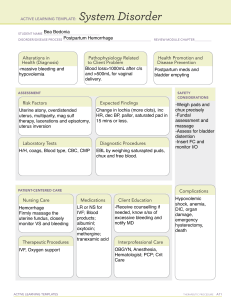
POSTPARTUM HEMORRHAGE I. INTRODUCTION The postpartum period or puerperium refers to the 6-week period after childbirth. Many physiologic and psychological changes occur during this period, enabling nurses to play major roles in assessment, comfort promotion and education. Protecting a woman’s health as these changes occur is important in preserving her future childbearing function and for ensuring that she is physically well enough to incorporate her new child into her family. Although the puerperium is usually a period of health, complications like hemorrhage, particularly, uterine atony, (which was the case of my patient) can occur, when they do, immediate intervention is essential to prevent long-term disability and interference with parent-child relationships. For this case study, we aim that: 1.) we will have better understanding of postpartum hemorrhage by reading books, articles and journals that are related with the disease; 2.) understand clearly the pathophysiology of the disease, risk factors, manifestations and treatment and modalities of the disease; and 3.) equip ourselves with skills and health teachings that are appropriate for the care of patients with postpartum hemorrhage, particularly uterine atony. II. NURSING ASSESSMENT A.PERSONAL DATA The patient is Mrs. X. She was 21 years old, born on October 27, 1986 from San Jose, Sta. Rita, Pampanga. She is a Filipino, married and a Roman Catholic. SOCIO-DEMOGRAPHICPROFILE MRS.X is a pure blooded Capampangan whose main concern is to make a living for her family and to save money for her future delivery. She works as a bank teller in one of the rural bank in Sta.Rita. His husband is a farmer and manages one of the family businesses. Mrs. X and her husband are religious—that they see to it they both go to church every Sunday. They believe that God must be the center of their family. Whenever a family member gets sick, they adhere to self-medication but if the condition is a bit serious, they go directly to the nearest hospital. Mrs. X lifestyle include: working for 8 hours, sleeping for <8 hours, eating nutritious meals (more fruits and vegetables, less in meat and fatty foods, avoids junk food and soft drinks) 3 times a day, etc. As a recreational activity, she watches television as soon as she goes home and do some cross-stitching. She does not smoke nor drink any alcoholic beverages. ENVIRONMENTAL FACTORS Their house is situated in San Jose, Sta. Rita, and a place near the main road. And in just a meter away from their home is a gasoline station. Jenney’s and tricycle are usually their means of transport. Their water supply comes from NAWASA. There are lesser pollutants in the air because their area is rural and that few vehicles are present. B. Maternal-Child Health History Mrs.X got married when she was 20 years old after her graduation. She got pregnant 3 months later. According to her, she visits her doctor every month for pre natal check-up and that she took all the vitamins prescribed by her doctor. Aside from urinary tract infection on her first trimester and 2 nd week of the last trimester, she had never encountered any other problems during the entire course of her pregnancy. She was screened for hepatitis B, and had several laboratory tests like complete blood count, blood typing, and fasting blood sugar. She was also given a shot of tetanus toxoid on her last trimester. Onset of Menarche: 15 years old Gravida- 1, Parity- 0/ Term-0, Preterm-0, Abortion-0, Livebirth-0 Family Health Illness History The different diseases that run in the family of Mrs. X are: • Father Hypertension, • Si ster hypertension Legend: • Parents • Si blings • Mother Diabetes Mellitus • rother Pulmonary tuberculosis B • ster none Mrs.X None C. .History of Past Illness According to the patient she was not sure whether she was fully immunized during her early years, but as far as she remembers, aside from minor illnesses such as simple fever, coughs and colds, she never had any major disease such as communicable diseases neither hospitalized. She has no allergy with food or any allergen in the environment neither to any medicine. She never experienced any serious accidents such as vehicular accident and fracture. History of Present Illness Mrs. X was admitted to the hospital (Rosario Memorial Hospital) last February 19, 2008, at around 4:50 in the morning because of labor pains. According to the patient, few hours prior to admission, she was asleep and suddenly felt some abdominal cramping, since the pain is not that really intense, she ignores it and went back to sleep. At around 3 am she was awakened by abdominal pain which was accompanied by flank pain and some vaginal discharge. She told this to her husband and decided to go to the hospital. Si Vital signs upon admission: BP- 100/70, PR-90, RR- 20, TEMP-36.8deg.cel. She was assessed by the resident on duty and found out she is already in labor. Internal examination was made and the results were: 6cm, 50% effaced. (+) BOW, FHT-140 beats/minute. Her attending physician was then notified and orders the following; NPO, IVF: D5LRS 1L + 1 ampule syntocinon, 1 ampule buscopan IV, Monitor FHT. In the course of labor induction, the cervix was not able to dilate in spite of uterine contraction, so the Doctors orders to have the patient under cesarean section. She was transferred to the operating room from the delivery room. After the delivery of the baby and placenta, the uterus was noticed to be relaxed and the bleeding did not stop. In spite of the intervention made, such as bimanual uterine massage, injection of methergine to the uterine muscle, and uterine artery ligation, nothing happened. The bleeding was not controlled. So, the doctor opted to have the last resort of intervention which is hysterectomy. D. Physical Examination (IPPA- Cephalo-caudal Approach) The patient was admitted last February 19, 2008 at around 3:50 am. I met the patient last February 20, 2008; unfortunately, I was not there during the operation on February 19, 2008. When I visited her, she was already on her 1st day post operative. I introduced my self, told her that I was assign to take care of her for few days. I stated my purpose and asked permission to do physical examination. Although she seems tired, in pain and quite depressed, she consented me in doing physical examination. GENERAL APPEARANCE The patient is in lying position; she was approximately 130lbs and approximately 5 feet and 2 inches tall. She was neat, well groomed and no foul odor. She grimaces every time she moves. She is slightly pale, seems tired, with labored breathing, because of pain, quite irritable but cooperative. Vital signs upon assessment are as follows: BP- 100/70mmHG, PR-105, RR-20, Temp- 37 degree Celsius. RMH Assessment Skin Assessment admission Feb. 20, 2008 upon Nursing Assessment Feb.21, 2008 Feb 22, 2008 The skin appears pale, warm to touch. The complexion is fair, slightly (+) Pallor, good skin (+) Pallor, good skin dry but with good skin turgor, warm to touch turgor, turgor. There is no skin lesions found Hair Nails Head Eyes vision Ears hearing The hair is long and black in color, it is quite oily and according to the patient, it is a little bit itchy. There is presence of little dandruff, but no foul odor smelled. The nails on both hand and feet are well-trimmed, slightly pink in color and are convex curved. Blanch test was made to test for capillary refill and there is prompt return of the color. The head is normal in size. No lesions neither mass was noted upon inspection. There is symmetry in facial movements. Black in color. The