NLPHL Treatment Approaches: State of the Art Updates
advertisement

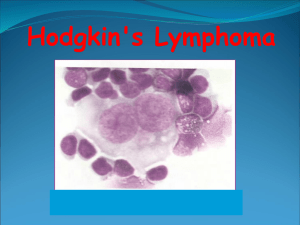
6/26/23, 5:39 PM SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… Clinical Lymphoma Myeloma and Leukemia Volume 23, Issue 7, July 2023, Pages 471-476 Review Article SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymphoma Michael S. Binkley 1 , Ranjana H. Advani 2 Show more Outline Share Cite https://doi.org/10.1016/j.clml.2023.03.014 ↗ Get rights and content ↗ Abstract Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is a rare variant of Hodgkin lymphoma characterized by a persistent risk of relapse but an excellent overall survival. Historically, it was treated similarly to classic Hodgkin lymphoma, but efforts have been made to deintensify treatment due to risk of late toxicity associated with intensive therapy. For patients with completely resected stage IA NLPHL, no further treatment may be considered, particularly for pediatric patients. For those with stage I-II NLPHL without risk factors such as B symptoms, sites>2, or variant pattern histology, lower intensity treatment with radiotherapy or chemotherapy alone may be sufficient. However, combined modality therapy is a standard treatment for favorable and unfavorable risk stage I-II NLPHL associated with excellent progression-free and overall survival rates. For patients with advanced stage NLPHL, the optimal chemotherapy is not defined, but R-CHOP appears to be an effective treatment. Efforts to study NLPHL through multicenter collaborative efforts are crucial to develop evidence based and individualized treatments for patients with NLPHL. Previous Next Keyword Management; Hodgkin lymphoma; Adolescents; Young adults Introduction Nodular lymphocyte-predominant lymphoma (NLPHL) is a rare subtype of Hodgkin lymphoma representing approximately 5% of newly diagnosed cases.1 Age of incidence is similar to that of classic Hodgkin lymphoma (cHL) with a peak occurring in the fourth decade of life.2 NLPHL has a male predominance, is diagnosed at early stages in approximately 75% of cases, and rarely is bulky or involves the mediastinum as shown in Figure 1A.3,4 Many years after its recognition as a distinct subtype of Hodgkin lymphoma, NLPHL was reported to have a distinct clinical course from cHL characterized by late relapses but an overall indolent course with excellent survival.5 Given its excellent prognosis and young age of diagnosis, significant efforts have been made to deintensify treatment to limit late therapy related effects for patients.6, 7, 8 Due to its rarity, most large studies guiding management are retrospective.2,3 https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 1/11 6/26/23, 5:39 PM SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… Download : Download high-res image (1022KB) Download : Download full-size image Figure 1. Pathologic factors for NLPHL. Panel A demonstrates the anatomic sites most commonly involved for patients diagnosed with NLPHL.4 Panel B shows an excisional biopsy specimen with a focus of variant pattern D emphasizing the importance of characterizing the full extent of the involved site. Diagnosis Workup for NLPHL is similar to that of cHL, and given the importance of assessing the immunoarchitectural patterns, excisional biopsy is essential when at all possible.9,10 As shown in Figure 1B, a core needle biopsy may likely not capture representation of all of the immunoarchitectural patterns present which can exist as small foci. NLPHL is avid on PET-CT similar to cHL, and therefore, bone marrow biopsy should only be considered for patients with cytopenias, B symptoms, or if having focally avid skeletal lesions.11 Pathology The malignant lymphocyte predominant cell (LP cell), is of B-cell origin and retains its B-cell receptor with expression of B-cell proteins (CD19/20/79).9 However, there are very rare cases of NLPHL with LP cells negative for expression of CD20.12 Similar to cHL, the LP cell represents approximately 1 out of every 100 cells and is surrounded by a vast abundance of immune cells.9 Characterization of the microenvironment resulted in 6 