An Artificial Intelligence Driven System
to Predict ASD Outcomes in ABA
David J. Cox1,2, Dana D’Ambrosio1, Jamie Pagliaro1, Rethink Data Team1
1
Rethink First; 2 Endicott College
Past researchers have sought to describe and predict how individuals with autism spectrum disorders
(ASD) are likely to benefit from applied behavior analysis (ABA) therapy. These studies, however, have had
limited generalizability due to sample sizes, simple modeling approaches, and failing to include more holistic
patient profiles. Further, few studies have embedded their results into technology platforms practitioners
can incorporate into treatment settings. In this article, we provide an overview of how we used 48 variables
spanning hours and characteristics of ABA, treatment goals characteristics, and patient characteristics to
predict goals mastered for 31,294 individuals with ASD receiving from 615 companies. Unsupervised
machine learning identified between 8-56 distinct patient clusters (depending on the algorithm) differing
along characteristics known to influence outcomes from past published research and patient characteristics
unpublished in past research predicting patient progress from ABA. Linear regression models (as used in
past research) led to an overall r2 value (r2=.90; MAE=1.30) that was ~.23 higher than previously published
studies. Machine learning improved predictions further (r2=.99; MAE=1.04). When predictions were made
within patient clusters, r2 ranged between .95-.99 (~.20-.24 points higher than past research) and MAE
ranged between 1.12-1.45. To close, we describe how this Artificial Intelligence (AI) system is embedded
within a technology platform continuously collecting data. This allows the system to improve over time and,
in turn, users of the AI system can use the results to improve ASD outcomes through use cases such as:
(a) real-time recommendations of ABA dosage based on unique patient characteristics; (b) feedback on
actual versus expected patient outcomes; and (c) how patient progress varies along social determinants of
health. In the future, these data and the underlying models could be leveraged by payors and providers
alike to support and enable their unique value-based care initiatives.
Keywords: outcomes; artificial intelligence; machine learning; autism; applied behavior analysis
Predictability is a common concern in the
delivery of healthcare services. Patients typically
want to know how likely it is that each of several
treatment options will be effective (e.g., Meyer et
al., 2021); and they want to know the potential
treatment length and cost relative to their personal
budget and calendar so they can plan and budget
accordingly (e.g., Bhargava & Loewenstein, 2015;
Han et al., 2012). Likewise, insurance companies
often want to know how potential treatment length
and cost so they can forecast expenses and plan
strategically for the future (e.g., Papanicolas et al.,
2018). Finally, healthcare practitioners want to
know potential treatment length, the possible range
Conflict of Interest: The AI system (patent pending) and
products leveraging this AI system are the property of
RethinkFirst.
Funding: No external funding was used to support the work
published herein.
Disclaimer: The AI system described herein is continuously
ingesting more data and the modeling methods are being
continuously refined to improve performance. Thus, all results
discussed herein should be considered as the static state of the
system at the time of writing in February, 2023.
in which outcomes can improve, and the resources
it will require so they can manage things such as
caseloads, waitlist communication, hiring, and
business operations (e.g., WHO, 2015).
It is through this lens that the current work sits
relative to one area of healthcare in the delivery of
Applied Behavior Analysis (ABA) services for
individuals with autism spectrum disorders (ASD).
The prevalence of ASD diagnosis has increased in
the previous 20 years from 1 in 150 to 1 in 44
children (Centers for Disease Control and
Prevention, 2021 ). As a result, stakeholders
(patients, parents, payors, and providers) are
increasingly aware of the variability in cost,
treatment duration, and patient outcomes. For
example, the average annual cost of treatment is
estimated to range anywhere between $17,227 to
$130,182 (Autism Speaks, 2022; Eldevik et al.,
2009); and individuals diagnosed with autism and
their families might receive ABA for between 5 to 40
hours per week for a duration ranging between 18
months to five years (Larsson, 2012). Such
variability in cost and duration of treatment following
AI SYSTEM TO PREDICT ABA OUTCOMES
an ASD diagnosis adds significant uncertainty to all
involved (De Groot & Thurik, 2015; Han et al., 2012;
Meyer et al., 2021).
Compounding
this
uncertainty
around
increasing amounts of ABA service delivery is a
lack of standardization for ABA dosage as a
function of patient presentation at intake and
throughout the duration of services. At the time of
writing1, the process of determining optimal dosage
of ABA for each patient is seemingly subjective.
Past research suggests a patient’s age, symptom
severity,
historical
treatment
duration,
personal/family needs, current abilities, and the
overall goals of therapy should play a role in how
many hours per week of ABA an individual might
need (e.g., APBA, 2020; Granpeesheh et al., 2009).
However, no known quantitative methodology with
robust empirical support allows clinicians to
translate those variables into a precise
recommendation of the optimal number hours of
ABA. Thus, a tool that provides reliable and precise
predictions based on patient data and published
best-practice evidence would help decrease the
subjectivity and uncertainty around ABA treatment.
In addition to decreased subjectivity and
reduced uncertainty around ABA treatment, board
certified behavior analysts (BCBAs) arguably have
an ethical obligation to improve in this area. The
Behavior Analyst Certification Board (BACB) Ethics
Code for Behavior Analysts includes several
guidelines that speak directly to this topic (BACB,
2020). For example, Guideline 2.08 requires
discussing the scope of treatment with a client
before starting services; Guideline 3.01 requires
BCBAs to identify and act upon opportunities that
lead to avoidable harm or wasteful allocation of
resources; and, Guideline 3.12 requires BCBAs to
advocate for appropriate services. Here, leveraging
a reliable, precise, and evidence-based method to
recommend ABA dosage allows the BCBA to
accurately communicate the scope of likely
treatment; why they believe benefits will be
maximized while avoiding wasteful allocation of
resources; and to know that the amount and level
of behavioral services they are recommending is
data-based.
Past researchers have sought to improve
predictability and aid BCBAs in their ethical
obligations by quantitatively modeling the
relationship between the hours that patients contact
1
February, 2023.
