Believe that all can achieve
Increasing classroom participation in
learners with special support needs
SECOND EDITION
JUAN BORNMAN & JILL ROSE
Van Schaik
PUBLISHERS
Published by Van Schaik Publishers
A division of Media24 Books
1059 Francis Baard Street, Hatfield, Pretoria 0083 South Africa
All rights reserved
Copyright © 2017 Van Schaik Publishers
No part of this publication may be reproduced, stored in a retrieval system, or transmitted
in any form or by any means – electronic, mechanical, photocopying, recording or
otherwise – without written permission from the publisher, except in accordance with the
provisions of the Copyright Act 98 of 1978.
Please contact DALRO for information regarding copyright clearance for this publication. Any
unauthorised copying could lead to civil liability and/or criminal sanctions.
Tel: 086 12 DALRO (from within South Africa) or +27 (0)11 712 8000
Fax: +27 (0)11 403 9094
Postal address: PO Box 31627, Braamfontein, 2017, South Africa
http://www.dalro.co.za
First edition 2010
Second edition 2017
eISBN: 978 0 627 03434 3
Commissioning editor Chandré Blignaut
Production manager Werner von Gruenewaldt
Editorial manager Daleen Venter
Copy editor Wendy Priilaid
Proofreader Annette de Villiers
Cover design by Gisela van Garderen
Cover image Cathy Gatland
Illustrations by Henriëtte Life & Cassey Healey
Photos by EyeScape Corporate Photography (Mariki Uitenweerde)
Typeset in 11 pt on 13.5 pt Bitstream Amerigo by Pace-Setting & Graphics, Pretoria
eBook conversion by InfoGrid Pacific
Every effort has been made to obtain copyright permission for material used in this book.
Please contact the publisher with any queries in this regard.
Gender references
For clarity it was decided to use she/her when referring to the teacher, and he/him when
referring to the learner. This is in no way intended to connote any sexual discrimination or
limitation.
Website addresses and links were correct at time of publication.
This book has been reviewed by independent peer reviewers.
ABOUT THE AUTHORS
Juan Bornman (PhD in AAC; M Communication Pathology; B
Logopaedia) is a registered speech-language therapist and audiologist and
professor. She also holds the position of director of the Centre for
Augmentative and Alternative Communication, at the University of
Pretoria. For the past 24 years she has been actively involved in the
disability field as trainer, researcher and activist for one of the most
vulnerable groups within the disability spectrum: those who are unable to
speak. Her training and research comprise a variety of topics within
rehabilitation by exploring strategies that increase participation, have an
evidence base and are sustainable with a long-term impact. She also focuses
on rehabilitation as a human rights issue for individuals with disability and
how to ensure equal access to justice for those with little or no speech. She
has published more than 46 papers in international peer-reviewed journals
and book chapters (some with a research focus and some with a clinical
focus). Besides this new edition of Believe that all can achieve, which is
about increasing classroom participation in learners with special needs in an
inclusive setting, she has published two other books: Just the same on the
inside, which is aimed at demystifying the ten most common types of
disability in children; and Stop the violence against people with disabilities:
an international resource with Dr Diane Bryen, which breaks new ground
in ensuring access to the criminal justice system for those individuals who
require and/or use augmentative and alternative communication (AAC). She
has done numerous presentations in South Africa and internationally on the
topic of AAC, and has frequently been invited as a research fellow to more
than 15 international universities. She has also participated in a number of
large-scale international research projects on issues related to participation,
multilingual issues in AAC assessment and intervention, and human rights.
At the 2016 International Society for AAC (ISAAC) conference in Toronto
she received the prestigious ISAAC Fellowship Award for outstanding and
distinguished achievement in the field of AAC.
Jill Rose is a physiotherapist with extensive clinical and educational
experience with children with disabilities. She has worked in special
schools and lectured post-graduate students in the fields of both education
and AAC. She has been extensively involved with NGOs that focus on
children with disabilities and individuals with HIV/AIDS. The current
education crisis in South Africa has catapulted her into the field of early
childhood development (ECD), where she is part of a team who supports
parents, trains crèche consultants, and facilitates home-based literacy
programmes. She brings 45 years of experience and a passion for children
to her work. She holds BSc (Hons) Physiotherapy (Wits) and an MA (AAC)
(UP). These qualifications underpin the transdisciplinary practice of which
she writes so passionately and her strong belief that all children and their
families have the ability and the right to participate in every aspect of life.
ACKNOWLEDGEMENTS
Our journey into education over the past two decades has been fascinating
and exciting, often yielding quite unexpected twists and turns. Our
companions during this journey have been numerous students, colleagues
and peers from whom we have drawn inspiration and who have helped us
explore this ever-changing landscape.
There is an African saying that if you want to walk quickly, you should do
so alone, but if you want to cover a long distance, you should share the
journey with others. No book comes together quickly and therefore we
would like to thank the following individuals who shared our journey:
Our families and friends who encouraged and supported us, and who
surrounded us with their love and prayers and forgave us our absence
when we were writing!
The many families and teachers who offered us insights into their daily
triumphs (and tragedies) and who generously shared their experiences
with us so that we could write true-life vignettes. In order to protect their
identity, we did not include their names, but we could not have done this
without them.
Katinka Clack, our research assistant, whose commitment and fine eye
for detail has been such an asset. Her patience and seemingly endless
energy to locate missing references helped us over the rocky parts!
Our colleagues at the Centre for AAC at the University of Pretoria:
Alecia Samuels, Constance Nthuli, Enid Moolman, Ensa Johnson, Karin
van Niekerk, Kerstin Tönsing, Refilwe Morwane, Robyn White, Shakila
Dada, Terrence Mahlangu and Vuledzani Madiba for their unconditional
support and doing everything they could to help – standing in for us,
sharing insights and ideas and making copious cups of coffee.
Liza Siefe, who assisted with the typing, creative design of complex
figures and tables as well as the technical editing, and never complained,
even when having to redo sections because we changed our minds.
Mariki Uitenweerde from EyeScape Corporate Photography who gave us
so much of her time pro bono to take all the photographs for the book –
her eye for fine visual nuances (and unwanted shadows!) enhanced the
visual appeal of the book.
Henriëtte Life and Cassey Healey for the illustrations in the book. Their
pictures are truly worth a thousand words.
Cathy Gatland, for the cover design and Figure 1.1, which started the
journey in such an appropriate way. We liked the book cover so much
that we kept it for the second edition!
Julia Read, publishing manager for the first edition, who first gave us the
opportunity to write this book, encouraged us all the way to the finishing
line and also made it accessible to a wide readership.
Chandré Blignaut, our commissioning editor for the second edition, for
believing in us, for outstanding guidance and willingness to continue
updating the text, and for accommodating us when we kept moving
deadlines.
Daleen Venter, our editorial manager, for guiding and directing us in the
writing process and for overseeing all the aspects of the content.
Everyone who reads the book and, most importantly, who will try to
implement some of the suggested strategies.
Finally, the biggest thank you is to God Almighty, who is the greatest
author of all. We thank Him for giving us this opportunity and
responsibility.
DEDICATION
To the three men in my life:
Werner, you are the love of my life, my best friend, my hero. Thanks for
being a fourth Musketeer who serves the King and leads our family with
honour, courage, adventure and servitude. I love being your wife!
Heinrich, coming so close to losing you during the time of writing this
book reminded us all to call on the name that is Hope – His love endures
forever. Don’t ever stop touching the lives of those around you – you are a
one-in-a-million young man! I love you.
Wikus, you are always pushing the boundaries, challenging us to see things
in a new light. You have banned all potential boredom from our family and
keep us active. Keep reaching for the stars now and in the years to come,
and remember that your life has a special purpose! I love you.
JB
I dedicate these pages to a loving God who sustains me, to my husband
Mike who has walked the hilltops and valleys with me, to my daughters
Sally and Sue who inspire me, and to all the children who have been the
light on the way.
Chapter 6 is dedicated to those pioneering the work in early childhood
development (ECD) in South Africa. Thank you for your passionate
commitment to giving the children of this country the start in life they
deserve.
JR
PREFACE TO THE FIRST EDITION
Kaleidoscopes have fascinated children and adults for centuries. Every time
one looks through the one end after shaking it, one sees different jewelled
patterns although it still consists of the same tube of mirrors containing
loose coloured beads, pebbles or other small coloured objects. An infinite
number of beautiful, symmetrical, arbitrary patterns show up because of the
reflection of the light in the mirrors. For this reason, its name, derived from
the Greek, is so fitting: kalos (“beautiful”), eïdos (“form”), and skopeïn (“to
view”).
Inclusion is like a kaleidoscope. Every learner and every teacher are a
unique blend of personal characteristics and background factors that affects
the experience of living and learning. These characteristics and background
factors are not static, but like the patterns in a kaleidoscope they change
with time and context. Children develop and their personality, behaviour,
knowledge and skills change, reflecting differently in the mirrors over time.
Similarly, external factors such as abuse, violence or death in the family,
food shortages and crumbling community structures cast shadows over the
mirrors of life.
This book aims to provide a multifaceted picture of inclusion in a
developing country context. From the outset the complex interaction
between all the different elements of inclusion is explored, with each
chapter showing a different pattern of the same kaleidoscope.
Traditionally, the education of children with disabilities focused on the
nature of specific conditions in an attempt to alleviate barriers to learning.
The disability, and not the impact of the impairment on participation at
school or at home, was emphasised and no clear indication of the wellbeing
of the child and the family (including strengths and assets) was given. This
narrow focus on “the disability” or “the problem” often overshadows the
many other aspects of functionality within the child and the family
environment. Therefore, it is not uncommon to find that little carryover of
concepts taught in the classroom takes place in activities outside the
classroom. Many teachers feel like pulling their hair out when, for example,
after a long school holiday previously “learnt” knowledge and skills have
not been maintained. This book explores how the integration of learning
into real-life contexts is the foundation of meaningful education.
In contrast to this traditional problem-focused approach, the current focus is
on the strengths, attitudes and positive functioning of children within
meaningful contexts, that is, the home, the school and the community. This
book draws widely on current research with a focus on playing, developing
social networks and participating in everyday activities as the basis for
learning. Within these chapters children are viewed as unique and their
individual learning styles explored.
To evaluate whether the strategies used to improve children’s learning are
effective, it is necessary to observe what children actually do when they
participate in their everyday environment. Decisions on how to use the
available contextual and personal resources to enhance functioning have to
be made across contexts in the best interests of the child. For teachers this
involves choosing approaches and strategies that will promote participation
in all learning activities.
In this book, the value of inclusion as the foundation for education is
addressed. The kaleidoscope metaphor highlights the relationships among
all the different elements of inclusion and the different people involved,
suggesting that there is no single solution that “solves” a problem. The
nature of inclusion is such that a diversity of approaches is necessary to
reflect the reality of current classroom situations. Coming to grips with the
reality of addressing issues related to inclusion thus requires not only
convergent reasoning with regard to solutions, but also divergent reasoning.
Although research focusing on convergent reasoning (i.e. focused on
specific disabilities and teaching approaches) is necessary, the need to
complement these studies with research focusing on divergent reasoning
(i.e. exploring the diversity of solutions derived in real life) comprises an
essential part of enhancing inclusion. Teachers need to understand how
planning the curriculum and instruction at the outset – bearing the diverse
learning styles and needs of learners in mind – has the potential to reduce
the time, costs and efforts associated with designing a high-quality
educational programme for all learners, especially those with disabilities. If
teachers are to truly embrace inclusion with a sense of real purpose and
commitment, training has to focus on strategies to improve their confidence
in order to plan an inclusive classroom effectively. One such a strategy that
is used throughout the book is that of personal narratives. We have focused
our professional lives (and most of our personal lives too) on listening to
various role players, such as parents, teachers and therapists, and many of
those true narratives are shared on the following pages.
In the social sciences, books are primary vehicles for creating and sharing
knowledge. This book, which is intended for peers who work in the field of
inclusive education, is no different and was developed as a product of more
than 15 years’ research and training in the field of augmentative and
alternative communication and severe disability. Our career paths
intertwined as we pursued different work opportunities that demanded
collaboration, consultation and cooperation. Through these interactions and
the numerous research and training seminars we conducted we became
sensitised to the issues related to the inclusion of children with disabilities.
Our understanding of how to use opportunities for participation and
learning optimally was increased, and we learnt many of the principles and
practices that we now showcase in this book.
Our vision in writing this book was to go beyond the rhetoric of explaining
why inclusion is important and how it should be done. It was never about
providing a “quick fix” or other short-term solutions, but rather about
sharing some of the myriad possible best-practice, evidence-based
techniques and strategies in an effort to build a deeper understanding of the
core issues. From the very beginning we knew that neither of us could write
this book alone. This book is a collaborative project in every sense of the
word. It is for this reason that we would like to thank the four critical
readers for their excellent peer reviews and their insightful suggestions that
have enhanced the value of the book. Our dream is that our colleagues in
the field will use this book to celebrate diversity in the classroom, to
capitalise on the strengths each learner brings to the learning–teaching
dyad, and to welcome every family member as part of the broader
classroom community.
Inclusion is like a kaleidoscope – every time you shake it, the pattern
changes.
PREFACE TO THE SECOND EDITION
Since the publication of the first edition of this book, inclusion indeed
turned out to be a kaleidoscope, both internationally and locally: new policy
statements and legislation around inclusion became available, as well as the
acceptance of the Curriculum and Assessment Policy Statement (CAPS) in
South Africa. The DSM-5 classification was accepted with important
implications for autism spectrum disorders. Likewise, changes were
suggested for the classification and understanding of cerebral palsy,
epilepsy and visual impairments. Exponential medical advances in
neuroscience, molecular biology and epigenetics has caused a paradigm
shift in the old “nature–nurture” debate regarding causes of disability.
Epigenetics has taught us that under the influence of external factors
(environmental influences) certain genes can be turned on and off. This
helps our fixed genetic material to be more flexible. In 2013, Dr Elizabeth
Blackburn who received the 2009 Nobel Prize for Medicine, warned that
toxic stress (brought on by long-term violence, abuse and poverty) reduces
the protective cover of the genome, thereby altering genetic material. This
research has already resulted in the approval of “epigenetic” medication for
cancer treatment, which may also be suitable for certain neurodegenerative
diseases. Ground-breaking studies have shown that even in the face of
significant adversity, some individuals show resilience and that the
capabilities which undergird resilience can be built more easily into the
younger child, but also across the lifespan. It is never too late! This research
may also result in faster therapeutic success. Whatever the outcome,
epigenetics certainly holds great potential for understanding and thinking
about human life.
Besides updating all the chapters to reflect current knowledge and practicebased evidence as well as evidence-based practice, a new chapter on early
childhood development has been added. The importance of the emotional,
physical and social development of young children on their overall
development and later academic performance is widely acknowledged.
Early childhood development is thus directly related to the adults these
children will become. With Grade R becoming a reality for many South
African schoolchildren, not having a chapter on early childhood
development would have been a grievous oversight. Understanding this
phase of development is important to maximise future development and
wellbeing.
Indeed, inclusion is like a kaleidoscope – every time you shake it, the
pattern changes.
ABRIDGED CONTENTS
List of figures
List of tables
List of abbreviations and acronyms
Part I Inclusive education: principles and practice
Chapter 1
Chapter 2
Chapter 3
Chapter 4
Chapter 5
Inclusion: changing paradigms
Participation
Assessment approaches in the school setting
Teaching practices
Differentiated teaching
Part II Inclusive education: functional abilities
Chapter 6 Early childhood development (ECD)
Chapter 7 Understanding children with challenging behaviour
Chapter 8 Understanding children with intellectual disability
Chapter 9 Understanding children with learning disabilities
Chapter 10 Understanding children with physical disabilities
Chapter 11 Understanding children with sensory disabilities
Chapter 12 Understanding children with autism spectrum disorder
Chapter 13 Understanding children with chronic medical conditions
Part III Functional approach to integrating disability and support
Chapter 14 Integrating disability and support
TABLE OF CONTENTS
PART I INCLUSIVE EDUCATION: PRINCIPLES AND PRACTICE
Chapter 1 Inclusion: changing paradigms
1.1 Introduction
1.2 Understanding “inclusion”
1.3 How is inclusion currently being addressed?
1.3.1 Knowledge and skills training approach
1.3.2 Collaborative team approach
1.3.3 Narrative approach
1.4 Who should be involved in inclusion?
1.4.1 Wide-angle lens: the child in the community context
1.4.2 Regular lens: the child in the school context
1.4.3 Close-up lens: the child in the home context
1.5 Conclusion
Chapter 2 Participation
2.1
2.2
2.3
2.4
2.5
2.6
Introduction
Participation
Inclusive education
Labelling
Collaborative teaming
Participation and learning model (PLM)
2.6.1 Curriculum
2.6.2 Factors that facilitate participation and learning
2.6.3 Barriers to learning
2.7 Conclusion
Chapter 3 Assessment approaches in the school setting
3.1 Introduction
3.2 The assessment process
3.2.1 The learner
3.2.2 The journey
3.2.3 The way
3.3 Individual support plans (ISPs)
3.4 Assessment approaches
3.4.1 Curriculum content
3.4.2 Curriculum modifications required
3.4.3 Assessment formats and achievement standards
3.5 Accommodations and supports
3.5.1 Accommodations
3.5.2 Supports
3.6 Assessment of skills
3.7 Conclusion
Chapter 4 Teaching practices
4.1 Introduction
4.2 Setting up the inclusive classroom
4.3 Classroom ethos
4.3.1 Create a warm, welcoming classroom environment
4.3.2 Establish mutual respect
4.3.3 Encourage participation
4.3.4 Provide decision-making opportunities in the classroom
4.3.5 Develop self-discipline
4.4
4.5
4.6
4.7
4.3.6 Become a role model
Getting to know each child
Teaching strategies for all learners
4.5.1 Teaching strategy 1: maximising time on task (academic
engagement)
4.5.2 Teaching strategy 2: managing time effectively
4.5.3 Teaching strategy 3: presenting effective lessons
4.5.4 Teaching strategy 4: teaching self-reflection
Unhelpful strategies: what not to do
Conclusion
Chapter 5 Differentiated teaching
5.1 Introduction
5.2 Elements of differentiated teaching
5.2.1 Content
5.2.2 Process
5.2.3 Products
5.3 Conclusion
PART II INCLUSIVE EDUCATION: FUNCTIONAL ABILITIES
Chapter 6 Early childhood development (ECD)
6.1 Introduction
6.1.1 What is early childhood development?
6.1.2 Core concepts of early childhood development
6.1.3 Managing the transitions
6.2 South Africa: setting the scene
6.2.1 Statistics
6.2.2 Constitution of South Africa (South Africa, 1996a)
6.2.3 South African legislation and policies
6.2.4 United Nations Sustainable Development Goals (2015)
6.3
6.4
6.5
6.6
6.2.5 Roles and responsibilities of government departments
Participation
6.3.1 Factors which facilitate the participation in ECD programmes
6.3.2 Factors which are barriers to participation in ECD programmes
Core concepts
6.4.1 The developing brain
6.4.2 Serve and return
6.4.3 Resilience
Out there making a difference
6.5.1 Government and non-governmental organisations (NGOs)
6.5.2 Where to begin
Conclusion
Chapter 7 Understanding children with challenging behaviour
7.1
7.2
7.3
7.4
7.5
Introduction
Emotion is part of behaviour
Defining challenging behaviour
Basic behavioural principles
Assessment
7.5.1 Describing the history and background of the behaviour
7.5.2 Describing the behaviour
7.5.3 Describing what happens before the challenging behaviour:
setting events and antecedents
7.5.4 Describing the function of the behaviour
7.5.5 A last word on assessment
7.6 Managing the behaviour: positive behaviour support
7.6.1 Level 1: Building emotional intelligence
7.6.2 Level 2: Prevention practices and positive programming
7.6.3 Level 3: Positive behaviour support
7.6.4 Level 4: Functional communication training
7.7 Crisis management
7.8 Conclusion
Chapter 8 Understanding children with intellectual disability
8.1 Introduction
8.2 Intellectual disability
8.2.1 What is Down syndrome?
8.2.2 What is fragile X syndrome?
8.2.3 What is foetal alcohol spectrum disorder (FASD)?
8.3 General approach to teaching children with intellectual disability
8.4 Specific strategies to accommodate learners with intellectual disability
8.4.1 Get to know the child: make observations
8.4.2 Collaborating with families
8.4.3 Collaborative learning and activity-based lessons
8.4.4 Visual schedules
8.4.5 Explicit requesting and the use of an attention-getting signal
8.4.6 Reference flip books
8.4.7 Augmentative and alternative communication strategies
8.5 Conclusion
Chapter 9 Understanding children with learning disabilities
9.1 Introduction
9.2 Types of learning disability
9.2.1 Attention deficit hyperactivity disorder
9.2.2 Dyslexia
9.2.3 Dyscalculia
9.2.4 Dysgraphia
9.2.5 Dyspraxia
9.3 Managing a child with a learning disability in the classroom context
9.3.1 Developing learning skills
9.3.2 Reciprocal teaching
9.3.3 Cognitive organisers
9.3.4 Taking notes in class: teaching this skill
9.3.5 Homework strategies
9.4 Most commonly used classroom accommodations
9.4.1 Teach problem solving
9.4.2 Teach reading comprehension strategies
9.4.3 Do not force oral reading
9.4.4 Introduce a personal dictionary of key terms
9.4.5 Reduce copying tasks
9.4.6 Accept calculators
9.4.7 Adapt assessment procedures
9.4.8 Grade on content, not spelling or handwriting
9.5 Ask learners how they learn best
9.6 Conclusion
Chapter 10 Understanding children with physical disabilities
10.1 Introduction
10.2 Normal development
10.3 Specific conditions
10.3.1 Cerebral palsy
10.3.2 Spina bifida
10.3.3 Muscular dystrophy
10.4 Supporting children with physical challenges in the classroom
10.4.1 Classroom ethos
10.4.2 Seating and positioning
10.4.3 Lifting
10.4.4 Accommodations
10.4.5 Assistive technology
10.4.6 Literacy and low technology
10.4.7 Literacy and high technology
10.4.8 Play
10.4.9 Peers
10.4.10 Classroom assistants or facilitators
10.5 Conclusion
Chapter 11 Understanding children with sensory disabilities
11.1 Introduction
11.2 Hearing impairment
11.2.1 What is a hearing impairment?
11.2.2 What causes hearing impairments?
11.2.3 Characteristics of hearing impairments
11.2.4 Strengths: resilience factors
11.2.5 Classroom management
11.3 Visual impairment
11.3.1 What is visual impairment?
11.3.2 What causes visual impairments?
11.3.3 Characteristics of visual impairments
11.3.4 Warning signs of visual impairment
11.3.5 Strengths: resilience factors
11.3.6 Classroom management
11.4 Deafblindness or dual sensory impairment
11.4.1 What is deafblindness?
11.4.2 What causes deafblindness?
11.4.3 Characteristics of deafblindness
11.4.4 Classroom management strategies
11.5 Conclusion
Chapter 12 Understanding children with autism spectrum disorder
12.1 Introduction
12.2 What is ASD?
12.2.1 Domain 1: Social communication and social interaction across
multiple contexts
12.2.2 Domain 2: Restricted, repetitive patterns of behaviour, interests
or activities
12.2.3 Severity
12.3 What causes ASD?
12.3.1 Genetic predisposition
12.3.2 Environmental factors
12.3.3 Other impairments often associated with ASD
12.4 Classroom strategies for managing children with ASD
12.4.1 Classroom arrangement for optimal learning
12.4.2 Predictable routines and visual schedules
12.4.3 Avoid change – be consistent
12.4.4 Communication skills in the classroom
12.4.5 Picture Exchange Communication System (PECS)
12.4.6 TEACCH
12.4.7 Sensory integration therapy (SIT)
12.4.8 Addressing poor concentration
12.4.9 Addressing academic difficulties
12.4.10 Addressing emotional vulnerability and developing social
competence
12.5 A tale of two mothers
12.6 Conclusion
Chapter 13 Understanding children with chronic medical conditions
13.1 Introduction
13.2 Medical conditions seen most frequently in the classroom
13.2.1 Asthma
13.2.2 Childhood cancers
13.2.3 Epilepsy
13.2.4 Diabetes mellitus
13.2.5 Heart defects
13.2.6 HIV/AIDS
13.2.7 Malaria
13.2.8 Malnutrition
13.2.9 Tuberculosis
13.3 Stakeholders in the management of children with medical conditions
in schools
13.3.1 Records of children with medical conditions
13.3.2 First aid training for staff
13.3.3 Ability to administer emergency or essential medication
13.3.4 Support framework where teachers identify need
13.4 Overview of challenges related to accommodation and support
13.5 Conclusion
PART III FUNCTIONAL APPROACH TO INTEGRATING
DISABILITY AND SUPPORT
Chapter 14 Integrating disability and support
14.1 Introduction
14.2 Inclusion in South Africa: current policy and practice
14.2.1 Reasons for optimism
14.2.2 Areas of continuing concern
14.3 Shaping the future: what will influence educational outcomes?
14.4 Conclusion
Index
LIST OF FIGURES
Figure 1.1
Figure 1.2
Figure 1.3
Figure 1.4
Figure 2.1
Figure 2.2
Figure 2.3
Figure 2.4
Figure 3.1
Figure 3.2
Figure 4.1
Figure 4.2
Figure 4.3
Figure 4.4
Figure 4.5
Figure 4.6
Figure 5.1
Figure 5.2
Figure 5.3
Figure 5.4
Figure 5.5
Figure 5.6
Figure 5.7
Inclusion is about accepting difference
Zoom lens model
Community involvement in action
Teacher role diversification
Inclusion means a sense of belonging in the community
Activity and participation domains in the ICF-CY
Participation and learning model
Building bridges
Two key assessment purposes
Using a mind map to display MAPS details
Inclusion is about involving all the learners in the class
General education and adaptations
Using a handmade timer
A mind map
Randomised questioning
The story of The three little pigs
Elements of differentiated teaching
Using different entry points to accommodate learning styles
Six-sided cubes
Scaffolds are structures that support
Example of a mind map for brainstorming ideas
Cyclical scheme for the life cycle of the silk worm
AiLgS song board
Figure 5.8
Figure 5.9
Figure 6.1
Figure 6.2
Figure 6.3
Figure 6.4
Figure 6.5
Figure 7.1
Figure 7.2
Figure 7.3
Figure 7.4
Figure 7.5
Figure 7.6
Figure 7.7
Figure 8.1
Figure 8.2
Figure 8.3
Figure 8.4
Figure 8.5
Figure 8.6
Figure 8.7
Figure 8.8
Figure 8.9
Figure 8.10
Figure 9.1
Figure 9.2
Figure 9.3
Figure 9.4
Example of a learning contract
Example of a homework sheet
Zola’s story: the challenges
ECD: 0–9 years
Core concepts of ECD
Resilience
A child being physically and verbally abused by his parents
Using a balloon or a punch bag to help manage anger
Attention-seeking behaviour
Multilevel behaviour management plan
Contingency map
Example of a social story: “All about hugs”
Manual signs used for escape-motivated behaviour
Manual signs used for attention-seeking behaviour
Example of the facial features of a child with Down
syndrome
Example of the features of a child with fragile X syndrome
Examples of the facial features of a child with FASD
Incorporating different learning styles in the classroom
Differentiated teaching worksheet for a literacy activity
Differentiated teaching worksheet for a spelling test
Interactive game: teaching greater than (>) and smaller than
(<)
Differentiated teaching worksheet for a maths test
Classroom schedule for Lesedi
Reference flip book that can be used in maths
Types of learning disability briefly covered in this chapter
Example of a prompt card used in reciprocal teaching
Using a buddy to make a carbon copy
Allow the use of calculators
Figure 9.5
Figure 10.1
Figure 10.2
Figure 10.3
Figure 10.4
Adapting test procedures
Physical disabilities
Different parts of the body affected
Example of the features of a child with hydrocephalus
Example of a baby with spina bifida myelomeningocele
before corrective surgery
Figure 10.5 Example of a boy with muscular dystrophy
Figure 10.6 Example of a comfortable, functional position for the
classroom
Figure 10.7 Example of a lap strap that provides sitting balance
Figure 10.8 Example of a lap tray that provides a working surface
Figure 10.9 A child should not be handled like a sack of potatoes
Figure 10.10 Examples of correct and incorrect lifting patterns
Figure 10.11 Example of adaptations that can be used with pens and
pencils
Figure 10.12 Example of a card holder
Figure 11.1 Sensory systems
Figure 11.2 Anatomy of the ear
Figure 11.3 One-handed alphabet
Figure 11.4 Impact of visual acuity loss
Figure 11.5 Visual field
Figure 11.6 Braille alphabet
Figure 11.7 Two-handed manual alphabet used by deafblind individuals
Figure 12.1 Two domains affected by ASD
Figure 12.2 Example of a “first-then” page
Figure 12.3 Iconicity of SASL signs
Figure 12.4 Motor complexity of SASL signs
Figure 12.5 Repeated handshapes of SASL signs
Figure 12.6 Example of a PECS suitcase showing PCS™
Figure 12.7 Example of a social skills story
Figure 13.1
Figure 13.2
Figure 13.3
Figure 13.4
Figure 13.5
Figure 14.1
Chronic medical conditions seen most frequently in the
classroom
Seizure classification
Malaria-prevention techniques
Roles of key stakeholders in managing children with
chronic medical conditions in schools
Parent engagement model
Basic beliefs, assumptions and attitudes that influence the
educational outcomes
LIST OF TABLES
Table 1.1
Table 2.1
Table 3.1
Table 3.2
Table 3.3
Table 3.4
Table 4.1
Table 4.2
Table 4.3
Table 5.1
Table 5.2
Table 5.3
Table 5.4
Table 5.5
Table 5.6
Table 7.1
Table 7.2
Table 7.3
Table 7.4
School’s and parents’ responsibilities
Example of a low-tech and a high-tech augmentative and
alternative communication device
Assessment formats, content modifications and achievement
standards
Applying MAPS to a particular learner
Choosing the most appropriate accommodations
Skills checklist for screening children with disabilities in an
educational context
Effective and less-effective classroom rules
Example of an SPSO worksheet
Effective teaching practices
Differentiated teaching worksheets: Grade 5 – making peanut
butter balls
Example of a six-sided cube lesson plan
Research grid for the social science theme “Our country”
Linear schema for describing an atom
Six steps for implementing AiLgS
Dos and don’ts of implementing AiLgS
Example of a completed scatter plot
Setting events checklist
Completed A-B-C chart
Behaviour function scale
Table 7.5
Table 7.6
Table 7.7
Table 8.1
Table 9.1
Table 9.2
Table 9.3
Table 10.1
Table 10.2
Table 11.1
Table 11.2
Table 11.3
Table 11.4
Table 12.1
Table 13.1
Table 13.2
Table 14.1
Table 14.2
Traffic light system to build emotional intelligence
Examples of different classroom schedules using Picture
Communication Symbols™
Designing a visual schedule
Example of different augmentative and alternative
communication devices
Three types of ADHD presentation
Example of a column-style note page
What makes a good learner?
Easy book adaptations
Adapting toys for children with physical disabilities
Degree of hearing loss and the effect on communication
Impact of visual acuity and visual field on visual skills
Increase font size to enhance visibility
Tactile differentiation activities
Different low-technology-aided systems
Understanding hypo- and hyperglycaemia
Types of accommodation or support
Reasons for optimism
Areas of concern
LIST OF ABBREVIATIONS AND
ACRONYMS
AAC
AAIDD
AAMR
ABC chart
ABET
ADD
ADHD
AIDS
AiLgS
APA
ARVs
ASD
ASHA
ASL
AT
BODMAS
BSL
CAAC
CAPS
Augmentative and alternative communication
American Association on Intellectual Developmental
Disabilities
American Association on Mental Retardation
Antecedents; behaviour; consequences
Adult basic education and training
Attention deficit disorder
Attention deficit hyperactivity disorder
Acquired immunodeficiency syndrome
Aided language stimulation
American Psychiatric Association
Antiretrovirals
Autism spectrum disorder
American Speech-Language-Hearing Association
American Sign Language
Assistive technology
Brackets, orders, division, multiplication, addition and
subtraction
British Sign Language
Centre for Augmentative and Alternative Communication
Curriculum and Assessment Policy Statement
CAST
CBA
CDD
COACH
CP
CRPD
dB
DBE
DBSTs
DEAFSA
DoE
DoH
DOTS
DSD
DSM-5
ECD
ECE
ECI
ELLI
FASD
FET
FM
GP
HIV
HOD
Hz
ICF-CY
ILAE
Center for Applied Special Technology
Curriculum-based assessment
Childhood disintegrative disorder
Choosing Options and Accommodations for Children
Cerebral palsy
Convention on the Rights of Persons with Disabilities
Decibels
Department of Basic Education
District-based support teams
Deaf Federation of South Africa
Department of Education
Department of Health
Directly Observed Treatment, Short-course
Department of Social Development
Diagnostic and Statistical Manual of Mental Disorders –
Version 5
Early childhood development
Early childhood education
Early childhood intervention
Extended Life-Long Learning Inventory
Foetal alcohol spectrum disorder
Further Education and Training
Frequency modulation
General practitioner
Human immunodeficiency virus
Head of department
Hertz
International Classification of Functioning, Disability, Health
– Children and Youth Version
International League against Epilepsy
ILSTs
INDS
ISP
IQ
LOLT
MAPS
MAS
MD
MMR
MUSCLE
NCLD
NEET
NGO
NPO
PDD
PDD-NOS
PECS
PGP
PIRLS
PLM
POWER
RAP
SASA
SASL
SCREAM
Institution-level support teams
Integrated National Disability Strategy
Individual support plan
intelligence quotient
Language of learning and teaching
McGill Action Planning System
Motivation Assessment Scale
Muscular dystrophy
Measles, mumps and rubella
Motor milestone a day; unusual gait; speech delay;
challenging behaviour; leads to early diagnosis
National Center for Learning and Disabilities
Not in education, employment or training
Non-government organisation
Non-profit organisation
Pervasive developmental disorder
PDD not otherwise specified
Picture Exchange Communication System
Personal growth plan
Progress in International Reading Literacy
Participation and learning model
Plan your essay; organise your thoughts and ideas; write
your draft essay; edit your work; revise your work and
produce the final essay
Read paragraph, ask yourself, put main idea and detail into
your own words
South African Schools Act
South African Sign Language
Structure; clarity; redundancy; enthusiasm; appropriate rate;
maximised engagement
SEE
SGB
SIAS
SIS-C
SIT
SPSO
STNR
TAC
TASH
TB
TEACCH
TRAVEL
TRRFCC
UN
UNESCO
UNICEF
WFP
WHO
Signing Exact English
School governing body
Screening, identification, assessment and support
Supports Intensity Scale – Children version
Sensory integration therapy
Situation-Problem-Solution-Outcome
Symmetrical tonic neck reflex
Treatment Action Campaign
The Association for Persons with Severe Handicaps
Tuberculosis
Treatment and Education of Autistic and related
Communication Handicapped Children
Topic; read; ask; verify; examine; link
Trustworthiness, respect, responsibility, fairness, caring and
citizenship
United Nations
United Nations Educational, Scientific and Cultural
Organization
United Nations Children’s Fund
World Food Programme
World Health Organization
PART
I
Inclusive education: principles and
practice
This section of the book provides the theoretical underpinning of the
construct of inclusion. A zoom lens metaphor is used to view inclusion as a
series of snapshots with the regular lens focused on the child in the school
context, the close-up lens on the child in the home context, and the wideangle lens on the child in the community. This metaphor is used as it does
not have a linear progression, but rather highlights the importance of
focusing on different environments, stages and people in the child’s life.
The child is therefore never seen in isolation, but always as part of a more
comprehensive system.
Included in this understanding of inclusion is the notion of participation –
the involvement in a life situation. Increased participation is seen as one of
the ultimate outcomes of inclusion. Participation is unpacked by exploring
the different factors that facilitate participation and learning (in line with
current thinking in the asset-based literature, which runs through the whole
text as a golden thread), without negating the impact of environmental
and/or personal barriers that hinder participation.
It is against this theoretical backdrop that assessment and teaching practices
(regular as well as differentiated) are explored. Narratives, case discussions
and vignettes are frequently employed to highlight important concepts as
these create common ground and facilitate insightful understanding of the
concept of inclusion.
1
Inclusion: changing paradigms
“Good morning, Teacher.” I look at the woman in front of me holding a girl’s hand, and
see respect, fear, uncertainty and some other unnamed emotions on their faces.
Smilingly I ask, “What can I do for you, Mam?” She glances at the little girl and then
starts to speak slowly, thinking about every word. “I want to bring Rachel to your
school. I think she will be happy at your school. You will be good for her.” I am
puzzled, because the little girl, who I now know is called Rachel, is clearly of schoolgoing age. “Is she not at school now?”
Looking down, the woman speaks in a soft voice. “Yes, she goes to Thuthuka
Primary School with her older brothers and her little sister, but the school said she
must not come back. They cannot help her. She cannot learn like the other children.
She just causes problems.” Realising that this is not a quick conversation, and
definitely not one that I would like Rachel to listen to, I interrupt the woman and call
one of the children playing outside. “Tumi, this is a new friend. Her name is Rachel.
Will you take her to go and play with you and your friends? Show her our vegetable
garden. I would just like to talk to her mother for a while.”
With the girls gone, I look at the woman questioningly, “Mrs …?” She smiles. “I am
Mrs Serudu, Rachel’s mother.” “Please tell me more about Rachel,” I urge. Mrs
Serudu sighs and starts to talk. “I had two boys and then I had this one. I was so
happy when it was a girl, because I knew that she would be able to help me in the
house with the chores. Looking after all the men is so much work. My husband goes
to work early in the morning and comes back late at night, and then everything must
be okay. The boys are just outside the whole time. But from the time Rachel was
small, I could see that she was not the same as the other two. First I thought it was
because she is a girl, but when I spoke to my friend who has girls, she said that this
is not a girl thing.”
I want to make sure that I completely understand Mrs Serudu, and therefore I ask,
“What is not a girl thing?” “Being slow. It is like this – my sons started walking when
they were about a year old, but she only walked when she was a year and a half. The
boys also started talking, you know their first words like ma-ma and ba-ba, but she
was always quiet. She only started talking when she was about three years old. I was
worried then that she didn’t hear well, but I took her to the clinic and the nurses said
her ears are fine. Even now, she is 11 years old, but she talks like a younger child. I
can say like one of seven years old. Also at school, I can say that she is a slow
learner, because she is now in Grade 2, and the teachers at Thuthuka say she is
going to fail again this year.”
At this point, Mrs Serudu looks down and starts fiddling with the handkerchief in her
hand. Then she reaches down, opens her handbag and takes out an envelope that I
can clearly see has been handled many times. I can also see that it is difficult for her
to continue. “This is her last school report.”
I take the report, and see all the 1s on the report, meaning that the skills have “not
achieved”.
EXAMPLE OF A REPORT CARD
PROGRESS REPORT: Foundation Phase
Name: Rachel Serudu
Date: November 2016
Grade: 2
Assessment criteria
Achievement level
Achievement description
Marks (%)
7
Outstanding achievement
80–100%
6
Meritorious achievement
70–79%
5
Substantial achievement
60–69%
4
Adequate achievement
50–59%
3
Moderate achievement
40–49%
2
Elementary achievement
30–39%
1
Not achieved
0%
Language
Home language
1
Not achieved
First additional language
1
Not achieved
1
Not achieved
Beginning knowledge
1
Not achieved
Creative arts
2
Elementary achievement
Physical education
1
Not achieved
Personal and social wellbeing
1
Not achieved
Mathematics
Mathematics
Life skills
General comments
Rachel did not perform well at school this year, and she will have to repeat
Grade 2 as she has not yet mastered the desired outcomes. She is lazy in class,
and often distracts the other learners. She does not pay attention to what the
teacher says.
While reading through Rachel’s report card, I can feel Mrs Serudu’s anxiety. I also get
a distinct feeling that she feels ashamed of this daughter for whom she had such high
hopes, and who now cannot do what is required of her at school. In my head I hear
my university professor’s voice telling us to always look for the positives – to look at
the child’s abilities and not at the problems. It is usually easy to see all the problems
a child has – that does not take a skilled teacher. The art is to look for the subtle or
unique skills that a child might have, and to focus on the identified strengths. That is
what separates good teachers from ordinary teachers, she used to say. On a report
card like this, what could I possibly say? And then my eye falls on the only 2 among
all the 1s.
“I see that Rachel likes the creative arts,” I say, and then for the first time Mrs
Serudu’s face lights up. “Yes, she really likes to paint and watch all the different
colours and how they mix, and she is very good at helping with the younger children.
She is very patient, and she makes us laugh, because she does funny things at
home. I don’t see how the teacher at Thuthuka can say that she is lazy, because she
is the one that always helps me. She can make a bed, and wash the dishes and
sweep the floor. She can also help her older brothers to care for the chickens. It is
just the thing at school, and now she doesn’t want to go to school anymore.”
Eventually I ask the question that has been on my mind the whole time: “Now if she
doesn’t want to go to school any more, why did you come to our school?”
“I hear that your school is different. That this is a happy school. That children like to
come to your school and that the teachers like to work at this school. I hear that you
don’t send people away, and that parents can come to school and are not scared to
talk to the teachers,” Mrs Serudu says, and then with a wide grin, “And I also hear
that in the afternoons some of the grannies from the old-age home come here and
read stories to the children. I want Rachel to also listen to the stories. I want her to
look at the books, and I want her to have friends.”
“And who tells you all these things?” I ask with a knowing smile, fully aware that all of
this is true. The answer comes confidently, “One of the people at my church, Maria
Dlamini. Her son also comes to this school. His name is Jabulani and he is in a
wheelchair. That made me think –, if Jabulani is happy here, Rachel might also be
happy …”
“Yes, I am also sure that Rachel will be happy in our school. I am also sure that she
will continue to grow and learn many new skills here in our school. Our school is
called an inclusion school …”
1.1 INTRODUCTION
So what is inclusion? What makes this inclusion school different from the
previous one? What will the principal tell Mrs Serudu about inclusive
schools? Will Rachel flourish in this new environment? It may be expected
that a book such as this would start with a clear definition of what inclusion
is, what it is not, and why it is important. Living in the 21st century, which
is also known as the “information era”, we expect clear-cut, easy-to-follow,
rule-governed instructions – but if this is what you are looking for, this is
not the right book for you! Rather, this book will take you on a journey of
discovery; it is not solely about reaching the destination (inclusion) but
rather about the fellow travellers on the road (Rachel, her family, her
friends, her teachers), how this journey impacts on each one, how they
change over the course of time and how they manage to bridge the gap.
1.2 UNDERSTANDING “INCLUSION”
Inclusion has become a commonly used word, not only in the education
field, albeit with differences in interpretation and application. Is inclusion
about place, curriculum, acceptance or participation? Is it about
implementing policies, such as Education White Paper 6 (Department of
Education, 2001)? Is it about successfully addressing “barriers to learning”?
Is inclusion about teachers who are trained in specialist psychologically
based pedagogy or about regular teachers who require certain additional
skills? It is about all of these things and more – hence the notion of
inclusion as a “bewildering concept” (Lawson, Parker & Sikes, 2006).
