Congenital Toxoplasmosis Case Study: Diagnosis & Impact
advertisement

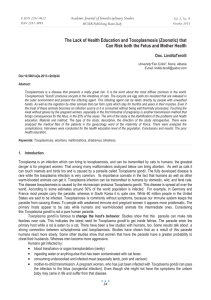
A Case Study on Congenital Toxoplasmosis In Partial Fulfillment of the Course Requirement in Medical Technology Enhancement Program (MEP 401) Submitted to: [Name of CEP Instructor] Submitted by: SHIENETTE GRACE CAMINADE KOBI CARL MANGOPOT KRIZA MAE NANTIN OCTOBER, 2021 CHAPTER 1 INTRODUCTION Toxoplasmosis is a disease resulting from infection with the parasite Toxoplasma gondii (T. gondii) a protozoan parasite that infects warm blooded animals, including humans. There are three major clinical manifestations of the disease, Ocular toxoplasmosis in immunocompetent individuals is one of the most frequently identified etiologies of uveitis, Toxoplasmic encephalitis in immunocompromised patients as observed in patients with hematologic malignancies, organ transplant recipients and lastly Congenital toxoplasmosis which is the main focus of this case study, due to the fact that the patient is pregnant and infected with toxoplasmosis, the congenital manifestation such as stated, results from the acquisition of infection during pregnancy and vertical transmission that may lead to a variety of complications, T. gondii infection during pregnancy can have devastating consequences in the fetus ranging from stillbirth which is the worst scenario that could occur if a pregnant woman is infected with toxoplasmosis, hydrocephalus, and ocular damage that could lead to blindness of the child when born. Some of the infected newborns present with minor symptoms of the infection only, but are still at risk of developing ocular lesion at any time due to the infection vertically transmitted from their mother. Congenital toxoplasmosis is a neglected infection, due to the fact that the mother is often asymptomatic with the infection of toxoplasmosis, the infection being asymptomatic for the pregnant mother is very alarming, countless amounts of vertical transmissions from mother to fetus has occurred, due to the unnoticed infection of toxoplasmosis, this issue must be studied well in order to come up with a better way in early detection of the infection to be able to avoid complications during pregnancy, although the symptoms may not be that severe for a pregnant mother that acquired the infection. As infected pregnant women are usually asymptomatic, the diagnosis relies only on serological tests. Maternal infection by Toxoplasma gondii during pregnancy may have serious consequences for the fetus, ranging from miscarriage, central nervous system involvement, retinochoroiditis. CHAPTER 2 PATIENT DATA A 28 year old woman named Krizza Batumbakal is 6 months pregnant with her 2nd baby, and she states that she is generally feeling unwell, has a headache, fever and swollen lymph nodes, she also states that she has been experiencing unusual muscle aches in her legs and arms. MEDICAL HISTORY Mrs. Batumbakal did not feel those symptoms way back her 1st pregnancy aside from the muscle aches that she experiences in her legs caused by the abrupt increase in weight due to pregnancy, she also stated that she has not been diagnosed with any disease before that could lead to the acquisition of the symptoms she stated, due to this unusual phenomenon she underwent a checkup to be able to assess the situation especially due to the fact that she is pregnant, this is a good measure in order to keep both her and the baby safe from complications during pregnancy. LABORATORY TESTS/RESULTS The following tests were done to the patient in order to assess the situation, a CBC was first done to check for the overall condition of the patient, and assess the cause of the symptoms that arose during her pregnancy. An ultrasound and fetal monitoring test was done to assess the condition of the baby inside the womb of the patient, a serologic test was done in order to assess the presence of a parasitic infection that correlates to the symptoms, the patient has a result of IgG antibody greater than 8.79 IU/mL which is considered positive for infection. Due to the detection of an existing infection which is suspected to be toxoplasmosis and also based on the symptoms of the patient, the physician requested the collection of CSF from the patient to confirm the type of infection. After the collection, it is then stained using immunofluorescence staining technique and viewed under the microscope, which confirmed the presence of Toxoplasma gondii infection. A Toxoplasma-positive reaction, stained by immunofluorescence CHAPTER 3 DEFINITION OF THE CASE ANATOMY & PHYSIOLOGY Muscle is one of the organ affected in this case study. Muscles of the human body that operate with the skeletal system, are controlled by the mind, and are involved with movement, posture, and balance. Striated muscle (or skeletal muscle), smooth muscle, and cardiac muscle are the three types of muscle. Smooth muscle is present in the walls of blood arteries, as well as organs like the