We want to reiterate that this is a relative claim as they are among
some of the largest studies to date examining these kinds of
2
2
ABA and the resulting outcomes. For example,
Linstead and colleagues (2017a) modeled the
relationship between treatment intensity and
mastered learning objectives for 726 children aged
1.5-12 years who received community-based
behavioral intervention services. Linear regression
and neural network models led to r2 values of .35
and .60, respectively. Similarly, in a separate study
by Linstead et al. (2017b), they used linear
regression to model the relationship between
treatment intensity/duration and goals mastered
within specific skill domains for 1,468 individuals
with ASD. Across goal domains, r2 values ranged
between .50 (social goals) and .67 (motor goals).
As a final example, Ostrovsky and colleagues
(2022) used a series of t-tests, effect size
measures, and Pearson correlations to quantify the
relationship between changes in standardized
assessment scores as a function of hours of ABA
and modality of supervision. For the 178 individuals
included in the study, they observed that clinically
significant improvements in function were
independent of the hours of ABA received.
Though broader limitations to this (and other)
past studies are described in more detail below, the
variance accounted for by these models was likely
impacted by several factors. First, the overall
sample sizes in these studies were relatively small2.
Second, as noted by the authors of several studies,
models have often been built without accounting for
the heterogeneity that comprises the broad
spectrum that is ASD and that was unlikely to be
fully captured in the studied samples. A final
limitation to past work in this realm (noted by
Ostrovsky et al., 2022) is the assumption of a linear
relationship between hours per week of ABA and
progress made. Dose-response curves in other
areas of behavioral healthcare are often decidedly
nonlinear (e.g., Dews, 1955; Levy et al., 2020;
Zoladz & Diamond, 2009). Thus, modeling
approaches that more flexibly account for nonlinear
relationships may perform better (e.g., the neural
network outperforming linear regression in Linstead
et al., 2017a).
PREDICTING PATIENT PROGRESS BASED ON
PATIENT & ABA CHARACTERISTICS
One technique that researchers have used to
create data-driven subgroups from larger datasets
relationships. “Small” here is in reference to the total number and
amount of heterogeneity present with the ASD population as a whole
and compared to the sample size in the current study.
AI SYSTEM TO PREDICT ABA OUTCOMES
is called cluster analysis (e.g., Ansari et al., 2018;
Charron et al., 2023; Hewlett et al., 2022). Cluster
analysis at its simplest can be defined as finding
groups in data (Hennig et al., 2016). For our
purposes here, cluster analyses would seek to
separate “all individuals with ASD in our sample”
into smaller subgroups based on the totality of their
demographics and clinical-developmental states
while they contact ABA. The idea is that modeling
relationships between contact with ABA and patient
progress might either be more accurate when
conducted within patient clusters or lead
researchers to differentially identify important
variables that predict patient progress for specific
clusters. In contrast to traditional modeling
techniques
where
the
relations
between
independent variables and a dependent variable is
known, cluster analyses are often more exploratory
as the researcher may not know how many clusters
should exist nor which patients should be grouped
in which cluster. Uncovering these relationships is
often the goal of the analysis.
Researchers have used cluster analysis
techniques to identify subgroups of individuals
within samples of data gathered from individuals
with ASD. For example, Parlett-Pelleriti and
colleagues (2022) published a review of how
unsupervised machine learning has been used to
identify patient clusters for individuals with ASD.
Table 1 shows the descriptive statistics of the
sample sizes and number of clusters identified
across the 36 studies included. Two items are of
note, here. First, considering the heterogeneity of
ASD, the sample sizes were relatively small with
the median sample size being 220, 78% of the
studies used less than 1000 participants, and all but
one used less than 5000 participants. It is unknown
what the clustering results might look like when a
larger sample of individuals with ASD are included.
The second item to note were the variables
used for clustering analyses and the resulting
number of clusters. The median number of clusters
identified across studies was three with results
largely clustering around the ASD diagnostic
criteria or assessment domains. This makes sense
as those were the data used for clustering in many
of the studies. But individuals with ASD are much
more than the developmental and behavioral
patterns contained in diagnostic or skills-based
assessments. Minimally, they may have comorbid
diagnoses or medical concerns that influence their
unique clinical course (e.g., Lingren et al., 2016).
Additionally, individuals with ASD (like the rest of
us) are embedded within larger socioeconomic,
3
Table 1. Descriptive statistics of research applying
unsupervised machine learning to cluster individuals with ASD
(Parlett-Pelleriti, 2022).
Maximum
Arithmetic Mean
Standard
Deviation
Median
Minimum
Current Work*
Sample
Size
20,658
1,218
Number of
Clusters
7
3.32
3,504
1.21
220
10
31,294
3.00
2.00
8-53
* NB: Because this is a “live” system, the overall sample size is
continuously increasing and the specific clustering results are
continuously being refined toward optimal.
familial, and educational contexts. Past researchers
have found that many variables outside of
diagnostic symptomatology will predict responseto-intervention such as health-related features of
neighborhoods and socioeconomic factors (e.g.,
Braverman & Gottlieb, 2014). Clustering analyses
that attempt to identify more holistic subgroups of
ASD beyond diagnostic and assessment
classifications will need to include a greater number
of variables.
A second limitation to past research
unmentioned thus far has been how a stakeholder
might use the information from the published
analyses. For example, practitioners might be
interested in answers to questions such as: How
might the models provide a recommended dosage
of ABA for an individual? How might practitioners
design treatment programs based on this
information? How could practitioners gain feedback
around the patients’ outcomes they observe and
what is expected based on these models? And,
when considering the entirety of a patients’ unique
human situation, what variables are most predictive
of intervention success, and which are least
predictive? Lastly, how might answers to these
questions be packaged into a system that makes
access to clustering and predictive models as
efficient as possible?
