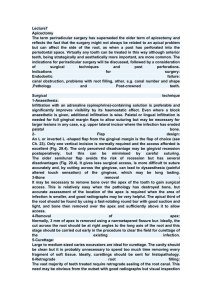
ROTARY INSTRUMENTS & APEX LOCATOR Dr. Ahmed Al-Bittar Lecturer at Al-Azhar University (Gaza/Palestine) ROOT CANAL TREATMENT PROCEDURES ➢Intra coronal preparation(access cavity) ➢Working length determination ➢Pulp extirpation ➢Intra-radicular preparation (cleaning and shaping) Cleaning and shaping of root canal system Basic Objectives in Cleaning and Shaping ◆Remove infected soft and hard tissue ◆Give disinfecting irrigants access to the apical canal space ◆Create space for the delivery of medicaments and subsequent obturation ◆Retain the integrity of radicular structures PRINCIPLES OF CLEANING AND SHAPING BIOLOGICAL OBJECTIVE ❖Removal of organic remnants and inorganic debris ❖Avoid pushing the necrotic debris to the periodontium ❖All instrumentation should be confined with canal space ❖Do no harm (tooth – periodontium) root canal systemanalsys MECHANICAL OBJECTIVE ❖Tapered preparation ❖preservation of the natural canal curvature , canal cross-section and tapered form ❖Preservation of the apical root anatomy ❖Creation of apical stop ❖Make the preparation in multiple plane ❖Keep the apical foramen as small as normal There were several problems with stainless steel instruments before the advent of NiTi: 1. Procedural errors, with instrumentation of curved canals (Zip formation, perforation, separation of the instrument...etc.) 2. Alteration of root canal morphology through the action of the restoring forces of stainless steel instruments 3. Instrumentation of curved canals was dealt with by: a. Precurving instruments and using a telescopic filing technique (step-back) b. Manufacture of intermediate sizes for use in the preparation of curved canals. 4. There is a substantial rise in instrument stiffness with increasing instrument size. Smaller sizes conform better to root morphology. 5. While manufacturers had recently marketed a number of new instruments based upon different crosssectional shapes, design concepts, and fabrication procedures, in a quest for improved cutting efficiency and flexibility, all of these brands had been fabricated from stainless steel. WHY ROTARY INSTRUMENTATION? Enhanced ability to collect and remove debris from the canal system. Better control for maintaining the central axis of the canal, reducing the incidence of ledging or perforating. Reduction in the time required for instrumenting the canal. Why Nickel-Titanium ?? • reversible rearrangement of the nickel and titanium atoms at the molecular level. A new endodontic file is composed of nickel and titanium atoms arranged in a body-centered cubic lattice structure NiTi alloys are unique in that applied stress (i.e. bending) causes a called the austenite phase. When this file is placed in a curved canal, the atoms rearrange into a closely-packed hexagonal array and the alloy is transformed into the more flexible martensitic crystal structure. This molecular transition enables these files to bend easily and around severe curves without permanent deformation. Nickel Titanium: A Super Elastic Alloy It was developed by W. F. Buehler, a metallurgist investigating nonmagnetic, salt resisting, waterproof alloys for the space programme in Maryland, USA. NiTiNOL term is used worldwide for this special type of alloy. 55 NiTiNOL: 55 wt% Ni and 45 wt% Ti and less than 2 wt% Co, nearly the same number of Ni and Ti atoms are combined, being reflected in the term equiatomic. 60 NiTiNOL: contains about 5% more nickel (lower ‘‘shape memory effect’’ and increased heat treatability, together with increasing hardness). Thermodynamic Properties Two specific properties made NiTi a very promising alloy for endodontics: Shape Memory and Superelasticity. Several effects were noted that relate to its specific crystal arrangement with two stable main phases, austenite and martensite: a shape memory effect as temperature and strain-dependent pseudoelasticity, all attributable to specific thermodynamic properties of the new alloy. This lattice organization can be altered either by *temperature or stress. *Files can be subjected to varying temperature & stress during manufacture, autoclaving & during root canal preparation. There are three NiTi phases in these alloys: • Austenitic NiTi (austenite) has a complex body-centered cubic structure and exists at higher temperatures and lower stresses. Materials existing in this phase are strong & hard. It is considered the most stable phase. • Martensitic NiTi (martensite) has a complex structure described as monoclinic and exists at lower temperatures