eyelids are symmetrically aligned and there are equal movements. Conjunctivas are shiny, smooth and pale pink in color .Pupils and constrict promptly when lighted. I also asked the patient to read the note posted on the wall which was approximately 12 feet away and she read it correctly. No deviation on the six occular movements. Color is same as the facial and skin. There is symmetry in size and position. Auricles are mobile, firm and not tender. The pinna recoils after it is folded. There is wet serumen that is brown i9n color. The tympanic membrane is gray in color and is semi transparent. The patient hears and responded well I washed the hair and I Well-combed and used anti dandruff negative for foul odor. shampoo. So the itching Still with little dandruff. was lessened. Same findings Same findings Same findings Same findings Same findings Same findings Same findings Same findings to whispered voice and watch tic test. Color is same of as the facial color, located in the middle of the face. It is symmetric and straight. No discharge, flaring, lesions and tenderness Nose and noted. sinuses I used cotton balls with alcohol and asked the patient to smell it while pinching each nostril alternately. The patient was able to smell on both nostrils. The lips is slightly pale in color, soft, moist and smooth in texture the gums are pink and there are 29 adult teeth, the Mouth and enamel are yellowish in oropharynx color. Tongue is smooth and (–) for lesions. The palate, uvula, oropharynx and tonsils appear smooth and pink in color. (+) bad breath. I asked the patient to move the head from left to right and flexed and hyper extended the head, (+) for smooth movements,(-) for Neck discomfort and the movements coordinated. (-) for lymph nodes upon palpation on the thyroid gland. RR-20 Thorax and BREATHS/MINUTE lungs I wasn’t able to assess the posterior thorax since the patient is in pain so I just observed the movements of the chest and he breathing pattern. (+) for Same findings Same findings Foul odor of the breath was lessened after doing oral care. I instructed the (-) bad breath patient to do oral care for at least 2times a day. ___________________ ________________ RR- 22 breaths/minute RR-18 breaths/minute Symmetric and full expansion of the chest. The spine is vertically aligned. Chest wall is intact, no tenderness and no masses found. labored breathing. BP is 100/70; heart rate is 105 beats/ minute. No Heart other abnormal sounds heard. (+) symmetric pulse volume and full pulsation on peripheral pulses of Peripheral both upper and lower vascular extremities. Jugular vein is system not distended. Skin is warm to touch, no edema found on both upper and lower extremities. Breast and I wasn’t able to palpate the axillae breast since they are very painful and very engorge so I just observed them. The right breast is much engorged than the left. The areola appears dark brown. The nipples are round and everted (+) for colostrums. Since the baby is cleft lip and cannot tolerate sucking, I instructed the mother to use breast pump to extract the milk. (+) dry, intact dressing, Abdomen The wound is still painful so I didn’t have the chance to palpate other organ on the surrounding area. But to what I had notice, the abdomen is slightly globularly enlarge. No mass and lesions found on other areas of the abdomen. Muskuloskeletal system BP is 100/80, PR- 85 BP- 100/80; PR- 88 Same findings Same findings The patient was able to use the breast pump so she was a little bit relieved. And was able to feed the baby using a dropper. I asked the permission of With intact and dry the doctor and the patient dressing to do wound dressing so that I could observe the wound. The incision is found in the midline, just below the umbilicus and just above the symphisis pubis. There are around 15 stitches, no discharge neither foul odor noticed on the wound area. I compared the size, Same findings shape and color of one side of the body to the other side, there is equal sizes and color on both Same findings sides. (-) for contractures, tremors, deformities, swelling, and tenderness. Movements are coordinated and are normally firm. There is equal strength on both sides of the body. Genital and (+) catheter, The urine is anal area still light red in color, around 500cc in amount (+) lochia rubra moderate in amount and smells like menstrual blood. The perineum is slightly edematous. No abnormalities found on the anal area. III. ANATOMY AND PHYSIOLOGY (+) catheter, red to light yellow in color around 200cc. (+) lochia rubra mild to moderate in amount. I did a perineal care so (-) for foul odor. (-) catheter, urine is light pink to light yellow in color. (+) lochia rubra minimal in amount. (-) foul odor. THE FEMALE REPRODUCTIVE SYSTEM The female organ is composed of external and internal genitalia. External genitalia comprised the mons pubis, clitoris, vestibule, urinary meatus, labia majora, labia minora, hymen, fourchete, perineum and the anus. The internal genitalia include the vagina, ovaries, fallopian tubes, uterus and the cervix. MONS PUBIS The mons pubis is a rounded elevation of the skin over the pubis. It is due to a pad of fat under the skin. The mons pubis is covered with hair at the age of puberty and it serves as a protection to external genitalia. CLITORIS Near the end of the cleft between the labia majora, the clitoris is evident; it is a small body of erectile tissue. It is a sensitive organ that is very important to the woman’s sexual response. VESTIBULE The urethra and the vagina open into the vestibule. The major vestibular glands (Bartholin) are tubulo- alveolar glands that secrete mucus. URETHRAL OPENING The opening of the urethra, the tubular vessel through which urine passes, is located midway between the clitoris and the vaginal opening. LABIA MAJORA The labia majora are two folds of skin that pass from the mons pubis backward. They join each other over the ridge formed by the body of the clitoris and unite again behind the opening of the vagina in the region known as the perineum. LABIA MINORA The two folds of delicate skin that arise just anterior to the clitoris are the labia minora. They cover part of clitoris as the prepuce and pass backward, bonding the vestibule of the vagina. Although sebaceous glands are present, no hair or sweat glands are found in the skin of the labia minora. FOURCHETTE It is the area where the labia majora join behind the vagina. PERINEUM The area of skin between the vaginal opening and the anus is the perineum. HYMEN The hymen is a thin membrane that partially covers the vaginal opening. If the hymen is extensive and still present at first intercourse, it may be broken or stretched as the penis enters the vagina and some bleeding and pain may occur, although more typically its presence is unnoticed. VAGINA The vagina is a flexible tube-shaped organ that is the passageway between the uterus and the opening of the vulva. Because during birth, the baby travels from the uterus through the vagina, the vagina is also known as the birth canal. When a man and a woman engaged in vaginal intercourse, the penis is inserted into the vagina. CERVIX The cervix is located at the bottom of the uterus and includes the opening between the vagina and the uterus. The cervix is composed of dense, collagenous, elastic connective tissue with a few smooth muscle fibers. It must become widely dilated at parturition. The ability to dilate probably is due to the softening of the intercellular substance, associated with an increased tissue fluid content. OVARIES The primary reproductive organs of a female are the ovaries, a pair of almondshaped