The purpose of this manuscript is to describe at
a high-level how researchers have been addressing
the abovementioned limitations while attempting to
provide answers to the practical practitioner
questions. To do this, we first provide an overview
of a patent-pending Artificial Intelligence (AI) based
system that: continuously collects data on patient
and ABA-related variables with a known relation to
patient progress from ABA therapy; aggregates the
data for analysis; uses unsupervised machine
AI SYSTEM TO PREDICT ABA OUTCOMES
learning to cluster patients and supervised machine
learning to predict goals mastered; and returns the
model outputs back into a technology platform to be
used by an end-user. Following this high-level
overview, we describe the general results of patient
clustering analyses and how predicting patient
outcomes is impacted when using these patient
characteristics. In total, this manuscript provides a
description of how the AI system functions,
continuously improves, and preliminary results
which will likely continue to improve.
HIGH-LEVEL SCHEMATIC OF THE AI SYSTEM
Figure 1 shows a high-level overview of the
patent-pending AI system. The system involves five
major steps. First, users interact with a web-based
platform to enter the raw data for the patient and
ABA-related variables used in the AI Engine (see
below for more details). The specific application
that captures these variables can differ depending
on the variable, end-user, and product they are
using. The output of this first step is raw data having
4
been collected and stored in a product-specific
database.
The second step of the AI system is to use
extract, transform, and load (ETL) workflows to
move the data from the product-specific databases
associated with its collection to a single, central
location (i.e., a data warehouse). Specifically, the
ETL workflows act on the output of the first step and
regularly move data from the product specific
databases to a centralized data warehouse within
the scope of a data model allowing for the data from
many of the tables to be related to one another. The
primary output of the second step is a set of
relational tables where each table contains some
portion of the total set of variables used for
modeling in the AI engine.
The third step involves a series of Python
scripts that conduct the data pre-processing and
analytics referred to as the AI Engine. The AI
Engine is described in more detail below. Here, the
primary points are that the Python scripts involved
in this workflow: (a) pre-process the data stored in
the relational tables in the data warehouse; (b)
Figure 1. High-level schematic of the AI system to predict patient clusters and patient outcomes based on contact with ABA therapy
and their unique patient cluster profile.
AI SYSTEM TO PREDICT ABA OUTCOMES
combine the variables from many related tables into
a single analytic data frame; (c) conduct
unsupervised machine learning relative to patient
clustering; (d) conduct a suite of statistical and
supervised machine learning analyses relative to
predicting patient outcomes using the patientrelated and ABA-related variables; and (e) deploy
two top-performing models as API endpoints—one
each for patient clustering and predicting outcomes.
The primary output of this third step are the
mathematical-computational models for patient
clustering and predicting patient outcomes.
The fourth step uses the primary outputs of step
three to build dose-response curves unique to
individual patients. Specifically, a user interacts
with a web-based tool to provide data specific to the
patient-related and ABA-related variables needed
for the finalized models from step 3. Once collected,
that data can be run through the clustering and
outcome prediction models to generate a unique
dose-response curve predicting estimated progress
as a function of the patient characteristics and a
range of hours of ABA the patient could contact.
The fifth step uses the dose-response created
in step four toward some practical aim. Few people
are likely interested in identifying patient clusters or
predicting outcomes simply for the sake of doing so.
Rather, they want to use the information to help
them do something better than they currently do. To
5
highlight what’s possible, we walk through three
possible use cases based on the output of step four
in the final section below. These include: (a) using
the dose-response curve to recommend hours per
week of ABA to optimize patient progress; (b) to
gain performance feedback between observed and
expected patient outcomes for a clinician’s
caseload or an organization as a whole; and (c) how
patient progress varies along social determinants of
health when accounting for the total milieu of
patient characteristics and their interactions. Before
we get to these use cases, however, we will first
briefly review how the AI Engine works and current
results around patient clustering and precision
predicting patient progress.
HIGH-LEVEL OVERVIEW OF THE AI ENGINE
As noted above, the AI Engine is comprised of
five distinct steps (Figure 2). These are: (a) preprocess the data stored in the relational tables in
the data warehouse, (b) integrate the various tables
into a single, analytic data frame, (c) conduct
unsupervised machine learning relative to patient
clustering; (d) conduct a suite of statistical and
supervised machine learning analyses relative
predicting patient outcomes using the patientrelated and ABA-related variables; and (e) deploy
two top-performing models as API endpoints—one
Figure 2. High-level overview of the steps that comprise the AI Engine portion of the AI system.
AI SYSTEM TO PREDICT ABA OUTCOMES
each for patient clustering and predicting outcomes.
In this section we provide a high-level overview of
what occurs in each section. Of note, manuscripts
that provide significant detail for steps (c) and (d)
are in preparation and will be published in the near
future.
Variable Selection. We sought to create a
comprehensive set of variables that capture patient
characteristics spanning diagnostic characteristics
(DSM-5), patient age and history of treatment,
clinical presentation of social and behavioral
excesses and deficits, medical and behavioral
health comorbidity, goal counts related to
developmental domain subsets, social drivers of
health, and barriers to progress/treatment. The 48
variables chosen for inclusion in the current
analyses were derived from published standards
(e.g., Autism Commission on Quality, 2022;
Behavioral Health Center of Excellence, 2022;
National Autism Center, 2009) and applicable
research literature that outline best practices. Once
selected, a team of experienced BCBAs and
BCBAs at the doctoral level (BCBA-Ds) narrowed
and rounded out the list of variables for inclusion
which were then solidified by a provider advisory
committee to ensure agreement on the likely
relation between included variables and patient
outcomes.
Pre-processing. Pre-processing is a series of
steps that convert the data from its raw form stored
in the data warehouse to a dataset on which
statistical and machine learning analyses can be
conducted (for reviews on methods, see Baskar et
6
al., 2013; Müller & Guido, 2017; Saleem et al.,
2014). Generally, pre-processing involves data
cleaning, data integration, data transformation, and
dimensionality reduction. These steps and the
strategies used within the current AI system are
shown in Table 2. Data cleaning often, at minimum,
involves employing explicit strategies around
handling missing data, outliers, and inconsistent
data. Data integration involves joining or merging
datasets together after aggregating each dataset at
the level required for analyses. Here, data were
aggregated and integrated at the individual patient
level spanning one week of ABA service delivery.
