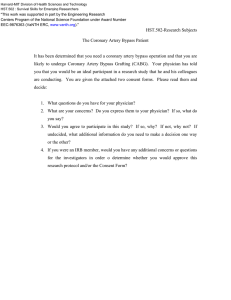
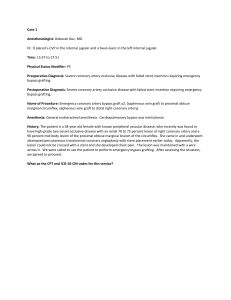
25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Official reprint from UpToDate® www.uptodate.com © 2023 UpToDate, Inc. and/or its affiliates. All Rights Reserved. Anesthesia for coronary artery bypass grafting surgery AUTHOR: Atilio Barbeito, MD, MPH SECTION EDITOR: Jonathan B Mark, MD DEPUTY EDITOR: Nancy A Nussmeier, MD, FAHA All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Jun 2023. This topic last updated: Jun 30, 2022. INTRODUCTION Coronary artery bypass grafting (CABG) is the most commonly performed cardiac surgical procedure in the United States [1]. Anesthetic planning depends partially on the expected surgical approach to revascularization. CABG is typically performed via a midline sternotomy incision with the aid of cardiopulmonary bypass (CPB). In selected patients, off-pump coronary artery bypass (OPCAB) without CPB may be accomplished via either a full sternotomy or a small anterior left thoracotomy incision, termed a minimally invasive direct coronary artery bypass (MIDCAB) approach. This topic will discuss anesthetic management of patients undergoing on-pump or off-pump CABG surgery. General considerations during the perioperative period for patients undergoing cardiac surgical procedures and cardiopulmonary bypass are also reviewed separately: ● Preoperative considerations (See "Preoperative evaluation for anesthesia for cardiac surgery".) ● Prebypass considerations • (See "Anesthesia for cardiac surgery: General principles", section on 'Monitoring'.) • (See "Anesthesia for cardiac surgery: General principles", section on 'Induction of general anesthesia'.) https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypass… 1/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate • (See "Anesthesia for cardiac surgery: General principles", section on 'Maintenance of general anesthesia'.) • (See "Anesthesia for cardiac surgery: General principles", section on 'Preparations for cardiopulmonary bypass'.) ● Cardiopulmonary bypass • (See "Initiation of cardiopulmonary bypass".) • (See "Management of cardiopulmonary bypass".) • (See "Weaning from cardiopulmonary bypass".) ● Postbypass considerations • (See "Anesthesia for cardiac surgery: General principles", section on 'Management during the postbypass period'.) • (See "Intraoperative problems after cardiopulmonary bypass".) PREBYPASS PERIOD The key steps that must be completed in the prebypass period are listed in the table and are discussed in a separate topic ( table 1). (See "Anesthesia for cardiac surgery: General principles".) The following sections note specific management considerations during the prebypass period for patients undergoing coronary revascularization. Avoidance and treatment of ischemia — It is particularly important to detect, prevent, and treat myocardial ischemia throughout the prebypass period. Monitoring for ischemia — We simultaneously and continuously monitor the electrocardiogram (ECG) to detect ST-segment depression or elevation and the transesophageal echocardiogram (TEE) to detect new regional wall motion abnormalities (RWMAs) (eg, hypokinesis or akinesis). Also, elevations in right or left ventricular (LV) filling pressures (eg, the central venous pressure [CVP] or the pulmonary artery wedge pressure [PAWP]) may indicate ischemia. These commonly employed monitoring modalities to detect ischemia have varying degrees of sensitivity and specificity [2]. (See "Anesthesia for cardiac surgery: General principles", section on 'Monitoring'.) We conduct an initial comprehensive prebypass TEE examination , followed by continuous use of the TEE to monitor for ischemia, as well as monitoring ventricular function and volume [3-5]. https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypass… 2/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Regional wall motion abnormalities indicating ischemia ( figure 1 and figure 2), as well as global left and right ventricular function are assessed. Details are described in a separate topic. (See "Anesthesia for cardiac surgery: General principles", section on 'Monitoring with transesophageal echocardiography' and "Anesthesia for cardiac surgery: General principles", section on 'Initial transesophageal echocardiography examination'.) Maintaining hemodynamic goals — Myocardial oxygen (O2) supply is determined by the oxygen content in the blood (hemoglobin level and saturation) and by coronary blood flow. Myocardial O2 demand is determined by factors that influence myocardial work (heart rate, myocardial wall stress, and contractility). (See "Angina pectoris: Chest pain caused by fixed epicardial coronary artery obstruction", section on 'Pathophysiology of myocardial ischemia'.) Hemodynamic and physiologic goals are prevention of ischemia by providing optimal myocardial O2 supply and minimizing demand ( table 2). (See "Anesthesia for noncardiac surgery in patients with ischemic heart disease", section on 'Prevention of ischemia' and "Anesthesia for noncardiac surgery in patients with ischemic heart disease", section on 'Treatment of ischemia'.) Specific hemodynamic goals include: ● Blood pressure (BP) is maintained within 20 percent of baseline (typically, a mean arterial BP 75 to 95 mmHg and/or diastolic BP 65 to 85 mmHg). ● A low to normal heart rate (HR) (eg, 50 to 80 beats per minute [bpm]) is maintained. Tachycardia compromises both oxygen supply and demand ( figure 3). ● Tachycardia with hypotension is typically treated by administering bolus doses of a pure alpha-1 agonist agent (eg, phenylephrine 50 to 100 mcg boluses or a phenylephrine infusion ( table 3)) to restore normal blood pressure. ● Tachycardia with hypertension is treated by increasing anesthetic depth (eg, administering a bolus dose of a rapid-acting opioid such as fentanyl 50 to 250 mcg or propofol 10 to 50 mg, or increasing the concentration of a volatile anesthetic agent) if the likely cause is pain or inadequate anesthesia. If anesthetic agents are not effective, small boluses of a beta blocker (eg, esmolol, metoprolol, or labetalol) or an infusion of nitroglycerin are typically administered ( table 4). ● Fluid administration is restricted, which helps to avoid fluid overload with resultant LV distention and increased wall stress. (See "Anesthesia for cardiac surgery: General principles", section on 'Prebypass fluid management'.) https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypass… 3/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Induction and maintenance of general anesthesia — The goals of general anesthetic induction and maintenance are to produce and maintain