An Official Publication of the
Philippine Pediatric Society, Inc.
Clinical Practice Guideline
·. ,·
,•.·
In The Approach And
Treatment Of Urinary Tract
Infection In Children
In The Philippine Setting
Categories reflectin.s_the~ality of evidence on which- ,ecommendations
are based
- -~·
~
- - E vid;ncc- fr°Z>m at IC<t-\1 DEflNlTION
one pr~periy randomized, contrr,J!ed
GRADE
I
II
Ill
-
-
trial
Evidence from at least one well desihrned in trial without
randomization from cohort or case-controlled analytical
'
studies _uncontrolled experiments
Evidence from opinion of respected authorities, based on
dinical experience, descriptive studies, or reports of expert
committees
THE CHILD WITH PROBABL~: URINARY TRi\CT INFECTION
I. The SUSPElT:
I. The n
t presenting with the · ·
as presented
in table I.
2. Febnle infants (>38 C) below 2 ·cars of a (Table l Downs)
3. Older children manifesting symptoms referable to urinary tract (Table I)
The evidence for trus recomm~odation Alli. Hoberman A (6,7,8)~ Shaw (9).
Downs()}
Table I
•
Jn generaJ manifestations of urinary tract infections are non-scientific.
However. there are some signs and symptoms that are associated with UTI.
CLINICAL
SIGN/S
Neonates
SYMPTOM
• Septic
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Temperature instability
Poor feeding
Vomiting
Lethargy or irritability
Jaundice
Fever
Poor weight
gain/failure to thrive
Diarrhea
Abdominal pain
Frequency, dribbling,
urgency dysuria
Weak urinary stream
Malodorous urine
Enuresis
Flank_.eains
Older Infant,
School Ag
Adokscr-nts
[+]
f+J
[+]
[f-J
[+]
[·ij
[+]
[+]
[+]
[+
[+]
[+]
f+J
I+J
(+}1
[+j
[+)
[+J
[+]
f+l
(+]
[+
I
r-
I- --4
(+]
{ii
(+]
1-
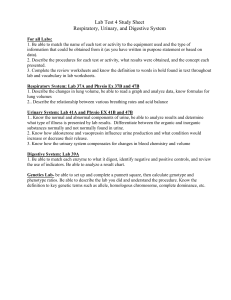
II. THE FOLLOWING L~ AN ALGORITHM ON THE DIAGNOSL~, WORK-UP,
TREATMENT AND FOUOW-UP OF CHILDREN WITH URINARY TRACT
INFECTION.
SUSPECTED URINARY TRACT INFECTION
UJNly-.. { ~ afUTI)
(+) ~ ~ o r N " I M O'T:mll
Bae1milri,pR9Clll m..,..
Oraa•aiwt~
...~r-----
Pll\'lli.:.u - - - - ~ •
E.~ a,;
1')111111 ~ WBClbpC« J ~
(+) u..e
ul ;a p-,..ty
caBc,c.,cdw.tpedlMD.
ABSENT
CBC ( C ~ prolcin, ESR)
BUN. Clalia.iac
Oplimal C-IU', ESll, Bblclad
AdllillO lbpil.:.
__ Psaltaal ~
(JV,l M) ___
KUB UTZ. pn: -t pool '\IOid
~~
a..,p.,. um< Culll&'\:
M,y a ! tooal ~
C...-7-14~,
Ua: ~ ari,iori,:,a
hac.d on initial 'Urine cas
(lf .wailabk)
Coq,lc:te 7-14 days Ct(
O{lrQlmc:rtl
-~
Pmp,yb.-ria
··-iiw1won~-----·"i:v;;:;:
ciclili;·;;;;
;;;ic-:c:o;;;
,.,...;;;;;edi;;•US1Dii iaaiil'• ----·--·-·--------· ..
Or nudca-<.~
Wbm .-dcd: ~ l i d c rmal IUD •"WM,' >.~A)
l a i r - pyclOIJllJlby ••
Olbr.r
..----···-·-·---··-----
~ I r ; < ~ ~ .. -
Urolol)' follow--wp • ,iccdcd
-----------Nephrology roDow-ap
Monilor 81ood ~
~ t;VCty
u
UmeCllllur'c
vflt (CIClllliniat)
5
W<:Q.S
-·····- - - ···- - · · - - -
Ill.