Data transformation refers to a set of mathematical
techniques whereby data are converted from their
original values to values likely to improve
subsequent modeling (Müller & Guido, 2017). For
example, data transformations might include:
generalization (e.g., converting from zip code to
state), normalization (e.g., log-transforms, min-max
scaling), feature reduction (e.g., removing variables
with little variability; combining features that are
similar in some way); or feature discretization (i.e.,
converting continuous data into bins or categories).
Unsupervised ML: Patient Clustering.
Unsupervised machine learning refers to a suite of
mathematical and algorithmic techniques aimed at
learning the underlying structure in data where the
answer is unknown (Patel, 2019). Clustering refers
to a suite of mathematical and algorithmic
techniques to find groups in data (Hennig & Meila,
2016). Combined, the goal of unsupervised
machine learning for patient clustering is to identify
patient subgroups within the larger dataset that are
Table 2. Overview of the sequence and strategies used in pre-processing data to prepare it for patient clustering analyses and to
predict patient outcomes.
Step
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Strategy
Drop patients and features where the amount of missing data would likely impact their reliability and are
likely to also impact model precision (e.g., patients with fewer than 100 sessions, features with 60% or
more missing data).
Identify and Winsorize outliers.
Impute missing data by chained equation (Buck, 1960; van Buuren & Groothius-Oudshoorn, 2011).
Use zip code for feature engineering (e.g., add neighborhood and economic SDOH proxies; convert to US
region and one-hot encode)
Aggregate and quantify patient developmental and familial characteristics (e.g., age, number of siblings).
Aggregate intervention characteristics across skill acquisition domains.
Aggregate intervention characteristics across reduction targets, intensities, and functional assessments.
Aggregate and quantify medical and behavioral health comorbidities.
Aggregate and quantify patient progress, generally, as well as across specific skill domains.
Aggregate and quantify hours per week of ABA contact per patient for the duration they are in the dataset.
Merge all datasets together aggregated at the level of patient-week (e.g., continuous variables convert to
arithmetic mean; categorical convert to one-hot encoded; ordinal convert to median).
Examine how aggregation influenced feature distributions and modify where significantly impacted.
Normalize feature scales using min-max to 0-1.
AI SYSTEM TO PREDICT ABA OUTCOMES
7
similar when considering the 48 variables that
comprise the final analytic dataset.
Table 3 shows the patient clustering
(N=31,294) fit metrics for four algorithms wherein
each takes a unique definition for how to define a
cluster3. Overall, maximum Silhouette Coefficients
ranged between 0.25-0.47, maximum CalinskiHarabsz indices ranged between 6,086.6613,718.52, and optimal patient clusters ranged
between 8-to-56 depending on the algorithm and
level of granularity a researcher or practitioner is
interested in obtaining or is practically useful for
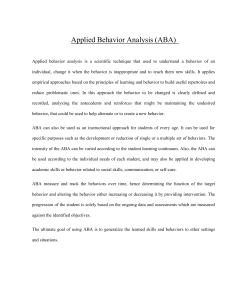
them. Figure 3 shows a three-dimensional plot of
the clustering results for agglomerative hierarchical
clustering wherein the underlying assumptions are
likely best justified based on the function of
clustering patients with ASD in the current context
(for a comprehensive treatment of these
assumptions see Hennig et al., 2016). Each color in
the plot represents a unique patient cluster and
each marker represents a unique patient.
A natural question is exactly how each of these
patient clusters differ from each other. Figure 4
shows 10 of the individual patient characteristics
included in the current analysis. Five of those
patient characteristics are variables that have been
associated with differential patient outcomes
following contact with ABA in past research (top five
panels). Five of the patient characteristics in Figure
4 have no known previous publications associating
the variable with differential patient outcomes
following contact with ABA at the time of this writing
(bottom five panels).
Figure 3. Example patient cluster visual using agglomerative
hierarchical clustering. Each color represents a unique cluster
as identified by the algorithm. Each individual marker
represents a single patient.
There are two important observations to be
made based on the results above and considering
the scope of this current manuscript. First, the
clustering algorithms consider all 48 variables
simultaneously with each cluster being a unique
combination of all patient characteristics. So, the
ten variables shown in Figure 4 should be
considered a demonstration of what this system
currently allows us to do. The current results should
be considered preliminary and will continue to
improve as the AI system collects more data and
our methodologies are further refined. Second, a
follow-up manuscript is in preparation that provides
significantly greater detail around the patient
Table 3. Overview of the best clustering fit metrics for the algorithms tested (N=31,294). For both metrics, a higher score indicates
better clustering.
Clustering Algorithm
Silhouette
Calinski-Harabasz
Optimal Clusters
k-Means
0.25
8,169.60
30
Agglomerative Hierarchical
0.47
13,718.52
8
HDBSCAN
0.37
2,377.78
56
BIRCH
0.39
6,086.66
18
Silhouette equals the ratio of average dissimilarity of each observation with its own cluster (a i) relative to the average dissimilarity to
𝑏 −𝑎
observations in the closest other cluster (bi)(Halkidi et al., 2016). This can be written as an equation: 𝑠𝑖 = 𝑖 𝑖 }. Calinski-Harabasz
max{𝑎𝑖 ,𝑏𝑖
equals the ratio of the sum of between-cluster dispersion and of within-cluster dispersion (Halkidi et al., 2016). As an equation:
𝑡
CH(CK)=
𝑡𝑟𝑎𝑐𝑒(∑𝐾
̅ 𝑗 −𝐱̅)(𝐱̅𝑗 −𝐱̅) )
𝑗=1 𝑛𝑗 (𝐱
𝑡𝑟𝑎𝑐𝑒(∑𝐾
̅ 𝑖 −𝐱̅𝑗 )(𝐱̅𝑖 −𝐱̅𝑗 )𝑡
𝑗=1 ∑𝑐(𝑖)=𝑗(𝐱
×
𝑛−𝐾
𝐾−1
. In more lay terms, Silhouette coefficients provide a sense of how well an observation
belongs to its assigned cluster compared to any other cluster; and Calinski-Harabasz indices indicate how well partitioned the
clusters are.
