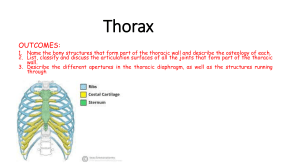
Thorax OVERVIEW OF THORAX THORACIC WALL Skeleton of Thoracic Wall Thoracic Apertures Joints of Thoracic Wall TABLE 1.1. Joints of Thoracic Wall Movements of Thoracic Wall BLUE BOX: Thoracic Wall. Chest Pain; Rib Fractures; Flail Chest; Thoracotomy, Intercostal Space Incisions, and Rib Excision; Supernumerary Ribs; Protective Function and Aging of Costal Cartilages; Ossified Xiphoid Processes; Sternal Fractures; Median Sternotomy; Sternal Biopsy; Sternal Anomalies; Thoracic Outlet Syndrome; Dislocation of Ribs; Separation of Ribs; Paralysis of Diaphragm. Muscles of Thoracic Wall TABLE 1.2. Muscles of Thoracic Wall Fascia of Thoracic Wall Nerves of Thoracic Wall Vasculature of Thoracic Wall TABLE 1.3. Arterial Supply of Thoracic Wall BLUE BOX: Muscles and Neurovasculature of Thoracic Wall. Dyspnea: Difficult Breathing; Extrapleural Intrathoracic Surgical Access; Herpes Zoster Infection of Spinal Ganglia; Intercostal Nerve Block Breasts Surface Anatomy of Thoracic Wall BLUE BOX: Breasts. Changes in Breasts; Breast Quadrants; Carcinoma of Breast; Mammography; Surgical Incisions of Breast; Polymastia, Polythelia, and Amastia; Breast Cancer in Men; Gynecomastia VISCERA OF THORACIC CAVITY Pleurae, Lungs, and Tracheobronchial Tree BLUE BOX: Pleurae, Lungs, and Tracheobronchial Tree. Injuries of Cervical Pleura and Apex of Lung; Injury to Other Parts of Pleurae; Pulmonary Collapse; Pneumothorax, Hydrothorax, and Hemothorax; Thoracentesis; Insertion of a Chest Tube; Pleurectomy and Pleurodesis; Thoracoscopy; Pleuritis (Pleurisy); Variations in Lobes of Lung; Appearance of Lungs and Inhalation of Carbon Particles and Irritants; Auscultation of Lungs and Percussion of Thorax; Aspiration of Foreign Bodies; Bronchoscopy; Lung Resections; Segmental Atelectasis; Pulmonary Embolism; Lymphatic Drainage and Pleural Adhesion; Hemoptysis; Bronchogenic Carcinoma; Lung Cancer and Mediastinal Nerves; Pleural Pain; Chest X-ray Overview of Mediastinum Pericardium BLUE BOX: Mediastinum Overview and Pericardium. Levels of Viscera Relative to Mediastinal Divisions; Mediastinoscopy and Mediastinal Biopsies; Widening of Mediastinum; Surgical Significance of Transverse Pericardial Sinus; Exposure of the Venae Cavae; Pericarditis, Pericardial Rub, and Pericardial Effusion; Cardiac Tamponade; Pericardiocentesis; Positional Abnormalities of Heart Heart TABLE 1.4. Arterial Supply to Heart BLUE BOX: Heart. Cardiac Catheterization; Embryology of the Right Atrium; Septal Defects; Atrial Septal Defects; Ventricular Septal Defects; Percussion of Heart; Stroke or Cerebrovascular Accident; Basis for Naming Cusps of the Aortic and Pulmonary Valves; Valvular Heart Disease; Mitral Valve Insufficiency (Mitral Valve Prolapse); Pulmonary Valve Stenosis; Pulmonary Valve Incompetence; Aortic Valve Stenosis; Aortic Valve Insufficiency; Echocardiography; Coronary Angiography; Coronary Artery Disease or Coronary Heart Disease; Myocardial Infarction; Coronary Atherosclerosis; Slowly Progressive Coronary Artery Disease; Angina Pectoris; Coronary Bypass Graft; Coronary Angioplasty; Collateral Circulation via Smallest Cardiac Veins; Electrocardiography; Coronary Occlusion and Conducting System of Heart; Artificial Cardiac Pacemaker; Restarting Heart; Fibrillation of Heart; Defibrillation of Heart; Cardiac Referred Pain Superior Mediastinum and Great Vessels Posterior Mediastinum TABLE 1.5. Aorta and Its Branches in Thorax Anterior Mediastinum Surface Anatomy of Heart and Mediastinal Viscera TABLE 1.6. Nerves of Thorax Auscultatory Areas BLUE BOX: Superior, Posterior, and Anterior Mediastinum. Variations of Great Arteries; BRANCHES OF ARCH OF AORTA; ANOMALIES OF ARCH OF AORTA; ; Aneurysm of Ascending Aorta; Coarctation of Aorta; Injury to Recurrent Laryngeal Nerves; Blockage of Esophagus; Laceration of Thoracic Duct; Variations of Thoracic Duct; Alternate Venous Routes to Heart; Age Changes in Thymus; Aortic Angiography; Radiography of Mediastinum; CT and MRI of Mediastinum OVERVIEW OF THORAX The thorax is the part of the body between the neck and abdomen. Commonly the term chest is used as a synonym for thorax, but the chest is much more extensive than the thoracic wall and cavity contained within it. The chest is generally conceived as the superior part of the trunk that is broadest superiorly owing to the presence of the pectoral (shoulder) girdle (clavicles and scapulae), with much of its girth accounted for by the pectoral and scapular musculature and, in adult females, the breasts. The thoracic cavity and its wall have the shape of a truncated cone, being narrowest superiorly, with the circumference increasing inferiorly, and reaching its maximum size at the junction with the abdominal portion of the trunk. The wall of the thoracic cavity is relatively thin, essentially as thick as its skeleton. The thoracic skeleton takes the form of a domed birdcage. The thoracic cage (rib cage), with the horizontal bars formed by ribs and costal cartilages, is also supported by the vertical sternum (breastbone) and thoracic vertebrae (Fig. 1.1). Furthermore, the floor of the thoracic cavity (thoracic diaphragm) is deeply invaginated inferiorly (i.e., is pushed upward) by viscera of the abdominal cavity. Consequently, nearly the lower half of the thoracic wall surrounds and protects abdominal rather than thoracic viscera (e.g., liver). Thus the thorax and its cavity are much smaller than one might expect based on external appearances of the chest. FIGURE 1.1. Thoracic skeleton. The osteocartilaginous thoracic cage includes the sternum, 12 pairs of ribs and costal cartilages, and 12 thoracic vertebrae and intervertebral discs. The clavicles and scapulae form