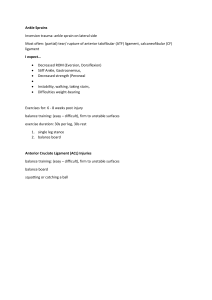
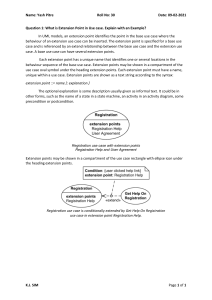
A 34 year-old male cyclist¹¹ came to the emergency room for severe leg pain¹. The patient fell from his bicycle and noticed a deformity on his right leg. He had difficulty in standing up² but decided to go home and rest. However, he noticed that the pain progressed³ and became worse compared to the immediate pain³ he felt after the accident, prompting him to go to the hospital. Physical Examination • Normal vital signs, except for heart rate of 110 beats per minute⁴, pain score of 8-9¹. • Severe pain on both passive and active dorsal and plantar flexion of right ankle⁵. • Noticed discoloration⁶, tense and shiny skin⁷, and anterior bulge of right leg⁸. • Weak right dorsalis pedis⁹. ● ● Xray showed proximal tibial fracture¹⁰ MRI showed fat suppressed T2-weighted images¹² through the anterior (4C) and lateral (4D) compartments confirm the findings ____________________________________ Classically, the presentation of acute compartment syndrome has been remembered by "The Five P's": ● pain, ● pulselessness, ● paresthesia, ● paralysis, and ● pallor ____________________________________ ¹A serious injury (proximal tibial fracture) can cause swelling or bleeding in a compartment. The fascia won’t expand to make room, so the swelling or bleeding puts pressure on the nerves and muscles ➛ compartmental pressure ➛ anterior bulge of right leg⁸ ____________________________________ ²diffuculty standing up; tibial fracture could have injured the deep fibula nerve nerve ● Deep fibula nerve innervates all 4 muscles of the anterior compartment, and so would affect their ability to perform respective actions. Muscles in the anterior compartment are: ● Tibialis anterior (dorsi flexor) ● Extensor digitorum longus (extends lateral 4 digits & dorsiflexes ankle) ● Extensor hallucis longus (extends great toe & dorsiflexes ankle) ● Peroneus tertius (dorsiflexes ankle & aids in eversion of foot) ____________________________________ ³Patients with compartment syndrome typically present with pain whose severity appears out of proportion to the injury If the pressure gets too high, the tissues can’t get enough blood, which contains oxygen and nutrients - ischemia ➛progressive pain The tissues can die (may lead to permanent damage to the area) earliest objective physical finding is the tense, or ''wood-like" feeling of the involved compartment. Pain is typically severe, out of proportion to the injury. Early on, pain may only be present with passive stretching. In the initial stages, pain may be characterized as a burning sensation or as a deep ache of the involved compartment. Paresthesia, hypoesthesia, or poorly localized deep muscular pain may also be present. ____________________________________ ⁴ elevated heart rate: hemodynamics are impaired - imbalance between venous outflow and arterial inflow ➛ hypo-perfusion. So heart works harder to compensate ____________________________________ ⁵ pain on passive & active dorsal & plantar flexion of right ankle: Tibialis anterior = ankle dorsi flexor Lack of oxygenated blood and accumulation of waste products result in pain and decreased peripheral sensation secondary to nerve irritation. Muscles of anterior compartment of leg: ● Tibialis anterior (dorsi flexor) ● Extensor digitorum longus (extends lateral 4 digits & dorsiflexes ankle) ● Extensor hallucis longus (extends great toe & dorsiflexes ankle) ● Peroneus tertius (dorsiflexes ankle & aids in eversion of foot) ____________________________________ ⁶ discoloration: increased pressure within a closed osteofascial compartment results in impaired local circulation ➛ ischemia ➛ necrosis thus the leg changes color as there's no proper oxygenation of the muscles in the compartment. ____________________________________ ⁷ tense and shiny skin: ● ● palpable tenseness in the involved compartment Increased tissue pressure (due to severed tibial artery causing blood to leak into compartment) in a confined anatomical space ● Involved compartment or limb will feel tense and warm on palpation ____________________________________ ⁹ Weak right dorsalis pedis: weak dorsalis pedis artery pulse may be a sign of an underlying circulatory condition ● ● ● ● dorsalis pedis artery (DPA) is a main artery of the foot. It is a continuation of the anterior tibial artery as it crosses the ankle joint. One of the primary functions of the DPA is to carry oxygenated blood to the dorsum of the foot anterior tibial artery is particularly prone to injury in diaphyseal fractures of the tibia. The peroneal artery has an anterior communicating branch to the anterior tibial artery. Hence, an occlusion of the peroneal artery may exist ____________________________________ ⁸ anterior bulge of right leg: Muscles in the anterior compartment are: ● Tibialis anterior ● Extensor digitorum longus ● Extensor hallucis longus ● Peroneus tertius borders of the anterior compartment are: ● Tibia ● Fibula ● Interosseous membrane ● Anterior intermuscular septum ____________________________________ ¹⁰ proximal tibial fracture: predisposing factor - most cases of ACS occur as a result of trauma involving a tibial fracture ____________________________________ ¹¹ 34 year-old male cyclist: occurs more commonly in males younger than 35, which may be due to a larger relative intracompartmental muscle mass and increased likelihood of being involved in high-energy trauma. ____________________________________ ¹²Muscle tears can be observed using magnetic resonance imaging (MRI) or ultrasonography. MRI may show increased signal intensity in an entire compartment on T2-weighted, spin-echo sequences - fat suppressed T2-weighted images https://my.clevelandclinic.org/health/diseases/15315-compartment-syndrome