urine bladder, intestines, and stomach, and is controlled in an involuntary manner. Cardiac muscle makes up the heart's bulk and is responsible for the essential pumping organ's regular contractions; it too is under involuntary control. Lymph nodes are located at the intersection of major blood vessels in the neck, axilla, thorax, abdomen, and groin. An adult has about 800 lymph nodes. In the body, lymph nodes are tiny structures that act as filters for foreign substances such as cancer cells and infection. The lymph nodes contain immune cells that may aid in the battle against infection by fighting and eliminating bacteria that have been brought in via the lymphatic system. PATHOPHYSIOLOGY Congenital toxoplasmosis is generally asymptomatic. Toxoplasmosis is more common in immunocompromised people with abnormalities in T-cell–mediated immunity, such as those with hematologic malignancies, bone marrow and solid organ transplants, or acquired immunodeficiency syndrome (AIDS). T gondii infection, whether primary or chronic (latent), is usually asymptomatic in immunocompetent people. A tiny proportion of these individuals develop retinochoroiditis, lymphadenitis, or, in rare cases, myocarditis and polymyositis. At birth, infected newborns exhibit anemia, thrombocytopenia, and jaundice. Mental retardation, convulsions, visual abnormalities, spasticity, hearing loss, and other serious neurologic sequelae may occur in affected survivors. CHAPTER 4 LABORATORY RESULTS TEST RESULT NORMAL INTERPRETATION RATIONALE VALUE CBC 1. WBC count 1. 2. Hemoglobin 3. Hematocrit 4. Platelet Count 2. 13 × 10^9 1. 5.8-13.2x /L 10^9/L 5 g/L 3. 30.5 4. 95 × 10^9 /L 2. 11.3- 1. NORMAL 2. DECREASED often indicates that the patient's body is fighting itself 3. DECREASED 14.8g/dL 4. DECREASED 3. 34.7-44.5 - A high white blood cell count against an infection disease and is or stressed. However, it is typical to have 4. 150-450 a high white blood cell count 10^9/μL during pregnancy. After all, the patient's body is already going through significant stress as result a of pregnancy. A high white blood cell count on its own is no cause for alarm. Headache, Fever, swollen lymphnodes are due to the high level of white blood cells. - It is typical for the hematocrit and hemoglobin concentrations to decrease during the first trimester of pregnancy, since the plasma volume grows faster than the red cell mass. The patient's iron intake should be twice that of nonpregnant women. Her body need this iron to produce more blood in order to provide oxygen to her baby. - At the beginning of the first trimester, the platelet count of all women decreases throughout pregnancy. Also, protozoal infections like T. gondii thrombocytopenia, cause or low platelet count. Ultrasound and A thorough ultrasound Fetal examination should be done Monitoring Test to rule out conditions including hydrocephaly, microcephaly, and intracranial calcifications.When instances of acute infection in pregnancy are discovered, it is important to act quickly. Treatments may be carried out to decrease the chance of fetal complications. When there are changes in the ultrasound examination, the procedure is followed by an assessment of the patient. Treatment with amniotic fluid is indicated. Serologic Test ELISA IgG antibody 0-3 IU/ml INCREASED A positive IgG test indicates greater than that the mother has been 8.79 IU/mL infected in the past or is currently infected. As shown in the table, it has an increased IgG antibody which is higher than the normal value. IgG testing must be repeated every 4 to 6 weeks until the antibody completely disappears. Indirect serological techniques, such as IgG and IgM antibody detection, are often employed in immunocompromised patients and pregnant women. The body produces IgG antibodies many weeks after infection and provides long-term protection. Immunoglobulin G levels increase during active infection and subsequently stabilize when the Toxoplasma infection ends and the parasite goes dormant. After being exposed to T. gondii, a person will have some measurable amount of IgG antibody in their blood for the rest of their life and will be immune (protected) from re-infection. CSF POSITIVE a cerebrospinal fluid (CSF) FOR sample is collected from the TOXOPLASM lower back from a pregnant OSIS woman using amniocentesis. INFECTION CSF will be stained using an immunofluorescence staining technique to confirm what type of infection it is. CHAPTER 5 SUMMARY A 28-year-old pregnant patient was found to have been infected with Toxoplasma gondii in her 6th month of pregnancy after the many laboratory tests that were done on her. The patient has presented symptoms such as muscle aches, headache, swelling of lymph nodes, and fever. The said parasite can be transmitted through fecal-oral route and any close-contact with cats and consumption of improperly prepared food can be two of the most possible reasons why a person can get infected with it. Moreover, the