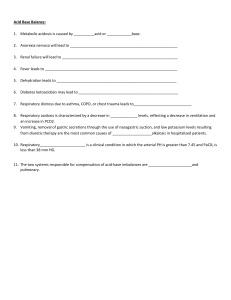
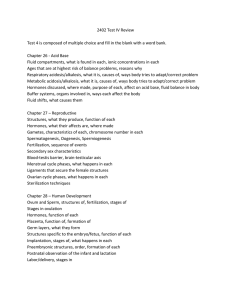
Week 1 FORTIS COLLEGE DR TARSHA STEWART Group of diseases characterized by uncontrolled and unregulated growth of cells Cancer Statistics Occurs in people of all ages Most cases are diagnosed in those over age 55 Higher in men than women Second most common cause of death in United States after heart disease Leading cause of death in people 40 to 79 years of age Both the incidence and mortality rate of cancer has been declining Incidences of lung, colorectal, breast, and oral cancer have decreased Other cancers have increased Greater than 14.5 million Americans are alive today who have a history of cancer Disease free In remission Under treatment Cancer- Carcinogens Carcinogens • • • cancer causing agents capable of producing cell alterations. Most are detoxified by protective enzymes and are excreted Failure of protective mechanisms allows them to enter a cell’s nucleus and alter DNA Carcinogens may be Chemical Radiation Viral Chemical carcinogens • Benzene • Arsenic • Formaldehyde Radiation can cause cancer in almost any human tissue Damage occurs to DNA Ultraviolet radiation is associated with melanoma and squamous and basal cell carcinoma **Sunlight is main source of UV exposure Viral carcinogens Epstein-Barr virus (EBV) • Burkitt’s lymphoma Human immunodeficiency virus (HIV) • Kaposi sarcoma Hepatitis B virus • Hepatocellular carcinoma Human papillomavirus (HPV) • Squamous cell carcinomas Preventing Promotion of Cancer To reduces the prevalence of cancer, modify at risk lifestyle habits. Promotion Characterized by reversible proliferation of altered cells Activities of promotion which are reversible: • Obesity • Smoking • Alcohol use • Dietary fat Biology of Cancer Two major dysfunctions in the process of cancer development: All cells are controlled by an intracellular mechanism that determines proliferation Cancer cells grown in culture are characterized by loss of contact inhibition. These cells: Grow on top of one another and on top of or between normal cells 1. Defective cell proliferation (growth) 2. Defective cell differentiation Defect in Cellular Proliferation Cancer Growth Latent Period Progression Metastasis May range from 1 to 40 years Characterized by • Increased growth rate of tumor • Invasiveness • Metastasis Main sites: • Brain and spine • Lungs • Liver • Adrenals • Bone Metastases - tumor cells must detach from the primary tumor and enter the circulation Length of latent period associated with mitotic rate of tissue of origin and environmental factors For disease to be clinically evident, tumor must reach a critical mass that can be detected Survive to rest in the capillary bed and adhere to capillary basement membrane Respond to growth factors, proliferate and induce angiogenesis, and evade host defenses. Four grades of abnormal cells Grade I Cells differ slightly from normal cells and are well differentiated Grade III Grade IV Cells are immature and primitive and undifferentiated Cell of origin is difficult to determine Grade II Cells are more abnormal and moderately differentiated Cells are very abnormal and poorly differentiated Classification of Cancer Cancer Staging Stage refers to the extent of your cancer, such as how large the tumor is and if it has spread. Knowing the stage of your cancer helps your doctor: understand how serious your cancer is and your chances of survival plan you the best treatment for identify clinical trials that may be treatment options for you Tumor Staging A cancer is always referred to by the stage it was given at diagnosis, even if it gets worse or spreads. New information about how a cancer has changed over time is added to the original stage. So the stage doesn't change, even though the cancer might. Immunological Defense Cytotoxic T cells • • Kill tumor cells directly Produce cytokines Natural killer cells and activated macrophages can lyse tumor cells B cells make antibodies that bind to tumor cells Cancer Treatment Curative therapy Surgery alone or periods of adjunctive systemic therapy Timeframe to “cure” may differ according to the tumor and its characteristics Control treatment Initial course and maintenance therapy Palliation goal Relief or control of symptoms Maintain quality of life Palliative care and treatment are not mutually exclusive and can take concurrently Chemotherapy Chemotherapy is Antineoplastic therapy Use of chemicals given as a systemic therapy for cancer Mainstay for most solid tumors and hematologic cancers Can offer cure, control, or palliative care Chemotherapy agents cannot distinguish between normal and cancer cell *** Side effects are result of destruction of normal cells May pose an occupational hazard Drugs may be absorbed through Skin Inhalation during preparation, transportation, andadministration Only properly trained personnel should handle cancer drugs Chemo care Myelosuppression is one of the most common effect of chemotherapy resulting in Thrombocytopenia and Neutropenia. Thrombocytopenia: Observe for signs of bleeding (e.g., petechiae, ecchymosis). Neutropenia: Take every measure to prevent infections in these patients. Hand hygiene is the mainstay of patient protection. Patients and their contacts, including health care team members, should follow handwashing guidelines. Oral care for the cancer/chemo Patient Oral assessment and meticulous intervention to keep the oral cavity moist, clean, and free of debris are essential to prevent infection and promote nutritional intake. Implementing standard oral care protocols that address prevention and management of mucositis promotes routine assessment, patient and caregiver teaching, and intervention. Routinely assess the oral cavity, mucous membranes, characteristics of saliva, and ability to swallow. Having a dentist perform all necessary dental work before starting treatment is recommended. Teach the patient to self-examine the oral cavity and how to perform oral care. Oral care should be done at least before and after each meal, at bedtime, and as needed through the day. A saline solution of 1 tsp of salt in 1 L of water is an effective cleansing agent; 1 tsp of sodium bicarbonate may be added to the oral care solution to decrease odor, ease pain, and dissolve mucin. Have the patient use a soft bristled toothbrush. Cancer Review Question 1 When caring for the patient with cancer, what does the nurse understand is the response of the immune system to antigens of