This bewilderment is seen at various levels in both the home and the school
context. The classrooms in which teachers are expected to teach probably
do not resemble the classrooms they attended, which contributes to their
feelings of bewilderment. Diversity is viewed as one of the major features
of classrooms in the 21st century (Ford, 2013; Mastropieri & Scruggs,
2010) and now reflects a “salad bowl” of our multilingual and multicultural
society. The salad bowl perspective is different from the “melting pot”
where all the different ingredients assimilate into “oneness”. The salad bowl
notion celebrates diversity, as it notes that all the ingredients maintain their
characteristic features but contribute to the final product with the goodness
of the salad being the result of all the different ingredients of which it is
made up. The focus of inclusion therefore should no longer be on the
“specialness” of the children and/or the education that they need, but rather
on increasing participation by the removal of barriers (the so-called barriers
to learning) in order for them to reach their full potential. Beukelman and
Mirenda (2013) describe both opportunity and access barriers in their
Participation Model. Opportunity barriers refer to those barriers imposed by
people other than the individual with the disability, such as policies and
certain educational practices, as well as knowledge, skills and attitudes.
Access barriers, on the other hand, refer to the capabilities, attitudes and
resource limitations of the persons with disabilities themselves, and can
include aspects such as poor language competence and delayed literacy
exposure. These barriers are described in more detail in Chapter 2.
Figure 1.1 Inclusion is about accepting difference
In summary, the move towards including children with disabilities into local
schools, the notion that “unknown is unloved”, and teachers who have had
little or no previous training in differentiated teaching present new
challenges. A general lack of support and resources, as well as the
prevailing negative attitudes towards disability, all contribute to the general
bewilderment in South African schools towards inclusion.
1.3 HOW IS INCLUSION CURRENTLY BEING
ADDRESSED?
As all teachers know, any one training approach has certain advantages and
disadvantages. At present, the majority of programmes used to equip
teachers to deal with inclusion rely on knowledge and skills training as well
as on the establishment of collaborative teams. While both of these
approaches are valuable, a third possibility, namely the use of narratives
(telling stories), will be explored.
1.3.1 Knowledge and skills training approach
The first and most obvious method is through the implementation of skills
training programmes. Many South African teachers can testify to
participating in different programmes of this type, for example the Sisonke
project, the Policy on Screening, Identification, Assessment and Support
(SIAS), and so on. However, these materials are not always accessible to
teachers, as some school administrators do not see the need for equipping
teachers with them. The focus of these knowledge and skills training
programmes is often on how teachers should improve their skills and
knowledge about inclusion and apply them within the classroom context,
without necessarily helping them to fully understand what is expected of
them. Research is showing that such teacher education programmes tend to
be fragmented and short term, lacking in-depth content knowledge
(Engelbrecht, Nel, Nel & Tlale, 2015). The ongoing structured programmes
provided try to meet teachers’ needs by focusing on multilevel instruction
so that teachers can prepare main lessons with variations that are responsive
to the individual needs of the different children, curriculum enrichment and
dealing with challenging behaviour. At grassroots level, however, teachers
are still experiencing difficulties in adapting the curriculum in order to
provide meaningful activities for children with disabilities and in
communicating with children with disabilities.
1.3.2 Collaborative team approach
The second method used to bring about inclusive schools is by creating
teams of parents and qualified professionals, which could include, among
others, therapists, psychologists, learning support teachers and curriculum
specialists. Who makes up the team, how the team should function and
what roles it should play may, however, differ between the different districts
and provinces in South Africa, depending on the resources available. In a
developing country, therapists might not be available and therefore the team
might simply consist of more experienced teachers who act as mentors.
Likewise, in an optimal situation the team should be competent together as
assessors, researchers and evaluators, general learning support facilitators,
specialist learning support facilitators, material developers, and health and
welfare workers, as well as counsellors (National Department of Education,
2007). In a developing country context such as South Africa, where a high
proportion of teachers have limited qualifications, this can be unrealistic.
Research has shown that, relative to rural schools, urban schools tend to
have better-qualified and more experienced teachers, and that teachers in
rural schools often work solitarily and without much material or human
support (Gardiner, 2008). Owing to the inequality of teacher training in the
apartheid era, a number of teachers’ qualifications have become obsolete,
and teachers with such qualifications are now regarded as under- or
unqualified. This refers mostly to those who have less than a senior
certificate examination pass (12 years of formal schooling) and a three-year
teaching diploma or degree. Despite enormous strides in reducing the
number of unqualified teachers (those who have only a Grade 12
qualification), there were 7 076 unqualified teachers on the Department of
Education’s payroll in 2013 (Hawker, 2013).
In addition to the district-based support teams (DBST), regular teachers
should therefore be empowered with knowledge and skills regarding
flexible and individualised instruction and assessment (differentiated
teaching) if they are to be able to teach in an inclusive classroom. This is in
line with the thinking that practice might best be developed “bit by bit in
the light of experience and insight” (Green, 2004). In other words, teachers
are not required to have all the knowledge and skills when they start
teaching, but they should develop new skills, which they can then translate
into classroom strategies. In South Africa, this is exactly what the
Department of Education proposes as a means of building capacity while
implementing inclusion.
This training model does not, however, negate the fact that specialist
knowledge is required, but rather supports the notion that collaborative
teamwork can empower teachers over time to handle specific situations.
The range of knowledge and skills that these teachers require is vast and
includes aspects related to
the children with the disabilities, and their abilities and needs
the various types of assistive devices that might be used (e.g.
augmentative and alternative communication systems, hearing aids,
electric wheelchairs)
the provision of differentiated learning opportunities for all the children
in a class (e.g. through curriculum adaptation and management of the
academic workload)
the preparation of typically developing children for the fact that a peer
with a disability will join the class in order to facilitate integrated play
and participation, and to instil a true sense of belonging in the classroom
for everyone.
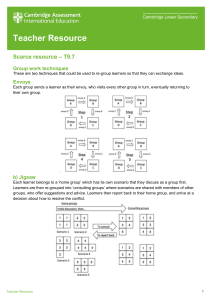
Another strategy that has become increasingly popular in inclusive
classrooms in many high-income countries is co-teaching, where the
classroom teacher is supported by a teacher trained in special education
(Solis, Vaughn, Swanson & McCulley, 2012). Five different evidence-based
co-teaching models have been described by Ford (2013):
1. One teach, one assist: here one teacher is responsible for teaching all
learners while the second teacher provides additional, focused support
for those learners who need it.
2. Station teaching: here learners are divided into three separate groups
who all work on the same activity: one group works with the classroom
teacher and one group works with the special education teacher while
the third group has independent work time.
3. Parallel teaching: here teachers plan lessons together before dividing
the learners into two groups, which are then both taught the same
lesson.
4. Alternative teaching: here one teacher is responsible for teaching and
the other for pre-teaching and re-teaching concepts to those learners
who need additional support.
5. Team teaching: here teachers provide instruction together in the same
classroom. They may take turns to lead instruction (teaching content)
and to model learner behaviour (e.g. how to take notes or ask questions
appropriately).
1.3.3 Narrative approach
The method for training teachers to meet the needs of the inclusive
classroom that is advocated in this book is that of using a narrative
approach; in other words, telling stories (about inclusion) that could both
inspire actions and raise questions (Cousins & Bissar, 2012). Teachers are
continuously in the midst of a blend of theory (their evolving ideas and
personal belief systems) and practice (their ability to teach and then reflect
on their own work), and narratives might possibly be the most natural way
for them to make sense of their work and lives (Marlowe & Disney, 2006).
The impact of perceptions and attitudes on teachers’ abilities to fully
understand inclusion is important. Consequently, a more effective and
sustainable approach to training might be to focus on where teachers are in
terms of their own beliefs and education experiences, emphasising life
stories and unravelling beliefs rather than focusing only on knowledge and
skills. Asking teachers to tell their own stories about inclusion thus gives
access to personal and idiosyncratic understanding, as it emphasises the
human understanding of inclusion, and therefore they will be asked to do
this throughout. Torey Hayden is a prime example of a teacher who writes
non-fiction first-person accounts of teaching and working with children
who face a range of educational barriers. Her narratives offer readers a real
look into the joys, challenges and struggles teachers and children alike face
in modern-day classrooms, while simultaneously offering hope and joy by
sharing some of the breakthroughs she has made (Hayden, 2012; 2014).
Inclusion is therefore not simply seen as an externally driven process, but
rather as something that impacts on individual lives. One of the major
factors that influences teachers’ views on inclusion is their own personal
experiences – these individual understandings are crucial in the
interpretation and translation of policy into practice (Bornman & Donohue,
2013; Donohue & Bornman, 2014a; Lawson et al., 2006). Teachers’
attitudes toward inclusion might be more positive if, along with training,
they received the appropriate service supports for their learners with
disabilities (Donohue & Bornman, 2014b). These supports depend on the
particular learner’s needs, and may include special equipment (e.g. a
speech-generating device or hearing aids), educational provisions and
accommodations (e.g. more time during test assessments), or a teacher’s
aide to help provide the learner with a disability more intensive, one-on-one
instruction.
1.4 WHO SHOULD BE INVOLVED IN INCLUSION?
It would be an oversimplification to think that inclusion is only about
teachers and learners. Many other role players are equally important, for
example school administrators, parents and school governing bodies
(SGBs). However, as this book focuses on the classroom, the role of the
teacher is described in more detail.
Inclusion is broader than just the teacher and the learner, as children are
influenced by their environment, and vice versa. In his bio-ecological
model, based on the ecological systems theory of development,
Bronfenbrenner (1999) describes the influences of the surrounding
environment on an individual and how this environment comes to influence
development. The environment and the individual’s specific characteristics
appear to work in tandem to influence personal development. In the bioecological model, the context is described by means of different systems of
influence that occur at specific levels, namely
the microsystem (this level is the closest to the child and his immediate
environment and thus includes him, his parents and his siblings)
the mesosystem (this level does not describe specific people, but rather
the communication and relationships between the people in the
microsystems, for example meetings between teachers and parents)
the exosystem (this level describes the contexts that do not involve the
child, but affects him nonetheless, like the parents’ workplace or school
policies developed by the SGB)
the macrosystem (this level is the furthest away from the child, and
denotes societal and cultural beliefs and values)
the chronosystem (this level represents the changes that occur over time
in any of the systems).
In a study conducted in the Eastern Cape, the researchers reported that the
implementation of inclusive education was seriously hampered by a lack of
preparedness of the role players at the different levels of the system, the
non-functioning or unavailability of support structures as a result of
inappropriate training, as well as a reluctance of role players to embrace
inclusion within the five levels represented in the bio-ecological systems
model (Geldenhuys & Wevers, 2013).
Similar to the bio-ecological model, and applied to the field of education, is
the ecosystemic perspective, which distinguishes between the following
levels (Donald, Lazarus & Lolwana, 2010):
The entire social system
The wider community
The local community (which includes local institutions such as libraries,
clinics, parks, hospitals and schools, as well as citizen associations such
as churches, non-governmental organisations (NGOs) and various
cultural groups, and also families and the peer group)
The individual
As with the bio-ecological model, the ecosystemic perspective emphasises
that all levels of the system should be seen as constantly developing and
interacting with one another in a reciprocal manner over time. This is also
the model that underpins the asset-based approach advocated by Ebersöhn
and Eloff (2006).
For the purpose of this book, a zoom lens metaphor will be used to illustrate
the bio-ecological and ecosystemic models (see Figure 1.2). Inclusion is
viewed as a series of three snapshots that depict different views of the
process. This emphasises the concept of holism as the child is regarded as
part of the community at large as well as part of the school context and
home. In other words, the zoom lens metaphor is capable of providing
increasingly refined pictures of the inclusion process that move from the
child in the community to the child in the home. It is important to note that
these lenses do not represent a linear progression, but attempt to engender
awareness of different angles at all times, therefore they encourage a
constant zooming in and out in order to understand each aspect and to note
that one cannot see a single aspect without being aware of the others.
Each of these lenses will now be explored in more detail, starting with the
wide-angle lens.
Figure 1.2 Zoom lens model
1.4.1 Wide-angle lens: the child in the community context
WHAT IS THE ROLE OF THE COMMUNITY?
Inclusion goes beyond the classroom – it goes straight to the heart of how
we as a community of human beings wish to live with one another
(Cologon, 2010). The community in which a school is situated should
therefore take ownership of that school, and at the same time the school
should aim to utilise all the possible resources in the community (Herd,
2008). In rural areas in particular, research has shown that for development
strategies to be sustainable, they need to integrate both educational issues
and community participation (Nelson Mandela Foundation, 2005).
Mnqagayi School is an example of such a school and is seen as a beacon of
hope in a busy, developing rural village. This school took over an unused
church building and initially had only four classes – from Grade 1 to Grade
4. After Grade 4, children had to commute to a nearby village, which led to
some of them dropping out of school because they could not afford to
commute every day. Through the efforts of the community members, the
school has been extended to Grade 7, and as a result of community
involvement, the government has provided furniture (Nelson Mandela
Foundation, 2005). The exciting fact is not only that the school is up and
running, but also that the church is back, using the school facilities.
Another example is to involve both children and community members in
creating gardens on the school grounds, as this has the benefit of making
the school environment more attractive. Children tend to respect and value
resources more if they find them appealing. Maintaining the garden also
develops skills and fosters commitment, and the produce (vegetables or
flowers) can be sold within the school and the community. This not only
creates strong links between the school and the community, but also builds
a sense of social connection.
Figure 1.3 Community involvement in action
On the other hand, schools can be used for a whole range of purposes other
than schooling, and these are often vitally important for the further
education of adults. Principals have reported that some schools use their
premises for meetings (47%), ABET learning centres (31%), public health
programmes (20%), private functions (16%), polling stations (12%), shelter
(3%), and other purposes (Nelson Mandela Foundation, 2005).
1.4.2 Regular lens: the child in the school context
WHAT IS THE ROLE OF SCHOOL MANAGEMENT TEAM?
The school management team includes the principal, vice principal(s) and
heads of departments (HoDs), as well as people from the district office.
They are responsible for decision making, the development of policies and
the implementation of these decisions and policies. In most schools,
principals are responsible for the school vision and the school’s position
regarding inclusion (Clifford, Menon, Gangi, Condon, & Hornung, 2012).
Their belief in and commitment to inclusion are critical, as they have to
decide on financing, the way services are delivered, the placement of
children in the classes and the in-service teacher training needs, among
other things.
In all schools, the school principals are central figures, with multifaceted
tasks and responsibilities: they teach with their colleagues (in all but the
biggest schools), implement curricula, develop and action management
criteria, and take account of the norms and preferences of the local
community (Nelson Mandela Foundation, 2005). The principal thus plays a
pivotal role in formal and informal interactions between the school and the
community. Research has shown that factors related to the principal were
more influential than child factors or educational environment factors with
regard to teachers’ attitudes toward inclusion (Fazal, 2012). “The best
support for inclusive practice is to have belief and support from the top
(principal and executive)” (a teacher, quoted by Shaddock, Giorcelli &
Smith, 2007: 4). Furthermore, principals were more likely to accept
inclusion if they had training and knowledge of disabilities, or held positive
beliefs about inclusion practices (Fazal, 2012).
Unfortunately, research in the Eastern Cape showed that principals
expressed a negative attitude towards inclusion (Geldenhuys & Wevers,
2013). Instead of being advocates for inclusion, they stated that there was
an urgent need for these learners to be removed from mainstream classes
and to be educated separately in special schools. Considering the systems
theory approach to inclusion, it is thus evident that these negative attitudes
have a ripple effect on the way inclusion is implemented.
Education officials at provincial and district offices have a critically
important role in the provision of back-up and appropriate support to
schools, principals and teachers. At present, many DBSTs are still in the
process of developing and implementing the support structures required by
teachers on the ground.
WHAT IS THE ROLE OF TEACHERS?
In inclusive classrooms, teachers require diverse knowledge and skills. The
focus should be on good teaching practices for all children by emphasising
commonalities rather than differences, although this too may be required as
children enter the classrooms (Hougaard, 2007).
Simon Herd (2008), a teacher and head of a middle school, suggests that
“turn-around teachers” are needed to drive inclusion – those who move
beyond telling it like it is, but who are telling it like it could be! These are
teachers who are motivated to see each child as an individual with
particular strengths and skills, regardless of the specific circumstances (e.g.
poverty, HIV/AIDS or disability) that may cloud the opportunities given to
the child. The child’s strengths should be used as the starting point for
learning.
Stop and reflect
Can you remember one of your own teachers who believed in you, for whom you
would walk the extra mile and work extra hard? Can you still remember how it
warmed your heart to know that that teacher thought you were special? Maybe it was
even that teacher who inspired you to become a teacher?
Turn-around teachers are creative and have a clear vision of what they want
to achieve and therefore they do not feel trapped in a pedagogy of chalk and
talk only. In this pedagogy, teachers talk while children have to concentrate
and listen, or teachers write volumes of basic information on the blackboard
for children to copy. Both of these teaching practices limit opportunities for
getting individual children to participate and learn in the classroom.
Throughout this book we will explore more creative ways of reaching all
the children in the class, and for creating classrooms that are interesting
(e.g. by displaying examples of work made by the children) and that
provide engaging learning opportunities.
Although it is true to say that all teachers have existing skills and tools in
their toolkits, it is equally true that in order to be or to become turn-around
teachers they require additional skills. Multiskilling refers to the attainment
of supplementary task-related skills and knowledge that empower an
individual to perform a broader range of tasks and functions in two or more
disciplines (Nicolaides, 2013). For teachers, this is not a new concept, as
the classrooms of the 21st century require them to function across a broad
range of activities. The Norms and Standards for Educators (National
Department of Education, 2009) highlights main roles, namely that of
learning mediator; interpreter and designer of learning programmes and
materials; leader, administrator and manager; scholar, researcher and
lifelong learner; community, citizenship and pastoral role player; assessor;
and finally learning area, subject, discipline or phase specialist.
Multiskilling is much more than simply transforming teachers into “jacks of
all trades”. It offers opportunities for job expansion and job enrichment in
the shape of new or expanded roles and responsibilities, skill sets and job
titles, and it usually implies in-service training rather than formal education.
It does not mean the loss of professional identity (teaching) nor does it
imply the demise of specialists (e.g. therapists, school nurses).
Opportunities exist for all teachers to maintain their professional identity
and at the same time develop or expand their roles and skills sets
(Nicolaides, 2013). Multiskilling can thus be seen as one possible initiative
whereby teachers are equipped with skills to deal with a wider range of
challenges that confront them in inclusive classrooms when having to
deliver high-quality education to all learners, irrespective of gender,
language, ability, and so on.
In the literature, four multiskilling levels have been identified (Bornman &
Uys, 2005). These levels are used to group the dynamic and overlapping
teacher roles on the basis of the National Department of Education’s (2003)
guidelines, and the Norms and Standards for Educators (2009) into a
theoretical framework (see Figure 1.4).
Figure 1.4 Teacher role diversification
The first multiskilling level is where teachers are required to support
children’s wellbeing in order to optimise learning. It entails two critical
roles – collaborative and pastoral:
Collaborative role. This is seen at many different levels, not only with
fellow teachers, school administrators and various people at the district
level, but also with parents and other community members. Research
shows that parents are more at ease with a teacher who has a pleasant
manner, who is knowledgeable about their child, who treats them as
equals, who involves them in decision making and who gives specific
and practical guidelines for addressing the child’s needs (Westling &
Fox, 2009).
Pastoral role. This requires teachers to have a thorough understanding of
the families and communities of the children they serve, as this reflects
psychosocial issues beyond teaching and learning functions (Ebersöhn,
Ferreira & Mnguni, 2008). The need for pastoral support such as
providing affection and attention, and facilitating a sense of personal
identity and social correctness is critical in countries such as South Africa
where children are losing their parents, siblings and other loved ones
(UNICEF, 2003).
At the second multiskilling level (professional, non-teaching roles) the
teacher has the role of scholar, researcher and lifelong learner:
Scholar role. The National Department of Education (2003) requires all
teachers to develop a personal growth plan (PGP) that enables them to
develop and improve in particular areas.
Researcher role. Albeit very different from the other roles, this role is
equally important. It may include tasks such as identifying problem
areas; collecting, analysing and interpreting data; applying findings; and
evaluating, designing and conducting research.
Lifelong learner role. The Norms and Standards for Educators (National
Department of Education, 2009) encourages teachers to aim for ongoing
academic and personal growth in broader professional and educational
matters.
At the third multiskilling level (administrative roles), teachers have to act
primarily as leaders, administrators and managers:
Leadership role. This manifests in the teacher’s relationship with parents,
children and the school community at large, and influences the overall
ethos and climate of teaching and learning at a particular school. As such,
teachers are vital role models, but in their everyday practices and
language they can also reinforce prejudice, discrimination and sexism
(Nelson Mandela Foundation, 2005).
Administrator role. All teachers should be responsible for record keeping
and report writing.
School manager role. Teachers in senior positions can be role models and
inspire others. They can build commitment and confidence as they give
direction and facilitate skills development. Furthermore, school managers
should be able to administer the different management processes
efficiently and effectively (e.g. preparing strategic plans).
Finally, at the fourth multiskilling level (advanced and specialised
teaching roles), the teacher’s main roles entail
acting as a learning mediator
interpreting and designing learning programmes and materials
(curriculum)
being an assessor
becoming a learning area/subject/discipline or phase specialist.
At this level it is expected that teachers can move beyond their basic
training and apply their teaching skills creatively. It requires them to be able
to observe individual strengths and potential problems in all learners and
then plan appropriate curricula for all the children in their classrooms. The
fourth multiskilling level is the focus of this book.
Multiskilling, if carried out effectively, will empower teachers and motivate
them to offer superior-quality teaching to all learners in their classrooms.
1.4.3 Close-up lens: the child in the home context
In much the same way as a classroom can constitute a comprehensive
context for a child, so can the home context. Teachers would therefore need
to look closely at the abilities, resources, protective factors and needs of the
child within the broader home context. By considering the home context,
teachers will be able to form a broader, more comprehensive picture of the
individual child.
WHAT IS THE ROLE OF PARENTS?
Teachers sometimes feel uncertain about the boundaries of their role and the
role of the parents (or caregivers). The teacher’s primary task is to educate
children, never losing sight of the child as part of a family in a community.
Most parents feel that it is their role to support their children with
schooling, but find it difficult for a variety of reasons. Melodie Hougaard, a
physician at the Johannesburg Hospital and parent of a child with barriers to
learning explains that from her personal experience, her belief is that each
parent would wish to be involved, cherished and appreciated in a school in
their community that recognises that all have the right to belong. She
highlights that this requires of schools to make the necessary
accommodations and that people change their perceptions and prejudices
(Hougaard, 2007).
How should teachers capitalise on the desire most parents have for wanting
the best for their children? Teachers should acknowledge that parents play a
critical role in reinforcing what the child has learnt, for example teachers
teach academic content in a classroom context while parents have the
opportunity to teach in real-life situations.
Stop and reflect
If children have learnt about “evaporation” at school, and can then have the
opportunity at home to see what happens when the kettle boils and the water turns
into steam, a rich learning opportunity is created.
Naturally occurring learning opportunities happen almost spontaneously
with typically developing children, but for children with disabilities it
involves more planning and effort (Beukelman & Mirenda, 2013. Turnaround teachers are skilled in encouraging parents to participate in school
activities without being threatened by them.
Although many parents have a strong belief in education and understand the
need for involvement with the school and a sound relationship with the
teachers, the reality is that many parents hardly ever (or never) set foot on
the school grounds. This leads to teachers feeling that parents do not
adequately cooperate with the school. We should, however, try to
understand why this happens. Some reasons might be that parents are not
literate themselves, or they might be embarrassed about their financial state,
non-payment of school fees and unfamiliarity with the school system
(Nelson Mandela Foundation, 2005). Parents might feel intimidated by their
child’s teacher (or even fear the teacher). Unfortunately, this fear creates an
uneasy working relationship that will not benefit the specific child (Lehohla
& Hlalele, 2012). Furthermore, research has shown that people in distress
do not want to make social contact – they are too emotionally drained to be
confronted by other people (and possibly more problems) (Westling & Fox,
2009). Situations like this challenge teachers to think of creative ways in
which to involve these parents in a supportive and undemanding way,
without disempowering them more by giving the kind of assistance that
makes them even more dependent. Teachers should guard against solving
all problems for families; they should rather encourage families to explore
ways of solving their own problems. This type of support is in line with the
asset-based approach and zoom lens metaphor that guide the underlying
philosophy of this book. The asset-based approach is strength based, and
uses all assets, resources, capacities and strengths when dealing with
challenges and providing support (Ebersöhn & Eloff, 2006).
While many parents of typically developing children are totally unaware of
the government’s policies and individual schools’ practices, the Education
White Paper 6 is a huge step forward for many parents of children with
disabilities. These parents are integral in selecting a school for their child
and for partnering with teachers to facilitate learning.
From the moment their children are born, parents have to act as advocates
for them. This would include representing the rights of their children at
local and national levels, giving talks, arranging community awareness
raising projects – tasks that they most probably were not familiar with but
that they quickly had to learn. Parents of all children would agree that they
want a “good life” for their children – that they should be happy, have
friends and develop their unique potential (Giangreco, Cloniger & Iverson,
2011; Matt, 2014). For some children this potential might be academic
skills, for some it might be functional academic skills (e.g. basic literacy
skills) and for others it might be functional skills such as domestic and
vocational skills. As parents and teachers may have different ideas about
what the educational goals for a particular child may be, effective
communication between parents and teachers is essential. Teachers must
consider those skills that are perceived by parents as relevant for their
children, and work towards the goal.
Stop and reflect
Max’s teacher is teaching him to roll a ball. His father thinks this is an unnecessary
skill; his immediate goal is that Max learns to put on his shoes. The teacher explains
to him that she is working on hand–eye coordination and bringing Max’s hands
together in the midline. The skills learned in the ball game can later be used for
putting on shoes – the father’s goal.
Initially the teacher must avoid being critical, as it is important to recognise
that parents generally know what is best for their children (Westling & Fox,
2009). Instead of sitting on the sidelines and being called to school to be
informed of decisions regarding their child, parents should actually
participate in decision making (Lehohla & Hlalele, 2012). In a research
study, parents of children with disabilities acknowledged that one of their
greatest concerns and worries about the future was related to the attitudes of
teachers and other professionals about the competencies of their children
(Giangreco et al., 2011).
Parents’ dreams and wishes for their children are called “valued life
outcomes” and should be pursued by teachers. The valued life outcomes
that parents have for their children (Giangreco et al., 2011) were as relevant
a decade ago as they are now:
Being safe and healthy
Having a safe and stable home in which to live (now and in the future)
Developing and maintaining meaningful relationships (a well-established
social network)
Being able to make meaningful choices and decisions
Participating in functional activities in various places
Culture impacts significantly on these valued life outcomes. A mismatch in
opinion between parents and teachers with regard to the goals of education
can also be expected if parents and teachers come from different cultural
backgrounds and hence have different perspectives. Cultural diversity is not
a negative aspect, but should be seen as an opportunity for growth, as
experienced by South Africa’s “Rainbow Nation”. Teacher training should
equip all teachers with the necessary skills to achieve cultural competence
(i.e. cross-cultural competence, intercultural effectiveness, cultural
responsiveness or ethnic competence (Lynch & Hanson, 2013)). This means
that teachers should have the ability to think, feel and act in ways that
acknowledge, respect and build upon ethnic, cultural and linguistic diversity
because cultural beliefs, traditions and practices may limit tolerance of
others and cause conflict with those who do not share the same culture
(Lynch & Hanson, 2013), Teachers need the ability to respond optimally to
all children, understanding both the richness and the limitations of the
sociocultural contexts in which they and their families operate, as well as
their own context and background. Cultural competence does not mean
knowing everything about every culture, but is rather a respect for
difference, an eagerness to learn and a willingness to accept that there are
many ways of viewing the world (Lynch & Hanson, 2013). Two teacher
characteristics are, however, essential: first, an openness to listen, learn and
change, and second, a commitment to engage in reflective practice.
Furthermore, culture, although important, is not the only variable that
results in a mismatch between parents and teachers – socioeconomic status,
educational experience, religion, gender, age and worldview all influence
who we are and how we perceive the world (Lynch & Hanson, 2013).
Westling and Fox (2009) give some valuable guidelines for working with
parents and families who come from a different cultural background to your
own:
Develop self-awareness about your own cultural identity and recognise
your own values, beliefs and customs.
Appreciate the uniqueness of each family and remember that cultural
background is not the only factor impacting on how they live.
Try to understand the communication styles within different cultures.
Develop an awareness of cultural norms, for example whether or not they
make eye contact, rules about proximity and the amount of touching and
whether it is appropriate.
Be sensitive to parents’ previous experiences of teachers. Ask parents for
feedback to ensure mutual understanding.
Appreciate the different ways families communicate: some families talk a
lot, while others do not verbalise their feelings.
Parents also carry the overarching responsibility and are integral to ensuring
that their child feels nurtured and loved, as that is the basic premise for
learning. If a child experiences success at home, this provides a positive
springboard for experiencing success in the classroom. Children who feel
safe and secure are more willing to participate in increasingly complex
learning challenges.
That said, how can parents practically be supported by teachers?
Set up an open line of communication. If teachers and parents share
information about a child, it is beneficial to all and therefore they should
strive to find a convenient way to communicate (e.g. face-to-face
meetings, text messaging via SMS or WhatsApp, telephone, e-mail, or
even a written note that can be sent between the home and the school).
Tap into community resources. Teachers can help parents by identifying
the various community agencies that can assist them. Parents are often
totally unaware of the types of support available in the community.
Teachers are a great help to parents when they make them aware of
community resources, for example how to access the library, church
groups and sports clubs.
Provide opportunities for parental support groups. Teachers can put
parents of children with similar problems in contact with each other so
that they can support each other. Research has shown that parents’
parenting skills improve as a result of participation in support groups,
their sense of isolation is reduced, they obtain important information
about services, and they feel a greater sense of emotional support
(Mandell & Salzer, 2007). Such groups are therefore critical to family
quality of life and wellbeing, and often also have the advantage of being
a safe place for parents to share experiences and help each other. Parents
can also be put in touch with formal support groups such as Autism SA,
Down Syndrome SA and others. (For a list of these support groups,
please look at the list of useful contacts at the end of this book.)
Formal training sessions. Teachers can present adult workshops at school
to help parents cope with their children at home.
To summarise, the responsibilities of the school and the parents are set out
in Table 1.1.
Table 1.1 School’s and parents’ responsibilities
School’s responsibilities
Parents’ responsibilities
Provide appropriate education up to 18
years of age.
Give consent for educational evaluation
and placement.
Ensure that assessment, assessment
materials and procedures and
interpretations are unbiased.
Cooperate with school and teachers as
equal partners and support school rules
and values.
Educate all children in the least-restrictive
environment.
Attend parent evenings, and teacher and
school meetings to discuss general
progress.
Ensure confidentiality of all children’s files
and records.
Reinforce procedures and school
practices (e.g. assist with homework).
Provide legal rights (constitutional and
education law) for all children.
Help maintain open communication with
school and teachers.
Provide opportunities for parental
involvement.
Become involved in school activities.
Source: Adapted from Mastropieri & Scruggs (2010)
WHAT IS THE ROLE OF SGBS?
Since 1994, South African parents have had the main legal responsibility
for their children’s education (Nelson Mandela Foundation, 2005). In an
attempt to give parents more rights in educational decision making (e.g.
about language, culture and/or the religious basis of the school), to
decentralise control and to ensure better governance at schools, formal
structures have been put in place. SGBs provide a powerful platform for
parent influence. According to the South African Schools Act (1996), SGBs
should be composed of parents, teachers, learners (in secondary schools)
and members of the school support staff. Their main task is to develop and
implement a school policy that safeguards the interests of all learners in the
school, and ensures that no learner is discriminated against on any grounds.
They therefore play a significant role in establishing inclusive practices in
schools. However, research revealed that SGBs are not really involved in
and concerned with the development of policies that support the
implementation of inclusion (Geldenhuys & Wevers, 2013). Transforming
parents’ legal rights to participate in education (via SGBs) into practice
remains an uphill battle.
WHAT IS THE ROLE OF THE OTHER LEARNERS IN THE CLASSROOM?
Classrooms are not just learning environments – they are much more, as
they are a cauldron of academic learning and social interaction. In
classrooms, children all have multiple roles to fulfil – they act as playmates
and friends, as fellow learners, as support systems, as “study buddies” and
as competitors. Positive peer pressure helps all learners to perform
optimally and develop new abilities.
Children with disabilities often do not have many friends, as it is not always
easy to communicate with them for a variety of reasons. However, if
children with disabilities are taught in their local communities and in
neighbouring schools with their peers, social relations will be strengthened
and socialisation will be further entrenched (Lehohla & Hlalele, 2012).
Peers have to be taught how to interact with these children, and different
strategies can be used, for example through didactic instruction (e.g. the
teacher can explain the disability to the class) or through more childfriendly approaches such as reading and/or telling stories that explain the
different disabilities in child-friendly terms (Bornman, Collins & Maines,
2005), modelling (the teacher can demonstrate the use of a communication
board during different activities) or through role play, where the teacher
assumes the role of the child with the disability so that the learners in the
class can practise interacting with a peer with disabilities in the class. All of
these strategies foster feelings of acceptance, individual value and
ultimately inclusion.
1.5 CONCLUSION
In this chapter we showed that inclusion is a broad term and described all
the efforts made by a school (teachers, principal and SGBs) and its
community to make all potential learners and their parents feel welcome
and valued. Structures and practices need to be put in place that will ensure
participation for all, irrespective of ability, gender, behaviour, culture,
economic status or any other reason.
We also explored some strategies and approaches that could be used when
attempting to establish an inclusive mindset and when becoming a turnaround teacher, such as using narratives and multiskilling, as an inclusive
school culture is one nurtured by constant teacher development. Individual
teachers and groups of teachers can bring about significant changes in their
schools and they need not wait until conditions are ideal to do so (Shaddock
et al., 2007).
In Chapter 2 we will be looking at participation.
REFERENCES
Beukelman, D.R. & Mirenda, P. 2013. Augmentative and alternative communication. Supporting
children and adults with complex communication needs, 4th ed. Baltimore: Paul H. Brookes.
Bornman, J., Collins, M. & Maines, B. 2005. Just the same inside! Understanding diversity and
supporting inclusion through circle time. London: Lucky Duck.
Bornman, J. & Donohue, D. 2013. South African teachers’ attitudes toward learners with barriers to
learning: attention-deficit and hyperactivity disorder and little or no functional speech. International
Journal of Disability, Development and Education, 60(2): 85–104.
doi/10.1080/1034912X.2013.786554
Bornman, J. & Uys, C.J.E. 2005. Multi-skilling in AAC intervention. In Alant, E. & Lloyd, L.L.
(Eds). Augmentative and alternative communication: beyond poverty. London: Whurr.
Bronfenbrenner, U. 1999. Environments in developmental perspectives: theoretical and operational
models. In Friedman, S. & Wachs, T. (Eds). Measuring environment across the life span. Washington
DC: American Psychological Association.
Clifford, M., Menon, R., Gangi, T., Condon, C. & Hornung, K. 2012. Measuring school climate for
gauging principal performance: a review of the validity and reliability of publicly accessible
measures. A quality school leadership issue brief. American Institutes for Research.
Cologon, K. 2010. Inclusion is really what teaching is. ARNEC Connections, 3: 45–48.
Cousins, S. & Bissar, D. 2012. Adapting to the digital age: a narrative approach. Research in
Learning Technology, 20. doi.org/10.3402/rlt.v20i0.18976
Crouch, L. & Perry, H. 2003. Educators. In Research Programme on Human Resources Development
(Human Sciences Research Council). Human resources developmental review 2003: education,
employment and skills in South Africa. Cape Town: HSRC Press.
Department of Education. 2001. Education White Paper 6. Special needs education: building an
inclusive education and training system. Pretoria: National Department of Education.
Donald, D., Lazarus, S. & Lolwana, P. 2010. Educational psychology in social context. Cape Town:
Oxford University Press.
Donohue, D.K. & Bornman, J. 2014a. South African teachers’ attitudes toward the inclusion of
learners with different abilities in mainstream classrooms. International Journal of Disability,
Development and Education, 62(1): 42–59.
Donohue, D.K. & Bornman, J. 2014b. The challenges of realizing inclusive education in South
Africa. South African Journal of Education, 34(2): 1–14.
Ebersöhn, L. & Eloff, I. 2006. Life skills & assets, 2nd ed. Pretoria: Van Schaik.
Ebersöhn, L., Ferreira, R. & Mnguni, M. 2008. Teachers’ use of memory-box-making to provide
psychosocial support in their pastoral role. Journal of Psychology in Africa, 18(3): 305–316.
Engelbrecht, P., Nel, M., Nel, N. & Tlale, D. 2015. Enacting understanding of inclusion in complex
contexts: classroom practices of South African teachers. South African Journal of Education, 35(3):
1–10. doi.org/10.15700/SAJE.V35N3A1074
Fazal, R. 2012. Readiness for Inclusion in Pakistani schools: perceptions of school administrators.
International Journal of Social Science & Education, 2(4): 825–832.
Ford, J. 2013. Educating students with learning disabilities in inclusive classrooms. Electronic
Journal for Inclusive Education, 3(1): 2.
Gardiner, M. 2008. Education in rural areas. Issues in education policy. Centre for Education Policy
Development (CEPD): Johannesburg
Geldenhuys J.L. & Wevers, N.J.E. 2013. Ecological aspects influencing the implementation of
inclusive education in mainstream primary schools in the Eastern Cape, South Africa. South African
Journal of Education, 33(3): 1–18.
Giangreco, M.F., Cloniger, C.J. & Iverson, V.S. 2011. Choosing outcomes & accommodations for
children: a guide to educational planning for students with disabilities. Baltimore: Paul H. Brookes.
Green, L. 2004. Nurturing democratic virtues: educators’ practices. South African Journal of
Education, 24(4): 254–259.
Hawker, D. 2013. Thousands of unqualified teachers are teaching SA children. ENCA. Available at:
https://www.enca.com/south-africa/thousands-unqualified-teachers-sa-schools
Hayden, T. 2012. Somebody else’s kids: they were problem children no one wanted … until one
teacher took them to her heart. New Zealand: Harper Collins.
Hayden, T. 2014. Silent boy and ghost girl 2-in-1 collection. New Zealand: Harper Collins.
Herd, S. 2008. Springboxed: engaging children through turnaround teachers. SAALED News, 28(4):
10–11.
Hougaard, M. 2007. The changing paradigm from inclusion to belonging. The Journal of Child and
Adolescent Mental Health, 19(2): iii–v.
Lawson, H., Parker, M. & Sikes, P. 2006. Seeking stories: reflections on a narrative approach to
researching understandings of inclusion. European Journal of Special Needs Education, 21(1): 55–
68.
Lehohla, M. & Hlalele, D. 2012. Inclusive classrooms: an ecosystemic perspective. Journal of
Human Ecology, 37(3): 189–201.
Lynch, E.W. & Hanson, M.J. 2013. Understanding families. Supportive approaches to diversity,
disability, and risk, 2nd ed. Baltimore: Paul H. Brookes.
Mandell, D.S. & Salzer, M.S. 2007. Who joins support groups among parents of children with
autism? Autism. The International Journal of Research and Practice, 11(2): 111–122.
doi.org/10.1177/1362361307077506
Marlowe, M. & Disney, G. 2006. Torey Hayden’s teacher lore: classroom behaviour management of
children with emotional and behavioural disorders. Teachers and Teaching: Theory and Practice,
12(3): 289–304.
Mastropieri, M.A. & Scruggs, T.E. 2010. The inclusive classroom: strategies for effective instruction,
4th ed. Upper Saddle River, NJ: Prentice Hall.
Matt, S.B. 2014. Perceptions of disability among caregivers of children with disabilities in
Nicaragua: implications for future opportunities and health care access. Disabilities Studies
Quarterly, 34(4): Matt DOI: http://dx.doi.org/10.18061/dsq.v34i4.3863
National Department of Education. 2003. Integrated quality management system: collective
agreement number 8 of 2003. Pretoria: Education Labour Relations Council.
National Department of Education. 2007. Guidelines to ensure quality education and support in
special schools and special school resource centres. Pretoria: National Department of Education.
National Department of Education. 2009. Norms and standards for educators.
http://www.policy.org.za/html/govdocs/notices/2000/not0082.html
Nelson Mandela Foundation. 2005. Emerging voices: a report on education in South African rural
communities. Pretoria: HSRC Press.
Nicolaides, A. 2013. The use of multiskilling in the southern African hospitality environment. Asian
Journal of Business and Management Sciences, 3(4): 64–83.
Shaddock, A., Giorcelli, L. & Smith, S. 2007. Students with disabilities in mainstream classrooms: a
resource for teachers. Canberra: Australian Government Department of Education, Employment and
Workplace Relations.
Solis, M., Vaughn, S., Swanson, E. & McCulley, L. 2012. Collaborative models of instruction: the
empirical foundation of inclusion and co-teaching. Psychology in the Schools, 49: 498–510.
South Africa. 1996. South African Schools Act. Pretoria, South Africa: Government Printer.
UNICEF. 2003. Africa’s orphaned generations. New York: UNICEF.
Westling, D.L. & Fox, L. 2009. Teaching students with severe disabilities, 4th ed. New Jersey:
Pearson.
2
Participation
In October of the year David turned six, his mother, Mrs Masambuku, went to register
him at the local primary school his older sister attends. She told the principal and
teachers that David was in a wheelchair and that, although he seemed to understand
everything, he had difficulty making himself understood. The school was reluctant to
accept the application. As she was familiar with the South African Schools Act
(SASA), Mrs Masambuku insisted that he be placed in the Grade 1 class. After the
first day of school the teacher, Mrs Mompei, burst into the headmaster’s office and
blurted out, “I don’t know where to start – he can’t even talk.”
2.1 INTRODUCTION
It is not difficult to identify with Mrs Mompei’s predicament. Often
teachers feel quite overwhelmed by the presence of children who, for one
reason or another, are “different” and often marginalised or excluded.
Consequently, many of these children are turned away from mainstream
schools and placed either in special schools or, more commonly, just stay at
home. At present it appears as if there are more than 500 000 children with
disabilities of school-going age who are not in the schooling system at all
(Martin, 2014). The Department of Basic Education budget (2014–2015)
for special schools was 12 times than that for inclusive schools, which calls
into question the commitment to inclusive education. There are many views
on inclusive versus special schools, but what cannot be denied is that there
need to be more and better-resourced inclusive schools, and that access to
special schools is very limited. The direct result is that many children with
disabilities have little or no access to formal education. The attitudinal and
knowledge-based barriers have to be addressed at the very highest levels of
policymaking and implementation, as well as in communities, homes and
schools (Donohue & Bornman, 2014a).
South African school statistics
30 055 schools and early childhood development centres
25 720 ordinary public and independent schools
3 759 early childhood development centres
448 special schools
Of these there are
791 ordinary public schools designated as full-service schools
80 special schools designated as resource centres.
Source: Department of Basic Education (May 2015)
The policy framework exists but there are significant problems with
implementation and consequently a large percentage of children with
disabilities are currently either completely excluded from compulsory
education, or unable to effectively access the curriculum in either special or
ordinary school settings (Department of Women, Children and People with
Disabilities, 2013).
The purpose of this chapter is to explore the opportunities, challenges and
creative approaches to education that will facilitate participatory learning
for all children within a single system.
In one way or another, teachers are always challenged by learner diversity
such as language, culture, religion, disability and learning styles. Disability
may be mild, moderate or severe. Severe disability is the term used to
describe an individual who needs long-term support in more than one major
activity of daily living, for example dressing, participating in activities and
mobility. For educational purposes, persons with severe disability are best
described in terms of the TASH (The Association for Persons with Severe
Handicaps – a human rights and advocacy organisation) definition as
individuals who are
…most likely for being excluded from society; perceived by
traditional service systems as most challenging; most likely to
have their rights abridged; most likely to be at risk for living,
working, playing and learning in segregated environments; least
likely to have the tools and opportunities necessary to advocate
on their behalf; and are most likely to need ongoing
individualized support to participate in inclusive communities and
enjoy a quality of life similar to that available to all people
(TASH, 2014, para. 6).
