Cardiovascular Dysfunction: Congenital & Acquired Heart Defects
advertisement

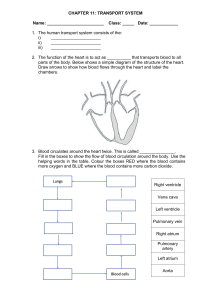
Cardiovascular Dysfunction UNIT 7 Dr. Korina Banks, DNP,MSN, RN Case study: Ryan Ryan is an 11-month old infant who was born with Down Syndrome. Ryan weighed 3.2kg (7lbs) at birth and a heart murmur was noted. Ryan was breastfed for 4 months. His mother states that at the time, he became “disinterested” in breastfeeding, only nursing 5 minutes before falling asleep. Because he was not gaining weight appropriately, his mother began feeding rice cereal twice daily. At 4 months, Ryan was diagnosed with an atrial septal defect, which has been monitored since. Ryan sits unsupported but does not stand or crawl. According to his mother, he “gets out of breath” when attempting these tasks. Since 5 month, Ryan has been taking digoxin and furosemide daily. Cardiac Defects Defects are categorized into congenital and acquired disorders Congenital Anatomic: abnormal function Acquired Infection Environmental - Autoimmune responses factors -Familial tendencies Pediatric Indicators of Cardiac Dysfunction Poor feeding Tachypnea/ tachycardia Hypoxia Failure to thrive/poor weight gain/activity intolerance Developmental delays Positive prenatal history Positive family history Diagnostic Evaluation History and Physical Examination Electrocardiogram Echocardiograph Cardiac catheterization Diagnostic catheterization Interventional catheterization Electrophysiology studies CONGENITAL HEART DISEASE Fetal Circulation Umbilical vein: During fetal life blood carrying oxygen and nutritive materials from the placenta enters the fetal system through the umbilicus via the large umbilical vein Blood then travels to the inferior vena cava through the ductus venosus Foramen ovale: shunts blood from right atrium to left atrium Ductus arteriosus: connects pulmonary artery to the proximal descending aorta. Chapter 42 Page 1226 Fig. 48-1. Changes in circulation at birth. A, Prenatal circulation. B, Postnatal circulation. Arrows indicate direction of blood flow. Although four pulmonary veins enter the LA, for simplicity this diagram shows only two. LA, Left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle. Congenital Heart Disease (CHD) Incidence: 5 to 8 per 1000 live births Major cause of death in first year of life (after prematurity) Most common anomaly is ventricular septal defect (VSD) Often children with CHD have another recognized anomaly (trisomy 21, 13, 18) Classification System Acyanotic defects Cyanotic defects Defects of increased pulmonary blood flow Defects of decreased pulmonary blood flow ASD Tetralogy of Fallot VSD Tricuspid atresia PDA Obstructive Coarctation of the aorta Aortic stenosis Pulmonic stenosis Mixed blood flow Transposition of the great vessels Hypoplastic left heart syndrome Comparison of Acyanotic and Cyanotic CHDs VSD • Increased pulmonary blood flow • Left to right shunting PDA Increased pulmonary blood flow Left to right shunting ASD Increased pulmonary blood flow Left to right shunting Coarctation of aorta Obstructive defect Increased pressure to head and upper extremities Decreased pressure to lower extremities Other Obstructive Defects Pulmonic stenosis Aortic stenosis Treatment of choice: balloon angioplasty Truncus Arteriosus Failure of normal septation and division of the embryonic bulbar trunk into the pulmonary artery and the aorta, which results in development of a single vessel that overrides both ventricles Blood from the left and right ventricles enters the common trunk, blood flow mixed Mortality is about 10% with highest mortality both truncal valve and aortic arch interruption. Long term complications include truncal valve regurgitation and conduit stenosis Truncus Arteriosus ONE GREAT VESSEL LEAVING THE HEART INSTEAD OF 2. Transposition of Great Arteries (vessels) • Septal defect or PDA must be present Transposition of Great Arteries TWO GREAT ARTERIES OF THE HEART ARE REVERSED. Tricuspid Atresia Decreased flow Will VSD pulmonary blood also have ASD (or PFO) and Tricuspid Atresia TRICUSPID VALVE FAILS TO FORM ASD RIGHT ATRIUM GOES TO LEFT RIGHT VENTERICAL UNDERDEVELOPED, VSD ALLOWS BLOOD LEFT VENTRICAL TO ENTER RIGHT VENRICAL AND PULMONARY ARTERY. Tetralogy of Fallot 4 defects Causes decreased pulmonary flow ‘Tet spells’ may occur Total Anomalous Pulmonary Venous Return (TAPVR Total Anomalous Pulmonary Venous Return (TAPVR) Hypoplastic Left Heart Syndrome CONGESTIVE HEART FAILURE (HF) The inability of the heart to pump an adequate amount of blood into the systemic circulation Congestive Heart Failure (HF) Right- or left-sided failure Right: systemic symptoms Left: lung symptoms Heart muscle may become damaged if left untreated Tachycardia and tachypnea at rest Dyspnea Retractions Activity intolerance infants manifest as poor feeding Weight gain – caused by fluid accumulation Hepatomegaly and/or cardiomegaly Increased pulmonary blood flow ECG indicates ventricular hypertrophy Clinical Manifestations Improve cardiac function Improve •Digoxin (improves contractility)- *high alert med- toxicity potential! •ACE inhibitors (reduces afterload, makes it easier to pump) •Beta Blockers •Resynchronization Therapy via pacing Remove accumulated fluid and sodium Treatment Goals Remove Decrease •Diuretics Decrease cardiac demands Improve tissue oxygenation Improve •Oxygen may be indicated, but we only use when necessary Case update: Ryan Ryan is brought to the cardiologist by his parents because he has been lethargic and has had diarrhea for 24 hours. Assessment as follows: Wt: 7kg (15.4 lbs) Temp 97.9* HR- 80 bpm RR- 35 bpm Potassium- 2.9 mEq/L digoxin- 2.5 ng/mL Do you have any concerns regarding this information? ACQUIRED CARDIAC DISORDERS INFECTIOUS & INFLAMMATORY CARDIAC DISORDERS Infective Endocarditis Patho: bacteremia causes vegetations to grow on valves; may become emboli Diagnostics: based on clinical manifestation; definitive diagnosis based on blood cultures Management: Immediate treatment with high-dose antibiotics Prophylaxis for high-risk patients: PCN (Clindamycin for PCN allergy) 1 hour before invasive or dental Rheumatic Fever Rheumatic Heart Disease Rheumatic fever (RF) Inflammatory disease occurs after Group A strep Affects joints, skin, brain, and heart Rheumatic heart disease (RHD) Most common complication of RF Damage to valves as result of RF Diagnostics: ASO titer Management: Antibiotics, salicylates Bed rest, quiet activity Prophylactic antibiotic therapy Kawasaki Disease Acute systemic vasculitis of unknown cause; not transmitted person to person Increased risk of coronary artery aneurysm Patho: extensive inflammation of vessels Diagnostics: based on clinical findings (see next slide) Management: High-dose IVIG within first 7 days of illness, high-dose aspirin therapy Quiet environment, promote rest Treat symptoms Assess for HF