unconsciousness, attenuate the hemodynamic responses to endotracheal intubation and surgical stimulation, and prevent or treat hemodynamic changes that lead to myocardial oxygen imbalance and ischemia. Hemodynamic manipulation is typically required in patients with ischemic heart disease to achieve a simultaneous state of unconsciousness while maintaining a favorable myocardial oxygen balance. Severe pain and endogenous catecholamine release during initial incision and subsequent sternotomy necessitate adequate depth of general anesthesia to prevent tachycardia and hypertension. Subsequently, it is appropriate to reduce anesthetic doses to avoid hypotension during the periods of reduced surgical stimulation that typically follow sternotomy. (See "Anesthesia for cardiac surgery: General principles", section on 'Induction of general anesthesia' and "Anesthesia for cardiac surgery: General principles", section on 'Maintenance techniques'.) Positioning — After sternotomy, placement of a sternal retractor is necessary for harvesting the internal thoracic or internal mammary artery (IMA) (see 'Incision, sternotomy, and harvesting of venous and arterial grafts' below). Retractor positioning is closely observed since the steel post attaching it to the operating table may compress the upper arm causing radial nerve injury, and may also be associated with brachial plexus injury [6-8]. In addition, when the retractor lifts the sternum, the patient's head may be lifted off the supporting head cushion, particularly in an older patient who has cervical spine arthritis. If this occurs, the retractor should be adjusted or the patient's head should be repositioned with additional pillow support. Other positioning considerations are discussed in a separate topic. (See "Anesthesia for cardiac surgery: General principles", section on 'Patient positioning'.) Incision, sternotomy, and harvesting of venous and arterial grafts — Incision, sternotomy, harvesting of peripheral vein(s) and/or a peripheral artery, dissection to free the IMA from the chest wall, and exposure of the heart and great vessels are the fundamental surgical steps that precede aortic and venous cannulation. CARDIOPULMONARY BYPASS Initiation, management, and weaning from cardiopulmonary bypass (CPB) are discussed in separate topics: ● (See "Initiation of cardiopulmonary bypass".) ● (See "Management of cardiopulmonary bypass".) ● (See "Weaning from cardiopulmonary bypass".) https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypass… 4/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate POSTBYPASS PERIOD Key steps for any cardiac surgical procedure in the period immediately after cardiopulmonary bypass (CPB) include venous and arterial decannulation, reversal of anticoagulation with protamine administration, insertion of temporary or backup epicardial pacing wires, and reinfusion of pump blood ( table 1). Hemodynamic stability must be maintained after weaning from CPB. Cardiovascular problems that result in hypotension are identified and treated ( table 5 and table 3). (See "Intraoperative problems after cardiopulmonary bypass", section on 'Cardiovascular problems'.) Recognition and management of other intraoperative problems that may occur during the postbypass period are discussed separately. (See "Intraoperative problems after cardiopulmonary bypass".) Postbypass transesophageal echocardiography — Transesophageal echocardiography (TEE) examination immediately after coronary artery bypass grafting (CABG) surgery emphasizes the following aspects [3,4,9]: ● Global left ventricular (LV) and right ventricular (RV) function are evaluated. ● LV regional wall motion abnormalities (RWMAs) are documented as part of the overall assessment of the adequacy of revascularization in territories of myocardium perfused by each of the major coronary arteries supplying the LV ( figure 1 and figure 2). Previously ischemic or hibernating myocardium may show improved function in the early postbypass period. However, myocardial stunning is common and consequently, myocardial segments that had abnormal contraction in the prebypass period may remain impaired even after adequate coronary blood flow has been restored. Significant deterioration of regional wall motion in previously normal myocardial segments may indicate a technical problem with a coronary graft (eg, poor quality of a bypass graft anastomosis, kinking, vasospasm, or embolization of air or microparticulate debris into the graft) ( movie 1). Poor graft flow can be confirmed by a Doppler flow probe applied to the graft. ST-segment changes on the electrocardiogram (ECG) or hypotension with low cardiac output may also be noted. Detection of such problems allows surgical correction prior to leaving the operating room. (See "Intraoperative problems after cardiopulmonary bypass", section on 'Surgical or technical problems'.) https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypass… 5/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate In patients who require ventricular pacing after CPB, a distinct septal motion abnormality termed "septal bounce" is often observed; this occurs due to the abnormal pattern of ventricular depolarization that accompanies RV epicardial pacing ( movie 2). Septal bounce can be distinguished from a true RWMA because septal thickening persists during ventricular pacing but is absent when the septum is ischemic. If this is difficult to discern visually, a brief pause in ventricular pacing may be helpful. New or worsening mitral regurgitation (MR) in the postbypass period should prompt a thorough evaluation for LV RWMAs indicating an ischemic cause of the MR. ● LV and RV chamber sizes are assessed to determine intravascular volume status ( movie 3). This is important because CVP and PAP measurements are poor predictors of intravascular volume and fluid responsiveness [10]. (See "Intraoperative transesophageal echocardiography for noncardiac surgery", section on 'Volume status'.) ● Hypotension after myocardial revascularization may occasionally be caused by dynamic left ventricular outflow tract (LVOT) obstruction with systolic anterior motion (SAM) of the mitral valve anterior leaflet [11]. ● If aortic dissection is suspected following decannulation (eg, in a patient with a calcific or diffusely atheromatous ascending aorta, or one who develops postbypass hypotension that is unresponsive to treatment), the ascending aorta is evaluated to identify this potentially fatal complication ( image 1). ● Adequacy of any additional surgical repair (eg, repair or replacement of a cardiac valve) is assessed. Additional considerations for the postbypass TEE examination