the pectoral (shoulder) girdle, one side of which is included here to demonstrate the relationship between the thoracic (axial) and upper limb (appendicular) skeletons. The red dotted line indicates the position of the diaphragm, which separates the thoracic and abdominal cavities. The thorax includes the primary organs of the respiratory and cardiovascular systems. The thoracic cavity is divided into three major spaces: the central compartment or mediastinum that houses the thoracic viscera except for the lungs and, on each side, the right and left pulmonary cavities housing the lungs. The majority of the thoracic cavity is occupied by the lungs, which provide for the exchange of oxygen and carbon dioxide between the air and blood. Most of the remainder of the thoracic cavity is occupied by the heart and structures involved in conducting the air and blood to and from the lungs. Additionally, nutrients (food) traverse the thoracic cavity via the esophagus, passing from the site of entry in the head to the site of digestion and absorption in the abdomen. Although in terms of function and development the mammary glands are most related to the reproductive system, the breasts are located on and are typically dissected with the thoracic wall; thus they are included in this chapter. THORACIC WALL The true thoracic wall includes the thoracic cage and the muscles that extend between the ribs as well as the skin, subcutaneous tissue, muscles, and fascia covering its anterolateral aspect. The same structures covering its posterior aspect are considered to belong to the back. The mammary glands of the breasts lie within the subcutaneous tissue of the thoracic wall. The anterolateral axioappendicular muscles (see Chapter 6) that overlie the thoracic cage and form the bed of the breast are encountered in the thoracic wall and may be considered part of it, but are distinctly upper limb muscles based on function and innervation. They will be mentioned only briefly here. The domed shape of the thoracic cage provides remarkable rigidity, given the light weight of its components, enabling it to: • Protect vital thoracic and abdominal organs (most air or fluid filled) from external forces. • Resist the negative (sub-atmospheric) internal pressures generated by the elastic recoil of the lungs and inspiratory movements. • Provide attachment for and support the weight of the upper limbs. • Provide the anchoring attachment (origin) of many of the muscles that move and maintain the position of the upper limbs relative to the trunk, as well as provide the attachments for muscles of the abdomen, neck, back, and respiration. Although the shape of the thoracic cage provides rigidity, its joints and the thinness and flexibility of the ribs allow it to absorb many external blows and compressions without fracture and to change its shape for respiration. Because the most important structures within the thorax (heart, great vessels, lungs, and trachea), as well as its floor and walls, are constantly in motion, the thorax is one of the most dynamic regions of the body. With each breath, the muscles of the thoracic wall—working in concert with the diaphragm and muscles of the abdominal wall—vary the volume of the thoracic cavity, first by expanding the capacity of the cavity, thereby causing the lungs to expand and draw air in and then, due to lung elasticity and muscle relaxation, decreasing the volume of the cavity and causing them to expel air. The Bottom Line OVERVIEW OF THORAX The thorax, consisting of the thoracic cavity, its contents, and the wall that surrounds it, is the part of the trunk between the neck and abdomen. ♦ The shape and size of the thoracic cavity and thoracic wall are different from that of the chest (upper trunk or torso) because the latter includes some upper limb bones and muscles and, in adult females, the breasts. ♦ The thorax includes the primary organs of the respiratory and cardiovascular systems. ♦ The thoracic cavity is divided into three compartments: the central mediastinum, occupied by the heart and structures transporting air, blood, and food; and the right and left pulmonary cavities, occupied by the lungs. Skeleton of Thoracic Wall The thoracic skeleton forms the osteocartilaginous thoracic cage (Fig. 1.1), which protects the thoracic viscera and some abdominal organs. The thoracic skeleton includes 12 pairs of ribs and associated costal cartilages, 12 thoracic vertebrae and the intervertebral (IV) discs interposed between them, and the sternum. The ribs and costal cartilages form the largest part of the thoracic cage; both are identified numerically, from the most superior (1st rib or costal cartilage) to the most inferior (12th). RIBS, COSTAL CARTILAGES, AND INTERCOSTAL SPACES Ribs (L. costae) are curved, flat bones that form most of the thoracic cage (Figs. 1.1 and 1.2). They are remarkably light in weight yet highly resilient. Each rib has a spongy interior containing bone marrow (hematopoietic tissue), which forms blood cells. There are three types of ribs that can be classified as typical or atypical: 1. True (vertebrosternal) ribs (1st–7th ribs): They attach directly to the sternum through their own costal cartilages. 2. False (vertebrochondral) ribs (8th, 9th, and usually 10th ribs): Their cartilages are connected to the cartilage of the rib above them; thus their connection with the sternum is indirect. 