From this definition it is clear that TASH focuses on the relationship
between the individual within the environment (“adaptive fit”) and the
ongoing nature of support in life activities.
2.2 PARTICIPATION
Participation is broadly defined as “involvement in a life situation” (WHO,
2007). In other words, it is about involvement in daily life. It appears as if
participation has two important components: being there (Kramer, Olsen,
Mermelstein, Balcells & Liljenquist, 2012), and being engaged or involved
in an activity while being there (Imms, Reilly, Carlin & Dodd, 2008). It
follows that participation restrictions are those factors which limit or
preclude full engagement in the activities of daily living.
The school statistics reflect the slow pace of the implementation of
inclusion, which limits the full participation of children with disabilities in
their most formative years. The continuum from exclusion to inclusion
demands an array of supports that will dismantle barriers to participation.
The intensity and nature of these supports will vary according to the
abilities of the individual and the demands of a particular activity. As long
as the emphasis is on the individual’s strengths, the goal of functional
participation is attainable. Existing strengths can be used as a scaffold for
teaching and learning. Research has shown that interaction with adults (e.g.
parents and teachers) is one of the most critical features of a child’s learning
(Almqvist, Uys & Sandberg, 2007). Once an individual is engaged, the
focus moves from
disability to ability
child in isolation to child in community.
Parents of children with disabilities are frequently met with the question:
“Tell me about the problems. What is it that your child cannot do?” The
question of what the child can do often surprises even the parents who, by
the time the child reaches school-going age, have spent much time, effort
and expense trying to “fix” the problems identified by themselves,
therapists, doctors and others.
2.3 INCLUSIVE EDUCATION
At the heart of education is the conviction that children are able to acquire,
maintain and generalise the knowledge and skills that enable them to
develop their unique abilities in their homes, schools and community
environments, thereby becoming valued members of society.
“Inclusive education” is the term used to describe an education system in
which all learners are accepted and fully integrated, both educationally and
socially (see Figure 2.1). Inclusive education implies education for all and,
according to UNESCO (2015),
…must take account of the needs of the poor and the
disadvantaged, including working children, remote rural dwellers
and nomads, ethnic and linguistic minorities, children, young
people and adults affected by HIV and AIDS, hunger and poor
health, and those with disabilities or special needs.
This document also underscores the fact that inclusive education should not
only respond and adapt to each learner’s needs, but that it should be
relevant to their society and respectful of culture.
Recent events in South Africa, and indeed in other parts of the world, have
produced yet more large groupings of vulnerable children whose families
have been displaced by xenophobia, wars and famines.
Figure 2.1 Inclusion means a sense of belonging in the community
It is important for teachers and parents, as well as for communities at local,
national and international levels, to realise that the move towards inclusion
is a process which has to be intentional. This movement began to gather
momentum only in the 1980s, and those involved in the first decades of the
21st century are really pioneers, shaping an educational future that
considers all learners equal. Freedom, dignity and equality, the core values
of the South African Constitution, provide the foundation for developing
inclusive societies of which inclusive schools are a vital part (South Africa,
1996a). Inclusive environments enhance the quality of life for all
individuals. UNESCO (2016) identified five major factors that have to
change in order for education to accommodate everyone:
Improving teacher effectiveness
Promoting learning-centred methodologies that emphasise hands-on,
experience-based, active and cooperative learning rather than the rote
learning of facts
Developing appropriate textbooks and learning materials
Ensuring that schools are safe and healthy for all children
Strengthening links with the community as relationships between
teachers, learners, parents and society are essential for developing
inclusive learning environments
In a recent study in Nicaragua with primary caregivers of children with
disabilities, one mother stated, “I want for her to be normal like my other
daughter, to go to school and everything, have a normal life”, while another
said, “For him to be happy and to learn a specialty and be able to maintain
himself and be independent” (Matt, 2014). This highlights the fact that
parents of children with disabilities want the same outcomes for their
children as those of children without disabilities.
What do teachers think? Matt Krause, a Grade 4 teacher in an inclusive
school, wrote about ten-year-old Nare:
A small person with huge impact. I can’t think of anyone who has
met Nare and whose life was not changed by simply meeting him.
There is no challenge to big and no obstacle to high. An
extraordinary little person. Nare went on an overnight tour with
the Grade 4 group and he was absorbed into the group as if he has
been part of them his whole life.
When school communities become inclusive, this implies that all
individuals are interdependent and valued; when children are treated
equally, they all benefit from the same opportunities (both formal and
informal). Once individuals are engaged, the scales are tipped in favour of
participation.
The word “participation” implies that an individual is purposefully involved
in activities and experiences across home, school and community
environments. It will become evident that although the school setting may
be the springboard for learning, opportunities to reinforce and use what is
learnt need to occur in all the child’s environments. This can only happen
when involved communities support teachers, parents and learners. There is
no substitute for community initiative and responsiveness. Unfortunately, it
is well known that children with disabilities participate less in activities
than their peers without disability (Anaby et al., 2014). Teachers, parents
and communities therefore need to take up the challenge and be proactive in
searching out community structures, and networking with individuals and
organisations that support inclusion.
2.4 LABELLING
The move towards inclusive education necessitates a shift in perceptions.
The process begins by perceiving all learners as potentially able and
creative. For this to become a reality, the focus must be on the child, for
example friendly, bright, challenging, mischievous, happy, sad, etc., and not
on the disability.
The diagnosis or “label” only serves to underline a child’s shortcomings. Of
course, diagnoses such as cerebral palsy, epilepsy, intellectual disability,
Down syndrome and, so forth, may be useful in certain circumstances, such
as when applying for a social grant; referring to the appropriate clinic;
justifying funding for a communication device, wheelchair, hearing aid, etc.
Words reflect and influence the way people think, and therefore it is
preferable to refer to a child with a disability as, for example, “a child with
autism” rather than an “autistic child”, and similarly “children with
disabilities” rather than “disabled children”. The distinction may appear
subtle but using the correct terminology puts the focus on the child rather
than on the disability. The critical factor in the classroom is not the
particular disability but rather the levels of support needed to enable each
child to participate fully. The core question: “What support does this child
need to facilitate learning?” will shift the focus from the complexities of
specific diagnoses to making adaptations and creating environments in
which learning can take place.
What does this mean for the teacher on the ground? It requires a paradigm
shift in attitude and action in terms of creating, together with other
stakeholders, nurturing environments in which all children can flourish.
Within this framework, teaching strategies can address cognitive and
communicative challenges, movement restrictions, sensory disabilities,
socio-emotional challenges, and more.
Stop and reflect
All children and young people of the world, with their individual strengths and
weaknesses, with their hopes and expectations, have the right to education. It is not
our education systems that have a right to certain types of children. Therefore, it is
the school system of a country that must be adjusted to meet the needs of all
children.
(B. Lindqvist, UN rapporteur, 1994)
The challenge may seem daunting and so it is for teachers on their own. The
support of a team of people who can share information and influence
decision making is often considered the determining factor for whether
inclusion will either succeed or fail. A team approach therefore implies
interaction among members to allow them to generate new ideas and realise
important goals – giving new meaning to the word “team” when treating it
as an acronym: Together Everyone Achieves More (Radić-Šestić,
Radovanović, Milanović-Dobrota, Slavkovic & Langović-Milićvić, 2013).
Teamwork and collaboration also find prominence in all-inclusive education
discussions and policy documents (Department of Education, 2001;
UNESCO, 2016).
2.5 COLLABORATIVE TEAMING
The different models of multidisciplinary or interdisciplinary teams are
extensively discussed in the literature (Bell, Corfield, Davies & Richardson,
2009; Beukelman & Mirenda, 2013; They all paint a picture of parents,
teachers, therapists, education support teams, medical teams, technology
experts, etc. getting together to plan and implement appropriate
programmes. That may indeed be the reality for schools where there are
abundant resources. However, for many schools, particularly those in lessresourced areas, the real issues are, for example, orphaned children,
overloaded teachers, few if any therapists, and infrequent or brief contact
with district-based support teams (DBSTs) and institution-level support
teams (ILSTs). The term “collaborative team” is probably more helpful and
inclusive, where team members (not necessarily paid or professional) are
drawn from the home, the school and the community. Collaborative teams
could include caregivers, teachers, siblings, friends, therapists, clinic sisters,
traditional healers, community-based health workers, members of nongovernmental organisations (NGOs), and others. Ideally, collaborative
teams should meet together but if this is not possible, creative ways of team
interaction and decision making should be explored. The challenge of
involving parents and caregivers is by no means unique to children with
disabilities, but they should always be considered core team members.
Establishing a common goal between teachers and families is central to
collaboration – when goals differ, collaboration is negatively affected,
ultimately impacting on the quality of education (Yeboah-Antwi et al.,
2013).
The initial challenge for the collaborative team is to describe an individual
with a disability based on his or her daily activities (i.e. the ability to
participate in them). In 2007, the World Health Organization (WHO)
addressed this issue in a document known as the International Classification
of Functioning, Disability and Health – Children and Youth (ICF-CY)
(WHO, 2007). In a nutshell, it moves away from the strong emphasis on the
medical diagnosis and consequently how to “fix” the individual (medical
model) to a framework that addresses the environmental and personal
factors that influence participation (social model). The narrow focus on “the
disability” or “the problem” has shifted to the broader aspects of
functionality and ability that already exist within the child’s and family’s
environments (Bornman & Almqvist, 2007). The responsibility of
dismantling barriers to participation falls on society rather than on the
individual.
The significance of the ICF-CY is that it considers the whole person, and
that participation patterns are evaluated across life’s domains. The ICF-CY
describes nine areas: learning and applying knowledge (learning and
thinking); general tasks and demands (ways of coping); communication;
mobility; self-care; domestic life; interpersonal interactions and
relationships; major life areas (work and education); and finally leisure,
which includes community, social and civic life (see Figure 2.2).
Figure 2.2 Activity and participation domains in the ICFCY
Source: Boa & Murphy (2007)
Stop and reflect
Is there a commonly held belief in South Africa that children with disabilities can
become literate and numerate, learn to think and problem solve, develop meaningful
relationships and be equipped for the workplace?
This is a profound question because if the answer is no, what would the point of
inclusion be?
2.6 PARTICIPATION AND LEARNING MODEL (PLM)
The participation and learning model (PLM) depicted in Figure 2.3 has its
origins not only in the ICF-CY but also in the participation model as
described by Beukelman and Mirenda (2013). It illustrates the symbiotic
relationship between the curriculum, assessment and learning. The efficacy
of teaching is wholly dependent on comprehensive assessment and the
development and implementation of an individual support plan (ISP) for the
child. In turn, the efficacy of assessment is determined by accurate
identification and reporting of what has been and is being learnt.
Figure 2.3 Participation and learning model
The PLM will be used as a framework for discussing the curriculum; the
impact of extrinsic and intrinsic factors (positive and negative) on
participation and learning; the process of assessment and goal setting; and
classroom settings and strategies.
2.6.1 Curriculum
Curriculum content and instruction should be adapted to facilitate
participation and learning. The teacher should guard against limiting or
“watering down” the desired outcome. Often children with disabilities are
described as passive, a state frequently referred to as “learned helplessness”
(Beukelman & Mirenda, 2013). This is the result of low expectations and
others doing things for children with disabilities which they could do for
themselves either independently or with some assistance. This may be well
meaning but the result can be disastrous. The challenge is to look at the
curriculum through the “eyes of the learner” rather than look at the learner
through the “eyes of the curriculum”. It is about seeing the bridges that are
already in place and planning how and where to build new ones (Figure
2.4). Differentiated teaching is a powerful way to dismantle barriers.
Figure 2.4 Building bridges
2.6.2 Factors that facilitate participation and learning
Educational texts often begin by identifying the barriers to learning. This is
true not only for individuals with complex needs but also for typically
developing learners. This “barrier-based” approach can be very
discouraging. There is no doubt that the barriers must be identified and
addressed, but the initial challenge is to focus on the abilities of the learner,
the support systems within the family and the community, and finally local
and national policies that facilitate teaching and learning (Rose & Alant,
2001). It is important that barriers do not become an “acceptable excuse”
for not striving to meet educational goals.
2.6.2.1 Policy that supports inclusion
In terms of policy, the move towards inclusion has a firm foundation in the
South African Constitution (1996a). The Bill of Rights states that
“everything must be done in the best interests of the child”. The South
African Schools Act (1996b) and the Education White Paper 6 (Department
of Education, 2001) are evidence of legislation giving flesh to the principles
of inclusion. That all children are equally deserving of education is no
longer debatable. In South Africa, significant resources have been allocated
to facilitate the process of equipping mainstream schools to admit and
support previously marginalised and excluded learners. Structures such as
district-based support teams (DBSTs) and institution-level support teams
(ILSTs) promote inclusive education by (i) facilitating visionary leadership
and training; (ii) putting in place coordinated school, learner and educator
support services; (iii) curriculum delivery; and (iv) the distribution of
resources. In spite of these support structures, it is evident that children with
disabilities are less likely to attend school than their typically developing
peers, and even if they do, the dropout rates are higher. Some of the special
schools, designated as special school resource centres, are equipped to
provide a range of support services to full-service (mainstream) schools.
The schools are in a process of change, but what does the future hold for
young learners? What about employment opportunities? The concept of
participation cannot have an arbitrary end point. Legislation such as the
Employment Equity Act (1998) opens doors for people with disabilities
(Department of Labour, 1998) in the job market. This is a crucial initiative
as for the 2013–2014 year, only 0,9 per cent of South Africa’s economically
active people were persons with disabilities (South Africa, 2015).
In addition, the White Paper on the Rights of Persons with Disabilities
(South Africa, 2015), which integrates South Africa’s 1997 White Paper on
an Integrated National Disability Strategy (INDS) with the UN’s
Convention on the Rights of Persons with Disabilities (CRPD) (UN, 2006)
was signed. The vision of this new White Paper is to create a free and just
society that is inclusive of all persons with disabilities as equal citizens. It is
built on nine strategic pillars:
Pillar 1: Removing barriers to access and participation
Pillar 2: Protecting the rights of persons at risk of compounded
marginalisation
Pillar 3: Supporting sustainable integrated community life
Pillar 4: Promoting and supporting the empowerment of children,
women, youth and persons with disabilities
Pillar 5: Reducing economic vulnerability and releasing human capital
Pillar 6: Strengthening the representative voice of persons with
disabilities
Pillar 7: Building disability-equitable state machinery
Pillar 8: Promoting international cooperation
Pillar 9: Monitoring and evaluation
This White Paper highlights the importance of the social model in
addressing disability; in other words, taking the environment into account.
It is also built on a rights-based foundation which attempts to mainstream
disability (also known as inclusion) and acknowledges the “life cycle” of
disability; in other words, acknowledging that the services provided to
children should continue as they grow and progress through various stages
of life. This is only achievable by incorporating empowerment and equality
as the cross-cutting themes in providing services to persons with
disabilities.
2.6.2.2 Practices that support inclusion
Practices are defined as customary or traditional ways of doing things.
Some examples of practices that support inclusion are the following:
Family-centred activities that make all family members, especially
parents or caregivers and siblings, feel accepted and valued
Teacher development programmes that provide both formal and informal
learning opportunities
School outreach programmes that provide opportunities for children
across the spectrum to get to know one another (this should be a two-way
process with typically developing children reaching out to their peers
with disabilities, and vice versa)
School outings that take children with disabilities into community
settings, for example parks, shops and restaurants
Shared activities with typically developing peers such as school plays,
concerts, outings, playgrounds, and so on
The use of sign language interpreters at gatherings such as public
meetings, churches, etc.
2.6.2.3 Attitudes that support inclusion
Attitudes involve three components, namely beliefs (the cognitive
component) that often attract strong feelings (the affective component) and
may then lead to specific actions (the behavioural component) (Hansen,
Harty & Bornman, 2016). Attitudes can be positively influenced by the
following:
Narratives. There is no match for the narrative or personal story in
changing attitudes (Lawson, Parker & Sikes, 2006). Stephen Hawking,
one of the world’s most renowned physicists, is totally dependent on an
augmentative and alternative communication (AAC) device to “speak”
for him, a computer to “write” for him and a powered wheelchair to
“move” for him. The 2014 movie about his life – The Theory of
Everything – was received very positively internationally, winning a
number of awards. In the movie, he gives an inspiring speech, saying,
“There should be no boundaries to human endeavor. We are all different.
However bad life may seem, there is always something you can do, and
succeed at. While there’s life, there is hope.”
Nkosi Johnson, the young AIDS activist who died when he was 12 years
old, spoke out about inclusion and acceptance not only locally but at
national and international gatherings. These are the visible heroes, but in
every community there are individuals with disabilities making their
mark, challenging and changing attitudes.
The following story of two South African teenagers – Lesedi, a youngster
with a severe physical disability and his friend Neo – is a vivid
illustration of “boys-will-be-boys” participation. Neo writes (personal
email correspondence):
Around that time my mother bought an Audi Q7 3.0 TDI Quattro® that Lesedi adored
with all his heart. As teenagers we were up to no good. One day we stole his father’s
Mercedes-Benz. What we did not check was the level of fuel in the car. We got stuck
in another suburb. We had left his wheelchair at home. It was me, Lesedi and Koti.
We could not leave him there and go home. So we slept in the car. My mother looked
for us the whole night in all suburbs of Polokwane until she found us the next day at
nine o’clock. She scolded us and took all of us to our homes after a serious lecture
on juvenile delinquency. Lesedi was just happy that he was in an Audi Q7. He kept
whispering “Quattro” throughout the whole way and I would just smile and look away
because I already knew the trouble awaiting me at home.
Quality of life is about belonging, having fun, believing in oneself and
being believed in by others, getting together with others and developing
independence (Bedell et al., 2013; Heah, Case, McGuire & Law, 2007).
Family initiatives. Families that involve others in their communities
generate hugely positive attitudes, especially when there are young
people involved. The South African story of the Mycroft family below is
a wonderful example of a group of young girls (supported by their
parents) who began fundraising for an electric wheelchair for Chaeli.
Stop and reflect
In April 2004, five young girls – Chaeli and Erin Mycroft, along with their lifelong
friends, the Terry sisters, Tarryn, Justine and Chelsea – started the “Chaeli
Campaign” to raise R20 000 for Chaeli’s motorised wheelchair. They did this in just
seven weeks. The Mycroft and Terry families then formalised this campaign as a nonprofit organisation focused on building the ability and potential of children with
disabilities in inclusive environments. In April 2012, Chaeli received a medal for
Social Activism at the Nobel Laureate Peace Summit. This organisation is unique in
its commitment to inclusion and youth empowerment. Their trendy website is worth
visiting and sharing: http://www.chaelicampaign.co.za/
Technology. The use of technology such as smartphones, iPads and other
tablets, computers, and AAC devices positively influences attitudes
because technological competence is highly regarded. It is a platform for
developing friendships, learning, social networking, accessing and
sharing information, leisure activities, and so much more.
Sharing lives. Participating in activities such as sponsored walks, picnics,
discos and soccer matches will often dispel unfounded fears and
uncertainties, and build bridges of acceptance.
2.6.2.4 Knowledge and skills that support inclusion
The move to inclusion is not happening in a vacuum. There are many
opportunities for formal and informal learning, such as the following:
Exposing children to narratives. One research project investigated the
effect of using a narrative approach combined with drawings to
determine Grade 1 children’s attitudes towards a peer with a disability
and also whether this approach might be useful in creating disability
awareness in children who had not previously been exposed to children
with disabilities (Bornman, 2006). Findings indicated positive attitudes
towards peers with disabilities, but also an awareness of their possible
social exclusion and isolation.
Formal learning opportunities. These are available to parents, teachers,
therapists, and others. They may be lecture or workshop based, presented
by tertiary institutions, government departments, non-governmental
organisations (NGOs), onsite or distance learning.
Informal learning. This happens when families, siblings, colleagues and
other members of the collaborative teams share ideas, skills and
knowledge. The importance of teaching children with disabilities and
their typically developing peers about disability cannot be
overemphasised. This could be facilitated by parents, therapists, teachers
or organisations such as Down Syndrome SA, Autism South Africa, the
Treatment Action Campaign (TAC), Epilepsy SA, and so on. There are
also some excellent websites such as http://kidshealth.org which explain
things in language children understand. These extracts illustrate just how
powerful information from the World Wide Web can be.
Example What is cerebral palsy?
Cerebral palsy (pronounced seh-re-brel pawl-zee) or CP is a condition that affects
thousands of babies and children each year. It is not contagious, which means you
cannot catch it from anyone who has it. It usually happens if the baby’s brain
development is disrupted inside the womb or it may come from a brain injury during
birth. The word cerebral means having to do with the brain. The word palsy means a
weakness or problem in the way a person moves or positions his or her body. A child
with CP has trouble controlling the muscles of the body. Normally, the brain tells the
rest of the body exactly what to do and when to do it, but because CP affects the brain,
a child may not be able to walk, talk, eat or play the way most children do, depending
on what part of the brain is affected.
Children with CP can have a mild, moderate or severe disability – it really depends on
how much of the brain is affected and which parts of the body that section of the brain
controls. If both arms and legs are affected, a child may need to use a wheelchair. If
only the legs are affected, a child might walk in an unsteady way, need adaptive
footwear or use crutches. If the part of the brain that controls speech is affected, a child
with CP may have trouble talking clearly or may not be able to speak at all.
Example What does autism mean?
Autism (pronounced aw-tih-zum) is what people usually call this condition, but the
official name is autism spectrum disorders, because doctors include autism in a group
of problems that children can have, including Asperger syndrome and others. These
problems happen when the brain develops differently and has trouble with an important
job: making sense of the world. Every day, our brains interpret (understand) the things
we see, smell, hear, taste, touch and experience, but when the brain has trouble
interpreting these things, talking, listening, understanding, playing and learning become
difficult.
A child’s symptoms could be mild, severe or somewhere in between. For example,
some children may be upset by too many noises or sounds that are too loud. Those
who have milder symptoms do not mind loud noises as much. Someone with mild
symptoms might need only a little bit of help, but a child with severe symptoms will
need a lot of help with learning and simply doing everyday things.
Children with autism often cannot make connections that other children make easily.
For example, when people smile, it usually means they feel happy or friendly; when
people are angry, it shows in their face or their voice, but many children who have
autism spectrum disorders have trouble understanding what emotions look like and
what another person is thinking. They may act in a way that seems unusual, and it can
be hard to understand why.
This kind of knowledge sharing is a core component of making inclusion
work.
2.6.2.5 Environments that support inclusion
There is a growing awareness of the need to make facilities universally
accessible, not only to those with physical disabilities. The notion of
universal design looks into designing products and environments that can
be used by all people, to the greatest extent possible, without adaptation or
specialised design (Centre for Universal Design, 2008). It is based on seven
principles:
Principle 1: Equitable use. This means the design should be useful to
people with different abilities. For example, ramps and curb cuts are not
only useful for people in wheelchairs but also for bikers and prams.
Lever handles are also easier to use than door knobs, irrespective of one’s
hand function.
Principle 2: Flexibility in use. This means that the design can
accommodate a wide range of individual preferences and abilities. For
example, traffic lights that “beep” do not only enable individuals with
visual disabilities to cross roads safely but benefit everyone.
Principle 3: Simple and intuitive use. This means that the design is
easy to understand, regardless of the user’s experience, knowledge,
language skills or current concentration level, for example infographics
regarding electricity use that are colour coded to show how much
electricity is being consumed (red, orange or green).
Principle 4: Perceptible information. This means that information is
communicated effectively to the user, regardless of ambient conditions or
the user’s sensory abilities, for example large flat light switches that can
easily turn on the power to illuminate a room.
Principle 5: Tolerance for error. This means that the design minimises
hazards and the adverse consequences of accidental or unintended
actions, for example showing the danger sign on paraffin containers or
electric fences.
Principle 6: Low physical effort. This means that the design can be
used efficiently and comfortably and with a minimum of fatigue, for
example travelators, escalators and lifts.
Principle 7: Size and space for approach and use. This means that the
size and space that is provided for approach, reach, manipulation and use
is appropriate, regardless of the user’s body size, posture or mobility, for
example wide interior doors and hallways. Likewise, careful
consideration should be given to the control panel in lifts, lowering the
height of the panel can make it accessible for individuals with dwarfism
and those in wheelchairs. Adding Braille and auditory feedback also
makes the panel accessible to individuals with visual impairments.
Universal design solutions help everyone, not only people with disabilities.
They make all areas of living and learning accessible to all. Now let us
consider the school environment. Where better to start than on the
playground? Is play, after all, not the work of children? Playgrounds can be
built for use by all children and made accessible by, for example, adapting
seats on swings and seesaws for children with physical disabilities, planting
a sensory garden with children with visual impairments in mind, etc.
2.6.2.6 Personal factors that support inclusion
Each individual brings unique strengths to living and learning. These will
be discussed in Chapter 3 when considering the assessment of children with
disabilities.
2.6.3 Barriers to learning
It is evident that there are many factors that support the learning process for
children with disabilities; however, there are often significant barriers, but it
should always be born in mind that a barrier is something that can be
overcome – it is not the end of the road. A barrier is never a reason to
abandon the inclusion plan for either an individual learner or the district as
a whole (Beukelman & Mirenda, 2013).
Barriers typically fall into two categories:
Environmental (extrinsic) barriers. These are those imposed by society
or the environment. They are known as opportunity barriers and cannot
be eliminated merely by the provision of specific supports; for example,
it is no use giving a child with cerebral palsy a computer if there is a
general belief that he will never have the skills to use it, or there is no
technical backup or power to charge it.
Personal (intrinsic) barriers. These are directly related to the individual
and his personal support systems. They are known as access barriers, and
refer to the limitations of the particular child and/or his support system.
It may be helpful to visualise these barriers as a house. Extrinsic refers to
the exterior (or outside) and intrinsic refers to the interior (or inside). Some
barriers may affect all learners equally, for example the school bus breaking
down, the school toilets being out of order, not having a school uniform,
inadequately trained teachers, and so on. Other barriers pertain only to
children with disabilities, for example inaccessible classrooms, a paucity of
learning supports and fewer learning opportunities.
2.6.3.1 Policy barriers
Policy barriers refer to the limitations of societies and support systems.
Regulated or legislated policy may be national (government legislation),
provincial (schools, clinics, hospitals) or local (communities). In South
Africa there are very progressive national policies, such as the South
African Schools Act (South Africa, 1996b) and Education White Paper 6
(Department of Education, 2001), which are in line with the Convention on
the Rights of Persons with Disability (UN, 2006), as well as the Convention
on the Rights of the Child (UN, 1989). Education is a fundamental “nonprogressive right”, making it immediately accessible. Economic and other
constraints can never be used as an excuse to deny access to education. All
children have a right to education now at the same time as challenges are
addressed and barriers dismantled (Huus, Dada, Bornman & Lygnegård,
2016). However, some local policies or rules may be restrictive and the
implementation unreliable.
2.6.3.2 Practice barriers
Practice barriers are unwritten rules and routines within families, schools
and communities that may limit opportunities for participation:
Admission to school may be turned down on the grounds that the child
will not benefit from the school programme.
Admission may be turned down on the grounds that the school is full.
A school wheelchair or communication device may not be taken home,
even for the holidays.
Children must be toilet trained before being accepted at school. Some
children with intellectual or developmental delays may take longer to
toilet train, and others with conditions such as spina bifida may never
develop bladder and bowel control.
A child may have to do chores at home or out in the fields before going
to school, sometimes resulting in absenteeism, being late for school,
fatigue, etc.
A child may need to take care of a sick parent or younger sibling.
2.6.3.3 Attitudinal barriers
Attitudinal barriers are opinions or beliefs that negatively affect
participation. Negative attitudes from adults and peers may result in low
self-esteem and low expectations in children with disabilities. Peer
discrimination and rejection often lead to the marginalisation of children
with disabilities (Beukelman & Mirenda, 2013). Several studies have
documented that children prefer peers who share similar characteristics (e.g.
gender, ethnicity and developmental status), and display a negative bias and
discrimination towards “different” peers such as those with disabilities
(Castelli, De Amicis & Sherman, 2007; Diamond & Tu, 2009). Children
with disabilities may be at higher risk for being victims of bullying (Flynt &
Morton, 2004). These attitudinal barriers are often the result of ignorance,
negative experience, use of language and deep-seated cultural beliefs, for
example:
Literacy skills are not important for children with intellectual disabilities.
Children who cannot speak intelligibly are deaf or “stupid”.
Children who have seizures are “bewitched”.
Hurtful words such as “defective”, “abnormal”, “damaged”, “ruined” and
“incapacitated” are used. Alternatives could be “challenged”, “limited”,
“uncommon”, “unusual” and “dissimilar”.
However, recent literature is building a strong evidence base to show that
the more intensive and regular contact children have with people with
disabilities (such as peers with disabilities in inclusive education), the more
positively children may feel about them (Hong, Kwon & Jeon, 2014).
2.6.3.4 Knowledge and skills barriers
Knowledge and skills barriers refer to inadequate knowledge and skills
levels of teachers, therapists, DBSTs and ILSTs. Lack of appropriate
training for teachers and other team members constitutes a major barrier to
inclusion (Donohue & Bornman, 2014b). These barriers can be difficult to
overcome as professionals will often say: “I won’t” rather than “I don’t
know how” (Beukelman & Mirenda, 2013). For families, the challenge of
gathering the relevant information and applying it to their child can be
overwhelming. Whether a child is born with a disability or becomes
disabled at a later stage, it is nearly always unexpected. Gathering and
assimilating information is a complex task. Very often the information is
confusing, conflicting and distressing. Sometimes statements made by
teachers, therapists and doctors make little sense to families and they are
often unable, or do not feel safe enough, to discuss their concerns. Some
examples follow:
: Your child will never talk.
: Does that mean he will never be able to tell me he loves me?
: Your child will probably not cope at high school.
: What will become of him (and me) if he can’t get work?
: Your child has autistic tendencies.
: That sounds scary. What does it mean?
: Don’t worry; you’re just an overanxious mother.
: Can he not see that this child is not like my other children?
: I have never had a child like this in my class.
: Does this mean you will not be able to cope with my child?
: Your child has problems because he does not get enough to eat.
: Does she not understand that I cannot find a job?
These are common scenarios that emphasise again and again the importance
of setting aside time to discuss parents’ concerns and build trusting
relationships. Knowledge acquisition is a lifelong process for teachers,
therapists and parents. In the past, mainstream and special-education
teachers were trained separately, which had a negative impact on both
groups. Teacher training should provide a foundational knowledge in both
general and special education (Donohue & Bornman, 2014b; Westling &
Fox, 2009). The acquisition of knowledge and skills is especially
challenging for teachers in rural or under-resourced schools because getting
to lectures or workshops may be difficult as transport is often unreliable and
expensive. Course content can be overwhelming, and frequently there are
inadequate resources and support structures to implement newly learned
strategies. Similarly, parents and therapists should actively engage in
knowledge building and skills development. Ideally, therapists should avoid
a “pull-out” therapy model where a child is taken out of the classroom to
receive one-on-one therapy in the therapist’s office and rather work with the
child, the teacher and the family in functional settings.
Environmental or extrinsic skills are those reflecting, among other things,
the expertise and competence of teachers and parents. Knowledge does not
necessarily translate into skills. Putting ideas or theory into practice can be
very challenging. In-service training and learning from the experience of
others are invaluable, especially where the demands may be varied and
complex, for example when teaching a child to use a communication device
such as a communication board or the GoTalk digital speaker (see Table
2.1).
Table 2.1 Example of a low-tech and a high-tech augmentative and alternative
communication device
Example of a communication board
(low-tech)
Example of the GoTalk digital speaker (hightech)
Example of a communication board
(low-tech)
Example of the GoTalk digital speaker (hightech)
Source: Go Talk 9 +™2
Source: Picture Communication Symbols™1
Pointing to the symbols on the
communication board will enable the
child to make himself understood.
Pressing the symbol on the digital speaker,
which has a pre-recorded message for each
symbol, will enable the child to “speak”.
1 Picture Communication Symbols (PCS) is a registered trademark of Mayer Johnson, a
Tobii Dynavox Company of Pittsburgh, PA (www.mayer-johnson.com).
2 The Go Talk 9 + is a product of the Attainment Company Inc. of Verona, WI
(www.attainmentcompany.com).
Parents and teachers must be able to model the use of these boards and
devices, and provide opportunities for functional use. Both systems require
the child to learn the meaning of the graphic symbols and then select the
ones he needs to use to communicate.
2.6.3.5 Physical barriers
Physical barriers refer to physical access as well as the freedom to move
about. Typical environmental barriers may include the following:
Inability to get to school because of expense, distance, rough terrain,
difficulties with getting on and off a school bus or a taxi. In addition,
some taxis will not take wheelchairs or demand an extra fare for doing
so.
Poor access to buildings and facilities (public and private).
Difficulty in manoeuvring in overcrowded schools and classrooms.
2.6.3.6 Personal barriers
Personal or intrinsic barriers are those within the child or in his personal
circumstances. There may be challenges in one or more of the skill areas
(cognitive, communication, motor, sensory, socio-emotional) and/or other
constraints, for example access to funding, family preferences, family
literacy levels, and so on.
Theoretically at least, the concept of inclusion seems to make sense, but
what is happening on the ground? Are there communities that are
embracing diversity? Are there schools where inclusion is becoming a
reality?
The Pathways story
The setting is Polokwane. Here there is a large special school that caters for children
with disabilities. There are difficulties teaching children with severe physical,
behavioural and intellectual challenges and in the end many are either turned away
or the parents remove them because little or no learning is taking place. There is a
paucity of local support, therapists are few and not only do most parents not attend
parents’ meetings but some children are more or less abandoned in hostel facilities.
Sound familiar?
So how does change happen – how do parents and communities begin to create
settings in which children will flourish? There are parents who yearn to have their
children accepted as part of the community, and there are children who need
opportunities to play and learn alongside their siblings, cousins and friends.
Some of the parents hear about a community-based organisation in KwaZulu-Natal
that has been working with a small group of children with severe disabilities –
children turned away by even the special schools and training centres, so they
decide to go and have a look. They come back to Polokwane with a vision in the
making – but as yet no money, no teachers, no premises … they name their school
Pathways and get going.
They approach a primary school teacher and share their dreams. She has no
experience with disability but has a firm belief that every child can and will learn. The
local church is approached to provide premises. Together, the parents and teacher
begin with a small group of children. Parents make financial contributions and
fundraising begins in earnest (no child is ever turned away for financial reasons). The
emphasis is on acceptance – of the child and his or her family. Gradually, social
interaction and learning begin to take place. They are all learning together and
interacting with the community in many different ways, for example
organising family days or events
encouraging local mainstream school groups to visit
visiting local mainstream schools
encouraging common activities – for example performing in a nativity play with
one of the local mainstream schools, going on outings
engaging volunteers from the community
engaging with local organisations such as churches, service organisations and
sports clubs, among others
taking the children shopping, to movies or to restaurants.
But there are difficulties to overcome: children who do not easily adapt to the school
environment; acquiring and adapting learning materials; family problems often made
more complex by issues of disability; difficulties in acquiring wheelchairs and other
assistive devices; training teachers, assistants and volunteers; accessing therapy
support; and many more. A start is made and issues are addressed systematically. A
dynamic individualised school programme is created in which there are opportunities
to participate in large groups, to learn in small groups and to receive one-on-one
instruction.
The most significant thing happening is that close ties with the community are being
forged. In particular, families are being supported and nurtured in small ways that are
not necessarily costly. For example, there is a safe place to discuss their concerns
with teachers and other parents, and they share practical tips on coping with the
activities of daily living such as dressing, feeding and toileting. Leisure and fun
activities provide places and spaces for families to relax.
After six years a local mainstream school, Mitchell House, invites Pathways to
participate in a full inclusion project. The motivation is twofold:
The wider community, having been exposed to learners in need of special support,
has come to accept them and their families as any other.
Mitchell House is building a new school campus and has glimpsed the possibility
of full inclusion. This vision will be one of the unique features of a forward-looking
school community.
Questions are raised on both sides. How are the children going to cope? How are the
teachers going to cope? How accepting will the parents of the typically developing
children be? Do they believe their own children’s education will be compromised? Are
the parents of Pathways afraid to move their children away from the nurturing small
group they know? At this point there has to be strong visionary leadership. A core of
parents and teachers must buy into the vision of dignity and equality for all learners.
However, there are problems, especially with parent involvement. The one or two
stalwarts are there (and have been from the beginning), but the others just hope that
whatever happens will be good for their children. Maybe they have run out of time,
energy and resources as they struggle with their lives. They are like many other
parent groups – hard to get involved – really involved, but the teachers don’t flag –
someone has to carry the vision.
The school is built with an Enrichment Centre, which will be the centre of the learner
support services. Some of the Pathways learners will spend most of their school day
in regular classrooms, others will have more time in the Enrichment Centre where
learning will take place. The learners become an integral part of school life:
All belong to an age-appropriate class and participate in assemblies, class outings
and sports days.
All the learners share playgrounds, libraries, and so on.
All the learners wear school uniforms.
The learners and their families are involved in every aspect of school life, for
example sports days, concerts, prize-givings, fundraising events, and helping to
repair books and other equipment.
Eight years have passed since the group began in the church hall, and significant
new challenges have arisen. Parents and teachers have been part of the learners’
growing years, some of whom are now young adults. What of their future? What have
their years in an inclusive educational environment prepared them for? Their typically
developing peers are moving on to tertiary education or looking for jobs.
Parents and teachers alike become acutely aware that the older learners will soon
have to leave school. They brainstorm. How are they going to prepare learners for
the transition to young adulthood? Life skill programmes, which have always been
part of the school programme, are expanded with a strong emphasis on functional
literacy and numeracy. The interface with the “working community” becomes the
focus. Knowledge they have acquired and skills they have learnt need to be
transposed into the workplace. Jobs may be paid or voluntary, home or community
based. The collaborative team identifies and approaches potential employers, and
engages with them regarding possible job placements. At this point support is given
to the young adult (employee) and also the employer by a person assuming the role
of job coach.
The Pathways story of inclusion is very encouraging. It is about a journey; a
story of breaking barriers, a story of participation. It is a story of children –
some with disabilities and some without – learning and growing together.
Who better to tell the stories than those who have been part of it?
Kamalan, a typically developing nine-year-old, shares his thoughts about being at
school with peers with disabilities:
I like being with the children. The children are kind to me. It is good fun to be
with them. We sing happy songs, play games in the sand pit, the trampoline,
handball and on the swings. We help to push the children in the wheelchairs
for “walks”. They always ask me if I am happy to do things with them.
Sometimes it’s like they know some games might not be so interesting for
me, but I still play because I enjoy it.
Kamalan’s father, Siva, sees it this way:
From Kamalan’s response there are obviously only positive feelings
associated with the Centre. We are always reminded of how every action
has a reaction – if Kamalan feels good, then the children from the Centre
surely must feel the same way. We want to teach our children good values.
What I see in Kamalan’s response is the association of some of the core
values of kindness, tolerance, patience, happiness and love. Sometimes we
need to be prompted to live out good values and the Enrichment Centre
definitely does this for my child.
Reflect on this talk given by Danica’s mother to a school gathering:
When first asked to say a few words, I was scared, unsure of what to say and
thought, oh no, I can’t do this. Then it dawned on me this is how many people must
have felt when inclusion was first mentioned, yet people that believed in it pushed
forward and I believe have made it work. I was asked to tell you what it has meant to
my children to be involved in inclusion. Well I know what I thought it has done for
them, but what did my children feel? So I asked them. My ten-year-old son told me
he now has a better understanding of the feelings and ways of children with
disabilities, and doesn’t need to stare. My daughter of five looked at me and then
said, “People’s eyes are different colours, people have different hair and some
people have different bodies and minds.” To her it was that simple. Well, my young
children had just taught their old mother something. I never looked at it in this way
before and quite honestly Danica was right.
An incident that sticks in my mind that proves inclusion does make a difference was
once when we were in CNA. The aisles are not very wide and it was rather busy.
There was a man in a wheelchair struggling to turn into the aisle because people
simply kept walking almost over him as though he did not exist. My children, without
hesitation, stopped, stepped aside, said good morning and once he had passed,
carried on. The look on the man’s face said more than a thousand words. He got this
huge smile and his eyes lit up. I don’t think it was because he could now get past; it
was more a smile of “Wow, those kids didn’t stare or make some horrible comment
but they actually acknowledged me as a human being”. At that moment I was a very
proud mommy and I truly believe it is because of my children’s exposure to inclusion
on a daily basis that they see disabilities as normal.
I have told you what it has done for my children but now I want to tell you what I have
learnt. In my very early 20s I did an equestrian course. One of the things I had to do
was teach children with mental disabilities. Often after the lesson I would go home
and cry, because I felt so sorry for those pupils. In my prayers I would thank God that
I was normal. I honestly believed that there was not much that these pupils could do
with their lives. Well, how naïve I was. The Enrichment Centre has a few pupils that
work at The Farmyard and Greener Tidings Nursery. It is all about teaching them life
skills. Seeing these children at work has taught me that there are many things I
thought they could not do that they do with ease. My prayers are now very different
and instead of asking God to help these children, I ask God to help all of us to have a
better understanding and to see them as normal. I also ask that inclusion becomes
part of many schools because I truly believe that we all benefit from inclusion.
What is your response to the Pathways story? Could something similar
happen in your community?
For many, the honest response may be “Yes. No. Well maybe.” That’s a
good start!
Encouraging stories begin to open the way. More details would reveal that
the path is not always smooth, that mistakes are made, that at times the
problems seem insurmountable, but it would also reveal the wonder of
seeing the child and family embraced by the school and wider community.
It is a huge challenge and responsibility for the teachers of the 21st century.
2.7 CONCLUSION
There are 500 000 South African children younger than 18 years who are
not in school. It is with their peers in schools, on the playground, on the
streets and in places of worship where they become part of the local
community and cultural life, and part of the reconstruction and development
of our country (Department of Education, 2001). Only then can we claim
that we cherish all the children in our country equally.
The sobering fact is that the number of school-aged children not attending
school has not changed between 2001 and 2013 (Statistics SA, 2014). It is
not only about disability but also about poverty, teenage pregnancy, abuse,
perceptions about the values of education, dropout rates, and so much more.
At the heart of the challenge is the will to establish communities and
schools where all children participate and thrive (Children’s Institute,
2011).
In this chapter, the participation and learning model has been used as a
framework to explore factors that facilitate participation and those that are
barriers to it. This model will further be used as a scaffold for the discussion
on assessment (Chapter 3), teaching practices (Chapter 4) and differentiated
teaching (Chapter 5). Thorough assessment of participation and learning
progress at home, at school and in the community will determine the
strengths that can be developed and the supports that need to be in place in
order to make the curriculum accessible to each and every child.
REFERENCES
Almqvist, L., Uys, C.J.E. & Sandberg, A. 2007. The concepts of participation, engagement and flow:
a matter of creating optimal play experience. South African Journal of Occupational Theory, 37(3):
8–13.
Anaby, D., Law, M., Coster, W., Bedell, G., Khetani, M., Avery, L. & Teplicky, R. 2014. The
mediating role of the environment in explaining participation of children and youth with and without
disabilities across home, school and community. Archives of Physical Medicine and Rehabilitation,
95(5): 908–917.