are discussed separately. (See "Anesthesia for cardiac surgery: General principles", section on 'Postbypass transesophageal echocardiography'.) TEE is also used for continuous monitoring throughout the postbypass period to assess ventricular volume and function, and to detect development of hypovolemia, hypervolemia, or low systemic vascular resistance [4]. (See "Anesthesia for cardiac surgery: General principles", section on 'Monitoring with transesophageal echocardiography'.) Transport and handoff in the intensive care unit — Preparations, transport, and handoff in the intensive care unit are addressed separately. (See "Handoffs of surgical patients", section on 'Operating room to intensive care unit' and "Anesthesia for cardiac surgery: General principles", section on 'Transport and handoff in the intensive care unit'.) https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypass… 6/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Further details regarding postoperative complications after on-pump or off-pump CABG surgery are addressed in the following topics [12]: ● (See "Early cardiac complications of coronary artery bypass graft surgery".) ● (See "Early noncardiac complications of coronary artery bypass graft surgery".) ● (See "Off-pump and minimally invasive direct coronary artery bypass graft surgery: Clinical use".) OFF-PUMP CORONARY ARTERY BYPASS SURGERY General considerations — Off-pump coronary artery bypass graft surgery (OPCAB) refers to coronary artery bypass grafting (CABG) without the use of cardiopulmonary bypass (CPB). This technique avoids potential morbidity associated with aortic cannulation and cross-clamping (eg, embolism of aortic plaque with consequent stroke), and with use of CPB (eg, systemic inflammatory response, platelet activation, fibrinolysis, bleeding, vasodilatory shock). (See "Intraoperative problems after cardiopulmonary bypass".) Outcomes such as death, cardiovascular events, and need for revascularization are no better and may be worse in many patients undergoing OPCAB compared to on-pump CABG [13-15] (see "Off-pump and minimally invasive direct coronary artery bypass graft surgery: Clinical use", section on 'Outcomes'). However, OPCAB is often selected for patients at high risk for stroke due to extensive atheromatous involvement of the ascending aorta. (See "Off-pump and minimally invasive direct coronary artery bypass graft surgery: Clinical use", section on 'Patient selection'.) OPCAB is usually accomplished via a standard midline sternotomy incision. In some cases, a small left anterior thoracotomy incision (termed minimally invasive direct coronary artery bypass [MIDCAB]) is suitable to approach an anterior coronary vessel, typically the left anterior descending artery [16]. (See "Minimally invasive coronary artery bypass graft surgery: Definitions and technical issues".) Details regarding patient selection, surgical techniques, advantages, disadvantages, and outcomes for OPCAB and MIDCAB are available in other topics. (See "Minimally invasive coronary artery bypass graft surgery: Definitions and technical issues" and "Off-pump and minimally invasive direct coronary artery bypass graft surgery: Clinical use".) Anesthetic management — Anesthetic management for OPCAB differs from management for on-pump CABG in the following ways: https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypass… 7/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate ● Less systemic anticoagulation is required (typically 100 to 200 units/kg of intravenous [IV] heparin, approximately one-third of the dose employed for CPB). Activated whole blood clotting time (ACT) is checked before partial clamping of the aorta or other vessels (eg, the internal mammary artery [IMA]). An ACT value of 250 to 300 seconds is targeted in most institutions, although evidence defining optimal ACT for OPCAB is lacking. This level of anticoagulation balances ischemic and hemorrhagic complications, particularly in patients recently receiving antiplatelet agents. ● We do not routinely administer an antifibrinolytic agent (eg, epsilon-aminocaproic acid [EACA] or tranexamic acid [TXA]) after systemic heparinization for OPCAB surgery. TXA reduces exposure to allogeneic RBC in OPCAB, but an optimal dosing regimen has not been established. In addition, its impact on clinically relevant outcomes in this setting is unknown [17,18]. ● Fluid loading (typically 15 to 20 mL/kg) to provide optimal preload is employed to maintain hemodynamic stability during coronary artery grafting and manipulation, rotation, and lifting of the heart required during OPCAB [19]. This is in contrast to the fluid restriction employed during the prebypass period for patients undergoing CABG surgery with CPB. (See "Anesthesia for cardiac surgery: General principles", section on 'Prebypass fluid management'.) The Trendelenburg (head down tilt) position is also frequently used to improve preload during off-pump manipulation of the heart [20]. (See "Patient positioning for surgery and anesthesia in adults", section on 'Trendelenburg'.) ● Vasoactive infusions (eg, phenylephrine and/or norepinephrine ( table 3)) are typically necessary to maintain hemodynamic stability during off-pump periods of manipulation of the heart [19]. In particular, marked hemodynamic instability is noted with displacement of the heart during mobilization for posterior coronary targets [19,21]. Constant communication between the surgical and anesthesiology teams is necessary to recognize and aggressively treat instability (eg, with adjustments in the positioning of the heart and vasoactive infusion management) [19]. ● Atrial pacing is used as a means of enhancing arterial blood pressure and cardiac output, especially when preoperative beta blockade-induced bradycardia is present [22]. ● Transesophageal echocardiography is particularly helpful to differentiate between hemodynamic instability due to myocardial ischemia (presenting as regional wall motion abnormalities [RWMAs] in the distribution of the coronary artery undergoing https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypass… 8/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate revascularization) compared with restricted chamber filling resulting from external compression of the heart [19,23]. ● There may be increased risk for myocardial ischemia after revascularization during the intraoperative and early postoperative periods since the heart was not protected from ischemia with CPB and administration of cardioplegia. Thus, close continuous monitoring of the electrocardiogram (ECG) and TEE images (while the TEE probe remains in place) for ischemic changes