the malignant cells? A. Metastasis B. Tumor angiogenesis C. Immunologic escape D. Immunologic surveillance Cancer Review Immunologic surveillance is the process in which lymphocytes check cell surface antigens and detect and destroy cells with abnormal or altered antigenic determinants to prevent these cells from developing into clinically detectable tumors When caring for the patient with cancer, what does the nurse understand is the response of the immune system to antigens of the malignant cells? A. Metastasis B. Tumor angiogenesis C. Immunologic escape D. Immunologic surveillance Cancer Review A patient with Hodgkin’s lymphoma who is undergoing external radiation therapy tells the nurse, “I am so tired I can hardly get out of bed in the morning.” Which intervention should the nurse add to the plan of care? Question 2 A.Minimize activity until the treatment is completed. B.Establish time to take a short walk almost every day. C.Consult with a psychiatrist for treatment of depression. D.Arrange for delivery of a hospital bed to the patient’s home. Cancer Review Walking programs are used to keep the patient active without excessive fatigue. A patient with Hodgkin’s lymphoma who is undergoing external radiation therapy tells the nurse, “I am so tired I can hardly get out of bed in the morning.” Which intervention should the nurse add to the plan of care? Having a hospital bed does not necessarily address the fatigue. A. The better option is to stay as active as possible while combating fatigue. B. Fatigue is expected during treatment and is not an indication of depression. C. Minimizing activity may lead to weakness and other complications of immobility. D. A Minimize activity until the treatment is completed. B Establish time to take a short walk almost every day. C Consult with a psychiatrist for treatment of depression. D Arrange for delivery of a hospital bed to the patient’s home. Cancer Review Question 3 The patient is being treated with brachytherapy for cervical cancer. What factors must the nurse be aware of to protect herself when caring for this patient? A. The medications the patient is taking B. The nutritional supplements that will help the patient C. How much time is needed to provide the patient’s care D. The time the nurse spends at what distance from the patient Cancer Review Brachytherapy-internal radiation The principles of ALARA (as low as reasonably achievable) and time, distance, and shielding are essential to maintain the nurse’s safety when the patient is a source of internal radiation. The patient is being treated with brachytherapy for cervical cancer. What factors must the nurse be aware of to protect herself when caring for this patient? A. The medications the patient is taking B. The nutritional supplements that will help the patient C. How much time is needed to provide the patient’s care D. The time the nurse spends at what distance from the patient Cancer Review A client has multiple elevated dry, rough, scaly papules on their forearms. How would these lesions be characterized? A Basal cell carcinoma B Actinic keratosis C Atypical nevi D Melanoma Cancer Review Actinic keratosis consists of: • Flat or elevated, dry, hyperkeratotic scaly papule. Often multiple. • May be rough or wartlike • Rough adherent scale on red base, which returns when removed • Often on erythematous sun-exposed area A client has multiple elevated dry, rough, scaly papules on their forearms. How would these lesions be characterized? A Basal cell carcinoma B Actinic keratosis C Atypical nevi D Melanoma Fluid and Electrolyte Imbalances CHAPTER 16 Body Water Over the Life span Body Water Over the Life span Fluids and Electrolytes Fluid Compartments Intracellular fluid (ICF) Extracellular fluid (ECF) Interstitial Intravascular (plasma) Transcellular **1 L of water weighs 2.2 pounds (1 kg) Body weight change is an excellent indicator of overall fluid volume loss or gain Electrolytes Electrolytes Substances whose molecules dissociate into ions when placed in water Cations: positively charged Anions: negatively charged Concentration of electrolytes is expressed in milliequivalents (mEq)/L Intra/Extra-cellular ICF Prevalent cation is K+ Prevalent anion is PO43− Mechanisms Mechanisms control Fluid and Electrolyte Movement Diffusion-Movement of molecules across a permeable membrane from high to low concentration Facilitated diffusionUses carrier s to help move molecules ECF Prevalent cation is Na+ Prevalent anion is Cl− Mechanisms Controlling Fluid and Electrolyte Movement Diffusion Facilitated diffusion Movement of molecules across a permeable membrane from high to low concentration Uses carrier to help move molecules Mechanisms Controlling Fluid and Electrolyte Movement Active transport Osmosis Process in which molecules move against concentration gradient Movement of water “down” concentration gradient from a region of low solute concentration to one of high solute concentration across a semipermeable membrane External energy is needed for this process Example-Sodium potassium Pump Requires no outside energy sources Mechanisms Controlling Fluid and Electrolyte Movement Osmotic pressure Measurement of Osmolality Amount of pull required to stop osmotic flow of water Calculate the plasma osmolality Osmolarity measures the total mOsm/L of solution Osmolality measures the number of mOsm/kg of water Plasma Osmolality = (2 × Na) + (BUN / 2.8) + (glucose / 18) Normal plasma osmolality is between 280 and 295 mOsm/kg Greater than 295 mOsm/kg= water deficit (hypovolemic) Less than 275 mOsm/kg= water excess (fluid excess) Osmotic Movement of Fluids The Osmolarity of the fluid around cell affects them Isotonic—same as cell interior Hypotonic—solutes less concentrated than in cells/hypoosmolar Hypertonic—solutes more concentrated than in cells/hyperosmolar Mechanisms Controlling Fluid and Electrolyte Movement Hydrostatic pressure Force of fluid in a compartment Blood pressure generated by heart’s contraction Oncotic pressure Colloid osmotic pressure Osmotic pressure caused by plasma proteins Fluid Shifts Edema is caused by Shifts of plasma to interstitial fluid Elevation of venous hydrostatic pressure Decrease in plasma oncotic pressure Elevation of interstitial oncotic pressure ******************************* First spacing— Normal distribution Second spacing— Abnormal accumulation of interstitial fluid (edema) Third spacing— Fluid is trapped where it is difficult or impossible for it to move back into cells