Bedell, G., Coster, W., Law, M., Liljenquist, K., Kao, Y.C., Teplicky, R. et al. 2013. Community
participation, supports, and barriers of school-age children with and without disabilities. Archives of
Physical Medicine and Rehabilitation, 94(2): 315–323.
Bell, A., Corfield, M., Davies, J. & Richardson, N. 2009. Collaborative transdisciplinary intervention
in the early years – putting theory into practice. Child: Care, Health and Development, 36(1): 142–
148.
Beukelman, D.R. & Mirenda, P. 2013. Augmentative and alternative communication: management of
severe communication disorders in children and adults, 4th ed. Baltimore: Paul H. Brookes.
Boa, S. & Murphy, J. 2007. Talking Mats Symbol Resource Set: goal setting. Scotland: University of
Stirling.
Bornman, J. 2006. Using a narrative and drawing approach to investigate Grade 1 children’s
depictions of disability. The Social Work Practitioner–Researcher, 18(2): 144–164.
Bornman, J. & Almqvist, L. 2007. Positive functioning: exploring its relevance for disability and
intervention. South African Journal of Occupational Therapy, 37(3): 2–3.
Castelli, L., De Amicis, L. &. Sherman, S.J. 2007. The loyal member effect: on the preference for ingroup members who engage in exclusive relations with the in-group. Developmental Psychology,
43(1): 347–359. doi:10.1037/0012-1649.43.6.1347
Centre for Universal Design. 2008. Environments and products for all people. Available at:
https://www.ncsu.edu/ncsu/design/cud/about_us/usronmace.htm
Children’s Institute. 2011. Children count: statistics on children in South Africa. Available at:
http://www.childrencount.org.za/indicator.php?id=6&indicator=15
Dahan-Oliel, N., Shikako-Thomas, K. & Majnemer, A. 2012. Quality of life and leisure participation
in children with neurodevelopmental disabilities: a thematic analysis of the literature. Quality of Life
Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation,
21(3): 427–439.
Department of Basic Education. 2015. Education Statistics in South Africa – 2013. Pretoria:
Department of Basic Education. Available at:
http://www.education.gov.za/Portals/0/Documents/Publications/Education%20Statistic%202013.pdf?
ver=2015-03-30-144732-767
Department of Education. 2001. Education White Paper 6. Special needs education: building an
inclusive education and training system. Pretoria: National Department of Education.
Department of Labour. 1998. Employment Equity Act, No. 55 of 1998. Available at:
http://www.hpcsa.co.za/hpcsa/UserFiles/File/EMPLOYMENT%20EQUITY%20ACT.pdf (accessed
on 9 February 2009).
Department of Women, Children and People with Disabilities. 2013. Baseline country report to the
United Nations on the implementation of the convention on the rights of persons with disabilities in
South Africa. Available at: https://ubuntucentre.files.wordpress.com/2010/09/country-report-finalbaseline-country-report-on-the-crpd-cabinet-approved-3.pdf
Diamond, K.E. & Tu, H. 2009. Relations between classroom context, physical disability and
preschool children’s inclusion decisions. Journal of Applied Developmental Psychology, 30: 75–81.
doi:10.1016/j.appdev.2008.10.008
Donohue, D. & Bornman, J. 2014a. The challenges of realizing inclusive education in South Africa.
South African Journal of Education, 34(2): 2–14.
Donohue, D.K. & Bornman, J. 2014b. South African teachers’ attitudes toward the inclusion of
learners with different abilities in mainstream classrooms. International Journal of Disability,
Development and Education, 62(1): 42–59.
Flynt, S.W. & Morton, R.C. 2004. Bullying and children with disabilities. Journal of Instructional
Psychology, 31(4): 330–334.
Hansen, M., Harty, M. & Bornman, J. 2016. Exploring sibling attitudes towards participation when
the younger sibling has a severe speech and language disability. South African Journal of Child
Health, 10(1): 47–51. doi:10.7196/SAJCH.2016.v106i1.1046
Heah, T., Case, T., McGuire, B. & Law, M. 2007. Successful participation: the lived experience
among children with disabilities. Canadian Journal of Occupational Therapy, 74 :38–47.
Hong, S.Y., Kwon, K.A. & Jeon, H.J. 2014. Children’s attitudes towards peers with disabilities:
associations with personal and parental factors. Infant and Child Development, 23: 170–193.
doi:10.1002/icd.1826
Huus, K., Dada, S., Bornman, J. & Lygnegård, F. 2016. The awareness of primary caregivers’ in
South Africa of the human rights of their children with intellectual disabilities. Child: Care, Health &
Development (in press).
Imms, C., Reilly, S., Carlin, J. & Dodd, K. 2008. Diversity of participation in children with cerebral
palsy. Developmental Medicine & Child Neurology, 50(5): 363–369.
Kramer, J.M., Olsen, S., Mermelstein, M., Balcells, A. & Liljenquist, K. 2012. Youth with
disabilities’ perspectives of the environment and participation: a qualitative meta-synthesis. Child:
Care, Health and Development, 38(6): 763–777.
Lawson, H., Parker, M. & Sikes, P. 2006. Seeking stories: reflections on a narrative approach to
researching understandings of inclusion. European Journal of Special Needs Education, 21(1): 55–
68.
Lindqvist, B. 1994. Special rapporteur 1994–2002: Bengt Lindqvist.
http://www.un.org/disabilities/default.asp?id=220 (accessed on 24 February 2009).
Martin, P. 2014. Children’s rights to basic education: a review of South Africa’s laws and policies. In
Proudlock P. (Ed.). South Africa’s progress in realizing children’s rights: a law review. Cape Town:
Children’s Institute, University of Cape Town & Save the Children South Africa.
Matt, S.B. 2014. Perceptions of disability among caregivers of children with disabilities in
Nicaragua: implications for future opportunities and health care access. Disabilities Studies
Quarterly, 34(4).
Mayer-Johnson, R. 1992. The picture communication symbols. Solana Beach, CA: Mayer-Johnson
Co.
Mycroft, Z. 2008. A parent’s experience. Presentation at the SAALED Congress: From inclusion to
belonging: widening the classroom circle, Bryanston, Johannesburg.
Radić-Šestić, M., Radovanović, V., Milanović-Dobrota, B., Slavkovic, S. & Langović-Milićvić, A.
2013. General and special education teachers’ relations within teamwork in inclusive education:
socio-demographic characteristics. South African Journal of Education, 33(3): Art. #717, 15 pages.
http://dx.doi.org/10.15700/201503070733
Rose, J. & Alant, E. 2001. Augmentative and alternative communication: relevance for
physiotherapists. South African Journal of Physiotherapy, 57(4): 18–20.
South Africa. 1996a. The South African Constitution and Bill of Rights. Available at:
http://www.paralegaladvice.org.za/docs/rights.pdf (accessed on 23 February 2009).
South Africa. 1996b. South African Schools Act 84 of 1996. Pretoria, South Africa: Government
Printer.
South Africa. 1997. White Paper on an Integrated National Disability Strategy (INDS). Pretoria,
South Africa: Government Printer.
South Africa. 2015. White Paper on the Rights of Persons with Disabilities. Pretoria, South Africa:
Government Printer. Available at:
https://www.ru.ac.za/media/rhodesuniversity/content/equityinstitutionalculture/documents/White%20
Paper%20on%20the%20Rights%20of%20Persons%20with%20Disabilities.pdf
Statistics SA. 2014. General household survey 2002–2013. Pretoria, Cape Town. Available at:
http://www.statssa.gov.za/publications/P0318/P03182013.pdf
TASH. 2014. About us. The Association for Persons with Severe Handicaps. Available at:
http://www.tash.org/about/
UNESCO. 1994. Framework for action on special needs education. Paris: UNESCO.
UNESCO. 2015. World Education Forum 2015. Available at: http://en.unesco.org/world-educationforum-2015/5-key-themes/inclusive-education
UNESCO. 2016. Ten questions on inclusive education. Available at:
http://www.unesco.org/new/en/education/themes/strengthening-education-systems/inclusiveeducation/10-questions-on-inclusive-quality-education/
United Nations General Assembly (UN). 1989. Convention on the Rights of the Child. Available at:
http://www.ohchr.org/EN/ProfessionalInterest/Pages?CRC.aspx.persons
United Nations General Assembly (UN). 2006. Convention on the Rights of Persons with
Disabilities. New York: United Nations.
Westling, D.L. & Fox, L. 2009. Teaching students with severe disabilities, 4th ed. New Jersey:
Merrill Prentice Hall.
World Health Organization (WHO). 2007. International classification of functioning, disability, and
health – children and youth. Geneva: World Health Organization.
Yeboah-Antwi, K., Snetro-Plewman, G., Waltensperger, K.Z., Hamer, D.H., Kambikambi, C.,
Macleod, W. et al. 2013. Measuring teamwork and taskwork of community-based “teams” delivering
life-saving health interventions in rural Zambia: a qualitative study. BMC Medical Research
Methodology, 13(84): 1–8.
3
Assessment approaches in the
school setting
In an effective education system, all learners are continuously assessed on
their educational progress in relation to the curriculum. Assessment should
focus on the characteristics and attainment of all learners, as well as how
each learner can individually learn within the curriculum.
3.1 INTRODUCTION
In the school setting, assessment is the process of gathering information that
enables teachers, together with members of the collaborative team, to meet
a child’s current and future educational needs. In other words, it helps a
teacher decide what to teach and how to teach it most effectively. Perhaps
then the most important question should not be how assessment is defined,
but rather if and how the information obtained through assessment is used.
The Department of Education has released a number of policy documents
and regulations that form part of the implementation of Education White
Paper 6, such as the National Strategy on Screening, Identification,
Assessment and Support (SIAS) (Department of Education, 2008); the
National Education Policy Pertaining to the Programme and Promotion
Requirements of the National Curriculum Statement Grades R–12
(Department of Education, 2012a); and the National Protocol for
Assessment Grades R–12 (Department of Education, 2012b); as well as the
current national South African education curriculum, the Curriculum and
Assessment Policy Statements (CAPS) (Department of Basic Education,
2011). The primary focus is to facilitate school access for children,
especially those who are either marginalised or totally excluded. For this to
become a reality, appropriate supports must be available. The SIAS
document states that “no assessment is meaningful if it does not ensure
access to support” (Department of Education, 2008: 31).
Stop and reflect
Are appropriate supports readily available in South Africa to make inclusion work?
This statement is a challenge for all involved in an education system in the
process of expanding its vision and service delivery. A cursory glance at
schools in South Africa would suggest that in many schools, access to
support is limited, and in some cases possibly even non-existent. The
solution is not simple but one thing is clear: the onus rests on the citizens of
a country to turn policy into practice.
South Africa has some of the most progressive human rights policies in the
world, as is also a signatory of the United Nation’s Convention on the
Rights of the Child (UN, 1989). As discussed in Chapter 2, education is a
non-progressive human right, which implies that it should be made
available to all, irrespective of whether funding is available or not. A rightsbased approach to education helps children realise their rights, as it is not
only academically effective but also inclusive, healthy and protective of all
children, and encourages the participation of the learners themselves, their
families and their communities (UNESCO, 2009). Teachers play a strong
proactive role in learning by creating a stimulating and supportive learning
environment (UNESCO, 2012). However, teachers alone are not enough –
everybody involved with learners (teachers; principals; non-teaching
support staff; parents; members of district-based support teams (DBSTs),
institution-level support teams (ILSTs) and school governing bodies
(SGBs); communities; etc.) should be informed and proactive. All must be
able and willing to ensure inclusion in the classroom and in learning for all
children, regardless of their differences.
Support can be arranged at five different levels: (i) levels 1 and 2 (very low
frequency or once per annum intervention); (ii) level 3 (moderate levels of
support); and (iii) levels 4 and 5 (very high to daily intervention by
specialised staff (Smit & Engelbrecht, 2011). The support required for
levels 1 to 3 can be offered at mainstream and/or full-service schools, while
support at levels 4 to 5 can be offered at full-service schools and/or special
schools.
Sindi’s story
As part of their hospitality studies, a group of Grade 10s are planning to operate a
coffee shop when there are extramural school activities at school, such as sports
days, parents’ evenings, and so on. They are breaking down the tasks to ensure that
everything will get done and that each individual has a clearly defined role, for
example cleaning and laying the tables, making scones, waiting on tables, and so on.
Sindi is sitting quietly in her wheelchair. Not only is she unable to move
independently but she is visually impaired. “Oh dear!” says one of the learners, “what
on earth can Sindi do?” “Well,” another says to Sindi, “what are you good at?” “I’m
not sure, but you all know that I like talking,” says Sindi. They all put on their thinking
caps. “I’ve got it,” says Mpho. “Why don’t you sit at the door and welcome people and
then chat to them while they wait to be seated? You can tell them about the delicious
things on the menu or maybe treat them to one of your good jokes.” “Great idea,”
says Sindi. “I hope one of our first customers is Linda’s brother – he’s totally
awesome!”
Assessment is about the setting of goals that inform teaching practice.
Tomlinson and Imbeau, (2010) describe assessment as today’s means of
understanding how to modify tomorrow’s instruction. Similarly the
participation and learning model (PLM), discussed in Chapter 2, illustrates
the relationship between assessment and classroom instruction. The
challenge is to use assessment strategies that will accurately reflect the
learner’s competencies as well as areas of need while keeping in mind that
the focus should be on the gathering of information, which can be used as a
scaffold for educational planning (Luke & Schwartz, 2007). Assessment
should reflect who the learner is, and what he or she knows (knowledge),
understands (concepts and principles) and is able to do (skills) (Westling &
Fox, 2009). Furthermore, the assessment should reflect both how the child
learns and how he can show what he has learnt.
3.2 THE ASSESSMENT PROCESS
Three critical elements of assessment are the following:
The learner. The learner is moving towards independence. The learning
that takes place at home, at school and in the community underpins the
development of autonomy in the child, which enables him or her to
become a valued, contributing member of society.
The journey. Learning and development never take place in a vacuum.
There are people to meet, things to think about, things to do and places to
go to. Take any one of these away and the learning experience becomes
pointless.
The way. This will be unique for each learner.
3.2.1 The learner
Teaching is about creating nurturing environments in which children can
learn and grow. This learning is almost always cooperative, whether in the
class as a whole or in smaller groups. The challenge for the teacher is to
ensure that the potential of each child is realised within these contexts, for
children to become interdependent as well as independent (Raymond,
1995). The concept of independence is quite complex. It does not mean
being able to live without the support of others. It does, however, mean
being in control. For example, after a terrible storm the classroom roof may
leak and the teacher may not have the skills (or the time!) to fix it, but she
does know how to arrange for someone else to come and do the job; a
learner may not be able to take a tight-fitting lid off his lunchbox but he
knows he can ask for assistance; a learner may not know how to edit a
Word document on a computer but he knows he can request help from his
teacher or a study buddy. In light of this it becomes clear that inclusion and
independence are inseparable. No child can become independent if he is not
sufficiently included or “plugged in” in his home, school and community.
Hold this thought when considering approaches to assessment and
intervention.
3.2.2 The journey
The very word “journey” implies a sequence of experiences and events,
with a vision of where one would like to go. In other words, the whole
assessment process should have a general direction as well as certain
“events”. Two of the most significant events relate to the two purposes of
educational assessment: informal assessment (also known as assessment for
learning) and formal assessment (also known as assessment of learning)
(see Figure 3.1).
Figure 3.1 Two key assessment purposes
The purpose of informal assessment is to continuously collect information
on a learner’s performance that can be used to improve learning. It thus
entails daily monitoring of progress, and can be done through observations,
discussions and practical demonstrations (Department of Basic Education,
2014). For decades, effective teachers have constantly been using these
strategies: providing more explanation when noticing that learners are
frowning, asking a learner to re-read a paragraph (this time aloud, maybe),
giving a learner a specific book based on the dozens of questions he or she
learner asks about the specific topic over the course of the year (e.g. a book
about sharks, or the galaxy). Sometimes it may even be as simple as
stopping during the lesson to observe learners or to discuss with them how
learning is progressing in order to provide them with feedback and to
impact on how teaching and specific lessons are planned. Learners should
also be taught to learn from and reflect on their own performance (self-
assessment). The results of informal assessment tasks are not taken into
account for promotion and certification purposes.
Formal assessment, on the other hand, is made up of all assessment tasks
that comprise the assessment tasks that are marked and formally recorded
by the teacher to systematically evaluate the learners’ progress. Formal
assessment tasks are subject to moderation for the purpose of quality
assurance and to ensure that appropriate standards are maintained
(Department of Basic Education, 2014). Examples of formal assessments
include tests, exams, practical tasks and projects, signed presentations,
demonstrations (e.g. retelling a story, performances such as acting or
designing a dance), and writing essays, poems, newspaper articles or
stories. Memoranda, rubrics, checklists and rating scales can be used to
observe, assess and record learners’ levels of understanding and skill.
As the arrows in Figure 3.1 indicate, the results from the informal
assessment impact on the formal assessment because if a teacher notices
that a learner requires longer time to complete a classroom activity, a test
adaptation such as allowing extra time can be given. Likewise, if a teacher
notices that the learner still does not understand some key terms and/or
definitions after the formal assessment, these can be retaught using a
different teaching strategy (e.g. using mind maps rather than a list). By
employing this strategy, a learner can benefit optimally from assessment
(Lombard, 2010).
Probably the most critical element of the journey is planning. For the
purposes of this chapter, the question is: “Where to start?” If one does not
get to the right station or taxi rank, the journey is doomed. Looking at
inclusion as a journey highlights the need for careful and accurate
assessment aimed at building on and expanding a learner’s current
knowledge and skills.
3.2.3 The way
In general, teachers are well trained and equipped to assess and plan how
best to achieve long- and short-term goals, but they are often confronted by
the challenges of diverse learners with complex learning needs and have to
be able to adapt both the assessment and the teaching strategies. “The way”
will be unique for each child. Following on the journey analogy, we know
there are many ways to arrive at a destination using different routes and
means of transport. For example, a child may take a shortcut home from
school one day and go via the shop the next day to buy a loaf of bread.
Similarly, a child may walk to school when the weather is fine and take a
taxi when it is raining or very cold. Some children may ride a bicycle to
school or catch a train. A mother may take a young child to school and let
him walk as he gets older and more responsible. These examples point to
the way individuals adapt to circumstances in both the short and long term.
It is no different for teaching and learning. There are many assessment
models that provide frameworks for assessment, and this chapter will
highlight some of them, specifically those that will assist teachers in
evaluating learners with complex learning profiles. Chapter 4 will discuss
various teaching strategies that will flow from the information and insights
gained during the assessment process.
The challenge is to gather as much information as possible so as to develop
an individualised support plan (ISP). This is developed by teachers in
consultation with parents and the rest of the collaborative team. The
assessment team has three primary responsibilities. They must select
appropriate assessment formats, set achievement standards and formulate
teaching strategies for each learner. Bear in mind that there may be learners
with significant disabilities who may not need any accommodations, for
example a child with polio who is mobile or a child with medically
controlled epilepsy. Assessment strategies must be embedded in the
teaching and learning culture of the school. Tomlinson and Imbeau (2010)
refer to developing respect for the identity of each learner by
getting to know the learner as an individual with unique personality
traits, talents, interests, and so on
expecting the learner to grow as a whole person
providing opportunities for the learner to explore and experience learning
opportunities that escalate as the learner becomes more proficient
presenting all learners with tasks that are equally interesting, important
and engaging.
Only when these core values permeate the assessment process will the
collaborative team be able to draw up an ISP to guide the process of
individualised learning and teaching.
3.3 INDIVIDUAL SUPPORT PLANS (ISPS)
The ISP is an educational plan designed for learners who need additional
support or expanded opportunities (Department of Education, 2008). The
ISP is typically developed by the ILST, which consists of members who are
well trained to help teachers address barriers to learning. ISPs contain longterm goals which are achieved by implementing the ongoing short-term
instructional decisions that teachers have to make. Monitoring the
effectiveness of the short-term goals improves the effectiveness of teaching
and enhances the learners’ progress. The data gathered in this way are then
also used to feed back into the ISP. As such, the ISP describes the goals the
team sets for a child during the school year, as well as any special support
needed to help achieve them. It consists of nine components:
Understanding current educational levels
Identifying barriers to learning in order to also identify support needs that
would improve teaching and learning
Considering appropriate related services and support
Planning the degree of participation in classroom settings
Justifying the use of regular or alternative assessment approaches
Justifying the use of regular or alternative achievement standards
Planning how and when the ISPs will be implemented
Formulating transition plans from one school phase to another as well as
school-leaving plans, which starts with determining a vision for the child
(as described later in this chapter) (Karan, DonAroma, Bruder & Roberts,
2010)
Deciding how progress will be measured and reported
In order to develop an ISP, a meeting is held at which the collaborative team
decides what will go into it. At the meeting, the team will discuss the
learner’s educational needs and come up with specific, measurable, shortterm and annual goals for each of those needs. Parents can actively
participate in developing the goals and determining which skills or areas
will receive the most attention. The ISP will be reviewed annually to update
the goals and to ensure that the levels of support meet the child’s needs.
However, ISPs can be changed at any time on an as-needed basis. If any
member of the collaborative team feels that the child needs more, fewer or
different supports, a meeting can be convened to discuss the concerns.
3.4 ASSESSMENT APPROACHES
For typically developing children, regular assessment formats and general
curriculum standards are the norm. So what then happens to children for
whom regular assessment and achievement standards are not appropriate?
For some, the assessment format will change. For others, the achievement
standards may change. Some need modifications to the curriculum, such as
the unwinding of the assessment criteria or the straddling of grades. Table
3.1 illustrates all of these formats and modifications, and also briefly gives
some learner profiles with each.
Why is Table 3.1 so significant? Each of the aspects will be highlighted in
the following section.
Table 3.1 Assessment formats, content modifications and achievement standards
Group
Curriculum
content
Curriculum
modifications
required
Assessment
format
Achievement
standard
Learner profile
examples
Group
Curriculum
content
Curriculum
modifications
required
Assessment
format
Achievement
standard
Learner profile
examples
1
Grade-level
content
No
modifications
Regular
assessment
General
curriculum
standards
Ageappropriate
intellectual
skills and/or
mild
communication,
motor, sensory
or
socioemotional
challenges
2
Grade-level
content
Unwinding of
the
assessment
criteria
Regular
assessment
Alternative
achievement
standards
Mild intellectual
impairment
and/or
communication,
motor or
sensory
challenges
3
Grade-level
content
No
modifications
Alternative
assessment
General
curriculum
standards
Ageappropriate
intellectual
skills and/or
significant
communication,
motor or
sensory
disabilities
4
Grade-level
content
Straddling of
grades
Alternative
assessment
Alternative
achievement
standards
Significant
intellectual
impairment
requiring
substantial
modifications,
adaptations or
supports to
access
curriculum
content
3.4.1 Curriculum content
The significance of Table 3.1 is that for all learners the content is always
curriculum based according to the child’s specific grade. The implication is
that all learners can participate in comprehensive learning programmes that
are aligned with the Curriculum and Assessment Policy Statements
(CAPS). This obviates the all-too-common practices such as regarding
learning colours and shapes as a prerequisite for “moving on”, or denying a
learner literacy exposure because he or she is considered too intellectually
disabled.
Curriculum-based assessment (CBA) is an approach to linking instruction
with assessment. It was developed in order to document the progress of
learners through the curriculum and to assist teachers in creating more
effective instructional environments (Mastropieri & Scruggs, 2010). As
such, it simply means that direct observation and recording of a learner’s
performance in the curriculum is used as a basis for gathering information
to make instructional decisions (Cohen & Spenciner, 2007). This type of
basic assumption that one should test what one teaches makes sense.
Research has also shown that this type of assessment enables learners to
form a deeper understanding of content (Tindal, 2013).
A further important feature of curriculum-based assessment is its focus on
long-term curriculum goals – in other words, what the teacher aims to
achieve by the end of the year. For example, the teacher looks at the
complete curriculum for all the words that the learners have to be able to
spell by the end of the year, and then creates 40 spelling tests, all containing
20 words, and administers one test every week. By keeping track of the
learners’ weekly scores on the spelling test, she can see if spelling ability
increases over the course of the year. Likewise, if a teacher wants to know
whether learners are progressing in reading and writing, she should observe
their reading and writing skills in the classroom. By collecting these data as
often as possible, she can accurately assess whether a child is making
progress or falling behind (Cohen & Spenciner, 2007). However, Tindal
(2013) warns that progress monitoring through CBA alone is insufficient;
rather, teaching should be tailored to meet the needs of individual learners.
3.4.2 Curriculum modifications required
Diversity is one of the key characteristics of an inclusive classroom. The
majority of learners in a class will not require any modifications, but
teachers will know that for some learners the curriculum is too difficult and
that some struggle to keep up. In Table 3.1, four groups of learners are
shown, of which two require no modification, although the learners in
group 3 would require alternative assessment. This could mean that a child
is blind and would require the curriculum in Braille, but no changes to the
content of the curriculum or the achievement standards are necessary. The
learners in group 2 refer to those who are described by teachers as “slow
learners” and they would require an unwinding of the assessment criteria –
in other words, slightly adapted achievement standards. The children in
group 4 are not expected to master all the outcomes outlined in the
curriculum, but they should achieve the main outcomes at the end of each
phase (e.g. Foundation, Intermediate or Senior).
3.4.3 Assessment formats and achievement standards
When looking at the assessment format, a teacher could decide to use the
regular assessment or perhaps do an alternative one. Teachers are trained to
do the former, but are less familiar with the latter.
According to the Department of Education (2008), the rationale for the use
of alternative assessment is twofold:
To ensure educational accountability to the learner, his family, his school
and the relevant educational authority
To gather information that can be used to motivate for appropriate
resources and funding. The aim is to establish the nature and extent of
support needed and then to plan the provision of and access to such
support.
WHICH LEARNERS SHOULD BE ALLOWED TO HAVE AN ALTERNATIVE
ASSESSMENT?
Alternative assessment is appropriate for learners who are unable to
participate in regular assessment. Assessment formats should be designed to
minimise the impact of learning, physical, cognitive, communicative and/or
sensory disabilities so that the learner can give his full attention to the task
at hand. For example, a child with significant motor disabilities may need
adaptive seating or access to a computer; a child with a visual field
impairment may need assessment materials placed in a specific location on
the work surface; and a child with an intellectual impairment may need to
respond by pointing to line drawings rather than written words.
However, in addition to the learners described above, it must be emphasised
that alternative formats can be used for learners who are academically
competitive (i.e. who still meet general curriculum standards). These
learners need no modifications to the curriculum, but they would need
alternative assessment formats. In reality, all learners have specific areas of
strength and weakness which can be accommodated within the regular
assessment and learning process. The motto is always: Give the child the
benefit of the doubt. It could take days or weeks for a teacher to get to know
the child and only then should assessment be undertaken. This is described
in more detail later in the chapter.
Some of these modifications can easily be implemented in the classroom,
while others require certain procedures prescribed by the Department of
Education to be followed (e.g. reports by educational psychologists and/or
occupational therapists). Amanuensis (someone else writes down the
answer) has been used with great effect in high school (Mavuso, 2015).
In some cases these modifications might not be enough, and other
alternatives could be considered, which are usually grounded in the reality
of the learners’ experiences, such as samples from their work over the past
year, interviews with parents and other team members (such as therapists),
videos made during the year and observations. Narratives, which are a form
of discourse that tell a story (the term stems from the Latin word gnarare,
which means “to know”) have also been used successfully, as they provide
insights into the way in which individuals look at their world (Nathanson,
2006). As such, narratives build upon a human need to create meaning and
to forge connections between scattered bits of knowledge and experience.
Two approaches that can be used when gathering information in order to
complete alternative assessment formats include personal mapping (e.g.
McGill Action Planning System or MAPS) and Choosing Options and
Accommodations for Children (COACH).
3.4.3.1 Personal mapping
Personal mapping is an inclusive interactive process that enables a teacher
to get to know a particular learner (Westling & Fox, 2009). Although the
approach can be used with all learners, it is a particularly useful tool for
teachers planning to include those with disabilities. MAPS is an example of
such a personal map, and is a powerful tool when used as part of the
assessment and planning process to build a vision (Karan et al., 2010;
Vandercook, York & Forest, 1989). The purpose of building a vision is to
create a long-term plan that incorporates all of the hopes and dreams shared
by the learner and those close to him – typically close family members.
However, sometimes other individuals who know the learner in a variety of
contexts may provide valuable information (Karan et al., 2010). For
example, family members might think that the child is withdrawn, but the
classroom aide may view the child as friendly and outgoing because she has
noticed that the learner is often surrounded by friends on the playground.
By involving more people the vision can therefore be expanded, as it may
be that the learner thrives in situations where he has an opportunity to
interact with peers of the same age.
MAPS is a collaborative team approach to information gathering and
programme planning (O’Brien & Pearpoint, 2007). There are seven key
questions in the process (see Table 3.2). The order in which they are posed
is not significant, but all seven must be used. It is a process that best
precedes the formulation of an ISP as it provides the school’s collaborative
team with important information to feed into the ISP. The MAPS process,
which focuses attention on capacities rather than deficits, generates
important benefits throughout the planning and implementation of the
child’s ISP.
Inherent in the MAPS process is the fact that the collaborative team is at the
heart of the process. Ideally, all members of the collaborative team should
participate – even young learners, siblings and peers can make valuable
contributions. The format is flexible but it starts off by describing what the
MAPS process is and how it will guide the discussion. The first question
aims to obtain a clear picture of who the learner is by asking questions
about, for example, his likes and dislikes, his personality traits, and so on.
The second question concerns the learner’s history (personal, medical and
educational). The third and fourth questions relate to the dreams (what is
longed and hoped for) and nightmares (what is daunting and scary) of both
the learner and his parents or caregivers. It is important that participants do
not become despondent if the realities of education or the threat of social
isolation or poverty are discussed. Dreams and nightmares are of equal
importance to the discussion. Many discussions fuel the nightmares rather
than the dreams (O’Brien & Pearpoint, 2007). The aim is to discuss both
dreams and nightmares so that the former can be realised and the latter
acknowledged and faced.
The fifth question focuses on the learner’s gifts, strengths and abilities. This
focus on the positives is in line with the asset-based approach that weaves
through this book like a golden thread. The concept of “giftedness” is
stressed not only in relation to academic ability, but also as one of the
attributes of personality.
The sixth question relates to the specific support needed to enable the
learner to participate fully in the school programme alongside his peers.
The final question considers what the learner’s ideal day at school should
look like and what can be done to make this a reality. The MAPS process
assists in bringing the learner and family closer to the daily life of the
school (O’Brien & Pearpoint, 2007).
The entire MAPS process can, if efficiently prepared and managed, take
about 90 minutes to conduct.
Stop and reflect
Refer to David’s story (page 21 in Chapter 2) and the response of his teacher, Mrs
Mompei: “I don’t even know where to start ….” Because David is in a wheelchair and
unable to talk, the assessment format will be alternative, unless there is evidence to
the contrary that the achievement standard will be the same as for typically
developing peers. Think about it. David is six years old. The question is not “Is David
ready for school?” but rather “Is the school ready for David?”
Mrs Hlalele from the district office has attended a training session where she heard
about the MAPS approach and, feeling that there was nothing to lose, suggests that
they try it. She puts together a team, and Table 3.2 shows what they discover.
Table 3.2 clearly shows how a picture of the learner emerges as well as a
vision and a plan. This gives the teacher a starting point from where to plan
her teaching approach. Some parents may have unrealistic expectations but
mostly parents have a deep understanding of the possibilities for their child.
One of the primary longings of parents is that their child be accepted and
given the opportunities to make friends (Giangreco, Cloninger & Iverson,
2011). This is not surprising. Looking at school readiness testing, social
skills are one of the key components, yet somehow this gets overlooked in
the older child or the child with disabilities. Parents are usually very aware
that social interaction and integration are core components of learning.
Can you still remember Rachel Serudu’s story in Chapter 1? Her team
decided to record her MAPS details in a mind map (see Figure 3.2).
Figure 3.2 Using a mind map to display MAPS details
Table 3.2 Applying MAPS to a particular learner
Name: David Masambuku Date: 29 January 2016
People present: Mrs Mompei (teacher); Mrs Masambuku (mother); Mrs Hlalele
(DBST member); Mrs Mbuyisa (care group) and Sandile (sister)
1. Who is
David?
(Personality,
characteristics,
likes and
dislikes)
David has a quiet, friendly nature. He enjoys watching other children
play, particularly those of the same age, and also wants to participate.
His speech is not intelligible, but he tries to say a few words, to point
and to use facial expressions to indicate when he is happy, sad or
angry. He gets bored easily and loves his cat and his grandmother best
– in that order! He needs help with most activities of daily living but can
eat finger food on his own (his mother cuts up his food so that he can
hold it). Indoors he crawls to get around but otherwise uses a
wheelchair. He has a smile that is irresistible. He loves books and
enjoys being read to. He also knows some letters, but cannot read yet.
2. What is his
history?
David was born prematurely after his mother was involved in a taxi
accident, and he was diagnosed with cerebral palsy at five months.
Because they lived in a small town that did not have any therapists, his
mother had to take him to Baragwanath Hospital each month where the
therapists gave her a home programme. For two years he has been
going to the local care group with his grandmother. His parents are
divorced and he lives with his mother, grandmother and ten-year-old
sister.
3. What are
your
dreams
and hopes
for David
over the
next year
and in
future?
(David’s
and his
mother’s
opinions)
David dreams that he will be able to run and play soccer with his school
friends. He wants to meet the Kaizer Chiefs and Bafana Bafana
goalkeeper, Itumeleng Khune, and when he leaves school he wants to
become a taxi driver. His mother wants him to be able to communicate
and develop real friendships, and never have to be sent away from
home. She wants him to go to school with his sister. One day, she
hopes that he will become as independent as possible and earn money
to help support the household.
4. What are
David’s
nightmares
and his
mother’s
nightmares
for
inclusion
David’s nightmare is that someone will let go of his wheelchair when
pushing him down a slope, that he will not have a friend and that he will
not be able to go to school with his sister. His mother’s nightmare is
that others will think that he is stupid or that children may tease him,
and that he may be abused or lonely, and that when she dies there will
be no one to look after him.
and for the
future?
5. What are
his gifts,
strengths
and
abilities?
People are drawn to David because of his warmth and sense of
humour. He loves books and has a remarkable memory – with a
particular skill for remembering and saying the names of various people
in his life. He is able to say a person’s name, but this needs to be
expanded (e.g. when he says a name it is unclear what he wants that
person to do). He is always prepared to try new tasks and activities,
and is able to concentrate for long periods.
6. What
support
does he
need in
order to be
included?
David needs a teacher who understands him and treats him with the
same respect as she does the other children; he needs a
communication system so that he can share thoughts and feelings with
others; he needs friends both in and out of school.
7. What
should
David’s
school day
look like
and what
must be
done to
make it
happen?
The people who have been and are likely to be involved with David’s
future must meet to draw up an ISP. The principal, mother and teacher
need to work together to determine how best to support him in class.
The principal should encourage the teacher to go on training
workshops that will build her skills. The DBST should facilitate contact
with a speech therapist who can help select and develop a
communication system. His classmates will be encouraged (and
shown) how to interact with and help him in various ways. His mother
will explore community structures such as Sunday school where he will
have the opportunity to be with other children and make friends.
Once again a clear “picture” of the learner emerges, as well as a vision and
a plan. In Rachel’s case her mother wants her to help around the house and
not leave the home for paid employment, but in order to achieve this,
Rachel needs a basic understanding of the world around her, including
functional literacy and numeracy. How else will she be able to do the
shopping or try out a new recipe?
In summary, personal mapping not only provides a wealth of information
but also serves as a platform for collaborative team building. Interaction
between those involved in the learner’s life begins to build trust and shared
responsibility for developing an appropriate ISP that will yield valuable
educational outcomes.
3.4.3.2 Choosing Options and Accommodations for Children (COACH)
COACH is another alternative assessment approach that is designed for
learners with moderate, severe or profound disabilities, and is based on the
principle that all children are capable of learning and deserve a meaningful
curriculum (Giangreco et al., 2011). It is a comprehensive planning and
assessment approach that begins with input from the parents and ends in an
educational programme to be carried out in inclusive environments
(Westling & Fox, 2009). The focus is thus on teamwork and collaboration
between the family and the child’s educational team. Unless professionals
are committed to collaborative teaming and working within the framework
of the family priorities, the process should not be undertaken. Furthermore,
COACH is guided by the principle of inclusion as it states that quality
instruction requires ongoing access to inclusive environments, and that
valued life outcomes (as determined by the collaborative team) inform the
selection of curriculum content (Giangreco et al., 2011). COACH also
assists educational planning by identifying family-centred priorities and
valued life outcomes; identifying support needs relevant to learning
outcomes; assisting in prioritising ISP goals; planning and adapting lesson
plans; scheduling participation in general education classes/activities; and
assessing the impact of educational experiences.
Quality ISP planning using COACH, or any other assessment approach, is
always a process rather than an event. A core value of COACH is that
educational placement must always be the least restrictive option where the
child can pursue his individually determined long- and short-term goals.
The COACH approach has six distinct steps:
Step 1: Family interview to enable the family to select learning priorities
for the learner for the new school year
Step 2: Additional learning outcomes to determine the learning
outcomes beyond the family-selected priorities, both from COACH and
the general education curriculum (CAPS)
Step 3: General supports to allow the child to participate optimally in
inclusive settings. These include support for personal needs (e.g. feeding,
dressing, personal hygiene and medication); physical needs (e.g.
positioning, transferring and using specialised equipment); sensory needs
(e.g. books in Braille, large-print materials, batteries for hearing aids);
teaching others about the child (e.g. an augmentative and alternative
communication (AAC) system, health emergency procedures, positive
behaviour supports) and providing access and opportunities (e.g.
community vocational experiences, literacy materials in first language)
Step 4: Annual goals to ensure the family’s priorities are reflected as ISP
goals
Step 5: Short-term objectives to pursue goals for the year
Step 6: Programme-at-a-glance to provide a concise summary of the
educational programme
COACH goal setting has two distinct components:
Cross-environmental goals. These do not reflect discrete skills but rather
outcomes spanning communication, academic, sensory, socio-emotional
and leisure functioning. For example, a visual scanning goal may require
the learner to scan the options in a soft-drink vending machine, make his
choice and insert the right amount of money in the slot.
Environmentally specific goals. These reflect functional skills
specifically at home, at school and in vocational settings, for example
learning the correct way to greet the principal as opposed to a friend on
the bus.
Peter’s story
Peter was a lonely seven-year-old who could not walk and was unable to speak. He
came from a very loving, warm family who provided for all his needs. He had lots of
toys and a beautifully decorated “little boy” bedroom. He even had his own TV! His
mother said that watching TV and videos was his favourite activity – not that there
was much activity. She described how he sat passively day after day and was quite
grouchy when he had to do anything else. Then she heard about a small school that
welcomed all children and decided that it was time to move Peter out of his “comfort
zone”. There was much protest from him but surprisingly not for long.
For the school, the first step was to get to know Peter and his family, and understand
their priorities for living and learning. The COACH approach was used as part of a
holistic assessment, and an ISP was drawn up. A trust relationship developed fairly
quickly as the family realised that the school was prepared to listen to them and treat
them as equals. After Peter had been at school for about two months, his father went
to see the teacher. “Let me tell you,” he said, “this weekend for the first time in years
Peter and I had fun together. I actually enjoyed my son. I don’t know how to thank
you.”
There are many questions raised by this true story. How is success defined?
How does one measure a father’s delight? What kind of ongoing support
will Peter and his family require for learning and growing? The point is that
change happens, and often faster than is expected, when programmes are
family centred.
When these alternatives (COACH and MAPS) are used, the learners are
usually working on alternative achievement standards.
3.5 ACCOMMODATIONS AND SUPPORTS
There is quite some overlap between the concepts and terminology
concerning accommodations and supports. For the purposes of this
discussion, accommodations are defined as tools and procedures that
provide equal access to instruction and assessment for learners with
disabilities, and supports refer to structured interventions delivered at
schools and in classrooms (Department of Education, 2008).
3.5.1 Accommodations
An accommodation is any item or action that helps the learner fit in and
participate. Teachers have to provide “outcome neutral” accommodations
that allow learners with disabilities fair and equal access to tests without
being disadvantaged by their impairments (Lovett & Lewandowski, 2014).
Glasses, hearing aids and wheelchairs are some of the more common
accommodations. Others might include using pictures instead of verbal
descriptions, reading instructions aloud, or making sure ramps are available
at access points. Not all learners with disability will need test assessment
accommodations – in fact, sometimes even children with the same type of
disability (e.g. a visual disability or a physical disability) will require
different types of accommodations. Children themselves and their parents
can usually tell teachers exactly what accommodations they need (National
Center for Learning Disabilities (NCLD), 2006). Accommodations can be
categorised into six main groups, but creative teachers are continuously
making adaptations in response to learners’ unique and changing needs (see
Table 3.3).
Table 3.3 Choosing the most appropriate accommodations
Type
Who can
benefit?
Questions to ask
PRESENTATION
Learners who
Does the learner have
cannot read
standard-size
print as a
result of
physical,
sensory or
intellectual
disability
have
intellectual
disabilities
have motor
disabilities
difficulty seeing
print?
a reading disability?
difficulty in
stabilising paper?
difficulty in following
instructions?
Accommodations
Large/bold print
Magnifying devices
Human reader
Audio tapes
Different
print/background
colours
Angle and intensity of
lighting
Clipboard to hold
paper
Altering format to
multiple choice/truefalse/fill in the blank
Simplified/repeated
instructions
Modelling the
response on a similar
task
Type
Who can
benefit?
Questions to ask
RESPONSE
Learners with
physical,
communication,
sensory or
learning
disabilities
Can the learner
write or draw using
pen/pencil/crayons?
respond verbally?
Does the learner
have a spelling
disability?
Accommodations
Adapting grip
Scribe
Tape recorder
AAC device
Switches
Spelling and
grammar device
Adapting the amount
of written output
Eye gaze selection
TIMING AND
SCHEDULING
Learners
with physical
disabilities
Can the learner
concentrate for the
required time?
with poor
concentration
Which activities
cause fatigue?
with healthrelated
disabilities
What length of
break is beneficial?
with special
diet and/or
medication
needs
Extended time
Frequent breaks
Multiple testing
sessions
Shifting from one
activity to another
Communication
technology
Technology for
writing
who tire
easily
SETTING
Learners who
are easily
distracted in
large groups
Do others distract
the learner?
Change room or
location
Is the learner
disruptive?
Change position of
learner in the
classroom
concentrate
better in
small groups
Are there
concentration
problems?
exhibit
challenging
behaviour
Is the background
noise distracting?
are deaf
Use
earplugs/headphones
Use a carpet in the
classroom
Type
Who can
benefit?
ENVIRONMENTAL
Learners with
physical
disabilities
Questions to ask
Accommodations
Are the facilities
accessible?
visual
impairments
Can the learner
move about in the
classroom?
auditory
impairments
Can the learner
reach things?
Are there auditory
prompts?
Ramps
Wider doors and
passages
Wheelchair-friendly
toilets
Classroom
organisation
Direction of light
source
Are there visual
prompts?
