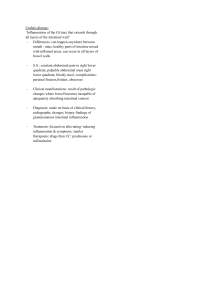
NCM 116: Care for Clients with Problem in Nutrients and Gastrointestinal Metabolism and Endocrine, Perception and Coordination Infection Chapter 1: Care for Clients with Nutritional Hemorrhage or burns Problem failure of protein synthesis, as in chronic Malnutrition according to WHO liver diseases Malnutrition, in all its forms, includes MARASMUS undernutrition (wasting, stunting, (Infantile Atrophy, energy-deficiency or underweight), inadequate vitamins or energy-protein deficiency; a protein-energy minerals, overweight, obesity, and resulting malnutrition diet-related noncommunicable diseases. 1.9 billion adults are overweight or obese, ETIOLOGY while 462 million are underweight. Inadequate caloric intake insufficiency of Around 45% of deaths among children diet, improper feeding habits under 5 years of age are linked to Metabolic abnormalities or congenital undernutrition. These mostly occur in lowmalformations and middle-income countries. At the same Severe impairment of any body system may time, in these same countries, rates of result in malnutrition childhood overweight and obesity are rising. The developmental, economic, social, and CLINICAL MANIFESTATION medical impacts of the global burden of Failure to gain weight followed by loss of malnutrition are serious and lasting, for weight until emaciation results. individuals and their families, for Loss of turgor in skin which becomes communities and for countries. wrinkled and loose as subcutaneous fat MALNUTRITION disappears from a worldwide perspective, is one of the Edema leading causes of morbidity and mortality in Low temperature and slow pulse childhood due to: Reduced basal metabolic rate 1. improper and / or inadequate food intake Fretful or listless 2. inadequate absorption of food Causes Diminished appetite and constipation are: followed by the so-called starvation type of 1. poor dietary habits diarrhea, with frequent, small stools 2. food faddism containing mucus 3. diseases Skin wrinkled 4. deficient supply of food Subcutaneous fat, disappears from abdomen 5. metabolic abnormalities first, then extremities, and finally face 6. emotional factors KWASHIORKOR a clinical syndrome resulted from a severe PROTEIN MALNUTRITION deficiency of protein inadequate caloric (PCM or PEM, Protein-Calorie (Energy) intake Malnutrition, Kwashiorkor) The most serious and prevalent form in ETIOLOGY industrially underdeveloped areas deficient intake of protein of good biologic Deposed child may become evident from value early infancy to 5 year of age, usually after weaning Impaired absorption of protein, as in chronic height and weight are accelerated with diarrheal states treatment but never equal those of abnormal losses of protein in proteinuria consistently well-nourished children. CLINICAL MANIFESTATION Early clinical evidence----vague, including lethargy, apathy, and irritability Inadequate growth, lack of stamina, loss of muscular tissue, increased susceptibility to infections, and edema Dermatitis and dyspigmentation Secondary immunodeficiency Anorexia, flabbiness of subcutaneous tissues, and loss of muscle tone LABORATORY DATA Concentration of serum albumin decreased Aminoaciduria Ketonuria in the early stage Low blood glucose values Potassium and magnesium deficiencies Amylase, esterase, transaminase, lipase, alkaline phosphatase, pancreatic enzymes decreased normocytic, microcytic, or macrocytic Anemia Bone growth delayed PREVENTION Diet containing an adequate quantity of protein of good biologic quality Adequate dietary instruction and food distribution Treatment of diseases: o Immediate management of any acute problems such as those of severe diarrhea, renal failure, and shock and, ultimately, the replacement of missing nutrients is essential. TREATMENT AND MANAGEMENT FOR DEHYDRATION For mild to moderate dehydration, feedings are administered orally or by nasogastric tube, when culturally appropriate, to prevent aspiration. A breasted infant should be nursed as often as he or she wants. For severe dehydration, intravenous (IV) fluids are necessary MILK: When dehydration is corrected, oral or nasogastric feeding starts with small, frequent feeds of dilute milk (66 kcal and 1.0g protein/100 ml at 120/ml/kg/24 hour) with nutrient supplementation. ANTIBIOTICS: o The routine administration of antibiotics such as Cotrimoxazolehas also been advocated. o Other antimicrobials are used only to treat overt infection