b o n e m u s t b e p a l pa ted
from above, t h e fingers p a lpating t h e upper edge of
the symph ysis t h rough t h e a b d o m i n a l wa l l , then
Copyrighted Material
Exan-zinalion of locopnortH
of
m o v i n g from s i d e t o
t h e b o n y s t r u c t u re s .
p a l p a te d from below ,
from
diSlurbance
p os i t i o n , o n e
99
A S I S ro ta te d
w i th t h e
whereas t h e
other is m o r e p r o m ll1 e n t a n ci
i n w a rd s ('in-
t h e gl u te a l l i n e . O n l y a d i ffere nc e of a p p r ox i m a t e l y
fl a re ' ) . H e n ce the t ri a ng l e for m e d b y b o t h A S rS a n d
2 c m is s i g n i fi c a n t .
W he re t h is c h a n ge i s c l i n ic a l l y rel e v a n t we fi n d
t h e n a v e l i s distorted. If t h i s i s n o t m e r e a s y m m e tr y ,
w e fi n d r e l a t i v e hy perto nus a t t h e l ower a b d o m e n
te n d e r n ess a t t h e symphysis with c o rresp o n d i n g TrPs
o n t h e s i d e o f i n fla r e a n d de creased t o n u s o n t b e
in the s t r a i g h t a b d o m i n a l m usc l es a n d h y per t o nus i n
s i d e o f o u t fl a re . ( F o r m o re a b o u t t h i s l e s i o n see
o n e b u t toc k , n o t n ec e ssa ril y accomp a n i ed b y p a i n .
C h a pter 8, p. 257)
,
Com p a r i n g res i s t a nce o f d e e p fas c i a s w h i l e s h i fti ng
e a c h o f the but t o ck s i n a c r a n i a l d i re c t i o n , t h e r e i s
i n c reased r e s i s t a n c e o n the side of t h e h y p er to n us ,
w he re the tuberosi t y
pa l pati o n
sacroi l iac
.
Th i s sh i ft i s p robil b i y
b l o c k age; i t was n o t
'
cases a n d speci fi c treal nlCllt
h a d no effect o n t h e
,
of o ur
The 'S'-reflex ( S ilverstol pe-S ko g l u n d )
S i l ve rstol p e
c l i n i ca l l y freq u e II I
c a l l ' p e l v i c d ysfu nc ti on
thrust ! )
t h ro ug h ou t t h e
that on
s t e p i s t o fin d a
ex a m i n a t i o n i n t h e
could
b e de te c t e d e i t h e r a t I
t uber
-
osities. However, whc
'
section of t h e
exam-
l e ft s i d e where
i n a ti o n , p ro v o k m g
we p r o d u ce
te n d er n ess
of t h e sy m p h y s i s w i t h t r i gg e r p o i n ts a n d h y p e r t o n us
c o n t r a c t i o n o f t he low lumbar p a r t o f t h e e r e c t o r
o f the a b d o m i n a l m us c l e s , t h e pat i e nt s h o w s forw a rd ­
s p i n a e w i t h d o rs i fle x i o n o f t h e p e l vi s . If t hjs i s t h e
d r a w n pos t ure . T h i s c a n be c o r rected b y s pec i fic
c a s e w e usua l l y find a v e r y t e n d e r poi n t i n t h e l a te r a l
,
t h e r a p y . I t i s p r e c i s e l y t h i s forward-drawn p osi t i on
ca used m a i n l y by i ncre a s e d te n s i o n o f t h e a b d o m i n a l
,
m u s c l e s , w h ic h i s the most rele v a n t l e s i o n a n d s h o u l d
be rout i ne l y l oo k e d for .
I
region o f t h e b u t to c k o f t h e s a m e s i d e a t t h e lev e l
o f t h e tip o f t h e cocc y x .
F r o m t hese fi n d i ngs
we
can
that
fo re te l l
at
h and w i t h
p a lpa ti o n of t h e sacro t u bero us l i g a m e n t w e w i l l
fi n d a h ar d a n d e xtreme l y t e n d e r p o int Th i s i s
i n creased t e n s i o n o t t h e m use-I e s o f t h e h a e- k a n d
rea c h e d b y t h e fi n ger a t I'he side o f t h e coccyx
I n t y p ica l c a s e s t h is g o e s hand i n
th is
.
p o i n t i n g i n a c l:t n i a l
i n cre ased te n s i o n
V ery fre que n t l y we a lso
fi n ger fe e ls
t h e l o w e r e x t rem i ty
e re c t o r sp i nae
,
s h a r p p a i n At t h e
.
I
t h e fi b u l a r h e ad w i t h
Origi n a l l y
we
b u t ! ock d i s a p pe a r
e ffect is p ro d u c ed
use d
X - r a y , th e
isc h i a l t u b e ros i t i e s and the symphysi s did n o t cha nge
po sitio n e v e n if at p a l p a t i o n the d i ffere n c e s w e re
,
consi d e ra b l e . W h a t , h ow ev e r , d i d c h a n ge was the
p os i t i o n of our pal p a t i n g fi n ge rs . T h e i m p ort a n t
c o n c l us i o n is t h a t i f we p a l p a te b o n e t h r o u g h s o ft
t i s s u e of u n eq u a l tension we m u st be p r e p a re d for
'palpa/ory { llusion ' , a p h e n o men o n w h i c h is m ost
i m port a n t i n the i l1 terpre ta t i on of fi n d i n gs by p a l ­
p a t i o n ( Fi g u re 4 . 1 2 ).
More about t h i s
It is much mOle
u n de rly i n g m.
d i a phragm
which
by
our
A ten der coccyx
A t e n der coccyx s h o u l d n e v e r b e m issed a t e x a m ­
i n a ti o n o f t h e p e l v i s ; i t i s fa r more fre que n t l y a s ig n
o f l ow - b a c k p a i n t h a n o f coccvgod y n i a (a m u c h l e ss
as simp l e as i t
is a t t h e ve n t ra l
.
reac hed
.
pa i nfu l t e n s i o n t h ro u g h O il I I
coccyx, a n d i t
l i te ra t u r e a l so
lig a m e n t .
fro m t h e
t h e p elvic
p a l p a t i ng fi nge r. (For m o re abo u t t h is s y n d ro m e
s e e C h a p t e r 8, p p 259-260)
common condition
Co rr e ct p a l p a l
the
p art
be
esse nce o f t h i s c h a ng e
toms are very va r ied
.
t h i s s t ri k i n g
It seems u n li k e l y
manoeuvres' for t r e a l
e v e r , w h e n t h e e ffe c t
moment the
b u t not
o f tenderness
t i p of t h e
coccyx t h a t
dow nsl i p or
p res e n ts th is
Figu re 7 . 2).
more difficult by
Innominate shear dysfunction
p o ss i b l e e v e n t o r e a c h t h e t i p of t he coccyx , i n
w h i c h c a s e a n e x t r e m e l y t e n d e r coccyx mu s t be
A cl i n i c a l l y i m po r t a nt c h a nge desc ribed by Gre e nma n
assumed.
'
made even
gl u tei present
may
not
be
(1 986) as i n n o m i n a t e s h e a r d y s fu n c t i o n ' is o c ca s i o n ­
I n a d d i t i o n to t h i s m ost imp or t a n t s i g n there c a n
a l l y fou n d , ma i n l y aft e r a fa l l (t r a u m a) ; i n t h e su p i n e
b e a v i s i b l e h y pe ralges i c z o n e o n t he s a c r u m , l o o k i ng
'
Copyrighted Material
1 00
Manip ula ti ve Therapy in Rehab ilitation of the Locom o t o r System
( a)
( b)
Figure 4.12 Pa l pa t o r y i l l u s i o n : p e l v i c X - r a y s h o w i n g s y m m e t rica l p o s i t i o n o f i s ch i a l t u b eros i t i es
t re a t m e n t . W h a t h a s c h a n ge d i s t ile p os i t i o n o f t h e e x a m i n e r ' s fi n ge rs
l i k e a c u s h i o n o f fa t covered by very s m o o t h ( t a u t )
s k i n ; P a t r i c k ' s s i gn m a y b e s l i g h t l y p o si t i v e on b o t h
s i d e s , a n d t h e s a m e i s t r u e o f t h e s t r a i g h t l e g ra i s i n g
t e s t , as w e l l as of s p a sm of t h e i l i a c u s .
(II) be fore a n d ( iJ )
a ft e r
L i g a m ent p a i n
Close l y re l a t e d to b o t h s a c ro i l i a c les i o n s a n d t o t h e
te n d e r coccyx t h e re i s t h e c o n d i t i o n k n o w n a s
Copyrighted Material
Examination of /OCDI110rOr function an d irs disturbance
'liga m e n t p a i n ' ( H a c ke t t , 1 95 6 ; B a r bor, 1 964) . I t i s
exami ned a n d e l icited b y tec h n iques t h a t a r e t hought
to prod uce tension i n the liga m e n ts. Accord i n g to
Hackett ( 1 956) and B a r bor ( 1 964) three l i gaments
are conce r n e d : these a re the sacroiliac, t h e i l io­
l u m bar and t h e sacrotub e r o u s ligaments. The first
two appear to be of consi d e ra b l e cli nical i mportance.
The fo l lowing te chn ique is used to p rovoke the p a i n .
The p a t i e n t l i e s s u p i n e on t h e t a b l e , a n d the
examiner (standing by t h e table) grasps the further
knee, flexes the patie n t ' s h ip and a d d ucts t h e k nee;
at about 90 degrees o f h i p flexion and add uction the
i l i olumbar l iga m e n t is tested ; if fl e x i o n goes fu rther
(7 0-60 d egrees) the sacroi l i ac l i ga m e n t s are tested.
I f the operator fee l s resistance to i n crease o n furt h e r
add uction he h o l d s t he pressure aga i ns t t he k n e e i n
t h e d i rection o f t h e a x i s o f t h e thig h . th us prod ucing
a ga pping e ffec t a t the site of t h e l iga m e n ts, and
m a i n ta i ns t h i s p ress u re for several second s . I f the
iliolumbar l i ga m e n t is te n d e r , t h e p a t i e n t fee ls p a in
in the gro i n ; i f t h e sacroi l i ac l i ga m e n t is t e n d e r , the
p a i n rad i a tes down t h e leg i n t h e S l d e r m a t o m e
( F i g u r e 4. 1 3) . B e fore testing the l i ga m e n ts t he
exa m i n e r m ust be s u re t h e sacro i l i a c j oi nts a re not
bl ocked in e i t h e r t h e sagi t t a l o r t h e horizo n t a l
planes.
On c l os e r scruti n y , however, i n t h e l a rge m aj o r i t y
of c a s e s w i t h a positive l i ga m e n t tes t, res i s t a nce t o
add uction is i ncreased o n t h e pai n fu l side, so t h a t
th e d i s t a n c e betwee n t h e a d d ucted k n e e a n d the
table i s considerably greate r on the pa i n ful s i d e .
Figure 4 . 1 3 Te s t i n g l i g a m e n t pa i n : t h e l eg i s flexed a t t h e
h i p a n d k n e e : ta k i n g u p the s l a c k i n t o a d d u c t i o n ( a rrow
2) and m a i n t a i n i n g press u re a l o n g t h e axis o f the thigh
( a rrow I ) . the t h e ra p i s t prod u ce s a gapping e ffec t
b e t w e e n the i l i u m a n d t he s a c r u m ( LS ) . p r o d u c i n g
t e n s i o n in t h e s a c ro i l i il c ( i l i o l u m b a r ) l i ga m e n t
[OJ
Obviously, l iga m e n ts c a n not b e t h e sou rce of t h is
increased resis t a n ce and m uscu l a r spasm m u s t be
looked for and trea ted . T h i s type o f p a i n is fo u n d
p a r t i c u l a rl y i n hypermobile p a t i e n ts suffe r i n g fro m
static p a i n .
Ex a m i n at i o n o f t h e l u m b a r s p i n e
Some criteria o f pelvic exa m i n a t i o n , particu l a r l y
w i t h t h e p a t i e n t standing, a r e a l s o va l i d fo r t h e
l u m b a r spi n e . E x a m i na tion of m o b i li t y s ho u ld s t a r t
w i t h a c t i v e move m e n t , a n d I reco m m e n d back­
be n d i ng. He re we a re n o t o n l y concerned with the
total ra nge of move me n t , but can fol l ow i t from the
t h o racol u m b a r region to the sacru m, n o t i n g reg u l a r­
i ty o r loca l hypo- or hypermobi l i ty . N o r m a l l y i t
s h o u l d b e poss i b l e t o fo l l ow the movem e n t down t o
t h e sacru m , a s t h e re is co n s i d e ra b l e mobi l i ty
between L5 a nd S l i n retroflex i o n . If mobi l i ty ceases
a bove S I , there is m ove m e n t restriction in the
seg m e n ts above and e v e n a t the sacro i l i ac j o i n ts . I n
hypermob i l i t y , on t he othe r h a n d , t h e re may be a
s h a r p b e n d at t h e t horaco l u mbar or a t the l u m bo­
sacral j u n c t i o n . T h i s i s a freq u e n t fi n d i ng, a nd of
i mportance; i f back-be n d i n g is n o t res t ricted b u t is
p a i n fu l , t h i s m a y be a s i g n of ten d e r spi n o u s
p rocesses.
When e x a m i n i n g side-bending, care s h o u l d be
t a k e n to see t h a t the p a t i e n t is i n n e i t h e r a forward­
n o r a backwa rd-be n t posi t i o n , t h a t t h e hands a n d
a rms slide sideways dow n the legs, a n d t h a t t h e l egs
a re s t r a i g h t . The patient bends a s fa r sideways as s h e
c a n , a nd we n o te ( 1 ) how fa r d o w n t h e fi n ge rtips
reach; (2) w h e t h e r the sp i n o u s processes a rch
s y mmetrically and regu l a rly to both sides; and (3)
wheth e r t h e re is rotation s y n k inesis: o n s ide-be n d i n g
i t is norm a l fo r the p e l v i s to rotate towards the
convexity of the c u r v a t u re , i.e . to the right w h e n
b e n d i n g to the l e ft. Loss o f t h i s sy n k i nesis is often
the fi rs t sign o f movement restrict i o n i n the l u m b a r
spi n e a n d/or i n the sacroiliac j o i n ts.
O n a nte flexion w i th t b e k n ee s h e l d stra i g h t , w e
n o te h o w close to t h e floor t h e fingertips re a c h , a n d
a t the s a m e t i m e note t h e a rc h o f the l u m b a r s p i n e
a n d t h e p o s i t i o n o f the p e l v i s , f o r i t is import a n t to
d isti nguish w h e t h e r the pelvis is m u c h bent forward
w h i l e the l u m b a r spi n e rema i ns a lmost stra ig h t , o r
w h e t h e r , on t h e contrary, t h e l u m ba r s p i n e a rc hes
fo rwa rd w h i le the pelvis is o n ly s l ig h t l y flexed with
regard to the legs. We then fol l o w the arch o f t h e
spi n e , n o t i n g w h e r e i t is exagge rated a n d w h ere i t i s
fl a t t e n e d . T h e r e i s freq u e n t l y a fl a t te n i ng a t t h e
t h o raco l u m b a r j u nction w h i c h s h o u l d be rega rded a s
physi ologica l, a n d l i t t le o r n o k y p h os i s a t t h e l u m bo­
sacral j u n ct i o n , with exagge rated k y phosis o f the
t h o racic spine ( w h ich i s not co nsi dered n o r m a l ) .
Obse rving t h e patie n t from t h e r e a r w e n o t e w h e t h e r
t h e transverse processes a n d the e rector s p i nae
Copyrighted Material
1 02
Manip u lative Therapy ;n Rehllbililation of the L o comotor System
m usc l e s a r e n o t m o re pro m i n e n t on o n e s i d e t h a n
o n the o t h e r , i n a n t efle x i o n . T h i s is a s i g n o f rotation
usually fo u n d i n sco l i osis. In t h e t h o racic regio n t h e
c o r r e s p o n d i n g p h e n o m e n o n i s p ro m i n en c e o f t h e
a rc h fo r m e d by t h e r i bs. I n a d d i t i o n to r o t a t i o n t here
can a l s o be tru n k d e v i a t i o n t o t h e side w h i c h i s
p a r t i c u l a r l y c h a racteristic i n root synd romes. W e
s h o u l d n o te n o t o n l y h o w fa r t h e fi ngert i p s a re from
the floor, but a l so the opposi t e - a pa t i e n t who c a n
l a y h e r h a n d s fl a t o n t h e floo r w h i l e b e n d i n g fo rward
wi t h knees s t r a i g h t ; hyper m obi l i t y i s as s i gn i fic a n t a s
re s t r i c t e d movem e n t . T h e p ropo r t i on s o f t h e p a t i e n t
- a r m , l e g a n d t r u n k l e ngt h - m u s t of c o u rse be t a k e n
i n to acco u n t .
Fo rwa rd - be n d i ng w h i l e s t a n d i n g m ay be p a i n fu l
a n d y e t n o t restricte d ; one reason i s the pa i n fu l a re '
d e s c r i b e d b y C y r i a x ( 1 97 7 ) . A l m o s t a t t h e begi n n i ng
of fo r ward-ben d i n g t h e p a t i e n t fee l s a s h a r p pa i n ,
a n d a s l i g h t e v a sive re a c t i o n c a n often b e s e e n i n t he
s p i n a l c o l u m n ; fo r w a r d b e n d i n g m a y t h e n p rocee d
w i t h o u t d i fficu l t y b u t o n s t r a ighte n i ng u p p a i n i s
a ga i n fe l t j us t b e fore t h e e r ect pos i t i o n i s reach e d .
Th i s p h e n o m e n o n i s n e v e r s e e n i n a n te fl e x i o n fro m
t h e s u p i n e p o s i t i o n a n d is d u e to con t r a c t i o n of t h e
e re c t o r s p i n a e m uscle o n stooping; i t is a n i m p o r t a n t
s i g n o f t r u e d isc l es i o n . I f, h o w e v e r the p a t i e n t fee ls
p a i n o n l y as s h e s t r a i g h t e n s u p , t h i s is a sign of
a rt i c u l a r b l o c k a ge ; i n s u c h c a s e s b a c k b e n d i n g i s a l so
r e s tricted
I f a n t e fl e x i o n is res t r i c t e d w h i l e s t a n d i n g w i t h
k n e es s traig h t , i t s h o u l d a l w a y s be e x a m i ne d w i t h
t h e p a t i e n t s i t t i n g o n a c h a i e t h is loca l i z e s t h e
m ov e m e n t restriction i n to t h e l u m b a r s p i n e . I f t h e re
is n o s u c h restrict i o n , t h e s t r ai g h t l e g r a i s i n g test i s
use d , w h ic h w i l l s h o w res t r i c t i o n d u e to te n s i o n i n
t h e h a m s t r i ngs
B e fore e x a m i n i n g move m e n t restrict i o n i n i nd i ­
v i d u a l segm e n ts o f t h e l u m b a r s p i n e i t is a d v i sa b l e
to e x a m i n e t e n s ion ( trigger p o i n t s ) i n certa i n musc l e s
co r res p o n d i n g to t h o s e s e g m e n t s . Th i s h a s a l re a d y
been d e il l t w i t h (see T a b l e 4 . 1 ) .
.
'
-
,
,
Figure 4.14 E x a m i n a t i o n of s p r i n g i n g of t he l u m b a r a n u
t h o r a c i c s p i n e . us i n g h e e l of t il e h a n c1 coll t a c t w i t h t he
a r m o u ts t re t c h e d
,
-
.
.
p rocess, i . e . o n t he tra n s v e rs e p rocesses o r o n e
v e rte b r a ; t h e h y p o t h e n a r o f t h e e x t e n d e d ot h e r a r m
i s the n p l ac e d across t hese fi nger t i p s , s p r i ng i n g t h e
v e r tebra a fte r ta k i n g u p t h e s l a c k i n t h e s a m e w a y
a s befo r e , aga i n t a k i n g ca r e t o a v o i d i r r i t a t i n g t h e
spi n o u s processes ( Figure 4. 1 5 ) .
I f i n cre a sed resista nce ca n b e fe l t a n d t h e pa t i e n t
fee l s p a i n , t h i s i s p ro b a b l y d u e t o a rt i c u l a r b l ockage .
I f, h o w e v e r , there is n o i nc r e a s e d resistance a n d y e t
t h e p a t i e n t fee l s pa i n , t h ere i s l i k e l y to b e a d i sc
lesi o n . T h e s p r i n g i n g tes t , howe v e r , ca n n o t l oca l ize
m o v e m e n t res tr ic t i o n o r h y p e r m ob i l i ty in a singl e
m otor segm ent p r eci s e l y To a c h i e v e t h is , s pe c i 6 c
m o b i l i ty t e s t s m u s t b e used .
.
To test re tro flexion (extension)
Exa m i nation of i n divid u a l seg m e nts i n
the l umbar spine
Te n d e rn ess is fi rst e x a m i n e d by p a l p il t i n g t h e
s p i n o u s p rocesses w i t h t h e fi n ge r ti p s ; te n d e rn e ss i s
u s u a l l y not q u i te s y m m e trica l , b u t m o r e p r o n o u nced
o n o n e side or t h e o t h e r Then the s p r i n g i n g test i s
a p p l i e d : th i s e x a m i n e s both res i s t a n c e a n d te n d e r­
n e s s o f d e e p s t r u c t u re s ( m a i n l y t h e d i scs a n d apo­
p h y s e a l j o i n t s) a n d a v o i d s i rr i ta t i o n of the s p i n o us
proce s s e s The t h e n a r e m i n e nce of one h a n d is
p l a ced o n one transverse p r oce ss and the hypot h e n a r
on t h e o t h e r ; v e r y s l ight p ressure is exerted by t h e
e x t e n d e d a r m t o t a k e u p t h e s l a c k , a n d t h e n to s p r i n g
the v e r t e b r a by a s l i g h t ex t r a p u s h ( F i g u r e 4 . 1 4) .
A n o th e r m e t h o d i s to u s e t w o fi ngerti ps o f one
h a n d , p l a c i n g o n e on e i th e r s i d e of the s p i n o u s
.
.
T h e p a t i e n t lies o n her side w i t h both h i ps and k nees
fle x e d . T h e h i p should b e I-l e x e d t o a b o u t 1 00 deg­
rees. The e x a m i n e r l e a n s a ga i n s t t h e p a t i e n t ' s k n e e s
w i t h h i s t h i g h s fi x i ng t h e s p i n o u s p rocess o f t h e
u p p e r v e r t e b r a 0 1' t h e e x a m i n e d se gm e n t w i t h o n e
fi nge r, rei n fo r ced by t h e fi n gers o r t h e o t h e r h a n d
p lac ed over i t . He n o w e x e r t s s l i g h t p r e s s u r e aga i n st
the p a t i e n t s knees in the p r e s u m e d d i re c t i o n o f t h e
i n te rv e r tebra l disc o f t h a t se g m e n t so as t o ta ke u p
t h e s l a c k , il n d t h e n s p ri n gs t h e segm e n t b y a s l i g h t
a d d i t i o n a l p u s h w i t h h i s t h i g h s : h e fee l s a s l i g h t s h i ft
of t h e p e l v i s a n d t h e l owe r v e r t e b r a a g a i n s t t h e o n e
t h a t is fi x e d . I n c a s e s o f b l ock a ge n o m o v e m e n t i s
fe l t i f th e sla c k h a s b e e n p r o p e r l y t a k e n u p . I f n o r m a l
s p r i n g i ng i s fe l t , d o r s i fl e x i o n til kes pl a ce be t w e e n
t w o a d j a ce n t v e rt e b rae as can be see n i n a n i m age
Copyrighted Material
,
'
,
Examination of locomotor .lill1etion and its disturbance
1 03
Figure 4.16 Te s t i n g r e t ro A e x i o n i n o n e l u m b a r segme n t :
t h e pa t i e n t l i es on h e r s i d e , the t h e r a p ist exert i n g
springing p ressLl re o n b o t h k n ees a n d fi x i n g t h e u p p e r
s pi n o us process w i t h b o t h h a nd s .
i n t e n s i fi e r. I f t h ere i s h y p e r m o b i l i t y t h e r e m a y b e
s o m e a d d i t i o n a l s h ift
( Fi g u re 4 . 1 6 ) ,
R e t ro fl e x i o n c a n a l so b e e x a m i n e d b y g r a s p i n g
b o t h t h e p a t i e n t s fe e t a b o v e the h e e l s w i t h o n e
'
h a n d , The p a t i e n t l i e s o n h e r s i d e w i t h s l i g h t l y be n t
k n ees a n d h i ps a n d t h e ex a m i n e r p u ts o n e fi nger o f
h i s o th e r
h a n d be twe e n t h e s p i n o us proce sses o f t h e
m o t o r segm e n t
he
i n te n d s
to
examine.
In
this
posi t i o n t he exa m i n e r s h i fts b o t h legs horizon t a l l y
i n a d o r s a l d i re c t i o n p r o d u c i n g re tro fl e x i o n of t h e
l u m b a r s p i n e , W i t h t h e fi n ge r o f t h e h a n d p a l pa t i n g
t h e s p i n o u s p rocesses h e
feels t h a t t h e adjace n t
s p i n o u s processes a p p ro a c h o n e anothe r . W h e n t h e
u p h e s p r i ngs t h e segm e n t i n t o
t h e re i s m o v e m e n t r e s t r i c t i o n
res i s t a n c e i s i n c re a s e d a n cl t h e seg m e n t d o e s n o t
s p r i n g ( F i gu r e 4 . 1 7 ) .
slack
is
ta ken
re t r o fl e x i o n .
If
Exam i n a tion of an te flexio n
T h e p a t i e n t aga i n l ie s on h e r s i d e w i th fl e x e d h i p s
a n d k n e e s . With o n e e l b ow t h e e x a m i n e r fixes t h e
u p p e r t h o r a c i c r e gio n w h i l e p us h i n g b o t h
fl e x e d
k n ees a ga i n s t t h e p a t i e n t ' s a b d o m e n , u s i n g h i s be l l y
and
t h i g h s ; t h i s p r od uc e s m a x i m u m
a n te fl e x i o n .
W i t h t h e i n d ex fi n g e r o f t h e h a n d fi xi n g t h e u p p e r
t h o r a ci c s p i n e he p a l p a t e s b e t w e e n t h e two s p i n o u s
p rocesses of t h e m o t o r segme n t , s e n s i n g mov e m e n t
( se p a r a t i o n o f t h e s p i n o u s p r o c e sses) a n d t e n s i o n ( a t
Figure 4.15 E x a m i n a t i o n of springing (as in Figure 4. ( 4 ) .
( a ) T o a v o i d p re s s u r e o n t h e s p i n o Ll s process, t w o fi nge rs
of t h e h a n d com i n g fr o m b e l ow a re p l aced on t h e
t r a n s ve rse p rocesses o n e i t h e r s i d e . ( b ) O n t h e s ke l e ton .
(c) W i t h the u l na r e d ge o f t h e e x t e n ci e d a r m over b o t h
fi n g e r t i p s o n t h e t r a n s ve rse p rocesses, t h e t h e r a p ist
s p r i ngs a l u m b a r ( t h o r il c i c ) v e r t e b ra
m a x i m u m fl e x i o n ) . W i t h h i s o t h e r h a n d over t h e
p a t i e n t s b u t t o c k s h e re i n forces flex i o n o f t h e h i ps
'
( this
h a n d m a y a l so be used fo r p a l p a t i o n i f t h e
p a t i e n t i s v e ry t a l l a n d the o p e r a t o r c a n n o t reach t h e
rele v a n t segment w i th t h e upper h a n d ) . The most
i m porta n t tech n i ca l d e t a i l i n t h i s m a n oe u vre i s t h e
fi x a t i o n o f t h e u p p e r t h o r a c i c s p i n e w i t h t h e e l b ow
Copyrighted Material
1 04
Man ip ulative
Figure 4.17
Therapy in Rehabililalion of Ihe Locomotor
E x a m i n a t i o n of l u m b a r
Syslem
s p i n e retro fl ex i o n by
m o v i n g b o t h legs i n a dorsa l d i r e c t i o n
Fi g ure 4.19
L a t e r o li e x i o n o f
the l umbar spine
the l u mbar s p i n e . Wit h the fi n gers of t h e other hand
he se nses move m e n t a n d , fi n a l ly, res i s t a n ce ( Figure
4 . 1 9) .
Fi g ure 4.18 Te s t i n g a n te fl e x i o n in o n e l u m b a r segm e n t :
t h e p a t i e n t l ie s o n h e r s i d e , t h e t h e r a p i s t p u s h i n g t h e
p a t i e n t ' s k n e e s a ga i n s t t h e c h e s t , e x e rt ing c o u n t e r­
press u r e w i t h h i s e l b o w . The h a n d on t h e p a t i e n t ' s
b u t tock i n c re a s e s a n te fl e x i o n o f t h e p e l v i s , w h i l e t h e
fo re fi nger o f t h e o t h e r h a n d pa l p a te s m ov e m e n t
( t e n s i o n ) b e tw e e n t h e s p i no u s processes
w h i le the k nee i s p u s h e d towa rds the a b d o m e n , i . e .
i n t h e d i rection o f the e l b o w ( Figure 4 . 1 8) .
Exam in a tion o f side-be n ding
The patient is in the s a m e posi t i o n as in t h e last
sect i o n b u t the lower leg is b e n t a t right a ngles to
the hip, the knee protrud i n g s l i g h t l y over the edge
o f the table; the upper leg is flexed even m ore so
t ha t the foo t lies be h i n d the thigh o f the lower leg.
The operator stands by the t a b l e , facing t he patient,
a n d grasps the hee l o f the lower l e g w i th one h a n d .
W i t h t h e other h a n d he fixes the p a t i e n t ' s fl a n k ,
t h e h e e l o f t h e h a n d crea t i n g a fulcrum a t t h e l e v e l
o f the motor segm e n t be i ng e x a m i n e d , w h i l e he
pa l p a tes between t h e s p i nous processes with one
fi nger, from above. The h a nd hold i n g the patient's
h e e l l i fts the lower leg, prod u c i n g l a t e ro flexion o f
Exa m i n atio n o f t h e t h o racic spi ne
and t h e r i bs
Active m o b i l i t y is first e x a m i n e d , w i t h the patient
seated astr i d e t h e t a b l e a n d p e r forming a n te- a n d
re tro fl e x i o n , side-be n d i ng a n d rotation . I n rotation
symme trica l move m e n t ca n be assessed by sight by
traci n g the l i n e formed by the spinous processes,
especially i n a slightly kyphotic position , a n d by not­
i n g the a ngle formed between the patient's shou lders
a n d the table.
As i n the l u m bar spine, t h e s pi nous processes a re
palpated for te nderness; t h i s is b e st done in a kyph­
otic p osition ( Figure 4.20). Spri n gi n g is performed
by the same tech n i q u e as t h a t d escribed fo r the
l u mb a r s p i n e .
Fo r the e x a m i n a t i o n o f passive move m e n t the
p a t i e n t sits o n t h e t a b l e with hands c l asped b e h i n d
her bead a n d t h e e l bows b rough t toge t h e r i n fron t
of t h e face . T o t e s t bac k-bend i n g t h e exami ner
stands by t h e side of t h e p a t i e n t , grasping both
e l bows from below, so a s to extend her t r u n k a n d
p a l p a te w i t h one finger o f the o t h e r h a n d between
t h e spi nous processes of the segme n t b e i ng ex a m i ned ,
sensi ng move m e n t a n d t h e n resista nce i n t h e e n d ­
pos i t i o n ( Figure 4 . 2 1 ) .
Copyrighted Material
Examination oj locomotor jun ction and its distu rbance
1 05
Figure 4.21 E x a m i n a t i o n of retrofl e x i o n of t h e t h o racic
spine
Fi gu r e 4.20 (a) Palpating t e n de rn e ss
of the tip o f t h e
the t h o r a c i c s p i n e , s e p a rated b y
a n t e fl e x i o n . ( b ) S k e l e t a l d i agra m
s p i n o u s processes of
To e xa m i n e
forwa rd-be n d i n g th e o p e r a tor grasps
t h e p a tie n t ' s e l b ows from above i n o r d e r to a n te flex
the t r u n k , a ga i n pa l p a t i n g b e t we e n
the s p i n ou s
processes w i t h o n e fi n g e r o f t h e o t h e r h a n d , fo r
m o v e m e n t a n d for t e n s i o n i n t h e e n d - p os i t i o n . I n
both t h e s e ex a m i n a t i o n s i t i s i m p o r t a n t t o m o v e t h e
patie n t so
as t o p r o v i d e m a x i m u m a n te- o r retro­
Figure 4.22 Exa m i n a t ion o f a n te fl e x i o n o f t h e t h o r a c i c
spine
fl e x i o n a t the s i te o f p a l pa t i o n ( Fig u r e 4 . 2 2 ) . I t i s
a lso po s s i b l e t o e x a m i n e
a n t e - a n d retrofle x i o n i n a
l y i n g on h e r s i d e ; t h i s
s i m i l a r way w i t h t h e patient
w i t h t h e l a t te r h a n d w h i l e h is o t h e r fo r m s
po s i t i o n i s u s e d f o r m o b i l iza t i o n in to r e t r o fle x i o n
a ga i n s t t h e r i b s , t he th u m b p a l p a ting t h e m o v e m e n t
( s e e Figure 6 . 3 5 , p .
o f t h e s p i n o u s processes a n d re s i s t a nce i n t h e e n d ­
p os i ti o n . T h e b e n d i n g m o v e m e n t m a y be p e r fo r m e d
a t t h e l e v e l of t h e p a t i e n t ' s s h o u l d e r ; if t h e u p p er
t h o ra c i c s p i n e i s b e i n g ex a m i n e d, t h i s h a n d may be
1 8] ).
To ex a m i n e s i d e - be n d i n g t h e o p e r a t o r s t a n d s
b e h i n d t h e p a t i e n t w i th o n e h a n d ro u n d t h e p a t i e n t ' s
r i b s a t t h e l e v e l of t h e s e gm e n t bei n g e x a m i n e d , t h e
t h u m b ag a i n s t t h e i n terspace b e twee n t h e s p i n o u s
processes o f t h e s e gm e n t a n d t h e o t h e r h a n d a ga i ns t
t h e p a t i e n t ' s s h o u l d e r . He s i d e- b e n d s t h e p a t i e n t
a fulcrum
a ga i n s t t h e p a t i e n t 's n e c k ; d u ri n g e x a m i n a t i o n o f t h e
t h oraco l u m bar s p i n e i t m a y be b e l ow the s h o u l d e r .
T h e o t h e r h a n d m u s t a l w a y s s t a b i l i ze t h e c h est fro m
Copyrighted Material
JIi/anipuia t i v e Therapy
1 06
in
Reh a b ilitation
of the L ocomotor System
figme 4.23 E x am i n a t i o n of l a t e r a l flexion of t h e thoracic
sp i n e , s ta n d i n g b e hi n d t h e p a t i e n t
c r e a t i n g a s o l i d fulcr u m , eve n i f t h e
a p pears to be fa r from t h e s pi n o u s
p ro c e ss es when the patient is e re c t . D u ri n g s ide­
b e n d i n g the t hu m b u s u a l ly reaches t h e s pi n o u s
processes, ow i n g to r o t a t i o n c o u p l e d w i t h s i de­
b e n d i n g (F i g u re 4.23 ) .
I f, h o w e v e r t h e p a t ie n t has a very b r o a d b a c k a n d
t h e exa m in e r has a v e ry s m a l l h a n d the fo l l o w i n g
tech n i q u e is more a p p ro p ri a te : t h e e x a m i n e r s t a n d s
a t t h e p a t i e n t s s i d e sl i g h t l y b eh i n d h e r , a n d grasps
the fu rth e r e l b ow rais i n g i t a bove h e r head . T h e
e x a m i n e r places h i s t h e n a r e m i n e n c e with t h e t h u m b
p a ra l l e l to the s p i n o us p ro c e s s e s o n t h e s i d e t o w h ic h
s i d e b e n d i n g is b e i n g e x a m i n e d . W i t h t h e t i p o f h i s
t h u m b h e fi x e s t he s p i n o u s process of t h e l ow e r
v e r t e b r a of t h e m o t o r s e g me n t . He now p ro d u ces
la tero flexion o f the tru n k by p ulling the p a t i e n t s
e lbow tow a rd s h i m s e l f, t h e the n a r a n d the th u m b
c r e a t i n g a fu lcrum loca l izing l a t e r ofl e x i on t o t he t i p
of t h e t h u m b (Figu re 4 . 24) .
To e x a m i n e rota t i o n t h e o p e r a t o r s i ts the p a t i e n t
a s t ri d e t h e t a b l e a n d g r a s p s o n e s h o ulder, p a s s i n g
h i s fore a rm u n d e r h e r a x i l l a o n t h e o t he r s i d e . He
fi rs t c a rri e s o u t ma x i m u m rota t i o n to o n e s id e ,
r e pe a t i n g t h e m a n o e u vre o n t h e o t h e r s i d e to
c o m p a re t h e two . For e x a m i n a t i on o f i n d i v i d ua l seg­
m e n ts a s l i gh t l y k y p h o ti c p o s i t i o n i s reco m m e n d e d ,
m a k i n g t h e s pino u s p rocesses m o re accessible b o t h
t o i n s pe c t i o n a n d t o p a l p a t i o n . I f t h e r e i s move m e n t
r e st r ic t i o n t h e b l oc k e d segment i s o ft e n v i s ib l e : t here
is very l i t t l e r o t a t i o n i f we fo l lo w fro m t h e l u m b a r
s p i n e i n t o t h e th or a c i c u p to the b l o c k e d segment,
w h e r e a s t h e re i s hypermob i l i ty above i t so t h a t the
l i n e of t he s p i n o us p r oc e ss e s a n g u l a te s O n the s ide
w h e re rotation is free we see the u n b r o k e n l i n e o f
the s p i n o u s p r oce s s e s fro m t h e l u m b a r u p to the
t h o ra c i c r e g i o n . Pa l pa ting the s p i n o u s p rocesses o f
the si d e
,
palpating thu mb
Figure 4.24 E x a m i nation o f l a tera l flex i on o f t h e t h o racic
sp i n e , s t a n d i ng a t the side o f the p a t i e n t
,
'
,
-
'
,
.
Figure 4.25 Exa m i n a t ion o f r o t a t i o n o f t h e t h o racic spi ne
the
segm e n t w i t h t w o fi n g e rs we fe e l
mobil ity, w h e re as o n t h e n o r ma l side
ro t a t i o n w i l l be felt fi r s t a t t h e u p p e r a n d a l i t t l e later
a t the l ow e r sp i n o u s p rocess ( Figure 4.25 ) . I t is most
i m p o r ta n t for the e x a m i n e r to ro t a t e the p a ti e n t
exact l y r o u n d h e r b o d y a x i s , a n d t o p a l p a t e w i th
r e l axed fingers w h i ch c a n fo llow t h e m o v e m e n t of
b lo c k e d
no re l a t i v e
Copyrighted Material
,
Examination of locom otor fUlI ction and i t s dis/I.Irban ce
1 07
the s p i n o u s p rocesse s . T h i s is n o t e a s y , a nd it is
there fo re a grea t a d v a n tage t o form a d i a g n o s i s b y
i n spec t i on; t h i s i s u s u a l l y poss i b l e i n k y p h o s i s u n less
t h e pa t i e n t is too obese . Rota t i o n r e s t r i c t i o n is m o s t
s i g n i fi c a n t in t h e l o w e s t t h o racic s p i n e a n d a t the
t h oraco l u m b a r j u n c t i on, and l e s s s o i n t h e m i d d l e or
upper t h o ra c i c regi o n s . (Rece n t i nvestig a t i o n s have
shown t h a t w h a t w e see and p a l p a te i n this case
conce r n s i n t h e fi rs t p l ace the s p i n o u s processes a n d
n o t necess a r i l y t h e e n t i re m o t o r segm e n t ; s e e p . 5 4
Figure 3 . 1 8 . )
M o b i l i ty o f t h e t h o r a c i c s p i n e c a n b e e x a m i n ed
w i t h t h e p a t i e n t pro n e , b r e a t h i n g s l o w l y i n and o u t :
n o t o n l y c a n w e s e e h o w t h e w h o l e of t h e t h o ra x
l i fts b u t t h e s p i n o u s p rocesses c a n b e see n s pre a d i n g
l i k e a fa n . This fa n - l i k e move m e n t c a n be fo l l owed
from t h e l u m b a r s p i n e u p to the ce rvico t h o racic
j u nc t i o n . T o a c h i e v e t h is we reco m m e n d i n s t r u ct i n g
t h e p a t i e n t fi rst t o b r e a t h e i n to h i s a b d o m e n ( l u m b a r
spine) a n d t h e n i n to h i s c h est, a n d as fa r u p a s h e
ca n . A s a
rule,
a t the
poi n t w b e re t h e re i s a n
i n te r r u p t i o n t h e re i s b l ock a g e ; a f t e r t re a t me n t w e
see t h e n o rm a l m o b i l i ty restored d u r i n g b re a t h i n g .
T h e exce p t i o n t o t h i s r u l e i s p a t i e nts w i t h a fau lty
resp i ra t i o n tec h n i q u e w h o a re u n a b l e to b r e a t h e i n to
t h e posterior w a l l of t h e t h o r a x e v e n w h e n pro n e .
Ribs
We n o w p roceed to examine t h e t h o r a x , p a r ti c u l a r l y
t h e ri b s . For scree n i n g i t i s usefu l t o move t h e fla t
h a n d s o v e r the r i b c a ge , n o t i n g a n y a sy m m e t ry , a n d
particula rly w h e t h e r a n y ri b i s p ro m i n e n t . J u s t a s we
Figure 4.26 P a l pa t i o n of resi sta nce at the (upper) ribs a t
retro A e x ion o f the t h o r a x . accord i ng t o K u b i s ( person a l
com m u nication)
pa l p a te t h e s p i n o u s p rocess fo r te n d e r n e s s , so we
p a l p a te the most p r o m i n e n t part o f t h e rib, the c o s t a l
a n g l e ; i n t h e region 0 1' t he u p p e r r i b s we h a v e first
to a b d uct the s h o u l d e r - b l a d e , by m o v i n g t h e e l b ow
th a t o n t h e o t h e r s i d e , i . e . i t h a s ' o ve r t a k e n ' t h e o t h e r
tow a rd s t h e s h o u l d e r of t he opposite s i d e .
r i b . The s i d e o f lesser m o b i l i ty i s u s u a l l y t h e s i d e o f
In t heory , a
rib can
be
b l oc k e d
both
in
the
m o b i l i ty r e s trictio n .
E . K u b i s ( u n p u b l is h e d o b s e rv a t i o n s ) h a s d e s c r i b e d
e x p i ra t o r y a n d the i n s p i r a tory posi t io n ; from t h i s i t
fo llows t h a t i t i s m o re
pro m i n e n t i f b l ocked
in
t h e b e s t m e t h o d o f d i a g n o s i n g blockage by i n c r e a s e d
i n h a l a t i o n , a n d l e s s s o i f b l o c k e d i n e x h a l a t i o n . Aga i n
re sista nce t o ( p a s s i v e ) m o b i l i ty d u ri n g back-be n d i ng :
i t i s w i s e r t o rely o n exa m i n a t i o n a n d com p a ri s o n of
t h e p a t i e n t s i t s o n t h e edge o f the t a b l e w i th t h e
m o bi l i ty ra t h e r t h a n on posi tio n ; t h i s m e a n s t h a t
h a n d o f t h e s i d e to be e x a m i n e d b e h i n d h e r h e a d ,
w e e x a m in e r i b m o ve m e n t o n b o t h s i d e s d u r i n g
so
b re a t h i n g i n a n d o u t , e x a m i n i n g b o t h by i n s pec t i o n
s t a n d s o n the o t h e r sid e , g r a s p i n g t h e e l b o w from i n
tha t
the e l b o w p o i n t s u p w a rd s . T h e e x a m i n e r
a n d palp a ti o n . It i s part icularly usefu l to i n s i s t o n
fro n t a n d prov o k i n g b a c k - be n d i ng . W i t h t h e fi n ge rs
d e e p in h a l a t i o n a n d ex h a l a t i o n : i n t h e fo rmer, t h e
o f t h e o t h e r h a n d at t h e costa l a ng l e of t h e r i b u n de r
restricted s i d e w i ll s t o p b re a t h i n g i n s o o n e r t h a n t h e
e x a m i n a t i o n h e crea tes a f u l c r u m a n d se n s es re s i s t ­
h e a l t h y s i d e ; d u r i n g e x h a l a t i o n t h e s a m e w i l l h a p pe n .
a nce to b a c k - be n d i n g, resis t a n c e t h a t i n cre a s e s i f
I t i s c l e a r l y recog n iz a b l e t h a t m o ve m e n t c o n ti n ues
t h e re i s b l o c k a ge ( F i g u r e 4 . 2 6 ) .
on one side but i s a rr e s t e d o n t h e o t h e r. A p a r t i c u ­
I t is i m porta n t t h a t t h e fi ngers fi x i n g t h e r i b s h o u l d
l a rl y s t r i k i n g phe n o m e n o n is t h e ' overt a k e ' p h e n o ­
b e l e v e l o n t h e cos t a l a n gl e ; c u ri o u s l y e n o u g h , t h e
m e n o n , fo u n d c h a racte r i s t ica l l y i n t h e regi o n of t h e
s h o u ld e r - b l a de i s n o o b s t a c l e to effe c t i ve p a l p a t i o n .
upper r i b s : p a l pa t i o n a p p r o x i ma tely i n t h e n i p p le
Resistance is
l i n e , or e v e n c l o s e r to the ste r n u m , ofte n s h o w s t h a t
b l ockage o f t h e seco nd t o fifth r i bs , i . e . t h e r eg i o n
t h e ribs a re n o t q u i te on t h e same l e v e l o n t h e two
w h e r e r i b b l ockage occurs m o s t freq u e n t l y . Care
t he p a t ient i s asked t o t a k e a deep brea t h ,
s ho u l d be taken t h a t o n ly b a c k - b e n ding t a k e s p l ace
sides.
If
t h e r i b t h a t stood lower w i ll u s u a l l y be h i g h e r t h a n
fel t t h ro u g h t h e s h o u l d e r- b l a d e
and no r o t a t i o n of t h e p a t i e n t ' s trunk.
Copyrighted Material
in
1 08
Man ip u lati v e Th erapy in Rehabilitation of
th e Locomotor System
( a)
Figure 4.27 E xa m i n a t i o n of a b l o c k e d first ri b b y fo rw a rd
of t h e head ro t a t e d to t h e o p p os i t e s i d e
be n d i n g
(
E xa m i n ation of the fi rst rib
I n d e ra n ge m e n t of t h i s r i b , p a i n i s fel t m a i n l y in t he
s h o u l d e r a n d i n the c e rv i c a l regio n : t h e re is a t y pic a l
tender spo t , w h ich can be p a l p a ted b e n e a t h the
clavicle towards t h e m a n u bri u m s t e r n i . The t y pic a l
re striction of moveme n t is i m p a i r e d a n teflexion of
t h e rotated h e a d : t h e e x a m i n e r s t a n d s b e h i n d the
s e a t e d p a ti e nt a nd r o t a t e s her head away from the
a ffec t e d r i b . W i th the rad i a l aspect o f t h e f o r e ll n g e r
of the o t h e r h a n d he c r e a te s a fu lcrum p a r a l l e l to
a n d a b o v e the c l a v i c l e , over which t h e r o t a t e d h e a d
a n d n e c k are b e n t fo rward ( Fi g u r e 4 . 27 ) . T h e re s u l t
o f t h i s ma n o eu v re i s c o m p a re d for b o t h sides.
I n cr ea s e d resis t a n c e a n d e v e n te n d e r n e ss m a y b e fe l t
o n s p r i n g i n g t h e first r i b from a b o v e ( see F i g u re 6.50,
p . 1 88 ) . D i r e c t m o v e m e n t p a l p a ti o n of t h e fi r s t r i b i s
pe r fo r m e d b y inse r t in g t h e fo re fi n ger be h i nd the clav­
icle, with the patient s u pin e and fol l o w i n g t h e move­
ment of t h e r i b d u r i n g i n h a la ti o n and exha l a t io n .
,
E x a m i n at i o n o f t h e cerv i c a l sp i n e
A fter genera l i n s p e c t i on o f the head a nd nec k posi t i o n
we test a c t i v e m o b i l i ty - ante- a n d re troflexio n , s i de­
b e n d i n g a n d rotation. W h e n d e a l i n g with the
ce rvica l spine it is i m p o r t a nt not t o o m i t e x a m i n a t i o n
of res i s ted i s o m e t r i c m o b i lity w h i c h r e l i a b l y rev e a l s
pa i n d u e to m u s c u l a r l e s i o n s : t h i s i s fre q u e n tl y
si g n i fi c a n t i n a c u te trau m a .
T h e best p o s i t i o n fo r t h e p a t ie n t d u r i n g p a l pa t i o n
is s u p i n e t h e h e a d resting a ga i n s t t h e exa m i n e r ' s
t h igh o r be l l y a n d s l i gh tl y rai s e d . I n t h i s po s i t i o n t h e
.
, ,
�
( b)
Figure 4.28 Palpa t i o n of t h e t r a n sv e r s e p rocesses of t h e
a t l a s ( a ) with t h e p a t i e n t s e a t e d : ( h ) cerv i c a l s p i n e . s u p i n e
m u scles are re laxed a n d w e can p a l p a t e n o t o n l y t h e
processes b u t a l so t h e t r a n s v e r se and a rtic­
u lar p ro ce s s e s , w h i l e if the head is sl i g h t l y raised we
can p a l p a t e the p o s t e r ior a rch of the a t l a s . In order
to p a l p a t e the l a tera l il s pe c t of the s p i n o u s p rocess
of C2, w h ich i s one of t h e p r i n ci p a l p a i n p o i n t s the
h e a d m u s t be b e n t to t h e o p p o s i te side. The tra ns­
v e rse processes of t h e a t l a s a re fe l t between the
mastoid p rocesses and t h e r a m u s of the mand ible.
but t h e y should be p a l p a t e d from b e l o w , w i t h t h e
p a t ie n t s e a t e d , because t h e y a re m o re p r o m i n e n t
t h a n t h e tra nsverse processes o f t he l ow e r ce r v i c a l
v e rtebrae ( Fig u re 4 . 28 ) .
For e x a c t o r i e n til t i o n i t i s i m p o rt a n t to l o cal iz e
cor r e c t l y t h e s p i n o u s p rocesses of C7 : t h i s is done
d u r i n g re t rofle x i o n o f t h e c e r v ic a l s p i n e . P l a ci n g one
fi n g e r on C7 a n d t h e n e x t o n C6, we will n o t e t h a t
w h i le C 7 re m a i n s in p l a c e . C6 m o v e s forw a rd a n d is
d i ffic u l t to p a l p a te in r e t r o fl e x i o n . ( N B : One s h o u l d
n o t rely o n the vertebra p ro mine n s b e i ng i n e V i ta b l y
spi n o u s
.
C7 .)
Exa m i n a ti o n of p Cl s s i v e m o b i l i ty m u s t begin w i t h
of t h e w h o l e o f t h e ce rv i ca l s p i n e .
The p a t ie n t i s s e a t e d a n d t h e e x a m i n e r m u s t fi x
t h e m o bi l i ty
Copyrighted Material
Examinatio/l
( i m m o b i l i z e ) t h e s h o u l d e r g i rd l e .
passive
of 10("01ll01Or f1ll1C1ion anrl ils dis/llrbana
1 09
He be g i n s w i t h
of t h e
r e t r o fl e x i o n : s t a n d i n g b y t h e s i d e
p a t i e n t h e moves h e r h e a d i n to r e t r o fl e x i o n w i t h o n e
hand
w h ile
the
other
fi x e s
the
cervicoth oracic
j u nc t i o n . In p a s s i v e a n te fl e x i o n t h e p a t i e n t ' s ch i n is
drawn to t h e
stern u m ;
t h i s i s a m o v e m e n t th a t is
o ft e n r e s t r i c t ed beca use o f s h o r t e n e d neck m u scles.
If m a x i m u m a n t e fl e x i o n is i m m e d i a te l y p a i n f u l , and
t h e r e i s n o m e n i n g i t i s o r a c u te rad i c u l a r p a i n , the
p a i n fe l t b y t h e p a t ie n t is us u a l l y d u e to r es t r i c t e d
a n t e fl e x i o n of t h e occi p u t aga i n st t h e a t l a s ; i f, how­
e v e r , pain i s fe l t a fte r
l ig a m e n t
pain
(see
1 5-20
pp.
s , this i s most p r o b a b ly
270-27 1 ) ,
A n te fl e x i o n
head a c h e ) . I n o r d e r to e x a m i n e s i d e - b e n d i n g o f t h e
cervica l s p i n e . t h e o p e r a t o r m u s t fi x t h e s h o u l d e r o f
th e s i d e towa rds w h i c h t h e h e a d is b e n t a n d c o m p a re
mo b i l i t y in b o t h d i re ct i o n s .
( I f he fi x e d
the shoulder
a w a y from w h i c h t h e h e a d is b e n t he w o u l d t h e n b e
e x a m i n i n g t h e s t r e tc h i ng o f t h e tra p e z i u s m u s c l e o r
e v e n o f t h e sc a l e n i . )
( a)
Rotation
With th e pa tien t 's h e a d a n d n eck e rect
The e x a m i n e r e i t h e r fixes the s h o u l d e r away from
w h i c h the h e a d is
tu r n e d ,
w i th one e l b o w , o b s e r v i n g
how c l ose he can b r i n g t h e c h i n to t h e s h o u l d e r o n
one
s i d e o r t h e o t h e r ; or h e cro s s e s b o t h h a n d s a n d ,
w i t h h i s fo re a r m , h e fi x e s fr o m b e h i n d t h e s h o u l d e r
towa r d s
w h i ch
the
head
is
t u r ne d ,
m o v i ng t h e
occ i p u t . H i s o t h e r h a n d m o v e s t h e c h i n . C a r e m u st
be t a k e n to p e r form r o t a t i on of t h e head and n e c k
ro u n d a v e r t i ca l a x i s
(Figu re
4.29).
With t h e head i n maxim um a n te flexion
The
examiner
s t a n d s be h i n d t h e p a t i e n t ; w i t h o n e
h a n d on t h e occ i p u t h e m ov e s t h e h e a d a n d n eck
i n to
maxi m u m
a n te fl e x i o n , w h i le
his o t h e r h a n d
h o l d s t h e p a t i e n t ' s ch i n . T h e ro t a t i o n h e n o w e ffec t s
is m a i nl y b e t w e e n t h e occ i p u t a n d C2, i . e . betwe e n
a t l a s a n d a x i s . Aga i n . c a re m u s t be t a k e n t o rota te
ro u n d t h e axis o f the head and the ce r v i c a l s p i n e ,
i . e . t h e o p e ra t o r m o v e s t h e occ i p u t f r o m o n e s i d e t o
t h e o t h e r . w h i l e t h e c h i n re m a i n s a l mo s t fi x e d . A
word of c a u t i o n : b e c a u s e t h e e x a m i ner is s t a n d i n g
b e h i n d t he p a t i e n t , i t i s t h e occ i p u t b e s e e s , a n d h e
( b)
Figure 4.29 Exa m i n a t i o n of ro t a t i o n of t h e e n t i re ce r v i c a l
h a n d s m o v i n g i n t h e s a m e d i re c t i o n :
spi n e : (a) b o t h
( b ) bot h hands
a n d a rm s m o v i n g i n oppo s i t e d i re c t i o n s .
l a t t e r i s p a r t i c u l a rl y u s e f u l fo r e x a m i n a t i o n o f
ro t a t i on i n r e t r o l1 e x i o n
The
is t h e r e fo re t e m p ted t o m o v e t h e c h i n l
t h e h a n d on t h e occi p u t t h a t ro t a t e s t h e h e a d , t h e
a x i s o f r o t a t i o n b e i n g c l o s e b e h i n d t h e fo r e h e a d . A t
With the pa tie n t 's c h in dra wn towa rds the
neck
t h e s a m e time s o m e degree o f t r a c t i o n i s a p p l i e d to
the h e a d .
A s l i ro u t ( 1 97 9 ) h a s s h o w n , move m e n t rest r i c t i o n
o f t h e ( '2/3 segme n t ca n b e sele c t i v e l y s h o w n b y t h is
mov e m e n t . A g a i n t h e ex a m i n e r s t a n d s be h i n d the
p a ti e n t , rota t i n g the head w i t h o n e h a n d o n the
occ i p u t and one o n the c h i n . The l a t t e r i s n e c e s s a ry
m a i n l y to fix t h e c h i n a ga i n s t the n e c k , w h i l e it i s
I n retro flexion
This rev e a ls bloc kage below C3 ; the grea ter t h e
r e t r o A e x i o n , t h e m o r e c a u d a l t h e seg m e n t c a u s i n g i t .
H e r e . t o o , t h e c h i n s h o u l d b e a l m o s t fi x e d w h i l e t h e
Copyrighted Material
110
Munip u la/ive Th erapy
in Rehab ili/O Iiol1 of the L o c o m %
r
Systel ll
h a n d on the occi p u t p r o d u c e s rotati o n . To fix the
p a t i e n t s s h o u l d e rs , t h e e x a m i ne r ' s a r m s s h o u l.d move
in opp o s i t e d i r e ct i o n s , i . e . rot a t i ng t h e p a t i e n t s head
to t h e l e f t h e grasps t h e c h i n w i t h h i s righ t h a n d
( p u s h i n g th e c h i n s l i g h t l y to t h e l e f t ) a n d t h e occi put
w i t h h i s l eft , p u s h i n g towards t h e r i g h t and re si s t i n g
rotation of t h e s h o u l d e r w i t h h i s l e ft fore a r m ( F i g u re
'
'
4.29b).
Afte r these more o r l e s s scree n i n g te c h n i q u e s w e
t o t h e mos t i m po r t a n t s p ec i fic tech­
m u s t p roc e e d
n i q ues.
S i de-be n d i ng
T h i s c a n be p e rfo r m e d wi t h t h e p a t i e n t s e a t e d
or
su p i n e ; i n e a c h c a se t h e e x a m i ne r b e n d s t h e p a t i e n t 's
h e a d s i d e w a y s w i t h o ne h a nd w h i l e t h e o t h e r crea tes
fu lcrum wit h t h e aid of t h e m e d i a l a s p e c t o f t h e
fo re fi n ge r a ga i n s t t h e tra nsverse p rocess of t h e lowe r
v e r t e b ra o f t h e s eg m e n t u n d e r e x a m i n a tio n . B o t h
the r a n g e o f m o v e m e n t and the res i s t a n c e i n e n d ­
po s i ti o n m u s t b e no te d . I n t h e s u p i ne p o s i t i o n the
p a t i e n t ' s head i s pr oj ec te d over the end of t h e t a b l e
a n d cr a d le d i n t h e exa m i n e r' s h a n d . I t is a d v i s a b le
to rot a t e th e h e a d s l i g h t ly i n t h e o pp o s i te d i re c t i o n
to t h a t of s i d e - b e n d i n g , a n d to l i f t i t (F i g u r e 4 . 30a) .
T h i s technique is a p p l i ca b l e from C 1I 2 to C5/6 a n d
a
( a)
e v e n C617 .
To e x a m i n e s i d e - be n d i n g a t C 1 I2 , the ce r v i c a l
s p i n e s h o u l d be k e p t s tra ig ht up to C2 w h i l e t h e
op e r a t o r rota tes the h e a d ro u nd a n axis t h r oug h t h e
b r i d ge of t h e n ose ( F i g u re 4 . 3 0 b ) .
So as to d e t e r m i n e on which s i d e th e a p o p h y s e a l
j o i n t is r e s t r i c t e d , s i d e - be n d i n g c a n be e x a m i n e d
w i t h t h e cerv i c a l s p i n e i n a n t e - o r i n r e t ro A e x i on , b y
r a i s i n g t h e h e a d i n t h e fo r me r c a s e , o r l o w e r i ng i t i n
t h e l a t te r. I f r est r i c t i o n i s fe l t i n a n tefl e x i o n t h e j o i n t
o n t h e o p po s i t e side is restricted in s id e -ben d i n g a nd
in a n t e A exi o n , if in r e t r o fl e x i o n , t h e j o i n t on t h e s i d e
to w h i c h l a teroflex i o n i s c a r r i e d o u t i s r es t ri c te d in
re t r o fl e x i o n a n d s i d e - be n d i ng .
Dealing w i t h t h e ce rvico thoracic j u n c t i o n , w i t h
t h e p a t i e n t seated t h e exa miner must ta k e care to
m a i n t a i n t h e w h o le of the cervicotho racic s p i n e
e r e c t , a n d t h e n e c k e v e n i n s l i g h t r e t ro fl e x i o n , w h i l e
the h e a d m u st b e s l i g h t l y ro t a t e d i n t h e d i rect ion
o p po s i t e to t h a t of the s i d e - b e n d i n g . With t h e t h u mb
of the o t h e r h a n d h e c re a t e s a f u l c r u m a g a i n s t t h e
sp i n ous processes o f t h e l o w e r v e rtebra o f the
ex a m i n e d s e g m e n t
( F ig u r e
4.31).
T h e s a m e e ffe ct c a n be a ch i e ve d w i t h t h e p a t i e n t
l y i n g o n h e r s i d e : t h e e x a m i n e r sta n d s i n fr o n t of t h e
pa t i e n t , cr a d l i n g h e r h e a d a n d ne ck i n h i s fore a r m
a n d t h u s p ro d u c i n g a s i d e - be n d i n g m o v e me n t , wh i le
t h e t h u mb of h i s o th e r h a n d fi x e s t h e spi n o u s p ro ­
cesses fro m above ( f r om t h e s i d e ; s e e F i g u re 4.34).
I n b o th cases t h e hand that side-bends the c e rv i c a l
s p i n e a l s o fi xes ( p u s h e s ) t h e s p i n o u s process o f t h e
u p pe r vertebra, with the thenar (hypo t h e n a r ) .
( b)
Figure 4.30 E x a m i n a t i o n o f p a s s i ve l a t e r a l nex i o n o f
i n d i v i d u a l s eg m e n t s o f t h e cerv i c a l s p i n e w i t h t h e p a t i e n t
s u pi n e : (0) i n t h e l o w e r c e r v i c a l spi n e : (iJ) he t ween the
a tlas a n d axis
Rotat i o n
T h e pa ti e n t i s s e a ted w h i l e t h e e x a m i n e r s t a n d s
b e h i n d h e r a n d fi x e s betwee n t hum b il n d fore fi n ge r
of o n e h a n d t h e verte b ra l a rc h of t h e lower ver t e b ra
of t h e r e l e v a n t segm e n t , from o ne t r a n s v e rse p r o c e s s
to the o t h e r . The e x a m i ner n o w ro t a t e s t he p a t i e n t ' s
head ( usu a l l y w i t h h i s o t h e r h a nd on t h e ch i n ) u n t i l
h e fe e l s t h a t t h e t r a n s v e rs e process is e n g ag e d
a g a i n s t h i s t h umb or forefi nger. He begins w i t h t h e
a x i s , establish i ng t h e ra nge o f m o ve m e n t be tween
a tl a s a n d a x i s . proceed i n g from one v e r t e b ra l a rc h
Copyrighted Material
Examination of /ocomOlOr function and its disturbance
111
o f s i n g l e m o b i l e segme n t s , a n d e q u a l l y s u i t a b l e for
optical r e g i s tr atio n . B e r g e r ( 1 984) has const ructed a
dev ice (cervicomotogra ph ) w h i c h is a h e l m e t fixed
t o the cei l i n g b y j o i n ts and r o d s . The p a t i e n t is
seated, l oo k i n g a t a fix e d poi n t in or de r to d e te r m i n e
t h e n e u t ra l po s i ti o n o f t h e h e a d . U s i n g t h e tec h n i q u e
desc r i b e d h e re t h e opera t o r fi rs t e x a m i n e s t h e seg­
m e n t C1/2 by fix a t io n of C2, t he n C2/3 by fixation
o f C3, a nd so o n down to C5/6; c a p a c i t y t r a n s d ucers
i n the rod j o i n ts m a k e e l e c t r o n i c r e co r d i ngs o f the
range o f m o v e m e n t p o s s i b l e . T h e r es u l t i n g gra p h is
a ' c e rv i c o m o to gr a m ' (Fi gu r e 4.32b, c) .
T h e r e a re two i m p or t a n t tech n i ca l d e t a i l s to be
noted i n this rotation tech n i q u e : ( 1 ) i f t h e e x a m i n e r
fi x e s t h e a r c h o f a v e r t e b r a h e m u s t do s o e x a c t l y i n
t h e n e u t r a l p o s i t i o n , i . e . h e m u s t sen se t h e co rr e c t
pos i t i o n ; (2) he m u s t n o t use fo rce to fix t h e verte­
b r a l arc h : t h e p a t i e n t s i m p l y stops t u r n i ng t h e h e a d
a t t h e m o m e n t when h e s e n ses t h e e x a m i n e r ' s fi ngers
c om i n g i n to contact w i th t h e artic u l a r p rocess from
b e h i n d b y s o m e retlex a c t i o n .
R o t a t i o n c a n a l so b e exami n ed i n t h e ce r v i co ­
aga i n s t
t h e e x a m i n e r ' s s h o u l d e r ( by t h e fo re a r m ) , n o s e a n d
c h i n t u r n e d towa rds h e r e l bow; t h e h e a d a n d n e c k
a re t h u s t u r n e d to the s i d e . The e x a m i n e r ' s hy po ­
t h e n ar a n d l i t t l e fi n ger a re at t h e c e r v i c o t h o r a c i c
j u n c t i o n from a bov e , the l i t t l e fi n ge r r o u n d t h e
s pi n o us process of C7 or Th l . The t h u m b of h is o t h e r
t h o ra c i c j u nc t i o n ; t h e p a t i e n t ' s h e a d i s h e l d
( a)
h a n d e x e r ts sp r i n g i ng p r ess u r e
p rocess, opposing
a ga i n s t
the spinous
f u r t h e r r o t a t i o n a f t e r t h e s l ack h a s
b e e n ta k e n u p (Fi g u re
4 . 32d) .
A s i m pl e s c r ee n i n g t e c h n iq u e is to h o l d t he s p i n o u s
p rocess be t wee n both t h u m b s , from C 7 d o w n t o Th3
i n s u c c ess i o n , as t h e p a t i e n t rota tes t h e n e c k as fa r
a s p o ssi b l e w h i l e m a i n t a i n i n g n ec k a n d t h o rax e r e c t .
T h e e x a m i n e r s e n s e s t h e m o v e m e n t of t h e s p i n o u s
process h e fi x e s be twee n h i s t h u m b s from s i d e t o s i d e .
S h ifting tech n iques
These a re u s e d
to
e x a m i n e j o i n t pl ay i n t h e ce r v i c a l
a n a n t e ro p o s t e rio r
i n a l a t e r o l a t e r a l d i rection . The e x a m i n e r s t a n d s
a t t h e s i d e of t h e s e a ted p a t i e n t a n d p u ts his a r m
ro u n d h e r h e a d i n s u c h a w a y t h a t h i s e l bo w i s i n
front of h e r fa ce or fo r e h e a d , w h i l e h i s l i t t l e fi n ge r
grasps t h e ve r te b r a l a rch o f the u p p e r v e r t e b r a o f
t he segm e n t to be teste d . W i t h t h e o t h e r h a n d
he fi x e s t h e v e r t e b r a l a rch o f the l o w e r v e r t e b r a
b e t w e e n th u m b a n d fore fi n g e r from b e h i n d . W i t h h i s
a r m on the p a t i e n t ' s h e a d h e now ( 1 ) p u s h e s t h e
h e a d a n d t h e u p p e r v e r t e b r a b a c k w a rd s , t a k i n g u p
t h e slack a n d fi n a l l y s p r i n g i n g t h e e n d - p o s i t i o n
a g a i n s t t h e t h u m b a n d fi ng e r of t h e fix i n g hand; o r
(2) h e s i d e - s h i ft s t h e p a t i e n t ' s h e a d a n d u p p e r
v e r t e b r a a g a i n s t e i t h e r t h e t h u m b or the fo r e fi n ge r
o f the fixing h a n d , fi rs t t a k i n g u p t h e s l a c k and t h e n
s p r i n g i n g t h e e n d - po si t i o n ( F i g u re 4.33a). I n t h i s w a y
s p i n e a n d c a n be c a r ri e d o u t i n
and
( b)
Figure 4.31 Exa m i n a t ion of l a t e ra l s p r i nging a t t he
ce rvico t h o ra c i c j u n c t i o n s . by a p u s h w i t h t h e t h u m b
aga i n s t t h e l a t e r a l a s p e c t o f t h e lower s p i n o u s process
t h e segm e n t ex a m i n ed
of
to t h e n e x t . The r a n g e of m o v em e n t s h o u l d i n c r e a s e
from one segm e n t to t h e n e x t . If t h e re is
bl o c ka ge i n a m o b i l e seg m e n t , the a b s e nce o f th i s
i ncrease i n one or both d i re c t i o n s s ho u l d b e n o te d
( Fi g u r e 4 . 32a).
T h i s t ec h n i q u e i s p a r t i c u l a r l y s u ita b l e fo r d e m o n ­
s t r a t i o n i n t h e l e c t ure h a l l of movement r e s tr i c tio n
ste p - w i s e
Copyrighted Material
1 12
Manip u lalive Therapy in
Rehabililalion of Ihe Locomotor Syslem
100
80
60
-
L
R
( b)
100
80
60
( a)
�I
--
--
R
2
3
( c)
Figure 4.32 (a)
E x a mination ( m o b i l i za t i o n )
of res t r i c t e d
r o t a t i o n i n t il e cerv i c a l s p i n e w i t h t h e p a t i e n t
( a rrow:
fi x a t i o n
by
the
thumb
seated
from behi nd ) .
( b ) ' Cervico m o togra m ' ( from M . B e rg e r . perso n a l
com m u n ic a t i o n ) s h o w s o n e x a m i n a t i o n o f r i g h t rota t i o n
("2/3 , and
C3/4 . rota t i o n to t h e l e ft ( t h i n l i n e s )
bei n g n o r m a l . (e) The s a m e case: ( 1 ) right ro t a ti o n on l y :
( t h i c k l i n es ) m o ve m e n t restrict i o n a t C 1 /2 a n d
h y p e r m o b i l i ty at
( 2 ) a ft e r t r e a t m e n t o f C l /2 ;
(d)
(3)
Examination (mobilization)
a f t e r t re a t m e n t o f C2/3 .
of ro t a t i o n at t h e
cervicothoracic j u nction
c a n e x a m i n e the c e rv i c a l segme n ts fro m C2!3
to C5/6 and a lso in t h e a n teroposterior
d irectio n , the occ i p u t a g a i n s t t he a t las - h e re I
reco m m e n d s l i g h t a n te fl e x i o n of t h e h e a d . T h e fi x i n g
h a n d sta b i l izes t h e a r c h o f the a x i s , b u t s h i ft i n g
occ u rs e x c l u s i v e l y between o cc i p u t a n d a t las b e c a u s e
no s h i ft i n g m o v e m e n t c a n occ u r between the
a n terior a rch of t h e atlas a nd the odontoid pro c e ss
(Figure 4.33a) .
From C617 to T I /2 o r e v e n TI/3 i t i s a g a i n o n l y
p o ssi b l e to ca rry o u t a n t e ropos terior s h i fts. w i t h t h e
p a t i e n t s e a te d . The exam i n e r a p plies h i s h a n d to t h e
m a ss of the p a t i e n t ' s upp e r trapez i u s m u sc l e . from
a bove, producing a b a c k w a rd s h i ft . w h i l e h e fi x es t h e
he
down
( d)
Copyrighted Material
Exarn inotiol1
of /OC011l0101' /ltnCliol1 a n d i t s dist urbal7ce
I 13
Figure 4.34 E x a m i n a t i o n o f t h e c e r v i c o t h o r acic j u n c t i o n
the patient lying on her side
with
may now push the
patient's head backwards or
u p w a r d s , i . e . J a te ral l.y i n t h e d i re ct i o n o f t h e fix i n g
t h u m b ; d o w nw a rd s t h e m o v e m e n t is l e s s e ffe c t i v e .
I n t h e cerv i c o t horacic re gi o n the h a n d c o m i n g from
a b ove again p u s h e s a ga i n s t t h e mass o f
the upper
m u s c l e t o p r o d u c e a backward s h i ft; i t m a y
a l s o p u s h u pwa rds, p r o d u c i ng a l a t e ral s h i ft a g a i n s t
t h e spi nous process of the u p p e r vertebra, i n the
d i r e c t i o n of t h e thu m b of t h e o t h e r ha n d fi x i n g t h e
s p i n o u s p r o c ess of t h e l ower v e r t e b r a from a b o v e
( Fi g u r e 4 . 3 4 ) . I t i s i m p o r t a n t that the p u s h fro m
be low should a l w ays be d e l iv e red a t t h e l ev e l o f th e
upper verte bra of t h e s e g m e n t , so t h a t t h e re a re n o
trapezius
Figure 4.33 E x a m i n a t i o n of dorsal shift (springi ng) of t h e
cra n i a l a ga i n s t t h e ca u d a l a dj a ce n t v e r t e b ra (a) in t h e
cervical s p i n e a n d ( b ) i n t h e c e rv i co t h o racic j u n c t i o n : t h e
h e a d a n d cra n ia l ve r t e b r a o f t h e e x a m i n e d segme n t a re
s h i fted (backwa rds), w h i l e m o b i l i t y ( re s i s t a nce) is fe lt a t
t h e spinous p rocess o r verte b r a l a rc h o f t h e l owe r v e r t e b r a
s e g m e n ts
separating
taking
the
the
e x a m i n i ng h a n d s !
Both
be carried
out w i t h m i n im u m force . To s i d e - b e n d t h e e l bow of
t h e a rm pe r f o r m i n g the move m e n t s h o u l d s h ift on
t h e e x a m i n a t i o n t a bl e a n d n o t be r a i s e d , the h a n d
rotating a n d side-be n d i n g t h e p a t i e n t ' s h e a d
a u t om a t i c a l l y . T h e s e tec h n i q u e s fo r ex a m i n i n g s h i ft
(j oi nt p l a y ) a re a m o n g t h e m o s t s e n s i t i v e , r e v e a l i n g
bl o c k a ge i n t h e c e rv i c a l a n d cerv i co t h o r a c i c s p i n e
t h a t is a s y e t u n exposed by a n y o t h e r t e ch n i q u e .
up
slack and
s p r i n g i n g s h o u ld
M ov e m e nt between a t l a s a n d occiput
1.
e x a m i n er sta n d s
pa t i e n t w i t h h i s fi n gers o n h e r
face and c h i n a n d b r i n gs t h e h e a d i n t o m a x i m u m
r o t a tion , s t a bi l i z i n g i t a g a i ns t h i s c hes t a n d ta k i n g
c a re to s e e t h a t t h e h e a d i s ere c t , ro t a t i ng c o r rect­
Without
u si n g
a n y fo rce , the
b e h i n d t h e s e a te d
sp i n ous
p rocess of the lower ve rtebra of the s e g m e n t
fi n g e r o r t h e th u m b o f t h e o t h e r h a n d a n d
h a n d be twee n h i s fo rea rm a n d c h e s t w h i l e
w i t h on e
the
m o v i n g h i s t r u n k b a c k w a r d s ( Fi g u r e 4 . 3 3 b ) .
ly round a v e r t ica l a x i s . Af t e r t a k in g u p the s l a c k
S h i ft c a n a l s o b e ex a m i n e d w i t h t h e p a t ie n t lyi n g
on h e r s i d e ; t h e e x a m i n e r s t a n d s i n f r o n t o f h e r ,
g r a sp i n g h e r h e a d i n h i s a r m a n d s t a b i lizing i t again s t
h i s c h e s t , w h i l e h i s l i t tle fi n g e r cl a s p s the verte bra l
arch of t h e u p p e r v e rt e b ra o f t he segme n t be i n g
e x a m i n e d . T h e o t h e r h a n d fi x e s t h e s p i n o u s process
of t h e l ower ve rtebra w i t h h i s t h u m b . The exa m i n e r
h e s p r i n gs maxi m u m r o t a t i o n w i th t h e m i n i m u m
F ig u re 4 .29a) . W i t h a fi n g e rtip of
o t h e r h a n d h e s e n s e s s p r i n g i n g a t the tra ns­
ve r s e process of the a t l a s . An a lte r n a tive m e t h o d
is to .fix the a t l a s w i th the t h u m b a n d fo re fi n g e r
a g a i n s t t h e t r a n sverse p rocess o n e a c h s i d e from
beh i n d , ( s e e F i g u re 4.28a, p. 1 08) a n d to g r a s p
of
force ( see
the
Copyrighted Material
1 14
Manipulalive Therapy in Rehabilitation of the Locomotor System
Figure 4.37
Exam i n a t i o n of a n te fl e x i o n b e t w e e n occi p u t
a t las w i t h fi x a t ion o f t h e tra n sve rse p rocesses o f t h e
a t las
and
Figure 4.35 E x a m i n a tion
and atlas
2.
with the
of
l a t e ra l
Aexion
bet wee n
occ i p u t
b e a d r o t a t e d to t h e o p p os i t e s i d e
the p a t i en t ' s head w i th the other arm in order to
produce a very sma l l rot a tory move m e n t w h i l e
sl ightly side-bending the head i n the opposite
d i recti o n . In order to reach t h ose transverse
processes from beh ind the d i vergi ng t h u m b a n d
fore fi nger m u s t be i ncli n e d , poi n t i n g upwards
beneath the occ i p u t .
S ide-bending - The p a t i e n t lies s u p i n e w i t h her
h e a d over the edge of t h e t a b l e ; t h e e x a m i n e r
rot a t es t h e h e a d so as t o l o c k C 1 I2, i . e . a t l e a s t
a b o u t 50 degrees. H e n ow side-be nds the head
aga i ns t the cervic a l spi n e (which is erect). Head
rotation need not exceed 50 d egrees, an i m porta n t
poi n t t o re m e m b e r w i t h elderly patients ( Figu re
4.35 ) .
3 . Retroflexion - The p a t i e n t is s u p i n e w i t h her
head ove r t h e e n d of the ta ble ; the exa m i ne r
pl aces o n e h a n d on the c h i n a n d the o t h e r on t h e
occiput, rota ting i t to lock the atlas/axis, a n d bend ­
ing i t back against the cervical s p i n e . Ca re must
be t a ke n n o t to grasp the occipu t too close to the
a tlas, so that th e fingers meet n o obs t ruction
befo re full back-be n d i ng is achieved (Figure 4.36) .
4. A nteflexion - The patient is supine on the table;
the exa m i ne r places h i s hand under h e r occiput
from o n e side so that h i s t h u m b is resting against
o n e transverse process o f the a t l as a n d h i s i ndex
finger against the o t her, p roduci ng fi x a t ion of t he
<l rch of the a t las. W i t h h i s other hand on the
p a t i e n t ' s fore head he i nd uces a n teflexion (Figure
4 . 37 ) . A n t e roposterior sh i ft o f the occiput aga i nst
the atlas has a l ready been described under s h i ft
techniques (see Figure 4.33b, p . 1 1 3 ) .
Exa m i nation o f t h e extrem ity j o i nts
Figure 4.36
Exa m i n a t i o n o f r e t ro A e x i o n
a n d occ i p u t w i t h
the
h e a d ro t a t e d
between a t l a s
B e fore goi ng i n to d e t a i l r m us t st ress o nce again that
correct o r d istu rbed fu nction of the locomotor
system concerns both the s p i n a l co l u m n and the
extre m ities, and t h a t if p a i n is due to such a d isturb­
a nce, fu nction m ust be norm a l ized , w h a tever i ts
loca l iza t io n . I t is often taken for gra n ted by neurolo­
gists, as well as m a n i p u lators, t h a t the s p i n a l column
has the ' d o m i n a n t role ' a n d that pain al most
n e cessa r i l y rad i a tes from the spine to the extremi­
ties, i n a somew h a t hiera rch ica l manner. This i s to
neglect the fact that n e rvous con trol is the res u l t o f
processed i nfo r m a tion from rece ptors, a n d t h a t
t h ese are most n u merous a t t h e periphery of t h e
b o d y , i . e . a t the h ands a n d fee t ; a ffere n t i n put is of
paramo u n t importa nce. [ t c a n be disastrous for t h e
p hysici a n to neglect distu rbance o f the e x t re m i t y
Copyrighted Material
Examination of iocomotor function and its dislLLrhance
joints or o f the temporom a n d i b u l a r joints (m asticat­
ory dysfunction ) .
The exam i n a ti o n o f i n d iv i d u a l j o i n ts fol l ows the
pattern a lready esta blished: active movement, resis ted
or isome tric move m e n t to show wh ether m uscles a re
at fa u lt, and passive mobi l i t y i n c l u d i n g j o i n t p la y .
I [ passive m o b i l i ty i n a j o i n t i s i m p a i red , there is
a 'capsular p a ttern ' ( Cy r i a x , 1 977) for e ach j o i n t , i . e .
i f there i s move m e n t restrictio n i n several d i rections
it shows characteristic proportions, or a patte r n . I f
i m p a i r m e n t d o e s not fol l ow t h i s p a t t e r n w e m a y
conclude t h a t t h e lesion is n o t i n t h e j oi n t b u t
a ffe c t i n g i t from w i t h o u t . T h e signi fica nce of joi n t
p l a y l i e s i n t h e fact t h a t i ts d i s t u rb a n ce i s the first
sign of a lesi on. The tec h n i q u e o f exa m i n a tion of
j o i n t play i s descri bed in Cha pte r 6 , as i t is i d e n tical
to that of j o i n t m obi lization .
The s h o u l d e r
Active m o b i l ity i n c l udes abduction and elevation o f
the a r m , rota tion, a n teflexion and re troflexion. The
most stri k i ng d i s t u rbance is the ' p a i n fu l arc' of
Cy ri a x ( 1 977 ) d ur i ng abducti o n : the patie n t may feel
sharp p a i n d u ri n g abduction to even less than 90
degrees, but when she passes this point s h e c a n t h e n
raise her arm t o a ful l 1 80 degrees. Th is phenom e n on
is d u e to d isturba nce o f the subacrom i a l b u rsa which
faci l i ta tes the g l i d i n g motion o f t h e head o f the
h u m e rus, with t h e ro tator cu ff under the coraco­
acromia l l ig a m e n t .
I sometric resis t a nce m ay s h o w tend erness of
some muscle i nsertions: against abd ucti o n , the supra­
spinatus ten d o n ; aga i ns t ex ternal rota tion , the i nfra ­
spi n a t us ; a n d aga i nst r a i s i n g the se m i - flexed a r m
( l i ke a wa i te r carr y ing a tray, Figure 4 . 38c), the long
biceps tendon . Te nderness i n t h e s u bsca p u l a ris m ust
1 15
be d iagnosed by d i rect palpation, as described i n
Chapter 6 , p. 225 .
If passive m o b i l i t y is i m p a i red a n d t h e character­
istic capsu l a r pa ttern of the shou l d e r j o i n t is prese n t ,
t h e lesion is in t h e capsule of t h e g le n o h u me r a l j o i n t ,
as is t h e case i n 'frozen shou lder ' . I f we exa m i ne
from the n e u tra l pos i t i o n , i . e. w i th the a r m i n
a d d uction , t h e el bow i n righ t-a ngle flexion a n d the
forea r m faci ng forw a rd , we find accord i n g to Cyriax
m a x i m u m restriction of exte r n a l rotation fo l l owed
by abd uction and internal rota tion. Rece n tly, how­
ever, Sachse (1 995) u s i ng the tech nique shown in
Figure 4.63 showed that i t i s abduct i o n w h i c h a s a
rule is restricted fi rst a n d most. I t is therefore
i m porta n t to exa m ine abd uction fi x i n g the sh oulde r­
blade from above; e x t e rn a l rotation s h o u l d be exam­
i ned by the exam iner s t a n d i n g be h i nd the seated
patient and grasping t h e forearms c l ose to t h e e l bow,
k e ep i n g the e l bows c losel y a d d ucted agai nst the
patie n t ' s tru n k a n d using the forearm as a lever to
produce extern a l rotation (Figure 4.39). B y drawing
the p a ti e n t ' s t h u mbs u p her back, o n both sides,
w e examine mainly i n te r n a l rota t i o n coupled with
extension a n d adduct i o n .
I f i t is o n l y abduction t h a t is restricted, a n d
ro tation is free , t h e l e s i o n is i n the subacro m i a l
b u rsa, whether th ere is a p a i n fu l arc o r n o t . I n this
case there i s often i m pa i red j o i n t p l a y . The e xa m i n e r
s t a n d s behind t he sea ted patie n t a n d a bducts h e r
a r m to 9 0 d egrees, t e l l i n g h e r t o re lax. W i t h h i s other
h a nd on t h e head of t h e h u m e r u s h e exerts v e ry
sligh t pressure from above i n order to take up the
slack, and then springs t h e j o i n t in the s a m e
d i re c t i o n . I n teresti ng l y , if t here i s a t r u e caps u l a r
p a ttern a nd yet i t is possible t o a b d u c t the a r m to
the horizontal, we fi n d normal j o i n t play, which
aga i n shows that the 'frozen s h o u lder' i s n o t d u e to
Figure 4.38 E x a m i n a tion aga i n s t iso m e t r i c res i s t a n ce o f t h e m u s c l e s o f t h e r o t a t o r c u ff a t t h e s h o u l d e r : ( a ) a g a i n s t
a d d u c t ed u pper a r m (supraspinat us): (b) against external rota t i o n ( i n f r a s pi n a t us); ( c ) aga i nst r a i s i n g of
t h e se m i - fl e x e d arm (long biceps t e n d o n )
a b d u c t io n o f the
Copyrighted Material
116
Man ip ulative Therapy
in Rehabilitation of the L o c o m o t o r System
Pa i n d u e to blockage of t h e sternoclavicular j o i n t is
a m uch less common con d i t i o n , u n less t h e re is
rhe u m a toid arthri tis. The patient experiences pa i n
w h e n m o v i n g t h e s h o u l d e r-blades (sh rugging the
s h o uld ers) ; p a ss i v e rotation of t h e should e r i s
restricted a n d direct pa lpation rev e a l s tenderness.
There is one d i agnostic p i t fa l l to b e avoided ,
however: t e n d e rness of the m e d i a l e n d of the
clavicle c a n be due to tension a t the a ttac h m e n t
poi n t o f the sternocle idomastoid m uscle.
The e l bow j o i nt
Figure
4.39 E x a mi n a t i o n
t h e shoulder w i t h t h e
Aexed a t r ig h t a n g l e s
of
a rms
p a s s i v e e x te rn a l r o t a t i o n o f
i n a d d u c t i o n a n d e l bows
I m p a i r m e n t h e re concerns m a i n l y fl e x i o n and ex­
tension , the former s u fferi n g more (capsular pattern ) .
I n addition t h e re is pronation a n d s u pi n a t i o n betwe e n
t h e ra d i u s a n d t h e u l n a . A s t h ere a r e t h re e bones
a r t i c u l a t i n g at the e l bow, however, j o i n t p l a y i s
c o m p l e x , and i n c l udes move m e n t between rad i u s
a n d u l n a . The most i m porta n t c l i n i c a l c o n d i t i o n i s
p a i n a t the e p ico n dyles, w h e re we fi n d i n a d d i tion
to loca l tende rness a t the e p i co n d y l e s , i m pa ired
l a t e r a l s p r i n g i ng, and typical m uscle s p a s m s which
wi l l be dea l t with e l sewhere.
T h e wrist j o i nt
of joint p l a y ( ca u d a l shi ft) with
arm i n 9 0 d e g r e e a b d u c t i o n ;
sp r i n g i n g p re s s u re i s a p p l i e d from a b o v e , o n t h e head o f
t h e hume rus
Figure
4.40 E x a m i n a t i o n
the patient
sea ted, her
b l oc kage. Joi n t p l ay, however, i s certai n ly impaired
if o n l y a b d u c t i o n is i n volve d , i.e. i n w h a t m i ght be
called ' periarthr i t i s ' i.f i t were not prefera b l e to d rop
this m i s l e a d i n g term and ca l l it ' a bd uction lesion '
( Figure 4.40) . Care m u s t be ta ken to place the h a n d
o n the h e a d o f t h e h u m e ru s a n d not on t h e labr u m
g l e n o i d a l e o f the sca p u l a .
Two more joints may c a u s e s h o u l d e r p a i n : the
acromioc l a v i c u l a r a n d the sternoclavicu l a r . I nv o lve ­
m e n t o f t h e forme r is a very frequent b u t r a r e l y
d iagnosed cond i t i o n , yet d iagnosis is not d i fficu l t : i f
we pus h t h e elbow of the affected s i d e aga i n s t t h e
opposi te s h o u l d e r . t h e p a ti e n t fe els pa i n and t h e
move m e n t is restricted compared w i t h t h e h e a l th y
s i d e . D i rect p a l p a t i o n o f t h e j o i n t i s a lso pa i n fu l .
This is a complex j o i n t c o n s i s t i n g of the r a d i u s a n d
u ln a , t h e ca rpa l b o n e s a n d t h e j o i n ts of t h e d ista l.
carpa l bones a n d t h e me taca rpals. For c l i n ical
loca l i za t i o n it is use fu l to k n ow that the proxi m a l
s kin fo ld o n the d orsa l aspect o f the w r i s t in dors i ­
flexion co rresponds to t h e radiocarpal j o i n t , w h ereas
the fold o n t h e p a l m a r as pect i n p al m a r flexion
corresponds to the carpom etacarpal j o i n ts . Active
move m e n t consists o f d o rsal a n d pa l m a r flexion and
ra d i a l a n d ulnar flexion. For correct t r e a t m e n t each
o f the movem e n ts m u s t be fu l l y u n d e rstood .
Dorsal fle x i o n takes p l a ce more i n the m i d -carpal
joint, the d i s t a l row o f the carpal bones gliding i n a
p a l m a r d i rection . I f this m o v e m e n t is i mp a i red ,
p a l m a r g l i d i n g (jo i n t play) m u s t be restore d .
Palma r fl e x i o n t a k e s p lace m a i n l y i n t h e rad io­
c a r p a l j o i n t , the prox i m a l row of the carpa l bones
g l i d i n g i n a d o rs a l d i rection (j o i n t play) . I f p a l m a r
flexion is i mp a i re d , dorsal g l i d i n g m u s t b e restore d .
U l n a r flex i o n co n s ists of a r a d i a l gl iding move­
ment o f t h e ovoid o f the wrist in re l a t i o n to the
rad i us ( a nd u l n a ) , by w h i c h t h e hand rotates i n to
u i n a r fl e x i o n . Th i s g l i d i n g move m e n t of t h e prox i m a l
row against t h e radius m u s t b e restored i f u l n a r
fl e x i o n is i m paired.
Th e most com p l ex o f t hese move m e n t s is rad i a l
A e x i o n . T h i s moveme n t is achieved b y a p p roa c h i ng
t h e base o f t h e first me taca rpal to t he sty l oid p rocess
of the ra d i u s . T h i s i s m a d e poss i b l e by a l oca lized
dorsi flexion b e t w e e n the sca phoid and the trapez i u m ,
w h i ch c a n b e palpated a s a p a l m a r pro t u b e ra nce i n
the prox i m i ty o f t h e styloid process d u r i n g rad i a l
Copyrighted Material
Examinalion oj locomotor Junc/ion and its distllrbance
1 17
flex i o n , T h u s radial fl e x i o n cannot be carried out i f
the h a n d i s i n p a l m ar flex i o n , w h e re a s i t i s fac i l i tated
by dors i fl e x i o n ,
T o res t o re t h i s mov e m e n t we m u s t therefore
res tore j o i nt play between the t r ap e zi u m a n d t h e
sca phoid , mov i ng t h e for m e r i n a palmar d i rect i o n ,
E ve n more f r e q u e n t l y , h owever, radial fl e x ion is
re st r i c te d by yet a n o t h e r m ech a n i s m : impa i re d
p ro n a ti o n o f t h e radius aga i nst the u l n a . O n m o v i n g
the h a n d i n t o ra d i a l a n d u l n a r fl e x i o n on a h o r i z o n tal
board we can e a s i l y see that t h e forearm m a k e s a
pro n a to ry s y n k i n e s i s d u r i n g radial fl e x i o n a n d a
s up i n a t o r y s y n k i n e s i s d ur i ng u l n a r flexion . Hi nd e r­
i n g this s yn k i ne s i s by placing a t h u m b u n d e r t h e
s t y l o i d process of t h e radius w i l l prev e n t r ad i a l
flex i o n , T h e same holds - i n t h e opposite d i rection
- for u l na r flexion. We m u s t th e re fo r e exa m i n e a n d
restore j o i n t p l a y i n t h e e lbow j o i n t a s w e l l : fo r
i m p a i r e d rad i a l fl e x i o n , l a t e r a l s pr i n g i n g of the
e l bow joint s h o u l d be use d , and fo r u l n a r flexio n ,
m e d i a l springing, This i s a l s o t h e mech a n i s m
u nd e rl y i n g s ty l o i d p r o c es s pa i n ,
I n a d d i t i o n to m o v e me n t t h a t ca n be ca rried o u t
a c t i v e l y t h e re i s , o f cou rse , j o i n t p l a y betw e e n e ach
of the c a rp a l b o n e s a n d b e t w e e n t h e c a r p a l bones
and the fo re a r m , a n d also between t he c a r p a l a n d
t he metaca rpal bones. a n d even between t h e bases
o f the me tacarpa l s , T h i s has b e e n s h own to b e of
considerable cl i n i c a l i mpo r t a n c e i n v i ew of t h e
freq u e n t occ u r re n ce o f t h e c a r p a l -tu n n el s y n d r o m e
W hereas t h e g l i d i n g move m e n ts of j o i n t p l a y c a n
normal ly be b ro u g ht about w i t h the m i n i m u m o f
force (i ndeed, i t i s d i fficu l t to e x e r t s o l i t tle force as
not to m ov e th e s e b o ne s ) in the c a r p a l - t u n n e l
syndrome there is i ncreased resista nce to j o i n t p l a y ,
I t c a n o n ly be d i agnose d , however, by exami n i ng
w i t h t h e m i n i m u m of fo rce , Th e c l i n i c a l co nseque nce
is clear: we t r ea t the carpal-t u n n e l syndrome by
remov i ng its m a i n cause, d i s t u r b e d j o i n t p l a y of the
bones t h a t fo r m the w a l l s of the carp a l t u n n e l ,
b e a r i n g i n m i n d th a t t h i s functi o n , t o o , i s i n fl u e n c e d
by move m e n t p a tt e rn s c o n t r o l l i ng t h e upper
,
Figure 4.41
Exa m i nation
of t h e
hip
joi n t for Patrick's sign
.
,
extremity.
T h e fi n g e r j o i n ts
a re d e a l t with i n Chapter 6 ( p . 1 6 1 ) .
The h i p joint
Alth ough t h e h i p i s a n e x t re m i t y j o i n t c l i n i c a l l y i t
o f the pe l v i s a n d fr e q ue n t l y the fi r s t sym ptom
i n lesions of t h e h i p joint is low-back p a i n The most
c on s t a n t s igns to be looked fo r are P a t r ick's sign
(Fi g u r e 4 . 4 1 ) , a tender fe m o r a l head in the g r o i n ,
restriction and tenderness on i n te rn a l ro tation ( Figure
4.42), a n d p a i n on m a xi m u m ac t i ve a b d u c ti o n w i t h
th e p a t i e n t ly i ng o n h e r s i d e . The re i s t e n de r n es s o f
t h e grea ter t r oc h a n te r a n d , i f t h e p a t i e n t a l s o
c o m p l a i n s of p a i n i n the k n ee s , tendern ess o f t h e
pes a n s e r i n u s on the t i b i a . The t y pi ca l ca p s ul a r
pattern is m a x i m u m d i s t u rba nce of i n tern a l ro t a t i o n
,
is pa rt
,
.
Figure 4.42 I n t ern a l
Copyrighted Material
rotarian of t h e hip joint
Copyrighted Material
EXlim inmioll
of lacoma/or fl lllClio/1 (Ind i/s di,\"IIIriJmICf
1 19
b r u x i s m , w i t h r e s u l t i n g, c h a n ge s i n t h e t ee t h , i s a l s o
sign i fi ca n t .
B e s i d e s a ff e c t i n g, t h e m a s t i ca t o r y m u sc l e s , d y s ­
fu n c t i o n
may
a l so a ffe c t t h e d i g a s t r i c u s : i ncre a s e d
t e n s i o n c a n b e fe l t i n t h e s u b m a n d i b u l a r regi o n . I f
t h e r e i s g re a t e r t e n s i o n on o n e s i d e , t h e re m a y b e
l a t e ra l d e v i a t i o n o f t h e h y o i d a n d t h y roid c a r t i l a g e ,
a n d i nc r e a s e d res i s t a n c e to s h i f t i n g o f t h e m i d - l i n e
s t r u c t u re s
away
from
the
d e v i a t i n g,
c h a r a c t e r i s t i c m u sc u l a r i m b a l a n c e
ity i n
t he
m a s t i c a t o ry
is
side.
The
i n cre a s e d a ct i v ­
m u sc l e s , w h i c h
a re
tigh t,
w h e re a s t h e m u s c l e s t h a t gov e r n t h e o pe n i n g o f t h e
mouth
(m8inly
t h e d i ga s t r i c u s a n d t h e d e e p n e c k
fl e x ors) a r e re l at i v e l y w e a k .
Exam i n ation of d i st u rbed
eq u i l i b r i u m
I h a v e a l re a d y s h ow n t h a t t h e s p i n a l c o l u m n p l a y s
an
i m po rt a n t
part
in
m a i n ta i ni n g
or
d isturbing
e q u i l i b r i u m , a n d i t i s t h e re fo re n e c e s s a r y t o a s s e s s
t h i s fac t o r in c a s e s o f d i s t u r b a n c e , i f p o ss i b l e by
d irect cl i n i ca l e x a m i n a t i o n .
H a u t a n t ' s t e s t i s very s u i t a b l e
fo r t h i s p u r p o s e :
the
p a t i e n t i s se a t e d i n a c h a i r w h i c h s u p p o r t s h e r b a c k ,
w i t h b o t h a r m s s t r e t c h e d for w a r d . The e x a m i n e r
s t a n d s fa c i n g h e r. w i t h h i s t h u m b s poi n t i n g a t t h e
Fi glll'e 4.43 Ha u t a n t 's t e s t : t h e p a t i e n t i s s e a t e d w i t h t h e
exa m i n e r
w a t c h e s d e v i a t i o n of t h e o u t s t r e t c h e d a r m s b y comp a r i n g
t iJ e pos i t i o n o f t h e p a ti e n t 's h a nds wi t h iJ is o w n t h u m b s
b a c k s u p p o r t e d a n d t h e eyes close d : t h e
p a t i e n t ' s h a n d s . T h e p a t i e n t c l oses h e r e y e s w h i l e
t h e exa m i n e r w a t c h e s f or a fe w s e c o n d s , t o see
i m b a l a n c e d u e t o c e r v i c a l l e s i o n i s so c h a ra c t e r i s t i c
w h e t h e r t h e p a t i c n t ' s h a n d s d e v i a te to one s i d e i n
that we
rc l a t i o n t o h i s o w n t h u m bs ( F i g u re 4 . 4 3 ) . A ft c r
ex a m i n a tion
can
s p e a k o f a ' ce r v i ca l p a t te r n ' ( see p .
273 ) .
out
if the
T h i s v e ry si m p l e e x a m i n a t i o n i s c a r r i e d
is
p a t i e n t c o m p l a i n s o f d is t u r b e d ba l a n c e a n d i f t h e t es t
re pe a ted i n d i f fe r e n t h e a d p os i t i o n s : b e n t b a c k , b e n t
s ta n d i ng o n t w o sc a l e s s h ows a d i ffe r e nce gre a t e r
fo rw a r d .
in
the
t u rn e d to
n e u t ra l
p os i t i o n ,
the test
t il e l e ft a n d t o t h e r i g h t . W h i l e
t h an 4
t h e patie n t c h a nges t he pos i t i o n o f h e r h e a d t h e
e x a m i n e r ilo l d s h e r h a n d s i n
ne utra l posi t i o n t o
p re v e n t d e v i a t i o n d u e t o s y n k i n e s i s o f t h e a r m s .
up,
t h e p a t i e n t fe e l s s a fe e v e n i f d i zz y ,
a n d d e v i a t i o n i s n o t c a u s e d by ne rv o u s n es s , a s i s
case
o ft e n t h e
s t ructed
i n Rombe rg's t e s t ( w i t h t h e pa t i e n t
sta n d i n g) . T h e s e c o n d a d v a n tage i s t h a t w i t h t h e
d e v i a t i o n o f t h e a rms i s poss i b l e . I n R o m b e rg ' s te s t ,
t h e o t h e r h a n d , i n w h i c h t h e s wa y i n g
of the
s i m ple
commu n i c a tion) b a s c o n ­
tech n i q u e to regis t e r t h i s d e v i a t i o n :
o n e o u t s t re t c h e d h a n d s h e h o l d s a p e n c i l a n d m o v es
i t fro m r i g h t to l e ft
body
and
b a c k to r a b o u t 1 cm o n p a p e r
th a t i s m ov i n g a t a c o n s t a n t sp e e d . I n th i s w a y d e v i ­
a t i o n c a n b e reg i s t e r e d [o r v a r i o u s h e a d p o s i t i o n s
(Figure
p Cll i e n t' s b a c k l e a n i n g, a ga i n s t a c h a i r , o n l y s i d e
on
a
t b e p a t i e n t i s se a ted a s b e fo r e , w i t h eyes c l o s e d : i n
Th i s t e s t h a s t w o g r e a t a d v a n t a g e s : b e i n g s e a t e d
a n d p ropped
kg.