3. Floating (vertebral, free) ribs (11th, 12th, and sometimes 10th ribs): The rudimentary cartilages of these ribs do not connect even indirectly with the sternum; instead they end in the posterior abdominal musculature. FIGURE 1.2. Typical ribs. A. The 3rd–9th ribs have common characteristics. Each rib has a head, neck, tubercle, and body (shaft). B. Cross section of the midbody of a rib. Typical ribs (3rd–9th) have the following components: • Head: wedge-shaped and has two facets, separated by the crest of the head (Figs. 1.2 and 1.3); one facet for articulation with the numerically corresponding vertebra and one facet for the vertebra superior to it. • Neck: connects the head of the rib with the body at the level of the tubercle. • Tubercle: located at the junction of the neck and body; a smooth articular part articulates with the corresponding transverse process of the vertebra, and a rough non-articular part provides attachment for the costotransverse ligament (see Fig. 1.8B). • Body (shaft): thin, flat, and curved, most markedly at the costal angle where the rib turns anterolaterally. The angle also demarcates the lateral limit of attachment of the deep back muscles to the ribs (see Table 4.6 in Chapter 4). The concave internal surface of the body has a costal groove paralleling the inferior border of the rib, which provides some protection for the intercostal nerve and vessels. FIGURE 1.3. Atypical ribs. The atypical 1st, 2nd, 11th, and 12th ribs differ from typical ribs (e.g., the 8th rib, shown in center). FIGURE 1.8. Joints of thoracic wall. Atypical ribs (1st, 2nd, and 10th–12th) are dissimilar (Fig. 1.3): • The 1st rib is the broadest (i.e., its body is widest and nearly horizontal), shortest, and most sharply curved of the seven true ribs. It has a single facet on its head for articulation with the T1 vertebra only and two transversely directed grooves crossing its superior surface for the subclavian vessels; the grooves are separated by a scalene tubercle and ridge, to which the anterior scalene muscle is attached. • The 2nd rib is has a thinner, less curved body and is substantially longer than the 1st rib. Its head has two facets for articulation with the bodies of the T1 and T2 vertebrae; its main atypical feature is a rough area on its upper surface, the tuberosity for serratus anterior, from which part of that muscle originates. • The 10th–12th ribs, like the 1st rib, have only one facet on their heads and articulate with a single vertebra. • The 11th and 12th ribs are short and have no neck or tubercle. Costal cartilages prolong the ribs anteriorly and contribute to the elasticity of the thoracic wall, providing a flexible attachment for their anterior ends (tips). The cartilages increase in length through the first 7 and then gradually decrease. The first 7 costal cartilages attach directly and independently to the sternum; the 8th, 9th, and 10th articulate with the costal cartilages just superior to them, forming a continuous, articulated, cartilaginous costal margin (Fig. 1.1A; see also Fig. 1.13). The 11th and 12th costal cartilages form caps on the anterior ends of the corresponding ribs and do not reach or attach to any other bone or cartilage. The costal cartilages of ribs 1–10 clearly anchor the anterior end of the rib to the sternum, limiting its overall movement as the posterior end rotates around the transverse axis of the rib (Fig. 1.5). FIGURE 1.13. Dissection of anterior aspect of anterior thoracic wall. The external intercostal muscles are replaced by membranes between costal cartilages. The H-shaped cuts through the perichondrium of the 3rd and 4th costal cartilages are used to shell out pieces of cartilage, as was done with the 4th costal cartilage. It is not uncommon for the 8th rib to attach to the sternum, as in this specimen. The internal thoracic vessels and parasternal lymph nodes (green) lie inside the thoracic cage lateral to the sternum. FIGURE 1.5. Costovertebral articulations of a typical rib. The costovertebral joints include the joint of head of rib, in which the head articulates with two adjacent vertebral bodies and the intervertebral disc between them, and the costotransverse joint, in which the tubercle of the rib articulates with the transverse process of a vertebra. The rib moves (elevates and depresses) around an axis that traverses the head and neck of the rib (arrows). Intercostal spaces separate the ribs and their costal cartilages from one another (Fig. 1.1A). The spaces are named according to the rib forming the superior border of the space—for example, the 4th intercostal space lies between ribs 4 and 5. There are 11 intercostal spaces and 11 intercostal nerves. Intercostal spaces are occupied by intercostal muscles and membranes, and two sets (main and collateral) of intercostal blood vessels and nerves, identified by the same number assigned to the space. The space below the 12th rib does not lie between ribs and thus is referred to as the subcostal space, and the anterior ramus (branch) of spinal nerve T12 is the subcostal nerve. The intercostal spaces are widest anterolaterally, and they widen further with inspiration. They can also be further widened by extension and/or lateral flexion of the thoracic vertebral column to the contralateral side. THORACIC VERTEBRAE Most thoracic vertebrae are typical in that they are independent, have bodies, vertebral arches, and seven processes for muscular and articular connections (Figs. 1.4 and 1.5). Characteristic features of thoracic vertebrae include: • Bilateral costal facets (demifacets) on the vertebral bodies, usually occurring in inferior and superior pairs, for articulation with the heads of ribs. • Costal facets on the transverse processes for articulation with the tubercles of ribs, except for the inferior two or three thoracic vertebrae. • Long, inferiorly slanting spinous processes. FIGURE 1.4. Thoracic vertebrae. A. T1 has a vertebral foramen and body similar in size and shape to a cervical vertebra. B. T5–T9 vertebrae have