because of concerns about emergence of microbial resistance. VITAMINS AND MINERALS: o Vitamins and minerals, especially vitamin A, potassium, and magnesium, are necessary from the outset of treatment. o Iron and folic acid usually correct the anemia. NUTRITIONAL ANEMIAS Deficiency of: Iron, Folate, B12, Protein corrected by supplementation Iron Deficiency Anemia (IDA) Iron deficiency (ID) is one of the most frequent, nutrition deficiency all round the world. Its prevalence is higher in children and childbearing age women. Iron deficiency anemia (IDA) o mainly affects child behavior and development, work performance and immunity. CAUSES OF IRON DEFICIENCY ANEMIA Diminished stores-Preterm small for date babies, Twins, Early cord clamping (100ml of blood) Diminished intake-Not breast feeding, Cows milk feeding, Iron poor diet Diminished absorption-Malabsorption, Low level of enhancers, High level of inhibitors Increased demands-Rapid catch up growth in preterm and SFD, Infancy puberty, Pregnancy and Lactation. Defective metabolism-Idiopathic pulmonary Hemosiderosis, Sideroblastic anemia, Congenital transferrin deficiency CLINICAL FEAUTURES Pallor, pica, dull, irritable, poor appetite Failure to thrive, easily fatigued Frequent infections Splenomegaly Tongue papillae are atrophied Malabsorption and protein losing enteropathy Nails-flat, thin, brittle, spoon shaped (koilonychia) Decreased attention span, poor school performance, cognitive impairment Severe cardiomegaly, Congestive Heart Failure (CCF) Assessment of Iron-Deficiency Anemia: Clinical and Laboratory indices. Laboratory indices - are the most common methods used to assess iron nutrition status. Having low hemoglobin, low hematocrit HYPOCHROMIC MICROCYTIC ANEMIA The most common cause for a hypochromic microcytic anemia is iron deficiency. The most common nutritional deficiency is lack of dietary iron. Thus, iron deficiency anemia is common. Persons most at risk are children and women in reproductive years (from menstrual blood loss and from pregnancy. Clinical Indices: o Pallor of the conjunctiva, tongue, nail bed and palm TREATMENT OF IRON DEFICIENCY ANEMIA Treat underlying cause: Oral iron therapy 3-6mg/kg in 3 divided doses (Hb rises by 0.4g/day) Vit C, empty stomach or in between meals for 6-8 weeks after Hb is normal: Parental iron therapy Blood transfusion rarely when severe infection with poor iron utilization PREVENTION FOR IRON DEFICIENCY ANEMIA Dietary modification Breast feeding and appropriate weaning diet Iron rich food Increase ascorbic acid Food fortification Iron supplementation Deworming MEGALOBLASTIC ANEMIA Also known as Vitamin B-12/Folate Deficiency Anemia, Macrocytic Anemia, or Megaloblastic Anemia Caused when RBC’s aren’t produced properly Due to: Drinking goats milk- is poor source Cooking- destroys folic acid Chronic diarrhea, malabsorption and recurrent infections -are prone In hemolytic anemias- due to increased erythropoiesis Treatment: phenytoin / antimetabolites CLINICAL FEAUTURES Pale Very sick Irritable Severe anorexia Failure to thrive Knuckle pigmentation (hands and nose) Tremor and developmental regression TREATMENT Can be treated with oral or intravenous folic acid supplements. Dietary changes also help boost folate levels. NUTRITIONAL MANAGEMENT AND PARENTERAL NUTRITION It is an intravenous administration of nutrition, which may include protein, carbohydrate, fat, minerals, and electrolytes, vitamins, and other trace elements for patients who cannot eat or absorb enough food through tube feeding formula or by mouth to maintain good nutrition status. NURSING DIAGNOSIS Imbalanced nutrition: less than body requirements related to inability to ingest food due to physiologic and/or psychologic factors as evidenced by body weight 20% or more below ideal weight range, pale conjunctivae and mucous membranes, poor muscle tone Risk for aspiration related to gastrointestinal tubes and tube feedings Risk for deficient fluid volume related to diarrhea and/or inadequate water intake Chapter 2: Care for clients with Gastrointestinal Problems ANATOMY OF GASTROINTESTINAL TRACT The GI tract is a 23- to 26-foot-long pathway that extends from the mouth through the esophagus, stomach, and intestines to the anus. The esophagus is located in the mediastinum in the thoracic cavity, anterior to the spine and posterior to the trachea and heart. The stomach is situated in the upper portion of the abdomen to the left of the midline, just under