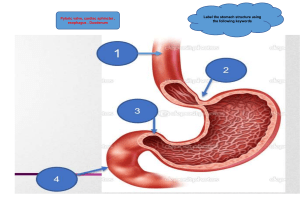
ACHALASIA PRESENTED BY CHARITY BANDA BSc 4TH YEAR STUDENT UNZA INTRODUCTION Achalasia is a disorder of the oesophagus where it loses the ability to move food along. The valve at the end of the oesophagus also fails to open and allow food to pass into the stomach CONT’ As a result, food gets stuck in the esophagus and is often brought back up. A ring of muscle called the lower esophageal (cardiac) sphincter keeps the opening from the esophagus CONT’ to the stomach shut tight to prevent Acid reflux (acidic stomach content moving back up into the oesophagus).Normally, this muscle relaxes when you swallow to allow the food to pass into the stomach CONT’ In achalasia, this muscle does not relax properly and the end of the oesophagus becomes blocked with food. It is sometimes known as cardio spasm OBJECTIVES GENERAL OBJECTIVE At the end of the lecture / discussion, students should be able to manage patients with achalasia CONT' SPECIFIC OBJECTIVES At the end of the lecture / discussion, students should be able to Define achalasia State the cause of achalasia CONT’ Explain the pathophysiology of achalasia State the Signs and symptoms of Achalasia Describe the management of patients with achalasia CONT’ Explain the signs & symptoms of achalasia Describe the management of patients with achalasia DEFINITION Achalasia is a disorder of the oesophagus that prevents normal swallowing as a result of failure of the lower oesophageal sphincter to relax allowing food to enter the stomach characterised by dysphagia, chest pain, heartburn, regurgitation and chest pains. Miller,(2003) ETIOLOGY The exact cause of achalasia is poorly understood. Researchers suspect it may be caused by a loss of nerve cells in the esophagus. There are theories about what causes this, but viral infection or autoimmune responses have been suspected. CONT’ Very rarely, achalasia may be caused by an inherited genetic disorder or infection. PATHOPHYSIOLOGY Achalasia is an inflammatory disease of unknown etiology characterized by esophageal aperistalsis and failure of LES relaxation due to loss of inhibitory nitrinergic neurons in the esophageal myenteric plexus. CONT’ Proposed causes of achalasia include gastroesophageal junction obstruction, neuronal degeneration, viral infection, genetic inheritance, and autoimmune disease. CONT’ Current evidence suggests that the initial disturbance to the esophagus, perhaps a viral infection or some other environmental factor, results in myenteric plexus inflammation. CONT’ Inflammation then leads to an autoimmune response in a susceptible population who may be genetically predisposed. Subsequently, chronic inflammation leads to destruction of CONT’ the inhibitory myenteric ganglion cells resulting in the clinical syndrome of idiopathic achalasia. Park, (2005) SIGNS AND SYMPTOMS Achalasia symptoms generally appear gradually and worsen over time. Inability to swallow (dysphagia), which may feel like food or drink is stuck in your throat CONT’ Regurgitating food or saliva Heartburn Belching Chest pain that comes and goes Coughing at night CONT’ Pneumonia (from aspiration of food into the lungs) Weight loss Vomiting MEDICAL AND SURGICAL MANAGEMENT DIAGNOSIS Oesophageal Manometry: Measures the rhythmic muscle contraction in the Medication Muscle relaxants: May be given orally or injected (Botox) directly to the oesophageal sphincter. CONT’ PROCEDURES Pneumatic dilation: A balloon is inserted into esophageal sphincter and inflated. This treatment is usually required to be repeated in about 6 years. CONT’ Heller myotomy: Muscle at the lower end of esophagus sphincter is cut down to facilitate the passage of food along the oesophagus into the stomach to check how well it relaxes when required. CONT’ Barium swallow: A chalky liquid that coats and fills the inside lining of digestive tract is given, followed by an X-ray of the upper digestive system is performed. CONT’ Endoscopy: A small, thin and flexible tube attached to the camera is inserted down the throat to check the inside of oesophagus and stomach. CONT’ Biopsy: Removal of tissue from the lower oesophageal sphincter to check for any hypertrophied musculature and absence of nerve fibres. CONT’ Treatment options are all directed at relieving the stasis caused by increased lower oesophageal sphincter (LES) pressure, non-relaxing LES and a peristaltic Oesophagus CONT’ Nissen fundoplication: Top of the stomach is wrapped to tighten muscles and prevent acid reflux. CONT’ Per-oral Endoscopic Myotomy: A tube is inserted through the mouth and an incision is made at the sphincter region to improve the passage of food into the stomach., if necessary an oesophagostomy can be performed CONT’ Self-care Chew the food well. Consume plenty of fluids with meals. Do not go to bed immediately after a meal. CONT’ Eat more frequent, smaller meals. Give the patient a semisoft bland diet and let him eat slowly and drink fluid with meals Sleeping with the head elevated CONT’ NUTRITION Take soft, easy to swallow foods like soup, mashed vegetables or porridge. Protein rich foods like chicken, soya, and fish CONT’ Ginger can also help in improving digestion and help in reducing heartburn. CONT’ Foods to avoid: Avoid citrus foods and foods that are rich in caffeine. Avoid spicy and fried foods CONCLUSION Achalasia is an esophageal motor disorder characterized by a loss of esophageal peristalsis and failure of the lower esophageal sphincter to relax in response to swallowing CONT’ The most common presenting symptoms are dysphagia to solids and liquids, regurgitation, and retrosternal pain. ASSIGNMENT Identify five problems that a patient with achalasia has and manage them using a nursing care plan. To be submitted next week Thursday. REFERENCES Harkness, A. G., and Dincher, R, J.,(1999), MEDICAL SURGICAL NURSING: TOTAL PATIENT CARE, 10th Edition, Mosby, Mousori Long, B, C.,(1993),MEDICAL SURGICAL NURSING: A NURSING CARE APPROACH,3rd Edition, Mosby, Mousori CONT’ Smeltzer, S. C., and Bare, B., (2004), MEDICAL SURGICAL NURSING, 10th Edition. Lippincott Williams and Wilkins, Hong Kong CONT’ Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. (2003). Retrieved August 6 2022 from https://medicaldictionary.thefreedictionary.com CONT’ Park, Woosuk M.D.; Vaezi, Michael F. M.D., Ph.D.. Etiology and Pathogenesis of Achalasia: The Current Understanding. American Journal of Gastroenterology: June 2005 - Volume 100 - Issue 6 - p 14041414