patient's health status was then assessed through the laboratory tests that were requested to perform on her. The diagnosis was confirmed through CSF testing in which a CSF sample was collected from the patient to determine the presence of the suspected parasite through immunofluorescence staining, , that eventually resulted to be positive for toxoplasmosis after the microscopic examination was done. CONCLUSION According to the information and results that were tackled above, the pregnant female patient had an ultrasound and fetal monitoring test and also underwent into many other tests including CBC, wherein her hemoglobin, hematocrit, and platelet count were decreased but her WBC count remained normal. The patient’s results in her serological test was found to have an increase in IgG antibody which gave a hint onto what type of infection is affecting the patient, and it was further confirmed that the infection was toxoplasmosis by staining a CSF sample collected from the patient, wherein Toxoplasma gondii was found under the microscope. In addition to that, the patient have also shown the same signs and symptoms of people with toxoplasmosis. In conclusion, Mrs. Krizza Batumbakal has a toxoplasmosis and it can be transmitted vertically which will eventually affect the health condition of the fetus. RECOMMENDATIONS The patient in this study is confirmed to be infected with Toxoplasma gondii and to prevent it from spreading in the patient’s placenta, it is recommended that she must take spiramycin, an antiparasitic drug used to treat toxoplasmosis. It is also advisable that she must undergo into an amniocentesis to determine if her fetus is infected with the said parasite or not. If the vertical infection is confirmed, both the patient and her baby’s health should be monitored and must be treated with pyrimethamine, sulfadiazine, and folinic acid. Additionally, if the patient gets treated with toxoplasmosis, in order to prevent reinfection from happening again, the patient must not drink any untreated water and must always wear gloves whenever she is gardening and if she ever gets pregnant again, it is advisable to avoid changing cat litter or adopt any stray cats. With these being said, the chances of being infected by Toxoplasma gondii again, or any other parasites that can be transmitted through eating will be reduced. CHAPTER 6 BIBLIOGRAPHY REFERENCES McAuley J. B. 2014. Congenital Toxoplasmosis. Journal of the Pediatric Infectious Diseases Society, 3 Suppl 1 (Suppl 1), S30–S35. https://doi.org/10.1093/jpids/piu077 Dubey, J. P., Miller, N. L., and Frenkel, J. K. 1970. The Toxoplasma gondii oocyst from cat feces. The Journal of experimental medicine , 132 (4), 636–662. https://doi.org/10.1084/jem.132.4.636 Montoya J. G. 2018. Systematic screening and treatment of toxoplasmosis during pregnancy: is the glass half full or half empty?. American journal of obstetrics and gynecology, 219 (4), 315–319.https://doi.org/10.1016/j.ajog.2018.08.001 Dunn, D., Wallon, M., Peyron, F., Petersen, E., Peckham, C., and Gilbert, R. 1999. Mother-tochild transmission of toxoplasmosis: risk estimates for clinical counselling. Lancet (London, England), 353 (9167), 1829–1833.https://doi.org/10.1016/S0140-6736(98)08220-8 Daffos, F., Forestier, F., Capella-Pavlovsky, M., Thulliez, P., Aufrant, C., Valenti, D., and Cox, W.L. 1988. Prenatal management of 746 pregnancies at risk for congenital toxoplasmosis. The New England Journal of Medicine, 318(5), 271–275. https://doi.org/10.1056/NEJM198802043180502 Gay-Andrieu, F., Marty, P., Pialat, J., Sournies, G., Drier de Laforte, T. and Peyron, F. 2003. Fetal toxoplasmosis and negative amniocentesis: necessity of an ultrasound follow-up. Prenatal diagnosis, 23 (7), 558–560. https://doi.org/10.1002/pd.632 Olariu, T. R., Blackburn, B. G., Press, C., Talucod, J., Remington, J. S. and Montoya, J. G. 2019. Role of Toxoplasma IgA as Part of a Reference Panel for the Diagnosis of Acute Toxoplasmosis during Pregnancy. Journal of clinical microbiology, 57(2), e01357-18. https://doi.org/10.1128/JCM.01357-18 Rahbari, A. H., Keshavarz, H., Shojaee, S., Mohebali, M. and Rezaeian, M. 2012. IgG avidity ELISA test for diagnosis of acute toxoplasmosis in humans. The Korean journal of parasitology, 50(2), 99–102. https://doi.org/10.3347/kjp.2012.50.2.99 Kodym, P., Machala, L., Roh´acov´a, H., Sirock´a, B. and Mal´y, M. 2007. Evaluation of a commercial IgE ELISA in comparison with IgA and IgM ELISAs, IgG avidity assay and complement fixation for the diagnosis of acute toxoplasmosis. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases , 13 (1), 40–47. https://doi.org/10.1111/j.1469- 0691.2006.01564.x Olariu, T. R., Blackburn, B. G., Press, C., Talucod, J., Remington, J. S. and Montoya, J. G. 2019. Role of Toxoplasma IgA as Part of a Reference Panel for the Diagnosis of Acute Toxoplasmosis during Pregnancy. Journal of clinical microbiology, 57(2), e01357-18. https://doi.org/10.1128/JCM.01357-18