the left diaphragm. It is a distensible pouch with a capacity of approximately 1500 mL. The small intestine is the longest segment of the GI tract, accounting for about two thirds of the total length. It folds back and forth on itself, providing approximately 7000 cm of surface area for secretion and absorption, the process by which nutrients enter the bloodstream through the intestinal walls. The large intestine consists of an ascending segment on the right side of the abdomen. The terminal portion of the large intestine consists of two parts: the sigmoid colon and the rectum. The rectum is continuous with the anus. FUNCTION OF THE DIGESTIVE SYSTEM The primary digestive functions of the GI tract are the following: To break down food particles into the molecular form for digestion. To absorb into the bloodstream the small molecules produced by digestion To eliminate undigested and unabsorbed food stuffs and other waste products from the body Health History and Clinical Manifestations: Pain- can be a major symptom of GI disease. Indigestion- most common symptom of patients with GI dysfunction Intestinal Gas-accumulation of gas in the GI tract Nausea and Vomiting-another major symptom of GI disease Change in Bowel Characteristics Habits and Stool PHYSICAL ASSESSMENT The physical examination includes assessment of the mouth, abdomen, and rectum. The mouth, tongue, buccal mucosa, teeth, and gums are inspected, and ulcers, nodules, swelling, discoloration, and inflammation are noted. People with dentures should remove them during this part of the examination to allow good visualization. DIAGNOSTIC EVALUATION Stool tests Breath tests Abdominal Ultrasonography DNA Testing Imaging Studies-Upper and Lower Gastrointestinal Tract Study (X-ray with barium), Computed Tomography, Magnetic Resonance Imaging, Gastrointestinal Motility Studies (Radionuclide testing also is used to assess gastric emptying and colonic transit time), endoscopic procedures, gastric analysis, gastric acid stimulation test, and pH monitoring, laparoscopy (peritoneoscopy) DIFFERENT DISORDERS FOR TEETH, JAW AND SALIVARY GLANDS Dentoalveolar Abscess or Periapical Abscess o abscessed tooth, involves the collection of pus Malocclusion o misalignment of the teeth Dental plaque and caries o Tooth decay PAROTITIS o Inflammation of the parotid gland Sialadenitis inflammation of the salivary glands Salivary Calculus (Sialolithiasis) o stones, usually occurs in the submandibular gland Neoplasms tumors or growths Cancer of the Oral Cavity associated with the use of alcohol and tobacco. Predisposing factors ingestion of alcohol, dietary deficiency, and ingestion of smoked meats. PATHOPHYSIOLOGY Malignancies of the oral cavity are usually squamous cell cancers. Any area of the oropharynx can be a site for malignant growths, but the lips, the lateral aspects of the tongue, and the floor of the mouth are most commonly affected CLINICAL MANIFESTATION Many oral cancers produce few or no symptoms in the early stages. Later, the most frequent symptom is a painless sore or mass that will not heal. A typical lesion in oral cancer is a painless indurated (hardened) ulcer with raised edges. Tissue from any ulcer of the oral cavity that does not heal in 2 weeks should be examined through biopsy. As the cancer progresses, the patient may complain of tenderness; difficulty in chewing, swallowing, or speaking; coughing of bloodtinged sputum; or enlarged cervical lymph nodes. MEDICAL MANAGEMENT Management varies with the nature of the lesion, the preference of the physician, and patient choice. Surgical resection, radiation therapy, chemotherapy, or a combination of these therapies may be effective. NURSING MANAGEMENT The nurse assesses the patient’s nutritional status preoperatively, and a dietary consultation may be necessary. The patient may require enteral (through the intestine) or parenteral (intravenous) feedings before and after surgery to maintain adequate nutrition. Promoting Mouth Care Ensuring Adequate Food and Fluid Intake Supporting A Positive Self-Image Minimizing Pain and Discomfort Promoting Effective Communication Preventing Infection Promoting Home and Community-Based Care Teaching Patients Self-Care, Continuing Care The patient should be instructed to eat slowly and to drink fluids with meals. As a temporary measure, calcium channel blockers and nitrates have been used to decrease esophageal pressure and improve swallowing. Achalasia may be treated