M . B erger ( p e rso n a l
4.44 ) .
T h e re is
s u b t l e d i ffe r e nce b e t w e e n t h e s i m p l e
a
H a u ta n t ' s t e s t
deviation:
in
and
B e rg e r ' s m e t h o d of regi s t e r i n g
t h e fo r m e r
both
hands
a re
tested
w i t h eyes shut i s t e s te d , the c h a nge in the d i re c t i o n
fo r d e v i a t i o n , a n d i f t h e re i s o n l y d i ve rge nce
o f s w a y i n g t h a t occurs i n h e a d r o t a t i o n ( fo r w a r d s o r
co n v e rg e n c e , t h e r e s u l t
backwards)
i s i n t e r p r e t e d a s t h e re s u l t o f l a b y r i n t h
i m b a l a nce , t h e p a t i e n t s w a y i n g i n t h e d i rec t i o n o f
the
laby r i n t h .
a ffe c t e d
d e v i a t io n t h a t t a k e s p l a c e
[n
Hauta n t 's
whe n
test,
any
t he patie n t turns h e r
h e a d i s t h e r e s u l t o f t h e h e a d pos i t i o n re l a t i v e t o t h e
trun k .
i.e.
t h e pos i t i o n o f t h e ce r v i c a l s p i n e . W e c a n
t h us d i s t i n g u i s h p a t h oge n i c a n d re l i e f p o s i t i o n s o f
the
head,
i.e.
pos i t i o n s
that
cause
or
fo u n d
rea c t i o n
to
i n t h t; n e u tra l
pos i t i o n . I n
fa c t , t h e
c h a nged
p os i ti o n
c a s t; s
h e <1 d
in
of
one h a n d
n e g a ti v e .
Devia tion
or
is
d e v i a te s t o t h e s i d e w h i l e t h e
ot h e r re m a i n s i n n e u t ra l p o s i t i o n , beca use i t i s t h e
d e v i a t i o n o f t h e c e n t re p o i n t b e t w e e n b o t h a r ms
which
co u n ts.
However,
in
w r i t i n g h a n d d e v i a t e s th e re
whether
the
d i re c t i o n ,
or
i n c re a se
d e v i a t i o n , a n d t h ose t h a t a bo l is h d e v ia t i o n if it h a s
been
di agnosed jf
is
D iagnosis
ation
other
hand
B e rg e r ' s
is no
if
the
i n the same
(d i ve rge nce).
r e v e rsed ) if d e v i ­
d e v i a te s
to t h e o p p o s i t e s i d e
is
test,
w a y of k n o w i n g
corro b o r a ted (or
d i s a p p e a rs ( o r p e r s i s ts ) a fter tre a t m e n t .
I t i s n ec e s s a ry t o d is t i n gu i s h be t w e e n d i s t u r b a n c e
of
ba l a n ce c a u s e d b y t h e p o s i t i o n
Copyrighted Material
of
the neck , and
120
Manip l liative Therapy
in Rehab ilitation of the Locomotor System
9
f
Figure 4.44 C e r v i cove r t i gogr a m (by c o u r t e s y of B e rge r ) :
in v a r i o u s pos i t i o n s , w i t h e y e s
t h e p a t i e n t holds t h e h e a d
c l o s e d , a n d m a k e s osci l l a t ory move m e n t s wi t h t h e
o u t s t re tc ll e d a r m s ; these move m e n t s a re recorded b y
p e n ci l on a mov i n g s t r i p o f p a p e r . ( 1 ) D u ri n g h e a d
o w i n g to d i sease, sy mptoms w i l l occ u r . T h e test i s
c a r r i e d o u t w i th the p a t i e n t s u p i n e , h e r he a d i n
re troflexion over the e n d of the t a b l e . T u rn i n g the
head fi rst to one side and t h e n to the other, we
e x a m i n e nystagmus in e n d-posi tion a nd watch the
p at i e n t for symptoms of d izziness, na usea , etc. Th is
te st i s particu l a rly conclusive i f there is n o m o v e ­
men t restriction i n the position that ca uses symptoms,
thus ruling out blockage as t h e i r possi b l e cause. For
d i agnostic pu rposes it may the refore be n ecessary to
treat move m e n t restrict i on (e.g. if left rota t i o n i n
retroflexion is restricte d a n d ca uses symptoms) a n d
t o repeat the test a fter m o b i li ty has been restored.
If the sym ptoms do not recur, then they were due
to the move m e n t restrictio n ; i f they persist, then
they a re d u e to vertebral a rtery i ns u ffic i e ncy (in this
case, o n the left) .
T h e pos i t i o n of t h e p a ti e n t d u ring de Kley n ' s t e st
m a y sometimes cause posit i o n a l ver tigo; this is a
benign cond i t i o n , n o t to be con fused with vertebral
artery i n s u fficiency, w h ich is serious. T h e d istinction
ca n be m a d e by repeating the test; i n positional
vertigo t h e re is a ' t r a i n i ng' e ffect so t h a t no ve rtigo
is p rovoked at the second o r t h i rd repe t i t i o n o f t h e
t e s t . The con d i t i o n a l so disappears a fter a few
seconds, even if t h e test position is m a i n ta i ned . I n
true vertebral artery insufficiency i f the de Kleyn test
i s positive the patient's con d ition gets worse owing
to ischaemia i f she maintains the test position w h i c h i n v o lves conside rable risk.
rot a t i o n to t h e r i g h t ( r ) there is d e v i a t i o n to t h e left ;
w i t h t h e h e a d s t r a i g h t ( g ) the a r m
returns to m i d ­
pos i t i o n ; a n d d u r i n g h e a d rot a t ion to t h e l e ft ( I ) t h e r e i s
no d e v i a t i o n . ( 2 )
A ft e r t r e a t m e n t of r e s t ri c t e d r o t a t i o n of
t h e occiput/atl a s t o t h e r i g h t , t h e r e i s no l o n g e r a n y
d e v i a ti o n
disturb a nce due to the position of the head with the
rest of the body i n space, i . e . to laby r i n t h i n e l e s i o n s .
To m a k e t hi s d istinction w e must ch a n g e the position
o f the p a t i e n t's head and tr u n k s i m u l t a neo u s l y
( s i t ti n g u p , l y i n g down, t urni n g from o n e side to the
other) to d e term i n e w h i c h position causes ve rt igo .
This type of v e rt i g o is u s u a l ly v e ry i n te n s e b u t o f
s h o rt d uration, so that it is enou g h to watch t h e
patien t s reactio n . W e s h o u l d , however, i n sist o n t h e
p a tien t k e e p i n g h e r e y e s o p e n w h ile c h a nging
posi tion; we c a n the n o b s e rve s p o n t a n e o u s n ystag­
mus, which u s u a l ly lasts o n l y a few seconds. (The
pati e n t w i l l alwa y s tend to close her eyes in t h i s type
of v e r tigo . )
T o d e t e r m i n e the r o l e of the verte b r a l a r t e r y i n
vertigo, d e K l e y n ' s te s t s a re u sefu l; here, too, it i s
the posit ion of t h e h e a d r el a ti v e t o t h e tru n k that is
decisive, i . e . neck positio n . If t he head is b e n t back
a n d rotated to o ne sid e , blo o d flow i s impa ired in
t h e vertebra l artery o n the side away from w h i c h the
head is t u r n e d . Hence, i f t h e vertebral a rtery o n t he
s i d e towa rds w h i c h t h e head is t u r n e d is insuffici e n t
'
Exa m i nati o n of d i stu rbed m uscle
f u n ct i o n
The great d ifficulty here is t h a t there is no exact
delimitation of what i s to be considered norm a l , a n d
diagnosis must b e b a s e d a l most exclusively on
c l i n ical e x a m i n a t i o n . Polymyoelectrography using
s urface electrodes i s so cumbersome that its use is
very l i m i ted.
Clinical k i n esiological e x a m i n a t i o n should com­
prise:
1. N e u rological screen i ng.
2. Examination of m uscle strength ( musc le tests) .
3. Exa m in a tion of s hort m uscles, fascia e , etc.
4 . Exa m i n a tion of hypermobility.
5 . Examin a t ion of posture standing a n d sitting.
6 . Exa m i n a t i o n o f s i m ple movement.
7 . Examination of gait with vari a t ions such as
walking o n tip-toe, on the heels, with a r m s raised,
etc.
I n the n e u ro l ogical e x a m i nation the signs of
speci a l i n te rest a re those c h a racteristic of m i n i m a l
b rain dysfunction: m ar ked asymmetry i n particular
of the face and t h e extrem ities, restlessness, c l u msi­
n e s s , etc.
Copyrighted Material
Exam ination
M u scle
tes t i n g
was
origi n a l ly
i n t ro d u c e d
of locomotor function a n d its
disturbance
121
to
exa m i n e p a r e s i s of i n d i v i d u a l m u s c l e s or of m u s c l e
g r o u p s i n s u c h d i s e a s e s a s p o l i o m ye l i t i s . Esse n ti a l l y ,
m u scle s t r e n g t h i s e x a m i n e d i n t h e course of s i m p l e
coord i n a te d m o v e m e n ts which m a k e i t poss i b l e to
exam i n e o n l y one sp e c i fi c m u s c l e or m u s c l e g r o u p .
S t a n d a rd c o n d i t i o n s m u s t be m a i n ta i n e d . so t h a t
Results are g r a d e d a s
res u l ts a r e c o m p a r a b l e .
fol l ows:
O . N o m uscl e a c t i v i t y a t a l l .
l . M u scle t w i tch w i t h o u t l o c o m o t o r e ffe c t .
2. Mov e m e n t w i t h exclusion of g r a v i t y ( i . e . o n l y i n
t h e h o r i zo n t a l p l a n e ) .
3. M o v e m e n t aga i n s t g r a v i t y b u t n o t aga i n s t
4.
(a)
a d d i t i o n a l resi s t a n c e .
5 . The a b i l i ty to p e r fo r m m o ve m e n t
resistance : (4) a gai n s t l i t t l e r e s i s t a n c e , ( 5 )
and
a ga i n s
t
normal
m u sc l e a c t i v i t y .
Beca u s e , i n o u r p a t i e n t s
t r u e p a re s i s i s fo u n d
,
o n ly i n r o o t sy n d ro m e s . c h a nges a r e u s u a ll y fo u n d
b e t w e e n gra d e s
4
and
5,
a l tho ugh t h e a b d o m i n a l
m u s c l e s a n d d e e p n e c k fl e x o r s m a y e x h i b i t g r ad e
Thus the distinction between grades
4
and
5
3.
is not
fm e e n o ugh f o r o ur p u rpose .
W i t h o u t go i ng
i n to deta i l s
a b o u t m u scle t e s t i n g . i t
i s esse n t i a l t o stress t h e fo l l o w i n g p ri n c i p le s : the
pos i t i o n o f t h e p a t i e n t m us t b e c o n s t a n t ; fi x a tio n ,
because t h i s d e t e r m i n e s w h i c h m u s c l e s t h e p a t ie n t
b r i ngs i n t o p l a y ; d i re c t i o n . s p e e d a n d re s i s t a n c e m u st
be c o n s t a n t t h ro u g h o u t t h e m o ve m e n t . I s o m e t r i c
(b)
e x a m i n a t i o n c a n re ve a l t h e d e g r e e o f force i n the
muscle but
not i m po r t a n t
fa u l ts o f coord i n a t i o n .
For t h e t y p e o f d i s t u rbance t o b e e x pected i n o u r
p a t i en ts i t i s n e c e s s a r y to m o d i fy t h e origin a l m u scle
test i n some p a r t i c u l a rs ; the most i m po r t a n t tech­
n iques are descr i b e d here.
In
the section o n
disturbed
move m e n t patterns I have distinguished those m u scles
with a te n d e n c y to we a k e n ( , pred o m i n a n t l y p h a s i c
m u scles ' ) a n d tho se w i t h a t e n d e ncy to h y peractivity
( ta u t n e ss
-
'
pred o m i n a n t l y postu r a l m us c l e s ' ) a ft e r
J a n d a ( 1 972) .
Exa m i n ation o f m uscles te n d i n g to
wea kn ess
G l uteus maxi m u s
B e fore
examine
pe rfo rm i n g
(Figure
the
4 .45)
'classic'
( h y per)extension
of
m uscle
the
hip,
test
we
with
the
p a t i e n t p r o n e , i n o r d e r to d i agnose t h e
( c)
Figure 4.45 Exa m i n a t ion of t h e g l u t e u s m a x i m u s by
dors i fl e x i o n ( h y p e rt e n s i o n ) of the h i p : ( a ) w i t h the l e g
s t r a i g h t ; ( b ) w i t h the l e g fl e x e d ; ( c ) w i t h t h e l e g in
e x t e rn a l rota tion
p a t te r n .
we a k er t h a n on the h e a l t h y s i d e , a n d may even b e
Ele ctro m y o g r a p h y h a s es t a b l ished t h a t t h e p r i m e
a b s e n t - y e t t h e strengt h of h i p e x t e n s i o n n e e d n o t
reduced .
movers i n h i p e x t e n s i o n a re t h e h a m s t r i ngs, fo l l o w e d
be n o ticeably
a l most i m m e d i a t e l y b y t h e g l u t e u s m a x i m us a n d t h e
o f t h e l u m b a r e rec tor s p i n a e w i t h m a rk e d h y p e r­
erector
spinae.
It
is
advisa b l e
to
palpate
the
h a m s t r i ngs a n d g l u t e us w i th o n e h a n d a n d t h e t w o
lumbar
e rectores
spinae
g l u t e us m a x i m u s is w e a k ,
with
the
other.
con traction
If
th e
i s r e t a rd e d ,
I n v e ry m a r k e d o v e r a c t i v i t y
t o n u s , e v e n w i th t h e p a t i e n t p ro n e , t h is m u s c l e m a y
c o n t r a c t fi r s t , before
t h e h a mstrings. I n the
most
s e v e re l y c h a n g e d m o tor p a t te r n s m u scu l a r c o n trac­
tion may start
Copyrighted Material
at
the upper part o f the t r a p e z i u s .
i 22
Mal1 ip ll/rilive Th erapy in Rehauili/(ll;ol1 or [he LocumolOr System
T h e m u s c l e test p r o p e r is p e r fo r m e d w i t h t h e
p a t i e n t p r o n e , h e r k n e e fl e x e d so as to i n h i b i t t h e
h a m s t r i ngs. Resista nce i s a p p lied against t h e t h i g h ,
a b ove the k n e e , t h r o u g h o u t t h e m o v e m e n t . I f w e
w i s h t o faci l i tate t h e g l u te u s m a x i m u s to t h e gre a test
e x t e n t , we ex a m i n e h y pere x te n s i o n o f the h i p w i th
t h e l e g i n e x t e r n a l rot a t i o n .
G l ut e u s m e d i u s ( F i g u re 4 . 46)
W e fi rst ex a m i n e s p o n t a ne o u s a b d u c t i o n o f the h i p
w i t h t h e p a t i e n t l y i n g o n h e r s i d e . t h e u n d e r leg
s l i g h t l y bent a t t h e k n e e a n d hip. Fi r s t we observe
t h e patient to see w h e t h e r s h e m a k e s a t r u e
abd u c t i o n , o r a combi ned movement rota t i n g t h e leg
o u t w a rd s w h i l e
fle x i ng t he
(a)
h i p . T r u e a b d uct i o n
e m p l oy s b o t h t h e t e n s o r fasc i a e l a t a e a n d t h e
abd uctors (glutei medii and minim i ) , and the
co m b i n e d m o v e m e n t i s p r o d u c e d m a i n l y by the
t e n sor fa s c i a e l a t a e . I t i s t h e refore a d v i s a b le to
p a l p a t e the te n s o r fasc i a e l a t a e w i t h one finge r a n d
t h e g l u t e u s m e d i us w i t h a n o t h e r , to s e e w h e t h e r
b o t h c o n tract d u r i n g a b d u c t io n . I f t h e r e i s o u tw a rd
rot a t i o n a n d h i p flex ion ( i n c o or d i m l t i o n ) t h e g l u t e u s
m e d i u s i s co n t r a c t i n g t o o l a t e . t o o l i t t l e , o r n o t
a t a l l . D u r i n g t h e m u sc l e t e s t t h e req u is i te resis t a nce
is given aga i n s t the l o w e r t h i rd o f the t h i g ll from
t he pe l v i s i s fixed in such a way
t h a t i n c oord i n a t i o n is preve n t e d . Even then one
s h o u l d p a l p a te t h e c o n t r a c t i o n o f both t h e t e n sor
the
s i d e , and
fa s c i a e l a t a e and
( b)
t h e g l u teu s med i u s , and w a tch
fo r u n d e sira b l e c o n t r a c t i o n o f t h e q ua d r a t u s l u m­
boru m .
Rectus a b do m i n i s ( Fi g u r e 4 . 4 7 )
The u s u a l t e s t o f t h e re c t u s a b d o m i n i s i s fo r t h e
p a t i e n t to s i t u p f r o m t h e s u p i n e posi t i o n , w i t h fl e x e d
k n e e s : to ' c u rl u p ' , l i ft i n g fi rs t t h e h e a d , t h e n t h e
s h o u l d e r s a n d t h e n t h e rest o f t h e t r u n k , w i th t h e
opera t o r fi x i n g t he fee t a nd p e l v i s . F o r o u r p u rposes
it is b e t t e r if the p a t i e n t flexes her l e gs and s i ts u p
u n a i d e d w i t h a r m s s t re tched forw a r d .
T h i s c a n o n l y be d o n e i f t h e a b d o m i n a l m u scles
a re f u n c ti o n i n g well - if these m u s c l e s a re very
s t ro n g the p a t i e n t may be a b le t o sit u p w i t h h e r
b a n ds h e l d b e h i n d h e r h e a d . A l t h o u g h b e nd i n g t h e
l e g s i n h i bi t s the h i p fl e x o rs t o s o m e d e g r e e . s i t t i n g
u p i s a l w a y s t h e re s u l t o f coord i n a te d s y n e rgy o f t h e
a b d o m i n a l m u scles a n d t h e h i p fl e xors. To e x a m i ne
t h e rec t i a b d o m i n i s a l o n e . t h e exa m i n e r p u t s h is
h a n d s u n d e r t h e h e e l s of the s u p i ne p a t i e n t . t e l l i ng
h e r to press t h e h e e l s d o w n w a r d s . S h e is t h e n told
to l i ft her head. s h o u l de r s and tfunk , i n success i o n :
t h e m o me n t t h e pa t i e n t s t a r ts u s i ng t h e h i p fl e x o rs .
t h e p ress u re of h e r h e e l s o n t h e e x a m i n e r ' s h a n d s
c e a s e s . T h e s t r o n ge r t h e a b d o m i n a l m u s c l e s . t h e
h i g h e r t h e p a t i e n t c a n l i ft h e a d a n d s h o u l d e rs
w i t h o u t re l a x i n g the p ress u re of t h e h e e l s .
( c)
Figure 4.46 Exa m i n a t ion of h i p abd u c t i o n w i t h t h e p a t i e n t
s i d e (gl u teus m e d i u s and m i n i m us ) : ( { / ) p u re
abduct i on correc t l y c a r r i e d o u t : ( b ) fillsc a b d u c t ion by
s u b s t i t u tion hy t h e h i p fl e x o r s . p a r t icu l a r l y by the t e n s o r
fasc i a e i a t a e : (c) t h e ' c l a s s i c ' t e s t f or t h e a h d u c t ms ( t h e
e x a m i n e r p <l l r <l t i n g t h e t e n sor fas c i a e I ;n � e w i t h t h e
fi n ge rs a n d (' h e g l u t e u s m e d i u s w i t h t h e t h u m b )
o n 11er
Lower p a rt o f the tra pez ius ( F i g u re 4.48)
To test t h i s m u sc l e t h e p a t i e n t m Li s t b e p ro n e . w i t h
t he arm
on
t h e t e s ted s i d e s t re t c h e d fo rward . W i t h
o n e h a nd t h e e xa m i n e r g rasps t h e o u t s t r e t c h e d a nn
a bove t h e e l bo w . w h i l e t h e o t h e r g r a s p s t h e i n fe r i o r
Copyrighted Material
EX(Jminali(J/1 of /ucOI1lOllJr fl lllC/ion a ll d ils dislllriJa n ce
1 23
t h e i n fe r i or sca p u l a r a n gle is s u f fi c i e n t to preve n t t h e
o u r p u rposes , i , e , t o
d i a g n o s e i n co o rd i n a t i o n , me re i n specti o n is u s u a l l y
s u ffi c i e n t : w e te l l t h e pro n e p a ti e n t to p u l l o n e
s h o u l d e r d o w n ( i n a c a u d a l d i re c t i o n ) I f t h i s m o v e ­
m e n t is carried o u t correctly, t h e i n fe rior sc a p u l a r
a n g l e moves i n a c a u d o me d i a l d i rection ( i , e , i n t h e
d i r e c t i o n of t h e fi b re s of the l o w e r t ra pezi u s m u sc l e ) ,
I f t h i s m u s c le is w e a k , howeve r, t h e i n fe ri o r s c a p u l a r
a n gle m o v e s med i a l l y l i ke a h o o k a n d p r o t r u d e s
u n d e r t h e s k i n , n o t u n like a n a l a r s c a p u l a , Th is i s
w h y the c a u d a l m o v e m e n t , usua l l y force fu l , c a n b e
s o e a s i ly preve n te d b y t h e e x a m i n e r ' s h a n d ,
s c a p u l a f r o m m o v i n g d o wn , F o r
.
Serratus a n terior
This m us c l e i s t es t e d with t h e patient o n a l l [o u rs ;
ca re m u s t b e t a k e n t o s e e t h a t s h e p u ts he r weigh t
n o t on h e r k n ee s b u t on h e r a r ms, a n d t h a t t h e
s h o u l d e rs are abd u c ted , The p a t i e n t i s w a t c h e d t o
see w h e t h e r an a l a r sca p u l a appears, To m a ke t h e
test m o r e d i ffi c u l t , t h e pati e n t may be t o l d to b e n d
h e r e l bows, Al though t h i s test c o n c e r n s m a i n l y the
serra t us a n t e ri o r i t i s a l s o affected by a we a k l o w e r
p a r t o f t h e tra p ezi u s , I f w e a k n e s s o f the serratu s i s
only s l igh t we m a y de tect a n alilr scap u l a e v e n b e t te r
w h e n the p a ti e n t h o l d s h e r il r m s h o r i zo n t a l l y
o u tstretc h e d for some t i m e ,
,
D e e p flexors o f t h e neck ( Figure 4.49)
test t h ese m u scles t h e p a t ie n t is supine and i s
to l d t o p u l. 1 h e r c h i n t o w a r d s h e r c h e s t i n a n a rc h i n g
m o v e m e n t Th e e x a m i n e r fi x e s t h e p a t i e n t ' s c h e s t
w i t ll o n e h a n d w h i l e t h e o t h e r , o n h e r fo re h e a d ,
res ists tle x i o n o f t h e h e a d a n d n e c k Th is m o v e m e n t
m u s t b e ca r e f u ll y distinguished fro m t h il t o f the
p a ti e n t pu s h i ng h e r h e a d fo r w a r d , w h i c h wi l l u s u a l l y
h a ppen i f t h e d e e p fl e x o rs a re w e a k ( i n c o o rd i n a ­
t i o n ) , b r i n g i n g i n to pla y t h e s t e rn o c l e i d o m a s t o i d s
a n d a l so t h e s c a l e n e s , T h e re i s a usefu l q u a n t i ta t i v e
To
.
Figure 4.47 E x a m i n a t i o n of t h e rec t u s a b d o m i n i s : t h e
p a t ie n t s i t s u p w i t h Ile x e d k n e e s , w i t h o u t fixa t io n :
( a ) 'exce l l e ll t ; ( iJ ) n o r m a I s t r e n g t h
,
'
Figme 4.48 E xa m i n a t i o n o f the l o w e r p a rt o f t h e
t r a p ez i u s : t h e p � t i e ll l m o v e s the s h o u l d e r- b l a d e a c t i v e l y ,
i n a c a u d a l d i rect i o n ( a ga i n s t r e s i sl o n c e )
a n gle o f t h e scap u l a
t e l l i n g t h e p a t i e n t to pull h e r
a n d s h o u l d e r d o w n : t h e e x a m i n e r r e s i s ts t h i s
move m e n t w i t h bot h h a n d s a n d i f t h e l o wer
t r a p e z i u s i s wea k , t l J e r e s i s t a n c e of t h e h a n d h o l d i n g
,
arm
,
Figure 4.49 Exa m i n a t i o n o f t h e
Copyrighted Material
deep n e c k fl e x o rs
1 24
Manip u lative Therapy
ill R ehabilitation of the Locomotor Systenl
test : we ask t h e p a t i e n t to l ie w i t h h e r head raised
as t h o ugh i n te n d i ng to read ( w i t h o u t l i fting the
t h o r a x ) . N o r m a l l y this posi t i o n can be m a i n t a ined
for h a l f a min ute or even l o n g e r b u t pa t i e n ts w i t h
w e a k dee p n e c k fle xors can h o l d i t for o n l y a few
sec o n d s .
,
Exa m i n ati o n of s h o rt (ti g ht)
m u sc l es
We have a l re a d y seen w h i c h m u scles te n d to shorten
t h e ' p red o m i na n t l y p o s t u r a l m us c l e s ' o f J a n d a
( 1 972). I n p ri n c i p l e we observe how f a r a m u s c le c a n
b e stretc hed w i t h o u t the use of fo rce: as t h is is done
m a i n l y by t h e same m a n o e u vres as post is o met r i c
r e l a x a t i o n , o n l y t h ose tech n i q ues t ha t d i ffe r a re
described here.
-
-
Tri ceps surae (soleus)
I f t h i s m uscle is shorte n e d , d o r s a l flexion of the a n k l e
j o i n t i s restricte d . This ca n be tested by a s k i n g the
p a t i e n t t o s q u a t d o w n : i f t h e t r iceps surae (soleus)
i s n o rm a l , s h e should be able to p l a c e the w h o l e foo t
o n t h e floor, i n c l u d i n g the hee l , b u t if the so l e us is
shortened, t h e heel w i l l n o t t o u c h t h e fl oor ( Fig u r e
4.50). I f, however, it is only the gas t roc n e m i u s t h a t
i s s h o r t e n e d a s is freq u e n t l y t h e c a s e dorsiflexion
o f t h e a n k l e joint will be red u ced i f t he knee is
stretched and i n c reased i f s h e flexes t h e k n e e ( Figure
4 .5 1 ) . For this reason i t is a mistake to ex a m i n e the
m obi l i ty o f t h e ankle j o i n t with t h e kn e e s e xten de d
,
( a)
,
.
H a mstr i ngs
The h a m stri ngs a re tested t h e s a m e way as i n the
s t r a i g h t l e g raisi ng test. The l e g t hat is not being
e x a m i ned s h o u l d be fixed to the t a b l e from a bove.
The h amst r i ngs a re considered s hortened i f t he
s t re tched leg c a n n o t be raised to an a ngle of 80
degrees fro m the horizo n t a l . N o te t h a t i f the legs a re
o u tstretched t h e l u m b a r s p i n e is n o t i n a neutral b u t
i n a lordotic position. Therefore if we w a n t t o
p e rfo rm t h e st r a i g h t leg r a i s i n g t e s t f ro m a n e utral
pos i t i o n , t h e leg w h ich is not examined is bent a t t h e
h i p a n d t h e k ne e , with the foot o n t h e t a b l e . In th is
case straight leg raising to 90 degrees s h o u l d
normally be expecte d . U nl i k e i n t h e straight l eg
raisi n g test for root syndromes, the p a t i e n t feels onl y
t h e stretch u n d e r t h e k n e e , b u t no real p a i n . This is
the m o s t freq u e n t reason why a s u bject cannot touch
the floor when be n d i n g fo rward with s trai g h t le g s .
H i p flexors ( Figure 4 . 52)
Th e se co m p r i s e
the i l i opsoas, t h e rect u s fe moris a n d
t h e tenso r fasc i a e latae. They a r e exa m i ned i n t h e
p os i t i o n for M e n n e l l 's t e s t s . The patie n t is s u pine
( b)
Figure 4.50 Scre e n i n g t e s t fo r s h o r t e n i n g of t h e s o l e u s :
t h e patient squats. (a) N o r m a l ; (b) shortened (the heel
d oes n o t t o u c h the fl o o r )
with the b u ttoc k s a t t h e ed g e o f the table, t h e leg of
the exam i n ed s i d e h a n g i n g o v e r t h e edge. The
p a t i e n t grasps t he flexed knee o f t h e o t h e r l e g a nd
draws i t to w a rd s her chest close e n ough to fl a t t e n
l u m b a r lordosis. I n t h i s position i t is possible to
Copyrighted Material
Examination
0/ locom% r fllnction and i t s disturbance
1 2S
Figure 4.51 ( a ) E x a m i n a t i o n of d o rs i fl e x i o n of t h e fo ot
leg stre tched; (b) w i t h k n e e b e n t . M a r k ed i n c r e a s e
i n d o r s i fl e x i o n w i t h t he k n e e b e n t i s c h a ra c t e r i s t i c of a
with
s h o r t ga s t ro c n e m i u s
assess t h e relev a n t c h a n g e s by i n s p e c t i o n : if the
i l i o p s o a s is s h o r t e n e d , t h e knee of t h e leg h a n g i n g
o v e r t h e e d g e o f t h e t a b l e wi l l be r a i s e d i n s t e a d of
being b e l ow or o n t h e leve l o f t h e p a t i e n t s h i p . I f
t h e rec t u s fe moris is s h orte ned , t he k n e e w i l l show
too l i t t le fl e x i o n ; i f the te n s o r fasc i a e l a t ae is
sh orte n e d , the leg w i l l be s l i g h t l y a b d u c t ed and t h e
pat e l la d e v i a t e d slightly o u t w a r d .
T h e e x a m i n e r c a n now pro c e e d to cons i d e r e a c h
m u scle , w i t h t h e p a t i e n t i n t h e s a m e p o s i ti o n . W i t h
one h a n d h e r e i n fo rc e s t h e fixation o f t h e k n e e ( h e l d
i n t he p a t i e n t ' s t w o h a nds) a n d t h e n ( I ) e x e r t s
press u re on t h e o t h e r k n e e from a b o v e in o r d e r t o
dete r m i n e t h e exact e x te n t o f s h o r te n i n g o f t he
iJ iopsoas ; ( 2 ) i n c r e a se s fl e x i o n of t he k n e e of t h e free
l eg (over t h e ed ge o f t h e ta b l e ) o r t e l l s the patie n t
t o fl e x i t a c t i ve l y - i f t h e rectus fe moris i s s h o r t t h e
k n ee w i l l i m m e d i a tely rise a b o v e t h e h o rizon ta l ; a n d
( 3 ) t h e exam i n e r wi l l t ry t o a d d u c t t h e k n e e . I f t h e
t e ns o r fasc i a e l a t a e is s h o rte n e d t h e re i s i m m e d i a t e
re s i s t a n c e to adducti o n , a n d the i l i o t i b i a l tract can
be seen to f o r m a groove o n t h e l a teral a s p e c t of the
t h igh by tighte n i ng.
'
( c)
Figure 4.52 E x a m i n a t i o n of the h i p fl e x or s : t h e p a t i e n t i s
s u p i n e w i t h h e r b u t tocks a t t h e e n d o f t h e t a b l e ; she
p u l l s one bent knee to the a b d o m e n . t o fl a t t e n l u m b a r
l o r d os i s , w h i l e t h e l e g t o be t e s t e d h a n gs o v e r the e d g e
o f t h e t a b l e . ( a ) The e x a m i n e r n o t es w h e t h e r t h e t h i g h i s
r a i s e d a b o v e t h e horizo n t a l a n d w h e t h e r t h e re i s
e x t e n s i o n o f t h e k n e e ; ( b ) b y pre s s u re o n t h e k n e e fro m
above he tests s h o r t e n i n g of t h e i l iopsoas; (c) be n d i n g
t h e k n ee p r o d u c e s h i p fl e x i o n i f t he rect us fe moris i s
short
The ( l u m b a r ) e rector spi n a e ( Figure 4 . 5 3 )
T h e r e is a s i m p l e t e s t for o ri e n ta t i o n : t h e s e a te d
p a t i e n t is told to draw h e r for e h e ad to h e r k n ees.
Th is i s h i n d e re d by a sh o r te n e d e re c t o r s p i n a e , but
t h e re a re m a ny fa c to rs t h a t m a y i n v a l i d a te the test:
Copyrighted Material
Manipulative Th erap v in Reh((iJ ili({/tion of tile LocoJllotur Sv;·tem
l 26
figure 4.54
t h e q u a d ra t u s l u m b o r u m : t h e
l i ft i ng t h e u p p e r p a ri o f h e r
b o d y b y a d d u c t i n g t h e e l how ( t h e pe l v i s m u s t n o t be
l i fted a n d may he fixed hy the e x a m i ne r)
Ex a m i n a t i o n o f
pa t i e n t l i e s o n
he r
side.
me n t t h e p a t i e n t l i e s o n h e r s i d e a n d l i fts t h e u p p e r
p a rt o f h e r body by a d d u c t i ng t h e e l h o w a n d s i d e ­
be n d i n g t h e t r u n k . C a r e m u s t b e ta k e n to see t h a t
d o e s n o t l i ft h e r p e l v i s , wh i c h i s b e s t fi x ed f r o m
exa m i n e r.
T h e tec h n i q u e of e x a m i n a t i o n of t h e pectora l e s ,
u p p e r t r a pe z i u s a n d l e v a t o r s c a p u l a e i s i d e n t i ca l t o
re l a x a t i o n t re a t m e n t , a n d is d es c r i b e d i n t h e r e l e v a n t
c h a p t e r . A t i n spection a s h o r t pectora l i s i s s h o w n by
rou n d or forwa rd-d rawn s h o u l d e rs , w h i l e h y p e r ton u s
of t h e u p p e r p a r t of t h e t r a p e z i u s is r e v e a l e d by t h e
she
a b o v e by t h e
Figure 4.53 E x a m i n a t i o n of s h o r t e re c t o r e s s p i n a e . t h e
p a t i e n t s i t t i n g . w i t h k n e e s bent : ( a ) d r a w i n g t h e fo re h e a d
t o t h e k n e e s : ( iJ ) h u m p i n g h e r b a c k w h i l e fix i n g t h e
p e ly i s w i t h h e r h a n d s
u pw a rd
convex
' G o t h i c ' s h a pe o f t h e s h o u l d e rs
( F i g u re 4 . 5 5 ) .
F o r ra p i d asse s s m e n t o f b o t h u p p e r tra p e z i i a n d
t h e o t h e r n e c k e x t e n sors , t h e s i m p l e s t test
i f t h e p a t i e n t h a s a s h o r t tr u n k a n d l o n g t h i g h s s h e
w i l l p e r fo r m t h e move me n t e a s i l y even w i t h a short
e r ec t o r s p i n a e ; con verse l y . i f h e r t r u n k i s l o n g a n d
th ighs s h o r t , s h e w i l l fa i l e v e n w i t h a n o r m a l e rector
s p i n a e . I t h e re f o r e p re fe r a m o d i fi c a t i o n of the tes t :
t h e p a t i e n t se a t e d . fi xe s h e r pe l v i s b y p l a c i n g the
h a n d s o n t h e i l i ac crests, and s i m p l y h u m p s her
s p i n e . If t h e l u m b a r part o f t h e e r e c to r s p i n a e is
the
pa ti e n t s c h i n t o h e r c h e s t . I f
'
is to
d ra w
the n e c k e x t e nsors
<l r e s h o rt . a g a p o f one o r t w o ( o r eve n t h ree ) fi n ge r s '
b re a d t h re m a i n s . S h o r t n e c k e x t e n s o rs a r e t h e most
fre q u e n t c a u s e o f i n a b i l i t y to b r i n g t h e c h i n d o w n
on to t h e c h e s t .
.
s h o rte ned, n o l um b a r k y p h os i s is o b t a i n e d .
C l i n i c a l l y n o l e ss i m porta n t t h a n a s h o r t e n e d
e r e c t o r s p i n a e i s hypertonus of t h i s m u sc l e e s p e c i
a lly i n t h e thoraco l u m b a r region ; it is m ost often
fo u n d i n p a t i e n ts w i t h i nc r e a s e d l u m b a r l o r d o s i s I t
m a y b e s e e n w h e n t h e p a t i e n t s t a n d s re l a x e d , a n d
d i s a pp e a r o n r e t ro fl e x i o n ( fi rs t degre e ) : i t m a y b e
fo u n d o n re t r o fl e x ion a o d d i sap p e a r w h e n the
p a t i e n t i s prone (second d e g r e e ) ; i n t h e m o s t s e v e re
c a ses it is fo u n d e v e n whe n the pa t i e n t is p ro n e .
T h e s e a re t h e c a s e s i n w h ic h h i p e x t e n s i o n from t h e
p r o n e p o s i t i o n i s i n i ti a t e d b y t h e e r ec t o r s p i n a e .
.
­
.
T h e q u a d ra t u s l u m b o r u m ( F i gure 4 . 5 4 )
The state of
t h i s m uscle c a n
be a s s e s s e d
while
the
p a t i e n t b e n d s s id e w a y s . b u t d i ffe r e n c e i n l e g l e n gth
m u s t of co u rs e , be r u l e d out fi r s t . For e x a c t a s s e s s .
E xa m i n at i o n of h y p e r m o b i l ity
( ra n g e of m ovem e nt)
N o t o n l y w e a k n e ss a n d t a u t n e s s , b u t h y p e rm o b i l i t y ,
too, i s m a i n l y t h e c o n s e q u e n c e o f m u sc u l a r a c ti v i t y
is d e t e r m i n e d b y t h e m u s c u l a r s y s te m . T h e s i g n i fi
c a n ce of hypermo b i l i t y fo r p a t h og e n e s is h a s a l re a d y
b e e n p o i n ted o u t ; h e re we a re concerned o n l y w i t h
e x a m i n a t io n a n d d i a gn os i s .
T o S a c h s e ( l 969) goes t h e c r e d i t for e l a b o r a t i n g
g u i d e l i n e s fo r t h e a s s e ss m e n t o f nor m a l r a n g e o f
move m e n t , a n d fo r a t te m p t i n g t o d e t e r m i n e t h e
c o n c ep t s o f h y p o m o b i l i t y , a v e r a ge m o b i l i t y a n d
hyperm o b i l i ty , a l l w i t h i n t h e ra nge o f t h e normal. I t
is, n e v e r t h e l e s s , i m po rt a n t t o b e a r i n m i n d the gre a t
v a r i a b i l i t y n o t o n l y b e t w e e n i n d i v i d u a l s , b u t a ls o
a c co rdi n g to a g e a n d s e x . What m a y be c o n s i d e re d
h y p e r m o b i l e i n a n a d u l t m a l e m a y be pe r fe c t l y
n o r m a l i n a fe m a l e . a n a d o l e s ce n t o r a c h i l d W i t h
or
Copyrighted Material
­
.
Ewminillioll of locomOlOr fitiluion (/I/ d ils dislU rhllnce
Figure 4.55 Ty p i c a l a p pea rance of a p a t i e n t w i t h
h y p e rt o n u s a n d h y pe ract i v i t y o f bo t h u p p e r t r a p e z i i ,
' G o t h i c sh o u l d e rs '
1 27
( a)
t h e s e l i m i t a t i o ns i n m i n d , r a n g e A ( i n t h e d i a g r a m s )
s t a n d s for h y p o m o b i l e to n o rm a L ra n ge B fo r s l i g h t l y
h y p e r m o b i l e a n d C fo r m a r k e d h y pe r m o b i l i t y , 1 g i v e
t h e c r i t e r i a o f S a c h se w i t h a d d i t i o n a l d a t a f ro m
K a p a n dj i ( 1 <) 74 ) ,
The s p i n a l c o l u m n
T h e to t a l
K a p a n dj i
range o f s p i n a l m o b i l i t y
( I <)7 4 ) , o n t h e b a s i s of X - ra y
a s L 4 5 d egr e e s
tor a n te l� e x i o n ,
135
is
g i ve n
by
examination,
d e g re e s
fo r
r e t r o A e x i o n , 75 d e g r e e s fo r l a te ro A e x i o n to o n e s i d e ,
a n d 90-95 d egree s f o r
r o ta
t io n
to o n e
T h i s i s d i ffic u l t t o assess c l i n ic a l l y :
side,
each
of the
pri n c i p a l s e c t i o n s o f t h e s p i n a l co l u m n m u s t b e
e x a m i n e d se p a ra t e l y
,
L umbar spine
The a v e r a g e r a n g e
of r e t r o l1 e x i o n
i s 3 5 d e g re e s
acco rd i n g t o K a p a n d j i ( 1 97 4 ) , C l i n i c a l e x a m i n a t i o n
sh ows a s h a r p be n d e i t h e r a t t h e l u m bosacral o r a t
t h e t h o ra co l u m b a r j u n c t i o n i n c a s e s o f h y p e rm o b i l i t y ,
I n o rd e r t o d e t e r m i n e t h e r a n g e w i t h i n t h e n o r m a l ,
Sachse ( 1 96<))
gives
t h e fol lowing
test: t h e p a t i e n t
l i e s p ro n e w i t h be n t e l bows po i n t i n g b a c k w a rds a n d
h a n d s A a t o n t h e t a b l e by h e r shoulde rs (F i g u r e
4,56a ) , By e x t e n d i n g h e r a r m s a t t h e e l bow s h e l i fts
the u p p e r p a r t o f her body w h i l e the e x a m iner fi x e s
t h e p e l v i s from a b o v e ; i n t h is w a y t h e l u m b a r s p i n e
( b)
Figure 4.56 Test i n g t h e range o f l u m b a r ( t ru n k )
re t rofl e x i o n , Ra nge A , h ypomo b i l e t o n o r m a l : B , s l ight
h y p e r m o b i l i t y ; a n d C. m a rked h y p e r m o b i l i ty ( A ft e r
Sach s e , 1 969)
Copyrighted Material
1 28
Man ipulative Therapy in Rehabilitation oj the Locomotor System
A
B
c
Figure 4.57
Tes t i n g t h e range
of l u m b a r
( t r u n k ) a n t e flexion
is force d into retroflex io n. Ra nge A is from up to 60
d e rees a t the e l bow, ra nge B between 60 and 90
degrees and range C above 90 d egrees (Figure
4.56b).
The average ra nge o f a n te fl e x i o n is 60 degrees.
C l i n ica l l y this is tested by the p a t i e n t b e n d i n g to
touch t h e floor, with knees and finge rs stretche d .
R a nge A g o e s u p to t h e po i n t w h e re the subject
touches the floor with h e r fingertips, B fro m t h i s
perform a nce to p u t t i n g t h e k n uckles on t h e floor,
a n d C beyond this, t h e pa t i e n t n o t o n l y able to lay
h e r hand flat on the fl oor, but sometimes even to
bring the chest t o the t h i g h s ( Figure 4.57 ) . T h i s most
popular test, unfortu n a tely, shows not only the degree
o f a n te fl e x i o n of the t r u n k but a l so the exte n s i b i l i ty
o f t h e h a m stri ngs; i t a lso l a rge ly depends o n t h e
proportions of the l e g s t o t h e tru n k a n d arms. For
simple t r u n k a n teflexion , t h e re fore, i t may be better
for the patient to sit and touch he r knees w i t h her
fore h e a d (see Figure 4 . 5 3 a ) , range A cove ring t h e
range o f a n teflexion up t o w h e re t h is is poss i b l e , a n d
r a n g e B is w h e re t h e pa t i e n t ca n p u t h e r fore head
between h e r knees.
The a v erage range of l a teral fl e x i o n is 20 degrees
t o each side; the cli n i c a l criterion accord i n g to
S a c hse ( 1 969) i s the s h i ft o f the axil l a re l a tive to the
m id - l in e . I n range A, t h e a x i l la of the convex side
sho u l d come to rest above the i n tergl u te a l l i n e ; in B
it s h o u l d rest above t h e b u ttock of t h e other side ,
w h i le i n C t h e a x i l l a s h i fts beyond the l a te r a l aspect
of the b u ttock o n t h e other side (Fi g u re 4 . 5 8 ) . The
range o f axia l rota tion is given by Kapa ndj i ( 1 974)
as 5 d egrees but is not c l i n ica lly teste d . W h e n testing
stoop i n g a n d side-ben d i n g the exa m i ne r m ust ta ke
i n to account t h e mobi l i t y o f the h i ps a n d the
proportions o f the p a t i e n t: t h e re may be ' fa lse '
h y pe rmobi l i t y d u e to a l on g t r u n k a n d sh ort legs, or
' fa lse ' h y pomo b i l i ty d u e t o long legs a n d a s hort
tr u n k , while the le ngth o f the a rms p l a y s a part in
stoop ing.
Beca use o f its unfavourable consequences, h ow­
ever, clinically the most i m p orta n t sign o f l u m ba r
h y pe rmobility is hy p e r lordosis when standing relaxed
and exaggerated l u m b a r k y p h os is w h e n sitting
rel axed.
Th o racic spin e
Tru n k rotation is tested c l i nically. Kapandj i ( 1 974)
gives 35 degrees to each side as the average. The
patient sits astride the table, tur n i n g fi rst to one side
a n d then the other. Accord ing to Sachse ( 1 969) range
A is u p to 50 degrees to each side, B from 50 to 70
degrees and C beyond 70 d egrees (Figure 4.59). ( N ote
that we have shown that t run k rotation l i ke side­
bending is a coupled movemen t concern i ng both t he
thoracic and the l u mbar spine, see Chapter 3, p. 55.)
O bvious l y the tests for stoopi ng, ret roflexion
(ex t e n s i o n ) a n d side-be n d i n g show t h e m o b i l ity of
the whole trunk, i nc l u d i n g the t h o racic spine, but i n
c l i n ical practice they a re used ( w i t h t h e patient
s t an d i ng) for assessme n t of t h e l u m bar s p i n e .
Copyrighted Material
Examination of locomotor function an d its disturbance
1 29
0'
_ _
A
....
.. ...
.. ..
.. ...
"
60'
80'
Figure 4.59 Te s t i n g t h e r a n ge of
Figure 4.58 Tes t i n g t h e range of
A e x i on
l u m b a r (tru n k )
tru n k
rotation
l a te r a l
K a p a n dj i ( 1 974) g i v es t h e r a n ge o f m o v e m e n t for
the t h o r a c i c s p i n e as 4 5 d eg re e s in a n t e fl e x i o n ,
25
degrees in r e t rofl e x i o n and 20 d e g rees to e a c h s i d e
i n l a te ro fl e x i o n .
Cervica l spin e
Here, too , i t
is m a i n l y r o t a t i o n t h a t
is c l i n i c a l l y
tested . Acco r d i n g to K a p a ndj i ( 1 97 4 ) t h i s is o n l y 5 0
degrees t o e a c h s i d e , w h e r e a s S a c h se
range A as u p to 70
d egrees
( J 969)
gi v e s
to e a c h s i d e , B f r o m 70
Figure 4.60 Tes t i n g t h e range of h e a d (ce r v i c a l ) rota t i o n
to 90 d e g re e s and C ov e r 90 d e g r e e s . R o t a tion i s
tested i n t h e e rect posi t i o n by b r i n g i n g t h e p a t i e n t ' s
c h i n a bove t h e s h o u l d e r .
d i s c re pa n c y b e t w e e n
passive d o r s i fle x i o n , ra nge A i s u p to 4 5 d e g r e e s , B
the a n a t o m i c a l a n d t h e cl i n ic a l d a ta i s d u e to t h e fa ct
b e t we e n 45 a n d 60 d e g r e e s a n d C b e y o n d 60 d egrees
that rota t i o n t a k e s p l ace i n t h e e re c t p os i t i o n , a n d
(F i g u re 4 . 6 1 ) .
The
t h u s also i n v o l ves t h e u p p e r t h o r a c i c s p i n e . O n s l ig h t
for w a rd - b e n d ing rota t i o n stops a t C7
and
t h e r a n ge
is red uced to a b o u t 5 0-60 d e grees ( Fi g u re 4 . 6 0 ) .
W i t h regard to t h e e l bow j oi n t , t h e re i s m ore
v a lgosi t y
in
th e
hyperm o b i l e
e l bow,
and
the
fol l owi n g test i s t h e re fo r e c l i n i ca l l y v a l u a b l e . The
T h e range of a n te fl e x i o n ( K a p a n d j i , 1 974) i s 4 0
p a t i e n t h o l d s b o th a r m s b e fore h e r c h e s t , pa l m s
degrees. t h a t of re t rofl e x i o n 75 d e g r e es a n d of l a tero­
u p w a r d s , w i t h h e r for e a rms h e l d together fro m
e l b ow to w r i s t ; s h e i s t o l d t o s t r e tc h h e r a r m s ,
fl e x i on 3 5 de gre e s t o e a c h s i d e . T h e range o f mobi l i t y
a t t h e c r a n i o ce r v i ca l j u n c t i o n i s g i v e n i n t h e c h a p t e r
on
Functional
a n a to m y
s p i n a l co l u m n , p.
and
ra d i ogra p h y
of
t he
k e e p i n g t h e e l bows toge t h e r . R a n g e A m o b i l i ty w i l l
e n able t h e pa t i e n t to k e ep t h e e l bows tou c h i ng u p
to a n
62.
a ngle
of 1 1 0 d e g r e e s , B to 1 1 0-1 35 d e g r e e s ,
w h i le b e y o n d t h i s i s range C ( Figu re 4 . 62) .
For t h e s h o u ld e r g i r d l e , t h e c h a r a c t e r i s t i c t e s t i s
Some extremity j o i nts
to bri n g t h e e l bo w towa rd s
the shoulder
o f t he
by
o p p o s i t e si d e ; r a n ge A m o b i l i ty e n a b l e s t h e p a t i e n t
Sachse ( 1 969) . For m e t a c a rpop h a l a n g e a l j o i n ts , a t
to br i n g t h e e l bo w t o m i d - l i n e , r a n g e B fro m t h e r e
He re aga i n I give
the fi g u r e s as d e t e r m i n e d
Copyrighted Material
1 30
iVlan ip l l lative Therapy in Rehabilitlltion of th e Locomotor System
Figure 4.61 Test i n g t h e range of dors i rlexion of t h e m e t a ca rpop h a l a n ge a l j o i n t s
Figure 4.62 Tes t i n g t h e r a n ge o f
e l bow
e x t e n s i o n , bo t h e l b ow s k e p t t o u c h i n g
to a p o i n t h a l f- w a y between t h e m i d l i n e a n d th e
o t h e r s h o u l d e r , w h i l e i n ra n ge C t h e e l bo w m a y
t o u c h t he opposite sh o u l d e r (Figure 4.63 ) . A n o t h e r
t e s t is to try to m a ke bo th h a nds m e e t be h i n d t h e
b a c k , o n e from a bove a n d t h e o t h e r f r o m b e l o w .
W i t h ra n ge A m o b i l ity the fi ngers m a y n o t to u c h , o r
m a y j ust c o m e i n t o c o n t a c t ; i n ra nge B t h e fi n ge rs
-
m a y t o u c h o r o v e r l a p as fa r as to t h e fi rs t p h a l a n x ;
i n C t h e w h o l e h a n d m a y ove r l a p ( Fi g u re 4 . 64 ) . I n
t h i s t e s t i t is i m porta n t n o t t o a l l ow h y p e r l o r d o s i s t o
occ u r .
I f we i n t e n d to e x a m i n e t h e sca p u l o h u m e r a l j o i n t
b y i t s e l f, i t i s m os t c o n v e n i e n t t o t e s t o n l y p u r e
a b d u c t i o n w h i le o n e h a n d fi x e s t h e s h o u l d e r - b l a d e
Copyrighted Material
Exarninnliol1 of /oeolll% r fllne/ion lin d i/s dis/urbllnee
I
1- - .... ....
I
B
A I
I
I
.... .... '"
/
.... /
//
131
/
/ /�\\
/
c
\
\
\
\
\
...
Figure 4.63 B r i n g i n g t h e e l bow t o w a r d s t h e s h o u l d e r of
t h e opposite s i d e
w i t h t h e c l a v i c l e , f r o m il b o v e . R a n g e A
d e g r e e s , B fro m l) ( ) t o 1 1 0 d e g r e e s a n d
de grees
is u p to 9 0
C over 1 1 0
( Figure 4.(5 ) .
The knee
joint
i s t e s t e d Co r
e x t e n s i o n ) , r a n ge A
degrees ) .
e x t e n s i o n ( o r h y p e r­
be i n g up to fu l l e x t e n s i o n ( 1 80
r a n ge B u p to 1 0 d e gre e s h y p e re x t e n s i o n
( 1 90 d e g r e e s ) a n d C b e y o n d I h i s fi g u re ( F i g u re 4 . 6 6 ) .
Fo r
are
the hip
j o i n t , i n t e rn a l
tes t e d , ra n ge
A
being
up
a n d exte r n a l rota t i o n
t o l)() d egre e s ( e x t e r n a l
ro t a t i o n ) , B b e t w e e n 9 0 a nd 1 20
C m ore t h a n 1 20 d e g r e e s (Fi gu r e 4 . 6 7 ) .
I t is i m po r ta n t to t e s t I he range o f m o b i l i t y i n
various regions o f t h e b o d y , b e c a use t h e re m a y b e
h y p e r m o b i l i t y i n o n e a n d a ve r a ge o r e v e n red uced
mobi l i t y i n a n ot h e r , w i t h o u t restri c t i o n o f moveme n t .
plus
i nternal
degrees
and
A
S l i g h t r c l a t i ve h y p e r m o b i l i t y o n t h e n o n - d o m i n a n t
sid e is
p h y s i o l ogica l ( H inzma n n
a n d S a c h se , 1 (8 8 ) .
Exa m i nation o f coord i n ated
m ove m e n t ( locom otor p atte r n s )
The exa mina tion
o f i n d i v i d u a l m usc l e s a n d t h e
mo b i l i ty a re fo l l owed by t h e
s t u d y o f m o re com p l e x m o v e m e n t p a t te rns, o r
s t e re o t y p e s . We b e g i n w i t h a s s e ss m e n t o f p os t u re
w i t h t h e p a ti e n t s t a n d i n g , as d e s c r i b e d a t t h e begi n ­
n i n g of t h i s c h a p t c r ( s e e F i g u r e 4 . 6 , p . 95 ) .
He re t h e fo l l o w i n g c r i t e r i a s h o u l d b e s t resse d :
w he t h e r t h e vert ica l l i n e from t h e e x t e r n a l o cc i p i ta l
pro t u b e r a n c e c o r r e s po n d s to t h e b o d y a x i s , i . e .
whether o u r p a t i e n t s t a n d s sym m e t ri c a l l y , a n d to
w h a t e x t e n t t h e two h a lv e s of h i s body d i ffe r.
The re l a t i ve p r o p o r t i o n of t h e e x t re m i t i e s t o t h e
asse s s m e n t o f o v e r a l l
B
tru n k a n d n e c k a re i m po r t a n t . a s i s l h e re l a t i o n s h i p
u p pe r p a r t to t h e l o w e r p a r t o f t h e tru n k . T h e
of t h e
p r o p o r t i o n s o f t h e prox i m a l
the
e x t re m i t ies
a re e q u a l l y
to t h e d i s t a l
s i g n i fic a n t .
c
s ec t i o n s o f
Figure 4.64 Ma k i n g bot h h a n d s m e e t be h i n d the s h o u l d e r
Copyrighted Material
1 32
Manipula live Therapy in Reh a b ilitation of
th e Locomotor System
Figure 4.65 Test i n g t h e ra n g e of a b d u c t i o n of t h e
sca p u l o h u me r a l J o i n t , w i t h t h e s h o u l d e r- b l a d e fi x e d
from above
B
�
-
-
-
-
-
-
-
_
_ _
1O
-
�10 cm
_
c
Figure 4.66
Tes t i n g
e x t e n s i o n ( h y pe r e x t e n s i o n ) of t h e k n e e j o i n t
Figure 4.67
Testi n g i n t e r n a l a n d e x t e r n a l rota r i o n o f t h e h i p j o i n t
Copyrighted Material
_ _
10'
Examinlllioll of /ocornOfor jUl1cfiol1 and ifS disturbance
The body c o n t o u rs i n form us a b o u t i ncreased
tonus o r fl a b b i n e s s . Th i s i s particu l a rl y i m p orta n t if
we com p a r e t h e two s i des ( t i g h t - loo s e c o m p l e x ) .
Not o n l y exaggera ted protrusio n , b u t a l so s h a r p
indent ations are i mpo r tan t , as is t h e flatte n i n g o f
contours. Th is is further confirmed b y pal pa t i o n
w h ich e n a b l es u s t o d i s t i n g u i s h t he t y p e o f resista nce
( resilience) o f i n d i v i d u a l tissue layers.
A n a l ysis of patterns o f move m e n t a n d pos t u re
may start with the p a t i e n t s i t t i n g on an a dj ustable
stool ( F i g u r e s 4 . 68 a n d 4.69) . T h e examiner notes
the po s i tio n of the fee t and o f t h e i l iac crests, the
c o u rse of the ( l u m b a r) s p i n e a n d the ton u s of t h e
abdom i n a l a n d gl u t e a l muscu l a t u re . I n correct pos­
t u re, seated, the fee t a re flat on t h e floor in sl i gh t
exte rna l rota tion, t h e t h i g h s h o rizo n t a l a n d s l i g h t l y
a p a r t , t h e pelvis rotated ( ti l te d ) fo rw a rd i f poss i b l e ;
there shou l d b e s l ight l u m bar l o rdosis ( n o k y p hosis)
a n d n o fl a b b i ness or t h e abdom i n a l or gl uteal m uscles.
S tooping and stra igh tening up ( Figures 4.70
and 4 . 7 1 )
For co rrect stoopi n g o n e foot s h o u l d b e placed i n
fro n t of t h e other a nd t h e k n e e o f t h e fo rward leg
s h o u l d be s l i g h t l y b e n t . The tru n k bends forward ,
starti n g with the h e a d , t h e body c u rl i n g up from the
head downwards as the g l u teal and a b d o m i n a l
muscles cont ract . T h e erector s p i n a e contracts fi rs t
a n d t h e n re l axes d u r i n g maxi m u m stoop i n g. Con-
Figure 4.68 S i t t i n g on a s t o o l : correct pos t u re
1 33
v e rse l y , at stra i ghte n i n g u p the k nees stretch w h i l e
t he t ru n k u n c u r l s , s t a r t i n g w i t h the l u m b a r s p i n e ,
fol l owed by t h e t h o racic s p i n e , the neck a n d fi n a l l y
t h e h e a d . Th i s , too, is the resu l t of coord i n a te d
c o n t r a c t i o n of t h e glute a l , a bdo m i n a l a n d back
m uscul a t u re . The t r u n k must never be l i fted l i k e a
rod ( Ieve r l ) nor must t h e a b d o m e n be a l l owed to
b u lge .
Trun k ro ta tio n, sitting (Figure 4.72)
T h i s test is more close l y conce r n e d with t h e t h o racic
s p i n e a nd shoulder girdle than w e re the p revious
tests. Again the pre-cond i t i o n is correct s i t t i n g
posture o n a s t o o l , w i t h a t e s t obj ect ( s u c h as a b o o k )
i n t h e h a n d res t i n g o n t h e l a p . Speci a l a t te n t i o n m u s t
be p a i d to r e l a x a t i o n o f t h e arms a n d shou lders,
w h ich m u s t not be d rawn fo rw a rd and e l e v a ted . Th e
pati e n t is now asked to p lace t h e book on a s h e l f
beh i n d h e r , a t t h e l e v e l o f h e r h e a d ; spec i a l attention
m u s t be p a i d to t ru n k ro t a t i o n , t h e action o f the back
a n d a b d om i n a l m uscles, fi x a t i o n of the s h o u l de r­
b l a d e s a n d tension i n the u p per p a r t o f the t r a p e z i u s .
I f the test is perfo r m ed properly we see h a r m o n ­
ious rotation from the thoraco l u m b a r j u nction u p ­
wards w h i l e the pelvis and l e g s re m a i n in p lace;
abdominal a n d back m u s c l e s a re m o d e r a t e l y active,
t h e i n fe r i o r a n g l e s of the sca p u l a d o n o t d i verge and
the n e c k m uscu l a t ure, i n particu l a r t h e u p p e r pa rt
o f the trapez i u s , rema i n s relaxed .
Figure 4.69 Two types of fa u l t y s i t t i n g p o s t u re
Copyrighted Material
1 34
/V/{Il1 ip l i /{(/i ve
Th emp v in Reha/Jili/[i/i O I l of /he Locol1l()/or Sys/ell1
( a)
( b)
Figure 4.70 ( a ) S t oo p i n g a n d ( b ) lift i n g a n
Figu re 4.71 T h e s a m e m o v e m e n t s
as
object
i n Figure
c o rr e c t l y
4 . 70 p e r fo r m e d
i ncorrect l y
Copyrighted Material
Exa mina{ion
Figure 4.72 T r u n k ro t a t i o n . s e a t e d . h o l d i n g
a n o bj e c t in t h e
Test m o ve m e n ts for the head a n d n e ck ( F i g u r e
4 .73 )
First w e obse rve t h e h e a d pos i t i o n w i t h t h e p a t i e n t
s t a n d i n g a n d s i t t i n g ; l or d o s i s s h o u l d n o t be too
m a r k e d a n d if t h e re i s a flat t h o ra c ic s p i n e the n e c k
w i l l a l s o be s t ra i g h t . T h e a n g l e b e t w e e n t h e
m a n d i b l e a n d n e c k s h o u l d b e a b o u t 9 0 d e g ree s .
D u r i n g h e a d t u rn i n g t h e e xa m i n e r observes n e c k
ro t a t i o n as w e l l as m u s c u l a r act i v i t y : l a te r o fl e x i o n
s h o u l d ta ke p l a c e o n l y a t e x t r e m e ra nge a n d sh o u l d
not be e x a gge r a t e d . lordosis s h o u l d not i n c r e a s e , t h e
s h o u l d n o t be l i fted n o r s h o u l d o n e
b e d ra w n fo rward; t h e ste rnocleidomastoid
s h o u l d e rs
shou lde r
shou l d n o t b e o v e rs t ra i ne d .
of /DCD111010r fUIiCiion and ils dislIIrbance
h a n d : (a) correct: (b)
1 35
fa u l t y
L ifting th e a rms ( Figu re 6 . 1 46)
W h e n l i ft i n g the a r m s the p a t i e n t a l so r a i s e s h e r
s h o u l d e rs c o n tr a c t i n g t he u p p e r fi xators o f t h e
s h o u l d e r girdle ( u p p e r p a r t o f t h e t r a pezi u s a n d the
l e v a to r sca p u l a e ) , fi x a t i o n o f t h e sho u ld e r - b l a d e s
f r o m b e l o w ( by t h e l o w e r p a r t o f the trapez i u s )
b e i n g i n s u fficien t. H o w e v e r . l i ft i n g o f the s h o u l d e rs
s h o u l d be o n ly sl i gh t a n d towards t h e e n d of t h e
,
m o v e me n t .
Weig h t carrying ( F i g u re 4 . 7 4 )
a fo rward-dra w n p o s i t i o n o f
causing t e n s i o n i n t h e u p p e r
fi x a t o r s of t h e s h o u l d e r gird l e . I f a w e i gh t i s ; 0 be
carried co rrec t l y th e s ho u l d e rs a re b e h i n d the l i n e
o f gr a v i ty o f t h e b o d y a n d t h e h e a d a n d neck r e m a i n
e r ec t . Th e h a n d ca r r y i n g t h e bri e f- c a s e s h o u l d also
be r e l a xe d .
Here the
the
head
typica l
fa u l t i s
and sbould ers,
Sta n ding o n o n e leg ( F i g u re 4 . 7 5 )
Figure 4.73 H e a d rota t i o n .
sea ted: ( a )
c o r re c t : (b ) fa u l t y
Special atte n t i o n s h o u l d be p a i d to t h e m u sc l es and
j o i nts o f t h e s u pp o r t i n g leg. t h e l i n e of g r a v i t y of t b e
body. t he p e l v i s , i n p a r t i c u l a r t h e i l i a c crests, a n d t h e
h i p s t a b i l i z e rs, especi a l l y t h e g l u t e a l m u scu l a t u r e ,
a n el t b e s p i n a l c u rv a t u re .
In c o rre ct p o s t u re on o n e l e g . a l l j o i n ts of the
s up porti n g leg are in the line o f gravity; the c e n tre
of gra v i t y . c o m p a r e d with s t a n c e on two l e g s , m o ve s
Copyrighted Material
l36
Manipulative Th erapy
in
Rehabilitation
of t h e
Locomotor System
a n d the quadrati l u mboru m , should contract i n a
coord i n a ted fas h i o n to stabil ize the h i p a n d t r u n k .
H t h e h i p abducto rs a re wea k . the m o s t fre q u e n t
fa ult, the pati e n t w i l l l i ft t h e i l i a c crest of t h e side
oppos i te to the s u pporting leg (Dej e r i n e , 1 90 1 ) ,
bringing t h e ce n t re o f gravi ty above t h e s u pporting
leg and t h us rel i e v i n g t he a b d uctors. (Tre n d e l e n ­
b u rg's sign , t h e lowering o f t he i l i ac crest on t h e
u n s u p ported s i d e , i s re l a t iv e l y r a r e : i t is seen i n
severe cases o f con ge n i ta l h i p l u x a t i o n but n o t even
in myopathy w i th extremely weak m uscles . )
Gait
Figure 4.74 Carry i n g
pos t u re
we ights: (a) correct: ( b ) fa u l t y
forward to the secon d a n d t h i rd m e t a ca r p a l h e a d .
The pe lvis s h o u l d rem a i n h orizon t a l a n d s p i n a l
c u rv a t u re s h o u l d there fore be a l most u ncha n ged .
The s t a b i l iz e rs of t h e h i p, i n particular the g l u teus
medius. s h o u l d contract. Both flexors and exte nsors
o f the h i p as w e l l as t h e a bdomin a l and back m uscles,
Fi gure 4.75 S t a nd i n g
on
o n e leg. back v i e w :
The e x a m in e r takes pa rt i c u l a r note of how the heels
touch the gro u n d fol l owed by the ball of t h e foot
and the toes, w h i le the h e e l is l i fted : h e s h o u l d also
n ote how weight is s h i fted fro m o n e l eg to the other,
how the p e l v i s moves with the spi n a l co l u m n , t he
position o f t h e head a n d the move m e n ts of the a rms.
In n o r m a l ga i t the steps a re even and t he weigh t
i s p l aced e q u a l ly o n each l e g in t u rn . The a rch of
t h e foot does not sag a n d the toes are active i n
p rop u lsion. The p e lv i s should re m a i n a l most hori­
zonta l , and i t sways from s i d e t o s i d e . more so in
women than i n men. T h e spi n a l col u m n c u rves from
one side to the othe r in a series o f w a v e s . the grea test
excursion b e i n g in the m i d - l u m b a r region ; t here is
some counter-exc ursion i n the t h o racic s p i n e . the
t horaco l u m b a r j u nc t i o n rema i n i n g above t he sac r u m .
Th e head s h o u l d move v e r y l i ttle a n d t he a rms
s h o u l d swi ng sym metrica l l y or s l i g h t l y more on t h e
( a ) correct; ( b ) fa ulty. S i d e v i ew: (e)
Copyrighted Material
correct:
(d) fa ulty
Examination of locomotor /imclion and its disturbance
1 37
l e ft, t h e movem e n t com i n g from the s h o u l de r. The
shou lder-blades are fixed from below, the upper
fix ators of t he s h o u l d e r girdle re laxed. The ce n t re o f
grav ity of the b o d y a n d that of the h e a d s h o u l d s h i ft
as l i ttle as possible, e i t h e r from one s i d e to the othe r
or u p and down, i .e. the pa t i e n t should n e i t h e r
waddle nor roc k .
Asymmetrica l ga i t a n d s t i ffness can also be h e a r d ,
and t he re fore the e x a m i n e r must l isten carefu l ly .
Ce rta i n fa u l ts become more m a r ked i f t h e pa tie n t
closes her eyes, w a l k s on tiptoe or o n t h e hee l s ; th ese
sho u l d be exa m i ned a s req u i re d .
Fi n a l l y , p a t i e n ts s h o u l d b e e x a m i n e d , if possible,
i n the i r typic a l work i n g p osition (e.g. typi ng, l i fting
weights, readi ng, a t a m a c h i n e , a t the computer, e tc . ) .
Exa m i nation of resp i ration
We h a ve a l ready seen i n C h a p t e r 2 t h a t respira tio n
is fi rst examined a t rest i n the s u p i n e posi tion
and t h e n w i t h the pati e n t sea ted o r s t a n d i ng. In
t h e supine posi tion a bdomi n a l respiration s h o u l d
predom i n a t e . U n d e r post u ra l con d i t ions t h e tru n k
broadens from the waist; the e x a m i n e r t h e r e fore
places his h a n ds on the patie n t ' s lowe r ribs, from
both sides. I f bre a t h i ng is correct, the h a n d s a re
moved apart, b u t i f the patient l i fts h e r thorax as s h e
breathes, the exami ner's h a n d s m o v e upwards. If
this fau lty bre a t h i ng pattern ( w i t h raised thorax) i s
v e r y p ronounced, the t h o r a x m a y rem a i n i n the
inha l a t ion position even w h i l e a t rest, t h e upper
clavicu l a r grooves are deep and t h e sternocleido­
mastoids, sca lenes and upper fixators o f the s h o u l d e r
gird le are t a u t . D u r i ng i n h a lation the c o l l a r bones
are l ifted, too. In less severe cases this fa u l t is
noticeable only when the patient takes a deep breath
while sitting; b u t i n more severe cases i t can be seen
even during breathing a t rest a n d i n t h e most severe
cases i t is evid e n t even a t rest in the s u pine position
(Figure 4.76). Respiration can be so badly co­
ordinated that a patient may draw the a b domen in
during i n h a l a tion a n d push it o u t while breathing out
(paradoxical respirati o n ) .
Inhalation and e x h alation s h o u l d h a v e about the
same duration ; the patient s h o u ld be able to breathe
i n for 7-1 0 s or longer, breat b i n g o u t for the same
length of time (except for professional s i n gers, w h o
breathe out for much longer) . There are, however,
patients who c a n n o t breathe i n (or o u t) for more
than 4 s , although they suffe r from n o respi ratory
disease ' The nostri ls expand d u ring tbe dee p
inhalation and t h e n n a rrow d u r i n g exhalatio n . It is
i m porta n t that the fac ial muscu la t u re s h o u ld be
relaxed , particu larly the lips, the m uscles of the j a w
and t h e tongue.
The exa m i n e r should watch c a refully fo r asym­
metry, partic u l arly i n a patien t who l ifts her shoulders
during i n h a l ation.
Figure 4.76
L i f t i n g t h e t h or a x d u r i n g i n h a l a t i o n :
marked
t e n si o n in t h e s t e r n oc l e i d o m a s t o i d e i , sca l e n i a n d t h e
u p p e r p a r t o f t h e t r a pezi i ; v e r y d e e p s u p r a c l a v i c u l a r
fossae
o n bot h s i d e s a n d t h e a b d o m e n i s drawn i n a t
inhala tion
I n t h e prone position
thoracic spine s h ould
bre a t hing. The a bsence
o f the t horacic sp i n e ,
pattern.
t h e respi ratory wave o f the
be observed d u ring deep
of a wave, a nd n o blockage
i m p l ies a fa u l ty breathing
Syn d r o m es
The l ower crossed sy n d r o m e ( a fter J a n d a ,
1 979)
There i s i m b a l an ce i n the fo l lowing p a i rs of m uscles:
( 1 ) weak glutei maximi a n d s hort h i p flexors; (2)
weak a bd o m inals (recti a bdom i n is) and short
lumbar erectores spinae; (3) we ak g l u te i m e d i i a nd
s hort tensors of the fasciae latae a n d q u a d rati
l u m b o ru m .
There is n o t o n l y a n tagon i s m b u t a lso 'compe t i ­
tio n ' o r s u b s t i t u t i o n : for w e a k g l u t e i m e d i i by t h e
tensors a n d quadrati l u mborum; for weak abdomina I s
by t h e i l i opsoas i n h i p flex i o n ; f o r w e a k g l u t e i
maxi m i by t h e erector s p i n a e ( a n d t h e h a m s tri ngs ) .
Obviously, i n this syndrome t h e correct mecha n i s m
of c u r l i ng u p i n s i t t i n g u p from t h e s u p i n e position
a n d i n stoopi n g is i n terfe red w i t h ; t h e res u l t is
Copyrighted Material
I It:
M{fl1ip l l llll i v c
Th erapy in
Relwb ili{lIIiOI1
of {he
L o c o l l 1 o { o r S " .\ { C I I I
3.
B e tw e e n t h e dee p neck fl exors ( l o ngus cervicis.
longus capitis a n d o m o - a nd t h yro h y o i d e u s) on
t h e o n e h a n d . a n d the n eck e x t e n sors ( cervica l
section of t h e e r ec t or s p i n a e . u p p e r p a r t o f t he
t r a p e z i us a n d leva t o r sca p u l a e ) on t h e o t h e r .
I n a d d i t i o n t h e re m a y be s h o r te n i n g o f t h e
u p p e r m os t p a r t o f t h e l i ga m e n t u m n uc h a e w i t h fi x e d
l o rdosis i n t h e u ppe r cervica l regio n .
Obviously. i f t h e lower fi x a tors o f t h e s h o u l d e r
girdle a re wea k . t h e u p pe r Il x a tors m u s t become
h y p e r a c t i v e and te n s e . H y p e ra c t i v i t y o f the p ector­
a l e s prod u ces rou n d s h o u l d e rs a n d fo rw a rd - d r a w n
s h o u l d e rs , n e c k a n d h e a d ; w e a k dee p neck Aexors
w i t h s h o r t exte nsors prod uce h y p e r l ord osis of the
upper cervical s p i n e . In ad d i t i o n to the re l e v a n t
m o ve m e n t p a t t erns. t h e res p i ra t i o n ste reotype i s
a l s o u s u a l l y a ffected .
H e re , too. o n e h a s to b e a r i n m i nd w h a t has bee n
s a i d a b o u t the l o w e r crossed s y n d rome. poss i b l e
i n te rre l a t i o n s b e t we e n b o t h s y n d ro m es a n d dys­
function a t the h a n d a n d e l bow.
Stratificati o n sy n d r o m e
Figure 4.77 ( II ) I n c r e a s e d
h y p e r l o rd o s i s
pelvic l i l l a n d (iJ) l u m b a r
i n c re a s e d fo rwa rd t i l t of t h e p e l v i s a s we l l as
i n c reased l u mbosacr a l ( Figure 4.770) a nd/or l u m bar
l o rd osis ( Fi g u re 4 . 77b ) . The h a m s t r i ngs a re u s u a l l y
s h o rt i n t h i s s y n d ro m e , b u t t h i s i s freq u e n t l y a
co m pe n sa tory m e c h a n i s m t h a t lesse n s p e l v i c t i l t .
I t m u s t be stresse d . however. t h a t e v e n the
a n tagon i s m of hip flexors a n d e x te nsors. a n d of
a d d uctors a n d a b d u ctors. i s o n l y one somew h a t
s i m p l i s t i c aspect. fo r a l l these m us c l es stab i l ize t he
h i p d ur i n g ga i t a n d stance . Some t i m e s t h e i m b a l a n ce
c a n be d u e to d y s fu n c t i o n o u tsi d e t h e p e l v i s . e .g . of
t h e foo t . as cou l d be guessed f ro m Fig u re 4 . 7 7 h .
w h e re w e fi n d ( u n i n t e n t i o n a l l y ' ) u n p ropo rtionaJ ly
strong m usc l e s a t t h e h i p and a v e r y wea k lower leg
a n d foo t . i.e. an i m po r t a n t d is p ro p o rt i o n w h i c h
c o u l d i m p l y com pensa tion o r w e a k s t a b i l izers o f t h e
foo t b y h i p s t a b i l i z e r s .
1.
2.
'
Test i n g
T h e u p per crossed sy n d ro m e
T h e re
[ n t h is s y n d ro m e , strata o f h y p e r t ro p h i c a n d wea k
m u scle gro u ps a l t e r n a t e : i n a ca u d ocra n i a l d i re c t i o n
t h e re a re w e a k m u s c l es o f t h e f o o t a n d leg, h y p e r­
trop h i c i sch iocrur a l m uscle groups. h y p o t rop b i c weak
gl u te a l s and u n d e rde ve l o p e d l u m b a r e rectores
s p i n a e . and above these t h e b u l g i n g hype rtro p h i c
thoracol u m ba r section o f t h e e re c t o res s p i n ae ; these
a re fo l l ow e d by fl a b by i n te rsca p u l a r muscles w i t h
h y p e rt ro p h ic ta u t u p per hxa tors o f t h e s h o u l d e r
g i rd l e a bove t h e m .
O n t h e v e n t r a l a s p e c t t h e lower sec t i o n o f the recti
a b do m i n i s buIges, but m o re l a t e ra l l y t h ere is a
groove correspon d i n g to t h e ta u t o b l i q ue a bd o m i n a l
m us c l e s ; l a te ral from t h i s t he a b d o m i n a l wa l l m a y
b u l ge aga i n i n t h e reg i o n o f t h e w a i s t ( ' ps e u d o ­
hernia ) .
Th i s s y n d ro m e i m p l i es i m b a la n ce i n t h e s t ra t u m
o f h ypermob i l i t y ( l a x i t y ) t h a t a l t e rn a t e s w i t h s t ra t a
o f i nc reased te n s i o n , h y pc r m ob i l ity b e i n g most
pr o n o u n ce d i n the Iow-back regi o n . I t a l so i l l u s t r a t e s
t h e i m porta nce o f d i s p r o p o r t i o n .
i s i m b a l a n c e i n t h e fo l lo w i ng m usc l e g ro u p s :
B e t w e e n t h e u p p e r <l n d l o w e r fi x a t o rs o f t il e
s h o u l der gird l e (i.e. the upper trapezi us. levator
sca p u l a e and fre q u e n tl y t h e sca l e n e s o n the one
h a n d . a n d t h e l o w e r tra pezius a n d the serratus
a n te r i or o n t h e o t h e r ) .
B e t w e e n t h e pecto rales a n d t h e i n tersca p u l a r
m u scles.
C l i n ica l e x a m i n a t i o n p ro v i d e s a wea l t h o f d a ta
conce r n i n g t he f u n c t i o n i n g o f t h e l oc o m o t o r syste m
a n d reflex c h a nges i n t h e tissues. T h i s e n a b l e s us not
only t o e s t a b l i s h d i ag n os i s . b u t t o com p a re before
and a ft e r t h erapy u s i n g t h e tec h n i q u es described
below, w h i ch prod u ce an i m m ed i a te re A e x e ffect.
I m med i a t e tes t i n g. i .e . co m p a r i son o f t h e s t a te
b e fore a n d a ft e r t re a t me n t . t h us co nstit u te s a fe ed­
b a c k which e n a b les u s to assess not only t re a t m e n t
Copyrighted Material
Ewminll /io/l
b u t d i a g n o s i s on t h e s p o t , a n aspect t h a t i s
indispe n s a b l e fo r t he c r i t i c a l t h era p i s t . T h i s b e co m e s
clear i f we com p a re our p roced u re w i t h t h a t of t h e
p h a r m acot h e ra p i s t . w h ose c l i n i c a l res u l ts a re a l w a y s
d i fficu l t t o assess i n view o f t h e e v e r-ch a n g i n g a n d
freq u e n t l y u n p re d i c t a b l e co u rse o f t h e d isease. I t i s
a l l t h e m o re i m po r ta n t , t h e re fo r e , t h a t we c a n s e e
i m m ed i a te l y c l e a r e ffec t s , o r com p l e te fa i l u res.
However, a pos i t i ve test is n o t ta n t a m o u n t t o t h e r a ­
pe u ti c success, beca use i f we h a v e t r e a t e d il n
irre l e v a n t l esion t h e e ffect m a y b e b u t s h o rt- l i ve d .
I f t h e i m m e d i a te e f fect i s i n co m p l e t e , t h i s l e a d s u s
t o l o o k c a re fu l l y for y e t a n ot h e r l e si o n .
I n p r i n c i p l e , e v e r y d e v i a t i o n from t h e n o r m fo u n d
a t c l i n i c a l e x a m i n <l t i o n c a n be m a de t h e o b j ect o f
testi ng: o b v i o u sl y , t h e most re w a rd i n g a re fi n d i ngs
that ca n be m e a s u re d : ra n ge o f move me n t o f j o i n ts ,
p a r t s o r m o b i l e sec t i o n s o f t h e s p in a l co l u mn , a n d
t h e s t r a i g h t l e g ra isi n g test. Howe v e r , i m prove m e n t
i n t h e s t r a i g h t l e g r a i s i ng t e s t s h o u l d be co n s i d e red
re l i a b l e on l y if t h e re i s a m a r k e d d i ffere nce i n
p e r fo r m a n c e be fore a n d a ft e r t re a t m e n t (20 deg r e e s
or m o r e ) a n d i f t h e test h a s beco m e m u c h less
pa i n fu l . S i d e dev i a t i o n i n Ha u ta n t 's test i s a l so
s ig n i fic a n t . as i s a s y m m e t r i c a l d i s t ri b u t i o n of we i g h t
o n t w o sca l e s be fore a n d a ft e r t re a t m e n t . Sys t e m a t i c
test i n g c a n e a s i l y s h ow t h a t eve n s l i g h t l y p a r e t i c
m u s c l e s i n rad ic u l a r s y n d ro m e s acq u i re s t r e n g t h
i m med i a t e l y a ft e r success fu l m a n ip u l a t i o n or e v e n
a fter t ract i o n , a n d t h a t e v e n t h e t e n d o n re ll e x m a y
i m p r ov e .
I t is a l s o poss i b l e to t e s t re fl e x ch a n ges: m uscle
spasIll , t r i gger p oi n ts h y pera lgesic zones, t h e s k i n
fo l d , s k i n s t re tc h i n g o r s h i ft i ng o f fa scia m a y a l l
b e i n f1 ue n ced i m m e d i a t e l y b y m a n i p u l a t i o n , loca l
a n a e s t h e s i a or n e ed l i ng , or s i m p l y by s k i n s t retc h i n g
or pos t - i s o m e t r i c muscle re l a x a tio n . I n s t r u m e n t a l
m e t hods such a s the m e a s ur e m e n t o f s k i n t e m pera­
t u re , con d u c t i v i ty , p l e t h y s m o g ra p h y , etc. m a y a l so
show re fl e x c h a nges a ffected by a n y t y p e o f t hera py.
Tes t i n g , however, a l s o i m p l ie s a m o re j u d i c i o u s
a t ti t u d e to t re a t m e n t . I t i s esse n t i a l to k now t h e
re l a t i v e i mpo r t a nce 0 1' n u merous fi n d i ngs a n d t h e i r
m u t u a l i n l� u e nce. F o r i n s t a n c e , i n d is t u r b a nce of t h e
J ow back , T m a y w a n t t o k n o w t h e i m po r t a nce o f
dysfunction a t t h e c ra n i ocervica l j u nc t i o n or a t t h e
foot , o r agai n , o f a s c a r i n a l e s i o n a t t h e s h o u l d e r :
i n s u c h a c a s e I m u s t n o t treM t h e p e l v i s b e fore I
treat t h e c ra n i ocerv i c a l j u nc t i o n or t h e foo t : n o r
m u s t I t r e a t t h e s h o u l d e r b e fore I h a v e d o n e
somet h i n g a bo u t t h e s c a r . I n o t h e r words, i n a case
w h i c h is n o t q u i te simple t h e patient h a s fi rs t to be
t h o r o u gh ly e x a m i ned and o n l y a ft e r a n a l y s i s o f the
fi n d i ngs c a n trea t m e n t be p l a n ned s o t h a t b y tes t i ng
we can d e c i d e n o t j u s t t h a t t h e p a t i e n t ' h as i m p ro v e d
(o r n o t ) b u t a l so w h i c h l e s i o n is p ri m a ry , w h ich i s
seco n d a ry , w h i c h i s m o re a n d w h ich is l e s s re l e v a n t .
A l t h o u g h o n e s h o u l d n o t re l y solely o n s u bj e c t i v e
asse ss m e n t , i t i s o f c o u r s e m o s t sign i fi c a n t i f t h e
,
'
o f /oco li / %
r IU l l e / i o n
il l l d irs (/is/urbul/Ci'
1 3 lJ
p a t i e n t h e rse l f ( a s is fre q u e n t l y t h e case ) fe e l s a n d
i m m e d i a te re l i e f a ft e r t h e a p p ropria t e
t r e a t m e n t . I t i s , i n fa c t . g o o d po l i cy to l e t t h e pa t i e n t
h e rse l f p a l p a t e p a i n p o i n t s a n d t r i gge r p o i n ts b e fore
a n d a fte r t r e a t m e n t , to assess the e ffec t h e rse l f. I f
t h e t h e r a p i s t p a l p a tes a fter tre a t m e n t , t h e p a t i e n t
s o m e t i m e s d o u bts w h e t h e r t h e s a m e a m o u n t o f force
has been a p p l ied as bdore t re a t m e n t, beca use s h e
fee l s l e s s .
I n a d d i t i o n to i ts d i a g n o s t i c v a l u e , test i n g i s u s e f u l
fo r i n d i ca t i o n of f u r t h e r t h e r a p y : e . g . i f traction h a s
bro u g h t rel i e f. f u r t h e r t r a c t i o n trea t m e n t i s p r o b a b l y
i n d i ca ted .
a p p r ec i a t e s
The cou rse of exa m i n a t i o n with
spec i a l reg a rd to c h a i n - react i o n
patter n s
T h e re i s a n i m port a n t q u e s t io n : w h a t s h o u l d t h e c a se
s h e e t o f a p a t i e n t w i t h d i s t u r b e d fu n c t i o n of t h e
l oc o m o t o r s y s t e m l o o k l i k e ? A ' m a n i p u l a t i v e case
shee t " )
Once t h e ex a m i n a ti o n t ec h n i q u es a r e k n ow n , t h e
q ue s t i o n o f h o w t o obta i n use fu l res u l ts i n p r a c t i ce
a n d a v o i d e rr o rs as fil l' as is h um a n l y poss i b l e m u s t
be a d d ressed .
T h e a ns w e r is n o t s i m p l e , as t h e obj e c t o f
e x a m i n a t i o n - d i s t u rbed fu n c t i o n of t h e loco m o t o r
s y s t e m a nd i ts re A e x c h a nges - c o n c e r n s m a n y
d i f fe re n t fi e l d s o f m e d i c i n e . Some p a t i e n ts prese n t
th e m se J v e s w i t h p ro b l e m s b e l o n g i n g to t h e fie l d o f
g e n e r a l m e d i ci n e : o t h ers w i t h m e t a b o l i c , e n docri n e ,
n e u rologic a l , rh e u m a t ol og i c a L o r t h o p a e d i c , gyn aeco­
logi c a L o t i a t r i c and o th e r s y m p t o m s : in some cases
t h e t r o u b l e l ies i n d i s t u rbed j o i n t m o b i l i t y in o t h e rs
i n d is t u r b e d m u scle fu n c t i o n , w h i l e i n o t h e r cases
pa i n with its s p ec i fi c reflex re a c t i o n s d o m i n a te s . T o
e x a m ine each patient from a l l o f t h ese aspects w o u ld
d em a n d fa r m ore t i m e t h a n t h e c l i n i c i a n h a s a t h i s
d isposa l .
W e m u s t t h e refore a p p roach e a c h c a s e fro m t h e
p o i n t o f v i e w o f t h e p a t i e n t 's com p l a i n t, a n d p roceed
from one fi n d i n g to the n e x t . E x pe r i e nce has s h ow n
t h a t t h e fi n d i ngs fo ll ow c e rta i n p a t t e r n s ( c h a i n s ) s o
t h a t i f w e fi n d ( a ) w e expect ( b ) a n d m u s t t h e n l o o k
for ( c ) .
I f t h e p a t i e n t i s abso l u t e l y u n k n o w n t o t h e e x a m ­
i ne r , h e m u st fi rs t l o o k a t g a i t a n d postu re, s e e h o w
t h e m u sc u l a t u re i s develo p ed , m a k e scre e n i n g t e s t s
of cerv i ca l . t h o racic and l u m b a r m o b i l i t y , p a l p a t e t h e
p e l v i s w i t h the p a t ie n t s t a n d i n g e x a m i n e Pa t ri c k ' s
s i g n w i t h t h e p a t ie n t s u p i n e , a n d exa m i n e rota t i o n
of t he f o o t - a t l e a s t .
A s , 11Ow e v e r the p a tie n t c a n be e x pected t o
prov i d e i n fo r m a t i o n a bo u t h i s c o m p l a i n ts , we m a y
proceed accord i ngl y . For i ns t a n c e , i f a p a t i e n t c o m e s
w i t h h e a d a c h e t ro u b l es ( a n d n e g a t ive n e u r o l og i c a l
fi n d i n gs) we m u s t t h o r o u g h J y e xa m i n e m o b i l i t y o f
Copyrighted Material
,
,
,
1 40
l?chahtiif,Hion of the Locom%
Manip u lillil'l'
typica l
t h e c ra n i oce r v i c a l
p o i n ts o n t h e
of
aspect of t h e
c a t o r y m us c l e s .
i s held
r System
pain
implies I
l a s , t h e l a te r a l
a n d t h e masti-
that may
111
I tl te r p l a y of s t r u c t u res
p r a ct i t i o n e r may we l l
u n d e r h i m . Th a t i s w h y
fe e l t he
o n e m p i r i c a l observ­
t h e forwa r d help
b y p r ov i d i n g a
ratio n a l
a p proach
to
d ra w n p os i t i o n , w e l o o k f o r a s t i ff t h o r a c i c k y p h o s i s ,
ation
f o r t a u t p ectoral is m u s c l e s , f o r h y pe r t o n u s o f t h e
s y s te m a t ic c l i n i ca l e x a m i n a t i o n d i rected a t d i s t u rbed
u p p e r t r a p e z i u s a n d l e v a t o r sc a p u l a e a n d f o r w e a k
f u n c ti o n .
lowe r parts of the trapeziu s ; and we must even bear
W e m u s t ask w h e t h e r t h ese c h a i n s a rc h a p h a z a rd
i n m i n d tha t t h e d i s t u r b a n c e m a y o r i gi n a te f r o m t h e
o r w he t h e r t h e re is s o m e u n d e r l y i n g p r i nc i p l e w h i c h
pelvis or even the lower extremities. I f the patien t
h e l ps u s t o u nd e rs t a n d a nd t h e r e fo r e p re d i c t t h e m .
a d o p t s t h i s forw a rd - d r a w n pos i t i o n w h e n s e a t e d , we
look fo r i nc re a s e d l u mb a r k y p h o s i s in the s i t t i n g
posi t i o n . We
a r a ised t h o r a x
T ra c i n g t h e e a r l y o n toge n e s i s o f p o s t u r a l a c ti v i t y
accord i n g t o V oj t a a n d P e t e r s ( 1 992) and K o l a r
( 1 996)
p r i n c i p l e beco m es c l e a L T h e m o s t
d ur i n g r e s p i rfil
e xa m i n e the
of t h e e x t e n s i o n
sca l e n u s m us c l e s ,
in the cranio-
the s p in a l col u m n )
c e rv i c a l j u n e l
temporoma n d i b u l a r
In shoulder
a t te n t i o n n o !
i nc l u d i n g t h e
c e rv i c o t h o r a c i c
h um erosca p u l a r
upper ribs, the
r a c e a n d i s t h e pre-
m a s t i c a t o r y m us c l e s .
How e v e r , the e x t e n s o rs
a rm we p a y
cervical spine
p a l t e rn h a d to d e v e l op:
but also to the
ribs and the
w e h a v e t o e x p e c t a pa i n fu l
p os t u r e , F o r t r u n k
m u scl e s
a n t ag o n i s t s
(trunk
extensors
k n e e e x t e n so r s a n d
k n e e n e x o rs ) b e c a m e s y n e rg i s t s for t h e m a i n te n a nce
a rc d u ri n g a b d u ct i o n , e x a m i ne j o i n t p l a y w i t h t h e
of p o s t u re and ga i t . F i r s t w e a n a lyse some b a s i c
a rm h o r i zo n t a l a n d e x a m i n e t h e c l a v i c u l a r j o i n ts .
fu n c t i o n s o f t h e loco m o t o r s y s te m .
P a i n fu l m u sc l e i ns e r ti o n s s h o u l d be s o u g h t ; w e m u s t
D i s t u rb a n ces o f t h ese b a s i c f u n c t i o n s , w i t h t y p i c a l
p a l p a te t h e e p i co n d y l e s a n d e x a m i n e j o i n t p l a y o f
t h e c a r p a l b o n e s . H e r e , t o o , d i s t u rb a n c e o f m us c l e
c h a i n s of a ffec t e d s t r u c t u res, a re g i v e n i n T a b l e 4 , 3 .
T h e p r a c t i c a l a d v a n t a g e s a re c l e a r ; n o t o n l y c a n
function in
shoulder gi rdle is
w e m ore re a d i l y assess t h e c o n d i t i o n of our p a t i e n t ,
i m po r t a n t , a n d a g a i n a fo rw a rd - d ra w n p o s i t i o n o f
b u t e a c h o f t h e d is t u rb a n c e s l is t e d c a n be t r e a t e d i n
the region of the
t h e s h o u l d e rs . i n v i cw o f
e v e n i f s e v e r a l m e t h ods m a y
weight carrying.
E v e n for
c h a n ge s i n t h e soft
(
e x a m ination
c l a r i t y ; such c h a n ge s
e x a m i ne t h e
a c terist i c
to m u s c l e s a n d j o i n ts .
erector
m us c l e s
trunci,
111
perform the
p i r i fo r m is ,
s p r i n g i n g tesl
a n d l yi n g o n
her s i d e ; w e
o f m usc l e s ( b u t n o t
s a c ro i l i ac j o i n ts a n d
t r i gger
o n s t a n d i ng, w e
painful
e x a m i n e a n te fl e x i o n s i t t i n g a n d t h e n p c r form t h e
t h e c h ro n i c s t a g e .
resi s t a n ce of fas c i a t o
o n the side t h a t i s n o t
symptoms; this is not
true o f hyperalgesic
zo n e s , h o w e v e r ,
s t r a i g h t l e g r a i s i n g test Th e n w e l o o k fo r t y p i c a l p a i n
T h e c h a i n re a c t i o n s g i v e n h e re a r e n o t m e a n t t o
p o i n ts a n d t e s t t h e l i ga m e n ts . I f pos t u re i s a ffect e d ,
b e c o m p l e t e n o r a re t h e y by fa r t h e o n l y o n e s . T h e y
t h e m u sc l es t h a t g o v e r n p e l v i c i n c l i n a ti o n s h o u l d
a re
be s y s t e m a t i c a l ly t e s t ed , a n d i f l o w - b a c k p a i n i s
' p r o g r a m m e s ' o f the m o t o r s y s t e m . A t y p i c a l c h a i n
p r o v o k e d b y we i g h t l i ft i n g , t h e p a t i e n t ' s s t o o p i ng
r e l a t e d to fo r w a r d - d r a w n pos t u re s t a n d i n g i s w o r t h
s t e r e o t y p e s h o u l d be e xa m i n e d .
These
examples may
t h e l oc om o t o r
system and i ls
d i s t u rb a n ce s of t h e
I ts e l f i s h ig h l y
o f symptoms,
i n g only function
t h i n k i ng o n l y
t e r m s o f the
applied, i.e. to
expression
of some
basic
functions
or
m e n t i o n i ng : h e r e a s a r u l e we fi n d i nc re a s e d t e n s i o n
s u ffi c e . T h e y s h o w h o w
d i ffi c u l t i s t h e
e n t i re o rga n l S ln ,
comp l e x a n d
the
w i t h TrPs i n t h e a bd o m i n a l m u sc l e s , i n creased
t e n s i o n in the w h o l e o f t h e bClCk a nd n eck m u seul a t u re ,
b u t tocks, a n d as a
rule at
a TrP i n t h e b i c e ps
of the site
d y s fu n c t i o n a t t h e fee t .
m e t h o d s t re a t -
m uscles d i sappe a rs i n
r e ll e x c h a nges a re
method, and not in
S i l l' e r s t o l pe a s ' p e l v i c
the method is
a v e r y t e n d e r TrP
a twi tch reaction i n the
which s e e m s v e ry
e l u s i v e , Y e t t o t re a t m a i n l y a t t h e s i te o f s y m p t o m s ,
l u m b a r regi o n , a g l u t e a l p a i n p o in t , T r Ps o f t h e
o f p a i n , i s t o fa i l , i f t h e t ro u b l e i s d i s t u rb e d f u n c ti o n .
coccygeu s a n d r e s p i r a t o r y d y s fu nc t i o n i n t h e u p p e r
Ill ,
It is by n o means e a s y to t h i n k i n terms o f
r e s p i r a t o ry t r a c t , ow i n g t o d y s fu ll c t i o n o f t h e p e l v i c
fu n c t i o n . I n s t e a d o f w e l l - d e fi n e d s t r u c t u re s , f u n c t i o n
d i a p h ra g m . T h e l a t te r fo r m s p a r t o f t h e a b d o m i n a l
Copyrighted Material
Examina/ion
cavit y w a l l a l o n g w i t h t h e
d i a p h r ag m
a n d t h e abdom­
re s p i ra t i o n .
B r ugger d e s c r i b e s w h a t h e c a l l s t h e ' s t e r n o ­
symp h y s e a l s ynd ro m e ' a s a c o n s e q u e n c e o f h a b i t u ­
ally s i t t i n g i n a ro u n d - s h o u l d e re d p o s i ti o n : fo r w a rd ­
d rawn h e a d wi t h i n creased t e n s i o n i n most of t h e
m u sdes o f t h e s h o u l d e r g i r d l e i n c re a s e d t e n s i o n i n
t h e short exte nsors o f t h e c r a n i o c e r v i c a l j u n ctio n ,
i n c reased t e n s i o n i n t h e a b d o m i n a l muscles a n d e v e n
i n t h e m u scles o f t h e t h i g h s . T o w h a t a n extent t h i s
d y s f u n c t i o n a l ch a i n i s reve rs i b l e can be d e m o n ­
s t rated i f t h e pa t i e n t c h a n ges i n to a n e r e c t ( lordot i c)
s i t t i ng p o s i t i o n w i t h t h e resu l t t h a t a re a s of t e n s i o n
w i t h T r Ps i n . t h e s e m u s c l e s i m m e d i a t e ly d i s a p pear
( see p . 24 6 ) .
I n a g r ea t n u m b er o f u s u a l l y s e v e re c a s e s w i t h
a c h ro n i c c o u rse we fi n d w h a t m a y b e c a U e d a
'c h a i n reac t i o n from s e ve r e n o c i ce p t i o n ' . U n l i k e the
fo rw a rd - d raw n p o s t u r e a n d t h e B r u gg e r c h a i n w h e re
the c o - c on t r a c t i o n pa tte rn h a s b e e n t h ro w n o u t o f
ba l a n ce , h e re we fi n d TrPs i n b o t h e x t e n s o rs a n d
fl e x ors m a i n l y o n o n e s i d e , b u t m u c h m o re fre­
q u e n t ly on the r i g h t . T h e re may be some (eq u a l ly
b a l a n c e d ) TrPs on t h e l e f t , too b u t these ar e m u ch
l es s pr om i n e n t . T h e m o s t s t r i k i n g fe a t u re a t fi r s t
g l a n c e is v e n t r a l pr o m i n e n c e o f t h e r i g h t s h o u l d e r
( w i t h t h e pa t i e n t supine) d u e to a TrP i n t h e u p p e r
p a r t o f t h e p e c t o r a l i s m a j o r , w i t h c o n c o m i ta n t TrPs
in the l o n gissi m us and s e r r a t u s a n t e r i o r .