3
The reader is referred to Hennig et al. (2016) for a
review of the assumptions and underlying
mathematics used to define a cluster via each
algorithm.
AI SYSTEM TO PREDICT ABA OUTCOMES
8
Figure 4. Demonstration of patient characteristics that differ among agglomerative hierarchical clusters. The top panel shows
differences in variables previously published in the literature. The bottom panels show differences in variables related to health that
could logically impact progress.
clustering methods, their evaluation, and how
these results were derived. Again, the scope of
this manuscript is to highlight the totality of the
system and what it can do. The first author can
be contacted for specific methodological
questions in the interim.
Supervised Machine Learning: Predicting
Patient Outcomes. Supervised machine
learning refers to a suite of mathematical and
algorithmic techniques aimed at learning the
underlying structure in data where the answer is
known (Müller & Guido, 2017). For our purposes,
the answer we know and want to predict is how
many goals each patient mastered during a given
period of time. The goal of supervised machine
learning is to create a mathematical equation (or
set of equations) that relates the patients-related
and ABA-related characteristics to how many
goals they mastered. Once built, the model can
be used to predict how many goals a new patient
is likely to master based on their unique set of
characteristics.
Different statistical and machine learning
algorithms range from less (linear regression) to
more (ensemble models) complex. Less complex
models are often more parsimonious though can
sometimes be less accurate than more complex
models. In contrast, more complex models are
often more accurate though, due to their
complexity, can sometimes be more difficult for
users to intuitively understand how the input
variables relate to the predicted output. As a
result of the tradeoff between model simplicity
and complexity, we analyzed a series of
increasingly complex statistical and machine
learning models for how well they could predict
patient progress as a function of contact with ABA
and each patient’s unique characteristics.
Table 4 shows an overview of the fit metrics
when assessing each algorithm using 10-fold
cross-validation with 80%-20% test-train splits.
That is, we started by first randomly splitting our
data into two datasets. One dataset was used to
train the model (80% of all observations) and a
holdout dataset was used to test the predictive
capabilities of the model (20% of all
observations). We then repeated this process
nine more times using a different selection of testtrain splits of the dataset with each iteration.
Table 4 shows the arithmetic mean of the fit (r2)
and loss (mean absolute error; MAE) metrics for
each of the 10-folds for each of the algorithms
using their default parameters.
Overall, the random forest regressor
algorithm led to the lowest MAE values across
Table 4. Average fit and loss metrics from 10-fold crossvalidation using the test data sets not included in model
training.
Algorithm
r2
MAE
Linear Regression
k-Nearest Neighbors
Support Vector Regressor
Random Forest
AdaBoost
0.90
0.91
0.99
0.99
0.88
1.30
1.27
1.06
1.04
1.32
AI SYSTEM TO PREDICT ABA OUTCOMES
both training and test datasets. To build a final
predictive model, we conducted hyperparameter
tuning via grid search across model parameters
of the number of trees and the maximum depth
allowed. The left panel in Figure 5 shows the
results of using the final model built using the
random forest algorithm. The final fit and loss
metrics of the top performing model with the
holdout test data were r2 = .99 and MAE = 1.12.
The right panel in Figure 5 shows the results of
using linear regression similar to researchers in
past published studies. Fit and loss metrics using
linear regression were r2 = .90 and MAE = 1.82,
respectively. Of note, the obtained r2 using linear
regression is .23 points higher than the highest
known previous model predicting goals mastered
by individuals with ASD as a function of
contacting ABA (Linstead et al., 2017b reported
an r2 of .67 for motor goals, MAE was
unreported). The predictive model using machine
learning was .32 points higher.
We conducted the same set of analyses for
each patient cluster in the dataset. That is, we
first isolated the data to only the patients in a
given cluster, assessed each algorithm using 10fold cross-validation with 80%-20% test-train
splits, conducted hyperparameter tuning via grid
search to identify a top model, and then made
predictions of patient progress on the holdout test
set. When predicting goals mastered within
unique clusters, r2 values ranged from .95-.99
and MAE values ranged 1.12-1.45. Of note, the r2
9
values obtained here are ~.20-.24 higher than the
cluster specific r2 values observed by past
researchers which ranged from .64 to .75
(Stevens et al., 2019). Thus, the AI system
approach taken in this work appears to be a
significantly more precise method for predicting
patient progress compared to previously
published research. This appears true, overall, as
well as within unique patient clusters.
As with the section on patient clustering,
there are two important observations to be made
based on the results above and considering the
scope of this manuscript. First, this system
continuously receives more patient data and we
are actively identifying better ways to collect and
incorporate data spanning a greater number of
variables. Thus, the results in this section should
be considered a demonstration of what this
system currently allows us to do. The current
results should be considered preliminary and will
continue to improve as the AI system collects
more data and our methodologies are further
refined. Second, a follow-up manuscript is in
preparation that provides significantly greater
detail around using machine learning to predict
patient outcomes across goals mastered and
changes in VBMAPP scores. Again, the scope of
this manuscript is to highlight the totality of the
system and what it can do. The first author can
be contacted for specific methodological
questions in the interim.
Figure 5. Predicted vs. observed goals mastered for the models derived using the random forest algorithm (left panel) and using linear
regression (right panel). In each panel, the red line shows where exact matches between observed and predicted occur.
AI SYSTEM TO PREDICT ABA OUTCOMES
Deploy as API endpoint. The last phase in
the AI Engine is to make the final, top-performing
models available to users of a technological
platform. Deploying machine learning models can
be accomplished in a number of ways (see
Treveil et al., 2020 for an introductory text). For
the technology ecosystem at RethinkFirst,
Microsoft Azure makes it easy to deploy machine
learning models as a REST API endpoint. Users
with access to this technology system can then
call the API endpoint with the requisite data fields
and have the model return a value. What value
gets returned, however, would vary with the use
case and how the API endpoint is embedded
within the product.
