RENAL PHYSIOLOGY
I. Introduction
A. The kidneys function to:
1. filter metabolic wastes out of blood, and they are
2. vital for homeostasis, by:
a. maintaining fluid and electrolyte balance
b. the maintenance of pH levels
c. their role in controlling blood pressure, with the renin angiotensin system.
[10VSL 530 Fig.14-4]
B. Kidney anatomy. Note the location of the following:
1. cortex, which contains the renal corpuscles (Bowman's capsule & glomerulus).
2. medulla, which contains collecting tubules and Loops of Henle.
3. minor and major calyces are the smaller spaces emptying into the renal pelvis
[10VSL 527 Fig.14-2] [10VSL 529 Fig.14-3] {Gartner & Hiatt 305 & 308}
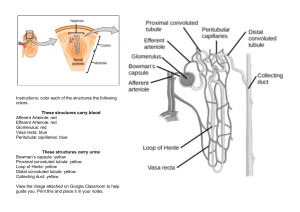
C. Nephron anatomy:
{SS535,fig.29-3} {SS536,fig.29-4} {MC478,fig.25-4}
1. The functional units of the kidney are called nephrons. There are >1¼ million per kidney; each
has ~3cm of tubes; the total length is 50 mi.
2. Nephrons resemble funnels with convoluted stems.
a. The proximal end forms a double-walled Bowman's capsule, which surrounds a cluster of
capillaries, called the glomerulus. Bowman's capsule has an outer parietal layer (a simple
squamous epithelium) and an inner layer of highly specialized podocytes, that coat the
glomerular capillaries.
b. A renal tubule extends from Bowman's capsule to the collecting tubule and is sectioned into:
i. the proximal convoluted tubule,
ii. the loop of Henle (with descending and ascending limbs) and
iii. the distal convoluted tubule, which connects with the collecting tubules (which run down
through medulla of the kidney and join the calyces).
[Renal Corpuscle, fig. 20-3]
D. Renal Circulation: renal artery → afferent arterioles → glomerulus → efferent arterioles →
peritubular capillaries (around renal tubule) → renal vein.
[10VSL 531 Fig.14-6]
II. Urine Excretion
Urine excretion by the kidney is accomplished by 3 successive processes:
A) Glomerular filtration, B) Tubular reabsorption, C) Tubular secretion.
[10VSL 529 Fig.14-3]
A. Glomerular filtration:
1. In the glomeruli, water & solutes filter out of the blood and into the Bowman's capsules. This
filtration rate is faster than ordinary capillaries because:
a. glomeruli have more pores than ordinary capillaries.
b. efferent arterioles are smaller than afferent arterioles; thus, there is an increase in blood
pressure within the glomerulus.
The glomerulus blood pressure = 70mm Hg. Other capillaries = 30mm Hg.
2. Because a pressure gradient exists between the glomerulus and Bowman's capsule, fluid
leaves the blood and enters Bowman's capsule.
This pressure gradient is the Effective Filtration Pressure (EFP).
The EFP is determined by 3 factors:
(a) Glomerular Hydrostatic Pressure
(b) Blood Colloidal Osmotic Pressure
{AK451}
{AK453}
(c) Capsular Hydrostatic Pressure
a. The glomerular hydrostatic pressure is the blood pressure within the glomerulus. It tends to
drive fluid out of the glomerulus and into Bowman's capsule. It is usually about +70 mm Hg.
b. The blood colloidal osmotic pressure is the osmotic pressure which tends to move water from
an area of low colloid concentration to an area of high colloid concentration. This tends to
move fluid from Bowman's capsule back into the glomerulus. The protein concentration in
blood is high and is low in the filtrate. Because osmosis of HOH is from high to low
concentration of HOH, HOH diffuses from the Bowman's capsule back into the glomerulus.
This averages -30 mm Hg.
c. The capsular hydrostatic pressure is the pressure exerted by the fluid in Bowman's capsule
(back toward the glomerulus). Averages -20 mm Hg.
3. Therefore, the effective filtration pressure equals 20 mm Hg (70 -30 -20).
There is a 20 mm Hg pressure gradient, between the pressure in the glomerulus and
Bowman's capsule, which causes fluid to flow out of the blood (within the glomerulus) and into
Bowman's capsule.
4. Normally the total glomerular filtrate averages about 125 ml/min. in men and lower in women.
5. The glomerular hydrostatic pressure is regulated by mechanisms which change the diameters
of the afferent and efferent arterioles and by changes in the systemic blood pressure.
a. Sympathetic impulses cause constriction of both the afferent and efferent arterioles; this causes
a slight drop in the glomerular hydrostatic pressure.
b. With intense sympathetic stimulation, the afferent arterioles become more constricted than the
efferent arterioles. This causes the glomerular hydrostatic pressure to fall and lowers the
amount of filtration.
c. The glomerular hydrostatic pressure is directly related to the systemic blood pressure. An
increase in blood pressure produces an increase in the glomerular pressure and thus an
increase in the filtration rate.
(The converse is also true).