MARKING
REPOR–TING
PROGRESS
Learners in
need of
alternative
assessment
formats
How can the
progress be shown
in the best way?
alternative
assessment
standards
Direct observation
Portfolio assessment
Continuous
assessment
Degree of progress
from the baseline
Curriculum-based
measurement
Narrative reports
i. Presentation accommodations. These allow adaptation or substitution
of materials presented (usually visually) in the assessment and learning
processes. These alternative modes of access are auditory, multisensory,
tactile and/or visual modifications. Some specific examples of changing
the presentation format include the following:
Providing verbal encouragement, test directions and assistance during
the test
Testing individually (Mastropieri & Scruggs, 2010)
Simplifying the language used (Bulloch, 2008)
Using multiple choice, comparison and direct questions for learners
who are deaf and who use Sign Language to communicate
(Department of Basic Education, 2014)
Providing prompts and feedback (including reinforcement)
(Mastropieri & Scruggs, 2010)
Allowing teachers to read the test and turn the pages (Bulloch, 2008)
Providing typewritten tests as typewriting may be easier to read than
handwriting
Defining unfamiliar or abstract words if their meanings are not being
directly tested
Simplifying and/or modifying test instructions (Bouwer, 2016)
Rephrasing instructions for learners who are deaf (Mavuso, 2015)
Providing multiple-choice tests with a bubble sheet response format
(Potter, Lewandowski & Spenceley, 2015).
ii. Response accommodations. These allow learners to complete
activities, assignments and tests in different ways and, if appropriate,
use some kind of assistive device or organiser. Some specific examples
of changing the response format include the following:
Providing oral instead of written tests (Lewandowski, Berger, Lovett &
Gordon, 2015)
Allowing options such as circling or underlining correct answers rather
than writing them down (or, to a lesser degree, circling responses in a
test booklet, which has officially been approved by education
departments in the US and in other countries (Potter et al., 2015)
Using open-book tests
Changing the spacing in tests to allow learners to fill in the answers on
the question sheet (Bouwer, 2016)
Using aids and/or different response modes, for example eye gaze
during maths tests for learners with severe physical impairments
(Bornman, Donohue, Maré, & Dada, 2016)
Allowing audiotaped, large-print, Braille or computer-based versions
of the test (learners with physical disabilities who use a computer to
complete written work need to be assessed using the same format)
Providing amanuensis for learners who have difficulty in expressing
themselves in writing (Mavuso, 2015)
iii. Timing or scheduling accommodations. These increase the allowable
length of time to complete a test or assignment and may also change the
way time is organised. Some specific examples of changing the timing
scheduling of the test include the following:
Extending the time limits (Mastropieri & Scruggs, 2010)
Spreading the test over shorter time sessions or even days (Mastropieri
& Scruggs, 2010)
Giving more tests with fewer items rather than fewer, longer tests
Allowing frequent breaks (NCLD, 2006)
iv. Setting accommodations. These change the location in which the test
or assignment is given or the conditions of the assessment setting, for
example
moving to a smaller and/or private room to complete a test
(Lewandowski et al., 2015)
moving to a quiet room such as the library or staff room
providing preferential seating (NCLD, 2006)
providing special lighting or acoustics (NCLD, 2006).
v. Environmental accommodations. These adapt or restructure the
physical environment to give access to facilities.
vi. Marking and progress reporting accommodations. These allow
teachers to make use of adapted or alternative reporting formats. Using
multiple-choice questions rather than fill-in-the-blank questions provide
learners with spelling difficulties and writing difficulties with
appropriate adaptive assessment opportunities (Venter, 2015).
Stop and reflect
Look at this multiple-choice question:
Circle one:
Herbivores all have the following characteristics:
a. They have incisors and molars.
b. It takes a long time for plants to digest in their stomachs.
c. Animals that belong to the cat family are usually herbivores.
d. Herbivores typically eat once or twice a day.
See how much less confusing it is when the instructions are just slightly modified?
3.5.2 Supports
The levels of support are specific to the needs of an individual. The
intensity of the support maybe intermittent, limited, extensive or pervasive
(Westling & Fox, 2009).
Clusters of support services and adaptive or therapeutic devices include the
following:
Related services, for example speech, physio- or occupational therapy;
intervention of psychologists or social workers
Adaptive technology, for example computers, communication devices,
hearing aids and wheelchairs
Prosthetic supports, for example splints or braces
Staffing, for example facilitators and classroom assistants
3.6 ASSESSMENT OF SKILLS
Teachers are trained to assess skills areas and have many test formats they
use and adapt successfully, but the “I don’t know where to start” reaction is
all too common when faced with a learner with complex learning needs.
Having engaged in a process like MAPS or COACH, the team may want to
systematically gather additional information about specific skills areas. One
such strategy would be the use of a skills checklist (see Table 3.4). Items in
this list provide no more than an overview of levels of function in different
skills areas. The comment column is really important because children
seldom fit into neat columns.
Table 3.4 Skills checklist for screening children with disabilities in an educational
context
SKILLS CHECKLIST
Name of learner:
Date:
Teacher:
Activity:
Key
N/A or not
observe d
1 = Severe
difficulties
2 = Definite
difficulties
3 = Suspected
difficulties
4 = Within
normal limits
1 Severe difficulties:
The learner finds it extremely difficult or impossible when performing the
required task.
2 Definite difficulties:
The learner experiences marked difficulty when performing the required
task.
3 Suspected difficulties: The learner experiences minor or subtle difficulties when performing the
required task.
4 Within normal limits: The learner is able to perform the required task at the same level as
typically developing peers.
Please TICK the correct response:
A
Learning skills/cognitive skills
A1
How well does the learner maintain
concentration for a table-top activity? (Length
of time = child’s age + 3 minutes)
N/A
1
2
3
4
Comments
A
Learning skills/cognitive skills
A2
How well does the learner search for a hidden
object? (Object permanence)
A3
How well is the learner aware that certain
actions have certain effects? (Cause–effect
behaviour)
A4
How well does the learner direct a person or
use an object to get something else?
A5
How well does the learner demonstrate the
function of an object? (Functional object use)
A6
How well does the learner identify an item from
a choice of three well-known objects? (Book,
ball, cellphone)
A7
How well does the learner match similar
objects in pairs? (Familiar objects)
A8
How well does the learner match similar
photographs/pictures in pairs?
A9
How well does the learner identify objects?
(e.g. “Show me the book, ball, cellphone.”)
A10
How well does the learner identify pictures and
photographs? (At least five pictures)
A11
How well does the learner identify line
drawings/symbols? (At least five symbols)
A12
How well does the learner recognise sight
words? (Own name, logos, e.g. SIMBA, CocaCola, Checkers, SABC)
A13
How well does the learner read and
understand single words?
A14
How well does the learner read and
understand simple sentences?
A15
How well does the learner read and
understand complex sentences?
B
Motor skills
B1
How well does the learner walk independently?
B2
How well does the learner sit in a classroom
chair?
B3
How well does the learner sit in a
wheelchair/other adaptive seating?
B4
How well does the learner manage physical
activities on the playground?
N/A
1
2
3
4
Comments
N/A
1
2
3
4
Comments
A
Learning skills/cognitive skills
B5
How well does the learner point to a desired
person/object?
B6
How well does the learner hold a
pencil/crayon?
B7
How well does the learner use a pair of
scissors?
B8
How well does the learner manipulate small
objects?
B9
How well does the learner manage dressing
skills?
B10
How well does the learner manage to use
eating utensils?
B11
How well does the learner imitate or copy
gestures (manual signs)?
C
Sensory skills
C1
How well can the learner see the
blackboard/whiteboard?
C2
How well does the learner visually follow a
moving object (e.g. the teacher’s finger)?
C3
How well can the learner identify a target item
out of a group of nine familiar items?
C4
If the learner cannot see, how well can he
identify objects by touching/feeling them?
C5
How well does the learner hear when being
spoken to?
C6
How well can the learner hear when being
called from a distance?
C7
How well can the learner hear when
instructions are given in a noisy situation?
C8
How well does the learner tolerate different
textures of clothing?
D
Social/emotional behaviour
D1
How well does the learner interact with family
members and caregivers?
D2
How well does the learner interact with peers?
D3
How well does the learner interact with
strangers?
N/A
1
2
3
4
Comments
N/A
1
2
3
4
Comments
N/A
1
2
3
4
Comments
A
Learning skills/cognitive skills
D4
How well does the learner make eye contact
during interaction?
D5
How well does the learner take turns in
interaction? (Turn-taking skills)
D6
How often does disruptive/aggressive
behaviour occur? (Often = 1, never = 4)
D7
How often does the learner hurt/injure himself?
(Often = 1, never = 4)
D8
How often does self-stimulation occur (e.g.
rocking, hand flicking)? (Often = 1, never = 4)
E
Communication skills
Desire to communicate
E1
1
2
3
4
Comments
N/A
1
2
3
4
Comments
N/A
1
2
3
4
Comments
N/A
1
2
3
4
Comments
How strong is the learner’s desire to
communicate?
Communication functions
E2
How well does the learner initiate or start an
interaction?
E3
How well does the learner draw attention to
himself?
E4
How well does the learner use social
comments and greetings?
E5
How well does the learner request objects?
E6
How well does the learner ask for help?
E7
How well does the learner show disagreement
or protest?
E8
How well does the learner use yes and no
responses?
E9
How well is the learner able to make
comments (i.e. expand on what is said or done
by others)?
E10
If a person cannot understand the learner, how
well can the learner try to repair the
communication breakdown by using other
means of communication to make himself
clear?
Communication modes
E11
N/A
How intelligible is the learner’s speech?
A
Learning skills/cognitive skills
E12
How well does the learner use simple
sentences (using any modality) to
communicate?
E13
How well does the learner use facial
expressions (smile, frown, etc.) to
communicate?
E
Communication modes
E14
How well does the learner use natural gestures
to communicate?
E15
How well does the learner use manual signs
(e.g. SASL) to communicate?
E16
How well does the learner point to objects as a
way to communicate?
E17
How well does the learner point to pictures or
photographs to communicate?
E18
How well does the learner use orthography
(print) to communicate?
Receptive language
E19
How well does the learner understand single
words?
E20
How well does the learner understand simple
instructions or questions?
E21
How well does the learner understand complex
questions and instructions?
E22
How well does the learner understand longer
explanations in class?
E23
How well does he understand more complex
language (jokes, idioms, etc.)?
N/A
1
2
3
4
Comments
N/A
1
2
3
4
Comments
N/A
1
2
3
4
Comments
3.7 CONCLUSION
Albert Einstein once said: “I never teach my pupils. I only attempt to
provide the conditions in which they can learn.” This shows that the best
teaching we can give is to provide the learners in our classrooms with
environments that provide learning opportunities.
Assessment (evaluation and goal setting) is one such an opportunity.
Assessment is a challenging process, especially when learners with
significant disabilities are marginalised or excluded for any reason. Chapter
1 alludes to a journey of which assessment is only a part. It is a journey of
exploration and discovery: the “real” child is revealed along the way within
his family and community. His strengths and assets are uncovered like a
treasure and used to plan ahead. The journey has rhythm: the ongoing cycle
of assessment and instruction, the movement of a precious child through the
phases of school and the continuous growth towards independence.
Discovering and unleashing that potential is what makes teaching
worthwhile.
REFERENCES
Bornman, J., Donohue, D.K., Maré, N. & Dada, S. 2016. Comparing two response modes in a
mathematics test for learners with severe physical disabilities: a South African example.
International Journal of Education Studies, 14(1, 2): 37–44.
Bouwer, C. 2016. Identification and assessment of barriers to learning. In Landsberg, E., Krűger, D.
& Swart, E. Addressing barriers to learning. A South African perspective, 3rd ed. Pretoria: Van
Schaik.
Bulloch, K. 2008. Adapting materials and strategies for special needs students. SAALED News,
28(1): 3–4.
Cohen, L.G. & Spenciner, L.J. 2007. Assessment of children and youth with special needs. Boston,
MA: Pearson.
Department of Basic Education. 2011. Curriculum Assessment Policy Statements (CAPS). Available
at: http://www.education.gov.za/Curriculum/CurriculumAssessmentPolicyStatements(CAPS).aspx
Department of Basic Education. 2014. Curriculum Assessment Policy Statements (CAPS). South
African Sign Language. Home language. Senior Phase. Grades 7–9. Available at:
http://www.education.gov.za/LinkClick.aspx?
fileticket=kexx5oS071U%3d&tabid=420&portalid=0&mid=2373
Department of Education. 2001. Education White Paper 6. Special needs education: building an
inclusive education and training system. Pretoria: Department of Education.
Department of Education. 2008. National Strategy on Screening, Identification and Support. Pretoria:
Department of Education.
Department of Education. 2012a. National Policy Pertaining to the Programme and Promotion
Requirements of the National Curriculum Statement Grades R–12. Pretoria: Government Printer.
Department of Education. 2012b. National protocol for Assessment Grades R–12. Pretoria:
Government Printer.
Giangreco, M.F., Cloninger, C.J. & Iverson, V.S. 2011. Choosing Outcomes and Accommodations for
Children (COACH): a guide to educational planning for students with disabilities, 3rd ed. Baltimore:
Paul H. Brookes.
Karan, O.C., DonAroma, P., Bruder, M.B. & Roberts, L.A. 2010. Transitional assessment model for
students with severe and/or multiple disabilities: competency-based community assessment.
Intellectual and Developmental Disabilities, 48(5): 387–392. doi:http://dx.doi.org/10.1352/19349556-48.5.387
Lewandowski, L.J., Berger, C., Lovett, B.J. & Gordon, M. 2015. Test-taking skills of high-school
students with and without learning disabilities. Journal of Psychoeducational Assessment, 1–11.
Lombard, B.J.J. 2010. Outcomes-based assessment: exploring the territory. In Meyer, L., Lombard,
K., Warnich, P. & Wolhuter, C. (Eds). Outcomes-based assessment for South African teachers.
Pretoria: Van Schaik.
Lovett, B.J. & Lewandowski, L.J. 2014. Testing accommodations for students with disabilities:
research-based practice. Washington, DC: APA Books.
Luke, S.D. & Schwartz, A. 2007. NICHY evidence for education: assessment and accommodations,
Vol. 2, Issue 1.
http://www.nichcy.org/Research/EvidenceForEducation/Documents/NICHCY_EE_Accommodations.
pdf (accessed on 12 January 2009).
Mastropieri, M.A. & Scruggs, T.E. 2010. The inclusive classroom: strategies for effective instruction,
4th ed. Upper Saddle River, NJ: Prentice Hall.
Mavuso, M.F. 2015. Identification of specific learning and language difficulties in the classroom and
assessment adaptation. In Dunbar Krige, H. (Ed.). Guidelines for assessment adaptation. Pretoria:
Van Schaik.
Nathanson, S. 2006. Harnessing the power of story: using narrative reading and writing across
content areas. Reading Horizons, 47(1): 1–26.
National Center for Learning Disabilities (NCLD). 2006. Accommodations for students with learning
disabilities. Available at: http://www.ldonline.org/article/Accommodations_for_Students_with_LD?
theme=print
O’Brien J. & Pearpoint, J. 2007. Person-centered planning with MAPS and PATH: a workbook for
facilitators. Toronto, Canada: Inclusion Press.
Potter, K., Lewandowski, LJ. & Spenceley, L. 2015. The influence of a response format test
accommodation for college students with and without disabilities. Assessment and Evaluation in
Higher Education, DOI: 10.1080/02602938.2015.1052368
Raymond, H. 1995. Inclusive education: stories and strategies for success – Chapter 3. Available at:
http://www.ualberta.ca/~jpdasd dc/inclusion/raymond/ch3a.html
Smit, M. & Engelbrecht, P. 2011. South Africa. In Russo, J.C. (Ed.). The legal rights of students with
disabilities: International perspective. Plymouth, UK: Rowman & Littlefield Publishers Inc.
Tindal, G. 2013. Curriculum-based measurement: a brief history of nearly everything from the 1970s
to the present. ISRN Education, 2013, Article ID 958530, 29 pages, doi:10.1155/2013/958530
Tomlinson, C.A. & Imbeau, M.B. 2010. Leading and managing a differentiated classroom.
Alexandria, VA: Association for Supervision and Curriculum Development.
United Nations Educational, Scientific and Cultural Organization (UNESCO). 2009. Policy
Guidelines on Inclusion in Education. Paris: UNESCO.
United Nations Educational, Scientific and Cultural Organization (UNESCO). 2012. Report of expert
panel: challenges in basic mathematics education. Paris: UNESCO.
United Nations General Assembly (UN). 1989. Convention on the Rights of the Child. Available at:
http://www.ohchr.org/EN/ProfessionalInterest/Pages?CRC.aspx.persons
Vandercook, T., York, J. & Forest, M. 1989. The McGill Action Planning System (MAPS): a strategy
for building the vision. Journal for the Association for Persons with Severe Handicaps, 14: 205–215.
Venter, R. 2015. Principles, purposes and nature of assessment adaptations. In Dunbar Krige, H.
(Ed.). Guidelines for assessment adaptation. Pretoria: Van Schaik.
Westling, D.L. & Fox, L. 2009. Teaching students with severe disabilities, 4th ed. New Jersey:
Pearson.
4
Teaching practices
4.1 INTRODUCTION
To accommodate the diversity that exists in schools today, teachers must
strive towards creating supportive classrooms with a strong sense of
belonging – ones that facilitate the development of children’s strengths and
address their diverse needs. This might sound like the Hollywood movie,
Mission Impossible, but turn-around teachers see opportunities where others
see impossibilities. In this chapter we will explore teaching strategies that
will encourage and facilitate the participation of all learners so that all can
achieve academically, socially and emotionally.
4.2 SETTING UP THE INCLUSIVE CLASSROOM
To be accepted and to belong are basic human needs, yet research shows
that many classrooms are highly structured places, dominated by
authoritarian teachers, where learners have few choices and limited
opportunities to develop relationships with teachers or classmates. This
leads to children feeling that they are not valued and not important
members of their class (Bucholz & Sheffler, 2009; Motitswe, 2012).
So what can teachers do to create a classroom where there is a true sense of
belonging? Mary Beth Hewitt (2007), a teacher, asked a number of children
how they knew that they belonged to a group, and this is what they said:
“They know my name”; “They spell my name right”; “They ask me what I
want to be called”; “They take time to talk to me”; “They smile at me”;
“They ask me to help”; “They recognise when I’m gone and welcome me
when I return”. These are not difficult or time-consuming strategies!
All teachers should aspire to create democratic, inclusive classrooms in
which mutual respect, cooperation and learning is valued. This type of
classroom will have a particular ethos, of which five critical characteristics
will be described.
4.3 CLASSROOM ETHOS
4.3.1 Create a warm, welcoming classroom environment
The first thing many teachers do at the beginning of a new year is to
decorate their classrooms. These teachers have discovered a great secret:
children are sensitive to the atmosphere in the classroom, and a warm
classroom environment can increase academic achievement and a sense of
pride and belonging in the school (Bucholz & Sheffler, 2009). If not set up
appropriately, classrooms can stifle creativity and not promote learning. The
colour used in the classroom is also important as it should maximise
information retention and stimulate participation, but not overstimulate
learners, which can happen when a large number of bright colours are used,
especially reds and oranges. Calmness, relaxation, happiness and comfort
are feelings elicited by using colours such as green and blue on classroom
walls (Smith, 2016). The choice of pictures on the wall reflects the teacher’s
respect for diversity (including cultural awareness as well as disability
sensitivity), and hence they should avoid stereotypical representations. For
example, pictures should show children in wheelchairs, children who use
hearing aids, cochlear implants, and so forth (VanHousen, 2013). Organise
furniture in such a way that there is enough space for all learners (including
those in wheelchairs) to easily move throughout the classroom. Arrange
desks so that they create opportunities for group engagement and learning
(when appropriate). Desks can be organised in a circle around the classroom
in smaller classes, but can also be used in larger ones, for example when a
music, drama or public speaking event is held (Hannah, 2013).
4.3.2 Establish mutual respect
Mutual respect implies that teachers and learners are equal participants in
learning. Some teachers might feel threatened by this concept, feeling that it
could potentially undermine their authority. In actual fact this is the way
children learn to respect themselves and others as they begin to understand
that their opinions and ideas are valued, and in this way learning is
enriched. Respect is an important concept to learn when addressing the very
real problem of bullying. If problems do arise, teachers should see it as an
opportunity to teach children to resolve conflict, which is a real-life skill.
The teacher should help the children to determine the source of the
problem, to examine the effects of the behaviour on the other learners and
to find alternative solutions.
Stop and reflect
Heinrich is a Grade 3 boy who suffered at the hands of the school bully with the rest
of his peers. After watching a school play about bullying, he confronted the bully, and
told him how his behaviour hurt the other children and how scared they all are of him.
This took the bully totally by surprise and he thanked Heinrich for talking to him,
saying that nobody had actually spoken to him about his behaviour and he did not
realise they were scared of him. He said that he did not have any friends, and bullying
was how he thought he could make the children notice him. He vowed to stop
bullying, and a year later became a popular peer. Even relatively young children can
be taught how to resolve conflict!
Many strategies can be used to develop mutual respect, for example
nickname research, so that children understand the negative effect of these
unkind labels, and “learner-of-the-week” displays in which all children have
the opportunity to “shine”.
4.3.3 Encourage participation
Participation can be achieved by focusing on learner assets and strengths, as
this determines the classroom ethos. In the past, there was a focus on one
single intelligence (IQ) as being the most important predictor of school
achievement. However the landmark work of Howard Gardner (1993) on
multiple intelligences has revolutionised how we view intelligence.
Professor Gardner identifies eight types of human intelligence that represent
different ways in which we process information:
Verbal-linguistic intelligence: this refers to the ability to analyse
information and produce work that involves oral and written language,
such as speeches, books and e-mails. Teachers can capitalise on this by
getting learners to do oral activities (storytelling, discussing,
interviewing) before doing written assignments, completing crossword
puzzles with vocabulary words, and playing games like Scrabble
(Lunenburg & Lunenburg, 2014).
Logical-mathematical intelligence: this refers to the ability to develop
equations, make calculations and solve abstract problems. Teaching
children to look at the writing process as a logical progression of tasks,
offering cause–effect as prompts for writing, teaching grammar rules, and
showing children how to search for patterns in the classroom, at school,
outdoors and at home will greatly support these learners (Bratcher, 2012).
Visual-spatial intelligence: this refers to the ability to comprehend maps
and other types of graphical information. Teachers can strengthen this
type of intelligence by using diagrams to teach writing concepts such as
triangles, clusters, webs and maps; using pictures as prompts for writing;
using colour coding for grammar errors (Lunenburg & Lunenburg, 2014);
and illustrating poems by drawing or using computer software (Bratcher,
2012).
Musical intelligence: this refers to the ability to produce and make
meaning of different types of sound. Teachers can capitalise on this by
reading poetry aloud and clapping to accentuate the rhythm of the words,
singing folk songs and having learners write new verses, listening to rap
music and getting learners to write their own (Lunenburg & Lunenburg,
2014).
Naturalistic intelligence: this refers to the ability to identify and
distinguish among different types of plants, animals and weather
formations found in the natural world. Learners benefit from activities
such as caring for classroom plants based on best practices research;
sorting and classifying natural objects such as plants and rocks;
researching animal habitats and writing essays on the topic; and
observing natural surroundings in preparation to writing about them
(Lunenburg & Lunenburg, 2014).
Bodily-kinaesthetic intelligence: this refers to using the body to create
products or solve problems, such as using drama and/or dance. Strategies
that are effective include acting out stories before writing them, writing
plays that include stage directions, playing charades to teach new
vocabulary words, and building objects using blocks, cubes or Lego to
represent concepts (Lunenburg & Lunenburg, 2014).
Interpersonal intelligence: this refers to an ability to recognise and
understand other people’s moods, desires, motivations and intentions. In
classrooms this can be encouraged by placing learners in learning groups
to design and complete writing projects; using peer groups for
brainstorming, revising and editing their work; connecting writing
activities to the community outside the school (e.g. get children to write a
newspaper report about a community activity); inviting guests to the
classroom to tell stories or to talk about writing; and using puppets to
teach writing strategies (Bratcher, 2012).
Intrapersonal intelligence: this refers to an ability to recognise and assess
moods, desires, intentions and motivation within oneself. Effective
strategies include teaching learners to keep personal journals; having
learners choose their best writing pieces for portfolios; allowing time for
self-reflection about writing; using life maps and personal topics as
springboards for writing; and writing essays from the perspective of
famous literary figures (Lunenburg & Lunenburg, 2014).
It is important that these multiple intelligences are not confused with
learning styles. Everyone has all eight types of intelligences, but at varying
levels of aptitude, and some might even still be undiscovered (Hattie, 2011).
Teachers should thus be encouraged not to ask: “How smart is the child?”
but rather: “How is the child smart?”
Learning styles, on the other hand, refer to the ways in which an individual
approaches a task. These have been categorised in a number of different
ways: some authors refer to visual, auditory and kinaesthetic styles; some to
impulsive and reflective styles; and some to right brain and left brain
(Tomlinson, 2014). Learning is dynamic (which means that it is ever-
changing) and complex, and therefore it is important that teachers are aware
of the different types of intelligences and learning styles to capitalise on
them (see Figure 4.1), but not to label children as only one type of learner.
Figure 4.1 Inclusion is about involving all the learners in the class
Stop and reflect
If Lesedi is very good at music, the names of the different planets in the solar system
can be taught in a song, as this will help her remember them better. Jackie, on the
other hand, learns by seeing, so to help him learn optimally the teacher could use
flashcards. To involve the whole class, each child can be given a board on which the
name of a planet is written, with one being the sun. The teacher can then ask the
children to sing the song that they learnt, and while they are singing, the children who
represent the different planets can arrange themselves in the correct order: Mercury,
Venus, Earth, Mars, and so on. Although these two activities have been designed
specifically to accommodate Lesedi and Jackie, it is clear that all the learners in the
class will benefit.
Another strategy that teachers can use to increase participation is through
creating special traditions for their classrooms as this helps create feelings
of belonging (Bucholz & Sheffler, 2009). For example, children can work
together to create a class pledge that they recite every morning before the
day begins. For example, Mrs Maake created one using the four Ls: We will
Laugh, we will Listen, we will Learn. We will have a Lovely day. For older
children, teachers can ask them to bring an inspirational quote that can be
shared before the lesson starts.
4.3.4 Provide decision-making opportunities in the classroom
It is well known that children are more inclined to accept and follow
classroom rules that they helped to create, and to participate enthusiastically
in projects that they helped design (VanHousen, 2013). In order to achieve
this, teachers can introduce some self-management tools, for example
teaching the children to hold class meetings and make collaborative
decisions on a range of activities each week (Bucholz & Sheffler, 2009;
Hannah, 2013; Shaddock, Giorcelli & Smith, 2007). These classroom
meetings can also teach learners to work together, to solve problems while
providing them with the opportunity to practise their social skills. Research
has also shown that if learners are given responsibilities and held
accountable for their actions within a predictable school and classroom
environment, teachers will need to spend less time on classroom
management and discipline (Jerome-Freiberg, Huzinec & Templeton,
2009).
Stop and reflect
A Grade 3 class was invited by a swimming instructor to participate in a swimming
activity in order to help them all become water safe. This activity was scheduled for
twice a week for a month. Before the activity began, the instructor emphasised that
everyone was expected to participate, as being water safe is an important life skill,
and that previous swimming experience was not a prerequisite. One child, Komotso,
adamantly refused to participate. The instructor had two choices of how to react: she
could have said: “You have to participate, it is compulsory, and if you do not, you will
have to see the principal and then get detention.” (The result of this might also have
created chaos and upset some of the other children in the class.)
The other option was that the teacher could have asked: “Why don’t you want to
participate when we will all be having fun?” Komotso explained that he was scared as
he fell into a dam when he was younger and that he felt as if he could not breathe
when he was in the water. The instructor then realised that he would require intensive
one-to-one instruction, and asked Komotso and his classmates how they thought he
could still participate without getting into the water. They came up with the following
options:
Komotso could keep a journal about every swimming lesson and describe what
everybody was doing.
Komotso could hold the stopwatch and see how his classmates’ speed improved.
Komotso could draw pictures and write instructions on what to do to help a
classmate who was absent.
Everybody in the class benefited from this, and Komotso kept his dignity and felt like
a valuable part of the class.
Komotso’s story illustrates the positive outcomes of learner-centred
problem solving and decision making. Giving children a role in decision
making allows them to take responsibility and ultimately increases their
motivation (Mol, 2007).
4.3.5 Develop self-discipline
The most important element for achieving self-discipline is consistency. A
teacher has to be absolutely consistent in how she keeps discipline in her
classroom. Children become angry and frustrated if the same behaviour
elicits different consequences in the same setting (Shaddock et al., 2007).
For example, sometimes a teacher punishes the learners if they talk during
lessons, while she does not seem to mind at other times. If the rules in the
classroom are consistent, this helps learners to feel safe as they know what
is expected of them (VanHousen, 2013). Classroom rules should be short
and sweet, stated in positive terms and kept to a minimum.
Stop and reflect
Mrs Louw uses the “Big 5” to teach her Grade R class about classroom rules:
Elephant: it has very large ears, which means it can listen well. Children can be
like elephants and also listen well.
Leopard: it takes its prey up a tree before starting to eat, which means that it is not
lazy and perseveres – it works hard before it can eat.
Buffalo: it has a thick skin that is not easily hurt, which means that one should not
worry about everything other children say.
Rhino: legend has it that if there is a fire, a rhino will always rush in and stamp it
out, so when friends fight, children should also try to stop the fight (fire), for
example by calling a teacher.
Lion: all the animals respect the lion, and the lion also respects the other animals,
which means that children should respect each other.
These rules should be displayed in the classroom for all learners to see.
Table 4.1 shows classroom rules for older children.
Table 4.1 Effective and less-effective classroom rules
Effective rules
Less-effective rules
Work quietly at your desk.
Do not disturb the other learners.
Always have clean hands when working
in your book.
You will be in big trouble if your book is dirty.
Put your hand up when you know the
answer.
Do not shout out the answer.
Give everybody a chance and listen to
each other.
Do not make a noise and interrupt others.
Stand up when visitors enter the
classroom.
Do not misbehave when there are visitors in
the classroom.
It is good teaching practice to give an explanation as to why a particular
behaviour is unacceptable. In the long term this helps children develop
problem-solving and critical-thinking skills. For example, rather than
simply saying: “Because I am the teacher” or “Because I said so”, the
teacher could say: “Because we have a classroom in which we respect each
other, and if we behave in that way, it shows that we don’t have respect for
ourselves or for others”. Words of admiration, praise and encouragement
are powerful tools for teachers as they reinforce positive behaviour (Gliebe,
2011). Teachers should also remember to acknowledge appropriate
behaviour and to explain to the learners that this type of behaviour is
valued. Children need to know that they are responsible for the choices they
make, and that every choice has a natural and logical consequence. For
example, if they decide to kick a ball in the classroom and accidentally
break a window, they may have to pay for the repair or do some community
service (e.g. clean the bathrooms or put out the chairs in the school hall for
a function).
4.3.6 Become a role model
Actions speak louder than words, and teachers should be aware of the fact
that children observe everything they do! As teachers shape learner
behaviour, they should be sure to model the behaviours they expect from
the learners (Shaddock et al., 2007). Teachers with character demonstrate
that integrity is something to strive for by modelling behaviours such as
telling the truth, respecting others, accepting and fulfilling responsibilities,
playing fair, earning and returning trust, and leading a moral life (Lumpkin,
2008). Teachers should thus strive to teach all learners that it is better to do
the harder right things than the easier wrong things. Learners respond well
to teachers with character who are willing to be role models.
4.4 GETTING TO KNOW EACH CHILD
You cannot teach a child if you do not know that child! In Chapter 3 we
explained that the main aim of assessment is to gain an understanding of the
child’s specific strengths and needs rather than to only assign a particular
mark to the child. Every child can learn, just not on the same day or in the
same way! Contrary to popular belief, a child’s disability may impact on
learning, or it may have little impact at all (Shaddock et al., 2007).
Moreover, children who have the same diagnosis may be alike in some
respects, but they will differ in personality, temperament, skills, interests
and capability. It is therefore incorrect to make assumptions that, for
example, all children with Down Syndrome enjoy hugging and cuddling.
The disability diagnosis is just one of many aspects that teachers need to
consider in the inclusive classroom.
If a teacher gets to know a child well, she can capitalise on what motivates
that particular child. Motivation can be defined as the thoughts that learners
have about themselves, school and schoolwork, which precedes
participation (Martin, 2005). How do we know when learners are
motivated? They pay attention, they start working on tasks immediately,
they ask relevant questions and volunteer answers, and they appear to be
happy and eager (Williams & Williams, 2011). Motivation is also
associated with positive thoughts (e.g. feeling confident, seeing the value of
school, focusing on learning, solving problems and developing skills) and
this results in productive behaviours (e.g. persevering, planning and
studying). Teachers should be conscious of small details, as everything they
do in the classroom influences learners either positively or negatively. So if
a teacher knows that a particular child is really interested in birds, she can
tap into this interest across themes and activities, for example in natural
science, art and even maths. This way the child feels valued and
acknowledged. However, the opposite is also true. Negative thoughts (e.g.
being anxious about tasks, performance and results; not feeling in control of
learning and avoiding failure) result in poor academic performance.
All learners also need to experience a feeling of belonging; in other words,
all children need to feel that “school is for me” – they have to feel
supported as individual learners and also as members of a cohesive group of
learners. In contrast, those learners who do not experience this sense of
belonging feel alienated, which invariably results in poor academic and
social outcomes.
Stop and reflect
Can you still recall Rachel Serudu’s story in the beginning of the book? One of the
factors hindering her learning was the fact that she remained an outsider, and that
she never felt like part of the school – she never had the feeling of “school is for me”.
What can schools do in order to become inclusive schools that create a
sense of belonging in which each child feels valued?
Establish a positive school and classroom ethos by conveying a real sense
of caring to all learners and making each one feel special, (Munns et al.,
2006).
Instil a fire for lifelong learning in all children by capturing their interests
(Williams & Williams, 2011).
Help learners outside of the classroom and at odd hours, and be devoted
to them (Williams & Williams, 2011).
Expand choices within the curriculum in order to support a wide range of
learning styles (Motitswe, 2012).
Set up a variety of extracurricular activities that cater for many different
interests, for example sport, chess, cultural dancing (Munns et al., 2006).
Provide peer support by using a “buddy system” as this helps to create a
collaborative learning environment in which learners feel free to ask
questions from their “buddies” rather than asking the teacher the
question, which results in effective learning (Thalluri, O’Flaherty &
Shepherd, 2014).
Ensure positive role models (Lumpkin, 2008).
Implementing such strategies teaches all children that their school and their
teachers will nurture them and help with both academic and extracurricular
activities. No learners will be left to fall through the cracks. When learners
experience a sense of belonging and achievement, they will be motivated to
participate in class activities.
4.5 TEACHING STRATEGIES FOR ALL LEARNERS
No matter how hard it is to teach a child with a disability, it is always harder
to be the child! Teachers are often scared when confronted with teaching in
an inclusive school as they fear that they will have to work much harder and
that they will need to adapt everything that they do, all of the time.
However, it is not about working harder, but rather about working smarter.
Once good teaching practices are in place, the accommodations that are
needed might be very small (see Figure 4.2).
Figure 4.2 General education and
adaptations
These two circles represent general education and the adaptations (special
education) that are required in the inclusive classroom. As teaching
practices improve, the fusion, known as differentiated teaching, should
become larger and the adaptations eventually fewer. A teacher once said: “If
children cannot learn from the way I teach, I should teach in a way that
they can learn.” This describes clearly the fact that the teacher is the one
who should be making the adaptations and not the learner, as it is easier for
teachers to change the way in which they teach than for children to change
the way in which they learn. In this chapter, we will be exploring four
different teaching strategies that could be used with all learners, irrespective
of whether they have a disability or not.
4.5.1 Teaching strategy 1: maximising time on task (academic
engagement)
There is a well-known saying that “practice makes perfect”. Gary Player
illustrated this when he said: “The harder I practise the luckier I get.” This
is also true for all classroom tasks and activities. The more time learners
spend reading, writing, doing maths or science, the better the learning
outcomes are likely to be. We simply cannot learn any new skill or develop
further ones without spending a certain amount of time grasping the new
content and practising our knowledge and skills.
Stop and reflect
Kayla is in Grade 4 in Mrs Botha’s class, but she is struggling academically, despite
the fact that Mrs Botha feels that she has the ability to do much better. In an attempt
to find out why Kayla almost never completes her work, why her books are not neat
and why she does so poorly in her tests, Mrs Botha decides to watch Kayla more
closely in the classroom. She makes an interesting discovery – Kayla is always the
last one to take out her book and her pen, she seems to take a long time before she
settles down and starts working, and as soon as she eventually starts, she stops
again either to sharpen a pencil, talk to a friend or ask permission to go to the toilet.
Instead of spending 30 minutes writing sentences, Kayla is only actively engaged in
the activity for about 15 minutes. Clearly this will have to change if she is to succeed
academically!
So what can be done to overcome this problem? First of all, teachers need
to ensure that the learners are physically and intellectually engaged in the
learning opportunities and activities, as this has been noted as one of the
strongest predictors of achievement outcomes (Hoxby & Murarka, 2008).
This will obviously depend on the specific subject that is being taught.
During a social sciences lesson, for example, learners can be expected to
answer questions posed by the teacher, to take notes or to draw up an
outline of the most important points (Mastropieri & Scruggs, 2010). During
a science lesson, on the other hand, they can perform experiments. Bear in
mind that some children who face barriers to learning might not respond in
the traditional ways. For example, a child with physical impairments might
not be able to participate in a science experiment, but can still be actively
engaged, and a child with visual impairment can be actively listening to the
teacher even though he may not be able to see her.
Second, teachers should bear in mind that their teaching style influences
how much children learn. Keeping all statements relevant to the lesson, as
well as the lesson objectives and possible questions, close at hand will
facilitate this process. It is often difficult for learners to differentiate
between the important information and trivia. It is particularly difficult for
children when the teacher is unprepared (e.g. she does not have all the
elements close by for a science experiment).
Children have reported the following classroom strategies to be helpful
(Nind, 2006):
When teachers provide help discreetly (and quietly)
When teachers give out handouts with a summary of the lesson
(particularly for certain subjects)
When teachers allow opportunities for group work
When teachers show that they care
When teachers provide opportunities for catch-up exercises
Teachers, on the other hand, compiled this list of classroom strategies that
they felt had the most positive academic outcomes (Mastropieri & Scruggs,
2010):
When teachers use time efficiently
When teachers have good relationships with learners
When teachers provide positive feedback and supportive comments and
responses
When teachers offer additional support for those learners in need
When comparing these two lists, it is interesting to notice how they
complement each other – it seems that effective classroom strategies are
about having a caring relationship with the learners, and that the learners
should be aware of this fact (the teachers’ pastoral role), and that teachers
should provide positive feedback and discreet help to those in need and,
finally, that there should be opportunities for additional assistance and
catch-up exercises.
What can teachers do to help individual learners, like Kayla, who really
seem to struggle to spend more time on their schoolwork? First, they should
ensure that the learners have the ability to do the work and that they are not
trying to avoid it because they fear that they might fail. Talk to the child and
if this is the case, try to match the child with a study buddy (Thalluri et al.,
2014). In some cases, the work is not challenging enough, and then the
child might be given some enhanced work to stimulate his thinking.
Second, a teacher can try to be physically close to them and prompt them to
get back to work, or use a specific hand signal to remind them to
concentrate (Mastropieri & Scruggs, 2010). Third, rewards or other positive
consequences can be given if the child does stay on task. Praise learners for
effort, e.g. “I can see you really tried your best!” or “Wow! You worked
hard!”, and provide feedback that encourages them to try different
strategies, e.g. “Can you think of another way to do it?”. Research is
showing that children who receive praise for effort, e.g. “You worked hard”
start believing that their accomplishments are the result of effort and
deliberate practice, whereas children who receive personal praise, e.g.
“You’re so smart” start believing that accomplishments are fixed traits, and
that they have no control over them (Gunderson et al., 2013). Furthermore,
if children are given specific praise, e.g. “You did a good job drawing”, task
persistence increases rather than when they are given generic praise, e.g.
“You are a good drawer”, as this generic praise then functions as personal
praise (Zentall & Morris, 2010).
Stop and reflect
If Kayla were in your class, how would you go about creating more opportunities for
her to remain on task?
4.5.2 Teaching strategy 2: managing time effectively
Time is an abstract concept, and teaching children to use time effectively is
crucial. Learners might find it difficult to know how much time is left to
complete an activity, and this often leads to their not finishing their work.
Can you still remember Kayla’s story? When children start writing tests that
have a time limit, the effect of this could be disastrous. For some children,
the transition between different classroom periods is especially difficult as
they do not have a good concept of time. How can a teacher assist children
with time management?
Teachers can help by giving a ten-minute warning: “The bell will ring in ten
minutes. You have to start thinking about finishing your work.” This will
prompt them to start finishing. In a test, a teacher can also help with time
management by allocating proportional times to the paper, e.g.: “We have
30 minutes and five questions. This means that you should spend about five
minutes on each question, and then at the end you’ll have a little time left to
read through your answers.” For younger children, a teacher may use a
kitchen timer that ticks audibly as this helps children to hear that time is
passing.
Figure 4.3 Using a handmade timer
Stop and reflect
Let us look at the example of a truly creative teacher at work in a rural part of the
Northern Cape province. In order to help the children understand the concept of time
passing, she made an enormous timer. She took two two-litre plastic cool-drink
bottles, filled the one with sand, and strapped them together at their spouts. It took
about five minutes for the sand to flow from the one bottle to the other. Five minutes
before the end of the lesson, she would turn the bottle around and say: “The
countdown has started. Five minutes left before the bell.” This helped children plan
their time better and prepare for the transition between periods. This creative
invention had a significant impact in the classroom and it did not even cost money!
(See Figure 4.3.)
Using this type of timer can also help when planning classroom activities.
For example, the teacher can say: “You have five minutes to organise
yourself into groups of four”, and then set the timer. This way, valuable
classroom time is not lost, maximising academic engagement opportunities.
4.5.3 Teaching strategy 3: presenting effective lessons
If you think back to your own teachers or university professors, what did
they do that helped you to learn best? Mastropieri and Scruggs (2010) have
developed a tongue-in-cheek acronym that highlights six critical
components of presenting effective lessons:
S
Structure
C Clarity
R Redundancy
E
Enthusiasm
A Appropriate rate
M Maximising participation through questioning and feedback
STRUCTURE
This refers to the way the different components of a lesson are planned, and
not that the learners should sit in neat rows and each complete a worksheet.
The teacher should start every lesson by explaining the main objective (the
learning outcome) in a way that is clear to the children, for example: “In
this lesson we are going to learn about halving and doubling. That means
that we’ll be looking at what happens when we cut things in two, like an
apple – then we have two halves. We will also look at what happens when
we put the two halves together again, we get one whole apple. Right, let’s
get started.”
After having explained the purpose of the lesson, the teacher should also
emphasise its critical elements and help the learners summarise them. A
simple situation–problem–solution–outcome (SPSO) schema on worksheets
(see Table 4.2) has proven to be effective in helping learners understand the
basic structure of lessons (Mortimore & Dupree, 2008). This type of
structure works particularly well for history and science.
Table 4.2 Example of an SPSO worksheet
Situation
Mark Shuttleworth wants to become the first African in space.
Problem
How can he achieve this? He is a businessman and not an astronaut.
Solution
He pays a huge amount of money to the Russian space programme, and
they train him.
Outcome
He becomes the first African in space and creates a lot of awareness about
the importance of science and that children should learn science and maths
at school.