USE CASES
Recommending
ABA
Dosage.
A
straightforward application of the finalized model
would be to have the model recommend the
optimal hours per week relative to goals
mastered. Figure 6 shows hypothetical data
wherein patient characteristics can be passed to
the predictive model along with a range of hours
of ABA the patient might contact. Such doseresponse curves are commonly used to identify
optimal therapeutic effect of an intervention in
behavioral pharmacology (e.g., Dews, 1955) and
have been used previously for analyses specific
10
to ABA (e.g., Ostrovsky et al., 2022; Stevens et
al., 2019). For each patient, there is likely to be a
point wherein little-to-no further progress would
be predicted if more hours of ABA were contacted
(the large filled-in circles in Figure 6). This point
of little-to-no further return could then be the
recommended hours per week of ABA.
Observed vs. Expected Patient Outcomes.
Another straightforward application of the
finalized model would be to retroactively compare
a patient’s actual progress to expected progress.
Specifically, a patient’s unique characteristics
could be passed to the model along with the
hours of ABA they contacted. The model would
return the number of goals expected to be
mastered based on other patients who present
with similar characteristics and received similar
amounts of ABA. By comparing the observed
patient progress to the expected patient progress,
the provider or their supervisor can get feedback
on how well they are providing services with
current clients. In turn, providers can follow-up
with specific patients and the supervising BCBAs
to identify why they are achieving less than
expected outcomes. And, for patients for whom
the provider is observing greater than expected
outcomes, providers can follow-up to identify if
there are variables predicting better success that
they can use with other patients to further
improve outcomes. Further, these data and the
underlying models could be leveraged by payors
Figure 6. Example use case wherein the predictive model produces an expected dose-response curve based on hours per week of
ABA along with the patient characteristics that determine cluster assignment. Each color would be a unique dose-response curve
predicted for a patient based on their unique profile.
AI SYSTEM TO PREDICT ABA OUTCOMES
and providers alike to support and enable their
unique value-based care initiatives.
Associated Social Determinants of Health.
Many aspects of our social environment have
been repeatedly shown to play a role in patient
outcomes and are referred to as social
determinants of health (e.g., Braverman &
Gottlieb, 2014). Because several of these
variables are included in the model, the user
could analyze these data to help identify and
potentially mitigate the effects of these variables
on patient outcomes. For example, similar to the
previous use case, a provider could
systematically identify how well each patient in
their organization or on their caseload is
performing relative to expected outcomes. The
provider could then determine whether
differences between observed and expected
outcomes were associated with unique variables
known to be a social determinant of health
(SDOH; e.g., race, neighborhood walkability,
income, education). By identifying specific SDOH
that impact the patients on their caseload or in
their organization, providers would better know
how to identify resources for those clients that
might mitigate this effect and improve their overall
outcomes. Similar to feedback on provider
performance, analyses related to SDOH could be
leveraged by payors and providers alike to
support and enable their unique value-based care
initiatives.
LIMITATIONS AND FUTURE DIRECTIONS
There are several limitations to the current
patent-pending AI system and underlying AI
Engine, each of which points to future directions
for building upon and improving the AI system as
described herein. The first limitation is that the
patients included in this work do not
comprehensively account for all possible
combinations of unique individual characteristics
that an individual with ASD might present to ABA
with (i.e., sampling bias). Nevertheless, the
current study did contain data from 31,294
individuals with ASD making it the largest known
published study on individuals with ASD at the
time of writing4. Thus, though all research and
technological systems will necessarily be
incomplete in terms of the included sample
(Jennings & Cox, 2023), the sample size in the
present work is 1.51 times larger than the next
4
February, 2023.
11
closest study (Lingren et al., 2016), 6.35 times
larger than the third largest study (Doshi-Velez et
al., 2014), and 142.25 times larger than the
median sample size used in previous cluster
analyses for individuals with ASD (ParlettPelleriti, 2022). For past work predicting patient
outcomes as a function of ASD, the current study
is 21.32 times larger than the sample size of the
second largest study (Linstead et al., 2017b).
A second limitation and area for future
direction relates to the variables chosen for
inclusion in patient clustering and for predicting
patient progress. We used domain expertise and
past published research to identify and include
variables with a logical or known relationship to
patient progress following contact with ABA.
However, behavior analysts have historically
underreported demographic variables within the
clinical literature (e.g., Jones et al., 2020) and
have only recently begun to consider how SDOH
might influence outcomes (e.g., Wright, 2022).
Further, it is possible that a different approach to
aggregating ABA session characteristics and
treatment plans would lead to better models—
work we are feverishly conducting. As noted in
the introduction, the purpose of this manuscript
was to showcase how this system currently
operates and its current effectiveness. Future
work using this AI system will include further
exploration of variable inclusion and feature
engineering.
A final area for future research involves more
direct measures around how the outputs of this AI
system impact clinical decision-making and
stakeholders more broadly. As shown in Figure 1,
the output of this system can inform a variety of
products for a variety of end users. By examining
how end users behave before and after use of the
AI system, future research will be able to identify
if and how clinician decision-making changes as
a function of the system and how those decisions
might influence patient progress. Outside of the
AI system and end products themselves,
however, there are likely to be additional,
unmeasured variables that interact with this
information to multiply influence the decisions
behavior analysts make. Without knowledge of
what those variables might be, collaboration with
end users will be crucial for identifying if and
where those additional variables might need to be
added to the AI system as a whole.