6. Glomerular filtration is inversely related to the blood colloidal osmotic pressure.
a. Specifically, a decrease in blood protein concentration causes a decrease in the blood colloidal
osmotic pressure.
This, in turn, causes an increase in glomerular filtration.
b. Kidney disease sometimes causes a loss of blood proteins into the urine. Therefore, this would
cause an increase in glomerular filtration.
B. Tubular reabsorption
1. Recall that normally the glomerular filtration rate averages ~125 ml/min. Obviously this is not the
volume of urine produced per min.
Thus, most of the filtrate is reabsorbed from the convoluted tubules, loops of Henle and
collecting tubules.
2. The water and solutes reabsorbed from the nephron enter the peritubular capillaries (around
the nephron).
3. The cells of the nephron are highly selective and absorb most efficiently, the molecules which are
vital to body needs, such as: Na+, Cl-, HCO3-, H2O, and glucose.
4. Reabsorption is not merely a physical matter of diffusion and osmosis but also involves active
transport (which requires energy).
Active transport mechanisms absorb nutrients, like glucose and amino acids, and some
electrolytes (salts).
{AK455}
5. Glucose and other nutrients are transported from the proximal tubule and re-enter the blood. This
is done so effectively that normally no glucose is found in the urine. If there is an excessive
amount of glucose in the blood (viz. above 150mg/100ml blood) then there will be some
glucose in the urine because the glucose transport mechanism cannot reabsorb it all.
6. If the ability of the glucose transport mechanism is reduced then glucose appears in the urine
(called glycosuria) even though the glucose level in the blood is normal. This condition is
known as renal diabetes or renal glycosuria.
7. Electrolytes are reabsorbed partly by active transport and partly by diffusion.
For instance, Na+ ions are actively transported from all parts of the tubule. Because Na+ ions
have a positive charge, they attract negative ions (viz. Cl-) which are drawn out of the tubule
back into the blood.
8. The transport of Na+ from the tubule into the blood also momentarily upsets the equilibrium
between the osmotic pressures of the blood and tubular filtrate.
a. To reestablish this equilibrium, water moves out of the tubule and into the blood, by osmosis.
b. The active transport of Na+ out of the tubule is the main factor causing osmosis of water out of
the tubule.
c. This is the reason for water reabsorption from the proximal tubule.
This is termed obligatory water reabsorption because the water is forced to leave the
tubule by the law of osmosis.
d. The distal and collecting tubules have the ability to vary the volume of water they reabsorb.
Therefore, the term facultative water reabsorption is used to describe this function of the
distal and collecting tubules.
9. Tubular reabsorption is controlled mainly by hormones.
a. How much water is reabsorbed is controlled by vasopressin (antidiuretic hormone; ADH),
which is released by the neurohypophysis (posterior pituitary gland).
The action and control mechanisms of vasopressin are extremely complex, but the end result is
clear. It causes the distal and collecting tubules to increase reabsorption of water, which
decreases the volume of urine.
Water balance cannot be maintained without the vasopressin mechanism.
b. The mineralo-corticoids are a group of hormones produced by the adrenal cortex. These
hormones regulate the reabsorption of electrolytes.
The most potent of these is aldosterone, which increases Na+ reabsorption and therefore
increases HOH reabsorption. The adrenal cortex is essential for life.
C. Tubular Secretion (excretion): See [figures 20-3 and 20-7]
1. In addition to reabsorption, the tubules secrete certain substances, which are moved from
the peritubular capillaries into the tubules.
2. Some substances are moved by active transport and some by diffusion.
a. Ammonia is secreted by diffusion.
b. K+ & H+ ions are secreted by active transport.
c. Some drugs are secreted by active transport: penicillin and para-aminohippuric acid (PAH).
This drug is administered in known doses and then the amount in the excreted urine is
measured.
In this manner tubular secretion can be evaluated.
{J&F427} {SBL452}
III. Diseases Associated with the Kidney:
A. Nephritis is inflammation of the kidney, which develops 10 to 20 days after an acute
infection (in the body).
1. During the initial or acute phase, red blood cells appear in the urine (hematuria) and so
does protein (proteinuria).
2. The major pathological effects are hypertension, edema and accumulation of electrolytes
and nitrogenous wastes in the blood (uremia).
3. In most cases recovery is spontaneous, but in about 2% of the cases the disease becomes
chronic.
{SB&L452} {Cr421}
B. Kidney stones (renal calculi) may be formed in the collecting tubules, pelvis, ureters or
urinary bladder.
These form for a variety of reasons:
1. Pyelonephritis is an infection of the kidney, which alters the pH;
this may cause ammonium phosphate stones.
2. Calcium stones are common in patients with hyperthyroidism.
3. Gout is another common cause of kidney stones.
This metabolic disease elevates uric acid excretion.
C. One can survive normally with one kidney, making kidney donors possible.
It is possible to live without any functional kidney if hemodialysis is used.
This is done by passing the blood through a dialysis tube coil.
The dialysate is body temperature and contains the proper concentrations of all the
blood plasma constituents.