surgically esophagomyotomy. The procedure usually is performed laparoscopically. DISORDERS OF THE ESOPHAGUS DYSPHAGIA- (difficulty swallowing) is the most common symptom of esophageal disease. ACHALASIA-absent or ineffective peristalsis of the distal esophagus, accompanied by failure of the esophageal sphincter to relax in response to swallowing. HIATAL HERNIA In a condition known as hiatus (or hiatal) hernia, the opening in the diaphragm through which the esophagus passes become enlarged, and part of the upper stomach tends to move up into the lower portion of the thorax. Hiatal hernia occurs more often in women than men. There are two types of hiatal hernias: sliding and paraoesophageal. CLINICAL MANIFESTATION The primary symptom of achalasia is difficulty in swallowing both liquids and solids. The patient has a sensation of food sticking in the lower portion of the esophagus. As the condition progresses, food is commonly regurgitated, either spontaneously or intentionally by the patient to relieve the discomfort produced by prolonged distention of the esophagus by food that will not pass into the stomach. The patient may also complain of chest pain and heartburn (pyrosis). Pain may or may not be associated with eating. There may be secondary pulmonary complications from aspiration of gastric contents. ASSESSMENT AND DIAGNOSTIC FINDINGS X-ray studies show esophageal dilation above the narrowing at the gastroesophageal junction. Barium swallow, computed tomography (CT) of the esophagus, and endoscopy may be used for diagnosis; however, the diagnosis is confirmed by manometry, a process in which the esophageal pressure is measured by a radiologist or gastroenterologist. MANAGEMENT CLINICAL MANIFESTATION Heartburn, regurgitation, and dysphagia, but at least 50% of patients are asymptomatic. Sliding hiatal hernia is often implicated in reflux. The patient with a paraoesophageal hernia usually feels a sense of fullness after eating or may be asymptomatic. The complications of hemorrhage, obstruction, and strangulation can occur with any type of hernia. Assessment and Diagnostic Findings: Diagnosis is confirmed by x-ray studies, barium swallow, and fluoroscopy. MANAGEMENT Frequent, small feedings that can pass easily through the esophagus. The patient is advised not to recline for 1 hour after eating, to prevent reflux or movement of the hernia, and to elevate the head of the bed to prevent the hernia from sliding upward. Surgery is indicated in about 15% of patients. Medical and surgical management: surgery to correct torsion (twisting) of the stomach or other body organ that leads to restriction of blood flow to that area. DIVERTICULUM A diverticulum is an outpouching of mucosa and submucosa that protrudes through a weak portion of the musculature. The most common type of diverticulum is Zenker’s diverticulum (also known as pharyngoesophageal pulsion diverticulum or a pharyngeal pouch). DIVERTICULITIS Common development with advancing years, associated with diets low in fiber Diverticulitis Is Inflammation of Diverticula Signs and symptoms: Fever, anorexia, nausea, lower left sided pain, bright-red rectal bleeding Complications: Hypovolemic shock, Sepsis The most common type of diverticulum is Zenker’s diverticulum (also known as pharyngoesophageal pulsion diverticulum or a pharyngeal pouch). CLINICAL MANIFESTATION Symptoms experienced by the patient with a pharyngoesophageal pulsion diverticulum include difficulty swallowing, fullness in the neck, belching, regurgitation of undigested food, and gurgling noises after eating. Dysphagia is the most common complaint of patients. Assessment and Diagnostic Findings: Barium Swallow, Esophagoscopy MANAGEMENT Because pharyngoesophageal pulsion diverticulum is progressive, the only means of cure is surgical removal of the diverticulum. Postoperatively, the patient may have a nasogastric tube inserted at the time of surgery. PERFORATION Perforation may result from stab or bullet wounds of the neck or chest, trauma from motor vehicle crash, caustic injury from a chemical burn or inadvertent puncture by a surgical instrument during examination or dilation. CLINICAL MANIFESTATIONS The patient has persistent pain followed by dysphagia. Infection, fever, leukocytosis, and severe hypotension may be noted. Pneumothorax are observed. GASTROINTESTINAL REFLUX DISEASE Gastroesophageal reflux (back-flow of gastric or duodenal contents into the esophagus) CLINICAL MANIFESTATIONS pyrosis (burning sensation in the esophagus), dyspepsia (indigestion), regurgitation, dysphagia or odynophagia (difficulty swallowing, pain on swallowing), hypersalivation, and esophagitis. ASSESSMENT AND DIAGNOSTIC FINDINGS endoscopy or barium swallow to evaluate damage to the esophageal mucosa MANAGEMENT The patient is instructed to eat a low-fat diet; Avoid caffeine, tobacco, beer, milk, foods containing peppermint or spearmint, and carbonated beverages; Avoid eating or drinking 2 hours before bedtime Elevate the head of the bed on 6- to 8-inch (15- to 20-cm) blocks Elevate the upper body on pillows If reflux persists, the patient may be given medications such as antacids or histamine receptor blockers CELIAC DISEASE Celiac disease is a digestive disorder caused by an abnormal immune reaction to gluten. Celiac disease is also known as:sprue, nontropical sprue, gluten-sensitive enteropathy Gluten is a protein found in foods made with wheat, barley,rye,oats,triticale and other grains. Some people with gluten intolerance have a mild sensitivity to gluten, while others have celiac disease which is an autoimmune disorder. SIGNS AND SYMPTOMS weight loss vomiting abdominal bloating abdominal pain persistent diarrhea or constipation pale, fatty, foul-smelling stooL COMMON BLOOD TEST complete blood count (CBC) liver function tests cholesterol test alkaline phosphatase level test Serum albumin test CLINICAL MANAGEMENT Eat only gluten-free products Risk Factors for Digestive and Gastrointestinal System Disease (Usually Self-Induced) Excessive alcohol consumption Excessive smoking Increased stress Ingestion of caustic substances Poor bowel habits Pain is the hallmark of acute abdominal problems o Visceral, Somatic, or Referred pain VISCERAL PAIN Caused by inflammation, distention (inflation of the organ), or ischemia (inadequate blood flow) Pain vague, dull, or crampy Is generally diffuse and difficult to localize Examples (most often hollow organs) o gallbladder (cholecystitis) o appendix (appendicitis) Presentation (from sympathetic stimulation) o nausea and vomiting o diaphoresis o tachycardia SOMATIC PAIN Produced by bacterial or chemical irritation of nerve fibers in the peritoneum (peritonitis) Is usually constant and localized to a specific area Often described as sharp or stabbing Examples o ruptured appendix o perforated ulcer o inflamed pancreas o Peritonitis can lead to sepsis death Presentation o Patient often hesitant to move o Lies on their back or side with legs flexed to prevent additional pain from stimulation of the peritoneal area o Often exhibits involuntary guarding of the abdomen o Rebound tenderness often noted during the physical examination REFFERED PAIN Pain in a part of the body considerably removed from the tissues that cause the pain Results from neural pathways from various organs passing thru or over a region where the organ was initially formed in the fetal stage Examples o Diaphragm injury- refers pain to neck or shoulders o Appendicitisrefers pain to periumbilical area o Gallbladder disorder- refers pain to right shoulder DISEASE ENTITIES Upper GI Disease o Gastroenteritis o Gastritis o Peptic ulcer disease Lower GI Disease o Colitis o Crohn’s disease o Diverticulitis o Bowel obstruction Other Organ Disease o Appendicitis o Cholecystitis o Pancreatitis o Acute hepatitis GASTROENTERITIS Inflammation of the stomach and intestines that accompanies numerous GI disorders Causes o bacteria or viral infections, chemical toxins, and other conditions Signs and symptoms o anorexia (loss of appetite), o nausea, o vomiting, o abdominal pain Management: o emergency management, o supportive therapy GASTRITIS An acute or chronic inflammation of the gastric mucosa Causes: o hyperacidity o alcohol or drug ingestion o infection Signs and symptoms o epigastric pain o nausea and vomiting o bleeding PEPTIC ULCER DISEASE Erosions in the GI tract from gastric acid Duodenal ulcers o most frequently in proximal duodenum o most common 25-50 years old in those under stress o pain at night when the stomach is empty Gastric ulcers o in the stomach o more common over 50 years of age in jobs requiring physical activity o usually no pain at night pain on full stomach Causes of peptic ulcer disease o H. pylori infection (treated with antibiotics) o Non-steroidal anti-inflammatory drug use o aspirin, Motrin, Advil o Acid stimulating products like alcohol, nicotine o Acid secreting tumor (ZollingerEllison syndrome) o * Zollinger-Ellison syndrome - is a rare condition in which one or more tumors form in the pancreas or upper part of the small intestine. This tumor is called gastrinomas. COLITIS An inflammatory condition of the large intestine characterized by severe diarrhea and ulceration of the mucosa of the intestine (ulcerative colitis) Incidence - most often 20-40-year old Cause is unknown Signs and symptoms o Nausea, vomiting, weight loss o Significant pain o cramping colicky o Grossly bloody stools or stool containing mucus CROHNS DISEASE A chronic, inflammatory bowel disease thought to be of autoimmune etiology, usually affecting the ileum, the colon, or both structures Exact cause unknown Most prevalent in white females, those under stress, and in the Jewish population The diseased segments associated with Crohns disease may be separated by normal bowel segments or skip areas Formation of fistulas from the diseased bowel to the anus, vagina, skin surface, or to other loops of bowel are common BOWEL OBSTRUCTION A partial or complete blockage of the large or small intestines Causes: o Adhesions o Hernias o fecal impaction o polyps o tumors Signs and symptoms – o decreased appetite, o nausea and vomiting o diffuse abdominal pain o constipation, and o abdominal distention Bowel obstruction, if untreated can lead to death APPENDICITIS A common abdominal emergency that occurs when the opening between the lumen of the appendix and the cecum is obstructed by fecal material or from inflammation from viral or bacterial infection Signs and symptoms: o early abdominal pain is diffuse o colicky o in periumbilical area (later RLQ), abdominal tenderness guarding o nausea o vomiting, chills o low-grade fever o anorexia If ruptured, increased risk of inflammation of peritoneum (Peritonitis) PERITONITIS It is inflammation of the peritoneum, the serous membrane lining the abdominal cavity and covering the viscera. Usually, it is a result of bacterial infection the organisms come from diseases of the GI tract or, in women, from the internal reproductive organs Peritonitis can also result from external sources such as injury or trauma (eg, gunshot wound, stab wound) or an inflammation that extends from an organ outside the peritoneal area, such as the kidney. The most common bacteria implicated are Escherichia coli, Klebsiella, Proteus, and Pseudomonas, Other common causes of peritonitis are appendicitis, perforated ulcer, diverticulitis, and bowel perforation. Peritonitis may also be associated with abdominal surgical procedures and peritoneal dialysis. Clinical Manifestations o At first, a diffuse type of pain is felt. The pain tends to become constant, localized, and more intense near the site of the inflammation. Movement usually aggravates it. The affected area of the abdomen becomes extremely tender and distended, and the muscles become rigid. Rebound tenderness and paralytic ileus may be present. Usually, nausea and vomiting occur and peristalsis is diminished, temperature and pulse rate increase, and elevation of the leukocyte count. Management: o Fluid, colloid, and electrolyte replacement (isotonic solution), o Analgesics, o Antiemetics, o Surgical treatment is directed toward excision (ie, appendix), resection with or without anastomosis (surgical connection between two structures) CHOLECYSTITIS Inflammation of the gallbladder, most often associated with the presence of gallstones Incidence: -more common in women 30-50 years old Signs symptoms o pain, often colicky, o in RUQ with referral to right shoulder o pain often after high fat content meal o nausea, vomiting common o pale, cool, clammy skin (sympathetic response) o giving Morphine may increase spasms PANCREATITIS Inflammation of the pancreas Alcoholism causes 80 of cases in the USA Signs and symptoms o severe abdominal pain o localized to LUQ or referred to back or epigastric area o nausea and uncontrolled vomiting retching o abdominal tenderness and distention o fever, o tachycardia, o diaphoresis o sepsis shock possible ACUTE HEPATITIS Inflammation of the liver Signs symptoms related to severity of disease o Associated with the sudden onset of malaise, weakness, anorexia, intermittent nausea and vomiting, and dull right upper quadrant pain or referral to right shoulder Usually followed within 1 week by the onset of jaundice of skin sclera, dark urine, claycolored stool RISK FACTORS OF HEPATITIS A Spread by fecal-oral route Health care practice without BSI (body