glands. At puberty, ovaries produce about 400,000 eggs. Each month an egg is released from the ovary and travels one of the fallopian tubes. If the egg is released around the time of sexual intercourse and it meets and fuses with male’s sperm, it becomes fertilized. If an egg is not fertilized, it moves from the fallopian tube to the uterus and passes out of the body in the next menstrual cycle. The ovaries contain many follicles composed of a developing egg surrounded by an outer layer of follicle cells. Each egg begins oogenesis as a primary oocyte. At birth each female carries a lifetime supply of developing oocytes, each of which is in Prophase I. A developing egg (secondary oocyte) is released each month from puberty until menopause, a total of 400-500 eggs. OVARIAN CYCLES After puberty the ovary cycles between a follicular phase (maturing follicles) and a luteal phase (presence of the corpus luteum). These cyclic phases are interrupted only by pregnancy and continue until menopause, when reproductive capability ends. The ovarian cycle lasts usually 28 days. During the first phase, the oocyte matures within a follicle. At midpoint of the cycle, the oocyte is released from the ovary in a process known as ovulation. Following ovulation the follicle forms a corpus luteum which synthesizes and prepares hormones to prepare the uterus for pregnancy. FALLOPIAN TUBES The oviducts or fallopian tubes vary from 8 to 14 cm in length. Each tube is divided into an interstitial portion, isthmus, ampulla and infundubulum. The fallopian tubes have fingerlike projections at the ends near the ovaries that sweep the egg into the fallopian tube after it is released from the ovaries. If sperm are present in the fallopian tube, fertilization (conception) may occur and the fertilized egg will be swept into the uterus by cilia (hair like projections inside the fallopian tube). UTERUS The uterus is a mascular organ that holds and nourishes the developing fetus during pregnancy. Although the uterus is normally about the size of a fist, during pregnancy it is capable of stretching to accommodate a fully developed fetus, which is typically about 50cm (about 20 inches) long and weighs about 3.5 kilograms (about 7.5 pounds). The uterine muscles also produce the strong contractions of labor. The uterus has three layers, the perimatrium which is the outermost layer, myometrium, the middle layer and the endometrium which is the innermost layer, and is richly supplied with blood vessels and glands. HORMONES AND FEMALE CYCLES The ovarian cycle is hormonally regulated in two phases. The follicle secretes estrogen before the ovulation; the corpus luteum secretes both estrogen and progesterone after ovulation. Hormones from the hypothalamus and anterior pituitary control the ovarian cycle. The ovarian cycle covers events in the ovary; the menstrual cycle occurs in the uterus. Menstrual cycles vary from between 15 and 31 days. The first day of the cycle is the first day of blood flow (day 0) known as menstruation. During menstruation, the uterine lining is broken down and shed as menstrual flow. FSH and LH are secreted on day 0, beginning both the menstrual cycle and the ovarian cycle. Both FSH and LH stimulate the maturation of a single follicle in one of the ovaries and the secretion of estrogen. Rising levels of estrogen in the blood trigger secretion of LH, which stimulates follicle maturation and ovulation (day 14, or mid cycle). LH stimulates the remaining follicle cells to form the corpus luteum, which produces both estrogen and progesterone. Estrogen and progesterone stimulate the development of the endometrium and preparation of the uterine lining for implantation of a zygote. If pregnancy does not occur, the drop in FSH and LH causes the corpus luteum to disintegrate. The drop in hormones also causes the sloughing off of the inner lining of the uterus by a series of muscle contractions of the uterus. IV.B Diagnostic and Laboratory Procedures Laboratory Procedure Hematology Indication: *CBC This blood test evaluates blood loss, anemia, blood replacement therapy and fluid balance and screens red blood cell status. *PTT & PT This test evaluates coagulation ability of blood Analysis and Interpretation: Laboratory Results 02- Date 02- 02- Normal Values 1st test: decrease level of hgb, hct,pt,ptt indicates bleeding, 19- 20- 21- 2008 2008 2008 Hgb. 100 105 115 115-155 g/L Hct. 31 30 35 .38-.48 WBC 7.5 8 -- 5-10x109/L decrease blood volume. 2nd test: low level of hgb hct. Indicates decrease level of blood volume. 3rd test (post BT): hgb and hct are within normal value. Compensated PMN 55 .62 -- .45-.65 Lymp. 25 .23 -- .20-.35 PT PTT 4.3 6 2.2 from blood loss. 12-15 sec. 35-45 sec 0 *BLOOD TYPING Involves mixing of maternal serum with standard reagent red cells that contain the antigens with which A+ most of the common clinical significant antibodies will react, thus, administration of unscreened blood may res8ult to adverse reaction. No HBsAG n Hepatitis B is contagious and can rea be transferred to the baby via ctiv placental transport. This test will e alert the caregivers how to handle blood products and proper care of the patient including the baby. Nursing Responsibilities Explain to client the procedure to be done. Observe sterile techniques when taking specimen. Instruct patient to submit specimen immediately to the laboratory. Explain to client the findings. Date Diagnostic ordered/ Procedure Date of Ultrasound results Dec. 11,2007 Analysis and Result Result Single live male fetus in Indications ceplalic presentation. of Ultrasound is about 29 weeks and 4 used to days AOG. perform Normohydramnios noninvasive, risk-free abdominal examinations. Used to detect tumors, cyst obstruction, and abscesses. Information gained from the use of ultrasound is Interpretation of useful throughout pregnancy. Nursing Responsibilities 1. Explain procedure to the patient. 2. Instruct patient to drink at least 6 to eight glasses of water or until she feels the urge to urinate. 3. Tell the patient to inform the nurse as soon as she feels the urge to urinate and hold it until the procedure was completed. IV. PATIENT AND HER ILLNESS A. DEFINITION OF THE DISEASE Hemorrhage, one of the most important causes of maternal mortality associated with childbearing, poses a possible threat throughout pregnancy and is a major potential danger in the immediate postpartal period. Traditionally, postpartal hemorrhage has been defined as any blood loss from the uterus greater than 500ml within 24-hour period. (St.John and Rouse, 2003). In specific agencies, the loss may not be considered hemorrhage until it reaches 1000ml. hemorrhage may occur either early (i.e. within the first 24 hours), as in the case of my patient, which happens during the operation, where in she already losses 1500ml of blood), or late (anytime after 24 hours during the remaining days of the 6-week puerperium). The greatest danger of hemorrhage is in the first 24 hours because of grossly denuded and unprotected area left after detachment of the placenta. As a way of remembering the causes of PPH, several sources have suggested using the 4T’s as a mnemonic. Tone diminished (uterine atony), tissue (retained placenta, placenta accrete), trauma (uterine inversion, uterine rapture, cervical laceration, vaginal hematoma) and thrombin (disseminated intravascular coagulation) (Society of Obstetricians and Gynecologists of Canada, 2002). INCIDENCE AND PREVALENCE Pospartum hemorrhage is the leading cause of maternal mortality. All women who carry a pregnancy beyond 20 weeks’ gestation are at risk of PPH and its sequelae. Although