is necessary [19]. ● Normothermia should be maintained during the intraoperative period. In one study of 1714 patients undergoing OPCAB, moderate-to severe hypothermia (<35.5°C) at the time of admission to the postoperative intensive care unit was associated with a higher mortality risk compared with those who were normothermic (adjusted hazard ratio [HR] 2.03, 95% CI 1.41-2.93) [24]. ● In some patients, it may be necessary to convert an OPCAB procedure to on-pump CABG with CPB due to intractable hemodynamic instability, malignant arrhythmias, global ventricular ischemia, and/or technical difficulty with adequate exposure and mobilization of target coronary vessels [19,25]. SOCIETY GUIDELINE LINKS Links to society and government-sponsored guidelines from selected countries and regions around the world are provided separately. (See "Society guideline links: Coronary artery bypass graft surgery".) SUMMARY AND RECOMMENDATIONS ● Induction and maintenance of anesthesia – Goals of general anesthetic induction and maintenance during coronary artery bypass grafting (CABG) surgery are to produce and maintain unconsciousness, attenuate the hemodynamic responses to endotracheal intubation and surgical stimulation, and prevent or treat hemodynamic changes that lead to myocardial oxygen imbalance and ischemia. Severe pain and endogenous catecholamine release during initial incision and subsequent sternotomy necessitate adequate depth of general anesthesia to prevent tachycardia. Subsequently, it is appropriate to reduce anesthetic doses to avoid hypotension during the periods of reduced surgical stimulation that typically follow sternotomy. (See 'Induction and maintenance of general anesthesia' above.) https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypass… 9/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate ● Avoidance and treatment of ischemia – It is particularly important to detect, prevent, and treat myocardial ischemia throughout the prebypass period. Specific hemodynamic and physiologic goals maintain optimal myocardial oxygen supply and minimize demand during induction and the prebypass periods ( table 2). (See 'Avoidance and treatment of ischemia' above.) ● Use of transesophageal echocardiography (TEE) – TEE is typically used for patients undergoing CABG to: • Conduct an initial comprehensive prebypass TEE examination, and a focused postbypass examination. (See 'Postbypass transesophageal echocardiography' above and "Anesthesia for cardiac surgery: General principles", section on 'Initial transesophageal echocardiography examination'.) • Continuously monitor for regional wall motion abnormalities (RWMAs) that may indicate ischemia ( figure 1 and figure 2 and movie 1), as well as for monitoring global ventricular function and volume status throughout the prebypass and postbypass periods. (See "Anesthesia for cardiac surgery: General principles", section on 'Monitoring with transesophageal echocardiography'.) ● Off-pump coronary artery bypass graft (OPCAB) surgery – Off-pump coronary artery bypass graft surgery (OPCAB) refers to CABG without the use of CPB. Anesthetic management differs from management for on-pump CABG in the following ways (see 'Offpump coronary artery bypass surgery' above): • Less systemic anticoagulation is required. • Antifibrinolytics are not administered. • Fluid loading (typically 15 to 20 mL/kg), Trendelenburg positioning, and vasoactive infusions (eg, phenylephrine and/or norepinephrine ( table 3)) are typically employed to maintain hemodynamic stability during surgical manipulation of the heart. ACKNOWLEDGMENT The editorial staff at UpToDate acknowledge Ryan Konoske, MD, who contributed to an earlier version of this topic review. Use of UpToDate is subject to the Terms of Use. REFERENCES https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 10/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate 1. Types of heart surgery. https://www-nhlbi-nih-gov.pbidi.unam.mx:2443/health/health-topic s/topics/hs/types (Accessed on June 28, 2016). 2. Mark JB. Multimodal detection of perioperative myocardial ischemia. Tex Heart Inst J 2005; 32:461. 3. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. Anesth Analg 2014; 118:21. 4. MacKay EJ, Zhang B, Heng S, et al. Association between Transesophageal Echocardiography and Clinical Outcomes after Coronary Artery Bypass Graft Surgery. J Am Soc Echocardiogr 2021; 34:571. 5. Metkus TS, Thibault D, Grant MC, et al. Transesophageal Echocardiography in Patients Undergoing Coronary Artery Bypass Graft Surgery. J Am Coll Cardiol 2021; 78:112. 6. Hickey C, Gugino LD, Aglio LS, et al. Intraoperative somatosensory evoked potential monitoring predicts peripheral nerve injury during cardiac surgery. Anesthesiology 1993; 78:29. 7. Chong AY, Clarke CE, Dimitri WR, Lip GY. Brachial plexus injury as an unusual complication of coronary artery bypass graft surgery. Postgrad Med J 2003; 79:84. 8. Jellish WS, Oftadeh M. Peripheral Nerve Injury in Cardiac Surgery. J Cardiothorac Vasc Anesth 2018; 32:495. 9. Yu S, Peffley S, Fabbro M 2nd, Mohammed AN. A Narrative Review of the 2020 Guidelines for Use of Transesophageal Echocardiography to Assist with Surgical Decision- Making by the Cardiac Anesthesiologist in the Operating Room. J Cardiothorac Vasc Anesth 2022; 36:258. 10. Marik PE, Cavallazzi R. Does the central venous pressure predict fluid responsiveness? An updated meta-analysis and a plea for some common sense. Crit Care Med 2013; 41:1774. 11. Owais K, Mahmood F, Khabbaz KR, Matyal R. Systolic Anterior Motion after Myocardial Revascularization-The Unusual Suspect. J Cardiothorac Vasc Anesth 2018; 32:1825. 12. Moazzami K, Dolmatova E, Maher J, et al. In-Hospital Outcomes and Complications of Coronary Artery Bypass Grafting in the United States Between 2008 and 2012. J Cardiothorac Vasc Anesth 2017; 31:19. 13. Lamy A, Devereaux PJ, Prabhakaran D, et al. Five-Year Outcomes after Off-Pump or OnPump Coronary-Artery Bypass Grafting. N Engl J Med 2016; 375:2359. 14. Shroyer AL, Hattler B, Wagner TH, et al. Five-Year Outcomes after On-Pump and Off-Pump Coronary-Artery Bypass. N Engl J Med 2017; 377:623. https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 11/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate 15. Quin JA, Wagner TH, Hattler B, et al. Ten-Year Outcomes of Off-Pump vs On-Pump Coronary Artery Bypass Grafting in the Department of Veterans Affairs: A Randomized Clinical Trial. JAMA Surg 2022; 157:303. 16. Winkler B, Heinisch PP, Gahl B, et al. Minimally Invasive Extracorporeal Circulation Circuit Is Not Inferior to Off-Pump Coronary Artery Bypass Grafting: Meta-Analysis Using the Bayesian Method. Ann Thorac Surg 2017; 103:342. 