Ill.«<,·
OSIS
·L. h. . t ref ·1 to table t
1h l\lfY nf
m,·( ntincnc~. ................ ,
<. 'h
- -""'- '-on. unH",rna ,,.,..e.~-1 such as
· 's cspccu1lly pelvic surseries, ambulatory problem etc
1
l
l
'
rn, SICAL
'XAMINATION:
th,lt\.\U~h ph sical enminntion i a ml»t. The examinet should look for ,__...,...,.....
th t C\x-xist,
mil i n such a p
f · I , r tu
l c indic.atin probable ncurogcnic Madders Lower extremities must
al he c ·nmined. Thorough
...,_...__
10n must be included Rectal
c, · min:itton 1s part of the c.uminntion
11\t \IIUI ly is
inf tJoo would
ha
CAVEAT:
Parallel combinations of test results maximize sensitivity. A study within one hour of
uri
Uecrion using careful on-site microscopy with a positive comb,nation for
leukocytes and bacteria has a sensitivity of 99% or greater. When any mponent of
uriMlyus II politi - such as LE. nitrite, blood, protans, microscopy for
leukocytes, microscopy of bacteria·, and the urinal · · considered po 'ti~. the
sensitivity is 100% but the pecificity is only 600/o-Hoberman (7), Lohr (ll),
HouSlon (I 2), Hoberman (13). Evidtnce is B/11
;~
f'
,-r,
1
,..I (
,.,,,r,.ie
·,,., ..
L' e )l n tt 1 <"('ff,,. ({(A i· i-r+
1~- ' 1'1 2 11,/'f
THE GOLD STANDARD rs ANY BACTERIAL GROwrH AFTER A
S~PRA~UBJC TAP. This is done in inf:
w ooe year of age. The bladder at
th1 s age is intraabdominal. A diaper that has been dry for thirty minutes. will indicate
~ bladder containinp. enough urine to avoid an empty tap. With a 3-c.c ~• e and an
m~h _Ion gau e 25 needle, punctw-c one centimeter above the symphysis pubis in the
Trine Culturt:
midline. For care givers that shun away from suprapubic taps. catheterization would
he the next best choice. Refer to table 2
Midstream catch in a cooperative and properly prepared patient wiJI give a high
sensitivity and specificity.
Table 2
•
Urine Culture: lottrprctttion ofUTI
Method of Collection
QuantitBtive Culture: lITI present
•
S~bic aspiration
Growth o urinary pathogen in
""'lemabd(cxcq,tioo is up to
2-3 X 10\ CRJhnl of coagu.lasoncgalJ\·c staphylococci)
•
CadldcrizatioD
Febrile infants QI' chiljhen usunlly
have 56,000 FUhnl evidence of
a single urinary pathogen, but
infeclion ma)' be present wilh counts
from >. OOOCF'Uhnl (Hobcnnan A
(7), Down (7), +
•
cl~void
lt-luia-.1111u·c patients at least
IYMIIIGCBtDSI on diffamt
Days with
pathogen..
to' CRU of the same
+ Culture of urine specimens obtained by catheteriz.ation has a specificity of 83% to
89°/ o compared with cultures of urine ~pecimens obt~ned by !,31>· If <:'~~ cultures of
> I OOOCFU/ml are considered, catheterized cultures have a 951/o sens1t1v1ty and 99G/o
specificity.
•
Routine ~ - of the urine after 2 days of antimicrobial therapy is
generally all& _ _.'tlf'/ if the infant or young child has had expected
clinical raponse and the uropathogen is determined to be sensitive tl) the
alltimicrobiaJ being_administered.
7
WARNING ON THE USE OF BAG SPECIMEN FOR CULTORE:
Culture of bag specimen is 100°/4 sensitive but have a pecificity of only 14-841/oTaylor (14), Puerto M (15). With prevalence rate of only 5%, the use of culture from
the urine specimens from a bag to rule in UTl is likely to r ~ h in a large number of
false positive results. Specifically, with prevalence of 5%. That is, 8So/. of positive
cultures of bag specimen would be f.alse - Dovm(5}. Evidence is Dill
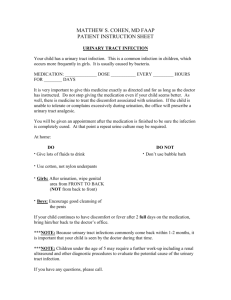
W. WORK-UP
Table 3
Reference
Do~n(5)
Less 3 yrs old
Pre\'alence
of
abnormalitv
51%
Down (5)
Any age group
38%
Age group
Detectable
by
ultrasowid
,;
42%
Detectable
Comment
byutzand
VCUG
100%
Emphasis on
VUR
100%
All
abnonnalitics
Burbigc KA
(16)
Children
Elzouki AY
Children
26%
Undec 14
79%
25-50%
75%
1001/4,
Boys
(including
lVP)
J00°/4
(17)
,<.>meUie JM
29°/.