immunoarchitectural patterns being described, A through F.13 Patterns A to D have nodularity and the diffuse patterns E and F require at least a focus of nodularity to retain a diagnosis of NLPHL versus T-cell/Histiocyte-rich large B-cell lymphoma (THRLBCL).9 Patients with variant pattern C to E more frequently present with advanced stage and bone marrow involvement.14, 15, 16 Several studies have reported a worse prognosis for patients with variant patterns C through F in both pediatric and adult patients, but the number of patients with pattern F in reported cohorts remains very few if any.3,17, 18, 19, 20 As many patients have multiple immunoarchitectural patterns present (see Figure 1B as an example), and as no studies have thoroughly evaluated whether increasing percentages of variant patterns portend a worse prognosis, the presence of any minor percentage of variant pattern is typically interpreted as variant pattern NLPHL. Due to the rarity of the LP cells amidst a vast abundance of immune cells and the nonspecific CD20 positivity, genetic sequencing of NLPHL remains very challenging to date. Genotyping efforts have demonstrated overlap of the observed somatic mutations seen for variant NLPHL and THRLBCL, while mutations in immune surveillance pathways for typical NLPHL are similar to those observed for cHL.21 Although there has been large success in genotyping cHL using circulating tumor DNA isolated from patient plasma,22 similar efforts for NLPHL are lacking but a small pediatric cohort demonstrated a lower allele frequency for 3 patients with NLPHL as compared to those with cHL, suggesting genotyping NLPHL using ctDNA may be more challenging than cHL.23 Finally, gene expression phenotyping has shown LP cells have greater similarity to Reed-Sternberg cells as opposed to malignant cells from other B-cell lymphomas.24 Given the existing biologic understanding, there have been 2 classifications proposed for NLPHL. The International Consensus Classification of Mature Lymphoid Neoplasms proposed reclassifying NLPHL as nodular lymphocyte-predominant B-cell lymphoma (NLPBL).25 However, the WHO concluded there was not enough biologic evidence to consider such a renaming currently. Additionally, the WHO recommends reporting patterns qualitatively given the aforementioned unknown utility of reporting percentage of variant pattern present.26 The classification of NLPHL as either a subtype of Hodgkin lymphoma or a separate B-cell lymphoma remains to be clarified with further biologic evidence, but it should be managed as unique from cHL or other B-cell lymphomas. https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 2/11 6/26/23, 5:39 PM SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… Management by Clinical Stage We have summarized treatment options for pediatric and adult patients by clinical stage in Table 1 and as summarized below. Table 1. Management Options by Stage and Patient Age (Pediatric≤21 Years53 and Adult≥16 Years54) Stage IA completely Age Management Systemic Therapy Radiotherapy Reference Pediatric Observation Appel et al.7 Adult Consider Binkley et al.3, Borchmann observation et al.8 resected I-IIA incompletely Pediatric Chemotherapy +/- resected 3 cycles CVP+/- R Response adapted Shankar et al.17 30 Gy Eichenauer et al.6, Binkley RT Adult Radiotherapy et al.3 alone I-IIB Pediatric Chemotherapy +/- 2cycles OEPA–2cycles Response adapted (21- Mauz-Korholz et al.28, RT COPDac +/- R 30 Gy) Friedman et al.53 20a-30 Gy Fuchs et al.32, Eich et al.54 Mauz-Korholz et al.28 non-contiguous involvement or 4 cycles ABVE-PC Adult Chemotherapy +/- 4 cycles of R-CHOP RT or 2*-4 cycles R-ABVD III-IV Pediatric Chemotherapy +/- 2cycles OEPA–4cycles Response adapted RT COPDac +/- R (25.5-30 Gy) Adult Chemotherapy 6 cycles R-CHOP Fanale et al.34 Adult - low disease burden Rituximab alone 4 doses R +/- R Advani et al.30 maintenance Adult - low disease burden and Active asymptomatic surveillance Borchmann et al.8 Abbreviations: ABVD = Adriamycin, bleomycin, vinblastine, dacarbazine; ABVE-PC = adriamycin, bleomycin, vincristine, etoposide, cyclophosphamide, and prednisone; COPDAC = cyclophosphamide, oncovin, prednisone, dacarbazine; CVP = cyclophosphamide, vinblastine, prednisone; OEPA = oncovin, etoposide, prednisone, adriamycin; R = rituximab; RT = radiotherapy. a *=if favorable by the German Hodgkin Study Group criteria Stage IA Without Risk Factors Completely Excised Following early reports of pediatric patients receiving no further treatment after surgical excision enjoying an encouraging rate of disease control,27 there has been interest in observing patients with stage IA NLPHL without adverse risk factors following complete surgical resection confirmed by PET-CT.28 The Children's Oncology Group conducted a prospective clinical trial investigating no further treatment for 52 pediatric patients following complete excision confirmed by postoperative PET-CT with an encouraging 5-year event-free survival of 77.1% as shown in Figure 2A.7 In that cohort, all relapses remained early stage involving either the initial site or an adjacent site with 13 of 52 patients ultimately relapsing.7 Large retrospective studies in adult patients offered no further treatment after surgical excision have also shown approximately three-quarters of patients may not develop progressive lymphoma within 5 years, but the pattern of relapse differs greatly from pediatric populations as at least half of patients go on to develop advanced stage NLPHL.3,8 Thus, caution must be used when employing observation for adult patients after excision as there may be an opportunity to definitively treat NLPHL using low intensity techniques such as radiotherapy alone that may be lost if choosing observation after surgical excision. https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 3/11 6/26/23, 5:39 PM SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… Download : Download high-res image (824KB) Download : Download full-size image Figure 2. Selected studies reporting outcomes for patients with NLPHL. Panel A shows outcomes for patients with Stage IA. Panel B shows outcomes for patients with stage I to II favorable NLPHL. Panel C shows results from a single study for patients with stage I to II unfavorable NLPHL by the German Hodgkin Study Group criteria. Panel D shows results for patients with stage III to IV NLPHL. Corresponding references are listed in superscript. Abbreviations: PFS = progression-free survival, EFS = event-free survival, OS = overall survival, RT = radiotherapy, CT = chemotherapy alone, CMT = combined modality therapy. Stage IA-IIB For stage IA incompletely excised without risk factors, radiotherapy alone using limited volumes is a standard treatment.3,6,29 As demonstrated by a large retrospective analysis of pooled data from the German Hodgkin Study Group prospective trials from 1988 to 2009, 8-year progression-free survival (PFS) was excellent after involved-field radiotherapy alone (91.9%) and not significantly different from extended-field radiotherapy or combined modality therapy.6 Further shrinkage of radiotherapy volumes using involved-site radiotherapy has also shown high rates of disease control in a cohort reported by Pinnix et al. with just over 2.5 years of patient follow up.29 Although rituximab alone achieves a high level of clinical response, it does not offer durable disease control as shown in Figure 2A.6,30 As the majority of patients with NLPHL do not present with mediastinal involvement (Figure 1A), many late effects associated with radiotherapy including cardiovascular toxicity and risk of secondary breast cancer observed for cHL do not pose significant long term risks.3 Although data is emerging, patients with variant immunoarchitectural patterns should be considered for combined modality therapy as a large retrospective study of adult patients with early stage NLPHL demonstrated worse progress-free survival for patients with variant pattern NLPHL treated with radiotherapy alone.3 For contiguous stage I to II favorable risk NLPHL with fewer than 3 Ann Arbor sites of involvement, radiotherapy alone with a dose of 30 Gy is a reasonable option with a 5-year PFS of 91.1% in a large multicenter retrospective study (Figure 2B).3 As an alternative treatment