17. Menkis AH, Martin J, Cheng DC, et al. Drug, devices, technologies, and techniques for blood management in minimally invasive and conventional cardiothoracic surgery: a consensus statement from the International Society for Minimally Invasive Cardiothoracic Surgery (ISMICS) 2011. Innovations (Phila) 2012; 7:229. 18. Myles PS, Smith JA, Forbes A, et al. Tranexamic Acid in Patients Undergoing Coronary-Artery Surgery. N Engl J Med 2017; 376:136. 19. Bianco V, Kilic A, Gelzinis T, et al. Off-Pump Coronary Artery Bypass Grafting: Closing the Communication Gap Across the Ether Screen. J Cardiothorac Vasc Anesth 2020; 34:258. 20. Chassot PG, van der Linden P, Zaugg M, et al. Off-pump coronary artery bypass surgery: physiology and anaesthetic management. Br J Anaesth 2004; 92:400. 21. Murkin JM. Hemodynamic changes during cardiac manipulation in off-CPB surgery: relevance in brain perfusion. Heart Surg Forum 2002; 5:221. 22. Gulielmos V, Kappert U, Eller M, et al. Improving hemodynamics by atrial pacing during offpump bypass surgery. Heart Surg Forum 2003; 6:E179. 23. Kapoor PM, Chowdhury U, Mandal B, et al. Trans-esophageal echocardiography in off-pump coronary artery bypass grafting. Ann Card Anaesth 2009; 12:167. 24. Nam K, Jo WY, Kwon SM, et al. Association Between Postoperative Body Temperature and All-Cause Mortality After Off-Pump Coronary Artery Bypass Graft Surgery: A Retrospective Observational Study. Anesth Analg 2020; 130:1381. 25. Tsaousi G, Pitsis AA, Ioannidis GD, Vasilakos DG. A multidisciplinary approach to unplanned conversion from off-pump to on-pump beating heart coronary artery revascularization in patients with compromised left ventricular function. Crit Care Res Pract 2014; 2014:348021. Topic 90607 Version 31.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 12/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate GRAPHICS Key periods during cardiac surgery Period Prebypass period Anesthetic goals Induction and maintenance of anesthesia Maintain optimal myocardial O2 supply and minimize demand to prevent or treat ischemia Antibiotic prophylaxis Timely administration of selected antibiotics Positioning Careful arm, hand, and head positioning to avoid injuries Fluid management Restrict fluid administration since initiation of CPB causes significant hemodilution Prebypass TEE examination Assess regional LV wall motion abnormalities Assess global LV function Assess global RV function Assess structure and function of cardiac valves Evaluate thoracic aorta, interatrial septum, and left atrium with left atrial appendage Detect development of ischemia, hypovolemia, hypervolemia, or low SVR Incision and sternotomy Treat hypertension and tachycardia due to painful stimuli Harvesting of the Reduce tidal volume internal mammary artery Briefly interrupt ventilation during sternotomy to avoid lung injury Anticoagulation for CPB Administer heparin and ensure adequate anticoagulation Antifibrinolytic administration Administer antifibrinolytic agent to minimize Perfusionist Confer with perfusionist if indicated completes CPB circuit setup, (confirm with ACT) microvascular bleeding priming, testing of alarms and circuit, adherence to checklist https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 13/34 25/7/23, 19:58 Initiation of CPB Anesthesia for coronary artery bypass grafting surgery - UpToDate Aortic cannulation Reduce systolic BP to <100 mmHg to reduce risk of aortic dissection Venous cannulation Treat hypotension or initiate CPB for malignant arrhythmias Retrograde autologous priming Gradual onset of CPB to reduce hemodilution from crystalloid prime Control of O2 delivery, CO2 removal, and pump flow assumed by perfusionist Discontinue controlled ventilation and anesthetic administration via the anesthesia machine Anesthetic administration Initiate volatile anesthetic administration via vaporizer attached to CPB circuit, or use TIVA technique Discontinue cardiac support (eg, inotropic agents, IABP) Monitor raw and/or processed EEG and expired anesthetic gas from the oxygenator to prevent awareness Monitor neuromuscular function; administer NMBAs to prevent movement or shivering Placement of aortic crossclamp and administration of cardioplegia Ensure complete myocardial arrest (absence of ECG electrical activity) Placement and monitoring of TEE assessment of coronary sinus catheter placement for retrograde cardioplegia delivery coronary sinus catheter and LV vent Maintenance of Cooling CPB TEE monitoring for aortic insufficiency and LV distension during antegrade cardioplegia delivery Monitor coronary sinus pressure TEE assessment of correct LV vent placement and effective LV decompression Maintain temperature gradient between venous inflow and arterial outlet <10°C Maintenance Maintain MAP ≥65 mmHg (or ≥75 mmHg for patients with cerebrovascular disease or severe aortic atherosclerosis) Monitor temperature at oxygenator arterial outlet temperature (surrogate for cerebral temperature) and other sites (eg, nasopharyngeal, bladder, blood) Maintain Hgb ≥7.5 g/dL (Hct ≥22%); suggest hemoconcentration if Hgb <7.5 g/dL, then transfuse https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 14/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate PRBC if necessary Maintain SvO2 ≥75%; suggest increase in pump flow if SvO2 <75% Rewarming Slow rewarming ≤0.5°C/minute, with temperature gradient between venous inflow and arterial outlet ≤4°C Avoid hyperthermia; target temperature is 37°C at nasopharyngeal site and 35.5°C at bladder site Monitor for awareness or return of neuromuscular function Removal of aortic crossclamp Weaning from Refer to UpToDate topic on weaning from cardiopulmonary bypass (CPB) CPB Post-bypass Defibrillate and administer antiarrhythmic agents if necessary to treat ventricular fibrillation Venous decannulation Ensure initial reinfusion of blood drained from the venous tubing into the pump reservoir in 50- to 100-mL aliquots TEE assessment for adequate ventricular filling Anticoagulation reversal, pump suckers turned off, intravascular vents removed Administer protamine slowly, treat protamine reactions Aortic decannulation Reduce systolic BP to <100 mmHg to reduce risk of aortic dissection Pacemaker management Ensure optimal pacemaker settings Postbypass TEE examination Assess regional LV wall motion abnormalities Ensure complete reversal of anticoagulation Assess global LV function Assess global RV function Monitor LV and RV chamber sizes to assess intravascular volume status Evaluate the ascending aorta to rule out dissection Hemostasis Ensure absence of residual heparin Check point-of-care and laboratory