or blood vessels>>>>>>>>>>>>>>>> Regulation of Water Balance Hypothalamic-pituitary regulation Osmoreceptors in hypothalamus sense fluid deficit or increase Deficit stimulates thirst and antidiuretic hormone (ADH) release Decreased plasma osmolality (water excess) suppresses ADH release Renal Regulation Primary organs for regulating fluid and electrolyte balance Adjusting urine volume Selective reabsorption of water and electrolytes Renal tubules are sites of action of ADH and aldosterone Adrenal cortical regulation Releases hormones to regulate water and electrolytes Glucocorticoids Cortisol Mineralocorticoids Aldosterone Regulation of Water Balance Cardiac regulation Natriuretic peptides are antagonists to the RAAS Hormones made by cardiomyocytes in response to increased atrial pressure They suppress secretion of aldosterone, renin, and ADH to decrease blood volume and pressure GI regulation Oral intake accounts for most water Small amounts of water are eliminated by GI tract in feces Diarrhea and vomiting can lead to significant fluid and electrolyte loss Gerontologic Considerations Structural changes in kidneys decrease ability to conserve water Hormonal changes include a decrease in renin and aldosterone and increase in ADH and ANP Subcutaneous tissue loss leads to increased moisture lost Fluid and Electrolyte Imbalances Fluid and Electrolyte Imbalances Directly caused by illness or disease (burns or heart failure) Result of therapeutic measures (colonoscopy prep, diuretics) Extracellular Fluid Volume Imbalances Abnormal loss of body fluids, inadequate intake, or plasma shift Dehydration -Loss of pure water without loss of sodium Fluid volume excess (hypervolemia) Excess intake of fluids, abnormal retention of fluids, or interstitial-toplasma fluid shift Clinical manifestations related to excess volume Weight gain is the most common Interprofessional Care Remove fluid without changing electrolyte composition or osmolality of ECF Diuretics Fluid restriction Restriction of sodium intake Removal of fluid to treat ascites or pleural effusion or shock Nursing Management Nursing Diagnoses Nursing Management Nursing Diagnoses ECF volume deficit Fluid imbalance Impaired cardiac output ECF volume excess Fluid imbalance Impaired gas exchange Nursing Management Nursing Implementation Daily weights Impaired tissue integrity I&O Activity intolerance Laboratory findings Cardiovascular care Acute confusion Potential complication: Hypovolemic Disturbed body image Potential complications: Pulmonary edema, ascites Nursing Management Nursing Implementation Nursing Implementation Respiratory care Patient safety Skin care-skin turgor assessment>>>>>>>>>>> Give IV fluids as ordered Carefully monitor rate of infusion Maintain adequate oral intake Assess ability to obtain adequate fluids independently, express thirst and swallow effectively Assist those with physical limitations Think Break??? Learning Assessment! A client with a sodium level of 183 is ordered to be started on a hypotonic solution. What is the most important nursing intervention for this client? A Give it slowly and monitor for signs and symptoms of cerebral edema. B Give the infusion rapidly in order to replace the Na+ loss. C Clarify doctor’s order because a hypotonic solution is contraindicated in hypernatremia D Maintain a patent IV. Think Break??? Learning Assessment! A client with a sodium level of 189 is ordered to be started on a hypotonic solution. What is the most important nursing intervention for this client? A Give it slowly and monitor for signs and symptoms of cerebral edema. B Give the infusion quick to replace the Na+ loss. C Clarify doctor’s order because a hypotonic solution is contraindicated in hypernatremia D Maintain a patent IV. Sodium Imbalances typically associated with parallel changes in osmolality Hypernatremia Plays a major role in ECF volume and concentration Generating and transmitting nerve impulses Muscle contractility Regulating acid-base balance Manifestations High serum sodium may occur with inadequate water intake, excess water loss or sodium gain Thirst Changes in mental status, ranging from drowsiness to seizures and coma Symptoms of fluid volume deficit Causes hyperosmolality leading to cellular dehydration Nursing Diagnoses Primary protection is thirst Potential complication: Seizures and coma Electrolyte imbalance Fluid imbalance Risk for injury Sodium Nursing Implementation Treat underlying cause Primary water deficit—replace fluid orally or IV with isotonic or hypotonic fluids Excess sodium— dilute with sodiumfree IV fluids and promote sodium excretion with diuretics Hyponatremia Results from loss of sodium-containing fluids and/or from water excess Clinical manifestations Mild—headache, irritability, difficulty concentrating. More severe— confusion, vomiting, seizures, coma Nursing Diagnoses Electrolyte imbalance Risk for injury Acute confusion Potential complication: seizures and coma solution (3% NaCl) Nursing Implications If the cause is abnormal fluid loss, Fluid replacement with isotonic sodiumcontaining solution Encouraging oral intake Withholding diuretics Drugs that block vasopressin (ADH) Convaptan (Vaprisol) Tolvaptan (Samsca) Potassium Sources Hyperkalemia Protein-rich foods Fruits and vegetables Salt substitutes Potassium medications (PO, IV) Impaired renal excretion Shift from ICF to ECF Stored blood Massive intake of potassium Regulated by kidneys High serum potassium caused by Some drugs Most common in renal failure Manifestations Dysrhythmias Fatigue, confusion Tetany, muscle cramps Weak or paralyzed skeletal muscles Abdominal cramping or diarrhea Potassium Nursing Diagnoses Electrolyte imbalance Activity intolerance Impaired cardiac output Potential complication: Dysrhythmias Nursing Implementation Stop oral and parenteral K+ intake Increase K+ excretion (diuretics, dialysis, Veltessa and/or Kayexalate) Force K+ from ECF to ICF by IV insulin with dextrose and a adrenergic agonist or sodium bicarbonate Stabilize cardiac cell membrane by administering calcium gluconate IV Use continuous ECG monitoring Potassium Hypokalemia Low serum potassium caused by Increased loss of K+ via the kidneys or gastrointestinal tract Increased shift of K+ from ECF to ICF Dietary K+ deficiency (rare) Renal losses from diuresis Manifestations of Hypokalemia Cardiac most serious Skeletal muscle weakness (legs) Weakness of respiratory muscles Nursing Diagnoses Electrolyte imbalance Activity intolerance