AI SYSTEM TO PREDICT ABA OUTCOMES
SUMMARY
All stakeholders alike would benefit from the
ability to predict likely patient progress as a
function of contact with ABA therapy and the
patient’s unique characteristics. Past researchers
have sought to describe and predict how
individuals with ASD are likely to benefit from
ABA therapy. However, the results of these
studies have had limited generalizability due to
sample sizes, simple modeling approaches, and
a lack of including robust patient cluster analyses
to individualize patient predictions. Further, few
studies have directly converted the insights
gained into a technology that others could
incorporate into their treatment settings to
improve patient outcomes. Above, we described
how we have built and are leveraging a patentpending AI system that: integrates the continuous
and ongoing collection of patient data in
treatment outcomes and patient characteristics;
allows us to identify robust patient clusters unique
from previous literature given its significantly
larger sample size; combines patient cluster
characteristics with ABA hours per week to
predict within 1.12 goals mastered within a 12month ABA treatment period; how the models can
be deployed back into a technological system for
user interaction; and three subsequent use cases
in: (a) real-time recommendations of ABA dosage
based on unique patient characteristics; (b)
feedback on actual patient outcomes relative to
expected outcomes; and (c) how patient progress
varies along social determinants of health.
REFERENCES
Ansari, W. E., Ssewanyana, D., & Stock, C. (2018).
Behavioral health risk profiles of undergraduate university
students in England, Wales, and Northern Ireland: A cluster
analysis. Frontiers in Public Health, 6, 120.
https://doi.org/10.3389/fpubh.2018.00120
Association of Professional Behavior Analysts (2020). ABA
Autism Guidelines: Applied Behavior Analysis Practice
Guidelines for Autism Spectrum Disorder. Retrieved from:
https://casproviders.org/wp-content/uploads/2020/03/ABAASD-Practice-Guidelines.pdf
Autism Commission on Quality (2022). ACQ Applied Behavior
Analysis Accreditation program standards and guide
(version
1.0).
Retrieved
from:
https://autismcommission.org/standards/
Autism Speaks (2022). Autism statistics and facts. Retrieved
from: https://www.autismspeaks.org/autism-statistics-asd
Baskar, S. S., Arockiam, L., & Charles, S. (2013). A
systematic approach on data pre-processing in data
mining. Compusoft: An International Journal of Advanced
Computer Technology, 2(11), 335-339.
12
Behavior Analyst Certification Board (2020). Ethics code for
behavior analysts. https://bacb.com/wp-content/ethicscode-for-behavior-analysts/
Behavioral Health Center of Excellence (2022). 2022
standards and new accreditation model. Retrieved from:
https://www.bhcoe.org/2022-standards-and-newaccreditation-model/
Bhargava, S., & Loewenstein, G. (2015). Choosing a health
insurance plan: Complexity and consequences. Journal of
the American Medical Association, 314(23), 2505–2506.
https://doi.org/10.1001/jama.2015.15176
Braverman, P., & Gottlieb, L. (2014). The social determinants
of health: It’s time to consider the causes of the causes.
Public
Health
Reports,
129(Suppl
2),
19-31.
https://doi.org/10.1177%2F00333549141291S206
Centers for Disease Control and Prevention (2021). Data &
Statistics on Autism Spectrum Disorder. Retrieved from:
https://www.cdc.gov/ncbddd/autism/data.html
Charron, E., Yu, Z., Lundahl, B., Silipigni, J., Okifuji, A.,
Gordon, A. J., ... & Cochran, G. (2023). Cluster analysis to
identify patient profiles and substance use patterns among
pregnant persons with opioid use disorder. Addictive
Behaviors
Reports,
17,
100484.
https://doi.org/10.1016/j.abrep.2023.100484
De Groot, K., & Thurik, R. (2018). Disentangling risk and
uncertainty: When risk-taking measures are not about risk.
Frontiers
in
Psychology,
9,
2194.
https://doi.org/10.3389/fpsyg.2018.02194
Dews P. B. (1955). Studies on behavior. I. Differential
sensitivity to pentobarbital of pecking performance in
pigeons depending on the schedule of reward. The Journal
of Pharmacology and Experimental Therapeutics, 113(4),
393–401.
Doshi-Velez, F., Ge, Y., & Kohane, I. (2014). Co-morbidity
clusters in autism spectrum disorders: an electronic health
record timeseries analysis. Pediatrics, 133(1), e54–e63.
Eldevik, S., Hastings, R. P., Hughes, J. C., Jahr, E., Eikeseth,
S., & Cross, S. (2009). Using participant data to extend the
evidence base for intensive behavioral intervention for
children with autism. Journal of Autism and Developmental
Disorders,
39(11),
1302–1310.
https://doi.org/10.1007/s10803-009-0732-7
Granpeesheh, D., Dixon, D. R., Tarbox, J., Kaplan, A. M., &
Wilke, A. E. (2009). The effects of age and treatment
intensity on behavioral intervention outcomes for children
with autism spectrum disorders. Research in Autism
Spectrum
Disorders,
3(4),
1014-1022.
https://doi.org/10.1016/j.rasd.2009.06.007
Halkidi, M., Vazirgiannis, M., & Hennig, C. (2016). Methodindependent indices for cluster validation and estimating
the number of clusters. In: C. Henning, M. Meila, F.
Murtagh, & R. Rocci (Eds.), Handbook of Cluster Analysis
(pp. 595-618). Taylor & Francis Group. ISBN: 978-1-46655189-3
Han, P. K. J., Klein, W. M. P., & Arora, N. K. (2012). Varieties
of uncertainty in health care: A conceptual taxnomy.
Medical
Decision
Making,
31(6),
828-838.
https://doi.org/10.1177%2F0272989X11393976
Hennig, C., Meila, M., Murtagh, F., & Rocci, R. (2016).
Handbook of Cluster Analysis. Taylor & Francis Group.
ISBN: 978-1-4665-5189-3
AI SYSTEM TO PREDICT ABA OUTCOMES
Hennig, C., & Meila, M. (2016). Cluster analysis: An overview.
In: C. Henning, M. Meila, F. Murtagh, & R. Rocci (Eds.),
Handbook of Cluster Analysis (pp. 1-20). Taylor & Francis
Group. ISBN: 978-1-4665-5189-3
Hewlett, M. M., Raven, M. C., Graham-Squire, D., Evans, J.
L., Cawley, C., Kushel, M., & Kanzaria, H. K. (2022).