Another type of worksheet structure is a mind map. Teachers, therapists,
psychologists, engineers and others have used mind mapping for decades to
facilitate learning, memory, summarising of facts, brainstorming and
problem solving. Basically, a mind map is a diagram used to visually
represent ideas, words, tasks or other items around a central key word or
theme by using different colours and pictures (Long & Carlson, 2011). To
make a mind map, one starts in the centre of the page with the main idea,
and then branches out in all directions according to the importance of the
concepts, producing a growing and organised structure composed of key
words and key images (Buzan, 2011). Consider the following example. It
shows a mind map for a lesson on mammals.
How can teachers teach learners to draw a mind map? See how easy it is
(refer to Figure 4.4):
Figure 4.4 A mind map
Write the title of the lesson in the middle of the page and draw a circle
around it, for example “Mammals”.
Draw lines radiating out from this circle and label them with the
subheadings (or important facts that relate to the subject), for example
“Characteristics”, “Examples”, “Food”, “Habitat”. These subheadings
will branch off the main fact like branches and twigs from the trunk of a
tree. Do not worry about the structure of your mind map – remember that
each one is unique and will not look like somebody else’s map.
As you start delving more deeply into the facts and uncover another level
of information (further specific facts) belonging to the subheadings
above, draw these as lines linked to the subheading lines.
Finally, for individual facts or ideas, draw lines radiating out from the
appropriate heading line and label them.
By helping learners to draw a mind map, the teacher provides structure and
helps learners to see what the most important concepts in the particular
lesson are. Older learners can be encouraged, while listening to their lesson,
to take down notes using mind maps for the most important facts or
keywords. What is more, mind maps are very quick to review as learners
can often refresh information in their minds just by glancing at it.
Remembering the shape and structure of a mind map can give learners the
cues they need to recall the information within it (Long & Carlson, 2011).
Mind maps can be drawn by hand, either as “rough notes” during a lesson
or as a more extensive means of thinking, planning and learning. There are
a number of software packages available on the Web for producing mind
maps (Mindtools, n.d.).
CLARITY
Teachers should always aim to speak clearly and to the point, and to use
language that children understand. This is particularly important in any
multilingual classroom. Younger children typically do not understand
sarcasm, and many children have great difficulty in understanding
figurative speech, for example “time flies”. When teaching new words, time
should be spent on practising the meaning of the word; for example: “Today
we will learn about synonyms. Synonym is another word for same. Can you
hear they both begin with ssss … synonym – same? Let’s think of a synonym
for big. Huge, enormous, gigantic ….” Teachers can use gestures to show
the meaning of words or to emphasise certain facts. Using gestures will also
be particularly helpful for children with hearing difficulties and those with
learning difficulties.
REDUNDANCY
This is closely linked to structure and means that teachers should emphasise
and reinforce the most important concepts in the lesson. Give the children
some questions that they can always keep in mind, for example: “What is
the main question I am trying to answer? What information do I need to
answer the question?” A specific teaching strategy that teachers can also
use to help with this is the “most important words” strategy. During a
reading activity, for example, the teacher reminds the learners to think about
the most important words in the text. The teacher gives some examples of
important words, and then learners work in groups to identify others. The
strategies that were described to assist with structure (namely SPSO and
mind mapping) would be beneficial.
ENTHUSIASM
Attitudes are contagious. Are yours worth catching?
D
&W
M
Children participate more and hence learn more in classrooms where
teachers are enthusiastic, creative and respectful, and hold high expectations
for themselves and for the children they teach (Tucker & Stronge, 2005).
Enthusiastic teachers create environments that encourage exploration and
thinking, and children experience learning activities as fun, valuable, useful
and focused, but not necessarily as easy. Research concerned with
enhancing academic performance for boys showed that productive
pedagogical relationships between enthusiastic teachers and boys,
characterised by humour, trust and an individual concern, are particularly
significant (Munns et al., 2006).
MAXIMISED PARTICIPATION THROUGH QUESTIONING AND FEEDBACK
Selecting materials with an appropriate difficulty and high-interest level,
together with the careful use of questioning and positive feedback, can
ensure active participation. This will develop each learner’s confidence,
responsibility and enthusiasm for learning.
The effective use of questions is an excellent teaching tool that can
encourage active learning if the right type of questions is asked! The
primary aim in classrooms should not be to present learners with masses of
information, but rather to help them explore, organise, integrate and extend
their knowledge and make it useful in different situations (Beatty, Gerace,
Leonard & Dufresne, 2006). Likewise, questions should focus on learning
(not on memory or recalling facts) and teachers should ask questions to help
learners discover what has been learned, to comprehensively explore the
subject matter, and to generate discussion and peer-to-peer interaction
(Tofade, Elsner & Haines, 2013). When asking a question, the teacher
should allow time for the learners to think of an answer, even if it feels like
a long time! Teachers should allow learners at least ten seconds to respond.
The teacher’s silence will usually encourage an answer. If no one has
answered the question after the ten-second wait and nobody is making eye
contact, try rephrasing the question or providing a hint to prompt a
response.
There are different types of questioning strategies that can be used, for
example:
Use closed questions. These questions require only “yes” or “no”
responses, and asking them at the beginning of a lesson is an effective
strategy as this helps the learners to relax and can give the teacher an idea
how much they already know about the topic. For example, in a
technology lesson the teacher can ask: “Have you ever noticed that the
television looks different when we look at it from the front, from above or
from the side?” or “Can you find all the vowels in the word ‘television’?”
Use open-ended questions. Open-ended questions are more complicated
than closed questions. Examples of open-ended questions include: “How
would you explain photosynthesis?” or “What are some key concepts in
the water cycle?” In an inclusive classroom, this helps teachers to gauge
the children’s level of understanding and modify or adjust their teaching
methodology to enhance learning.
Encourage children to ask questions. In addition to asking specific
questions, teachers should encourage children to also ask questions, as
this is usually a sign that they are listening and learning (Mastropieri &
Scruggs, 2010). This can be achieved by informing the class during the
start of the lesson that you want them to interject by raising their hands
and asking questions at any time. As the lesson continues, teachers might
want to check with the learners to see if they have questions. It is
particularly useful to do so just before moving on to a new concept
because it provides an opportunity to review the main points of the
section.
Use questions to determine what children have learnt. Questions are
effective for determining whether learners are grasping the concepts
being taught. This can be done by asking them if they have any questions
before moving on, or by asking them to raise their hands or nod if they
understand the concept. If a number of learners do not raise their hand,
the teacher needs to revise the concepts.
Use repetition. The same question can also be repeated a few times
throughout the lesson to ensure that the most important concepts are
learned. By the third or fourth repetition, all of the learners should know
and remember the concept.
Use randomised questioning. To ensure that all learners have an
opportunity to answer questions in a fun manner, randomised questioning
can be used. In this strategy, the teacher creates notecards with the
learners’ names on them and then shuffles the cards. After asking the
question and keeping the class in suspense, the teacher draws a card and
reveals the name of the learner who has to answer (see Figure 4.5).
Figure 4.5 Randomised questioning
Identify common pitfalls and how to deal with them. A common pitfall is
the question: “Does everyone understand?” Children usually do not
answer questions that are directed at the group. Some may nod, but this is
not an effective way to gauge the group understanding. Another pitfall is
to ask learners to raise their hand if they do not understand. Most
children are afraid to single themselves out in a group as the one “who
doesn’t understand”. Also, try not to start a question by using a specific
learner’s name, for example “Freddy, can you explain what a
cumulonimbus cloud looks like?”, as this will probably cause the other
learners not to think, as the question is not directed at them. Rather say:
“What are the features of a cumulonimbus cloud? Freddy, can you
explain to us what it looks like?”
Questions have a certain difficulty level, and to develop thinking and
problem-solving skills, the questions that teachers ask should reflect various
difficulty levels (McComas & Abraham, 2005; Tofade et al., 2013).
Thinking and problem-solving skills are both critical to ensure academic
success, but as they do not develop spontaneously they have to be taught.
According to Bloom’s taxonomy, questions are asked on one of six different
levels. However, in a recent study with Grade R teachers in rural KwaZuluNatal, it was found that although some teachers used utterances on all six
levels of Bloom’s taxonomy, by far the highest frequency of utterances was
found on levels 1 and 2 – the easiest levels (Higham, Tönsing, & Alant,
2010). Consider the example of asking questions on the different levels of
Bloom’s taxonomy after reading the story of The three little pigs.
Figure 4.6 The story of The three little pigs
Source of symbols: Detheridge, Whittle & Detheridge (2002)
Story: Author’s own
Level 1. Remembering facts; in other words, retrieving relevant
knowledge from long-term memory, recognising and recalling facts
(Krathwohl, 2002; Tofade et al., 2013). Examples of this would be to ask
children to label pictures, and asking them about numbers and colours.
“What material did the first little pig use to build his house?”; “Which
house was the strongest?”; “What did the wolf do?”
Level 2. Understanding; in other words. finding out if children can
interpret the lesson, if they can give examples, summarise the events,
explain why things happened and compare facts (Krathwohl, 2002).
Examples of this would be to ask the children to retell the story in their
own words, or to ask questions such as: “What happened first?”; “What
happened next?”; “If we don’t use sticks, grass or bricks, what else can
we use to build houses?”
Level 3. Application; in other words, using a procedure in a given
situation (Krathwohl, 2002; McComas & Abraham, 2005). Examples of
this would be to ask the children to break up the story into events, and
then to put them back into the correct sequence again. You can even ask
the children to think what the mother pig would have said to the reporter
from SABC 3 News about the sequence of events.
Level 4. Analysis; in other words, breaking up the story into its parts to
find out how they relate to each other and also to determine the overall
purpose of the story (Krathwohl, 2002). “What did we learn from this
story?”; “Was the wolf a good guy or a bad guy?”; “What would you
have done if you were the third little pig?”
Level 5. Evaluation; in other words, making judgements based on criteria
and standards, and providing critique (Krathwohl, 2002). “Explain if you
think this is just a fairy-tale or if this is still an important story for today’s
children.” However, teachers should realise that in class discussions, this
type of question can lead to digressions in the lesson plan, as answers are
longer and more elaborate, and may not be easily anticipated by teacher
(McComas & Abraham, 2005).
Level 6. Creation; in other words, using the same concepts, putting the
concepts together in a different way to form a new story or to plan and
produce a different product (such as a picture or a poem) (Krathwohl,
2002). “Write your own poem about three little pigs.”
Similar to the strategies for asking questions, there are also strategies for
answering questions:
Repeat the question. If a learner asks a question, the teacher should
paraphrase or repeat it before answering so that that the whole class can
hear it.
Commend and appreciate all questions. It takes courage from a learner to
ask a question, therefore when a question is asked, compliment it with:
“That’s an excellent question” or “I’m glad you asked that”. Make sure
that all questions are answered sincerely as learners usually know when a
teacher’s response is not genuine.
Be honest when answering questions. What happens when the teacher
does not know the answer? Let the learner know that you will find out
and respond later. Remember to praise and appreciate these questions
too!
Giving correct feedback to learners can make a significant difference to
their ability to learn and is one of the most significant activities a teacher
can engage in to improve academic achievement (Hattie, 2011). There
should be a strong link between the learner’s answer and the teacher’s
comment. Teachers should aim to always provide feedback that is
instructive (explain where and why the learner made a mistake) as this has a
positive impact on learning by reducing any misunderstanding (Hattie &
Timperley, 2007). When appropriate, feedback can involve the whole class,
while at other times it might be directed at specific individuals. In addition,
effective feedback is timely. Other strategies that will enhance feedback
include the following:
When marking learners’ work, teachers should take time to write
comments (both praising and corrective) and give their reasons where
appropriate. This way, children learn where they went wrong, which is
more valuable than just receiving a mark.
Teachers should provide timely feedback. Generally, teachers should give
feedback as soon as possible after the completion of the task. For
example, if learners receive feedback no more than a day after a test or
homework assignment has been handed in, learning is enhanced. The
longer learners have to wait for feedback, the weaker the connection to
their effort becomes, and the less likely they are to benefit (Hattie &
Timperley, 2007). However, in some instances, temporarily withholding
feedback allows learners to internalise and process the demands of the
task.
Teachers should help learners to get it right. If learners know that
teachers want them to succeed and are willing to explain how this can be
achieved, learning improves (Spiller, 2009). Learners should be given
opportunities to improve, to try again and to succeed.
Teachers should ask learners to monitor and give feedback to peers, as
well as compare their work to the memorandum (self-correction) as this
can deepen understanding and learning (Spiller, 2009).
4.5.4 Teaching strategy 4: teaching self-reflection
Self-reflection is a metacognitive activity – in other words, an activity that
helps a person think about thinking, such as thinking about what you know
and do not know (Lew & Schmidt, 2011). Teachers not only have to be
reflective themselves (as part of the scholarly role), but they also have to
teach learners to become self-reflective (Colley, Bilics & Lerch, 2012). In
order for teachers to increase their self-evaluation skills, they can reflect on
the following self-reflection questions:
LISTENING
Think about a time when your active listening skills really paid off. What
was the situation? What did you achieve?
What have you done to improve your listening skills?
GOAL SETTING AND ACHIEVEMENT
Recall an important goal that you were set in the past. What strategies did
you use to achieve it? Which were successful?
How do you meet deadlines?
Think about a difficult task you had to undertake. What extra effort did
you exert to achieve the goals and to accomplish the task?
Think about a time when you did not achieve a goal or meet a deadline.
What did you do? What was the outcome?
Honest self-reflection is an important part of being a good teacher. Selfreflection implies that teachers must regularly evaluate which strategies
were successful in the classroom and which were not, so that the latter can
be avoided. Table 4.3 can be used by teachers as a tool to gauge their own
performance regarding effective teaching practices. The answers provided
could be turned into immediate, positive and concrete goals. Teachers
should be encouraged to use this tool honestly, to work hard at their goals
and to watch how their teaching transforms for the better! The teaching
practices displayed in this table refer to good practice, irrespective of
whether or not there are learners in the group who require support.
Table 4.3 Effective teaching practices
Assessment criteria
4
Exceptional mastery
2
Partial mastery, with assistance
3
Adequate mastery
1
Not yet mastered
1
Plan lessons carefully.
Manage time effectively.
Get all learners to stay on task.
2
3
4
Manage learner behaviour effectively.
Know individual learners and have appropriate expectations for each.
Establish effective classroom rules and routines.
Interact with learners in a caring, positive way.
Provide clear instructions.
Provide learners with a structure of the lesson, outlining the most
important concepts.
Use clear and understandable language.
Review and teach again if necessary.
Show enthusiasm.
Provide instructive and timely feedback.
Use both lower-order and higher-order questions in teaching.
Monitor learners’ progress.
Teachers are encouraged to put effort into self-reflection if they do not want
to stagnate and present the same ineffective and outdated lessons year after
year, causing boredom for themselves and learners alike. Teachers who are
unable to reflect and grow professionally are nothing but glorified
babysitters, and so it is understandable that they no longer enjoy their
career. Teachers should be encouraged to be turn-around teachers who can
adapt to the ever-changing world of education, moving with the times and
new teaching strategies. Once teachers have managed to increase their own
self-reflection skills, they also find it easier to carry this skill over to their
learners. Learners should be taught to think about and organise information
gathered from reading, discussions or other activities, as these are
prerequisites for lifelong learning.
4.6 UNHELPFUL STRATEGIES: WHAT NOT TO DO
While it is always best to know which strategies are helpful to children, it
might also be a good idea to look at some that have been reported as
unhelpful (Tomson & Chinn, 2001) so that one can guard against them:
When teachers go through the work too fast
When teachers do not stick to the point (this makes it difficult for
learners to grasp the most important facts)
When teachers expect learners to do too much copying (from the
blackboard, etc.) or when teachers dictate the whole lesson
When teachers read test results out loud
When teachers use sarcasm or ridicule (this belittles learners and many of
them do not understand exactly what was meant)
4.7 CONCLUSION
In this chapter, the strategies for setting up an inclusive classroom with a
sense of “belonging” were described. According to Mara Sapon-Shevin
(2010), inclusion means that all belong – nobody has to fight for an
opportunity to be part of a classroom or a school community. It means that
all children are accepted and that children do not have to earn the right to be
included or struggle to maintain it. It is not the responsibility of the child to
prove that he is entitled to be educated with his peers.
Next, methods for establishing a classroom ethos that radiates respect,
encouraging participation, providing opportunities for decision making,
developing self-discipline skills and becoming a role model were described.
The chapter continued by demonstrating why and how teachers should get
to know each child, and concluded by looking at effective teaching
strategies that can be used with all learners.
Chapter 5 will explore the way teachers can differentiate the classroom in
order to include all learners.
REFERENCES
Beatty, I.D., Gerace, W.J., Leonard, W.J. & Dufresne, R.J. 2006. Designing effective questions for
classroom response system teaching. American Journal of Physics, 74(1): 31–39.
Bratcher, S. 2012. The learning-to-write process in elementary schools. New York, NY: Routledge.
Bucholz, J.L. & Sheffler, J.L. 2009. Creating a warm and inclusive classroom environment: planning
for all children to feel welcome. Electronic Journal for Inclusive Education, 2(4): 1–13.
Buzan, T. 2011. Buzan’s study skills: mind maps, memory techniques, speed. London, UK: BBC
Active.
Colley, B.M., Bilics, A.R. & Lerch, C.M. 2012. Reflection: a key component to thinking critically.
The Canadian Journal for the Scholarship of Teaching and Learning, 3(1): 2–21.
doi:http://dx.doi.org/10.5206/cjsotl-rcacea.2012.1.2
Detheridge, T., Whittle, H. & Detheridge, C. 2002. Widgit Rebus Symbol Collection. Cambridge:
Widgit Software Ltd.
Gardner, H. 1993. Multiple intelligences: the theory in practice. New York: Basic Books.
Gliebe, S.K. 2011. The development of self-control in young children. Lutheran Education Journal.
Available at: http://lej.cuchicago.edu/research-in-education/a-study-of-the-relationship-betweencognitive-emotion-regulation-optimism-and-perceived-stress-among.selected-teachers-in-lutheranschools
Gunderson, E.A., Gripshover, S.J., Romero, C., Dweck, C.S., Goldin-Meadow, S. & Levine, S.C.
2013. Parent praise to 1–3 year-olds predicts children’s motivational frameworks 5 years later. Child
Development, 84(5): 1526–1541. Available at: http://doi.org/10.1111/cdev.12064
Hannah, R. 2013. The effect of classroom environment on student learning. Unpublished honours
thesis. Western Michigan University, US. Available at:
http://scholarworks.wmich.edu/cgi/viewcontent.cgi?article=3380&context=honors_theses
Hattie, J. 2011. Visible learning for teachers: maximizing impact on learning. New York, NY:
Routledge.
Hattie, J. & Timperley, H. 2007. The power of feedback. Review of Educational Research, 77(1): 81–
112. doi:10.3102/003465430298487
Hewitt, M.B. 2007. Helping students feel they belong. CYC Online. Online journal of the
International Child and Youth Care Network (CYC-Net). Issue 101. Available at: http://www.cycnet.org/cyc-online/cycol-0706-hewitt.html
Higham, S., Tönsing, K.M. & Alant, E. 2010. Teachers’ interactions during storybook reading: a
rural African perspective. Early Education and Development, 21(3): 392–411.
Hoxby, C. & Murarka, S. 2008. New York City charter schools: how well are they teaching their
students? Education Next, 8(3): 54–61.
Jerome-Freiberg, H., Huzinec, C. & Templeton, S. 2009. Classroom management – a pathway to
student achievement: a study of fourteen inner-city elementary schools. The Elementary School
Journal, 110(1): 64–80.
Krathwohl, D.R. 2002. A revision of Bloom’s taxonomy: an overview. Theory and Practice, 41(4):
212–218.
Lew, M.D.N. & Schmidt, H.G. 2011. Self-reflection and academic performance: is there a
relationship? Advances in Health Sciences Education, 16(4): 529–545. Available at:
http://doi.org/10.1007/s10459-011-9298-z
Long, D. & Carlson, D. 2011. Mind the map: how thinking maps affect student achievement.
Networks, 13(2): 1–7.
Lumpkin, A. 2008. Teachers as role models: teaching character and moral virtues. Journal of
Physical Education, Recreation and Dance, 79(2): 45–49.
Lunenburg, F.C. & Lunenburg, M.R. 2014. Applying multiple intelligences in the classroom: a fresh
look at teaching writing. International Journal of Scholarly Academic Intellectual Diversity, 16(1):
1–14.
Martin, A. 2005. How to help your child fly through life: the 20 big issues. Sydney: Bantam.
Mastropieri, M.A. & Scruggs, T.E. 2010. The inclusive classroom: strategies for effective instruction,
4th ed. Upper Saddle River, NJ: Prentice Hall.
McComas, W.F. & Abraham, L. 2005. Asking more effective questions. Available at:
http://cet.usc.edu/resources/teaching_learning/material_docs/Asking_Better_Questions.pdf
Mindtools. n.d. Available at: http://www.mindtools.com/
Mol, A. 2007. The motivation of learners. SAALED News, 27(2): 6–9.
Mortimore, T. & Dupree, J. 2008. Dyslexia-friendly practice in the secondary classroom. Exeter:
Learning Matters.
Motitswe, J.M.C. 2012. Teaching and learning methods in inclusive classrooms in the Foundation
Phase. Unpublished master’s dissertation: UNISA: Pretoria.
Munns, G., Arthur, L., Downes, T., Gregson, R., Power, A., Sawyer, W. et al. 2006. Motivation and
engagement of boys: evidence-based teaching practices. Canberra: Commonwealth Department of
Education, Science and Training. Available at:
http://www.dest.gov.au/sectors/research_sector/publications_resources/profiles/documents/motivatio
n_engagement_boys_pdf.htm (accessed on 11 April 2007).
Nind, M. 2006. Conducting systematic review in education: a reflexive narrative. London Review of
Education, 4(2): 183–195.
Sapon-Shevin, M. 2010. Because we can change the world: a practical guide to building cooperative
inclusive classroom communities, 2nd ed. Thousand Oaks, CA: Corwin.
Shaddock, A., Giorcelli, L. & Smith, S. 2007. Students with disabilities in mainstream classrooms: a
resource for teachers. Canberra: Australian Government Department of Education, Employment and
Workplace Relations.
Smith, S. 2016. Colors in the classroom learning environment – color your world. Available at:
https://smithsystem.com/resource-library/article-library/color-world/
Spiller, D. 2009. Assessment: feedback to promote student learning. Teaching Development/W hanga
Whakapakari Ako. University of Waikato. Waikato, New Zealand. Available at:
http://www.waikato.ac.nz/tdu/pdf/booklets/6_AssessmentFeedback.pdf
Thalluri, J., O’Flaherty, J.A. & Shepherd, P.L. 2014. Classmate peer-coaching: a study buddy support
scheme. Journal of Peer Learning, 7(8): 92–104.
Tofade, T., Elsner, J. & Haines, S. T. 2013. Best practice strategies for effective use of questions as a
teaching tool. American Journal of Pharmaceutical Education, 77(7): 155. Available at:
http://doi.org/10.5688/ajpe777155
Tomlinson, C.A. 2014. The differentiated classroom: responding to the needs of all learners.
Alexandria, VA: ASCD.
Tomson, M. & Chinn, S. 2001. Good practices in secondary school. In Fawcett, A. (Ed.). Dyslexia:
theory and practice. London: Whurr.
Tucker, P.D. & Stronge, S.H. 2005. Linking teacher evaluation and student learning. Alexandria, VA:
Association for Supervision and Curriculum Development.
VanHousen, D. 2013. Effective classroom management in student-centered classrooms. Unpublished
Master’s dissertation. St John Fisher College, Rochester, NY. Available at:
http://libguides.sjfc.edu/citations
Williams, K.C. & Williams, C.C. 2011. Five key ingredients for improving student motivation.
Research in Higher Education Journal, 12(1): 1–23.
Zentall, S.R. & Morris, B.J. 2010. Good job, you’re so smart: the effects of inconsistency of praise
type on young children’s motivation. Journal of Experimental Child Psychology, 107: 155–163.
doi:10.1016/j.jecp.2010.04.015
5
Differentiated teaching
Be not afraid of going slowly. Be only afraid of standing still.
B
K
5.1 INTRODUCTION
Every child is unique and every child can learn, just not on the same day in
the same way. Based on this notion, differentiated teaching (also known as
differentiation) uses an approach to teaching and learning that provides
them with multiple options for receiving information and making sense of
ideas (Tomlinson, 2014). In a nutshell, differentiated teaching is thus the
process of identifying learner’s individual learning strengths, needs and
interests, and responding appropriately by adapting lessons to match them.
It has become a popular approach to helping diverse groups of children
learn together in the same classroom, and thus requires teachers to be
flexible in their approach to teaching, for example adapting the curriculum
and method of presenting information to learners rather than expecting
them to change in order to fit the curriculum, as discussed in Chapter 4. The
curriculum therefore sets the content of what has to be taught, but it is up to
teachers to decide how they will do it.
In other words, differentiated teaching allows teachers to plan and carry out
varied approaches to content (what children learn), process (how children
learn and how teachers teach) and product (how children demonstrate what
they have learnt) in anticipation of or in response to learner differences in
readiness (prior knowledge, understanding or skills), learner interest
(curiosity and passion) and learning style (how the learner learns best)
(Shaddock, Giorcelli & Smith, 2007). The reason why differentiated
teaching is used is to maximise each learner’s growth and individual
success by meeting all learners where they are and to assist in the learning
process (Tomlinson, 2014).
5.2 ELEMENTS OF DIFFERENTIATED TEACHING
Tomlinson (2014) identifies three key elements of the curriculum that can
be differentiated: content (what is taught); process (how it is taught); and
products (assessment). Each one of these will be described and examples
given.
5.2.1 Content
Teachers should evaluate the way learners in the class access the curriculum
content and how they can incorporate a range of different strategies to help
with this (Logan, 2011). They should also consider how they can align
learning outcomes with specific activities. For example, Mrs Viljoen is a
maths teacher who is teaching a Grade 5 class about halving and doubling,
and she is also working with metric volumes (millilitres and litres as well as
grams and kilograms). In order to get the children to participate, she decides
to teach these concepts in a fun activity, namely making peanut butter balls
(after having made sure that none of the children in the class is allergic to
peanuts). She provides the whole class with the same recipe:
Peanut butter balls (24 balls)
½ cup (120 g) honey
½ cup (120 g) peanut butter
1 cup (250 g) milk powder
1 cup (250 g) instant oats
2 teaspoons (10 ml) vanilla essence
Mix all ingredients and then form the mixture into 2.5 cm balls (the size of a R5 coin).
Lay the balls on a tray lined with waxed paper. Refrigerate or leave in cool place until
set.
Figure 5.1 Elements of differentiated teaching
She then designs three differentiated teaching worksheets for her class.
Table 5.1 shows how Mrs Viljoen divides her class into four groups. Groups
1 and 3 are essentially the same in terms of their learning potential and
cognitive skills, and it is for this reason that they need no modifications to
their worksheets or to the assessment standards. However, what
differentiates these two groups is that the learners in Group 3 have
significant sensory or motor impairments. This implies that although the
content on the worksheets is the same for these two groups, the learners in
Group 3 may require Braille, or they may need their worksheet on a
computer as they use an onscreen keyboard due to their physical
impairments. The children in Group 3 thus require an alternative form of
assessment not in terms of content, but in terms of the methods used in the
assessment, although they also meet the general achievement standards as
set out in the curriculum.
Table 5.1 Differentiated teaching worksheets: Grade 5 – making peanut butter balls
Groups
1
2
3
4
Worksheets
Worksheet 1
Worksheet 2
Worksheet 1
Worksheet 3
Groups
1
2
3
4
Worksheets
Worksheet 1
Worksheet 2
Worksheet 1
Worksheet 3
Examples of
children in
different
groups
Typically
developing
according to
age for the
Grade (11 yr =
Grade 5)
Mild
intellectual
impairment or
learning
disability
Typically
developing but
with sensory or
physical disability
Significant
intellectual
disability
Curriculum
content
Grade level
content
Grade level
content
Grade level
content
Grade level
content
Modification
No modification
Unwinding of
assessment
criteria, e.g.
reduce
number of
items
No modification
to curriculum, but
alternative
assessment, e.g.
amanuensis
Straddling of
grade (working
on same theme
but at a lower
grade level)
Assessment
format
Regular
assessment
Regular
assessment
Alternative
assessment
Alternative
assessment
Achievement
standard
General
achievement
standard
Alternative
achievement
standard
General
achievement
standard
Alternative
achievement
standard
Objectives
and
materials
used
Double and
halve the recipe
Ingredients in
ml and ℓ, g and
kg
Double and
halve the
recipe
Ingredients in
ml and g only
Double and halve
the recipe
Ingredients in ml
and ℓ, g and kg
Double and
halve the recipe
Ingredients in
non-standard
units (cup;
teaspoon)
Use drawings or
concrete objects
to also double
and halve the
recipe
The learners in Group 2 might have mild cognitive impairments or learning
problems. These children often present as “slow learners” in the class, and
although the teacher thinks that they will be able to master the curriculum,
they will do so at a slower pace. The modification that they would thus
require is an unwinding of the curriculum. For example, the children in
groups 1 and 3 will double the 250 g of oats (2 × 250 g = 500 g) and then
double it again (2 × 500 g = 1 000 g = 1 kg), while the children in Group 2
will only double it once (2 × 250 g = 500 ml) so that they do not have to
work with the decimal. Although a regular assessment format can then be
used to assess these children, alternative achievement standards have to be
set.
It should be mentioned that gifted learners would also fall into Group 2, but
for them the curriculum will not be unwound, but enriched (enhanced) in
order to provide more advanced knowledge, and to teach them more
concepts at a faster pace. Differentiated teaching has been associated with
higher achievement for gifted and talented learners (Munro, 2012), but a
more in-depth discussion thereof is beyond the focus of this book.
Group 4’s learners will have significant intellectual impairments and
therefore the teacher will need to straddle the grades for them. This means
that they will work on the same thematic knowledge and skills, but at a
lower grade or phase level (Engelbrecht, 2013). Not only will they require
alternative achievement standards, but the format of the assessment will
also be alternative. The teacher will therefore not expect these learners to
double and halve the ingredients as she would with the other learners, but
they will have to halve and double the non-standard units, for example the
tins or packets. This means that while the learners in the other groups are
doubling 250 g, the learners in Group 4 will be required to double one cup
of oats (2 × 1 cup = 2 cups) or two teaspoons of vanilla essence (2 × 2
teaspoons = 4 teaspoons). By participating in the activity in this way, these
learners will have a sense of belonging and feel that they are part of the
group.
From this example it is clear that Mrs Viljoen does not have more work to
do, although she initially had to plan her lesson in more detail. The
outcomes that all the children had to achieve were therefore not exactly the
same, although they all participated in the same activity (also refer to Table
3.1 in Chapter 3). Please note that the children are not seated according to
their worksheets. For example, all the children with Worksheet 1 are not
grouped together – they should be in mixed groups (flexible grouping), but
they receive a worksheet that is appropriate for their specific ability. The
only reason why the teacher has to know in which group she will place each
learner is to assist her with planning, not to label the children.
When planning a differentiated teaching lesson, the content of instruction
should include the same broad concepts, principles and skills for all learners
(e.g. halving and doubling), but the level of complexity should be
appropriate for individual learners in the class (hence the three different
worksheets). A teacher should align the activity (making peanut butter
balls) with the learning outcomes, and then decide how best to simplify (in
other words, how to make it easier for those learners who will not be able to
achieve the same outcomes, e.g. halving and doubling).
There is a range of other differentiation strategies that might be useful to
teachers when adapting the content of their teaching.
Figure 5.2 Using different entry points to accommodate learning styles
5.2.1.1 Finding entry points
This strategy (see Figure 5.2) allows learners to explore a given topic
through as many as five different entry points or avenues (Shaddock et al.,
2007), and it is clear that these can be matched to individual learning styles,
for example:
A narrative entry point (telling a story about the topic or concept)
A logical-quantitative entry point (using numbers or other scientific
approaches to the topic or concept)
A foundational entry point (examining the philosophy and vocabulary
that is relevant for the topic or concept)
An aesthetic entry point (focusing on the sensory features of the topic or
concept)
An experiential entry point (using a hands-on approach where learners
can work directly with materials that represent the topic or concept)
Stop and reflect
Mrs Mbeki starts off the new classroom theme Safety and the role of paramedics by
asking Zodwa, who is the chatterbox in the class, to tell a story about the work that
paramedics do, asking Kyle to calculate how many patients a paramedic can treat in
one day if he spends 45 minutes with each one, asking Gretha to draw up a list of
words that are relevant when attempting to understand the work of paramedics (e.g.
intubation, splints, ventilator, defibrillator, decontamination), and asking Thabo to
explain what a paramedic will see and hear at an accident scene. Finally, the whole
class is given facemasks and gloves similar to those used by paramedics, and
instructed to take each other’s pulse.
5.2.1.2 Complex instruction
Classrooms of the 21st century depict a new paradigm in which teachers are
no longer seen as the central and only communicator in the classroom who
is responsible for transmitting knowledge. This echoes the viewpoint of
Galileo Galilei (1564–1642), one of the fathers of modern-day science: “We
cannot teach people anything. We can only help them to discover it within
themselves.” Complex instruction is a teaching strategy that uses
collaborative groups, multiple intelligences and positive group experiences
while disregarding gender, ethnicity, ability and socioeconomic status. In
complex instruction, teachers use cooperative group work in diverse
classrooms to teach high-level academic skills (Logan, 2011). They assign
open-ended, interdependent group tasks, and organise the classroom to
maximise learner interaction. Effective complex instruction tasks do not
have only one correct answer and do not involve the memorisation of
routine learning. Complex instruction is an effective strategy for
encouraging participation as it requires that all learners work together in
small groups, acting as academic and linguistic resources for one another,
thereby drawing on the strengths of each individual in the group (Shaddock
et al., 2007). When implementing this strategy, teachers pay particular
attention to the equal participation of all learners, and use specific strategies
to facilitate this.
When designing complex instruction activities, teachers have to ensure that
the task will require multiple abilities from all the learners in the group –
hence the task should tap much more than only intellectual ability. Can you
still remember the example of Mrs Mbeki’s Safety and the role of
paramedics lesson in the “stop and reflect box” in the previous section
where she determined outcomes for each of the different types of
intelligence? Learners experience intellectual autonomy as they solve
problems and create physical, artistic, musical and dramatic products that
reflect their understanding.
So how does complex instruction work? As an example, divide learners into
groups of four, and give each a specific role, for example either as the team
captain, facilitator, resource manager or reporter. The groups are given an
open-ended complex problem that they have to solve together and are told
that they must each be responsible for each other’s learning. If one member
of the group has difficulties with the task, it is the role of the others to help
him to understand. At the end of the lesson one member of each group will
be chosen to present their findings to the rest of class, but they do not know
in advance who that will be so they must all be capable of reporting back.
However, teachers know that the academic nature of group discussions and
the products the group have to develop can sometimes be disappointing.
Research has shown that this might be due to a lack of understanding on the
learners’ part as to exactly what is expected of them and what elements
make up a good product (Abram, Scarloss, Holthuis, Cohen, Lotan &
Schultz, 2001). This can be addressed by giving the groups some evaluation
criteria (e.g. use of headings, clear introduction, three application examples,
at least five facts, comprehensive conclusion, reference list), resulting in the
groups spending more time evaluating their products and discussing their
task and the content of their product. The important lesson from this
research is thus that all group discussions should have clear and accessible
criteria for evaluation as this improves the academic nature of group
discussions and the individual learning gains made by all learners.
5.2.1.3 Compacting the curriculum
“This is so boring!” must be one of the phrases most dreaded by all
teachers, as this immediately decreases participation. One way to respond to
this statement is to ask the learners to be more specific in describing why
they are bored. Ask them to differentiate between Boring 1 situations: “I
already know that; could you give me an opportunity to show you?” and
Boring 2 situations: “At the present time I do not know enough about the
topic to be interested in it.” One strategy through which boredom can be
combated is by compacting the curriculum, as already learned material
(prior knowledge) is avoided (Renzulli & Reis, 2014).
Curriculum compacting is a strategy that was originally designed to allow
gifted learners the opportunity to be engaged in meaningful learning by
eliminating content that they already know, followed by enriched learning
opportunities such as self-study (Munro, 2012). However, it has now also
been used successfully with learners with disabilities who are often kept
from learning about a topic in depth because of a lack of basic academic
skills (reading, writing, language, etc.) (Shaddock et al., 2007). In order to
use this strategy effectively, a teacher needs to be knowledgeable about the
curriculum and be able to decide what is really important and what can be
skipped or eliminated, hence it is a good idea for teachers to start with a
lesson that they really feel comfortable with. Confidence develops when
one starts a new activity from one’s comfort zone, increasing one’s
willingness to explore and implement new strategies (Fisher, 2008).
Two kinds of curriculum compacting are frequently used:
Basic skills compacting. This is mostly used in subjects and content areas
such as spelling, mathematics and language studies.
Content compacting. This is often used in subjects such as social studies,
science, literature, maths applications and problem solving.
How can teachers go about compacting the curriculum? Basically, it
involves the following steps:
Determine which of the learners are potential candidates for curriculum
compacting. Teachers would probably not need to get too far into the
school year before they have a sense of which learners complete their
work quickly and accurately, who seems to have a wealth of outside
information, and who consistently scores well with little apparent effort.
Likewise, teachers will also notice that some children really struggle to
finish on time and need additional support. Both of these groups would
benefit from curriculum compacting.
In order to assist teachers to make this decision, they should assess all
learners before beginning a new topic to determine what they already
know and what needs to be mastered (Fisher, 2008). Pre-testing is easily
used to document proficiency, and can be done from the textbook (or
whatever curricular materials are being used), or teachers can create their
own pre-tests. They do not have to be extensive. To use spelling as an
example, it can be as simple as pre-testing the learners on that week’s
words before they have been given the list. With other subjects, the pretest should cover the main objectives that teachers expect the learners to
master in the lesson.
Examine the pre-test results. Teachers will be able to see which learners
have already mastered large sections of the content. Getting back to the
spelling example: if a learner scores 100 per cent on the spelling pre-test
before even seeing the list, he should not have to spend the whole week
learning these words. He has just proved that he has mastered that
content, and will definitely benefit from a compacted curriculum.
Plan for the learning that needs to happen. Planning takes into account
what the learners already know (as determined by the pre-test). If we
continue with the spelling example, this learner could be given more
difficult words that he has not yet mastered, and still do the same
assignments (e.g. writing a story in which the words are used). For other
subjects, the compacting process can be more complex. For example,
Amelia’s pre-test results show that she has mastered six of the eight
learning objectives of her science lesson. That means that she has
mastered a lot of the content, but not all of it. For the sections she has not
yet mastered, she will be learning with the rest of the class. However, for
the sections she knows, she can be allowed to do some extention work or,
alternatively, can do some catch-up work in another subject.
Plan how the freed-up time can be spent. The teacher plans this
depending on the available resources, available space, available time, the
child’s interests, and the teacher’s own flexibility. Examples include,
among others, exploration of the topic in greater depth, independent work
on the topic, working with a mentor who can expand the learners’
horizons on the topic, moving ahead in the curriculum, and writing an
essay on the topic (Fisher, 2008).
None of us likes to relearn something that we have already mastered, so let
us not place obstacles in the way of learners who want to learn something
new!
5.2.1.4 Cubing
This is a versatile differentiation strategy that can be used to explore
different aspects of a topic and to add novelty to instructions given by the
teacher (teachers should therefore not use this strategy so often that the
novelty wears off). Learners often enjoy this strategy as it challenges their
problem-solving and thinking skills while providing opportunities for
sharing ideas about the topic or subject. It uses a six-sided cube with
different commands or tasks appropriate to the level of the group displayed
on each side.
The six parts include describing, comparing, associating, analysing,
applying and arguing – which is similar to Bloom’s taxonomy that was
described in Chapter 4 (see Table 5.2 and Figure 5.3).
Table 5.2 Example of a six-sided cube lesson plan
Level of Bloom’s
taxonomy
Explanation
Cubing example
Instruction words
teachers can use
1. Remembering
facts
Retrieving
relevant
knowledge;
recognising
and recalling
facts
Ask learners to physically
describe it. Urge them to
describe it according to
colour, shape, texture, size
and the parts it is made up
of.
Name; label; omit;
list; define; select;
choose; specify;
match; record;
identify; describe;
memorise; recall
2. Understanding
Determining
if learners
can interpret
the lesson,
explain why
things
happened
and compare
facts
Ask learners to compare it.
Encourage them to think
what it is similar to and
what it is different from.
Tell; report; show;
explain; identify; find;
discuss; classify;
describe; translate;
recognise; say in your
own words
3. Application in
an Iowa
farming
community
Using the
information
or procedure
in a given
situation to
predict
Ask learners to associate
it. Open up their minds and
encourage them to think of
what comes to mind when
they think of it. People?
Places? Things? Feelings?
Stimulate creativity and
include everything that
comes to mind.
Solve; select; teach;
show; collect; explain;
exhibit; predict;
inform; classify;
illustrate; determine;
produce; develop;
simulate; experiment;
demonstrate;
discover; dramatise
4. Analysis
Breaking up
the
information
into parts
and then
finding out
how the
parts relate
to each other
and to the
overall
purpose
Ask learners to analyse it.
Tell them how it is made
and what the traits and
attributes are. Encourage
them to think how it came
about.
Survey; dissect;
outline; contrast;
identify; compare;
discover; organise;
correlate; illustrate;
prioritise; combine;
separate;
differentiate;
distinguish;
investigate; subdivide
Level of Bloom’s
taxonomy
Explanation
Cubing example
5. Evaluation
Making
judgements
based on
criteria and
standards,
and
providing
critique
Ask learners to argue for or
against it. Divide the class
into groups and encourage
them to take a stance.
Allow them to use any kind
of reasoning whether it is
logical or silly, or even
anywhere in between.
Rate; judge; revise;
choose; defend;
justify; decide;
assess; contrast;
support; compare;
criticise; support;
recommend;
appraise; conclude;
interpret
6. Creation
Combining
facts;
changing to
a new
scenario
Ask the learners to apply it.
Encourage them to tell you
what you can do with it and
how it can be used.
Plan; adapt; invent;
create; develop;
design; initiate;
generate; make up;
compose; predict;
integrate; rearrange;
assemble;
collaborate;
categorise;
hypothesise;
formulate; incorporate
Source: Adapted from Duckart (2007); Ewing Cockroft (2007)
Figure 5.3 Six-sided cubes
HOW CAN A TEACHER PLAN A LESSON THAT USES CUBING?
Instruction words
teachers can use
Identify the key concepts in the topic or subject, what learners should
understand, and what they should be able to do. Use the curriculum as the
basis.
Make sure that the learners understand all the instructions on the cube,
for example what “analyse it” or “compare it” means.
Give all learners the opportunity to complete the activity according to the
directions on the cube. Every learner in the group gets an opportunity to
roll the cube. Allow the learners enough time to complete the task and
ask a representative from each group to give feedback to the whole class.
5.2.1.5 Group work and flexible grouping
All teachers are aware of the value of group work. Imagine teaching a
group of learners with different ages, backgrounds and abilities. Is a group
activity in which all learners will participate still possible? There are
various options:
Small groups. This type of group is frequently used in classrooms, and
can provide learners with opportunities for working with peers who have
similar needs, such as reinforcement or enrichment. Teachers usually
facilitate these groups and create opportunities for participation by
learners in the small groups.
Collaborative groups. The essence of collaborative learning (or
cooperative learning) is that it is learner driven and the team spirit that
develops motivates learners to contribute to each other’s learning.