Impaired cardiac output Potential Dysrhythmias Nursing Implementation KCl supplements orally or IV Decreased GI motility Always dilute IV KCl NEVER give KCl via IV Hyperglycemia push or as a bolus Should not exceed 10 mEq/hr Use an infusion pump Calcium Functions Formation of teeth and bone Blood clotting Transmission of nerve impulses Myocardial contractions Muscle contractions Obtained via Balance Control from dietary intake Parathyroid hormone Need vitamin D to absorb Present in bones and plasma Increases bone resorption, GI absorption, and renal tubule reabsorption of calcium Ionized calcium is biologically active Changes in pH and serum albumin affect levels Calcitonin Increases calcium deposition into bone, increases renal calcium excretion, and decreases GI absorption Calcium Nursing Diagnoses Hypercalcemia High levels of serum calcium caused by Hyperparathyroidism (two-thirds of cases) Cancer Manifestations Fatigue, lethargy, weakness, confusion Hallucinations, seizures, coma Dysrhythmias Bone pain, fractures, nephrolithiasis Polyuria, dehydration Electrolyte imbalance Acute confusion Impaired physical mobility Potential complication: Dysrhythmias Nursing Implementation Low calcium diet Increased weight-bearing activity Increased fluid intake Hydration with isotonic saline infusion Bisphosphonates—gold standard Calcitonin Calcium Nursing Diagnoses Hypocalcemia Manifestations Low serum Ca levels caused by Positive Trousseau’s or Chvostek’s sign Decreased production of PTH Laryngeal stridor Dysphagia Numbness and tingling around the mouth or in the extremities Multiple blood transfusions Alkalosis Increased calcium loss Dysrhythmias Electrolyte imbalance Impaired breathing Activity intolerance Potential complication: Fracture, respiratory arrest Nursing Implementation Treat cause Calcium and Vitamin D supplements IV calcium gluconate Rebreathe into paper bag Treat pain and anxiety to prevent hyperventilationinduced respiratory alkalosis Calcium Tests for hypocalcemia. A, Chvostek's sign is contraction of facial muscles in response to a light tap over the facial nerve in front of the ear. B, Trousseau's sign is a carpal spasm induced by C, inflating a BP cuff above the systolic pressure for a few minutes. Phosphate Serum levels controlled by parathyroid hormone. Maintenance requires adequate renal functioning and has a Reciprocal relationship with calcium Hyperphosphatemia Manifestations Management High serum PO43− caused by Tetany, muscle cramps, paresthesia's, hypotension, Identify and treat underlying cause Acute kidney injury or chronic kidney disease Excess intake of phosphate or vitamin D dysrhythmias, seizures (hypocalcemia) Calcified deposition in soft tissue such as joints, arteries, skin, kidneys, and corneas (cause of organ dysfunction) Restrict intake of foods and fluids containing phosphorus Oral phosphate-binding agents Hemodialysis Volume expansion and forced diuresis Correct any hypocalcemia Phosphate Hypophosphatemia Low serum PO43− caused by Malnourishment/malabs orption Diarrhea Use of phosphatebinding antacids Inadequate replacement during parenteral nutrition Manifestations CNS depression Management Oral supplementation Muscle weakness and pain Ingestion of foods high in phosphorus Respiratory and heart failure IV administration of sodium or potassium phosphate Rickets and osteomalacia • Monitor serum calcium and phosphorus levels every 6 to 12 hours Magnesium Cofactor in enzyme for metabolism of carbohydrates, DNA and protein synthesis, Blood glucose control, BP regulation, and ATP production Acts directly on myoneural junction Hypermagnesemia Management High serum Mg caused by Important for normal cardiac function Increased intake of products containing magnesium when renal insufficiency or failure is present Prevention first—restrict magnesium intake in high- 50% to 60% contained in bone Only 1% in ECF Absorbed in GI tract Excreted by kidneys Excess IV magnesium administration Manifestations Hypotension, facial flushing Lethargy Nausea and vomiting Impaired deep tendon reflexes Muscle paralysis Respiratory and cardiac arres risk patients IV CaCl or calcium gluconate if symptomatic Fluids and IV furosemide to promote urinary excretion Dialysis Hypomagnesemia Causes Manifestations Magnesium Prolonged fasting or starvation Resembles hypocalcemia Treat underlying cause Chronic alcoholism Fluid loss from GI tract Muscle cramps, tremors Prolonged parenteral nutrition without Hyperactive deep tendon reflexes supplementation Chvostek’s and Trousseau’s signs Confusion, vertigo, seizures Diuretics, protonpump inhibitors Hyperglycemic osmotic diuresis Dysrhythmias Oral supplements Increase dietary intake Parenteral IV or IM magnesium when severe Fluid and Electrolyte Imbalances A client with a sodium level of 179 is ordered to be started on a hypotonic solution. What is the most important nursing intervention for this client? A Give it slowly and monitor for signs and symptoms of cerebral edema. Sodium-Normal Range? Hypernatremia or Hyponatremia? B Give the infusion rapidly in order to replace the Na+ loss. C Clarify doctor’s order because a hypotonic solution is contraindicated in hypernatremia D Maintain a patent IV. Fluid and Electrolyte Imbalances A client with a sodium level of 179 is ordered to be started on a hypotonic solution. What is the most important nursing intervention for this client? A Give it slowly and monitor for signs and symptoms of cerebral edema. B Give the infusion rapidly in order to replace the Na+ loss. C Clarify doctor’s order because a hypotonic solution is contraindicated in hypernatremia D Maintain a patent IV. Acid Base Balance Acid Base Balance Maintain a steady balance between acids and bases to achieve homeostasis Health problems lead to imbalance Diabetes Chronic obstructive pulmonary disease (COPD) Kidney disease PH Measure of H+ ion concentration Increase H+ concentration= acidity Decrease H+ concentration= alkalinity Blood is slightly alkaline at pH 7.35 to 7.45 Less than 7.35 is acidosis Greater than 7.45 is alkalosis A normal pH is maintained by a ratio of 1 part carbonic acid to 20 parts bicarbonate. Acid Base Balance Mechanisms Three mechanisms to regulate acidbase balance and keep pH between 7.35 and 7.45 Buffer system Respiratory system Renal system Buffer System Respiratory System Primary regulator of acid-base balance CO2 + H2O H++ HCO3− Act chemically to change strong acids to weak acids or bind acids to neutralize them