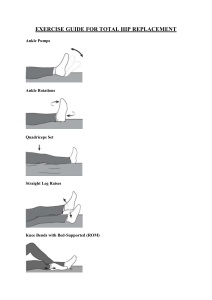
First Part of Exam The information you learn in this course will improve your understanding of how the human body functions and how to instruct your clients during a workout session as a personal trainer. You will also be able to create physical training programs for your clients that are tailored to their goals. If you happen to work in the medical profession, you can apply the information you attained from this Corrective Exercise course to improve your understanding of how the human body works and provide the best care for your patients. A medical professional will be able to help their client avoid worsening current injuries or preventing unnecessary injuries. If fitness and personal training is your area of interest, you can apply the information you learned in this course to deepen your awareness of the body's physiology. With this information, you'll be better equipped to prevent and treat injuries, as well as design workout regimens that are uniquely tailored to the objectives of your customers. You should also be able to answer most of the questions your clients are asking regarding the exercises they perform during their workout routine. The ability to guide them throughout their journey to a safe and healthier lifestyle should be what a fitness instructor or personal trainer strives for. Finally, whether you are in the medical field or the fitness industry, this program will broaden your understanding of human physiology and confidently answer most questions your clients are having. Also, importantly always refer to a medical professional if your client is not feeling right and get a medical clearance before any workout. Second Part of Exam A) The muscles responsible for hip abduction and external rotation are: Gluteus medius Gluteus minimus Tensor fasciae latae Superior gemellus Inferior gemellus Obturator internus Obturator externus Quadratus femoris Piriformis Strengthening these muscles can reduce the discomfort in Tom's knees by improving the stability and function of his hip joints Due to the frequent neglect of these muscles, it is common for people to develop weakness with hip abduction and external rotation. We tend to spend our days sitting, especially after the pandemic when people worked from home. That ultimately causes your gluteal muscles, hip abductor, external rotators, and hip flexors to tighten and weaken. Those who go to a fitness center, tend to train the larger, more superficial muscles of the legs, such as the quadriceps, hamstrings, and gluteus maximus, which are the primary targets of many conventional lower-body workouts like squats and lunges. These workouts do not really trigger or activate the smaller and deeper hip muscles in charge of the external rotation and abduction. That being said, muscle imbalances, overuse injuries, and repetitive physical motions can contribute to a weakening of the hip abductors and external rotators. Weak hips will result in knees and lower back pain. To avoid this discomfort, the person can perform exercises that target these muscle groups mentioned in the first answer “a)” to increase hip joint strength and stability. B) Tom will do exercises while having a resistance band wrapped around his lower thighs. This will then trigger the gluteus medius and minimus located by the hip abductors, piriformis, and obturator muscles found by the external rotators. By using these bands, Tom will consciously push his knees out against the resistance and will activate those neglected muscles mentioned above. Tom should seek to improve his motor control. To do so, it is crucial that he performs the band squats slowly with a tempo. That will result to activate his hip muscles while maintaining good control of his glutes. It is crucial to reduce any type of injury and reinforce motor control. C) Using the Lower Extremity Functional Scale (LEFS), I would ask Tom to score on a scale of 0 to 4, with 0 denoting "extreme difficulty" and 4 denoting "no difficulty", when performing functional tasks like walking, squatting, and jogging The LEFS would provide a baseline for monitoring Tom's improvement over time and information about his perceived functional limitations and how they affect his daily activities. D) The three components of motivation I would use to improve my sessions with Tom would be focusing on autonomy, competence, and relatedness. Autonomy: I would encourage Tom to have a say in his workout plan. For example, I could ask him which exercises he likes and which he finds difficult, and then modify our workouts accordingly. In a hypothetical scenario where Tom is feeling overwhelmed with his exercise routine, I would ask him what modifications or adjustments he thinks would be helpful and allow him to take ownership of his exercise plan. Competence: I would provide Tom with encouraging feedback as he completes his routine. Along the process, I would also encourage him and establish attainable goals. In the situation where Tom is feeling disappointed by a lack of development, I would recommend setting more manageable objectives until he reaches his ultimate goal. Small victories have a compound effect in the long term. Relatedness: I would build a welcoming setting that encourages a feeling of belonging and community. Additionally, I would actively listen to Tom's worries and offer support when necessary. In a situation where Tom is feeling alone or distant, I would urge him to go to group fitness classes or any group activities to meet people who have similar interests. E) Exercise: Dumbbell Row with One Arm Standing with your feet shoulder-width apart, keep your spine neutral, and hinge forward from your hips. One hand should be holding a dumbbell with the palm facing the body. Movement: Pull the dumbbell towards the ribcage while maintaining the shoulder blade retracted and