Cluster analysis of the highest users of medical, behavioral
health, and social services in San Francisco.Journal of
General Internal Medicine. https://doi.org/10.1007/s11606022-07873-y
13
Ostrovsky, A., Willa, M., Cho, T., Strandberg, M., Howard, S.,
& Davvitian, C. (2022). Data-driven, client-centric applied
behavior analysis treatment-dose optimization improves
functional outcomes. World Journal of Pediatrics.
https://doi.org/10.1007/s12519-022-00643-0
Papanicolas, I., Woskie, L. R., & Jha, A. K. (2018). Health care
spending in the United States and other high-income
countries. Journal of the American Medical Association,
319
(10),
1024–1039.
https://doi.org10.1001/jama.2018.1150
Jennings, A., & Cox, D. J. (2023). Starting the Conversation
Around the Ethical Use of Artificial Intelligence in Applied
Behavior
Analysis.
PsyArXiv
Preprints.
https://doi.org/10.31234/osf.io/zmn28
Patel, A. A. (2019). Hands-on unsupervised learning using
Python: How to build applied machine learning solutions
from unlabeled data. O’Reilly Media, Inc. ISBN: 978-1-49203564-0
Jones, S. H, St. Peter, C. C., & Ruckle, M. M. (2020).
Reporting of demographic variables in the Journal of
Applied Behavior Analysis. Journal of Applied Behavior
Analysis,
53(3),
1304-1315.
https://doi.org/10.1002/jaba.722
Parlett-Pelleriti, C. M., Stevens, E., Dixon, D.. & Linstead, E.
J. (2022). Applications of unsupervised machine learning in
autism spectrum disorder research: A Review. Review
Journal of Autism and Developmental Disorders.
https://doi.org/10.1007/s40489-021-00299-y
Larsson, E. V. (2012). Applied behavior analysis (ABA) for
autism: What is the effective age range for treatment? The
Lovaas Institute for Early Intervention Midwest
Headquarters
White
Paper.
Retrieved
from:
https://childsplayautism.com/wp-content/uploads/EffetiveTreatment-Range-1.pdf
Saleem, A., Asif, K. H., Ali, A., Awan, S. M., & Alghamdi, M.
A. (2014). Pre-processing methods of data mining.
IEEE/ACM 7th International Conference on Utility and
Cloud
Computing,
451-456.
https://doi.org/10.1109/UCC.2014.57.
Levy, H. C., Worden, B. L., Davies, C. D., Stevens, K., Katz,
B. W., Mammo, L., Diefenbach, G. J., & Tolin, D. F. (2020).
The dose-response curve in cognitive-behavioral therapy
for anxiety disorders. Cognitive Behaviour Therapy, 49(6),
439-454. https://doi.org/10.1080/16506073.2020.1771413
Lingren, T., Chen, P., Bochenek, J., Doshi-Velez, ManningCourtney, P., Bickel, J., …, & Savova, G. (2016). Electronic
health record based algorithm to identify patients with
autism spectrum disorder. PLoS ONE, 11(7), e0159621.
https://doi.org/10.1371/journal.pone.0159621
Linstead, E., Dixon, D. R., French, R., Granpeesheh, D.,
Adams, H., German, R., …, & Kornack, J. (2017a). Intensity
and learning outcomes in the treatment of children with
autism spectrum disorder. Behavior Modification, 41(2),
229-252. https://doi.org/10.1177/0145445516667059
Linstead, E., Dixon, D. R., Hong, E., Burns, C. O., French, R.,
Nocak, M. N., & Granpeesheh, D. (2017b). An evaluation
of the effects of intensity and duration on outcomes across
treatment domains for children with autism spectrum
disorder.
Translational
Psychiatry,
7(9),
e1234.
https://doi.org/10.1038%2Ftp.2017.207
Meyer, A. N. D., Giardina, T. D., Khawaja, L., & Singh, H.
(2021). Patient and clinician experiences of uncertainty in
the diagnostic process: Current understanding and future
directions. Patient Education and Counseling , 104(11),
2606-2615. https://doi.org/10.1016/j.pec.2021.07.028
Müller, A. C., & Guido, S. (2017). Introduction to Machine
Learning with Python. O’Reilly Media, Inc. ISBN: 978-1449-36941-5
National Autism Center. (2009). National Standards Project:
Phase
1.
Retrieved
from:
https://nationalautismcenter.org/national-standards/phase1-2009/
National Autism Center (2015). National Standards Project,
Phase 2. Randolph, MA: National Autism Center. Retrieved
from:
https://www.nationalautismcenter.org/nationalstandards/
Stevens, E., Dixon, D. R., Novack, M. N., Granpeesheh, D.,
Smith, T., & Linstead, E. (2019). Identification and analysis
of behavioral phenotypes in autism spectrum disorder via
unsupervised machine learning. International Journal of
Medical
Informatics,
129,
29–36.
https://doi.org/10.1016/j.ijmedinf.2019.05.006
Towards AI (2023). Centroid neural network : An efficient and
stable
clustering
algorithm.
Retrieved
from:
https://towardsai.net/p/l/centroid-neural-network-anefficient-and-stable-clustering-algorithm
Treveil, M., & Dataiku Team (2020). Introducing MLOps: How
to Scale Machine Learning in Enterprise. O’Reilly Media,
Inc. ISBN: 978-1-492-08329-0
World Health Organization (2015). Health systems financing:
The path to universal coverage. Retrieved from:
https://apps.who.int/iris/bitstream/handle/10665/155002/W
HO_HIS_SDS_2015.6_eng.pdf
Wright, P. (2022). Social determinants of health and applied
behavior analysis: Leveraging the connection to make the
world a better place. CEU Event available from:
https://behavioruniversity.com/social-determinants-healthaba
Zoladz, P. R., & Diamond, D. M. (2008). Linear and non-linear
dose-response functions reveal a hormetic relationship
between stress and learning. Dose-Response: a
publication of International Hormesis Society, 7(2), 132–
148. https://doi.org/10.2203/dose-response.08-015.Zol