Respiratory center in medulla controls breathing Increased respirations lead to increased CO2 elimination and decreased CO2 in blood Decreased respirations lead to CO2 retention Respiratory and renal systems need to be functioning adequately H2CO3 Acid Base Balance Renal System Alterations Conserves bicarbonate and excretes some acid Imbalances occur when compensatory mechanisms fail Arterial blood gas (ABG) values give objective information about Classification of imbalances Acid-base status Underlying cause of imbalance Body's ability to regulate pH Overall oxygenation status Three mechanisms for acid excretion Secrete free hydrogen Combine H+ with ammonia (NH3) Excrete weak acids Respiratory (CO2) or metabolic (HCO3) Acidosis or alkalosis Acute or chronic Blood Gas Values Acid Base Balance Respiratory Acidosis Respiratory Alkalosis Carbonic acid excess caused by Carbonic acid deficit caused by Hypoventilation Respiratory failure Hypoxemia from acute pulmonary disorders Compensation Hyperventilation The Kidneys conserve HCO3– and secrete H+ into urine Compensation Rarely occurs when acute Can buffer with bicarbonate shift Renal compensation if chronic Acid Base Balance Metabolic Acidosis Metabolic Alkalosis Excess carbonic acid or base bicarbonate deficit caused by Base bicarbonate excess caused by Ketoacidosis Lactic acid accumulation (shock) Prolonged vomiting or gastric suction Gain of HCO3– Severe diarrhea Compensatory mechanisms Renal excretion of HCO3– Decreased respiratory rate to increase plasma CO2 (limited) Kidney disease Acid Base Balance Normal Values PH 7.35-7.45 CO2 7.5-35 HCO3 22-26 A client who was involved in a motor vehicle crash has had a tracheostomy placed to allow for continued mechanical ventilation. How should the nurse interpret the following arterial blood gas results: pH 7.48, PaO2 85 mm Hg, PaCO2 32 mm Hg, and HCO3 25 mEq/L? A Metabolic acidosis B Metabolic alkalosis C Respiratory acidosis D Respiratory alkalosis Normal Values A client who was involved in a motor vehicle crash has had a tracheostomy placed to allow for continued mechanical ventilation. How should the nurse interpret the following arterial blood gas results: pH 7.48, PaO2 85 mm Hg, PaCO2 32 mm Hg, and HCO3 25 mEq/L? PH 7.35-7.45 A Metabolic acidosis CO2 7.5-35 C Respiratory acidosis Acid Base Balance HCO3 22-26 B Metabolic alkalosis D Respiratory alkalosis pH 7.48, PaO2 85 mm Hg, PaCO2 32 mm Hg, and HCO3 25 Normal Values (Acid( PH 7.35-7.45 (ALK) PH 7.35-7.45 *** CO2 7.5-35 *** CO2 7.5-35 HCO3 22-***26 (Respiratory) PH-ALK CO2-Alk (Resp) HCO3 22-26 HCO3-normal (Met) (Metabolic) Respiratory Alkolosis Acid-Base Mnemonic—ROME Respiratory Opposite Alkalosis ↑ pH ↓ PaCO2 Acidosis ↓ pH ↑ PaCO2 Metabolic Equal Acidosis ↓ pH ↓ HCO3− Alkalosis ↑ pH ↑ HCO3 − Case study A diabetic ketoacidosis is a metabolic acidosis indicated by a pH <7.35 and a HCO3− <20 mEq/L. The PCO2 will be within the normal range if the acidosis is uncompensated but will be <35 mm Hg if compensation has occurred. The PaO2 will not be affected. Administration of insulin to promote normal glucose metabolism and administration of fluids and electrolytes to replace those lost because of the hyperglycemia. Anthony is a 54-year-old male with a history of nausea and vomiting for the past week. He has been self-medicating himself with baking soda to control his abdominal discomfort. Case Study 1. What type of acid-base imbalance would you expect Anthony to have? 2. What is causing it? 3. What type of compensation would you expect or not expect? Explain. Answers 1.Metabolic alkalosis 2. Loss of gastric acid and excess bicarbonate with baking soda ingestion 3. There is limited compensation for metabolic alkalosis. The kidneys can respond by increasing excretion of bicarbonate. The respiratory system can respond by decreasing respirations, but once the carbon dioxide level increases, stimulation of chemoreceptors results in increased ventilation. Case Study 1.What will Anthony's ABGs look like? 2. What is the treatment? Answers 1.The metabolic alkalosis in this case would be reflected by a pH >7.45 and a HCO3− >30 mEq/L. Because of the duration of this condition, compensation may be indicated by a PCO2 >45 mm Hg. 2. Determine the underlying cause of the vomiting if possible and stop the use of baking soda (sodium bicarbonate). Antiemetic drugs and nasogastric intubation may help relieve the vomiting, and IV replacement of fluids and electrolytes may be necessary Practice Question Normal Values PH 7.35-7.45 A client who was involved in a motor vehicle crash has had a tracheostomy placed to allow for continued mechanical ventilation. How should the nurse interpret the following arterial blood gas results: pH 7.48, PaO2 85 mm Hg, PaCO2 32 mm Hg, and HCO3 25 mEq/L? A Metabolic acidosis CO2 7.5-35 B Metabolic alkalosis HCO3 22-26 C Respiratory acidosis D Respiratory alkalosis Practice Question Normal Values PH 7.35-7.45 A client who was involved in a motor vehicle crash has had a tracheostomy placed to allow for continued mechanical ventilation. How should the nurse interpret the following arterial blood gas results: pH 7.48, PaO2 85 mm Hg, PaCO2 32 mm Hg, and HCO3 25 mEq/L? A Metabolic acidosis CO2 7.5-35 B Metabolic alkalosis HCO3 22-26 C Respiratory acidosis D Respiratory alkalosis Dosage Calculation Queston #1 34.A client is prescribed 1800 units of heparin sulfate subcutaneously. The available dose is 2500 units/0.5mL. The nurse will administer ______ (Round to the nearest tenth.) Question #2 35. A dose of 6.5 g of medication has been ordered for a client. The medication comes in 4 g/0.4 mL. The nurse will administer ___ mL. Round to the nearest tenth. Dosage Calculation Queston #1 34.A client is prescribed 1800 units of heparin sulfate subcutaneously. The available dose is 2500 units/0.5mL. The nurse will administer __0,5____ (Round to the nearest tenth.) Question #2 35. A dose of 6.5 g of medication has been ordered for a client. The medication comes in 4 g/0.4 mL. The nurse will administer _0.65__ mL. Round to the nearest tenth. Chapter 23 Integumentary Problems DR TARSHA STEWART Skin Care Environmental Hazards Sun exposure Ultraviolet (UV) rays UVA—tanning UVB—sunburn Sun protection Protective clothing Sunscreen Risk Factors Fair skin Blonde or red hair, blue eyes Outdoor sunbathing Living near the equator or high altitudes History of skin cancer Skin Disorders Nonmelanoma Skin Cancers Actinic keratosis-elevated dry, rough, scaly papules