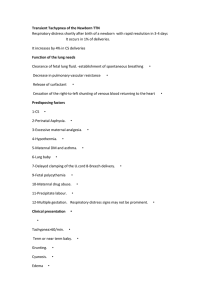
Respiratory Distress in Neonates Dr Ghamdi, Mohammad Assistant Professor Consultant Pediatrician & Neonatologist NRP instructor • Objectives After completing this lecture, audiences should be able to: 1. Evaluate and diagnose the most common causes of respiratory distress in the newborn 2. Differentiate between cardiac and respiratory causes of respiratory distress in the neonate. • 3. Differentiate between the normal chest radiograph and the radiographic patterns of various respiratory disorders 4. QUIZ Pulmonary Causes for Respiratory Distress in Neonates • Parenchymal conditions • Developmental abnormalities • Mechanical abnormalities Pulmonary Causes for Respiratory Distress in Neonates • • • • • Parenchymal conditions Transient tachypnea of the newborn Respiratory distress syndrome Pneumonia Meconium aspiration syndrome Pulmonary Causes for Respiratory Distress in Neonates • • • • • Developmental abnormalities Congenital diaphragmatic hernia Lobar emphysema Cystic adenomatoid malformation Pulmonary sequestration Pulmonary Causes for Respiratory Distress in Neonates Mechanical abnormalities • Pneumothorax • Pneumomediastinum Respiratory Distress in Neonates • The major signs of neonatal respiratory distress are tachypnea and cyanosis, in which tachypnea is defined as a respiratory rate consistently greater than 60 breaths/min. Respiratory Distress in Neonates • Nasal flaring (decrease airway resistance) • Grunting. • Chest retractions Suprasternal ( upper airway obstruction) Intercostal subcostal retraction Cyanosis NORMAL LUNG NORMAL LUNG Pulmonary Causes for Respiratory Distress in Neonates • • • • • Parenchymal conditions Transient tachypnea of the newborn Respiratory distress syndrome Pneumonia Meconium aspiration syndrome Transient Tachypnea Of The Newborn • Described by Avery 1966. • This relatively benign, self-limited disease also is known as RDS type 2 or wet lungs. • It occurs in approximately 11 per 1,000 live more in boys, more in cesarean section, and in infants who have perinatal asphyxia. Transient Tachypnea Of The Newborn • Delayed clearance of fetal lung fluid. • The syndromeis characterized by tachypnea that appears shortly after birth and usually clears within 1 to 5 days. Transient Tachypnea Of The Newborn • TTN is characterized by the presence of diffuse parenchymal infiltrates . • Accumulation of fluid in the various intralobar spaces. Clinical Diagnosis Of TTN • CXR – Pulmonary vascular congestion (1) – Perihilar streaking (2) – Incr lung volume (3) – Fluid in fissures 1 1,2 3 NORMAL LUNG increased pulmonary interstitial markings in both lung fields Transient Tachypnea Of The Newborn • In most cases, the clinical course is benign, and mechanical ventilation almost never is required. Respiratory Distress Syndrome • RDS is primarily a disease of preterm infants Near-term infants may be affected. • The condition is more common in boys . • The incidence is approximately six times higher in infants whose mothers have diabetes Respiratory Distress Syndrome • Multiple birth, cesarean section prior to the onset of labor, perinatal asphyxia. • Immature type II alveolar cells produce less surfactant, causing an increase in alveolar surface tension and a decrease in compliance. Pathogenesis surfactant pulmonary vascular W pulmonary perfusion atelectasis hypoxia hypercapnia acidosis respiratory metabolic surfactant deficiency capillary damage alveolar necrosis pulm vasospasm Clinical Diagnosis Of RDS • CXR Ground glass Air bronchograms Decr lung volume 1 2 1 2 3 3 4 5 6 7 NORMAL LUNG Clinical Diagnosis Of RDS Clinical Diagnosis Of RDS Bell shaped thorax 4 Clinical Diagnosis Of RDS Respiratory Distress Syndrome • Infants who have RDS may do well with nasal continuous positive airway pressure or may require ventilation. • Surfactant often improves pulmonary mechanics significantly but has little effect on overall outcome,which is favorable in most cases. Radiographic