Collaborative groups come in all sizes and configurations, depending on
the aims of the lesson. Because team success depends on individual
learning, members share ideas and rephrase instructions to help each
other. In this environment, learners convey the idea that learning is
valuable and fun to each other (Chinn & Chinn, 2009). These groups are
particularly effective for open-ended problem-solving investigations. In
order for collaborative groups to function optimally, all group members
should be engaged and interested in the task (or activity) at hand as this
reduces the risk for off-task behaviour or social loafing. Joint attention
(learners focusing on the same task, looking at the same information and
talking about a common topic), mutual respect and balanced participation
(no learner dominating or withdrawing from the group) have also been
reported as important ingredients of effective collaborative groups
(Chinn, 2006).
Performance-based groups. Although this type of group consists of
learners with similar needs who might need additional support to
complete an activity, it is different from traditional ability groups, as they
are not static. Performance-based groups are formed for short periods on
the basis of a particular need rather than in response to predetermined
performance levels (Dunlosky, Rawson, Marsh, Nathan, & Willingham,
2013). Hence these groups work well for teaching a learner a particular
skill.
Pairs. Learners are sometimes grouped in pairs. After the teacher has
presented the lesson, pairs are given the opportunity to share ideas and
information, and to plan how they would solve a particular problem.
Teachers could also encourage the learners to first write down their own
ideas, and then the pairs can meet to share ideas and strategies. This
strategy encourages divergent thinking and provides learners with
immediate feedback on their approaches to problem solving.
All of these groups can be used with various learners in various situations,
but the group strategy that is promoted in this book is flexible grouping.
For some teachers, particularly those teaching in farm schools, flexible
grouping will not be a new concept. It is a differentiating strategy in which
children of varying ages, backgrounds and abilities are grouped and
regrouped – allowing opportunities to work with others that are similar and
different from themselves (Engelbrecht, 2013; Shaddock et al., 2007).
Teachers are realising that grouping and regrouping children in a variety of
ways throughout the school day can make them more productive and the
teacher’s task a lot easier! In this way, Rachel might be in one group for
maths, in another for reading, and in yet another for arts and crafts. The
groups are thus not static, and the different groups she is assigned to may
vary according to the specific aims of the lesson, the activities, or individual
abilities and interests (Engelbrecht, 2013; Ford, 2005;). Nagel (2001) also
cautions that in addition to knowledge, power (having a voice and a choice
in the group and being included in decision making) and affection (having a
sense of acceptance and belonging) should also be kept in mind when
placing children in groups.
As with all of the differentiation strategies that have already been discussed,
flexible grouping requires a period of adjustment – but rest assured, the
results will be worth the effort!
5.2.2 Process
In this section, the second main element involved in differentiated teaching,
namely process (how information is taught and how the learners understand
main ideas and information), is described and examples given.
5.2.2.1 Scaffolding
We have all seen a house being built. In this process, the workmen put up a
temporary structure of poles and planks around the house to stand on while
they work. As the building becomes higher, so do these structures, which
are called scaffolds (see Figure 5.4). No roof can be erected without a
scaffold. In his sociocultural theory, Lev Vygotsky hypothesised that
children’s development works in much the same way (Samana, 2013). As
the child develops, adults provide these scaffolds, which enable children to
learn new skills. Scaffolding is thus really a technique that refers to an adult
controlling specific elements of the activity that the child is not yet capable
of performing and, in doing so, allowing the child to concentrate on and
complete those elements that are within his competency range (Samana,
2013). Scaffolding in the classroom can help teachers organise what to
teach and how to provide meaningful contexts linked to the child’s stage of
development. Initially the teacher would thus coach the learners in the
particular subject, through explanations and demonstrations, while
gradually reducing the amount of support as the child masters the specific
knowledge or skill (Alake & Ogunseemi, 2013). Scaffolding is therefore a
temporary support made available for children’s learning until they can
perform at the expected level without the support.
Figure 5.4 Scaffolds are structures that support
There are a number of activities that can be used to scaffold learning. Some
examples follow:
Alter the amount of work or the size of a project if necessary.
Start projects off small and then gradually build them up to expand them.
As an alternative to mind maps, teachers can also help learners to make
research grids (adapted from Mortimore & Dupree, 2008).
Table 5.3 Research grid for the social science theme “Our country”
Things I know
Find out
Information
Nine provinces
The location of all the provinces
The names of their capital cities
Country map
Internet
School library
Things I know
Find out
Information
Neighbouring
countries
The names of the neighbouring
countries
The names of their capital cities
One interesting fact about each
country
Atlas
Newspapers
TV news or radio news
bulletins
Provide more time to complete in-class work. Some learners who work
very slowly might be paired to sit next to a learner who works quickly,
who can encourage them to finish.
Learners who never finish work on time because they are too precise can
be seated next to a study buddy who works at a faster pace.
Implement flexible time schedules (make assignments due over the
course of a week – if a range of time is given during which the
assignment can be handed in, learners will be more likely to comply)
(Shaddock et al., 2007).
Make all learners aware of expectations and roles, for example by
developing schedules that are clearly displayed, and informing learners
about when activities will occur and their individual level of involvement
in these activities (Subban & Round, 2015). Using schedules will not
only assist with managing the group, but will also improve the
effectiveness of the lesson (Gibson, 2011).
Use a computer with spellcheck and word-prediction software that can
support writing, for example Word Q or EZ-Keys. For some learners with
motor difficulties, the reduced number of keystrokes might have a
significant impact on the amount of work they are able to produce. In
addition, when learners see that their written work is more accurate (as a
result of the spellcheck), this encourages them to try to produce more.
Use themes that really interest the learners. For example, instead of
having a lesson called “technology”, it could be called “gadgets and
gizmos” and each child can be asked to bring their favourite electronic
gadget to class and demonstrate it to everyone. By doing this, the interest
level in the class will be increased, impacting favourably on
participation.
Vary the materials used and increase the use of visual material. Teaching
new concepts by using short video clips, or filming learners reciting
poetry, or using audio books alongside a written text appear to have great
success in today’s classrooms (Subban & Round, 2015).
Reduce the amount of text that learners have to produce by using closed
text or sentence starters. For many learners, it is really scary to receive a
blank sheet of A4 paper with the instruction: “Write about your holiday”.
It would really help these learners if the teacher were to provide them
with a mind map (preferably in colour) with some directions, as shown in
Figure 5.5.
Figure 5.5 Example of a mind map for
brainstorming ideas
Provide a visual scheme to help learners understand the specific content
that is being taught in the lesson. In Chapter 4, the keywords mnemonic
SPSO (situation–problem–solution–outcome) scheme was described for
subjects that have that type of structure. Research has effectively shown
the value of using keyword mnemonics as a learning technique
(Dunlosky et al., 2013). In subjects where there are specific cycles, a
cyclical schema can be used, and for other subjects linear cycles can be
used. Two examples are provided from the natural sciences, namely the
life cycle of the silkworm and the elements of an atom. Notice how these
examples differ, depending on the specific content that is taught (see
Figure 5.6 and Table 5.4).
Figure 5.6 Cyclical scheme for the life cycle of the
silk worm
Table 5.4 Linear schema for describing an atom
Atom
Scientists always thought this was the smallest form of matter,
but then they discovered even smaller parts.
Nucleus
This is the solid centre of the atom where almost all the weight
lies. It is very small – if the atom were the size of a cathedral,
the nucleus would be the size of a fly!
Proton
and
neutron
The nucleus has two parts: protons (+ load) and neutrons (–
load). The nucleus can have more than 100 protons that are
kept together by strong nuclear power.
Three
quarks
Each proton and neutron consists of three smaller parts, called
quarks. The strong nuclear power is transmitted by the quarks
that appear out of nowhere and that fly about.
String
The latest theories say that all the little parts in the atom are like
little vibrations in a string – exactly like a violin string that can
produce different notes.
?????
Strings might be the end – but some scientists believe there is
even more that can be discovered.
5.2.2.2 Aided language stimulation
Aided language stimulation (AiLgS) is a useful classroom-based strategy
that impacts on how children learn by providing them with a strong
receptive (understanding) language foundation (Dada & Alant, 2009;
Goossens, Rosalie & Snyder, 2008). When using AiLgS, the teacher points
to graphic symbols (pictures) on a communication board while speaking,
thereby providing the learners with an additional cue (visual
supplementation). In other words, they not only hear the teacher’s voice, but
they also see the pictures of the words, which helps them understand and
remember. This strategy is particularly helpful in multilingual classrooms
(Bornman & Tönsing, 2016). Figure 5.7 shows an AiLgS song board, which
was used when safety in the house was discussed with a group of Sepedispeaking Grade 1 learners.
Figure 5.7 AiLgS song board
Source: Songboard made with Picture Communication Symbols™1
1 Picture Communication Symbols (PCS) is a registered trademark
of Mayer Johnson, a Tobii Dynavox Company of Pittsburgh, PA
(www.mayer-johnson.com).
What is the impact of AiLgS on the teaching process? In the past, a lot of
emphasis in classrooms was placed on children’s ability to produce
language (in other words, their expressive language abilities). Teachers
routinely make use of many questions (e.g. “Where is the fire?”),
commands and “show me” strategies (e.g. “Show me the house”). AiLgS
challenges this perception and states that the emphasis should be on output,
as it is based on the notion that teachers should put in (provide input) before
expecting anything out (expression/output) (Goossens et al., 2008).
Therefore, if a teacher is expected to teach in English, but she knows that
the children speak Sepedi at home, they should first be provided with the
English vocabulary and understand it before they can be expected to use it
expressively. The teacher should thus continue to talk and point to the
pictures, even if it might initially look as if the children do not understand.
AiLgS is typically implemented in the class in six steps. Let us take a closer
look at each of these in Table 5.5.
Table 5.5 Six steps for implementing AiLgS
Step 1
Arrange the classroom for optimal learning.
Step 2
Decide on the level of graphic representation of the majority of the class.
Step 3
Select a fun and suitable activity (content).
Step 4
Prepare the necessary materials.
Step 5
Practise using AiLgS on your own.
Step 6
Implement AiLgS and measure both your own and the learners’ progress.
In step 1, the classroom should be arranged in terms of seating for optimal
learning (Subban & Round, 2015). For example, a group work activity may
benefit from the rearrangement of desks to facilitate group discussion.
Rearranging the classroom also implies that all kinds of disruption and
distractions should be kept to the minimum. For example, it might be better
to close the classroom door so that children are not distracted by what they
see outside or, if possible, a carpet could be put into the classroom that
could absorb some of the noise. The teacher can also plan different table
arrangements. For example, when children are placed in their small groups,
a kidney-shaped table placement can be considered (this works well when
there are six learners or fewer), a V-shaped table placement (for 6–10
learners) or even a U-shaped placement (for 10–12 learners).
After having decided what type of table arrangement is most appropriate,
the teacher should decide where each learner should sit. Obviously there are
no hard and fast rules but the following guiding principles might be useful:
Learners who use augmentative and alternative communication (AAC)
should sit centrally as this makes it easier for everybody to see what they
are saying (if they are using a communication board) or even to hear the
voice output devices clearly (if they use a speech-generating device such
as the GoTalk).
Blind learners or those with severe visual impairment should sit close to
the teacher to facilitate optimal use of their residual vision, or so that the
teacher can touch them if need be.
Learners with challenging behaviour should not sit next to each other.
Children who give the most feedback should be evenly dispersed among
children who give minimal or no feedback.
In step 2, the teacher should consider the learners’ level of graphic
representation; in other words, their perceptual skills. Generally, the
sequence in which symbol development takes place is from
object symbols → pictorial symbols → traditional orthography (print)
This means that young children will probably first recognise a real object
(e.g. use a CD cover to indicate “music time”), followed by a recognition of
pictures (this can be either photographs, pictures from a book, hand-drawn
pictures or even formal graphic symbol systems). A whole range of
different symbols is available, each with its unique attributes, advantages
and disadvantages (Bornman & Tönsing, 2016). The last level of difficulty
is traditional orthography, where the learners have to rely on the written
words. As the focus of AiLgS is on facilitating receptive language, a
combination of print and pictorial symbols would be recommended for the
majority of learners. The emphasis is on learning the symbols as easily as
possible, so that an immediate effect is noticeable. Teachers should also
take the ease of symbol production into consideration (e.g. if the pictures
have thick black lines, they are easier to photocopy). In certain instances,
digital cameras have been used with great success when learners go on an
outing for making individual storybooks, remnant books that act as diaries,
and communication books. These photographs also aid memory, and seeing
themselves in the photographs heightens the pleasure of the activity for
many learners. Other possible sources are to use the internet to search for
pictures, which can then be printed.
In step 3, the teacher has to select a suitable and fun activity for
implementing AiLgS. Age appropriateness should be one of the guiding
factors (e.g. Grade 2 learners will enjoy a lesson about birds of prey, while
younger children might enjoy a lesson on farm animals). When using a
group activity, it is important to always include an element of surprise – if
the teacher asks questions in a particular sequence, some of the children
stop concentrating if they know that it is not yet their turn. In order to hold
everybody’s attention, a teacher can do the following:
Have a box with all the children’s names (or even their photographs with
their names) and then draw their name out of the box randomly.
The teacher can dress up and wear a funny hat or glasses – this helps to
ensure that she remains the focal point of interest, and it tempts almost all
the children to look at the “funny teacher”, which is much more effective
than continuously having to say: “Look at me!”
The teacher can use a spinner that selects a child randomly.
After the teacher has picked the first child, she can use the “Pick a friend
strategy”, which means that every child gets to pick the next child. By
doing this, the children cannot predict who will have the next turn, and
hence they all continue to pay attention.
Step 4 entails the preparation of the necessary materials. All the symbol
backgrounds should preferably be coloured for better visual clarity and for
quick reference. For example, all the nouns can be coloured yellow, verbs
pink, descriptors blue, and so on. These coloured symbols should then
preferably be placed on a black hardboard to reduce any visual distractions.
It lightens the workload if teachers work together in the preparation of these
materials (e.g. three teachers each make a different song board, and then
share them, thereby giving each one access to all three boards).
Step 5 requires teachers to practise the AiLgS strategies on their own.
Teachers need to develop the skill of pointing to symbols while speaking.
One of the most important AiLgS principles is that a ratio of 80 per cent
statements to 20 per cent questions should be used. The most important
things to do and not to do are given in Table 5.6.
Table 5.6 Dos and don’ts of implementing AiLgS
What to do
What not to do
Focus on receptive abilities
(understanding).
Do not focus on expressive abilities (speaking)
only.
What to do
What not to do
Make statements.
Do not ask too many questions.
Focus on all the children.
Do not be distracted by individual children.
Finally (step 6), teachers can implement AiLgS in their classrooms and
evaluate the progress made by themselves and by learners.
5.2.3 Products
The final component of planning differentiated teaching is by looking at the
product; in other words, how the learners can demonstrate what they have
learnt (Logan, 2011).
5.2.3.1 Learning contracts
Learning contracts can be used effectively to assist teachers when formally
planning the outcome of teaching (the product). A learning contract is
basically a short agreement in writing between a teacher and a learner that
outlines what the learner is expected to learn, what method will be used to
teach this (including who and what can help), what the time span is in
which it will be learnt, as well as how it will be assessed (Shaddock et al.,
2007). Do not be intimidated by the term learning contract – the focus is on
learning, not on contract! In other words, it is a personal learning plan.
Teachers can set these learning contracts for a specific school term, for a
theme or even for one or two days, depending on the level of the children in
the group. In order to become familiar with the strategy, it is suggested that
teachers start with shorter contracts until they feel comfortable using them.
Although it is a formal written agreement, it does not have to be complex.
By using learning contracts, learners are encouraged to take more
responsibility for their own learning, and to set realistic deadlines and
outcomes and evaluate their own progress. Both the teacher and the learner
should also have the opportunity to renegotiate the contract if it is not
working. In order to decide whether the goals of the learning contract have
been met or not, a variety of strategies can be used, ranging from simple
informal peer assessment (e.g. checklists) to formal assessments.
Figure 5.8 Example of a learning contract
Source: Adapted from Challis (2000)
5.2.3.2 Alternative forms of assessment
In the earlier sections of this chapter (when the content and process of
differentiated teaching was described) it was emphasised that the focus
should be placed on the individual learner’s strengths and that care should
be taken not to focus on the weaker areas. For a large group of learners,
reading and writing are particularly difficult, and yet, when assessing the
learner’s knowledge about a specific topic, this is very often the method
that is frequently used.
Stop and reflect
What other strategies can you think of? Think outside the box: talk to your colleagues
in the staff room and find out what methods they use to assess learners’ knowledge.
Make a list of possible ways and try them out.
EXAMPLES OF ALTERNATIVE ASSESSMENTS
Allow learners to draw answers rather than write them.
Let them design cartoons to show that they understand the particular
topic.
Ask them to make posters to convey their understanding of a particular
concept.
Let them write and act out their own little drama (or song) in which they
explain the content of the lesson.
Let them develop a PowerPoint presentation.
Allow learners to use shortened tests so that they do not have to write out
long paragraphs that are difficult and full of spelling mistakes (one often
loses the essence of what the learner wants to say if the work is full of
spelling and grammar mistakes).
Provide support for learners by proofreading (e.g. allow them to hand in
a draft piece of work first before their final attempt).
Provide opportunities for spoken responses (oral exam) rather than
written responses.
5.2.3.3 Homework
Homework has been the source of many disagreements – between teachers
and learners (if the homework has not been done), between parents and
their children (if children do not want to sit down and do their homework),
between different learners (if they did not understand the homework
requirements in the same way), between teachers and parents (if the parents
did not help with a difficult assignment), and last but definitely not least,
between parents and teachers (if parents feel that teachers give too much or
inappropriate homework). Researchers in Canada have found common
themes when investigating parents’ comments regarding homework:
Homework is too difficult or the assignment is unclear.
Homework cuts into family time and causes stress at home.
Children are left with little time to play as a result of too much
homework (Cameron & Bartel, 2008).
Would South African parents agree with this? Regardless of these research
findings, teachers are usually under pressure to set and mark homework.
Homework can have many different purposes – it can be used to reinforce
the lesson that was taught that day, or to extend learning (e.g. when a
project is given in which the learners have to do additional reading on the
topic), or to prepare learners for new material so that the topic is not totally
foreign to them when the teacher introduces it in class. So apart from
academic benefits such as better study habits and skills, homework also has
some non-academic benefits, such as better self-discipline and greater selfdirection, and it may even increase parental involvement in learning (Carr,
2013). In this chapter differentiating the curriculum was described, and this
obviously implies that homework should also be differentiated.
The following guidelines might be helpful when setting homework:
Ensure that the homework is relevant, and reassure parents at parents’
evenings that unnecessary homework will be avoided at all costs. In
doing so, parents are bound to cooperate with teachers regarding homework (Mortimore & Dupree, 2008).
Ensure that all learners write down what is expected of them and when
the homework is due. In some cases, teachers might decide to photocopy
the week’s homework for learners, enabling them to know what they
have to achieve that week.
Ensure that teachers’ expectations are realistic and that the homework is
doable in the amount of time allocated. Bear in mind that learners in the
intermediate and secondary phase receive homework from all their
teachers! Research shows that homework should be limited or it could
even have a negative effect. Secondary school learners should spend
between 1½ and 2½ hours daily on homework, while primary school
learners should spend one hour or less per day (Cooper, Robinson &
Patall, 2006).
Ensure that each learner has the knowledge and skill to be able to do the
homework. A one-size-fits-all approach cannot be followed, as the
teacher has to differentiate the homework in exactly the same way in
which the lesson was differentiated (Carr, 2013). If children need
assessment, accommodations (e.g. providing extra time) should also be
provided for homework.
Figure 5.9 Example of a homework sheet
Despite the homework debate in the research literature, one must never
forget the benefits of doing homework, such as learning about being
responsible; learning about time management and the importance of
finishing a project; and, finally, learning about how to develop good study
habits. Figure 5.9 shows an example of an effective homework sheet that
clearly outlines what is expected.
5.3 CONCLUSION
In this chapter the planning of a differentiated teaching lesson by adapting
the content, process and product was discussed. However, one should
always remember that the reason why all of this is necessary is to encourage
all children, and in particular those who are not reaching their full potential
and who are falling behind in their schoolwork, to succeed. Teachers create
the environment in their classrooms and have the power to make a child’s
life miserable or happy, but most importantly, teachers are part of a team
who believe that all learners are capable of learning and achieving (Logan,
2011). Teachers who are risk taking, flexible, empathetic, organised and
tenacious, and who will take whatever steps they need to make ideas clear
to their learners, are those teachers who have turned Mission Impossible
around to become Mission I’m Possible!
REFERENCES
Abram, P., Scarloss, B., Holthuis, N., Cohen, E., Lotan, R. & Schultz, S.E. 2001. The use of
evaluation criteria to improve academic discussion in cooperative groups. Asia Pacific Journal of
Education, 22: 16–27.
Alake, E.M. & Ogunseemi, O.E. 2013. Effects of scaffolding strategy on learners’ academic
achievement in integrated science at the junior secondary school level. European Scientific Journal,
9(19): 49–155.
Bornman, J. & Tönsing, K.M. 2016. Augmentative and alternative communication. In Landsberg, E.,
Krüger, D. & Swart, E. (Eds). Addressing barriers to learning: a South African perspective, 3rd ed.
Pretoria: Van Schaik.
Cameron, L. & Bartel, L. 2008. Homework realities: a Canadian study of parental opinions and
attitudes. Ontario Institute for Studies in Education, University of Toronto.
Carr, N.S. 2013. Increasing the effectiveness of homework for all learners in the inclusive classroom.
School Community Journal, 23(1): 169–182.
Challis, M. 2000. AMEE Medical Education Guide No.19: Personal learning plans. Medical Teacher,
22(3): 225–236.
Chinn, C.A. 2006. Learning to argue. In O’Donnell, A.M., Hmelo-Silver, C. & Erkens, G. (Eds).
Collaborative learning, reasoning, and technology. Mahwah, NJ: Erlbaum.
Chinn, C.A. & Chinn, L. 2009. Collaborative learning. Education.com. Available at:
http://www.education.com/reference/article/collaborative-learning/
Cooper, H., Robinson, J.C. & Patall, E.A. 2006. Does homework improve academic achievement? A
synthesis of research, 1987–2003. Review of Educational Research, 76(1): 1–62.
Dada, S. & Alant, E. 2009. The effect of aided language stimulation on the receptive language
abilities of children with little or no functional speech. American Journal of Speech Language
Pathology, 18(1): 50–64.
Duckart, T. 2007. Prewriting: cubing. The Cache. http://www.humboldt.edu/~tdd2/cubing.htm.
(accessed on 12 November 2008).
Dunlosky, J., Rawson, K.A., Marsh, E.J., Nathan, M.J. & Willingham, D.T. 2013. Improving
students’ learning with effective learning techniques: promising directions from cognitive and
educational psychology. Psychological Science in the Public Interest, 14(1): 4–58.
Engelbrecht, A. 2013. Managing classroom environment in large multi-level classes. In Engelbrecht,
A. & Swanepoel, H. (Eds). Embracing diversity through multi-level teaching for foundation,
intermediate and senior phase. Pretoria: Van Schaik.
Ewing Cockroft, B. 2007. Differentiated strategy 101: cubing a lesson. Paper presented at the Ohio
Catholic Education Association Convention, Cincinnati, Ohio.
Fisher, T. 2008. Curriculum compacting: one way to help advanced students move ahead and learn at
their own level. Teacher Professional Development Sourcebook. Available at:
http://www.teachermagazine.org/int_page.html?
url=http://www.teachermagazine.org/tsb/toc/2008/09/10/index.html (accessed on 7 November 2008).
Ford, M.F. 2005. Differentiation through flexible grouping: successfully reaching all readers.
Naperville, IL: Learning Point Associates.
Gibson, V. 2011. Differentiating instruction: teaching differently to improve reading instruction.
Saint Paul, MN: Read Naturally.
Goossens, C., Rosalie, N. & Snyder, P. 2008. What’s in your AAC briefcase? Paper presented at the
13th Biennial Conference for the International Society for Augmentative and Alternative
Communication, Montreal, Canada.
Logan, B.E. 2011. Examining differentiated instruction: teachers respond. Research in Higher
Education Journal, 13: 58–69.
Mayer-Johnson, R. 1992. The picture communication symbols. Solana Beach, CA: Mayer-Johnson
Co.
Mortimore, T. & Dupree, J. 2008. Dyslexia-friendly practice in the secondary classroom. Exeter, UK:
Learning Matters.
Munro, J. 2012. Effective strategies for differentiating instruction. Paper presented at the Research
Conference: School improvement – What does research tell us about effective strategies? Melbourne.
Nagel, G.K. 2001. Effective grouping for literacy instruction. Boston: Allyn & Bacon.
Renzulli, J.S. & Reis, S.M. 2014. The schoolwide enrichment model: a how-to guide for talent
development, 3rd ed. Waco, TX: Prufrock Press Inc.
Samana, W. 2013. Teacher’s and students’ scaffolding in an EFL classroom. Academic Journal of
Interdisciplinary Studies, 2(8): 338–343.
Shaddock, A., Giorcelli, L. & Smith, S. 2007. Students with disabilities in mainstream classrooms: a
resource for teachers. Canberra: Australian Government, Department of Education, Employment and
Workplace Relations.
Subban, P.K. & Round, P.N. 2015. Differentiated instruction at work. Reinforcing the art of
classroom observation through the creation of a checklist for beginning and pre-service teachers.
Australian Journal of Teacher Education, 40(5): 117–131. doi.org/10.14221/ajte.2015v40n5.7
Tomlinson, C.A. 2014. The differentiated classroom: responding to the needs of all learners, 2nd ed.
Alexandria, VA: ASCD.
PART
II
Inclusive education: functional
abilities
The 21st century heralds significant changes in the field of education. For
individuals with disabilities in particular, a dramatic shift from separatist
special schooling to inclusive schooling is happening.
In line with the biopsychosocial model of disability, a clear distinction
should be made between the terminology of impairment and disability. The
term “impairment” refers to the actual structural or physical limitations of
the various body parts, such as the ear or the eye, which would result in
problems of hearing or seeing respectively. The term “disability” refers to
functional aspects, for example how the impairment affects the person and
how he copes with the difficulties brought on by the impairment in his daily
life. In other words, impairment refers to biological dysfunctions, whereas
disability refers to the process of exclusion (Sandvin, 2004). The
implication is that two people may have the same degree of impairment but
the one who copes better from day to day, for example makes friends,
enjoys school and develops independence, is less disabled than another who
does not go to school and is totally dependent on others for his daily needs.
The focus of this section moves from an understanding of specific
conditions to developing insights into the different contexts in which an
individual functions. The impact of disability is not about the individual in
isolation but, more importantly, about the individual in home, classroom,
school and community contexts.
Using the term “disability” is in line with the WHO’s international
classification, International Classification of Functioning, Disability and
Health for Children and Youth (ICFCY) (WHO, 2007), which views
disability as the product of person–environment interaction, and provides a
multidimensional framework of four components, namely body functions
and structures –for example conditions with an identifiable basis (i.e.
physical, sensory, intellectual, neurological and/or medical) –
activities/participation, and environmental factors (Simeonsson, 2009). In
the disability advocacy field, the term “disability” is the preferred
terminology as it raises awareness among the general public with regard to
the specific needs of these individuals. The understanding of the impact is
core to applications for grants, for example care dependency or disability
grants.
Part II of this book (comprising chapters 6 to 13) looks at the most typical
conditions that teachers would be exposed to in the classroom context. A
standalone chapter (chapter 6) on early childhood development has been
added in line with the international swell of evidence supporting the facts
that learning starts at the very beginning of life (Shonkoff, 2014). It is
hoped that by school teachers becoming better informed about the
challenges faced in this sector they will become passionate advocates for
early learning. The other seven chapters in this section of the book consider
specific disabilities. Definitions, characteristics and the possible causes and
management are discussed. This is important information for teachers as
they expect questions from parents in this regard: “Why did it happen?”;
“What did I do wrong?”; “What can I do to help?” The focus of these
chapters remains firmly on the strategies and approaches that can be used to
provide the appropriate accommodation and support, which can turn the
concept of inclusion from a mere dream into an exciting reality.
Why is such a substantial part of the book dedicated to specific disabilities?
The first-ever World Report on Disability was published by the World
Health Organization and the World Bank in 2011, and it revealed that more
than one billion people – or 15 per cent of the world’s population – are
disabled, of whom approximately 200 million encounter significant
difficulties in their daily lives. Furthermore, 80 per cent of people with
disability live in developing countries (United Nations, 2006) – a staggering
800 million people! This is higher than the 1970 disability estimates of 10
per cent (World Health Organization, 2005) indicating that disability
prevalence is high and growing. Trends in environmental factors, for
example road traffic accidents, violence, conflict and war, diet, natural
disasters, and substance abuse, may be contributing factors (Mathers &
Loncar, 2006). Substance abuse has also led to the largest preventable
intellectual disability – foetal alcohol spectrum disorder (FASD) (Paulson,
2013). Furthermore, advances in the medical field have led to improved
survival rates for children born prematurely or with other health conditions,
and some of these may result in disability (Blencowe et al., 2012). A sharp
increase in autism spectrum disorder (ASD) internationally has been noted,
and occurs in all racial, ethnic and socioeconomic groups (Beukelman &
Mirenda, 2013).
Disability can be seen as both a cause and a consequence of poverty
(Filmer, 2008). This is because disability increases the risk of poverty,
while poverty creates the conditions for increased risk of disability.
Many poor people live in areas where medical, educational and other
services are either scarce or totally absent, hence moderate to severe
disabilities are not always detected early, while milder developmental
problems are left untreated. This results in developmental problems
becoming specific disabilities, the impact of which is irreversible. Under
the old medical paradigm, clinicians and other rehabilitation specialists
were primarily responsible for intervention, but the role of mainstream
service providers, like teachers, has become more prominent in the
biopsychosocial model of disability.
Consequently, when moving towards the biopsychosocial model of
disability and a philosophy of inclusion, it must be acknowledged that
services to people with disability are too important to be left only to the
professionals. Communities must become aware of persons with disabilities
in their midst and of what can be done to assist them in becoming more
active, participating members of society (McConkey, 1996).
On the positive side, children with disabilities and their parents often have
contact with teachers as mainstream schools are relatively easily accessible
to all South Africans, even those living in rural and remote areas.
Furthermore, many children with disabilities have siblings who might
already be attending these schools, thereby providing a logical point of
contact. It is therefore clear that all teachers need to be equipped with the
necessary knowledge and skills to teach learners who experience a broad
range of disabilities so that they can participate meaningfully in classroom
activities.
REFERENCES
Beukelman, D.R. & Mirenda, P. 2013. Augmentative and alternative communication. Supporting
children & adults with complex communication needs, 4th ed. Baltimore, MD: Paul H. Brookes.
Blencowe, H., Cousens, S., Oestergaard, M., Chou, D., Moller, A., Narwal, R., Adler, A., Garcia,
C.V., Rohde, S., Say, L. & Lawn, J.E. 2012. National, regional, and worldwide estimates of preterm
birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis
and implications. The Lancet, 379: 2162–2172.
Filmer, D. 2008. Disability, poverty, and schooling in developing countries: results from 14
household surveys. World Bank Economic Review, 22(1): 141–163. First published online 15 January
2008. doi:10.1093/wber/ lhm021
Mathers, C.D. & Loncar, D. 2006 Projections of global mortality and burden of disease from 2002 to
2030. PLoS Med, 3(11): e442. doi:10.1371/journal.pmed.0030442
McConkey, R. 1996. Innovations in evaluating services for people with intellectual disabilities.
Chorley, England: Lisieux Hall Publishers.
Paulson, J. 2013. Environmental toxicants and neurocognitive development. In Batshaw, M.L.,
Roizen, N.J. & Lotrecchiano, G.R. (Eds). Children with disabilities, 7th ed. Baltimore, MD: Paul H.
Brookes.
Sandvin, J.T. 2004. Can standards of living surveys help us understand the living conditions of
disabled people? In Tøssebro, J. & Kittelsaa, A. (Eds). Exploring the living conditions of disabled
people. Lund, Sweden: Studentlitteratur.
Shonkoff, J.P. 2014. Changing the narrative for early childhood investment. JAMA Pediatrics,
168(2): 105–106.
Simeonsson, R.J. 2009 ICF-CY: a universal tool for documentation of disability. Journal of Policy
and Practice in Intellectual Disabilities, 6(2): 70–72.
United Nations. 2006. World programme of action concerning disabled persons. Available at:
http://www.un.org/esa/socdev/enable/diswpa04.htm (accessed on 16 February 2009).
World Health Organization. 2005. Disability including prevention, management and rehabilitation,
World Health Assembly Resolution 58.23. Geneva: World Health Organization.
World Health Organization. 2007. International classification of functioning, disability, and health –
children and youth. Geneva: World Health Organization.
World Health Organization (WHO) and the World Bank. 2011. World report on disability: summary.
WHO/NMH/VIP/11.01. Available at: http://www.refworld.org/docid/50854a322.html
6
Early childhood development
(ECD)
6.1 INTRODUCTION
It is easier to build strong children than to repair broken men.
F
D
In The Diary of a Zulu girl, blogger Zola Songo writes:
I am a product of an early 1990s Early Childhood Development (ECD) site.
The kind that is not sustained by government grant or diligently paying
parents. An ECD site that runs on the back of a woman that desires nothing
more than an educated community, though she herself did not get an
opportunity to make it past second grade.
They call my gran Gogomhlophe which means Whitegranny and I am told
that it is because she could always somehow manage to put porridge on the
table and without fail it would be accompanied by the luxury of milk (of
course the sugar would be stirred into the porridge while it was in the pot
and the milk would be diluted with water). I remember the porridge had an
unpleasant smell but there is no arguing that it filled our stomachs and
therefore made us happier and more productive children. I often wonder
how she managed her philanthropic pursuits since she was a widow with no
trust fund nor pension. She saved all of us that were under her care from
many lurking dangers like being hit by cars while aimlessly playing in the
street, being raped because our guardians could not account for 100% of
our time and drunk, depressed men were everywhere. Many of us did not
live with our parents as they had migrated to the big cities to find work. It
was no longer like the 60s, 70s and 80s when only the men left to work at
the mines. Women were also leaving now. The elderly stayed to raise us.
Twenty-five years down the track it baffles me why there is still a state of
such a crisis in ECD. Why women as frail as my grandmother are still
holding the fort and still making do with food they sometimes have to bring
from their own homes. I am aware that we are not going to fix all of the
countries inadequacies in 25 years but not stimulating children’s brains and
making that a priority is like steering the Titanic to its doom.
So now I work for an organization that’s purpose is to identify and help with
the registration of ECDs. For every unregistered site we find and bring to the
attention of Department of Social Development, we are all a step closer to
feeding children porridge with real milk as well as a midday meal and
assisting that site with hiring teachers that are properly trained to stimulate
the cognitive development of every child, even those with special needs. I
will personally know that my taxes reach “a little me” and give others a
better start in life.
Zola’s vivid account of her early experiences highlight the critical
challenges faced not only in South Africa but around the world as
communities and governments focus on how best to enable children to
thrive. Figure 6.1 illustrates the factors highlighted in her account.
Figure 6.1 Zola’s story: the challenges
Stop and reflect
Which parts of Zola’s story would you match with each area in this diagram? What
are the challenges?
Life is a journey. Although the prime responsibility of teachers on that
journey is to accompany children of school-going age, the challenge is to be
acutely aware of what comes before going to school and what happens after
leaving school. The focus of this chapter is on the young child with
particular reference to inclusion of children with disabilities. Children who
are at risk of developmental delay, or have an established risk such as
having a disability, and their families deserve a proactive response that will
result in lifelong inclusion.
Early childhood inclusion embodies the values, policies and
practices that support the right of every infant and young child
and his or her family, regardless of ability, to participate in a
broad range of activities and contexts as full members of families,
communities and society. The desired results of inclusive
experiences for children with and without disabilities include a
sense of belonging and membership, positive social relationships
and friendships, and development and learning to reach their full
potential. The defining features of inclusion that can be used to
identify high quality early childhood programs and services are
access, participation and supports (DEC/NAEYC, 2009).
6.1.1 What is early childhood development?
Early childhood development (ECD) refers to a comprehensive approach to
policies and programmes for children from 0–9 years of age within their
families and communities. Only in South Africa does it span this age group
– elsewhere in world it refers to the 0–6 year olds.
ECD programmes protect the rights of all young children and are essential
for their growth and development. The term ECD is often used to describe
pre-school programmes but in actual fact that is only one aspect of early
childhood development. The wider context looks at the child and his family
as a whole. Remember the zoom lens metaphor which looked the child at
home, at school and in the wider community? ECD is an umbrella term
embracing the right to family care, health, nutrition, shelter, safety, security
and education, as shown in Figure 6.2.
Figure 6.2 ECD: 0–9 years
Adapted from Berry, Biersteker, Dawes, Lake & Smith (2013)
For the purposes of this chapter, the term ECD will be used to discuss the
development of infants, toddlers and young children (0–4 years) in the
home, pre-school and crèche environments. Internationally, the term early
childhood education (ECE) is commonly used. At five years of age,
children enter Grade R classes in mainstream, pre-school or special schools.
ECD embraces the emotional, cognitive, sensory, spiritual, moral, physical,
social and language development of the young child. The four concepts that
underpin ECD are illustrated in Figure 6.3.
6.1.2 Core concepts of early childhood development
The focus is on the first years of life because skills beget skills (Heckman,
2012) or, put another way, everything a child learns is built up or scaffolded
on previous learning.
There is worldwide consensus on the economic sense of quality ECD
programmes:
Investing in young children is not only the right thing to do from
an ethical point of view, but it is also the smart thing to do from
an economic point of view for the children, as well as their
families, their communities and society at large (Denboba et al.,
2014).
Heckman and Kautz (2012) also make a strong case for the cost
effectiveness of early childhood education for disadvantaged and at-risk
children. They explain that if the investment is done earlier, there is less
need for later costly educational interventions and better quality of life
outcomes across the lifespan. Long-term outcomes are positive and the
evidence is seen in more years of school attendance, higher wages, healthier
lives and also lower rates of criminal behaviour (Heckman, Pinto &
Savelyev, 2013; Jones, Greenberg & Crowley, 2015; Shonkoff, Garner,
Siegel, Dobbins, Earls, McGuinn & Wood, 2012). Critically important
outcomes of ECD include the early development of cognitive and character
skills such as social skills, self-regulation, attentiveness, curiosity,
perseverance, conscientiousness, planning and independence. These are
some of the character skills, also sometimes called “soft skills”, that turn
knowledge into know-how and individuals into productive citizens
(Heckman, 2006). Self-regulation is the cornerstone of early development,
and encompasses using the right skills at the right time in response to urgent
situations as well as maintaining focus and attention, and regulating
thoughts, behaviours and emotions (Gillespie & Groves, 2006). It is one of
the most important skills needed to manage challenging behaviour, and will
be described in more detail in Chapter 7.
Assessments often focus on cognitive skills which in the young child are
not the only predictors of long-term outcomes. Ensuring children with
disabilities have as many opportunities to develop their character skills as
their typically developing peers needs to be intentional. Examples are as
follows:
Giving a toddler with a severe physical disability time to do things his
way may be challenging, but it creates an opportunity to foster
independence and perseverance
Giving a young child who cannot speak a speech-generating device to
participate in a morning ring or tell a joke is highly motivating and
interactive
Taking a toddler with low vision for a tractor ride and afterwards
encouraging him to walk round it, touch it and use his other senses to
explore it will satisfy his curiosity.
Stop and reflect
There are so many ways we use our senses to learn, as this true story illustrates.
At Forest Town School in Johannesburg, Lisa, an endearing four-year-old with severe
cerebral palsy, is enjoying a physiotherapy session. She is balancing on a huge red
ball with her fingers in her mouth.
Physio: Lisa why have you got your fingers in your mouth?
Lisa: Because I want to taste what they look like!
6.1.3 Managing the transitions
Quality early education programmes do not exist in a vacuum. An
awareness of the process of transition for a child moving from home to an
ECD programme and then on to primary school is critical. This is true for
all children, but especially important for children with disabilities, those
from poor homes and those with chronic childhood diseases who may need
specific accommodations and support. All levels of transitions (activity to
activity, home to ECD programme, ECD centre to school) need to be
intentionally managed. Teachers and parents should form strong
collaborative teams sharing the same short- and long-term vision and goals
(Westling & Fox, 2015). From a professional point of view, primary school
teachers have a huge stake in the implementation of quality ECD
programmes. They are the very ones who regularly face the challenge of
children in their class who may not yet be school ready.
Teachers need to build an understanding of the principles of ECD so as to
be able to share and motivate community leaders and policymakers to speed
up the provision of quality ECD services. Zola’s story at the beginning of
the chapter is a testimony to an individual committed to making a
difference. Teachers have a vital role as ECD advocates. In addition, many
of the principles of ECD remain relevant for much of a child’s schooling.
For children with disabilities this may be even more pertinent as families
and teachers build an understanding of the strengths of each child and
identify gaps that may hinder learning in order to address them in a timely
manner.
Definition
An advocate is someone who fights for something or someone, especially someone
who fights for the rights of others.
The core concepts illustrated in Figure 6.3 highlight the importance of
ECD.
Figure 6.3 Core concepts of ECD
Source: Adapted from Heckman (2014)
6.2 SOUTH AFRICA: SETTING THE SCENE
6.2.1 Statistics
There are an estimated 5,3 million children in South Africa under the age of
five (Statistics South Africa, 2012), and they are divided as follows:
Under the age of one year: 1,1 million
Between one and two years of age: 2,1 million
Between three and four years of age: 2,1 million
Statistics South Africa’s general household survey (2014) reports that 48
per cent of children from birth to four years of age attend day-care or
educational facilities outside their homes. No mention is made of the
quality of programmes, many of which are child-minding centres. In South
Africa, the terminology within the field is confusing – the widely used term
ECD practitioner does not reflect either the specific role nor the
qualifications of the person. For example, a part-time unqualified individual
with a Grade 8 and ECD pre-school teacher with a degree may both have
the same title of ECD practitioner.
Definition
The term ECD practitioner refers to all persons who work in the field of ECD
education and training, such as teachers, trainers, facilitators, lecturers, caregivers and
development officers. They include those qualified by their experience, and who are
involved in providing services in homes, centres and schools. In respect of teachers
and trainers, ECD practitioners include both formally and non-formally trained
individuals providing an educational service in ECD (Department of Basic Education,
Social Development and Health, 2012).
Similarly, the terminology used for describing ECD centres or sites does not
clearly reflect the quality or standard of services. For example, parents may
perceive that having their five-year-old in a crèche with partially trained
practitioners equates with a Grade R programme in a school or pre-school
setting with qualified teachers. Empowering parents to ask the right
questions about the qualifications of staff and the quality of the programmes
is challenging, especially when parents themselves may not have had a
good education.
Definition
The term ECD centre refers to any building or premises that is maintained or used for
the admission, protection and temporary or partial care of more than six children away
from their parents. ECD centres may or may not operate for gain. Depending on
registration, an ECD centre can admit babies, toddlers and/or pre-school-aged
children. The term ECD centre can refer to a crèche, a day-care centre for young
children, a playgroup, a pre-school, after-school care, etc. ECD centres are sometimes
referred to as ECD sites (Department of Basic Education, Social Development and
Health, 2012).
So what are the values and policies that should undergird quality inclusive
ECD programmes?
6.2.2 Constitution of South Africa (South Africa, 1996a)
The values enshrined in the South African Constitution should but do not
always permeate the lives of all the citizens of the country. These values
flow like a golden thread through this book and it is critical that parents and
teachers know the rights of all children and especially, as we help build an
inclusive society, those of children with disabilities and their families.