maternal mortality rates have declined greatly in the developed world, PPH remains the leading cause of maternal mortality elsewhere. The direct pregnancy-related maternal mortality rate in the United States is approximately 7-10 women per 100,000 live births national statistics suggest that approximately 8% of these deaths are caused by PPH (Berg, 1996). In industrialized countries, PPH usually ranks in the top 3 causes of maternal mortality, along with embolism and hypertension. In the developing world, several countries have maternal mortality rates in excess of 1000 women per 100,000 live births, and the World Health Organization statistics suggests that 25% of maternal deaths are due to PPH, accounting for more than 100,000 maternal deaths per year (Abouzahr, 1998). TONE This is a failure of the myometrium at the placental site to contract and retract and to compress torn blood vessels and control blood loss by a living ligature. When the placenta is attached, the volume of blood flow at the placental site is approximately 500800 ml per minute. Upon separation, the efficient contraction and retraction of uterine muscle staunch the flow and prevent a hemorrhage, which would otherwise ensure with horrifying speed. Causes of atonic uterine action resulting in PPH are as follows: 1. Incomplete placental separation. If the placenta remains fully adherent to the uterine wall it is unlikely to cause bleeding. However, once separation has begun, maternal vessels are torn. If placental tissue remains partially embedded in the in the spongy decidua, efficient contraction and retraction are interrupted. 2. Retained cotyledon, placental fragment or membranes. These will similarly impede efficient uterine action. 3. Precipitate labor. When the uterus has contracted vigorously and frequently resulting in duration of labor that is less than 1 hour, then the muscle may have insufficient opportunity to retract. 4. Prolonged labor. In a labor where the active phase lasts more than 12 hours uterine inertia (sluggishness) may result from muscle exhaustion. 5. Polyhydramnios or multiple pregnancies. The myometrium becomes excessively stretched and therefore less efficient. 6. Placenta previa. The placental site is partly or wholly in the lower segment where the thinner muscle layer contains few oblique fibers: this result in poor control of bleeding. 7. Abruptio placenta. Blood may have seeped between the muscle fibers, interfering with effective action. 8. General anesthesia. Anesthetic agents may cause uterine contraction, in particular the volatile inhalation agents, for example halothane. 9. Mismanagement of the third stage of labor. It is salutary that this factor remains a frequent cause of PPH. Fundus fiddling or manipulation of the uterus may precipitate arrhythmic contraction so that the placenta only partially separates and retraction is lost. 10. A full bladder. If the bladder is full, its proximity to the uterus in the abdomen on completion of the second stage may interfere with uterine action. This also constitutes mismanagement. Other predisposing factors which might increase the risks of postpartum hemorrhage are: previous history of postpartum hemorrhage or retained placenta, high parity resulting in uterine scars tissue, presence of fibroids, maternal anemia and a woman with HIV/AIDS. TISSUE The diagnosis is reached when the placenta remains undelivered after a specified period of time (usually ½ to 1 hour following the baby’s birth). The conventional treatment is to separate the placenta from the uterine wall digitally, effecting a manual removal. Selinger et al (1986) noted that waiting for 1 hour before resorting to this intervention will almost halve the number of woman who will require manual removal with its accompanying risks. Failure of complete separation of the placenta occurs in placenta accrete and its variants. In this condition, the placenta has invaded beyond the normal cleavage plane and is abnormally adherent. Significant bleeding from the area where normal attachment (and now detachment) has occurred may mark partial accrete. Complete accrete in which the entire surface of the placenta is abnormally attached, or more severe invasion (placenta accrete or pecreta) may not initially cause severe bleeding, but it may develop as more aggressive efforts are made to remove the placenta. This condition should be considered possible whenever the placenta is implanted over a previous uterine scar, especially if associated with placenta previa. All patients with placenta previa should be informed of the risk of severe PPH, including the possible need for transfusion and hysterectomy. Blood may distend the uterus and prevent effective contraction. Finally, retained blood may cause uterine distention and prevent effective contraction. TRAUMA Damage to the genital tract may occur spontaneously or through manipulations used to deliver the baby. Cesarean delivery results in twice the average blood loss of vaginal delivery. Incisions in the poorly contractile lower segment heal well but are more reliant on suturing, vasospasm, and clotting for hemostatsis. Uterine rapture is most common in patients with previous cesarean delivery scars. Any uterus that has undergone a procedure resulting in a total or thick partial disruption of the uterine wall should be considered at risk of rupture in a future pregnancy.This admonition includes fibroidectomy; uteroplasty for congenital abnormality; cervical ectopic resection; and perforation of the uterus during D&C, biopsy, hysteroscopy, laparoscopy, or intrauterine contraceptive device placement. Trauma may occur following very prolonged or vigorous labor, especially if the patient has relative or absolute cephalopelvic disproportion and the uterus has been stimulated with oxytocin or prostaglandins. Trauma may also occur following extrauterine and intrauterine manipulation of the fetus. Finally, trauma may result secondary to attempt to remove a retained placenta manually or with instrumentation. Cervical laceration is most commonly associated with forceps delivery, mothers have often been unable to resist bearing down before full cervical dilatation, and manual exploration or instrumentation of the uterus may result in cervical damage. Vaginal sidewall laceration is also most commonly associated with operative vaginal delivery, but it may occur spontaneously, especially if fetal hand presents with the head. Lacerations may occur during manipulations to resolve shoulder dystocia. Lower vaginal trauma occurs either spontaneously or because of episiotomy. Spontaneous lacerations usually involve the posterior fourchete; however, trauma to the periurethral and clitorial region may occur and can be problematic. THROMBOSIS The failure of the blood to clot is such an obvious sign that it can be overlooked in the midst of the frantic activity that accompanies torrential bleeding. It can occur following severe pre-eclampsia, antepartum hemorrhage, amniotic fluid embolus, intrauterine death or sepsis. Fresh blood is usually the best treatment as this will contain platelets and the coagulation factors V and VIII. The expert advice of a hematologist will be needed in assessing specific replacement products such as fresh frozen plasma and fibrinogen. C. PATHOPHYSIOLOGY: Over the course of pregnancy, maternal blood volume increases by approximately 50% (from 4L to 6L). The plasma volume increases somewhat more than the total RBC volume, leading to a fall in the hemoglobin concentration and hematocrit value. The increase blood volume serves to fulfill the perfusion demands the low resistance uteroplacental