typical characteristics of thoracic vertebrae. C. T12 has bony processes and a body size similar to a lumbar vertebra. The planes of the articular facets of thoracic vertebrae define an arc (red arrows) that centers on an axis traversing the vertebral bodies vertically. D. Superior and inferior costal facets (demifacets) on the vertebral body and costal facets on the transverse processes. Long sloping spinous processes are characteristic of thoracic vertebrae. Superior and inferior costal facets, most of which are small demifacets, occur as bilaterally paired, planar surfaces on the superior and inferior posterolateral margins of the bodies of typical thoracic vertebrae (T2–T9). Functionally, the facets are arranged in pairs on adjacent vertebrae, flanking an interposed IV disc: an inferior (demi)facet of the superior vertebra and a superior (demi)facet of the inferior vertebra. Typically, two demifacets paired in this manner and the posterolateral margin of the IV disc between them form a single socket to receive the head of the rib of the same identifying number as the inferior vertebra (e.g., head of rib 6 with the superior costal facet of vertebra T6). Atypical thoracic vertebrae bear whole costal facets in place of demifacets: • The superior costal facets of vertebra T1 are not demifacets because there are no demifacets on the C7 vertebra above, and rib 1 articulates only with vertebra T1. T1 has a typical inferior costal (demi)facet. • T10 has only one bilateral pair of (whole) costal facets, located partly on its body and partly on its pedicle. • T11 and T12 also have only a single pair of (whole) costal facets, located on their pedicles. The spinous processes projecting from the vertebral arches of typical thoracic vertebrae (e.g., vertebrae T6 or T7) are long and slope inferiorly, usually overlapping the vertebra below (Figs. 1.4D and 1.5). They cover the intervals between the laminae of adjacent vertebrae, thereby preventing sharp objects such as a knife from entering the vertebral canal and injuring the spinal cord. The convex superior articular facets of the superior articular processes face mainly posteriorly and slightly laterally, whereas the concave inferior articular facets of the inferior articular processes face mainly anteriorly and slightly medially. The bilateral joint planes between the respective articular facets of adjacent thoracic vertebrae define an arc, centering on an axis of rotation within the vertebral body (Fig. 1.4A–C). Thus small rotatory movements are permitted between adjacent vertebrae, limited by the attached rib cage. THE STERNUM The sternum (G. sternon, chest) is the flat, elongated bone that forms the middle of the anterior part of the thoracic cage (Fig. 1.6). It directly overlies and affords protection for mediastinal viscera in general and much of the heart in particular. The sternum consists of three parts: manubrium, body, and xiphoid process. In adolescents and young adults, the three parts are connected together by cartilaginous joints (synchondroses) that ossify during middle to late adulthood. FIGURE 1.6. Sternum. A. The thin, broad membranous bands of the radiate sternocostal ligaments pass from the costal cartilages to the anterior and posterior surfaces of the sternum—is shown on the upper right side. B. Observe the thickness of the superior third of the manubrium between the clavicular notches. C. The relationship of the sternum to the vertebral column is shown. The manubrium (L. handle, as in the handle of a sword, with the sternal body forming the blade) is a roughly trapezoidal bone. The manubrium is the widest and thickest of the three parts of the sternum. The easily palpated concave center of the superior border of the manubrium is the jugular notch (suprasternal notch). The notch is deepened by the medial (sternal) ends of the clavicles, which are much larger than the relatively small clavicular notches in the manubrium that receive them, forming the sternoclavicular (SC) joints (Fig. 1.1A). Inferolateral to the clavicular notch, the costal cartilage of the 1st rib is tightly attached to the lateral border of the manubrium—the synchondrosis of the first rib (Figs. 1.1A and 1.6A). The manubrium and body of the sternum lie in slightly different planes superior and inferior to their junction, the manubriosternal joint (Fig. 1.6A & B); hence, their junction forms a projecting sternal angle (of Louis). The body of the sternum, is longer, narrower, and thinner than the manubrium, and is located at the level of the T5–T9 vertebrae (Fig. 1.6A–C). Its width varies because of the scalloping of its lateral borders by the costal notches. In young people, four sternebrae (primordial segments of the sternum) are obvious. The sternebrae articulate with each other at primary cartilaginous joints (sternal synchondroses). These joints begin to fuse from the inferior end between puberty (sexual maturity) and age 25. The nearly flat anterior surface of the body of the sternum is marked in adults by three variable transverse ridges (Fig. 1.6A), which represent the lines of fusion (synostosis) of its four originally separate sternebrae. The xiphoid process, the smallest and most variable part of the sternum, is thin and elongated. Its inferior end lies at the level of T10 vertebra. Although often pointed, the process may be blunt, bifid, curved, or deflected to one side or anteriorly. It is cartilaginous in young people but more or less ossified in adults older than age 40. In elderly people, the xiphoid process may fuse with the sternal body. The xiphoid process is an important landmark in the median plane because • Its junction with the sternal body at the xiphisternal joint indicates the