T h e m u s d e s i n v o l ve d a re g i v e n i n Ta b l e 4 . 4 .
A s a r u l e i t i s s u ffi c i e n t t o t r e a t t h e m o s t r e le v a n t
TrP, o r a rest ricted j o i n t re levant t o t h e corr e s p o n d
i n g m usc l e ( e . g . t h e fi b u l a r h e a d a n d t h e b i ce p s
fe m o r i s) , a n d t h e e n t i re c h a i n ca n be e x p e c t e d t o
vanish.
I t s h o u l d be p o i n te d o u t h e re t h a t v i sc e r a l c h a n g es
prod ucing reactions i n the locomotor system fre­
quently t r i gg e r o f f c h a i n s o r p a t t e r n s t h a t a re o f gre a t
d i a g nost i c v a l u e a n d p rov i d e a b a s i s for r a t i o n a l
tre a t m e n t . I t i s o f p r a c t ic a l s i g n i fi c a n c e t h a t s u ch
c h a i n s a r e u s u a l l y fo rmed on o n e s i d e of the b o d y .
It is obvious t h at t h e se c h a i ns m a y c o m b i n e a n d
fo r m m os t c o m p l ex p a t te r n s .
The
t h e r ap e u t i c c o n s e q u e nces a re n o less
i m p o r t a n t , fo r t h e l i n k s in these c h a i n s r e a c t o n e a c h
o t h e r : t h u s , t re a t i n g a j o i n t may n o r m a l ize a m usc le
trigger p o i n t , o r v i c e ve rs a ; trea t me n t o f o n e tri gg e r
p o i n t may a ffect o t h e rs i n the c h a i n , as does t r e a t ­
ment o f a j o i n t i n a key r e g i o n . I n c h ro n i c c a s e s a n
i mm o b i l e fa s c i a o r sca r m a y b e h i gh ly re l e v a n t - a n d
re levance is d e ci s i v e . T h e k e y t o t h i s , h ow e v e r , i s a
d e e p e r u n d e r s t a n d i n g o f fu n c t i o n (d y s fu n c t i o n ) .
i n a l m u scl e s w h i c h a r e esse n t i a l f o r
,
,
,
­
and
its
14 1
dis t l l rbance
i n the c o n v e n ti o n a l , i . e . p a t h ol o g i c a l , w a y or w h e t h e r
w e s h o u l d a p p r o a c h i t a ccor d i n g to t h e p r i nc i p l e s o f
fu n c t i o n a l p a t h o l o gy .
fi r s t a n d fu n d a m e n t a l t a s k i n c l a s s i fi ca t i o n ,
a n d h e n c e a lso i n d i agnos i s , i s w h e t h e r we h a v e
to deal ( m a i n l y ) w i t h patho logy o r d y s f u n c t o n .
2 . Fu n c t i o n ( p h y s i o l o g y ) is as re a l as is a n a t o m y
1 . The
( p a th o l o gy ) .
3 . P a t h o l og y
c a n be
d e fi n e d
as
a r u le
both
as
to
l o c a l i z a t i o n and n a t u re . Fu n c t i o n o n the o t h e r
h a n d i s t h e re s u l t o f t h e c o r r e l a t i o n
a n d i n ter­
p l a y o f a w h o l e ch a i n o f d i ffe re n t s t r u c t u r e s o f
va rious loca l i z a t i o n .
4. E ve n w h e re t h e re i s s t ru c t u ra l p a th o logy t h e r e
a re a l s o c h a n g e s i n fu n c t i o n w h i c h c a u se c l i n i ca l
sy m p to m s .
5 . T h e c l i n i c a l p i c t u re c o r r e l a te s m a i n l y w i t h t h e
c h a n g e s i n fu n ct i o n , m u c h l e s s w i t h s t r u ct u r a l
p a t h o l og y . V e r y fr e q u e n tly i n deed p a t h o l ogical
c h a n ges d o n o t m a n i fe s t t h e m s e l v es so lo n g as
f u n c t i o n i s not i m p a i r e d . O n t h e other h a n d ,
c h a n ge s i n fu nction b y t h e m selves m a y c a u s e
v er y m a r k e d c l i n i c a l c h a n g e s in t h e a b s e n c e o f
a n y ( s t r u c t u ra l ) p a t h o l o gy .
6. Fo r t h e s a m e reasons even c l e a r ly d i a g n o s e d
p a t h o l o g y ca n be c l i n i c a l l y i r re l e v a n t (d isc
herniation
a t CT, s p o n d y l o l i s t h e s i s , sco l i os i s ,
e t c. ) , w h e re a s t h e d y s fu nc t i o n w hi ch c a n u s u a l ly
7.
8.
9.
10.
1 1.
The f u n ct i o n a l approach
of /oconlO/or jimc/ion
be d i a g n ose d o n l y by c l i n i c a l m e a n s c a n be o f
d e c i s i v e i m po r ta n c e .
If we d i rected o u r t h e r a peut i c efforts a t t h e
p a t h o l o gi c a l c h a n g e s o u r t h e r a p y w o u l d fa i l i n
s u c h cases; o n t he o t h e r h a n d , e v e n i f t h e
p a t h o l og i c a l c h a n ge s a re i m po r ta n t , we s t i l l m a y
i m p ro v e t h e p a t i e n t ' s c o n d i t i o n i f w e i m pro v e
fu n ction - Eor t h i s is ex actl y wha t c a n be a c h i e v e d
by rehabi l i tation . I t is, however, necessary to be
a w a re o f the l i m its o f w h a t ca n b e a c h i e v e d .
The d i a gn os t i c ta s k i n p a t h o l ogi c a l d i a g n o s i s i s
t o l oca l i ze t h e l e s i o n e x a c t l y a n d to d e t e r m i n e
its n a t u r e ( p r i n c i p l e o f l o ca l i z a t i o n ) .
The d i a g n o s t i c t a s k i n d y s f u n c t i o n i s to d e t e r­
m i n e t h e p a t h o ge n e t ic c h a i n a n d to a s s ess t h e
c o r re l a t i o n a n d r e l e v a n ce o f t h e i n d i v i d u a l l i n k s
( h o l i s t i c p r i n ci pl e ) .
The
mechanism
p rod u c i n g p ai n d u e to
p a t h o l o g i c a l c h a n ge s c o rre s p o n d s to t h e n a t u re
of t h e p a t h ol o gy i n t he c a s e ; if, o n t h e o t h e r
h a n d , f u n c t i o n is c h a n g e d , t h e m ec h a n i s m i s
m a i n l y d u e to i n c re a s e d t e n s io n a s a resu l t o f
d ys fu nct i o n .
I f t her a py is s u ccess f u l i n c o n d i t i o n s ca used by
pathol ogic a l c h a n ge s , it is co n t i n u e d u n t i l t h e
l e s i o n h a s h e a l e d , o r t h e d e c i s i o n t o operate is
taken.
the p rev i o u s c h a pt e r s i t s h o u l d be o b v i o u s t h a t
th e d e c i s i v e fi rst s t e p i n d i a g n o s i s i s t o decide
w h e t h e r we have t o a p p ro a c h t h e p a t i e n t ' s p r o bl e m
From
1 2 . I f t h e r a py i s s u ccessfu l i n c h a n ges d u e to d y s ­
f uncti o n , we s h a l l
a n o t h e r l i n k of
Copyrighted Material
probably d e c i de t o t r e a t
t h e p a t h o g e n e t i c c h a i n . If we
142
Manipulative Th erapy i n Reha bilitation
of t h e Locomotor S vstflll
Table 4.3 Chain reactions
Body
area
and .limCliol1
Fin dings
Paris
affected
Toe and foo t fl e x o r s , t r i ce p s s u r a e .
Lower e x t re m i t y - g a i t : s t a n c e
p hase , e x t e n s i o n ( i m p a i re d fl e x i o n )
h a m s t r i ngs, g l u t e i . p i r i fo r m i s , p e l v i c
d i a p h r a g m , l u m b a r e re c t o r s p i n a e
C a l c a n e a l s p u r . A c h i l l e s t e n d o n , fi b u l a r he a d .
i s ch i a l t u be ros i t y , cocc y x . i l i a c cres t ,
t roc h a n t e r
J o i n t d y s f u n c t i o n ( b l o c k a ge )
m a j o r a n d s p i n o u s processes L4-S I
S m a l l j o i n t s of foot
a n d a n k le , A b u l a r
h e a d . s a croi l i a c j o i n t . l o w l u m b a r s p i n e
Lowe r e x t r e m i ty
-
g a i t : s w i ng
p h a s e , fl e x i o n ( i m p a i re d
ex tension )
o f t h c fo o t a n d t o c s , a n t c r i o r
abdomin is,
t h o r a c o l u m b a r e re c t o r s p i n a e a n d u p p e r n e c k
[ n c re a s e d t e n s i o n
IldC<
E x t e n so r s
t i b i a l i s , h i p A e x o r s , a d d u c t or s , re c t i
e x t e nsors
" H " h m ""
PO' " "
Pes a n s e r i n u s , pa t e l la . s y m p h y s i s ( u p p e r
and
l a tera l a s p e c t ) , x i p h o i d
J o i n t d y s fu n c t i o n ( b l o c k a g e )
K n e e . h i p , s a c ro i l i a c j o i n t , u p pe r l u m b a r s p i n e
a n d t h oracol u m b a r j u n c t io n
Tru n k : body s t a t i cs
I n c re a s e d t e n s i o n (i n m u s c l e
p a i rs )
I
Te n d e r
S C M : s h o r t c r a n i ocerv i c a l e x t e n s o r s , sca l e n i
+ d e e p n e c k A e x o rs + diga s t r i c i : t rapez i i
+ l e v a t o re s
sca p Lt l a e , i l i o p s o a s + rec t i
a b d o 01 i n i s : e r e c t o r s p i n a e + q u a d ra t us
a t ta c hmen t p o i n t s
( re fe rred pa i n )
I
J o i n t d y s fu n c t i o n ( b l o c k a g e )
Poste r i o r a t l a s a rch a n d t ra n sve rse processes.
s p i n o u s p rocess o f a x i s . l i n e a n u c h a e . m e d i a l
e n d o f co l l a r b o n e , h y o i d , u p p e r
a n d v e rt e b ra l
lowest
m a r g i n of sca p u l a , x i p h o i d , s y m p h y s i s .
r i b s , i l i ac c re s t s
Cra n i oce r v i Cil l j u n c t i o n ( T M J ) . c c r v i c o t h o r a c i c
j u n c t i o n , u p p e r r i b s . t h orac o l u m b a r .i u n c t i o n ,
l u m b o s a c ra l
L i ft i n g t h e t h o r a x a t r e s p i r a t i o n
I n cre ased t e n s i o n
I
I
Te n d e r a t t a c h m e n t p o i n t s
J o i n t d y s fu n c t i o n ( bl o c k a g e )
a n d s a c ro i l i a c j u n c t i o n
U pp e r se c t i o n s of a b d o m i n a l m u s c l e s ,
sca l e n i , SCM, l e v a t o r e s , t r a p c z i i .
s h ort e x t e n s o rs o f t h e c r a n i oc e r v i c a l j u n c t i o n ,
p e c t o ra l e s ,
l e v a t or s c a p u l a e a n d t r a p e z i u s
Pos t e r i o r a t l a s a rch a n d t r a n s ve r se processes,
s p i n o u s process o f
s t e r n ocos t a l j u n c t i o n s a n d u p p e r r i bs
Cra n i o c e rv i c a I
j u nClio n ,
j u n ct i o n . upper
U pp e r e x t re m i t y
i m p a i re d fl e x i o n
-
pre h e n s i o n ,
I n c re a s e d tension
I
I
Te n d e r a t t a c h m e n t p o i n t s
J o i n t d y s fu n c t i o n ( b l oc k a g e )
a x i s , l i nea n u c h a e , me di a l
m a r g i n o f s ca p u l a .
e n d o f col l a r b o n e . u p pe r
F i n ge r
ce rv i c o t h o ra c i c
ribs, t h o r a c i c s p i n e
a n d wri s t e x t e n sors. t h e n a r , s ll p i n at o r s ,
i n fraspi n a t u s ,
biceps, d e l t o i d e u s . s l I p r a - +
u p p e r tl x a t o rs o f t h e s h o u d e r g i r d l e ,
i n t e rsc a p u l a r m u s c l e s
Proc. s t y l o i d e ll s + l a t e r a l e p i c o n d y l e .
a t t a c h m e n t o f s u p ra -
a n d i n fr a s p i n a t u s ,
sca p u l a e a n d t h e
a t t a c h m e n t poi n t s o f l e v a t o r
s p i n o u s process o f a x i s
E l bo w . a c ro m i o c l a v i c u l <l r j o i n t . m i d - ce rv i c a l
spine. cervicothoracic j u nc t i o n . upper ribs
Copyrighted Material
Examinrllion of loenmolO)" JimCiion
a n d i l s dislllrbol1ce
1 43
Table 4.3 C h a i n react ions (cont inued)
Boilv
a rell
Findings
111 1 11 l"n elio/l
U p p e r e x t re m i t y
p re h e n s i o n .
i m p a i r ed e x t e n s i o n
},""
PariS ajjecied
I n c re a s e d t e n s i o n
�
I
F i n g e r a n d w r i s t fl e x o r s . p ro n a to rs .
s u b sca p u l a ri s . p e c t o ra l i s .
" ' , , " ,, "" p o i o ,"
a t l a s p r o c e ss
( b l o c k a ge )
e n d o f co l l a r b o n e .
E r b ' s p o i n t . tra nsverse
M e d i u l e p i co n d y l e . mecl i a l
ste rn o c os t a l j u n c t i o n .
J o i n t d y s fu n c t i o n
S C M , sca l e n i
C a r p a l b o n e s ( ca r p a l t u n n e l ) . e l b o w .
g l e n o h u m e r a l j o in t , c e r v i co t h o r a c i c a n d
c r a n ioce r v i c a l j u n c t i o n + u p p e r r i b s
Head and neck . fee d i n g.
m a s t i c a l i o n . spee c h
s h ort
e x te nsors o f t h e c ra n i oc e r v i c a l j u n c t i o n ,
M as t i c Mory m u s c l e s . d ig a s t r i c u s , SCM .
I n cr e a s e d t e n s i o n
t r a p e z i u s . l e v a t o r , d e e p n e c k fl e x o r s ,
pe c t o r a l i s
Hyoid.
poste r i o r a t l as
a rc h a n d t r a n s v e rse
proce s s , s p i n o u s process o f
axis, l i nea n uchae,
upper ribs
u p per m a r g i n o f s c a p u l a , a ng l e of
Joint dysfunction
T a b l e 4.4 C h a i n due
to
nocice p t i o n
011 Ihe dorsill {(sp eC!
SCM. sca l e n i
S h or t neck e x t e n s o r s ,
P e c t or a l i s m a j o r u p p e r p a rt
L o n g i ss i m u s . serra t u s a n I .
sp l e n i i . s e m i s p i n . c a p . .
u p p e r t ra p e z i u s
S u bs ca p u l a r i s
I n fras p i n a t u s , te res m i n o r
Pe ct or a l i s m i n o r
R h o m boi d e i
Obl ique
abdom ina Is
Sh o r t t o e e x t e ns o r
Biceps
Pronator
Fi n ge r fl e x ors
Te m po r o m a n d i b u l a r J o i n t . c r a n i o c e r v i ca l
j u n c ti o n , ce rv i c o t h o r a c i c j u n c t i o n
1 5 . T h e refore w h oe v e r o n ly t r e a t s d y s fu n c t io n a t
O i l I i i I' l'elllJ'llI IIspecl
S h o r t adductors
( b lo c k a g e )
L o n g i ss i m u s
b i ce p s fe m o ris
S h o r t t oe fl e x ors
Trice p s
Gl utei.
S u p i n a tor
Fi n g e r e x te nsors
h a v e to t re a t t h e same l e s i o n ag<1 i n , we s h o u l d
fi rs t c o n s i d e r w h e t h e r t h ere i s n o t <1 more
i m por t a n t l e s i o n w h i c h we h a v e m i ssed o r u n d e r­
r a t e d t h e fi rst t i m e . To c h a n ge t re a t m e n t e a c h
t i me i s t h e rou t i n e approach.
13. I n p a t h o l ogica l co n d i t i o n s , s u ccess i s a c h i e v e d
by e ffective d rugs ( p h a rmacotherapy), o r p o ss i b ly
by su rge ry. r n d ys fu n c t i o n , s u c c e s s d e p e n d s on
the correct c h oice o f t h e re l e v a n t link, o r links,
o f a c h a i n a t the r i g h t m om e n t .
1 4 From w h a t h a s b e e n s a i d , i t fo l l o w s t h a t t h e
f u n c t i o n il l a p p roach i s m u c h m o rc d i ffi c u l t . We
may com p a r e p a t ho l o g y t o the ' h a rdware' a n d
d ysf u n c tio n t o t h e ' softw a r e ' of t he m otor syste m .
t h e p o i n t w h e re p a i n i s fe l t i s lost - o r ra t h e r h i s
pat ie n t i s .
1 6 . B e c a u s e c h il n ge s i n fu n c ti o n a r e re v er s i b l e i n
n a t u re i t c a n b e e x p e c t e d th a t , i f a d e q u a t e l y
t r e a ted ( a nd t h e c a s e i s n o t com p l i c a ted ) , t h e
e f fe c t o f t re a t m e n t i s i m m e d i a t e , g i v i n g t h e
i m p re s s i o n of a ' m i r a c l e c u re ' , w h i c h , h o w e v e r ,
c a n be p red icta b l e .
1 7. T h e r e l a t i o n sh i p between c a u s e a n d e ffe c t
u s u a l l y pres e n ts n o m aj o r p r o b l e m i n co n d i t i o n s
c a u sed by s t r u c t u r a l p a t h ology. O n t h e o t h e r
h a n d , i t c a n be v e ry s u btle i n c h a n ges d u e t o
d y s fu n c t i o n ; w h a t w a s o r i g i n a l l y t h e c a u s e m a y
b e c o m e seco n d a ry a n d v i c e v e rsa . C h r o n i c p a i n
o f a n y origi n w i l l p r o d u c e c h a n ges i n m o t o r
p a t t e rn s o r stereotypes w h i c h , i n t u r n , w i l l c a u se
dysfu nc t i o n p e r p e t u a t i n g p a i n . C h r o nic j o i n t
m o v e m e n t re s tric t i o n a n d trigger p o i n t s c a u s e
i mp a i re d m o b i l ity o f t h e fasc i a e , w h ic h i n t u r n
p ro d uce j o i n t m o ve m e n t res t r i c t i o n a n d m uscu­
l a r t r i gg e r poi n ts .
1 8 . S t a t i s t i c a l m e t h o d s a re v e r y u s e f u l i n we l l. ­
d e fi n e d p a t h o l o g y a nd should be m a n d a t ory i n
t h i s fi e l d . I t i s , however, m u c h m o re d i ffi c u l t t o
a p p l y t h e m i n c h a n g e s o f fu n c t i o n . E v e n fo r
diagnos i s , t h e s a m e c l i n ica l c o n d i t i o n ( e . g .
h e a d a c h e ) c a n be t h e res u l t o f a l o n g c h a i n o f
v a r i o u s d i s t u r b a n c e s , t h e re levance o f e a c h l i n k
con s t a n t l y c h a n g i n g . I n t h e r a p y , i f we h il v e
t re a t e d o n e l i n k su cc essfu l l y , i t w o u ld be n on ­
se n s i ca l t o repeat t h e s a m e t re a tm e n t . I f,
Copyrighted Material
1 44
Manip ula t i ve Th erapy
in
Rehabilitation of the Locom otor System
t h e r e fore, t h ere a re s t i l l sy m p t o m s l e ft, we have
to treat another l i n k in the cha i n . If the p a t i e n t
is t h e n withou t symptoms, t h i s b y n o m e a n s
i m p l i e s t h a t t h e fi rst tre a tm e n t was o f n o a v a i l .
Howeve r , t h is is very d i fficu l t t o assess by
sta t i s t ics.
1 9 . Psyc h o l ogy i s i mporta n t in every type o f p a t i e n t
fo r i ts i n fl ue nce on the a u to n o m o u s nervous
syste m , e.g. stress. In dysfunction, h owever,
psyc h o l ogy is part o f the pathoge n e t i c c h a i n
because t h e locomotor system is the e ffector o f
o u r m e n t a l a c t i v i t y , the orga n o f v o l u n ta ry
mov e m e n t . T h i s i s fu rther borne o u t by the fact
t h a t pa i n i s the most const a n t s y m p t o m , a n d t h a t
t e n s i o n a n d i ts re lax a t i o n p l a y a very i m po r t a n t
rol e . [ t is, however, necessary to decide h o w
re l e v a n t t h e psychol.ogica l factor is i n e a c h c a s e
and how am e n a b le to t re a t m e n t .
20. Mod e rn technol ogy e n a b les us to d i agn ose
pa t h ol ogical lesions m u ch more e ffe cti v e l y , e v e n
i f i r releva n t , a n d a lso to m a k e t h e m objective.
I n dysfu nc t i o n , tec h n o l ogy i s usually of li ttle use
a n d very c u m b e rs o m e . C l i n ical s k i l l rema i n s
decisive. This, however, is considered ' s u b j ective'.
s u ffi c i e n t w a r n i ng; t h e mos t i m porta n t s i gns are
re p e a te d relapses, the decreasi ng e ffec t of a l l
the rape u t i c measu res a n d progressi ve deterioration.
There is o n e i m porta n t warning note t o so u n d : how­
ever desirable i t i s to test immed i a te ly a fter treatment,
a p ositive res u l t , i.e. i m med i a te i mproveme n t of
objective fi n d i ngs, a n d s u bjective re l i e f, do not pre­
c l u d e pathology, i nc l ud i n g t u m o u rs . because of con­
com i t a n t b l o c k a ge a n d o t h e r reflex cha nges t h a t are
s u sce p t i b l e to a d e q u a t e therapy.
I n the case h istory described below, recurre n t
b l ockage i rrespect i ve o f m a n i p ulation l e d us to
s u s pect (correc t l y ) a t u m o ro u s grow t h .
C a s e h istory ( A . F . , b o r n 1 9 1 5)
T h i s p a t i e n t u n d e r w e n t s u rg e ry fo r a s u b c u t a n e o u s t u m o u r
o n t h e l e ft h y p o t he n a r , w h i c h c a u s e d pa i n a n d , t h e
same
year, fo r a D u p u y t re n ' s c o n t rac t u r e o f t h e fo urth ri n ge r o n
t h e l e f t h a n d . I n s p r i ng 1 95 9 . h e com p l a i n e d o f p a i n i n t h e
the n ec k , w i t h s t i ffn e s s . The p a i n g ra d u a l l y
a d m i t t ed t o h o s p i t a l i n
M a y 1 96 1 : pneu momye lography ( PMG) w a s n e g a t i v e . B y
a u t u m n , fo u r m a n i p U l a t i o n s h a d g i v e n n o re l i e f. W h e n
a g a i n a d m i t ted on 1 3 O c t o b e r . t h e p a t i e n t h e l d h i s h e a d
back
of
i n c r e a s e d a n d t h e p a t ie n t w a s
s l i g h t l y b e n t forw a rd a n d ro t a t e d to t h e r i g h t . A l l rota t i o n ,
es pec i a l l y to t h e l e ft , w a s i m pe d e d hy pa i n . E r b ' s poi n t was
Prob l e m s of d iffe r e nt i a l d i a g n os i s
T h e r e a re two m a i n catego ries: the fi r s t concerns
h e a d a c h e , visceral p a i n e t c . , which may be due e i ther
to d is t u rbed fu nction o f the vertebral col u m n or to
some other l e s i o n o f the locomoto r system such as
m uscle spasm, o r to visce ra l d isease. This ca tegory
cove rs the w h o l e fi e l d of medi c i n e , and the p ro b l e m
w i l l freq u e n t l y h a v e to b e solved w i t h the co l l a bor­
a t i o n o f speci a l ists in the releva n t branches o f
m e dici n e .
T h e seco nd c a tegory concerns lesions i n the
locom o tor system which m a y be d u e e i t h e r to
d i stu rbed f u n c t i o n or ( m a i n l y or p a r t l y ) to structu r a l
c h a n ges ( p a t h ology ) . This i n v o lves diffe re n t i a l d i a g­
nosis i n the l ocomotor system itse l f, i . e . t h e m a i n
object o f o u r therapy; e rrors i n d i ffe re n t i a l d i agnosis
i n t h i s c a t egory a re most u n fo r t u n a te and lie e n ti rely
w i t h i n o u r respo n s i b i l i ty .
I n ge n e r a l t e r m s , t h e p i tfa l l s are i n fl a m m a tory,
m e t a b o l i c o r neopla stic d i seases. S o m e scre e n i n g
tests s h o u l d be perfo r m e d a s a r o u t i n e procedure
( e r y t h rocyte sed i m e n t a t i o n rate , u r i c acid level and
X - ra y pictures). However, pa rtic u l a rly in the i nitial
stage o f the d isease, i t i s u s u a l l y i m poss i b l e to
recogn i ze the true n a tu re o f t h e co n d i t i o n , a n d such
patie n t s m a y be j us t as we l l treated w i t h re fl e x
( p hysica l ) t h e r a p y , i nc l u d i n g m a n i p u l a t i o n , as w i t h
a n a lgesics. T h e gre a t a d v a n tage of the u p - to-d ate
tec h n i q ues descri bed i n this book i s t h a t they c a n n o t
h a r m the p a t i e n t .
I f i t is i m possible to recog n i ze p a t h ology i n the
i n i t ial stages, the cou rse of t h e d isease s h o u l d g i v e
p a i n fu l o n the r i g h t ; s p i n o u s p rocesses
C2-C4 w e re pa i n fu l
was a broad hypera lgesic z o n e o n the
b a c k o f the n e c k . The r i g h t h a n d s h owed a s t a t i c
( fu n c t i o n a l ) t r e m o r . A t P M G w i t h 30 m l o f a i r by l u m b a r
r o u t e w i t h t h e p a t i e n t s e iil e d a n d b e n t fo rward, i t w a s c l e a r
t h a t a t C 2 t h e s p i n a l cord w a s m a r k ed l y d i s p l aced i n a
d o r s a l d i re c t i o n . The a i r p e n e t r a t e d in f ro n t o r t h e cord
a n d from t h e re u n d e r the a rc h of C l . T h e fl u i d s h owed
t y pic a l a l b u m i n o c y t o l o gi c il l d i ss o c i a t i o n . A root syn d r o m e
a p p e a r e d a f t e r P M G , s u r p r i s i n g l y , i n t h e C 8 segm e n t .
D i ag n os i s w a s a n e u r i n o m a o n t h e v e n t r a l aspect o r t h e
c o r d , p a r t i a l l y i n t ra d u r a l : a t o pe r a t i o n a n e u r i n o m a o f t h e
root o f C 2 ( r i g h t ) , w h i c h pro t r u d e d i n t o t h e i n t ra d u ra l
v e n t r a l c o rd s p a c e , w a s re m o v e d . T h e p a t i e n t w a s re l i e ved
o n pa l p a t i o n . T h e re
o f u n b e il r a b l e pil i n so o n a ft e r o p e r a t i o n . a l t h o u g h s l i g h t
p a i n p e rs i s te d .
I n o w l i s t s o m e typic a l p i tfa l.l s and suggest h o w t h ey
m a y b e a v o i d e d . I f re l a pses occ u r regu l a r ly at the
s a m e segme n t of the spi n e , despite pre ven tive
m e a s u res ( i n cl u d i ng re med i a l exercise ) , the prin­
c i p a l cause w iJ I be v isce ral d i sease a ffecting that
segm e n t , tumour, or some other pa t h ology of
correspo n d i n g l o ca l i za t i o n . When sacroil iac b l ockage
recu rs in you ng p a t i e n t s we m ust consider the
possi b i l i ty o f a n kylosing spon d y l i t i s . In women a fter
the c l i macteric, osteoporosis m ust be borne i n m i n d .
D iffe re n t i a l d i agnosis i s p a r t ic u l a r l y d i fficu l t but
i mporta n t i n the a c u te stage after i nj u ry . T here a re
cases i n which we c a n a c h i e v e i m m e d i a te re l i e f. but
i t is essen t i a l to rule out m aj o r trauma such as
fract u r e , l ux a t i o n , torn l i ga m e n ts or m uscles a n d
m u scle s h e a t h s , a n d h a e m a to m a .
A b n o r m a l fu n c t i o n may be d u e to a n o m a l y , i n
w h i c h case d i rect t re a t m e n t is useless a n d fu t i l e -
Copyrighted Material
Copyrighted Material
I'vIanip lila/ivc
Ir/
Rehab ili/l1liOi!
Locom%
re fe r red for r a i n d u e to ' m e re ' d i s t u r b e d func t i o n
r
o f t h e i n n u m e ra b l e p i t fa l l s a r o u n d h i m � no d a n g e r
a r e m o s t l y o u t p a tients w h o c a n n o t b e exa m i n e d a s
i s g re a te r t h a n t h a I o f o v e r-assu ra n c e . T h i s c h a p t e r
t h or o ug h l y a s t h o s e i n a hos p i ta l w a rd , T h e r h y
o n d i ffe re n t i a l d i a g n o s i s Cil n n ot b e m o re t h il n il
i n c h a rge 0 1
cases m u s t
-
a w a re
Copyrighted Material
5
Indications for treatment
Indications
for
treatment
should
not only or clinical d i a gnos i s but
be
mainly
genic analysis, determining which
the
result
of pa tllo ­
3. Soft tiss u e
(b) connective tissue stretch, pull or p ressure
lesion is most
(c)
i m po rtan t at a give n moment and is t he refore likel.y
to be the most effective object of ther apy. Every
of the patient's condit ion . For if our the rap y is
determined by the
(e )
at
and
(a) massage
(b) local anae sthes ia - need l ing
(c) electrica l stim ulation
control examination
the con dition of the p at ie nt should have changed.
imp l ying
a
change
in
fu rther treatment.
(d) ac u punc t u re
If the
(e) treatment of scars
pa tient 's condition is u nc hanged , treatment was not
(f) other methods of physical therapy
(g)
adequate and should not be rep eated without good
reason. A series of repet i t i ve therapeutic me a s ures
of t h e same type is more often than not out o[ place.
Critic<ll
asse s sme nt or the preced ing treatment and
constant correction of pl anne d t h e ra peu tic
measures
5.
It should be poi nte d out again that this concerns
soft tissue manipulation versus reflex therapy.
Remedial e xerc i se.
6. Correct i on of fa u lty statics .
7. Jmmobilization (supports ) .
8. Pharmacot h erapy .
9.
are e s sen t i al .
e x teroce p tive stim u lation .
4. Reflex therapy:
p rin ci p l es set out he re , it is
effcctive
likely to be
shifting of fasciae
(d) post-isometric relaxation
measure we take should thus result from a fresh
examination, to ke ep up to date w it h the course
m anipulat io n :
(a) skin stretch
10.
Surgery.
R e gi men.
pathogenesis and not conventional clinical d i agnosis .
S truct ura l p a t hol ogy must first be ruled out or be
found irre l eva nt to the case. For example, if the
patient s uffe rs from headache or pain at the sh o uld e r
Manipulation
and if my an a l ys i s shows that this is the result of
Manipulative
dysfunction of the cervical sp ine , this will be the
movement re striction (blockage) of a joint or a
obj ective of treatment. If, however, d ysfun ction of
spinal mobile segment, and
the cervical sp ine is due to
relevant to the patient's symptoms.
a
forward-drawn postu re
stanciing, and clisappears when the patie nt sits, the
cause must be sought at the pelvic girdle, or even at
the lower
extremity.
Hence treatment should start
only aiter compl ete examination.
Bea r i ng
treatment
this in mind,
is
indicated
is
if this is co n sid ered
many of the questions
frequently as k e d can be answered easily : what about
spond ylosis, disc p rolapse , scol ios is , j u ven ile osteo­
c h ond rosis, spondylolisthesis, osteop oros i s , or anky­
losing s pondy l it is? The an s wer
Methods of treatment
if t h e re
is
st rai ght for ward :
these conditions do not form the obj ecti v e
m a ni pulative treatment.
Nevertheless,
for
if in such
conditions movement restriction ( bloc kage ) is found
l. M a n i pu l <lt ion.
and considered harmful, then it should be treated
2. Traction.
with ad eq u ate manipUlative techniques.
147
Copyrighted Material
ill
of
Copyrighted Material
Indications for treatment
usually very gentle (the 'indirect method' of the
American
4
=
osteopat hs) .
S egmental hypermobility; all ty pes
lative treatment,
pa rticularly
of
m a ni pu­
thrust techniques,
should be avoided.
From
'She was manipulated three times within 1
149
week by a
qua l ifi e d chiropractor (the patient was supine an d the
reclination and ex­
manipulation consisted of rotation,
tension of the head ) '. This was followed by a short period
of
unconsciousness
and
later
by
t etraplegi a : artificial
respiration had to be ap plied and maintained for 36 hours.
po int of view we d i sti nguish
between technique s which p r od uce relative shift of
articu l a r facets a nd th os e whic h produce d istraction
(gapping). As a rule the latter are the most effective.
the technical
Recovery took several weeks and was co mp le te 4 months
later.
Thrust techniques in acute wry neck ( tort ic ollis) are
questionable in themselves,
but to
use the d angerous
combination of 'rotation, reclination and extension'
This
problem
problem .
With
op i nion
up- to-date
it is rather a
tec h niques
pseudo­
no
harm
should ever ensu e fro m m a nipulat i on, and in fact the
problem boils
need
mistakes.
what is contraind icated
is fault y
do wn to the
To put it briefly,
tec h niq ue .
to
avoid technical
What are the crucial faults? These are (1) the
p redom in a nt
a
(2) applying
p atient is properly
use of thrust techniques;
high-velocity thrust before the
relaxed and before taking up the slack (see Chapter
6): (3)
try ing
d isaster
to force
manipul a tion
of
any type
distraction as
de
rule brings relief, and therefore pain
a
aga inst painful muscle spasm or in a d irection that
in all d irections at
causes pain:
and
(4) th rust techniques should be avoided
in cervical back - ben d ing and rot ati on, because of
poss ible impingement on the vertebral artery; (5)
thrust manipulation should not be repeated at short
intervals ( le s s than 1-2 weeks).
In this connection I must also stress that too
insistent examination of mo bility in a painful
direction can be positively harmful, and at the
crani ocervical j unction even d angerous .
The d iscussion of contraindications derives from
the fact that serio us complications have been
des­
cribed in the literature, even with a fatal outcome
(Grossiord, 1966; Lorenz and Vogelsang, 1972; the
Memor an dum of the German Association of Manual
Medicine, 1979: K rueger and Okazaki, 1980: D vorak
and Orelli , 1 98 5) . Basing their calculations on the
re sults of a questionnaire sent to doctors of the Swiss
Association of Manual Medicine, the last two authors
compute the number of serious c omplicati ons a fter
m anipulation (thr u st techniques) at 1:400000. By f ar
the most imp ortant cause of serious complication is
undoubtedly damage to the vertebral artery.
U nfort unately, it is an almost constant feature of
this literature that the technique res pon s ible for the
d am age is not described - as if posto perat ive
complications were described with no details of the
operation techn iq ue used. There is one example
quo ted by Dvorak and Orelli (1985), however, which
seems to me so characteristic that I s hall comment
on it here:
A female patient of 35 collapsed while a ttendi ng a funeral
from wry neck for 3 w e e k s afterwards.
and suffered
(see
A n other grave mistake is the
is given much space in the medical
literature, but in my
Kleyn's test , p. 120).
use of thrust techniques
in short success io n for painful conditions which d o
not s how im provement ; co mplications occur m ost
frequently wit h such repetit io ns .
From this descript ion of a poss ibly dangerous
'technical mistake' s o m ething like a contraind ication
can be deduced : if it is a mistake to per form manip u­
lation in a p a in fu l d irection, then manipul ative
therapy must be discarded altogether if we prod uce
p ain in all directions. In fact , in mere d isturbance of
functi on (i.e. the object i ve of manipulati ve therap y )
pain is never found in all d i recti o n s at o nce:
is court ing
Contraindications
o nce is usually a
out of place.
sign of pathology
manipulation is
For
obvious
reasons
manipulation
of
hyper­
mobility is undesirable, but not manipulation
a
blocked
of
segment in an otherwise hypermobile
patient.
Thi s
b rings
indications'
us to another
which is often
category of
'contra­
strongly emp h a s iz e d :
tumours, in particular those with destructive changes;
acute i n flammatory conditions (such as tuberculosis) ;
fracture, etc. It is clear that no one in his senses
would try to treat this type of pathology by manipu­
lation; on the other hand, we know that, particularly
in the initial
stages of
such conditions ,
diagn ostic
s pecialist sees such
pa t ients in h osp ital, at a later stage, when the diag­
nosis is already easier. Nevertheless, usin g adequate
gentle techniques, the patient should come to
no more harm than from the ad m inistration of
analgesics - and suffer fewer side-effects. To m a k e
the point even clearer: if in a case of diagnosed
p athology concomitant blockage is considered harm­
ful to the patient's condition (as it frequently is ) ,
there is n o reason why this blockage should not be
treated if we know ho w . I have myself given manipu­
lation in acute decompensation of (benign) posteri o r
fossa tumour, with excellent temporary results.
Blockage at the craniocervical j unctio n can cause
great deter ior a tion in patients with insu ffi ciency of
the vertebral artery, and should be treated by expert
mobilization. It is most unfortunate that this condition
is considered by m any to offer a cont raindicat i on,
simply because technical errors in this s ituation are
particularly dis astrous .
error is often unavoidable. The
Copyrighted Material
ManipLiialivl'
/,01'01110101' Sr.,/(11I
ii1 Rehabi!ilalil1il
The course of manipulative treatment
treatment (mobilization)
In a routine case which is neithcr very severe nor
,1cute we treat those restrictions of
we think
I
expect some unpleasant reaction at the end of the
or during the next day or two, and if possiblc
IS �dvlsed about w hat to correct (or a vo id ) in her
dally regimen. A bout 2 weeks is a reasonable in ter val
the organisrn
to reac t and I
exami n a tio n is
more
(;x21mination; our di a gnu st i c
conclusions on first examination might be ca l led a
working hypothesis (except for very simple cases),
a
hypothesis on w hich we base the first therapeutic
ste ps : It IS at the second examination thilt th is hvpothverified and
on a plan
ITc;;liment.
the patient ffCi,
improved
tile conclusions
that
first exami
w ere
well founded. and we p roceed to treat what remains
to be cl e a red up. We m ay invite the pa t ie n t for re­
e x amination after 3 or 4 w e e ks , and if all goes well,
agall1 after 6 weeks . However, even if improvement
up the patient for sev eral
we should fol
1 lis, in view 01 Ihe
chronic
11
I I n p rovement
s,'(ond
1
examination, the first question must be: did she feel
bet ter for a few days, or not at all ? Treatment
sometimes produces a very marked but short-lived
effect.
At r e- examin a tion (wo distinct conditions
he found: ( .1
l ived, followed by relaps e , we must seek the under­
(e.g. cardiac ischaemia in recurrent lesions in the
upper thoracic sp ine) , for to go on treattng 010\'[would be mOll
ion in such
usele,s
as a rule,
be treated
by
expected to
10US cases w:11 not
manipulatIOn
have
alone
and can
a chronic course.
It
be
th en
is
important to. follow up the patient for a cO ll slde r a ble
time, 6 months or more, at intervals.
ma ni pulatio n lor tile
rliso be consJ(ic:reci.
of
True. IlE'l1Ipulation is
the
only if we
cmc:nt restrictioll
lIIeally relevanl.
the other hand, when a dmi ni steri ng manipulative
tre atme nt we should ne ver overlook bloc k a g e in key
regIOns, be cause this is mo st likely (0 c a us e relapse.
In other words , we indicate mi1nipulation for clinic-
h lock a ge in
This i,
alh
. aspect
revic)J1s in on1,:r
lu
introduci::r:
III
re gu lar feal
11111](.1, t h e r e is n strong
case to be made tor manip ula tive treatmcnt, for
example, in ch ildre n , physically very exposed indi­
VIduals, etc. (see Ch a pte r 8).
prevent
in to
�
rehabIiltalJon. Bcaring thiS
111
I.e.
Ilildings are
1
tre:ltment has given
ly reason is
lying cause, This then bec ome s our m a i n concern
preVclrlt
of these dlsturb:Jnccs.
1 he patien t feet;
because the
nostie enol. If the effect IS always good but shorl­
menl
1I.self to restored
w ay the
Important than the
,
whole
patient is
control examinal
it may be givell :1I:(\tI1l.:r chan ce , but
illl re-examination
after
if painless (
? ay,
If manip u lat i on has brought no rel ief at alL nor
any
impor t ant ,
which she can perform
seve ra l times a day.
Its or (which
uch
re l a psed ; (2)
on g ll1 al
have be e n corrected but new factors are
the condition
now producing similar symptoms.
In the lat ter case, we can consider the pati ent
.
Improved even if her complaints (her pai n ) seem to
be the s ame . There is even a highly characteristic
legion: th e le:;inllS
to
from one
to
in a caudal
next, until they
In
the
case ,
former
however,
we
must
ask
ourselves whether the first diagnosis was corr ect . 01
com plete ; whether we did not overlook an undcr­
lyi n g condition which may have produced relapse
at a key
column, an
position
ill
altogether
whether the
Ilw
at the othu
or the
elc.);
serious
appeared
If the case is very severe, i.e. if the b l ockage is
hard and palI1ful, and there is r estr i ction of larDer
b
.
.
sectIOns of the splllal column, then this type of
treatment IS lI1sufficlent and repeated mobili z a t ion
required, i.e. two
we should
times a
such
teach the
',elf-
Traction is essenti ally
�
a
form of manipulation, but
unlI e other methocls it is ge n erall y accepted in
tr aditIOnal medicine. W ithin the fr a m ewor k of mani­
pulative techniques, traction of the lumbar and
role: it is
:1
tli in (rue racllllllLn , y nd r o me s and
l umb31
w hene ve r [
.
of disc
is miH.k. In fact, if traction relieves s ymptoms III lhe
lu m bar regIon, then the diagnosis of disc lesion is
corro b ora t ed . In both th e cervical and the lumbar
cervlcti \jllllrtl column
region traction can be very use ful in sllch c onditio.ns
as acute wry neck and acute !umha go. Thc es<;enti21
tecl1l1icrd
ails are givcln
pter 6.
one i mportant
ever:
llilkver our
10 be macie,
1
the lIsefulrr,::;:, ,)1
tractIOn, It IS esse nt i a l to. test each case and apply
traction only where It gives reliel. If there is no
relief. we m ust first modify the t e chni q u e and then
.
.
deS is t lilt s til l fads. One of the reasons why traction
IS
fi rst
be
Copyrighted Material
badly to l er l l k d
I rellkd by
(e.g. in
hlockage, which
;
hefo e traction
;,ynclromcs). It
;
,
nUl
iUi/i,
opillion that manual 1
Chapter 6 are much b,'1
scalp, to adjanlill
tissue (metaca [[1;1!
In
aid
of special tables,
151
nly by soft
and even
II
to the ribs and
4.
m.'IIIi11etli
head).
Post-isometric relaxation (PIR): here, too, the
barrier is first engaged by stretching the muscle
Soft tissue manipulation
to the pOint where minimal resistance is encoun­
tered. This method, which will be described in
Soft tissue,
in particular
the
deeper layers of
connective tissue in muscles and fascia, is closely
detail in Chapter 6, has a similar effect to that
of the spray and stretch method (Travel! and
related to the motor system, both anatomically and
Simons,
III function. It is the function of soft tissue to be
to obtain muscle relaxation. It is effective not
stretchable while able to re�ist strf'tching, and to be
only in the trentment of
points) in the
[1111 ;11\0
shifted (even to a consldel ;Ible
yet
able to resist shift.
have
\983) and appears to be
most, pain point:;
usually been considered
points of attachment
secondary to changes
tension, or POIflIS
function. This is not
the muscle. It
particularly in chronic
or
Iginating in
com­
pletely painless
endocrine disorders (tile
be taught sell-IJ
or constitutional factol
only if there
!rI al
it
is possible to detect a (pathological) barrier that can
be overcome by adequate treatment, thus restorIng
function in the same way as in restricted joints or
muscles in spasm. If there are significant hyper­
algesic zones (HAZ). and in particular increased
resistance when shifting fascia, and, of course, trigger
points (TrPs), it is advisable to treat such soft tissue
lesions before performing joint mobilization (mani­
pulation), as the treatment itsf'lf miW howe con�idcr­
able mobilizing efFect.
(and should)
effective
particular
TrPs in the muscle; otherwise it is useless. An
effective alternative is stimulation of the antag­
onist (reciprocal inhibition).
Exteroceptive stimulation
The skin surface with its abundance of nerve
receptors is frequently underrated. As a result of
civilization it is largelY clepriveci of niltmal stimuli
by clothing, and
regions,
the feet, by shoe,
I. Skin stretching: this
algesic skin zones. II
of some massage
skin,
(the
like rolling a fold 01
'pince roulee' of Maiu,lk
01 L t'ube
lies it
and Dicke (1951)), but
is absolutely painless, much less time-consuming,
and can (and should) be used by the patient
himself. Skin stretching should only be indicated
for increased tension in the skin surface or, more
precisely, for increased resistance to stretching
over a specific area of the skin. It can be applied
to a very small area, such as the hyperalgesic fold
between the toes in a radicular syndrome, or the
skin over a periosteal pain point, with very good
applied
effect. Being entirely
even to hyperalgesic
2. Connective tissue
connective tissue, and
tissue, in taut muscles
can form a fold bet\h'lll nUl
hand) which engage,
tension. Where a fold
by the fingers may engage the baffler.
3. Whenever we find restriction of mobility of the
deep layers of connective tissue against bone
(mainly in the deep fasciae), restoration of normal
mobility is indicated. This also applies to the
..
a specific method
stimulate
must be
is by stroking of
C'hanges in
carefully chosen
lowered, most
muscular tonus,
frequently require
t:hronic pain
Lreatment,
indication
points (e.g. epicond\
even if everything
is reiative increased or decreased surface sensibility
over a certain area, most characteristically the sole
of the foot. Self-treatment is easy and includes
walking barefoot and playing with small objects.
Reflex therapy
This acts on the same tissues and structures as
manipUlative
traditional
therapists.
III the soft
methods, principally
It acts particularly
tissues.
Massage
This term covers
(11
ues which
have developed from lime Immemoriai; they are
applied to the soft tissues and even to the perio­
steum. It is not within the scope of this book to deal
with massage in any detail. Rationally applied, i.e.
from the clinical point of view, it should be used
Copyrighted Material
152
Manipulative Therapy in Rehabiliwlion oJ the Locomotor System
when and where changes are found in the tissue,
It is interesting that, just as after manipulation, so
changes that consist mainly in altered tension. The
after successful local anaesthesia or d r y needling, the
experienced masseur adapts his technique so as to
immediate relief we obtain is often succeeded the
give relief, i.e. to lessen tension in the muscles as
next day by a painful reaction, after which the thera­
well as in the skin and the connective tissues. Deep
peutic effect establishes itself. This treatment should
fricton may
therefore not be repeated before 6 or 7 days have
be applied
to
pain points on the
elapsed. Repetition is indicated if the method has
periosteum.
Bearing this in mind, it would seem that massage
proved successful, yet some pain remains.
is a universal method applicable in all reflex changes
produced by pain (nociceptive stimulus); indeed, it
is widely used in this way. Some techniques are
Electrical stimulation
pleasurable, giving immediate relief and being very
Here we obviously face a variety of methods with
popular with patients. There are other massage tech­
similar effects, which are apparently interchange­
niques which are painful. Unfortunately, the effect
able. To these must be added methods of physical
of massage is usually only short-lived, whereas the
therapy such as transcutaneous electrical stimu­
procedure is very time consuming. It is, moreover,
lation, and other forms of electrotherapy which
a
produce a similar effect on skin receptors and in the
purely
passive form of treatment, demanding
almost no cooperation from the patient. We there­
subcutaneous tissue. They have to compete. too,
fore prefer to indicate massage only as a preparation
with other traditional methods including not only
for other, more active and more effective methods
massage, but poulticing, cuppin.g, capsicum plasters,
of treatment, and not as the sole therapy.
etc. The clinician has therefore
a
wide range of
choice, the 'ideal' method being painless, without
risk, without side-effects and if possible applicable
Local anesthesia - needling
by the patient herself.
One of the most widely used methods of treating
painful lesions is local anaesthesia, or needling. It
may appear unorthodox to deal with these two
Acupuncture
methods together, yet one does not simply use local
It would be burying one's head in the sand not to
anaesthetics to relieve pain for the short period
mention the ancient method of acupuncture in this
during which the anaesthetic has effect; the popu­
context, the more so as it is now w i de ly used and
larity of local anaesthesia is due to the fact that its
discussed. There can be no doubt that acupuncture,
e ffect far outlasts the direct (pharmacological) effect
too, achieves its results by evoking reflex mechan­
of the anaesthetic, and seems not to be dependent
isms. Difficulties arise the moment we attempt closer
on it; in fact, Kibler (1958) uses sodium bicarbonate,
analysis and classification of the mode of action. The
and even subcutaneous air or gas have been used.
orthodox acupuncturist indicates treatment according
Direct proof has been provided by Frost e/ al. (1980)
to disease, without reference to the pathogenesis,
in their 'controlled
double blind comparison of
although the more 'enlightened' admit that acupunct­
Mevipacain injections versus saline injections for
ure should be used in cases of disturbed function
myofascial pain',
rather than in structural pathology. The choice of
showing that, if anything, the
physiological saline solution was more effective. The
acupuncture points according to the viscera and of
common denominator of all these methods is, of
'meridians' without clinical examination of t hese
course, the use of the needle. The effect, how­
points is based
ever, appears to depend very much on the needle
scientific verification. For scientific analysis. there­
purely on tradition and not on
touching the painful structure exactly, if possible
fore, it will be necessary to examine not only t he
so as to reproduce the pain of which the patient
complex method as a whole, but its simpler elements,
complains, whether an anaesthetic is used or not. If
one by one.
One such element is the effect of the needle: dry
we succeed in finding the exact spot, we produce
analgaesia
immediately.
whether
we
use
local
needling was reintroduced to modern medicine by
anaesthetic, a saline solution, or simply a dry needle
Travel! and Rinzler (1952) and I myself proved the
(Lewit, 1979).
analgesic needle effect (Lewit. 1979) in 271 out of
Local anaesthetics are of course necessary if we
312 applications of the needle to pain points, in 241
want to induce anaesthesia of nervous structures,
patients. There is sufficient clinical evidence of the
for example in nerve-root infiltration or epidural
efficacy of the treatment.
infiltration in radicular pain.
On the other hand, there appears to be
a
growing
One special method using local anaesthesia is that
tendency even among modern Chinese doctors to
of producing blobs on the skin by intracutaneous
choose their points not according to the tradition.al
application within a hyperalgesic skin zone. Here
'meridians', but on the basis of the segme ntal t h eo r y
again a similar or more intense effect can be obtained
of innervation. Instead of needling. electrical stimu­
by using d istilled water.
lation is also being introduced (Chang Hsian Tung.
Copyrighted Material
Copyrighted Material
of
Copyrighted Material
1i'·1/menl
lS5
established in a number oi
should be told
which should be great
increases: she
corr e ction
gra duall y , and
at regular
intervals of a few weeks.
Treatment of faulty statics
The ci iagn () s is of fa u lty statics has been de s c ribe d in
Ch a p ter s:; ancl 4. In so far as the cause is muscular
or extcl'Ilill in tl uences , faulty statics must
be treated accordingly. The most i mportant is a
i m b a l an c e
forward-drawn posture due to dysfunction of the
muscles of the pelVIC
Here we are concerned
in t he
pelvic region, (lnd
heel -p a d or by raisilil'.
posit ion . This is a nH
would a pp ear at first
aid is const antly used.
if the pam
C'h ilpt c r 8, p 258).
panlcularly
by
a
sitting
than
if the
at a
It is not a matter of indifference whi c h type of
correc t ion is used. A heel - pa d fitted into the shoe is
practical, but has the disa d vantag e that the shoe fits
less well. If po ssible , it is better to lower ( sho rten)
the heel
of th e other shoe. This is advisable on ly
where the d i fference is not greater than 1-2 cm.
Where the difference is grea t er, the whole sole m ust
be thicker on the side of
short
so as not to
p osition of
make too much
th e two feet .
If the pe I vis i:;
no apparent
the base of
difference in
the vertebral
find that obliqu1I1
corrected, we shall
I
the patient
permanent chan ge in
is sitting or standi
be straightforward. [01 I
Ilcrcnce in
leg length is due to f ai rl y recent trauma. In flat foot
on one s id e only, we can see the effect of an arch
support if the p,ltient stan d s with her weig h t on th e
outer edge o[ tile sole, ancl we observe that this
stt'aightens the pelVIS.
In the majontv of case s, how cve r , obliq uity
develops slowlv d u nng g rowt h . and as it increases
compensation dev elop s ancl assessment is i m poss ible
without exact X - r a y analysis s\lch as that described
correction
in C hap ter 3. However.
can never be a quesl
alone,
but must be decided
Clinically, static pa i n h
chronic
course, as a rule dele!
cXllmmation
static load, i.e. standil!!;
we expect signs of pel vlc
d e viation,
eO!Tcction
and pelvic sh ift (sec Chapter
should bring about clinical imp rov e ment . As shown,
however. spinal stat i c s can be checked rel iab ly only
by X-ray u n cler standard conditions: hence it would
usually be incorrect to indicate static correction on
clinical g rounds alone. If clinical and X-ray findings
are in agree me nt , we are j usti fi ed in indicating
correction.
There arc some p r a ct ical poi n ts that must be
st resse d here. The first is the immediate reaction to
a heel- p a d . If a thin S(It.,
I
uncler
the foot of a no r ma l
10 put
h e r legs
her weig h t e qual ly on
straight, she will
II pelvic
correction ( a thlll
Ischial tuber os ity when the patient is seated, in ad di tio n to the
he el - pad when standing.
obliquity may re spo n d
in three
different ways: she may
c(Hofort-
able, she may feel no
In t he first two cases
object.
the I' ll1 ent to
outset. and she
should be i nstruc t e d to wear the pad in her house­
slippers as well as in her o ut d o or shoes. In the last
case, however, there may be an un favoura bl e reaction,
ancl time is needed for the p a tie n t to adapt . She
to prescribe
The most frequent and most serious fault in
sitting. of course, is excessive lumbar ky p hosis due
to hype rmob i lity of the lumbar s pi ne. If we do n ot
presc r i h e supports we should adv ise the patie nt to
sit in the oriental manner, with feet crossed and
knees apart, or on her heels in the J a pa n e se
way.
Another p o sit i on is thelt advocated by BrU g ger (see
IO f ward and the
p. 246), in which I
thoracolumbar
balanced,
sim ply to raise I
or
a saddle.
Immobilization
In acute lesions
�ysLem, muscle
spasm clea rly indicates that r est and i mmobi .lization
is required. This can be particularly evident
acute trauma. when the healing
a fter
of damaged tissue
makes immobi.lization imperative.
Immobilization
itself becomes a problem , however, once the con­
dition becomes chronic, and if we aim at full recovery,
i.e. the restoration of normal function, immobiliza­
tion presents an outright obstacle. T h us immobiliza­
tion, for us,
measure in
can never be more than a te m porary
provement
no hope of functional
immobilization
Unlike immobilization.
not g re a t ly interfere
ion, i.e. imwhere there is
permanent
necessary evil.
supports need
wllll(: p rotecting
L.J nf ort un a tel y ,
[L'1l1 in working
conditions in techni cal l y advanced countries, and
h y p er mobile subjects with lax muscle s and l igamcnts
frequently find it diffficuIt to adapt, in particul ar if,
as in most modern means of public transport, j olting
the patient
agalns!
static over strain
is added.
Copyrighted Material
Rchunilirutio}i
Copyrighted Material
Copyrighted Material
6
Therapeutic techniques
r e l ax at i o n
is essential in o rd er to
[n the precedi ng ch a pte r s the i m port a n ce and the
relaxed, and his
dia gn osis of disturbed function of the locomotor
proc u re relaxation of the patient. As a rlli e the
system have been explained, and [ have desc r ibed
direc t i on in wh i c h the thernpist's hand
the cl i n ic a l l y s i g nifican t reflex changes i n v o lve d and
tinues the line of his fore a r m , but whenever possible
m o ves
con­
indicated the most important therapeutic m ethods. As
the movement should come from the whole body: it
it is impo ssible to describe nil these techniques in
often co m es from the Feet. as in throwing the d i scus .
detail in this ch a pte r , 1 here confine myself p rincip a l ly
to ma n ipula tive techniq ues nnd the s peci fic forms of
reme d i al exercise, with a few anci llary tec h niques.
The t h e r a pi st' s movement must n e ver be forced,
c ram ped or e x haust i n g: if he is e asi l y tired he must
be making a t echni c a l error. For manipulation of the
spi n a l column the body of the therapist and that of
the p atie nt must
Ma n i p u l at i o n
m ov e
in harm ony , like a c oup l e of
dancers : this is the secret of ge n tl e , flowi n g and
elegant tec h n iqu e and is also valid for examiniltion.
The sole a i m o f manipulation is to restore normal
m o bility mainly of joints, inc l ud i n g j oi n t play, but
<1lso mobility between soft tis sue l a ye rs , or soft t i ss ue
and bone. Two major types of man i pula t i o n can be
Fixation
One o f the bon es a rt ic u l ati ng i n the joint bei n g
distinguished: (I) mobilization tec h n iques : and (2)
m a n ipul a ted should be fi xed
thrusting tech n i q ues. I will sta r t, however, wi t h a few
mobilized. In ex t re mity joints it is us u a l l y the proxi­
wbile
the other
is
mal j oint that is fi x ed, i.e. supported by the table or
gene ra l p r inci ples.
by the body of the therapist. For elTective fix at i on
it is advisable to move oilly one j o in t. Tn the spinal
The positi o n i n g of the pati e nt
column fixation is ach i e ve d by correct posi t ion ing
The p atie nt shou l d l ie (o r sit or s t a n d) so that she
can
re l ax, so
thnt the j oin t to be treated is ac c essi b le,
and so that one of the arti c ul at i ng bones is either
('looking') and where poss i b l e by dire c t contact with
the therapist's ha n ds . Good fixation of the pe l v is can
be obtain ed if the patient sits astride the table.
fixed by the pati e nt's own weight or can eas i l y be
fixed by the therapist. The height of the m a n ipu ­
lation table from the floor should be adjustable as
required: in g ene ral , it sho ul d c orr es p on d to the
The position of the joi nt a n d the
d irection of treatm e nt
distance of the t herap ist' s fingertips from the floor
The j oint to be tre a t e d must not be in
when he sta n ds erect wi th arms hanging l oosely
ill w hich the c aps u le and the l igaments are over­
down and fingers stretched.
a
position
stretched, i.e. it must not be locked. The direction
oJ treatment (manipulation) may c or respo n d to the
i mpaired j oi nt mobility or to joint play,
The position of the therap ist
i.e.
to
relative shi ft or di s t r a c t io n (Figure 6.1).
This is in many ways decisive fo r the therapist's
Ac cor d ing to Kaltenborn (J 976) the direction of
in or d e r to be
joint p l a y is not purely haphazard, and depends on
te ch ni q ue . He must be
com forta b l e
15K
Copyrighted Material
Therapeutic techniqlles
u u
n
n
Figure 6.1 Possible directions
LJ
n
of joint play
whe the r the concavity of the joint is proximal or
Figure 2,6, p, 14), In the for m e r case, shi ft
of the distal partner. w h ich has to b e restored, is i n
the opposite direction to t he impa i r e d movement.
whe reas in the l atte r case t h e s hift of t h e distal
partner is in the same dire c t i on as impa ired mobili ty,
For this reason the first phalanx should be s h ifted
main ly i n a p a lm a r direction (if flex ion i s rest ricted )
and t he ca rpa l bones against the radius in a dors a l
di rection if pal m a r fl e x io n is res tricted (see F ig u r e
6.3, p, 162),
distal (see
s ure we have i nd eed reached the end-position. by
s l i ghtly decreasing t h e range of mov eme nt and the n
i n c reasing it agai n. to e s tablish w h e t h e r we mee t
re s i s tance a t the same poin t : in ot h e r words, we
spring the jo i n t in end -po s iti on . w h ich is exac t l y
what we d o in pass i v e mobi l iza t i on, R e pe a ti n g tbis
procedure several times will show that even in il
norma.l joint the range of movement increilses. i,e,
we rea c h t h e b a rrier ( take up the slack) after a
l on ger interval. In a re stricted joint this increase w ill
be much more abr u pt. The re are t wo m i s takes to be
avoided in this t y pe of s pringing (repetitive) mobil­
izati on: (1) we must be careful to remain in end­
position a n d not return to the n e u t r a l position of the
joint, i,e, t h e rang e of the springing movement must
be sm al l and v e ry well con t ro l le d ; (2) springing back
is even more importa n t fo r t h e re s t o ration of
m o b ility than is t h e pre ssure we exert; therefore even
i f t he ra nge of movement i n c reas e s. we must n ever
i ncre ase o u r p r e ssu re , The join t must be al lowed to
move back almost to the ini tial end-po s i tion, In t his
way
This i s a crucia l step before trea tment begins. whether
merely s tre t c h ing of soft tiss u e o r s h iFti n g a fascia.
pos t-isometric muscle relaxation, or t r eatm e n t o f a
join t. We try to b ring t h e joi nt to the barrie r, i,e,
c l ose to end ra nge either of normal func tion or, m o re
freq uen t l y a n d parti cularly in extremity joints, of
j oi n t play, Distra ction of t h e joint is helpful, In the
spinal col u m n it is not always possib l e to make t h e
dis t i nc t ion between mobility and j oin t play. the
move ment of a s ing l e mob i le segment (in i t s e l f
i m po ssibl e to achi eve b y active moveme n t ) playing
to some extent the role of joint p l ay , The barrier or
end-position is never reac hed s ud d e n ly in norm a l
m o v emen t ; sudden re sistance i n the end-position is
a sig n of blockage, We know tha t we have taken u p
the slack th e mome n t w e sense t h e first slight
incre ase of resistance, This must be car ried out very
gently, w ith t h e pat i en t rel axed, The most impo r t a n t
so urce of error is to mistake active resistanc e by t h e
pat i e nt for t h e sig n that w e h ave taken u p t h e s l ack,
This in va ri abl y happens if we cause p a i n - s ome t h ing
to be a v o i de d at all costs,
Ma n i p u l ation proper
Afte r taking up
the range of s pringing will increase but
never
pressure w e exert.
Thi s type of mainly passive mobi l i za t ion is effe ct­
ive in joints that are not e x cessive ly fixed by m u s c l e
spa s m whe n blocked. suc h as t h e sac roi l ia c and
acromiocl avicular j o i nts. and many e xt rem ity joi nts,
[t is les s efFec t ive in t h e spi na l column, howev e r.
a n d here pas sive mobi l ization is used mainly as a
p re p a r a t i on for thrusting te c h niques. and as after­
t reatment. To make mobiliza t i on of the spin a l column
ful ly effective w e ha v e learned to u s e tec h niques of
musc u l a r faci l it a t i on and inhibition (neuromuscular
the amount o f
Ta k i n g up the slack (en g a g i n g t h e
barrier)
we have two ma in me ans
mov e m e n t: (l) by gen t l y
sp r i n gi n g the joi n t in end-position (mobilization); or
(2) by making a t h rust from en d -po s i t ion,
of re s t o ring
ISl)
t h e slack
restric ted
Mobilization
At the first s lig h t inc rease in re s i s t a nc e while we are
taking up the s lack (engage t h e barrie r), we make
techniques),
Mobilization using neuromuscular techniques
Some t ec h n iq ue s aim at spe cific muscles or muscle
gro ups. w hile oth ers have a more gene r a l effec t .
by
Isometric confl'action of muscles i n tension, followed
( M it ch e l l et al., 1979) or.
p refe r to cal l it, PIR - post-is ometric r e l axa tion ,
Un like the widely used t e c h niq u e developed by
Kaba t (1965), we use onl y minimal resistance dur i n g
t h e isometric pha se, Afte r the slack has been taken
up, the pat i ent ex erts only a minimum of pres s ur e
in the opposite d irectio n from tha t of t h e movement
rest ricti on. holding it for about 10 s, She is the n told
to ' le t go'. and the o p erator wa i ts, or even repeats
the 'Ie t gol', u n t i l h e fee l s tha t the pat i e n t has tru ly
relaxed, On ly t h en does he carry out his movement
in the directio n of t h e re s t ric t io n - but then o n l y to
t h e point where the s l i g h te st res i s tance is felt, i,e,
only as fa r as t he pa tien t 's re l axa tio n w i l l a l low. It
is important to pro fi t from h e r relaxat ion as long as
the range of movement increases spontane ously: this
may be for 10 s or even longe r. When the t h e rapis t
feels no fu r t h er relaxation the procedure is repe a t e d
from t h e ne wly ga ined position: the g r ou n d t h a t has
relaxation - isometrics
as I
Copyrighted Material
160
in Rehabilitation of the LocomoLOr
Manipulative Therapy
been won must n o t be lost again. If re l a x a t i o n has
been satisfactory, the time a l l owed for isometric
resista nce m a y be s l i g h t l y reduced, but if rel axation
is i n s u fficie nt, resista nce may be pro l o n ged for up to
h a l f a m i n u t e . This procedure can be rep e a t ed for
as long a s the the rapist con t i n ues to observe i n cre as­
i n g ra n ge of move m e n t, b u t u s u a l l y t h ree to five
repe t i ti o n s suffice. I have to s t ress a t this poin t
t h a t l e n g t hen i ng of a musc l e or i ncreased ra nge of
move m e n t owing to re laxation must be achieved
exclusively by the p a tie nt s re l a x a tion w hich is on ly
m o n i tored by the t h e r a p i s t never by passive st retch!
Re l axation i s an active process: 'we cannot relax the
pa tient'.
Antagonist inhibition - By stimulation of the
a ntagon ists it is possib le to a c hie ve i n hib i t i o n of
muscle s in s p a s m ( h arbou ring TrPs) as effectively as
by PIR. This me t h od has been u n d u l y u n derrated,
asssuming that it is effective o n l y if considera b l e
fo rce i s used, t h e n giv i n g the i mp ressio n t h at t h e
the rapist h a s t o strugg l e with t h e pa tie nt. This is
avoided very simp l y: t he pat i e n t p u ts up o n ly
moderate or s l ight resista nce (in the direction of the
a n t agon ists) a n d t h e t h era pist uses rhyth m i c i nte r­
mitte n t sti m u l i. Th i s is so e asy th a t we n ow comb i n e
PIR w i t h rhythmic a n ta go n i s t stim u l a tion ( w i t h t h e
patie n t in t h e s a m e posi tion)
Direct repetitive rhythmic muscle pull, under certain
conditio n s, to produce mobiliza t i o n di rectly, e .g . t h e
t h e r a p i s t ca uses r h y t h m ic a l contraction s of th e
scale n us i n orde r to m o b i l ize the first t w o ribs o r o f
t h e psoas to mobilize the thoracolumbar juncti on.
These techniq ues are a p p l ied to specific musc l e s
o r m uscle groups.
The foll owing tec h n iques have a far more ge n era l­
ized e ffect .
Respiration ( s e e p . 2 7 e t seq. ) - I t i s o f grea t
practical significance that, as a rule, i n h alation h a s a
facil itating a n d e xhalation a n inhibiting e ffect o n
m uscles. Therefore, it i s usu a l l y a p propri ate t o com­
b i ne inh a lation with isome tric resista nce a nd exha l­
a tion with re l a x a tion. However, t h ere are i m porta n t
e xcept ions t o t h i s rule: during re troflexio n o f t h e
thoracic s p i n e , maxim u m exh a lation p roduces addi­
tional m obil ization of the t h oracic spi n e i nto retro­
flexion by contractio n ( facil ita tion) of the t h o racic
e rector spinae, w h ile i n a kyphotic positio n o f the
thorax deep in h a l a ti o n p roduces mobilization i nto
flex i o n . Even m o re importa nt is the mobilizin g effect
o f res pira t i o n during s i d e-bendi n g ( G ay m ans, 1980) ,
d u e to a lternating fa cilitation a n d i n h i b i ti o n o f
indi v i d u a l segm ents o f the s p i n a l colu m n ( see p . 27) .
As t h e e v e n segme n t s a re facilitated during in­
h a l a ti o n and inhib ited during exhalatio n , in these
segmen ts we comb ine t h e isometric p hase w ith
inhala tio n , a nd relaxation w ith e x h a l atio n; in the
odd segm e n ts t h is i s reve rsed. To be effecti ve,
respiratio n m ust be suffic i e nt l y s l ow, and dee p . The
i ntense faci l i t ative ( inh ibi t ory) effect o n m u scles of
'
,
.
System
'respiratory syn k i nesis' (see pp. 28-29) can be u sefully
a p p l i ed, e . g . in isometric ce rvical or lumba r tract i on .
Eye movemenls - These facilitate the movement
o f t h e head a n d trunk i n the direction o f the patient's
gaze and i n h i b i t m ov eme n t in t h e opposite direction .
This h o lds for l i fting t h e head and tru n k a s we l l as
for stooping and rota tion; it i s not t r u e for side­
bending, but loo k i n g up fac i l itates straighte n i n g u p
from side -be ndin g. E y e movements s h o uld not be
exaggerated, howeve r; accordi ng to G a y m an s (1980)
maxim u m excu rsion has an i nhi bitory effect.
A b o ut using t h e force o f grav ity fo r PIR, se e
p . 210.
Combinations - It is obvious t h a t t h ese methods
le nd themse lves to use fu l com b i n ation, i n pa rticular
PIR w i t h respiratio n and eye movemen ts. This has
the e n ormous adva n tage of a u tomation: i n stead of
te l l i n g t h e p a t i e nt to 'press w i th mi n imum force o n l y a few gra ms', we n ow te l l he r to look to the
right and breathe i n slow l y (if rotation to the l eft is
restric ted), a nd t h e n to l ook to the l e ft a nd breathe
o u t, t h u s a u tomatica l ly producing the correct resist­
a nce during the isometric phase, followed by re lax­
a t i o n . For t h e m obi lization of side-bendi ng i n an
eve n segm e n t, afte r taki ng u p the slack we ask the
p a t i e nt to look u p a n d breathe i n slowly, and then
to look down a n d b reathe out.
I now come to some of t h e problems of correct
com b i nati o n , w h ich is not a lwa ys an easy ma tte r.
As l o o k i n g up faci l itates i n h a latio n and i n h ibits
exhalation, and loo k i n g dow n has t he reverse effect,
looki ng up mllst n o t be combined w i t h e x h a l a tion
n or l ooki ng dow n with breat h i n g i n . We m ust a l so
bear i n mind t h a t l o o k i n g up facili ta tes retroflex i o n
a n d looking d o w n fac i l i tates a nteflexion (stooping) ,
w h i c h m a y o r m a y n o t b e useful i n a gi ven case . T h u s
i n mobilizing s ide-bending i n a n even seg m ent i t will
be use ful to p roceed in the mann e r described in t h e
precedi n g pa r agr a ph. If, how ever, we wish to mobil­
ize an odd segme nt, it w o u ld be wrong to tell the
patient to look u p and breathe o u t during the iso­
metric p h a se, beca use l ooking up i n h ibits exh alation.
It could be e q u a l ly wrong to tell t h e p a t i e n t to look
dow n, for t h at wo u l d in h ibit the straighte n i ng-up
reactio n needed dur i ng the isomet ric .p h ase, w h i l e
t h e si tuatio n wo uld b e e v e n worse i f the patient
loo ked u p duri n g re l axa tion. The re fo re we do not
com b i n e resp iration with eye movements i n mobil­
izatio n of side-b endi ng i n a n odd segm ent. In the
cervicothoracic junction it is essen t i a l for the neck
to be held in ret roflexion duri n g the mob ilization of
side-bending. I t is therefore very convenient to
comb i n e l oo k i ng u p with inhal a t i o n , b u t not look ing
down w ith exh a l a tion because the p a t i e n t wil l bend
h er n eck forward if she looks down .
It is very impor ta n t that the patient brea thes
s l owly so that b o t h the isometric a n d the re l axa tion
phase are lo n g e n o ugh. It is t h e refore useful first to
te l l the patie n t , for example, to l ook to t he right and
Copyrighted Material
,
Thallpeuric lechl1irlllCS
only a moment later to tell her to breathe in
slowlv: similarly, to tell her to look first to the
left
only then
finds
difficult
hreathe out
If a
1f:nt
161
Records
MGlhods of docllf1lt:ntatiol1
legion:
told to hold her breath for a few seconds at the end
marie, typed,
every
colollled, etc.,
practitioner will adopt the one he or she tinds most
of inhalation.
suitable. The essential is that in every case the
she should be
However, a patient with such bad
coordination that slow hreathing (no more than
attained .. must be
cannot
correctly, because
to
4 s)
technique used and its precise location, side and
he
faulty respiration
direction are recorded. Without this docur1ltlntation
it
impossible
evaluate results, to
from
compatible with normal functioning of the motor
faIlure or to deal with pOSSible complIcations as
system. If our combinations are well thought out,
described in the literature.
they not only improve the technique by what we may
call automation,
iveness
also Increase its
After-treatment
the'summa[lon of stimuli; frequentl)
or three repetitions are sufficient to restore normal
It is essential to advise the patient after the first
mobility.
treatment, so that he knows what he may do and
what he should avoid. It is particularly important to
tell
whether
shoud re"t cornpletely.
he should move about.
This technique consists of a fast but not torcetul
Oil the
Ie ought
know
that there may be a painful reaction during the next
movement of small amplitude, starting from end­
I or 2 days. If possible give him some some simple
position (i.e. after taking up the slack). A barrier
specific exercises. If possible, the patient should have
give way.
seems
as a rule
a comfortable
hear a
Immedll!llll.y afterwlHds we senStl
hypotonli1 and
observe increased mobility.
The thrust must be applied only after the slack
has been taken up completely, and this is possible
only
patient
prlln
after treatment. If there
serious
analgesic should be prescribed and
fnrther
appointment arranged.
After these general remarks, I will now deal with
the individual joints.
completely relaxed. There are
three technical pre conditions:
must
(I)
Extremity joints
to sense the momt:nl of complek relaxation: (2) lhe
patient having relaxed properly, the end-position is
reached (the barrier is engaged) with a minimum of
In the manipulation of extremity joints we use almost
force;
excl
(3) the thrust
start from
end-position,
tensioll hefore delivt;nng
i.e. we must never
the thru,,[, as whell wt: lift tbe arm before delivering
a blow - the typical beginner's error, because it
aimed
As examination
loint play
play.
restoring
lechnically identical
with tile mobilizallon of these joints, I desC(lbe both
here.
corresponds to a type of movement we are used to.
Here, however, it is
enables
patient
this
thwart
II
crucial mistake, because it
contract
IHuscles
Interphalangeal joints
For mobilization (rind exarnIlHIIH)n), dorsop;limar
manoeuvre, which is
only if the patient's musculature is taken by surprise
and laterolateral shifts and distraction can be used.
(see Figures 2.7, 2.8 - pp.
The therapist fixes the proximal phalanx between
14, 15).
With Ihese conditions fulfilled, thrusting
lation
never forceful; as can
the thrust corresponds
4.3
the thumb and forefinger of
,ecn from
II
weight
the
not
or his
of hiS
hand, either
body, whilc with the
hand
mobilizes
I
distal
more than 1000 g. Although the high-velocity thrust
phalanx in the required direction. It is advisable to
is typical of thrusting techniques, there are situations
keep one's fingers at right angles to the shifting move­
in which
relatively slow incre8se in pressure
velocity thrust')
release
even 1
suffice
ment, and at the same time to apply clistraction,
which makes the shifting movement easier
obtain
more
'click'; indecd, we may
the click at times during mobilization and even just
by engaging the barrier and waiting for complete
relax8tion.
Testing
Metacarpophalangeal joints
These joints me almost
and thc'refore
roLHion can be used as
dorsopalmar and
laterolateral shifts and (of course) distraction. Wbile
Immediately after treatment, whether this consists
with one hand the therapist fixes the patient's palm
of mohilizi1tion or thfllsting techniques, the effect
a[!ainq his own hody or the lahle, he may carry out
must
any
checked
k.sting (see
5).
these shi
Copyrighted Material
with the
By far
most
Maniplliative Therapy in Rehabililalion of Ihe LocomOlOr Syslem
162
e ffective m a noe uv re , however, is t ract i on , w h i c h ca n
a ls o b e u s e d a s a t h ru s t ( p u l l). It is a s i m p le method
to teach patie n ts for se l f- tre a t m e n t
.
The carpometacarpal joint of the thumb
This is the on ly ca r p om e ta c a r p a l j o i n t which is
highly mob i l e, a n d of all t h e fi nger j o i n ts it i s
p r o ba b ly t h e mos t s usce ptib l e to sy m p tom s . Treat­
m e n t is therefore i m por ta n t The t herapis t must first
fix the trapeziu m b e twe e n t h e th u m b a n d fo refi nge r
o f o n e h a n d . To find the t ra pe ziu m he should first
p a l p a t e the styloid process of the rad ius; distal to
t his there is a groove which corresponds to t h e
sc aphoi d and then t he w r i s t broadens again: t h i s i s
t h e site o f t h e tra p e zi u m . W ith the t h umb a n d
forefi nge r o f t h e o ther h a n d , the the r a pi s t grasps the
first m et acarp a l bone as close to the j oin t as possible,
so as to exa m i n e join t p l a y between th e two. For
m o b ilization it is better to gra s p the e n d p h a l a n x of
the t h u m b w i th t h e l i tt l e fi nger of the hand that
moves the firs t m etaca rpa l , so as to p u l l it and thus
distract the joint. This can be don e w i th the p a tie n t s
hand in p r onatio n or su p in a t ion (the t h e r a pist
c han gin g hands ac cor di n g l y ) . This traction m a kes
the s h ift i n g moveme n ts of joint p l ay much more
effec t i v e
If tr act i o n i s sufficien tly stro n g the t her a p is t can
pr od u ce a gap p i ng effect (wit h ou t fixation of the
t ra p e zium) by a s l igh t ( low ve l oc i ty ' ) thru st i n a
palmar direction, with the pat ient's ha nd in supina­
tion, and in a dors a l direction with the hand in
pron a tio n If the t he r api st is us i ng tra ct io n on l y
( w i th or wit h o u t a t hr ust) a n y fi x a t i on of the w r ist
w i l l suffi ce : t h is tech n i q u e is t h e n very suitable for
s e l f-t reat men t . Mobilization ca n also be carried o u t
b y PIR, w h i c h is both e ffe c t i ve and ext rem e l y ge n tl e :
w h i l e t h e t h era p i s t a p p l i e s v e ry sl i ght traction, t h e
p a t i e n t is tol d to resi s t wi t h t h e least possible force
for abo u t 10 s, after w h ich he is told to ' l e t go'.
W i thout incre a s ing the force of h i s tra ctio n t he
t he ra p i st wa tches the p a t i e nt relaxing, a n d repeats
t h e p roce d u r e three to five times ( Figure 6.2) .
.
,
'
.
-
.
,
Figure 6.2 Tre�tment of the first carpometacarpal joint:
(a) in supination p,llmar shift of the first metacarpal:
(b) in pronation dorsal shifl: both under considerable
traction
The wri st j o i nts
I f pa l m ar fl ex ion is res t r ict ed we m ust restore j oin t
play by mov i n g t h e c arp a l bones in the radiocarpa l
j o i n t in a d orsa l d i rec t i on. The the ra pis t grasps the
s u p i nated hand of the pa tie n t close to the r a d i o
car pa l j oi n t fixes the d istal end of the forea rm a ga i nst
his own knee or the ta b l e , a n d prod uces a dorsa l
shift of t he w r i s t (Figu re 6.3). Th is tec h n ique is w e l l
suited for se l f- t reatme n t . I f ulnar flexion is restricted
th e s a me tech n iq u e can be used, but pressure should
be a pp l i e d m ai n l y a t t h e u l n a r e n d of the rad iocarp a l
j oi n t i.e. against the pis i for m bone.
If d o rsal flexion is restricted, j o i n t pl a y m ust be
restored by m ov i ng the d istal r ow of the carpal
,
­
,
,
Figllre 6.3 Dorsal shift of the carpal bones against the
foreann: mobilization of the rildiocarpal joint
Copyrighted Material
Thernp('/(Iic lecillliqlles
163
Figure 6.4 Palmar shift of the distal
of carpat bones against the
row; mobilization of the
miel-carpal joint
row
proximal
n st the p roxi mal row, in a palm a r
( Fig ur e 6.4). The t herap ist grasps the
patient's hand in pro na tion, round the p roxi m a l end
of the metacarpal bones, fixes t he d ista l e nd of the
forearm ag a i ns t his own knee or the t ab l e , a n d
p rod uce s a pal m a r shif t of the d ist a l row of t h e
carpal bones again st t h e proximal. Again this is an
ideal technique fo r self-treatment. If r ad i a l flexio n
is restricted ow i ng to b l oc kage between the scap h o i d
and t he trapclium. t h e silme tech nique can be used
but the pressure is a p p lied m ai n l y a t the rad i a l end
of the mid-carpa l joi n t .
There is a s i m p l e way t o l ocate the rad i o ca r p a I
and the carpometacarpal .io ints exa c t l y : if we e x t e n d
the wrist against t he forearm, t h e skin fold on the
do rsal aspect is at the l e ve l of the c ar po me t a ca r p al
.io i nt, and if we t1cx the w rist the skin fold on the
palmar aspect is at t he le vel of the r a d i o c arpal jo i n t.
The most specific and also t h e most important
te ch n i que is that of shifting one carpal bone against
its ne igh bo ur , in a dorsal or pa l m a r d ir ec t i on . This
is part icu larly import a n t in the carpal-tunnel s y n ­
drome (see p. 267).
The exami n a tion te chni q u e is simple: one carpa l
bone is grasped between the thumb and fore fi n ge r
of each hand, and t he therapist m ov e s the two
adjacent b on es against each other in the d orsa l a nd
palm a r direction, respectively. For d i a g n os is it is
crucial to use the m i n i mum of force, beca use u n d e r
normal co n d i t i o n s fricti on here i s s o negligible that
the slig h t est possible p res s u re will produce some
movem ent. The ques t ion of fixa t ion is there fore less
imp o rta nt he re , al tho u g h the therapist must s u pp ort
the pillient's hand to ensure t h at it is com p l ete ly
relaxed. If no movemen t c a n be fe l t w h e n t h i s mini­
mum rorce is applied, the re is restricti on: the LIse of
greater force ren d e rs diagnos is i m pos s ib le .
This techniq u e can a l so be used for mo b i li za tio n ,
but the f ol l o wing m e t h o d i s pr e fe ra ble , a s it p r o v i d e s
be t ter fixatio n . The therapist p lac e s both thumbs on
the dorsal aspect of o n e carpal bone and bo t h fore­
fingers (one above the ot h e r) on t h e p a l m a r aspect
bon es
a gai
dire c tio n
the adjacent carpa l bone: he t h e n exe rts s light
w i th pi n ce rs shifting one bone against
the other. He t hen reverses the d ire c t i o n of the shift
by pla c in g both t h u m bs on t h e p a l m a r aspect and
both fo re fin ger s on t he dorsa l aspect of t h e same
two bones (Figure 6.5). The m o v em e n ts a re rhythmic
and r ep e t i t i v e . Obv i o us l y , t his moveme n t ca n a lso
be effe cted with a s ingle h a n d, t h e t h u mb on one
and the forefinger on the next ca rp al bone: in this
way t h e patien t ca n be taught to p rac tise s elf­
tre a t m e n t (see p. 200).
To locate single carpal bo n e s exactly we m ust start
with o n e a n d f e e l o u r way to t h e n e x t . I have a l re a dy
s h own how to l ocate t he sc a p h o i d and the t ra pe ziu m
(se e p. 162). The capi t a t e forms the most p ro m i n en t
po i n t of the w r i s t at pa l m a r flexion. The triquetrum
lies below the p isifo rm . (The latt e r c an be m o b ili ze d
against the triquetrum to both sides as w e l l as
p rox imod i s tal l y . )
This te ch niq u e c a n be used both for d iagn o s i s and
for t re a tm e nt , not o nly for t h e c a rpa l bones them­
selves but a l so for the carpometacarpal jo ints and
the in te rmetacarpa l joi n ts . Tec h n ic a l l y it i s, of course,
m ost importilnt to place the finge rs on ad.iace nt
bones; if the thera pist p l aces his fi nge rs too close
togeth e r (on the same bone ) by mistake, he will
obtain no m o v e m e n t , w h i l e if they are too far a pa r t
(so tha t t h ere is a bone i n b e tw e e n ) there will be
t oo m u c h mobil ity. The range of shift between two
ad j ace n t ca r p a l bones is only slig h t .
In a d d i tio n to t hes e s h i fti ng tec h n iqu e s t h e re i s a
d is t rac t i on t ech n i q u e with high - ve l o c i t y t h r u s t w h i c h
is very effective a nd en t i r e l y innoc u o u s if c or r ec t l y
applie d (Figure 6.6). The t he r a p is t stands in front of
the pa t ien t , who is s eat ed with h e r arm stretched
for w ard a n d downward . The therapist p la ces both
thumbs on the p a t i e n t ' s distal bone (where r e s t r ic­
t i o n has bee n found), ilnd both hands round the
wrist, w i t h tbe hand i n pronati o n . The slack i s t a k e n
up by a very gentle p u l l i n the directi on o f the long
axis of the patient's arm, a nd t h e w ris t is t h e n s ligh t l y
dors i flexed over the t h e rap i s t ' s thumbs. The th rus t
of
p re s s ure , as
Copyrighted Material
164
Manipulative Therapy in Rehabilitation of
the Locomotor System
Figure 6.6 Traction high-velocity thrust o n the os
(a) finding the os capitum and making contact:
(b) ta kin g up slack and delivering the thrust
capitum:
The elbow
Here m o b i liza t i o n is used mainly for the trea tment
of p a inful epico n dyles (in comb i nation w i t h m uscle
rel axatio n ) . The most i m portant techniques a re
distraction a nd l a tera l gapp i n g (springi ng) which is
a l so sign ifica n t for diagn osis .
Fi g u re 6.5 Shifting one c a rpa l bone against the
examination; (b) mobilization by shearing
next:
(a)
is del ivered by a s u dden pull exactly alo ng t h e axis
of the pa tient's arm, producing distractio n of the
j o i n t. Th ere a re two mistakes to be avo i d ed: (1)
traction m us t n o t be rele ased before the t h r u s t is
delivered; and (2) no further d o rsiflexion at the wrist
m ust occ u r d u r ing the t hrust (pull ) .
Distraction
The patie n t l ies su pine. the a rm to be t rea ted flexe d
a t the e l bow (Figure 6.7) . The therapist fixes the
patient's forea rm aga i nst h i s sho ulder a n d p l aces the
ha n d tha t w i l l perform the tractio n on the forearm.
c l ose to the elbow. W ith his other hand o n the a rm,
close above the elbow, he fixes the pati e n t's arm to
t he t a b l e from above. Tra c t i o n is carried out a long
the long axis of the arm by t he ha nd o n the forearm;
The dista l rad i o u l n a r j o i nt
This is the last j o i n t that c a n be t rea ted a t the wrist,
d e p e n d i n g fo r i ts function o n the u pper radiou lnar
j o i n t . For both exa m i n ation and trea tme n t the
tec h n i q ue is broadly tha t alre a d y descri bed for single
ca rpal bo nes: the therapist grasps the end of t h e
rad i us a n d the ul n a each be twee n the t h u m b a n d
forefinger of o ne h and, p rod u c i n g a d o rs a l or palmar
s h i ft . For treatme n t he p l a ces both t h u m bs o n the
dors a l aspect of the rad i us a n d both forefin gers o n
t h e palmar aspect of the u l na, to p rod u ce rel a tive
s h i ft . After a few repeated rhy thmic m o biJiza tions
he reverses the p i n cer m ovement by p l ac i n g both
thumbs on t h e dorsal aspec t of the u l n a a n d both
forefingers on the palmar aspect of the radius .
Figure 6.7 Traction of the elbow joint
Copyrighted Material
Therapeutic techniques
165
it is g re a t l y e n h a nced if the t he rapist presses the
thu m b of the other hand (close above the e l bow)
aga i n s t the hand exerting the p u ll , and a t the s a m e
time increases t h e flexio n o f the e l b o w by pressing
his shoulder against the patien t's fo rearm; this
produces leverage at the elbow , t h e the rapist's
th u m b serv i n g as the fu lcru m .
Latera l gapping (springing) (Figure 6.8)
The p a tien t m a y be seated or s u p ine, w i t h t he
affected a rm stre tched out b u t n o t ove rs t retched
(the e l bow must not be locked). The t h erapist stand s
facing t he elbow (from the radial or u l nar side) a nd
wi t h one hand a bove t h e wrist fixes the forearm
aga inst his body; w i t h the oth e r ha n d he takes the
e l bow from the s i d e , the t h u m b above a n d fingers
below. Pressing t his h a n d ge n tly a g a i n s t the elbow
from the side, he takes up t h e s lack, and w i t h a
ge n tle extra push springs the joi n t, producing gapping
of the point on the o p posite side. If the rad i a l
e p i c on d yle is pa i n fu l, as a rule t h e re i s no sprin g i n g
( o r it is i m paired) i n the u l norad i a l d irection, wh i l e
if t h e u l n a r epic o n d y l e i s pai nfu l w e some t i m e s find
re stJicted radio u l n a r spri nging.
For the purpose o f mobi l ization, s p r i n g i n g is
re p e a te d rhythmica l l y. The same tec h n i q u e is a l so
used to deliver a h i g h -velocity t hrust after t a k i n g
up th e slack ( i n a radial or u l n a r d i rectio n ) . Fast
s h aki n g is most e ffective. For sel f- trea t m e n t see
Figure 6.70, p. 200.
The re a re two import a n t tec h n ical deta i ls: the
thera pist stands a t the level o f t h e e l bow joint so
that the h a n d s pri ngi ng the joint or delivering the
t h rust is supported b y h is trunk, i. e . the move m e n t
origina tes in the t he rap ist's p e l v i s or e v e n in h i s l egs;
and the hand grasping the patien t's forearm is t h e re
fo r fix ation o n l y, a n d must n ot be ( m is)used for
leverage.
If a h igh-vel ocity t h rust i n a rad i a l o r u l n a r
direction i s not successfu l, a th rust ca n be applied
Figure 6.9 Shaking mobilization of the elbow joint into
extension
aga i ns t t h e head of t h e radius w i t h the thu mb, fro m
t h e d o r s a l aspect, t h e a r m b e i n g stre tched . Th i s tech­
nique may be too v i o l e n t , a n d we have i n t rod uced
i nstead a n e q u a lly effective ge n t l e rocking techniq u e .
The patient is s e a t e d o r s u pi n e; t h e t h e r a p i s t grasps
the o u tstre tched a rm wi th both h a n d s , j u s t above
the e l bow, ho lding it in maximu m supi n ation a nd
s h akin g it gently a n d rhythm ica ll y w h i l e t h e p a t i e n t
i s f u l ly relaxed (Figu re 6.9).
Sachse (personal com munica t i o n ) a c h i eves a s i m i ­
l a r effect by rhyt h m i c s t a bilization: w i t h t h e pa tie n t
seated a n d t h e elbow flexed, t h e thera pist h o l d s the
p a t i e n t's u pp e r a r m w ith both hands, fixi n g t h e h a n d
i n h i s a rm p i t, a n d tells h e r to extend a n d flex t h e
a r m rhyth m ic a l l y , wh ile h e resists the p a t i e n t ' s
move m e n t s .
The sho ulder joint
Figure 6.8 Springing the elbow in a radial direction
Where w e find a typic a l caps u l a r pa ttern ( see p . 115),
mobil iza t i o n techn i q ues a re pract ica l l y use less and
even the usua l t raction tech niques give little or n o
res u l t. Surprisingly , what w e might c a l l isometric
tract ion brings re lief of p a i n and may even improve
m o b i lity. It is best for the p a t i e n t to sta nd or t o s i t
(Figure 6.10a); the t herapist p l aces h i s right s h o u lder
u nder the right axilla (or the le ft u n d e r the left),
pressing aga i n s t t he pa t i e n t's thorax. He grasps t h e
affected a r m w i t h one h a n d a b ove t h e wrist a n d the
other above the e l bow, a n d te lls the patient to re sist
Copyrighted Material
Monipulolive
I (i(\
traction very
Therapy in
Rehabilirmion of Ihe
s l i g h t l y a n d t h e n to
b re a t h e i n
L o col1loror Sysrem
s l ow ly
a n d t h e n to h o l d h e r b re a t h . Afte r t h i s t h e p a t i e n t
told
is
l e t go a n d to bre a t h e o u t s l o w l y
to
If
.
re l a x a t i o n i s s a ti s fa c t o r y t h e t h e r a p i s t fe e l s t h e
'
patie n t s arm l e n g t h e n i ng
but he must not pu l l .
-
This
p r o c e d u re
a cco rd i n g
re p e a t e d
is
to the degree of
i m po r t a n t t h a t t h e
is
a bo u t
three
times,
re l ax a t i o n a c h ieved . It
t hera pist
should
prop
his
s h o u l d e r a ga i n s t t h e p a t i e n t ' s t h o r a x , n o t t h e a r m ,
w h i c h is se m i - a bd uc t e d . Wi t h t h e a x i l l a o v e r t h e t o p
o f a c u s h i o n e d c h a i r - b a c k t h i s tec h n i q u e is very
.
s u i t a b l e fo r se l f- t re a t m e n t . I t i s u s e f u l if t h e p a t i e n t
i s t a l l e r t h a n t h e t he r a p i s t . A n o t h e r tech n i q u e , w i t h
t h e pa ti e n t s u p i n e
,
i s a s fo l l o w s : s h e a b d u c t s h e r a rm
as fa r as s h e ca n : t h e t h e ra p i s t p l a ces a b u t t oc k
between the pa tient's arm a n d c hest, exerting a
s l i g h t p u ll
on t h e a rm
to t a k e u p t h e s l ac k . T b e
p a t i e n t i s t o l d t o r e s i s t , b re a t h e i n , h o l d h e r b re a t h ,
a n d t h e n t o re l a x a n d b r e a t h e o u t ( F ig u r e 6 . l Ob )
If a b d u c t i o n o n l y
is r e s t r i c t e d , a n d
we
.
( a)
fi n d a t
e x a m i n a t i o n th a t j o i n t p l a y i s i m p a i re d w h e n w e
s p r i n g t h e h e a d o f t h e h u m e r u s a ga i n s t t h e s c a p u l a
1 1 5 ) . w e r e s to re j o i n t
a s fo l l ow s : t h e p a t i e n t s i t s w i th h e r a r m
from a b o v e ( s e e F i g u r e 4 . 4 0 , p .
pl a y
a b d uc te d : t h e t h e r a p i s t p l a c e s h i s s h o u ld e r u n d e r t h e
p a t i e n t ' s e l b o w , so t h a t
t h e a r m i s h o r i zo n t a l
.
He
t h e n p l a c e s o n e h a n d ( w i t h t h e ra d i a l a s p e c t ) o n t h e
h e a d of t h e h u m e r u s fro m o n e sici e , w h i l e t h e o t h e r
h a n d t o u c h e s t h e fos s a g l e n o id a l i s of t h e s h o u l d e r­
b l a d e from t h e o t h e r s i d e . W i t h s l i g h t p r e s s u r e o f
on e h a n d a g a i n s t the o t h e r h e takes u p t h e s l a c k a n d
t h e n s p r i n g s t h e j o i n t p ro d u c i n g a t r a n s l a to r y m o v e ­
( b)
H e t h e n c h a nges h a n d s a n d
s p r i ngs t h e j o i n t i n t h e o p p os i te d i re c t i o n . By r a i s i n g
F igure 6.1 0
.
m e n t ( Fi g u re
6.1 1 ).
o n e e l b o w a n d l o w e r i n g t h e o t h e r , t h e t h e ra p i s t m a y
s p r i n g t h e j o i n t i n a n o bl i q u e d i recti o n . t h u s fi n d i n g
t h e d i re c ti o n o f m a x i m u m r e s t ricti o n a n ci t h e n
t re a t i n g i t .
Th i s t e c h n i q u e i s b o t h e a s y a n d e ffec t i v e . Ca re
m u s t b e t a k e n , h o w e v e r , to have t h e t h e ra p i s t ' s h a nd
.
located exac t l y a t
ther�pist. i n
( 0 ) Tra c t i o n
the
of t h e s h o u l d e r o v e r t h a t of t h e
t h e l o n g a x i s o r t h e a rIll : t h c
( h ) T ra c t i o n o f t h e s h o u l d e r i n
a x is o f t h e ar m . o v e r t h e
d i re c t i o n o r
pat i e n t m a y s i t or s t a n d .
t h e d i re c t i o n o f t h e l o n g
t herapisr's h i p . the patient
supine
t h e h e a d o f t h e h u me r u s , a n d h is
o t h e r h a n d a t t h e fo ssa g l e n o i d a l i s .
The acro m ioclavicu l a r j o i nt
To
free
t h i s j o i n t , t h e most
i mporta n t t e c h n i q u e
c o n s i s t s of s p r i n g i n g i t i n a ve n t rodorsa l a n d a c r a n io
­
c a u d a l d i rec t i o n ( Fi g u r e 6 . 1 2) . T h e p a t i e n t is s u p i n e ,
t h e t h e ra p i s t s t a n d i n g b y t h e s i d e o f t h e t a b l e . To
c a r ry o u t ve n t roclorsa l s p r i n g i n g he p l a ce s h i s ( r i g h t )
t h e n a r e m i n ence aga i ns t t h e ( r i g h t ) c l a v i c l e , fi x i n g
t h e p a t i e n t's shou l d e r with his o t h e r ha n d He now
.
a p p l i e s ge n tl e pre s s u re a g a i n s t t h e c l a v i c l e from
a bove , a nd
t h e n re l e a ses it. If j oin t p l a y
is normal ,
he w i l l fe e l t h e c l a vi c l e s p ri n g b a c k a n d wiJl bot h
fe e l a n d s e e m o v e m e n t b e t w e e n t h e e n d of the
cl a v i c l e a n d t h e s h o u l d e r . Th is s p r i n gi n g i s a bs e n t i n
ac rom i oc l a v ic u l a r
blockage.
To
re s t o re
it.
the
t h e ra p i s t re p e a ts t h i s g e n t l e p u s h w i t h h i s t h e n a r
F igure 6 . 1 1 Tra n s l a t o r y m o h i l i za t i o n o f
b o t h h a nds i n o p po s i t e d i re c t i o n s .
using
Copyrighted Material
the shoulder
joint
t h e p a t i e n t seated
Th erapeU lie lechn iques
1 67
( a)
( c)
( b)
Figure 6. 1 2
Mooilization
v e n t r o d o rs a l
ami (h)
of t h e
a c r o m i oc l a v ic u l a r j o i n t by s p r i n g i n g
the
e m i n e nc e , w i t h o u t e v e r i n creasi ng fo rce, a n d t h e n
re l eases i t . A fter a bo u t five repe t i t i o n s a t t he rate o f
two p e r seco n d , h e u s ua l l y se nses some spri ngi ng:
after 1 5-20 repe titions the ra nge n o longer i ncreases.
For cran ioca u d a l s p r i n g i n g , t h e t h e ra p ist a t the
side o f t h e t a b l e fixes the ben t e l bow from below
w i t h h i s cupped hand, placing t h e t henar e m i n ence
of the other h a n d on t h e clavicle from a bove a n d
giv i n g a s l ig h t s p r i n g i n g p u s h fo l lowed by release, a t
t h e r a t e o f t w o p e r seco n d . I f h e n e i t h e r fee l s n o r
sees springi n g between t h e c l a v i c l e a n d t h e s h o u l de r ,
he rcpeats the m a n o e u v r e , as t o r dorsoven tral
springi ng.
I t a p pears that i t i s t he s p r i n g i n g back that frees
the j o i n t, a n d t here fore t he worst mistake i s to
i n c re ase p ress u re if no s p r i n g i n g has bee n felt ( a s
t h o u g h t r y i n g t o re l ease a s p r i n g by press u re o n i t ) .
Trea t m e n t shou l d a l ways be a p p l i e d i n both
d i rections, as move m e n t m a y be b l o c k e d s e p a ra t e l y
i n each .