for patients with stage IA to IIA limited extent of involvement (amenable for radiotherapy), investigators at University of British Columbia reported excellent PFS (89%) for patients treated with ABVDx2 followed by a PET-directed approach with 86% receiving chemotherapy alone without radiotherapy (Figure 2B).31 Additional benefits of combined modality therapy include the potential for lower radiotherapy dose as per the German Hodgkin Study Group HD16 trial and shrinkage of involved nodal site decreasing radiotherapy exposure to critical organs.32,33 For patients with stage I to II unfavorable risk NLPHL with B-symptoms, a larger number of involved nodal stations, or variant pattern histology, combined modality therapy should be considered as it has demonstrated robust disease control in a pooled analysis of prospective https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 4/11 6/26/23, 5:39 PM SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… trials performed by the German Hodgkin Study Group (10-year PFS of 72.1%, Figure 2C).2 Stage III-IV As a minority of patients present with advanced stage NLPHL, there is a paucity of robust studies to guide management decisions, particularly for pediatric patients. Early reports of improved disease control using R-CHOP have since been validated by Fanale et al.34,35 with an encouraging 5-year PFS of 85.7% for 16 adult patients with stage III to IV NLPHL (Figure 2D). Thus, the increased alkylating chemotherapy dose may be beneficial for advanced stage NLPHL as compared to ABVD-based regimens.36 Finally, 84 patients enrolled on the German Hodgkin Study Group HD18 trial (which investigated PET-adaptation of therapy) had NLPHL, and those with a negative PET-CT after 2 cycles of escalated BEACOPP had improved 5-year PFS compared with those who had a positive scan, 90.2% vs. 70.1%, respectively.37 Less intensive options include rituximab alone for which nearly all patients obtain at least a partial response and may alleviate symptomatic disease despite not being a definitive option.30,38 Finally, active surveillance has been suggested as a viable option in the absence of high risk clinical features and may be employed for patients with good clinical follow up.8 Some examples of high-risk disease factors include variant pattern histology and splenic involvement which are both associated with transformation to aggressive large cell lymphomas and may warrant more immediate treatment.18,39 To date, the optimal approach to manage patients with stage III to IV NLPHL remains undefined. Relapsed NLPHL As relapses for NLPHL may occur even decades after initial diagnosis and treatment, long-term clinical follow up is important.5 At time of relapse, a repeat excisional biopsy and PET-CT should be obtained to confirm relapse, determine burden of disease, and evaluate for progression of variant subtype or transformation. Patients who relapse within 1-year after initial diagnosis have been reported to have a worse prognosis.40 Management of relapse depends on the relapse stage, prior therapies given, and whether the patient has bulky disease or is symptomatic. Reasonable approaches may include active surveillance, rituximab monotherapy, radiotherapy, combined modality therapy, and in cases of transformation or if progressing with aggressive disease even autologous bone marrow transplantation.3,40,41 Transformed Disease There is a small but persistent risk of developing transformation to aggressive large cell lymphomas for patients diagnosed with NLPHL.39 Transformation is associated with an increased risk of death.42 Treatment of transformed disease should include chemotherapy with or without autologous stem cell transplantation.39,43, 44, 45 Additionally, CD19 CART trials have included patients with transformation from NLPHL.46 Future Therapies Given the excellent outcomes observed for early stage NLPHL, introduction of alternative regimens, novel agents, and checkpoint inhibitors may be most appropriate for advanced stage and relapsed NLPHL. Nevertheless, alternative regimens have been reported for small cohorts. There was a 100% response rate for a