inferior limit of the central part of the thoracic cavity projected onto the anterior body wall; this joint is also the site of the infrasternal angle (subcostal angle) formed by the right and left costal margins (Fig. 1.1A). • It is a midline marker for the superior limit of the liver, the central tendon of the diaphragm, and the inferior border of the heart. Thoracic Apertures While the thoracic cage provides a complete wall peripherally, it is open superiorly and inferiorly. The much smaller superior opening (aperture) is a passageway that allows communication with the neck and upper limbs. The larger inferior opening provides the ring-like origin of the diaphragm, which completely occludes the opening. Excursions of the diaphragm primarily control the volume/internal pressure of the thoracic cavity, providing the basis for tidal respiration (air exchange). SUPERIOR THORACIC APERTURE The superior thoracic aperture is bounded (Fig. 1.7): • Posteriorly, by vertebra T1, the body of which protrudes anteriorly into the opening. • Laterally, by the 1st pair of ribs and their costal cartilages. • Anteriorly, by the superior border of the manubrium. FIGURE 1.7. Thoracic apertures. The superior thoracic aperture is the “doorway” between the thoracic cavity and the neck and upper limb. The inferior thoracic aperture provides attachment for the diaphragm, which protrudes upward so that upper abdominal viscera (e.g., liver) receive protection from the thoracic cage. The continuous cartilaginous bar formed by the articulated cartilages of the 7th–10th (false) ribs forms the costal margin. Structures that pass between the thoracic cavity and the neck through the oblique, kidney-shaped superior thoracic aperture include the trachea, esophagus, nerves, and vessels that supply and drain the head, neck, and upper limbs. The adult superior thoracic aperture measures approximately 6.5 cm anteroposteriorly and 11 cm transversely. To visualize the size of this opening, note that this is slightly larger than necessary to allow the passage of a 2-inch × 4-inch piece of lumber. Because of the obliquity of the 1st pair of ribs, the aperture slopes antero-inferiorly. INFERIOR THORACIC APERTURE The inferior thoracic aperture, the anatomical thoracic outlet, is bounded as follows: • Posteriorly, by the 12th thoracic vertebra, the body of which protrudes anteriorly into the opening. • Posterolaterally, by the 11th and 12th pairs of ribs. • Anterolaterally, by the joined costal cartilages of ribs 7–10, forming the costal margins. • Anteriorly, by the xiphisternal joint. The inferior thoracic aperture is much more spacious than the superior thoracic aperture and is irregular in outline. It is also oblique because the posterior thoracic wall is much longer than the anterior wall. By closing the inferior thoracic aperture, the diaphragm separates the thoracic and abdominal cavities almost completely. Structures passing from or to the thorax to or from the abdomen pass through openings that traverse the diaphragm (e.g., esophagus and inferior vena cava), or pass posterior to it (e.g., aorta). Just as the size of the thoracic cavity (or its contents) is often overestimated, its inferior extent (corresponding to the boundary between the thoracic and abdominal cavities) is often incorrectly estimated because of the discrepancy between the inferior thoracic aperture and the location of the diaphragm (floor of the thoracic cavity) in living persons. Although the diaphragm takes origin from the structures that make up the inferior thoracic aperture, the domes of the diaphragm rise to the level of the 4th intercostal space, and abdominal viscera, including the liver, spleen, and stomach, lie superior to the plane of the inferior thoracic aperture, within the thoracic wall (Fig. 1.1A & B). Joints of Thoracic Wall Although movements of the joints of the thoracic wall are frequent—for example, in association with normal respiration—the range of movement at the individual joints is relatively small. Nonetheless, any disturbance that reduces the mobility of these joints interferes with respiration. During deep breathing, the excursions of the thoracic cage (anteriorly, superiorly, or laterally) are considerable. Extending the vertebral column further increases the anteroposterior (AP) diameter of the thorax. The joints of the thoracic wall are illustrated in Figure 1.8. The type, participating articular surfaces, and ligaments of the joints of the thoracic wall are provided in Table 1.1. TABLE 1.1. JOINTS OF THORACIC WALL IV, intervertebral. The intervertebral joints between the bodies of adjacent vertebrae are joined by longitudinal ligaments and intervertebral discs. These joints are discussed with the back in Chapter 4; the sternoclavicular joints are discussed in Chapter 6. COSTOVERTEBRAL JOINTS A typical rib articulates posteriorly with the vertebral column at two joints, the joints of heads of ribs and costotransverse joints (Fig. 1.5). Joints of Heads of Ribs. The head of the rib articulates with the superior costal facet of the corresponding (same-numbered) vertebra, the inferior costal facet of the vertebra superior to it, and the adjacent intervertebral (IV) disc uniting the two vertebrae (Figs. 1.4 and 1.8A). For example, the head of the 6th rib articulates with the superior costal facet of the body of the T6 vertebra, the inferior costal facet of T5, and the IV disc between these vertebrae. The crest of the head of the rib attaches to the IV disc by an intra-articular ligament of head of rib within the joint, dividing the enclosed space into two synovial cavities. The fibrous layer of the joint capsule is strongest anteriorly, where it forms a radiate ligament of