Premalignant skin lesions Basal cell carcinoma Most common type of skin cancer Least deadly Squamous cell carcinoma Potential to metastasize Pipe, cigar, and cigarette smoking Immunosuppression leads to a dramatic increase in incidence Skin Disorders Malignant Melanoma Cause unknown Environmental factors Genetic factors Atypical/Dysplastic Nevus Dysplastic nevi (DN) ABCDE Rule Risk Factors Red or blonde hair Asymmetry Light-colored eyes Border irregularity Fair skin that freckles Color change Diameter greater than 6 mm Evolving in appearance Chronic sun exposure Family history Malignant Melanoma Diagnosis Breslow Measurement Treatment Dermoscopy Determined by Incisional Site of original tumor Stage of the cancer Includes wide surgical incision and adjuvant therapy Tumor biopsy thickness Breslow measurement Clark level Skin Infections and Infestations Types Bacterial infections Allergic Dermatitis Cutaneous Drug Reactions Associated with allergies and hypersensitivity reactions Steven Johnson syndrome (SJS) Skin sloughs off Viral infections Infestations and insect bites Family history and exposure Fungal infections Patch testing Avoidance of causative agent Stop offending drugs Supportive care Toxic epidermal necrolysis (TEN) Benign Dermatologic Problems Types Acne vulgaris Psoriasis Seborrheic keratosis Interprofessional Care Diagnostic/Surgical Phototherapy Skin scraping Radiation Electrodesiccation Electrocoagulation Curettage Punch biopsy Cryosurgery Excision—Mohs procedure therapy Laser technology Drug therapy Nursing Management Control of Pruritus Break the itch/scratch cycle Cool environment Hydration, wet compresses, moisturizers Topical drugs Psychologic Effects Reinforce prescribed regimen Support groups Camouflage Surgical Procedures Cosmetic Procedures Nursing Management Topical procedures Injection Elective surgery Laser surgery Face lift Liposuction Preoperative management Informed consent Patient teaching Postoperative management Pain management Monitor for signs of infection and adequate circulation Skin Grafts Uses Types Free skin grafts Autograft and isograft Reconstructive microsurgery Skin flaps Engineered skin substitutes Chapter 24 Burns DR TARSHA STEWART BURNS Burns Occur when there is injury to the skin or other tissues of the body caused by heat, chemicals, electrical current, or radiation The patient with a burn injury may have a multitude of problems Most burn accidents are preventable Types of Burn Injury Thermal burns Chemical burns Smoke inhalation injury Electrical burns Cold thermal injury BURNS Thermal Burns Caused by flame, flash, scald, or contact with hot objects Most common type of burn injury Severity of injury depends on Temperature of burning agent Duration of contact time Degree of Burns BURNS Chemical Burns Result of contact with acids, alkalis, and organic compounds Alkali burns can be more difficult to manage because they cause protein hydrolysis and melting Alkalis found in cement, oven and drain cleaners, heavy metal cleaners Organic compounds include phenols and petroleum products Smoke Inhalation Occurs from breathing noxious chemicals or hot air Cause damage to respiratory tract Major predictor of mortality in burn victims Rapid initial and ongoing assessment is critical Airway compromise and pulmonary edema can quickly develop Inhalation Burns Three types Upper airway injury Lower airway injury Metabolic asphyxiation Burns Metabolic Asphyxiation Upper Airway Injury Carbon monoxide (CO) and hydrogen cyanide inhaled Impairs oxygen delivery to tissues, resulting in Hypoxia Elevated carboxyhemoglobin levels Death when levels reach greater than 20% May occur in absence of burn injury Injury to mouth, oropharynx, and/or larynx Thermal burns Inhalation of hot air, steam, or smoke Mucosal burns of oropharynx and larynx manifested by Redness Blistering edema Upper Airway Injury Swelling may be massive and onset rapid Eschar and edema may compromise breathing Edema from facial and neck burns can be lethal Internal pressure from edema may narrow airway Obstruction can occur quickly, presenting airway emergency Burns Lower airway Burns Injury to trachea, bronchioles, and alveoli Tissue damage is related to duration of exposure to toxic fumes or smoke Pulmonary edema may not appear until 12 to 48 hours after burn May manifest as acute respiratory distress syndrome (ARDS) Electrical Burns Result from intense heat generated from an electric current May result in direct damage to nerves and vessels, causing tissue anoxia and death Electrical Burns Severity of injury depends on Amount of voltage Tissue resistance Current pathways Surface area Length of time current flow was sustained Burns Electrical Burns Current that passes through vital organs produces more lifethreatening sequelae than current that passes through other tissues Electric sparks may also ignite patient’s clothing, causing a thermal flash injury Severity of injury can be difficult to determine since most damage occurs below the skin Electrical current can cause muscle spasms strong enough to fracture long bones and vertebrae Patients at risk for dysrhythmias or cardiac arrest, severe metabolic acidosis, and myoglobinuria Myoglobin from injured muscle and hemoglobin from damaged RBCs travel to kidneys Acute tubular necrosis (ATN) Acute kidney injury Classification of Burn Injury Extent of Burn Lund-Browde Considered more accurate Rule of 9s Used as initial Assessment Sage Burn Diagram Burns Severity of Burns Severity of burn injury is determined by location of burn wound Face, neck, chest Respiratory obstruction from edema, eschar Hands, feet, joints, eyes Self-care difficult Ears, nose, buttocks, perineum High risk for infection Complications Circumferential burns of extremities can cause circulation problems distal to burn Possible nerve damage to affected extremity Patients may also develop compartment syndrome Risk Factors Preexisting heart, lung, or kidney disease contribute to poorer prognosis Diabetes and peripheral vascular disease put patient at high risk for delayed healing Physical weakness make it challenging for patient to recover Alcohol or drug use Malnutrition Concurrent fractures, head injuries, or other trauma leads to a more difficult time recovering Burn Care Pre-Hospital Remove person from source of burn and stop burning process Rescuer must protect themselves from being injured Electrical and chemical injuries Remove patient from contact with source Small thermal burns