substance isolation) or infection control precautions Household or sexual contact with an infected person Living in an area with HIV outbreak Traveling to developing countries Poor handwashing hygiene practice especially after toileting Disease often self-limiting, lasts 2-8 weeks, low mortality rate RISK FACTORS OF HEPATITIS B Serum hepatitis transmitted as blood born pathogen can stay active in body fluids outside body for days Health care practice without infection control precautions Infant born to Hepatitis B virus (HBV) infected mother Engaging in sex with infected partners and/or multiple partners Drug use by injection Patients receiving hemodialysis RISK FAVTOR OF HEPATITIS C Health care practice without infection control precautions Blood transfusion recipients Engaging in sex with infected partners and/or multiple partners Drug use by injection Patients receiving hemodialysis GASTRIC CANCER This type of cancer is more common among middle-aged males. Predisposing factors: o lifestyle related and history of cancer in the family Clinical manifestations: o progressive loss of appetite, o gastric fullness, o dyspepsia or indigestion, o hematemesis, o melena, o weight loss, o anemia, o fatigues Collaborative surgery: o Total gastrectomy, o Chemotherapy, o Radiation HIATAL HERNIA OR DIAPHRAGMATIC HERNIA Two types: o sliding hiatal hernia; o paraesophagealrolling hernia Sliding hiatal Hernia o protrusion of the esophagogastric junction into the thoracic cavity and back into abdominal cavity Paraesophageal Hernia o protrusion of the fundus of the stomach and the greater curvature into the stomach and esophagus. Clinical Manifestations: o heartburn, dysphagia, dyspnea, nausea and vomiting, gastric distention Collaborative Management o Medications: antacids to relieve heartburns, antiemetics to relieve nausea and vomiting Nursing Interventions: o Modify diet: high protein diet, small frequent feedings, avoid foods and beverages that can cause too much acidity,avoid evening snacks, promote lifestyle changes Management: o Surgery-Nissenfundoplicationor gastric wrap-around ASSESSING ABDOMINAL PAIN Onset - when did it begin? Provocation/palliation - what makes the pain worse/better? Quality - described in the patients own words Region/radiation - if the patient can use one finger the pain is localized if the patient rubs their hands over the general entire abdomen it is diffuse Severity - on a scale of 0-10 (0 being no pain and 10 being the worse) Time - how long has the pain been present? DIAGNOSTIC PROCEDURE RADIOLOGIC o The digestive tract can be outlined by x-rays by utilizing the administration of a contrast medium. The contrast medium is swallowed by the patient in order to visualize the upper GI tract. These procedures are referred to as “Barium Swallow," or “Small Bowel Follow-Through." To visualize the lower GI tract,the contrast medium is instilled rectally.This procedureis called a“Barium Enema." GASTRIC ANALYSIS o Examination of gastric contents and gastric juice provides information used in diagnosis. For example, the following may be determined: (1) The presence, amount, or absence of hydrochloric acid. (2) The presenceof cancercells. (3) The types and amounts of enzymes present. STOOL EXAM o Stool samples can be examined on the ward and in the laboratory to determine the presence of substances that aid in diagnosis. o For example: (1) On the ward, nursing personnel can determine the color, consistency, and amount of stool. The presence of unseen blood (occult) can be determined with a simple test. (2) In the laboratory,tests can be performed to determine the presence of fat, urobilinogen, ova, parasites,bacteria,and other substances. ENDOSCOPY o is a visual examination of the interior through the use of special instruments called endoscopes. In relation to the digestive system, the term endoscopy is used to describe visual examination of the inside of the GI tract. o There are many different types of endoscopes, each designed for a specific use. Generally, the scope consists of a hollow tube with a lighted lens system that permits multi-directional viewing. The scope has a power source and accessoriesthat permitboth biopsy and suction. BLOOD TESTS o There are many blood tests that can be used to assist in the identification and measurement of gastrointestinal disorders. Impaired glucose utilization may be detected by abnormal blood glucose levels. MANAGEMENT OF GASTROINTESTINAL PROBLEMS Majority of