A n o t h e r use fu l t echn i q u e is t h a t o f tracti o n
the acromion i n
acrom iocln v i c u l a r j o i n t
c l a v i c l e aga i n s t
a c r a n i o c a u d a l d i re c t i o n . (e) T ra c t i o n m o b i l iza t i o n of t h e
(a) a
m o b i l iza tion ( F i g u re 6 . J 2c) . T h e p a t i e n t i s s e a t e d o n
a l o w stoo l , w i t h the t h e rapist o n t h e s i d e o f t h e
l es i o n . be h i n d t h e a bd ucted a r m . He grasps t h e a r m
a bove t h e e lbow a n d w i t h t h e t h e n a r e m i n e n ce o f
t h e o t h e r ( r i g h t) h a n d o n t h e ( le ft) c l a v i c l e h e fixes
t h e l a te r a l e n d o f t h e cl avicle b y s l ight pressure from
above . He a p p l i e s tracti o n th ro u gh t h e a r m , w h i c h
i s s l i g h t l y raise d , a b d ucted a n d d r a w n forward,
making a ge n t l e movement of rota tio n ; h e m a y se n se
a d i s t i n c t crack i n g sou n d under the h a n d fi x i ng t h e
clav icle .
The stern oclavicu l a r joint
S i m p le b l ockage o f th is joint without a r t h rosis is
re l a t i v e l y rare. The most e f fect i ve tech n iq ue i s
ga p p i n g t h e j o i n t: w i t h h a nds cross e d , t h e t h e r a p i s t
p laces one pisifo r m aga i nst the m e d i a l e n d of the
clavicle from b e l ow, and t h e o t h e r p isi form against
the m a n u b ri u m o f t h e s te r n u m from above. B y s l ig h t
p ress u re p a r t i n g t h e h a n d s , t h e s l a c k is t a k e n u p : t h e
Copyrighted Material
1 68
Manipulative Therapy
in Rehabilitation of the Locom% r
System
from the trunk, so that both his ha nds p e r fo rm as a
s i ngle u n i t .
The toes
Figure 6.13 S pr i n g i ng t h e s t e r n o c l a v i c u l a r j o i n t w i t h
c ro s s e d h a n d s
t herapist t h e n springs t h e j o i n t i n to d istraction
(Figure 6 . 1 3 ) .
T h e shou lder-b l a d e
T h e s h o u l der-blade l ies fl a t o n t h e t h o racic wall a n d
a l though t h e re is no a rtic u l a t i o n , i t i s free l y m o b i l e
beca use of the synov i a l b u rs a e . A l t h ough t h e r e
c a n n o t be blockage o f the t y p e fo u n d i n a rticu­
l a t i o n s , t here may be some res trictio n (bin d i ng);
mobi liza tion c a n t h e re fo r e be use fu l .
The p atie n t l i e s prone w i t h h e r head turned
towards t h e t he rapist a t the side o f t h e table ( Figure
6. 1 4) . The t h e r a p i s t grasps t h e h e a d of the h u m e ru s
i n both h a n d s - one a bove a n d t h e other b e l o w rou n d the patient'S s h o u l d e r , a n d carries o u t a
c i r cli n g mov e m e n t . W i t h the upper h a n d he m a y
exe rt s o m e press u re o n the moving sca pula from
a bove, or o n the con trary he may l i ft the sca p u l a
from t h e t h orax with h i s finge rti ps. [ t i s import a n t
t h a t t h e m o v e m e nt the t h e rapist i m parts to the
sca p u l a over t h e p a ti e n t ' s shoulder should come
Figure 6.14 M o b i l i za t i o n o f t h e s h o u l d e r- b l a d e a g a i n s t
w a l l ( a lso use ful fo r r i b m o b i l i z a t i o n )
t h e t horacic
What has been sa i d a b o u t the fi nger j o i n ts i s e q u a l ly
valid for the toes. However, the co n d i t i o n that is
spec i fi c for the foot i s pa i n i n the metatarso phal­
a ngea l j o i n ts ; here t h e tech n i q u e that gives most
rel ief is traction i n a s l i g h t ly plantar d i rect i o n . Fo r
this m a noeuvre the t h e rapist grasps t h e first p h a l a n x
o f the toe betwee n h i s t h u m b a n d t h e fl e x e d fi rs t
phalanx of h i s fore fi nger, w h ich is p l a c e d u n d e r t h e
first p h a l a n x of the patient's toe. W i t h the o t h e r
h a n d he fix e s t h e correspo n d i ng metatarsa l . A ft e r
ta k i n g u p t h e s l a c k he i ncreases traction s i m u l ta n ­
e o u s l y w i t h s o m e p l a n t a r flexion, u s i n g t h e first
p h a l a n x o f h i s flexed fore fi nge r a s a fu l c r u m .
A l t h o ugh t h e r e i s n o real t h rust. o r only a v e r y l o w ­
v e l o c i t y thrust, a c l i c k c a n freq u e n t l y be h e a r d . T h i s
i s a s i m p l e tec h n i q u e , b u t ca re m ust b e taken not t o
press the j o i n ts , w h i c h a r e v e r y t e n d e r.
A t e c h n i q u e t h a t pa t i e n ts fi nd agree a b l e consists
of s p re a d i ng t h e metata rsals fa n-wise ( Figure 6 . 1 5 ) .
T o d o t h i s t h e therapist s t a n d s a t t h e foot of the
t a b l e w h i l e t h e p a t i e n t s i t s fac i n g him, on t h e t a b l e ,
with k nees be n t a n d h e e l s res t i ng on t h e t a b le . The
therapist ta kes the m e t a t a rs a l s in both h a n d s , the
t henar above w h i l e the fi n gers form a fulcrum on
the p l a n t a r aspect: he then s p re ads the dors u m o f
the foot.
The tarso metata rsa l j o i nt and the joi nts
between the tarsal b o n es
The term ' Lisfra nc's a n d C h o p a rt' s j o i n t ' is fre q u e n t l y
used for these j o i n ts . As a r u l e i t i s better to d i a gnose
a n d t re a t speci fi ca l l y t h e j o i n t s betwee n s i n g l e t a r s a l
bones a s we ll as the t a rsometa t a r s a l j oi n ts . A very
effective t ech n i q u e for t re a t i n g Lisfra nc's j o i n t (al l
t h e t a rsometa ta rs a l j o i n ts) and Chopart's j o i n t ( t he
articu lation between both the cuboid a n d nav icular
bone wi th the talus and calcaneus) toge t h e r is a s
Figure 6.15 S p r e a d i n g t h e m e t a t a rs a l s fa n -wise .
Copyrighted Material
Therapeutic techniques
169
fol lows ( F i g u r e 6 . 1 6 ) . T h e p a tie n t l i e s s u p i n e w i t h
t h e l e g b e n t a t t h e k n e e , t h e h e e l o n t h e t a b l e . The
t h e r a p i s t s t a n d s a t the s i d e of t h e t a b l e and grasps
the p a t i e n t ' s l e g abo ve the a n kJ e w i t h one h a n d ,
from a b o v e . H e t h e n p l aces t h e r a d i a l aspect o f
t h e o t h e r h a n d p a r a l J e l e i t h e r t o Lis fra n c ' s o r t o
Chopart's j o i n t on
t h e p l a n t a r aspect
from t h e
m e d i a l s i d e o f t h e foo t , a n d ta k e s u p t h e s l a c k w i t h
s l i g h t press u r e ; h e t h e n s p r i ngs t h e j o i n t i n a c r a n i a l
d i re c t i o n ( Fi g u re 6 . 1 6 ) . H e s h o u l d k n o w t h a t t h e
prox i m a l
end
of
the
fi ft h
m e t a t a rs a l
( w h i ch
is
p ro m i n e n t) l i e s m o r e prox i m a l t h a n t h e prox i m a l
e n d o f t h e fi r s t m e t a t a rs a l , so t h a t h i s i n dex fi n g e r
Figure 6.17 Trac t i o n m a n i p u l a t i o n ( mo b i l i za t i o n ) o f t h e
by t h rust or b y r h y t h m i c a l s h a k i ng
t a rsa l b o n e s
fo l l ows a n o b l i q u e c o u rse .
The
fo l l o w i n g tec h n i q u e s c o r r e s p o n d
to
t h ose
described for s i n g l e c a r p a l bones: for d i a g n o s i s o f
b e t w e e n t h e c u n e i fo r m b o n e s a n d t h e n a v i c u l a r , a n d
j o i n t p l a y t h e t h e ra p ist fi x e s t h e p r ox i m a l b o n e ( m ost
between
fre q u e n t l y a tarsal b o n e ) b e t w e e n t h u mb a n d fo re­
c a l c a n e u s . T h e m o s t fre q u e n t s i t e o f re s t r i c t i o n i s ,
the
navicular
a nd
the
cuboid
and
the
fi n ger. w h i l e t h e t h u m b and fo r e fi n g e r o f h is o t h e r
h o w e v e r , t h e seco n d , t h i rd a nd fo u r t h ta rso m e t a ­
h a n d g r a s p t h e b a s e of a m e ta t a r s a l b o n e , t o e x a m i n e
t a rs a l j o i n ts .
d o rso pl a n t a r s h i ft . To c a rr y o u t t h i s m a n oe u v r e
A ft e r t h i s s h i ft i n g tech n i q u e a s i m i l a r l y ' u n i v e rs a l '
e x a c t l y i t i s b e s t fi rs t to t a k e u p t h e s l a c k i n a d o r s a l
t ra c t i o n tech n iq u e s h o u l d b e e m p l oyed ( Fi g u re 6 . 1 7 ) .
d i rect i o n , s p r i n g i n g t h e j o i n t i n t h e s a m e d i re c ti o n ,
The patie nt lies prone, h e r legs slightly bent at the
a n d t h e n to t a k e u p t h e s l a c k in a p l a n t a r d i re c t i o n
k n e e . T h e the r a p i s t p u ts t h e fi ngers of b o t h h a n d s
a n d a g a i n s p r i n g the j o i n t i n e n d - p os i t i o n .
r o u n d t h e p a t i e n t ' s i n step w i t h b o t h t h u m bs o n t h e
F o r m o b i l i za t i o n , h o w e v e r , i t i s be tte r fi rs t to p l ace
p l a n t a r a s p e c t o f t h e d i s t a l o f t w o adj a ce n t b o n e s
b o t h t h u m bs o n t he p l a n t a r aspect and both fo re­
( e . g . o n t h e b a s e of t h e t h i rd m e t a t a rs a l ) . H e t a k e s
fi n g e rs o n the d o rs a l aspect of two a d j a c e n t b o n e s ,
u p t h e s l ac k b y s li g h t p l a n t a r flex i o n a n d t r a c t i o n
to t a k e u p t h e s l a c k by s l i g h t p re ss u r e , a n d t h e n by
a l o n g the l o n g a x i s of t h e foo t , a n d ca n t h e n d e l iv e r
t h r u s t b y a s u d d e n p u l l . Rece n t l y I h a v e d ev e l o p e d
s l ig h t l y i n c r e a s i n g and t h e n re l e a s i n g p re s s u r e ( a t
a
t h e b a r r i e r ) r h y t h m ica l l y t o m o b i lize t h e j o i n t i n o n e
a t ec h n i q u e t h a t i s ge n t l e r , m o re e ffec t i v e , a n d agree­
d i re c t i o n . T h e p os i t i o n o f t h e t h u m bs a n d fore fi n gers
able t o the p a t i e n t ; t h i s c o n s i s t s in s i m p l y s h a k i n g
i s t h e n reversed to pe rfo r m m o b i l i z a t i o n in the s a m e
t h e fo o t r h y t h m i c a l l y u p a n d d o w n r a t h e r fa s t ( s e v ­
w a y i n t h e o p p os i te d i re c t i o n ( s e e F i g u r e 6 . 5 , p . 1 64 ) .
T h i s is
an
a l m o s t u n iv e rs a l t e c h n i q u e w h i c h m a y
be u s e d fo r t h e t a rs o m e t a t a rs a l j o i n ts , t h e j oi n ts
e r a l s h a k es per seco n d ) , w h i le m a i n t a i n i n g t r a c t i o n .
T h i s m u s t b e d o n e w i t h a rel a x e d h a n d , s o a s to s e n s e
A
t h e o p ti m u m r h y t h m .
f e w seco n d s o f t h i s s h a k i n g
m o b i l i z a t i o n i s s u fffic i e n t . I t c a n a l s o b e u s e d t o t re a t
t h e cun e i fo r m , t h e c u b o i d a n d t h e n a v i c u l a r .
The s u bta l a r j o i nt
T h i s j o in t is form ed by t h e t a l u s , the calca n e u s a n d
t h e n a v i c u l a r . T o e x a mi n e j o i n t p l a y a n d m o bil i ze
t he j o i n t , t h e t h e r a p i s t gra s p s t h e p a t i e n t ' s i n s t e p
with one h a n d and cups the other round h e r heel
( F i g u r e 6 . 18) ; t h e p a t i e n t i s s u p i n e . W i t h t h i s g r i p
the
t h e ra p i s t c a n p e rform
most
of t h e
possible
m o v e m e n ts b e t we e n t h e c a l c a n e u s and t h e fo r e fo o t :
l a t e r a l fl ex i o n , r e l a t i v e r o t a t i o n , p l a n t a r fl e x i o n a n d
d o r s a l fl e x i o n o f t h e i n s t e p .
A
v e ry
e ffec t i v e
traction
tech n i q u e
has
been
d e v e l oped fo r t h e pos te r i o r p a r t o f t h e s u b t a l a r j o i n t
( Fi g u r e 6 . 1 9 ) . T h e p a t i e n t i s s u p i ne w i t h t h e h e e l
o v e r t h e free e d ge o f t h e ta b l e ; t h e t h e r a p i s t sta n d s
a t t h e f o o t o f t h e t a b le a n d g r a s p s t h e l e g a bove t h e
a n k l e , w i t h o n e h a n d , from t h e s i d e , h is th umb a b o v e
t h e m e d i a l m a l l eo l u s , for fi x a t i o n . The o t h e r h a n d
Figure 6.16 M o b i l i za t i o n of t h e t a rsom e t a ta r s a l a n d
t r a n s verse t a rsal j o i n ts (After Sachse , ( 973)
cups t h e h e e l f r o m t h e m e d i a l a s p e c t a n d p u l ls i t i n
a d i s t a l a n d u p w a rd d i rec t i o n . A ft e r t a k i n g u p t h e
Copyrighted Material
1 70
Mflnip l I /fl l i v e Th erapy
in
R ei1f1 h ililflliun of lire LOCU / 1 / U l O r SyslCl l 1
Figure 6.19 G a p p i n g t h e s u b t � l a r
heel
joi n t b y p u l l i n g o n
the
c o u l d l o c k t h e a n k l e j o i n t . H e n ow t a k e s u p t h e s l a c k
by
a
s l i g h t p u l l a l o ng t h e l o n g a x i s a t t h e l e g , a n d
t h e n m a kes
a
t h r u s t i n t h e s a m e d i re c t i o n .
as a
ru l e
o b ta i n i n g a ' c l i c k ' .
A n a l t e r n <1 t i v e t e c h n i q u e i s to gr a s p t h e fo re fo o t
w i t h o n e h a n d a n d t h e h e e l w i t h t h e o t h e r .. ca r r y i n g
o u t t r a c t i o n : i n t h i s c a se t h e s u b t a l " r j o i n t i s a l so
t re a te d . In b o t h c a s e s t h e m o s t
C O III III on
m i s t a k e is
e x a gg e r a t e d d o rs i fl e x i o n of t h e fo o t . a n d too m u ch
Figure 6 . 1 8 E x a m i n a t i o n o f m o b i l i t y ( m o b i l i z a t i o n )
of t h e calca n e u s a g a i n s t t h e i n s t e p i n a ( 1 1 ) m ed i a l a n d
( h ) l a t c r<l l di rect i o n
fo rce a p p l i e d to t a k i n g u p t he s l a c k .
The t i b i ofi b u l a r j o i nt
Fo r d i a g n o s i s .
s l a c k h e m a y m o b i lize
or
de l i v e r
a
t hr u s t t o ga p t h e
fi b u l a r
head
as
on
fo r m o b i l iza t i o n ,
the tibia
in
il n
d i rec t i o n , a s o n t h e c i rc u m fe re n c e o f
p o s t e r i o r p a r t o f t h e t a l o c a l ca n e a l j o i n t .
we
move the
il n t c ro p o s t c r i o r
il
c i rc l e ( Fig u r e
6 . 2 2 ) . T h e p a t i e n t i s s u p i n e , t h e k n ee b e n t a n d t h e
fo o t o n t h e t a b l e . T h e t h e ra p i s t s i t s s o as t o fi x t h e
The a n k l e j o i nt
H e r e j o i n t p l a y c o n s i s t s of a r e l a t i v e a n te ro p o s t e r i o r
s h i ft o f t h e t a l u s a ga i n s t t h e fo r k fo r m e d b y t h e d i s t a l
e n d o f t h e t i bia a n d fi b u l a . For e x a m i n a t i o n a n d
m o b i l ization t h e p a t i e n t i s s u p i n e , t h e k nee s l i g h t l y
be n t a n d t h e h e e l o n t h e ta b l e ( F i g u re
6.20).
The
t h e ra p i s t s t a n d s a l o n gs i d e l h e l e g a n d gr a s p s t h e h e e l
i n o n e h a n d , s u p p o r t i n g t h e fo o l w i t h h i s fore a r m to
h o l d it a t r i g h t a ng l e s to t h e l e g . He t h e n t a k e s up
t h e s l a e k by s l i g h t p r e s s u r e f r o m a b ove a n d s p r i n gs
i t r h y t h m ica l l y in t h e sa m e d i re c t i o n .
T h e re i s a l s o a v e ry e ffec t i v e trac t i o n t e c h n i q u e
( Figure
6.2 1 ).
The
patient
is
su pine
s t r e tc h e d ; t h e t h e ra p i s t s t a n d s at t h e
end
with
legs
of the ta b l e
a n d grasps t h e p a t i e n t 's i n s t e p w i t h c l a s p e d h a n d s ,
t h e t h u m bs p a ra l l e l o n t h e s a l e to s t a b i l ize t h e foot
at righ t a n g l e s t o the l e g .
He
m u st ta k e c a re not to
h o l d the foot in m a x i m u m d o r s i fle x i o n beca use t h a t
Figure 6.20 E xa m i n a t i o n o j" j o i n t p l a y a n d m o b i l i z a t i o n
t he a n k l e j o i n t b y s p r i n g i n g t h e l e g a gd i n s t t h e h e e l
of
Copyrighted Material
TilempC l I lic reci1 l 1 i q l l fs
17 1
b l o c k a g e : w h a t we Il nd is s o m e resi s t a nce , as t h o u g h
t h e pate l l a w a s m o v i n g o v e r a n u n e v e n o r r o u g h
s u rface. T h is s e n s a ti o n i s e v e n m ore m a rk e d i f s o m e
pressure is a pplied to t h e p a te l l a fro m a bo v e . W h i l e
t h e p a t i e n t l i es s u p i n e w i t h t h e l e g s t re t c h e d a t t h e
k n e e , t h e t h e r a p i s t g r a s p s t h e p a te l l a betwee n t h e
t h u m b a n d fi ngers of o n e h a n d , w h i l e t h e o t h e r h a n d
e x e r t s s l i g h t press u re fr o m a bo v e w i t h t h e t h e n a r
e m i n e nce o r w i t h t h e t h u m b . W i t h b o t h h a n d s a c t i n g
i n u n i s o n , t h e t h e r a p i s t n o w moves the p a te l l a s o a s
to sense w h e re t h e ro u g h n e s s l i e s ; h e t h e n s l i g h t l y
i nc reases p r e s s u r e so a s to sm oo t h o u t t h e r o u g h
ness, w i t h o u t c a u s i n g p a i n A ft e r a fe w re p e t i t i o n s
h e fe e ls t h a t r o u g h n e s s a n d r e s i sta n ce h a ve s u b s i d e d .
A t t h i s m o m e n t , t o o t h e p a t i e n t fee l s c o n s i d e r a b l e
re l i e f. Th i s t e c h n i q u e ca n be t a u g h t to pa t i en ts fo r
­
,
Figure 6.2 1 TI'a c t i o n m a n i p u l a t i o n of t h e a n k l e j o i n t
,
pat i e n t
'
s t o e s w i t h h i s b u t t o c k s , g r a s p i n g t h e fi b u l a r
h e a d b e t w e e n t h u m b a n d fo re fi n ge r :
h a n d h e fi x e s t h e t i bi a b e l o w
the
with
the o th e r
k n e e . With
his
fingers ro u n d t h e fi b u l a r h e a d h e m a k e s a d ors a l a n d
v e n t r a l sh i ft ro u n d t h e t i bi a , t o d e t e r m i n e w h i ch
restrict e d . Fo r m o b i l i z a t i o n h e
s l a c k i n t h e r e s t r i c t e d d i re c t i o n a n d
r h y t h m i c a l l y s p r i n gs t he e n d -posi t i o n . I t i s u s e fu l t o
r e i n fo r c e t h e t h u m b a t t h e fi b u l a r 11 e a d with t h e
t h u m b o f t h e o t h e r h a n d , w h i c h fo l l ows t h e r o t a t o r y
m o ve m e n t round t h e t i b i a . The same e f fect c a n
be a c h i e v e d b y susta i n e d m o d e r a te press u re a ft e r
e ngaging the b a rr i e r t o o b t a i n m y o fa s c i a l re l e a s e .
d i rect i o n
is
mos t
takes up the
s e l f- t re a t m e n t .
treated first b y ( d i s ) t r a c t i o n
(Figure 6 . 2 3 ) . The s i m p l e s t is t o l a y t h e
p a t ie n t p r o n e o n a m a t on t h e fl o o r t h e knee b e n t
a t r i g h t a n g l e s . T h e t h e r a p i s t ( s t a n d i n g ) p u ts o n e
foo t o n t h e t h i g h j us t a bove t h e k n e e a n d gra s p s t h e
l e g w i t h b o t h h a n d s ro u n d t h e a n k l e , p u l l i n g i t i n a
v e rtica l d i r e c t i o n .
A s a t t b e e l b o w , l a t e r a l. spring i n g t o g a p t h e j o i n t
o n t h e m e d i a l o r l a te ra l a s pect i s a n i m p o r t a n t
t ec h n i q u e ( Figu re 6 . 24 ) . The p a t i e n t l ie s s u p i n e , t h e
l e g st re t c h e d b u t n o t o v e r - s tre t c h e d . T h e t h e r a p i s t
sta n d s b y t h e t a b l e a l o n gs i d e t h e a ffected k n e e ; w i t h
o n e h a n d h e g r i p s t h e p a t i en t s a n k l e , l i ft i n g i t s l i g h t l y
a bo v e t h e ta b l e . W i t h t h e o t h e r h a n d s u p ported b y
t h e t r u n k he e x e r t s s li g h t p r e s s u r e a t t h e l e v e l of t h e
j o i n t s p a c e to t a k e u p t h e s l a c k , a nd t h e n s p r i n g s t h e
j o i n t m e d i a l l y . I n o r d e r to s p ri n g t h e j o i n t l a te ra l l y ,
t h e t h e r a p i s t m u s t s i t o n t h e t a b l e be t w e e n t h e
p a t i e n t s l e gs f a c i n g t h e k n e e j o i n t . F a s t sh a k i n g i s
t h e m o s t e ffect i v e m o b i l i z a t i o n .
T o a p p l y a s l i g h t t h r u s t , w b i c h i s s o m e t i m e s u s e fu l ,
w e us e t h i s t e c h n i q u e b u t fi r s t a s k t h e p a t i e n t to
b e n d a nd s t retc b t be k n e e ; w h i l e t h e p a t i e n t a c t i v e l y
stretc h e s t h e j o i n t t h e t h e rap i s t d e l i v e rs a s l i g h t
The
knee j o i n t c a n b e
te c h n i q ues
,
'
The k n ee j o i nt
Th e tech n iq u e of e x a m i n a t i o n a n d r e s t o r a t i o n of
j o i n t p l a y begi n s w i t h t h e p a t e l l a : w i t h t h e l e g
e x t e n d e d a n d t h e q u a d r i c e ps m u s c l e re l a x e d , t h e
p a t e l l a should b e fr e e l y m o b i le a g a i n s t t h e fe m ur i n
a l l d i re c t i o n s If t h e re is rest rict i o n , t h e r e i s no re a l
.
Figure
tibia
'
6.22 M o h i l i z a t i o n o f t h e fi b u l a r h e a d a ga i n s t t h e
Figure
,
6.23 K nee traction w i t h t h e p a t i e n t pro n e
Copyrighted Material
1 72
Manipulalive Therapy
Figure 6.24 L a t e ra l
in Rehabilitation of the Locomotor
springing (gappi ng) of the k nee joint
t h rust a t t h e k n ee joint, with his ha n d , i n a m e d i a l
or l a te r a l d i rection w h i le fi x i n g t h e h e e l w i t h h i s
other hand.
A s w i t h t h e e l bow, i t is i mporta n t t h a t t h e
t h e ra p i s t s h o u l d s t a n d a t the l e v e l o f the k n e e , so
that the hand that s prin gs the j o i n t is s u pported by
the move m e n t of the trunk; the h a n d t h a t grasps the
h e e l is t h e re fo r fixation only, a n d should never
deliver a thrust.
The hip j o i nt
T h i s j o i n t , as an a l most idea l b a l l -a n d -socket joint,
h ardly a l l ows s h ifting m o ve m e n t . I t here fore o n l y
descri be tract i o n tech n i q ues he re ; t h e y are t h e most
i m p orta n t a n d t h e most e ffec t i v e . Traction m a y be
carried out e i t h e r a l ong the l o n g a x i s o f the leg, or
i n t h e d i rection o f the fe m oral neck.
In the fo rmer case ( Fi g u re 6 . 2 5 ) , t h e p a t i e n t i s
s u p i n e w i t h a strap fi x i n g the p e l v i s . The t h e r a p i s t
s t a n d s a t the foot o f the t a b l e ; a stra p pass i n g rou n d
h i s w a i s t is fas tened r o u n d t h e p a t ie n t ' s l e g above
the a n k le . W i t h both hands on this strap, the
t h erapis t t akes u p the sla c k b y very sl ight tracti o n ,
t h e leg b e i n g in 1 0 d egre es a b d uctio n , flexion a nd
ro t a t i o n at t h e h i p j o i n t . W h e n he fe els that the
Figure 6.25 Trac t i o n of t h e h i p j o i n t a l o ng the l o n g � x i s
s t r a p ; ( b ) a p p l y i n g the s e c o n d s t r a p
of
System
p a t i e n t has re laxed h e de l i vers a h igh-veloc i ty th rust
b y p u l l i n g sudd e n l y with both h a nds a n d t r u n k , thus
p u l l i n g the femora l head sl ightly out of t h e socke t .
(This mov e m e n t i s o n l y of a fe w m i ll i m etres , a s
v i s u a l ized b y X-ra y . ) W h e n traction is re leased t here
is a t i n y t h u d .
T h e fo l lowi.n g tec h n i c a l details are i m port a n t : ( 1 )
t h e therapist s h o u ld take up the s l a c k w i t h as l i t tle
force a s possi b l e , i . e . by w a i t i n g for t h e patient to
re l a x or by begi n n i ng w i t h P I R ; (2) the therapist
m ust not release h i s p u l l before giv i n g the t hrust; (3)
h e must n o t sq ueeze the a n k l e with h i s hands.
I use traction by P I R muc h m o re ofte n than this
h i gh-velocity thrust. As the fo rce used in t h e former
is m i n i m a l , strap p i n g is u n necessary. G rasping the
p a t i e n t 's heel t h e t herapist te l l s h e r to resist tracti o n ,
i . e . t o p u l l up h e r l e g w i t h m i nimum force and h o l d
t h i s movem e n t for a bo u t t o s . Tow a rds t h e e n d o f
t h i s i s o m e t r i c p h ase the pa t i e n t should b reathe i n ;
s h e i s then t o l d to ' l e t go' a n d to breathe out. A l l
t h a t t h e t h e rapist now fe els i s t h a t the leg l e ngthens
b y re laxation, without any fu rther p u l l . This man­
oeuvre is re peated t h ree to five times.
For traction i n the d i rec t i o n o f the fe moral neck
the pa t i e n t i s supine a n d t he bu ttock is on the edge
o f the t a b l e , fo r m i n g a fu lcrum ( Figure 6 . 26 ) . The
therapist sits o n a stool by the side of the table, t h e
patie n t's l e g o v e r h i s s ho u l d er, wi th be nt k nee . He
now grasps tbe patien t 's t h igh w i t h both h a nds, his
fo rea rm in the gro i n , a n d gives a s l ig h t obliq ue pu l l
i n t h e di rection o f the fe moral neck. The patient p u ts
up slight res i s t a n ce by p u l l i n g t h e b e n t leg in t h e
opposite d i rection, w i t h the pel vis ( i . e . in t h e di rection
o f the opposite shoulde r ) . The patie n t holds t h i s
resistance duri n g s l o w in h a l a t i o n , then s h e h o l d s his
breath, aft e r w h i c h s h e is told to 'let go' a nd bre a t h e
o u t . A ga i n , d u r i n g re l a x a tio n t h e t h igh i s fe l t t o
l e n g t h e n ( g i v e ) s l i g h t l y . T h i s tech n ique is much less
e ffective when passive pull only i s used. with or
w i t h o u t t h rusting.
The d i ffi c u l ty w i t h t h i s techn i q u e l i es i n maki ng
the p a t i e n t u n derstand w h a t to do during the
the leg. using
Copyrighted Material
two
s t r a ps: ( a ) fi x a t i o n o f
the
pa t i e n t w i t h one
Th erap e l l lic lechlliques
1 73
Figure 6.26 Tra c t i o n of the h i p j o i n ! a l o n g t h e a x i s of t h e
n e c k , o v e r t h e edge of t h e ta b l e
Figure 6.27 M o b i l i z a t i o n of t h e t e m p o ro m a n d i b u l a r j o i n t
isometric p h a s e , for i t is not j ust t h a t s h e h a s to flex
he r h i p . She has a t the same time t o pull her hip up
in a cra n i a l d i recti o n but not to flex t h e k n ee. To
achieve t h i s , it is best i f the t h e ra pist d e m o n s t ra t e s
this moveme n t by passively fl e x i n g t h e p a t i e n t ' s
knee a n d push i ng t h e h i p u p w a r d s . O n l y w h e n the
patient h a s fu l l y u n d e rstood this, c a n she d o i t
a ct i v e l y . D u r i n g re l a x a t i o n i t is m o s t import a n t for
the p a t i e n t to l e t t h e therapist bear the full weight
of h e r l eg o n his s h o u ld e r . O n ce t h e p a t i e n t has fu l l y
u n d e r stoo d a n d l e a r n e d how to do t h is , a n ybod y
with w h o m t h e p a t i e n t lives or w h o is at h a n d c a n
rep l ace the t h e r a p i s t as a l l h e d o e s is to h o l d h i s
h a n d s i n the pa t ie n t s g r o i n .
A s t h e l o w e r e x t r e m i t y i s accessi b l e to both the
patie n t ' s hands, many o f t h e tech n i q ues descri bed
a re u s e f u l fo r s e l f- t re a t m e n t .
a n d t h e b e n t fo re fi nger o n the c h i n , the s l a c k is t a k e n
u p b y p ressu re on t h e m o l a rs from above. The patient
resists t h i s pull d ur i n g exhalation and relaxes d ur i n g
i n h a l a ti o n .
M o s t freq u e n t l y , however, m o v e m e n t res trict i o n
is d o m i n a te d by s p a s m o f t h e m a s t i catory m u scles
which have to be relaxed (see Post -isometric re l a x ­
ation, p. 211).
fe m o r a l
.
'
The temporo m a n d i b u l a r j o i nt
For t re a t m e n t , l a te r o l a te r a l move m e n ts of t h e j a w
are m o s t conve n i e n t , a n d aga i n PI R p r o v i d e s t h e
g e n t l e s t a n d m o s t e ffect i v e tec h n i q u e ( F i g u r e 6.27 ) .
T h e p a t i e n t i s se a t e d w i th h e r h e a d tu rned to o n e
side; t h e therapist stands b e h i n d h e r , s t a b i l izing t h e
pati e n t 's head aga i ns t h i s ow n chest. The p a t i e n t i s
told to o p e n h e r m o u t h , i . e . to let h e r c h i n d r o p ; t h e
t hera p i s t cradles the m a n d i ble from the side, betwe e n
t w o fi n ge rs , m o v i n g i t t o t h e opposite s i d e , towards
his chest. When h e has ta k e n up the slack h e a s k s
the pa t i e n t to breathe o u t d u r i ng the isom e t ric p hase
a n d i n d u r i n g re l a x a t i o n (see p . 29). D u ri n g re lax­
ation t h e ma n d i b l e moves i n the d i re c t i o n o f t h e
a ffected j o i n t . The proce d u re i s r e pea t e d t h ree to
fi v e times.
A g oo d a l ternative is s i m p l e tract i o n . With a
t h u m b on the m o l a rs on each side of t he ma n d i bl e ,
,
T h e sp i n a l c o l u m n
The p r i n c i p l e s set o u t a t t h e begi n n i n g o f t h i s
c h a p t e r a l s o h o l d fo r t h e spi n a l col u m n . There a re ,
however, s o m e s p e c i fi c tech n ic a l p o i n t s t o b e d e a l t
w i t h ; for i n s t a n ce , i t is obviously more d i fficu l t t o
m o v e a s i ngle m o b i l e segm e n t t h a n a s i ngle extre m i ty
j o i n t . F u r t h e r m o r e , i t is more d i ffi c u l t to d i s t i n g u i s h
j o i n t p l a y f r o m functi o n a l move m e n t i n t h e s p i n a l
col u m n . A s i t i s n o t possible to m ove a s i ngle
segm e n t acti v e l y , passive m o v e m e n t repres e n t s a s it
w e re j o i n t play. This d i fficu l t y appJies particu l a rly t o
s hif t i n g tec h n i q ues, a n d less to d i stracti o n . Tech­
n iques that p rod uce ga p p i n g t h us c l e a rl y use j o i n t
p l a y for t h e i r e ffe ct, ( e . g . rota t i o n i n t h e l u m b a r
s p i n e , d o r s ov e n t r a l t h rusts i n t h e t horacic s p i n e ) .
Because of t h i s r e l a t i v e d i ffi c u l ty in m o v i n g s i ngle
joints we d is t i ng u i s h specific a n d n o n -specific tech­
n iques.
There a re several w a y s o f a c h i e v i n g a specific
effect: the ideal w a y , a l t hough n o t a l ways practicab l e ,
is d i rect fi x a ti o n of a t l e a s t o n e p a r t n e r ( t h i s c a n
a l ways b e d o n e i n a n e x t re m i ty join t ) . A n other w a y
is to a p p l y ' locking' tech n i q ue s i f l e v e rage is u se d ;
t h i s i s t o gre a t a d v a n t a g e , for exa m p l e , w h e n moving
t h e head i n o r d e r to m a n i p u l a te the c e rv i c a l s p i n e ,
or t h e legs a n d pelvis i n order to m o b i l ize t h e l u m b a r
Copyrighted Material
1 74
Munipululive Th erapy
ill
Rehabili/alion of Ihe
Locom olOl' Syslem
such a t ec h n i que speci fic we m u s t
the segm e n ts e x c e p t for the o n e
we w i s h t o m a n i p u l a te . T h e p r i n ci p le of ' l oc k i n g '
consists of b ri ngi ng i n to an ex t r e m e p o s i t i o n the
s e g m e n t s w e do not move, u n d e r a cert a i n degree
o f te n s i o n . The me c h a n i s m is e i t h e r a pp o s i t i o n of
bony s tr u c t u res or tension of l i ga m e n t s . Even h e r e ,
h ow e v e r . we have to t a k e u p the s l a c k to m a ke a n y
type o f m a n i p u l a t i o n e ffec t i v e . I t c a n t h us be s e e n
t h a t t h e ' lo c k i ng' i s o n l y rel a t i v e , a n d i f leverage i s
forc e f u l , treatm e n t w i l l never be speci fic. Leverage
i s , of course, very a d v a n t ageous, but i t m u s t b e
a p p l i e d w i t h v e ry l i t t l e force t o make l ock i n g tech­
n i q ues e ffe c t i v e . I t i s , t h e r e fore, p r e fe ra b l e to rely
s p i n e . To
ma ke
try to ' l o c k ' a l l
on fi x a t i o n rat h e r t h a n on l o c k i ng.
Loc k i n g i s a c h i eved m a i n ly by a carefu l combi­
n a t i o n of s i d e - bend i n g and rot a t i o n , m a k i n g use of
coupled m o v e m e n t s . L o r d os i s i n t h e l u m b a r s p i n e
m e a n s th a t t h e re is s i d e - be nd i n g coup l e d w i t h
rot a t i o n i n t h e o pp os i t e d i rect i o n ; he nce we ach ieve
l oc k i n g by r o t a t i on a n d s i d e - b e n d i n g in the s a m e
d i rection . I n k y p ho s i s t h e o p p o sit e i s t r u e . and we
t h e re f o r e h a v e t o co m b i n e s i d e - b e n d i n g a n d rotation
i n t h e o p p os i t e d irect i o n . In t h e th oracic spine, s i d e ­
b e n d i n g i s a l w ays co u p l e d w i t h rot a t i o n t o t h e
op p o s i t e s i d e ( i n s c o l i o s i s , r o t a t i on is a l w a y s to t h e
s a m e s i d e ) a n d therefore l oc k i n g e n t a i ls s ide-ben d i n g
a n d rota t i o n t o t h e same s i d e . I n t he cerv i c a l s p i ne
there is a l wa y s s i d e - b e n d i n g a nd r o t a t ion to t h e
s a m e side, a n d h ere we a c h i e ve l ock i n g by s i d e ­
b e n d i n g and ro t a t i o n t o t h e o p p o s i te s i d e .
A n o b v i o u s way of a c h i e v i n g so m e deg r e e of
s p ec i fi c i t y i s by d i rect contact. C l e a r l y , a v e r te b r a
m a y be fi x e d by d irect contact i n a t l e a s t one
d i rection: for i n stance, by fi x a tion of a sp i no u s
process from t h e side w e p r e v e n t rotati o n of that
vertebra i n t h e o p p o s i te direction . If we exert
p r ess u r e , s p ri n g a v e r te b r a o r a p p l y a t h r u s t , som e
of t h e force w i ll be e ffec t i v e a t t h e site w h e r e it i s
a p p l ied . Indeed, c h i ro p r a c t o r s b e l i eve t h a t a h i gh­
v e l oc i t y thrust a pp l i e d w i t h s u fficie n t e n e rgy acts
l i k e a h a m mer o n a n u ncemen ted b r i c k wa l l , throw­
i n g one brick out and leaving all t h e rest i n p l a c e .
To achieve t h e m a x i m u m s p e c i fi c e ffec t , a combi­
nation of l everage a n d locking t ech n i q u e s w i t h d i rect
contact and fixation i s most com m o n l y u s e d . How­
e v e r a d v a n t a g e ous t hese tec h n i q ue s , t h e y a re e ffect­
i v e o n l y i f l e v e rage a nd lock i n g a r e a p p l i e d e x a c t l y
to the site w h e re t h e oth e r h a n d m a ke s co n t a c t .
From t h i s it w o u l d a p p e a r ob v i o u s t h a t the h a n d
t h a t m a k e s con t a c t fi x e s o r m o v e s the v e r t e b r a in a
d i r e c t i o n opposed to t h e d i recti on of le ve rage
a p p l i e d by the o t h e r h a n d . T h i s i s u s u a l l y true, b u t
t h e re are certa i n t e c h n i q u e s i n w h i c h both h a nds
move in t h e s a m e d i rectio n , a s a single fo rc e , t h e
segme n t b e l. ow the treated v e rtebra b e i n g fi xed b y
p o si tion i n g ( e . g . the pelv i s fi x e d by t h e pa t i e n t s i t t i n g
a s t r i d e t h e ta b l e ) . T h i s type of tec h n i q u e g iv e s
consi d e rable leverage, a n d m ust d e pe n d m a i n l y o n
loc k i n g . I t i s u s e d m o s t fre q u e n t l y i n p u re t r a c t i o n
tech n i q u e s w h i c h , a l t hough t h ey a re w i t h o u t ri s k and
a re ce r t a i n l y effec t ive , are o f doubtfu l spec i fi c e ffect
u n less very gen t l y a p p l i e d .
Th e r e a re a l s o n o n -s p e c i fi c t e c h n i q u e s t h a t c a n be
u s e f u l in m ob i l i z i n g l o n g e r sect ions of t he s p i n a l
c o lu m n . S u c h a
g e n e r a lly
n o n - s p e c i fi c
but widely
u s e d tec h n i q u e is t h a t o f traction a l ong the l o n g a x is
of t h e s p i n e . I t s i m p o r t a nc e a n d i n d ica t i o n h a v e
b e e n d iscussed i n C h a p t e r 5 ( p . 1 5 0 ) .
I n o r d e r to a v o i d c o n f u s i o n i t is i m po r t a n t to
d istinguish between trClction a lo n g t h e l o n g axis o f
t h e s p i n a l col u m n a n d d istrac t i o n of i n te rverte b r a l
j o i n ts . T h i s d i s t i nc t i o n is c l e a re s t i n t h e l u m b a r
r e g i on , wh e r e t ra c t i o n a lon g t h e l o n g ax is acts on t h e
i n te rvertebral d i scs, w h e re a s d i straction o f th e a po ­
p h ys e a l joi n ts is p rod u ced by r o t a t i o n ro u n d t hat sam e
a x i s . I n t h e cervica l spi n e , on t h e o t h e r h a n d , t ra c t i o n
a l o n g t h e l o n g a x i s a llects t h e d i scs a n d t h e j o i n ts.
The lu mbar spi n e
Traction tech n i q ues
I n te r m i t te n t m a n u a l traction is t h e most i m p or t a n t
o f t hese m e t hods. I f t h e p a t i e n t c a n l i e p r o n e i t i s
b e s t i f sh e p rovide s h e r o w n fi x a t i on b y h o l d i n g o n
t o t h e e n d o f t h e t a b l e . T h e t h e rapist grasps b o t h
t h e p a t i e n t ' s l eg s j u s t a b o v e t h e a n k l e , a n d w i t h
slight traction m a k e s s u re t h a t s h e i s c o m p l e t e l y
re l ax e d . He m ust t h e n e s t a b l i s h t h e cor re c t r h y t h m
o f t r a c t io n , i n order to l ocal ize t he e ff ec t i n t h e low
b a c k . I f t h e rh y t h m is too slow, t h e patie n t ' s w h o l e
body w i l l m o v e sl i g h t l y , up a n d dow n , on t h e t a b l e .
B y q u i c k e n i n g t h e r h y t h m t h e t h e r a p i s t w i l l fi n d a t
w h ic h poi n t o n l y t h e legs a n d p e l v is m o v e w h i l e t h e
l o w back re m a i ns s t i l l , l i k e a n o d a l poi n t i n a
s t a n d i n g wave. W h e n t h i s rhy t h m h a s bee n fo u n d ,
t h e p a t i e n t fee l s t h e i n t e r m i t te n t t ra c t ion exactly i n
t h e l o w b a c k . Th i s s h o u l d b e d o ne w i t h l i t t l e force .
b u t once t h e r hy t h m is e s ta b l i sh e d e a c h p u l l m a y be
re i n fo rced a n d occasion a l l y som e t h i n g l i k e a t h r u s t
d e l i ve red.
I t can be a l so v e r y use fu l t o a p p l y r h y t h m i c
t ract i o n by o n e l eg o n l y , i f t he p a t i e n t fe e l s re l i ef.
O b v i o u s l y t h i s m e t hod i m p l i es m a n ua l tra c t i o n o n l y .
The t h e r a p i s t must avoid s q u e e z i n g t h e l e gs a bove
th e a n k l e .
I f t h e p a t i e n t ca n n o t s t re tch o u t , a s i s o ft e n t h e
c a s e in t h e a c u t e s t a ge . i n te r m i t t e n t t ract i o n is
c a rr i e d o u t i n kyphosis (Figu re 6.280 ) . For t h i s the
p a t i e n t l i es on her b a c k with her l eg s bent a t the h i p
a n d k n e e . I f t h e t a b l e i s a d j u s ta b l e i t s h o u l d be a s
l ow as possi b l e . T h e t h e r a p i s t s t a n d s a t t h e s i d e o f
t h e t a b l e , h i s foot o n i t , s o a s t o h a v e h is k n e e a n d
t h i g h u n d e r the pa t i e n t ' s rl e x e d knees. u s i n g h e r l e gs
as a l e v e r . Exe r t i n g pressure on t h e p a t i e n t ' s a n kl e s
fr o m a bove. h e l i fts t h e p a t i e n t ' s p e l v i s w i t h a
Copyrighted Material
Therap eutic techniques
t h a t s h e is r e l a x e d w i t h
her b u t t ocks clea r o f t h e tab l e . By i n c re a s i n g a n d
loweri n g t h e pressure u p o n t h e a n k les i n te rm i tt e n t
traction i n k y p h osis is a c h i e ved ( a t a rh y t h m o f about
two p e r second ) . Obvious l y this t e ch n i q u e wo r k s o n l y
i f t h e t h e r a p i s t s l ow e r l e g is l o nger t h a n the p a t i e n t ' s
thighs; i t i s usua l l y necessary f o r h i m to kee p h is
shoe o n , a n d pe r h a p s p l a c e a l i t t l e board u nd e r t h e
foo t . As i n t h e a c u t e s t age o f l u mb ago a n d r o o t pai n ,
ky phosis i s fre q u e n t l y t h e r e l ie f positi o n ; i f w e l l
to l e ra ted , t h i s t ec h n i q u e p l a y s t h e ro le o f fi rst a i d .
T h e r e a re t w o v e r y e ffe c t i v e a n d ge n t l e traction
m e t h o d s t h a t m a k e u s e o f PIR. For t h e fi rst th e
p a t ie n t l i es p ro n e ( Figure 6.28b ) , w i t h h e r h e a d ne a r
roc k i n g m o t i o n , m a k i n g s u r e
'
1 75
to the e n d o f the t a b l e . The t h e r a p ist s t a nds at t h e
head o f t h e table and p u t s t h e h e e l of h i s h a n d s o n
t h e p a t i e n t ' s b u t tocks from above. He tells t h e
patien t to b re a t h e o u t slowly a n d d eepl y , and feels
resistance i nc re a s i n g . T h e patie n t i s t h e n to l d to t a k e
a s l ow , d e e p b re a t h , a n d a s s h e does s o t he b u t toc k s
move down a n d t h e l u m b a r s p i n a l l o rdosis fl a t t e n s
This is fo l lowed by long, deep e x h a l a t i o n a n d agai n
t h e buttocks tend to move upwards. The therap i s t
resists t h i s m o ve m e n t , w h i c h is fo l lowed by re l a x ­
a t i o n or a c a u d a l m ove m e n t of t h e bu ttocks d u r i n g
i n ha l a t i o n . Resistance to each u pward move m e n t o f
the b u ttocks d u r i ng e x h a la t i o n i ncreases t h e i n t e nsity
o f t h e tracti o n . This resist a nce i s even more e ffective
if i n te r m i t t e nt.
As a n a lte r n a t i v e : the t h e ra p ist s ta n d s a t the side
of t h e patient and prod uces traction with his crossed
h a n d s , one over the low thoracic spine and the o t h e r
on the sacru m .
For traction w i t h P I R i n k y p hosis t h e p a t i e n t i s
prone ove r t h e e n d o f t h e tabl e , h e r legs h a n g i n g
down from t h e h i ps ; t h e t a b l e should be h i g h e nough
fo r t h e fee t to be clear of the floor; i f t h e fee t d o
t o u c h t h e floor, t h e l e g s must s ti l l h a n g re l a x e d . T h e
t h e rapist s t a n d s a t t h e s i d e of the p a t i e n t ' s low back.
placing t h e h e e l o f o n e o f h i s c ro ssed h a nds o n the
sacrum ( from above ) a n d t h e other from b e low o n
t he sp i n ous p rocess o f a l umbar v e rtebra , accord i ng
to t h e s i t e w h e re t ract i on is req u i red . H e now te l l s
t h e p a t i e n t to give s l ig h t re s i s t a n c e to t h e traction
h e a p p l i e s by a s l i g h t p u s h on t h e sacr u m , i n a cauda l
directi o n , a n d with the oth e r h an d in a cranial
d irecti o n . The patient is told to breathe o u t s l o w l y
a n d t h e n to ' l e t go' a n d bre a the i n . T h i s tec h n i q u e
c a n b e u s e d for se l f-tre a t m e n t , t h e p a t i e n t ra i s i ng
h e r b u ttoc k s w h i l e breat h i ng o u t , a n d d ro pp i n g
( re l a xi ng) t h e m whi le bre a thing i n . Th e effect of
.
,
( a)
( b)
Figure 6.28 (a) Tract i o n of t h e l u m b a r s p i n e i n k y p h os i s ( s u p i n e ) . ( 0 ) I s o m e t r i c tract i o n of t h e l u m b a r s pi n e (pro n e ) :
l e f t . i n creased re s i s t a nce d u r i n g ex h a l a t i o n ; r i g h t . t he b u t tocks m o v e i n a c a ud a l d i r e c t i o n d u r i n g i n h a l a t i o n
Copyrighted Material
176
Manipulative Th erapy i n Rehah ilitation of t h e Locomotor Syslel11
e x h a l a t i o n i s , however, m u c h less i n t e nse i n l um b a r
kyp hosis t h e n i n t h e prone lord o t i c positio n .
T h e re a re m a n y wel l - k nown methods o f traction
pe r formed on spec i a l tables, i nc l u d i n g i n te r m i t te n t
tracti o n , b u t n o n e c a n compete w i t h m a n u a l t raction
by a s k i l l e d therapist. There is one pri nciple that
m u s t be stress e d , h owever, both in man u a l a nd
especi a l l y i n ta b l e tractio n : it must not be p a i n f u l. I f
t h e p a t i e n t fee l s d iscomfort, t h e t he r a p i s t m u s t fi n d
a pos i t i o n i n w h i c h t ra c t i o n i s we l l tole r a t e d , or e l se
a b a n d o n it. Pa i n d u ri ng traction i s freq u e n t l y due to
b l o c k a ge in the l u m b a r s p i n e or t h e sacroi l i a c j o i nts;
t h i s c a l l s fo r tre a t m e n t .
M a n i p u lati o n
I n m a n i p u l a t i o n i t i s useful t o b e g i n by u s i n g t h e
s p r i ngi ng tech n i q u e described fo r the examina t i o n
o f retrofl e x i o n i n i n d i v i d u a l m o b i l e segm e n ts (see
pp. 1 02-1 03). T h e patie n t l i es with b o th h i ps and
knees flexed. The t h e r a p i s t l e a n s his thigh a g a i n s t
t h e pati e n t ' s k n ee s , fixing the s p i n o u s process o f the
upper verte bra of the treated segme n t w i t h one
fi n ger, re i n forced by the fi n ge rs of the other h a nd
p l aced over it. H e now tells t h e p a t i e n t to p ress her
k n e e s s l ightly agai nst t h e t h e rapist's t h igh (but not
s o h a rd as t o p u s h him a w a y ) a n d to breathe i n a n d
then t o h o l d h e r breath. A t t h e e n d o f t h i s isometric
phase the p a t i e n t is told to ' l e t go' and bre a t h e out.
W h i l e the p a t i e n t relaxes t h e t h e ra p i s t has the
i m pressi on th a t the h a n d s on the s p i nous process a re
s i n k i ng i n to a hoUow, as the m o b i .l i zed spi n a l
segme n t moves i n to lordosis. T h e proce d u re i s
re peated from t h is posi t i o n , a bo u t th ree t i m e s (see
Figu re 4 . 1 6 , p . 103).
The most popu l a r m a n i p u l a t i ve tec h n ique is p rob­
ably that o f ro t a tio n , with t h e pa t i e n t lying on her
side (Fig u re 6.29). S h e should be i n a ' n e u t ra l '
posi t i o n , i . e . n e i t h e r i n fl e x i o n n o r e x te nsi o n . The
leg t h a t lies o n the table is not fu l l y e x t e n ded w h i le
the o t h e r is b e n t a t the h i p a n d k n e e , so t h a t the
foot i s fixed by the s l i g h t l y ben t k ne e o n t h e t a b l e ;
t h e o t h e r k n e e is b e n t a n d p roj ects over t h e e d g e 0 1'
t h e t a b le . The t he rapist stands in fro n t o f t h e p a t i e n t
so as t o fi x t h e fl exed knee w i t h h i s t h igh . Passi ng
h i s h a n d ove r t h e pati e n t s h ip, he fixes i t with h i s
fo rearm w h i l e w i t h t h e u l n a r aspect o f the h a n d h e
fixes the pa rt of t h e l u m b a r s p i n e t h a t is ca u d a l to
t h e l o w e r vertebra of t h e segm e n t being treated; o ne
or two fi n ge rs are used to fi x the spinous process o f
t h a t ve rtebra . I n t h i s w a y h e c a n completely fix t h e
l umbar s p i n e , up t o the segme n t to be t re a t ed . T h e
e l bow of t he therapist's o t h e r arm l ies o n the
patie n t's s h o u l d e r ( u n less the p a tie n t is much t a l l e r
t h a n the th e rapist, i n w h i c h c a s e i t l i es o n t h e a r m
b e l ow t h e sho u l d e r ) a n d i t i s h e l pfu l i f the p a t ie n t
s l i ngs t h i s a rm rou n d t h a t o f t h e therapist. W i t h the
t h u m b o f the h a n d com ing from the s h o u l.der the
t h e ra pist esta blishes contact w i t h the spi nous process
o f the u p per vertebra of the segme n t to be t rea ted .
Obviously i f t h i s is t h e l u m bosacra l segment it i s
s u fficie n t for t h e h a n d passing ove r t h e p a t i e n t ' s h i p
to fi x the pelvis a lo n e . I n o r d e r to t a k e u p t h e slack
it is best to tell t h e patient t o look i n the d i rect ion
o f m ob i l ization ( i . e . away from the t hera p i st ) a s
fa r a s he c a n a n d t o wa i t fo r c o m p l e t e rela x a t i o n a t
t h e ba rr i e r . W i t h t h e pati e n t th us posi tioned , t he
thera pist fixes the shou l d e r ( o r a r m ) from a bove and
t e l l s the pa t i e n t to look towards h i m a n d brea t h e i n
s lo w l y , a n d t o h o l d his b re a t h ; the therapist resists
rotation ( i n the opposite d i rection from m o b i l iza­
t i o n ) . The p a t i e n t is then told to look in the d i rection
o f m o b i l i z a t i o n and to breathe ou t s l ow l y . I n this
way the range of rota t i o n a u tomatica l l y i ncreases,
'
Figure 6.29 R o t a t i o n m o b i l i z a t i o n o r t h r u s t m a n i p u l a t i o n o f t h e l u m b a r s p i n e w i t h t h e p a t i e n t o n h e r s i d e . i n n e u t r a l
pos i t i o n
Copyrighted Material
Th erap elltic techn iqlles
1 77
Figure 6.30 A c t ive repe t i t i v e m o b i l i z a t i o n of t h e l u m b a r s p i n e w i t h t h e p a t i e n t l y i n g on h e r s i d e
pos i tion is r each e d a n d fixed by t h e
p ro c e d u re i s repe a ted a bo u t th ree
t i mes. Q u i te freq u e n t ly a spontaneous ' c l i c k ' is heard
d u ri n g re l a x a t i o n . W h e n the s l ac k i s ta k e n u p ( a n d
end-position is re a ched ) , h e m a y m a k e a n a d d i t i o n a l
t h r u s t aga i nst t h e s h o u l d e r.
Th i s is a fu l l y a u toma t i c m o b i l i za t i o n t e c h ni q ue ,
t h e p a t i e n t res i s t i n g w h i l e l ooking towards t h e t h e ra­
pist and b rea t h i n g in, a n d re l a x i n g when l o o k i n g
a w a y from h i m a n d brea t h i ng o u t . I t s h o u l d b e t h e
basic tec h n i q ue u s e d i n ex te nsion restrict i o n . I t
prod uces ga p p i n g o f t h e u p p e r i n te rvertebra l j o i n t
a n d c a n b e used through o u t t he l u m b a r s p i n e a n d
e v e n a t t h e t h or a colu m b a r j uncti o n .
A repeti t ive tec h n i q u e from t h e e x tr e m e pos i t i o n
re a c h e d by r e l a x a t i o n ca n b e u s e d , as a mod i fica t i o n .
With h i s h a n d over t h e pa t ie n t s b u t t ocks to m a i n ­
tain fi x a t i o n , the thera pist te l l s h e r to t u rn t o a n d
fro ; h e may ev e n rei n fo rce t h e fi x i n g h a nd by t h e
other ( F i gu r e 6 . 30) .
T h e o t h e r te c h n i q u e o f si m i l a r i m p orta n c e i s
mo b i l i z a t i o n i n fl e x i o n ( fo r fl e x i o n r e s t r i c t i o n , F i g u r e
6 . 3 1 ) . The p a tien t a ga i n l i es o n her sid e , b u t in a
somewhat k y p h o t i c posi t i o n , th e l eg on t h e t a b l e
fl e x e d a t t h e h i p a n d k nee. T h e o t h e r ( u pper) l e g
h a ngs ove r the e dge of t h e t a b l e (exce p t w h e re t h e
s t ra i g h t l eg ra i s i ng test is h i g h l y posi tive, i n w h i c h
case s h e b e n d s t he leg so as to fix t h e foot a t t h e
k n ee o f t h e low e r l i m b ) . T h e t he r a pis t fi r s t fixes t h e
p e lv i s i n a n obliq ue pos i t i o n , i . e . not pe r pe n d i c u l ar
to t h e table b u t ti l t e d forwa rd so t h a t t h e w e i g h t of
t h e h a n gi n g leg e n h a nces k y p hosis. The t h e rapist
uses h i s other h a n d to p u l l fo rwa rd t h e a r m o n w hi c h
the pati e n t i s l yi ng, s o as t o i ncrease kyp hosis s ti l l
furt h e r. Th i s m u s t b e done w i t h great ca re, s o a s not
to stra i ghten t h e pel v is, i.e. not to re t u rn i t to t h e
perpe n d i c u l a r . T h is pos i ti o n is e ss e n tia l for the
success o f the tec h n i q u e .
a nd
it
new
t h e ra p i s t . T h e
'
The therapist fixes the pa t i e n t s l e g w i t h h i s th igh ,
pass i n g h is fore a r m over the h i p , the h a n d p o i n ti n g
i n the d i rection o f t h e c a u d a l ve rtebra o f the segm e n t
to be treated. With t h e e lbow of t h e other arm against
the p atie n t s shoulder, the the rapist te l l s t h e patient
t o look t o t h e ce i l ing i n ord e r to obta i n rotati on of
the trunk away from h i mself, to take u p the s la c k .
The t h u m b of t h e h a n d over the shoulder fixes t h e
spinous p rocess of the u pper v e r te b ra fr o m a bo v e , by
a downward p ul l with t h e d istal p h a l a n x of t he t h u m b .
Aga i n , i f t h e t h era p i st is not t a l l , i t i s better for t h e
p a t ie n t to sling h e r a rm rou n d t h e t h e ra p ist's, so t h a t
t h e therapist can exert pressu re a g a i n s t t he patien t ' s
a r m below the s h o u lder. I n t h i s posi t io n t h e patient
is told to p ress h e r hip s l igh tly aga i n s t the th e r a p i s t ' s
hand so a s to l i ft both hip a n d leg, a n d t o hold t h is
press u re fo r about 10 s, w h i l e b rea t h i n g i n a n d to h o l d
her breath. She is then t o l d to ' let g o ' a n d b rea th e
o u t and , as she re l a x e s , the h a n g i n g leg a n d h ip
'
'
Figure 6.31 M o b i l i z a t i o n or thrust m a n i p u l a t i o n of t b e
l u m ba r s p i n e w i t h t h e p a t i e n t o n h e r s i d e i n k y p h o s i s ,
t h e l o w e r l e g be n t a n d t h e u p pe r h a n g ing d o w n ov e r t h e
e d g e of t h e
table
Copyrighted Material
1 7R
Manip ll iarive Th erapy
il1 Rehab iliriltion of rh e LocomOlOr System
produce fu r t h e r hip rota t i o n a n d l u m b a r k y p h o s i s ,
a n d t h e t h era p i s t c a n fe e l t h e d i s t a n ce between his
b a r r i e r is re a c h e d b e t w e e n t h e s o ft t i s s u e s a n d b o n e .
The m o s t se r i o u s m i s t a ke i s t o i ncrease p re s s u r e
h a n d s i n c r e a s i n g . Th i s p rocedure ca n be re peated
b e fore a n y m o v e m e n t h a s b e e n fe l t . A p p a r e n t l y , i t
th re e to five times. If the slack has b e e n taken u p , th e
i s t h e r e l e ase o f press u re I h ilt m a k e s t h e j o i n t s p r i ng.
h a n d on t h e p a ti e n t 's h i p may a ls o give a t h r u s t i n
t h e sa m e d i recti o n . I n every case, t h e t h u m b o n the
s p i n o u s p rocess m llst m a i n t a i n fi x a t i o n .
How t llis te c h n i q u e ca n a l s o b e u s e d fo r m u sc u l a r
re l a x a t i o n a n d s e l f- t re a t m e n t i s d escri bed l a te r i n
t h i s c h a p te r
s t retch i n g .
(see
F i g u re
6.115),
a l so
it
se rves
The t e c h n i q u e p r o d u c e s s o m e d e g r e e of rota t i o n
a n d ga p p i n g o f t h e j o i n ts a n d e ffec t s tra c t i o n w i t h
a n t e f1 e x i o n a nd gre a t m uscu l a r re l a x a t i o n . Fo r t h i s
r e a s o n i t i s a d v is a b l e to u s e t h i s fl e x i o n tech n i q u e i n
d is c l e s i o n . f o r both fl e x i o n o r e x t e n s i o n re s t r i c t i o n
o n t h e p a i n fu l s i d e .
There a r e v e ry m a n y o t h e r t e c h n i q u e s i n u s e ,
p a r t i c u l a r l y t h ru s t i n g m a n i p u l a t i o n i n a dorsov e n t ra l
d i re c t i o n w i t h the p a t i e n t pron e o r o n h e r s i d e , b u t
t h e y d o n o t s e e m t o m e to be of s u c h v a l u e as to b e
worth descri b i n g h e r e .
The pelvis
T h e o n ly j oi n t t h a t i s t r e a ted by m a ni p u l a t i o n i s t h e
sacroi l i a c . F o r m o b i l iza t i o n , excel l e n t r e s u l t s ca n b e
a c h i e ve d w i th mov e m e n ts i n t w o a l m o s t p e rpe n d ic­
u l a r p l a n e s , the s a g i tta l ( n u t a t i o n of the s a c r u m in
re l a t i o n
to
the
innominate)
and
the
h o rizon t a l
( g a p p i n g t h e d o rs a l p a r t o f t h e sacroi l i a c j o i n t by
( b)
spr i n g i n g the i l i u m a g a i n s t the s a c r u m ) . A s t h e re a re
no m u s c l e s to m o v e or fix t h e sacroi l i a c j o i n t , t h e
s i m p l e p a ss i v e r e p e t i t i v e t e c h n i q u e w i t h a m i n i m u m
of force is a l w a y s effe c t i v e , prov i d e d t h a t t h e r e i s n o
s t r u c t u r a l c h a n g e p re s e n t .
F o r m o b i l i z a t i o n i n t h e s a g i t t a l pla n e , t h e p a ti e n t
i s pron e , w h i l e t h e t h e r a p i s t s t a n d s a t t h e s i d e o f t h e
t a b l e , faci n g t h e p a t i e n t ' s p e l v i s , a n d w i t h crossed
h a n d s p l a c e s o n e p i s i form on t h e pos t e r i o r s u p e ri o r
i l i a c s p i n e from b e l o w , a n d t h e o th e r on t h e c a u d a l
e n d o f t h e sac r u m ( F i g u re 6.320 ) . With s l i g h t p ress u re
he t a k e s up the s l a c k a n d ca n n o w s p r i n g t h e j o i n t
n o t s o m u c h b y press i n g b i s h a n d s d o w n w a rd s a s by
s e p a ra ting t h e m , aga i n w i t h v e ry l i t t l e forc e . It i s
m o s t i m porta n t t h a t a ft e r s l i g h t l y
i n c r e a si n g h i s
p re s s u r e t h e t h e r a p ist r e l e a s e s i t , e v e n i f a t fi r s t t h e re
is no r e s p o n s e i n t h e b l ocked j o i n t . A fter a b o u t five
repe t i t i o n s w i t h n o i n cr e a s e i n fo rce h e s h o u l d b e g i n
to s e n s e m o v e m e n t , a n d m o b i l ity i s u s u a l l y restored
to n o rm a l a ft e r about 15 r e p e t i t i o n s . T h e tec h n i q u e
s h o u l d be perfor m e d a t o n e o r t w o moves t o t h e
seco n d . The fo l l o w i n g p o i n ts a r e i m po rt a n t : t h e
p i s i fo r m m o v i n g t h e s a c r u m m u s t be a t t h e c a u d a l
e n d , j u s t a bove t h e coccy x , o t h e rwise t h e l e v e r i s too
s h o r t ; and t a k i n g up the slack i m p li e s bony con tact
- t h e t h era p ist m u s t mov e b o n e . not s k i n . There fore
I1 rs t t h e s o f t t i ss u e s a re very s l i g h t l y s h i ft e d u n t i l a
( c)
Figure 6.32 ( a ) M o b i l i z a t i o n of the s a c r o i l i 8 c j o i n t . w i t h
c r o s s e d h a n d s ( a l so u s e d for e x a m i n a t i o n ) . ( h l M o b i l iza­
t i o n o f the upper pari o f the s a c r o i l i a c j o i n t . ( c ) M o b i l ­
i za t i o n o f t h e l o w e r p a ri o f t h e sacro i l i a c joint
Copyrighted Material
Th erapelllic Icc!Jniqllcs
For mo b i l i z a t i o n i n t h e h o r i z o n t a l p l a n e , a diag­
n o s tic tech n i q u e ( see F ig u r e 4 . 1 0 , p. 98) c a n be use d ,
w i t h the pa t i e n t l y i n g on h e r s i d e . Once a ga i n , a l l
I h a ve s a i d a bo u t a p p l y i n g m i n i m um pressu re a n d
the i m po r t a n c e o f r e l e a si ng i t i s v a l i d . Th e r e i s o n e
i m po r t a n t det a i l to be b o r n e i n m i n d : a l t h o u g h t h e
therapist m ov e s t h e a n t e r i o r s u p e r i o r i l i a c s p i n e , h e
m u s t n o t r o t a t e t h e pe l v i s , b u t s h o u l d only p r od uc e
gapp i n g o f t he posterior p a r t of t h e sacro i l i ac j o i n t;
t h e p a t i e n t 's upper or bot h be n t k n ee s m u s t l i e o n
t h e t a b l e , a n d t h e t h e ra pist must th e r e fo r e p u s h the
i l i a c spine d o w n w a rds a n d b a c k w a rds with h i s
fo r e a r m o b l i q u e l y po i n t i n g ( a n d s l i d i n g ) i n a ve n t r o­
cra n iomedial d i recti o n . U s i ng t h i s tech n i q u e h e m a y
a lso a p p l y a t h r u s t a ft e r ta k i n g u p t h e s l a c k .
I f t h e upper p a r t of the s a c r o i l i a c o n l y is i n volve d ,
t h i s s t r u c t u re i s m o s t e ffe c t i v e l y t re a t e d w i t h t h e
p a t i e n t l y i n g o n t h e o t h e r s i d e , t h e l ower leg s l i gh t l y
b e n t . t h e u p p e r k n ee ( or b o t h b e n t k n e e s ) o n t h e
t a b l e . T h e t h e r a p i s t s i ts below t h e p a ti e n t ' s bu t t o c k s ,
fa c i n g h e r h e a d : w i t h one h a n d he e xe r ts press u re
aga i n s t t h e a n t e r i o r s u p e r i o r s p i n e i n a d or s a l
d i re c t i o n , t h e t h u m b o f h i s o t h e r h a n d prod u c i n g
co u n t er-press u re o n t h e b a s e o f t h e s a c r u m , j u s t
b e l o w t h e p o s t e r i o r s u pe r ior sp i n e , i n a v e n t r a l
d i rec t io n , r h y t h m i c a l l y sp r i n g i n g t h e i l i u m a ga i n s t
t he s ac r u m ( Fi g u re 6.32b ) .
I f i t i s m a i n ly t h e lo we r e n d o f t h e sacru m w hich
is i n v o l ved , t h e p a t i e n t l ies i n the s a m e p o s i t i o n b u t
t h e t h e ra p i s t s i ts a b ove h e r p e l v is. W i t h o n e h a n d
h e g r asp s t h e s u p e r i o r i l i ac s p i n e a n d w i t h t h e u l nar
a spect or the other h a nd h e m a kes c o n t a c t a t the
c a u d a l e n d of t h e s a c r u m ; r o t a t i n g b o t h h a n d s i n
oppos i te d i r e c t i o n s h e p roduces n u ta t i o n o f the
s a c r u m agai nst the i l i u m ( F i g u re 6.32c ) .
K u b i s ( 1 970) h a s described a no t h e r thrust t e c h ­
n i q u e i n t h e s a g i t t a l p l a n e (Figure 0 . 33 ) . T h e p a t i e n t
l i es o n h e r s i d e , o n e i c g o n t h e t a b l e s t r e t c h e d a n d
t h e o t h e r be n t a t h i p a nd k n e e , w i t h t h e foo t stabi l ­
ized b y t h e k n e e b e n e a t h i t . T h e t h e r a pi s t s t a n d s a t
Figllre 6.33
Thrusting tech nique i n
a
179
t h e side o f t h e t a b l e , f a c i n g the p a tien t ' s pelvis, and
fi x e s t h e k n ee with his th igh w h i le r o t a t i n g t h e
sh o u l d e r a w a y fro m h i m s e l f . H e now m a kes contact
with h i s p i s i fo r m (or th e fi rst p h a l a n x o f the b e n t
fo r e fi n g e r ) press i n g o n th e caudal t i p of the sacru m ,
to t a ke u p t h e s l a c k i n a d o rsove n t ra l d i rec t i o n , a n d
d e l i v e r s a t h r us t i n t h e same d i re ct i o n . Th e re a re two
i m p o r t a n t t e c h n i c a l p o i n ts to be n o t ed: t he thera­
pist's fo r ea r m de l i v e r i n g the t h r u s t must l ie i n t h e
d i re c t i o n of the t h r u s t , w h ich means that h e m us t
bend over t h e p a t i e n t ; a n d p e l v i c rota t i o n m u s t b e
a v o i d e d , t h e t h ru s t b e i ng o n l y dorsove n t r a l .
T h i s tech n iq u e produces a n a n te ri o r sh ift o f t h e e n d
of t h e sacrum aga i n s t t h e i l i um which i s fi x e d beca use
the patie n t i s lying o n it; the re s u l t is a move m e n t of
n u tation rou n d a fro n t a l a x i s a t S2, a c tin g o n t h e j o i n t
on the side o n wh i ch t h e p a t ie n t is l y i ng.
For tre a t m e n t of symphyse a l s h i ft we h a ve decid ed
not to use ' r e po s i t i o n m a n oe u v res', as w e a r e n o w
awa re o f p a l p a to ry i ll us i o n (see Figures 4 . 1 0 , 4 . 1 1 ,
p . 98) a n d r e l y s u ccess fu l l y o n s o ft tissu e tec h n i q u e s ,
i. e . mo v i n g t h e b U l t ocks (deep fasc i a e ) i n a c r a n i a l
d i rect i o n , o r susta i n ed s l i g h t p ressu re a t t h e s i te o f
hyperto n u s o f the b u t tocks.
I n n o m i n ate shear dysfu n ction
( G re e n m a n )
Here , w h a t c a n b e c a l l ed a ' r e p o s i t ion m a n o e u v r e '
is always very s u ccessfu l . On t h e s i d e of ' o u t fl a r e '
( s e e p. 99 ) , i . e . w h e r e t h e a n te r i or su p e ri o r i liac sp i n e
( A S I S ) is fl a t t e r a nd m o r e l a t e r a l , t h e t h e r a p i s t
adducls the t h i g h w i t h t h e hip a n d k nee be n t at rig h t
angles ( s e e Fig u re 4. 1 3 ) u n t i l t h e s l a c k i s ta ke n u p .
The pa t ie n t is t h e n told to e xert s l i g h t coun ter­
pressure i n t o a b d u c t i o n for about 10 s a fter w h i c h
re l a x a t i o n i nto adduction ta kes p l a ce : t h is i s repeated
two to t h r e e t i me s . T h i s ca n b e fol l o w e d b y i n ter­
m i t t e n t resisted add uction ( a n tago n ist i n h i b i t i o n ) .
On the o p pos i te s i d e ( , i nfl a re ' ) wh ere t h e AS IS i s
m o re prom i n e n t a n d med i a l , t h e s l a c k i s taken u p
dorsove n t r a l d i rect i o n , aga inst the t i p o f t h e sacrum
Copyrighted Material
( A fter Kubis, 1 970)
1 80
Manipulative Therapy in Rehab ilitation of the Locomotor System
4.41)
aga i n st t h e w a l l , h e r h e a d a g a i n s t h e r a rms . The
a n d a d d u c t i o n r e s i s t e d fo r a b o u t 1 0 s ; r e l a x a t i o n i n to
t h e r a p i s t stands b e h i n d h e r , p u t t i ng t h e heel or j us t
a d d u c t i o n fo l l ow s . T h i s is r e p e a t e d two or t h ree
a fi n ger o f o n e h a nd o n t h e s p i n o u s process o f t h e
in a b d u ct i o n l i k e in P a trick 's test ( s e e Fig u re
t i m e s , and may be fo l lo w e d b y i n te r m i tt e n t a n t a go n ­
c a u d a l v e r t e b r a o f t h e s t i ffest segm e n t , a n d te l l s the
ist i n h ibition.
p a t i e n t to re l a x i n t o e x t e n s i o n so as to take u p the
s l a c k . The p a t i e n t then i s told to press h e r back
gently aga i n s t the hand at the spinous process a n d
T h e c o ccyx
to b r e a t h e i n s l owly. A s l i g h t i n crease i n k y p h os i s
In t he m aj o r i t y of cases o f a t e n d e r coccyx , P I R of
6 . 1 23)
fo l l o ws at this stage . T h e p a t i e n t t h e n is told to h o l d
is v e r y effective,
h e r b re a t h , to s t r a i g h t e n u p aga i n a n d t o b r e a t h e o u t
and c a n be a d m i n i s t e red a s self-tre a t m e n t . I t is o n l y
a s m uch a s s h e ca n . The t h e r a p i s t u s e s j u st h i s fi nge rs
i n e x c e p t i o n a l c a s e s t h a t m a n i p U l a t i o n p e r rectum i s
t o i n d i c a t e t h e point i n to w h ich the p a t i e n t s h o u l d
t h e g l u t e i m a x i m i ( see F i g u r e
necessary; e v e n w h e n c a re fu l l y p e rform e d t h is i s
b r e a t h e o u t , w i th o u t e x e r t i n g a n y press u r e : m a x i ­
u n pl e a s a n t a n d e v e n p a i n fu l . I t i s a v e r y e ffec tive
m u m l o r d o s i s i s a c h i e v e d by t h e s y n k i n e t i c co n trac­
te c h n i q u e , y e t t h e me c h a n i s m i s s t i l l o b s c u r e ; the
tion o f t h e p a t i e n t ' s back m u sc l e s . N o t only i s t h i s
s a crococcyge a l j u n ct i o n i s not a true j o i n t , and t h ere
tech n i q u e v e ry c o m fo r t a b l e fo r t h e p a t i e n t , b u t i t
i s no m o v e m e n t restri c t io n .
l e n ds itse l f r e a d i l y t o sel f-tre a t m e n t , a s soon a s t h e
For m a n i p u l a ti o n t h e p a t i e n t l i e s p r o n e w i t h h e r
h e e l s r o t a t e d o u tw a r d s , o r is o n k n e e s a n d e l bows.
patient
has
r e a l ized
b re a t h e i n to ( F i g u re
w h ich
s e g m e n ts
6.34) . Th i s
she
m us t
te c h n i q u e , w h i c h i s
The t h e r a p i s t i n s e rts his fore fi n ger i n to the rect u m ,
n o t q u i te s p ec i fi c , is p a r t i c u l a rl y s u i te d fo r t r e a t m e n t
fi rs t asce r t a i n i n g w h e t h e r t h e l e v a t o r a n i i s n o t t e n s e
o f s t i ff th oracic k y p h o s e s .
For spe c i fi c e x t e n s i o n m o b i l i z a t i o n i n t h e t h o racic
o n b o t h s i d e s ; i f i t i s , h e m u s t re l a x i t by massage o r
6.35),
P I R o f t h e g l u t e i m a x i m i w h i c h co n t r a c t a n d rel a x
spine (Figure
a t th e s a m e t i m e a s t h e l e v a t o r a n i . Th e n by m o v i n g
h e r h a n d s c l a s p e d be h i n d h e r h e a d ; t h e t h e r a p i s t
t h e coccyx h e fi nd s t h e e x a c t s ite of the sac ro­
s t a n d s i n fro n t o f h e r , h is s h o u l d e r a n d u p p e r a r m
coccyge a l s y n c h r o n d rosis . H e m a y now move the
l e a n i n g a g a i n s t t h e pa t i e n t ' s e l bows, h is fore a r m
the p a t i e n t l i es o n her s i d e w i t h
coccyx in a dorsal d i rect i o n , o r s i m p l y e x e rt p r ess u re
u nder the arm lying on the t a b l e . I f the pat i e n t can
on
b r i n g h e r e l bows toge t h e r i n fro n t of h e r neck , t h e
the
sac rococcygea l
synchrondrosis
with
the
i n s e rted fi n g e r and the t h u m b o n the e n d of t h e
therapist
s a cr u m .
fore fi n g e r of h i s o t h e r h a n d is p l aced on the sp i n o u s
A ft e r two or t h ree
repe t i t i o n s h e
must
d e te r m i n e w h e t h e r t h e coccyx i s s t i l l te n d e r o r n o t .
p roce ss
may
of
the
grasp them
ca u d a l
with
verte b ra
one
of
hand.
the
The
blocked
segme n t . He n o w m o v e s t h e p a t i e n t i n to r e t r o A e x i o n
( a s a t exa mi n a t i o n ) , so a s t o t a k e u p t h e s l a c k . A t
T h e t h o ra c i c s p i n e
t h i s p o i n t h e te lls t h e p a t i e n t t o p ress h e r e l bows
H e re t h e re a re n o p u re traction t ec h n i q u e s s u c h as
we
use
in
the
lumbar
and
cerv ica l
re g i o n s .
A
m a n o e u v re freq u e n t l y practised by l a y m e n p e r h a ps
provides t h e n e a rest t h i n g to t ra ct i o n : t h e p a t i e n t
( s t a n d i n g o r s e a t e d ) crosses h e r a r m s o v e r h e r c h e s t ,
with
her
hands
on
her
s h o u ld e rs
or
fa ce .
The
therapist s tands beh i n d her a n d passes his hands
r o u n d t h e p a t i e n t ' s body to c u p t h e fu rt h e r e l b o w ,
pre s s i n g t h e p a t i e n t ' s t h o racic s p i n e a n d ribs a g a i n s t
his own chest,
to
take
up the
s l ack.
He
then
s t ra i g h t e n s u p i m p a r t i n g a t h r u s t t o the p a t i e n t ' s
e l bo w s , i n a n u p w a r d d i rect i o n , a t t h e s a m e t i m e
pre s s i n g h e r c l os e r to h i s o w n c h e s t . T h i s u n sop h i s t­
i c a t e d a n d n o n -spec i fi c t e c h n i q u e i s q u i te h a r m less
u n less the p a t i e n t s u ffe rs fro m s e v e r e o s t e o p orosi s .
A s s t i f f i n c re a s e d k y p h o s i s i s p r o b a b l y t h e most
freq u e n t
d isorder
in
the
t h o ra cic
regi o n ,
back­
b e n d i n g mob i l iz a t i o n i s pro b a b l y the tech n i q u e most
freq u e n t l y c a l l e d fo r . I n order to m a k e fu l l u s e of
the
pa t i e n t ' s
own
m u sc u l a t u r e
it
is
poss i b l e
to
e m pl o y n o t o n ly PIR b u t a l so t h e a c t i v e c o n t ra c t i o n
of t h e e r ector s p i n a e d u r i n g m a x i m u m e x h a l a ti o n .
For t h e fi rs t te c h n i q u e , t h e p a t i e n t sits fa c i n g a
wa l l ,
leaning
both
k n ees
and
h e r crossed
arms
Figure 6.34 M o b i l i z a t i o n o f the t h o r a c i c s p i n e i n t o
s i t t i ng (ex h a l a t i o n )
extension
Copyrighted Material
Therapeutic tech niq ues
Figure 6.35 Mob i l i z a t i o n of t h e t h o r a c i c s p i n e i n to
e x t e n s i o n w i t h t h e p a t i e n t l y i ng on h e r s i de ( ex h a l a t ion)
s l igh t l y i n to a n t e fl e x i o n ( th e t h era pis t resisti ng) a n d
t o b re a t h e in slow l y . As i n the prece d i n g tech n i q ue ,
a s l i g h t i n crease i n kyphosis i s u n a vo i d a b le a t this
st age . A fter this the p a t i e n t i s told t o relax and
ach i eve max i m u m e x h a l a t io n , especial ly a t the poi n t
w here she fee l s t h e therapist's fi nge r . A s e x h a l a t i o n
reac hes t h e maxi m u m , t h e tho racic s p i n e m o v e s
spo ntaneo us l y i n to retro flex i o n . The p roce d u re i s
re peated a b o u t t h ree t i m es.
Befo re proceed i n g to describe thrusting tech n i q ues
i n t h e tho racic spine I will deal with m o b i l ization
i n to flexion . Flexion restriction i s usually fou n d
where t h e k y p h o t i c a rch of t h e th oracic s p i n e i s
flattened, w h ich i s most freq u e n t l y t h e case i n the
upper thoracic region a n d a lso a t t h e thoraco l u m b a r
j u nction.
A very co n ve n i e n t way o f m o b i l izing i n to fle x i o n
is prov ided by the e x a m i n a t i o n tec h n i que (see
Figure 4 . 2 2 , p . 105 ) . The t herapist thus moves the
pa tient into a n teflex i o n w i t h t h e s u m m i t of the arch
at t h e po i n t whe re his finger is p laced ; h e tells the
pa t i e n t to look u p and breathe in, and t h e n to look
down a n d breathe out. Th i s p roce d ure is repeated
t h ree to five t i m es .
F o r the u pper t horacic spi n e , w h e re restricte d
anteflexion is re l a t ive l y freq u e n t , t h e r e i s another
mobi lization tec h n i q u e t h a t is p a rt i c u l arly effective.
It is applied on the side w h e re m uscu l a r spasm
(TrPs) i n the spinal erectors is fo u n d . The patien t
(Figure 6.36) s i ts on the ta b l.e a n d tbe thera p i s t
s t a n d s behind h e r ; w i t h o n e h a n d h e g r a s p s t h e
p a t i e n t ' s h e a d , h i s pa l m o n the occ i p u t o n the s i d e
of the l e s i o n ( i . e . h e uses t h e l e ft h a n d i f t h e l e s i o n
is on t h e righ t ) . He m o v e s t h e head i nto a n teflex i o n ,
side-be nding a n d rot a t i o n to t h e opposite s i d e t o
take u p t h e slac k . W i t h the t h u m b o f t h e o t h e r h a n d
he fi x e s t h e transve rse p rocess o f the lowe r vertebra
181
of t h e segm e n t to be treated . He then tells the
p a t i e n t t o look towards the side o f the lesion and to
bre a t h e in slowly, then to look in the other d i rection
a n d breathe o u t . This proced u re i s repeated a b o u t
t h re e t i mes.
To restore side-be n d i ng we use the s a m e tech­
n i q u e as for examination (see Figures 4 . 2 3 , 4.24, p .
1 0 6 ) , t h e only d i fference b e i n g t h a t the thu m b i s
placed o n t h e s p i n ous process o f the ca u d a l vertebra
to fi x it, a n d n o t a t the i n terspace for p a l p a t i o n . For
m o b i l ization we m a ke use of the a ltern a t i n g muscle
faci l i tati o n and i n h i b i t i o n described by G a y m a n s
( 1 980) .
The patie n t is s e a ted on the t a b l e , h e r legs h a ng i n g
o v e r the s i d e ; the t h e r a p i s t sta n d s b e h i n d h e r w i t h
o n e h a nd ro u n d her r i b s a n d t h e t h u m b o n the s i d e
o f t h e s p i n o u s p rocess. T h e o t h e r h a n d i s p l aced o n
the p a t i e n t ' s n e c k (fo r t h e u pper thoracic), s h o u l d e r
( fo r t h e m id-thoracic), or u n d e r h e r a x i U a ( for t h e
lower t horacic s pi n e ) , a n d b e n d s the p a t i e nt's t r u n k
s i deways so a s to t a k e u p t h e s l a c k . I f a n e v e n
segm e n t is b e i n g treated, t h e p a t i e n t is told to l o o k
u p a n d b r e a t h e i n , the t h e r a p i s t t h e n feel i n g
i n c reased resistance to t h e s i d e - be n d i n g ; a fter a slow
deep brea t h the patie n t is told to h o ld h e r breath
a n d then t o relax a n d b rea t h e o u t (but n o t to l o o k
down , w h ich would i n volve ben d i n g forward). D u ri n g
t h i s exh a l a t io n t h e therapist m u st w a i t u n t i l he fee l s
resista nce to s l a c ke n ; the r a n ge of s i d e - bend i n g
a u t o m a ti ca l l y i ncreases. I n t h e o d d segm e n ts fa ci l i ­
tation a n d i n h i bi t i o n a re reversed: t h e patie n t i s
t o l d to breathe o u t slowly ( afte r breath ing in) , t h e
t h e r a p i s t feeli n g resistance to side-ben d i ng. Whe n
Figure 6.36 One-sided m o b i l iza tion o f t h e t h oracic s p i n e
i n to k y p h o s i s , t h e p a t i e n t s e a t e d : t h e t r a n sverse process
i s fixed w i t h the t h u m b
Copyrighted Material
1 82
Man ip u lrl live Th erapy in Rehabili/{Ilion of {he
Locorn o{nr S VSICIIl
e x h a l a t i o n is com p l e te s h e i s told to b re a t h e i n
s l ow l y , a n d towa rds t h e e n d o f i n h a l a tion resi s t a n ce
to side-be n d i n g s l a c k e n s a n d the r a n ge of m o v e m e n t
i ncreases. Th is p roce d u re is r e p e a t e d two o r t h r e e
ti mes.
I n very b r o a d s h o u l d e red p a t i e n ts, w h e n a
t h e r a p i s t w i t h sma l l h a nds h a s d i ffic u l t y i n reach i n g
t h e s p i n o u s process w i t h h i s t h u m b , w e d e sc r i bed
( C h a p t e r 4 , Figure 4.24 ) a s u i t a b l e tec h n i q u e : t h e
t he r a p i s t s t a n d s a t t h e s i d e o f the p a ti e n t u s i n g h e r
f a r (raised ) e l bow fo r s i d e - be n d i n g; the t h e nar a n d
t h u m b o f h i s o t h e r h a nd form a fulcru m . D u ri n g
m o b i l i z a t i o n h e h a s to stabilize t h e p a t i e n t ' s t horax
with his own t ru n k , lea n i n g back and b e n d i n g h i s
knees.
Th ere a re s e v e r a l i m porta n t tec h n ica l poi n ts to
n o t e : the t h e ra p i s t m u s t never fo rce sid e - b e n d i n g
b u t w a i t for it to i ncrease s po n t a n e o u s l y , a n d on l y
fol l ow the p a t i e n t ' s re l a x a t i o n w i t h h i s h a n d s . Th i s
u s u a l l y occu rs towards the e n d o f brea t h i n g in or
o u t . The e ffect of t h i s phenome n o n d e c re ases i n a
ca u d a l d i rect i o n , particu l a r l y i n t h ose seg m e n ts
w here resi s t a nce i ncreases d u r i n g ex h a la t i o n , to be
foH owed b y rel a x a t i o n d u r i n g i n h a l a ti o n . Th is is
prob a b l y because the s t a bi l i ty of the t h o r a x as a
w hole i n c reases d u r i n g i n ha l a t i o n . T h e o t h e r p o i n t
t o w a t c h , a s I p o i n te d o u t w h e n describing e x a m i n a ­
t i o n tech n i q u e is t h a t t h e h a n d which s t a b i l izes t h e
t h o r a x f r o m t h e s i d e m u s t c re a te a s t r o n g f u l c r u m ,
the p a l m l y i n g i n the a x i l l a ry l i n e a n d t h e t h er a p i s t ' s
fo re a r m b e i n g perpe n d i c u l a r t o t h e lateral chest
w a l l . E v e n i f t h e patient is broad s h o u l d e re d a n d tbe
t he ra p i s t h a s small hands, h i s t h u m b s t i l l reaches
t h e spinous p rocess d u ring si d e - b e n d i ng , owing to
rota t i o n of the ver t e b r a e . T n e v e ry d a y practice t h e
therapist ra re ly co u n ts to see w h e t he r he is dea l in g
w i t h a n odd o r a n e v e n segm e n t , b u t si m p ly starts
by t e l l i n g t h e pati e n t to look u p a n d brea t h e in; if
resista n ce i ncreases d u ri n g i n h a l a t i o n and re l a x a t i o n
fo l lows d u ri n g e x h a l a t i o n , h e i s s a t i s fi e d . I f n o t , h e
t ries the reverse proced u re , begi n n i n g w i t h e x h a l a ­
t i o n . T h i s tec h n i q u e is a lso v ery usefu l fo r mo b i l iza­
tion of the r i b , but not to d e l i v e r a t h rust .
For m o b i l i z a t i o n i n rota t io n t h e patient s h o u l d s i t
a s t r i d e t h e e n d o f t h e t a b l e w h i l e t h e t h e ra p i s t sta nds
b e h i n d h e r a t t h e end, pass i n g o n e a r m under t h e
p a t i e n t ' s a x i l l a t o g rasp t h e o pposite s h o u l d e r ( Figure
6 . 37). A s l i g h t l y ky p h otic pos i t i o n is reco m m e n d e d ,
t o m a ke t h e spi n o u s p rocesses more prom i ne n t . The
o t h e r h a n d is placed w i t h the palm a ga i n s t the ribs
and the t h u m b o n t h e spi n o u s process of the c a u d a l
vertebra o f t h e t re a te d segm e n t , from t h e s i d e . To
a c h i e v e good fi x a t i o n t h e t h e rapist's a rm is abd ucted
so that the fo r e a r m fol l ows t h e d i re c t i o n o f the
t h u m b , a n d the p a l m s t a b i l izes t h e ribs. rt fixation i s
a d e q u a te little l o c k i n g i s n e e d e d . T h e p a t i e n t i s now
to l d to l oo k toward the s i d e to w h ic h m ob i l ization
i s being ca rried o u t ta k i n g u p t h e s l a c k i n t h is way.
The pa t i e n t is t h e n t o l d to l o o k t o the o pp os i te side ,
,
,
brea t h i n g i n slowly , to h o l d h e r b reath ( t h e i s omet r i c
p hase ) , a n d t h e n t o look t h e o t h e r way aga i n ,
b re a t h i n g o u t s l o w l y . D u r i ng t h i s re l a xa t i o n p h a s e
the range of mobi l i ty i n creases s p o n t a n e o u s l y . T h e
proce d u re is re p e a ted t w o o r t h ree t i m es .
Th e fo l l o w i n g tec h n ic a l po i n t s a re i mporta n t :
fixa tion s h o u l d h e s u c h t h a t t h e t h u m b a t t h e s i d e
o f t h e spi n o u s p rocess of t h e caucl a l v e rt e b r a
rema i ns in p l a c e . W h e n t h e pa t i e n t l o o k s t o wa rds
the s i d e of mohi l izati o n , t h e re fo r e , her eyes a n d
h e a d s h o u l d n a t u r a l l y t u r n as fa r a s t he c l asped
h a n d s b e h i n d h e r head a l low, i n t h e d i re c t i o n of
rot a t i o n ; the t ru n k , however, s h o u l d o n l y re l a x , a n d
not active ly press. T h e t r u n k m u s t a l way s ro t a t e
a b o u t i t s ow n a x i s .
The sa m e t e ch n i q u e ca n a lso b e u s e d t o d e liver a
t h ru s t , a fter t h e slack has b e e n t a k e n u p , i . e . at t h e
e n d o f t h e re l a x a t i o n p h a s e , if i t is thought a d v isa h l e .
I n t h i s c a s e t h e t h e r a p i s t m a y i n cr e a s e k y p h osis a n d
s l ightJ y sid e - b e nd t h e t r u n k i n t h e d i r e ct i o n oppos t te
to t h a t o f rota t i o n , to o b ta i n be t l e r l o c k i n g I r t h e
fi x a t i o n is good a n d t h e pa t i e n t re l a x e d , t h i s is n o t
absol u tely necessa ry.
Th i s tech n i q u e is u s e d m a i n l y i n the low t h o r a c i c
spine and t h e t h o r ac o l u m ba r regi o n , b u t i t c a n a lso
be a p pl ie d t o the l u m h a r s p i n e .
T h e re is a no t h e r v e r y e f fective a n d l e ss s p eci fi c
t e c h n i q u e fo r mo b i l iz a t i o n a s we l l as to d e l i v e r a
t h r u s t fo r m a n i p u l a t i o n of t he t h o r a c i c s p i n e i n t o
rotation ( Fi g u re 6 . 3 8 ) ; the t h e ra p i s t 's h a n d on t h e
pa t i e n t ' s s h o u l d e r ro t a t i n g her, a n d t h e t h u m b or t h e
pisi form of t h e o t h e r h a n d on t h e t r a n s v e rse p roces s ,
a c t i n g i n t h e s a m e d i rec t i o n . C a r e fu l l o c k i ng i s
esse n t i a l . T h e pa t i e n t is seated a s fo r t h e p re c e d i ng
tec h n i q u e a n d the t h e r a pis t grasps t h e fa r s h o u l d e r,
w i t h his arm across the p a t i e n t ' s chest , r r o m b e h i n d .
.
Figure 6.37 Ro t � t i o n m o b i l i za t i o n ( m a n i p U l a t i o n ) i n
k y p h o s i s , wi t h t h e l owe r ve r t ebra o f t h e t e s t e d
segm e n t Il xed b y t h e t h e r il p i s t ' s h a nd a n d t h u m b
slight
Copyrighted Material
Therapeutic rechniques
( b)
Figure 6.38 (II)
R o t a t i o n m a n i p u l a t i o n of t h e t h o ra c i c
scakd with her trunk l e a n ing s l ig h t l y
b a c k w a rds, ro t a t e d a n d b e n t t o t h e s a m e s i d e , b o t h the
t h e r a p i s t ' s h a nd s a c t i n g in t h a t d i re c t i o n . W i t h t h e
pa t i e n t s i t t i ng e r e c t , t h e s a m e rot a t i o n tech n i q u e c a n b e
u sed t o ma n i p u l a t e a r i b , c o n t a c t b e i n g m a d e a t t h e
a n g l e o f t h e r i h i n s t e ad o f a t t h e t ra n sverse p rocess.
spine, t he patient
'1 83
g i v i n g a p u s h to the tra nsvers e process in the s a m e
d i rect i o n .
The fo l l ow i n g tec h n i c a l p o i n ts a r e i m porta n t : t h e
a x i s o f rota t i o n is t h e p a t i e n t ' s t ru n k , a n cl h e r h e a d
m ust not d e v i a te from side t o s i d e . O n l y a l i tt l e s i d e ­
be n d i n g is needed a n d i s performed by m e a n s of t h e
h a n d across t h e p a t i e n t 's c h es t , n o t by the therapist
bending his own t ru n k s i deways. T h e thrust is d e l iv­
e red by the t h e ra p ist rota t i n g his own body from t h e
l e g s a n d p e l v i s , so that b o t h h i s h a n d s a c t exactly a t
t h e s a m e m o m e n t . A s t h e re i s n o fixa t i o n from
be low, o n l y very l i ttle force m u st be use d . I nstead
o f h i s thumb, t h e thera p i s t m a y use h i s the n a r or
pisifo r m . Mobi l izat i o n a l o n e is, howeve r , u s u a l l y
s u f fi c i e n t , as m uscu l a r spasm a n d he nce a lso m u sc u ­
l a r relaxation a re d e c i s i v e a t t h e t h o raco l u m ba r
j u n cti o n .
A tec h n icaJJy s i mp l e b u t not v e ry spec i fi c tech ­
n i q u e fo r mob i l izing the thoraco l u m b a r j u nc t i o n
h a s been s uggested by F. G a y m a n s ( u n p u b l i shed
observ a tion s ) , m a k i ng use of t h e r h y t h m ic a l pull o f
the psoas ( Figure 6 . 3 9 ) . The patie n t l i e s o n h e r s i d e ,
w i t h t h e uppe r h i p be n t a t right angles. The t h e r a p i s t
s ta nds a t t h e side of the tab l e so a s to res i s t further
fl e x i o n o f the p a t i e n t ' s k n e e w i t h his o w n t h i g h . He
now te l l s the p a t i e n t to l o o k as fa r to t h e opposite
side a s she can, p ro d u c i n g ro tation of t h e head a n d
trun k ; a t t h e s a m e t i m e t h e p a t i e n t pushes h e r b e n t
k n ee aga i n st the t h e r a p i s t ' s t h i g h . A l te rn a t i v e l y ,
t h e therapist may tel l t h e p a t i e n t to res i s t w i t h h e r
k nee w h i l e h e h i mse l f r h y t h m ically p u s h e s i t i n to
e x te ns i o n . M o b i l i z a t i o n is obta i n e d by t h e t ru n k
rota t io n a n d t h e r h y t h m ical p u l l o f t h e psoas m u scle
a t the u p p e r tra n sve rse p rocesses o f t h e t h o raco l u m ­
b a r j unction i n a n opposite d i rect i o n , T h e techn i q ue
s h o u l d be performed at a b o u t two pushes per
seco n d . T h i s tech n i q u e i s ideal for s e l f- t re a t m e n t ,
t he p a t i e n t resisti n g rhy t h m i c a l k n e e fl e x i o n w i th h e r
o u ts t retched a rm .
(b) D e t a i l o f ( a )
T h r u st tec h n i q ues
He n o w ob t a i ns l o c k i n g by side-be n d i n g a n d rota­
tion to the same s i d e , so that the a rch so fo rmed
c u l m i nates a t the sit e o f the segm e n t to be trea ted .
Rota t i o n o r I h e t r u n k m ust be carried o ut a b o u t the
v e r t i c a l a x i s of t h e t r u n k , t he head rem a i n i n g fixed .
This is a c h ieved by t h e t herapist bend i ng the patien t
s i d eways, u s i n g h i s e l bow on the p a t i e n t ' s c h e s t a n d
h i s h a nd o n the shou l d e r; h e m u s t s t a n d be h i n d the
pa tient w i t h h i s l e gs we l l apart so t h at h e h i mse l f
c a n ro t a t e a ro u n d t h e p a t i e n t . A fter ta k i n g u p t b e
slack h e has two options: f o r m ob i l ization he te l l s
the p a t i e n t t o loo k i n t h e opposite d i rection and
s lowly to brea t h e in, hold h e r brea t h a n d then t o
look i n the d i rection o f m ob i l iz a t i o n a s fa r as s h e
ca n a n d brea t h e ou t . This i s re peated two o r th ree
times. Or he d e l i ve rs a t h rust by fu r t h e r i ncreas i n g
rota t i o n a t t h e p a ti e n t s s h o u l d e r , s i m u l ta n e o usly
'
First a very ge n tle yet very e ffective traction tec h ­
n i q u e : the t h e r a p i s t s t a n d s beh i n d the sea ted p a t i e n t
w i t h a c u s h i o n between h i s chest a n d the p a t ie n t 's
b a c k , so t h a t t h e top edge o f t h e c u s h i o n fixes the
s p i n o u s process o f the lower vertebra of the segm e n t
to be treated. H e n o w t h re a d s one a rm t h ro u g h t h e
patie n t 's a x i l l a a n d w i th t h e fore arm a n d p a l m
sta b i l izes the patie n t 's h e a d a n d n e c k o n o n e s i d e ,
T h e o t h e r ha n d reaches across t h e p a t i e n t's c h e s t to
grasp h e r fa r h a n d . He now p u l l s that ha n d through
the other axi l la , a t the level of the upper edge of the
cushion. B y p u l ling i n a d o rsa l d i rection o n t h e h a n d
i n the a x i l l a a nd on his o w n a r m i n t h e p a t i e n t ' s
a x i ll a , th e s l a ck i s ta k e n u p; t h e t h rust fol lows a s t h e
therapist straightens h i s c h e s t , t h u s p u s h i n g t h e
c u s h i o n fo rwa rd a n d a t the s a m e ti m e s l i g h tly l i fti ng
the p a t i e n t w i t h his chest and a r m s (Figu re 6040).