Cover with clean, cool, tap waterdampened towel Cooling within 1minute helps minimize depth of injury Large thermal burns If unresponsive— circulation, airway, breathing If responsive— Airway, breathing, circulation Large thermal burns Cool burns for no more than 10 minutes Do not immerse in cool water or cover with ice Remove burned clothing Wrap in dry, clean sheet or blanket Burn Care Pre-Hospital Care Phases of Burn Management Chemical burns Remove chemical particles or powder Flush area with water Inhalation injury Watch for signs of respiratory distress Treat quickly and efficiently 100% humidified oxygen if CO poisoning is suspected Emergent (resuscitative) Acute (wound healing) Rehabilitative (restorative) Emergent (resuscitative) phase is time required to resolve immediate problems resulting from injury Up to 72 hours Main concerns Hypovolemic shock Edema Ends when fluid mobilization and diuresis begins Burns Emergent Phase Pathophysiology Fluid and electrolyte shifts Greatest threat is hypovolemic shock Caused by a massive shift of fluids out of blood vessels because of increased capillary permeability Can begin as early as 20 minutes postburn Capillary permeability increases Blood leak into the interstitial space, causing edema & decreased blood volume. Hematocrit increases, blood is more viscous. Decreased blood volume and increased viscosity produces increased peripheral resistance Burn shock, a type of hypovolemic shock, rapidly ensues and, if not corrected, can result in death. Fluid and electrolyte shifts Colloidal osmotic pressure decreases More fluid shifts out of vascular space into interstitial spaces Third spacing occurs Exudate and blisters appear Edema in unburned areas Burns Emergent Phase Pathophysiology Fluid and Fluid and electrolyte electrolyte shifts shifts Normal insensible RBCs are hemolyzed loss: 30 to 50 mL/hr by circulating Increased factors released at insensible losses in time of burn, as well the severely as direct result of burned patient insult of burn injury Net result of fluid Thrombosis in shift is intravascular capillaries of burned volume depletion tissue Edema High hematocrit Decreased blood caused by pressure hemoconcentration Increased pulse Fluid and electrolyte shifts K+ shift develops first because injured cells and hemolyzed RBCs release K+ into circulation Na+ rapidly moves to interstitial spaces and stays there until edema formation ends Effects of Burn Shock Burn shock is shown above the purple line. As the capillary seal is lost, interstitial edema develops. Cellular integrity is altered, sodium (Na) moves into the cell and potassium (K) leaves the cell. The shifts after the resolution of burn shock are shown below the blue line. Wand sodium move back into the circulating volume through the capillary. Albumin stays in the interstitial. Potassium is transported into the cell and sodium is transported out as the cellular integrity returns. Emergent Phase Cardiovascular Inflammation and healing Neutrophils and monocytes accumulate at injury Fibroblasts and new collagen fibrils begin wound repair within first 6 to 12 hours after injury Immunologic changes Skin barrier is destroyed Bone marrow depression occurs Circulating levels of immune globulins are decreased Defects occur in function of WBCs Patient at greater risk for infection Clinical Manifestations Shock from hypovolemia Pain Blisters Paralytic ileus Shivering Altered mental status Cardiovascular system Dysrhythmias and hypovolemic shock Impaired circulation to extremities with circumferential burns- if untreated can lead to Tissue ischemia Paresthesia Necrosis Impaired microcirculation and increased viscosity results in sludging Corrected by adequate fluid replacement Venous thromboembolism (VTE) Prophylaxis with anticoagulants Emergent Phase Respiratory Respiratory system Upper airway burns May occur with or without smoke inhalation Lower airway injury Need fiberoptic bronchoscopy and carboxyhemoglobin blood levels Watch for signs of respiratory distress Chest x-ray may appear normal on admission; changes can occur over next 24 to 48 hours ABGs may be within normal range on admission and change over time Other cardiopulmonary problem Patients with preexisting heart or lung disease are at increased risk Heart failure Pulmonary edema Pneumonia Emergent Phase Resp Urinary System Urinary system Acute tubular necrosis (ATN) Decreases blood flow to kidneys causes renal ischemia Management Airway management Early endotracheal intubation Escharotomies of the chest Fiberoptic bronchoscopy Humidified air and 100% oxygen High fowler’s position Suctioning, chest PT Bronchodilators Fluid Theraoy 2 large-bore IV lines for greater than 15% TBSA For burns greater than 20% TBSA central line may be considered Arterial line placed if frequent ABGs or invasive BP monitoring needed Parkland (Baxter) formula for fluid replacement Emergent Phase Wound care Open method Wound Care Cleansing and gentle debridement Can be done on a shower cart, in a shower, or on a bed or stretcher Surgical debridement May need to be done in the OR Necrotic skin is removed Releasing escharotomies and fasciotomies may be done Burn is covered with topical antimicrobial No dressing over wound Usually limited to the care of facial burns When open burns wounds are exposed, staff should wear PPE Disposable hats Masks Gowns Gloves Use sterile gloves to apply antimicrobial ointment and sterile dressings Shower Once-daily shower Dressing change in morning and evening Newer antimicrobial dressings can be left in place from 3 to 14 days Infection can cause further tissue injury and possible sepsis Source of infection is patient’s own flora Skin, respiratory, GI Emergent Phase Wound care Wound Care Allograft Homograft skin From skin donor cadavers Used with newer biosynthetic options Facial care Covered with ointment and gauze Not wrapped to limit pressure Eye care for corneal burns Antibiotic ointment is used Artificial tears for moisture, Periorbital edema may frighten patient Keep ears free of pressure Do not use pillows Raise patient’s head with rolled towel Hands and arms should be extended and elevated on pillows or foam wedges Splints may be used on hands and feet Wraps may reduce edema Keep patient’s perineum clean and dry as possible Indwelling catheter Perineal care Fecal diversion device if loose stools Laboratory tests to monitor fluids and electrolytes ABGs to assess oxygenation PT for ROM exercises Emergent Phase Wound