Progression Of BPD 1d 10d RDS Findings Complete Opacification 5mo 20d Cysitic Lucencies Larger cysts, Increased volume, Fibrosis strands Meconium Aspiration Syndrome • MAS is defined as respiratory distress in an infant born through meconium-stained amniotic fluid whose symptoms cannot otherwise be explained. Meconium Aspiration Syndrome • Meconium is composed of desquamated cells, secretions, lanugo, water, bile pigments, pancreatic enzymes, and amniotic fluid. Meconium Aspiration Syndrome • Meconium-stained amniotic fluid occurs in approximately 15 percent of deliveries, causing meconium aspiration syndrome. • Chemical pneumonitis • Inactivation of surfactant • Partial or complete airway obstruction Meconium Aspiration Syndrome • • • • Coarse infiltrates Widespread consolidation Hyperinflation Pneumothorax and pneumomediastinum may be present Clinical Diagnosis Of MAS • CXR – Lung overinflation (1) – Patchy/ splotchy densities (cloud like) NORMAL LUNG Meconium Aspiration Syndrome Secondary pulmonary hypertension is a frequent associated finding. The management of MAS remains a challenge. Persistent pulmonary hypertension • Common clinical features are severe cyanosis and tachypnea. • The lung fields may appear clear with decreased pulmonary vascularity. • The heart size may be normal or increased. Pneumonia • Pneumonia may be acquired in utero, during delivery (or perinatally), or postnatally in the nursery or at home. • It may be classified as either early- (7 d of age) or late onset (7 d of age). Pneumonia • bacterial infection takes time to develop, with respiratory consequences occurring hours to days after birth. • Risk factors for pneumonia include prolonged rupture of membranes, prematurity,and maternal fever Pneumonia • the chest radiograph may reveal classical patchy infiltrates, but the findings also may be indistinguishable from RDS. • The presence of a pleural effusion supports the diagnosis of pneumonia; it has been reported in up to 67% of cases Diagnosis Of Neonatal Pneumonia • CXR – Diffuse granular pattern (less uniform than RDS) (1) – Normal lung volume (2) – Pleural effusion (?) 1 ? 2 Pneumonia NORMAL LUNG Pneumonia • Pneumonias that are acquired at birth most often are caused by group B Streptococcus, but Escherichia coli, Klebsiella sp, and Chlamydia trachomatis also are seen. Pneumonia • Management • includes oxygen therapy, ventilatory support, antibiotics,and often vasopressor support such as dopamine and dobutamine. Pulmonary Causes for Respiratory Distress in Neonates • • • • • Developmental abnormalities Congenital diaphragmatic hernia Cystic adenomatoid malformation Lobar emphysema Pulmonary sequestration Congenital Diaphragmatic Hernia • CDH occurs in 1 in 2,000 to 4,000 births. • Males are affected more often (male:female ratio of 1.5:1), and the recurrence risk in future pregnancies is 2%. • CDH is a developmental abnormality of the diaphragm resulting in a defect that permits abdominal viscera to enter the chest. • Usually the defect occurs before the eighth week of embryonic life. Clinical Diagnosis Of CDH • CXR Loops of bowel in L thorax (may initially be opaque, a air) R mediastinal shift Pulmonary hypoplasia Decreased contralateral lung volume Congenital Diaphragmatic Hernia • In the delivery room, the neonate typically presents with respiratory distress shortly after birth. • Physical examination may show the abdomen to be scaphoid. • Air entry is reduced on the affected side, and the heart sounds are displaced. Congenital Diaphragmatic Hernia • Immediate treatment includes intubation and mechanical ventilation, and a nasogastric tube should be passed for decompression. Congenital Diaphragmatic Hernia • The presence of associated major malformations increases the mortality markedly, as does liver herniation • If there are no other anomalies and the defect is not part of a genetic syndrome, the prognosis after neonatal surgical repair usually is good, with overall survival rates