and higher stresses. Materials existing in this phase are soft & ductile. It is considered an unstable phase. • The R-phase is an intermediate phase with a rhombohedral structure that can form during forward transformation from martensite to austenite on heating and reverse transformation from austenite to martensite on cooling. The R-phase transformation shows unique properties, which attract widespread interest for practical applications. The more the alloy works in this phase, the more the characteristics of compliance and strength are established. The Ni-ti rotary endodontic instruments will thus be able to shape the root canal following the original root canal anatomy even if complex, without reaching elevated values of stress. A. Shape memory : By shape memory we mean the capacity of NiTi alloys to reacquire its initial shape through heating after strain. This property that is considered more relevant to orthodontics than endodontics. Transformation between austenite and martensite occurs by a twinning process at the atomic level, and the reversibility of this twinning is the origin of shape memory. Twinning: Martensite's crystal structure has the unique ability to undergo limited deformation in some ways without breaking atomic bonds. This type of deformation is known as twinning, which consists of the rearrangement of atomic planes without causing slip, or permanent deformation. When martensite is reverted to austenite by heating, the original austenitic structure is restored, regardless of whether the martensite phase was deformed. Thus, the name "shape memory" refers to the fact that the shape of the high temperature austenite phase is "remembered," even though the alloy is severely deformed at a lower temperature. B- Superelasticity/Pseudoelasticity The transition from the austensitic to martensitic phase can also occur as a result of the application of stress, such as occurs during root canal preparation. We define elasticity as the property of bodies to deform by the action of external forces and once these external forces cease the ability to return to the original state. This characteristic (superelasticity) is particularly evident when for example, using a finger, we try to bend two identical endodontic instruments, one in stainless steel, the other in NiTi. The stainless steel endodontic instrument presents a higher stiffness while the NiTi instrument is particularly compliant. The use of endodontic instruments in NiTi is particularly advantageous for shaping the canal system in harmony with the original anatomy. NI-TI VERSUS STAINLESS-STEEL Nickel titanium ▪Excellent flexibility (2-4 times) ▪ Plastic deformation ▪ Conforms to canal curvature ▪Expensive ▪Less cutting efficiency ▪Nickel allergy Stainless steel Less flexible Permanent deformation Straightens and transport canal cheaper more cutting efficiency •Advantages and disadvantages of Nickel Titanium Advantages • • • • • • Shape memory Superelasticity High flexibility Good resiliency Corrosion resistance Softer than stainless steel Disadvantages • Poor cutting efficiency. • NiTi files do not show signs of fatigue before they fracture. • Lower torsional strength than St.st Visual examination is not a reliable method for evaluation of any NiTi instrument. Their breakage can occur without any visible sign of unwinding or permanent deformation. CLASSIFICATION OF ROTARY INSTRUMENTS • Low-Speed Rotary Instruments Gates-Glidden burs Peeso instruments • Rotary Instruments for Canal Preparation CONVENTIONAL LOW SPEED HP 8,000-20,000 RPM, used with GGD and pesso drills 8,000-20,000 RPM GGD are of sizes 50-70-90110-130-150, made of carbon steel, the cutting part is flame shaped, side cutting, used in orifice enlargement and preparation of the coronal and middle thirds, removal of gutta percha in retreatments Gates gidden drills : 50,70,90,110,130,150 Pesso drills: 70,90,110,130,150,170 Gates glidden drills Pesso drills Pesso drills are of sizes 70-90110-130-150-170, made also of carbon steel, with longer cutting part, both end and side cutting used for post space preparation BASIC DESIGN FEATURES OF ROTARY FILE FLUTES Depression between cutting blades, to collect tissues and debris The deeper the flutes, the higher the cutting efficiency and the more debris removed PITCH Distance between corresponding points on two adjacent cutting edges INSTRUMENT TIP 1.Active/cutting Active tips: It has cutting edges on its surface and can help to shape the narrow, calcified canals. However, it has a disadvantage of accidental apical