cohort of 9 patients with stages I to IV NLPHL treated with bendamustine and rituximab.47 Despite the high PD-1 positive T-cell rosettes and PD-L1 positive LP cells,9,48 only scant clinical evidence suggests relapsed cases may respond to checkpoint inhibition.49 Finally, given the mature B-cell phenotype of NLPHL, patients with NLPHL are included in clinical trials for B-cell lymphomas including patients with multiply relapsed/refractory lymphoma targeting the NFKB pathway.50 Conclusion Although NLPHL is a rare type of Hodgkin lymphoma without many dedicated clinical trials or large studies to establish firm treatment standards, the majority of patients will enjoy high overall survival independent of treatment selection. Although late relapses do occur, patients tend to be diagnosed at young ages and should be considered for definitive treatment options as most will not have a relapse within 10 years of diagnosis. Large international collaboration is underway within the Global nLPHL One Working Group (GLOW) and will shed further light on appropriate risk stratification of patients based on pathologic factors and reveal age specific risks of progression to advanced stage and transformation.51,52 Disclosure There are no conflicts of interest to disclose. Acknowledgments The human body art used for Figure 1A was in part produced using Servier Medical Art (https://smart.servier.com ↗). Servier Medical Art by Servier is licensed under a Creative Commons Attribution 3.0 Unported License (https://creativecommons.org/licenses/by/3.0/ ↗). We also thank Dr. Yaso Natkunam for providing interpretation of the immunoarchitectural patterns displayed on Figure 1B. https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 5/11 6/26/23, 5:39 PM SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… Recommended articles References 1 SH Swerdlow, E Campo, NL Harris, et al. WHO classification of tumours of haematopoietic and lymphoid tissues, International Agency for Research on Cancer. WHO Press., Lyon, France (2008) Google Scholar ↗ 2 DA Eichenauer, A Plütschow, M Fuchs, et al. Long-term follow-up of patients with nodular lymphocyte-predominant Hodgkin lymphoma treated in the HD7 to HD15 trials: a report from the German Hodgkin Study Group J Clin Oncol, 38 (7) (2020), pp. 698-705 CrossRef ↗ 3 View in Scopus ↗ Google Scholar ↗ MS Binkley, MS Rauf, SA Milgrom, et al. Stage I-II nodular lymphocyte-predominant Hodgkin lymphoma: a multi-institutional study of adult patients by ILROG Blood, 135 (2020), pp. 2365-2374 View PDF 4 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ C Laurent, C Do, P-A Gourraud, et al. Prevalence of common non-Hodgkin lymphomas and subtypes of Hodgkin lymphoma by nodal site of involvement Med (Baltimore), 94 (2015), p. e987 View in Scopus ↗ 5 Google Scholar ↗ DP Regula, RT Hoppe, LM. Weiss Nodular and diffuse types of lymphocyte predominance Hodgkin's disease N Engl J Med, 318 (4) (1988), pp. 214-219 View in Scopus ↗ 6 Google Scholar ↗ DA Eichenauer, A Plutschow, M Fuchs, et al. Long-term course of patients with stage IA nodular lymphocyte-predominant Hodgkin lymphoma: a report from the German Hodgkin Study Group J Clin Oncol, 33 (2015), pp. 2857-2862 View in Scopus ↗ 7 Google Scholar ↗ BE Appel, L Chen, AB Buxton, et al. Minimal treatment of low-risk, pediatric lymphocyte-predominant Hodgkin lymphoma: a report from the children's oncology group J Clin Oncol, 34 (2016), pp. 2372-2379 View in Scopus ↗ 8 Google Scholar ↗ S Borchmann, E Joffe, CH Moskowitz, et al. Active surveillance for nodular lymphocyte-predominant Hodgkin lymphoma Blood, 133 (2019), pp. 2121-2129 View PDF 9 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ S Younes, RB Rojansky, JR Menke, D Gratzinger, Y. Natkunam Pitfalls in the diagnosis of nodular lymphocyte predominant Hodgkin lymphoma: variant patterns, borderlines and mimics Cancers (Basel), 13 (2021), p. 3021 CrossRef ↗ 10 View in Scopus ↗ Google Scholar ↗ RT Hoppe, RH Advani, WZ Ai, et al. NCCN Guidelines® Insights: Hodgkin lymphoma, version 2.2022 J Natl Compr Canc Netw, 20 (2022), pp. 322-334 CrossRef ↗ View in Scopus ↗ Google Scholar ↗ https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 6/11 6/26/23, 5:39 PM 11 SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… JF Grellier, L Vercellino, T Leblanc, et al. Performance of FDG PET/CT at initial diagnosis in a rare lymphoma: nodular lymphocyte-predominant Hodgkin lymphoma Eur J Nucl Med Mol Imaging, 41 (2014), pp. 2023-2030 CrossRef ↗ 12 View in Scopus ↗ Google Scholar ↗ JR Menke, MA Spinner, Y Natkunam, et al. CD20-negative nodular lymphocyte-predominant Hodgkin lymphoma: a 20-Year consecutive case series from a tertiary cancer center Arch Pathol Lab Med, 145 (2020), pp. 753-758 Google Scholar ↗ 13 Z Fan, Y Natkunam, E Bair, R Tibshirani, RA. Warnke Characterization of variant patterns of nodular lymphocyte predominant Hodgkin lymphoma with immunohistologic and clinical correlation Am J Surg Pathol, 27 (2003), pp. 1346-1356 View in Scopus ↗ 14 Google Scholar ↗ R Agbay, S Loghavi, Z Zuo, et al. Bone marrow involvement in patients with nodular lymphocyte predominant Hodgkin lymphoma Am J Surg Pathol, 42 (2018), pp. 492-499 CrossRef ↗ 15 View in Scopus ↗ Google Scholar ↗ S Hartmann, AS Soltani, K Bankov, et al. Tumour cell characteristics and microenvironment composition correspond to clinical presentation in newly diagnosed nodular lymphocyte-predominant Hodgkin lymphoma Br J Haematol, 199 (3) (2022), pp. 382-391 CrossRef ↗ 16 View in Scopus ↗ Google Scholar ↗ P Panjwani, S Epari, M Sengar, et al. Bone marrow involvement in nodular lymphocyte predominant Hodgkin lymphoma occurs in tumors with a variant pattern Leuk Lymphoma, 56 (2015), pp. 236-238 CrossRef ↗ 17 View in Scopus ↗ Google Scholar ↗ AG Shankar, AA Kirkwood, GW Hall, et al. Childhood and Adolescent nodular lymphocyte predominant Hodgkin lymphoma - a review of clinical outcome based on the histological variants Br J Haematol, 171 (2015), pp. 254-262 CrossRef ↗ 18 View in Scopus ↗ Google Scholar ↗ S Hartmann, DA Eichenauer, A Plutschow, et al. The prognostic impact of variant histology in nodular lymphocyte-predominant Hodgkin lymphoma: a report from the German Hodgkin Study Group (GHSG) Blood, 122 (2013), pp. 4246-4252 View PDF 19 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ Hartmann S, Soltani AS, Bankov K, et al. Tumor cell characteristics and microenvironment composition correspond to clinical presentation in newly diagnosed nodular lymphocyte predominant Hodgkin lymphoma. Google Scholar ↗ 20 RV Untanu, J Back, B Appel, et al. Variant histology, IgD and CD30 expression in low-risk pediatric nodular lymphocyte predominant Hodgkin lymphoma: a report from the Children's Oncology Group Pediatr Blood Cancer, 65 (2018) 10.1002/pbc.26753 Google Scholar ↗ https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 7/11 6/26/23, 5:39 PM 21 SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… B Schuhmacher, J Bein, T Rausch, et al. JUNB, DUSP2, SGK1, SOCS1 and CREBBP are frequently mutated in T-cell/histiocyte-rich large B-cell lymphoma Haematologica, 104 (2019), pp. 330-337 CrossRef ↗ 22 View in Scopus ↗ Google Scholar ↗ V Spina, A Bruscaggin, A Cuccaro, et al. Circulating tumor DNA reveals genetics, clonal evolution, and residual disease in classical Hodgkin lymphoma Blood, 131 (2018), pp. 2413-2425 View PDF 23 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ L Raman, M Van der Linden, C De Vriendt, et al. Shallow-depth sequencing of cell-free DNA for Hodgkin and diffuse large B-cell lymphoma (differential) diagnosis: a standardized approach with underappreciated potential Haematologica, 107 (2022), pp. 211-220 View in Scopus ↗ 24 Google Scholar ↗ V Brune, E Tiacci, I Pfeil, et al. Origin and pathogenesis of nodular lymphocyte-predominant Hodgkin lymphoma as revealed by global gene expression analysis J Exp Med, 205 (2008), pp. 2251-2268 CrossRef ↗ 25 View in Scopus ↗ Google Scholar ↗ E Campo, ES Jaffe, JR Cook, et al. The international consensus classification of mature lymphoid neoplasms: a report from the clinical advisory committee Blood, 140 (2022), pp. 1229-1253 View PDF 26 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ R Alaggio, C Amador, I Anagnostopoulos, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms Leukemia, 36 (2022), pp. 1720-1748 CrossRef ↗ 27 View in Scopus ↗ Google Scholar ↗ B Pellegrino, MJ Terrier-Lacombe, O Oberlin, et al. Lymphocyte-predominant Hodgkin's lymphoma in children: therapeutic abstention after initial lymph node resection–a study of the French Society of Pediatric Oncology J Clin Oncol, 21 (2003), pp. 2948-2952 View in Scopus ↗ 28 Google Scholar ↗ C Mauz-Körholz, T Lange, D Hasenclever, et al. Pediatric nodular lymphocyte-predominant Hodgkin lymphoma: treatment recommendations of the GPOH-HD study group Klin Padiatr, 227 (2015), pp. 314-321 View in Scopus ↗ 29 Google Scholar ↗ CC Pinnix, SA Milgrom, CY Cheah, et al. Favorable outcomes with de-escalated radiation therapy for limited-stage nodular lymphocyte-predominant Hodgkin lymphoma Blood Adv, 3 (2019), pp. 1356-1367 View PDF 30 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ RH Advani, SJ Horning, RT Hoppe, et al. Mature results of a phase II study of rituximab therapy for nodular lymphocyte-predominant Hodgkin lymphoma J Clin Oncol, 32 (2014), pp. 912-918 View in Scopus ↗ 31 Google Scholar ↗ PTM Cheng, D Villa, RP Tonseth, et al. https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 8/11 6/26/23, 5:39 PM SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… Outcome of limited-stage nodular lymphocyte-predominant Hodgkin lymphoma and the impact of a PET-adapted approach Blood Adv, 5 (2021), pp. 3647-3655 View PDF 32 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ M Fuchs, H Goergen, C Kobe, et al. Positron emission tomography–guided treatment in early-stage favorable Hodgkin lymphoma: final results of the international, randomized phase III HD16 trial by the German Hodgkin Study Group JCO, 37 (2019), pp. 2835-2845 CrossRef ↗ 33 View in Scopus ↗ Google Scholar ↗ P Borchmann, A Plütschow, C Kobe, et al. PET-guided omission of radiotherapy in early-stage unfavourable Hodgkin lymphoma (GHSG HD17): a multicentre, open-label, randomised, phase 3 trial Lancet Oncol, 22 (2021), pp. 223-234 View PDF 34 View article View in Scopus ↗ Google Scholar ↗ MA Fanale, CY Cheah, A Rich, et al. Encouraging activity for R-CHOP in advanced stage nodular lymphocyte–predominant Hodgkin lymphoma Blood, 130 (2017), pp. 472-477 View PDF 35 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ GP Canellos, P. Mauch What is the appropriate systemic chemotherapy for lymphocyte-predominant Hodgkin's lymphoma? J Clin Oncol, 28 (2010), p. e8 View in Scopus ↗ 36 Google Scholar ↗ KH Xing, JM Connors, A Lai, et al. Advanced-stage nodular lymphocyte predominant Hodgkin lymphoma compared with classical Hodgkin lymphoma: a matched pair outcome analysis Blood, 123 (2014), pp. 3567-3573 View PDF 37 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ DA Eichenauer, S Kreissl, I Bühnen, et al. PET-2-guided escalated BEACOPP for advanced nodular lymphocyte-predominant Hodgkin lymphoma: a subgroup analysis of the randomized German Hodgkin Study Group HD18 study Ann Oncol, 32 (2021), pp. 807-810 View PDF 38 View article View in Scopus ↗ Google Scholar ↗ DA Eichenauer, A Plütschow, M Fuchs, et al. Rituximab in newly diagnosed stage IA nodular lymphocyte-predominant Hodgkin lymphoma: long-term follow-up of a phase 2 study from the German Hodgkin Study Group. Leukemia, 34 (3) (2020 Mar), pp. 953-956 CrossRef ↗ 39 View in Scopus ↗ M Al-Mansour, JM Connors, RD Gascoyne, B Skinnider, KJ. Savage Transformation to aggressive lymphoma in nodular lymphocyte-predominant Hodgkin's lymphoma J Clin Oncol, 28 (2010), pp. 793-799 View in Scopus ↗ 40 Google Scholar ↗ DA Eichenauer, A Plutschow, L Schroder, et al. Relapsed and refractory nodular lymphocyte-predominant Hodgkin lymphoma: an analysis from the German Hodgkin Study Group Blood, 132 (14) (2018), pp. 1519-1525 View PDF 41 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ S Akhtar, S Montoto, A Boumendil, et al. High dose chemotherapy and autologous stem cell transplantation in nodular lymphocyte-predominant Hodgkin lymphoma: a retrospective study by the European society for blood and marrow transplantation-lymphoma working https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 