Copyrighted Material
] 84
Man ipu/IJlive Th erapy in
Rehabilitation of the
Locom otor System
Figure 6.39 R o t a t i o n m o b i l i z a t i o n o f the t h o r a co l u m b a r j u n c t i o n witiJ the p 8 t i e n t on h e r s i d e . l oo k i ng t o the o p p o s i t e
side d u r i n g r h y t h m i c a l i s o m e t r i c c o n t r a c t i o n o f t h e r i g h t i l i o p s o a s
T h e fo l l o w i n g tech n i q ue i s v e r y wi d e ly used . The
t h e s p i n o u s p r o c e s s l y i n g i n t h e groove b e t w e e n t h e
p a t i e n t i s s u p i n e her h a n ds clasped b e h i n d h e r neck
b e n t m i d d le fi n ge r a n d t he t h e n a r e m i n e n c e . A ft e r
and
this
,
b o th
( F i g u res
e lbows
t o u c h i n g in fro n t o f the
chin
6 . 4 1 and 6 . 4 2 ) . The t h e rapist stands by t h e
th e t h e ra p i s t t ur ns t h e p a t i e n t
on
t o h e r b a c k so
t h a t she i s l y i n g o n the h a n d m a k i n g c o n t a c t a t t h e
s i d e o f t h e t a b l e a n d grasps b o t h e l bows w i th t h e
tra n s verse
hand
e lbows t h e t h e r a p i s t n o w b r i ngs t h e t h o ra c ic s p i n e
n e a re r
t o t h e p a t i e n t s h e a d . t u r n i n g the
'
w i t h t h e h a n d gras p i n g t h e
p rocesses:
c u l m i n a te s e xa c t l y a t t h e s i te
n o w two a l t e rn a t i v e s :
p a t i e n t� t o w a r d s h i m . He b e n d s t h e m i d d l e fi n g e r of
in t o k y p h o s i s , w h i c h
t h e ot h e r h a n d so t h a t the fi n ge r t i p touches the p a l m ,
of t h e c o n t a c t h a n d . He h a s
a n d a pp l ie s t h e m i d d l e p h a l a n x o f
t h e b e n t fi n g e r t o
( 1 ) h e m a y fu r t h e r i n crease flex i o n s o a s to ta k e u p
t h e t r a n s v e rse process o f t h e c a u d a l vertebra o f t h e
the s l a c k . t e l l i n g t h e p a t i e n t t o b re a t h e i n a n d o u t
bloc k e d s e gm e n t o n t h e n e a r s i d e , a n d t h e t h e n a r
(this can be
e m ine n c e t o th e t r a n s v e rs e process o f t h e fa r s i d e ,
a n d d e l i v e r t h e t h r u s t i n t o fl e x io n d u r i n g exha l a t i o n :
o r ( 2 ) he
repeated as
a
p re p a ra tory m o b i l i z a t i o n ) ,
b e n d t h e t h ora x b a c k ( o r l e t
fulcrum fo rmed b y t h e h a n d
p a t i e n t ' s b a c k ( b u t n e v e r s o f a r as t o l e t
may
slightly
i t fa l l b a c k ) o v e r t h e
u nd e r the
Figure 6.40 Trac t i o n thrust t e c h n i q u e a p p l i e d t o t h e
t ho r a c i c s p i n e , u s i ng a c u s h i o n , t h e p a t i e n t seated
Figure 6.41 P o s i t i o n o f t h e t h e r a p i s t ' s h a n d s d u r i n g
m a n i p u l a tion o f the thoracic s p i n e w i t h the pa t i e n t
s u p i ne
Copyrighted Material
Therapeutic techniq ues
Figure 6.42 M a n i p u l a tion of t h e t h or a c i c s p i n e w i t h the
1 85
Figure 6.43 M a n i p u l a t i o n w i t h crossed hands m a k i n g
patient supi ne
t h e o p p o s i t e tra nsverse p roce sses of t w o
vertebrae, w i t h t h e p a t ie n t pro n e
contact on
a dj a ce n t
the shou lder-blades touch t he t a bl e l ) i n order to
ta ke u p the s l ac k , asking t h e p a ti e n t to breathe i n
a n d out s l ow ly ( t h is m a y b e re p e a te d ) a n d t h e n
deliver t h e thrust i n the same d i rect i o n , d u r i n g
ex h a l a t i on .
I t may be d i ffic u l t for t h e p a t i e n t t o bring h e r
elbows toge ther, i n w h i c h case i nstead o f c l a s p i ng
her h a n d s s h e should hold them w i th t h e finge rtips
j u st touching. A n o t h e r possib l e d iffic u l ty i s t h a t
some t h e rapists beg i n to fee l pain i n t h e m i d d l e
fi n g e r ; they s h o u l d use the c u s h i o n tech n i q u e ( s e e
Figure 6.40) , o r try a p iece o f I n d i a r u b b e r i n t h e
croo k o f the m iddle fi n ger.
Because of t h e i r s i m p l i c i t y a n d p o p u l a rity, d i rect
t h rust tech niq ues a pplied to the thoracic s p i n e , with
the pati e n t prone. m u s t be descri bed . N o sop h i s ti­
cated loc k ing tec h n iq u e is i nvolved, and t h e re is no
question of d istinguis h i ng fle xion and exte n s i o n . The
thrust m ust be d i rected a t the caudal vertebra i n t h e
blocked segm e n t , prod ucing ( l i k e a l l poste roanterior
thrusts) gapping o r d istraction o f t h e i n tervertebral
a pophysea l j o i n ts , which a re a l most i n the coro n a l
plane i n the thoracic spi n e . The springing tech nique
described for exa m i n a t i o n , with the patient s u p i n e
(see Figure 4 . 1 5 , p . 1 0 3 ) can be u s e d after t a k i n g u p
the s lack.
Another tec h n i que can be used b o t h fo r mobi l iza­
tion a n d for a h i g h -ve locity t h rust, p rod ucing some
rota tion as we l l . The patient l ies prone, and the
therapist by the side of t h e table crosses h i s hands,
pl a c i n g the p i s i form of one hand on the transverse
process of o ne verte b r a and t h a t o f the o t h e r h a n d
0 0 t h e transverse process of the adjace n t ve rtebra
(Figure 6.43). He takes up the slack by s l ight d i rect
press u re and w h i l e the p a ti e n t b re a t h e s o u t he m a y
deliver a th rust to prod uce ga p p i n g of t h e a rticu­
lation o n the side of the h a n d movi n g the caudal
vertebra o f the b l oc ked segm e n t , i n this w a y
,
res t o r i n g r o t a t i o n to t h a t side . I nstead of delive ring
a h igh-ve l oc i t y t h rust, he m a y s i m p l y ge n t ly increase
his press u r e , springing the j o i n t w h i l e the p a t i e n t
bre a t h e s o u t . T h i s type o f m o b i l iza tion c a n b e
c a r r i e d o ut a s a n o n -specific treatment, i n the rhythm
of resp i r a t i o n , i n one segm e n t after t h e other, rathe r
l i k e massage.
All t h e tec h n i q ues described fo r the t h o racic s p i n e
a re applicable f r o m T 3 dow n ; t h e cervico t horacic
j u n ction req u i re s tec h n iques that are d escri bed i n
the s e c t i o n o n t h e ce rvica l s p i n e . Rotation tec h­
n iques are t h e methods o f choice i n the thoraco l u m ­
b a r reg ion.
T h e ribs
The tec h n i q u e I mysel f u s e most frequ e n tl y , particu­
l a r l y for t h e upper ribs, is a modi fication of the
d iagnostic technique o f Kubis t h rough the shoulder­
b l a d e (see Figure 4.26, p. 1 07 ) . It is a lso used by
Mitche l l el at. ( 1 979) with the patie n t s u p i n e . As
presented h e r e , it closely resembles the m o b i lization
tec h n i q u e o f t h e thoracic spine i n to extension
( Figu re 6.44 ) . The patie n t lies o n h e r s i d e , the u p p e r
arm r a i s e d o v e r h e r h e a d , w i th t h e e lbow b e n t. The
therapist s t a n d i n g a t t he side of t h e table p u ts o n e
pal m a g a i n s t t h e p a t i e n t ' s e l bow a n d t h e fi n g e rs o f
t h e o t h e r h a n d o n the r i b to be treate d . B y push i n g
t h e e l bow b a c k , u s i n g t h e h a n d fixing t h e r i b a s a
fu lcrum, he takes up t h e slack i n to retroflexion . A t
t h i s point t h e p a t i e n t is told t o press aga i nst t h e
therapist's h a n d s l i g h t l y , slowly breathing i n . S h e i s
t h e n told to ' l e t g o ' a n d breathe o u t fo r as l o n g a s
possible, d i recting h e r b r e a t h to t h e ri b i n q uesti o n .
W h e n maxi m u m e x h a l a t i o n i s reache d , r e t roflexi on
Copyrighted Material
J 86
Manipulative Therapy
in Rehabilita/iOtl
of the Locomotor System
I f we fi n d , on co m p a r i n g t h e t w o sides, t h a t o n e
is restricted d u ring ex h a l a t i o n , t h e fo llowing
t ec h n i q u e ( G ree n m a n , 1979) is usefu l : the p a t i e n t
l i e s s u p i n e , w h i l e t h e t h e ra p i s t s t a nd i ng a t t h e side
of t h e table p l aces his t h u m b on o n e o f t h e u p p e r
r i b s fro m a b o v e , c l ose to t h e stern u m . The patie n t
i s t o l d to b re a t h e i n a n d o u t ; d u ri ng m a x i m u m
e x h a l a t i o n t h e t h e ra pist l i fts t h e p a t i e n t 's tru n k i nto
s l i g h t a n te fl e x i o n a n d gives a l i ttle push on th e rib
from a bove , with his t h u m b . For t reatme n t of a
l owe r r i b the t h e r a p i s t ' s t h u m b m u s t l i e m o re
l a t e ra l ly on the a rch of t h e r i b , a n d d ur i n g e x h a l a t i o n
t h e p a t i e n t's t r u n k i s n o t o n l y l i fted i n to a n teflexion
but is a l so b e n t to t h e side o f t he ri b be i n g trea t e d .
I f i n h a l a t i o n is restricted , Gree n m a n ( 1 979) m a kes
use o f m uscle p u l l . I n the regi on o f t he two Li pper
ribs h e uses t h e p u l l of the sca l e n es, fo r the m i d d l e
r i bs t h e pectora l i s a n d fo r t h e lower ribs the se rra t u s
l a t e r a l i s . The pa t i e n t i s s u p i n e a n d m usc l e p u l l i s
o b t a i n e d by res i s te d side-be n d i n g o f the p a t i e n t ' s
h e a d ( sca l e n e s ) , b y res isted a d d uction o f the a r m
( pectora l i s ) a n d by ra ising t h e a r m a g a i nst resistance
(serra t u s ) . The the r a p i s t ' s other a rm reaches across
the p a t ie n t 's n eck o r chest w i t h the fi n ge rs c x e r t i n g
a m o b i l izing force aga i n s t t h e l a t e r a l a rch o f t h e
b l ocked rib from be l ow, or fi x i n g t h e a d j a c e n t l ower
rib from a bove d u r i ng i n ha l a t io n . Fo r t h i s the
t h e ra p i s t bends t h e pa t i e n t's neck or further arm
towa rds h i m se lf. p rod u c i n g s i d e - be n d i ng o f the neck
and thorax towards h i ms e l f. I f severa l ribs a re
restricted i t is i m porta n t to t r e a t the 'key' rib; t h i s
i s t h e u p permost o f t h e gro u p if i n h a la t i o n i s
restricted, a nd t h e lowest i f e x h a l a t i o n is a ffecte d .
T h e re a re t h ree w a y s o f a p p l y i ng a h i gh-velocity
thrust. Tn t h e fi rst, t h e p a t i e n t is s u p i n e w i t h h e r arms
c rossed o v e r her chest and hands o n h e r s h o u l d e rs ,
t h e a r m o n the s i d e o f t h e r i b t o b e treated l y i ng
u p permost . The t h e ra p i s t sta n d s a t the op posi te side
o f the ta b l e a nd grasps t h e fa r s h o u l d e r or upper
a rm so a s to t u rn the pati e n t 's s h o u l d e r towa rds
h i mse l f. He now a p p l i es the t h e n a r e m i n e n ce t o t h e
a n gle o f t h e b l oc k e d r i b ( Figu re 6.45 ) . T o d o t h is
e ffectively he m u s t h a v e h i s t h u m b i n op posi t i o n , fo r
o n l y then is the t h e n a r e m i nence con t racted a n d fi rm
(Figu re 6.46) . W i t h h is free h a n d t h e t h e r a pist now
grasps the upper a rm l y i n g benea t h the one h e u s e d
to t u rn t he p a t i e n t t o w a rds h i m s e l f and t u rns her
a w a y o n to t h e thenar e m i n e nce o f t h e contact h a n d ,
so t h a t the a ng le of t h e r i b fo rms t h e m ost p rom i n e n t
poi n t o f t h e b a c k . H a v i n g s t a b i l ized t h e p a t i e n t i n
t h i s pos i t i o n , t h e s l a c k i s t a k e n Li p by t h e p a t i e n t ' s
o w n weight, a n d s h e is t o l d to b re a t h e i n a n d o u t .
D u ri ng e x h a l a ti o n t h e th rust is d e l ivered through t h e
u p p e r a r m , v e rt ica l l y towards t hc t h c I"<l p i s t 's t h e n a r
e m i n ence l y i n g be n e a t h ( Figu re 6.47).
The fo l lo w i n g tec h n i c a l d e t a i ls a re i m port a n t :
when h e t u rns t h e p a t i e n t a w a y fro m h i m se l f t h e
t h e r a p i s t m u s t t u rn h e r o v e r t h e m i d-line, i . e . over
the s p i n a l co l u m n , and a t t h e s a m e t i m e keep t h e
ri b
Figure 6.44 R i b m o b i l i z a t i on i n to dorsili A e x i o n d u ri n g
t h e pa t i e n t o n h e r s i d e
exhalation,
i n c re ases spontaneo usly, t h e t h e r a p i s t o n l y mon i tor­
ing the re l e ase . Th i s p roc e d u r e i s re p e a te d a b o u t
t h ree t i m e s .
A ga i n , a s i n d i agnosis, t h e s h o u lder-b l a d e i s n o
o bstacle to t h e fixation o f t h e r i b d u ri n g re t ro fl e x i o n .
T h e fi r s t r i b , however, c a n b e nei t h e r treated n o r
d i a gnosed i n t h i s w a y , w h i le t he second r i b i s t h e
m o s t d i ffi c u l t . The ri bs to w h i c h th i s technique i s
m ost fre q u e n t l y a p p l i e d a re t h e t h i r d , fo u r t h a nd
fi ft h . It is tech n i ca l l y i mporta n t to raise the u p p e r
a r m vertic a l l y to obta i n a p u re m o ve m e n t o f
re troflex ion a s , i f t h i s i s n o t t h e case, one e a s i l y
o bt a i n s rot a t i o n , w h ich i s h i g h l y u n de s i r a b l e , M a x i ­
m u m e l e v a tion o f t h e s ho u l d e r i s th e re fore necess­
ary; i f t h e re is pain in t h e shou l d e r this may prove
t o be an obstac l e , and t h e re fore I fre que n t l y begi n
w i t h t re a t m e n t of t h e sho u l d e r i tse l f ( a necess i ty i n
a n y case i f t h ere is a s h o u ld e r l es i o n ) before go i n g
on to tre a t t h e r i bs ,
Some ge n t l e m o b i l iz a t i o n m a y b e obta i n ed w h i l e
e xa m i n i ng t h e ' ov e r t a ke p h e n o m e n o n ' (see p . 1 07 )
( w h ic h i s fre q u e n tly fou n d a t t h e second to fifth
ribs). The t h e r a p i s t has both t h u mbs on the re l e v a n t
r i b o n e i t h e r sid e , a b o u t 5 c m l a te r a l t o the stern u m ,
resisting r i b m o v e m e n t from a bove, w i t h very l i t t l e
force , d u ri n g i n h a l a t i o n ; h e exe rts s l i g h t p ress ure
from above d uring exh a l a tion ( m a i n l y on the s i d e
t h a t i s ' overta k e n ' , i . e . restricte d ) . As a r u le t h e
overtake p h e n om e n a disappear i m m e d ia te ly .
T h e tech n i que described f o r m o b i l i z a t i o n o f t h e
s h o u l d er- b l a d e ( s e e Figure 6. 1 4 , p. 1 68 ) c a n a l so b e
u s e d for the r i b s . T h e t h e r a p i s t l i ft s t h e shou l d e r w i t h
t h e h a n d t h a t h a s grasped i t from below, w h i l e t h e
oth e r h a n d o n t h e s h o u l d e r- b l a d e exerts s o m e pres­
s u re o n the sca p u l a fro m above, u s i n g the m e d i a l
e d g e o f t h e sca p u l a a s a fulcru m . B y m o v i n g t h e
sca p u l a u p a n d dow n , i n creasing p ressu re t o t h e ribs
d u r i ng e x h a l a t i o n , m o b i l iz a t i o n c a n be a c h i e ve d . I f
corre c t l y a p p l i e d , pa t i e n ts l i ke t h is tech n iq u e .
Copyrighted Material
Therapelilic lechn ill " l!s
Fi g ure 6.45
1 117
M a n i p u l a t i o n of t h e r i b s w i t h t h e p a t i e n t
s u p i ne , p re p a ra t o ry p h a se : t h e t h e r a p i s t t u rn s t h e p a t i e n t
towards h i m s e l f'
Figure 6.47 D e l i ve r i n g t h e t h r u s t t h ro u g h the p a t i e n t 's
u p p e r a r m vertica l l y t o w a rd s t h e t h e ra p i s t ' s t h e n m ( s e e
F i g u re 6 . 4 6 ) i n co n t a c t w i t h t h e a n gle o f t h e r i b
therapist's
trunk and
shou lders,
v e r t i ca l l y
from
a bov e .
Fo r t h e l o w e r r i b s a
oppos i t i o n o f t h e t h u m b l )
d i ffe re n t t h rust is fre q u e n t l y
effective, u s i n g a tech n i q ue close l y simil a r t o
m a n i p u l a t i on i n ro ta t i o n res triction of t h e t horacic
s p i n e (see Fig u re 6.38) . F o r this the pat i e n t s i t s
a s t r i d e t h e e n d of the ta b l e , w h i l e t h e t h e ra p ist
s ta n d s behind h e r , his fe e t w e l l apart, a n d p a s s e s his
a rm under t h e a x i l l a of t h e oppos ite side, t o g r a s p
t h e s h o u l d e r o n the side o f the rib to be tre a te d . T h e
th u m b o f t h e othe r h a n d i s o n t h e a n g l e o f t h e r i b,
w i t h t h e fo r e fi n g e r e ncircl i ng i t . B y rota t i ng the
patient round her body a x i s t h e s l ac k is taken u p
a n d t h e t h rust fo l l ows b y the t h e r a p i s t s i m u l t a n ­
e o u s l y i nc r e a s i n g rota t i o n a t t h e s h o u l d e r w h i l e t h e
u p p e r t h oracic s p i n e i n fl e x i o n . A t t h a t p o i n t the
contact h a n d must be in m a x i m u m s u p i n a t i o n so as
not to make c o n t a c t betwe e n t h e r i b a n d t h e b o n y
base o f t h e fi r s t p h a l a n x of the t h u m b , i n stead of the
m u s c u l ar thenar e m i nence .
A s i m i la r b u t· h a rd e r t h r u s t i n g tech n i q u e i s
p e r fo r m e d w i t h t h e p at i e n t p ro n e , h e r h e a d tu rned
to the side of the r i b t o be t re a ted ( F i g u re 6.48) . I f
t h i s is a n u p p e r rib, t h e p a t i e n t ' s a r m h a n gs down
over t h e edge of t h e t a b l e i n order to produce
abduct i o n of t h e s h o u l d e r - b l a d e ; o t h e r w i s e i t m a y
l i e p a r a l l e l t o t h e pa t ie n t 's t ru n k . The t h e rapist
sta nds a t t h e side o f t h e rib t o b e treated a n d a p p l ies
the p i s i fo r m o f one hand to t h e a n g l e o f t h e r i b . He
m a y now r e i n fo rce this h a n d by grasp i ng i t j u s t
a b o v e t h e w r i s t w i t h h i s o t h e r h a n d . The s l a c k i s the n
t a k e n up by press ure o f both a rm s a n d t h e t h rust is
d e l i v e r e d d u r i n g e x h a l a t i o n . I t co m e s from the
Figure 6.48 T h r u s t ma n i p u l a t i o n a t t h e
w i th t h e p a t i e n t p ro n e
m o re
Figure
6.46
Pos i t i o n o f t h e t h e r a p ist's h a n d s d u r i n g
r i b w i t h t h e pa l i e n t s u p i n e ( fu l l
m a n i p U l a t i o n of a
Copyrighted Material
a n gl e
of a rib,
1 88
Manip ulcll i ve Therapy in Rehab ililation
of the Locomotor System
c o n t a c t h a n d on t h e r i b d e l i v e rs a p u s h or a p u l l i n
a n d m o b i l i za t i o n . T h e t h e r a p i st s t a n d s b e h i n d t h e
t h e s a me d i recti o n .
se a te d p a t i e n t , s u p p o r ti n g h e r b a c k a g a i n s t h i s own
Tre a t m e n t o f t h e fi r s t r i b : a s i n d i a g n o s i s , t h e
c h e s t w h i l e o n e band su p p o rts t h e b e a d ; t b e fi rst
t r e a t m e n t o f t h i s r i b d i ffers fro m t h a t o f a l l t h e
p b a l a nx o f h i s o t h e r fo re fi n ge r is p l a ce d on t h e first
o t h e rs . F o r m o b i l i z a t i o n I u s e
a
tech n i q u e t h a t i s a s
s i m p l e a s i t i s effec t i v e : t h e t h e r a p is t s t a n d s b e h i n d
rib from a b ove ; with s l i gh t pressu re d o w n w a rd s he
t a k e s up the s l a c k . Q u i c k rep eti tive s p r i n gi ng ( s h a k­
t h e p a t i e n t sea ted o n t h e t a bl e , a n d s t a b i l izes t h e
i n g) ca n n o w be a pp l i e d , or
n e c k o r s h o u l d e r fro m t h e s i d e . H e p l aces h i s o t h e r
s a m e d i re c t i o n d u ri n g e x h a l a t i o n
a
t h rust de l i v e re d i n t h e
( Fi u re 6 . 5 0 ) .
h a n d o n t h e s i d e o f t h e pa t i e n t ' s h e a d , o n t h e s i d e
o f t h e l e s i o n , a n d t e l l s h e r t o re s i s t a rh y t h mic p u s h
( t w o p e r se co n d ) d e l i vered s o ft l y a n d g e n tly from
t he s i d e ; t h i s p ro d uces a r h y t h mi c c o n tracti o n of t h e
scal e n u s w h i c h
m ob i l izes b o t h t h e fi rs t a n d
second r i b . T h i s is
a
t re a t m e n t
6.49) .
( Fig ur e
the
t ec h n i q u e i d e a l ly s u i ted for s e l f­
T h e cervical sp i n e
Tract i o n
M a n u a l t r a c t i o n c a n be p e r fo r m e d w i t h t h e p a t i e nt
I n o r d e r to d e l iver a t h r u s t , t h e s p rin g i n g tech­
n i q ue i s m o s t e ffe c t i v e . I t is a l so use f u l for d i a g n o s i s
s u p i n e or s e a te d ; i n t h e fo rm e r case t h e h e a d m u st
p roj e c t o v e r the edge o f t h e t a b le . As t h e m e t h o d
o f c h o ice is a u to m a t i c i so m e t r i c t r a c t i o n , re q u i r i ng
v e ry l i t t l e f o r c e , t h e t h e ra p i s t s i m p l y cradles the h e a d
w i t h b o t h h a n d s , a nd te l l s t h e p a t i e n t to l o o k u p
t o w a r ds h e r b row w h i l e b re a t h i n g i n ; w h e n he s e e s
t h e s t e rn o m a s t o i d s a n d sca l e n i a u t o m a tic a l l y con­
t ra c t
,
and a t t h e same t i m e fe e l s re sista nce aga i n s t
t r a ct i o n , he te l l s t h e p a t i e n t to h o l d h e r b re a t h , a n d
then t o l o o k d o w n t o w a r d s h e r ch i n w h i le b re a t h i ng
o u t a n d rel a x i n g . D u r i n g t h is re l a x a t i o n t h e t h er a p i s t
6.5 1a).
fee l s the p a t i e n t 's n e c k l e n g t h e n i n g ( F i g u re
So as to e n h a n ce r e l a xa t io n a n d to g i v e c o m f o r t ,
t h e t h e r a p i s t may p r o p t h e p a t i e n t s h ea d up a b o v e
'
h i s thighs a n d move b o t h h i s h a n d s on e i t h e r s i d e o f
h e r n e c k f ro m t h e s h o u l d e rs u p towa rd t h e o cc i p u t
carryi n g o u t m a s s age a n d tract i o n a t t h e s a m e t i m e .
Figure 6.49 R e pe t i ti v e m o b il i z a t ion o f t h e fi rst a n d
rhy t h mic c o n t r a c t i o n o f t h e
s e c o n d r i b s b y i s o m e t ric
sca le n u s
If t h e p a t i e n t is s e a te d
( F i gu re 6 . 5 1 b ) , t h e
thera­
pist s t a n d s be h i n d h e r d ra w i n g h e r ag a i n s t h i s c h e s t
,
to f a c i l i t a t e re l a x a t i o n . He t h e n t a k e s h e r head i n
b o t h h a n d s , h i s pa l m s on h e r c h e e k s , t h u m bs a t t h e
m a s t o i d a n d e l bows o n h e r s h o u ld e rs, w i t h o u t e x e r t ­
i n g p r e ss u r e . H e g i v e s t h e s a m e o r d e r a s be f o r e ; h e
d o e s n o t s e e t h e s t e rn o m a s t o i d s con t r a c t , b u t fe e l s
i n creased res i s t a n ce e v e n m o re s t r o n g l y t h a n i n t ile
fo r m e r posi t i o n
,
a n d fee l s
the
neck
l e n g l h e n i ng
d u ri n g re l a x a t i o n .
A s i t e m p l oys P I R , m a n u a l trac t i o n i s b o t h gen t l e r
and m o r e e ffe c t i v e t h a n m e c h a n i c a l tr a ct i o n . The
l a t t e r may b e app l i ed w i t h the p a t i e n t s u p i n e o n
ta ble t i l t e d d o w n w a rd tow a r ds
t he fee t ,
a
or s i t ti n g
a s l i ng p u l l i n g u p w a rd s . I t is m o s t i m p or t a n t
t h a t t h e p u l l s h o u l d be exerted o n t h e occ i p u t a n d
n o t o n t he c h i n .
with
M o b i l izat i o n
Side - b e n ding
This ca n b e c a r r i e d o u t w i t h t h e p a t i e n t se a te d or
s u p i ne . T h e p h e n o m e n o n o f a l te r na t i n g Il x a t i oll a n d
re l a x a t i o n
Figure 6.50 S p r i n g i ng a n d t h r u s t i n g m a n i p U l a t i o n of the
fi r s t r i b
d u ring
bre a t h i n g
in
and
out
can
be
effective l y u s ed for t h e c e r v i c a l spin e . T h e t h e ra p i s t
s t a n d s b e h i n d t h e p a ti e n t u s i n g t h e r a d i a l a s p e c t o f
Copyrighted Material
Therap eutic tech niques
1 89
(a)
Figure 6.52 S i d e - be n d i ng m o b i l i z a t ion w i t h t h e patie n t
seated
( b)
6.5 L ( a ) Tract ion w i t h t h e p a t i e n t s u p i n e : v e ry
t r a c t i o n w i t h b o t h h a n d s c ra d l i n g t h e
p a t i e n t ' s occ i p u t . ( b ) Tract i o n o f t h e cerv i c a l s p i n e w i t h
t h e p a t i e n t se a t e d : t h e t h e r a p i s t res t s h i s a r m s o n t h e
p a t i e n t 's s l lO u l d e rs
Figure
ge ntle ( isometric)
one h a n d a n d a
to fi x t h e tra nsve rse
of t h e segm e n t b e i n g
t r e a t e d , w h i l e h i s o t h e r h a n d o n t h e ot her s i d e o f
t h e p a t ie n t ' s h e a d b e n d s h e r h e a d a n d n e c k so as t o
t a ke u p t h e s l a c k i n t o s i d e - b e n d ing ( F i g u re 6 . S2) . I n
t h e even s e g m e n t s ( CO , C 2 , C4 ) , resistance increases
d u r i n g i n h a l a t i o n a n d w e ca n t h e refore a c h i ev e
grea te r fa c i l i t a t io n by te l l i n g the p a t ie n t fi r s t to l o o k
u p a n d then to b re a t h e i n slowly. A fte r t h i s she is
told to look down and b rea t h e out slowly, u n less we
prefe r to keep t h e n eck i n s l i g h t re troflex i o n (in the
lower ce rvi cal s p i n e , i f the patient is seated ) . in
which case it is better to tell h e r to 'let go' or ' relax'
and t h e n t o brea t h e o u t .
I n t h e odd seg m e n ts ( C I , C3 , C S ) , the patient i s
o n l y told to b re a t h e o u t slowly ( a ft e r ta k i ng a s h o r t
brea t h ) , a n d t h e n t o b r e a t h e i n s l o w l y a n d d ee p l y .
A tech n i q u e w h i c h is i d e n t i c a l w i t h that d escribed
fo re fi n g e r
p r o c e s s o f the lower v e r t e bra
fo r e x a m i n a ti o n (see Figure 4.30, p . 1 1 0) c a n a lso b e
u se d . T h e t h e ra pist t a k e s u p t h e s l a c k in t h e segme n t
w h e r e he h a s d i agnosed res t r i c t i o n , a n d fee l s
i n crea s i n g resistance as t h e p a t i e n t l o o k s t o w a r d s
h e r b r o w a n d breathes i n (in t h e e v e n segme n ts ) o r
bre a t h e s o u t ( i n t h e o d d segm e n ts ) . A ft e r t h i s h e
w a its u n t i l h e fee l s resistance d is a p p e a r d u ring
e x h a l a ti o n and l oo k i ng towards the ch i n or i n ha l a­
tion respect ivel y , a n d e ncou rages the p a t i e n t to re l a x
i n to si d e - be n d i ng. I f h e m a ke s t he cruci a l m i s t a k e
o f fo rc i n g side-be n d i ng, t h e e ffects o f spontaneous
rel a x a t i o n w i l l be l ost. T h i s tec h n i q u e i s a p p l ica b l e
fo r segm e n t s C I -C6. T h e m a n o e u v re i s u s u a l l y
repe a te d o n c e o r twice .
S i d e - b e n d i ng s u pi n e as described i n C h a p t e r 4
( Figu re 4 . 30 b ) s t a rtin g w i t h exh a l a tion is the t e c h ­
n i q u e o f cho ice for mobil ization o f t h e atlas/axis; m o re
t h a n one repe t i t i o n is o n l y excep t i o n a l l y re q u i re d .
T h e t e c h n i q u e s for side-be n d i n g m o b i l iza t i o n o f
t h e cervicothoracic j u nction a r e t h e s a m e a s fo r
d i agn osis (see Fig u re 4 . 3 1 ) . Th rough o u t t h e cervico­
t h o racic j u nctio n i n h a lation i n creases resistance to
s i d e-bending w h i le e x h a l a t i o n h a s a mobi l iz i n g
e ffec t . T h e p a t ie n t i s therefore told fi rs t to look u p
a n d then to breathe i n s l o w l y , a n d a ft e r i n h a l a t i o n
to relax a n d breathe o u t ( i f she w a s told to l o o k
d ow n , s h e w o u l d b e n d her h e a d fo rward a n d t h u s
' u n lock ' t h e ce rvical spine a n d lock the ce rvico­
thoracic j u n c t i o n ) . Care must be taken to h o l d the
patient's head in the s i d e - b e n d i n g position, using t h e
fi n g e r s , m a i n ta i n i n g retroflex i o n a n d rotation to t h e
opposite s i d e w h i l e t h e upper vertebra i s fixed by
the therapist w i th the t h e n a r e m i nence o f t h e same
hand. The t h u m b o f the o t h e r hand m e a n w h i l e fixes
t h e spinous process o f t h e lower vertebra o f the
segm e n t b e i n g t re a t e d .
Copyrighted Material
1 90
/vlaniplIlative Therapy
in Rehab ilita tion of th e Locomotor System
It is tec h n ica l l y e a s i e r ( though l ess c o m fo r t a b l e for
the t h e r a p i s t ) to carry o u t t h i s mob i l iza t i o n w i t h the
p a ti e n t lying o n her side. H e holds th e p a t i e n t as
d u ring diagnosis (see Figure 4.34, p. 1 1 3). S t a n d i ng
i n fro n t of the patie n t , the t h e ra p ist cradles the head
a n d n e c k in h is fore a r m , with h i s elbow o n the ta b le
o r slightly above it. He now t e lls t h e pati e n t to look
up to h e r fo re h e a d , a n d to b r e a t h e i n slowly . After
i n h a la t i o n the p a t i e n t i s t ol d to h o l d her b re a t h a n d
t he n t o re l a x a n d to breathe o u t slow l y . When the
t h era p ist fee l s the re l axation h e has o n l y to move
his e l bow s l i g h t ly forw a rd , fol lowing the p a t ie n t 's
re l a x a t i o n a n d h i s h a nd wil l a u toma tica l ly move t h e
p a t i e n t ' s h e a d i nto l a t e r a l flex i o n , r e t r o fl e x ion a nd
r otati o n i n t h e d i rection opposite to the side­
be n d i n g
W i t h both these tech niq u e s ( t h e pa t i e n t l y i n g on
h e r side, o r s e a t e d ) i t i s pos s i b l e to d e l iv e r a t h rust
a fte r t a king u p t h e s l a c k , a n d t h i s a l s o a fte r m o b i l iza­
tion. I f t h e p a t i e n t is s e a t e d the thrust is d e l i v e re d
by t h e t h u m b aga i nst t h e s p i n o u s process, the hand
h o l d i n g t h e h e a d and neck prov id i ng the fixation. I f
t h e p a t i e n t i s l y i n g o n h e r s i d e , i t i s t h e h a n d crad l in g
t h e h e a d a n d n e c k t h a t d e l ivers t h e th rust i n t h e
s a m e d i re c t i on as m o b i l izatio n , w h i l e t h e t h u m b o n
t h e s p i nous p rocess p r o v i d es the fixation.
,
.
,
Rotation
This is carried out w i t h t h e p a t i e n t seated . Ag a i n the
tech n iq u e is b a s i ca l ly that of exa m i n a tion ( s ee
Figure 4.32a, p . 11 2) . W h i l e the the r a p i s t fixes t h e
arch o f t h e lower ve rtebra o f t h e t r e a t e d segm e n t
b e t w e e n t h u m b a n d fo r e fi nge r h e r otat e s t h e h e a d
i n t h e direction of m o b i l i za t i o n u n t i l t he s l a c k i s
t a ken u p . He t h e n te l l s t h e pati e n t to l oo k up and
t o brea the i n slowly, to hold h e r bre a t h a n d t h e n to
l o o k down and to b reathe out, obtain ing automatic
mobi l ization in the restricted d i recti on, w h i l e h e
m a i n t a i ns fi x a t i o n of t h e lower ve rtebra . Th is i s
r e pe a te d t w o or th ree times. (Lo ok i n g up a n d
breathing i n sl i g h t l y increases r e s i s tance against
rota t i o n w h i l e l oo k i ng down and e x h a l a t i o n b ri ngs
a bo u t re l a x a t i o n . )
If this v e r y ge n tle tec h n i q ue i s n o t s u ffic i e n t l y
e ffecti v e , i t i s poss i b l e to te l l t h e patie n t a fter the
slack has been t a k e n u p i n rota t i o n , to look i n the
o pp o s i t e d i rection to m o b i l i z a t i o n and t o bre a t he i n ,
t h e n to h o l d h e r brea t h , a nd t o loo k i n t h e d i rection
o f mobi lization a n d to b re a t h e out. This m e t hod
seems very logica l , b u t is fre q u e n t l y too forcefu l .
For rot a t i o n i n t h e ce r v i coth oracic j u nc t i o n the
patie n t is seated, w h i l e the t h e ra p i s t s t a n d s be h i n d
h e r a n d fi x e s the s p i n o u s process o f t h e lower
v e r teb r a o f t h e se g m e n t to be treated, placing h i s
t h u m b on th e side from w h i c h the h ea d a n d n e c k
a r e ro t a t e d . H e h o l d s t h e pati e n t s head with h is
arm, from a b o v e , so t h a t h i s e l bow is i n fro n t o f h e r
forehea d a nd h i s l i t t l e finge r at t h e a rch of t h e upper
,
'
vert e b ra o f th a t segm e n t . H e rot a tes the h e a d t o t a k e
up t h e slack, t h e n te l l s t h e p a t ie n t to l o o k i n t h e
di rection away from rota tion a n d to breathe i n a n d
hol d h e r breath. S h e then looks in t h e d i rection of
mobi l ization and b rea thes o u t This m a n oe u v re is
r e p e a te d from each new position g a i n e d ( see F ig u re
4.32d). With the same tec h n iq u e i t is p os s i b le t o
d e l i v e r a t h rust by i n c reasing h e a d r o t a t i o n a n d
t r a c tion t he t h u m b p ro v i d i n g fi x a t i o n a t t h e sp i n o Lls
.
,
process.
Mob ilization of the occi put a g a i nst the
atlas
T h i s is p e r fo r m e d by exactly t h e s a m e tec h n i q ues a s
u s e d i n d ia g n osis I n t h i s s eg m e n t t h e fac i l i t a t i n g
e ffe c t of i n h a l a t i o n a n d the i n h i b i tory e f f ect o f
e x h a l a t i o n o n m uscle a ct i v i ty i s t h e greatest, a n d t h i s
is t r ue fo r a l l directions.
.
Anteflexion (see Figure 4.37, p . 1 1 4 )
U s i n g t h e s a m e techn i q u e , the t h e r a p i s t b e n d s t h e
to ta k e u p t h e s l a c k : h e t h en t e l l s t h e
p a t i e n t t o l o o k t o w a r d s h e r fore h e a d a n d bre a t he i n .
T h e t h e r a p i s t resists the p a t i e n t ' s a u tomatic head
retroflexion. A ft e r i n h a lation t h e p a t i e n t i s t o l d t o
l ook d o w n w a rds a nd to b re a t h e o u t s l o w l y : head
a n t e fl e x i o n a u tom a t i c a l l y fo l lows. This i s re peate d
two or three times.
h e a d fo r w a rd
Retroflexion ( se e Figu re 4.36, p . 1 1 4)
After ta k i n g u p t h e s l a c k w i t h the head r o t a ted a n d
i n retro1k x i o n , t he t h e r a p i s t a s ks t he p a t i e n t to d o
no more t h a n to breathe i n s l o w l y H e w i l l se nse
i ncreased resista nce to ret rofle x i o n , t h e n he te l l s t h e
p a t i e n t to bre a t h e o u t s l o w l y a n d le t t h e h e a d fa l l
back. ( In this case, l oo k i n g u p d u r i n g t h e firs t p h a s e
w o u l d i n terfe re w i t h i n creased resist<l nce to retro­
fl e x i o n , w h i l e look i n g down d u r i n g t h e re l <l x a tion
p h ase would i n t e rfere with retroflexion . ) Fo r rel a x ­
a t i o n i nto re troflexion i t is w i s e r n o t t o ro�<' t e t h e
patie nt's h e a d more t h a n 4 5 d e g re e s : t h e p a tie n t
relaxes be tt e r a n d we a v o i d t h e o d i o u s com b i n a tion
of retro flexion w i t h m a x i m u m rota t i o n o f t h e
cerv ica l s p i n e .
.
Side-bending (see Figu re 4 . 3 5 , p . 1 1 4)
Afte r t a k i n g u p t h e s l ack w i t h the patie nt's h e a d
ro t a t e d a n d side- b en t , t h e t h e ra pist tells h e r to l o o k
t o w a r d s h e r brow and to b re a t h e i n s l o w l y : h e w i l l
fe e l i ncreased resistance to s i d e - be n d i ng. After
h o l d i ng h e r b r e a t h t he p a t i e n t is told to look towards
her chin and breathe o u t ; t o w a rds the e n d of
exha lation t h e patient s p o n t a n e o u s l y re l ax e s i n t o
l a te ra l A e x i o n . ( S e e a l so gravi t y P I R o f t h e sterno­
m astoid musc l e , Figure 6.96.)
Copyrighted Material
Thel'llp elllic techn iq l l es
Rotation
p a t i e n t s ea ted ,
the t h e r a p is t b r i n gs t h e h e a d
w i t h t h e m i n i m u m o f for c e ,
ta k i n g u p t h e slac k a n d st a b i l i z i n g t h e h e a d , i n a x i a l
r o t a ti o n , a g a i n s t h is c h e s t . H e n o w t e l l s t h e p a t i e n t
to l o o k up a n d to b re a t h e i n s l o w ly , w h i l e h e fe e ls
i n cr e a s e d re sis t a nce to r o t a t i o n . The p a t i e n t is t h e n
told t o l o o k downwa rds a n d b re a t h e o u t : d ur i ng o r
tow a r d s t h e e n d o f e x h a l a t i o n , rota t i o n o f t h e he a d
i n c r e a s e s a l m o s t s p o n t a n e o u s l y . I n t h i s cas e l o o k i n g
u p a n d d o w n is b e t t e r t h a n l o o k i n g fi r s t to o n e a n d
t h e n t o t h e o t h e r s i d e , because l ess f o rc e i s p r od u c e d .
A ft e r atlas · mo b i l i za t i o n , t h e t h e ra p i s t should
make s u r e that t h e T r P s o f t h e short e x te nsors
c ro s s i n g t h e p o s t e r i o r a rc h o f t h e a t las and a t t h e
upper e n d of t h e ste rnomasto i d h ave d i s a p p e a r e d :
t h i s i s t h e m o s t i m p o r t a n t c r i t e r i o n o f s u c c es s f u l
trea t m e n t of t h i s segme n t .
W i t h the
i n t o m a x i m u m ro t a t i o n ,
19 1
p a t i en t ' s h e a d ca n b e v e ry s l ig h t l y r o t a t e d a w a y from
t he t h e r a pis t , b u t c a r e m u st be t a k e n n o t t o ro t a t e
so fa r t h a t t h e segm e n ts we w a nt to t r e a t are l o c k e d .
I n t h e p o s i t i o n described ( Figure 6.53a ) , t h e t h e r a ­
pist t a k e s u p t h e s l a c k b y g i v i n g a s l i g h t p u l l w i t h
both h a n ds i n a c r a n i a l d i rect i o n , a ft e r w h i c h t h e
t h r u s t i s d e l i ve red e i t h e r ( I ) w i t h both h a n d s g i v i n g
a p u l l ( p us h ) i n t h e s a m e d i re c t i o n , o r ( 2 ) d e l i v e r i n g
t he t h r u s t i n t o t r a c t i o n w i t h a s l i g h t l a t e r a l l1 e x i o n
tow ards the t h e r a p i s t . I n b o t h cases t h e t w o h a n d s
m u s t o p e ra t e as a si ngle u n i t . The t h r u s t m u s t
t h ere fore c o m e fro m t h e t h e ra p i s t ' s tru n k , o v e r t h e
s h o u l d e r s to t h e h a n d s , w h e t h e r p u re t r a c t i o n i s
a p p l i e d or t r ac t i o n w i t h s i d e - b e n d i n g. Th is t e c h n i q u e
c a n b e used for C I -C5 .
Thrust tech n i q u es
W i t h few excep t i o n s , cases o f s e r i o u s c o m p l i c a t i o n s
a fter m a n i p u l a t i o n occ u r red a fter h i g h - v e l o c i t y t h rusts
had been used in thc cerv ica l r e gi o n . F u rt h e r sc r u t i n y
showed t h a t
m a n i p u l a t ion h a d bee n a pp l ie d w i t h
fo rce , w i t h o u t fi rs t t a k i n g u p the slack. T h i s i s a n
e x t re m e l y fa u l t y t e c h n i q u e , a n d t o m a ke m a t t e r s
worse a c o m b i n a t i o n of m a x i m u m ro t a t i o n w i t h
re t ro fl e x i o n w a s e m p l oy e d . T h e l o g i c a l conseq u e n c e
is t h a t . o f the large n u m b e r o f t e c h n i q u e s t o c h o o s e
fro m , we a v o i d t h o s e t h a t p ro d u c e m u c h ro t a t i o n
a n d p a r t i c u l a rly r o t a t i o n i n re t ro fl ex i o n . T h e m o s t
im p o r t a n t a n d freq u e n t l y u s e d t e c h n i q u e s a re t h ose
in w h i c h t h e t h r u s t is d e l i v e re d i n t h e d i r ec t i o n of
tra c t i o n , in a c ra n i a l d i rection ; w i t h the a p o p h y se a l
j o i n t s t i l ted a t a bo u t 45 d e g ree s from t h e h o r i zo n t a l
p l a n e i n the m i d - a n d l o w e r ce r v i c a l s p i n e , a n d
a lm os t h o r i zo n t a l a t CO, C I a n d C 2 , tra ct i o n pro d u c e s
g a p p i n g oJ these j o i n ts, i n a d d i t i o n to d i s t r a c ti o n o f
the i n terverte b r a l d iscs.
( a)
Traction high - velocity th rust applied to th e
crania l vertebra of th e blocked seg m e n t, with
th e patient supine
The p a t i e n t ' s h e a d i s o v e r the e d g e of the t a b l e , w i t h
t he t h e ra p i s t faci n g a n d c r a d l i ng i t [rom a bo v e w i t h
t h e o cc i p u t o n h i s fo re a r m a n d t h e fi n g e r s o n the
p a t i e n t ' s c h i n . W i th the rad i a l s u r face o f the fi rs t
p h a l a n x of t h e fo r e fi n g e r o f t h e ot h e r h a n d h e m a kes
c o n t a c t with t h e t r a n s v e rse p rocess o f t h e u p p e r
vertebra o f t h e t rea ted segme n t , side - b e n d i n g t he
cerv i c a l s p i n e o n l y so fa r as n o t t o s l i p o v e r t h e
tra n sve rse p rocess ( i f t h e u p p e r v e r te br a i s t h e a t l a s ,
v e ry l i t t l e si de - b e n d i n g is n e e d e d be c a u s e the tra ns­
ve rse p r o c es s e s o f t h e a t l as a r e l o n g e r and n a t u ra l l y
j u t b e y o nd t h e o t h e rs . The l ower t h e t r a n s v e rse
process, the fu r t h e r we bend the cerv ica l s p i n e ) . T h e
( b)
Figure 6.53 T r a c t i o n t h rust i ng m a n i p u l a t ion of t h e
c e rv i c a l s p i n e w i t h t h e pa t i e n t s u p i n e : ( a ) co n t a c t i s
m a d e a t t h e t ra n s v e rse process o f t h e u p p e r v e r t e b r a o f
t h e s e g m e n t t re a te d , o r ( b ) a t t h e mastoid p r o c e ss for
COi l , w i t h t h e h e a d rota ted
Copyrighted Material
1 92
M an ip l l ialive Therapy in Rehabililalion of Ihe L o co rn O l O r Syslem
For t h e occipitoatlantal segm ent t h e t h e r a p i s t
rotates t h e h e a d so as to lock the a tlas/ax is at a b o u t
45 d e g r e es a n d m a k es contact a t t h e mastoid pro­
cess. If h e w a n ts to a pp l y l a teral flexion a t t h e s a m e
t i m e , h e m u s t bea r i n m i n d t h e rot a t i o n o f t h e h e a d ,
i . e . the s i d e b e n d i n g m us t be a t r i g h t a n g l e s to the
s a g i t t a l p l a n e o f t h e ( rota ted ) head ( F i g u r e 6.53b).
,
-
s e g m e n ts
t he
C4-C7 .
Below
this
t h e t h e ra p i s t ' s
finge rs b e c o m e i n e ffe c t i v e ; t h e y m e re l y p ro d u c e a
slight
pu l l
of
the
c e r v i ca l s p i n e i n a n u p w a r d
i s g i v e n b y t h e o pe r a t o r s
t h e s p i n o u s p r o c e s s of T 1 or T2 .
d i re c ti o n w h i l e t h e t h r u s t
,
b reastbone
Both
aga i nst
these
traction
'
techniques
a re s a fe
a nd
if
c o r r e c t l y a p p l i e d a re v e ry ge n t l e . H o w e v e r , t h e y a re
n o t a b s o l u t e ly s p e c i fi c beca use t h e t h r u s t is g i v e n to
,
the u p p e r ve rtebra o f the blocked segme n t , w h i l e
Traction lo w- velocity th rust applied t o th e
cra nial vertebra of the blocked segm e n t, with
th e p a tie n t sea te d ( Figure 6 . 5 4 )
cl as p ed
h e a d a n d t h e e l bows fa r a p a r t . T h e
t h e r a p i s t sta n d s b e h i n d t h e p a t i e n t a n d th re a d s h i s
fo r e a rm t h r o u g h t h e tr i a n g l e fo r m e d by t h e pa t i e n t s
u ppe r a r m a n d fore a r m , fi rst on o n e a n d then on the
o t h e r s i d e . H e m a k e s c o n t a ct w i t h b o t h fore fi ngers
and m i d d l e fi n g e rs crossed o n the s p i n o u s proccss of
the u p per vertebra o f t h e s e gm e n t t o b e t re a te d . T h e
pa t i e n t is n o w t o l d t o re l a x a n d l e t h e r head fa l l
fo rw a r d . The t h r ust i s d e l i v e r e d b y t h e fi n g e r s
i n c r e a s i n g t h e i r press u re i n a forw a rd a n d u p w a r d
d i r e c t i o n . T h i s t e c h n i q u e is most e a s i l y app l ie d to
The
pa t i e n t
l ow e r v e r t e b ra i s n o t fi x e d . T r a c t i o n m a y
t h e r e fo r e a rfect s o m e of t h e m o r e c a u d a l s e g m e n t s ;
t h i s n e e d n o t , h o w e v e r , b e c o n s i d e re d h a r m fu l .
the
s i ts o n t h e t a b l e w i t h h e r h a n d s
b e hi n d h e r
Rota tion thrust with the patie n t sea ted ( Fi gure
6.55)
'
T h e p a t i e n t s i ts o n a l o w s t oo l ; t h e t h e ra p i s t s t a n d s
b e h i nd her, pass i n g o n e h a n d a n d fo r e a r m i n fro n t
of t h e p a t i e n t ' s face ( b r o w ) s o t h a t t h e e l bo w i s i n
fro n t o f t h e fo re h e a d a n d t h e h a n d be l o w t h e
occ i p u t , t h e l i t t l e fi n g e r c l a s p e d ro u n d t h e a rc h o f
t h e u p p e r v e r t e b r a of t h e b l o c k e d s e g m e n t a n d t h e
occiput com forta b l e aga i n s t t h e t h e ra p i s t s c h e s t .
T h e nec k is t h u s he l d i n a k y p h o t i c p os i t i o n W i t h
t h e t h u m b o f t h e o t h e r ha n d , t h e t h e r a p i s t fi x e s t h e
'
.
s p i n ous process o f t h e l o w e r v e r t e b r a o f t h e segm e n t
o pp o s i t e t o t h e d i rec tion i n w l1ich t h e
h e a d i s r o t a t e d , so as to k e e p it i n n e u t ra l p o s i t i o n .
T h e a r m ro u n d t h e p a t i e n t s h e a d now r o t a tes i t a n d
t h e u p per v e r t e b r a o f t h e b l o c k e d segm e n t , so a s [ 0
t a k e up t h e s l a c k , t h e t h u m b o f t h e o t h e r h a n d
h o l d i n g t h e s p i n o u s p ro c e s s o f t h e l ow e r v e r t e b ra i n
m i d p o s i t i o n T h e t l H u s t i s t h e n d e l i v e re d w i t h t h e
o n the s i d e
'
-
Figure 6.54 ( a ) Tr a c t i o n m a n i p u l a t i o n of t h e
the fi n ge r s
c e r v i co t h o r a c i c j u n c t i o n : ( b ) a p p l ica t i o n o f
.
Figure 6.55 Ro t a ti o n t h rust i n g m a n i p u l a t i o n o f t h e
ce r v i c a l s p i n e w i t h t h e p a t i e n t seate d , u n d e r t ra c t i o n , i n
k y p h o s i s w i t h t h e t he ra p i s t s ' s t h u m b fl e x i n g t h e l o w e r
vertebra o f t h e treated s e gm e n t a t t h e s p i no u s p rocess
Copyrighted Material
Th erapelilic Icchniques
h a n d ro u n d
the
1 93
p a t ie n t ' s h e a d , m a i n l y i n t o t r a c t i o n
i n a c r a n i a l d i re c t i o n , s l i g h t l y i n cre a s i ng rota tion a t
the same time.
T h i s tech n i q u e i s h ig h l y s p ec i fic , a s t h e l o w e r
ve rte b r a i s fi x e d ; i f t h i s fi x a t i o n i s c o r r e c t . rota ti o n
is o n l y m o d e r a te a n d t h e re i s a lw a y s k y p h os i s a n d
t ra c t i o n
d u ri n g t h e t h r u s t .
This means t h a t t h e
te ch n i q u e i s q u ite sa fe .
Self- m o b i l i zati o n
S e l f- t rea t m e n t - se l f- m o b i l i z a t i o n - c o n s t i t u t e s a l i n k
b e tween m a n i p u l a t i v e t h e r a p y a n d re m e d i a l e x e r c i s e .
( a)
As t h e m o d e rn m o b i l i z a t i o n tech n i q u e s m a k ing u s e
of m u scu l a r fa c i l i t a t i o n a n d i n h i b i t i o n a re a l re a d y
b a s e d o n t h e a c t i v e coope r a t i o n o f t h e p a t i e n t, it i s
logi c a l t h a t t h e t r e n d s h o u ld be t o t e a c h t h e pa t i e n t
i n c r e a s i n g l y h o w to d e a l w i t h h e r p r o b l e m s h e rs e l f.
To use o n e ' s o w n m us c l e s to m o v e o n e ' s s p i n e ,
e v e n w i t h con s i d e r a b l e force , is n o t h i ng n e w . I n d e e d ,
t h e u s u a l mov e m e n t s p e r fo r m e d i n p h y s i c a l tra i n i n g
- som e w h a t force f u l , fa s t a n d n o n -specific - do m o re
h a rm t h a n go o d . M o v e m e n t re s t ri c t i o n goes h a n d i n
hand
w i t h m u sc l e s p a s m p r o t e c t i n g t h e
b locked
segme n t . Force f u l m o v e m e n t s u d d e n l y a p p l i e d to
that segm e n t i s l i k e l y o n l y to i n c rease s p a s m , w i t h
t h e re s u l t t h a t t h e n orm a l a n d h y p e r m o b ll e se g m e n ts
w i l l be m o b i l i ze d , w h i l e t h e a ffected segm e nt s w i l l
b e fi x e d eve n m o re fi r m l y b y m u s c l e s p a s m .
S e l f- m o b i l i za t i o n m u s t t h e re f o re b e a s g e n t l e a n d
( b)
Figure 6.56 (II) S e l f- m o b i l i z a t i o n of the l e ft s a c ro i l i ac
( a fter S a c h s e ) : ( b ) s e l f- m o b i l i za t i o n of the s a c r oi l i a c
j o i n t w i th t h e p a t i e n t l y i n g o n h e r s i d e
joint
slow a s t h e m o b i l i z a t i o n t e c h n i q u e s w e u s e , m o v i n g
t h e segme n t a fter t h e s l a c k h a s b e e n t a k e n u p ; i t
m u s t a l s o be a s s p e c i fi c a s poss i b l e . P r e c i s e c l i n i c a l
d i agnosis a n d i n d i c a t i o n a re m a n d a tory.
s u p e rior, so a s to p r o d u c e r h y t h m i c a l s p r i n g i n g p r e s ­
s u re i n a v e n trocra n i a l d i recti o n , a n d re i n forces i t
w i t h t h e o t h e r fo r e a r m a n d h a n d , i n t h e d i re c t i o n o f
m o bi l i z a t i o n ; t h i s prod u c e s gapp i n g of t h e s a cro i l i ac
j o i n t (Figure 6 . 5 6b ) . In i t s e lf, t his i s an e a sy m a n ­
Self-mobil ization of the sacroi l i a c j o i nt
( S a c hse a n d S c h i l d t , 1 98 9 ; Fig u re 6. 5 6 0 )
o e u vre , t h e d i ffi c u l t y l y i n g i n t h e n e e d t o t e a c h t h e
p a t i e n t t o e x e rt pressure i n t h e correct d i recti o n , a n d
The p a t i e n t is k n e e l i n g on t h e t a b l e , c lo s e to t h e
n o t t o u s e force .
edge, h e r t r u n k s u p po r t e d o n h e r e l b o w s . O n e k n e e
ha ngs ove r t h e e d ge o f t h e t a b l e , w i t h t h e i ns t e p
s u p p o r t e d j u s t a bo v e t h e h e e l o f t h e o t h e r f o o t . I n
t h i s pos i t i o n t h e p a t i e n t m u s t r e l a x s o t h a t t h e p e l v i s
Self- m o b i l i zation of the ( l ower) l u m b a r
sp i n e. a nte- a n d retrofl exion ( F i g u re 6.57)
s l o p e s o b l i q u e l y d o w n w a rds f r o m t h e i l i u m , w h i c h
T h e p a t ie n t s i t s on her h e e l s , s u p p o r t i n g h e r s e l f w i t h
is s u p p o r t e d b y t h e k n e e o n t h e t a b l e . I n t h i s w a y
o u ts t r e tch e d a r m s r e s t i n g o n h e r k n e e s . B y c o n ­
the s l ack is raken up al t h e sacroi l i ac joint o f t he
s u p p o r t e el
s i el e . T h e
tension in
t h e re g i o n of h e r s a c ro i li a c j o i n t , s h e
moment
the
p a t i e n t senses
t r a c t i o n o f t h e g l u t e a l m u s c l e s ( g l u te i m a x i m i ) s h e
r a i s e s h e r pe l v i s , p r o d u c i n g k y p h o s i s o f t h e l u m b a r
spine;
after
relaxation
the
pel v i s
fa l ls
fo rw a r d ,
m a k e s a ve ry s m a l l el o w n w a rd s p r i n g i n g mov e me n t
p r o d u c i n g l o r d o s i s a t t h e l u m b o s a c ra l j u n ct i o n . Th i s
w i t h t h e k n e e o v e r t h e edge o f t h e t a b l e , movi n g i n
exe rcise
a ve r t i c a l d ire c t i o n a n d t h u s m o b i l i z i n g t h e s a c roi l i a c
position of t h e p e l v i s w h i l e s ta n d i n g .
is i m po r t a n t fo r t ra i n i n g i n
t h e correct
joi n t on the supported side.
A n o t h e r v e r y effe c t i v e t e c h n i q u e i s d e r i ve d from
m o b i l i z a t i o n l y i n g o n the s i d e (see F i g u r e
4 . 1 0,
p.98).
Ly i n g on h e r s i d e w i t h h e r l o w e r l e g exte n d e d , t h e
p a t i e n t s t a b i l i ze s h e r p e l v i s w i t h t h e k n e e o f t h e
Self- m o b i l i zati o n of t h e l u m b a r spi n e.
rotation ( F i g u r e 6.58)
T h e p a t ie n t l i e s on h e r s i d e n e a r t h e edge of t h e
u p p e r fl e x e d l e g o n t h e t a b l e . S h e n o w p u ts t he w r i s t
t a b l e . The l o w e r l eg i s s t r e t c h e d o u t , t h e u p p e r l e g
of h e r u p p e r h a n d o n h e r u p p e r s p i n a i l i a c a a n teri o r
b e n t a t t h e k n e e s o t h a t t h e t o e s a r e h o o ked be h i n d
Copyrighted Material
1 94
M a n ip u la t i v e Therap v
in Rehab ilita tion of t h e L o c o m o tor System
t h e l ow e r l e g . I f sel f- m o b i l i z a t i o n i s d i re c t e d to t h e
p e r s e co n d , p rod u c i n g repe t i t i v e m o b i l i za t i o n ; o r s h e
l ow l u m ba r spine, the t o e s r e s t b e l o w t h e knee of
m a y e x e r t s l i g h t pressure o n t h e k n e e w i t h t h i s h a n d ,
f r o m a b o v e , re s i s t i n g h e r o w n press u r e [ o r a b o u t
t h e s u p p o r t i n g l eg ; i f t h e u p p e r l u m b a r s p i n e , o r u p
t o t h e t h o r a co l u m b a r j u n c t i o n i s t o be t r e a t e d , t h e
1 0 s w h i l e b r e a t h i n g i n , a n d t h e n re l a x i ng , b re a t h i ng
u p p e r l e g i s s u p ported a b o v e t h e k n e e a n d t h e n t h e
out
l o w e r l e g s h o u l d b e s l i g h t l y fl e x e d a t t h e k n ee . W i t h
repe a te d t h re e to fi v e t i m e s .
t h e h a n d t h a t l i e s u p p e r m o s t t h e pa t i e n t h o l d s t h e
fa r e d ge o f t h e t a b l e fo r s t a b i l i za t i o n , w h i l e t h e o t h e r
and
i n cr e a s i n g
There is
rota t i o n . T h i s
m a n oe u v r e
is
a l s o a v e r y e ffe c t i ve g ra v i t y - i n d u c e d
pa t i e n t shou l d turn h e r head to the
e x e rc i s e fo r s e l f- m o b i l i z a t i o n . i n t o rota t i o n a n d
fl e x i o n i n t h e l u m b a r s p i n e , w h ic h i s i d e n t i c a l w i t h
P I R of t h e l u m b a r p a r t of t h e e r e c t o r s p i n a e a n d i s
t hat
d e s c r i b e d l a te r ( s e e F i g u re 6 . 1 1 5 ) .
( l ow e r ) h a n d l i e s o n t h e
( u p per)
fl e x e d k n e e . T h e
sicle o p p o s i t e t o
of ro t a ti o n ; she m a y now e x e r t press u r e r h y t h m ­
i c a l l y w i t h t h e h a n d l y i n g o n t h e k ne e , o n c e o r t w i c e
Self- m o b i l izat i o n o f the l u m b a r s p i n e i nto
retrof l ex i o n a n d latera l flex i o n , sta n d i n g
( Fi g u re
6.59)
H e r e , fi x a t i o n i s d e c isive . The p a t i e n t m a y e i t h e r fi x
t h e u p pe r v e r t e b ra o f t h e s e gm e n t t o b e t r e a t e d , w i t h
t h e ra d i a l s u rface of
her
fore fi n g e r , from a b o v e ; o r
s h e m a y fi x t h e l o w e r v e r t e b r a w i t h t h e t i p s o f h e r
t h u m b s , t h u s crea t i n g a fu l c r u m . B y b a c k b e n d i n g a s fa r
as
or
side­
t o t h e fi x a t i o n p o i n t ( fu l c r u m ) s h e
t a k e s u p t h e s l a c k , a n d t h e n m a kes a s l i g h t r e p e t i t i ve
m o ve m e n t , r h y t h m i ca l l y s p r i n g i n g t h e se g m e n t
a bove o r b e l o w t h e t h u m bs o r fo re fi n ge rs respect i ve l y .
F i x a t i o n fro m a b o v e ( b y t h e fore fi n ge rs ) is i n d i c a ted
if t h e re i s h y p e r m o b i l i t y a b o v e the seg m e n t t re a t e d ,
and
from
b e l ow
(by
the
t h u mbs)
if
t h e re
( a)
( b)
( b)
Figure
6.57 Se l f- m o b i l i z a t io n
(a) a n teAexion:
Figure
o f t h e lowe r l u m b a r s p i n e :
( b ) re t ro A e x i o n
6.58
spine. the
R o t a t i o n se l f- m o b i l i za t i o n or t h e l u m b a r
pa t i e n t l y i n g o n h e r s i d e : ( a ) l o w e r . ( h ) u p p e r
lumbar spine
Copyrighted Material
is
Th uap eli lic lech n i q l l e5'
( a)
( b)
( e)
( d)
Figure 6.59 S e l f- m o h i l i za t i o n of the l u m h a r s p i n e . t h e p,l I i e n t s t a n d i ng. Fi x a t i o n of t h e upper v e rt e b r a of t h e tre a t e d
segme n t from a b o v e , w i t h t h e forefi nge rs: (a ) b a c k - be n d i n g : ( b ) sid e - b e n d i n g . Fi x a t i o n wi t h t h e t h u m h s from b e l o w :
(e) back-be n d i ng:
(d) side-bending
Copyrighted Material
[ 95
1 96
Manip u la t i v e Therapy
in Rehab ilitation
of the
LocomolUr
Svstem
hyperm o b i l i ty below. Obvious l y t h e l u m bosacra l
segm e n t is a l ways treated from above. I t is esse n tia l
t h a t a n y fo rceful moveme n t of l a rge range s h o u l d
be avoid e d ; o n l y t h e s m a l l, specific spri nging move­
ment s h o u l d be pe rfo r m e d , ab ove or below the
fu lcrum w i t h t h e sp i n e fixed b e l ow or above respect­
ivel y , moving once or twice per seco n d ,
Self- m o b i l i zation o f the th oraco l u m b a r
spine i n t o rotation
Th is corresponds to the tec h n i qu e d e scribed a bove
( see Figure 6.39, p. 1 84). The p a t i e n t l ies on h e r side
w i t h the l ower leg stretched o u t and the upper leg
be n t both at the h i p and at t h e k n e e a t a b o u t right
angles, Wi t h h e r o u tstretched lowe r arm the patient
fi x es t h e t h igh o f t h e flexed leg from a bove, turn i ng
h e r h e a d a n d neck i n to maxim u m rotation w h i l e
l o o k i n g a t a n o bj e c t pl a ced be h i nd h e r b a c k , I n t h i s
posi t i o n s h e e x e rts rhythmic pressure a ga i n s t the
o u tstretched arm, w i t h h e r k n e e , about twice per
seco n d . It is the rhyt h m ic contraction of the psoas
that prod uces the m o b i l i z a t i o n effect .
,
Ante- a n d retroflexion self- m o b i l i zation o f
the t h o racic spine (Figu re 6 . 60)
The
p a t i e n t is s u p ported o n both knees a n d elbows.
Mov i n g t h e thoracic spine into kyphosis she breathes
i n , t h e n moves i n to lordosis while s h e breathes out
to t h e m a x i m u m . T h e more c r a n i a l t h e m o b i l ization
req u i red, the further fo rward the e l bows a re p l a ce d
( a n d t h e chest lowere d ) , w h i l e for mobi l izat i o n a t
t h e t horaco l u m bar j u n ction it may be bette r t o
p e rfo rm t h e exe rcise o n h a n ds a n d knees.
Fi gure 6.60 Sel f- m o b i l iz a t i o n of (a) a n te fle x i o n and ( b )
retro A e x i o n
o f the m i d - a n d lower t h o ra c i c s p i n e
Retroflexion self-mobil izat i o n of t h e
t h o racic spine d u r i n g exha l ation
(Figure 6 . 6 1 )
The p a t i e n t s i ts o n t h e table w i th b o t h arms
s t retched by h e r side a n d t h e h a nds i n s u pi na t i o n
wi t h t h e fi n ge rs s p r e a d fa n-wise, S h e now breathes
i n l i g h tly, then d ur i n g max i m u m exh a l a t i on she
bends h e r tho racic spine backwards, at the same
time i ncreasi ng s u p i n ation o f the hands, C a re m u s t
be t a k e n n o t t o r a i s e t h e s h o u lders a n d n o t to b e n d
e i t he r t h e h e a d or the l u m b a r s p i n e backwards. I f
t h i s exe rcise is correctly p erformed the patient
s h o u l d fee l s l ig h t pain in t h e t horacic sp i n e a t
m a x i m u m e x h a l a t i o n a n d retroflex i o n . A v e r y good
a l tern ative is described o n p, J 80 (Figure 6.34) ,
Antefl ex i o n self- m o b i l i zation of the
t h oracic sp i n e i n i n h a l at i o n (Figure 6 . 62)
Th e p a t i e n t s i ts on h e r heels, bending forward so as
to have her fore head o n the t a b le , In t h i s pos i tio n
s h e breathes into her bac k . She e a s i l y l e arns h o w to
Figu re 6.61 Retro fl e x i o n sel f-m o b i l i z a t i o n of t h e t h oracic
spine with the p a t i e n t seate d . using max i m u m e x h a l a ti o n
a n d o u t w a rd r o t a t i o n o t t h e a r m s . w i t h fi ngers
w idespread
d i rect i n h a l a t i o n into the s t i ff s e g m e n ts ; t h is s h o u l d
w i t h t h e t h e ra p i s t ' s fi n g e r , a n d t h e n
fi rs t be c h e c k e d
by t h e p a t i e n t .
Copyrighted Material
Therapelllic lechniq lles
197
s l a c k a t t h is s e g m e n t . B y r e pe a t e d r h yt h m ic a l move­
m e n ts i n t h e s a m e d i rection s h e sp r i n g s t h e s e gm e n t
i n to retrofle x i o n , t h e head moving back horizo n t a l ly.
Rotat i o n self- m o b i l ization at the
cervicothoracic j u nct ion ( F i g u r e 6.65)
Rota t i o n o f t h e o u t st re tch e d arms w i t h fi n ge rs
s p rea d w i d e h a s s o m e m ob i l i z i n g e ffect on t h e
cerv icothoracic j u nc t i o n ; t h i s e ffe c t i s e n h a n ce d if
each a r m rota tes i n a n o p p os i te d i rectio n , one f r o m
s u pi n a ti o n i n to p ro n a t i o n a n d the other v i c e v e rsa .
T h i s a l o n e is n o t e n o ug h , however; t h e e x e rcise
becom e s very effective i f t h e h e a d i s a l s o rota ted , i n
t h e s a m e r h y t h m a s t h e a r m s a n d pre fe rabl y faci ng
t h e h a nd that is ro ta ti n g i n to p r on a t i o n ( t h e thumb
down ) . Care m u s t be taken n o t t o l i ft t h e should ers,
w h ic h s h o u l d be relaxed. This tech n ique s h o u l d n o t
be u s e d i f t h e re i s hypermobi lity i n the u p p e r
th oracic region.
Figure 6.62 A n te fl e x i o n se l f- m o b i l i z a t io n or t h e t h o r a c i c
s p i n e in i n h a l a t i o n . t h e pa t i e n t s q u a t t i n g a n d bending
fo r w a rd
I n h a lation self-mobil ization of the u pper
ribs (Figure 6.63)
p a t i e n t i s s e a ted ove r the e d ge of the table w i t h
k nees a part, i n anteflexion, a n d h e r h e a d i s t u rn e d
t o w a rds the s i d e to b e m o b i l ized . O n e arm h a n g s
b e t w e e n t h e k n e e s a n d t h e o t h e r at h e r s i d e . I n t h i s
pos i t ion t h e r i b s [0 be m o b i l ized b u lge s l i g h t l y a n d
i f t h e p a t i e n t r e l a x e s h e r s h o u l der- b l a d e s . she fee l s
s o m e t e n s i o n a t t h e s i t e ( t h e s l ack is b e i ng t a k en u p ) .
S h e now b r e a t h e s i n t o t h ose r i b s . s e p a ra t i n g the m
d u ri n g i n h a la t i o n .
The
her
Retroflex i o n self- m o b i l ization o f t h e
u p p e r thoracic s p i n e a n d t h e
cervicothoracic ju nction ( Figure 6.64)
The p a t i e n t i s seated, h e r back s u pported by t h e
chai r-back a t t h e l e ve l o f the lower ve rtebra ( s p i n o u s
process) of t h e se g m e n t to be t reate d . S h e now s h i f t s
her h e a d a n d sp i n e backwards, so as to take up t h e
Self- m o b i l ization of the fi rst rib
Th is corresponds to t h e te c h n i q u e d e s c r i b e d above
( s e e F i g u re 6.49, p . 1 88 ) ; the p a t i e n t si m pl y uses her
o w n arm, r e s is t i n g w i t h head and neck the r h y t h m ­
i c a .l i m p u lses gi v e n by h e r h a n d .
Retroflexion a n d rotation self­
m o b i l izatio n of the cervical spi n e
(Figure 6.66)
With t h e u l n a r s u rface o f bo t h h a n d s the p a t i ent
fixes the lower v e r te b r a o f t h e segment to be t re a te d .
Now she ei t h e r s h ifts h e r head back s o as to t a k e up
t h e slack a n d t h e n springs the segme n t i n to retro­
flexion by a small rep e t i t i v e m o v e m e n t (see a l s o
Ret roflexi o n sel f-mobi l iza tion of t h e u p p e r thoracic
spine a n d cervicot horacic j u n c t i o n ) ; or she r o t a t e s
h e r h e a d to take u p the slack and then makes
rhyth m ica l ro ta t i o n movements springing ( m o b i l iz ­
i n g ) the segme n t i n to rotatio n . Instead of s p r i n g i n g
the segment i nto rotatio n , s h e may ( a ft e r ta k i n g u p
the slack) l o o k u p , br e a t h i n g i n slowly, a n d then l o o k
t o t h e s i d e o f t h e desired mobilization w h i l e s l o w ly
b r e a t h i n g o u t , a u t o m a t i c a l l y i ncreasing the r a n ge of
r o t a t i o n . The e x e r c i s e is re p e a t e d t h r e e t i m e s .
S ide-be n d i n g self- m o b i lization of the
cervica l spine ( Fi g u re s 6.67, 6.68)
p a t i e n t m a y place the p a l m of h e r h a n d aga i nst
t h e side of h e r n e c k , so t h a t t h e thumb is s u p p o r t e d
by the clavicle a n d t h e u l n a r s u rface forms a fulcrum
a t t b e transverse process of the lower v e r t e b ra o f
t h e affected segm e n t , u s i ng h e r o t h e r h a n d to bend
the h e a d to t h a t side to take u p the slack ( F ig u re
6.67), a tec h n ique that is only s u i ta b l e for se gm e n t s
C l -2 a n d C2-3 . A l te r n a ti v e l y , she may p u t h er t h i r d
The
Figure 6.63 I n h a la t i o n se l f- m o b i l ization o f t h e right
u p pe r ribs
Copyrighted Material
1 98
Maniplila/ive Th erapy in Rehabili/a/ion of /he Lucom u/or S vs/em
Figure 6.64 A n t e · a n d r e t r o fl e x i o n s e l f- m o b i l iza t i o n of t h e u p p e r t h o r a c i c s p i n e a n d t h e c e r v i c o t h o r a c i c j u n c t i o n . t h e
s e a t e d o n a ch a i r w i t h t h e back s u p p orted a t t h e l o w e r v e r t e b r a o f t h e a ffe cted seg m e n t : t h e h e a d a n d t h e
s p i n a l co l u m n a re s h i fted (0) fo r w a r d s a n d (/J) backwa rds
pa t i e n t
a n d fo u r t h fi n ge r s r o u n d h e r n e c k from b e h i n d .
fi x i ng t h e a r c h o f t h e l o w e r v e r t e bra o f t h e s e g m e n t :
w i t h t h e o t he r h a n d p a s s i ng o v e r t h e c rown o f h e r
head she pulls
i t away
fro m t h a t s i d e . o v e r t h e
fu l c r u m fo r m e d b y he r fi n g e rs, t o t a k e u p t h e s l a c k
( Fi g u re 6.68) .
I n b o t h pos i t i o n s P I R i s n o w a p p l i e d . m a k i n g u s e
of
the
p ri n c i p l e
of
a l te rn a t i ng
inh i b i t i o n d u r i n g i n h a l a t i o n a n d
faci l i t a t i o n
and
exha l a tion ( see p.
1 89 ) . W h e n t re a t i n g an even s e gm e n t t h e p a t ie n t
fi rst l oo k s u p a n d b r e a t h e s i n s l o w l y . holds h e r
b re a t h , a n d t h e n re l a x e s w h i l e l o o k i n g d o w n a n d
bre a t h i n g o u t . F o r a n odd segm e n t s h e b eg i n s b y
b r e a t h i n g o u t s l o w l y . re l a x a t i o n ta k i n g p l a c e d u r i n g
i n h a la t i o n . T h e e x e rcise is r e p e a t e d t h ree t i m e s : c a re
m u s t be t a k e n t h a t s i d e - b e n d i ng is p e rfo r m e d s t r i c t l y
i n t h e c o ro n a l p l a n e . With h e r fi n gers rou n d h e r
n e c k t h e pa t i e n t m a y a c h i e ve good fi x a t i o n d o w n to
C5 , or to C6 if her n e c k i s s l e n der. T h e fi n g e r s s h o u l d
go round
the
posterior
arch
from
behind
one
tra nsverse process to t h e n ex t .
Ante- a n d retrofl exio n self- m o b i l i zati o n
between occiput a n d atlas ( F i g u re 6 . 69 )
Th e p a t i e n t t u rns h e r h e a d s o as t o l ock t h e a t l a s/axis.
Figure 6.65 R o t a t i o n
sel f- m o b i l iza t i o n
at the
c c r v i co t h o r a c i c j u n c t i o n . b y a c o m b i n a t i o n o f rh y t h m i c
rota t i on o f t h e a r m s i n o p p o s i t e d i r e c t i o n s . w i t h t h e
s pre a d . a n d h e a d rota t i o n i n t h e d i rec t i o n o f t h e
p ro n a t e d a rm
tl n gers
To m o b i l i ze i n t o a n te A e x i o n . s h e
take
nose .
u p the
sl a c k . b re a t h i n g out
p u l l s her ch i n in to
sha rply t h rough t h e
looking down. a n d m a k i ng
i n t o a n te Ae x i o n
a
b r i s k m ove m e n t
a t the s a m e t i m e . To m o b i l i z e i n to
re troflex i o n s h e l i ft s he r ch i n to t a k e u p t h e s l a c k .
Copyrighted Material
TherapCUlie lecl1l1iqucs
Figure 6.66 R h y t h m i c re pe t i t i v e se l f- m ob i l i z a t i o n o f t h e c e r v i c a l s p i n e , w i t h t h e
u l n a r c d ge of
both h a n ds: ( a )
fo rwa rd s h i ft ; ( i» ba c k w a rd s h i ft : ( e ) ro t a t i o n
the upper
s p i n e : w h i l e o n e h a n d s i u e - b e n d s t h e head to t h e
o p p o s i t e side, t h e o t h e r fi x e s t h e t r a nsve rse p rocess o f
t h e l ower v e rt e bra o f t h e t r e a t e d seg m e n t
Figure 6.67 S i d e - b e n d i ng s e l l'- m o b i l i z a t i o n o f
cerv i c a l
arch o f t h e l o w e r
v e r tebra
.1 99
fixed by t h e
Figure 6.68 S i d e - b e n d i n g se l f- m o b i l i z a t i o n o f t h e m i d ­
h a n d fi x e s t h e ve r t e b r a l
a rc h w h i l e t h e o t ll e r r e a c h e s o v e r t h e c r o w n to b e n d the
h e a d s i d e ways
a n d lowe r ce rv i c a l spi n e : o n e
Copyrighted Material
2 00
Manip u / a r i v f Th e rojJ v in Rehabilira rioll of r h e L o mrn o r o r Svsrnll
Figure 6.70 Sc: l f- m o b i l i za t i o n o r t h e e l bow i n
d i re c t i o n
a
rad i a l
Self- m o b iliza tio n o f th e e lb o w i n a ra dial
dire ctio n ( Fi g u re 6 . 70 )
T h e p a ti e n t grasps t h e e dge o f a t a b l e , w i t h t h e
stretched
in
supination
that
so
the
arm
thumb
l ies
p a r a l l e l w i th t h e e d ge of t h e t a b l e . T h e o t h e r h a n d
grasps
the
elbow
fro m
the
u l n a r side,
ga p p i n g
( m o b i l i z i n g ) i t by r e p e a t e d r h y t h m i c a l p r e s s u r e o r
by a fa s t s h a k i n g m o v e m e n t i n a r a d i a l d i r ec t i o n .
Figure 6.69 S e l f- m o b i l iza t i o n b e tween a t l a s and o cc i p u t
w i t h t h e h e a d r o t a t e d ( a ) i n t o a n t e fl e x i o n a n d (b) i n to
r e t r o fl e x i on
Mob iliza tio n o f o n e c a rp a l b o n e against th e
n ex t ( Fi gure 6 . 7 1 ; see a l so Figure 6 . S b , p. 1 64 )
The tip o f the t h u m b is p l a c e d o n o n e c a r p a l b o n e
l o o ks up a n d b re a t h e s in s h a r p l y , m a k i n g a b r i s k b u t
( e . g . the os ca p i ta t u m ) a n d the t i p o f the fo reflnger
s l igh t
on
m o v e m e n t i n t o r e t r o fl e x io n . Ca re m u s t be
taken n o t to move the c e r v i c a l sp i n e b e l ow the a x i s .
i ts n e i g h b o u r
s m a l l s h i ft
Latera l flexi o n self- m o b i l i z a t i o n between
occ i p u t and a t l a s
(in
this
case
t he
os l u n a t u m ) ,
prod uci n g a s lig h t s h e a r i n g p r e ss u r e re s u l t i ng i n a
( Fi g u re 6 . 7 1 a ) .
I f tile fi n g e rs c h ange
p osi t i o n , the s h ift w i l l t a k e p l a c e i n i h e oppo s i te
d i recti o n . P a t i e n ts w h o fi n d th i s too d i ffi c u l t m a y use
a s i m p l e t r a c t i o n t e c h n i q u e : the r a ti e n t fi x e s her
T h e b e s t t ec h n i q u e i s i d e n t i c a l to g ra v i ty- i n d u ce d
fo re a r m aga i n s t her k n e e , w h i le her o t h e r h a n d
PIR o f t h e s t e r n o c le i d o m a s t o i d m u sc l e ( s e e Fig u r e
grasps t h e carpa l (or
6.96).
w i s h es to t r e a t , b e tw e e n h e r t h u m b a n d fo refinge r
even
m e ta c a r p a l ) b o n e s h e
(Fi gure 6 . 7 1 b ) .
S e l f- m o b i l i z ati o n o f t h e ext r e m ity j o i n ts
O b v i o u s l y , se l f-trea t m e n t c a n a l s o b e a p p l i e d to t h e
e x t rem i t y j o i n t s . T h i s i s p a r t i c u l a rl y t r u e fo r t h e
lower e x t r e m i t i e s , b ec a u se
the
p a ti e n t
has
both
Tra ctio n o f th e fin g e rs, i n c l u ding th e first
m e ta ca rpa l
T h e d i s t a l p h a l a n x is gras p e d by t h e l i t t l e fi n ge r
the other hand, w h i le
h a n d s f r e e . I t h e r e fo r e d e a l o n l y w i t h a fe w i n s t a nces
of
o f t re a t m e n t of t h e u p per e x t re m i ty j o i n t s .
fll1 g e r grasp
Copyrighted Material
the
first
the
phalanx
t h u m b a n d fore­
the m e t a ca r p a l
or
Th erapeutic tech niq ues
20I
F u n cti o n a l tech n i q u es
( a)
( b)
Figure 6.71 ( a) S h e a r i n g se l f- m o b i l i z a t ion of c a r p a l
b o n e s , u s i ng th u m b a n d fo re fi n g e r . ( b ) S e l f - t re a t me n t o f
the c a r p a l bones using traction
of the th u m b . Traction a n d even m o b i l ization can
be ap p l ied to t h e metaca rpophalangeal joints a n d
t h e ca rpometaca rpa l j o i n t of the t h u m b (see Figure
6.2).
Self-applied traction a t th e shou lder
This can b e performed over the padded back of a
c h a i r , prefera b l y by the tech n i q u e of isometric
tract i o n a nd r e l a x a t i o n , t h e o t h e r h a n d grasping
t h e a rm a b ove the e l bow . The patient resists h e r
o w n (slight) t r a c t i o n a nd bre a t hes i n aga i n s t t h e
b a c k o f t h e c h a i r ; she t h e n rel axes and breathes
o u t , d i strac t i o n r e s u l t i n g from re l a x a t i o n (see Figure
6.9).
Two very gentle a nd s u rprisi ngl y e ffective tec h n i q ues
of (oste o p a t h ic) ' i n d i rect' m a n i pu l a t i o n s h o u l d b e
m e n t i o n e d . Their popu l a rity i s l i ke l y to i ncrease i n
fu ture. The t e r m ' i n d i rect' mea n s that, u n l i k e tech­
n iq ues described so fa r, the p a t h o logical (restrictive)
ba rri e r i s e ngaged n e i t h e r fo r d i agnosis n o r i n order
to obta i n re lease. T h e fi rs t of these techn iq u e s has
b e e n termed 'functio n a l ' . T h i s method a t t e m p ts to
fi n d a re l i e f posi t i o n in w h i c h p a t h o l ogica l te nsion
( a nd pain) is re l ieved a nd to o b ta i n good re l a x a ti o n
i n t h i s positi o n . Once this is fo u n d a n d re lease i s
obta i n e d ten s i o n ( te n derness) gra d u a l l y n o r m a lizes
i n every pos i t i o n .
T h i s m e t h o d i s b a s e d s o l e l y on p a l p a t i o n a n d
t herefore i t is d i fficu l t t o present let a lo n e i l l ustrate
i n a textbook. A t best this is a n a t t e m p t to give an
idea of what s h o u l d b e a c h i e v e d by the m e t h o d .
At palpa tory e x a m i n a t i o n o f t h e l e s i o n e d segme n t
w i t h t h e patient seated, t h e t h u m b a n d t h e fore finger
o n both sides of t h e spinous process, i ncreased
tension is fe l t o n one side, described as rota t i o n
( G re e n m a n ) ( p a l p a tory i ll usion ow ing to one-sided
m uscul a r spasm). I n de e d , one of t h e fi n gers se nses
p ro m i n e n ce and t h e other a groove . O n b e n d i n g
forward, backward, to t h e s i d e s a nd possibly a t
rotati o n , t h e exa m i n e r fee l s that i n some pos i t i o n s
this a s y m m e try i n creases, i n o t h e rs i t d i s a p p e a rs . W e
h a v e to b e a r i n m i n d t h a t i f t h e p a t i e n t side-bends
t h e joint o n t h e side o f l a t e roflexion moves i n to
extension a n d t h a t on t h e opposi te s i d e i n to fl e x i o n
(see F i g u r e 4.4), ow i ng to coupled movem e n t ; t h i s
i s a lso true f o r rota t i o n .
H a v i n g localized t h e a s y m m e t r i ca l , lesioned
segm e n t with t h e patie n t seated , both h a nds clasped
beh i nd her neck, the e x a m i n e r grasps bo t h h e r arms
a bove t h e elbows (see Figure s 4. 1 6, 4 . 1 7 ) a n d first
bri ngs t h e patient i n to t h e position i n w h i ch asym­
m e try d i m i n ishes. Th is u s u a l l y h a ppens either in
flex i o n or e x t e n s i o n . In t h e l a t te r , side-flexion to t h e
side of spasm is a d d e d , a s i n t h i s c a s e side flexion
a m o unts to furth e r exte n s i o n . I f i n this way good
rel a x a t i o n a n d s y m metrical te n s i o n i s a c h i e v e d , t h e
exa m i n e r first supports t h e patie n t i n this position
to e n h a nce relaxatio n . Wi t h the patient well relaxed,
h e now slowly reduces back- a n d side-fle x i o n ,
re turn i n g i n to re l ie f position t h e m om e n t te n s i o n
reappears, re peating t h e m a n o e u vre u n t i l n o m o re
asym metry recurs. Then he moves fu r t h e r i n to
a n teflexion u n t i l he notices t h a t fu l l flexion a n d side­
b e n d ing to t h e opposite side n o l onger creates
tension or tenderness, i . e . fu l l re lease is obta i ned.
I f , on the o t h e r hand, symme try i s obta i ne d i n
flex i o n , t h e exa m i ne r moves the patie n t i n to side­
fle x i o n to t h e opposi t e side of spasm (of ' rota t i o n ' ) ,
support i n g h e r i n t h i s r e l i e f positi o n , a n d t h e n
proceeds grad u a l ly as described fo r re trofle x i o n .
I n t h e cerv ica l s p i n e the tech n i qu e is simi l a r . T h e
Copyrighted Material
Copyrighted Material
Therap eulie lechniques
203
of re l e a s e we m a y c h a n ge b o t h t h e i n t e n s i t y a n d t h e
d i rect i o n
of
p ress u re ( p u l l )
to
a c h i e v e b e t t e r re s u l ts .
I t mus t n o t be fo rce d , a n d t h e p <l t i e n t
fe e l
s h o u ld
neve r
pa i n .
S k i n stretc h i n g
As
explained
in Chapter
4 (p. 86),
a n a re a
of
the
before
s k i n m a y b e h e l d b e twee n t h e fi nge r t i ps or w i t h the
aspect of the c rossed h a n d s , from the l i t t l e
fi n ge r to t h e wrist ( a ccord i n g t o t h e size of t h e a re a
i n v o l ve d ) , a n d s t r e t c h e d w i t h a m i n i m u m o f force ,
so as to ta k e up t h e s l ac k . On f u r t h e r s t re tc h i n g a
s p r i n g i n g resi sta nce is fe l t . I f t h e r e is a h y pera l ge s i c
z o n e ( H A Z) , t he s l a c k is t a k e n u p soon e r a n d t h e re
is m u c h less s p r i n g . I f t h e t h e ra p i s t t h e n h o l d s t he
sk.i n i n t h is end -posi t i o n , res i s t a n c e w e a k e n s u n ti l
ul n a r
( a)
nor m a l s p r i n g i n g i s restored ( Fi g u re 6.72) . T h e H A Z
usua l l y n o l o n g e r d e t e c t a b l e . I f t h e H A Z i s a c a u s e
of pain, t h i s stre t c h i n g m e t hod is q u i te a s effe c t i v e
as ne e d l i ng, e l e c t r os t i m u l a t i o n a n d s i m i l a r t r e a t m e n t .
Moreove r , i t is e n t i re l y p a i n less a nd c a n b e us e d by
is
the pa t i e n t h e rse l f.
I f t h e a re a
is
m a r k ed o n t h e s k i n , t h e e f fe c t
tre a t m e n t can b e m e asure d ;
co m m u n i c a t i o n ,
M.
of
B e rg e r ( pe r s o n a l
1 982) h a s c o n s t r u c t e d a n e l e c t r i c a l
i n s t r u m e n t t h a t s t re t c h e s t h e s k i n r h y t h m i c a l l y w i t h
a c o n st a n t
after
( b)
6.73 D e r m a tote n s i og r a m recorded by Berge r
com m u n i c a t i o n ) : ( a ) be fore s k i n s t retc h i ng.
poor e l a s t i c i t y : (b) i n c r e a s e d ( n o r m a l ) e l a s t i c i t y a ft e r
Figure
( p erso n a l
st retching
c a n b e reco r d e d ( F i g u re 6 . 7 3 ) .
S t re t c h i n g i s partic u l a r l y u s e fu l i n s m a l l areas
where i t is d i fficul t to fold t h e s k i n , a s b e t w e e n t h e
fi n g e rs o r toes i n root synd romes i f t h e re i s a n H A Z .
S k in s t r e t c h i n g i s a lso very u s e f u l a c ro s s t h e c a r p a l
Fo lds of soft c o n n e c t i v e tiss u e me t a k e n be tw e e n
tunnel.
t h e t h u m b a n d fore fi n g e r
force t h a t
Stretching a connective tissue fold ( F igure 6 . 74)
way
of the two h a nds;
in this
p u l l o r s t r e tc h i s p roduced a n d t h e s l a c k i s t a k e n
o n l y to s t re t c h . n e v e r t o
secon d s r e s i s t a nce g i v e s a n d t h e
tiss u e fo ld s t re tc h e s un t i l a n e w ba r r i e r is reached
a n d n o r m a .1 springing i s re s to r e d . This t e c h n i q ue c a n
b e a p p l ied to subcut a n e o u s t i s s u e a n d t o active s c a r s
w i th t e n d e r p o i n t s and s u rroun d e d by a n HA Z . I t
u p . C a re m us t b e t a k e n
p i n c h . A ft e r
a
few
c a n a l s o b e u s e d f o r s h o r t ( t aut) musc l e s . I n t h e c a s e
o f a l a rge m u s c l e
such as
t h e h a m s tri ngs , t h e
prod u c e d b e t w e e n t h e p a l m o f o n e
fi n gers
of
of
the o t h e r . Th i s
obta i n i ng
m u sc l e
is
hand
fold
is
a n d the
the most effe c t i v e way
stretch
while avoiding
the
s t re tc h r e fl e x (Fi g u re 6.74 ) .
Pressure
If a
fo l d c a n not
with a
e x e rted
b e fo rm e d . s l ig h t pre s s u r e m a y be
finger
(Figure
6.75).
With
l i ttle
p re s s u r e t h e s l a c k i s fi rs t ta k e n u p , a n d a ft e r a s h o r t
l a te n cy
period
t h e fi n g e r s i n k s i n t o t h e d e e p l a ye rs
is r e a c h e d . T h i s is m o s t e ffe c t i ve
s u pe r fi c i a l m u sc l e s i n c l u d i ng t h e e re c t o r s p i n a e
a n d t h e g l u t e u s m a x i m u s ; i t c a n a lso b e a p p l ied by
u n t i l a n e w ba r r i e r
in
a p i nce r m o ve m e n t i n m u s c l e s in w h i c h TrPs a r e
d i a g n o s e d i n t h i s w a y , a s in t h e tra p e z i u s
Figure 6.72 S k i n
st r e t c h i ng
sternoc l ei d o m a s t oid .
Copyrighted Material
and t h e
deep
I t i s a l so u s e f u l i n t re a ti ng
204
Mal l ipula l i ve Th erapy
in
Rehab ililalion of lhe Locomolar
5yslem
figure 6.76 St retch i n g ( s h i ft i n g) t h e g l u t e a l fascia
is u s u a l ly a p p l i e d . The rh y t h m i s t h e
e v e ry case: fi rs t we t a k e u p t he s l a c k , a n d
a f t e r a f e w s e c o n d s t h e t h e r a p i s t fe e l s t h e b a r r i e r
g i v e : myofasc i a l re l e a s e con t i n u es u n t i l t h e n o r m a l
ba r r i e r is re a c h e d . M a n y o f these tech niq ues h a v e
b e e n e l a borated by R. W a rd ( p e r s o n a l c o m m u n i ­
c a tion , 1989) . Som e a re desc r i b e d i n d e t a il b e l o w .
a n d s t retch i n g
sa me in
Figure 6.74 Fo l d i ng connective t i s s u e
Shifting (stretching) the deep gluteal fascia
from abo ve
Figure 6.75 Pressing d e e p soft t i s s u e s
scars w h e re i t i s i m p os s i b l e to fo r m a skin fol d .
Pressure o n m u scles appears t o h a v e a n i n h i b I tor y ,
relaxing e ffect a n d is a n a l te r n a tive to PI R .
S h ifti ng (stretch i n g ) deep fasciae
The m o s t i m p o r t a n t function restored by soft t i ss u e
m a n i p u l a t i o n appears to be t h a t of m o b i l. i ty of t h e
fasc i a e ; t h i s is bound up w i t h t a u t nes s ( s h o r t e n i n g )
o f the m uscles, esta b l i s hed o nly a ft e r ca refu l d iag­
nosis o f res t rict i o n . Ch a n ge s i n the fa sciae a re most
ch a r a c t e r i s t i c i n t h e c h r o n i c s t a ge ; i t i s i m p ort a n t to
k n ow t h a t the restricted s i d e need not be the side
w h e re pa i n is fe l t . However, i t i s t h e a s y m m e t ry
w h i c h is c h a racteri s tic ( t h e ' t ight-loose complex ' ) .
F o r t re a t m e n t o f fa sc i a e a com b i n a t i o n o f s h i f t i n g
T h e t h e rapi s t s t a n d s a t t h e side to be treated; t h e
p a t i e n t i s p r o n e , her fe e t o v e r t h e end of t h e t a b l e .
He p u ts s li gh t p ress ure aga i nst t h e m a s s o f t h e gl u t e i
f r om abov e , and some p re s s u r e i n t h e t h o r a co l u m ­
b a r area w i t h t h e o t h e r h a nd . T h e patient i s n o w t o l d
to p r e s s her to e s upwa rd aga i n s t t h e edge o f the
t a b l e (on the t r e a t e d s i d e ) a n d t o stretc h t h a t a r m
above her h e a d , w i t h fi n g e r s exte n d ed ; s h e m u s t l oo k
towards t h e t h e r a p i s t a n d b re a t h e o u t . t o i n c r e a s e
tension ( ex h a l a tion i n c r ea s e s tension in this situ­
a tion , as in isometric l u m ba r t racti o n ) . T h e n s h e i s
told to b r e a t he i n s l ow l y : d ur i ng i n h a l a t i o n , resista nce
s l a c k e n s and reJease occ u rs . T h i s m a n oe u v re i s
re p e a t e d t w o or t h ree t i mes. I f there is no s a t i s ­
factory release, the p a t i e n t s h o u l d be told to c o u g h
occa s io n a l ly a f t e r i n h a l a ti o n . A f t e r t re a t m e n t , w h ic h
should be a g re e ab l e to t h e p a t i e n t , t h e s k i n is o f t e n
flushed (Figure 6.76) .
The gluteals c a n also be s h i fted from be low, and
o n the re s t ric t e d s i d e r e l e a s e can be o b ta i n e d a ft e r
e ngagi ng t h e barrier. H e re b re a t h i n g in or o u t has
little e ffe ct. M e r e p r e ss u r e where m a x i m u m h y p e r ­
to n u s is fe l t h a s a s i m i l a r e f fect.
Shifting the lumb odorsa l fascia upwards
The p a t i e n t t a k e s the
same p os i t i o n as above: the
t issues of t h e t h orax i n a
c r a n i a l d i recti o n with one h a n d , w h i l e t h e o t he r
a p p l i e s pressu r e i n t he l u m b a r regi o n . The p a t i e n t
is told to breathe i n , to h o l d h e r brea t h , a n d t h e n
to b r e a t h e o u t : re lease occu rs d u r i n g e x h a l a t i o n .
t h e r a p is t s h i fts t h e soft
Copyrighted Material
Therapelltic techn iques
Figure 6.77 Stretching
the s h o u l d e r- o l a cle
(sh i fting)
t h e dorsal fa scia
205
over
Figure 6.79 S t retch i n g ( s h i ft i n g ) the fascia over the
l a t e r a l a s pect of t h e tru n k
e x a m i n e a n d t o t r e a t t h i s cond i t i o n . t h e t h e r a p i s t
F i g u r e 6 . 7 8 S t retch i n g ( s h i rt i n g) t h e e10rsa l fasc i a e
s t a n d s be h i n d t h e se a t e d p a t i e n t , s l i g h t l y to t h e s i d e
t ra n s v e rs e l y
sid e - b e n d i n g m u s t
which
to
p il t i e n t p u ts h e r
arm
be
p e r fo r m e d .
The
over her head, with the hand
Aga i n . i f re le a s e i s n o t s a t i s fa c t o r y . a s li g h t c o u g h
a t t h e n a pe o f t h e n e c k . o n t h e s i d e w h i c h i s to
w i l l i m p rove i t ( F i g u re
s t re tc h e d Th e t h e r a p i s t g r a s p s
6 . 77 ) .