perforation or transportation. E.g. Quantec file. INSTRUMENT TIP 2.Passive/non cutting No cutting edges present and create a concentric circle at the end of the root. Eg. ProfileGT,lightspeed ,etc INSTRUMENT TAPER : CONSTANT & VARIABLE EXPRESSED AS THE AMOUNT OF THE DIAMETER INCREASES EACH M.M ALONG ITS WORKING SURFACE FROM THE TIP TOWARD THE FILE HANDLE INSTRUMENT SEPARATION. Torsional Fatigue Cyclic Fatigue CYCLIC FATIGUE TORSIONAL FATIGUE Fracture of Rotary NiTi Basically, there are two modes of rotary instrument separation. Torsional fracture and flexural fracture. Torsional Fracture: Occurs when an instrument tip is locked in a canal while the shank continues to rotate, thereby exerting enough torque to fracture the tip. Flexural Fracture: With every 180o of rotation, instrument flexes and stretches again and again resulting in the cyclic fatigue and subsequent fracture of the instrument. GUIDELINES FOR USING ROTARY ENDODONTIC INSTRUMENTS 1. Access Opening 2. Confirm apical patency 3. Create a glide path 4. Copious irrigation 5. Use lubricant 6. always clean the file file flutes from debris Coronal Flaring Apical patency Reproducible glide path EDTA Gel Rotary Systems Three main components are important when we talk about the rotary system. The file, the handpiece and the motor. A. Understanding Torque The term torque is used for the forces which act in the rotational manner. The amount of torque is related to mass of the instrument, canal radius and apical force when worked in the canal. As the instrument moves apically, the torque increases because of increased contact area between the file and the canal wall. Theoretically an instrument used with high torque is very active but chances of deformation and separation increase with high torque. Thus, as the file advances further into the canal, the pressure should be loosened to prevent the torque. The file having the greatest cross-sectional mass will be able to withstand the greatest torsion. B. Role of the Handpiece Handpiece is a device for holding instruments, transmitting power to them and position them intraorally. Both speed and torque in a handpiece can be modified by incorporation of the gear system. Various types of gearing systems can be incorporated in the handpieces but gearing is limited by the need to maintain the drive concentrically through handpiece and the head. Depending on the manufacturer and condition of the handpiece, each handpiece has different degree of effectiveness depending upon the torque values. Thus, one must take care while choosing appropriate handpiece, according to required speed and torque. C. Motors Torque control motors allow the setting of torque produced by the motor. In low torque control motors, torque values set on the motor is less than the value of torque at deformation and separation of the instruments. Where as in high torque motors, the torque value is higher as compared to torque at deformation and separation of the rotary instruments. During root canal preparation, all the instruments are subjected to different levels of torque. If torque level is equal or greater than torque at deformation the instrument will deform or separate. Thus, with low torque control motors, motor will stop rotating and may even reverse the direction of rotation when instrument is subjected to torque level equal to torque value set at the motor. Thus, instrument failure can be avoided. Where as in high torque motors, instruments may deform or separate before the torque value of motor is achieved. Hence, we can say that torque control is an important factor to reduce NiTi fracture. WHAT IS TORQUE? According to Marzouk Simonton and Gross , torque is the ability of the handpiece to withstand lateral pressure on the revolving tool without decreasing its speed or reducing its cutting efficiency. Torque is dependent on the type of bearing used and the amount of energy supplied to the handpiece. Mangat P, Raina A, Vaidya S, Bhatacharya A, Dhingra A, Sharma V. Torque and Speed in Endodontics: A Review. IJOCR 2018;6(2):97-100. INSTRUMENTATION MOTIONS : A. Rotary or Reciprocation? Rotation: Many engine-driven nickel-titanium files used for canal preparation rely on rotational motion, a reaming action, which affords substantial control in small, curved canals. These instruments are usually designed without an actively cutting tip and have less tendency to transport the apical preparation. The files are available in a large variety of shapes, designs, and material composition. Use of these instruments by dental