head of rib that fans out from the anterior margin of the head of the rib to the sides of the bodies of two vertebrae and the IV disc between them (Fig. 1.8A & B). The heads of the ribs connect so closely to the vertebral bodies that only slight gliding movements occur at the (demi)facets (pivoting around the intra-articular ligament) of the joints of the heads of ribs; however, even slight movement here may produce a relatively large excursion of the distal (sternal or anterior) end of a rib. Costotransverse Joints. Abundant ligaments lateral to the posterior parts (vertebral arches) of the vertebrae provide strength to and limit the movements of these joints, which have only thin joint capsules. A costotransverse ligament passing from the neck of the rib to the transverse process and a lateral costotransverse ligament passing from the tubercle of the rib to the tip of the transverse process strengthen the anterior and posterior aspects of the joint, respectively. A superior costotransverse ligament is a broad band that joins the crest of the neck of the rib to the transverse process superior to it. The aperture between this ligament and the vertebra permits passage of the spinal nerve and the posterior branch of the intercostal artery. The superior costotransverse ligament may be divided into a strong anterior costotransverse ligament and a weak posterior costotransverse ligament. The strong costotransverse ligaments binding these joints limit their movements to slight gliding. However, the articular surfaces on the tubercles of the superior 6 ribs are convex and fit into concavities on the transverse processes (Fig. 1.9). As a result, rotation occurs around a mostly transverse axis that traverses the intra-articular ligament and the head and neck of the rib (Fig. 1.8A & B). This results in elevation and depression movements of the sternal ends of the ribs and the sternum in the sagittal plane (pump-handle movement) (Fig. 1.10A & C). Flat articular surfaces of tubercles and transverse processes of the 7th–10th ribs allow gliding (Fig. 1.9), resulting in elevation and depression of the lateral-most portions of these ribs in the transverse plane (bucket-handle movement) (Fig. 1.10B & C). FIGURE 1.9. Costotransverse joints. Conformation of articular surfaces, revealed in sagittal sections of the costotransverse joints, demonstrates how the 1st–7th ribs rotate about an axis that runs longitudinally through the neck of the rib (A), whereas the 8th–10th ribs glide (B). FIGURE 1.10. Movements of thoracic wall. A. When the upper ribs are elevated, the AP dimension of the thorax is increased (pump-handle movement), with a greater excursion (increase) occurring inferiorly, at the end of the pump handle. B. The middle parts of the lower ribs move laterally when they are elevated, increasing the transverse dimension (bucket-handle movement). C. The combination of rib movements (arrows) that occur during forced inspiration increase the AP and transverse dimensions of the thoracic cage. D. The thorax widens during forced inspiration as the ribs are elevated (arrows). E. The thorax narrows during expiration as the ribs are depressed (arrows). F. The primary movement of inspiration (resting or forced) is contraction of the diaphragm, which increases the vertical dimension of the thoracic cavity (arrows). When the diaphragm relaxes, decompression of the abdominal viscera pushes the diaphragm upward, reducing the vertical dimension for expiration. STERNOCOSTAL JOINTS The 1st pair of costal cartilages articulates with the manubrium by means of a thin dense layer of tightly adherent fibrocartilage interposed between the cartilage and manubrium, the synchondrosis of the 1st rib. The 2nd–7th pairs of costal cartilages articulate with the sternum at synovial joints with fibrocartilaginous articular surfaces on both the chondral and sternal aspects, allowing movement during respiration. The weak joint capsules of these joints are thickened anteriorly and posteriorly to form radiate sternocostal ligaments. These continue as thin, broad membranous bands passing from the costal cartilages to the anterior and posterior surfaces of the sternum, forming a felt-like covering for this bone. Movements of Thoracic Wall Movements of the thoracic wall and the diaphragm during inspiration produce increases in the intrathoracic volume and diameters of the thorax (Fig. 1.10D & F). Consequent pressure changes result in air being alternately drawn into the lungs (inspiration) through the nose, mouth, larynx, and trachea and expelled from the lungs (expiration) through the same passages. During passive expiration, the diaphragm, intercostal muscles, and other muscles relax, decreasing intrathoracic volume and increasing the intrathoracic pressure (Fig. 1.10E & C). Concurrently, intra-abdominal pressure decreases and abdominal viscera are decompressed. This allows the stretched elastic tissue of the lungs to recoil, expelling most of the air. The vertical dimension (height) of the central part of the thoracic cavity increases during inspiration as contraction of the diaphragm causes it to descend, compressing the abdominal viscera (Fig. 1.10F). During expiration, the vertical dimension returns to the neutral position as the elastic recoil of the lungs produces sub-atmospheric pressure in the pleural cavities, between the lungs and the thoracic wall. As a result of this and the absence of resistance to the previously compressed viscera, the domes of the diaphragm ascend, diminishing the vertical dimension. The AP dimension of the thorax increases considerably when the intercostal muscles contract. Movement of the ribs (primarily 2nd–6th) at the costovertebral joints around