the elbow tight to the body. Return the dumbbell to the starting position by lowering it. Specified Muscles: Biceps, Rhomboids, Trapezius, and Latissimus Dorsi Brachii Joint Actions: Elbow flexion, scapular retraction, shoulder horizontal adduction, and shoulder horizontal extension. Joint posture: Scapula retracted and depressed, elbow in 90-degree flexion, shoulder in a neutral posture. Common mistakes: Rounded shoulders, lifting with momentum, significant elbow flare, and spine hyperextension. Progressions: Increasing the dumbbell's weight, performing the exercise on one leg only, or pausing at the top of the movement. Regressions: Lower the dumbbell's weight, carry out the exercise with two hands rather than just one, or substitute a resistance band for the dumbbell. Adjustments: When the client has rounded shoulders, cue the client to move their shoulder blade back and downward towards their spine to fix this. Elbow Flare: During a movement, the elbow may flare outward as a form of compensation. To remedy this, instruct the client to maintain a close-to-body position for their elbow throughout the activity. Hip Rotation: The spine twists as a result of the hip on the opposite side of the dumbbell rotating forward. To remedy this, instruct the client to maintain a forward-facing hip position and a tight core throughout the activity. F) Exercise: Reverse Lunge Starting Position: Stand with your feet hip-width apart, tighten your abdominal muscles, and take a single, backward stride, landing on the ball of your foot. Bend both knees while bringing the rear knee closer to the ground. Keep your torso upright and your front knee over your ankle. The front foot must be pushed through to stand up again. Target Muscles: Hamstrings, quadriceps, glutes, and core Joint Actions: Knee, hip, and ankle dorsiflexion Joint Position: Dorsiflexed ankle, 90-degree flexed hip, and 90-degree flexed knee Common mistakes: Knee valgus (knock knees), a forward torso lean, and excessive low back arching. Correct Compensations: To prevent knee valgus, cue the client to keep their knee in line with their second toe. Instruct the client to resist a forward lean by keeping their chest up and their core tight. Encourage the client to keep their spine neutral to avoid overarching their lower back. G) Having high proximal stability (core, hips, and shoulders) allows for improved control and movement of the distal joints (knees, ankles, and elbows), according to the link between proximal stability and distal mobility. Poor proximal stability can cause compensations in the distal joints, which can result in injury or poor performance. I would employ hamstring activation exercises that also emphasize hip stability to promote Tom's mobility without utilizing hamstring stretches. These activities could involve: Single-Leg Glute Bridge: This exercise works the glutes, the core, and the hamstrings. Lay on your back with your knees bent and your feet flat on the ground to begin the workout. Push through the heel of the other foot to raise your hips off the floor while raising one leg off the ground. Hold for a short while before lowering yourself back down. On the opposite side, repeat. An exercise that works the hamstrings and the core is the straight leg raise. Lie on your back with one leg straight and the other bent to begin the workout. Maintaining a straight knee, raise the straight leg off the ground and hold for a few seconds. Repeat on the other side, lowering yourself back down. H) Compensations during the modified Thomas Test can include excessive low back arching or elevating the opposing leg off the table. I would instruct Tom to engage his core and drive his low back into the table to stabilize his pelvis if his opposing leg was lifting off the table. Tom should contract his core and tuck his pelvis down towards the table to flatten his low back if he has an overly arched low back. When the opposing leg rises off the table during the modified Thomas test, this is one of the frequent compensations. This suggests that the tight hip flexors on that side are trying to make up for the stiff hip extensors. I would first advise Tom to actively contract his glutes on the opposing side while performing the test in order to address this compensation. As a result, the pelvis will be stabilized and the opposing leg will be kept from rising off the table. Then, I would have Tom practice hip extension exercises like the glute bridge or hip thrusts to improve hip extensor mobility. If the compensation during the modified Thomas test was that the knee of the tested leg lifted off the table, this would indicate weakness in the hip flexors or lack of core stability. To correct this compensation, I would cue Tom to engage his core muscles by pulling his belly button towards his spine and pressing his lower back into the table. Additionally, I would have Tom perform exercises to strengthen his hip flexors, such as the standing hip flexor march or lying leg lifts. Third part of exam. A) The Lower Extremity Functional Scale (LEFS), Is an assessment tool composed of 20 questions widely used to determin and mesure how well people do daily tasks. For clinicians, they can measure a patient’s initial function, ongoing progress and set functional objectives. It also helps helps identify functional impairment that are caused by one or both lower extremities. The columns of the scale are summed to produce the final score. The scoring cap is set at 80. interpreting the score The score decreases as impairment increases. The Upper Extremity Functional Index (UEFI) measures the functional impairment brought on by pain and upper limb dysfunction. The final UEFI score can have a value of 0 or 80. Scores closer to 0 denote severe limitation, while scores closer to 80 denote minimal to no restriction. B) The Upper Body Multi-Joint Movement