tests of coagulation if bleeding persists Manage anemia, thrombocytopenia, and coagulopathy if necessary Chest closure Observe for RV compression and dysfunction, coronary graft compromise, pacing wire displacement, or lung https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 15/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate compression Transport to ICU and handover Ensure optimal patient condition prior to transport Immediate availability of airway equipment, emergency drugs, and defibrillator on the transport bed Continuous monitoring of ECG, SpO2, and intraarterial BP during transport Use of a formal protocol for communication and transfer of technology during handover to the ICU team O2: oxygen; CPB: cardiopulmonary bypass; TEE: transesophageal echocardiography; LV: left ventricular; RV: right ventricular; SVR: systemic vascular resistance; ACT: activated clotting time; BP: blood pressure; CO2: carbon dioxide; IABP: intraaortic balloon pump; TIVA: total intravenous anesthesia; EEG: electroencephalography; MAP: mean arterial pressure; Hgb: hemoglobin; Hct: hematocrit; SVO2: mixed venous oxygen saturation; ECG: electrocardiogram; SpO2: peripheral oxygen saturation; ICU: intensive care unit. Graphic 108173 Version 2.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 16/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate LV perfusion territories The regional distribution of LV segmental wall motion abnormalities detected by TEE can be used to help determine the location of disease within the coronary arteries. The diagram displays the typical territories of myocardium perfused by each of the major coronary arteries supplying the LV in the TEE mid-esophageal four-chamber view, TEE mid-esophageal two-chamber view, TEE mid-esophageal long-axis view, and TEE transgastric LV short-axis view. Anatomic variations and coronary collateral flow may produce different patterns of coronary perfusion in individual patients. LV: left ventricle/left ventricular; TEE: transesophageal echocardiography; LAD: left anterior descending; Cx: circumflex; RCA: right coronary artery. Modified from: Shanewise JS, Cheung AT, Aronson S, et al. ASE/SCA guidelines for performing a comprehensive intraoperative multiplane transesophageal echocardiography examination: recommendations of the American Society of Echocardiography Council for Intraoperative https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 17/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Echocardiography and the Society of Cardiovascular Anesthesiologists Task Force for Certification in Perioperative Transesophageal Echocardiography. J Am Soc Echocardiogr 1999; 12:884. Graphic 104112 Version 2.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 18/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate LV segmental anatomy The regional distribution of myocardial ischemia can be detected as segmental LV wall motion abnormalities by TEE. The entire LV in the 17segment model can be imaged in long-axis using a combination of the TEE mid-esophageal four-chamber view (a), TEE mid-esophageal two-chamber view (b), and TEE mid-esophageal long-axis view (c). Alternatively, all 17 LV wall segments can be imaged using the TEE transgastric LV short-axis views at the levels of the LV base (d), papillary muscles (e), and apex (not shown). Alternatively, an earlier version of a 16-segment LV model that excludes the apical cap is often used for TEE studies. LV: left ventricle/left ventricular; TEE: transesophageal echocardiography. https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 19/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Modified from: Shanewise JS, Cheung AT, Aronson S, et al. ASE/SCA guidelines for performing a comprehensive intraoperative multiplane transesophageal echocardiography examination: recommendations of the American Society of Echocardiography Council for Intraoperative Echocardiography and the Society of Cardiovascular Anesthesiologists Task Force for Certification in Perioperative Transesophageal Echocardiography. J Am Soc Echocardiogr 1999; 12:884. Graphic 104113 Version 2.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 20/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Myocardial ischemia: Factors governing O2 supply and demand Factors that ↓ O2 supply Factors that ↑ O2 demand ↑ Heart rate* ↑ Heart rate* ↓ Arterial O2 content ↑ LV systolic wall stress (LV afterload) ↓ Hemoglobin ↑ Systolic blood pressure (SBP) ↓ SaO2 ↑ LV chamber size (↑ LV end-diastolic ↓ Coronary blood flow ↓ Coronary perfusion pressure (CPP) = diastolic blood pressure (DBP) – LV enddiastolic pressure (LVEDP) volume [LVEDV]) ↓ LV wall thickness ↑ Contractility ↓ DBP ↑ LVEDP ↑ Coronary vascular resistance A number of clinical conclusions should be drawn from this table. First, increased heart rate (tachycardia) is harmful because it both decreases oxygen supply and increases oxygen demand. Second, severe anemia or severe hypoxemia is harmful because of reduced supply. Third, increases in LVEDV and LVEDP, which often (but not always) occur together, are harmful because of both decreased supply (decreased CPP) and increased demand (afterload). Fourth, the ideal blood pressure is patient-dependent, but severe hypotension is likely to reduce supply (DBP) more than its beneficial effect on demand (SBP). But, conversely, severe hypertension typically increases demand (afterload) more than it improves supply (DBP). Left ventricular (LV) afterload is best defined as LV systolic wall stress. Based on Laplace's law, LV systolic wall stress = (LV systolic pressure × LV end-diastolic radius) / 2 × LV wall thickness. Therefore, factors that increase LV afterload include increased SBP and/or increased LV radius or LVEDV. Note that the normal (chronic) compensatory response to these hemodynamic changes is for the LV walls to thicken or hypertrophy, which works to normalize systolic wall stress, but requires months or years for change to occur. Therefore, of the hemodynamic variables that often change during the perioperative period, increases in SBP or LVEDV are harmful, owing to their deleterious effects on LV afterload. O2: oxygen; SaO2: oxygen saturation of arterial blood; LV: left ventricular; SBP: systolic blood pressure. * Affects both supply and demand. Original figure modified for this publication. Royster RL, Butterworth JF IV, Groban L, et al. Cardiovascular Pharmacology. In: Essentials of Cardiac Anesthesia. Kaplan JA (Ed), Saunders Elsevier, Philadelphia 2008. Illustration used with the permission of Elsevier Inc. All rights reserved. https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 21/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Graphic 91907 Version 8.