students in laboratories has demonstrated fewer preparation errors compared with the use of stainless steel hand instruments. Reciprocation: It has been clinically utilized to drive stainless-steel files since 1958 but limited to the straight portion of the canal. With the discovery of Niti, the superelasticity allowed it to reach the apex with reciprocating motions. Examples of reciprocating systems: WaveOne and Reciproc (Single File Systems) Rotary instrument reciprocation can be symmetrical or asymmetrical. • Symmetrical reciprocation is defined as file motion that is equal in both directions. Eg. The file will rotate 90° forward and then rotate an equal amount (90°) in reverse. • Asymmetrical reciprocation is defined as file motion such that the forward rotation is greater than the reverse rotation. When a file rotates more in the forward direction than the reverse, it will eventually make a complete forward rotation. E.g. 150° forward motion alternating with a 30° reverse motion. Since this asymmetric pattern results in a net forward motion of the file, it is said to be “progressive”. Please note that the only conclusive factor in comparison between rotary and reciprocating motions is that reciprocation motion provides higher resistance to “Cyclic Fatigue”, all other properties are still under debate. Asymmetrical Rotation Type of rotation motion that is independent of the motor and handpiece. It is related to the design of the file. Revo-S (Micro-Mega, Besanc ßon, France) ProTaper Next (Dentsply Tulsa Dental Specialties) OneShape (MicroMega) Clinically, this provides 3 significant advantages: • • • Reduced engagement due to the swaggering effect which limits undesirable taper lock Affords more cross-sectional space for enhanced cutting, loading, and debris clearance Allows files to cut a bigger envelope of motion compared to a similarly-sized file with a symmetrical mass and axis of rotation. This means a smaller-sized and more flexible file can cut the same-size preparation as a larger and stiffer file with a centered mass and axis of rotation. OTR (Optimum torque reverse ) Or ATC (Adaptive torque control ) ATC manages the files stress in a smart way , when torque limit is reached , instead of going reverse mode , motor reciprocates till the stress is reduced , once back to below pre-set torque level , file will again rotate in continuous rotation ROTARY NI-TI INSTRUMENTS FIRST GENERATION Pro file Pro file GT Light speed Quantec Quantec Pro-file The first-generation rotary systems had neutral or slightly negative rake angles “radial land” area. This flat area prevents the file from locking in the dentin, while cutting occurs through a passive planing action. To appreciate the evolution of instruments, it is useful to know that all first-generation files had passive cutting radial lands, fixed tapers over the length of their working parts, and required a considerable number of files to achieve preparation objectives. SECOND GENERATION Pro taper K3 BioRace Pro Taper Universal BioRace K3 • • • They have actively cutting edges without radial lands Fewer instruments are required to fully prepare a canal. The helical angle is lower than in first-generation files, which greatly reduces the tendency for a screwing effect during use. THIRD GENERATION Hyflex CM Profile GT X Twisted file Twisted file Heat treatment (thermal processing) is one of the most fundamental approaches toward adjusting the transition temperatures of NiTi alloys and affecting the fatigue resistance of NiTi endodontic files. M-wire (Mechanical )was introduced in 2007. Its unique nano-crystalline martensitic microstructure exhibits higher strength than conventional superelastic NiTi wires. It is produced by applying a series of heat treatments to NiTi wire blanks. Manufacturers focused on using heating and cooling methods that resulted in a reduction of the cyclic fatigue associated with the file, which in turn would reduce the risk of instrument fracture while working with canals with prominent curvatures. The phase transition point of the nickel titanium alloy between martensite and austenite can be identified and optimized to result in a metal, better than NiTi itself. M-wire technology, R-phase technology, Controlled Memory Wire and Electrical Discharge Machining were notable changes brought in terms of innovation in NiTi metallurgy. M-wire instruments include: • • • ProFile GTX, ProFile Vortex Vortex Blue. • Vortex Blue: New NiTi rotary instruments made out of M-wire, show a unique “blue color” not seen in