9/11 6/26/23, 5:39 PM SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… party Am J Hematol, 93 (2018), pp. 40-46 CrossRef ↗ 42 View in Scopus ↗ Google Scholar ↗ I Kalashnikov, T Tanskanen, J Pitkäniemi, et al. Transformation and outcome of nodular lymphocyte predominant Hodgkin lymphoma: a finnish nationwide populationbased study Blood Cancer J, 11 (2021), pp. 1-6 Google Scholar ↗ 43 I Biasoli, A Stamatoullas, V Meignin, et al. Nodular, lymphocyte-predominant Hodgkin lymphoma: a long-term study and analysis of transformation to diffuse large B-cell lymphoma in a cohort of 164 patients from the adult lymphoma study group Cancer, 116 (2010), pp. 631-639 CrossRef ↗ 44 View in Scopus ↗ Google Scholar ↗ TA Eyre, K Gatter, GP Collins, et al. Incidence, management, and outcome of high-grade transformation of nodular lymphocyte predominant Hodgkin lymphoma: long-term outcomes from a 30-year experience Am J Hematol, 90 (2015), pp. E103-E110 CrossRef ↗ 45 View in Scopus ↗ Google Scholar ↗ SS Kenderian, TM Habermann, WR Macon, et al. Large B-cell transformation in nodular lymphocyte-predominant Hodgkin lymphoma: 40-year experience from a single institution Blood, 127 (2016), pp. 1960-1966 View PDF 46 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ B Thapa, PF Caimi, KM Ardeshna, et al. CD19 antibody-drug conjugate therapy in DLBCL does not preclude subsequent responses to CD19-directed CAR T-cell therapy Blood Adv, 4 (2020), pp. 3850-3852 View PDF 47 View article CrossRef ↗ View in Scopus ↗ Google Scholar ↗ REI Prusila, K-M Haapasaari, K Marin, et al. R-Bendamustine in the treatment of nodular lymphocyte-predominant Hodgkin lymphoma Acta Oncologica, 57 (2018), pp. 1265-1267 CrossRef ↗ 48 View in Scopus ↗ Google Scholar ↗ J Gunawardana, K Bednarska, SC Law, et al. The tumor microenvironment of nodular lymphocyte predominant Hodgkin lymphoma is a unique immunobiological entity distinct from classical Hodgkin lymphoma Blood, 132 (2018), p. 4123 View PDF 49 View article CrossRef ↗ Google Scholar ↗ Raisa Gorbacheva Memorial Research Institute of Pediatric Oncology, Hematology and Transplantation, Pavlov University, St. Petersburg, Russia, AV Kozlov, IV Kazantzev, et al. Nivolumab in pediatric Hodgkin's lymphoma CTT, 8 (2019), pp. 41-48 CrossRef ↗ 50 View in Scopus ↗ Google Scholar ↗ DA Stevens, R Ewesuedo, A McDonald, et al. Phase 1 study of KT-413, a targeted protein degrader, in adult patients with relapsed or refractory B-cell non-Hodgkin lymphoma JCO, 40 (16_suppl) (2022) TPS3170–TPS3170 Google Scholar ↗ https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 10/11 6/26/23, 5:39 PM 51 SOHO State of the Art Updates and Next Questions |Treatment Approaches for Nodular Lymphocyte-Predominant Hodgkin Lymp… AC Lo, A Major, L Super, et al. Practice patterns for the management of nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL): an international survey by the Global NLPHL One Working Group (GLOW) Leuk Lymphoma, 63 (8) (2022), pp. 1997-2000 CrossRef ↗ 52 View in Scopus ↗ Google Scholar ↗ MS. Binkley Characterizing the immune microenvironment for nodular lymphocyte-predominant Hodgkin lymphoma Br J Haematol, 199 (2022), pp. 310-312 CrossRef ↗ 53 View in Scopus ↗ Google Scholar ↗ DL Friedman, L Chen, S Wolden, et al. Dose-intensive response-based chemotherapy and radiation therapy for children and adolescents with newly diagnosed intermediate-risk hodgkin lymphoma: a report from the children's oncology group study AHOD0031 J Clin Oncol, 32 (2014), pp. 3651-3658 View in Scopus ↗ 54 Google Scholar ↗ HT Eich, V Diehl, H Görgen, et al. Intensified chemotherapy and dose-reduced involved-field radiotherapy in patients with early unfavorable Hodgkin's lymphoma: final analysis of the German Hodgkin Study Group HD11 trial J Clin Oncol, 28 (2010), pp. 4199-4206 View in Scopus ↗ Google Scholar ↗ Cited by (0) View Abstract © 2023 Elsevier Inc. All rights reserved. Copyright © 2023 Elsevier B.V. or its licensors or contributors. ScienceDirect® is a registered trademark of Elsevier B.V. https://www.sciencedirect.com/science/article/pii/S2152265023001118?via%3Dihub 11/11