.
t he
e l bow w i t h
be
one
h a n d w h i l e t h e o t h e r fix e s t h e p a t i e n t ' s h i p f r o m
a b o v e . He b e n d s her si d e w a y s over h i s own t h i g h s o
Sh ifting the tissues from side to s ide in
ilS
opp osite directions
F i r s t we co m p are the
to t a k e u p t h e s l a c k . H e
t e l l s t he p a t i e n t to
re s i s t a n c e)
then
look up and b r e a t h e i n ( w h ich i n c re a s e s
degree o f s h i ft
a t ta i n a b l e in t h e
so ft t i s s u e s ; w i t h aile h a n d a t the l e v e l o f t h e s h o u lde r
­
b l ades a n d t h e o t h e r a t t h e w a i s t . w i t h the pa t i e n t
to h o l d h e r b re a t h , a n d t h e n to
re lax
.
a nd
brea the
o u t , t o o b ta i n re l e a s e . T h i s i s repe a t e d t w o o r t h re e
ti m es (Figure 6.79) .
p ro n e , we m o v e t h e h a n d s i n o p p o s i t e d i re c t i o n s , a n d
com p a re res i s t a n c e . If t he r e i s a n y d i ffe r e n c e , t h e
d irec t i o n o f r e s t r i c te d m o t i o n i s t r e a t e d . T h e p a t i e n t
looks t o w a r d s t h e s i d e
a ll
w h i c h s h i ft i s r e s t r i c ted i n
t h e t h o r a c i c reg i o n , w h i l e
fi n g e rs , a n d
stretc h i n g
b re a t h e i n . t o hold her b re il t h ,
slo w l y .
that arm a nd
r a i s e s t h e t o e s . S h e the n i s t o l d
A ga i n ,
i f re l e a s e
occa s i o n a l c o u g h m a y
be
is
to
a n d to breathe
out
sa tisfactory,
an
not
h e l p fu l
Treatmen t of fasciae on the ven tral aspect o f
the tru n k
W i t h t he p a t i e n t s u p i n e w e c a n s h i ft t h e m a s s o f t h e
pectora l is f r o m t h e s i d e a n d c o m p a re t h e tw o s i d e s .
Restriction
on
one
side
ca n
be
tre a te d
d i r e c t i o n o f i n c re a s e d resi s t a n c e , s i m pl y
in
the
by e n g a g i n g
t h e b a r r ier a n d J e tt i n g t h e pa t i e n t b r e a t h e i n s l o w l y ,
(Fig u re 6.78).
h o l d h e r bre a t h , a n d the n
taken that our
Stretch ing the tissues on both sides of th e
but
trun k
fi n ge r s
b re a t h e
O Ll t . Ca re m u s t b e
do n o t p o k e
the p il t i e n t ' s r i b s
g l i d e a s o n t h e s u r f a ce o f a b a rre l . Re s t r i c t i o n
t h e re is fre q u e n t l y l i n k ed w i t h TrPs of t h e s u bsca p u ­
R e s t r i c t i o n m a y a f fe c t b o t h s i d es o f t h e t r u n k . i n
l a ri s , t h e p a t ie n t c o m p l a i n i ng of c h e s t a n d ( w o m e n )
w h ich c a s e t h e re i s re s t r i c t i o n a t s i d e - be n d i n g. T o
of b r e a s t p a i n
Copyrighted Material
.
206
Manipulative Th erapy ill
Rehabilitation of the Locomotor System
I n cases of deep p e l v i c or perinea l p a i n . s h i ft i n g
o f soft tissues ove r t h e e d ges o f t h e p u b ic b o n e m a y
be i m p a i red o n o n e s i d e ; to restore m o b i l i t y we
e n gage t h e barrier so as to obta i n re lease, w h i c h
fo l l ows a fter a s h o rt l a tency per i o d .
The sca l p
W i th t h e pati e n t s i t t i ng, we ca n e x a m i n e mobi l i t y o f
t h e sc a l p i n re lation to the s k u l l , i n a l l d i rect i o n s ,
a n d compa re t h e t w o sides. One o r two fi ngers (or
t h e t h u m b ) a re s u fficie n t to e ngage t h e restricted
b a rr i e r , a n d afte r t h e typica l l a te n cy p e r i od re l e ase
fo l l ows, u n til n o r m a l mobi l i ty i s restored . The
t h e ra p i s t uses h i s free h a n d t o fix the p a t i e n t 's h e a d .
C a r e m u s t be t a k e n not to l e t t h e fi n gers s l i p over
t h e patie n t ' s h a i r. Res t r icted m o b i l i t y o f the sca l p i s
a v e r y i m po rta n t fi n d i n g i n p a t i e n ts w i t h h eadache
a n d/or v e r t igo a n d s h o u l d never be m i ss e d .
The neck a n d t h e extre m ities
A t t h e neck a n d the e x t re m i ties t h e re is gre a t
m o b i l ity of the s o ft tissues. i f w e a p p ly rota t i o n a l
m o ve m e n t around t h e i r l o ng a x i s . At t h e extremi ties
and even at the cervicothoracic j u n c t i o n we can
e i t he r move the w h o l e mass of so ft tissue in one
d i rection. or twist one hand aga i nst the o t h e r , as
w h e n wri ngi ng a cl oth. A t the n e c k we m a y rotate
soft tissues i n the d i rection o f t h e t h u m b o r o u r
fi ngers. I n t h e fo rmer case w e c a n act o n l y u p o n a
n a rrow strip, i n the latter u pon the grea te r p a r t o f
t h e n e c k . as o u r d i a gnosis req u i res. The importa n t
poi n t is h o w best to iden ti fy a n d e n gage a
p a t h ological barrier, a n d t h e n to obta i n re l e a s e . A
typical barrier is regu l a r l y fou n d i n the soft tissue
close to periost e a l pain p o i n ts (m astoid processes,
e p i c o nd y l e s . wrists, ro u n d the k n ees and a n kles ) .
T h e a n a l gesic e ffec t o f norma l iz i n g s u c h a barr i e r i s
most rewa rd i n g . A t the neck, norm a l i za tion o f soft
tissue m o b i l i t y can gre a t l y increase t h e range of
ce rvical motion w h e re restri ction i s u s u a l l y
a t t r i b u ted to j oi n t d y s f u n c t i o n ( Figu re 6.80 ) .
Figure 6.80 Rot a t ion of s o rt l i ssues rou n d t he neck for
t re a t m e n t of re s t r i c t e d mobi l i t y
the s o ft tissue p a d on t h e p l a n t a r s u r face o r t h e heel
is n o t re a d i ly s h i fted on one s i d e . The t h e rapist then
app l i es s o ft tissue m a n i p u l a t i o n by p ressi ng with h i s
fi ngers o r t h u m b s i n the rest ricted d i rect ion ( Fi g u re
6 . 8 1 ) . I n cases of p a i n fu l A c h i lles t e n d o n (see p. 235 )
and p a i n a t i ts a t t a c h m e n t po i n t . we a l so freq u e n tl y
fi n d tenderness i n t h e soft tissue b e t w e e n t he t e n d o n
a n d the bones. I n such cases t h e t i ssue must be
s t retched betwee n two fi ngers; if t h e re is i n creased
resista nce t he t i ssue must be held i ll s t re t c h u n t i l
rel e ase occurs ( Fi g u re 6.82 ) .
S o m e speci a l soft tiss u e tech n iq u es
I n root s y n d romes rad i a t i ng to t h e toes a n d fi n gers
t h e re i s not o n l y a n HAZ a t the s k i n fol d between
the t oes ( fi ngers ) , but as a r u l e t h e re i s also i ncreased
resistance ( ' b i n d ' ) i f we t r y to move one m e tacarpa l /
ta rsa l b o n e aga i ns t t h e n e x t , i n a d o rsopl a n t a r
d i rection , i n t h e a ffected segme n t . I n s u c h a case i t
i s most e ffec t i v e t o e ngage t h e barr i e r i n a p i n c e r
move m e n t , w i t h b o t h t h umbs o n one metatarsal a n d
both fore fingers o n t h e o t h e r ; s l ig h t p r e s s u r e is
m a i n t a i n e d u n t i l re l e ase is fel t . We t h e n c h a nge the
t h u m b a n d fo refi ngers over, to restore mobi l i t y in
t h e opposite d i rectio n .
[ n cases o f pa i n fu l c a l c a ne a l s p u r we may fi n d t h a t
Figure 6.IH S h i ft i ng s o ft t i s s u e s a t t h e h e e l p a d
Copyrighted Material
Th erapeutic techniq ues
207
Figure 6.83 Exa m i n a t i o n ( t re a t m e n t ) o f soft t i ssue a t t h e
e p icon dyle
Figure 6.82
tendon
Stre tch i n g
soft tissue b e n e a t h t h e A c h i l l e s
Periostea l poi nts
Eve n a t p e r i o stea l
p o i n t s we can fi n d
pa t h o l ogica l
i n t h e v ic i n i t y of a t t a c h ­
m e n t po i n t s o f t e n d o n s a nd l iga m e n t s , i . e . w h ere
t e n s i o n i s c re a t e d . I f we s h i f t t h e s u b p e r i os t e a l t i s s u e
close t o t h e p a i n p o i n t , w e fi n d t h a t sh i f t i n g i s
r e s t r i c t e d i n a t le a s t o n e d i re c t i o n a n d t h a t t h e re i s
a h a rd ( p a t h o l ogical) b a r r i e r . I t i s , h o w e v e r , n e ce s ­
b a r r i e r s , m o s t fre q u e n t l y
s a ry t o com p a re i t w i t h a s y m m e t ri c a l p a i n l e s s a re a
o n t h e n o n - a ffected s i d e . O n exa m i n a t i o n o f t h e
e p i c o n d y l e s we m a y fi n d i t e a s y to s h i ft soft tissues
i n a l l d i re c t i o n s , b u t n o t , h o w ev e r , i f t h e r e is
( ch r o n i c ) pa i n . I n the d i re c t i o n of res t r i c t i o n we
eng a ge t h e b a r ri e r i n ord e r to obta i n re l ease. As
on l y m i n i m u m force is used t a n ge n ti a l to the p a i n
p o i n t . t h i s te c h n i q u e i s p a i n l es s , u n l i k e pe r i o s t e a l
m a ssage o r d e e p fr ict i o n , y e t q u i t e as e f fec ti v e a n d
e a s i e r to c o n tro l b e c a u s e we k n o w e x a c t l y w h e n the
b a rri e r has been re a c h e d a n d w h e n fu l l release is
ach ieved ( Fi gu r e 6.83 ) .
Wh a t h a s bee n s a i d a bove h o l d s fo r most p e r i o s te a l
p a i n p o i n t s , such a s t h e a n t e r i o r p o s t e r i o r i l i a c s p i n e s ,
t h e pes a n s e ri n u s o n t h e t i b i a e tc . Spe ci a l m e n t i o n ,
h owever, h a s t o b e m a d e o f t h e s p i n o u s p r o c e s s es .
Te n d erness, as a ru l e , is fo u n d at t h e i r t i p ;
h o w e v e r , o n care fu l e x a m i n a t i o n i t i s n e v e r e x a c t l y
i n m i d -l i ne b u t e i t h e r on t h e r i g h t o r t h e l e ft s i d e o f
t h e t i p o f t h e s p i n o u s p r o c e s s . O n t h e te n d e r s i d e
w e t h e n p a l p a t e i ncreased resista nce t o p ress u re
p a r a l le l to t h e sp i n o u s p ro ce s s , i . e . in a ve ntra l
d i re c t i o n . For t r e a tmen t we t h er efor e a p p l y p a r a ­
v e r t e b ra l press u re w i t h o u r fi n g e r t i p : a fte r e n ga gi n g
t h e b a r r i e r w i t h m i n i m u m fo rce, re l e a s e is o b t a i n e d .
Te n d e r s p i n o u s processes a re m o s t freq u e n tly fo u n d
i n y o u n g h y p e r m o b i l e p a t i e n ts , b u t n e v e r w h e n
morph ological c h a n g es l i k e B a a s tr u p ' s p h e n o me n o n
a re p re s e n t i n e l d e r l y p a t i e n ts . A n o t h e r v e ry
fre q u e n t l y te n d e r spi n o u s process is a t t h e a x i s . I t i s
t h e l a t e r a l bord e r w h i c h is t e n d e r a n d t h e r e fo r e o n e
h a s t o s i d e - b e n d t h e p a t i e n t 's h e a d t o t h e n o n ­
p a i n fu l s i d e to fi n d t h e p a i n p o i n t . T h e re we sh i f t
the soft t i ss u e s o v e r l y i n g th e p a i n fu l a re a so as t o
fi n d re s t r ict i o n , co m p a r i n g t h e fi n d i ngs w i t h t h e n o n ­
p a i n f u l s i d e . A fter t a k i n g up t h e s lack i n t h e
re s t r i c t e d d i re c t i o n , re l e ase i s o b t a i n e d .
S elf-treatment
p a t i e n t h ersel f can e a si l y pe rfor m s tr e tc h i n g o f
a n a re a o f s k i n , fo l d i n g o f s u b c u t a n e o u s ti s s u e
i n c l u d i n g a s c a r , o r e v e n s t r e tch i n g of a m u scle b y
t h i s t e c h n iq u e , p rov i d e d t h a t t h e s i te o f t h e lesi o n i s
w i t h i n r e a c h o f her h a n d s . S h i ft i n g ( m ov i n g) t h e sc a l p
a g a i n s t the s k u l l , o r t h e p a d o f s o ft t i s s u e o n t h e
h ee l , s h o u ld prese n t n o p ro b l e m , n o r sh o u l d t w i s ti n g
the soft t i s s u e o n t h e extre m i t i e s ( i n the c a s e o f t he
The
Copyrighted Material
208
Manipulative Therapy in
Rehabilifafion of fhe
LOC0l110fOr Sysfern
Figure 6.85 S e l f- t re a t m e n t o f s h o r t fa sciae
the neck
at
the side of
Figure 6.84 As fo r Fi g u re 6.79: se l f- t re a t m e n t
fo r ge t t h a t t h e
b o d y s u r fa c e i s r i c h l y
en tire
s u pp l i e d
o n e ) . S e l f- t r e a t m e n t o f t h e t r u n k i s
m o re d iffi c u l t , b u t t h e re a r e m a n y s t r e tc h i n g te c h ­
rece p t o r s w h ich a re m o s t l y d e p r i ve d o f n a t u ra l
s t i m u l i b y c l o t h i n g a n d s h oe s . T h e reg i o n s m o s t
n i ques d es c r i b e d i n t h e li tera ture ( A n d e r s o n 1 980) .
N e v e r t h e l e ss a few t e c h n i q u e s a re prese nted h e r e .
To stretch t h e fa sc i a o n o n e s i d e o f t h e t r u n k , t h e
p a ti e n t s t a n d s w i t h h e r legs a p a rt a n d p uts o n e a r m
g e n e r o u s l y re p r es e n te d i n t h e cere b r a l c o r t e x are t h e
fa c e , i n p a r t i c u l a r t h e l i p s t h e hands a n d t h e fe e t
w i t h t h e t h u m b a n d t h e b i g toe .
C l i n ica l d i s t u r b a n c e i n t h e fe e t i s c h a r a c t e r i zed b y
o v er
i n a d e q u a t e re a c t i o n t o m e re s t r o k i n g, w h i c h is
p e rc e i ve d e i t h e r as u n p l e a s a n t e . g . t i c k l i n g o r t h e re
is n e x t to no re a c t i o n t h e fee t g i v i n g t h e i m p r e s s i o n
o f b e i n g ' d e a d ' . The two s i d e s c a n a l s o be asym­
m e t r i ca l . T h e s e c h a n g e s a s a r u l e go hand i n h a n d
w i t h a l te red ton u s o f the soft t i ss ll e s a n d m u s c l e s .
Ch a n ges i n s e n s i b i l i t y a n d to n u s c a n b e t r e a t e d b y
e x t e r oce p t iv e s t i m u l a t i o n s t ro k i n g . A s t h i s m ll s t b e
d o n e re p e a te d l y s e l f- t re a t me n t i s req u i red . Fi r s t
h ow e v e r , t h e t h e r a p i s t m u s t d e c i d e t h e c o r r e c t
i n te n si t y : i t req u i res co n s i de r a b l e experience t o
sense t h is .
S ti m u la ti o n c on s i s t s o f a s t e a d y s m o o t h move me n t
o f t h e r e l a x e d a n d s e n s i n g h a n d i n fu l l co n t a c t w i t h
the b o d y su r fa c e . Not o n l y s y m m e try of p e rce pt i o n
a n d t o n u s i n c l u d i n g tha t o f m u sc l e s i s a c h i e v e d i n
t h i s w a y ; b o t h h y po t o n u s a nd i n c re a s e d t o n u s a r e
co r r e cted as n o r m a l iza t i o n i s a c h i e ve d .
F o r se l f· t re a t m e n t t he p a t i e n t uses h i s h a n d s o r
d r y r o u gh face fl a n n e ls. We do n o t encou rage b r u s h e s
or m a s s a ge fl a n n e l s . Fo r sel F- t r e a t m e n t of t h e h a n d s
w e re c o m m e n d a d i s h o f r i ce o r l e n t i l s i n w h i c h t h e
p a t i e nt m ov e s h e r fi n ge rs, or a s m o o t h s p h e re ( b a l l )
a r m s , usi ng o n l y
,
t h e n grasps the e l b ow
and increas­
i n g t h e p u l l so as to ta k e u p t h e sla c k . L o o ki n g u p ,
s h e b r e a t h e s i n s l ow l y h o l d i n g her bre a t h a n d t h u s
i n c r e 2 s i n g r e s i s t a n c e to s i d e be nd i n g S h e t h e n l o o k s
d o w n w h i l e b re a t h i n g o u t ; s i d e b e n din g s h o u ld
i n crease. Th is is repeate d t h ree t i m e s ( F i g u re 6.84).
T o s t r e t c h t h e fa s c i a a t t h e s i d e o f t h e n e c k , t h e
p a t i e n t si ts a n d s t a b i l i z e s h e r s h o u l d e r b y h o l d i n g
t h e e d g e o f a c h a i r or a b e n c h w i t h h e r b a n e! . The
o t h e r h a n d p a sses over t h e crow n of her head ,
p u l l i n g i t i n to s i d e - I� e x i o n to t a k e u p t h e s l a c k S h e
t h e n l o o k s u p a n d b re a t h e s i n , h o l d s h e r b r e a t h t h u s
i n c r e a s i n g resis t a n c e , a n d t h e n re l a x e s to o b t a i n
r e l e a s e (F i g u re 6 . 8 5 ) .
and
b e hind
h e r head ; she
with her o t h e r h a n d ,
b e n d i ng
s i d ew ay s
,
-
.
-
.
,
Exteroceptive sti m u l at i o n
stro k i n g ( H . H e r m a c h )
So far w e h a v e c o n s i d e re d p r im a r i l y n o c i c e p t i ve and
pro p r ioce p t i v e
a ffe r e n t s . We
s hO U ld . h o w e v e r . n e v e r
with
,
.
Copyrighted Material
.
,
,
-
,
.
Th erapeUlic tech n i q u es
rol led between t h e fi ngers; fo r t h e fe e t a bag fi l l e d
w i t h rou n d pebbles o r wooden b e a d s o n w h ich t h e
pat i e n t ca n s t a n d is usefu l .
Therapy i s t h us a p p l i e d to a re a s o f c h a nged
percept i o n of tact i l e s t i mu l i . I f every stroking by the
thera pist is pe rce ived as u npleasa n t , the patie n t
sho u l d start w i t h se l f- t re a t m e n t ; i t i s t h e n bet ter fo r
her to stro k e herse l f u n t i l s h e c a n tole rate b e i n g
touched by t h e t h e ra p is t .
T h e trea t m e n t chosen d e p e n d s o n a n a l ysis of the
dysfu n c t i o n , i.e. w e start w h e re we expect the most
important l i n k o f the pat hoge n e t i c c h a i n . This can
be a n a rea o f sudden c h a nge (see ' s trati fication
syndrome ' , p . 138). I n genera l , hypotonus is more
l i kely to be the p r i m a ry cause as it is freq u e n t l y com­
pensatory. Hypoto n u s s h o u l d n o t be confused w i t h
re laxation: the fo rmer is fl a b b y , the l a tter wel l sprung.
Com p l i a nce o f the patient i s o f p a r a m o u n t tech n i cal
i m porta nce fo r i n te n s i t y , rhythm and d i recti o n . O u r
aim i s t o a c h ieve e l astici ty w h e re flabbiness i s fou n d ,
o r re lease o f hyperto n u s . M ucb h a s t o b e l e a r n e d by
experience.
The d i rection i n w h ich stro k i ng is carried o u t m u s t
be cons i d e red. M o s t freq uen tly strok ing is d o n e i n
t h e d i rection o f the l o n g a x is o f t h e treated
e x tremities and o f the trunk and neck , i.e. i n t h e
d i rection o f the principa l m usc l e fi b r e s . A t t h e
a b d o m e n , w h e re fi b res fol low d i ffe re n t d i rect i o n s
a n d w h e re peristaltic m o t i o n o f t h e i n te s t i n e s p l a y s
a role , the therapist m u s t fi n d t h e a p propriate
tech n i q u e . If i nc reased sensibil ity is d u e to d i s t u rbed
d iges t i o n the hands have to move i n c i rc l e s . A fter
a bdom i n a l opera t i o ns w i t h lowe red t o n u s of the
abdom i n a l muscles both cra n i ocaud a l a n d transverse,
latero latera l s t ro k i ng is i n d icated . In t h e a x i l l a r a n d
ingu i n a l region w h e re n u merous m u s c l e s cross we
reco m m e n d s t ro k i n g both in t h e d i rection of the
m uscle fi b res a n d i n a perpe n d i c u l a r d i rect i o n .
Active scars surounded by a n H A Z w i t h cha nged
sensib i l i ty and tissue tonus a re i n d icated for this type
of trea tment. I t i s particu l a r l y i m porta n t to give
trea t m e n t to the soles o f t h e fee t if there is i ncreased
or l owered sensibi l i t y - i n order e i t h e r to ' q u i e te n '
them or t o 'wake t he m u p ' . T h e l a tter c a n be o f p a r t i­
c u l a r i m porta nce i n fl a t fee t caused by dysfu n c t i o n .
H e r e repeated s t i m u l a t i o n is usua l l y requ i re d .
As cha nges i n surface sensibi l i t y g o h a n d i n h a n d
w i th cha nges i n t o n u s we can i n fe r t h a t w h e n we fi n d
changes i n t o n u s , sensi b i l i t y w i l l b e a t least s l i g h t l y
a l tered. Hence ex teroce p tive s t i m u l a t i o n c a n b e
rega rded as a spec i fi c m e t h o d of reg u l a t i n g t h e t o n u s
of soft t i s s u e s a n d o f m uscles, e v e n i n v o l v i ng l a rge
a reas, whether tonus is i n creased or lowere d . It i s
therefore very useful to p repare t h e p a t i e n t fo r
remed i a l exercise.
Poss i b l e cou n te r i n d ications are skin d isease and
burns. Once the skin has recov e re d , adequ ate ext ero­
ce ptive s t i m u l a t i o n can be o f gre a t he l p to restore
adequate fu nction i n s k i n receptors . I n a d e q u a te
209
e m o tional reaction is a co n tra i n d i c a t i o n to some
degree. The t h e r a p i s t h a s t o keep c a l m a n d create
confidence by letting the p a tie n t stroke h e rse l f u n t i l
she fee l s comfor t a b l e a n d h e r a n x iety subsides.
Post- iso m etric m u s c l e r e l axati o n
(PIR)
( M ET) as d escribed b y M i tc h e ll e l at. ( 1 979) is
t he most prom i ne n t o f t h e m ob i l iza t i o n t e c h n iques
using m u scu l a r faci l i ta ti o n a nd i n h i b i t i o n . A s it
obviously acts o n m u scles with i ncreased te n s i o n , I
bega n to use i t pre fe re n t i a l ly for the treatm e n t o f
t h e s e m uscles. T h i s i s a t v a r i a nce w i th M i tc h e ll
h i m s e l f, w h o writes: ' I sometric con t raction . . . c a n be
used fo r a rticu l a r m o b i l iza t i o n tech n i q ue s . W h e n
isome t rics a re used fo r j o i n t m o b i l ization , max i m a l
co ntractions a re n o t d e s i r a b l e si nce they tigh t e n , o r
freeze, t h e j o i n ts . Mod e r a te co n tractions a r e m uch
more appropriate for j o i n t m o b i l ization . . . W h e n a
m u scle a n d i ts fasciae m u s t be stretch e d , h a rd
m a x i m a l con tract i o n s a re usefu l . . . .
I n m y experience, howeve r , t h i s m e th o d is as
a d v a n tageous fo r m uscle re l a x a t i o n as i t has p roved
to be fo r j o i n t mobi l iz a t i o n , if t h e re is m uscle spasm
and particularly if there a re trigge r poi n ts (TrPs) . If,
however, a m u scle or (especi a l ly ) fasciae are s h o r t
o r ta u t , stretch is used to o b ta i n m y o fasc i a l re lease
(see S o ft tissue m a n ipulati o n ) . The p roce d u re I
reco m m e n d is as fol lows: the m uscle is fi rst brought
i n to a position i n w h i c h i t attains i ts maximum l e ngth
without stretching, taking u p the s l a c k in t h e same
way a s in joint mobi l iza t i o n . I n t h i s ( e x trem e ) posi­
t i o n t h e patient is asked to resist w i t h a m i n i m u m
o f force (isometrica l l y) . T h i s res i s t a n ce is h e l d for
a b o u t 10 s , a ft e r w h i c h the p a t i e n t i s told to ' l e t go'
( re l a x ) . It i s now essen tia l to w a i t u n t i l the therapist
senses t h a t the patient h a s i n d e e d re l a x e d , a fter
w h ich he c a n u s u a l l y o b ta i n a greater range o f move­
ment by p ure relaxa tio n , not stretc h . The time d u ring
w h ic h relaxation takes place c a n v ary considera b l y ,
from several seco n d s to half a m i n u te ; t h e longe r , the
better: we s h o u l d neve r cut i t s h o r t , fo r re l a x a t i o n
is t h e re a l goa l . The refo re i t is essen t i a l to sense i t .
I f re l a x a t i o n p roves t o be u ns a t isfactory, however,
t h e re i s a s i m p l e and relia b l e way of i m p ro v i n g i t :
by len g t h e n i n g t h e isome tric phase to a s m u c h a s
h a l f a m i n u t e . However, i f r e l axa t i o n h a s b e e n sa tis­
factory from t h e start, i t is possible to shorten the
isom e t ric p h ase. The p roced u re i s repeated t h re e to
five t i m e s ; the gro u n d g a i n e d each time s h o u l d n o t
be lost d u ring t h e follow i n g p h a s e . If re l a x a t i o n i s
g o o d , t h e t hera pist s e n se s t h a t t e n s i o n is, so to s p e a k ,
' th a w i n g away', i n w h i c h c a s e rep e t i t i o n a d d s n o t h i n g
to t h e res u l t .
T h e good res u l ts obta i ne d w i t h P I R techn i q ue s a s
descri bed here ca n be sign i fi can t l y i mproved b y
com b i n i n g P I R with m e t h od s t h a t affect t h e pos t u ra l
PIR
'
Copyrighted Material
2 1 ()
Manipulative Therapy in
Rehahilitation of the Locomotor System
m uscul a t u re as a w h o l e , such as e y e move m e n ts ,
i n h a l a tion a n d e x h a l a t i o n . Lo o k i n g to th e s i d e fa c i l i ­
t a tes r o t a t i o n ( b u t not s i d e - b e n d i n g l ) ; l o o k i n g u p
fa c i l i t a te s s t raigh te n i ng u p , a nd l o o k i n g d o w n faci l i ­
t at e s s t oo p i n g I n h a l a t i o n fac i l it a tes m uscu l a r con­
traction, wh ereas p ass iv e e x h a l a t i on inhi bits m u sc u l a r
a ct i v i ty a n d faci l i tates re laxa t i o n . Th e r e a re importa n t
exce p tions a n d m o d i fica t i o n s however ( e g t h e j a w ) ,
attributable t o r e s p i r a t o r y syn k i n e s i s i . e . w h e n
movem e n t i n o n e d i re c t i o n i s c ou p l e d w i t h i n h a l a t i o n
w h i l e move m e n t in the opposite d i re c t i o n g o e s w i t h
e x h a l a t i o n : t h u s , b e n d i n g fo rw a rd i s usua l ly l i n ked
w i t h e x h a l at i o n a n d stra i g h t e n i n g up w i t h i n h a .l a ti o n :
it is difficult to brea t h e in w h i le stoop i ng, or to
b rea t h e o u t wh i l e s trai g h t e n i n g u p . This i s a l s o true
for s i d e-be n d i ng and b ac k w a r d -bend i ng ( s e e M o b i l ­
ization i n to r e t ro fl e x i o n p. 1 80 , F i gu re 6 . 3 4 ) . The
fO l l o w i n g p o i n t i s of practical v a l u e : a t i n h a lation
with t h e t ru n k i n e x t e n s i o n the d ee p back m uscles
re l a x , w h e reas during e x h a l a t i o n t h e y c o n t r ac t (see
Isometric traction, p. 1 75 , Figure 6 2 8 ) . This is i m port­
ant for the m a s t i c a t o r y and s u b m a n d ib u l a r m uscl e s ,
t h e stern o m a s toids, s ca l e n i , pectora l e s , q ua d rati
l u m bo r u m , e tc. See a l s o ' G a y m a n ' s effect' , p. 27 .
W h erever poss i bl e , t h e fo rce o f gra v i ty is used a s
d escribed by Z bo j a n ( 1 988 ) , fo r i s o m e t r i c res i s t a n ce
and for relaxa t i o n . The force of grav i t y is used t o
give resis t a nce, fo llowed by rela x a t i o n . Accord i n g to
Z b oj a n , w h e n gra v i ty i ndu c e d re l a x a t i o n i s used
alone, t h e con traction and rel a x a t i o n ph a s e s s h o u l d
each last for 2 0 s . W h e n c o m b i n e d with r e s pi r a t i o n
t h e s e p h a s e s s h o u l d coinci d e with t h e respira tory
p ha s e s . G r a v i ty - i n d uced P I R is a m e thod of se l f­
trea t m e n t rig h t from t h e begi n n i ng.
The e ffects o f tre a t m e n t c a n b e ascer t a i n e d n o t
o n l y i n t h e m u s c l e tre a t e d , w h e r e t r i g g e r p o i n ts a nd
t e n s i o n s ho u l d have d i s a pp e a re d b u t p a i n p o i n t s
s i t u a ted m o s t freque n t l y w h e re t h e t e n d o n i s
a t t a c h e d t o t h e perioste u m , w i l l a l s o h a v e d is­
appear ed . At t i m e s , t h ese p a i n poi n ts a re more l i ke l y
to be d u e to r e fe r r ed p a i n i n w h ich case P I R i s a s
e ffective a s loca l a naesth e s i a or n e e d l i n g .
Th is m e t h o d i s h i g h l y specific i n f a n-s h a p e d m uscles
whose fibres m us t be treated w h e re i n c reased
t e n s i o n is fou n d . Th at i s u s u a l l y in t h e d i rection of
p a i n fu l a tta c h m en t p o i n ts (e.g. p a i n p o i n t s on the
ribs o w i n g to TrPs i n the pectora l is ) . H e n ce o n e
reaso n f o r fa i l u re is i n s u f fi ci e n t s p e ci fi c i t y T h i s
m e t h o d i s u s e l e ss w he re t he r e is no increased m uscl e
t e n s i o n . T h e r a p e u t i c fai l u re m a y a lso be d u e to a n
u n d e rl y ing c a use p rod u c i n g renewed m uscular
tension, such as j oi o t b l ockag e o r v iscera l d isease i n
t h e co rr e sp o n d i n g s e gme n t .
Theoretically, S h er ri n g ton 's post-isometric ( me d u l­
l a ry ) i n h i b i t i o n c a n n o t e x p l a i n t h e e ffec t i ve n ess o f
t h i s m e t h o d beca use o f th e l o ng l a t e n c y period.
Com pared with the classic method o f Kabat ( 1 96 5 ) ,
n o t o n l y i s r e s i s t a n c e m u ch w e a k e r , b u t active
s t r e t c h i s also avoided. Th e e x p l a n a t i o n o f t h e
.
.
.
,
,
.
-
,
,
,
,
.
,
exce l l e n t res u l ts fu rn ished b y t h i s m e t h o d m a y b e
s oug h t i n t h e fa c t th a t (I ) d u r i n g resista n ce o f
m i n i m a l force o n l y very f e w m uscle fi b res a r e a c t i v e ,
t h e o th e rs r e m a i n i n g i nactive, while (2) d u r i n g
re l a x a t ion t h e s t r e t c h reflex i s avoided , (I r e fl e x
w h i c h is brought a bout e v e n by passive a n d n o n ­
p a i n f u l stretch . On t h e o t h e r h a n d t h e r e a r e
s i t u a t io n s i n w h i c h t h e p a t i e n t e x pe r i e n ce s some
p a i n d u ring P I R a n d yet goes o n re l a x i n g ( e . g . i n
'ligame n t p a i n ) . A fter t h e p roc e d u re , however,
t he r e is a n a l g e s i a . Th is m e t hod d e m o n s t ra tes v e r y
c l e a r l y t h e c l os e i n terre l a t i o n b e t w e e n t e nsion a n d
p a i n a nd re l a x a t i o n a n d a n a l g e s ia
This method i s co m p a ra b l e with the 'spray and
st retch ' m e t h od o f Travell ( 1 976) b u t pl aces gre a t e r
e m p has i s o n re l a x a t i o n . I n d e e d , s t re t c h i s n o t
e s se n t i a L as l e n g t h e n i n g is m e re l y t he p roof of
successf u l r e l a x a tion ( d eco n t r a ct i on ) In some of t h e
gravi ty-i n d u ced t e c h n i q u e s a n d i n re l a x a t i o n o f t h e
g l u t e i , n o s t r e t c h takes place. S t re t c h se e ms to b e
req u i red o n l y w h e re t h ere i s t rue m u sc l e s h o r t e n i n g
( t a u tn es s ) d ue to c o n n e c t i v e t i ssue c h a n g e s c a l l i n g
fo r soft t is s u e m a n i p U l a t i o n .
To show the e ffec t i v e n e s s o f o u r m e t h o d , 3 5 1
pa i n ful m u s c l e g r o up s or m u s c l e a t t a c h m e n t s were
treated i n 244 p a t i e n t s . There was i m m e d i a te
a n a lgesia i n 330 i n s t a n ce s , w h e r e a s o n l y i n 2 1 w a s
t h e r e no e ffect.
R e ce n t l y using i n te r m i t te n t res i s t a n c e , we find i t
ve r y useful t o comb i n e P l R w i t h c o n t ra c t i o n of t h e
a n tago n i s t : i n the po s i t i on t he pa t i e n t h a s reached
by P I R , s h e p re s s e s l ightly a g a i nst m o d e r a t e re s i s t ­
a nce by t h e the r a p i s t i n t h e d i re c t i o n rea c h e d b y
r el a x a t i o n . H e c h a n ge s t he counter- p ress u re r h y t h m ­
ica l l y s e v e r a l t i m e s p e r sec o n d . Th e p a t i e n t m a y a l so
m a k e a m a x i m u m m o v e m en t in t h e d i rection o f
mobi l iza t i o n .
,
'
.
,
.
,
,
,
Treat m ent o f i n d i vi d u a l m u sc l es
a n d p o i nts of atta c h m ent
T h e te c h n i q u e s
descr i bed here a re useful not
fo r t herapy, b u t a lso for d i agnosis.
on ly
Tension i n the masti catory muscles
Te n s ion
in the m a s t i c a t o r y m u s c l e s ( T r Ps) ca n b e
p a l pated i n the te m p or a l r e g i o n ( t h e t e m p o ra l is),
w h i l e fo r s c r e e n i ng p a l p a t ion t h rough t h e c h e e k s
w i t h t h e m u scles relaxed shou l d reve a l a s y m m e t ry . A
h e a l th y s ubj e c t s h o u l d be a b l e to i n s e r t t h re e k n uc k l e s
betwee n the upper and lowe r i n c i sors. F o r accurate
d i a g n os i s of TrPs, w h i ch a r e ofte n very tender, it i s
n e cessa ry to p al p a t e th rough t h e o p e n m o u t h . If this
procedure is pai nfu l , the tem poroma ndibu l a r joi n t
w i l l also b e te n d e r o n pa l p a t i o n , e i t h e r owing to
referred p a i n o r b e c a u s e t h e e x tern a l p t e r y go i d
attaches to t h e m e n i sc u s of t h a t j o i n t The m a s s e t e r
Copyrighted Material
,
.
Therapelltic techn iques
21 1
( a)
(a)
( b)
( b)
Figure 6.86 (a) P I R 01 t he m a sse t e rs, i n t e rn a l p t e rygo i d s
a n d t h e t e m p o r a l m u scles: ( /J ) se l f- t re a t m e n t
t re a t m e n t
fro n t o f i t , a n d TrPs h e re s h o u l d be p a l p a ted
p i n ce r gri p , w i t h one fi nge r i ns i d e the m o u t h
and t h e o t h e r on t h e c h e e k . T h e i n t e r n a l p t e ryg o i d
i s palpa ted with a s i m i l a r p i n c e r moveme n t , be h i n d
t h e m a ssete r , a bo v e a n d be h i n d t h e l a s t m o l a r , t h e
p a l p a t i n g fi n ge rs h o l d i ng t he ramus o f t h e mand i bl e .
W i t h t h e exce p t i o n o f t he exte rn a l pte rygoi d , P I R
of t h ese muscles is perfo r m e d by fi rst t a k i n g u p t h e
s l a ck : t h e m o u t h is o pe n e d , t h e n closed aga i n s t
isomet ric r e s i s t a nce w i t h t h e m i n i m u m o f force ;
rel a x a ti o n c o m e s w i th o pe n i ng of t h e m o u t h . Fo r t h is
m a n o e u v re to be e ffect i v e , res p i ratory sy n k i n e s i s i s
esse n t i a l . T h e p a t i e n t is told to b re a t h e o u t a ft e r t h e
s l a c k h a s bee n t a k e n u p by o p e n i n g h e r m o u t h , t h e n
t o o p e n t h e m o u t h w i d e a s i n y a w n i n g , a n d ta ke a
d e e p bre a t h (F i g u r e 6 .86a ) . I r t h e m u s c l e s i n q u e s t i o n
a re the t e m pora l i s a n d/or t he i n t e rn a l p t erygo id , we
m a y i n t roduce d e v i a ti o n to t h e side d u r i n g t h e
re l a x a t i o n p h a s e , t o t h e opposite s i d e i n t h e tem por­
a l i s and to the same side i n the p terygo i d .
Fo r s e l f- t re a t m e n t t h e pa t i e n t s i ts a t a ta b l e , o n e
e l bow o n t h e t a b l e , w i t h t h e h a nd p r o p p i n g h e r
for e h e a d : t h e fi n g e r s o f t h e o t h e r h a nd a re o n t h e
lowe r i n c i sors. A ft e r o p e n i n g h e r m o u t h to t a k e u p
the slac k , s h e b re a t hes o u t ; d u r i n g i n h a l a t i o n s h e
ope n s h e r m ou t h a s w i d e as poss i b l e . The h a n d o n
t he forehead s h o u l d pre v e n t a n te flexion , w h ich
w o u l d i n te r fere with m a x i m u m o pe n i n g o f t il e
m o u t h ( F i g u r e 6.86b ) .
T o t r e a t the e x t e r n a l pte rygoid t h e p a t i e n t i s
s u p ine, h e r m o u t h s l i g h t l y o pe n . T h e t h e r a p i s t p l aces
h is t h u m b s on the m a n d i ble from above; t h e p a ti e n t
i s told t o p ress h e r ch i n forward a g a i n s t h i s t h u m bs ,
w h i le b r e a t h i n g i n ; s h e holds h e r brea t h , t h e n
b r e a t h e s o u t , l e tting t h e ch i n d rop back. F o r se l f­
trea t m e n t she u s e s h e r o w n t h u m b s ( F i g u re 6 . 87 ) .
The m a i n a n t a g o n i s t o f t h e mastica tory m u s c l e s i s
t h e d i g a s t r i c u s w h i c h a t ta c h e s t o t h e
hyo i d .
Increased t e n s i o n is b e s t d i a g n o sed by s h i f t i n g t h e
t h y roid c a rti l a ge f r o m s i d e to s i d e . I f t e n s i o n i s
m a rked o n o n e s i d e , d e v i a ti o n o f t h e c a r t i l a ge to t h a t
s i d e can e v e n be seen.
Fo r PIR t h e p a t i e n t should be s u p i ne ; with o n e
h a n d the t h e ra p i s t resi s ts t h e o pe n i n g of t h e mo u t h
w h ile t h e t h u m b o f t h e o t h e r exerts m ini m a l p res­
sure o n t h e hyoid o n t h e side of i n c re a sed t e n s i o n
( d e v i a t i o n ) . T h e h y o i d i s pa l p a t e d a bo v e a n d l a t e r a l
to t h e t h y roid ca rti lage. T h e p a t i e n t o p e n s h e r m o u t h
l i es i n
by
a
Figure 6.87 (a)
P I R of t h e
Copyrighted Material
exte rn a l pte rygo ids: (/J) self­
212
Manipulative Therapy in Rehabilitalion of th e Locomotor System
D u r i n g t h e resistance p h a s e s h e s l ig h t l y ope ns h e r
m o u t h a n d b re a t hes i n , h o ld i ng h e r breat h a n d t h e n
re l a x i n g w h i l e brea t h i n g o u t ; s h e c loses h e r m o u t h .
w h i l e h e r t h u m b moves t h e h y o i d ve ry ge n t l y
( Fi g u re 6.88b) .
I f the re is i ncreased te n s i o n (TrP) i n the m y l o h y ­
oid m u s c l e i n the s u b m a n d i b u l a r region b e h i n d the
c h i n , sel f- t re a t m e n t i s t h e only possi b l e a p p roach .
The p a t i e n t p resses t h e tip of h e r tongue aga i nst t h e
h a rd palate w h i le b r e a t h i n g i n , a n d lets the tongue
drop back w h i l e b r e a t b i n g o u t .
Tension in the reg ion of the posterior
a rc h of t h e atlas (Figure 6 . 89)
( a)
Te n s i o n a n d t e n d e rn e ss ( T r P s ) in t h i s regio n , i . e . of
the short ex tensors o f the cra n iocervical j u nction ,
c a n be p a l p a ted o n l y w i t h tbe patient s u p i n e , h e r
h e a d i n a n t e fl e x i o n . F o r t reatme n t tbe p a t i e n t s i ts
on the t a b l e , with t h e therapist s t a n ding be h i n d her,
and l e a n s aga i n s t h i s ches t . The therapist p l aces both
t h u mbs o n t h e p a ti e n t's occ i p u t , with h i s fi n gers o n
the m a l a r bones fro m a b o v e . T o t a k e u p t h e slack,
t h e therapist ti l ts the head s l i g h t l y fo rward so as to
d ra w t h e p a t ie n t ' s chin i n t o her neck . H e t h e n te l ls
t h e p a t i e n t to look u p a n d breathe in s l o w l y wh ile
resi s t i n g the patient's tende ncy to raise h e r h e a d : the
patient is t h e n to l d to look down and breathe out
slowly, le a n i n g back and bringing ber chin e v e n
closer to t h e t h ro a t ( s h e m u s t n o t b e n d forwa rd) .
This ma noe uvre i s repeated a b o u t t h ree ti mes.
For s e lf-trea t m e n t . the patie n t ( Figu re 6 . 90) uses
her o w n h a n d s , placing her fi ngers on t h e occiput
a n d her t h umbs o n the ma l a r bone. I n order t o b r i n g
the c h i n i n tow a rd s t h e t h roat d u ring relaxa t i o n , t h e
p a t i e n t m us t l e a n backwards over a l o w cha ir-back.
,
Te n s i o n in the levator sca p u l a e
( Fi g u re 6 . 9 1 )
T h e typica l p a i n p o i n t s a re o n t h e lateral surface
the spinous process o f C2 and o n the s u p e r i or
border of t h e scap u l a . TrPs a re s i t u a te d ab ove t h e
u p p e r m e d i a l a ngle o f th e sca p u l a o n t h e neck. For
treatm e n t the patien t is s u p i ne w i t h her head at t h e
end of the t a b l e a n d the e l bow o f t h e fl e x e d a rm
raised above h e r h e a d . The therapist exerts p ressure
on the sca p u la by p r e s s i n g in a caudal d i rection
aga i n s t t h e e l bow, fl x i n g i t with h i s t h i g h . Us i n g both
hands h e now bends the h e a d to t h e opposite s i d e ,
r a i s i n g a n d t u r n i n g i t v e r y s l ig h t l y i n t h e same
d i rection u n t i J t h e s l ack i s taken u p . Th i s i s fe l t
soon e r o n t h e s i d e o f i n creased tension t h a n on t h e
o t h e r s i d e . The p a t i e n t t h e n l o o k s tow a rds the si d e
t h a t is be i n g trea ted, a n d slowly breathes i n . w h i l e
t h e therapist resists t h e a u to m a t ic tendency t o turn
to tbat side. H e t h e n te l l s the patient t o 'let go' a nd
brea t h e O Li t . D u ri ng t h e e n s u i ng re la x a t i o n t h e head
is s l ig h t l y moved s i d e wa rds a n d fo rwards. H e may
of
( b)
Figure 6.88
(0)
P I R of
the d igastricus: ( b ) se l f-treatment
a ga i n s t very s l ig h t resi s t a n c e and breathes in, hoJ d s
h e r brea t h , a n d t h e n breathes o u t a n d re laxes. D u ring
re laxatio n , t e n s i o n i n t h e d i gas t ricus w i l l a u t o m a t i c­
a l l y give u n d e r t h e therapist's th umb w h e re r e l ease
i s fe l t ( F i g u r e 6.88a ) .
F o r self-tre a tm e n t t h e p a t ie n t s i ts a t t h e t a b l e ,
ch i n i n o n e c u pped h a n d , w h i l e t h e t h u m b o f t h e
o t h e r h a n d l i e s l a teral t o the h y o i d o n t h e tense s i d e .
Copyrighted Material
Th erapelltic techniques
( a)
( a)
(b)
( b)
Figure
6.89
the
o f tensi on
j u nction : (a)
PIR
cra n i o c e rv i c a l
s h o r t e x t e n so r s
of
the
i n t h e s h o rt e x t e n s o rs o f t h e
res i s t a n c e : (h) relaxa t i o n o f
c r a n i o ce r v i c a l j u n c t i o n
Figure
6.90
Se l f� t re a t nl e n t of t e n s i o n i n t h e
t he cra niocervica l j u n c t i o n
e x t e n sors o f
Copyrighted Material
s h ort
213
214
I'vl aniplliative Th erapy in Rehabilitation of the LocomolOr System
Figure 6.91 Ex a m i n a t i o n a nd PIR o f te n s i o n in t h e
Figure 6.93 G ra v i t y - i n d u c e d P I R o f t h e l e v a t o r sca p u l a e
lev a t o r sca p u l a e ,
a n d t h e upper part of
t h e trapez i u s : l d t , w i t h s h o u l d e r s
r i g ht. w i t h s h o u l d e r s l owered
w i t h fi x a t i o n o f the sca p u l a p u s h e d
d o w n by t h e t h e ra p i s t p r e ss i n g his t h igh o n t h e patie n t 's
e l bow
raised:
a l so t e l l t h e p a t i e n t t o p u ll o n e e l b o w u p s li g h t l y ,
tow a r d s t h e s i d e a w a y fro m w h ic h t h e h e a d i s b e n t .
u p t h e s l a c k . He then
w h i l e h e r e s i s ts t h e m o v e m e n t , a fte r w h i c h h e a g a i n
asks
pa t i e n t t o l o o k
the
resist i ng t h e p a t i e n t ' s a u t o m a t ic t e n d e n c y t o
move
is
t o w a r d s t h e s i d e of t h e l e s i o n ; the p a t i e n t !TI u s t be
I f , h o w e v e r , t h e p a t i e nt c a n n o t r a i s e h e r a r m to
b r e a t h e out d u r i n g re l a x a ti on ; m e a n w h i Je t h e h e a d
t h e u t m o s t , th e t h e r a p i s t s t a n d s a t that side o f t h e
t a b l e t o w h i c h re l a x a t i o n i s c a r r i e d o u t . H e p u s h e s
is m o v e d fu r t h e r t o t h e s i d e u n t i l t h e s l a c k h a s a g a i n
b e e n t a k e n u p . R e s i s t a nce m a y a l s o be g i v e n aga i n s t
moves
the
head
sideways
and
fo r w a rd .
Th is
t o l d to bre a th e in d u r i ng this m a n oe u v r e . and to
r e p e a ted two o r three t i m es .
h e r s h o u l der d o w n w i t h o n e h a n d , w h il e t h e o t h e r
t h e s h o u l d e r , from abo v e ; i n t h i s c a s e t h e p a t i e n t i s
r o u n d t h e b a c k o f h e r occ i p u t a n d n e c k prod u ce s
t o l d to l i ft h e r s h o u l d e r a g a i n s t t h e res i s t a nce o f t h e
s i d e - b e n d i n g , s l ig h t l y fo rw a rd a n d i n to rota ti o n , s o
t h e ra p i s t , w i t h t h e l e a s t p o ss i b l e force : a f t e r a b o u t
a s to t a k e u p t h e s l a c k . Th e n P I R t a k e s p l a c e a s
1 0 s s h e s h o u l d ' le t g o ' . T h e t h e r a p i s t s h o u l d t h e n
described above.
b e n d t h e h e a d a n d n e c k s i d e w a y s a ga i n . to t a k e u p
t h e s l a c k . I n b o t h c a s e s t h e proce d u re is re p e a t e d
Ten s i o n i n the upper p a rt of the
trapezi u s m uscle ( F i g u re 6 . 92)
a b o u t t h re e t i m e s .
T h e e ffe c t o f P I R o f t h e l e v a t o r sca p u l a e a n d t h e
u p p e r t r a p e z i us c a n
be e n h a n c e d
by
il il t a go il is t
The u pp e r t r a p e z i u s s h o u l d b e t r e a t e d if te n d e r a n d
sti m u l a t i o n : the patient, with the head i n n e u t r a l
t a u t . T h e p a t i e n t i s s u p i n e , w h i l e t h e t h e ra p i s t fi x e s
p o s i t i o n , l e e1ll s a g a i n s t t h e h a n d o f t h e t h e r a p i s t
t h e s h o u l d e r f r o m a b o v e w i t h o n e h a n d , s id e - b e n d i ng
a n d r e s i sts s l i g h t pre s s u re f r o m t h e s i d e to w h i c h
t h e h e a d a n d n e c k w i t b t h e o t h e r h a n d so as to t a k e
re l a x a t i o n too k p l a c e ; t h i s p r e ss u re t h e t h e r a p i s t
i n t e r m i t t e n t l y i n c re a ses a n d d e c re a se s .
Fo r s e l f- t re a t m e n t o f b o t h t h e u p p e r t r a p e z i us a n d
t h e l e v a t o r sca p u l a e , gra v i ty- i n d u c e d P I R i s m o s t
e ffe c ti v e . T h e p a t i e n t sits aga i n s t
a
l ow c h a i r- b a ck
w i t h b o t h a r ms h a n g i n g d o w n o v e r i t . to e n s u re
straight
post ure.
In
this
po s i t i o n
she
raises her
s h o u l d e rs w h i l e l oo k i ng u p a n d b r e a t h i n g i n ; a fter
h o l d i n g h e r b re a t h she b r e a t h e s out s l ow l y w h i le
l e t t i ng t h e s h o u l d e rs d ro p ( F i g u re 6 . 9 3 ) . No good
re J a x a t i o n of t h e s e m u s c l e s c a n b e o b t a i n e d w i t h
ro u n d e d s h o u l d e rs a n d t h e h e a d d ra w n fo rwa rd .
Tension i n the sca l e n e m u scles
( F i g u re s 6 . 94 a n d 6.95 )
I n m o s t cases t e n s i o n of t h e sca l e n u s d o e s n o t c a u s e
F i g u r e 6.92 E x a m i n a t i o n a n d P I R o f t e n s i o n i n t h e u p p e r
p a r t o f t h e t rapezi us
d i r e c t p a i n b u t i s o f g re a t c l i n i c a l s ign i fi c a n c e . A s a
r u l e t h e s ca l e n e s a re t e n s e i f t h e o t h e r u p p e r fi x a tors
Copyrighted Material
'Th erapeulic techn iques
2 1 .'>
o f t h e s h o u l d e r g i rd l e a re t e n s e ; t h e y p l a y a d e c i s i v e
role i n fa u lty r e s p i r a t i o n . ca u s i n g t h e p a t i e n t to l i ft
h e r t h o ra x , a n d
in
t h e s y n d ro m e
o f the
upper
t h o r a c i c o u t l e t . T e n s i o n i n t b e pectora l e s a n d p a i n
p o i n ts a t the s te r n ocosta l j u n c t i o n o f t h e u p p e r r i b s
s e e m to be co n n ec ted w i t h t e n s i o n of t h e sca l e n e s .
T h i s m a y e x p l a i n w h y t e n s i o n of t h e
t o p r od u ce
a
s e n s a t i on
scalenes seems
of o p p r e s s i o n
in
many
patien ts,
w h o t h u s fe e l gre a t relief after P I R .
D y s fu n c t i o n o f t h e fi rs t r i b goes h a n d i n h a n d w i t h
T r P s of t h e s ca l e n u s o n t h e s a m e s i d e , c o r r e s p o n d i n g
t o E rb ' s po i n t . T h e s e c a n be a b o l i s h e d by P l R o f t h e
sca l e n u s .
O n e x a m i n a t i o n , t e n s i o n i n t h e s c a l e n u s c a u se s
res t r i c t i o n o f retro A e x i o n of t h e rot a ted h e a d to t h e
o p p o s i t e s i d e . I f t h e r e i s m a rked c e r v i c a l l o rd o s i s .
t e n s i o n o f t h e sca l e ne s m a y r e s t r i c t s i d e - be n d i ng o f
sea ted , s i m u l a t i n g te n s i o n
i n t h e u p p e r part of t h e t r a p ez i u s
t h e h e a d w i t h t h e p a ti e n t
.
For e x a m i n a t i o n . as fo r t r e a tm e n t , th e p a t i e n t s i ts
o n the t a b l e , wh i l e t h e t h e r a p i s t s t a n d s be h i n d h e r
a n d s u p p o r t s t h e s h o u l d e r o n t h e s i d e to be t r e a t e d
.
w i t h o n e h a n d fi x i n g t h e u p p e r r i b s of t h e s a m e s i d e
by press u re on t h e p a t i e n t s c h e s t . W i t h t h e o t h e r
'
h a n d t h e t h e r a p i s t t u rns t h e p a t i e n t s h e a d to t h e
o t h e r s i d e . b e n d i n g h e a d a n d neck backwards so as
'
Figure 6.94 E X 8 lTI i n a t i o n a n d PI R of t h e sca l e n u s
to t a ke
u p t h e s l a c k . H e n o w t e l l s t h e p a t i e n t to l o o k
t o t h e s i d e o f t r e a t m e n t , resisting a u t o m a t i c m o v e ­
m e n t w i t h m i n i m a l p ress u re o n t he pa t i e n t ' s t e m p l e
,
te l l i n g h e r to b re a t h e i n s l o w l y ; t h e t h e r a p i s t r e s i s t s
t h i s i n h a la t i o n b y p re ss i n g t h e o t h e r h a n d a g a i n s t
t h e pa t i e n t ' s c h e s t w i t h c o n s i d er a b l e fo rce . T o d o
t h i s h i s e l bo w s h o u l d be r a i s e d a n d b r o u g h t fo rw a r d .
A ft e r fu l l i n h a l a ti o n t h e pa t i e n t i s t o l d to l o o k t o t h e
breathe out. let t i ng the
h e a d a n d n e c k d r o p i n to r e t r o A e x i o n ( h e m u s t n o t
p u s h ! ) . T h i s p roced u r e i s repeated a b o u t t w o o r
t h re e t i m e s . T h e r e i s p e r h a p s n o m u scle t h a t b e t t e r
s i d e o f re l a x a t i o n a n d to
l e n d s i ts e l f t o re l a x a t i o n t h a n the sc a l e n u s .
F o r s e l f- t re a t m e n t , g r a v i t y i n d u c e d PIR i s dfe c t ­
-
i v e . T h e p a t i e n t l i es o n h e r
s i d e , l i f t i ng h e r h e a d ,
s h e holds her brea t h
t h e n s l o w l y s i n k s b a c k t o t h e t a b l e w h i l e bre a t h i n g
o u t . T h i s is re p e a te d t h r e e t i m e s ( F i g u re 6 . 95 ) . I f ,
h ow e v e r , r e s p i ra t i o n is at f a u l t c o rrect i o n o f bre a t h ­
i n g is t h e m e t hod o f c h o i ce .
l oo k i n g u p a n d b r e a t h i n g i n ;
,
Te nsion i n t h e sternocleidom asto ids
( Figure 6.96)
Th e r e i s f r e q u e n t l y a p a i n p o i n t a t t h e med i a l e n d
o f t h e c l a v icl e a n d a t the transv e rs e proce ss of t h e
a t l a s . T h e re are , h o w e v e r , n u m e ro u s t r igge r poi n ts
to be fo u nd in t h e c o u rse of t h e m u s c l e ( t h e c l a v i c u ­
la r a s w e l l a s t h e stern a l d i v i s i o n ) pa rtic u l a rl y b e l o w
t h e m a s t o i d p rocess, r e fe rri n g pain t o t h e fa ce a n d
c ra n i u m . Te n s i o n i n t h e s t e r n oc l e i d o m a s t o i d m u s c l e
,
Figure 6.95 G t'a v i t y - i n cl u cecl P I R o f t h e sca le n i : a bove.
with h e a cl r a i sed : below. with head l o w e red
m a y a l s o prod uce te n s i o n i n t h e s u b c l a v i c u l a r p a r t
of t h e p e c t o r a l i s m u scle .
Copyrighted Material
21 6
Manipu/alive Therapy
in
Rehabililalion of th e
Loco m otor System
Figure 6,96 G r a v i t y - i n d u c e d P lR of t h e
Left : w i t h h e r h e a d
of t h e t a b l e , t h e
p a ti e n t b rea t h e s i n a n d looks u p . a u to m a t i c a l ly
c o n trac t i n g t h e sternocl e i d o m a s t u i d a n d s l i g h t l y
l i ft i n g h e r h e a d . R i g h t : s h e b r e a t h e s o u t a n d
r e l a x e s , t h u s l e t t i ng t h e h e a d d ro p
s t e r n oc l e i d o m as t o i d m u s c l e .
t u r n e d to the s i d e over
For tr e a tm e n t of t h i s co ndition, gravity-induced
P I R is t h e most effective m e t h o d . The p a t i e n t l ies
s u p i n e , with h e r h e a d rotated a n d resti n g over t h e
edge o f t h e t a b l e , t h e c h i n s u pp o r te d b y t h e e d ge of
the t a b l e , a c t i n g a s a f u l c r u m . I f t h e l e ft sterno­
mastoid is to be treated, t h e h e a d is ro t a t e d to the
r i g h t . I n t h i s pos i tion the p a t ien t is told to look u p
a n d t o take a slow dee p bre a t h ; d u ri n g d e e p
i n s p i r ation the sternomasto i d m u scle s l i gh t l y con­
tracts, lifti ng the h e a d , w h i c h is pivoted on t h e e d g e
o f the ta ble . I n th is position s h e h o l d s h e r brea t h ;
a fte r this she l o o k s to the c h i n a n d d u ring s l ow
e x h a l a tion t h e p a t i e n t relaxes, t h e top of the head
is lowered, and a slight s t re t c h i ng o f t h e sterno­
cleidomastoid ensues. This m a n o e u vre is re peate d
about t h re e t i m e s .
T h i s t e c h n i q u e gives exce l l e n t re sults i n t h e
treat men t of a b l o c k e d a t l a n to-occ i pital j o i n t , a n d
c a n be u s e d fo r self-tre a tment o f this j o i n t . I t h a s a
m a rk e d ana lgesic e ffect on pai n ful or te n d e r trans­
v e rse processes of the a t l a s .
the
edge
t h e f u l l y abd ucted a r m a b o u t 2 cm, b re a t hing i n
slowly a n d to h o l d h e r bre a t h . S h e t h e n r e l a x e s a n d
breathes o u t s l o w l y , r e p e a t i ng t h is proce d u re a b o u t
three t i m e s . She s h o u l d n o t re l a x s u d d e n ly, a s t h is
w o u l d cause b r u s q u e s t r e tc h i n g .
I f the sternoco s t a l p a r t of t h e p e c to r a l i s m u s c l e i s
t e n s e t h e p a t i e n t t e n d s to be ro u n d s h o u l d e re d ; fu l l
e l e v a t i o n o f t h e a r m i s re s t r i ct e d (Figure 6.98 ) , a n d
t h e tendon i n t h e a x i l l a i s t a u t o n p a l p a t i on . a s well
as t e n d e r . T r P s C il n be p a l p a te d by a p i n c e r m o v e ­
m e n t w i t h t h e fi n g e rs b e t we e n t h e m u s c l e a n d t h e
r i b s , a n d t h e t h u m b on t h e s u rface o f t h e c h e s t .
Fix a t i o n and treatm e n t a re s i m i l a r to t h a t p r e s c r i b e d
for the u p p e r part o f the muscl e . O nce the p a t i e n t
h a s u n d e rstood t h e c o r rect pos i t i o n a n d d i re c t i o n .
grav i t y- i n d u ced P I R is c a r r i e d o u t by the p a t i e n t
h e rs e l f .
Tensi o n i n the pectora l i s m aj o r
I ncreased t e n s i o n (sho r t e n i ng) of t h e u p p e r (clavicu­
lar) p a r t o f the pectora l is ( Figure 6 . 97) res u l ts i n a
forw a rd-drawn pos i tion of the s h o u lders. For both
ex a m i n a t i o n and t r ea tm e n t, the p a t i e n t i s s u pin e , h e r
arm abducted a t ri g h t a ngles . T h e t h e r a p ist sta nds
a t t h e side of t h e a ffected m uscle ; w i t h h i s forearm
h e fixes the pa t i e n t 's stern u m from a bove and
palpates the tendon b e n e a t h the cl avicle with h i s
fingers; i t should n o t b e tense even a t m a x i m u m
abduction. T h e other arm brings t h e p a t i e n t ' s a rm
i n to m a x i m u m a b d u c t i o n o v e r t h e side of the t a b l e ,
to t a k e up t h e s l a c k . F o r tre a t me n t the patient is t o l d
to lift her arm aga i n s t the therapist's h a n d , using
l ittle force , w h i le br e a t h i n g in slowly. Once t h e
p a t i e n t h a s fo u n d t h e correct d i rection of abduction,
t h e force of gravity is s u ffi c i e n t to hold i t , a n d t h e
p a t i e n t i s rea d y for self-trea tme n t: she is told to l i ft
( a)
Figure 6.97 ( a ) E x a m i n a t i o n a n d PI R of t b e c.Ia v i c u l a r
p a r t o f t h e p e c t o r a l i s . ( b ) ( S e e o p p o s i t e ) G r a v i ty­
i n d uced p r R (se l f- t re a t m e n t ) 0 1 the c l a v i c u l a r part o f
t h e p e c t o r a l i s : t o p . i n h a l a t i o n and s l i g h t r a i s i n g o f t h e
a r m : b o t t o m . e x h a l a t i o n a n d r e l a xa t i o n l e t t i n g the a nn
fa l l
Copyrighted Material
Th erap eutic techniq ues
Figure
217
6.97 (contin ued)
TrPs o f t h e pectora l i s ca n a l so b e
b y s t i m u l a t ion o f t h e a n t a g o n i st
the l a tissi m u s dors i . The p a t i e n t is s e a t e d , t h e
therapist s ta n d i ng b e h i n d h e r ; s h e l i fts her a r m to
Te n s i o n and
e ffec t i v e l y t r e a te d
,
the
level o f her
s h o u lder w i t h the
e lbow fl e x e d .
press u re w h i c h
t h e therapist i s exerti n g aga i n s t h e r e l b o w from
be h i n d
S h e r e s i s t s the m o d e r a te i n t e r m ittent
.
Copyrighted Material
21 8
l'vIan ip u /ilIive Therapy in Rehah ilita tioll
0/ the Locomotor
System
( a)
( b)
Figllre 6.98 ( a ) E x a m i n a t i o n l1 n d P I R of t he ste rn a l part of the pectora l i s ma jor. ( h ) G ri l v i t y - i ncluce d PIR ( se l f- t r e a t me n t )
o f t h e a r m ; righ t . e x h a l a t i o n a n d rcia x a t i o n , l e t t i n g t h e a r m d ro p
o f t h e p e c t or a l is major: l e ft , i n h a l a tion a n d s l i g h t ra i s i n g
P a i n poi nts o n t h e ribs ( Figu re 6,99)
T h e s e p o i n t s a re f o u n d m o s t freq u e n t l y i n t h e m i d ­
a x i l l a r y a n d mid-clavic u l a r
tS
line,
a nd t h e i r tre a t m e n t
of p a r t i c u l a r i m p o r t a n c e . T h e s e p a i n p o i n t s are
the p o i n ts o f a t ta c h m e n t of
fi bres
of
the
pectorales
a n d se r r a t u s m u s c l e s w i t h i n c r e a s e d te n s i o n . Fo r
t re a t m e n t o f p a i n p o i n t s i n t h e m i d -cl a v i cu l a r l i n e
t h e p a t i e n t l i e s s u p i n e : t h e t h e r a p i s t l i fts t h e p a t i e n t ' s
a r m t o pro d u c e t e n s i o n i n those fi. b r e s t h a t a r e
d i re c te d t o w a r d s t h e p a i n poin t . Th is ca n b e pa l ­
p a t ed w i t h the t h u mb a t t h e p a in p o i n t , and o f t e n i s
v i s i b l e to t h e e y e . Once t h e c o r r e c t d i rec t i on h as
b e e n e s t a b l i s h e d , t h e t h e r a p i s t t a kes up t h e s l a c k b y
e l e v a t i o n o f t h e p a t i e n t 's a r m H e t h e n te l l s h e r t o
press ge n t l y a g a i n s t t h e h a nd h o l d i n g t h e a r m u p a n d
to b re a t h e i n a ga i n s t t h e t h u m b ( o r t h e n ar
e m i n e n ce ) a ll t h e p a i n p o i n t . T h i s is fo l l o w e d b y
e x h a l a t i o n a n d r e l a x a t i o n o f t h e < tr m i n t o f u r t h e r
.
Figure 6.99 S pecific t re a t m e n t of p e c t o ra l i s fi b res
a t t a c h ed to a p a i n p o i n t o n a rib
Copyrighted Material
Thaap elllic techniques
Figure 6.100
P I R o f the
re l a x a t i o n
G ra v i t y - i n d u c e d
s h o u l d e r l o w e re d d u ri n g
p e c t o ra l i s m i n o r: l e ft , t h e s h o u l d e r
e l e v a t i o n , A ft e r t w o o r t h re e r e p e t i t i o n s t h e t h e r a ­
p i s t fee l s t h a t the t e n s i o n h a s d i s a pp e a red , a n d t h is
u s u a l l y m e a n s t h a t t h e t e n d e r n e s s at the p a i n p o i n t ,
t o o , h a s b e e n a bo l i s h e d .
M. pecto ra l i s minor
2 .1 9
over t h e edge o f t h e t a b l e , r a i s e d : r i g h t , t h e
Te n s i o n i n the serrat u s a nterior
( Fi g u re
6. 1 0 1 )
T h is m u s c l e a t t a c h e s a t t h e r i b s i n t h e a x i l l a r l i n e ,
a n d t h e re a re p a i n fu l t r i gger p o i n ts c l ose to a n d a t
these a t t a c h m e n t poi n t s . F o r e x a m i n a t i o n t h e p a t i e n t
( Figu re 6 . 1 0 0 )
T h i s m u s c l e a t t a c h e s a t t h e c o r a c o i d p rocess a n d a t
t h e t h i rd t o fi ft h r i b s , w h e re p a l p a t i o n c a n b e pa i n fu l .
I n c re a sed t e n s i o n p r o d u ces fo rw a rd - d ra w n s h o u ld e rs
a n d a c c o r ci i n g to H o n g a n d S i m o n s ca n be a c a u s e
o f t h e u p p e r t ho r a c i c o u t l e t s y n d ro m e . Pa i n from
TrPs close to the a t la c h m e n t p o i n t s at t he ribs re fe rs
to t h e u l n a r aspect o f t h e u p pe r e x t re m i t y .
F o r t re a t m e n t w e u s e g r a v i t y - i n d u c e d P I R . T h e
p a t i e n t i s s u p i n e close t o t h e e dge o f t h e t a b l e wi t h
h e r a r m h a n g i n g d o w n o v e r t h e e d ge : t h e sl a c k i s
ta ke n up by t h e weig h t o f t h e a r m . S h e n ow raises
h e r s h o u l d e r a n ci a r m w h i l e b r e M h i n g i n s l owl y ,
h o l d s h e r b r e a t h a n d t h e n l e ts t h e a r m d ro p ,
b re a t h i n g o u t a n d re l a x i n g .
l i e s o n h e r si d e , t h e l o w e r l e g ( o n t h e t a b l e ) s t re t c h e d
o u t w h i l e t h e u p p e r i s b e n t a t t h e hi p : t h e k n e e o n
the table s t a b i l izes h e r tru n k . The exa m i n e r raises
t h e p a t i e n t ' s a r m so a s to c re a t e t e n s i o n a t t h e
p ai n fu l a t t a c h m e n t p o i n t a t t h e r i b s . T h e tech n i q u e
u s e d fo r r e l a x a t i o n i s s i m i l a r to t h a t s h o w n i n Fig u re
6 . 9 9 fo r t h e p e c t o r a l i s . For s e l f- t r e a t m e n t , gra v i ty ­
i n d u c e d P I R i s u s e fu l . T h e p a t i e n t l i e s o n h e r s i d e
i n the same position as d u ri n g exa m i n a ti o n ; she
b r i n gs h e r a nn i n to a b d u c t i o n w i t h r e t ro fl e x i o n , u n t i l
s h e h a s t a k e n u p t h e s l a ck . S h e t h e n bre a t he s i n
w h i l e ra i s i n g t h e a r m s l i gh t l y ( F i g u r e 6 . 1 0 1 , a b o ve ) ,
h o l d s h e r b r e a t h , a n d t h e n le t s t h e a r m d ro p b a c k
to t h e o r i g i n a l pos i t i o n , w h i l e s h e b r e a t h es o u t a n d
re l ax e s ( F i g u re 6 . 1 0 1 . b e l o w ) .
Copyrighted Material
220
Manipulalive Therapy in Rehabililalion of
the
Locomotor
Figure 6.101 G r a v i t y - i n d u c e d P I R of t h e s e r r a t u s
Syslem
Figu(e 6.102 G ra v i t y - i n d uced rel a x a t i o n ot t h e
latissimus
a n terior
dors i : above t h e e l b ow s l i g h t l y ra ised . be l ow i t d rops
M u sc u l u s latissi m u s d o rsi ( Fi gure 6 . 1 02)
pronation i n order to t a k e u p the slack. T h e p a t i e n t
i s t h e n told to s u pi n a te w i t h m i n i m a l fo r ce the
the ra p i s t r e s i s t i n g f o r a b o u t 1 0 s , a ft e r wh ich h e te l l s
t h e pa t i e n t t o ' l e t g o ' . W h e n re l a xa t i o n i s ach i e v e d ,
t h e t he r a pist b r i ng s the forearm fu rther i n to pro­
n a t i o n u n ti l the s l a ck has been t a k e n up once more.
A fter t h ree to five re petitions there is u s u a l l y no
d i ffe r e n ce be t w e e n the two sides, a n d p a i n should
be reduce d . For self-trea t m e n t the p a t i e n t pe rforms
t h e t h e rapist's m ove m e n t s w i t h h e r o w n h a nd s .
I f t h e ex te n sor s a r e i n tensio n TrPs c a n eas i l y b e
fo u n d a t t h e fore a r m ; t h e fl e x io n o f b o t h w r i s t a n d
fingers i s restricted o n t h e side o f t h e ten s i o n . i . e . we
c o m p a r e how fa r t he fi n ge rt i p s are from the forearm,
on each side, a t m a x i m u m c o m b i n e d flexion of the
wrist and fi n ge rs . F o r tre a t m e n t (Fi g u re 6. 104) t h e
t her a p i s t places h i s p a l m on t h e b a c k o f t h e p a t i e n t ' s
h a n d a n d h is fingers over h e r fl e x e d fingers, t a k i n g
up t h e s l a c k i n to flex i o n o f t h e fi n g er s a n d h a n d . He
then tells t h e p a t i e n t t o press her fingers s l i g h t l y i n to
extension ; a ft e r r e s i st i ng this p ressu re for a b o u t
1 0 s the t h e ra pist te l l s th e pa t i e n t t o ' le t go ' , i ncreasing
flex i o n of t h e w r i s t a n d fi n gers as fa r as re l a x a t i o n
a Uows. The p roce d u re i s r e pe a t e d a b o u t five ti mes.
For se lf- t r e a t m e n t t h e p a t i e n t p l a ces h e r t hen a r
e m i n e n ce a n d t h u m b o v e r h er flexed fi ngers .
,
This m uscle l i n ks t h e s h o u lder gird l e to the pelvic
g i rd l e ; i t a tt a c h e s a t the h u m e rus a n d t o g e t h e r w i t h
t h e teres major a d d ucts a n d e x te n ds the a r m . Ther e
c a n b e TrPs below the a x i l l a a n d f u r th e r d o w n t h e
b a c k . Pain rad i a tes from t h e shoulder-blade down
t h e u ln a r a s p e c t o f the arm. For t r e a t m e n t g r a v i ty
i n d uced P I R is most p r a ct i c a l . T h e p a t i e n t l ies o n
h e r s i d e , her back close t o t h e e d ge o f t he t a b l e ;
above a n d b e h i n d her h e a d she p l a c es her a r m , be n t
a t t h e e l bow w i t h the forearm h a n g i n g down. S h e
n o w ra ises t h e e l b o w w h i l e s l ow l y b r e a th i n g i n ; a ft e r
h o l d i n g h e r b r e a t h she J e ts the el bow drop a nd
b re a t h es o u t .
,
­
P a i nfu l lateral h u m eral epicondyle
In
a d d i tion to b l o c k a ge a t the e l bow t h e re is usually
tension in the s u p i n a tor, i n t h e extensors of the h a n d
a n d fi n gers, a n d i n the biceps. If t h e s u p i n a to r i s
t e n s e ( Figure 6 . 1 03 ) there i s r e s tr i c ted p ro n a t i o n on
t h e a ffected side. For t re a t me n t t h e p a t i e n t m a y b e
s u p i n e or s e a t e d , w i t h the e l bow flexed and fixe d b y
t h e t h e r a p i s t a ga i n st t h e p a t i e n t 's tru n k . He stands
fa c i n g the p a t i e n t a n d b r i n g s h i s fore a r m i n t o
Copyrighted Material
.
Th erapelltic techniq ues
( b)
( a)
Figure 6. 103
( a)
(al
Exa m i n a t i o n a n d t r e a t m e n t of te n s i o n i n t h e s u p i n a tor. (b) S e l f- t re a t m e n t
( b)
Figure 6. 104 ( a l Exa m i n a ti o n a n d t re a t m e n t of t e n s ion i n t h e e x t e n sors of t h e h a n d a nd
Copyrighted Material
finge rs. (b)
S e l f- t re a t m e n t
22 1
222
Man ip ulative Therapy in Rehab ilitlltion of t h e L o co m o {o r System
bri ngi ng h e r w r i s t i n to fl e x i o n . S h e t h e n co n t i n u e s
s a m e m a n ne r as t h e thera pist.
I f t h e b i c e ps i s i n te n s i o n , e x te n s i o n o f t h e e l b o w
i s ( s l i gh t l y ) r e s t r i c t e d . For t r e a t m e n t (Figu r e 6 . 1 0 5 )
t h e thera pist exte nds the patient's e l b o w so as to
i n the
take
up
the
slack a nd
asks
her
t o e xe rt
s l ight
I n te r m i t t e n t a n ta g o n i s t s t i m u l a t i o n is b o t h s i m ple
and
e ffective
with all
three m u scles i n volved in
pain
a t t h e l a t e r a l e p i co n d y l e . T h e p a t i e n t e x e rts m o d e r ­
a te p r e ss u re i n t h e d i re c t i o n o f r e l a x a t i o n , a g a in s t
res i s ta nce by the t h e ra p i s t ,
i n c r e a s i n g a n d l o we r i n g i t .
ra p i d l y a n d r hy t h m i c a l l y
c o u n t e r- p re s s u r e fo r a b o u t 1 0 s , fo l l o w e d by re l a x ­
a t i o n i n to ex t e n s io n .
Th i s i s re p e a t e d t h re e t o fi v e
s e l f-tre a t m e n t t h e p a t i e n t u s e s h e r o w n
k n ee a s a fu l c r u m ; s h e may a l s o use g r a v i t y - i n d u ce d
P I R by a l t e r n a te l y u ft i n g t b e fo r e a r m a b o u t 2 c m ,
h o ld i n g t h i s p o s i t i on fo r a b o u t 20 s , a n d t h e n
times.
For
re l a x i n g i n to e x t e n s i o n fo r a n o t h e r 20 s .
P a i nfu l m e d i a l h u mera l epicondyle
I n t h i s c o n d i t i o n t e n s i o n i s fe l t i n t h e fl e x o r s a t t h e
t r e a t m e n t ( Figu re 6 . 1 06) t he p a t i e n t
s i t s f a c i n g t h e t h e r a p i s t , w i t h h e r e l bow fl e x e d a n d
fore a r m . For
t h e h a n d i n d o r s i fl e x i o n a t t h e w ri s t . T h e t h e r a p i s t
threads
his
fi n ge rs b e twe e n t h e p a t i e n t s
'
thumb
and
fo r e fi n ge r , fro m t h e r a d i a l t o t h e u l n a r s i d e , w i t h h i s
t h u m b o n t h e d o r s a l s u rface o f t h e h a n d ac t i n g a s
a
f u l c r u m . He t h u s
takes u p t h e s l a c k i n t o pro n a t i o n
by s l i g h t l y p r e s s i n g h i s li ng e r s a ga i n s t t h e u l n a r s i d e
o f t h e p a t i e n t s p a l m . He t h e n t e l l s t h e p a t i e n t to
r e s i s t t h i s m ov eme n t b y s l i g h t cou n t e r- p ress u re i n to
s u p i n a t i o n. A ft e r a b o u t 1 0 s t h e p a ti e n t is to l d t o ' l e t
go ' , i n c r e a s i n g p ro n a t i o n a n d d o r s i fl e x i o n d u r i n g
re l a x a t i o n . Th i s p r oc e d u r e i s r e p e a t e d t h r e e to five
tim es.
'
F o r se l f- t re a t m e n t t h e p a ti e n t h o l d s t h e a ffe cted
h a n d in
the
h a nd she
t reated ,
the dors a l
same way, but with h e r o t h e r
g r a s p s t h e u l n a r a s pect o f t h e h a n d b e i n g
on t h e p a l m a r s i d e , p l a c i n g h e r t h u m b on
aspect a s a fu l c r u m s o as to t il k e u p t h e s l a c k i n to p ro­
n a t i o n S h e t h e n r e p e a t s t h e t h e ra p i s t ' s m o v e me n t s .
.
P a i n a rising i n t h e long head o f t h e biceps
T h i s sh o u ld be
a rm a t
the
d i agnosed
b y ra ising t h e se m i - fl e x e d
s h o u l d e r , a ga i n s t re s i s t a n c e . To p a l p a t e
t e n d e r n ess o f t h e l on g t e n d o n o f t h e b i c e ps b e twee n
t h e t u b e r c l e s a n d t h e c r i s t a e of the h u m e r u s is v e ry
mi s l e a d i n g , because t h e re a r e fre q u e n t l y pa i n fu l
a ttach m e n t p oi n t s o f t h e s u bsca p u l a r i s a n d t h e
i n f r a sp i n a t u s a t b o t h t he s e s t r u c t u r e s .
( b)
Figure 6, 1 0 5
(a)
E x a m i n a t i on a n d t rea t m e n t o t t e n sion i n t h e b i c e p s brach i i . ( i» Se l f- t re a t m e n t
Copyrighted Material
Th erapetllic lecil niq w.l
( a)
223
( b)
Figure 6. 1 06
(a)
Ex a m i n a t i o n a nd
Fo r t r e a t m e n t ( F i g u r e
t re a t l1l e n t
6. 1 07 )
o f te nsion i n t h e tl e x o rs of t h e h a n d a n d fi ngers. ( h ) Se l f- t rc a t m c n t
t he patie n t sits in
fro n t of t h e t h e ra p i s t w i t h h e r h a n d be h i n d h e r b a c k
Ten s i o n i n the s u p raspinatus m u scle
t h e d o r s a l a s pect o f t h i s h a n d p a ss i n g o v e r t h e
I n this co n d i ti o n , a b d u c t i o n a ga i n s t r e s i s t a nce i s
buttock on t h e opposi te s i d e . The therapist grasps
pa i n fu l a n d t h e re is a T r P i n t h e fo ssa s u p ra sp i n a t a .
stands
t h i s h a n d , b r i n g i ng i t i n t o p r o n a t i o n to t a k e u p t h e
For
s l a c k . I n this pos i t i o n t h e pa t i e n t i s t o l d to a p p ly
p a t i e n t s e a t e d o n t h e t a b l e ( F i g ure 6 . 1 09 ) a n d b r i n gs
s l i g h t c o u n t e r- p re ss u re ( i n t o s u p i n a t i o n ) , resisted for
t h e p a t i e n t' s tle x e d a r m i n t o a d d u c t i o n in fro n t o f
t re a t m e n t
the
t h e ra p i s t
be h i n d
the
a b o u t I Cl s b y t h e t h e r a p i s t . T h e p a t i e n t is t o l d to
h e r ches t . t o t a ke u p t h e s l a c k . I n t h i s pos i t i o n t h e
'Jet go' and re l a x i n t o !,ron a t i o n a n d s i m u l t a n e o u s
e x t e n s i o n a t t h e e l b ow. T h i s i s r e p e a t e d t h ree t o fi v e
p a t i e n t i s t o l d t o e x e r t s l i g h t c o u n te r- p re s s u r e i n to
a bd u c t i o n a n d to b re a t h e i n ; t h e t h e r a p i s t r e s i s t s t h i s
t i m e s . F o r s e l f- t r e a t m e n t t h e p a t i e n t d e a l s w i t h h e r
press u r e fo r a b o u t l Os , w h e n t h e p a t i e n t is told to
own h a n d i n e x a c t l y t h e s a m e w a y .
' l e t go' a n d b re a t h e o u t . D u ri ng this re l a x a t io n p h a s e
t h e t h e r a p i s t bri ngs t h e a r m fu r t h e r i n t o a d d u ct i o n .
Pain arising i n the m . triceps
( Fig u re
This
6 . 108)
is
repeated
a bout
t hr e e
t i m es .
For
s e l f­
t r e a t m e n t t h e p a t ie n t d oe s e x ac t l y t h e s a m e , u s i n g
TrPs in t h e t r iceps may c a u se e p i c o n d y l a r p a i n . A
her own h a n d .
TrP of t h e l o n g h e a d of t h e t r i c e p s , w h i c h a t t a c h e s
to t h e sca p u l a , ca uses p a i n a t t h e a x i l l a ( K ro b o t ,
1 99 4 ) . T h i s pa i n i s p r o v o k e d by p u s h i n g t h e a rm
aga i n s t res i s t a n c e . Tre a t m e n t ( s e l f- t re a t m e n t ) is b y
gra v i ty-i n d u ce d P I R :
the
p a t i e n t l i fts
h e r e l bo w
Tensi o n i n t h e i nfraspinatus m u scle
I n t h i s c o n d i ti o n e x te rn a l r o t a t i o n aga i n s t res i s t a n ce
is
pa inful
and
there
are
TrPs
in
the
fossa
a b ove h e r h e a d w i t h t h e Fo re a r m h o r i zo n t a l ; s h e n ow
i n fr a sp i n a t a .
s l ig h t ly ra i s e s h e r fore a r m for a b o u t 20
a ft e r t h a t
a d v a n t a ge o u s ( F i g u r e 6 . 1 1 0 ) . T h e p a t ie n t l ies s u p i n e
another 20 s.
w i t h h e r a rm i n a b d uc t i o n o v e r t h e s i de o f t h e ta b l e
she
lets
i t d rop
and
re l a xes
[or
S,
H e re
gravi t y - i n d uced
PIR
is
most
R h y t h m i c i n te r m i t t e n t c o n t r a c t i o n o f t h e b i c e p s
a n d t h e e l b ow b e n t a t r i g h t a ng l e s , t h e fore a r m
a g a i n s t l i t t l e r e s i s t a nce w i l l e n h a n c e the e ffect o f
p o i n t i n g t o w a r d s t h e h i p . B y re l a x a t i o n t h e s l a c k i s
re l a x a t i o n .
t a k e n u p i n i n t e r n a l r o t a t i o n a t t he s h o u ld e T . T h e
Copyrighted Material
224
Manipulative Therapy in Rehabilitation of th e Locomotor System
( a)
( b)
Figure 6.107 ( a ) E x a mi n a t i o n a n d t re a t m e n t of t e ns i o n i n t h e biceps if t h e l o n g t e n d o n is p a i n fu l . ( b ) S e l f- t re a t m e n t
( a)
( b)
Figure 6.108 Grav i t y - in d uced P I R of t h e triceps: (a) the fore a r m r a i se d : ( b ) rela x a t ion
Copyrighted Material
Th erapeUlic techniques
225
( b)
( a)
Figure 6. 109 ( 0 ) E x a m i n o t io n a n d t r e o t m e n t of te n s i o n i n t h e s u p ra s p i n a t u s . ( b ) Se lf- t re a t m e n t
Figure 6.110 Gra v i ty - i n d uced P I R of t h e
i n fras p i n a t u s m u s c l e : t h e a r m i s h e l d o v e r
the
e d g e o f t h e t a b l e , i n i n t e rn a l ro t a t io n . Left : the
a rm is slightly raised; righ t : it d ro p s , re l a x e d
pa t i e n t n o w l ifts t h e fore a r m a b o u t 2
em,
holding i t
fo r a bo u t 2 0 s , t h e n rel a x i n g i n to i n te r n a l r o t a t i o n
for a n ot h e r 20
s.
p o i n t s . The
T h i s i s re p e a t e d a b o u t t h r e e t i m e s .
adduction
and
p a tie n t
i s s u p i n e , h e r a r m a b d ucted a s
fa r a s h e r c o n d i t i o n a l l o w s , t h e e l b o w fl e x e d a t r i g h t
Ten sion i n the s ubsca p u laris m uscle
,
h e t o u c h e s t he m u s c l e , t h e
H e r e , t o o , grav i t y - i n d uced P I R i s t h e t re a t m e n t o f
choice. The
I f t h i s m u sc l e co n t ra c t s
mome nt
p a t i e n t w i l l r e a c t o n t h e a ffec t e d s i d e .
a n g l e s a n d t h e fo r e a r m i n e x te r n a l ro tation (Figure
i n t e rn a l
r o t a t i o n resu l t , i . e . t h e ' froze n s h o u l d e r ' p os iti o n I t
.
6 . 1 1 1 0 ) , r e l axed s o as to t a k e up t h e slack by the
wei g h t of t h e fo re a r m . S h e n o w r a i se s her a rm
about
ap p e a r s t h a t t h e re is i n d e e d a c l os e re l a t i o n s h i p
2 em
between t h e m u scl e a n d t h i s c o n d i t i o n , a n d t h a t
re l a x e s i n to e x t er n a l rota t i o n . I f s p a s m i s s o sever e
p a i n f u l s p a s m o f th e s u bsca p u l a ri s , w i t h
a n d h o l d s t h i s p os i t i o n for a t l e ast 20 s , t h e n
.
t r i gger
t h a t exte r n a l ro t a t i o n is too l i t t l e fo r g ra v i ty to b e
a c c o m p a n i e s froze n s h o u l d e r from t h e out­
s e t . B e s i d e s t h e c l i n ica l p i c t u r e o f 'frozen s h o u l d e r '
with p a i n r a d i a t i ng to t h e w r i s t , t h e re may s i m p l y b e
p a i n i n t h e s h o u l d e r or t h e s h o u lder- b l a d e , or e v e n
i n t h e thorax ( i f this p a i n is o n t h e l e ft , i t m a y i m i t a te
c a r d i a c p a i n ) There m a y be p a i n a t t h e l u ngs, w i th
re sp i r a to r y r e s t ri c t i o n
D i rect p a l p a t i o n is e s s e n t i a l for d i a g n o s i s . For this
t h e p a t i e n t i s s u p i n e with the u pper e x t r e m i t y i n
e ffe c t i v e i n t h e s u p i n e p o s i t i o n , t h e p a t i e n t m a y l i e
p oin t s
,
.
.
o n t h e a f fe c t e d side (Figure
6.1 1 1 b ) .
The p r o ce d u re
m u s t be re p e a t e d t h r e e to five t i m e s . This is o n e o f
t h e fe w e ffe c t i v e m e thods o f d e a l i n g w i t h a frozen
s h o u ld e r .
P I R o f b o t h t h e i nfra s p i n a t u s a n d s u b sca p u l a r i s
c a n be c o n s i d e ra b l y e n h a n ced b y r h y t h m i c p re s s u r e
of
l i t t le force against the p a t i e n t
'
s fo r e a rm
,
i n the
d i recti on of r e l a x a ti o n . T h i s i s r e s i s t e d b y t h e p a t i e n t .
s l ight a b d u c t i o n . T h e t h e r a pist grasps the pa t i e n t s
'
h a n d a n d g i ves a x i a l t r a c t i o n w h i l e w i t h t h e fi n gers
o f the o t h e r h a n d h e pe n et r a t e s ove r the e d g e of the
l a tissi m u s do r s i o n to the v e n t r a l aspect
s c a p u l a w i t h the s u b s c a p u l a r i s m u s c l e a n d i ts
of
Tension in the erector s p i n a e
the
I ncreased t e n s i o n a n d p a i n , incl u d i n g trigge r p o i n t s ,
tr i gge r
a re v e r y fre q u e n t in a l l p a r t s of t h e e rector s p i n a e
Copyrighted Material
226
Manipl liati ve Th erapy in Rehab ilitation of the Locomotor System
( a)
( b)
Figure 6.111 (a)
G ra v i ty-i nd uced P I R of t h e s u bsca p u l a r i s . T h e a r m is he ld over t h e e d g e o f t h e . " h l e . I n e x t e r n a l
is s l i g h t l y r a i s e d : righ t , it d ro p s . re l a x e d . ( b ) G r a v i t y - i n d u c e d P J R o f t h e s ubsca p u l a r i s i n a
froze n s h o u l d e r w i t h seve re m o ve m e n t re s t r i c t i o n : l e ft . the fore a rm rn i sed i n i n w ard r o t a t i o n of t h e s h o u l d e r : r i g h t . t h e
fore a rm l o wered i n o u t w a rd rota t io n of t h e s h o u l d e r
rot a t i o n . Le ft , t h e a r m
Figure
6 . 1 12 G r a v i ty - i n d u ced P I R o f t h e ce rvi c a l a n d u p p e r t ho r a c i c e r e c t o r s p i n a e : t h e ro t a t e d h e il d over t h e edge o r
t h e table i s
(left )
sl ightly
raised ( i n h a l a t i o n ) a n d
then
( righ t )
re l a x e d . w h e re u pon i t d r o p s ( e x ha l a t i o n )
Copyrighted Material
Th erap eu / ic techniques
m uscl e .
If t h e m u s c l e is s h o r te n e d , fu l l s t r e tc h i s
o b t a i n e d b y a n t e A e x i o n , s i d e - b e n d i n g a n d ro t a t i o n
to e a c h s i d e .
227
o p p o s i t e d i re c t i o n ; t h e t h e r a p i s t res i s t s t h e a u to­
m a t i c c o u nter- p ress u re w h i l e t h e p a t i e n t b r e a t h e s in
p a t i e n t i s t h e n told to look t o the s i d e
o f rota t i o n a n d to b re a t h e o u t . Th i s is r e p e a t e d
s l ow l y . The
Treatment o f the cervica l a n d u p p e r
thoracic part o f the erector s p i n a e
a b o u t t h re e t i m e s .
For t re a t m e n t o f t h e u p p e r t ho r a c i c e re c t o r s p i n a e
t h e tec h n i q ue i s t h e s a m e , e x ce p t t h a t t h e t h e ra p i s t
H e r e , gra v i ty- i n d uced
d oe s n o t fi x t h e s h o u l d e r , b u t t h e u p p e r r i b s , i n a
s l i g h t l y o ve r t h e e n d of t h e ta b l e a n d t u rn e d tow a rd s
t h o r aci c s p i n e
( Figure 6 . 1 1 2 ) :
P I R is u s e f u l a n d s i m p l e
t h e p a t i e n t l i e s p ro n e , h e r h e a d o n l y
m a n n e r s i m i l a r to r e s t r i c t e d a n t e flex io n of t h e u pp e r
(s e e
Figure 6 . 3 7 , p . 1 82 ) .
t h e s i d e o f i n te n d e d t r e a t m e n t , so t h a t i t i s s u p por t e d
b e t we e n t h e c h i n a n d t h e m a s t o i d p r o ce s s . I f t h e
cervica l p a r t o f t h e m u s c l e is to be re l a x e d , t h e h e a d
is o n l y v e r y s l i g h t l y l i ft e d , so t h a t t h e c e r v i c a l p a r t
c o n t r a c t s : t h i s p os i t i on is h e l d f o r a w h i l e , t h e p a t i e n t
s l o w l y b r e a t h i n g i n . T h e n s he re l a xe s , s l o w l y d r o p ­
p i n g h e r h e a d . J [ t h e u p p e r t h o ra c i c p a r t of t h e
m usc l e is to be t re a te el , t ile h e a d is r a is e el fu r t l 1 e r .
u n t i l c o n t r a c t i o n is fe l t. A g a i n t h e p a t i e n t b r e a t h e s
i n sl o w l y , w h i le eI u r i ng e x h a l a t i o n s h e r e l a xe s a n d
d r o ps h e r h e a d o v e r t h e e d g e o f t h e t a b l e . Th i s is
r e p e a ted a b o u t t h r e e t i m e s .
The e r e c t or s p i n a e o f t h e ce r v i c o t h or a c i c j u n c t i o n
a n d in t h e u p pe r t h o r a c i c r e g i o n is a ls o t r e a te d w i t h
t h e p a t i e n t seateel i n fro n t o f t h e t h e ra p is t . Fo r t h e
cervico t h o r a c i c r e g i o n ( F i g u r e 6 . 1 1 3 ) t h e t h e ra p i s t
fi x e s t h e s h o u l d e r o n t h e s i d e o f t re a t m e n t w i t h o n e
h a n el , w h i le t h e o t h e r p a s s e s r o u n d t h e patie n t 's
h e a el t o bend i t forw a rd t o the s i d e a n d i n to ro t a t i o n
a w a y f r o m t h e a ffe c te d s i d e , u n t i l h e h a s t a k e n u p
t h e s l a c k . The p a t i e n t is t h e n t o l d to l oo k i n t h e
Treat m e nt o f the l ower t h o racic a n d
u p p e r l u m b a r p a rt of the erector s p i n a e
T h e p a t i e n t is s e a t e d (Figu re 6 . 1 1 4 ) , her h a n d s
c l asped b eh i n d her n ec k . The the ra p ist stands
be h i n d b e r a n d t h re a d s b i s a r m u n d e r t h e a x i l l a o f
t b e p a t i e n t to t h e s h o u l d e r o n the o p p o s i t e s i d e ( t he
s i d e of tre a t m e n t ) , so as to o b t a i n a n t e A e x i o n , s i d e ­
b e n d i n g a n d ro ta t io n . Th e s u m m i t o f t b e c u r v e t h u s
obtai ned
maxi mum
s h o u ld
tension
c o r r e s po n d to the
( t r i g ge r p o i n t ) . I n
po i n t
of
o rd e r
to
a c h i e v e this the t h e ra p ist s u p p o r t s t h e p a t i e n t w i t h
h i s t h i gh , w h i c h a c t s as
a
f u l cr u m , p l a c i n g h i s k n e e
o n t h e t a b l e o n the s i d e t o wa r d s w h ic b th e p a t i e n t
i s b e n t a n d ro t a t e d . A ft e r t a k i n g u p t h e s l ac k i n
a n te A e x i o n , s i d e - b e n d i n g a n d ro t a t i o n , t h e p a t i e n t i s
told t o l o o k i n t h e o p p o s i t e d ire c t i o n a n d t o b r e a t h e
s l owl y i n to t h e t o p of the c u rve , w h i l e t h e t h e ra p i s t
r e s i s t s t h e a u to m a t i c t e n d e n c y fo r h e r t o t u r n to t h e
o p p o s i t e s i d e . A ft e r t h is , t h e p a t i e n t i s t o l el t o l o o k
towards the si de o f
r o t a ti o n
a n d t o b re a t h e o u t ,
a u t o m a t ic a l l y re l a x i n g over t h e t h e ra p i s t ' s t h ig h .
T h i s is r e p e a t e d a b o u t t h r e e t i m e s , the f r e e h a n d
c h e c k i n g m u scle r e l a x a t i o n .
For
with
the
l a s t t w o t e c h n i q u e s i t i s i m p o r t a n t to s t a rt
a n te A e x i o n
d o w n to t h e TrP t o be t re a t e d a n d
o n l y t hen to s i el e - b e n d , a n ci to ro ta te t h e h e a d - b u t
o n l y s o fa r a s t o cre a t e t e n s i o n i n t h e e r e c to r s p i n a e .
Figure 6. 1 1 3 P l R o f t h e ce r v i co t h o r a c i c p a r t
spinae with the patie n t seated
erector
of
the
Figure 6.114 P I R o f t h e t h oraco l u m b a r p a r t o f t h e
e re c t o r s p i nae w i t h t h e p a t i e n t s e a t e d
Copyrighted Material
228
/v/anipuiative Therapy in Rehabilitation of the LOCOIIWlOr S vstCI I I
Treatm e nt of the low l u m ba r erector
spinae
G r a v i ty -i n d u ce d r I R i s m o s t s u i ta b l e , a s i t is a lso a
m e t h o d of s e l f- t r e a t m e n t
( Figure
6 . 1 1 5 ) . B e ca u se
t h e p o s i t i o n i s i d e n t ic a l w i t h t h a t u se d for m o b i l ­
i z a t i o n of t h e l u m b a r sp i n e i n to fl e x i o n ( s e e F i g u r e
p . 177), t h i s tech n i q u e can a ls o be used for s e l f­
m ob i l izati o n of t h e l u m ba r s p i n e . T h e p a t i e n t l i e s on
6.31 ,
her s i d e in
k y p h o s is ,
and knee, the
t h e lower l e g b e n t a t t h e h i p
u p per h a n g i n g o v e r t h e e d ge of
the t a b l e bri n g i n g the pe lv i s i n to a forw a rd - t i l te d
p o s i t i o n : s h e l o o k s u p a t t h e c e i l i n g i n order to r o ta t e
t h e h e a d a n d s h o u l d e r i n t h e o p p o s i te d i re c t i o n from
that o f t h e p e l v i s . I n t h is p o s i t i o n t h e p a t ie n t r e l a x e s
a n d t h e w e i g h t of t he le g h a ng i n g d o w n is s uffici e n t
to t a k e u p t h e s l a c k of t h e low l u m b a r e r e c t o r s p i n a e .
2 em, breathing
i n sl o w l y ; d u ri n g e xp i ra t i o n s h e l e t s t h e l e g fa l l
T h e p a t i e n t t h e n l i fts t h e l e g a b o u t
s l ow l y ,
i n c re a s i n g
l umba r
k yp h o s i s
and
pe l vic
rota ti o n . Th i s tec h n i q u e m a y be u s e f u l l y a p p l i e d i n
t h e t r e a tm e n t o f p a i n a t t h e s p i n o u s processe s , m o s t
f r e q ue n t l y b e t w e e n
L4
a n d S I ; t h e p a i nful s ide must
l i e u p pe rmo s t. Here i t is h e l p f u l i f t h e t h e r a p i s t fi rst
fixes t h e t e n d e r s p i n o u s p rocess from above, to g i v e
t h e p a t i e n t t h e ex a c t fe e l o f t h e d i re c t i o n o f t h e p u l l
of t h e h a ngi n g l e g .
For s e l f- t re a tm e n t of the e rector s pi n a e wh i.le
s e a te d , the fo l lo w i n g te c h n i q u e is e ffe c t i ve (Figure
6 . 1 1 6) : w i t h h e r hand o n t h e top of h e r head t h e
p a t i e n t b r i n gs h e a d a n d tru n k i n to a p o s i t i o n o f
a n te fl e x i o n , s i d e - b e n d i ng a n d r o t a t i o n , tre a t i n g t h e
e rec to r s p i n a e o n t h e c o n v e x s i d e . T h e c u r v e s h o u l d
c u l m i n a t e a t t h e p o in t w h e re t r e a t m e n t i s ind i c a te d .