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 22/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Total time spent in diastole Total time spent in diastole each minute plotted as a function of heart rate in beats per minute. The reduction in diastolic interval leads to diminished time for diastolic coronary artery blood flow. Reproduced with permission from: Green MS, Okum GS, Horrow JC. Anesthetic Management of Myocardial Revascularization In: A Practical Approach to Cardiac Anesthesia, 5th ed, Hensley FA, Martin DE, Gravlee GP (Eds), Lippincott Williams & Wilkins, Philadelphia 2013. Copyright © 2013 Lippincott Williams & Wilkins. Graphic 94174 Version 9.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 23/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Vasopressors and inotropic agents used in the operating room: Adult dosing* ¶ Drug Ephedrine Functional class (predominant receptor or mechanism of action) Inotrope/chronotrope/vasopressor (alpha1-adrenergic receptor agonist; beta1- and beta2adrenergic receptor agonist) Bolus dose 5 to 10 mg boluses Infusion dose N/A Comm Tachyphyl occur with repeated d to indirect postsynap release of norepinep Cardiovas effects att by drugs t ephedrine into adren nerves (eg or those th deplete norepinep reserves (e reserpine) Administe extreme c (eg, in sma increment of 2.5 mg) patients u monoamin oxidase (M inhibitors methamp since exag hypertens responses threatenin dysrhythm occur Phenylephrine Vasopressor (alpha1-adrenergic receptor agonist) 50 to 100 10 to 100 mcg boluses mcg/minute Often sele treat hypo or https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 24/34 25/7/23, 19:58 Norepinephrine Anesthesia for coronary artery bypass grafting surgery - UpToDate Inotrope/vasopressor (alpha1- and beta1-adrenergic receptor agonist) (may begin infusion if repeated bolus doses are necessary) 0.1 to 1 mcg/kg/minute 4 to 8 mcg (may begin infusion if repeated bolus doses are necessary) 1 to 20 mcg/minute normal or HR is pres Genetic polymorp lead to va individual responses or 0.01 to 0.3 mcg/kg/minute Often sele first-line a during no surgery, p for treatm most type Norepinep mcg is approxima equivalent potency to phenyleph mcg Periphera extravasat high conce may cause damage Epinephrine Inotrope/chronotrope/vasopressor (alpha1-adrenergic receptor agonist; beta1- and beta2adrenergic receptor agonist) 4 to 10 mcg initially; up to 100 mcg boluses may be 1 to 100 mcg/minute or 0.01 to 1 mcg/kg/minute used when initial response is inadequate Note changing effects across dose range: Low doses have primarily beta2adrenergic effects at 1 to 2 mcg/minute or 0.01 to 0.02 mcg/kg/minute First-line t for cardiac and for an May be administe or via an endotrach in emerge Low doses bronchodi effects an cause arte vasodilatio decreased Intermedi cause incr HR and BP High dose vasoconst https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 25/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Intermediate doses have primarily beta1- and beta2adrenergic effects at 2 to 10 mcg/minute or 0.02 to 0.1 mcg/kg/minute with possi hypertens adverse m effects Individual responses related eff variable High doses have primarily alpha1adrenergic effects at 10 to 100 mcg/minute or 0.1 to 1 mcg/kg/minute Vasopressin Vasopressor (vasopressin1 and vasopressin2 receptor agonist) 1 to 4 units 0.01 to 0.04 units/minute Doses >0.04 units/minute up to 0.1 units/minute are reserved for salvage therapy (ie, failure to achieve adequate BP goals with other vasopressor agents) ¶ Effective f treatment hypotensi refractory administra catecholam sympatho such as ep phenyleph norepinep No direct e HR Little effec can cause splanchnic vasoconst Individual responses related eff variable Periphera extravasat cause skin Dopamine Inotrope/vasopressor/dosedependent chronotropy (dopaminergic, beta1-, beta2-, and N/A 2 to 20 mcg/kg/minute Low doses exacerbat https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 26/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate alpha1-adrenergic receptor agonist) Note changing effects across dose range: Low doses have primarily dopaminergic effects at <3 mcg/kg/minute hypotensi beta2 stim High dose cause vasoconst adverse m effects, an arrhythmi Intermediate doses have primarily beta1- and beta2adrenergic effects at 3 to 10 mcg/kg/minute High doses have primarily alpha1adrenergic effects >10 mcg/kg/minute Dobutamine Inotrope/vasodilator/dosedependent chronotropy (beta1and beta2-adrenergic receptor agonist) N/A 1 to 20 mcg/kg/minute Exacerbat hypotensi possible d dose-depe vasodilatio beta2 stim concurren administra potent vasoconst such as norepinep vasopress necessary Milrinone Inotrope/vasodilator (phosphodiesterase inhibitor) N/A 0.375 to 0.75 mcg/kg/minute (a (decreases rate of cyclic adenosine monophosphate [cAMP] loading dose of 50 mcg/kg over ≥10 degradation) minutes may be administered, but Exacerbat hypotensi due to vas (via phosphod inhibition) https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 27/34 25/7/23, 19:58 Isoproterenol Anesthesia for coronary artery bypass grafting surgery - UpToDate Inotrope/chronotrope/vasodilator (beta1- and beta2-adrenergic receptor agonist) N/A may be omitted to avoid hypotension) concurren administra potent vasoconst such as norepinep vasopress necessary 5 to 20 mcg/minute Exacerbat hypotensi due to dos dependen vasodilatio beta2 stim or 0.05 to 0.2 mcg/kg/minute May cause arrhythmi Not availa most setti N/A: not applicable; HR: heart rate; IV: intravenous; IM: intramuscular; BP: blood pressure; PVR: pulmonary vascular resistance. * Dose ranges are based on adult patients of average size. ¶ Refer to related UpToDate content on hemodynamic management during anesthesia and surgery. Graphic 119747 Version 4.