unit and to provide a reserve for the blood loss that occurs at delivery. At term, the estimated blood flow to the uterus is 500-800ml/minute, which constitute 10-15% of cardiac output. Most of the flow traverses the low resistance placental bed. The uterine blood vessels that supply the placental site traverse a weave of myometrial fibers. As these fibers contract following delivery, myometrial retraction shortened length following each successive contraction. The blood vessels are compressed and kinked by this crisscross latticework, and, normally, blood flow is quickly occluded. The arrangement of muscle bundles has been referred to as “physiologic sutures” of the uterus (Baskett, 1999). Uterine atony, is failure of the myometrial fibers to contract and retract. The uterus must remain in a contracted state after birth to allow the vessels at the placental site to seal. This is the most important cause of PPH and usually occurs immediately following the delivery of the baby, up to 4 hours after delivery. Patient actual pathophysiology: POSTPARTUM HEMORRHAGE Prolonged and difficult labor Labor augmented with oxytocin Myometrium failed to contract and retract Failure to compress torn blood vessels UTERINE ATONY HEMORRHAGE Boggy Uterus Bright red blood Decrease BP Tachycardia Pallor Palpitations COMPENSATED D. PREDISPOSING FACTORS OF POSTPARTUM HEMORRHAGE The factors that predisposed Mrs. X to cause uterine atony are the labor that is augmented with oxytocin and the labor that is prolonged and difficult. The patient is nuliparous, so, she doesn’t know how to bear down. E. SIGNS AND SYMPTOMS Blood Volume Blood Pressure Loss (systolic) Signs and Symptoms Degree of Shock 500-1000 (10-15%) Normal 1000-1500ml (15-25%) Slight fall (80100mmHG) 1500-2000ml (25-35%) Moderate fall (7080mmHg) Palpitations, compensated tachycardia, dizziness Weakness, Mild tachycardia, sweating Restlessness, pallor, Moderate oliguria 2000-3000ml (35-50%) Marked fall(from5070mmHg) Collapse, air hunger, anuria Severe Signs and symptoms appeared to Mrs. X aside from having a boggy uterus, blood that is bright red in color, are tachycardia as evidenced by PR-110, palpitations, pallor and BO of 90/60mmHg. These symptoms are compensatory mechanisms of the heart to pump more blood in response to blood loss. Fortunately, the patient was able to compensate with this situation. F. TREATMENT The following is a plan for managing obstetric hemorrhage if therapeutic management such as fundal massage or bimanual uterine massage is unsuccessful. This was adopted from Bonner (2002). The word “ORDER” is a useful mnemonic for remembering the basic outline ORGANIZATION 1. Call experienced staff (including obstetrician and anesthetist) 2. Alert the blood bank and hematologist. 3. Designate a nurse to record vital signs, uterine output, and fluids and drugs administrator 4. Place operating room on standby. RESUSCITATION 1. Administer oxygen by mask. 2. Place 2 large-bore intravenous lines. 3. Take blood, cross match of 6 U PRBC’S, and obtain a CBC count, coagulation factor level, creatinine value and electrolyte status. 4. Begin immediate fluid replacement with NS or Ringer lactate solution. 5. Transfuse with PRBCs as available and appropriate. DEFECTIVE BLOOD COAGULATION 1. Order coagulation screen (International Normalized Ratio, activated partial thromboplastine time) fibrinogen, thrombin time,blood film, and D-dimer results are abnormal. 2. Give FFP if coagulation test results are abnormal and sites are oozing. 3. Give cryoprecipitate if abnormal coagulation test results are not corrected with FFP bleeding continues. 4. Give platelet concentrates if the platelet count is less than 50x10 to the 9/L and bleeding 5. Use cryoprecipitate and platelet concentrate before surgical intervention. EVALUATE RESPONSE 1. Monitor pulse, blood pressure, blood gas status, and acid-base status, and consider monitoring of central venous pressure 2. Measure urine output using indwelling catheter. 3. Order regular CBC counts and coagulation tests to guide blood component therapy REMEDY THE CAUSE OF BLEEDING 1. If antepartum, deliver fetus and placenta. 2. If postpartum, use oxytocin, prostaglandin, or ergonovine. 3. Explore and empty the uterine cavity, and consider uterine packing. 4. Examine the cervix and vagina, ligate any bleeding vessels, and repair trauma. 5. Consider arterial embolization. 6. Ligate uterine blood supply (ie, uterine, ovarian,and/or internal iliac arteries). 7. Consider hysterectomy. V. PATIENT AND HER CARE A. Medical Management 1. Medical Management/ Intravenous Fluid, Blood Transfusion, Oxygen Therapy Date Ordered/ General Date Description Indications/ Purpose Client’s Response to the Treatment Treatment Performed Feb.19, 2008/ Feb. 20, 2008 Intravenous Feb21, 200* Fluid D5LRS 1L x 3132 gtts/min Isotonic Solution – have the same concentration as blood and plasma. Used to restore vascular volumes. This was indicatede to the patient as an access for medications and to No allergic reaction restore vascular volumes since she will undergo surgery 4 “u” FWB RBC and plasma. WBC and platelet not viable after 24 hrs. To replace blood loss during the surgery and to prevent hypovolemia. No allergic reaction As a compensation to maintain adequate supply of hemoglobin in the body. Nursing Responsibilities Determine what type of IVF to infuse. Always check for IV patency. Check for IVF’s proper regulation. Check for fluids to follow. Feb.19, 2008 Blood Transfusion Nursing Responsibilities Determine what blood products to infuse in the Doctor’s Order sheet. Check for vital signs of the client before, 15 mins. after starting BT and after BT. Monitor BT regulation strictly. Monitor patient for any allergic reactions. Stop BT if untoward reactions happen such as fever, rashes, etc. Maintain a KVO regulation for the IVF. Oxygen Therapy Feb. 19, 200 In the OR As an assistive way patient to help clients with The accepted the compromised treatment and was 2-3 LPM via oxygen status. relieved from DOB. nasal cannula For patients with No allergic breathing and reactions. airway problems. Nursing Responsibilities Determine the amount of oxygen to be given in Doctor’s Order sheet. Check for the patency of the cannula to be used. Maintain regulated amount of oxygen given to patient. Humidify the oxygen to be given to patient. Observe precautionary measures while giving the therapy like avoiding smoking, preventing static electricity/ removing combustible and igniting materials. Indwelling To prevent bladder No allergic Feb.19,, 2008 Indwelling Foley Catheter distention and reaction. Date Removed: Catheter, French injury during Feb 21, 2008 18 surgery Nursing Responsibilities: Determine Doctor’s order for the insertion of the catheter. Explain the procedure and the purpose of IFC insertion to the client. Prepare all the necessary equipments. Maintain the sterility of the catheter and apply KY gel to lubricate catheter before insertion. Insert the catheter with the dominant hand while opening the labia with less dominant hand. Inject 5-10 cc of NSS to keep the catheter anchored, observe for backflow of urine. Monitor the amount of urine in the urine bag. 2. PHARMACOTHERAPY Generic Name/ Brand Name/Stock/ Indication Date Ordered/ Route/ Date Dosage/ Performed Frequency Oxytocin/syntocinon Injecton:10units/ml/ indicated to the Feb 19, 2008 patient to induced labor. 