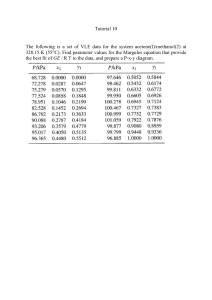
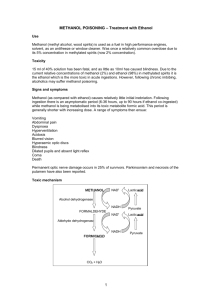
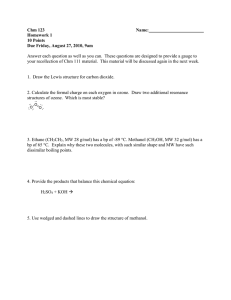
By Khadiga Mohammed Abdelrahman Assistant Lecturer of Forensic Medicine & Toxicology Agenda • Sources and Uses • Mode of poisoning • Fetal dose • Toxicokinetic • Pathophysiology • Clinical picture • Cause of death • Investigation • Treatment Methanol /Methyl alchol/ Wood alchol الكحول االحمر • Volatile, colorless ,odor similar to ethanol • methanol not fit for human use Sources and uses • Source: Wood distillation(wood alchol) • Uses: 1. Adulteration of ethanol 2. Factory : ❑Photocopying fluid ❑Windshield washer fluid ❑Perfume ❑Gasoline antifreeze ❑Paint solvents ❑Household cleaners ❑Airplane fuel Mode of poisoning • Accidental: (children-addict-adulteration-workers) • Epidemic poisoning • Intentional • Suicidal(worker,windshield washer) Fatal dose • 15 ml…blindness • 60-80 ml fatal dose Toxicokinetic • Absorption (rapidly absorbed by GIT-lung-skin) • Distribution (rapidly distributed to total organs with water content) • Metabolism and Excretion: 90% slowly metabolized (zero order elimination) by liver, cumulative drug So Elimination half life of 14 -18 hrs 10% excreted unchanged by lung and kidney Metabolism Anerobic respiration N.B • NAD dependent glycolysis…….will be inhibited • No glycolysis >>>hypoglycemia • NADH dependent mechanism increase ….increase conversion of pyruvate to lactate …lactic acid…acidosis Pathophysiology Pathophysiology Pathophysiology Pathophysiology 1. Methanol itself is harmless in small amounts and a CNS depressant(but in large amounts) 2. Osmolar gab due to methanol itself 3. Poisoning is mainly from methanol toxic metabolites 4. Formaldehyde is 33 times more toxic than methanol 5. Formic acid is 6 times more toxic than methanol 6.Metabolic acidosis (due to methanol products)is a consequence of the metabolism of methanol to toxic organic acids, Formic acid & Lactic acid in the most seriously ill are responsible for the acidosis & decrease in plasma bicarbonate. 7.The formate metabolite of methanol is : A mitochondrial toxin Inhibiting cytochrome oxidase lead to anerobic respiration…tissue hypoxia and more acidosis • Optic nerve injury and blindness 8. End organ damage &basal ganglia affection Clinical picture • Early : 1. GIT manifestation,colic,nausea,vomiting 2. CNS depression symptoms,euphoria,dizziness,lack of coordination,confusion…etc 3. no acidosis Clinical picture • Late:after a latent period(12-24 h), This latent period is longer with ethanol co-ingestion ✓Metabolic acidosis with elevated anion gap…..air hunger(Kussmaul breathing) ✓Ocular toxicity(Blurry or hazy vision or defects in color vision Photophobia, snowfield vision, Central scotoma, total blindness) ✓Coma,features of heart failure and cardiac arrhythmias may be seen in individuals who have ingested large amounts of methanol Cause of death • Sever metabolic acidosis • CNS depression,respiratory depression and circulatory failure(circulus hypoxicus) Differential diagnosis • Other causes of metabolic acidosis: ➢toxicological considerations for metabolic acidosis : salicylates, acetaminophen, iron, carbon monoxide, cyanide, alcoholic ketoacidosis, and ingestion of other alcohols, such as ethylene glycol. ➢ Nanotoxicological considerations :diabetic ketoacidosis, sepsis, and uremia. ➢Other toxic alcohols with elevation of osmolar gab: Ethanol, ethylene glycol Investigation a.For Detection of Methanol and its Products • Serum methanol level(after latent period it will be non significant) • Serum formaldehyde or formic acid level b.For detection of complications due to methanol products: • Fundoscopy: hyperemic red optic disc • Arterial blood gases: Blood gas analysis in severe toxicity reveals severe metabolic acidosis with pH < 7.3 and HCO3 < 20 mEq/L. • Serum lactic acid is raised Investigation • Electrolytes should be done in all cases to calculate : • the anion gap(high anion gab metabolic acidosis). • and Serum osmolality • Osmolar gap of more than 25 between calculated and measured one indicates presence of abnormal alcohol. • serum amylase or lipase( for pancreatitis complication) Investigation N.B • Therefore, as methanol is metabolized, the osmolar gap decreases and the anion gap increases Investigation c.For differential diagnosis: • Blood ethanol level Urine analysis • (calcium oxalate crystals) for D.D ethylene glycol • Serum &Urine ketones ( for D.D. with diabetic ketoacidosis, alcohalic ketoacidosis in ethanol toxixity) d.For management: • Kidney function test, Liver function test (for assessment of elimination systems) Management • History and clinical picture • Investigation • Treatment: Treatment options for methanol toxicity include supportive care, fomepizole (Antizole, 4-Methylpyrazole or 4MP), ethanol,NaHCoo3, dialysis and theoretically, folate) 1. ABC: A:maintain airway B:assisted ventilation if needed C:mangment of coma if occurred 2. Decontamination :IF early, gastric lavage may be used ,no role of activated charcoal. Why? 2. Sodium Bicarbonate: Life threatening complication of methanol intoxication is severe metabolic acidosis. Hence correction of acidosis is of prime importance With Repeat arterial blood gas analysis • 3.Antidotes: A. Ethanol : competitive antagonist ,ADH enzyme has a higher affinity for ethanol than for other alcohols. Close watch should be kept on hypoglycemia and electrolyte imbalance, especially hypokalemia A. Fomepizole :inhibit alcohol dehydrogenase enzyme to prevent metabolism of methanol B. Folate/folic acid: this degrades formic acid into carbon dioxide and (CO2 + H2O) 4.Enhanced elimination: Hemodialysis: • Clears both methanol and formate • Corrects the acid-base disorder • Indication: o Severe acidosis (pH < 7.1 and HCO3 < 10). o Fluid or electrolyte disturbance o End-organ toxicity o Significant amounts of toxic metabolites o Methonal level>50 mg/dl Remember • • • • • Methanol is metabolized to its toxic metabolite, formic acid/formate. Formic acid is responsible for the metabolic acidosis and end-organ toxicity. End-organ toxicity includes primarily retinal damage. Methanol is osmotically active. A normal osmolar gap is not reassuring and should be expected in the presence of an anion gap acidosis believed to be related to toxic alcohol poisoning. • The mainstay of treatment is fomepizole, supportive care and resuscitation, and dialysis.