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 28/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Drugs used to lower blood pressure in the operating room: Adult dosing* ¶ Functional Drug class (predominant receptor or mechanism) Bolus dose Infusion dose Comments Beta blocking agents – Generally avoided in patients with acute decompensated heart failure Esmolol Beta1-selective adrenergic 10 to 50 mg, which may be receptor blockade repeated (every 5 to 15 minutes depending upon the initial dose used, the desired effect, and the patient's risk for hemodynamic decompensation) Metoprolol Beta1-selective adrenergic receptor blockade 1 to 5 mg, followed by 2.5 to 15 mg every 3 to 6 hours N/A Commonly used agent to treat suspected myocardial ischemia due to tachycardia with normal or elevated blood pressure Labetalol Blockade of Initial bolus of 5 0.5 to 2 postsynaptic alpha1- to 25 mg, which may be followed mg/minute up to a maximum Often selected as a first-line agent to adrenergic receptors and by repeated boluses every 10 of 10 mg/minute non-selective beta blockade minutes (up to 300 mg) (generally reserved for for beta1- and beta2-adrenergic receptors 50 to 300 mcg/kg/minute Rapid onset and very short duration of action Clearance is not dependent on renal or hepatic function due to rapid metabolism by plasma esterases hypertensive emergencies) treat concomitant hypertension and tachycardia Use cautiously in patients with obstructive or reactive airway disease Avoid in hyperadrenergic states (eg, pheochromocytoma https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 29/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate or cocaine or methamphetamine overdose) since beta blockade and loss of beta2-mediated vasodilation induced by labetalol can lead to severe hypertension when prior alpha1adrenergic blockade is incomplete Calcium channel blocking agents – Use cautiously in patients with increased ICP Nicardipine* Clevidipine Selective dihydropyridinetype calcium channel blocker; selective arteriolar smooth muscle relaxation 100 to 500 mcg Selective dihydropyridinetype calcium channel blocker; selective arteriolar smooth muscle relaxation N/A 5 to 15 mg/hour Predominantly arteriolar vasodilator Commonly used for neurosurgical patients Initial dose 1 to 2 mg/hour, with rapid titration up to 16 mg/hour Rapid onset and short duration of action Clearance is not dependent on renal or hepatic function due to rapid metabolism by plasma esterases Direct vasodilators (direct relaxation of vascular smooth muscle) – Generally avoided in patients with increased ICP Hydralazine Highly selective Initial bolus of vasodilation of arterial 2.5 mg followed by repeated resistance vessels boluses every 5 minutes to a N/A Minimal or no effect on the venous circulation Relatively slow onset compared with other antihypertensive maximum 20 mg agents Nitroglycerin (glyceryl Nitrodilator that causes increased 10 to 40 mcg, which may be trinitrate) release of NO, resulting in repeated and/or 10 to 200 mcg/minute or Continuous monitoring using an intra-arterial https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 30/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate smooth muscle relaxation followed by infusion 0.1 to 3 mcg/kg/minute catheter is warranted as soon as feasible, particularly if higher doses are used SL or paste forms of nitroglycerin paste (1 to 2 inches) formulations also available Nitroprusside Nitrodilator that directly releases NO, resulting in smooth muscle relaxation N/A 10 to 200 mcg/minute or 0.1 to 3 mcg/kg/minute Continuous monitoring using an intra-arterial catheter is necessary Cyanide accumulation may occur Other antihypertensive agents Fenoldopam Selective agonist for D1 dopamine receptors; binds with moderate affinity to alpha2adrenoceptors N/A Initial dose at 0.1 mcg/kg/minute titrated up to a maximum of 1.6 mcg/kg/minute Rarely used in perioperative settings Generally avoided in patients with glaucoma or increased ICP N/A: not applicable; ICP: intracranial pressure; NO: nitric oxide; SL: sublingual. * Dose ranges are based on adult patients of average size. ¶ Refer to related UpToDate content on hemodynamic management during anesthesia. Graphic 119750 Version 2.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 31/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Hemodynamic management of hypotension during and after weaning from CPB CVP PAP PADP or PAWP* Cardiac output Blood pressure LV function by TEE RV function by TEE Diagnosi Low Low Low Low Low Normal or hyperdynamic Normal or hyperdynamic Hypovolem Low or normal Low or normal Low or normal High Low Normal or hyperdynamic Normal or hyperdynamic Vasoplegia High or High Low or High Low Normal Normal or Pulmonary hypocontractile hypertensio normal ¶ normal High Normal or low Normal or high ¶ Low Low Normal Hypocontractile, often dilated Right ventricular dysfunction Normal or high Normal or high High Low Low Hypocontractile, often dilated Normal Left ventricular dysfunction CPB: cardiopulmonary bypass; CVP: central venous pressure; PAP: pulmonary artery pressure; PADP: pulmonary artery diastolic pressure; PAWP: pulmonary artery wedge pressure; LV: left ventricular; TEE: transesophageal echocardiography; RV: right ventricular. * PAWP should not be measured prior to neutralizing heparin following CPB. Initially, PADP is measured, the PADP may overestimate PAWP when patients have elevated pulmonary vascular resistance (eg, pulmonary hypertension). ¶ PADP or PAWP are indirect measures of LV filling pressure. With RV dysfunction and dilation, ventricular septal shift may increase LV filling pressure despite low or normal LV filling volume. Graphic 93595 Version 8.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 32/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Type A aortic dissection with aortic insufficiency Intraoperative TEE image of the aortic valve, aortic root, and proximal ascending aorta in a long-axis view, with color-flow Doppler imaging in diastole demonstrating severe aortic regurgitation with an acute aortic dissection. The presence of an intimal flap in the aortic root (arrowheads) is diagnostic for Stanford type A aortic dissection. Severe aortic regurgitation is present as a mosaic regurgitant jet in the LVOT caused by acute enlargement of the aortic root due to the dissection. LVOT: left ventricular outflow tract; Ao: ascending aorta; TEE: transesophageal echocardiography. Graphic 108394 Version 2.0 https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 33/34 25/7/23, 19:58 Anesthesia for coronary artery bypass grafting surgery - UpToDate Contributor Disclosures Atilio Barbeito, MD, MPH No relevant financial relationship(s) with ineligible companies to disclose. Jonathan B Mark, MD No relevant financial relationship(s) with ineligible companies to disclose. Nancy A Nussmeier, MD, FAHA No relevant financial relationship(s) with ineligible companies to disclose. Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these are addressed by vetting through a multi-level review process, and through requirements for references to be provided to support the content. Appropriately referenced content is required of all authors and must conform to UpToDate standards of evidence. Conflict of interest policy https://www-uptodate-com.pbidi.unam.mx:2443/contents/anesthesia-for-coronary-artery-bypass-grafting-surgery/print?search=Anesthesia for coronary artery bypa… 34/34