A ft e r t a k i n g up t h e s l ac k , t h e p a t i e n t l o o k s i n t h e
o p p o s i t e d i re c t i o n fro m the ro t a t i o n , r e s i s t i n g t h e
a u t o m a t i c m o v e m e n t i n t h e r e v e rse d i r e c ti o n b y t h e
6.1 16
Se l f- t re a t m e n t of t b e e rect o r s p i n a e , s i t t i n g :
h e a d i n d u c e s a n t e fl ex i o n , ro t a t i o n a n d
s i el e - b e n d i n g o f t h e t ru n k . t h e c u r v e cu l m i n a t i n g a t the
p oi n t w h e re tre a t m e n t i s a p p l i e el
Figure
the
hand on the
h a n d o n h e r h e a d , w h i l e s l o w l y b re a t h i n g i n . S h e
h o l d s h e r b re a t h a n d t h e n l o o k s i n t h e o p p os i t e
d i r e c t i o n ( t h a t o f ro t a t io n ) a n d b re a t h e s o u t , a u t o ­
m a t i c a l l y p r o d u c i n g re l a x a t i o n . T h e p ro c e d u r e i s
re p e a t e d a b o u t three t i m e s . W h e re g r a v i ty - i n d u ced
P I R i s used n o
o th e r
s e l f- t re a t m e n t i s n e e d e d .
P a i n c l o s e t o the m e d i a l a n g l e o f the
sca p u l a i n the middle trapezius
Figure 6.115 Gra v i t y- i n d uced P I R o f t h e lowe r l u m b a r
patient on h e r s i d e : l e f t , the leg
h a n g i n g ov e r t h e side o f t h e t a b l e is s l i g h t l y r a i se d
( i n h a l a t io n ) ; r i g h t , t h e leg d rops i n r e l ax a t i o n ( e x h il l a tion )
e recto r s p i n a e w i t h t h e
P a i n c l o s e to t h e m e d i a l a n g l e o f t h e sca p u l a w i t h a
p a i n p o i n t a t t h i s s i t e is t h e r u l e i n rad i c u l a r
sy n d r o m e s i n t h e u p p e r c' x l re m i t y a n d i s also
fre q u e n t l y fo u n d i n n o n - ra d i c u l a r ce r v i co b r a ch i a l
s y n d r o m e s . Fo r d i a gn o s i s t h e e x a mi ne r a d d u cts t h e
p at i e n t ' s e l bo w towa rds t h e c h e s t s o a s t o cre a te
t e n s i o n a t t h e a t t a c h m e n t p o i n t o f t h e m uscle at t h e
s c a p u l a . I n cr e a s e d te n s i o n c a n frequ e n t l y be see n ,
t h e m u scle protru d i n g l i k e a r o p y b a n d : a t t h i s poi n t
a p a i n f u l T r P c a n be fo u n d b y s n a p p i n g p a l p a t i o n .
Trea t m e n t fo l l o w s t h e s a ill e t e c h n i q u e as t h a t fo r
d i a g n o s i s ( Fi g u re 6 . 1 1 7 ) . Fo r t h i s p u r p o s e the
p a t i e n t ' s e lbow is a d d ucted t o w a r d s her chest i n the
h o r i zo n t a l p l a n e , t o take u p t h e s l a c k . She i s s e a t e d
i n fro n t o f t h e t h e r a p i s t w h o t e l l s h e r t o g i ve s l igh t
co u n t e r - p ress u r e w i t h h e r e l b o w a n d to b re a t h e i n to
Copyrighted Material
Therapell tic techniq ues
229
( a)
( a)
( b)
PIR of t h e m i d d le
t r a p e z i u s : t h e p a t i e n t l i e s on h e r s i d e w i t h t h e a r m o v e r
t h e e d g e of t h e t a b l e . ( II ) S h e ra i ses h e r e l bow s l ig h t l y ,
t h u s c o n t ra c t i n g t h e m i d d l e trape z i u s , a n d b r e a t hes i n :
( b ) s h e l e t s t h e a rm d ro p , re l a xes a n d brea t h e s o u t
Figure 6.118 G r a v i t y - i n d uced
the p a i n fu l a re a . S h e h o l d s h e r b re a t h , t h e n r e l a x e s
a n d br e a t h e s o u t s l ow l y I n s e l f- t r e a t m e n t t h e p a t i e n t
u s e s h e r o t h e r ha n d a g a i n s t h e r elbow, i n t h e same
w a y a s the t h e ra p i s t . Grav ity- i n d uced PIR m a y be
ev e n b e t t e r . The p a t ie n t l ie s on the no n - p a i n f u l s i d e
a t the e d ge of t h e ta b le , h e r a r m h a n g i n g a l m o s t
v e rtica l l y over t h e edge. S he n o w r a i s e s t h e e l bow
s l i g h t l y , brea t h i n g in s l ow l y ; s h e holds her bre a t h
a n d t h e n l e t s t h e a r m dro p w h i le b r e a t h i n g o u t
s l o w l y (Figu re 6. 1 1 8 ) .
.
Tension i n t h e q u a dratus l u m bo r u m
For t a u tness o f t h i s m u scle s e e p. 1 2 6 ( F i g u re 4.54).
be p a l p a t e d by a p i n ce r m o v e m e n t of
the t h u m b a nd fo r e fi nge r a t the w a i s t , c o m p a r i n g t h e
two s i d e s . T h e p a ti e n t m a y b e p r o n e o r s u p i n e ; d e e p
trigger po i n t s a re b e t ter p a l p a ted w i t h t h e p a ti e n t
l y i ng o n h e r side. Te n s i o n i n t h i s m u sc l e m a y i n ter­
fere with s i d e - b e n d i n g of t h e t r u n k , a n d ca u s e p a i n
a t t h e l o w e s t ribs a n d o n t h e i l i ac crest. I t i s tre a ted
very simply by gravity-i nduced PIR ( Fi g u r e 6. 1 1 9) .
TrPs sh o u l d
,
( b)
Figure 6.1 17 ( a ) Exa m i n a t i o n a n d tre a t m e n t of t e n s i o n i n
t h e m i d d l e t ra p e z i u s . ( b ) S e l f- t re a t m e n t
Copyrighted Material
230
iVlanip u lalive
Th erapy in Relw/)ilit{l/iull of
Ihl'
L o co m u t o r
S vslem
b re a th e s o u t s l o w l y . t h e m u s c l e r e l a x e s a n d s i d e ­
be n d i n g i n c r e a s e s i t s r a n g e , T h i s tech n i q u e i s p a rt i ­
c u l a r l y e ffect i v e ; h o w e v e r . i t o n l y w o r k s a u to m a t i ca l l y
i f t h e p a t i e nt h a s i n d e e d c o m p le t e l y re l a x e d w h e n
t a k i n g up t h e s l a c k ,
T h e i l i opsoas m u scle
I n c re a s e d t e n s i o n
i n t h e p s o a s m u s c l e i s fe l t
(Tr Ps)
t h r o u g h t h e a b d o m i n a l w a l l . p a ra l l e l t o t h e s pi n a l
c o l u m n . w h i l e t e n s i o n (Tr P s ) o f t h e i l i a c u s i s p a ra l l e l
t o Po u p a r t ' s l i ga m e n t i n t h e i n no rri i n a t e , For t re a t ­
m e n t (Figure
exam i n a ti o n
6 , 1 20) we u s e t h e
( s e e F i g u re 4,52,
s a m e p os i t i o n a s fo r
p,
1 25 ) .
e m p loy i n g
g ra v i ty - i n d uced P I R T h e p a t i e n t is t o l d to l i ft h e r
Figure 6. 1 1 9 G r a v i t y - i n d uced P I R o f the q u a d ra t u s
l u m b o rLI lll wi t h t h e p a t i e n t s ta n d i n g w i t h legs a p a r t .
bend i n g s i d e w a y s : I d t . t r u n k s l i g h t l y ra i sed d u r i n g
k nee s l ig h t l y ( a b o u t
2
m ) a n cl t o bre a t h e i n s l ow l y .
a n d t h e n s l o w l y t o l e t t h e k n e e cl ro p w h i l e b re a t h i n g
out.
i n h a l a t ion a n d looking up: right. i n creased side-bending
d u ri n g e x h a l a t i o n , l o o k i n g d o w n
and
re l a x i n g
Ten s i o n i n the rectus a b d o m i n is
I n c r e a s e d te n s i o n i n t h e s t r a i g h t a b d o m i n a l m u scles
T h e p a t i e n t s t a n d s w i t h h e r l e gs a p a r t a n d re l a x e s
may m a n i fe s t i t se l f in t r i g g e r p o i n ts c a u s i n g re ferred
i n t o m a x i m u m s i d e - be n d i n g ( t a k i n g u p t h e
p a i n s i m u l a t i n g v i s cera l cl i s e a s e . a s well
slack),
ca use
O n l o o k i n g u p w h i l e t a k i n g a s l o w d e e p b r e at h . h e r
pai n , It may
q u a d ra t u s l u m bo r u m a u t o m a t i ca l ly co n t ra c t s . sl i g h t l y
back-be n d i n g rest ri ct i o n .
ra i s i n g t h e t r u n k ; w h e n t h e p a t i e n t l oo k s d o w n a n d
t ri gg e r
points
is
as
low- back
a fo rw a r d - d r a w n p os t u re a n d
best
D i re c t p a l p a t i o n o f t h e
p e r fm m e d
with
a
p i ncer
( a)
Figure 6. 1 20 ( 0 ) G r a v i t y - i nd uced P I R o f t h e
patient l i es su p i ne w i t h her
b u tt o c k s a t t h e e d g e o f t h e t a b l e . d r a w i n g
o n e k n e e t o t h e c h e s t w h i l e t h e o t h e r leg
h a n g s o v e r t he e d ge o f the t a b l e , L e f t . t h e
l e g i s s l ig h t l y r a i s e d : r i g h t , s h e l e t s i t d r o p , i n
r e l a xa t i o n , ( iJ ) G r a v i t y - i n d u c e d P I R of t h e
i l i opsoas: t h e
r e c t u s a b ci o m i n i s : t h e p a t i e n t l i e s s u p i n e w i t h
a t t h e e d �l' o f t h e { a b l e . h e r
e d g e . O n e is s u p p o r t e d
b y a s t o o l w h i l e t il e b u t t oc k o f t h e fre c ­
h a n g i ng l e g is r a i s e d b y i\ c u s h i o n . L e ft. t h e
l e g i s s l ig h t l y r a i s e d at t h e k n e e : r i g h t . she
lets it d r o p . i n r e l a x i1 l i o n
h e r b u t t ocks
l egs h a ngi n g o v e r t h e
( b)
Copyrighted Material
Th erapeulic lechn iques
( a)
23 I
( b)
Figure 6. 1 2 1 G ,'a v i t y - i n d uced P I R of t h e re c t u s fe m o r i s : t h e p a t i e n t 's b u t t oc k s a r e n e a r t h e e d ge of t h e t a b l e . o n e k n ee
drawn ( 0 (he c h cs ( w h i l e t h e o t h e r h a ngs o v e r t h e e d g e o f ( h e t a b l e , ( a ) T h e l e g i s s t r e t c h e d a t t h e k n e e f o r 20 s: (b) it
h a ngs d o w n re l a xe d fo r 20 s
m o ve m e n t by a h a n d on
each
s i d e of t h e s t r a i g h t
a b d o m i n a l m u sc l e : i n c r e a s e d te n s i o n i n t h e a bd o m ­
i n a l w a l l is e a s i l y p a l p a t e d . It is a l so v e ry e a s y to
p a l p a t e t h e t e n d e r a t t ach m e n t p o i n t s o n the upper
aspect of the p u b i c s y m p h y s is a n d t h e l o w e r a s p ec t
of the x i p h o i d p r o c e ss a n d t h e a dj a ce n t pa rts of t h e
lower ribs.
F o r t re a t m e n t , g ra v i t y - i n d u c e d P I R i s m o s t
e ffe c t i v e : t h e pa t i e n t is s u p i n e w i t h h e r b u t tocks a t
t h e e n d o f t h e t a b l e , h e r le gs h a ng i n g o v e r t h e e d ge .
A s t o o l i s p la c e d u n d e r t h e foot of t h e s i de w h ic h i s
n o t be i n g t rea t e d : t h e p a t i e n t is t h c n t u r n e d to t h a t
s i d e , s o t h a t a cu s h i o n c a n be i n se r t e d u n d e r t h e
b u t to c k o f t h e s i d e to b e t r e a t e d , l i ft i n g t h i s s i d e o f
t h e p e l v i s . I n t h i s posi t i o n t h e p a t i e n t r e l a x e s t o t a k e
u p t h e s l a c k b y t h e w e ight of t h e h a n g i n g l e g . She
t h e n l i fts t h e k n e e o f t h a t le g a b o u t 2 C ol . h o l d i n g i t
s l igh t l y r a i s e d d u ri n g s l ow i n h a l a t i o n . A ft e r t h i s s h e
h o l d s h e r b re a t h , b e fo r e l e t t i ng i t d r o p a n d b re a t h i n g
o u t s l o w ly . T h i s m a noe u v re is re p e a t e d a b o u t t h ree
t i mes ( F i g u r e 6. 1 20b ) . T h i s t e c h n i q u e a c t s m a i n l y o n
the i n se rtions a t the s y m p h ysis: if we w i s h to act
p r i m a r i l y o n t h e x i p h o i d p ro c e s s a n d t h e u p p e r p a r t
o f t h e s t r a i g h t a b d o m i n a l m us c l e , i t i s better f o r t h e
p a t ie n t t o r a i s e h e r h e a d a n d s h o u l d e rs a n d b re a t h e
i n , t h e n l e t t h e h e a d a n d s h o u l d e rs d r o p w h i l e s l o w l y
b r e a t h i n g o u t . T h i s e x e rc i se c a n b e used fo r s e l f­
t r e a t m e n t . t h e p a t i e n t p e rform i n g it t w o or t h ree
t i m e s in s u ccess i o n .
20 s. S h e t h e n l e t s it d ro p i n to fl e x i o n a n d rel a x e s
f o r a n o t h e r 20 s . Th i s i s r e pe a t e d a b o u t t h r e e t i mes
( F i gu r e 6. 1 2 1 ) ,
L u m bosacro i l i a c ' l i g a m e nt' p a i n
W h e n l i ga m e n t p a i n i s t e s t e d , increa sed t e n s i o n i s
u s u a l l y fo u n d o n t h e a ffe c te d s i d e , toge t h e r w i t h
m o v e m e n t r e s t r i c t i o n i n to a d d u ction
t h i s cond i t i o n P I R
is
(see p . 1 O J ) . I n
the t r e a t m e n t o f c h o i c e ( F i g u r e
6. 1 22 ) : t h e p a t i e n t i s s u p i ne , t h e t h e r a p i s t a t t h e
o p p o s i te s i d e o f t h e ta bl e to t h e l e g to be tre a t e d .
T h e p a t ie n t l1 e x e s t h a t l e g a t t h e h i p a n d k n e e ; t h e
t h e r a p i s t g r a s p s t h e k n ee, b r i n g i n g i t i n to a d d u c t i o n
a n d fl e x i n g t h e h i p so a s to fi n d the pos i t i o n i n w h i c h
t h e re is t h e g r e a t e s t resista n ce to a d d u c t i o n a n d t h e
m o s t pro n o u n ced p a i n , w h e t h e r t h i s pa i n corresponds
m o r e t o the i l i o l u m b a r o r to t h e s a c r o ili a c l iga m e n t .
W h e n t h e t h e ra p i s t h as t a ke n u p t h e s l a c k i n to a d ­
d u c t i on i n t h a t pos i t i o n , t h e p a t i e n t i s t o l d to res i s t the
p r e s s u r e of h i s h a n d , s l i g h t l y , for a b o u t 1 0 S , a n d t h e n
t o ' l e t go ' . D u r i n g re l ax a t i o n , a d d u c t i o n i s i n c r e a s e d
( t h i s m a y be p a i n fu l , b u t i f t h e p a t i e n t goes on re l a x­
i n g i n s p i te o f i t , t he p a i n is n o t c l i n ic a l l y i m porta n t )
a n d w h e n t h e s l a c k h a s b e e n t a k e n u p a g a i n t he
p r o c e d u re is r e p e a te d from the n ew l y ga i n ed position ,
t h re e t o five t i m e s . For self- tre a t m e n t t h e p a t i e n t u s e s
h e r h a nds, o n e m a i n t a i n i n g fl e x i o n a t t h e h i p w h i l e
t h e o t h e r m o v e s t h e k n e e i n to a d d u c t i o n .
Tensio n (TrPs) i n the rect u s femoris
P a i nfu l (te n d e r ) coccyx
The fe m o r a l n e rv e s t re t c h t e s t i s a s c h a ra c t e r i s t i c
h e re a s fo r t h e L 4 ro ot s y n d r o m e a n cl f o r pse u d o ­
ra d i c u l a r ( re fl e x ) s y m p t o m s c a u s e d b y b l o c k age a t
T h i s co n d i t i o n is m o s t fre q u e n t l y d ue to i n c re a s e d
tension i n the gl uteus m a x i m us and the l evator a n i .
t h e L3/4 segm e n t . I n a d d i t i o n t h e re a re TrPs i n t h e
re c t u s fe m o r i s . F o r trea t m e n t , g r a v i t y-i n d u c e d P I R
c ho i ce
i s t h e s i m p l e s t a n d m o s t e ff e ct i v e te c h n i que : t h e
pos i t i o n i s t h e s a m e as fo r t re a t m e n t of t h e i l i o psoa s ,
but i n s t e a d o f l i ft i n g h e r k n e e , t h e p a t i e n t exte n d s
t h e k n e e a n d l i ft s t h e l e g , h ol d i n g i t h o r i zo n ta l fo r
P I R o f t h e g l u t e u s m a x i m u s i s t h e t r ea t m e n t o f
( F i g u re 6 . 1 23 ) : t he p a t i e n t i s p r o n e , w i t h t h e
h e e l s r o t a t e d o u t w a r d s . The t h e ra p i s t c r o s s e s h i s
h a n d s , p l ac i n g o ne o n ea ch buttock a t t h e l e v e l o f
t h e a n u s . A s a r u le h e fe e l s i n c r e a s e d t e n s i o n b u t
t h e r e is n o tenderne s s . The p a t i e n t i s t o l d t o press
her b u t toc k s toge t h e r w i t h v e ry l i t t l e force and to
Copyrighted Material
232
Manipulative Therapy in
Reha bilitil t i o n
of the
( a)
L o co l l 7 o t o r Systell l
( b)
Figure 6 . 1 22
(a)
E x a m i n a t i o n a n d t re a t m e n t
of
t e n s i o n i n m u s c l e s in cases
( a)
k nown
a s l iga m e n t p a i n . (iJ)
S e l f· t r e a tm e n t
( b)
Figure 6.123
treatment
(a)
Exa m i n a t i o n a n el
t re a t m e n t of
te n s i o n i n t h e gl u t e u s m a x i rn u s . (or l e mk rn e s s or t h e
cocc v x .
(/0 ) Se l f­
s , t h e n to l e t go ' .
D u r i n g rel a x a t i o n t h e th e ra p i s t fe e l s t h e te n si o n i n
t h e m u s c l e s d i m i n i s h i ng . T h i s is re p e a te d t h re e t o
fi v e t i m e s , a n d p a lp a t i o n of the c o ccy x is t h e n e a s i e r
p a t i e n t ' s l e g o u t w a rds (i . e . i n t e r n a l ro t a t i o n at t h e
and usually p a i n less.
i nt e rn a l ro t a t i o n a t t h e h i p i rr c re a s e s . This p roc e d u r e
m a i n t a i n t h i s press u re fo r a b o u t t o
'
h i p)
to
t a k e u p t h e s l a c k a n d t e l l s t h e p <1 t i e n t t o g i v e
,
s l i g h t c o u n t e r - press u re , w h i c h h e res i s t s f o r a b o u t
10 s b e fo r e t e l l i n g h e r to ' l e t go ' . D u r i n g re l axa t i o n ,
For se l f-trea t m e n t t h e p a ti e n t i s s u p i n e , w i t h h e r
i s r e pe <1 t e d t h re e to fi ve t i m e s . F o r s e lf-tre a t me rr t ,
h a n d s u n d e r h e r b u t t o c k s , fe e l i n g i n c re a s e d t e n s i o n
gra v i t y - i rr d u c e d P I R is m o s t u s e f u l : t h e p a t i e n t i s
a s s h e p r e s s e s t h e b u t to c k s to g e t h er
s u p i n e . h e r l e g b e rr t a t t h e
hol d i ng the
,
knee a t right angles,
p re s s u r e fo r 20 s a n d t h e n rel a x i ng fo r a n o t h e r 20 s .
rota t e d o u t w a rd s ; s h e n o w t u r n s o n to h e r s i d e , s o
A s t h e gl u te u s m a x i m u s c o n tracts a n d r e l a x e s , s o
t h a t the l e g i s h o r i z o rr t a L F r o m t h is p o s i t i o n s h e
d o e s t h e l e v a to r a n i .
r a i se s t h e l e g a fe w ce n t i m e t r e s , h o l d s i t t h e re fo r
I f t h i s m e t h o d fa i ls , t h e c a u s e i s u s u a l l y t e n s i o n i n
the
t h e n be t r e a t ed I n
e x ce p t i o n a l c a se s t h e re i s n o i n c re a se d t e n s i o n , a n d
p i r i fo r m i s
which
m us t
.
t h e coccyx t h e n h a s to b e t r e a t e d p e r rectu m .
s
a n d t h e n l e t s i t d ro p a n d re l a x e s f or
20
s. T h i s
P a i n at the isc h i a l tuberosity
This s y m p t o m i s c a u s e d b y i n c r e a s e d te n s i o n in t h e
Te nsion i n t h e p i rifo r m i s m u scle
T h i s i s p a l p a t e d a s pa i n ful
20
is re p e a t e d t h ree t i m e s .
h a m s t r i n g s ; s t r a igh t l e g ra i s i ng i s r e s t lic t e d a n d t h e r e
resi s t a nce a b o v e a n d
a r e TrPs i n t h e m u s c l e s . G ra v i ty - i n d u ced P I R i s t he
t h e g r e a t e r t r o ch a n t e r . F o r t r e a t m e n t
m o s t e ffe c t i v e tech n i q u e . T h e p a t i e n t is p r o n e , h e r
( F i g u r e 6 . 1 24) t h e p a t i e n t i s p r o n e w i t h t h e k n e e
l e g s h a n g i ng o v e r t h e e d g e o f t h e t a b l e . S h e l i fts t h e
medial
bent
at
to
right
a ngl e s .
The
t h e r a p ist
ro t a tes
the
a ffe c t e d I e £' fo r
Copyrighted Material
20
s a n d d ro p s i t w h i l e r e l a x i n g fo r
Therapelllic techniques
233
( a)
( b)
(a) Exa m i n a t ion a n d
of tension i n t h e
p i r i fo r m i s . ( 6 ) G r a v i t y - i n d uced
PIR of the p i r i f o r m i s: the p a t i e n t
p r o n e , t u rn e d t o t he s i d e of
t r e a t m e n t , w i t h the b e n t leg
h o rizo n t a l . Left, the l e g s l i g h t l y
raised (20 s ) ; right, re l a x a tion
Figure 6.124
t rea t m e n t
(20 s) w i th
is
t h e leg re s t i n g o n t h e
table
a n o t h e r 20 s, r e p e a t i n g t h i s t h ree t i m e s ( Fi g u re
t h e fo o t i n w a rd s H e t h e n r a i s e s the stre tched l e g ,
6. 1 2 5 ) .
m o v i n g i t i n to a d d ucti o n a t t h e same ti m e , a n d
.
I n te r m i t te n t s t i m u l a t i o n o f t h e a n t a g o n i s t s gre a t l y
r o t a tes t h e fo o t in wards u n t i l t h e s l a c k h a s b e e n
e n h a n c e s P I R i n c a s e s of l i ga m e n t p a i n a n d TrPs
taken u p . From t h is pos i t i o n t h e p a t i e n t is t o l d to
of t h e
e x e r t very s l ig h t p re s s u re a g a i n s t t h e t h e r a p i s t ' s
hamstri ngs,
p i r i fo r m i s
,
a d cl u ctors. T h e p a t i e n t exerts
t h e a b d uctors and
m o d e r a t e p re s s u r e
ag a i n s t t h e r e s i s t a n c e o f t h e th e r a p i s t i n t h e d i re c t i o n
of re l a x a t i o n , w h ic h h e r h y t h m i ca l ly c h a n g e s .
hand,
p re ss i n g
at
external
about 10
' l e t go ' . D u r i n g re l a x a t i o n
rota t i o n
Pain
towa rds
t h e ra p i s t resists for
of
the
fo o t ,
r o ta t i o n .
The
s before t e l l i n g h e r to
h e i n cre a ses i n t e rn a l
stra i g h t
leg
ra i s i n g
and
a d d u cti o n , to t a k e u p t h e s l a c k , b e fo re re p e a t i n g t h e
p r o c e d u r e t h r e e t o fi v e t i m e s . Fre q u e n tl y , p a i n i s fe l t
the head of the fi b u l a
T h i s i s d u e t o t e n s i o n i n t h e b i ceps fe moris, a n d i s
r e l a t e d t o b l oc k age o f the fi b u l a r h e a d . T h e p a t i e n t
i s s u p i n e ( Fi g u r e 6 . 1 26 ) a n d t h e t h e r a p i s t a t t h e e n d
o f t h e t a b l e . W i t h h i s r i g h t h a n d he grasps t h e r i g h t
foot (or t h e l e ft w i t h h i s left ) , h i s t h u m b at t h e h e e l
and l i t t l e fi n g e r a t t h e l i t t l e t o e , to b e a b l e t o rota te
a t t h e fi b u l a r h e a d d u r i n g re l a x a ti o n .
F o r s e lf- tre a t m e n t t h e p a t i e n t s t a n d s w i th fee t
a p a r t , t h e foo t t o be t r e a t e d r o t a ted i n w a rd s a n d
p r o p p e d a g a i n s t , fo r exa m p l e , a t a b l e - l e g . To t a k e
u p t h e s l a c k s h e takes a s t e p fo rw a rd w i t h the o t h e r
fo o t , prod u c i n g s o m e flex i o n o f t h e h i p b y r o t a t i n g
Copyrighted Material
234
MOJlip u / a r i v e Th erapy in Rei7aiJi/irarion of rile
LocomOlOr SvsrC'Y/1
Figure 6. 127 Se l f- t rea t m e n t : t h e p a t i e n t p resses h e r
w h ile the other
foo t e n h a n ces t h a t rota t io n . w i t h t h e k n ee s l i gh t l y ben t.
S h e p resses h e r foo t a ga i n s t t h e t a b l e - leg. i n t o e x t e rn a l
ro ta t i o n ( a b o u t 1 0 s ) a n d t h en re l a xes. i n c re a s i n g k n e e
fl e x i o n i n t h e free leg so a s to i n crease i n w a r d ro t a t i o n
o f t h e foo t
i n w a rd -rota t e d foot a ga i ns t a t a b l e - l e g ,
h e r t r u n k . S h e t h e n p r e s s e s t h e fo o t a ga i n s t t h e
t a b l e - l eg i n t o e x t e rn a l r o ta t i o n . A ft e r a b o u t l O s s h e
rel a x e s , i n c re a s i ng t r u n k r o t a t i o n b y b e n d i n g t h e
k n e e o f t h e free l e g ( F i g u r e 6 . 1 27 ) .
Figllre 6 . 1 25 G I'� v i ty-i n d uc e d P I R o f the h a m s t r i n g s : the
l i e s p r o n e , her l e gs d a ngl i n g o v e r t h e end of t h e
t 8 b l e . t o u ch i ng t h e gro u n d . A b o v e , s h e ra i s e s o n e l e g for
20 s: b e l o w . she d ro ps the leg and re l a xes fo r 20 s
p� t i e n t
A p a i n f u l g reater trocha nter (TrPs a t the
a d d u ctors)
T h i s i s d u e t o t e n s i o n , m a i n l y i n t h e t h i g h a b d u ctors.
m o s t freq u e n tl y with TrPs
at
the t e n s o r fas c i a e l a ta e
b u t a lso i n t h e g l u te u s m e d i u s . TrPs o f t h e g l u t e u s
m e d i u s a r e fo u n d b e l o w t h e pos t e r i o r a s p e c t o f t h e
i l i a c c r e s t , w h e re a s TrPs o f t h e t e n s o r fa s c i a e l a t a e
a re b e l o w t h e s u p e r i o r i l i a c s p i n e a n d c l o s e to t h e
g re a t e r troc h a n te r . I n a d d i t i o n , t h e t e n so r fasci a e
l a t a e m a y c a u se p a i n a t t h e a t t a c h m e n t a t t h e u p p e r
m a rg i n o f t h e p a t e l l a , a n d t h e fasc i a l a t a a n d t h e
i l i ot i bia l tract c a n be tender al p a l p a t i o n . The most
freq u e n t c a u s e o f p a i n a t t h e gre a t e r t roc h a n t e r is a
p a i n f u l co n d i t i o n o f t he I l i p j o i n t .
For e x a m i n a t i o n a n d PI R o f t h e a b d u c t o r s t h e
fo l lo w i n g
6 . 1 28 ) :
tech n i q u e
shou ld
be
w i t h t h e pati e n t s u p i n e , the
a d o p te d
leg
( Fi g u re
on t h e p a i n fu l
( t a k i ng u p
t h e s l a c k ) b e l o w t h e o t he r l e g. w h i c h i s fl e x e d .
S t a n d i n g o n t h e fa r s i d e , t b e t h e ra p i s t fi x e s t h e pe l v i s
o n t h e s i d e o f t h e l e s i o n , f r o m a bove , w h i l e h i s o t h e r
h a n d moves t h e leg i n t o ad d u ct i o n to t a k e u p t h e
s l a c k . T h e p a t i e n t is t o ld t o e x e rt s l i g h t co u n t e r­
p r e s s u re , i n to a b d u c t i o n , fo r a b o u t [ 0 S, a n d is t he n
t o l d t o ' le t go ' , a n d t h e p roc e d u r e i s r e p e a t e d t h re e
s i d e i s b r o u g h t i n to ma x i m u m a d d u c t i o n
t o fi v e t i m e s .
Gr a v i t y - i n d u c e d
Figure 6. 126 Exam i n a t i o n a n d t r e a t m e n t of t e n s i o n i n
t h e b i ce p s fe m o r i s . for t e n d e r n e s s o f t h e fi b u l a r h e a d
PIR
is
most
u s e fu l
fo r
se l r­
t r e a t m e n t . T h e p a t i e n t l i es on h e r s i d e a t t h e e n d o f
t h e t a b l e . t h e l o w e r l e g (-l e x e d a t t h e b i p a n d k n e e ,
Copyrighted Material
Th erap cu tic t echn i q u es
2:15
( b)
( a)
Figure 6. 1 28 ( a ) Exa m i n a t i o n a n d t re a t m e n t o f t e n s i o n
i n t h e a b d u c t o r s . fo r a p a i n fu l t r o ch a n t e r m a j o r .
(b ) G r a v i t y - i n d uced P I R (se l f-t rea t m e n t ) w i t h t h e p a t i e n r
l y i n g o n h e r side a t t h e e n d o f t h e t a b l e . t h e lowe r l e g
flexe d . t h e u p p e r h a n g i ng o v e r the e d ge o f t h e t a b l e :
above. u p p e r l e g s l i gh t l y r a i se d : b e l o w . t h e p a t i e n t h a s
l e t t h e leg d ro p . re l a xe d
t h e u p p e r h a n g i n g ove r t h e e d ge o f t h e t a b l e . W h e n
i n to a b d u c t i o n , a ga i n for at l e a s t 20 s . T h e p ro ce d u re
t h e p a t i e n t re l a x e s , t h e s l a c k of t h e a b d u c t o r s i s
re p e a t e d t h ree to five t i m e s , a n d t h e w h o l e
e x e rc i s e s h o u l d be p e r fo r m e d t w o or t h r e e t i m es a
t a k e n l i p b y t h e we i g h t o f t h e h a n g i n g l e g . T h e
p a t ie n t is t h e n t o l d to l i ft t h a t l eg a b o u t 2 e m a n d
h o l d i t i n t h i s p os i t i o n f o r a b o u t 20 S , a n d the n t o
l e t i t fa l l s l o w l y a n d re l a x fo r a n o t h e r 20 s . Th is
p roce d u re is r e p e a t e d a b o u t t h re e t i m e s .
is
day
(Figure 6. 1 29b ) .
Tension i n t h e toe exte nsors
T h i s i s fe l t 8 S p a i n o n t h e a n t e r i o r a s pe c t o f t h e t i b i a .
W i t h t h e p a t i e nt s e a t e d o r s up i n e ( Fi g u r e
Tension i n the add u ctors
6. 1 30),
th e
t h e r a p i s t p l aces h i s h a n d o v e r t h e toes to b r i n g b o t h
Te n s i o n h e re c a u ses p a i n i n t h e p e s a n se r i n u s o n t h e
foot a n d toes i n to m a x i m u m p l a n ta r fl e xi o n , to t a k e
t i b i a : t h is i s fre q u e n t l y a s ig n o f h i p l e s i o n , w h i c h
u p t h e s l a c k . The p a t i e n t i s t o l d to res i s t s l i g h t l y fo r
s h o u l d be t r e a t e d fi r s t . I f p a i n pe r s i s t s t h e foll ow i n g
about
tech nique
r e pe a t e d t h ree to fi v e t i m e s . S h e m a y p e r fo r m t h i s
s h o u ld
be
( F igu re
tried
6 . 1 2 90 ) :
the
p 8 t i e n t is s u p i n e , cl ose to t h e e d ge o f t h e t a b l e : t h e
1 0 s then
to re l a x , 8 n d
t h e proce d u re i s
m a n o e u v re h e rse l f.
t h era p i s t br i ngs t h e l e g o n t h e l e s i o n ed s i d e o v e r t h e
edge o f the
t a b l e , i n to m a x i m u m a b d u c t i o n a n d
e x t e n s i o n , t a k i n g u p the s l a c k . T h i s m o v e m e n t i s
res i s t e d by t h e p a t i e n t fo r a b o u t 1 0 s , bef o re t h e
p a t i e n t r e l a x e s , a n d t h e proce d u re i s re p e a te d t h re e
to fi v e t i m e s .
Te n s i o n i n t h e s h o r t a d d u c tors i s s h o w n b y a
pos i t i ve P a t r i c k ' s t e s t . I f t he t e n s i o n is n o t d u e to
s o m e u n d e r l y i ng fac t o r , we u s e grav i t y - i n d uced P I R .
T h e p a t i e n t is a s d u r i n g P a t r i c k ' s test a n d re l a x e s
A p a i nful Ach i l l es t e n d o n
T h i s i s a s i g n o f te nsi o n i n t h e s o l e u s m u s c l e . For
t r e a t m e n t t h e p a ti e n t l i e s p ro n e , w i t h t h e knee o n
l h e l e s i o n e d s i d e fl e x e d ( Fi g u r e 6 . 1 3 1 ) . T h e t h e r a p i s t
p a l p a t es t h e ten d o n to m a k e s u re w h i c h s i d e o f i t i s
p a i nfu l , a n d t h e n b ri ngs t h e foo t i n t o d o rs a l fl e x i o n
s o a s t o c re a te te n s i o n a t t h e p a i n fu l s i d e , w i t h t h e
fo o t e i t h e r i ll p r o n a ti o n o r i n s u p i n a t i o n . A f t e r t h e
i n to
s l a c k h a s b e e n ta k e n u p , t h e p a t i e n t i s to l d to e x e r t
a b d u c t i o n , u n d e r the i n fl u e nce o f g ra v i ty , t o take u p
c o u n t e r - p re ss u re w i t h m i n i m u m f o r c e fo r a bo u t l O s ,
t h e s l a ck . S h e t h e n r a ises t h e
about 2 c m a n d
t h e n to r e l a x ; t h e p roce d u r e is r e p e a te d t h r e e t o
h o l d s t h i s p o s i t i o n fo r a t l e a s t 2 0 s ; s h e t h e n re l a xes
fi v e t i m e s . D u r i ng t he re l a x a t i o n p h Cl s e dors i fl e x i o n
the
a bdu c te d
and
fl e x e d
lower
k nee
e x tre m i t y
Copyrighted Material
236
Manip ulative Therapy
in Rehabilitation of the Locomotor
System
( 8)
Figure 6. 129
(a)
E x a m i n a t i o n a n d t r e a t m e n t of t e n s i o n i n
P I R o f t h e s h o rt
is raised s l i g h t l y (20 s ) ;
b e l o w , t h e k n e e d rops i nto fu l l abduction o f t h e t h ig h ,
t h e a d d uctors. ( b ) G ra v i t y - i nd uced
a d d uctors: a b ove, t he k n ee
t h e p a t i e n t re l a x e s fo r
( 8)
Figure 6.130
20
s
( b)
( b)
(a)
E x a m i n a t ion a n d t re a t m e n t of te n s i o n i n t h e e x te n sors
s h o u ld i ncre ase n o t i cea b l y , a n d t h e p a t i e n t s h o u l d
be encouraged t o cooperate to t h i s e n d . F o r s e l f­
t re a t m e n t t h e p a tie n t is s e a t e d , u s i n g b o t h h a n d s
(F i g u re 6 . 1 3 1 b ) .
A p a i nf u l calca n e a l spur
T h i s cond i t i o n i s d u e to i ncre a s e d t e n s i o n i n t h e
m uscles a tt a c h e d to the p l a n t a r a p o n e u r o s i s w i t h
TrPs i n t h e q u ad r a t u s p l a n t a e a n d the s h o rt toe
G r a v i t y- i n d uced P I R i s b e s t a c h i eved w i t h t h e
p a t i e n t s t a n d i n g , h e r h a n d s o n t h e t a b l e ; t h e affe ct e d
leg is sligh t ly i n fro n t of the other, a n d b o t h k n ees
s l ig h t l y bent. B y b e n d i ng forw a rd s h e t a k e s up t he
s la c k i n to d o rs i fl ex i o n ; s h e t h e n r e s i s t s i n t o p l a n ta r
fl e x i o n fo r a b o u t 20 s , r e l a x i n g i n to d o r s i fl e x i o n
( Figure 6 . 1 31c).
o f t h e foot a n d toe s . ( /J ) Sel f- t re a t m e n t
fl e x o rs .
6 . 1 32a)
F o r tre a tm e n t of tbis
it
is
fi r s t
nece s s a ry
to
con cl i t i o n
t re a t
( Fi g u re
movemen t
r e s t ri c t i o n between the t a rs a l b o n e s , e tc . T h e p a t i e n t
i s p ro n e , w i t h k n e e s b e n t . The t h e ra p i s t g r a s p s t h e
foo t , w i t h o n e h a n d r o u n d t h e h e e l a n d t h e o t h e r
r o u n d the d i st a l p a r t of the foo t , p r o d u c i n g d o r s i ­
fl e x i o n m a i n l y o f t h e m e t a t a rs a l s , and e v e n o f t he
Copyrighted Material
Th erap eu lic lechniq l l es
( a)
237
( b)
Figure 6.131 (a) E x a m i na t i o n and t re a t m e n t of t e n s i o n
t he soleus, fo r a t e n d e r Ac h i l les te n d o n . (b ) Se l f­
in
t re a t m e n t .
(e) G ravity-in duced
( e)
P I R of t h e s o l e u s w i t h
in d o rs i fl ex i o n : a b o v e , t h e patient resists
d o rsi fl e x i o n for 20 s : b e l o w , she re laxes i n to dors i flexion
for a n o t h e r 20 s
t h e a n k le
Copyrighted Material
23�
Manipu/{{/iv('
Th erapy
in Rehabilillltion of the
Locomotor System
( a)
( b)
Figure 6. 1 3 2 (0) E x a m i n a t i o n � n d t re a t m e n t of t e n s i o n i n t h e p l a n t a r a p o n e u rosis fo r a t e n d e r c a l c a n e a l s p u r .
( b ) G ra v i t y - i n d u c e d P I R o f t h e p la n t a r a rc h , s t a n d i n g : a b ove , t h e p a t i e n t a rc h e s her foo l ( 2 0 5 ) ; b e l o w . s h e re laxes (20 5 )
toes, i n re l a t i o n t o t h e calcaneus. u n t i l te n s i o n i s fe l t
i n t h e s a l e . The p a t i e n t i s t h e n told t o fl e x t h e
extended toes, w i t h l i t t l e force, aga i n s t t h e the ra­
pist's resis t a n c e , m a k i n g (I S it were a ' hollow' foo t .
This i s h e l d fo r a b o u t 1 0 s, t h e n the patient is told
t o relax and t h e p roce d u re r e p e a t e d t h re e to five
t i m e s . I t is most i m porta n t to a v o i d p l a n t a r fl e x i o n
o f t h e fo o t .
For se l f- t re a t m e n t t h e p a t ie n t i s s t a n d i n g, p u t t i ng
some w e i g h t on t h e fo o t to be tre a te d ; s h e fi rs t
a rc h e s t h e foo t . d ra w i n g i n h e r t o e s . A ft e r 2 0 s s h e
re l axes t h is posi t i o n . fl a t te n i n g the p l a n t a r arch
( Fi g u r e 6 . L 32b ) .
R e m e d i a l exercise
I n the prece d i n g p a r t of t h i s boo k , d ea l i ng w i t h se lf­
mob i l iza t i o n , post-iso m e tr i c re l a x a ti o n a n d soft
tissue m a n i p u l a t i o n , t h e re is grea t e m p hasis o n
self-trea t m e n t . T h e tech n i q ues prese n ted cou l d be
regarded a s a form o f remed ia l e x e rcise, with w h i c h
t he y certa i n l y have m u c h i n co m m o n .
T h e m a i n t a s k o f re m e d i a l exercise i n d i s t u rbed
function o f the loco m o t o r system is to corr e c t fa u l t y
moveme n t pa tterns ( s t e reotypes ) t h a t a re relevant
t o t h e patie n t ' s compla i n ts , The most i m port a n t
p a t h oge n i c m e c h a n i s m , t o b e t re a ted fl rs t , i s motor
i m b ala nce between m uscl e gro u p s , m a n i fested b y
fa u l t y move m e n t o r p o s t u r e .
T o d o t h i s i t is esse n t i a l to u n d e rs ti1 n d w h i c h
muscu l a r fu nctions a re a t fa u l t . a n d t h e i r m u t u a l
corre l a t i o n : wea k n ess, i n h i b i t i o n , hyperactiv i t y , ta ut­
ness, hypo- o r h y p e r to n u s . Asym m e t ry must be
ta k e n i n t o acco u n t . i n part icu l a r conce rn i n g m u s c l e
tone.
I f t he re is e x a gge ra t e d a c t i v i t y of certa i n m uscles,
i t is l i k e l y that they c o m p e n s a t e the wea k n ess of
other m u scle gro u p s . O n t h e o t iJ e r h a n el , m a r k e d
t a u t n e s s ( s h o r te n i ng) o f a m u sc l e lll a y i n h i b i t i ts
a n tagon ist. H owever, m otor function a n d elysfunction
usually resu l t from a c h a i n react i o n and t h e re i s
probably n o strict fo r m u l a w h i c h ca n be a p p l ied to
e v e ry patie n t .
Th i s i s w h y m e thods have been cl e v e loped i n
rec e n t y e a rs wh ich ci a n o t a t t e m p t t o t r a i n speci fi c
Copyrighted Material
co-
m u scles or m u s c l e g ro u ps
u s c l es w i l l
o rd i na t e d m u scle fu n c t i o n
m o t o r faci l i t a t i o n ' . Th e
co m m o n , w h i c h
o n e fo o t : t h i s is m a d e m o re d i ffic u l t o n
a w a re o f t h e i n h i b i te d m u s c l e ; she m u s t fe e l i t . T h i s
fe a t u re i n
III
be made
boa r d : o n l y b y g re a t l y i m p rov i n g m o t o r c o o rd i n a ­
m e a n s t h a t fo r a c e r t a i n p e r i o d t h e p a t i e n t l e a r n s
t i o n c a n h e k e e p h i s b a l a n ce - c o ns e q u e n t l y s o m e
c o n s c io u s co n trol o f t h e m u s c l e , u n t i l correct f u n c t i o n
i n h i b i t e d ( w e a k ) m us c l e s w i l l a u t om a t i ca l l y c o m e
becoms
i n to p l a y a n d s o m e h y p e r a c t i v e a n d/or e v e n t a u t
a v o i d e d i s t re m o r d u r i n g tra i n i n g - t h i s i s a s u re s i g n
a u to m a ti c .
One
da nger
to
be
carefu l l y
m u s c l es w i l l b e fo rce d t o l o o s e n u p .
that t h e patient is e x h austed.
W e ca n n o t d e a l w i t h t h e s e m e t h od s i n d e ta i l h e r e ,
t h e y h a v e rec e n t l y be e n p u b l is h e d
the Spine,
Liebenson,
t ra i n i ng w e a k m u s c l e s .
1 9%)
( Rehabilitation of
We m il y he g i n w i t h
i rh l a nce
I f w e fi n d t h i s
c o n t ra c t s l i tt l e ,
T h e r e a re s o m e ge n e r, ' !
i t i s m o s t i m po r t a n t n el ,
l a te r t o 5 0 m i n u te s . T h e
m usc l e�,
it
p os t u r a l
with the
fa c i li ta t i o n i s t o
fo o t i n o u t w a r d
p a t t e r n s is p a rt i c u l a r l y
if
end of the
p ro n e ( s e e
movem e n t , i n
F i g u r e 4.45 , p.
m i n u tes m a y b e t h e I i m i l
u s e i n h i b i te d
The g luteus maxi m u s
1 11 1 ,
t ra i n s b y c o n t ra c t i n g
t h e pa t ie n t
c o n sc i o u s l y a n d
i s e a s i l y recog n i z e d b y
then extending
p e r form a n ce begi n s t o d e t e r i o ra t e
obv i o u s l y b e s t t o begi n w i t h s i m p le r t a s ks a n d t o
c o n t ra c t e d . I n s e v ere c a s e s , p a r t i c u l a r l y
e re c t o r s p i n a e i s h y p e r a c t iv e , i t i s i m p o r t a n t t o
t r a i n m o re c o m p l e x m o ve m e n ts l a te r . T h u s i t i s b e s t
i f t h e p a t i e n t fi rst t r a i n s l y i n g o n t h e fl o o r , a n d o n l y
red u c e l u mb a r l o rd o s i s , For t h i s t h e p a t i e n t s h o u ld
p l a c e b o t h forea r m s ( o r a c u s h i o n ) u n d e r t h e
l a te r u n d e r t h e i n fl ue n ce o f gra v i ty ; a ga i n , i t i s e a s i e r
a b d o m e n , a n d c o n t r a c t t h e a b d om i n a l m us c l e s . S h e
the glutei
I
the l umbar
for t h e pa t i c n t t o be s e a t e d , s i n ce i t i s m uc h m o re
t h e n c o n sc i o u s l y c o n t r a c t s o n e b u t t o c k , l i ft i n g t h a t
d i ffi c u l t to fix t h e pe l v i s c o r r e c t l y w h i l e s t a n d i n g .
l e g v e r y slig h t l y s o a s n o t t o c o n t r a c t t h e l u m b a r
W h a t t h e p a t i e n t i s t a u g h t m u s t b e p r a c t i se d a t
h o m e , s o t ha t a t a l a t e r s t a ge s h e n e e d n o t v i s i t t h e
e re c t o r s p i n a e a n d n o t t o b r i n g t h e l u m b a r s p i n e i n to
l o rdosis. T h e p a t i e n t m a y b e t o l d t o ' l i ft h e r l e g a n d
physiotherapist s o
s t r e t c h i t a s fa r
Iy.
t i e s s h o u l d b e t ra i n e d
il c t i v i d a i ly
acti v i t i e s req u i red o f
For s t r e n gt h e n i n g
e ffe c t i v e i f t h e
A s t h e t e c h n i q ue s
p os i t i o n o r i f s h e
hy p e r a c t i v e m us c l e s h a ve
she can p a l p a t e
and s o f t t issu e m a n i p u l ; 1 1
t o t h e t re a t m e n t o r m u se u l :) r
H a v i n g l e arned I
use b o t h t h e g l u t e i
the pelvis (the
T h e te c h n i q u e u s e d
Tra i n i n g wea k m u scles
t a u g h t to
( t i l t) o f
fu n c t i o n ) .
o f the
fo r s e l f-m o b i l i z a t i o n
l o w e r l u m b a r s pi n e into a n te - or re t r o fl e x i o n
a p p r o p r i a te h e r e ( s e e F i g u re 6.57, p . 1 94) .
A s e xp l a i n ed a b o v e ( s e e p . 1 2 1 ) , t h e re i s n o t r u e
p a r e s i s i n o u r p a t i e n t s . we a k n e s s be i n g t h e r e s u l t o f
i n h i b i t i o n a n d d i s u s e . I t i s t h e re fo re u p t o t h e p a t i e n t
is
The g l uteus medius
to l e a r n h o w to u s e t h e s e w e a k e n e d m u s c l e s aga i n .
For
To t e a c h t h e pa t i e n t we s h o u l d d i s t i n g u i s h fa c i l i t a ­
t i o n a n d t ra i n i n g .
e ffe c t i v e : t h e p a t i e n t l i e s o n h e r s i d e , a n d a s t h c
Fac i l i t a t i o n i m p l i es
fa c i l i ta t i o n
the
fo J l o w i n g
is
most
g l u te u s i s w e a k , s h e m a k e s a ' fa l se a b d u c t i o n ' a s
described i n
tra i n w e a k m u sc l e s . H e re
method
plays a p r o m i n e n t ro l e .
t h e ra p i s t p e r fo r m s
and lets t h e leg
o f t h e w e a k ( i n h i b i te d )
g l u t e u s m e d i us
I.
I t :; r t h i s t h e
i ng , n o r m a l i z a t i o n o f
repeats t h i s m a nocuvre,
c a n be a c h i e v e d , t h e
p a l p a t e s t h e a u t ()[n a li c
I. h e gl u t e u s
becom i n g t h e s a m e a ,
medius with her
h a s beco m e
fee l of i t ' ,
ce p t i ve s t i m u l a t i o n is
is a l so i m porta n t , m ore i n m u s c u l a r n y p e rl o n u s ,
h o w e v e r : s i t t i ng i n a be n t p os i t io n c a u s e s h y pe r t o n us
she
is
t o l d to con tract the m uscle consciously,
c h e c k i n g w i t h h e r fi ng e r s ( feed b a c k ) a n d t h u s
of most p os t u r a l m u s c l e s . S t r a i gh t e n i ng u p greil t l y
a c h i e v i n g c o r re c t a b d u cti o n , i . e . a b d u ctio n u s i n g
faci l i ta t e s r e l a x a t i o n . Before t ra i n i n g a m u s c l e i t i s .
s i m u l t a n e o u s l y b o t h t he g l u t e us m e d i us a ncl t he
o l' c o u rse , esse n t i a l t o t r e a t e v e r y TrP.
t e n s o r fasc i a e l a ta e .
Copyrighted Material
240
ManiplIlative Th erapy in
Rehabilitation of the Locomotor
The recti a b d o m i n is
The test for t h i s muscle is fo r t h e p a t i e n t to s i t up
from t h e s u pine positi o n , keeping the legs b e n t at
t h e h i ps a n d kn ees. For coord i n a t e d con traction of
the g l u t e i m a x i m i the p a t i e n t m a y p ress her h e e l s
aga i n s t a h a rd c u s h i o n o r other obstac le; it i s a grave
m i s t a k e to fix the foot from above. I f the p a t i e n t
ca n n o t do t h i s , w i t h o u t h e r l u m b a r e r e c t o r s p i n a e
bein g too short, the a bd o m i n a l muscles m a y be
trained by the patient sitting w i t h bent knees, and
lying d ow n slowly w i t h her spine i n ky phosis and
her neck in a n te fl e x i o n , the contracted abdom i n a l
m uscles a l l owing t h e v e rtebrae to touch t h e t a b l e
one a fter t h e o t h e r (ecce n tric contracti o n ) (Figure
6 . 13 3 ) . The exercise m u s t be stopped the m o m e n t
l u m b a r k y p h osis ca n n o t b e m a i n t a i n e d a n d i f t h e
p a tien t 's fee t a re lifted from t h e tabl e . A fter a few
days o r weeks of practice , the patie nt wi l l be able to
li e down correc t l y i n t h i s w a y , and the n she w i l l al s o
be able to sit u p by t he same method .
I t m a y be e a s i e r for t h e p a t i e n t to start tra ining
h e r abdomin a l m u scles j u s t b y lifting t h e pelvis w h i l e
l y i n g s u p i n e A more difficult pos t u r a l exercise i s to
contract t h e deep a b d o m i n a l m u scles i n B r U gger's
relief position (see Figure 6 . l 44, p. 246 ) , c o n tracti ng
the abd o m i na l muscles w i t h o u t ra i s i n g her thorax. I n
ord e r to restore t h e pos t u ra l fu nction o f t h e abdom­
inal m uscles a n e ffe ctive m a n o e u v r e i s to b r i n g the
,
.
System
weight forwa r d a n d b a c k , a t the s a m e t i m e contract­
i n g the abd o m i n a l m uscles. U n t i l this becomes
a u tomatic t h e patient ca n check by p a l p a t i o n .
The fol lowing exercises also t r a i n coord ina ted
contraction o f t h e gl u t e i m a x i m i a n d the ab d o m i n a l
recti.
Th e 'pelvic see-saw' (Figure 6. 1 34)
The pa tient is s u p ine with k ne e s b e n t and fee t o n
t h e t a b l e . B y con t racting h e r erector spi nae she
b r i ng s h e r l u mbar sp i n e i n to lordosis, a nd b r e a t h i ng
quietly she relaxes the e rector s p i n a e w h i l e
co n t r acting both t h e a bdom i n a l m u s c l es a nd t h e
g l u te i maximi, bringing the l u m b a r s p i n e flat o n t h e
table. O n c e s h e has m a stered t h i s p h ase the patie n t ,
w i t h h e r lumbar spine s t i l l fl a t o n t h e t a b l e , p u t s h e r
k nees toget h e r and l i fts i n kyphosis fi rst the pelv is
and then the l u mb a r spine, up to the low thoracic
re gi o n i n caudocra n i a l order. The l u m b a r e rector
s p i n a e m us t be kept relaxed, the recti abdo m i n i s a n d
g l u t e i m a x i m i contracted a n d the k n ees toge ther.
The pat i e n t t h e n l i es do w n ag a i n reve rs i n g t h e order
of t h e e x e rcise, from t h e t h o racic s pine to the pelvis.
,
.
The 'cradle '
The patie n t l i es s u pi n e , d r a w i n g h e r knees to h e r
chest w i t h h e r a r m s ; s h e t h e n p u s h e s t h e k nees
again s t her c l asped h a n d s , t h us l i ft i n g her pelvis a n d
l u m b a r sp i n e , a n d contracting the g l u t e a l m u sc l e s .
A t t h e s a m e t i m e s h e l i fts h e r h e a d a n d chest.
contracting the abdom i n a l m u scles. By rhythmic
( a)
( b)
Figure 6.1 33 Tr a i n i n g t h e recti a b d o m i n i s b y l y i n g
d o w n from a s i t t i n g p o s i t i o n , keeping t h e k n ees b e n t :
(a) correct a n d ( b ) fa u l t y
Figure 6.134 T h e ' p e l v i c s e e -sa w ' : ( a ) b r i n g i n g t h e
l u m b a r s p i n e i n t o l o r d o s i s , su p i n e : ( b ) l i fting t h e p e l v is
a n d l u m b a r s p i n e f r o m t h e t a b l e , in k y p h o s i s , a n d
r e t u rn i n g i t to t h e p r e v i o u s pos i t i on
Copyrighted Material
Th erapelllic techn iques
24 1
nose w i t h t h e o t h e r h a n d a n d i n h a l e . A fter t h i s
resisted in h a l a t io n , i t is e a s y fo r h e r to d raw i n t h e
a n a l regi o n . O n ce t h e patient has learned th is, she
can d o i t without i n h alation. She then l e a rns this
m a n oe uvre w h ile s i t t i n g and s t a n d i ng. She s h o u l d
n e v e r press t h e b u t tocks toge t h e r .
This i s a n exercise w o m e n s h o u l d pe rform a s a
routi n e after d e livery, j ust as t h e y s h o u l d tra i n t h e
abdo m i n a l m uscles.
The lower part of the trapezius muscle
Fi g ure 6.135 T h e ' c ra d l e ' : a b o v e , t h e k n ees a re d ra w n to
t h e h i ps a re e x t e n d e d aga i ns t res i s t a n c e
b y the arms, and the t r u n k l i ft e d
t h e c h es t : b e l ow ,
press ure o f h e r knees aga i n s t her hands she swings
herse l f i n to a s i t t i n g pos i t i o n , before d ro p p i n g back
to the fi rst ( Figu re 6. 1 35 ) . A t a l a t e r stage the patie n t
may d o this e x e rcise w i t h o u t t h e h e l p of h e r h a nds,
which a re s t re tched fo rward . S t ronger gluteal and
abdom i n a l m u scles, and the i r i mproved coord i nation ,
can b e ach ieved i n t h i s way.
T h i s m u scle h a s a key role i n t h e corr e c t fi x a tion o f
the s h o u l d e r . T h e fo llow i n g e x e rcise s h o u l d be
carried out to fac i l i ta t e contraction (Figure 6. 1 3 6 ) :
the p a t i e n t sits o n h er he e l s a nd b e n d s forward t o
r e s t h e r forehead o n t h e t a b l e i n fro n t o f h e r ; t h e
arms ca n be a l on g t h e t r u n k , re l ax e d . I n t h i s position
t h e m ed i a l bord e r o f the shou l d er-blade d ive rges
from t he spi n a l c o l u m n in a ca u d a l d i recti o n . The
t h e rapist t e l l s the p a t i e n t to draw her s h o u l d e r-blade
i n a c a u d a l d i rectio n , by con tracting the lower part
o f the trapezius. Correctly performed , t h i s move­
m e n t brings the me d i a l border o f t h e shoulder-blade
parallel with the s p i n a l colu m n , the lower a ngle
be i n g p u l led in a c a u d a l - m e d i a l d i rection. O nce the
the rapist h a s p a lpated good contraction o f t h e lower
part of the trapezi u s , the patient should a lso palpate
i t with t h e t h u m b o r i n dex fi nger o f h e r own
fu rthermost hand (feed back ) . The s h o u l d er-b l ades
m u s t not be drawn together.
O n ce th e p at i e n t has mastered this proce d u r e , she
le a r n s to d o i t lying p r o n e , flat o n the ta ble , check i ng
the contraction with h e r fi nger. S h e c a n t h e n con­
tract both the low e r t rapezi i , l y i n g w i th both arms
by h e r sides i n i n te r n a l rota t i o n . S h e s l i g h tly l i fts
both a rms, t h e n her head a n d neck, k e e pi ng the
neck i n line w i th the thoracic spine, the m a n d i bles
a t r i g h t angles to t h e neck. I f the lower trapez i i are
contracted , the upper trapez i i remain rel axed ow i n g
The pelvic d i a p h ra g m
The importance o f t h e pelvic d ia p h ragm c a n be
compared to t h a t of the abdom i n a l muscles: both
fo rm t h e w a l ls of the abdom i n a l cavity , playing a
vital role in postu re a n d respira t i o n . U n l i ke the
abdomi n a l wall, t h e pelvic d i a p h ragm is hidden a n d
therefore rem a i n s u n notice d . When e l i c i t i n g t h e ' S '
reflex (see p. 99) we find a TrP i n the m . coccygeu s .
A n i n d i rect sign i s hypertonus o f t h e a d d u ctors .
For tre a t m e n t i t is a d v i sable first to relax the
adductors and flexors of the h i p . To make the patient
u n d e rstand how to tra i n the w e a k p e l v ic d i a p hragm,
i t is usefu l for her to l e a rn to ' d raw i n ' h e r navel,
c hecki ng t h a t moveme n t w i t h h e r fi n ge rs . O n ce s h e
has u n d e rstood t h i s , she lies o n her side w i t h h e r
fi n gers flat o v e r h e r a n u s a n d tries to draw i t i n . This
is not easy a t fi rst; t h e re fore she should hold h e r
Fi gure 6.136 Squatting o n h e r heels, tr u n k b e n t over
t h ighs, th e p a t i e n t contracts t h e l o w e r part of t h e
trapezius
Copyrighted Material
242
Manipula tive Therapy il1 Rehabilitation of th e Locomotor S vstem
Figure 6.138 O n hands and k n e e s w i t h
a book on the
o c c i p u t - c o rr e c t p o s i t i o n
t h e t rapezi i rem a i n i ng re l a xed and the recti
abdom i n is con t racted . Th e back a n d neck s h o u l d be
as fl a t as a board .
The deep flexors of the neck
Figure 6. 1 37 T h e p a t i e n t o n h a n d s a n d k n ee s fo r
e x a m i n a t i o n a n d t r a i n i n g of t h e s e r ra t u s l a t e r a l i s : ( a ) fi rst
pos i t i o n ; (b) arms b e n t (corre c t ) : ( e ) fa u l t y po s i t i o n w i t h
a rms be n t
to re flex i n h i b i t i o n . Th e patie n t fi r s t relaxes t h e
n e c k , t h e n t h e a r m s a n d lastly the s h o u l d e r - b l a d e s .
O nce t h e p a t i e n t has learned to con tract the l o w e r
part o f t h e t r a pezius w h i l e p r o n e , s h e can d o t h e
same upright (sitting o r sta n d i n g ) , aga i n fi rst check ing
up o n t he contraction w i t h her fi ngers.
The s i m p lest exercise is head a n teflexion aga i nst
resistance: the patie n t is sea t e d , her c h i n sup ported
from below by the c u p ped h a nds, givi n g res ista nce
to head a n t e fle x i o n ( i s o m e t r i c a s w e l l as isoto n i c
resis t a n ce m a y be us e d ) .
A v e r y e ffec t i v e exercise consists o f d ra w i ng t h e
c h i n i n t o t h e n eck w h i l e s i t t i ng, w i t h the t h oracic
spine b e n t backwards over t h e low back of a ch il i r
(Figure 6. 1 39) , repeating t h e movem e n t severa l t i mes.
Tra i n i n g for s o m e of the m o st
i m p o rta nt stereotypes ( m ovement
patte r n s )
Sta n d i n g on both feet
The serratus l atera l i s
T o t r a i n t h is m us c l e ( Figu re 6 . 1 3 7 ) , t h e p a t i e n t is o n
h a n d s a n d k nees, w i t h h e r weight m a i n l y on the
h a n d s , w h ich (I re i n i n ter n a l rota t i o n , the fi n ge rs
poin t i ng a t e a c h o t h e r . The s h o u l d e r-blades m u s t b e
k e p t we l l a p a r t a n d t h e t h o racic s p i n e h e l d i n a
stra ight I i n e . The patie n t i s t h e n told to bend h e r
arms a t t h e e l bows. Correct fi x a t i o n o f t he tr u n k a n d
shou l d e r g i rd l e i s m o s t i m porta n t : t h e s h o u l d e r­
blades m ust be k e p t a p a r t (by the serra t i ) a n d fixed
from below by t h e lowe r p a r t o f t h e tra pezii. T h e
n e c k is h e l d straight. i n pro longa t i o n of t h e thoracic
spine. Contraction of t h e a b d o m i n a l m usc les i s
necessary to keep t h e tru n k s tra igh t : t h i s is m a d e
easier i f t h e p a t i e n t breathes o u t w h i l e b e n d i n g h e r
a rm s .
O n h a n d s a n d knees ( Figure 6. 1 3 8) w i t h a b o o k
resting o n t h e occ i p u t has a s i m i l a r e ffe ct, t ra i n i n g
correct fi x a t i o n o f the s h o u l d e r g i rd l e by con t raction
o f t h e serrati la terales a n d t he lower part of t h e
tra pezi i , a s w e l l as by coord i n ated contraction of t h e
neck e x te nso rs a n d d e e p flexors, t h e upper part of
Copyrighted Material
An i m port a n t c r i t e r i o n fo r sta n d i n g pos t ur e is t h a t
i t s h o u l d be stable, w i t h t h e m i n i m u m of m uscu l a r
Figure 6. 1 39 Tra i n i n g t h e d e e p n e c k flexors h y d r a w i n g
t h e c h i n i n w i t h t h e t h o r a c i c s p i ne b e n t h a c k w a rd s o v e ,
t he l o w b a c k of a c h a i r
Th erapelltic techniq l l es
243
T h i s is p a r t i c u l a r l y true for the t r u n k : t h ere
a lw ay s s o m e a ct i v i t y at th e level of the l e gs t h u s
i m p l y i n g t h a t the fee t a re d e c i s i v e . This is n o t a m e r e
coi n c i d e nc e : toge t h e r w i t h t h e h a n d s a n d the m o u t h
t h e y a re re l a t e d to t h e l a r ge s t a rea o f the c e r e b r a l
cortex a nd a re richest in se n s o r y rece ptors. For t h i s
r e a s o n t h e a c t i v e role of t h e fe e t i n s t a n d i n g c a n
h a r d l y be o v e re st i m a t e d . I t i s , h o w e v e r , j e o p a r d i z e d
s e r i o u s l y by w e a r i n g s h oe s , c a u s i n g w h a t c o u l d be
a c t i v i ty .
is
,
c a l l e d ' c h r o n i c s e n s o r y d e p ri v a t i o n ' .
The key t o t r a i n i n g p h y s i o l o g i ca l s t a n d i n g l i e s i n
activa t i o n o f t h e fe e t . I n C h i n e se g y m n a s t i cs t h e
subject s t a n d s w i t h h i s f e e t s l i g h t l y a p a rt a n d i n
i n w a rd rot a t i o n w i th s l i g h t l y b e n t k n ee s . This p o s i ­
t i o n g r ea t l y f a c i l i t a t e s t h e ac t i v i ty of t h e toe fl e x o r s :
the p a t i e n t g r i p s t h e I� o o r . O b v i o u s l y t h i s is e a s i e r
to d o w i t h o u t s ho e s .
T h e s ta b i l i ty of t h is type o f s ta n d i ng ca n be t e s t e d
ve ry s i m p l y : t h e e x a m i n e r g i v e s a s l i g h t u n e x p e c te d
p u s h to t h e p Cll i e n t ' s t r u n k from i n fro n t or b e h i n d :
i f s h e s t a n d s t h e u s u a l w a y w i t h fe e t i n o u t wa r d
rota t i o n , s h e is l i k e l y t o lose h e r b a l a nce. S t a n d i n g
w i t h fee t i n s l ig h t i n w a rd r o ta t i o n a n d be n t k n e es,
sta b i l i t y i s g re a t l y e n h a nced . T h i s , h o we v e r i s not
the only e ffe c t : t h e pe l v i s w i l l a u t o m a t i c a l l y be in a
n e u t r a l p o s i t i o n , t h u s g re a t l y i m p ro v i n g b o d y statics,
i . e . t h e pos t u re o f the t r u n k . head and n e c k .
'
'
,
Sta n d i n g o n o n e leg, o r wa l k i n g
B e i ng a n asym m e t r i c a l F u n c t i o n t h i s i s u s e f u l t o
correct a s y m m e t ry S t a nd i ng o n o n e l e g i s related t o
w a l k i n g , w h i c h e n ta i l s a l t e r n a te s t a n d i n g o n e a c h l e g.
Some a s y m m e t ry is f r e q u en t a n d a s a rule we c a n
d i s t i n g u i s h t h e s u p p o r t i n g l e g , t h e one on w h i c h the
subj e c t p u ts m o re w e i g h t w h e n s t a n d i n g a t e a s e . T h e
a s y m m e t r y s h o u l d n o t be too m a rk e d , however. B o t h
when s t a n d i n g on o n e l e g a nd i n w a lk i ng , i t is e sse n t i a l
to a c t ivate the fee t a n d t o es . When s t a n d i ng t h e k n ee
should s l i gh t l y bend and t h e toes s h o u l d grip t h e
�l o o r : w h e n wa l k i n g t h e heel s h o u l d touch t h e fl o o r
fi r s t a n d t h e n the t o e s be u s e d fo r p r o p u l s i o n
Figure 6 . 1 4 0 A l t e r n a t e for w a r d a n d b a c k w a r d s h i ft i n g o f
t h e legs, s u p i n e
.
.
.
A ltern a te forward a n d backward sh ifting o f the
legs, supine (Figure 6. I 40)
The pa ti e n t is
asked to s h i ft her s l i g h t l y a b d ucted
t h e d i rec t i o n o f i ts long a x is .
The re i s co n t r a c t i o n o f th e g l u t e u s me d i u s a n d a t
t h e same t i m e t h e re i s a l te rn a t i n g c o n t ra c t i o n o f t h e
i n te rn a l a n d e x t e rn a l r o t a tors o f t h e h i p . T h e a b d o m ­
i n a l a n d g l u t e a l m uscu l a t ur e p r o v i d e s fixa t i o n o f t h e
p e l v i s a n d l u m b a r spi n e . I n t h i s way t h e pa t i e n t
l ea rn s to fix h e r p e l v i s a n d t r u n k d u r i n g l e g r o t a t i o n .
leg ' i n t o t h e d i s t a n c e ' i n
Rota tion of the h ip with th e leg in abductio n
d i s t a n ce ' . T h e
i s p u l l e d u p by t h e q u a d ra t u s
pe l v ic o bl i q u i t y . T h e g l u t e u s
m e d i u s of t h e a b d u c t e d l e g is c o n t r a c t e d w h i l e t h e
a b d o m i n a l a n d g l u t e a l m u s c u l a t u re fi x e s t h e pe l vi s .
I n t h i s pos i t i o n t h e p a t i e n t r o t a t e s t h e foo t a n d t h e
l e g ( see F i g u r e 6 . 1 40) .
other
Flexion a n d extension of th e upper leg, lying
o n th e side ( F i g u re 6 . 1 4 1 )
p a t i e n t i s i n t h e s a m e position a s for t h e
p r e ce d i n g exercise; she l i ft s ( a b d u c ts ) t h e stre t c h e d
u pp e r l eg. D u r i n g le g fl e x i o n a t a l l j o i n ts ( d o rs a l
fl e x i o n of t h e a n k l e , b e n d i n g h i p a n d k n e e ) t h ere i s
a l s o s l ight k y p hosis o f t h e lumbar s p i n e a n d d u r i n g
e x t e n s i o n wi th a l l t h e e x t e l1sors a c t i v e , t h e l u m b a r
s p i n e m o v e s i n to s l i g h t l o r d o s i s . C o r r e c t c o n t raction
of t h e a b d o m i n a l m u sc l e s a n d t h e g l u t e i s ho u l d
p re v e n t h y p e r l o r d o s i s d u r i n g extension . T h e t h e rap i s t
ca n h e l p t h e p a ti e n t by g i v i n g some r e s i s t a n ce
( d u r i n g flex i o n ) to the k n e e or t h e b i g t o e ; a n d
d u r i n g e x t e n s i o n , to t h e h ee l , or to t h e b i g toe from
b e l ow
These exercises teach the p a t i e n t c o o r d i n a t i o n
d u r i n g wa l k i n g
The
,
.
The p a t i e n t
a n d p u s hed
l ie s
her b a c k w i t h o n e leg a b d u c t e d
( a s i n t h e p r e ced i n g e x e rc i se ) i n to t h e
on
'
l eg
l u m b o r u m to p r o d u c e
.
Copyrighted Material
244
IVianipuLa t i ve Therapy in Rehab ilitation of the
Figu re 6.141
(a)
Fl e x i o n a n d
(b)
Locomotor System
e x t e n s i o n of the u p pe r leg, w i t h the p a t i e n t on h e r side
Sta n ding on one leg ( s e e Figure 4 . 7 5 , p .
correct fixation o f th e pelvis a n d trunk
136) :
The
p a ti e n t fi rst sta n d s on b o t h l egs, a n d then p u ts
h e r w e i g h t on o n e l e g . S h e now has to fi x both h i p
a n d p e l v is. S h e t h e n l i fts t h e o t h e r l e g b y b e n d i n g
the h i p a n d k n e e a l m o s t a t ri gh t angles. S h e s h o u l d
b e able to kee p her p e l v i s h o rizon t a l wi t h o u t losing
h e r b a l a nce. Correct fi x a t io n of the pelvi s and tr u n k
a re r e q u i r e d , fo r w h i c h t h e k e y m u scle is the gl uteus
m e d i u s ; t h e p a t i e n t should p a l p a t e i t on the side o f
t h e s u p p o rting leg. I f s h e fe e l s t his contraction s h e
s h o u l d c h e c k u p w i t h both h a nds o n t h e crest o f the
i l i a , to m a k e s ur e that the pelvis is horizon tal.
S itt i n g (see Figure
4.68,
p. 133)
Sitting erect o n th e floor, fo r trun k ro ta tion
( Fi g u re
6 . 1 42)
p a ti e n t s i ts on h e r i sc h i a l tuberos i t i e s , the legs
p a ra l l e l and s l i g h tl y bent, h e r h a n d s cl asped on t h e
occi p u t . By coord i n a te d contraction of t h e t r u n k
m uscu l a t u re , t h e s p i n a l co l u m n i s h e l d e rect; correct
fi x a t i o n of t h e s h o u l d e r- b l ades is also essenti a l .
From t h i s p o s i t i o n the p at ie n t c a rries o u t a x i a l
rotation , be n d i n g n e i t h e r backwards, for w a r ds n o r
s i d e w ay s . G o o d faci l i t a t i o n c a n b e o b t a i ned if s h e
l oo k s to t h e s i d e of rotation a n d u pw a r ds, b re a t h i n g
i n d u ri n g rota t i o n to t h e s i d e a n d breathing o u t
d uring rotation b a c k t o n e u tra l posi t i o n . ( I n t h e
kyp h o t ic p o s i t i o n i t is t h e re v e r s e : b re a t h i n g o u t
fac i l ita tes rota t i o n ) A l l t h a t h o l d s for trun k r ota t i o n
w h i l e s e at e d c a n be a ppl i e d d u ri n g t r u n k rotation
standing, w i th l e gs a pa r t .
The
Figure 6.142 ( a ) S i t t i n g erect o n t h e fl o o r . ( b ) Tru n k
rotation
L a te ra l m o ve m e n t o f th e th o rax, sitting
( F i g ur e 6. 1 4 3 )
.
T h e p a t ie n t i s seated, p re fe r a b l y i n fr on t o f a m i r ro r
a n d mov e s h e r thorax to t h e side i n t h e d i re c t i o n o f
Copyrighted Material
,
Th erapeu tic [echniq l l es
Figure 6. 143 L a t e r a l move m e n t s o f t h e t h o r a x with
the patie n t sea ted: (a)
a re h e l d h o r i z o n t a l l y . S h e d oe s t h is
of h e r t r u n k m uscu l a t u re , c h i e A y
the a b d o mi n a l m u s c l es, kee p i n g t h e t r u n k s t ra ig h t
a n d a v o i d i ng a croo ked pos i t i o n . T h e t h e r a p is t c a n
faci l i t ate t h i s exercise b y e f fe c t i n g r es i s ta n c e a g a i n s t
t h e p a t i e n t ' s ri b s , fi r s t from o ne and t h e n fro m t h e
o t h e r si d e . U p r i gh t posture is a l so fac i l i ta te d b y
b re a t h i n g out o n m o v i n g to the s i d e a n d in w h i l e
re tu r n i n g t o n e u t r a l pos i t i o n ; t h i s is d u e t o c o n t r a c t ­
i o n of the obli q u e abdo m i n a l m u s c l e s .
the
arms,
w h ic h
by correct c o n t r o l
Con trolling th e pelvis wh ile s ea te d
The p a t i e n t s i ts o n a s too l , fa c i n g a m i r r o r ( s e e
Figure 4 . 6 8 , p . 1 3 3 ) . S he fi r s t i n t e n t i o n a l l y re l a xe s
her a b d o m i n a l a n d g l ut e a l m u s c l e s , b r i n g i n g th e
l u m b a r s p i n e i n to l o rd o s i s . S h e t h e n s l ow l y c o n t racts
the g l u t e a l a n d a b d o m i n a l m us c l es t o c a u s e l u mb a r
kyphosis. The
s ho u ld e r g i rd l e s h ou ld m o v e a s l i t t l e
as possible d u ri n g t h i s e x e r c i s e .
correct
and ( b ) fa u l t y
B r u gger's re l i ef position
( F i g u r e 6 . 1 44 )
p o i n ts o u t t h e
p os i t i o n ,
ove r l o a d i n g t h e i n te rv e r t e b r a l d i s c s , p re s s i n g on the
ste r n u m and the p ub i c sy m p h ys i s a n d c a u s i n g a
forw a rd - d ra w n neck, w i t h h y perl ordosi s of the cran i o­
In
a
245
n u m be r o f p u b l i c a t i o n s B r u gg e r
d e l e t e ri ous
e ffect of
s i t t i n g i n a ky p ho t i c
c e rv i c al j u n c t i o n . This c re a t es increased t e n s i o n i n
most o f t h e post u r a l m u sc u l a t u re .
he h a s t h e p a t ie n t a d op t t h e
po s i t io n : seated o n the ed g e of a stool wi t h
t h e k n e e s a p a r t a n d o u t wa rd rota ted fee t , res t i n g h e r
w e i g h t o n h e r le gs , she c o mp l e t e ly re l axes t h e
g l ut e a l a n d a b d o m i na l m u s c le s ; th e p e l vis i s ti lt ed
fo rward , c r e a ti n g consid era b l e l u m b o s a c r a l l o r d o s is
w i t h t h e a b d o m e n p r o tr u d i n g . Once th e p a t i e n t h a s
fo u n d t h is p o s i ti o n , t h e u p p e r l u m bar, t h o racic a n d
ce rv i c a l s p i n e straighten u p . a n d a l l t h e p os t u r a l
m u s c u l a t u r e r e l a x e s ; t h e e n t i re s p i n a l co l u m n i s
app arently i n b a l a nce.
For m a x i m u m r e l i e f
fo l l o w i n g
Copyrighted Material
246
IVlanipulalive Therapy
in Rehabililalion of the L O C0l1 1 0 l O r Syslel1l
�
8
o
o
o
o
o
o
( a)
Figure 6.144 ( a ) B r ugge r ' s re l i e f p o s i t i o n . ( b ) T h e u s u a l
k y p h o t i c p o s i t i o n ( s h a d i n g ) a n d t h e re l i e f pos i t i o n ( b l a c k )
( b)
[ t i s s i m p l e to t e s t t h e i m m e d i a t e e ffe c t o f t h i s
p a t i e n ts w i t h v a r i o u s t y pe s of b a c k p a i n p a r t i c u l a r l y
m ,ln o e u v r e : wh i l e i n t h e u s u a l k y p ho t i c p os i t i o n
i n t h e l ow b a c k . I n t h e a u t h o r ' s o p i n i o n t h e y a re most
e v e n m o d e ra te p re s s ure o n th e u p p e r t r a p e z i i
.
the
pe c t o r a l s . b i c e p s . b r a c h i or a d i a l s . q u a d r i c e ps a n d c a l f
m uscles
is
u n p l easa n t
i f not
positive l y
p a i n fu l ;
.
u s ef u l
fo r
p a t i e n ts
with
p a i n fu l
tension
in
t he
s h o u l d e r - g i rd l e m u scu l a t u r e . a n d fa u lt y re s p i r a t i o n
( h e a d /s h o u l cl e r a n d c h e s t pa i n ) . T h e p a tie n t n e e cl n o t
w h e re a s i n t h e re l i e f p o s i t i o n i t i s p a i n les s. a n d e v e n
u s e t h i s ch a i r e x c l u s iv e l y . b u t m a y c h a n g e h e r s i t t i n g
a s t h e t h e r a p i st p a l p a t e s t h e m a l l o f t h ese m u sc l e s
p os i tio n . Fi r m w e d g e -s h a pe d c h a i r c u s h i o n s a re a l so
re m a i n rel a x e d .
a v a i l a b l e . w h i c h m a y s e rve t h e s a m e · p u rpose e v e n
this
b e t t e r . I f t h e p a t i e n t c a n l e a n a g a i n s t t h e b a c k of a
ra t h e r e x t r e m e s i t t i n g posi t i o n . i t m a y r e p r e se n t a
c h a i r . i t m u s t be s h a ped so as to g i v e t h e s u p port a t
W h a te v e r
the
t h e o re t i c a l
impl ications
of
c o m p e n s a t i o n fo r s i t t i n g i n k y p h os i s . t h e pos i t i o n
most
pe o p l e
adopt
if
the y
re l a x
their
m uscles
wi t h o u t pro p e r s u p p o r t . T h e f a c t re m a i n s t h a t i t
the
c o r re c t
height.
which
freq u e n t l y
is
wh e re
k y p h o s i s p e a k s M a n y p a t i e n t s h a v e to c h a n g e t h e i r
.
s i t t i n g p os i t i o n .
fr e q u e n t l y g i v e s r e l i e f i n p a r t ic u l a r t o p a ti e n ts w h o
e a s i l y ' flo p ' i n to a k y p h o t i c s i t t i n g po s t u r e a n d a re
t e ns e . I t is u s eful to p r o fi t fro m t h is p o s i t i o n for
p a t i e n t s w h o seem to be a b l e t o re l a x in t h is w a y .
e v e n i f o n l y t e m pora r i l y . I n t e re s t i n g l y . t h e p o s i t i o n
g re a t l y fa c i l i t a te s n o r m a l r e s p i ra t i o n .
Stoo p i n g
Prepara tio n: u n c u rling fro m sitting on th e
heels (Fig ure 6. 1 4 5)
S p e ci a l ch a i rs a re n o w m a d e . s l i g h t l y t i l te d fo rwa rd
T h i s is a u s e fu l p r e p a r a tory e x e rc i s e . T h e p a t i e n t s i ts
wi t h a s u p port for t h e knees, s o t h a t t h i s p o s i t i o n ca n
on h e r h e e l s . re l a x e d . a n d b re a t h i n g q u ie t l y . w i t h h e r
e a s i l y be m a i n ta i n e d . T h e y a re r e co m m e n d e d fo r
h a n d s on t h e fl o o r i n fro n t o f h e r k n e e s : s h e i s i n
Copyrighted Material
a
Th erapell tic techlliq lles
Figure 6. 1 45 U n c u rl i n g from s i t t i ng on t h e
heels: (a ) with hands
l o r d o t i c pos i t i o n w i t h t h e pe l v i s t i l t e d fo rward . B y
contraction o f t h e g l u te a l a n d a b d o m i n a l m us c l e s t h e
p e l v i s is t i l te d b a c k a n d t h e l u m b a r s p i n e bro ug h t
i n to k y p h o s i s . B y co o rd i n a ted con tract i o n o f t h e
a b d o m i n a l a n d b a c k m u s c u l a t u re , a n d fi x a t i o n o f t h e
pe l v i s by the g l u t e i t h e pa t i e n t l i fts h e r a rm s fro m
t he g r ou n d w h i l e the l u m ba r a nd t h o r a c i c s p i n e c u r l
u p i n success i o n .
.
A n te- an d retro flexion of th e spinal column
while s tanding
floor:
(b) s t raighten i n g
up
bre a t h e
o u t aga i n s t resista nce, o r m a y press h e r
t he floor. This fo rces t h e a b dom i n a l
m u scles t o c o n t r a c t , a n d t h i s con tracti on s h ould b e
m a i n ta i n e d as the p a t i e n t s t r a i g h t e n s u p , k ee p i n g
h e r c h e s t as close as possi ble to th e t h i g h s o r pelvis,
t o a v o i d l e ve r a ge by t h e t r u n k . The p a t i e n t m a y
c heck u p on h e r abdo m i na l m u scles by p a l p a t i n g
w i t h o n e h a n d ( feedback ) .
T h e p a ti e n t s h o u l d m a k e a h a b i t of p u tt i n g o n e
foot fo rward w h e n s h e has to s t oo p , e v e n s l i g h t l y
( e . g . a t t h e k i tch e n s i n k p e e r i n g i n to t h e b a t h r o o m
mirro r , or in fron t of a c u p b o a r d ) , le a n i n g h e r s l i g h t ly
b e n t k n e e and th i g h aga i n s t i t .
fi n g e rs
to
,
A n o t h e r p r e p a ra t o ry e x e rc i s e ['o r s t oop i n g c o n s i s t s
of t rai n i n g c o r r e c t c u r l i n g u p o f t h e s p i n a l col u m n .
Sta n d i ng e re c t . t h e p a t i e n t con t racts her a b d o m i n a l
a n d g l u t e a l m u s c u l a t u re t o fi x t h e pe l v i s , a n d
a n te tl e x i o n begi n s w i t h t h e h e a d a n d n e c k fo l lowed
by t he t h o rax and a b d o m e n , t h e p e l v i s r e m a i n i n g i n
the o r i g i n a l pos i t i o n . T h e pa t i e n t ca n no t usua l l y
re ach furthe r t h a n to h e r k n e e s , w i t h h e r h a n d s .
F r o m t h i s pos i t i on s h e s t r a i g h t e n s u p . begi n n i n g w i t h
the l u m b a r s p i n e
'
on the
247
'
Retrofl ex i o n
As o u r e y e s a n d h a n d s a re i n fro n t o f LI S , most o f
o u r w o r k . w h e th e r s i t t i ng o r s t a n d i n g , occu rs i n a
fo rwa rd- b e n t pos i ti o n . H e n c e , as a co m pe n s a t i o n ,
ba c k - b e n d i n g is fre q u e n tl y a v a l u a b l e e x e rc ise
B a c k b e n d i n g of t h e l u m b a r s p i ne i n i ts m ost spe c i fi c
for m has b e e n described as se l f- m o b i l i za t i o n ( s e e
Figure 6,58). A less s p e c i fi c b u t very e ffe c t i v e e x e r ­
c i s e is to p u t bot h palms o n t h e b u t t o c k s w h e r e t h e y
form a fu l c r u m , a n d to b e n d b a c k . It c a n be e v e n
m o r e a d v a n t a g e o u s for t h e p a tie n t to l i ft h e rse l f o n
bot h a r m s i n t o re tr o fl e x io n ( s e e F i g u re 4 . 5 6 ) u p t o
[0 t i m e s . R e t r o tl e x i o n c a n be e n ha n ced i f the p a t i e n t
e x h a l e s de ep l y a t m a x i m u m retro fl e x i o n , Accord i n g
t o McKe nzie t h is is effective i n m a n y types o f back
p a i n i n c l u d i ng d i s c l e s io n ; t h i s e x e rcise should be
performed 10 t i m es and r e p e a ted 10 t i mes a d a y
e v e n i f i t c a u ses some p a i n , s o lon g as t h e p a i n d o e s
not ra d i a t e i n t o t h e l e g s .
,
-
,
Lifting a n object from th e gro u n d (see Fig ure
4. 70, p. 134)
The p a t i e n t p u t s one foot fo rward a n cl b e n d s t ru n k
a n d k n ees s i m u l t a ne o u s l y . [ n t h i s way the l o a d i s
e v en l y d i s t r i b u ted b e t we e n leg, p e l v ic and tr u n k
m u s c u l a t u re . T o r e t u r n t o a n e rect posi t i o n , b o t h
knees a re s t r e t c h e d wh i l e the g l u t e a l m us c l e s
s t ra i g h t e n t h e p e l v i s a n d t h e abdo m i n a l m u scles
co n t ro l t h e u n c u rl i n g of t h e s p i n a l colu m n . To
fa c i l i t a t e t h e a b d o m i n a l m u s c l e s , the p a t i e n t m a y
Copyrighted Material
248
Manipulalive
Therapy in
Rehabilillilion of Ihe
LocOl1l otor S VSINII
Lift i n g the a r m s
Raising a n d lo werin g the shoulders
( Fi g u re 6 1 47 )
h e re i s to i m prove fixa t i o n o f t h e
t h e lower fi x a tors o f t h e s h o u l d e r­
b l ad e ( s e r r a t u s a n te r i o r a n d t h e lo w e r tra pez i i ) a n d
The
t o r e l a x t h e u p p e r fi x a t o rs w h i c h a re a ttached a t t h e
fi x a to r s , res i s t e d b y t h e th e ra pi s t T h e p a t i e n t re la x e s
ce rvic a l
d e l i b e r a t e l y , a n d fi n a l l y p u l ls
The principle
s hou l d e r g i r d l e b y
,
spine.
patient
is
one shou ld e r
se a te d e re c t , t h e a rm s h a n g i n g
is r a i s e d b y c o n t r a c t i o n o f t h e
,
down;
upper
.
fi rst
one
a n d then the
o t h e r s h o u l d e r cl ow n , by t h e l owe r fi x a t o r s . T h i s
Mo ving t h e a rms forward, prone ( F i g u r e 6 . 1 46 )
T h e p a t i e n t i s pro n e , b o t h arms s t r e t c h e d o u t , p a l m s
d o w n w a r d s , a n d the fore h e a d o n t h e fl o o r . T h e
p e l v i s i s fi x ed b y t h e g l u te a l
l a t u re . T h e t h e ra p i s t b r i ngs
e x e rc i s e s h o u l d b e c a r r i e d o u t fi rs t o n o n e s i d e , a n d
t b e n o n b o t h s i d e s toge t h e r . I t t e a c h es t h e p a t i e n t
c o n t ro l o f c o n t r a ct i o n a n d re l a x a t i o n o f t h e re l e v a n t
m uscles.
a n d abdom i n a l m us c u ­
the s h o u l d e r- b l a d e i n t o
L ifting both arms, s ittin g
correct p osi t i o n by c o n t r a c t i o n o f t h e l o w e r p a r t o f
the tr a p e z i u s
.
T h e p a l m s a re
n o w fl a t o n t h e fl o o r.
fi x e d , t h e p a t i e n t
T h e pa t i e n t s i t s e re c t on a s t oo l , b e fo r e
K e e p i n g t h e s h o u l d e r- b la d e w e l l
r a ises h e r h e a d s l igh t l y , m ov i n g h e r o u ts t r e t c h e d
i n s u c h a w a y a s to t u r n t h e p a l m s
fo rwa rds w h i l e k e e p i n g t h e u l n a r s u r face o f t h e
hands o n t h e fl o o r . T h e lower fixa t o rs o f t h e
s h o u ld e r- bl a d e re m a i n c o n t racted, w h i l e t h e u p p e r
fi x a t ors a re r e l a x e d .
a r ms fo rward
Figure 6.146 M ov i n g rhe a rm s forwa rd, prone:
m i rror.
u p p e r fi x a t o rs , i . e . a t fi rst o n l y li p t o 9 0 d e g r e e s a n d
fi n a l l y t o 1 80 degre e s . T h i s fi x a t ion
m a i n t a i n e d w h e n l ow e r i ng the
(II) fi rst p h �se; (b)
Copyrighted Material
a
the s h o u l d e r- b l a d e s from be l ow, as
fi r m l y as s h e ca n , t o avoid a c t i v a t i n g the u p p e r
fi x a t o r s . M a i n ta i n i n g t h is fi x a t i o n , s h e s l o w l y raises
h e r arms a s fa r a s she can w i t h o u t a c t i va t i n g t h e
She now fi x e s
second
phase; (e)
t h ird
p h ase;
s h o u l d a l so
a rms.
(d) fa u l ry
be
Th erapeu tic tech n iq u e.)
Figure 6.148 Li ft i n g the arms over t h e h e a d :
a n d (b) fa u l t y
(a)
249
correct
Breat h i n g
Figme 6. 1 47 R a i s i n g a n d l o w e r i n g t h e s h o u l d e rs to t ra i n
( a c t i v e ) re l a x a t i o n o f t h e ( u p p e r ) t r a pe z i u s : (iI) re l a x e d
A rs t a n d e n d - p os i t i o n : ( ll ) s h o u l d e rs raised
T h e m o s t s e r i o u s fa u l t h e r e i s l i ft i n g t h e t h o r a x
d u ri n g i n h a l a t i o n . D u r i n g e x a m i n a t i o n , w i t h h i s h a n d s
o n b o t h s i d e s o f t h e p a ti e n t ' s t h or a x , t h e t h e r a p i s t
may e n co u rage t h e pa t i e n t by e x e r t i n g s o m e p r e ss u re
d u r i n g e x h a l a t i o n a n d by
re l e a s i n g t h i s p r e ss u re
d u r i ng i n h a l a t i o n to p ro d u ce w i d e n i n g or n a rr o w i n g
L ifting th e a rms abo ve th e head
(Figure 6. 1 48 )
o f t h e t h o r a x . U s u a l l y , t h i s d o e s n o t s u ffi c e .
T h e p a t i e n t s i t s e re c t o n a s t oo l , ra i s i n g h e r a rm s
t h e sca l e n e s , w h e re t h e y h a v e b e e n fo u n d s h o r t e n e d
The fi r s t ste p i n t r e a t m e n t s h o u l d b e r e l a x a t i o n o f
a b ove t h e h e a d a s s h e d o e s , fo r i n s t a n c e , w h e n
( se e p . 2 1 3 , F ig u r e 6 . 90 ) . I n s e v e r e c a s e s t h e m a n ­
com b i n g h e r h a i r . C a re m u s t b e t a k e n t o fi x t h e
o e u v re d e s c r i b e d b y S a c h s e a n d S a c h s e ( 1 975) i s
s h o u l d e r- b l a d e c o r r e c t l y , t o re l a x t h e u pp e r fi x a tors
a d v i s e d : t h e p a t i e n t , s e a t e d o r s u p i n e , i s a s k e d to
a n d t o co n t ro l t h e pos i t i o n of t h e h e a d .
p re s s h e r fl e xed e l bows d o w n w a r d s aga i nst r e s i s t ­
a n c e , w h i l e b re a t h i n g i n d e e p l y . For se l f- t r e a t me n t
s h e m a y p re s s h e r e l b o w s d o w n o n t h e a rm s o f a n
Sitting e rect, turning t h e h e a d ( s e e F i g u r e 4 . 7 3 ,
a rm c h a i r .
p. 1 35)
T h e pa t i e n t si ts e re c t o n a stoo l , t u r n i n g
her
head.
I f t h e p a t i e n t lifts h e r t h o r a x m o r e o n o n e s i d e
t h a n t h e o t h e r , t h i s us u a l l y rev e a l s wea k n es s o f t h e
The re s h o u l d b e a x i a l r o t a t i o n o f t h e cervi c a l a n d
l owe r t r a pe z i u s o n
t h o r a c i c s p i n e , t h e s h o u l d e r - b l a d e s fi x e d f r o m b e l ow ,
w h i c h m u s t b e t r e a t e d se p a r a t e l y .
t h e u p pe r fi x a tors re l a x e d . I n t h i s w a y coord i n a te d
t h e s i d e o f i n c r e a s e d l i ft i n g ,
W e t h e n t r y to m a k e c o r r e c t b re a t h i n g a u t o m a t i c ,
by t h e m e t h o d o f G a y m a n s ( 1 980) : t h e p a ti e n t s i t s
h e a d rota t i o n i s a c h i e v e d .
e re c t o n a s t o o l , b o t h fe e t o n t he gro u n d ( h i g h h e e l s
Correct wei ght carry i n g
(see Figure
a re p ro h i b i te d l ) . T h e h e a d i s e re c t , i . e . t h e e y e s l o o k
4.74,
a t a n o bj ec t p l a ce d a t e ye l e v e l , w h i l e t h e t i p o f t h e
p . 1 36 )
For correct w e i g h t ca rry i n g , t h e p r o p e r fi x a t i o n o f
t o n g u e p re s s e s a g a i n s t t h e h a rd p a l a t e a bo u t o n e
fi n g e r ' s b r e a d t h b e h i n d t h e t e e t h . T h e h a n d s l ie i n
t h e s h o u l d e r- b l a d e i s esse n t i a l , a s d ur i n g l i ft i n g o f
t h e l a p , c l a s p e d i n s u p i n a t i o n , t h e fi n ge r t i p s e x e r t i n g
t h e a r m s . H e r e , h o w e v e r , i t i s a l so i m p o r t a n t t o re l a x
s l ig h t press u re o n t h e b a c k o f t h e h a n d s , o r w i t h t h e
t h e s u bc l a v i c u l a r p a rt o f t h e p e c t o r a l i s t o m o v e t h e
fi n ge rs o v e r t h e th u m b i n s u pi n a t i o n i n fro n t o f t h e
h e a d a n d sho u l d e r b a c k , i n re l a t i o n t o t h e s p i n a l
a b d o me n ; i n n o c a s e m a y t h e s h o u l d e rs b e r a i se d .
co l u m n . Coord i n a ted c o n t r a c t i o n o f t h e i n te rsc a p u l a r
T o faci l i ta te i n h a l a t i o n t h e p a t ie n t m a y l i ft h e r t o e s ,
m u scl e s i s t h e re fo re necessa ry . T h e m o m e n t t h e
w h i l e t o fa c i l i t a te e x h a l a t i o n s h e p re s s e s h e r toes
p a t i e n t succeeds i n b r a c i n g h e r s h o u l d e rs b a c k , t h e
against
w e i g h t s h e c a rr i e s ceases t o a ffe c t t h e c e r v i c a l s p i n e
p e r fo r m e d i n fro n t o f a m i rr o r , t o m a k e s u re t h e
c l a v i c l e s d o n o t m o v e u p a n d d o w n . A n a l t e r n at i v e
i s B ru gge r ' s re l i e f p os i t i o n ( s e e F i g ure 6 . 1 44, p . 246 ) ,
a n d t h e u p p e r fi x a t o rs o f t h e s h o u l d e r g i rd l e r e m a i n
re l a xed . N o t o n l y i s t h e re r e l a x a t i o n o f t h e s h o u ld e r
g i rd l e , b u t a l so h o l d i n g a n o t t o o h e a v y w e i g h t , l i ke
the
fl o o r .
T h is
e xercise
should
fi rst
be
a b r i e f-case , beco m e s possi b l e w i t h a l m o s t r e l a x e d
a n d poss i b l e c o m b i n a t i o n s .
O nce t h e p a t i e n t h a s m a s t e red correct respi ra t io n ,
hands.
s h e g e t s a fee l i n g fo r t h e r i g h t w a y to b re a t h e , i . e .
Copyrighted Material
250
Manipulative Th erapy in Rehab iliwtivn o{ the Locomotor Systcm
how to broaden t h e t horax fro m t h e waist u pw a rd s
w i t h o ut these fac i l i t a t i n g m a n o e u v res, so t h a t s h e
c a n b re a t h e correctly d u ring her d a i l y a c t i v i ties.
A ccord i n g to G a y m a n s ( 1 980) , high heels constitute
a serious i m pe d i m e n t to correct respira t i o n . Abdom­
inal resp i ra t i o n must be practised w i t h t h e pa t i e n t
supine.
I f t h e pa tie n t is u n a b l e to b re a t h e i n to t h e thoracic
s p i n e while p ro n e , t h e same faci l i t a t i n g position
should be a dopted as for self-mob i l i za t i on o f the
t horacic spine i n to fl e x i o n (see Figure 6 . 62 , p . 1 97 ) .
I t i s a l so i m p o r t a n t for t h e p a tie n t t o re l a x h e r
fa cia l m u scles a n d t h e m us c l e s contro l l ing t h e
tongue a n d j a w . S u c h is the i m por l a n c e o f correct
r es p i r a tion that a ny gross fa u l t is bound to jeopard­
ize the rest of the motor p a t terns and even t h w a r t
the e ffec t of mobil iza t i o n tech n i q ues.
T h e hands. thei r pos i t i o n a n d e v e n to n u s h a ve a
m a rk e d i n fl ue nce on re s p ir a tio n . This can be q u i t e
i m porta n t i f a p a t i e n t ca n n o t rel a x h is h a n d s .
Figllre 6. 1 49 R h y t h m i c l i ft i n g o f t h e k n e e by n e x i o n o f
t h e t o e s a ncl t h e a n k l e . wi t h t h e p a t i e n t s e a te d
metacarpa l s ; or by r o t a t or y move m e n t s a t t h e i n te r ­
p h a l a nge a l J o i n t s .
The feet
T h e fee t a re a k e y region of t h e motor s y s te m .
U n l i ke the h a n d s t h e y a re rarely u nsho d . S hoes n o t
o n l y m o d i fy t he i r mobi l i ty, t h e y a l so d e p rive t h e m
o f m o s t o f the n o r m a l s e n sory i n pu t s . I t i s t h e refore
i m porta n t to advise p a t i e n ts to w a l k b a r e fo o t
whenever there is a reaso n a b l e opport u n i ty. Because
of this se nsory deprivation stroking p l ays a p 3 1·ticu­
l a rty i m po r ta n t role i n the t re a t m e n t o f fe e t - both
if the p a t i en t ove r-reacts a n d even m o re so i f s h e
d o e s not r e a c t a t a l l ( ' d e a d fee t ' ) .
