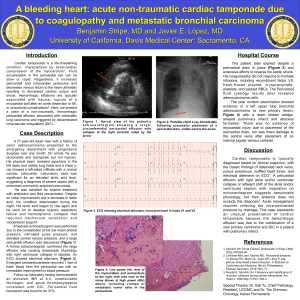
PRESENTED BY GROUP 9 DONNA MC CARTHY, TISHARA MC CARTHY VITRA KUARSINGH RAMPERSAD CARDIAC TAMPONADE • Cardiac tamponade is also known as pericardial tamponade, cardiac compression or simply tamponade. • It is associated with pericardial effusion. • Cardiac tamponade can occur acutely(a rapid increase of fluid into pericardial space, as little as 200 mL) or sub acutely (slow accumulation of fluid into pericardial sac over weeks or months, causing pericardium to stretch and accommodate up to 2 L of fluid without severe increases in intrapericardial pressure. DEFINITION 1.Cardiac tamponade is a life-threatening compression of the heart by fluid or blood accumulated in the pericardial sac. 2.Cardiac tamponade is a medical emergency that occurs with the collection of material such as fluid, blood, pus, or clots leading to increased intrapericardial pressure causing compression of all cardiac chambers and ultimately hemodynamic collapse. Cardiac tamponade can be the consequence of: 1.Pericarditis ETIOLOGY 2.Pericardial effusion 3.Malignant disease 4.Renal failure 5.Radiation therapy 6.Invasive cardiac procedures with perforation 7.Cardiovascular surgery ETIOLOGY 8.Chest trauma 9.Aortic dissection 10.Anticoagulant therapy RISK FACTORS 1.HIV 2.History of heart failure 3.TB 4.Lupus and some other autoimmune conditions 5.Medications eg, phenytoin, hydralazine PATHOPHYSIOLOGY As a result of the surrounding tense pericardial fluid, the heart is compressed, and the diastolic pressure within each chamber becomes elevated and equal to the pericardial pressure. The compromised cardiac chambers cannot accommodate normal venous return, so the systemic and pulmonary venous pressures rise. PATHOPHYSIOLOGY • The increase of systemic venous pressure results in signs of right-sided heart failure (e.g., jugular venous distention), whereas elevated pulmonary venous pressure leads to pulmonary congestion. • In addition, reduced filling of the ventricles during diastole decreases the systolic stroke volume, and the cardiac output declines PATHOPHYSIOLOGY These derangements trigger compensatory mechanisms aimed at maintaining tissue perfusion, initially through activation of the sympathetic nervous system (e.g., elevation of the heart rate). Nonetheless, failure to evacuate the effusion leads to inadequate perfusion of vital organs, shock, and ultimately death. CLINICAL MANIFESTATIONS Manifestations may vary based on the severity of the tamponade. These include: 1.Jugular vein distention 2.Hypotension 3.Muffled or distant heart sounds CLINICAL MANIFESTATION CLINICAL MANIFESTATIONS • Pulsus paradoxus (a decrease in systolic blood pressure greater then 10 mmHg during inspiration) • Anxiety and restlessness • Chest pain radiating to neck, shoulders, or back • Presyncope, syncope, unconsciousness • Dyspnea • Oligo-anuria CLINICAL MANIFESTATIONS • Shock • Cyanosis • Orthopnea • Edema • Cough • Dysphagia • Fever (dependent on etiology) DIAGNOSTIC EVALUATION 1.Medical history and history of present illness. 2. Physical exam: This will include taking vital signs such as pulse, blood pressure checking for pulsus paradoxus (blood pressure drops unusually each time you take a breath)and respiration. Auscultation of heart and breath sounds. DIAGNOSTIC EVALUATION 3. Echocardiogram: -Determine the presence of pericardial fluid - Exact distribution of pericardial fluid - Cause of tamponade, if possible - Determine the safest and most logical method of pericardial drainage, if needed. 4. Electrocardiography- May demonstrate diminished QRS and T-wave voltages. DIAGNOSTIC EVALUATION 5. Chest X-ray – shows an enlarged, globeshaped heart or “water bottle” (“Bocksbeutel”) appearance if cardiac tamponade is present. DIAGNOSTIC EVALUATION 6. Thoracic CT scan – looks for fluid accumulation in the chest or changes to the heart. 7. Magnetic resonance angiogram - to see how blood is flowing through the heart. DIAGNOSTIC EVALUATION 8. Heart catheterization: This test allows the inside of the heart and blood vessels to be seen by using a device that’s inserted into an artery and then threaded toward and into the heart. 