care is supportive and aimed at treating signs and symptoms presented Position of comfort with ability to protect airway in the case of vomiting Abdominal pain control - EMS needs to contact medical control for medication orders (Morphine 2mg IVP every 2 minutes, max 10 mg) IV to replace fluid loss (vomiting, diarrhea, internal hemorrhage) Shock (hypovolemic, septic) possible and then aggressive care required COLOSTOMY A colostomy is a surgically created, artificial opening (stoma) into the colon through the abdomen. It may be temporary or permanent. Fecal diversion is utilized in order to rest a portion of the colon following intestinal surgery, in preparation for further surgery, or in cases of severe inflammatory disease (such as Diverticulitis). . Chapter 3: Care for Clients with Anorectal Disorder Anorectal disorders are a group ofmedicaldisorders that occur at the junction of the anal canal and the rectum. Wide range of disorders of the rectum including diarrhea, hemorrhoids, abscesses, fistula, fissures,anal itching, warts and rectal prolapse. Anal Fistula An anal fistula is a small tunnel that develops between the end of the bowel and the skin near the anus (where poo leaves the body). They're usually the result of an infection near the anus causing a collection of pus (abscess) in the nearby tissue. When the pus drains away, it can leave a small channel behind. Anal fistulas can cause unpleasant symptoms, such as discomfort and skin irritation, and will not usually get better on their own. Surgery is recommended in most cases. Symptoms of Anal Fistula o skin irritation around the anus o a constant, throbbing pain that may be worse when you sit down, move around,poo or cough o smelly discharge from near your anus o passing pus or blood when you poo o swelling and redness around your anus ANAL FISSURES An anal fissureis a small tear in the thin, moist tissue (mucosa) that lines the anus. An anal fissuremay occur when you pass hard or large stools during a bowel movement.Anal fissures typically cause pain and bleeding with bowel movements. Common symptom: bleeding HEMORRHOIDS Hemorrhoids are swollen veins in your lower rectum. Internal hemorrhoids are usually painless, but tend to bleed. External hemorrhoids may cause pain. Hemorrhoids, also called piles, are swollen veins in your anus and lower rectum, similar to varicose veins. Hemorrhoids are one of the most common causes of rectal bleeding. Cinical manifestations: o pain, bleeding, itching, swelling Assessment: o Digital Exam, Visual inspection Management: o Hemmorrhoidectomy(if bleeding) PILONIDAL SINUS A pilonidal sinus (PNS) is a small hole or tunnel in the skin. It may fill with fluid or pus, causing the formation of a cyst or abscess. It occurs in the cleft at the top of the buttocks. A pilonidal cyst usually contains hair, dirt, and debris. It can cause severe pain and can often become infected. No exact cause but believed to be a combination of changing hormones (because it occurs after puberty), hair growth, and friction from clothes or from spending a long time sitting. The signs of an infection include: o pain when sitting or standing o swelling of the cyst o reddened, sore skin around the area o pus or blood draining from the abscess, causing a foul odor o hair protruding from the lesion o formation of more than one sinus tract, or holes in the skin TREATMENT AND MANAGEMENT For Anal Fistula: o Fistulotomy – a procedure that involves cutting open the whole length of the fistula so it heals into a flat scar; o Seton procedures – where a piece of surgical thread called a seton is placed in the fistula and left there for several weeks to help it heal before a further procedure is carried out to treat it For Anal Fissures: Laxatives, topical analgesics, Glyceryl trinitrate; Surgery: lateral sphincterotomy For Hemorrhoids: Over-the-counter creams, ointments, suppositories or pads, hydrocortisone and lidocaine, which can temporarily relieve pain and itching. Surgical procedure: External hemorrhoid thrombectomy For Pilonidal Sinus: broad-spectrum antibiotic, surgery using local anesthesia NURSING MANAGEMENT Relieving Constipation-adequate hydration and high fiber foods Reducing Anxiety-maintains patients’ privacy, individualizes plan of care Relieving Pain-provide comfort measures, hot sitz bath, warm compress, analgesics Promoting Urinary Elimination-encourage voluntary voiding, before resorting to catheterization if indicated Health Education