for live born infants of 60% to 80%. Congenital Cystic Adenomatoid Malformation • CCAM consists of a multicystic mass of dilated bronchiolar like spaces that proliferate at the expense of alveoli. • The result is the formation of a rubbery lesion that enlarges following air and fluid trapping. Congenital Cystic Adenomatoid Malformation • Males and females are affected equally. Approximately 50% of the cases present as lifethreatening respiratory distress in the neonatal period. • The condition is more common on the right side, and usually only one lobe is involved. Congenital Cystic Adenomatoid Malformation Congenital Cystic Adenomatoid Malformation • Treatment is by surgical resection of the lesion. The survival rate has been reported to be 100% in neonates who do not have hydrops fetalis, but is much lower in those who have hydrops. Congenital Lobar Emphysema • CLE is characterized by air trapping and overdistention of segments and lobes of the lungs. • Clinical symptoms include respiratory distress, mediastinal shift. • The upper lobes are involved in 90% of the cases. • The diagnosis can be made by simple chest radiograph Congenital Lobar Emphysema Congenital Lobar Emphysema • It is more common in males (2:1). Sometimes the lesion can be mistaken for pneumothoraxor CDH. • There are associated anomalies in 14% to 40% of cases (cardiovascular) • The prognosis is favorable Pulmonary Sequestration • Lobar sequestration is composed of abnormal lung tissue that has no connection with the normal tracheobronchial tree. • It is more common in males (3 to 4 times), and 50% of patients have respiratory distress due to compression of the rest of the lung parenchyma. Pulmonary Sequestration • In more than 65% of cases, there are associated anomalies, including CDH (20% to 30%),. • The definitive treatment is resection of the lesion. Pulmonary Causes for Respiratory Distress in Neonates Mechanical abnormalities • Pneumothorax • Pneumomediastinum Pneumothorax • A pneumothorax (pneumo=air; thorax=chest) is a collection of air in the pleural cavity surrounding the lung. It is caused by the rupture of one or more alveoli which allows air to escape from the lung. • The pneumothorax compresses the lung and prevents normal lung expansion during inspiration. Usually a pneumothorax occurs on one side only but it may be bilateral Pneumothorax • Clinical Features • sudden deterioration with desaturation • increase in respiratory distress and/or diminished chest movements • circulation may become compromised • blood gases may show hypoxia, respiratory and/or metabolic acidosis. • Clinical signs include • unequal or decreased air entry • displaced apex beat Pneumothorax • WHO IS AT RISK OF PNEUMOTHORAX? • 1. All infants with respiratory distress, whatever the cause. • 2. Infants with meconium aspiration are at increased risk. • 3. Infants that need intubation and ventilation at resuscitation. • 4. Infants that are intubated and are ventilated in the nursery. Pneumothorax • The suspected clinical diagnosis can be confirmed by: A chest X-ray which will show air in the pleural space. Pneumothorax Outline of affected lung Mediastinal shift Air above diaphragm ? • Transillumination of the chest. The chest wall on the side of the pneumothorax transilluminates well while the chest wall on the normal side does not Pneumothorax • Transillumination is unreliable in : infants with increased thickness of the chest wall e.g. term infants and oedema infants with pulmonary interstitial emphysema (who may show a 'false positive' result) QUIZ QUIZ QUIZ Select tube size based on weight and gestational age Consider shortening tube to 13-15 cm Tube Size (mm) Weight (inside diameter) (g) Gestational Age (wks) 2.5 Below 1,000 Below 28 3.0 1,000-2,000 28-34 3.5 2,000-3,000 34-38 3.5-4.0 Above 3,000 Above 38 Tip-to-lip measurement Depth of insertion Weight (kg) (cm from upper lip) 1* 2 3 4 7 8 9 10 * Babies weighing less than 750 g may require only 6 cm insertion.