1amp incorporate IV. Client’s Action/ Response the Mechanism of Medication with Action Actual Side Effects Causes potent and selective stimulation of to No reactions. uterine and mammary gland smooth muscle Nursing Responsibilities monitor and record patient’s uterine contractions since it has to be titrated every 15 minutes. monitor vital signs since it can increase blood pressure. do not give oxytocin via IV bolus injection. It must be administered by infusion Bisacodyl/ Feb.21 2008 Dulcolax, Biscolax To help the patient in passing out flatus, 1 suppository Laxative per rectum Stimulate laxative that increases peristalsis, No reactions. probably by direct effect on smooth muscle of the intestine. to soften stools to prevent straining. Nursing Responsibilities Before giving for constipation, determine whether patient has adequate fluid intake, exercise and diet. Tell patient about dietary sources of bulk including cereals, fresh fruit and vegetables. Tell patient to take drug with full glass of water. CefazolinSodium/ MAXCEP Feb.19, 2008 Cefalexine/ indicated to patient Feb. 20, 2008 to prevent infections Feb22,2008 and eventually speeding up wound healing. 1.gram, IV, q6/ mg, IV, q6 500mg tid. Anti-infective/ Antibiotic Second generation cephalosporin that inhibits cell-wall No reactions. synthesis, promoting osmotic instability; usually bactericidal. Nursing Responsibilities Ask the patient if he is allergic to penicillins or cephlosporins. Perform skin test prior administering the first dose. Instruct patient to report adverse reactions promptly. If a large dose is given, monitor for signs of superinfection. Tell client to take oral forms with food. Use cautiously in breast-feeding women and in patients with history of colitis or renal insufficiency. If the patient has difficulty in swallowing, crush tablet forms. Advise lactating mothers not to breast feed. Methylegonovine Feb19,2008 maleate/ mathergine 0.2mg/ml injection/ indicated to patient to stimulate uterine contractions. 1ml IV/ uterus Increases motor activity of the No reactions. uterus by direct stimulation Nursing Responsibilities Contraindicated for induction of labor, before delivery of placenta; in patients with hypertention and toxemia. Monitor and record blood pressure, pulse rate, and uterine response; report sudden change in vital signs, frequent periods of uterine relaxation, and character and amount of vaginal bleeding. Use cautiously in sepsis, obliterative vascular disease, and hepatic, renal or cardiac disease. Metronidazole Feb. 19, 2008 hydrochloride/ Flagyl/ 500mg/vial/ to prevent infection 500mg IV/ q6 An amebicide/ antiprotozoals. A direct acting trichomonocide No reactions. and amebicide that works at both intestinal and extratestinal site Nursing Responsibilities Tell patient to avoid alcohol and alcohol containing medications during therapy at least 48 hours after therapy is completed. Give oral forms with meals to minimize GI distress. Tell the patient metallic taste and dark or red-brown urine may occur. The IV should be administered by slow infusion only. Don’t give IV push. Do not refrigerate flagyl IV. Nalbuphine hydrochloride/ Feb. 19, 2008 10 mg, IV, q4 A narcotic and No reactions. to 6h. for opiod analgesic. Nubain/ 10mg/ml/ used as a pain reliever to the patient severe pain Binds with opiate receptors in many sites in the CNS (brain stem, and spinal cord) altering both perception and emotional response to pain. Nursing Responsibilities Contraindicated in patients with hypersensitivity to the drug, emotional instability, history of drug abuse, head injury, and increase intra cranial pressure. Use cautiously in hepatic and renal disease. These patients may overreact to customary doses. Monitor respirations of neonates exposed to the drug during labor. Monitor circulatory and respiratory status and bladder and bowel function. Hold dose and notify the doctor if respirations are shallow and rate is below 12 breaths /minute. Warn the patient to avoid hazardous activities that require alertness until CNS effects of the drugs are known Tranexamic acid/ Hemostan/ 500mg/5ml IV FEB.19, 2008 500mg capsule/ Feb21, 2008 indicated to patient in order to prevent hemorrhage. 500 mg, IV, q8 500mg/tid An antifibrinolytic agent used mainly in the treatment and prophylaxis No reactions. of hemorrhage associated with excessive fibrinolysis. Nursing Responsibilities It is contraindicated to patient with active intravenous clotting because of the risk of thrombosis. Hemorrhage due to DIC should not be treated with anti fibrinolytic compounds unless the condition is predominantly due to disturbances in fibrinolytic mechanisms. 3 .Diet Type of Diet NPO Date Ordered/ General Date Started/ Description Date Changed Feb.19, 2008 Client’s Response &/ or reaction to the Diet Indicated to the No reaction patient pre and post op to avoid vomiting during surgery and to Indications/ Purpose Sips of water Feb20, 4pm 2008/at Pure water Soft diet Feb.21,2008 DAT if (+) BM Feb.22, 2008 Low residue diet containing very few uncooked foods. Is easily chewed and digested Is ordered when the client’s appetite, ability to eat, and tolerance for certain foods may change. prevent aspiration after surgery and to avoid abdominal discomforts. Indicated to patient No reaction to prepare the stomach for soft diet and to avoid abdominal discomforts To prepare the No reaction stomach for solid foods. When normal intestinal motility has returned. Nursing Responsibilities Determine patient’s diet in the Doctor’s Order sheet. Instruct client of the appropriate diet. Enumerate different foods suited for the diet. 4. Activity/ Exercise Type Exercise Date Ordered/ of General Date Started/ Description Date Changed Indications/ Purpose Client’s Response &/ or reaction to the activity/ exercise & No reaction Passive Exercise Feb 19, 2008, Movements with Pre-operative Feb. 22-23, assistance. post-operative 2008 assistance for patient Flat on Bed Feb.19, 21, 2008 Person remains To remove effects No reaction on bed without of spinal pillow. anesthesia to prevent spinal headache and prevents opening of the surgical wound. Nursing Responsibilities Determine patient’s type of exercise in the Doctor’s Order sheet. FOB: do not use pillows Passive ROM: assist client in every activity to prevent him/her from falls. Assist client in stretching- flexing and extending of extremities. Advice client to dangle feet when sitting on bed. B. Surgical Management Alter native names Vaginal hysterectomy; abdominal hysterectomy; Laparoscopic hysterectomy; Supracervical hysterectomy; Radical hysterectomy; Removal of the uterus Definition A hysterectomy is a surgical removal of the uterus, resulting in the inability to become pregnant (sterility). It may be done through the abdomen or the vagina. Description Hysterectomy is an operation that is commonly performed. There are many reasons a woman may need a hysterectomy. However, there are non-surgical approaches to treat many of these conditions. Talk to your doctor about non-surgical treatments to try first, especially if the recommendation for a hysterectomy is for a cause other than cancer. During a hysterectomy, the uterus may be completely or partially removed. The fallopian tubes and ovaries may also be removed. A partial (or supracervical) hysterectomy is removal of just the upper portion of the uterus, leaving the cervix intact. A total hysterectomy is removal of the entire uterus and the cervix. A radical hysterectomy is the removal of the uterus, the tissue on both sides of the cervix (parametrium), and the upper part of the vagina. A hysterectomy may be done through an abdominal incision (abdominal hysterectomy), a vaginal incision (vaginal hysterectomy), or through laparoscopic incisions (small incisions on the abdomen -- laparoscopic hysterectomy). Your physician will help you decide which type of