100°/4
Dl\.-f.SA
scan and IVP
(18)
Hobcrman
(19)
Hiraoka
Includes
M
Infants and
young children
-
Notw;cful
100%
Less & months
Jr;.
Good
screemng
100-/4
(20)
Follow up UTJ
if normal
ultrasound,
work up if
with
MucciB
(21)
Strife (22)
.
14%
3%
--
DMSAasa
screening
Children (girls)
38%
l3%
100%
Uses nuclear
. .
Riclwood
UTJ
Children
99°/4
sensitive,
43%
Children
(23)
-
cystograrn
specific
Honkincn
Children
(inadequate
as a slndv)
1&9/4
52o/.
(24)
Complete
wale
up will need
VCUG/noclear
- ---~AUi
·-
-
0
~ ltrasonography alone as a work up for patients with proven urinary tract infection is
madequate. lt is sensitive(99-95% Cl 96¾-100%) but it its' !>-pecificity modest (430'o32%-55~1o)- Rickwood (23) Evidt!?~~ is A/IL
The use of voiding cystourclhrogr~phy (or nuclear cystogram) evaluates the presence
or absence of vesicourctcral reflu .
Vesicouretera) reflux is the most common abnonnality found in-patients with urinary
tract infection. The prevalence is 30'% to 400/4 - Down ( 5-table 6 and table 7 review
of literatw·e): Evidence is A/ll
i:
TREATt,,JENT:
.
•
•
Somt- antimicrobials for oral treatment of UTI
Amoxicillin
20-40 mg/kg/day in 3 doses
TMP in combination with SM.X
kg per day in 2 doses
6-12 mg TMP. 30-60 SMX per
Sulfisoxazole
l20-l50 mg/kg/day in 4 doses
Cefixime
8 mg/kg/day in 2 doses
Cephalexin
50-100 mg/kg/day in 4 doses
Cefpdoxime
10 mg/kg/day in 2 doses
Cefprozil
30 mg/kg/day in 2 doses
Loracarbef
f 50-30 mg/kg/day in 2 doses
Some antibiotics for p reoul treatment of UTl
Ceftriaxone
75 mglkg every 24 hours
C efota."Xime
hour ·
150 mg/kg/day divided every 6
Ceftazidime
150 g/kg/day divjded every 6
hours
Cefazo1in
SO m~g/day divided every 8
hou rs
Gentamicil}
7.5 mg/kg/day divjded
hours
9
CV~
8
every 8
Tobramycin
hours
100 mgl!.wday divided every 6
Ticarcillin
houB
100 mg/kg/day divided every 6
Ampicil1in
hours
•
Prophylactic antibiotics - low serum levels but with high urinary ]eve)
-1--las minimal effects on fecal flora
- Low cost and well tolerated
½ of the regular dose given at bedtime
•
Some antimi~robial for prohylaxis of UTI
TMP in combination with SMX
kg as single bedtime dose
2 mg TMP~IO mg of SMX per
Or 5 mg of TMP, 25 mg of
SMX per kg twice per week
:Nitrofuraotoin
l-2 mg/kg as single daily dose
SuJfisoxaz.ole
10-20 mg/kg divided every 12
hours
Nalidi.'ric Acid
hours
30 mg/kg divided every I 2
Methe-namine mandelate
75 mg/kg di"ided every I 2 hour
Bibliography:
1. Siegle SR, Sokoloff B. Asymptomatic and symptomatic urinarv tract
infoction in infancy.
·
·
Am J Dis Child 1973; 125:45-47
2. Mc lntyre PB, Gray SV, Vance JC. Unsuspected infections in febrile
convulsions Med J Aust 1990; 152, I 83
3. Pryles CV. luders D. The bacteriology of the urine in infants and
children with gastroenteritis. Pediatrics 1961 : 877-885
4. Shortlife. Ch 57. Urinary tract inftX--tion in infants and children.
th
Campbellls 7 edition: Walsh, Retick, Vaughn, Wein
5. Downs SM. Technical Report: Urinary Tract infections in febrile
~fants and Young Children: ·Pediatrics Vol I 03 No4 April
10