an axis passing through the necks of the ribs causes the anterior ends of the ribs to rise—the pump-handle movement (Fig. 1.10A & C). Because the ribs slope inferiorly, their elevation also results in anterior–posterior movement of the sternum, especially its inferior end, with slight movement occurring at the manubriosternal joint in young people, in whom this joint has not yet synostosed (united). The transverse dimension of the thorax also increases slightly when the intercostal muscles contract, raising the middle (lateral-most parts) of the ribs (especially the lower ones)—the bucket-handle movement (Fig. 1.10B & C). The combination of all these movements moves the thoracic cage anteriorly, superiorly, and laterally (Fig. 1.10C & F). THORACIC WALL Chest Pain Although chest pain can result from pulmonary disease, it is probably the most important symptom of cardiac disease (Swartz, 2009). However, chest pain may also occur in intestinal, gallbladder, and musculoskeletal disorders. When evaluating a patient with chest pain, the examination is largely concerned with discriminating between serious conditions and the many minor causes of pain. People who have had a heart attack usually describe the associated pain as a “crushing” sub-sternal pain (deep to the sternum) that does not disappear with rest. Rib Fractures The short, broad 1st rib, posteroinferior to the clavicle, is rarely fractured because of its protected position (it cannot be palpated). When it is broken, however, structures crossing its superior aspect may be injured, including the brachial plexus of nerves and subclavian vessels that serve the upper limb. The middle ribs are most commonly fractured. Rib fractures usually result from blows or crushing injuries. The weakest part of a rib is just anterior to its angle; however, direct violence may fracture a rib anywhere, and its broken end may injure internal organs such as a lung and/or the spleen. Fractures of the lower ribs may tear the diaphragm and result in a diaphragmatic hernia (see Chapter 2). Rib fractures are painful because the broken parts move during respiration, coughing, laughing, and sneezing. Flail Chest Multiple rib fractures may allow a sizable segment of the anterior and/or lateral thoracic wall to move freely. The loose segment of the wall moves paradoxically (inward on inspiration and outward on expiration). Flail chest is an extremely painful injury and impairs ventilation, thereby affecting oxygenation of the blood. During treatment, the loose segment may be fixed by hooks and/or wires so that it cannot move. Thoracotomy, Intercostal Space Incisions, and Rib Excision The surgical creation of an opening through the thoracic wall to enter a pleural cavity is a thoracotomy (Fig. B1.1). An anterior thoracotomy may involve making H-shaped cuts through the perichondrium of one or more costal cartilages and then shelling out segments of costal cartilage to gain entrance to the thoracic cavity (see Fig 1.13, right side). FIGURE B1.1. Thoracotomy. The posterolateral aspects of the 5th–7th intercostal spaces are important sites for posterior thoracotomy incisions. In general, a lateral approach is most satisfactory for entry through the thoracic cage (Fig. B1.1). With the patient lying on the contralateral side, the upper limb is fully abducted, placing the forearm beside the patient’s head. This elevates and laterally rotates the inferior angle of scapula, allowing access as high as the 4th intercostal space. Surgeons use an H-shaped incision to incise the superficial aspect of the periosteum that ensheaths the rib, strip the periosteum from the rib, and then excise a wide segment of the rib to gain better access, as might be required to enter the thoracic cavity and remove a lung (pneumonectomy), for example. In the rib’s absence, entry into the thoracic cavity can be made through the deep aspect of the periosteal sheath, sparing the adjacent intercostal muscles. After the operation, the missing pieces of ribs regenerate from the intact periosteum, although imperfectly. Supernumerary Ribs People usually have 12 ribs on each side, but the number is increased by the presence of cervical and/or lumbar ribs, or decreased by failure of the 12th pair to form. Cervical ribs are relatively common (0.5– 2%) and may interfere with neurovascular structures exiting the superior thoracic aperture. Lumbar ribs are less common. Supernumerary (extra) ribs also have clinical significance in that they may confuse the identification of vertebral levels in radiographs and other diagnostic images. Protective Function and Aging of Costal Cartilages Costal cartilages provide resilience to the thoracic cage, preventing many blows from fracturing the sternum and/or ribs. Because of the remarkable elasticity of the ribs and costal cartilages in children, chest compression may produce injury within the thorax even in the absence of a rib fracture. In elderly people, the costal cartilages lose some of their elasticity and become brittle; they may undergo calcification, making them radiopaque (i.e., appear white in radiographs). Ossified Xiphoid Process Many people in their early 40s suddenly become aware of their partly ossified xiphoid process and consult their physician about the hard lump in the “pit of their stomach” (epigastric fossa). Never having been aware of their xiphoid process before, they fear they have developed a tumor. Sternal Fractures Despite the subcutaneous location of the sternum, sternal fractures are not common. Crush injuries can occur after traumatic compression of the thoracic wall in automobile accidents when the driver’s chest is forced into the steering column, for example. The installation and use