Assessment and a Lower Body Multi-Joint Movement Assessment, is primarly used to examine a client's movement patterns while identifying all areas of constraint or asymmetry. Thus, we can pinpoint any mobility, stability, or motor control problems that the corrective exercise programme needs to address. C) Monday: ● Wall slides (3 sets of 10 reps) for shoulder mobility ● Half-kneeling pallof press (3 sets of 10 reps each side) for core stability ● Hamstring stretch (hold for 30 seconds each side) Tuesday: ● Scapular retractions (3 sets of 10 reps) for upper back strength ● Plank (3 sets of 30 seconds) for core stability ● Calf stretch (hold for 30 seconds each side) Wednesday: ● Rest Thursday: ● Shoulder internal rotation stretch (hold for 30 seconds each side) ● Clamshells (3 sets of 10 reps each side) for hip stability ● Quad stretch (hold for 30 seconds each side) Friday: ● Shoulder external rotation stretch (hold for 30 seconds each side) ● Bridging (3 sets of 10 reps) for glute strength ● Ankle mobility drill (10 reps each side) Saturday: ● Rest Sunday: ● Shoulder blade protraction/retraction (3 sets of 10 reps) for upper back strength ● Dead bug (3 sets of 10 reps) for core stability ● Hamstring stretch (hold for 30 seconds each side) D) The comprehensive analysis helped me identify the area of weakness of my client. After I determined the impairments, I create a corrective exercise program in order to help the client prevent injuries and promote proper movements. Its purpose, is to improve overall body function. I chose stretching exercises like shoulder internal rotation and wall slides focus on shoulder mobility, which may have been noted as a functional index deficit. Similar to this, core stability exercises like the plank and dead bug target this issue, which may have come up during the movement assessment.To target particular stiffness or limitation, workouts like hamstring stretches and ankle mobility drills are also included. Nutritionist: Question 1 Importance of goal setting: Having a goal-setting, allows the trainer and the client to focus on a positive outcome. It also increases motivation and satisfaction when achieving the desired goals. Without goals, the nutrition coach will have a hard time setting a timeline to attain the desired results. It prevents the client from feeling overwhelmed and gives clarity to decision-making. Various types of Goals nutrition coaches should be concerned with are: ● ● ● ● ● Eliminating processed foods Improve energy through dietary improvements Increasing their athletic performance by having a healthy diet Creating realistic goals Making a meal plan and sticking to it. The above-mentioned types of goals fall into having a Healthy body and mind. where it might be slightly complicated, is to determine your clients' nutritional level. For example, for a person that only wants to be fit and feel energetic during the day, will likely be easier to explain and create a program for that person than for someone that is an athlete and wants to improve his marathon. The seven steps involved in goal setting process are: 1. Thinking about the final results one wants to achieve: One has to decide whether it was that goal he wants to achieve. Next, whether the person is ready to devote time and energy to this? If the answer is NO, then there is no worth doing that. 2. Choosing SMART Goals: ● ● ● ● ● S-Specific M-Measurable A-Attainable R-Realistic T-Time-bound For instance, many people decide to reduce weight but don't specify how much or by when they want to achieve it. A particular objective, such as losing 20 pounds by the second week of May, specifies the precise amount of weight to shed as well as the deadline for accomplishing the goal. 3. Writing down goals: Writing down the goals on a paper is more realistic than keeping it only in mind. One can put personal goals written on paper and stick them on a mirror or near their computer screen. 4. Creating an action plan: The majority of people don't create an action plan to achieve their goals. A good action plan should have the overall goal one is trying to achieve and the steps necessary to reach the goal. According to Forbes, creating an action plan this way activates a different part of your brain and cements the goals in your mind. 5. Creating a timeline: It is a part of the action plan. It helps to visualize the roles, tasks, and milestones to achieve the goals. Once the goal is set, one must stick to it as efficiently as possible. 6. Taking action: After all of these are done, it's time to take action. 7. Re-evaluation and assess the progress: Keeping strong motivation and determination is important to achieve the goal Question 2 By definition, the glycemic index is simply based on the time carbohydrate food are broken down into glucose and sugar level in your blood after consuming a meal. Usually, the reference food is white bread or glucose. GI of foods is rated between 0 100. Foods with 0-55 values are considered to have low GI and 55-100 is very high GI. The carbohydrates that have a higher value of GI(>55) or above, are digested or break down quickly in the blood, hence they increase blood glucose levels. Example white bread. While carbohydrates with a lower value of GI break down or are digested slowly, hence they release glucose gradually in the blood. Example oats. Not all carbs raise blood glucose levels. Fructose has only GI value of 17. Nevertheless, thanks to the pancreas, it releases a hormone called insulin that regulates the glucose level in our blood steam. Fibres are a form of carbohydrate, but unlike carbs, they are neither digested nor broken down by the body. Blood sugar levels are kept under control by fibres. They lower the risk of many illnesses, particularly heart disease. Peas and beans are examples of legumes that are good providers of fibre. Question 3