9. Renal profile and Complete blood count 10. Creatine kinase and isoenzymes: elevated in myocardial infarction and cardiac trauma. 11. HIV testing. COMPLICATIONS 1.Heart failure 2.Pulmonary edema 3.Bleeding 4.Shock 5.Death MEDICAL MANAGEMENT 1.Pericardiocentesis: To drain the fluid from the pericardium using a needle. 2.Inotropic drugs, such as dobutamine: To improve heart function and lower blood pressure. 3.Anti-inflammatory medicines such as aspirin, ibuprofen, steroids. 4.Diuretics, such as furosemide or spironolactone. MEDICAL MANAGEMENT MEDICAL MANAGEMENT 5.Oxygenation 6.IV fuids 7.Blood transfusion (trauma or open heart surgery) 8.Treatment of the underlying cause MEDICAL MANAGEMENT Surgery: Surgical creation of a pericardial window allows drainage of the effusion. Implantation of a pericardio-peritoneal shunt in cancer patients whose disease is causing the fluid accumulation. Pericardiectomy to remove the pericardium if all other interventions fail. MEDICAL MANAGEMENT For recurrent tamponade: Sclerosing the pericardium – introduction of either corticosteroid, tetracycline or antineoplastic drugs in the pericardial space. NURSING MANAGEMENT NURSING ASSESSMENT The Nurse will obtain a history of the patient focusing on: NURSING ASSESSMENT The Nurse will obtain a history of the patient focusing on any surgery, trauma, cardiac biopsy, viral infection, insertion of a transvenous pacing wire or catheter, or myocardial infarction. The Nurse will elicit a medication history to determine if the patient is taking anticoagulants or any medication that could cause tamponade as a drug reaction. NURSING ASSESSMENT Assess the patient following the ABC approach. Closely monitoring the patient ’s vital signs; of blood pressure, temperature, pulse and respiratory rate. Also noting, skin color and capillary refill. Assess cardiovascular status: monitor for jugular vein distention and presence of Kussmaul’s sign (jugular venous distention upon inspiration) Assess the patients consciousness level for decreased cerebral perfusion. NURSING ASSESSMENT • The Nurse will: • Assess the patient’s and relative's degree of fear and anxiety, as well as their ability to cope with a sudden illness and threat to self. GOALS AND EXPECTED OUTCOMES The patient will demonstrate relief of pain with stable vital signs. The patient will be able to maintain adequate cardiac output. The patient will demonstrate utilization of coping mechanisms to reduce anxiety. The patient will maintain appropriate fluid volume. NURSING DIAGNOSIS • Decreased Cardiac Output related to a reduction in ventricular filling secondary to elevated intrapericardial pressure as evidenced by irregular heartbeat, pulsus paradoxus, blood pressure of 89/58, restlessness, dyspnea upon exertion, and fatigue. • Acute Pain related to increased intrapericardial pressure as evidenced by pain score of 10 out of 10, verbalization of pressure-like chest pain and guarding of the chest. NURSING DIAGNOSIS • Risk for fluid overload related to decreasing plasma protein, increased sodium, and presence of water retention secondary to cardiac tamponade. INTERVENTIONS • PERICARDIOCENTESIS • The Nurse will obtain baseline vital signs before pericardiocentesis. • Have an emergency pericardiocentesis tray available. • Reinforce the physician’s explanation of a pericardiocentesis and ensure the patients consent form is signed. • Prepare the patient for the procedure. • Measure, describe, and record the amount of pericardial fluid removed. INTERVENTIONS • Label all specimens for laboratory analysis and send them promptly to the laboratory. • Cover the site of the pericardiocentesis with a sterile dressing and inspect the dressing for bleeding or leaking fluid. • Reinforce the dressing if it becomes moist. • Patient is placed in bed with the elevation of the lower extremities – aides to increase venous return. • Continue to monitor vital signs until they are stable. NS INTERVENTIO • PHYSIOLOGIC NEEDS • PAIN • Assess pain using pain scale and administer anti-inflammatory drugs dobutamine and analgesics as prescribed for pain and symptomatic relief. • Monitor therapeutic effects of medication. • Educate patient on deep breathing exercises, and relaxation techniques. • Help the patient to assume a comfortable position. INTERVENTIONS • OXYGENATION • The Nurse will: • Administer supplemental oxygen, via nasal canula as prescribed. Ensure "NO SMOKING" sign is in place. • Establish continuous oxygen saturation monitoring using a pulse oximeter. • Position patient with head of the bed elevated, in a semifowler’s position • Review ABG's INTERVENTIONS Monitor ECG continuously for any signs of dysrhythmia. Monitor patient’s vital signs every 15 minutes during the acute phase Observe for signs of decreasing peripheral tissue perfusion such as slow capillary refill, facial pallor, cyanosis, and cool, clammy skin. INTERVENTIONS • NUTRITION AND ELECTROLYTE BALANCE • Provide prescribed diet. • Administer IV fluids as prescribed for volume expansion. • Ensure that all IVs are infusing properly. • Monitor and record intake and output, measuring urine output hourly. • Monitor for edema and ascites. • Monitor electrolyte levels. INTERVENTIONS • MAINTAINING TISSUE INTEGRITY • Provide frequent oral hygiene • Assist with ADLs • Change linens regularly or as they become soiled. • Change the patient’s position frequently and with an interval of at least every 2 hours as tolerated. INTERVENTIONS • PROMOTING COMFORT • Decrease environmental stimuli such as noisy television • Adjusting the temperature in the room • Adjusting lighting in the room • Provide privacy during interventions • Use communication techniques such as listening and empathy. • Keep a calm attitude when interacting with the patient. INTERVENTIONS • SAFETY AND SECURITY • The Nurse will monitor the environment for hazards and remove them. • Keep the bed in a low position, with side rails elevated. • The Nurse will instruct the patient on bed rest, to stay in bed. INTERVENTIONS • REDUCING ANXIETY • The Nurse builds a therapeutic relationship with the patient and relative. • Explain the procedures appropriately and keep the explanations basic so that the patient will easily understand. • Advise the patient to express his or her feelings and emotions about the procedure and the condition. • Acknowledge and be aware of the patient’s feelings and anxiety. INTERVENTIONS • Explain to the patient that the chest pains does not necessarily lead to myocardial infarction. • Reassure the patient and the significant others that monitoring the patient continuously will guarantee prompt intervention. • Encourage the patient to be part of setting goals and planning of care. • Encourage the patient to have ample sleep and rest. INTERVENTIONS • LOVE AND BELONGING • The nurse involves the patient and relatives in all aspects of planning care. • Relatives and friends are encouraged to visit and spend as much time possible with the patient. • The nurse engages in active listening and uses touch appropriately. INTERVENTIONS • SPIRITUALITY • Observe the patient for cues that may indicate an underlying spiritual need. • The Nurse engages in active listening and displays a caring attitude. • The Nurse accepts the religious beliefs and practices of the patient and does not try to impose his/her beliefs on the patient. • The Nurse engages in prayer for the patient at their request. PATIENT TEACHING/EDUCATION Review Review all medications with the patient—purpose, adverse effects, dosage, and special precautions. Educate Educate the patient on the symptoms of tamponade and when to return to the hospital. Encourage Encourage patient to keep clinic and imaging appointments. The patient will demonstrate relief of pain as evidenced by a pain score of 2 out of 10 with stable vital signs. The patient will maintain adequate cardiac output. EVALUATION The patient will demonstrate utilization of coping mechanisms to reduce anxiety. The patient will maintain appropriate fluid volume.