of air bags in vehicles has reduced the number of sternal fractures. A fracture of the sternal body is usually a comminuted fracture (a break resulting in several pieces). Displacement of the bone fragments is uncommon because the sternum is invested by deep fascia (fibrous continuities of radiate sternocostal ligaments; Fig. 1.6A) and the sternal attachments of the pectoralis major muscles. The most common site of sternal fracture in elderly people is at the sternal angle, where the manubriosternal joint has fused. The fracture results in dislocation of the manubriosternal joint. The concern in sternal injuries is not primarily for the fracture itself, but for the likelihood of heart injury (myocardial contusion, cardiac rupture, tamponade) or lung injury. The mortality (death rate) associated with sternal fractures is 25–45%, largely owing to these underlying injuries. Patients with sternal contusion should be evaluated for underlying visceral injury (Marx et al., 2009). Median Sternotomy To gain access to the thoracic cavity for surgical operations in the mediastinum—such as coronary artery bypass grafting, for example—the sternum is divided (split) in the median plane and retracted. The flexibility of ribs and costal cartilages enables spreading of the halves of the sternum during procedures requiring median sternotomy. Such “sternal splitting” also gives good exposure for removal of tumors in the superior lobes of the lungs. After surgery, the halves of the sternum are usually joined using wire sutures or clips. Sternal Biopsy The sternal body is often used for bone marrow needle biopsy because of its breadth and subcutaneous position. The needle pierces the thin cortical bone and enters the vascular spongy bone. Sternal biopsy is commonly used to obtain specimens of marrow for transplantation and for detection of metastatic cancer and blood dyscrasias (abnormalities). Sternal Anomalies The sternum develops through the fusion of bilateral, vertical condensations of precartilaginous tissue, sternal bands or bars. The halves of the sternum of the fetus may not fuse. Complete sternal cleft is an uncommon anomaly through which the heart may protrude (ectopia cordis). Partial clefts involving the manubrium and superior half of the body are V- or U-shaped and can be repaired during infancy by direct apposition and fixation of the sternal halves. Sometimes a perforation (sternal foramen) remains in the sternal body because of incomplete fusion. It is not clinically significant; however, one should be aware of its possible presence so that it will not be misinterpreted in chest X-ray, as a being an unhealed bullet wound for example. A receding (pectus excavatum, or funnel chest) or projecting (pectus cavinatum, or pigeon breast) sternum are anomalous variations that may become evident or more pronounced during childhood. The xiphoid process is commonly perforated in elderly persons because of age-related changes; this perforation is also not clinically significant. Similarly, an anteriorly-protruding xiphoid process in neonates is not unusual; when it occurs, it does not usually require correction. Thoracic Outlet Syndrome Anatomists refer to the superior thoracic aperture as the thoracic inlet because non-circulating substances (air and food) may enter the thorax only through this aperture. When clinicians refer to the superior thoracic aperture as the thoracic outlet, they are emphasizing the arteries and T1 spinal nerves that emerge from the thorax through this aperture to enter the lower neck and upper limbs. Hence, various types of thoracic outlet syndrome (TOS) exist in which emerging structures are affected by obstructions of the superior thoracic aperture (Rowland and Pedley, 2010). Although TOS implies a thoracic location, the obstruction actually occurs outside the aperture in the root of the neck, and the manifestations of the syndromes involve the upper limb (see Chapters 6 and 8). Dislocation of Ribs Rib dislocation (“slipping rib” syndrome) is the displacement of a costal cartilage from the sternum—dislocation of a sternocostal joint or the displacement of the interchondral joints. Rib dislocations are common in body-contact sports; complications may result from pressure on or damage to nearby nerves, vessels, and muscles. Displacement of interchondral joints usually occurs unilaterally and involves ribs 8, 9, and 10. Trauma sufficient to displace these joints often injures underlying structures, such as the diaphragm and/or liver, causing severe pain, particularly during deep inspiratory movements. The injury produces a lump-like deformity at the displacement site. Separation of Ribs “Rib separation” refers to dislocation of the costochondral junction between the rib and its costal cartilage. In separations of the 3rd– 10th ribs, tearing of the perichondrium and periosteum usually occurs. As a result, the rib may move superiorly, overriding the rib above and causing pain. Paralysis of Diaphragm Paralysis of half of the diaphragm (one dome or hemidiaphragm) because of injury to its motor supply from the phrenic nerve does not affect the other half because each dome has a separate nerve supply. One can detect paralysis of the diaphragm radiographically by noting its paradoxical movement. Instead of descending as it normally does during inspiration owing to diaphragmatic contraction (Fig. B1.2A), the paralyzed dome ascends as it is pushed superiorly by the abdominal viscera that are being compressed by the active contralateral dome (Fig. B1.2B). Instead of ascending during expiration, the paralyzed dome descends in response to the positive pressure in the lungs. FIGURE B1.2. Normal and paradoxical movements of diaphragm.