hysterectomy is most appropriate for you, depending on your medical history and the reason for your surgery. Indications Hysterectomy was indicated to the patient to control bleeding and eventually preventing other complications like hypovolemia and shock II. NURSING CARE PLAN (PATIENT-BASED) 2nd Priority: Risk for Infection NURSING NURSING SCIENTIFIC DIAGNOSIS EXPLANATION Subjective Risk for infection Risk for infection is the After 4 hours of • Determine • To be able The patient shows cues: related to condition wherein the NPI and patient’s level to know where understanding and (-) presence of person looses his body interventions, of the nurse will appreciation to incisional defenses that makes patient will be understanding start his health the health Objective woundsecondary him susceptible/ aware of the of the problem teachings. teachings given. cues: to limited making him at risk for possible and establish • • Weakness knowledge different infections and interventions that rapport. baseline data noted regarding proper diseases. In the case of could minimize • Assess the and know the wound care. a one day post-op her risk of having patient and get manifestations patient, the primary infection brought initial vital of the defense of the body by her condition. signs. problem. CUES • Limited range of motion • Irritable and restless • Pallor • With intact dressing. which is the skin was broken allowing microorganisms to enter in the body and cause infections and diseases. Manifestations of impending infection include elevation of OBJECTIVE INTERVENTIO RATIONALE EVALUATIO S N NS • To have a Aseptic • Provide techniques health teachings help minimize regarding the aseptic contamination techniques of the wound applicable to by wound care. microorganis • Demonstrate ms. WBC primarily the proper way of • lymphocytes and fever. cleaning a known surgical wound. antiseptic that Use of betadine helps reduce is advised. microorganis • Encourage ms. the use of clean • and sterile dressing is a dressing and good place for changing it microorganis regularly or as ms to live. prescribed. Changing it • Encourage regularly proper way of prevents it hand washing. from Betadine is The contamination. • Encourage • patient to washing is the maintain good best way to personal prevent the hygiene like spread of doing bed bath infection. regularly and • oral care. personal • Encourage hygiene client to wear removes Hand Good clean and loose microorganis clothes. ms in the body. • Promote comfort • measures such loose clothes as changing of facilitate linens. aeration of the Clean and wound thus • Encourage to promoting have fewer faster healing. visitors/ • minimize linens reduce interaction with the other people. microorganis Clean ms in the • Monitor vital environment. signs • frequently. reduces the This microorganis • Encourage m that the client to eat and patient could drink prescribed get from diet that is others and nutritious and promote good balance. These rest. include CHON- • rich, CHO-rich there are and Vit.-rich deviations foods like from the chicken/fish normal range. and fruits & • vegetables. and balance • Advise client meals provide to drink sufficient medications and energy to supplements client and prescribed by good the physician resistance to religiously. the body. • To know if Nutritious Medicatio ns and supplement help prevent complications of the disease and promote cure and recovery to patient. 1st Priority: Pain CUES NURSING DIAGNOSIS SCIENTIFIC EXPLANATIO OBJECTIVE N NURSING INTERVENTIONS RATIONALES EVALUATIO N Subjective Acute Pain Pain is an After 3 hours of • Perform • cues: related to tissue unpleasant sensory nursing comprehensive subjective verbalizes a “Masakit ya injury secondary and emotional intervention, the assessment of pain experience and decrease in pain ing meopera to surgical experience that is patient will to include location, must be scale of below ku.” intervention. normally associated verbalize characteristic, described by the 5/10, grimaces are with injury to body decrease level onset, duration, client in order to diminished and Objective tissues. The basic of pain. quality, intensity, plan effective achieved cues: elements of pain are and its treatment. tolerance to • With limited mobility the sensory precipitating impulses generated factor. Facial grimace noted receptors in the • Encourage use nervous system. of relaxation These sense organs, technique such as called nociceptors, focused breathing. • • • • With guarding behavior Irritable and restless Weakness noted by injury-sensitive convert mechanical, chemical • Monitor vital stimulations that signs. assess injure or threaten • Create a quiet, The patient activity. • Relaxations techniques help reduce skeletal muscle tension, which will reduce the intensity of pain. thermal, or tissues into Pain is a • Personal factors can influence pain • Pain scale above 8/10 impulses that are nondisruptive and pain transmitted along environment. tolerance. peripheral nerves to the spinal cord, and • Administer from there to higher analgesic as • brain centers. ordered. and quiet Comfortable atmosphere promote a relax feeling and permit the client to focus on the relaxation • Provide technique rather socialization as than external diversional activity. distraction. • Keeping the • Administer pain client busy will medication as reduce the pain order. sensation. Socialization is a means to divert the attention of the client. • To alleviate or if not, reduce the pain experience. CUES NURSING DIAGNOSIS SCIENTIFIC EXPLANATIO OBJECTIVE N NURSING RATIONALE EVALUATIO INTERVENTIONS S N Subjective Disturbed Disturbed Sleeping After 4 hours of • Determine • To be able The patient will cues: Sleeping Pattern Pattern is the NPI and patient’s level of to know where have periods of “ Eku related to pain condition wherein interventions, understanding of the nurse will rests because of making secondary to the person cannot patient can the problem and start his health the reduction of Mipatudtud” parenting role. achieve adequate achieve rest establish rapport. teachings. pain and Objective rest due to different periods due to • Assess the • disruptions in the cues: disruptions that reduction of patient and get baseline data • Weaknes could be physical pain and initial vital signs. and know the s noted (pain), as in the disruptions in • Promote manifestations Drowsine case of my patient. the conducive of the environment. environment for problem. ss psychological observed (anxiety), • • Droopy eyes • Frequent yawning noted • Limited range of motion • Irritable and restless • Pallor • With dry environmental (poor environmental conditions), etc. Manifestations are seen during the day and theses include drowsiness, lack of energy, frequent yawning, etc. To have a sleep such as: • Keeping a well-fixed bed. • A well fixed bed reduces • Keeping the strain a quiet that the environment by patient lowering voice feels. during interaction • • ss Keeping Le a well-ventilated interaction environment by reduces the opening windows, strain that the patient • Encourage feels. environment. VII. TEACHING PLAN: CARE OF THE SURGICAL WOUND (CESAREAN SECTION) I. LEARNER: A POST CESAREAN WOMAN WITH SURGICAL WOUND II.LEARNING OBJECTIVES: Upon completion of the instructional session, the client will: 1. 2. 3. 4. 