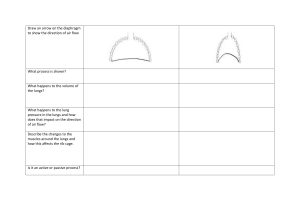
Oxygenation The basic human needs Nurses are responsible for promoting normal respiratory function regardless practice area. Nurses also help to improve breathings in clients with altered respiratory function. Respiration = the process of gaseous exchange between the individual and the environment Ana Physio of Respiratory System 1. The Airways A. Upper Airways Nasal Cavity Pharynx Larynx B. Lower Airways Trachea R. and L. main stem bronchi Segmental bronchi Terminal bronchi C. Functions of the Upper Airway Transport of gases to the lower airways Protection of the lower airway Warming, filtration and humidification of air D. Functions of the lower airway Clearance mechanism - cough - mucociliary system - macrophages -lympatics Absorb oxygen from the air taken in by the upper respiratory tract and release carbon dioxide Nares= the openings of the nose Vestibule= cavity inside the nostril Vibrissae= hairs that line the vestibule Carina= the bifurcation of trachea 2. The Pleura Serous membranes that enclose the lungs. The pleural space is a potential space between the 2 pleurae. Only few ml of fluid is found in the pleural space. 3. The lungs R. lung= 3 lobes, L. lung=2 lobes Lung volumes and Capacities… 4. Thorax and Diaphragm Protects the heart and lungs. Has 12 pairs of ribs Diaphragm is the main respiratory muscle Accessory Muscles=scalene, sternocleidomastoid, parasternal, trapezius and pectoralis muscle Planning 1. Adequate supply of O2 from the environment. ↑ altitude=↓O2 concentration 2. Deep breathing and coughing exercises 3. Positioning. Semi-fowler’s and high fowler’s promotes maximum lung expansion 4. Maintain patent airway. Causes of Airway Obstruction - tongue - mucous secretions - edema of airways - spasm of airways - foreign bodies 5. Adequate hydration. 6. Avoid environmental pollutants 7. Chest Physiotherapy Percussion= forceful striking of the skin with cupped hands Postural drainage= expulsion of lung secretions from various lung segments through gravity. Done before meals Provide good oral hygiene after each procedure 8. Bronchial Hygiene Measures A. Steam Inhalation Purpose: - to liquify mucous secretions - to warm and humidify inspired air - to relieve edema of airways - to soothe irritated airways - to administer medications Dependent nursing action Inform the client and explain the procedure Place the client semi-fowler Done 15-20 minutes Provide good oral hygiene every after procedure B. Aerosol Inhalation Done among pediatric clients to administer medications 9. Suctioning: to clear airways from mucous secretions Oropharyngeal and Nasopharyngeal Suctioning 1. Assess indication for suctioning Audible secretions during respirations Adventitious breath sounds 2. Position: Conscious: Semi-Fowler’s Position Unconscious: Lateral Position 3. Suction catheter sizes (Fr.) A=12-18 I= 5-8 C= 8-10 4. Suction Pressure (mmHg) A= 10-15 C=5-10 I= 3-5 ( portable ) A= 100-120 C= 95- 100 I= 50-95 (wall outlet) 5. Techniques: Sterile- lower airway Clean – upper airway 6. Lubricate catheter: Nasopharyngeal= water soluble lubricant Oropharyngeal = sterile H2O or PNSS 7. Oral Tracheal Length-3-5” 2-3” Duration-10-15 sec 5-10 sec Rest period-20-30 sec 2-3 min. Lubricant- c. H2O/ KYJ NSS/Sterile H2O 10. Incentive Spirometry = done to enhance deep inspiration 11. Administration of Supplemental Oxygen Indication= Hypoxemia Signs of Hypoxia - Restlessness - increased PR - Rapid, Shallow respiration and dyspnea - light headedness - flaring of nares - cyanosis 11. Oxygen Systems - nasal cannula = 2-6 lpm - simple face mask= 5-8 lpm - non-rebreathing mask= 6-15 lpm - O2 tent - venturi mask - face mask Oxygen- color/odorless, tasteless and dry gas that supports combustion Alterations in Respiratory Functions Hypoxia= insufficient oxygenation of tissues Clinical signs of Acute Hypoxia 1. Nausea and vomiting 2. Oliguria, anuria 3. Headache 4. Apathy 5. Dizziness 6. Irritability 7. Memory loss Clinical Signs of Chronic Hypoxia 1. 2. 3. 4. 5. fatigue, lethargy Pulmonary ventilation increases RBC count increases Hgb concentration increases Clubbing of fingers Altered Breathing Patterns A. RATE - Tachypnea= rapid respiratory rate - Bradypnea= Slow respiration rate - Apnea= cessation of breathing B. VOLUME - Hyperventilation= excessive amt. of air in the lungs deep rapid ventilations. - Hypoventilation=decreased rate and depth of respiration causes retention of CO2. C. RHYTM - Cheyne-stokes= from deep-shallow then apnea. - Kussmaul’s = HYPERVENTILATION - Apneustic= prolonged gasping, then inefficient expiration - Biot’s= shallow breaths interrupted by apnea. D. EASE OF EFFORT - dyspnea= difficulty in breathing - orthopnea= DOB except in sitting or upright position Lung Volumes and Lung Capacities Tidal Volume The tidal volume is the total amount of air inhaled or exhaled during normal breathing. On an average 500 ml of air is utilised during normal respiration in a healthy man. Inspiratory Reserve Volume An inspiratory reserve volume is a supplementary volume, ranging between 2500 to 3100 ml of air which could be inhaled effectively after the inspiration of a standard Tidal Volume. Expiratory Reserve Volume The extra volume of air that can be exhaled from the lungs with effort following a normal tidal volume expiration. An expiratory reserve volume is about 1200 ml that could be forcibly exhaled out after the expiration of a standard tidal volume. Residual Volume/Reserve Volume The residual volume is the total volume of air that is around 1100 ml to 1200 ml, residing in the lungs after the reserve volume is exhaled or breathed out. Lung Capacity Total Lung Capacity The total lung capacity is the total volume of air in the lungs after a forced inspiration. The lung capacity of a healthy man is around 6000 ml. TLC = TV + ERV + IRV + RV Vital Capacity The vital capacity is the total volume of air that can be breathed out after inhalation limit or maximum air that a person can breathe in after forced expiration. It is an essential measure of a person’s respiratory health. A decreased vital capacity indicates restrictive lung disease where the lungs cannot expand completely. The improper functioning of lungs indicates obstructive lung disease, where the lungs are blocked in the airways. VC = TV + ERV + IRV Inspiratory Capacity The amount of extra air inhaled above tidal volume during a forceful inspiration. The average inspiratory reserve volume is about 3000 mL in males and 2100 mL in females. IC = TV + IRV Functional Residual Capacity Functional Residual Capacity is the volume remaining in the lungs after a normal exhalation. In a healthy individual, this is about 3L. FRC = ERV + RV