traditional superelastic (SE) NiTi instruments. The “blue-color” oxide surface layer of vortex Blue files is a resultant of the heat process that produces titanium oxide on the surface to improve cutting efficiency & wear resistance. The relatively hard titanium oxide surface layer on the Vortex Blue instrument may compensate for the loss of hardness compared with ProFile Vortex M-wire by improving the cutting efficiency and wear resistance. CM Wire A novel NiTi alloy with flexible properties that was introduced to endodontics in 2010. CM NiTi files are manufactured using a special thermomechanical process that controls the memory of the material, making the files extremely flexible but without the shape memory of other NiTi files. Instruments made out of CM Wire: • • The HyFlex TYPHOON CM They exhibit a lower percent by weight of nickel (52 Ni % wt) than the common 54.5–57 Ni % wt of the great majority of commercially available SE NiTi rotary instruments. FOURTH GENERATION Wave One Reciproc SAF(SELF-Adjusting File ) Wave One Reciproc Self adjusting file In 2011, both WaveOne and Reciproc (VDW) were launched as single-file shaping techniques. Both files are made out of M-wire. Innovation in reciprocation technology led to a fourth generation of instruments for shaping canals FIFTH GENERATION Pro taper Next One shape Revo S Revo S Glide Path Concept=securing an open pathway to the canal terminus that subsequent engine-driven instruments can follow. -Working Length Reconfirmation -Copious Irrigation inside pulp chamber -Never Force any instrument. ELECTRONIC APEX LOCATOR An electronic device used to determine the working length. The apex of the root has a specific resistance to electrical current, and this is measured using a pair of electrodes typically hooked into the lip and attached to an endodontic file Disadvantages: 1. teeth with an immature apex 2. teeth with root resorption 3. Large radicular cysts 4. Contact between the instrument and a metallic restoration 5. The canal still contains traces of the old canal obturation 6. Contraindicated in patients with pacemakers Advantages: 1- Time saving 2- More accurate than radiographs that have the following problems : ▪ ▪ ▪ ▪ a two-dimensional image of a three-dimensional structure When the apical foramen exits to the side of the root or in a buccal or lingual direction. Dense bone and anatomical structures can make the visualization of root canal files impossible by obscuring the apex The deposition of secondary dentine and cementum can move the apical constriction further from accepted limits causing preparation errors. • Disadvantages OF EAL : A) Can provide inaccurate readings in following cases:i. Presence of pulp tissue in canal iii. Use of narrow file ii. Too wet or too dry canal iv. Blockage of canal v. Incomplete circuit vi. Low battery B) Chances of over estimation C) May pose problem in teeth with immature apex. Advantages of radiographic methods of working length determination 1. One can see the anatomy of the tooth 2. One can find out curvature of the root canal 3. We can see the relationship between the tooth and anatomic structures. ❑ Disadvantages of radiographic methods of working length determination ❑ Varies with different observers ❑ Two-dimensional view of three-dimensional object ❑ Cannot interpret if apical foramen has buccal or lingual exit ❑ Risk ofradiation exposure ❑ Time consuming ❑ Limited accuracy ❑ Superimposition of anatomical structures EAL >>They are basically used to locate the apical constriction and not the radiographic apex. Anatomy of Apical foramen Figure 1 Idealized anatomy of apical portion of root (a) major apical foramen, (b) minor apical foramen (apical constriction) that may be coincident with the cemento dentinal junction (CDJ), (c) cementum, (d) dentine and (e) root apex The ability to distinguish between minor diameter and major diameter of apical terminus is most important for the creation of apical control zone. The apical stop is the mechanical alteration of the apical terminus of root canal space which provides resistance and retention form to the obturating material against the condensation pressure of obturation. PARTS OF ELECTRONIC APEX LOCATOR MECHANISM OF ACTION OF APEX LOCATOR ❑Root canals are surrounded by dentine and cementum that are insulators to electric current. At the apical foramen there is a small hole in which conductive materials within the canal are electrically connected to the periodontal ligament that is a conductor of electric current. ❑The resistive material