care Drug therapy Analgesics and sedatives Morphine Hydromorphone (Dilaudid) Haloperidol (Haldol) Lorazepam (Ativan) Midazolam IV pain medication for fastest onset of action Tetanus immunization Given routinely to all burn patients Antimicrobial agents Topical agents Silver sulfadiazine Mafenide acetate Systemic antibiotic not usually used in controlling burn wound flora Started when diagnosis of sepsis is made Nutritional therapy priority once fluid replacement needs addressed Early and aggressive nutritional support within hours of burn injury Decreases complications and mortality Optimizes burn wound healing Minimizes negative effects of hypermetabolism and catabolism Acute Phase Begins with mobilization of extracellular fluid and subsequent diuresis Ends when Partial thickness wounds are healed or Full thickness burns are covered by skin grafts Pathophysiology Necrotic tissue begins to slough Granulation tissue forms Partial-thickness burns heal from wound edges and dermal bed Full-thickness burns must have eschar removed and skin grafts applied Partial-thickness wounds form eschar Once eschar is removed, re-epithelialization begins Full-thickness burn wounds require Surgical debridement Skin grafting Acute Phase Laboratory Values Sodium Hyponatremia can develop from Excessive GI suction Diarrhea Water intoxication From excess water intake Offer juices, nutritional supplements Infection Potassium Hyperkalemia may occur if patient has Renal failure Adrenocortical insufficiency Massive deep muscle injury Large amounts of potassium are released from damaged cells Assess for manifestations of hyperkalemia Burn wound colonized by patient’s own flora WBCs have functional deficit and patient is immunosuppressed Partial-thickness burns can convert to full-thickness wounds in the presence of infection Watch for signs and symptoms Hypothermia or hyperthermia Increased heart and respiratory rate Decreased BP or Decreased urine output Causative organism of sepsis usually gram-negative bacteria Obtain cultures and Lactate level Acute Phase Complications Cardiovascular and respiratory systems Same complications can be present in emergent phase and may continue into acute phase In addition, new problems might arise, requiring timely intervention Neurologic system No physical symptoms unless severe hypoxia from respiratory injuries or complications from electrical injuries occur Disorientation Combative Hallucinations Frequent nightmare-like episodes Delirium More acute at night Occurs more often in older adults Usually, transient Complications and sequelae can last for years Musculoskeletal system Limited ROM Skin and joint contractures Gastrointestinal system Paralytic ileus Diarrhea or Constipation Curling’s ulcer Endocrine system Increased blood glucose levels Increased mobilization of glycogen stores gluconeogenesis Increased insulin production to insulin insensitivity Hyperglycemia may also be caused by high caloric intake needed A nurse is caring for a client who has sustained severe burn injuries after a gas tank explosion. The nurse assessed that the burned areas are as follows: the head, entire right arm, half of the left arm, and the entire front torso. The nurse uses the rule of nine and estimates that the client has burned what percentage of body surface area? A 18% B 26% C 36% D 40.5% A nurse is caring for a client who has sustained severe burn injuries after a gas tank explosion. The nurse assessed that the burned areas are as follows: the head, entire right arm, half of the left arm, and the entire front torso. The nurse uses the rule of nine and estimates that the client has burned what percentage of body surface area? A 18% B 26% C 36% D 40.5% A client is brought to the Emergency Room after being trapped in a burning house. The client's facial hair is singed, their voice is hoarse, and they are coughing up black sputum. Which is the priority nursing intervention for this client? A Monitor pain level B Evaluate airway patency C Insert indwelling catheter D Elevate burned limbs above heart Remember ABCs All steps would need to be completed but ensuring that the airway is patent is the top priority. A client is brought to the Emergency Room after being trapped in a burning house. The client's facial hair is singed, their voice is hoarse, and they are coughing up black sputum. Which is the priority nursing intervention for this client? A Monitor pain level B Evaluate airway patency C Insert indwelling catheter D Elevate burned limbs above heart Bod was out playing golf when a thunderstorm arose out of nowhere. As he sought shelter he was stuck by lighting. EMS were alerted by Bob's companions and her was transported to the hospital. On arrival he is alert with a respiratory rate of 20. Which nursing intervention would be appropriate for this client? A Cover burned areas with dry dressings B Remove clothing that is stuck to the skin C Insert one 24-gauge IV in the client's hand D Withhold pain medication to preserve level of consciousness Emergency interventions for electrical burns: • Remove patient from electrical source. • If unresponsive, assess circulation, airway, and breathing. • If responsive, monitor airway, breathing, and circulation. Provide supplemental O2 as needed. • Monitor vital signs, heart rhythm, level of consciousness, respiratory status, and O2 saturation. • Remove nonadherent clothing, shoes, watches, jewelry, glasses or contact lenses (if face was exposed). • Cover burned areas with dry dressings or clean sheet. Establish IV access with 2 large-bore catheters if burn >15% TBSA. • Begin fluid replacement. • Identify entrance and exit wounds. • Obtain arterial blood gas to assess acid-base balance. • Insert indwelling urinary catheter if burn >15% TBSA. • Elevate burned limb(s) above heart to decrease edema. • Give IV analgesia and assess effectiveness frequently. • Identify and treat other associated injuries (e.g., fractures, head injury, thermal burns). Bod was out playing golf when a thunderstorm arose out of nowhere. As he sought shelter he was stuck by lighting. EMS were alerted by Bob's companions and her was transported to the hospital. On arrival he is alert with a respiratory rate of 20. Which nursing intervention would be appropriate for this client? A Cover burned areas with dry dressings B Remove clothing that is stuck to the skin C Insert one 24-gauge IV in the client's hand D Withhold pain medication to preserve level of consciousness That’s all folks!!!