W h e n w a l k i n g i t is i m po r t an t for the fee t to p l a y
a n a c t i v e ro l e . parti c u l a rly i n t h e act o f p r op u l sion .
w he n t he toes s h o u l d be a c t i v e . So as to tra i n a c t i v i ty
o f t h e toes, t h e pa tient s h o u ld grasp objects on t h e
floor such as penci l s . P repa ration for usi n g the t o e s
fo r p ropu l s i o n w h e n wa l k i ng is fo r t h e s e a t e d p a t i e n t
rh y t h m ica l ly to l i ft h e r knee by b e n d i n g t h e toes a n d
exten d i n g t h e a n k l e ( Figure 6 . 1 4 9 ) . In t h e s w i n g
p h a s e . t o o , t h e fee t s h o u l d p l a y a n a c t i v e ro l e : fl e x io n
o f t h e l e g s h o u l d be i n i t i ated by e x t e n s i o n of t h e b i g
toe. R u n n i ng i n d e e p s a n d is i d e a l .
Patients w i t h a h a l l u x v a l g u s s h o u l d t ra i n
a b d u c t i o n o f t h e b i g toe . T h i s req u i res conce n t ration
a t fi rs t ; t h e patient m a y s t a r t by moving the toe
pass i ve l y a nd o n l y grad u a l l y try active m o v e m e n t .
S h e s h o u l d stim u l a te t h e a b d uctor po l l icis b revis b y
s t ro k i n g i t on t h e m e d i a l s u rface of the foot. T h i s
exe rcise is not o n l y prev e n t i v e , i t a l so re l ieves p a i n
a t the ha l lu x v a lgus.
The h a n ds
There is fre q u e n t l y hypertonus - 'crampe d ' h a nds.
P l a y i ng w i t h a soft b a l l or rice is a d v i sa b l e . Stro k i ng
a n d massage of t h e h a n d s is r e co m m end e d : t h is m a y
b e ca rr i e d o u t along t h e a x i s of t h e fi n ge rs a n d
S u p p o rts
So fa r J h a v e d e a l t m a i n l y w i t h tech n i q u es t h a t
restore or correct m o b i l ity; i t is beyond t h e scope o f
t h i s b o o k to dea l w i t h i m m o b i l iza t i o n tech n i q u e s . I t
i s u s e fu l , however. t o reco m m e n d s i m ple s u p ports
t h a t can be made by p a t i e n t s at h o m e .
O n e i s a soft c e r v i c a l co l l a r o f l a t e x fo a m ( F i g u r e
6 . 1 5 0 ) . fi tted to t he s h ape or t h e n e c k . T h e soft
materia l . pl a ced round t h e n e c k t o fo rm a t u be .
becomes a s o ft a n d y e t su fficient support fo r t h e
cervica l s p i n e ; cove red i n some s o ft m a t eria l , i t can
be secu red by t a pe and protects t h e p a t i e n t from
j o l t i n g in p u b l i c t r a nsport v e h i c l e s .
Hypermobile p a t i e n ts w i t h m a rked l u m b a r kypho­
sis w h e n seated s h o u l d ca rr y a n in fl a t a b l e cush ion
w i t h them to use when t hey lean a g a i n s t a cha i r­
b a c k . e tc . ( Figure n. 1 5 1 ) . The c u s h i o n s h o u l d be o n l y
s l ig h t l y i n fl a te d . a n d fi t ted to the top of t h e k y p h o s i s .
fi x e d by braces o r a b e l t . T h i s is of p a r t i c u l a r va l u e
fo r ca r d rivers; i t i s n o t o n l y e a s i l y a d a p ted t o each
i n d i v i d u a l case, but a lso a d a p t s i t se l f to the p a ti e n t ' s
move m e n ts .
Hypermob i l e p a t i e n ts w h o freq u e n t l y s u ffe r from
low-back pa i n in bed ( ' l i ga m e n t ' p a i n ) may profit
from a fi r m pelvic b e l t . fixed between t he pe l v i c
c r e s t s a n d t he gre a t e r t roc h a n lers. I t s h o u l d be
suffficiently b r o a d . a n d l i ned with a m a t e r i a l t h a t
does not i rritate t h e s k i n . I t m ust be fa s t e n e d fi r m l y
( Figu re 6 . 1 5 2 ) . The e ffect is noticeable o n l y a ft e r i t
h a s b e e n worn fo r a fe w wee k s . Pa ti e n t s w i t h fla bby
abdom i n a l m uscles, o ften acco m p a n i e d by obes i t y ,
should wear a fi rm belt o r ( i n t h e c a s e o f wo m e n
p a t i e n ts ) fi r m e l a s t i c p a n t i es.
Copyrighted Material
Th erapeutic techn iques
Figure
Figure 6. 150 Soft s u p p o r t i n g col l a r
6. 152 Pelvic belt ( A ft e r
cri b e d h e r e . P r o b a b l y
25 1
Cyri a x , ( 977)
T h e re a re i n n u m e ra b l e m e t h od s e m p l oy i n g r e fl e x
t h e m e t h od most p o p u l a r w i t h
d octors i s loca l a n a e s t he s i a . A s s h o w n i n C h a p t e r 5 ,
t h e re s e e m s to be l i t t l e d i ffe re n ce b e t w e e n t h e e ffect
o f l o c a l a n aesthesia and d r y n e e d l i n g , p r o v i d e d t h a t
t h e r i g h t t e c h n i q u e i s e m ployed. This is i n good
a g r e e m e n t w i t h the r e s u l t s of Frost el £11. ( 1 980 ) , w h o
fo u n d i n a d o u b l e - b l i n d test t h a t p h y s i o l o g i c a l s a l i n e
sol u ti o n w a s , i f a n y t h ing, m o r e e ffective t h a n loca l
a n a e s th e t i c . The c r u c i <l l te c h n ica l po i n t i s t h a t t h e
n e e d l e m ust touch t h e pa i n p o i n t . I t is n o t e n o u g h
for the p a t i e n t to fee l pai n : t h i s p a i n m u s t be
s u f fi ci e n tly i n t e n se for t h e p a t i e n t to react, and t h e
t her a p i s t sh oul d s e a r c h t h e p a i n fu l a re a to fi n d t h e
m o s t p a i n fu l s p o t . O n ly t h e n ca n f u JI a n d i m m e d i a t e
re l i e f b e fe l t , a re l i e f t h a t i s j us t a s i n te nse a s i f a n
a n aesthetic h a d b e e n used , bu t w i t h o u t t h e
a c c o m p a n y i ng a n aest h e s i a . ( T h i s m u s t a l way s b e
teste d . ) I t i s a te c h n i c a l a d va n t a ge of d ry n e e d l i ng
that the p o s i ti o n o f the n e e d le can be corrected if
no a n a l gesi c e ffec t has been obtained. O nce loca l
a n a est h e t i c h a s been a p p l i e d , of c o u r s e , n o
correction is p o ss i b l e . I f t h e p a i n p o i n t h a s n o t b e e n
reach e d , the therape u t ic e ffe c t o f l o c a l a n a esthe s i a
i s u s u a l l y s l ig h t , o n ce t h e a n a e s t h e s i a w e a rs o f f.
I f, h o we v e r , n e rve b l oc k i s i n d i c a t e d ( i . e . n e rve
r o o t i n fi l tr a t i o n ) , t h e n the a pp l i c a t i o n o f l o c a l
a n aesthetic is n ecess a r y . These a re we l l - k n o w n a n d
w i d e l y p u b l ished tec h n iques w h i c h w i l l n o t be dea l t
m e c h a n i s ms ( s e e
with here.
Figure 6. 1 5 1 I n fl a t a b l e support i n g c Ll s h i o n fo r l u m b a r
l a t e ra l v i c w : (h) back v i e w
k y p h os i s : ( a )
H i nts o n reflex t h e r a p y
Chapter 5 ) which
c a n n o t b e des-
Copyrighted Material
7
Clinical aspects of disturbed function of
the locomotor system
[n this c h a pter the gen era l principles of t h eor y ,
re.levance assessed, bu t o n ce th i s has been d o n e we
d iagn o sis and t he ra py w i l l be app lied to specific
n e ed t h e diagnosi s of disturbed function fo r t h e vast
c l inica l enti ties or s yn dro m es, in which disturbed
m ajo ri ty of patien ts 'withou t any speci fi c di a g nos is '
9).
As these conditions form the s u bj e c t of
fun c ti on of t h e locomotor system and of the s p in a l
( see
column in par ticu l a r has a si gn ifican t ro l e . It s h ould
all c l assic textb ooks of rheum a t o logy or ort hopae d ics ,
p.
be re m e m bered tha t fami l ia r c l i nic a l pictures suc h
however, we may pass them by and devote ou r
as b a ck p a in, low- b a ck pain, s h oulder p ain
attent ion to our main su bj e ct .
,
head­
a c h e, etc., have rarely been considered from this
For a n a mn e sis , refe r to the begin n i ng of C ha pt er
poin t of vi ew ; there is, therefore, l i tt l e on the sub j ec t
to be found in the literature ( M enne l l 1952; BrUgger,
4. H e re, too, a part is p l a yed not onl y by the fac t o rs
acting upon the mechanical fun c tio ni n g of the sp in a l
,
1977; Cyr iax, 1977; Tr a ve l l and Simons, 1983, 1993;
M a i gne , 1996). Nevertheless, this ap proa c h must b e
used t o s h ow t h e p r a c ti ca l app lication o f a l l .
been put forward in the pr e c e ding c h a p ters . It is
of grea t c o n s e q u e n ce for medical t h e ory that t h is
new appr oac h h a s reve a .l ed un susp ec ted features in
t h es e fa miliar clin ical entitie s. This h as been made
possi b l e bec a use t h e t h era p e utic m e as u res we use
are h ighl y spe c i fic ; neverth e less , th e y can only be
call ed upon a n d ap p l ied to the best a dva nt age if the
c l inical d i a gn o sis h as be e n draw n u p acc u ra t e l y . As
t h e nu mber of pr ofess iona l s w o rk ing in this field
rapidl y in c re a ses , the b ody of c l inic al data grows
apac e .
column, but also by those th a t a ffect the (a uto ­
n o m i c ) ne r v o u s syste m - the weill h e r, c o l d or heat,
i nfection, h o rmo na l c han g e s (including menstru­
a tio n ), and last but not l east , p syc ho l ogic a l fa c tors .
For p recise c l inica l ana l y sis, back pain is far too
i l l -defi ned, and i t is necessary to treat the various
sections of the spin a l colu mn ( t h e back) one by o n e .
The first subj ect i s low - ba c k pain.
Low-back pain
The de r m a t o me chart shows that in t h is region
a
great n um be r of seg m e n t s c onverg e , fro m th e t hora­
co l umb a r j un cti o n to the sacral segme nts (se e Figure
4.2,
pp .
90-93),
with the possibi lity of referred pain
from the whole o f th i s vast region.
Furthermore, the
most p o w e rfu l forces (m u scle s ) act here, where the
Backache
trunk
[n backache, at le as t , the signific a nt ro l e of the spin a l
column i s b e y ond doubt. However, the p ro ble m i s
t rad i tional l y treilte d main ly or even ex c l usi ve l y
morphological ly, which gives t h e im pr e ssion that a l l
w e h a v e t o d o i s t o find t he under l y ing inflamma tory,
degenerative, meta b ol i c or neoplastic diseas e , or
ma l forma ti on , or at l eas t a gross mec h a nical obs t a c l e
has
its
mo v eme nt
of
greatest mobility and
the
lower
e x tre m i ties
where the
must
be
transferred to the tfunk . All of t h is e x p l a ins the great
v ulner a b il i t y of the region and is a p ointe r to
the
many possi bl e pathoge ni c factors that have to be
b o rne in min d , a nd the r e l e vance of w hich must be
assessed in every c ase . The most important disturb­
the
an c e s of fun c tion causing certain types or low-back
pain and their resp ec t ive therapies are now re v iewed .
diagnosi s of d isturbed function, such traditional
disorders undou bted l y have to be e xc l ud ed , or their
It may be useful to add t hat tile term ' low-back pain'
i nc l ucles pain radia t i ng to both sides, tow a rds the
such
as
disc herniation.
Before turning t o
252
Copyrighted Material
Clinical aspects
hips, huttocks or groin,
and
that this pain is usualh
of distllrhed
01
.1
system, e.g. the
spine.
vstCI1I
253
the cervical
Thera py
Low-back pain due to ligamental and
muscular overstrain
If exogenic strain is the main cause, we should try
to correct posture and faulty movement patterns at
In this type of low-back pain. not only need there
work; If thc underlying cause is faulty statics and
be no morphological lesion, but the spinal column
muscular imbalance. correction of statics and/or
as such may he functioning normally. at least at the
remedial exercise are indicated. In the hypermobile
a support during static loading is important, particu­
outset As this first category is not homogeneous,
some further definition is required: the cause of
strain may be
cxogenic
like
physical labour. or more I
under conditions
posture or bad movem\'nl
excessively heavy
performed
faulty
even. this overstrain
larly in public transport vehicles. Where obesity
is a relevant factor. weight reduction is essential.
of muscle
For immediate
tension, of triggcI
Ii(.�ntly.
ion points is mosl
[lilei/or
antagonist inhibition.
movement patterns
Finally, it is
such as difference in lelY
imbalance may
rosis, muscular imbalmlcc,
the craniocervical
etc. the common denlJrninl\\or
which must not
ligamental overstrain.
back pain.
S y m pt o m s
Discomfort and pain are usually the consequence of
activity, postural even more than dynamic, and they
Increase as activity continues. Often it is postural
strain that is more disagreeable than movement.
Thus. any position that has to be held for any length
of time is registered as a strain, patients feeling the
[n
cases
need to change position,
which is
there is pain (stiffness)
gradually overcome,
11\l"r by
pain as a sign of fatigue.
Clinical signs
and in
:111:1 lysed
:I
in each case. The typical imbalance
region
This condition may accompany the preceding one.
It
must
not
be
is
between
the
111
the lumbo­
gluteal
and
the
thought
to
be
identical
to
coccygodynia: it is low-back pain due to a tender
coccyx of which the patient is often unaware. In an
earlier paper I showed that onlv one-fifth of the
patients with a
godynia: the
pain. On the 01
'coccygeal pain'
painful
sacroiliac dysfuncl
·reilex or even
to a painful ischial I
These consist of changes
faulty movement patte!!1"
sacral
A tender coccyx
frequent cause:
cases. and rarely
1rl
lower
injmy the most
olle·fifth of the
tenderness of
the coccyx. PsycilOloglcal tension and anxiety are
frequent.
abdominal musculature on the one hand. and the hip
Acxors and the back muscles on the other. This is
S y m pt o m s
frequently made worse by hypermobility, which
Low-back pain, particularly when sitting; there may
results in what is called 'ligament pain' (p.
101).
The
be constipation anel even dyspareunia. Pain may be
hvperactive erector spinae as well as the iliopsoas
can be tender. The most typical tender periosteal
referred to the groin and hips, but this is not very
characteristic,
points arc the spinous processes, in particular the
last two and the spinel
. If
Clinical signs
there is marked asymmetry
The diagnostic
the iliac crest and the
the coccyx which
imbalanced scoliosis
touch; this is
lumborum.
dorsal aspect. A�
Baastrup-',
rosis of the spinous
which makes
thought to play a pan.
important sign
Ip;lInful) tip of
I. he slightest
iatlta than the
is kyphotic,
Another
of the spinous processes.
of the gluteus
is usually found in hypennol.lIle younget patients
piriformis. There rnay be a pOSitive straight leg
without osteochondrosis. and where there are typ­
raising test. Patrick's sign and spasm in the iliaci, and
ical X-ray changes no pain or tenderness is found on
there is often an HAZ visible on the sacrum in the
the spinous processes. Quite frequently we have to
form of a fat cushion. TrPs are found in the levator
look for the cause in other regions of the motor
ani (per rectum).
Copyrighted Material
Copyrighted Material
Clinical aspects of disturbed junction of
Table 7.1 Clinical signs uf bluckage of the
joints of the
lumbar spine
and
of
the
sacroiliac
Sign
the locomotor system
255
joints
Segment
Lilck of pelvic rotary syn kinesis
Straight leg raising: hamstrings spasm
Femoral nerve stretch test: spasm of rectlls fe mor is
Spasm of thoracolumbur erector spinae
Spasm of quadratus lumborulll
Spasm of psoas
Spasm of lumbar erector spinae
Piriformis spasm
TIL
LJI4
++
+
L415
L51S1
Sacroiliac
+
+
++
+
+
+
+
+
++
++
++
++
+
++
lIiiicus spasm
Painful iliac c rest
+
+
P,linful gre,-ilcr trochanter
+
Painful posterior
superior il ia c spine
L4 segment (hyperalgesia)
Pain nldiating in L5 segment (hyperalgesia)
Pain radiating in S I segment (hyperalgesia)
Patrick's sign (ildductlll' spasm)
Tenderness of the symphysis
Tenderness at the ends or sacroiliac joint
+
P,lin radiating in
+
+
+
+
+
+
+
+
+
++
+
+
the hip joint. It is therefore the most e ffect i ve type
of conservative treatment.
Allhough self-treMment is difficult, o n ce the
patient has learned what to do du r i n g the iso metric
phase, and how to re l ax, the role of the therapist
is negligible. Any relative or fr iend can help
the pa tient, regularly, once a day if po s si b l e , for
about 5 minutes. If there is i m b a la n c e of t h e muscles
of the pelvic gir d l e, most frequ en t l y weakness of
the glutei, particularly of the a b duc t o r s , with hyper­
activity in t h e hip flexors and adductors, it is
important to rel a x the taut m u s cle s and train the
weak ones.
In coxarthrosis a well-planned regimen is e ssen ­
tial, sett i ng down how much w a l k in g the p ati e n t is
+
+
+
+
+
++
Blockage of the joints of the lumbar spine and
of the sacroiliac joints
Low-back pa in due to blockage of a p op h ysea l j oints
and to bloc k a ge of the s a cro i li a c joints sha res a
com mon therapeutic approac h and t h e s e conditions
also have some clinical features in com mon.
Symptoms
If th e state is acute there is severe mo v e men t
res t r i ct ion, and stra i ghtening up usuall y presents
more diffi culty than s too p i n g; there may be pa in on
sn eez ing or cough i ng . In more chronic cases there is
usu all y stiffness after rest lying down or s i tting, w h ich
im prove s on movem e n t . B a ck - b ending is more fre­
quently rest rict ed than stooping, and the most char­
a l lowed to do. p re fer a bly on soft g rou n d with t h i ck
acteristic com pla i nt is d i f fi cu l ty in straightening LIp
crepe rubber soles and c ar ryi ng a stic k on t h e side
not affec ted - regular e x erc is e in t h e supi ne position
should be performed. and sw im ming and cycling are
to be encouraged. Loads should be carri ed on the
affected side.
after stoo p i n g. Side-bending can be restricted and
P. J. (1911) fell Oil the I. i g,h t hip, and felt sharp pain down
and in the groin. as well as in the low back. She
walked with a stick. ,\Ie found a positive Patrick's sign: the
femoral head was painful and so was active abduction of
the right lower leg. Internal rotation was n ot painful.
Immediate relief was obr,lined by traction along the axis
of the rig ht leg. Two months later there was no pain, and
t hi s state persisted for many years.
the leg
painful, at least to on e s i d e , a nd typi c a l l y t here is no
rota t ion of the pel vis on side-bending. Pain is usua l l y
a sym me tr i ca l and may radiate to t he h ips , buttocks,
lower abdomen, groin, lower extremiti es, and towards
the thoracic spine.
Clinical signs
Typical s i gns of b lo c k ag e are found in all the j oints
affected, including tenderness and resistance to
springing ( see p. 102). The more s pec i fic s i gns a re
given in Table 7. I; t h e thora colu m b ar junction
IS
formed by the segm e nts TIO-U; seg m en t
is
L2/3
affected only in exce ptio n a l ca se s .
This patient illustrates an acute l esion of t he hip
joint without cox arthros is.
NOle: A posi t ive stra i g ht l e g ra ising t est is due to
Copyrighted Material
256
Manipulative Therapy in Rehabilitation of the Locom%
s p a sm of the h a m strin gs while the
stre tch test is po s it ive in s p a s m of the
j ust as Patrick's sign is c a used by
a d d u c t ors. The c h aracteri stic m u scle
r System
femoral nerve
rec tus fe m o ris ,
spasm of the
s p a s m s ( TrPs)
for each segment are very im portant features of the
clinical p i c ture of e a c h type of b l ock age: s p a s m of
t he p s oa s [o r t he a b d o m in al pain in t h o racolumbar
l e sio n s ; spa s m of t he rectus femoris for pain from
t he thigh to the knee in lesions of L3/4; p i r ifo rmis
spasm for p a i n in the b uttocks i n L4/S lesions; an d
iliacus spasm for pse u dogy n a e co l o g i cal symptoms
( a lgomen o rrh oe a ) in lesions of LS-S1.
Low-back pain due to disc lesion
T h e c ases gr o u p ed under this head i n g are those In
which there is n o radic u l a r s y nd ro m e It is essenti a l
to k n o w when a disc l e s ion should be s u s p ec ted in
lum b a g o even without signs of root compression. If
t h i s is the case, we have to d ea l with a lesion n o t
o nl y of function but ( a ls o ) of stru ctu re.
Figure 7 1 Typical posture
in acute elisc lesion (,sciatic
..
scoliosis')
.
Symptoms
spi n e if b l oc k a g e is absent or if it persists after
b loc k a ge has been treated. [f man u al lumb a r tr ac t ion
gives relief, this is a g o o d diag n ostic test.
Unless acute, the co urse is as a r u l e m ore severe
tha n in the cond itio ns alre a d y d e alt with, that is to
Therapy
say, artacks la st l o nge r and the condition has a
te n d e n c y to r e l a pse. Pain at c o u ghing, etc. is more
p r o mi n en t. The post ure th a t is p arti c ul arly harmful
is th a t of s ligh t l y b e n din g forward, as o v e r a wash­
basin while sh a v i n g , where c o n tr a ct i o n of the erec t o r
s pi n a e is at its m a xi mu m a nd t he r e is therefore
maximum pressure on t he disc. Another c h ar a cter­
i s tic co m p l a i n t is of p a i n w he n tu rn in g over in
bed and w h e n ris i n g from t h e recumb e n t a n d s i t ti n g
positions.
rest in the relief position is
(by hand)
in this p o s itio n because it may pro c ure immediate
r e lie f (se e Fi gu r e 6.2S, p. 175). If pain continues in
the rel ie C p os iti o n , e p i d ural inflltration with l oc al
a n aesthe t i c may bring a b o u t immediate relief. The
met h od of str a i n and cou nter st r a i n (see p. 2(2) c a n
be very u sefu l even at this s tag e if the exagge r a te d
relief p o s i t i o n is well tolerated This may, and
s houl d , be co m b ine d with the usual ph arm ac o
ther a py as p i ri n (u n le ss c o n t rain d i ca ted ) remaining
one of the most e ffect ive drugs.
In the more chronic cases, t rac ti o n is again very
im p o rta nt as l o n g as it gives relief. I f t h ere is
s eg m e n t a l movement restrictioll this sho u l d also be
treated b y moblization and/or manipulation: so ft
tissue l e sions, of t h e fasciae in p a rt i cula r , should be
given d u e attention. A ls o ch a n ges in ot h e r parts or
the motor s y s tem if c o nsi d er e d rel evant, mllst be
tr ea t ed . The McKenzie method, in particular his
ex t e n si o n tech n iq ue s if tole rated, are very eff ec t ive
( l is t e n ing to the p a t ien t s sy m pt o m s ) see p. 247.
Most i mpo r ta n t here is t h e establishment or a
suit a ble reg i me n av o i d i n g the most dangerous
ca uses of strain sllch as th e forward-bent p o s i ti o n
j o lt i n g in ve hicl e s , etc., combined with judicious
remedial exercises; the lumbar region should also be
well p r o te c ted a g a i nst c h i l l . Comp l ete rest should
not be e nco urage d l o ng e r tha n it is absolutely
necessary.
In acute cases c om pl et e
recommended; traction may be attempted
,
,
­
,
Clinical signs
In a c ute cases we s ee the cha ra c te r isti c a n t a l ges i c
po si t i o n a d o p te d in ac u te root lesion (Figure 7.1),
i.e. k y ph o sis a nd lu m b ar sc o lio s i s , m o s t freq ue n tl y
towards the s i d e of the le s i o n ( s e e Figure 3.8, p . 44).
S t oop ing is s e v erely l i m ite d and the straight leg
rais i n g test marke d l y p o sit ive (except in l e sio ns at
th e L3/4 s e gm en t where the femoral nerve stretch
test is p o si tive) All movement di s tu r bin g the
a nalgesi c posture is severely rest ri cte d . If t h e patient
is c a p a b le of lying prone, s p ri n g ing of th e lumbar
spine is very painful, p a r tic ul a rl y at the site of the
les i o n . Nevertheless, if bl ockage of individual seg­
m e n t s is examined this m a y be a bs e n t
In the m ore c h ro nic cases it is s t o o pi n g that is
usually most im p a ire d while the pa tie n t is sta n d ing
but with the pa ti e n t se a te d a n te flexion m a y be
n o r m a l . Another d i a gn o s tic sign is the p a i nf u l a r c
( C y ria x, 1977) (see p. 102). The strai ght leg r a isin g
test, a n d the fe m o ra l nerve stretch test in L3/4
lesi o ns may be m ar ke d ly positive, much more so
than when th ere is only joint b l oc k a ge . A most
useful d ia gn ostic sign is pain on s p rin g ing the lumbar
.
.
,
,
,
,
'
'
,
,
o. F. (71) seen 22 December 1986, complained of low-hack
pain worsening all standing or walking. particularly when
going down stairs, jolting. carrying loads, or turning over
Copyrighted Material
Clinical
in bed, on coughing or
both
legs dorsally. more on I
after excessive effort (liI:,nl'
The patient gave a history of headache. eprcondylar pain.
and (since
omy
1979.
j 977) occasional low-back pain. Cholecystect
At examination there was 3ntalgesic kyphotic posture.
back-bending restriction and side-bending restriction. yet
stooping was normal and the straight
leg raising test was
aspects of disturbed
Iystem
operator adducts
257
on the side
until the
where the anterl()r
slack is taken up:
patient to press
against his hand into abduction, This is resisted for
about 10 s, the patient slowly breathing in, and
relaxing while the therapist increases adduction,
producing inward rotation of the innominate. On the
side where the anterior spine is more prominent and
negative. There was severe pain on springing the lumbar
medial (inflare) the therapist o btains outward rota­
spine with the patient prone, but there were no signs of
tion against resistance, using the thigh as a lever.
segmental movement restriction (blockage) in the I.umbar
spmc.
During the tirst months
deteriorated. standing
condition
imel
1(,:1singly
only
difficult. and lumbar tr,UIOII
comfortable position w;", I
c\amin-
ation there was hypertrophIC
spine and a narrow spined
of silcroiliflC
b1ockflge. which in our
experience, ho�cvcr
The clinical
back pain freqllcnrh
cases of failed
is most important
At CT a massive prolap"
The patient was
According to Greenman, this manoeuvre is carried
out on the side
hOSI'1
complete recovery with I
eXercise,
at first only in the rccumbent postltOn.
P ioUl
The patient S.
1\hrch 2nd
..
complained about
1.1\\
1994,
rlll.klting into the
grom and thigh on both sides. There was intense pain on
from low-back pain
j 7, after a fall on her buttocks. Her periods
were irregular [rom the menarche on, and during her first
delivery in 1966 birth pains were felt in her low back. A
coughing or sneezing, She had suffered
Severe pain on jolting, turning over in bed,
coughing and sneezing and especially on springing
without segmental blockage were typical for lum­
bago with some pseudoradicular pain, caused by disc
prolapse in a narrow spinal canal.
since the age of
second
delivery
miscarriage. In
was
was
before
term
1969 pain radiated
and
year and she was
Pelvic distortion (sec
improved until
this
19
in the fell of
1971.
She was
into the left
1991. This time she
her condition is
condition is always
e corre-
highly characteristic
sponds to the lesion,
must be
distortion
treated. If treatment
subsides spontaneously,
a
one
leg: for this pain
Even if the case is
lar, however, it is
had
first operated for disc herniation in the spring of 1970.
pain recurred Within a
After operation she felt well, but
Figures 3.12, 3.13, p.
she
into her left leg and she
particu-
hint that there IS a leSIOn
craniocervical junction
that
requires
III
the
treatment.
invalid since
1983.
in early December
with nallsea and
At examination
the right. her
any trunk
trunk deviating to
mobillty. There was
marked tenderness at the groin.
Straight leg raising was greatly restricted. Dorsiflexion of
Adolescent girls with pelvic distortion frequently
the left big toe was weak. There was blockage at
suffer from algomenorrhoea. This may be related to
sacroiliac joint.
iliac spasm which is most frequently due to con­
comitent lumbosacral movement restriction.
the right
A tender point was found laterally at her
buttocks, and on pressure at the sacroiliac ligament. The
coccyx. too, was tender on palpation.
Therapy: first pressure was applied to tbe sacrotuherous
ligament (m. coccygeus) after which the coccyx was no
Innominate shear dysfunction (Greenman)
longer tender. The sacroiliac joint was also mobilized. This.
Greenman (1 986) descnh:d
change of the pelvis
witb hypotonus of I
plhll:ional
however, gave little relief Outfbrr of the anterior spina
II
shear dysfunction'. and
then noted. Reposition
There can be a shill
carried oul.
After
principal finding is, however
symptoms had
riar superior iliac spines
(troin and leg.
to be flatter and more
point in the
is more prominent
muscular tone on the Side
the same side,
and inflare with
of
the more prominent
spina and hypotonus on the opposite side is the rule
ill the lower abdomen.
For treatment very simple reposition manoeuvres
3re used: using the patient's thigh as a lever, the
The coccyx
was also tender. Pressure at the sacrotuberous ligament
was therefore repeated and the gluteals were relaxed. She
was re-examined on March 23rd. She had deteriorated
again after i\'larch 18th, with pain in her legs and groin on
both sides. Her pelvis was shifted to the
Copyrighted Material
side and again
25S
A1anipli/alive Therapy in
there
Re/wiJilillllio/l of Ihe LocomOlOr SY.INIJ/
was innominate shear dysfunction.
repeated after which
hospital.
she
stood
straight
was
leave the
Reposition
and could
I n n o m i n ate s he a r d ys fu n c t i o n pr o v e d to be the
most relev a n t les i o n i n this p ati ent .
l i t t l e or no abdominal respiration. Attachment points
of the straight abdominal muscles
are
tender at
palpation in particular at the symphysis. At the same
time there is h y p er t o ll u s of the gluteal muscles, at
least on Olle side, and Oil that side th e re is increased
r e s i st a n c e a ga i n s t c r a n ial s h i ft of the gluteal muscles
(a
pathological barrier ) . On thc sidc of hypcrtollus
the ischial tuberosity appears to be lower. There is
Dysfunction of the abdominal and gluteal
muscles with a forward-drawn position and
an apparent shift o n the symphysis, too, at pa l p a t i o n .
Forward-clrawn position (owing to te ns ion in the
symphyseal shift
a bcl o m i na l muscles ) necessarily causes tension in the
There is yet a n ot h e r (apparent) shift a t t h e pu b i c
whole of the back and dorsal neck musculature.
symphysis a n d the isc h i a l tuberosity (see Chapter 4 ,
o n o n e side ) ; t h e abdomen is drawn in and there is
An elegant diagnostic test follows from this: if we
find forward-clrawn posi t ion with i n cr e a s e cl tension
in t he back ancl neck muscles when the pillient loo k s
at an obj ect at eye level, we seat the patient. If
tension i n the back and neck m us c l e s then dis­
appears, we can conclude that ten s i o n even at the
neck has its origin in the pelvic girdle.
(a)
(b)
pp.
98-99)
w h ich goes hand i n h a nd w i t h muscular
spasm: i n coordi n a t i o n of the glu te a l a n d abd ominal
musculature
pos i t i o n
and
a
( Figure 7.2).
c h a racte risti c
forward-drawn
TrPs are found re gu l a r l y in the
straight a b dom i na l m usc l es whic h are t e n s e
Figure 7.2 Typical
forward-drawn position
( at
least
of the entire
body including the head
pressure on the gluteal muscles
Copyrighted Material
(a) before and (I))
after treatment by
Copyrighted Material
Copyrighted Material
Clinical nspecis
region, T h e rapy mllst be
its very favour able efkcl
pos it i o n (se e Figure 6, I
For
relief
type
o f pain d escribed h y Maign e ( 1 964) as dorsalgie
inicrscaj!ulllire in which the spinolls processes of T5
or T6 are very te n d e r on palpation and i n which
nndtl1gs In the thoracic re g i o n are otherwise
n egative: the prima r y lesion i s, accord i ng to Maign e ,
i n t h e lower cervical spine,
Pain of this locali?cltion can be due t o a thoracic
TrP causIIlg the S re flex which is related to a TrP
in the m, coccygeus, [t can also be caus e d by trigger
mid thoracic
points in t he erector
region, and it is h ere [11,,[
However, on examinat
rolling it under our
anee can be felt in th;ll
upper I umbar re gion
restriction of trunk roLdlOIl
d y sfu n ction )
There are, of course llUiHCiOUS ullier rnuscIcs w i th
trigger points causing pain in the thoracic regi o n ,
i n particulcrr the pectoralis mcrjor and min or, the
serratus and the Icrtissimus d orsi ( see Chapter 6), It
is p arti c ularl y i mp orta n t to poi n t out the su b s capu­
laris, whi ch is a very frequent source of pain in the
upper part of the t hor a x o n either s i d e, because it is
so hidden that it causes no local but o n ly referred
pam, so that i t IS ad visabl e to examine it routi nely
in cases of thorac i c
Clilse, It
may even cause movellle nl
o n ly
Blockage in the thOl:lcic
the interverte bral
the
joints between the
the same typ e of pain,
acute, pain m ay be WOl
this is, of cour s e , more
where it is uselul to know
111 or
ou t causcs the gre a test pain, The imp ort a nce
exact
d iffere ntial d iagnosis as against ple urisy is obvious,
Both for d iag n osis and for therapy the t e chniques
described in Chapters 4 and 6, respective ly, are
essential and n eed n ot be re pecrted here.
M uscle s pasm of the ere ctor s pincre i s freque n tly
founcl in the thoraci c spine even without blockage
or crfter hlockage has been treated, and in such cas e s
P IR of the thoracic ercc:tol
rewarding
(see Figures 6,112-6,1 i i).
Just as th ere is acute
there can be (though
of pain in the thorax
segme nt or, more
can be eve n more
neck, because the pat
respircrtio n. As mere
:11 [Ilc;
pain ful. first aid is more likely to be local
anaesthesia, which IS n ot difficult as the trans­
versocostal joint is easy to reach, Eve n here there i s
the danger o f diagn ostic error: a similar crcut e pain
'
'-
,
,
,
,
of disfllrbed
oj'
Sl'stem
26 1
at r e sp i r a t io n
can
pneumonia
before the typica I
More rcrrely
in tense pain
which they localtze below th e I r ribs (upper abdo­
m e n), Pain is us ucrlly provoked by deep rcspiration
crnd forceful move men t of the upper ext r emit y on
the painful side, These patients have usually
u n d ergone man y visceral exam i n at i ons which are all
ncgative, In these p a tien ts we d i agnose the syn dro m e
o f the sl i p ped rib', described (amon g o thers) by
Cyriax, The rib a t fa ult is usually the tenth, Once we
think of t h i s possibility the d iagn osis is easy: we
our fingers
stand b e hind the
abdominal
round the last rib,
the fingers
cavity a n d e xert
the patie n t
crgai n st our thenar
experie nces sharp
I n a fres h ccrse
mobilize the r i b
pain, If that
with our hooked
d oes n ot bring
diagnos t ic) to
treat the rib by local anacslllcsia at its in ner margin,
If reJicf by t he s e conservative measur e s is not per­
manent and pilin keeps recurring, surgical removal
of the rib is ind i cated ,
Fincrlly, a s men t i oned above, restrict e d trunk
rotatio n , widely believed t o be due to thorac olumbar
d y sfun c t i on, is o n e of t he most frequen t causes of
low-hack pain, and can also cause in terscapular pain
because of spasm of the erector spinae, It is also a
of psoas
frequent cause of
u nctio n of
spasm, and of pam
in the
the last two r i b s
quadra tus lumbpi
exceptional for
at its own site, Palll
secondary to a
but more frequGl tly
muscles,
'
Neck pain
Unlike low-back pain, n e ck pain is clinically simpler,
although t he 'cervical syndrome' is even more
compJex than the clinical pictures of lesions of the
lumbar s pine and pelvis,
Here, too, wc can d istin guish between pain cause d
or due t o
o n ly b y overstrain (either
by faulty
muscular imbaI:HlC<')
s ta t ics, The comrnonrst
overstrain of
the neck is caused
head bent
to faulty statics
F i g ure 3,36, p,
i n the region of !
Chapter 4 (p. 1
described in
Sym ptoms
First d iscomfort and then pain caused by overstrain
usually after workin g i n a sitting position, Another
Copyrighted Material
262
/V/allipllimivc
complaint
buses, tractOis
asymmetrical
and/or ahoulder'
j{,:hu/J!iilatiOI1 of Ihe Locomolor SYS!{l1l
The most frequent cause
C213, in exceptio nal cases
, important to realize that
by jolting in
Pain is usually
towards the head
usually illvolved. most frequently
another
C'l/6 the cervicothoracic ju n ct i o n or sometimes the
occiput/atlas. These segments rcquire treatment, but
arc better diagnosed after treatmcnt or C213. because
acute pain and spasm make di a gnos is difficult. The
typical pain point is the lateral aspect of the spin ous
process of C2 on the convex sid e. A p a i n point
between the upper medial edge or the sGlpula and
the spinous processes to which the middle part of
th e
2!t2chcs should be l o oked for: tlus IS
by a cervicobrachial
or
,
Clinical signs
Signs typical of muscular imbalance (if present);
faulty posture which must be examined in a relaxed
sitting position without a support, and standing.
Fault y breathing by lifting the thorax should nol b e
overloo ked. The mos t typical periosteal pain points
are the lilteral edge of the spinous process of C2
(more
on the right) ;md the upper edge
of the
Important muscular
I rapezius, the levator
trigger points
scapulae and t
( Any spi nous,
articular o r I
l1Iay, of course, be
tend er on
cases restricted
mobility 01
impor tant
Therap y
First. reversible changes in function (TrPs, segmental
movement restrictions and soft tissue lesio ns) are
t reated. The patients have to avoid head anteflexion;
remedial exercise must include correction of faulty
posture and breathing patterns. A supporting c ollar
is useful in jolting vehicles ( see Figurc 6.150). PIR
of muscles with trigger points and painful insertions
is effective. ft is important to provide correct back
support when
h.151). Whenever
articular dysfunction is
movemen t
manipulation.
found , this
It must
the cause of neck
pain can b e
region. In that case
treatment
und erlying cause.
Acute wry neck.
One of the most frequent causes of neck pain is, of
c ourse, blockage of mobile segments o f the cervical
spine; this has t o be diagnosed by the methods give n
in Chapter 4. Blockage w i th severe muscular spasm
is also the mos t freque n t cause of what is cailed
acute wry neck.
,
Therap y
The
[rilction with the p atien t
6.51. p. 189), which
and at the same time
should the n t re a t the
fr e es
o ther segme n ts which are usually involve d. Residual
muscle spasm, most frequently III the trapezius. is
trcated by PIR.
There is a possible diagn ostic pitrilll in relilpsing
acute wry neck - the i nitial stage or a spasmodic
torticollis. In such cases, although pain hecomes less
at e ach relapse, rotation and inclin8tion o[ the bead
become w orse and we see the lypical spasm of the
stern,xleidom3stoid on o n e sicle ancl tbe sple nius o n
the
be co mcs less and
Ir
ng concerns m eninge a l
use acute pa in in t b e
'nation. however. there
rciiL\ion (meningeal signs)
h loc kage
III which blockage is not
acute
rorms of the cervical
syn d rome, as described later in this c ha p t er. It is
unusual if neck pain is not combllle d with pain in
the regio n of the shoulder. i.e. clermatome C4. 10
which pain radiates from about as many slructures
as in the low-back region. In adclitio n 10 the large
C4 d ermatome, there is a characteristiC hyperalgesic
zone in blockage of the craniocervical junction
below and posterior to the mastoid process.
.
S y m pt o m s
Th e condit
b e d with
times aftel
again after
complains
side of the
In:qlhntly after rest in
position, some­
windo w open, or
neck: the patient
usually only on one
towards one
Clinical signs
other pain
motor function
extremities
of what I have a lrea cly
p ai n in Chapter 2 (p. 31).
of block8ge of lumbar
mobile segme nts. the segmen t of r a d i a tin g i.e.
pseud oradicular, pain was includ ed. C l inic al experi­
ence shows that, as in true radicular syndromes.
we e n counter pseudoradicular syndromes only in
.
Not only is the head held very stiffly, it is usually
also rotated and i nclined. Rotation and bending t o
the opposite side i s most res tricted, b u t anteflexio n
Copyrighted Material
0/
Copyrighted Material
Copyrighted Material
Clin ical
asp ects of disturbed fu nction 0/ the lo c o m o t o r syslem
265
pa i n , too, ca ll re s u l t from a ffec t i o n s of t h e h e a r t , g a l l
p a t te rn ' , w h i c h res t r i c ts p r i m a r i l y e x t e r n a l r o t a t i o n
bladder a n d the stomac h .
a n d a b d u c t i o n . Rece n t l y , howe ver, S a c hse ( 1 996)
u s i n g his t e c h n i q u e o f e x a m i n a t i o n , s h ow e d t h a t it
i s a b d u c t i o n w h i c h i s A rs t a n d m o s t re s t r i c te d . In
Pa i n or i g i nati n g i n t h e u p p e r r i b s
s e v e re c a s e s t h e re i s m u sc l e a t ro p h y i n the d e l t o i d ,
The A rs t fo u r r i bs p r o d uce p a i n ra d i a t i n g i n to t h e
t h e s u p r a - a n d i n fra s p i n a t u s m u sc l e s , a n d t h e r e c a n
s h o u l d e r . I n l e s i o n s o f t h e s e c o n d t o fo u r t h r i b ,
be s e v e re v as o m o t o r d i s t u rb a n ce i n t h e w h o l e o f t h e
s h o u l d e r- b l a d e .
u pp e r e x t re m i t y w i t h cya n o s i s , o e d e m a a n d e v e n
In l e s i o n s of t h e A r s t r i b ( s e e F i g u re 4 . 2 7 , p . 1 08 )
s h o u l d e r pa i n m a y be t h e o n l y c o m p l a i n t . A t e x a m ­
glossy s k i n o n t h e fi n gers ( , s h o u l d e r-a r m sy n d rome ' )
p a t i e n ts
a l so
fe e l
pain
in
the
a
,
fre q u e n t m a n i fe s t a t i o n o f a l god y s t r o p h y .
i n a t i o n t h e re i s u s u a l ly t e n d e rness a t t h e v e r t e b r a l
m a r g i n of t h e sca p u l a in l e s i o n s o f t h e s e c o n d to
T h e ra p y
fo u r t h r i b , a n d te n d e rn e ss of t h e ( u n d e r l y i n g ) a n g l e
i n t h e a c u te s t il ge w e h a ve to c o m b a t pai n , u s i n g t h e
o f t h e r i b i s · fo u n d o n l y a ft e r sc a p u l a a bd u c t i o n .
c l assic a n a l ge s i c s b u t a v o i d i n g n a rc o t i c s i f poss i b l e .
Te n d e rn e ss o f t h e tl rst ri b c a n b e p a l p a ted a t i ts
i t i s a l s o i m po r t a n t t o c o m b a t p a i n i n d i re c t l y , b y
attach ment
the
t re a t in g a l l c o n c o mi ta n t d i s t u r b a nces o f t h e c e rv i c a l
c l a v i c l e . H e r e , t o o , m o v e m e n t r e s t ri c t i o n i s t h e m o s t
s p i n e d own t o T h 3 a n d a n y m u s c l e s p a s m in t h e
fre q u e n t c a u s e o f p a i n a n d t h e refore t h e p ri n c i p a l
s h o u l d e r. T h e u s u a l m o b i l iza t i o n a n d m a n i p u l a t i o n
to
the
m a n u b r i um
sterni
below
t e c h n i q u e s a re u s e l e s s i n d e a l i n g w i t h t h e s h o u l d e r
obj e c t o f t h e r a py .
j o i n t i ts e l f, b u t t h e re i s o n e tech n i q u e t h a t m a y g i v e
re l i e f a t a n y s t a g e o f t h e d i s e a s e - traction u s i n g P I R
T h e sc a p u l o h u m er a l j o i nt
( see F i g u r e 6 . 1 0 , p . 1 66 ) , T h e m o s t spe c i fi c t r e a t ­
T h e c l i n i c a l p i c t u r e of i n v o l v e m e n t o f t h i s j o i n t
m e n t , w h i c h s h o u l d a l w a ys b e g i v e n a t r i a l , i s g r a v i t y ­
h a s b e e n d e s c r i b e d i n c l a s s i c t e r m s b y Cy r i a x ( 1 97 7 ) .
i n d uced P I R o r i n A l t r a t i o n o f t h e s u bsca p u l a r i s , T h i s
I t corresponds t o t h e ' frozen s h o u l d e r ' w h i c h is
i s i n d i c a t e d w h e n e v e r we d i agnose a trigger poi n t i n
u n i q u e in a r t h ro l ogy b e u l U s e it is ca u se d by c o n ­
t h i s m u sc l e (see C h a p t e r 6 , Fi g u re 6 . 1
t r a c t u r e o f t h e j o i n t capsule ( D e Seze , 1 960, 1 96 1 ;
s h o u l d be t r i e d ( o r s ub s t a nces w i t h s i m i l a r e ffe c t .
C y r i a x , 1 97 7 ) .
s u c h a s tri a mc i n o l o n e ) a s a n i n t r a - a r t i c u l a r i nj ec t i o n ,
I 1 a) .
Cort i s o n e
b u t s h o u l d be re p e a ted o n l y a fe w t i m e s a n d o n l y i f
i t a l l e v i a te s t h e p a i n . I t i s a d v i s a b l e fo r t h e p a ti e n t
S y m pt o m s
In p a t i e n ts o f 4 5 -6 5 yea rs of a ge , m o re u s u a l l y
t o w e a r h e r a r m i n a s l i n g d u r i n g t h e a c u te s t a g e a n d
wo m e n , pa i n
t o perfo r m o n l y i s o m e t r i c e x e r c i s e s . M o re a c t i v e
o f s e v e re i n te n s i t y s e t s i n ,
fe l t i n
t h e s h o u l d e r , ra d i a t i n g d o w n t h e a r m e v e n t o t h e
e x e rc i s e c a n be u nd e r t a k e n i n t h e s e c o n d s t a ge ,
wri s t . a n d b e i n g w o r s t a t n i g h t ( i n bed ) , o r w h e n t h e
a rm h a n gs d ow n , c a r r y i n g a w e i g h t , or on m o v i n g
w h e n p a i n h a s s u bs i d e d , b u t i t s ho u l d n e v e r b e s u c h
a s t o p r o v o k e t h e p a i n a ga i n .
t h e s h o u l d e r. A t A rs t t h e re i s o n l y s l i g h t res t r i c t i o n
o f m o v e m e n t , b u t i n t h e c o u rse o f a fe w w e e k s
t h i s d e t e r i o r a t e s . I t is poss i b l e t o d i s t i n g u i s h t h re e
stages
(as
Cyri a x
p o i n ts
out),
each
Pa i n p r o v o k e d b y a r m a b d u ct i o n
l a s t i n g 3-4
Pa i n d u r i ng a b d uction o f t h e a r m i s m o r e c o m m o n
m o n t h s : d u r i n g t h e fir s t s t a ge p a i n i s i n te n s e a n d
t h a n t h e c a p s u l a r p a t te r n . I t is ca u s e d b y d i s t ur b a n ce
t h e s y m p t o m s e x a ce r b a te ; d u r i n g t h e s e c o n d s t a ge
of t h e m e c h a n i s m by w h i c h t he h e a d of t h e h u m e r us
p a i n s u b s i d e s a l t h o u g h m ov e m e n t is s t i l l res t r i c t e d ;
s l i ps t h ro u g h u n d e r the
and
d u r i n g a b d u c t i o n . T h i s m o v e m e n t i s l u b r ica t e d by
during the
t h i rd
' thaws', so t h a t
in
stage
about
the
I
frozen
year the
shoulder
pa t i e n t
is
c o r a c o h u m e ra l
l i ga m e n t
t h e b u r s a s u b d e l t o a c ro m i a l i s , a n d i f the m ec h a n is m
s y m p t o m - fre e .
i s i m p a i red X - r a y s o m e t i m es reve a l s c a l c i fi ca t i o n s .
C l i n i ca l s i g n s
t h e ro t a t o r c u f f ( , i m p i n ge m e n t s y n d r o m e ' ) .
I t c a n a l so be c a u se d by i m p i n ge m e n t o f t i s s u e s o f
A t e x a m i n a t i o n w e fi n d t h e t y p ical c a ps u l a r p a t te r n
( Cy r i a x , 1 97 7 , sec Fi gure 4 . 3 9 , p , 1 1 6 ; S a c h s e , 1 996,
S y m pt o m s
Figure 4 . 6 1 ) . I t i s worth n o t i n g t h a t j o i n t p l a y ( s e e
T h e re m a y b e p a i n p r o v o k e d b y il b d u c t i o n o f t h e
Figure 4 .40, p .
a r m , o r e v e n m e r e l y m o v e m e n t res t r i ct i o n , o r t h e re
1 1 6)
re m a i n s u n a ffe c t e d a s l o n g a s
a b d u c t i o n o f t h e a r m i s poss i b l e to a b o u t 9 0 d e g r e e s ,
m a y e v e n be s e v e re s po n t a n e o u s pa i n . Two t y p e s o f
w h i c h i s fu r t h e r p r o o f t h a t i t i s o n l y t h e c a ps u l e t h a t
i m p a i re d m o ve m e n t m a y b e p r e se n t :
restricts m o b i l i t y . The t y p i c a l pa i n p o i n t i s a t t h e
a ttach m e n t o f t h e d e l t o i d m uscle t e n d o n a n d t h e
1 . T h e p a t i e nt a b d u c t s t h e a r m t o t h e p o i n t a t w h i c h
s u bsc a p u l a r i s m u s c l e . T h i s m u s c l e m i g h t be c a l l e d
t h e ' m uscle o f t h e froze n s h o u l d e r ' , a n d s p a s m h e re
t h e h u m e r a l h e a d beco m e s e n gaged u n d e r t h e
l iga m e n t a n d a t t h i s p o i n t t h e p a t i e n t fee l s p a i n ,
is p a r t i c u l a r l y i m po r t a n t i n t h e e a r l y stages of t h i s
b u t o n c e h e ove rco m e s t h i s ' o b s t ac l e ' , a b d u c t i o n
synd rome
m a y co n t i n u e to 1 80 d e g r e e s w i t h o u t s y m p t o m s .
-
it
is
respon s i b l e
for
t he
' c a ps u l a r
Copyrighted Material
Copyrighted Material
Clin ical aspeCis
re m e m b e r t h a t t h e
c o n ci i ti o n
fa i l u re i n
treatme n t is d u e to
pil t i e n t' s
h a b i ts ra t h e r t h a n to i n e f fe c t i v e m e t h o d s of
t re a t m c n t . Fi m l i l y , i f t h e re a re s o ft t i s s u e c h a nges,
soft t issue m a n i pu l a t i o n i s i n d i c a t e d ( s e e Figu re
0 . 7 0 ) . Restri ctio n is u s u a l l y fou n d w h e n m o v i n g t h e
soft tissues a ga i n s t the u n d e r l y i n g b o n e at the e l bow
and com p a r i ng t h e two s i d e s . S tro k i ng ( e x te ro ­
c e p t i v e s t i m u l a ti o n ) c a n b e v e ry e ffec t i v e e v e n i n
severe cases.
i s a cramped w a y o f
of disturbed
t h ese a re t h e
t h o ra c i c - o u t l e t
Iyslem
and
267
the
The carpal-tun nel syndrome
T h i s c o n d i t i o n is a ttrib u ted t o c o m p ressi o n o f t h e
m e d i a n n e rve i n the t u n n e l for m e d b y t h e c a r p a l
b o n e s and crossed by t h e l ig a m e n t u m c a r p i t r a n s ­
v e rs u m , compress i o n fi rs t a ffec t i n g t h e vesse l s
s u p p l y i n g t h e n e rv e .
S y m pto m s
Medial epicondylar
Sy m pt o m s
Pain at the medial
C l inical signs
Te n s i o n i n t h e fl e x o rs
a nd
i m p a i re d s p r i n g i n g 0 1
d i re c t i o n . Li ft i n g w i t h t h e a r m I n s u p i n a tion i s
pa i n ful (gol fe r 's e l bo w ) .
The p a t ie n t c o m
even pain, in
waking u p i n the
h i m up in the n ight
stage p i n s
and needles and
the day,
pa rticu l a rl y o n 1
I. S o b t a i n e d
when the arms
the hands
fe l t a t t h e
i m proves t h e b l o o d
w r i s t a n d m a y rad i a t e u p t h e a r m . S t ra i n o n t h e
h a n d s exace r b a te s t h e s y m p t o m s .
C l inical signs
Th e rapy
R e l a x a t i o n 0 1 t h e finger and h a n d flexors, m a n i p u ­
l a t i o n o f t h e e l bo w i n a m ed i a l d i re c ti o n , s o ft t i s s u e
tec h n i q ues. a n d i C n ecessa ry, loca l a n aest hes i a . Usc
o f cort i s o n e s h o u l d he the e x ce p t i o n . S t ro k i ng the
skin can be ve ry e ffec t i v e .
Pain at t h e w rist
The st ructure most frell I
is
t h e s t y l o i d process 0 1 t h e
cl ose l y l i n ke d w i t h l a tc LI i
spri n g i n g o f t h e e l bow
pp. 1 64- 1 65 ) . A n o t h e r
r a i n fu l ( w i t h o r w i t h o u t a r t h ro S I S ) I S t h e fi r s t
c a rpometaca r p a l j o i n t . I n b o t h t h e s e c o n d i t i o n s t h e
symptoms a r e l oca l , gen e ra ll y ge t t i n g w o rs e w i t h
stra i n . T h e m o s t s i gn i fic a n t s i g n i n a pa i n fu l s t y l o i d
process, b e s i d e s l oc a l te n d e rness, i s restricted rad i a l
A e x i o n o f t he h a n d . T h e rapy s h o u l d be m a i n l y
d i rected to t h e u IlCl e r l y i n g d i s t u r b a n c e of fu n c t i o n
a t t h e e l bo w c a u s i n g i m p a i r m e n t o f pro n a ti o n ­
s u p i n a t i o n w h i c h a re esse n t i a l fo r rad i a l ( a n d a ls o
11 I I
De
u l n ar) fl e x i o n ( s e e
Q u e rva i n 's t e n d o v a g llll l
co n d i t i o n . Joi n t m o b i l
see
for l e s i o n o f t h e fi rsl
Fig ure 6.2 ( p . 162) .
I n rare cases there
o n e ca use be i n g b l oc k age
t r i q u e tr u m . This ca n
t h e i n i t i a l s tages w e h ave t o provoke t h e
s y m p t o m s f o r e x a m i n a t i o n ; t h e s i m p l e s t m e t h od i s
r a i s i ng t h e a rms whil e t h e p a t i e n t is s u p i n e . Press u re
o n t h e m e d i a n n e r v e a bo v e the w r i s t m a y e l ic i t a
s h a r p t i n g l i n g p a i n (Ti n e l 's s ig n). I n t h e m o re
a d v a n c e d stage I h e re
1 0 the a re a
w e a k ness w i t h
s u p p l ie d by t h e
rnusc l e m ust
a t ro p h y o f t h e
stage of
a l wa y s be teste cl .
t h e d isease d o w e
O n e o f t he
m o s t s i gn i fic a n t
j o i n t p l a y between
1 64 ) .
In
T h e ra py
I f j o i n t p l a y is i m p a i red i t m u s t fi rs t b e restored by
m o b i l i z a t i o n ( s e e Figu res 6.5 and 6.6, p . 164) and t h e
pa t i e n t m us t be t a u ght s e l f- m o b il i za t i o n ( s e e Figure
6 . 7 1 ) . T n t h e few cases in w h i c h j o i n t p la y i s not
i m p a i re d , o r if m o b il i z a t i o n b r i n gs n o re l i e f, l oc a l
a n aest h e t i c s h o u l d b e a pp l i e d i n t h e c a rp a l t u n n e l .
I f t h e re i s t i g h t ness o f t h e ligame n t u m t ra n sver s u m
this should be
i o n a ] cases
s h o u l d local a p p l i c a t i o n o f
a t t e m pted.
In t h e a d v a nced
atrophy and
typical EMG
c h a n ges
, o pe r a t i o n
h i n d e r the s u ccess
is ind icated.
The thoracic-outlet
( ,scalenus
syndrome ')
Entrapm en t syn d r o m es
The re a re two i m po r t a n t a ffect i o n s i n t h e u p p e r
e x t re m i ty t h a t a re q u i t e oft e n fou n d i n combi n a ti o n :
T h i s is a tt r i b u te d t o c o m p re ss i o n of t h e b r ac h i a l
p l e x u s m a i n l y a t t h e g a p b e t w e e n t h e a n terio r a n d
m i d d l e sca l e n u s a n d i t s a t ta ch m e n t a t t h e first ( o r
Copyrighted Material
26R
Man ip ulalive Th erap v
in Rehabililmion of the Locomotor System
cerv ical) r i b , a l so between t h e clavic le a nd t h e fi rs t
r i b , c a u s i n g n u m bness a n d t i n g l i n g p a i n i n the upper
extremity, t h i s b e i n g most i n te n s e i n the h a nds a n d
fi ngers. T h u s , i t i s not u n l i ke t h e carpal- t u n nel
syn d rome. I n fa ct, at the time the s y n d rome was
d i s tinguished, many cases a t prese n t d i agnosed as
carpa l - t u n n e l syn dromes w e re a t t r i b u t e d to t h e
sca l e n u s s y n d r o m e .
The thoracic-o utlet syn d rome i s a p p a re n t ly t h e
res u l t o f a com p l e x o f lesions i n s tr u c t u re s form i n g
t h e t h o racic o u t l e t , e a c h req u i r i n g separate d i agnosis
a n d p ro d u ci n g its speci fic sy m p to m s . T h ese a r e
i n creased tension of t h e sca l e n u s (see Figure 6 . 94 ) ;
i n creased t e n s i o n of the o t h e r u pper fi x a t ors o f t h e
shou l d e r g i r d l e a n d the pectora l i s m inor; move m e n t
restriction i n t h e lowe r cervica l a n d u p p e r thoracic
s pi n e ; and m o ve m e n t restriction o f t h e u p per ribs,
i n partic u l a r o f the fi rs t r i b . It i s n o w o n d e r, i n view
o f this complexity, t h a t doctors u n fa m i l i a r with t h e
d i agnosis of these d i s t u r b a nces o f fu nct i o n i n d i cated
o p e ra tion instead o f conservative t r e a t m e n t o f t h e
u n d e rl y i n g cause o f the con d it i o n . T h i s s y n d ro m e
w a rra nts ope r a t i o n o n l y i n exce p tiona l cases w here
m a r k e d n e u ro l ogical s i g n s are present a n d m y e l o­
p a t h y can be e x c l u d e d .
Sym ptoms
P r i n c i p a l l y dysaesth esi a - i . e . n u m b ness a n d p i n s a n d
n e e d l e s - w i t h pa i n i n t h e u p pe r extre m i t y , m o re o n
t h e u l n a r aspect, i n c l u d i ng the h a n d s , w h i c h gets
worse w h e n heavy ca rry i n g has to be done. The
s y m ptoms v a ry acco r d i n g to w h i c h structure (l esion)
plays t h e p r i n c i p a l ro l e .
C l i n i c a l signs
The fo l l ow i n g tests a re useful: Adson's m a n o e u v r e ,
i . c . weake n i ng (d i s a p p e a r i ng) p u l se a t the rad i a l
artery on be n d i ng t h e h e a d b a c k a n d t u r n i ng i t t o
t h e s a m e s i d e ; raising t h e a b d ucted a r m be n t a t the
e l bow a n d obse rving the rad i a l pulse; or p u l l i n g the
a r m down ( a s i f ca rryi ng a heavy case) a n d obse rv i n g
t h e p u l s e . A J I these tests show concom i t a n t com pres­
s i on of the s u b c l a v i a n artery. More i m porta nt, h ow­
ever, i s d i agnosis of d is t urbance of the struct ures
form i n g t h e t h o racic outlet. I n view o f the ro le of
t he sca l e n i a n d the upper fi x a tors o f t h e s h o u lder­
blade i t is obvious that d i s t u rba nce o f b re a t h i n g by
l i fti n g the t h orax i s fre q u e n t l y decisive. O n l y in
exce ptio n a l cases a re true n e u rologica l signs fou n d
( a t ro p h y o f m uscles o f the h a n d ) ; ce rvical myelo­
p a t h y m us t then be ruled o u t .
Therapy d e p e n d s on the a n a lysis o f c l i n i ca l find­
i n gs a n d their re l e v a n c e , a n d i s l ess a tec h n i c a l
q uest i o n t h a n one o f p a t hoge n i c c o n s i d e r a t i o n s .
Combined lesions
A s w i t h l o w - b a c k p a i n , pa i n i n t h e u p p e r e x t re m i t ies
is usua l l y a tt r i b u t a b l e n o t to one speci fic l es i o n but
to a co m b i n a t i on of severa l . As we have seen in the
thoracic-o u t l e t syndrome, w h i c h is d u e to a com p l e x
o f i n t e rco n n ected lesions, a l l t h e s y n d romes
affecting t h e u p per e x trem i t ies form c h a i n s , as
described i n Ta b l e 4.3 ( p p . 1 42- 1 43 ) . A key role i s
t h a t of m u scular i m b a l a nce a t t h e s h o u l d e r girdle,
prod u c i n g tension o f t h e u p pe r fi x a tors, a n d o f fa u l t y
respiration w i t h l i fti n g of t h e t h o ra x a n d i ncreased
tension in t h e sca l en e s . T h i s i ncreased tension is
tra n s m i tted to t h e m uscles of the uppe r arm and
fore a r m and i n fl u ences t h e epicond y l es. Secondary
movem e n t restriction of t h e spi n a l a n d e x t re m i t y
j oi n ts s o o n fo l l ows, w h i c h i ncreases m uscle s pa s m .
We c a n t h u s s e e combi na tions not o n l y i n space, s o
t o s p e a k , b u t a lso i n t i m e : p a i n radia t i n g from t h e
neck into t h e shoulders may be fo l l owed by p a i n i n
the e p icondyles, t h e styloid process, a n d then by a
ca r p a l - t u n n e l s y n d rome fo l l owed b y dysaesthesia
d u e t o b l ock age o f the fi rs t r i b . The p r i m a ry lesion
n ee d not be in the spinal col u m n or the trunk, b u t
may eq u a l l y we l l be i n t h e l i m bs . A ffere n t stimu­
l a ti o n i s decisive a n d t h e re a re a b u n d a n t rece ptors
i n t h e peri p h e ry. A l l t h i s h a s to be considere d a n cl
weighed up in ord e r to i n d i c a te t h e prope r pl ace
and the prope r time for spec i fic trea t m e n t , n o r
s h o u l d t h e poss i b i l i t y o f v isce ra l involvem e n t or a
T r p a t t h e d i a p h ragm be fo rgo t te n .
The cervicocran ial sy n d rome
Th i s sy n d rome covers headache of ce rvica l origin a s
well as oth e r d i s t urba nces m a i n l y o f e q u i l i b r i u m ,
i n c l u d i ng m i n o r n e u rological disorders such a s
cervica l nystagm u s . The u nd e rl y i n g d i s t u rbance o f
t h e cervical spine ca n be t h e sa m e as i n s i m p l e n e c k
p a i n . I t is, o f cour s e , true t h a t the cause i s more
fre q u e n t l y a lesion in t h e u pper cerv ical s p i n e , i n
pa rticular a t t h e cervicocra n i a l j u n ction, j u s t a s t h e
lower cervical s p i n e is more l i k ely to produce p a i n
i n t h e u p per e x tre m it y , b u t t h e re a re freq u e n t
excep t i o n s . T h i s i s u n d erst a n d a b l e i f we consider t h e
m usc u l a t u re : long m u scles l i k e t h e sternocleido­
mastoid, t h e sca lenes, trapez i i , and l e v a t ores scapu­
lae, with t h e i r fr e q u e n t spasms a n d trigge r poi nts,
cover al l o f t h e cerv ica l regi o n and may react to
lesions a t any segm e n t o f t h e cervica l spine.
Appare n t l y , t h e re action of the n e rvous sys t e m
d e te r m i n es w he t h e r t h e pa t i e n t w i l l s u ffe r o n l y fro m
p a i n i n the n e c k , or i n t he s h o u l d e r or a r m , or m a i n l y
fro m headache, a l though t he s a me d i s t u rba nce o f
fu n c t i o n may u n d e r l i e t he m a l l .
Headache o f cervical origin
This is a n e x t re m e l y freq u e n t co n d i t ion a n d is in m y
o p i n i o n t h e commonest s i n g l e t y p e o f h e adache . I t
i n c l u d e s ' tension heada c h e ' w h i c h w a s t h o u g h t t o be
m a i n l y psyc ho logica l : increased m u sc l e tensi o n , as
Copyrighted Material
Clinical aspeCis
we
have
see n ,
is d u e t o
cl a s s i c d e s c r i p t i o n
m a n y fa ctors, a n d
( W o l ff , 1 948) i nc r e a se d
in
i ts
t e n s io n of
the neck m u s c l e s is part o f the c l i n ical picture of
t e n sio n h e a d a c h e . I n crea sed m us c l e te n s i o n is the
c o n seq u e n c e of practica l l y a I I d is t u r b a n ces of t h e
c e r v i c a l s p i n e , from exoge n ic ove rstra i n , fa u l.t y
pos t u re a n d m uscu l a r i m b a l a nce to m ovemen t
re s t r i ct i o n t h r o u g h o u t the cervical s p i n e . There is,
of c ou r s e , a c lose r e l at i o n s h i p betwee n h e ad a c h e ,
i n c re ase d te n s i o n a n d psyc h o l ogical problems ( s ee
p . 84 ) , but t h i s does not a l te r t h e fact t h a t i n c re ase d
m u sc l e t ension is a physiological p h e n o m e n on a n d
t h a t i t sh o u l d be t re a te d b y t h e m o s t s u i t a b l e
p h y s i o l o gical methods. N o r is ' v a somotor' h e a d a c h e
i nco m pa t i b l e w i t h h e a d a c h e of c e rvic a l origi n : the
m e r e fact t h a t a d i s t u r b a n ce in t he ce rv ica l re g i o n
causes heada c h e s hows t h e p re s e n c e of a fa c t o r o f
r e fl e x o r i g i n . I f w e assume t h a t d ist urbed f u nc t i o n
p l a y s t h e role o f a nocice ptive s t i m u l us, then a
vaso m o t o r rea ction is part of t h e typical re a c t i o n ,
p a i n as a ru l e p ro vo k i ng v asoc o n st ric ti o n .
As t h i s type of h e a d a c h e is v e r y fre q u e n t , it s h o u ld
not be d ia g n ose d o n l y per excil lsion em , i . e . o n l y a fter
a n y o t h e r or i g i n has been r u l e d o u t , a s m ost
n e u ro l o g i c a l t e x t boo k s t e a c h . A d m i tted l y , se r i o u s
p a t h ology m u st be e x c l u d e d � b u t i t s h o u l d be
rem embe red t h a t h e a d a c h e of cervical origin has it s
o w n c h a racteristic fe a t ur e s , a n d as a n i m po rt a n t
c l i n ica l e n t i ty i t s h o u ld b e d i a g nosed a s suc h .
S y m pto m s
A l l t h at i s c h a ra c t e ri s ti c
f o r v e r t e b ro ge n i c disorders
83-84) is t r u e fo r head ache of ce r v i c a l
origi n . I w a n t to i n s i s t p a r t i c u l ar l y on t h e pos i t i o n
o f t h e h e a d , i . e . h e a d a c h e d u e to h e a d a n te fle xion
fo r l o n g p e rio d s at wor k , <l nd h e a d a c h e o n w a k i n g ,
due t o a n u n favourable pos i t i o n o f t h e head d u r i n g
s l e e p . A n ot h e r fe <l t ur e of g re a t impor t a n c e is asym­
me t r y , i . e . t h e f a c t t h a t h e adache o f ce rvical o r i g i n
is u s u a l ly o n e - s i d e d o r a t least more i n t e n s e on o n e
si d e th a n o n t h e o t h e r. [ t i s a l so p a rox y s m a l i n
ch a racter, i . e . t h e re a re eit h e r p a i n - free i n t e r v a ls or,
if pain does n o t e n t i re l y disa ppe a r , t h ere a re at l e ast
pa roxysms o f i n t e n se p a i n . S u m m i n g u p a l l o f t h e
fea t u res l isted i n C h a p te r 4 - i n c l u d i n g t h e r o l e o f
p s y c h o l o g i c a l , e n d o c r i n o l ogica l o r e v e n a l l e r g ic
factors - we c o m e t o t h e c o n c l u s i o n t h a t ce rvic al
(s e e
pp.
headache
has
many
migra i n e .
At this
fe a t ures
in
com m o n
with
poi n t t h e loca l i z a t i o n of c e rvic a l h e a d a ch e
T h i s d iagnosis is ce rtai n l y i n d i ­
c a t e d i f t h e p a t i e n t co m p l a i n s o f p a i n radiat i ng from
the neck i n t o t h e occi p u t and fro m t h e re towards
t h e eyes a n d t e m p les, mo re t o one s i d e t h a n t he
o t h e r . Howe v e r , t h is in i tse l f is i n s u ffic i e n t for a
d i a g no s is . I n young p a t i e nts, p a r ti cu l a rl y a d o lesce n ts
a nd chil d r e n . h e ad a c h e is freq u e n t l y t h e fi rs t si g n o f
dis t urbed cerv i ca l fu n c t i o n long be fore n eck p a i n h as
b e e n fe l t . [ n s u c h c<lses t h e p a i n m a y be localized i n
m u s t b e d i sc u sse d .
the
oj disturbed /ilnClion of the 10(,011l0tor s vslem
269
fo re h e ad o r t h e te m p o r a l
r e gi o n . E v e n p a i n
( b u t not t ypica l t r i ge m i n a l
n e u r a l g i a I ) c a n be o f cerv i c a l origi n . This i s l e ss
surpr i s i n g t h a n it m a y see m : T r a ve l l ( 1 98 1 ) s t u d i e d
referred p a i n fro m tri g ge r poin ts i n t h e ste rno­
c l e id o m a stoid : this was f re q uen t l. y l oca l ized in the
fa c e .
ra d i a t i n g i n to t h e face
C l i n i c a l s i g ns
i mporta n t a re , o f cou rse , the signs o f
disturbed cervical functio n , w h ich a re c o m m o n to
n e c k p a i n , a n d i n c l u d e sig ns o f m u scu l a r i m b a l a nce,
sp a s m , fa u l ty res p i r a t i on a n d s e gm e n t a l lesions,
p a rt i c u l a rly of t h e c r a n iocerv i c a l j u n ction . The m os t
i mpo rt a n t p a i n points a re o n the lateral s u rface o f
t h e sp i n o u s process of t h e a xis ( m o re fr e q u e n t l y o n
t h e r i g h t) , a t t b e posterior arch o f the a t l a s ( i n the
s h ort e x t e n so rs) , a t t he transverse p r oce ss of the
a t l as and in the sternocleidomasto i d . The fre q u e n t
p a i n points on t h e occi p u t i tse l f a re usu a l l y secon d a ry ,
a n d t h e re may sometim es be odd p a i n poi n ts o f
a t ypical loca l i za t i o n on t h e s k u l l . There i s a n i m port­
a n t p a i n p o i n t a t the temple i n the t e m po ra l i s m u sc le
( not to be con fused with a pa i n f u l temporal a rte ry ! ) :
o t h e r m ast ic a t o ry muscles m a y a lso ca use h e a d a c h e ,
a n d s h o u l d b e exa m i n e d fo r tri g ge r poi n ts e v e n
t h ro u g h t h e open mou t h . Even t h e p a i n p o i n t
c o r resp on d i ng to t h e notch o f t h e fi rs t d i v i s i o n of
t h e t rige mi n a l n e rve at t h e orbit can be o f cervical
or igin .
Ty pical h ype ra l g e s i c s k i n zo nes are fou n d m e d i a l l y
be low t h e m astoid p r oc es s e s , a t t h e temples a n d
e y e bro ws a n d a t t h e fore h e a d a bove t h e eyebrows
a n d o n bot h sides o f the n ose . W h a t may be ca l led
t h e ' t y p ic a l ' s o ft tissu e l e sion i s rest ricted mob i l i ty
of t h e scalp a g a i n s t t h e sk u l l . This can re a d i l y be p a l ­
p a ted a n d t h e two sides c o m p a r e d . I t i s o ft e n a v e r y
re leva n t lesion a n d i s e a s y to tre a t ( s e e Cha p ter 6 ,
p . 206 ) . I t i s fre q u e n t l y l i n k e d to s i m i l a r c h a n ges of
t he c e rv ica l fasciae.
T h e most
T h e ra py
s a m e r u l e s as for a n y o the r
cerv i c a l reg i o n . It m a y be wort h
s tress i n g t h a t h e re the si g n i fi ca n ce of m o v e m e n t
restriction at t h e cr a n i oc e rvi ca l j u nc t i o n is so gre at
t h a t it is good po l ic y to tre a t this first, as m u s c u l a r
i m b a l a n ce ca n n o t be i m p roved u n ti l t h i s obstacle h a s
b e en remove d . Move m e n t restric tion b e t w e e n atlas
a n d occi p u t m u s t b e e x am i n ed in all d i rections. I f
p a i n regu l a r l y be g i ns o n w a k i ng, we must e n q u i re
a bout t h e s l ee p i n g position of t h e pat i e n t . W hile
t r i gg e r poi n ts i n t h e m uscles a n d at peri os te a l points
o f a tta c h m e n t a re best treated by P I R , p a i n points
o n t h e s k u l l a r e b e s t t re a ted b y soft tissue tech n i q u e
o r needling. A t e n d e r te mpor a l i s m u scle ca n be
t reated by P I R (together w i t h t h e m a ss e te r ) or b y
m ere press u re or local a n aest h e t i cs. The h ypera l gesic
zones on the fo re h e a d , te mples a n d round the nos e
T h is
fol l ows
the
d i s t u r b a n ce of t h e
Copyrighted Material
270
of the
Mnnipulntive Therapy in Reh a b ilita tion
Locomotor S V.\"/elll
r es p o n d ve ry we l l to s k i n s t r e t c h i n g ( se e below ) ,
w h i le restricted m obi l i t y of t h e sca l p r e s po n d s t o s o ft
t i ss u e techniq ues.
the
tem poromand i b u l a r j o i n t
(T M J ) and m u s c u l a r
t r i gge r p o i n ts (TrP ) . I n t h e fo r m e r
we
!'i n d s i g n s o f
ma loccl u s i o n , s u c h a s m i s s i n g te e t h , a b a d l y m a t c h e d
p r o s t h e s i s a nd c r o s s b i t e . [ n m u s c u l a r d y s fu n c t i o n
occ l u s i o n is n or m a l b u t i f t h e r e i s iI history o f
b r u x i s m we m a y s e e i n creased a c t i v i t y o f t h e
m a s t icatory m u s c l e s o r d e v i a t i o n o f t h e t h y ro i d
ca r t i l age I f m u s c u l a r d y s fu n ct i o n i s t h e m a i n fact o r ,
t e n d e rn e s s a t t h e T M J w i l l s u b s i d e a f t e r m usc l e
re l a x a t i o n - t h i s i s m u c h l e s s l i k e l y i n p r i m a r y TMJ
-
,
Th e mandibulocranial s yndrome
T h a t t h i s s y n d rom e is i m p o r t a n t is c l e a r n o t o n l y
from i ts f r e q u e n t occurrence b u t b e c a u s e i t p rod uces
a l m os t the same s y m p t o m s as t h e cervi cocra n i a l
syndrome a n d is o fte n fo u n d i n c o m b i n a t i o n w i t h i t .
Th is i s true n o t o n l y fo r p a i n ( h e a d a c h e ) b u t a l s o
for d i s t u r b a n ce s of e q u i l i br i u m i n c l u d ing ve r t i go
I n d e e d , i t fo rms c h a i n reactions w i th the cervical
s p i ne a n d the cerv i ca l m u s cle s ( s e e C h a p t e r 4,
p. 143). C h a n g e s i n the orofa c i a l s y s t e m w i t h fa c i a l
a s y m me tr y a re oft e n l i n ke d w i t h s c o l i o s i s
.
l e s i o ns .
.
.
S y m pto m s
I n a d d i tion t o symptoms t y p i c a l for t h e ce r v i c o ­
c ra n i a l s y n d r o m e t h e re m a y be bruxis m , p a i n i n t h e
region of t h e e a r ( t h e tem porom a n d i b u .l a r j o i n t ) a n d
t h e face m a y be ve ry p r o m i n e n t , a s we l l as d ysphagia
due to t r i g g e r p oi n t s i n t h e d i g a s t r i c u s .
T h e r a py
Post-i s o m e t r i c re l a x a ti o n ( P I R ) o f t h e re l e v a n t
m u scles i s the t re a t m e n t o f c h o i c e , fo l l ow e d b y se l f­
tre a t m e n t ( s e e C h a p t e r 6 ) . I r t h e j oi nt i s i n v o l v e d ,
i s o m e t r i c tra c t i o n i s a u s e f u l a d d i t i o n . H o w e v e r ,
w h e re t h e re is m a l occl u s i o n , p r o s t h e t ics a n d/or
o r t h o d o n t i cs a re esse n t i a l I n m o s t cases, d i s t ur b ­
a n ce o f f u nc t i o n i n t h e o r o f a c i a l s y s t e m is bou nd u p
w i t h c h a n ge s e l s e w h e re i n t h e l oc o m o t o r s y st e m ,
p a r t i c u l a r l y i n t h e c e rv i c a l s p i n e , a n d t h e p r i m a r y
t a s k is to d is c o v e r i n a j ud icious m a n n e r t h e m o s t
re l e v a n t l i n k i n t h e c h a i n .
Cli n i cal s i g n s
There m a y b e rest ricted o p e n i ng of t h e m o u t h ( i t i s
n o r m a l l y p o s s i b le t o i n s e r t t h ree k n u c k l e s b e t w e e n
t h e upper a n d t h e lower i n c i s o rs ) . D u ring o p e n i n g
and clos i n g of t h e m o u t h t h e re m a y be d e v i a t i o n
o f the c h i n to o n e side a n d t h e re may be a " popping'
sound a t t h e j o i n t . There m a y be tenderne ss a t
the temporo m a n d i b u l a r j o i n t . T h e fo l l ow i n g t r i gge r
p o i n t s should be loo k e d fo r : a t the te m po r a I m u s c l e
a t the tem p l e , b e h i n d a n d b e low the j a w - b o n e fo r
s c r e e n i ngs; t h e masset e r a n d the i n t e rn a l p t e rygo i d
m u s c l es a r e b e t t e r p a l p a t e d t h ro u g h t h e o p e n
mouth. I t is i n t e r e s t i n g t h a t w h i l e t h e p a t i e n t i s
u s u a ll y aware of p a i n in t h e tem p l e s , trigge r p o i n ts
in the other m a s ti c a t o r y m uscles - more p a i n f u l O il
p a l p a t i on - are observed o n l y at exa m i n a t i o n .
P a l p a t i o n of t r i g g e r p o i n t s i n t h e d i g a s t ric u s
( b e h i n d t h e a n g l e of t h e m a n d i bl e a n d t h e c h i n )
is more d i ffi c u l t a n d l e s s rew a r d i n g . The s i m p l e s t
w a y to d i a g n o s e i n creased te n s i o n is to move t h e
t h yr o i d ca rti l age a n d/or the h yo i d from s i d e to s i d e .
I ncreased resistance here is c h a r a ct er i s t i c a n d e a s i l y
a ssesse d . There is a l so t e n d e rness a t t h e l a te r a l e d g e
o f the hyoid on t h e s i d e of i n c r e a s e d ten s i o n . W i t h
m a r k e d i n cre a s e o f t e ns i o n o f t h e d i ga s t ri c m u s c l e
o n o n e side, the t h y r o i d cart i l age can b e see n t o
,
T . L . ( l lJ4 7 ) , h rs t s e e n 2 6 N ov e m b e r I lJt: 7 . co m p l a i ned
of
of
righ t : t h e re I-I d S v o m i t i n g fo r 2 d a y s .
S u b s e q u e n t l y , o n l y sho r t ,-, t t a c k s o r d i zzi n ess o c c u r r e u
w h e n s i d e - b e nd i n g t h e n e c k or b e n d i n g fo r w a r d : t h i s l a s t e d
ro r d b o u t a m o n t h . La t e r t h e r e was h e a d a c h e a n d p il i n i n
t h e n e c k , m a i n l y on s i d e ro t a t i o n . c"ro m I lJoS t h e r e w a s a
h is t ory or heil d a c h e at t h e o cc i p u t ra d i o t i n g t o t h e eyes
a n d l a s t i n g for s e v e r a l h o u rs , w i t h n a u s e a . N o h i s t o ry or
vert igo on wakening ( 1 7
pulling
to
August )
with
a
se n s a t i o n
the
,
d is e a s e .
At
ku on
t h e l e f t ; d e v i a t i o n a t H a u ta n t 's t e s t
w a s t o t h e left , d i s a p p e a r i n g a t h e a d ro t a t i o n to t h e l e f t
a n d a n t e fi e x i o n . E x a m i n a t i o n s h o wed o n l y i n c r e a s e d
t e n s i o n w i t h t " igge r poi n t s a t t h e m a s s e t e r o n bo t h s i d e s .
a n d a t t h e h y o i d . P l R o f t h e d i g a s t r i c w a s c a r r i ed o u t o n
bot h s i d e s , a f t e r w h i c h d e v i a t i o n a t H a u t a n t ' s l e s t
d i s a p p e a re d . At c o n t rol e x a m i n a t i o n o n I II De c e m b e r
t h e re were no s y m p t o m s n o r d e v i <ll i o n . a l t b o u g h t h e re w a s
s t i l l a d i ffe r e n c e on t w o sca l e s .
[ 1\ t h i s c a s e t h e sym p t o m s we re prod u c e d by t h e
oro fac i a l sy s t e m .
e x a m i n a t i o n , r e a d i ngs o n t w o sca l e s we re .'1 0
t h e righ t a n d 3 5 kg o n
,
d e v i a te .
Diffe r e n t ial d iag n o s i s
To d i s t i n g u i s h t h e cerv icocra n i a l f r o m t h e m a n ­
d i b u l oc ra n i a l synd r o me t h e p h y s i ca l fi n d i n gs are
d e c i s i v e . I f the two s y n d r o m e s a re com b i n e d , t h e
i n te n s i ty o f t h e signs ( c h a nges ) in t h e c e rv i c a l reg i o n
a n d the oro faci a l system is d e c i s i v e . I t i s n o less
i m po r t a n t to d i s t i n g u i s h between a p r i m a ry l e s i o n of
,
Anteflexion headache
is o f e x ce p t i o n a l c l i n i c a l i m p o r t a n c e b e c il u s e
nowadays l a rge n u m b e rs o f peop l e w o r k s e a te d ,
w i t h t h e h e a d be n t forwa r d , H y permo b i le s u bj ec t s
w b o a re susce p t i b l e t o l iga m e n t p a i n a re p a r t i c u ­
l a rl y p ro n e t o t h i s type o f h e a d a c h e . A n o t h e r g ro u p
i s m a d e u p o f p a t i e n t s a fter i n j u ry . T h e l a rg e s t
g r o u p o f s u ffe re r s , h ow e v e r , a re schoolc h i ld re n ;
a n d ac c o r d i n g t o G u t m a n n ( 1 968) , w h ose opi nion I
s h a re , " s c h o o l he a d a c h e - o r i g i n a l l y c o n s i d e re d t o
Th i s
'
be psyc h o l og i c a l
mecha nism.
Copyrighted Material
-
is usua l l y attri b u t a b l e t o t h is
Copyrighted Material
272
Mani;nl liiliVe
Rciw!>iiitation
of' the
Locomotor
Ha u ta n t ' s test i n
f lt/quent.l y i n t h a t
restric t i o n . T h i s t y pe o f
(,hstur b a llcc 0 1 c y u i l i b r i u m , w h ich
i s fa r m o re f req u e n t than d i zzi n e s s . i s a l most
i nv a r i a b l y of cervica l origi n o r stems from d i s t u rbed
fu n c t i o n of t h e oro faci a l syst e m , b o t h s h ow i n g t h e
'cerv ic a l patte rn ' w h ich i s e x p l a i ned b e l o w , a n d
w h i c h d i sa pp e a rs a fter t reatmen t o f m o v e me n t
restric t i o n . Th ese pa t i e n t s are o f t h e type w i t h
m o ve m e n t res t riction i n t h e cran iocc rvical j u n c t i o n ,
i n w h o m N orre e/ 0 1 . ( 1 9 7 6 ) descri bed cer vica l
nystagmus.
S y m pto m s
T h e s e v a ry
v e r t i g o or
d i zziness
Classic
- Typica l
a tt a c k s l a�1
d a y s ; t h e pa tien t
s uffe rs from
IS a b l e t o i nd ic a t e
or a n ticlockwise):
v e rt i go i s a cco m p a n ie d b y n a usea a n d v o m i t i n g .
u s u a l ly co u p l e d w i t h t i n n i t u s a n d d i s t u r ba n c e o f
h e a r i n g . T h e re a r e Jess severe cases, i . e . shorter,
w i t h o u t d i s t u rbed a u d itio n , a n d a roc k i n g sensation
( sea-sick ness) may ta ke t he p l ace o f t h e t y p i c a l
rot a t i o n .
A polymorpholls group of short atta cks of diz z i cert a i n h e a d pos i t i o n s a n d/or
t o t h e t ru n k , t h e p a ti e n t
move m e n ts
having the
or pulled to
one side,
a n d a pprehe n s i v e
o f fal li n g.
u s u a l l y a bsent ,
b u t headache
d e p e n d e nce o n
d i s t u r bed equ i l i br i u m is
i vert igo' or d i zz i n e s s
plit l c' n t s s u ffe r s hort
a t t a c k s o f true rota t i o n a l v e rt i go on c h a n g i ng t h e
p os i t i o n o f t h e h e a d i n space, i . e . t oge t h e r w i t h t he
re s t o f t h e b o d y , a n d n o t n ecessa r i l y c h a n g i n g the
pos i t i o n o f t h e h e a d r e l a t iv e t o t h e t r u n k . T h e s e
a ttac k s , a l though s h o r t , a re v e ry i n te n s e , a n d i f t h e
e y e s re m a i n o p e n s p o n t a n e o u s n y s ta g m u s o f very
short d ura t i o n c a n b e observed .
Se vere a ttacks of short dura/ion p ro v o k e d b y
c e r t a i n p os i t i o n s o f t h e h e a d rel a t i v e t o t h e t r u n k ,
I h e grou n d : d ro p
d u ri ng w h ich
a t tacks , ce Ivicil l
w i t h o u t l oss o f
Sysleil!
fea r o f fa l l i n g . H e
fe e l i n g t h a t t h e g ro u n d
fac e . T h i s a l s o h a p p e n e d
I I G fel t t h a t t h e c a r w a s u p ­
t h e a i r. I n 1 9:;9, l y i n g u n d e r a
c a r w i t h h i s h e a d t u r n e d to t h e r i gh t , he fe l t s h a r p p a i n a n d
d i zz i n e ss w h i c h d i s a p p e a r e d w h e n h e t u rneci h i s h e a d t o
and a
the
left.
R e pe a t i n g
s u ffe ring from
b o r d e r cas e " , I
- i . e . p a t i e n ts
l lpe of a ttack, o r
c h l l n g i n g d u ring t h e
disease.
( l90tl ) . , u rg c:o n : cOll c u s s i o n a i t c l a c a r a cc i d e n t i n
1 94K T w o d a y s l a t e r , s l i g h t d i zz i n es s w h e n b e n d i n g t h e
h e a d t o t h e ri g h t . T h r e e y e a rs l a t e r . t i n n i t u s a n d a c u t e
pa rox ysm of M e n i e r e ' s d i s ea s e . usu a l l y l a s t i ng lor 2-3 l b y s .
'exper i m e n t '
t r e a t e d by tra c t i o n . D i z z i n ess
seven
In
and
ti mes,
he
he h i mse l f
a fee l i n g o f u n c e rt a i n t y
1 960 h e s h owed a r i g h t d c v i <l l i o n w h e n
r o l a t i n g t h e h e a d t o t h e I d t . O n t u rn i n g from s u p i n e
p o s i t i o n t o l y i n g o n t h e r i g h t . t h ere w a , s po n t a n e o l l s
p e rS i s t e d .
r o t a t ; n n � 1 n v'tn.=rn u s a n t i r l nc k w i se . I n I h i s c a s e a l l fo r m s
of
o f p a i n i n t h e occip u t
11 !( ar i ng, s e n s a t i o n of d i zz i ­
F. M ,
( 1'!1'I " l i! ! n e d
when
n es s .
g a i t w i t h t h e fe e l i n g t h a t
s h e \\
T u r u i n g o v e r i n b e d p rod u ce d
n a USCr'l
date
from 1 982 . S h e
sough t
t r e a t nh.:: n L
d e l i v e r i e s . il p p c l1 d e c t ­
s t one s . A l l e r g i c t o m ost d rugs.
At examina t i o n on 4 J a n u a r y I 'JSS, the re a d i n g o n two
sca l e s w a s 40 kg o n t h e r i g h t a n d 3 7 k g on t h e l efl ;
I-la u ta n t ' s t e s t s howed d e v i a t i o n t o t h e r i g h t w h i c h w a s
aggra v a t e d o n t u r n i n g t h e h e a d t o t h e l e fl or b e n d i n g i t
b a c k w a r d s , b u t t h e r e w a s n o d e v i a t i llil w h e n t u rn i n g t h e
h e a d t o t h e r i g h t o r b e n d i ng i t fCH"\v il rd . T h e r e W il S
m o v e me n t rest r ic t i o n o f C l -2 a t r i g h t r o t ;l t i o n il n d s i d e H e r c a s e h i s t o ry i n c l ud e d n o rma l
omv
al 1 4,
gall
b e n d , ,) !,
A rk !
C 5 t il de
re ad i n g o n
C5-1i J n ci a t h r u s t ,1 1
H a u t a n t 's t es l and t h e
o n t h e righ t a n d 35 k g o n
d !l ei
t h e k ft
J a n u a r y 1 'J 8 L)
At
t here
was
wa s st i l l fe l t a t t h e
" L' � \ d i n g o n t w o sca l e s w a s 3 5
L.' ll s i o n
t h e l e fr :
sy m p t o m s i n
t he re w e r e
CC r V I GL ']!'(.. <l, b u t r es t r i c l i o n a t
no
Til 1 2- L J ,
w i t h s p a s m of t h e psoas and t h e t h o r a co l u m b a r e re c t o r
spi n a e . T h I 2-L 1 was t re a te d w i t h m o b i l i z a t i o n t o t h e left.
T h e r e w a s fur t h e r i m p ro v e m e n t b y I () Fe b r u a r y , w h e n
bloc kage a t CO-- I w a s t r e a t e d .
Th ree m on t h s l a t e r (5 A p ril ) . d i ZZ i n e s s . [l a i n a n d b l u r r e d
v i s i o n reappe a re d , t h e re w a s a d i ffe r e n ce o f Ii kg i n
re a d i ngs o n t w o sca l e s , a n d d e v i a t i o n ,1 1 H a u t a n t ' s t e s t .
T h e r e w a s b l oc k a g e a t C2-3 a n d S P il S Il1 of t h e PSOil S ; i n
a d d i t i o n . t h e re was a d i ffe re n ce i n t h e h e i g h t o f t h e
, I m d a t t h e t u b e r oss i s i sc h i i .
T h e re was n o re s t r i c t i o n
a t t he
c o n S C l O u s n c: s s ,
Mixed
this
p rov o ked a ge n u i n e M c n i c f<! a t t a c k , w h i c h
t he l e i:
( p u l l i ng
t he s l) l lu l
no side
On 27
X - r a y ( s t a n d i n g ) s h owed
of the c e r v i c a l s p i n e , to
m a n i pu l a t io n of t h e p e l v i s
t h e l e ft ( s t re tched) l e g )
i n t h e A P v i ew , w i t h
I U ' l1ba r {) r t h e c e r v i c,1 i s p i n e .
co m p l a i ne d of h e a d a c h e : t he
t w o ;,[ilks ;,I!owed d d i ffere n ce of 5 kg a n d
K. J.
re a d i ng 0 1 1
Three
I-I.a u ta nt ' s t e s t s h o w e d d e v i a t i o n o n l y w i t h t h e h e a d b e n t
back and r o t a t e d t o t h e r i g h t . T h e r e l e v a n t fi n d i n g il t t h i s
con t rol e x a m i n a t i o n w a s s p a s m o f t h e i ll l e l'llCl i p t c r ygo i d s .
t re a t ecl b y P I R .
ye a rs
l a t e r t hese ' m a j o r ' a t t a c k s c c a s e d b u t
lhe
Copyrighted Material
Clin ical
O n J J u n e the p a t i e n t co m p l a i n e d of p a i n b e t w e e n t h e
a n d o f a few d a y s o f h e a d a c h e a n d
d izzi n e s s . We fo u n el m o v e m e n t r es t r i c t i o n a t CO- I a n d
( a g a i n ) a s h i ft a t t h e s y m p h ys i s a n d t h e i sc h i a l t u b e ros i t i e s .
and d e v i a t i o n a t H a u t a n t 's t e s t . T h e s e s y m p t o m s w e re
shoulder-blades
treated.
O n 5 J u l y s h e fe l t m a i n l y l o w - b a c k pa i n w i t h m ove m e n t
L2-3 : t h is w a s t re a t e d . T h e re w e r e a l m o s t n o
sym p t om s o n 27 J u l y w h e n t h e r i g h t e x t e r n a l p t e r y go i d w a s
t rea ted fo r s p a s m . D u r i n g Fe b r u a ry J 989. h e a d a c h e a n d
d i zzi n e s s rec u rr e d . O n 1 5 M a rch there w a s d e v i a t i o n a t
H a u t a n t 's t e s t , t he hyoid was deviated t o t h e righ t , t here
w a s ag a i n s y m p h y se a l s h i ft a n d u n e ve n i sc h i a l t u b e ros i t i e s .
We r e l a x e d t h e r i g h t d i ga s t r i c ll s : i n s t e a d of ' re po s i t i o n i n g '
we a p p l i e d s o f t t i ss u e tec h n i q u e s t o t h e h u t tocks, o b ta i n i n g
restriction at
s y m m e t ry at t h e sy m p h y s i s a n d t h e i sc h i a l t u b e ro s i t i e s . T h e
pa t i e n t
re m a i n e d
m o veme n t
(late
w i t hout
sym ptoms
until
a
jerky
J u n e ) c a used s h a r p pa i n a t t h e n e c k . r i g h t
a r m a n d b e h i n d t h e r i g h t e a r , b r i n g i n g o n a rec u r r e n ce o f
a t H a u t a n t " s test o c c u r re d o n l y
o f t h e h e a d , a n d t h e re was a s h i f t a t t h e
h e r symptoms. Deviation
a t b a c k - be n d i n g
s y m p h ys i s a n d t h e i sc h i a l t u b e ro s i t i e s . Th i s w a s t r e a t e d
o o l y by p r e ss u re 0 11 t h e l e f t gl u t e u s m a x i m u s ;
t i s s u e t e c h n iq u e a l l s y m p t o m s d i s a p p e a r e d .
a ft e r t h i s soft
The p a t i e n t w a s w i t h o u t s y m p t o m s u n t i l e a r l y N o v e m b e r
1 91'9, w h e n s u s t a i n e d w o r k s t ress c a u s e d a r e c u r r e n c e . O n
29 N o v e m b e r t h e re w a s d e v i a t i o n t o t h e r i g h t a t H a u t a n t ' s
t e s t . a forw a rcl - d r a w n pos i t i o n o r t h e pe l v i s w i t h s l i g h t
s h i ft
to
the
left.
T h e re
was
m o v e me n t
restriction
at
T h S -6 a n d i n c r e a s e d t e n s i o n i n t h e righ t g l u t e u s m a x im u s ,
t h e a b d o m i n a l m u scles a n d t h e e re c t o r s p i n a e , m o re
p a r t i c u l a r l y t o t h e r i g h t . Pos t u re a n d m u s c l e t e n s i o n w e re
n o r m a l i z e d a ft e r p r e s s u re a p p l i e d to t h e r i g h t g l u te u s
m a x i m u s , a n d H a u t a n t ' s t e s t be c a m e n e ga t i v e . M o ve m e n t
re s t r i c t i o n a t
T h S-6 w a s t re a t c d b y speci fi c m a n i p U l a t i o n .
T h i s very com p l icated c a s e is i n teresti ng fo r m a n y
reasons - a l i v i ng e x peri m e n t . T h e s a m e t y p e of
h ea d a che a n d d i zz i n e s s w a s caused b o t h by move­
men t restriction a t t h e c ra n i ocervical j u nction , a n d
b y spasm o f t h e masticatory m u scles. A s lon g a s t h e
u n derlying d i s t u rbance a t the pe l v is re m a i n e d
u n t reated, w i th i ts conseq u e n t fa u l t y sta nce and s i d e
deviation , re l a pses were freq u e n t . Tr e a t m e n t b y
sp e c i fi c ' repos i t i o n ma noeuvres' g a v e t h e s a m e re s u l ts
as soft t i s s u e t e c h n i q u e s a i m e d a t t e n s i o n i n t h e
gl u t ea l m uscles, w h ic h revea led ' p a l patory i l l us i o n '
d u e t o cha nges i n t e n s i o n o f t h e so ft tissues ove r l y i n g
the b o n e . Ex a m i n a t io n a n d treatme n t o f the w h o l e
motor system i s s h o w n to b e n eces s a r y i n comp l i ­
ca t e d re l apsing c a s e s .
When q u e s t i o n i n g t h e patient, i t i s esse n t i a l to
make it q u i te c l e a r w h a t h e o r she m e a n s by
'd izziness ' , for the word is u s e d to d e s cribe the
fee l i ng or fe a r o f fa l l i n g from a h e i g h t , a n a ttack of
fa i n t i ng or w e a k n ess d u e to c i rc u l a t or y d i sord e r , or
eve n for i n toxication (cerebe l l a r d i stu r b a n ce ) a n d
ata x i a . W h e n t h e p a t i e n t com p l a i n s o f d i zzi.ness,
t he n cross-exa m i na t i o n m u s t first e l icit more explicit
i n fo r m a t i o n : d o e s t he w o r l d seem t o be t u r n i n g
c l oc k w i se o r a n t i-c l oc k w i se ro u n d h i s h e a d ? Does
he fe e l p u l led to one s i d e , o r to the ot her?
{{speers of rlislUrb�d /LI IlClion vf Ihe loco m v l O r S VSlem
273
C l i n i ca l signs
O n l y i f it is poss i bl e to e x a m i ne t h e p a t i e n t d ur i n g
a classic a t t a c k of t r u e v e r t i go c a n w e obs e rve t h e
typic a l s i g n s o f l a b y r i n t hin e disorder, s u c h a s
n y s t ag m u s to the ri g h t w i t h d e v i a t ion to t h e l e ft , a n d
d e v i a t i o n to t h e s i d e of t h e w e a k e r la b y ri n th - i . e .
d u r in g R o m b e rg's t e s t , s ta n d i n g w i t h eyes closed
with t h e h e a d i n n e u tral posi t i o n , t he re is d e v i a t i o n
to t b e s i d e ; w i t h t h e head t u rned to t h e s i d e o f t h e
w e a k e r l a byrin t h t h e t ru n k mo v es backwa rds, w h i l e
i t m o v e s fO lw a r d i f t h e h e a d i s t u r n e d to t h e oppos i t e
s i d e . I f, however, we e x a m i ne the pa t i e n t i n b e t w e e n
a t t a c k s , a n d t h e re a r e n o pathologic a l neurological
fi n d i ngs, t h e re i s l i t t l e to observe u n less we carry o u t
H a u ta n t ' s t e s t a s descr i b e d i n C h a p t e r 4 ( p. 1 1 9) .
U s i n g t h i s a s a rou ti n e e x a m i n a t i o n m e th o d a
c h a racte ristic p a ttern emerges i f t h e r e is a cervi c a l
fa ctor, rega r d l e s s o f t h e t y p e of d i s t u r bance o f
e q u i l i b r i u m . 1 n 7 2 exa m i n a tions of 69 p a t i e n t s I
fo u n d t h e m os t con s t a n t p