of the canal (dentine, tissue, fluid) with a particular resistivity forms a resistor. ❑If an endodontic file penetrates inside the canal, and approaches the canal terminus, the resistance between the end of the instrument and the apical portion of the canal decreases, because the effective length of the resistive material inside the canal decreases . Apex locators use the human body to complete an electrical circuit.One side of the circuitry is connected to an endo instrument & the other end to the patients body- (patients lip or by an electrode held in the patients hand).The impedance between the lip and the periodontal ligament (PDL) is a known value,6.5 KOhm so as the file tip is advanced toward the PDL, the EAL detects the changing impedance values and indicates the approach to the apex on its screen. FIRST GENERATION Resistance apex locators: Measures the resistance to flow of direct current Disadvantages: conductive fluid such as irrigant, exudate or hemorrhage in the canal would permit current flow and gave a false reading SECOND GENERATION Impedence apex locators: measure the opposition to flow or impedance to alternating current. Disadvantages: A major disadvantage of second generation apex locators is that root canal has to be free of electroconductive materials to obtain accurate readings. Presence of electroconductive irrigants changes the electric characteristics and lead to inaccurate readings. Impedence = Capacitance + resistance, so any change in the capacitance of the circuit along with many other variables will affect accuracy. THIRD GENERATION Frequency dependent apex locator Based on the fact that different parts of the canal, give difference in impedance between high and low frequencies, that is least in coronal part of the canal, and highest in the apical part They are based on the fact that different sites in canal give difference in impedance between high (8 KHz) and low (400 Hz) frequencies. The difference in impedance is least in the coronal part of canal. As the probe goes deeper into canal, difference increases. It is the greatest at cementodentinal junction. FOURTH GENERATION - Measures the capacitance and the resistance separately, instead of the resultant impedance - A significant disadvantage of the fourth generation devices is that they need to perform in relatively dry or in partially dried canals so difficult to use in cases of heavy exudates or weeping canals. FIFTH GENERATION - Increased accuracy in determining the place of apical foramen. - Perform very well in the presence of blood and exudate, but they experience considerable difficulties while operating in dry canals. SIXTH GENERATION - Adaptive apex locator This apex locator is intended to overcome the disadvantages of fourth- and fifthgeneration EALs. It eliminates the need of drying the canals. Examples of 6th generation apex locator are -Adaptive apex locator -Raypex 6 HOW TO USE??? Clinical use: 1. Analyse the root anatomy for curvature and establish an estimated working length from the pre operative radiograph. 2. The coronal aspect of the canal should be opened/prepared to provide straight line access or a “glide path” to the apical aspect of the root canal. 3. Modern apex locators generally function well in the presence of fluids and irrigants in the root canal, but prior to using the apex locator excess irrigating fluids are removed from the access cavity. 4. Once the lip hook and file holder are attached, in most cases a size 15 or 20 file is advanced into the root canal until the blue scale on the apex locator reaches the “apex and red triangle ” on the screen of the root ZX. This indicates that the file is now at the apical foramen . 5. A diagnostic radiograph is taken with the file at this length. If the radiograph confirms the file to be at the apex this length is effectively the “canal length”. 6. Since the apical constriction is on average 0.5 mm from the apical foramen, the working length is calculated by subtracting 0.5 mm from the canal length. The canal can now be prepared to the working length. If you are an advocate of patency filing, a size 10 file should be placed to the canal length to maintain the patency of the root canal CONCLUSION The electronic apex locators are now considered the most ideal method to measure the working length of a root canal. They can be used alone without the need of radiographs. However , It is recommended combined use of an apex locator along with the radiographic technique for accurate clinical measurement of Root Canal working length .