5. C-1 Describe signs and symptoms of wound infection. P-2 Identify equipment needed for wound care. P-3 Demonstrate wound cleansing and bandaging. A-4 Describe appropriate action if questions or complications arise. A-5 Identify date and time of follow-up appointment for suture removal B. CONTENT OUTLINE I. Wound infection including signs and symptoms II. Identification of wound care equipment III. Demonstration of wound cleansing and bandaging on the patient’s wound IV. Resources available for patient’s questions including health clinic, emergency department. V. Follow-up treatment plan; where and when C. TEACHING METHOD/STRATEGY 1. Lecture/explain 2. Lecture/identify/show/practice 3. Demonstrate/ act out the steps and techniques 4. Lecture/explain 5. Lecture/ when, where/ time of follow-up treatment D INSTRUCTIONAL MATERIAL 1. Handout 2. Betadine solution, cotton buds, bactroban ointment, sterile gauze, surgical tape. 3. Handout 4. Handout 5. Written instruction E. EVALUATIVE TOOL 1. Oral questioning 2. Return Demonstration 3. Return demonstration 4. Oral questioning 5. Oral questioning III. INSTRUCTIONAL PROCEDURE 1. Statement of the objective of teaching surgical wound care 2. Presentation of the subject matter 3. Demonstration of cleansing and dressing wound 4. Facilitate asking questions 5. Evaluation D. PROCEDURE TEACHER’S ACTIVITY PATIENT’S ACTIVITY -Have you been informed of your operation this - Yes, before I signed the consent afternoon? -Where you told on what to expect of you after the -Yes, I was told to lie flat on my operation? back for 6 hours and do deep breathing, coughing and turning after 6 hours. - What else? -I just want to ask about my wound, What will I expect to my wound and how can I prevent infection just in case? - Wound infection will slow the healing of your -How will I prevent that? What is wound. Signs and symptoms include wound is the proper way of handling my warm to touch, malallignment of wound edges and wound? purulent drainage. Other signs of infection include fever and malaise. - That’s my job. I will show you on how to - why do we have to do this assemble the equipment and the steps and techniques on proper wound cleansing and dressing so that you will be doing this on your own - it’s really a value then when you go home. With this you will minimize your possible risk of acquiring infection - (patient listen attentively) - Now I will show you on how to assemble the equipment and show the steps and techniques on proper wound cleansing and dressing. These are the materials: 1.Betadine solution 2. Cotton buds 3. Bactroban ointment 4. Sterile gauze 5. Surgical tape 6. Clean scissor The steps: Wash hands before and after cleansing the wound. Use antiseptic such as alcohol before touching the wound. Use cotton balls with betadine in cleaning the wound from the wound in an outward direction to avoid transferring of microorganisms/ bacteria Use cotton buds to apply bactroban ointment to -Now I understand, I will also asked my husband to watch, listen and if he could assist you so that he may know how to do this when we get home. the wound from top to bottom. Use sterile gauze to cover the wound. Be sure that the wound is covered entirely with the sterile dressing. Place surgical tape to secure the dressing and in the opposite direction from the body action. - What else do you want to know? -My wound is quite big. Is there possibilities that I will have complications? -Yes there are possible complications of operative wound. Aside from infection, it also bleeds and it may open. If not cared well. Well, all you have to do when bleeding occurs is that you must apply pressure dressing to the wound and go to the nearest hospital. If it opens, the wound should be quickly supported by large sterile dressing soaked in sterile saline. Notify the doctor then go to the hospital. - Anyway I will provide you a written instruction on how to handle such cases and I will also give you the phone number of the hospital so that you can call immediately. - Here is your schedule for your follow up treatment. Go back here on Feb. 23, 2008 at 10am at Rosario Memorial Hospital building 2 room 201. - Thank you very much also. But before I will end our session. Is it okay with you if I will ask you few questions? -What are again the signs and symptoms of wound infection? - What will I do just in case -Okay I really appreciate that. Thanks a lot. -Thank you very much. This is really a big help. - Yes of course. -What is the purpose of wound cleansing and - fever, the wound will have dressing? purulent discharge and it may be warm to touch. - Before you leave tomorrow, will it be possible if - to prevent wound infection and you and your husband will demonstrate to me possible complications. wound cleansing and dressing? But of course I - Oh yes of course. That would be will be there to guide and supervise you. great! - on feb. 23 at 10 am here in the - Okay, When is your Check-up? hospital at 2nd floor room201. -Okay then. So thank you very much. I know you - Yes. Thank you very much. really understood what I’ve thought you. That ends our session. - Have a good day! - okay! CONCLUSION Understanding one’s disease is the best way for us to have the best knowledge and health teachings that we could give to our patient. It is through this case study that we realized that presence of an infirmity affects the totality of one person. One might face/accept it very well but others might not. It is our duty as health care providers to take the initiative to find and provide for possible explanations/ support that our clients need. As for this case- Post partum hemorrhage, the pathophysiology of the disease is the main key to have better understanding of the disease process itself. With this, risk factors are modified; possible preventions are given and proper treatments and cure are provided. It is recommended that: • Thorough assessment including health histories of the patient must be done to identify the etiology and manifestations of the problem. • Reading of various literatures about the disease will provide additional information of the problem. • Collaboration with other health care providers such us the attending physician and other therapist help to gain better understanding of the disease. • Health teachings are to be provided to patients in a less technical way/ or in a simple way that they can understand. It is well appreciated by the patient if visual presentations/ pamphlets are to be given for them to read. • The best way for the nurse to be efficient in his/her care to client is to gain the trust of the patient and make his/her presence be felt always by the patient in times he/she needs it. III. BIBLIOGRAPHY/ REFERENCES Books 1. Maternal and Child Health Nursing: Care of the Childbearing and Childrearing Fmily volume 1 5th edition. By Adele Pilliteri 2. Foundation of Maternal- Newborn Nursing 4th edition. By Sharon Smith Murray, Emily Stone Mc Kinney 3. Maternal and Child Nursing Care 2nd edition. By Marcia L. London, Patricia W. Ladewig, Jane W. Ball, Ruth Bindler. 4. Progress in Obstetric and Gynecology. Edited by John Studd, Seang Lin Tan, Frank D. Chervenak 5. Fundamentals of Nursing, Concepts, Process, and Practice updated 5th edition By Barbara Kozier, Glenora Erb, Kathleenn Blais, Judith M. Wilkinson 6. Physiology and Anatomy 9th edition by. Esther m. Greisheimer, Mary P. Weideman 7. Nurse’s Drug Handbook 2004. vol 1 and 2, by Wilson et. Al. Electronic Media file://F:\eMedicine-Postpartum Hemorrhage article by John R. Smith, Md, FRSC,FAC file://F:\the Reproductive system.htm file://F:\Postpartum Hemorrhage.htm file://F:\women’s health Advisor 2005_Severe Postpartum Bleeding MicrosoftEncarta 2006 HOLY ANGEL UNIVERSITY ANGELES CITY MASTER OF ARTS IN NURSING NURSING CONCEPT 1 ADVANCE MATERNAL AND CHILD HEALTH CARE A CASE STUDY ON POSTPARTUM HEMORRHAGE SUBMITTED BY: CATHERINE P. LANSANG SUBMITTED TO: MRS. ELIEZER DIZON