Inclusive educational programmes from a very young age are the most
effective means of combating discriminatory attitudes, and achieving
quality education for all (Schulze, 2010).
The South African Constitution, in Section 28 of the Bill of Rights (South
Africa, 1996a.) states that:
(1) Every child has the right (a) to a name and a nationality from
birth; (b) to family care or parental care, or to appropriate
alternative care when removed from the family environment; (c)
to basic nutrition, shelter, basic health care and social services; (d)
to be protected from maltreatment, neglect, abuse or degradation;
(e) to be protected from exploitative labour practices; (f) not to be
required or permitted to perform work or provide services that (i)
are inappropriate for a person of that child’s age; or (ii) place at
risk the child’s well-being, education, physical or mental health or
spiritual, moral or social development;… (2) A child’s best
interests are of paramount importance in every matter concerning
the child.
In Section 29 of the Bill of Rights it states that everyone has the right to a
basic education (South Africa, 1996a). These rights are also echoed in the
United Nation’s Convention on the Rights of the Child (UN, 1989).
6.2.3 South African legislation and policies
At this time in South Africa’s history it is our God-given
responsibility to run with the education policies and legislation
that are in place. If we don’t make it happen, who will?
A
D
T
(2009)
F
,
.
)
The seven Acts, White Papers and other pieces of legislation and policies
described below are foundations and scaffolds for the stimulation and
education of all South African children. It is important for advocates to
have the knowledge both to share with local communities and to keep the
government accountable.
6.2.3.1 The South African Schools Act (South Africa, 1996b)
This Act defines basic education as including one year of pre-school to
Grade 9 and as such does not include the age group of 0–4-year-old
children. The Department of Basic Education (DBE) is responsible for
primary and secondary school education.
6.2.3.2 White Paper 5 on Early Childhood Education (National Department of
Education, 2001a)
This White Paper focuses on Grade R implementation, but does address the
need for ECD services for younger children. In 2015, 95 per cent of
children enrolled in Grade 1 had attended Grade R the year before. It is,
however, disturbing that the impact of Grade R programmes is small,
especially in poor areas (Samuels et al., 2015).
6.2.3.3 White Paper 6 Inclusive Education (National Department of Education, 2001b)
White Paper 6 is rooted in the premise that all children can and will learn
with the right supports in place. The goal is the provision of education
programmes which build on the capabilities of all learners, thereby enabling
full participation. The concern is that there is only passing reference to ECD
in the document: “district support teams are to include early childhood and
adult basic education centres” (Ngwena & Pretorius, 2012).
6.2.3.4 Children’s Act 38 of 2005
This Act states that it is the government’s responsibility to provide quality
ECD services, giving due consideration to children with disabilities. The
Children’s Act focuses on centre-based services and does not address the
critical component of those who do not have access to such centres due to
disability, poverty, transport, etc.
6.2.3.5 National Development Plan (2030)
The National Development Plan is the government’s vision for South Africa
up to 2030 with provisioning of ECD as one of the priorities. It reflects the
serious intention of the government to provide services for young children.
Five critical areas have been identified: (i) nutrition; (ii) health services;
(iii) social services; (iv) caregiver support; and (v) opportunities for early
learning. Key challenges facing the field are that many teachers and crèche
practitioners are not qualified; that many ECD centres are not following
accredited curricula; that parental involvement is limited; that programmes
and support materials do not cater for children with disabilities; that
addressing the needs of malnourished children is difficult; and that safety
standards are questionable.
6.2.3.6 National Curriculum Framework (2012) for children from birth to four
This framework describes the strategies which support the ECD vision of
the National Development Plan. The vision is “working with and for all
children in the early years in a respectful way to provide them with quality
experiences and equality of opportunities to achieve their full potential”
(Department of Basic Education, Social Development and Health, 2012:
12).
Seven key areas are prioritised in this framework, namely (i) families; (ii)
the rights of children; (iii) play; (iv) ECD practitioners; (v) children with
disabilities; (vi) first language teaching and learning; and (vii) transitions.
Seamless transitions are to be carried out by parents and teachers preparing
the child for change, discussing it while it is happening and helping the
child to reflect and adapt.
6.2.3.7 National Integrated Early Childhood Development Policy (2015)
This policy has the goal of providing comprehensive ECD services to all
infants, young children and their caregivers until the year before they enter
formal school at the age of six, or for children with disabilities at the age of
seven – the age of compulsory schooling. Inclusion of children with
disabilities and children from poor families in ECD services and
programmes is a core component of this policy. It embraces prevention,
early screening and intervention, and opportunities for early learning with
appropriate support.
6.2.4 United Nations Sustainable Development Goals (2015)
On 25 September 2015, world leaders adopted the 2030 Agenda for
Sustainable Development to end poverty, fight inequality and injustice, and
tackle climate change by 2030. This agenda includes a set of 17 Sustainable
Development Goals (UN, 2015). Goal 4 of this document focuses on
education, and specifically on ensuring inclusive and quality education for
all, and promotes lifelong learning. One of the specific targets set is: “By
2030, ensure that all girls and boys have access to quality early childhood
development, care and pre-primary education so that they are ready for
primary education”. However, Dr Pia Britto, a senior advisor on ECD at
UNICEF, warns that if we reduce ECD to one area of development (such as
education), this will limit the power of ECD to transform individuals and
societies as it takes much more than education for a child’s brain to develop
(Britto, 2015). She explains that ECD has been documented to be one of the
most cost-effective strategies for poverty alleviation, and that it thus fits
into goal 1, which is focused on eradicating poverty. Goal 2, focused on
ending hunger and improving nutrition, is also addressed in ECD, as
children who receive early stimulation along with nutrition supplements
have better outcomes than those who receive only nutrition supplements,
thereby amplifying the impact of nutrition. Furthermore, ECD interventions
buffer the negative effect of stress, thereby improving absorption of
nutritional intake. Likewise, all 17 sustainable development goals bear
direct relevance to ECD.
6.2.5 Roles and responsibilities of government departments
The responsibility for ECD pre-school or crèche services lies across
government departments. This multisectoral collaboration obviously has
advantages but can also be a minefield to navigate. The complex nature of
the roles and responsibilities of different government departments is not
unique to South Africa, but this summary illustrates the overlap of areas of
responsibility which frequently lead to significant challenges in the setting
up and accessing of ECD services.
In South Africa there are five core government departments tasked with the
implementation of ECD programmes:
The Department of Social Development (DSD) is the lead department
in the implementation of fully resourced, coordinated and managed ECD
programmes for children from 0–4 years of age. It is responsible for the
registration, funding and the ongoing monitoring of both home- and
centre-based ECD services.
The Department of Basic Education (DBE) is responsible for the
curriculum of children from 0–4 years, and for the provision of services
for children in Grade R, which includes the Grade R curriculum. It also
has the task of developing resources and training ECD practitioners.
The Department of Health (DoH) has oversight of health-related
matters including antenatal care, immunisation, nutrition and the
management of childhood illness. The prevention of mother-to-child
transmission of HIV has a high priority.
The Department of Higher Education and Training has the
responsibility of ensuring appropriate qualifications for ECD
practitioners and Grade R teachers.
The Department of Cooperative Governance and Traditional Affairs
is concerned with the provision of childcare facilities and the
implementation of municipal bylaws pertaining to childcare facilities.
The South African Constitution and the policies as they relate to ECD
demand participation on a wide scale involving national and local
government, local communities and families. The policies are in place but
implementation is slow and at present quality ECD remains inaccessible to
the majority of South African children.
6.3 PARTICIPATION
The core value of participation was discussed at length in Chapter 2 and the
principles are just as relevant for young children, including both typically
developing and those with disabilities. Much of the difficulty in
implementing inclusive education is due to the fact that inclusivity is not
always a guiding principle that dictates the behaviour and action of families
and communities. Including young children with disabilities in regular
groups such as mother’s groups, faith-based children’s programmes, local
libraries, playgroups, playgrounds and, most importantly, ECD programmes
will set the foundation for inclusive schooling. Unless inclusion is a core
value in families and communities, the implementation at school level will
not succeed. Consider the participation and learning model with reference
to ECD programmes. What are the factors that facilitate participation in
ECD programmes and what are the barriers?
6.3.1 Factors which facilitate the participation in ECD
programmes
There is a wide range of factors which make it more likely that children will
attend and benefit from ECD programmes such as high-school-educated
parents; quality antenatal care; accessible health facilities; breastfeeding;
adequate parental leave; post-natal care sensitive to feelings of depression
and anxiety, especially of mothers; good nutrition and access to safe water;
appropriate family and community support structures; and high-quality
home and centre-based ECD services. This long list is not comprehensive
but it is obvious that all community leaders have an important part to play
as educators, encouragers and advocates for young children.
Stop and reflect
Three-year-old toddlers of parents who have completed high school have two to three
times the number of words in their vocabulary than peers whose parents did not
complete their education. Unless children from low-education families are engaged in
language-rich settings, these children may never catch up with their peers (Hart &
Risley, 1995).
6.3.2 Factors which are barriers to participation in ECD
programmes
There are significant barriers which need be identified and systematically
dismantled. These would include, among other things, limited
understanding and appreciation of the importance of ECD, inadequate
infrastructure, inaccessible services, cost of services, child/teacher ratios,
scarce training opportunities, and hence limited knowledge and skills of
pre-school teachers. Again, the list is long, but once more community
leaders have a significant role in identifying and addressing the challenges,
one step at a time.
What counts in life is not the mere fact that we have lived. It is
what difference we have made to the lives of others that will
determine the significance of the life we lead.
N
M
90
Become an advocate
Take a look at this YouTube clip and use it to share knowledge and generate
discussion.
Every child is a somebody.
https://youtu.be/ah7CCB6X9b0
A
resource
for
ECD
advocacy
from:
6.4 CORE CONCEPTS
6.4.1 The developing brain
Brain development is dependent on a combination of the child’s genes as
well as his experiences and the environment in which they occur. It is the
case that both nature and nurture influence brain development. It follows
that early experiences, both positive and negative, will impact the
developing brain for better or for worse (Shonkoff, 2011: 234). The process
is poetically described by Shonkoff et al. (2012: 9) as “nature dancing with
nurture over time”.
Because the brain is neatly encased in the skull, it may not be immediately
obvious that it is a living, growing part of the body ready and waiting to
respond and learn. This is true at birth, at one year and three years, through
school into adulthood. There is a dynamic relationship between the
structure of the brain, also described as brain architecture, and its ability to
make new connections, also described as brain plasticity. Strong brain
architecture is dependent on the experiences of the child, especially
relationships with responsive, dependable and caring adults (Shonkoff,
2014b). Early experiences, both positive and negative, can affect the brain’s
structure – with lifelong implications. There is no waiting period for
learning. The significance of this is equally important for children with
disabilities as for typically developing children. Children learn by
practising, with the initial attempts at a learning new skills faltering and
imperfect. For young children, early experiences are always functional and
usually fun, for example returning a mother’s smile, rolling over to get a
toy, learning to hop and to read, etc.
Definitions
Brain architecture describes the structure of the brain.
Brain plasticity refers to the brain’s ability to change/reorganise itself throughout life. It
may compensate for injury and disease or other adverse conditions such as abuse and
poverty.
Early learning is critically important as in the first few years of life 700 to
1 000 new neural connections form every second. Although the first 1 000
days of a child’s life are significant in terms of development, there is
growing evidence that new pathways can be laid down well into adult life
due to the plasticity of the brain (Center on the Developing Child, 2016a).
When a child grows up in a nurturing home and community, the
foundations of living and learning which enable that child to thrive are in
place. The brain grows from the bottom up as each new experience builds
on previous learning. Parents and teachers can scaffold children’s learning
by carefully assessing children’s abilities and providing just the right level
of challenge and support to help them to succeed.
6.4.2 Serve and return
One of the most important building blocks of brain architecture is the
responsiveness of an adult to the cues of the infant (Shonkoff, 2013).
Described as the “serve and return interaction”, it is one of the ways the
young brain builds brain cell connections. It can be compared to a game of
tennis where the ball is served by one player, in this case the young child,
and then returned by the other player, in this case the adult. It can be seen in
caring adults responding to the babbling, facial expressions, eye-gaze and
gestures of the infant. The adult response with eye contact, sounds, songs,
words and/or physical actions engages the child and facilitates the
development of trust, language, communication, physical and socioemotional skills, for example imitating the babbling of a child; playing
peek-a-boo; baby wiggles and Mom tickles, etc. It can also be described as
following the child’s lead, and continues well into childhood. Herein lies
the challenge for many parents and teachers of children with severe
disabilities in that it may be very difficult for the baby/young child to
initiate interaction due to their disabilities, for example low vision, hearing
impairment, cerebral palsy, etc. Caregivers need to be sensitised to
recognise the far subtler cues that children, especially those with severe
disabilities, may give, for example widening of the eyes to signal enjoyment
or increasing the rate of breathing to signal apprehension.
As the brain cell (neurone) connections rapidly multiply, it is imperative to
provide appropriate opportunities for children to learn. Waiting for
developmental milestones to happen before considering the next stage can
seriously limit the child’s ability to participate and here current best practice
is to follow the try-and-see approach versus the wait-and-see approach. If a
child is unable to communicate using his spoken voice, provision of other
ways for him to communicate such key word signing, graphic symbols and
technology will enhance participation. Likewise, if child cannot move
independently, a walker, wheelchair or scooter will provide functional
mobility so core to participation (Bastable, Dada & Uys, 2016).
6.4.3 Resilience
Significant adversity in early childhood such as poverty, abuse, fractured
family relationships, trauma, violence and stress negatively affect child
development, as is evident from the current research done in epigenetics
(Romens, McDonald, Svaren & Pollak, 2015), yet not all children
experience lasting harm. The term resilience is used to describe the ability
of some children to overcome serious hardship. Resilience stems from the
Latin word resilire, and means to rebound, recoil or spring back. It is a
general concept that can be defined broadly as the capacity of a dynamic
system (e.g. a young child) to withstand or recover from significant
challenges that threaten its stability, viability or development (Masten,
2013). When examining young children, resilience usually refers to
pathways or processes that lead to positive adaptation or to development in
the context of adverse experiences (Center on the Developing Child,
2015b). The unconditional love and support of adults, access to quality
early-learning settings and safe living environments are some of the factors
which influence resilience. New insights into brain development and
plasticity, how stress interacts with development, and how genes and
experience interact in shaping development hold great promise for
increasing resilience in young children and preventing adverse conditions
for the developing brain (Romens et al., 2015; Shonkoff, 2014b). Resilience
can be developed throughout life but as the brain and other structures are
more pliable in the early years, sooner is much better than later.
The concept of resilience can be represented by the seesaw in Figure 6.4.
On the right-hand side are adaptive skills and protective experiences which
outweigh the adversity on the left-hand side. It illustrates the tipping of the
scales in a positive direction despite the presence of significant hardship on
the other side. The understanding of this concept is important in terms of
strategies that can be used to counter the impact of adversity on a child’s
development (Center on the Developing Child, 2015b).
Figure 6.4 Resilience
Source: Adapted from Center on the Developing Child (2015b)
A loving, committed and stable relationship of at least one parent or
caregiver can make all the difference to the effects of stress on the
developing brain. The security, responsiveness and protection this
relationship provides can buffer the child from the negative effects of stress
(Morgan, 2013). An understanding of the three main responses to stress
sheds light on the concept of resilience:
Manageable stress is a part of healthy development, and indeed some
stress provides positive learning experiences, for example going to a new
crèche, having an immunisation injection or persisting with a frustrating
task/routine.
Tolerable stress is more severe than manageable stress, for example the
death of a beloved granny, seeing a neighbour’s house burning down,
having a big operation, etc. If this kind of stress is not continuous and the
child is protected by secure relationships with adults, the effects on the
brain and other organs will be temporary.
Toxic stress refers to levels of stress which have long-term implications
for brain and other organ development (Center on the Developing Child,
2015a). When negative stresses are overwhelming, especially in the
absence of secure adult relationships, this can tip the scales negatively
and impact brain development with lifelong repercussions. Figure 6.5
depicts parents physically and verbally abusing their child.
Stop and reflect
33 per cent of South African parents use some form of stick or object to discipline
their children (Dawes, De Sas Kropiwnicki, Kafaar & Richter, 2005). The most
common age of children being disciplined this way are four-year-olds.
11,3 per cent of learners experienced some form of corporal punishment at school
(Stats SA, 2015).
Figure 6.5 A child being physically and verbally abused by his parents
Supportive relationships with parents and other close adults form a
protective shield from the damaging effects of toxic stress. An
understanding of resilience must influence policy and also practice.
Interrelated factors that trigger toxic stress include neglect, physical and
verbal abuse, poverty, mental illness, family breakdown, substance abuse,
sexual abuse, discrimination and violence in the home and the community
(Center on the Developing Child, 2015a; Center on the Developing Child,
2015b). Children with disabilities are particularly vulnerable to sexual
abuse (Bornman, 2015), so it becomes imperative that policies address
these issues and underpin practice in both local and national settings. It is in
the local context that teachers and other leaders in the community have the
responsibility to work on changing attitudes, dismantling barriers and
building knowledge and skills.
6.5 OUT THERE MAKING A DIFFERENCE
6.5.1 Government and non-governmental organisations (NGOs)
The responsibility of national government to provide quality ECD services
cannot be disputed. However, non-governmental organisations (NGOs)
have a vital role to play and have done so in the field of ECD for a long
time. Support of and engagement with local and international NGOs can
reap rich rewards for children and their families. The United Nations
Children’s Fund (UNICEF) is closely involved with government and
NGOs, as well as academic and research institutions in South Africa and
indeed around the world.
South African NGOs with ECD focus
Training and Resources in Early Education (TREE) was established in1984 in
KwaZulu-Natal. It specialises in the provision of early childhood development
resources and training to ensure that young children develop their full potential.
http://www.tree-ecd.co.za/
Pebbles started its work on five wine farms in the Western Cape in 2004. The vision is
to support a community as a whole rather than a child in isolation, enabling them to
help a vulnerable child or a whole family in crisis. Their programmes embrace
education, health, community, nutrition and protection. http://www.pebblesproject.co.za
Cotlands, an ECD organisation based in Gauteng and operating in five provinces, was
established in 1936. It addresses education and social challenges by establishing early
learning playgroups and toy libraries in under-resourced communities to serve
vulnerable children aged from birth to six years. http://www.cotlands.org.za
Ntataise, which means to lead a young child by the hand, was birthed on a farm in the
Free State in 1980 with the aim of helping women who live in underprivileged areas to
establish their own ECD programmes. Ntataise now operates in seven provinces.
http://www.ntataise.co.za
Save the Children South Africa is part of the international organisation founded in
1919. Their ECD vision is giving young children under five a safe, stimulating and
quality early living and learning environment. http://www.savethechildren.org.za
6.5.2 Where to begin
Peter Rosenbaum (2012), a well-respected developmental paediatrician
with a special interest in childhood disability, and his colleague Dr Gorter
wrote an article with the catchy title The “F-words” in childhood disability:
I swear this is how we should think! The concepts apply to children of all
ages and need to be embedded in the very earliest programmes of both
typically developing children as well as those with disabilities. We will
unpack the F-words: family, function, fitness, fun, friends and future.
6.5.2.1 Family
Throughout this book, family is emphasised as the foundation of successful
living and learning. The term family is difficult to define because of the
emergence of different groupings of people, young and old, living in the
same household and reflecting the various cultures and contexts within
which they live (Schlebusch, 2015). Family members are usually, but not
always, related by blood ties or marriage, and usually, but not always,
supportive of one another. Family structures are diverse and although many
children live in nuclear families (parents with biological or adoptive
children) others live, for example, in extended families, single-parent
families and child-headed households or families. Many factors such as the
high divorce rate, the HIV/AIDS pandemic, unemployment, the changing
roles of men and women, the demands of the workplace and the movement
of people from rural to urban areas impact family dynamics. Ante- and
postnatal depression and anxiety affect one third of mothers in South Africa
(Hall et al., 2016). Teachers need to be aware of the implications of this
enormous diversity so as to gain a deep understanding of the issues and
realities that families face and be able to ensure they get the appropriate
support. It is a fact that for most parents the “how to” of parenting only
happens on the job, and parents of children with disabilities have extra
concerns and challenges in raising their children. Studies have shown that
this group of parents is more likely to face challenges in areas of both
physical and mental health than those of typically developing children
(Brehaut et al., 2011) and often lack confidence and competence. Being in
touch with parents’ hopes and fears, and acknowledging their priorities or
agendas is the best place to start.
6.5.2.2 Function
Function describes what people do, for example roles in the family or
community, responsibilities at school (including pre-school), position in a
sports team or job. In the International Classification of Functioning,
Disability and Health; Children and Youth (ICF-CY) (WHO, 2007) function
is placed in two categories:
Activity, which refers to the carrying out of an action or task by an
individual
Participation, which refers to involvement in life situations
For young children, their work is to play. We could call them players. It
may be free play or structured play. Wherever and whenever possible,
children must be part of the action. It important to let them do things their
own way, never depriving them of opportunities for participation.
Two other important ICF-CY components are described by Rosenbaum and
Gorter (2012):
Performance, which refers to what a child normally does
Capacity, which describes what a child can do at its best
The significance is that children must be encouraged to participate in the
way they best know how (performance) and as they practise doing this, they
will eventually get better at it (capacity). Performance will thus improve
with practice, and so children need to be given as many opportunities as
possible to be involved in activities across domains of home, pre-school and
in the community (Rosenbaum & Gorter, 2012). An example would be a
child learning to feed himself. Initial attempts are always very messy but if
the child is given countless opportunities in all environments, he will learn
the skill. Importantly, it is not only physical skills but social skills that come
to the fore. Looking back to the discussion on soft or character skills, it is
obvious that mealtimes are a setting in which many of these skills are
learned and practised, for example choice making (what to eat and how to
eat), curiosity (new tastes and textures), self-regulation (waiting, finishing,
planning), socially acceptable behaviour (saying “please” and “thank you”),
and so on.
6.5.2.3 Fitness
Recent research has shown that children with disabilities and those with
chronic illnesses are not as fit as their peers, and also not as fit as they
might be (Van Brussel et al., 2011). Opportunities to be physically active
may be limited not only by their specific challenges but also by the attitudes
and expectations of those around them. For all children, the drug of
technology draws them away from physical activity. The move to more
active lives for families has to be intentional. Choice of activity would
depend on the abilities and preferences of the child as well of the family, for
example going for a walk, gardening, dancing, swimming, playing touch,
kicking a ball, playing with the dog, batting a balloon, etc. Activities which
include other children should be high on the agenda.
6.5.2.4 Fun
Fun is about what children (and adults) really enjoy doing. Often the doing
is more important than the actual accomplishment. So how do we increase
levels of participation and engagement?
Find out what the child wants to do. It especially important for children
with disabilities to be given opportunities to express their preferences and
make choices from a very young age (Beukelman & Mirenda, 2013).
Early choice making gives the child control, the power to select what he
wants to do, where he wants to do it and who he wants to do it with, for
example “I want to play on the seesaw in the park with my cousin Dan”.
That might be a whole lot more fruitful than mom tipping out a box of
Lego on the floor, which just that day might not be what the child feels
like doing. It is one of the foundational building blocks of developing
independence.
Adapt the chosen activities to ensure success. Simple adaptations such as
sewing Velcro onto dress-up clothes, gluing old cotton reels onto big
puzzle pieces, following routines within games using visual schedules,
building up the grips on pencils and crayons, and so on, can make all the
difference.
Allow the child to do the activity his way. Always encourage the effort
and be ready to provide support when needed. Waiting for “please help
me” is always preferable to “let me show you how”.
Did you know that…?
When children play with water and sand, they learn about texture, shape, size,
volume, solitary or cooperative play.
Playing lowers anxiety and stress levels.
When children play ball games, they learn about following instructions, balance,
coordination, hand–eye coordination, teamwork, winning and losing.
When children play with blocks, they learn to create, match, sort, count, construct
and demolish.
When tidying up, children learn about sorting, matching, categorising, fitting and
ordering.
When children play imaginary games, they learn about emotions, creativity,
communication, language and social skills.
When children play with children of other nationalities or races, they learn about
similarities, not differences.
Giving children choices from a very early age develops independence.
When children are read to, they learn that pictures have meaning, words have
meaning and, most importantly, someone loves them enough to take the time.
When children complete a challenging puzzle or follow complex Lego instructions,
they learn about perseverance.
Stop and reflect
Which of the “Did you know?” questions refer to the development of cognitive skills
and which to character skills? Is there an overlap?
6.5.2.5 Friends
Friends are important to everyone. The need to love and be loved is
universal, and every child needs intimate as well as more casual friendships.
Quality of friendship is more important than quantity (Rosenbaum &
Gorter, 2012). Parents and teachers of very young children can facilitate the
process by creating opportunities and providing supports for joint activities,
for example playing games where there are opportunities for turn taking,
banter and small talk; playing hide and seek; role-playing games (“I’m the
mommy and you’re the baby”), and so much more (Center on the
Developing Child, 2015b).
6.5.2.6 Future
Rosenbaum and Gorter (2012: 6) write: “All children, including children
with disabilities, are in a constant state of ‘becoming’”, therefore, teachers
need to acknowledge parents’ expectations and dreams, and remain positive
without losing sight of reality. Of course, even very young children have
their own dreams and expectations “I want to be a policeman”, “I want to
be a mommy”. Sights must always be set on functional outcomes which will
enable children to participate happily and meaningfully in society. Parents
and teachers of young children with disabilities need to be constantly
reminded to build a secure environment where family, fun, fitness, friends
and function are the building blocks of the child’s future.
6.6 CONCLUSION
The purpose of this chapter was to challenge teachers to become advocates
for ECD. The indisputable benefits of ECD for all children, both those with
disabilities and typically developing children, were highlighted. Various
policies, frameworks and plans, some with a local and some with an
international focus, pertaining to ECD were discussed, as well as the part
played by different government departments. This was followed by
describing core concepts of brain development as well as the vital role
played by NGOs. Finally, the importance of family, function, fitness, fun,
friends and future was teased out. The golden thread running through the
chapter was the significance of nurturing relationships; active participation
in family, educational and community settings; the provision of appropriate
supports and the life-giving value of learning through play; and last but not
least, the significant economic benefits of ECD.
REFERENCES
Bastable, K., Dada, S. & Uys, C.J.E. 2016. The effect of a non-powered, self-initiated mobility
program on the engagement of young children with severe mobility limitations in the South African
context. Physical & Occupational Therapy in Pediatrics, 1–20.
Berry, L., Biersteker, L., Dawes, A., Lake, L. & Smith, C. (Eds). 2013. South African child gauge.
Cape Town: Children’s Institute, University of Cape Town.
Beukelman, D.R. & Mirenda, P. 2013. Augmentative and alternative communication. Supporting
children and adults with complex communication needs, 4th ed. Baltimore: Paul H. Brookes.
Bornman, J. 2015. Accessing justice via key role players: a view from South Africa. In Bryen, D.N.
& Bornman, J. (Eds). Stop violence against people with disabilities! An international resource.
Pretoria: Pretoria University Law Press.
Brehaut, J.C., Garner, R.E., Miller, A.R., Lach, L.M., Klassen, A.F., Rosenbaum, P.L. & Kohen, D.E.
2011. Changes over time in the health of caregivers of children with health problems: growth curve
findings from a 10-year Canadian population-based study. American Journal of Public Health (in
press).
Britto, P. 2015. Why early childhood development is the foundation for sustainable development.
UNICEF Connect. Available at: https://blogs.unicef.org/blog/why-early-childhood-development-isthe-foundation-for-sustainable-development/
Center on the Developing Child. 2015a. Key concept of toxic stress. Harvard University. Available at:
http://www.developingchild.harvard.edu
Center on the Developing Child. 2015b. The science of resilience (in brief). Harvard University
Available at: http://www.developingchild.harvard.edu
Center on the Developing Child. 2016a. Building core capabilities for life: the science behind the
skills adults need to succeed in parenting and in the workplace. Harvard University. Available at:
http://www.developingchild.harvard.edu
Center on the Developing Child. 2016b. From best practices to breakthrough impacts: a sciencebased approach to building a more promising future for young children and families. Harvard
University. Available at: http://www.developingchild.harvard.edu.retrieved (accessed on 22 June
2016).
Dawes, A., De Sas Kropiwnicki, Z., Kafaar, Z. & Richter, L. 2005. Corporal Punishment of South
African Children: A National Survey. Paper prepared for distribution at the regional consultation of
the United Nations study on violence against children. Save the Children, Sweden & Human
Sciences Research Council (HSRC), Cape Town.
DEC/NAEYC. 2009. Early childhood inclusion: a joint position statement of the Division for Early
Childhood (DEC) and the National Association for the Education of Young Children (NAEYC).
Chapel Hill: The University of North Carolina, FPG Child Development Institute.
Denboba, A.D., Sayre, R.K., Wodon, Q.T., Elder, L.K., Rawlings, L.B. & Lombardi, J.
2014. Stepping up early childhood development: investing in young. Singapore: Department of
Singapore Statistics.
Department of Basic Education, Social Development and Health. 2012. The South African National
Curriculum Framework for Children from Birth to Four. Available at:
http://www.education.gov.za/Portals/0/Documents/Publications/National%20Curriculum%20Framew
ork%20for%20children%20from%20birth%20to%20four.pdf?ver=2014-12-04-144326-000
DSD, DWCPD and UNICEF. 2012. Children with Disabilities in South Africa: A Situation Analysis:
2001–2011. Pretoria: Department of Social Development/Department of Women, Children and
People with Disabilities/UNICEF.
Gillespie, L.G. & Seibel, N.L. 2006. Self-regulation: a cornerstone of early childhood development.
YC: Young Children, 61(4): 34.
Hall, K., Sambu, W., Berry L., Giese, S., Almeleh, C. & Rosa, S. 2016. South African early
childhood review 2016. Cape Town: Children’s Institute.
Hart, B. & Risley, T. 1995. Meaningful differences in the everyday experiences of young American
children. Baltimore, MD: Brookes.
Heckman, J. 2014. Heckman Equation. Available at: http://heckmanequation.org/content/whitehouse-summit-early-education (accessed on 1 April 2016).
Heckman, J. 2012. Heckman Equation. Available at:
http://heckmanequation.org/content/resource/invest-early-childhood-development-reduce-deficitsstrengthen-economy (accessed on 10 March 2016).
Heckman, J.J. 2006. Skill formation and the economics of investing in disadvantaged children.
Science, 312(5782): 1900–1902.
Heckman, J. & Kautz, T.D. 2012. Hard evidence on soft skills. National Bureau of Economic
Research, Working Paper No. 18121, June 2012, Available at http://www.nber.org/papers/w18121
Heckman, J., Pinto, R. & Savelyev, P. 2013. Understanding the mechanisms through which an
influential early childhood program boosted adult outcomes. American Economic Review, 103(6):
2052–2086.
Jones, D.E., Greenberg, M. & Crowley, M. 2015. Early social-emotional functioning and public
health: the relationship between kindergarten social competence and future wellness. American
Journal of Public Health, 105(11): 2283–2290. http://doi.org/10.2105/AJPH.2015.302630
Masten, A.S. 2013. Risk and resilience in development. In Zelazo, P.D. Oxford handbook of
developmental psychology: self and other, Vol 2. New York: Oxford University Press, 579–607.
Morgan, B. 2013. Biological embedding of early childhood adversity: toxic stress and the vicious
cycle of poverty in South Africa. Research and policy brief. Medical Imaging Research Unit,
Department of Human Biology, University of Cape Town & Department of Psychiatry, Stellenbosch
University.
National Department of Basic Education. 2015. National Curriculum Framework (NCF). Pretoria:
Department of Basic Education.
National Department of Education. 2001a. Education White Paper 5: Early Childhood Education:
meeting the challenge of Development in South Africa. Pretoria: Department of Education.
National Department of Education. 2001b. Education White Paper 6: Special Needs Education:
building an inclusive education and training system. Pretoria: Department of Education.
National Scientific Council on the Developing Child. 2007. The science of early childhood
development: closing the gap between what we know and what we do. Available at:
http://www.developingchild.harvard.edu
Ngwena, C. & Pretorius, L. 2012. Substantive equality for disabled learners in state provision of
basic education: a commentary on Western Cape Forum for Intellectual Disability vs Government of
the Republic of South Africa. South African Journal on Human Rights, 28: 81.
Romens, S.E., McDonald, J., Svaren, J. & Pollak, S.D. 2015. Associations between early life stress
and gene methylation in children. Child Development, 86(1): 303–309.
Rosenbaum, P.L. & Gorter, J.W. 2012. The “F-words” in childhood disability: I swear this is how we
should think! Child: Care, Health and Development, 38(4): 457–463. doi:10.1111/j.13652214.2011.01338.x
Samuels, M.L., Taylor, S., Shepherd, D., Van der Berg, S., Jacob, C., Deliwe, C.N. & Mabogoane, T.
2015. Reflecting on an impact evaluation of the Grade R programme: method, results and policy
responses. African Evaluation Journal, 3(1): 10 pages. DOI: http://dx.doi.org/10.4102/aej.v3i1.139
Schlebusch, L. 2015. Families raising a child with autism spectrum disorder: determining the
relationship between family routines and family quality of life. Doctoral dissertation, University of
Pretoria.
Schulze, M. 2010. Understanding the UN Convention on the Rights of Persons with Disabilities: a
handbook on the human rights of persons with disabilities. New York, NY: Handicap International.
Shonkoff, J.P. 2011. Protecting brains, not simply stimulating minds. Science, 333(6045): 982–983.
Shonkoff, J.P. 2013. Strengthening adult capacities to improve child outcomes: a new strategy for
reducing intergenerational poverty. Spotlight on Poverty and Opportunity: The Source for News,
Ideas and Action, April 22. Available at: http://spotlightonpoverty.org
Shonkoff, J.P. 2014a. A healthy start before and after birth: applying the biology of adversity to build
the capabilities of caregivers. In McCartney, K. Yoshikawa, H. & Forcier, L.B. (Eds). Improving the
odds for America’s children. Cambridge, MA: Harvard Education Press, pp. 28–39.
Shonkoff, J.P. 2014b. Changing the narrative for early childhood investment. JAMA
Pediatrics, 168(2): 105–106.
Shonkoff, J.P., Garner, A.S., Siegel, B.S., Dobbins, M.I., Earls, M.F., McGuinn, L., & Wood, D.L.
2012. The lifelong effects of early childhood adversity and toxic stress. Paediatrics, 129(1): 232–
246.
South Africa. 1996a. The South African Constitution and Bill of Rights.
http://www.paralegaladvice.org.za/docs/rights.pdf
South Africa. 1996b. South African Schools Act 84 of 1996. Pretoria: Department of Education.
South Africa. 2005. Children’s Act 38 of 2006. Pretoria: Department of Social Development (DSD).
South Africa. 2012. National Development Plan 2030 (NDP). Pretoria: Government Printer.
South Africa. 2015. National Integrated Early Childhood Development Policy. Pretoria: Government
Printer.
Statistics South Africa. 2012. South Africa’s young children: their family and home environment.
Report No. 03-10-07 (2012). Pretoria: Statistics South Africa. Available at:
http://www.statssa.gov.za/publications/Report-03-10-07/Report-03-10-072012.pdf
Statistics South Africa. 2014. General household survey. Statistical release P0318. Pretoria: Statistics
South Africa. Available at: http://www.statssa.gov.za/publications/P0318/P03182014.pdf
Sukbunpant, S., Arthur-Kelly, M. & Dempsey, I. 2013. Thai preschool teachers’ views about
inclusive education for young children with disabilities. International Journal of Inclusive Education,
17(10): 1106–1118, doi:10.1080/13603116.2012.741146
United Nations (UN). 1989. Convention on the Rights of the Child. Treaty Series, 1577, 3. Available
at: http://www.ohchr.org/en/professionalinterest/pages/crc.aspx
United Nations (UN). 2015. Sustainable development goals. Available at:
http://www.undp.org/content/undp/en/home/sdgoverview/post-2015-development-agenda.html
Van Brussel, M., Van der Net, J., Hulzebos, E., Helders, P.J. & Takken, T. 2011. The Utrecht
approach to exercise in chronic childhood conditions: the decade in review. Pediatric Physical
Therapy, 23(1): 2–14.
Westling, D.L. & Fox, L. 2015. Teaching students with severe disabilities, 4th ed. New Jersey:
Merrill Prentice Hall.
World Bank, Washington, DC. Children for high returns. Copyright World Bank. Available at:
https://openknowledge.worldbank.org/handle/10986/21094/ Licence: CC BY 3.0 IGO.
World Health Organization (WHO). 2007. International Classification of Functioning, Disability,
and Health – Children and Youth Version. Geneva: World Health Organization.
7
Understanding children with
challenging behaviour
7.1 INTRODUCTION
“Why is this child so naughty? Is he trying to control me? Is he retaliating
because I reprimanded him? What should I do when he does that? Will a
child like this ever change?” These are just some of the questions teachers
ask when they have children in their classroom who display problem
behaviour.
Since the mid-1980s there has been a shift in the assessment and treatment
of challenging behaviour (problem behaviour), away from the form of the
behaviour (what the child does) to the function of the behaviour (why the
child does certain things – what he hopes to achieve by displaying this
behaviour) (Beukelman & Mirenda, 2013; Kuhn, 2012). In order to address
problem behaviour successfully, the function of the behaviour should be
identified and understood, and then be replaced by behaviour that is socially
more acceptable. We cannot simply punish this type of behaviour because
punishment disregards the function of the behaviour, it is ineffective (as all
teachers who have tried it will testify!) and the child learns little if anything.
Punishment, by definition, is an after-the-fact procedure as it follows the
problem behaviour (LaVigna & Willis, 2005). In this chapter, challenging
behaviour will be described from a functional perspective – in other words,
how one can go about understanding why children display certain
behaviours, and what they aim to achieve through them.
7.2 EMOTION IS PART OF BEHAVIOUR
Emotion is the natural way in which all humans react to their environment,
and emotional regulation refers to how an individual interprets and reacts to
a situation. This is obviously affected by previous experiences as well as the
individual’s skill in interpreting situations (sometimes also referred to as
emotional intelligence). Most adults will be able to testify that at some point
they have experienced a certain situation in which they did not know
whether to laugh or cry! If a group of young children is playing, and one
gets hurt, a variety of reactions will be seen: one child might run away,
another might try to comfort the hurt one, one might start to cry with the
hurting friend while yet another might decide to run and call an adult for
help. Not one of these can be described as the “best” reaction. Rather, these
should all be seen as different emotional reactions to an event that all of
them experienced as stressful and their interpretation of what the “best
reaction in the situation” is. This reaction is obviously influenced by their
previous experiences – if they have been in a similar situation before, they
might have been taught to call an adult for help.
Toddlers will initially look at their parents’ faces and reactions for cues
about how to react. Often when a toddler starts walking and falls, he first
looks for the mother’s reaction before deciding whether it hurts enough to
cry (when he sees fear and shock on her face) or if it is not too bad (when
she smiles and encourages him to try again). If children experience a feeling
of security and safety in the home context, it teaches them to regulate their
own behaviour in a positive way. It makes them feel in control of the
situation and therefore it also boosts their self-esteem.
In the classroom, teachers can also teach mindfulness strategies, which
implies that they should learn to read the children’s signals and respond
appropriately. For example, when the children are tired, alter the activity to
a less strenuous one; when their attention starts drifting, get them to stand
and stretch. The learner most affected could be given an opportunity to take
a note to the teacher next door so that he gets a break, or if certain children
sitting next to each other trigger undesirable behaviours such as pushing
and fighting they could be seated elsewhere in the classroom. If the teacher
is able to read the child’s signals correctly, she can also teach the child the
vocabulary that accompanies the particular emotion, for example: “I see you
are angry. When one is angry it feels as if your face goes red and your heart
starts beating very fast. I also feel like that sometimes, and then I clasp my
hands tightly. Sometimes I walk away and sit somewhere until I feel a bit
better.” Teachers can also use a balloon with an angry face drawn on it, and
encourage children to blow up the balloon, just as their cheeks blow up,
when they become angry (Bornman, 2007). Older children can be
encouraged to punch or kick a punch bag (see Figure 7.1). Research has
shown that these mindfulness strategies decrease severe aggressive
behaviour and increase social competence (Thompson, 2011). In the past,
aggressive challenging behaviour in people with intellectual disability was
treated with medication, but research is showing that this should no longer
be seen as an acceptable routine treatment for this population (Tyrer et al.,
2008).
Figure 7.1 Using a balloon or a punch bag to help manage anger
The most important part of providing children with emotional roots is to
help them identify particular emotions and to teach them to name them
(moving beyond happy, sad, angry, scared and shy), and finally also to help
them judge the intensity of the emotion. An emotional thermometer (a
thermometer cut out of paper representing emotions) is a good way to teach
children to gauge the intensity of the emotion. For example, there is a
difference between being annoyed, being angry and being furious. Give
them a paper thermometer and have them colour the measuring part up to
the appropriate height level. This will soon teach them that all emotions are
not necessarily experienced with the same intensity – every time one is
annoyed does not have to end in a temper outburst!
Discussing emotions can be done very effectively in a group context.
Children can be asked to describe how they feel when they are jealous,
disappointed, excited, and so on. They can also be asked how they judge
their friends’ emotions, for example: “How do you know your friend feels
hurt and left out? What does she do?” Furthermore, fictitious case studies
can be used with great effect – a teacher can describe a familiar scenario
and ask children to describe how different children in this scenario feel, for
example: “Maria has tuckshop money. There is a new girl in the class, and
Maria shares her tuckshop sweets with her, but gives nothing to her old
friends. How do you think Maria, or the new girl, or the old friends feel?”
All of this forms part of the frequently talked-about emotional intelligence.
7.3 DEFINING CHALLENGING BEHAVIOUR
So what does it mean when a child displays challenging behaviour? There
are many different definitions, but generally there is consensus that it refers
to culturally abnormal behaviour(s) of such intensity, frequency or duration
that it
interferes with, or is at risk of interfering with optimal learning
limits participation with peers or adults
places the physical safety of the person or others in serious jeopardy
restricts access to ordinary community facilities (Emerson & Hatton,
2014; Kuhn, 2012; LaVigna & Willis, 1995; Powell, Dunlap & Fox,
2006).
Central to this definition is the important role of culture, and teachers need
to discuss parental expectations, as parents might just think that they have a
naughty child while the teacher has a different perspective. Challenging
behaviour typically emerges between two and three years of age, and can
take on many different forms. It includes behaviour directed at other
persons (such as hitting, biting and scratching), self-stimulation or other
stereotypic behaviour (such as flapping hands in the air, moving fingers in
front of the eyes, pacing, drumming, flipping light switches on and off, and
rocking back and forth), self-injurious behaviour (such as head banging,
hand biting and face slapping), pica (eating inedible things, such as chalk
and soil), destroying objects, sexual behaviour (e.g. public masturbation),
toileting problems (e.g. soiling and wetting), tantrums (prolonged
screaming and crying), as well as other disruptive behaviours (e.g. falling
on the floor or playing with the lights in the classroom) (Durand, 1990;
Powell et al., 2006). From this description it is clear that the focus of this
chapter is not on children who are regarded as the naughty or difficult
learners who fail to listen to the teacher – it is on children who display
serious behaviour problems.
Although gender is not a major risk in itself, some children appear to be
more vulnerable to displaying challenging behaviour, and this includes
children who
have a severe degree of intellectual impairment (Kuhn, 2012; Orsati &
Causton-Theoharis, 2013; Shapiro & Batshaw, 2013)
have autism spectrum disorder (ASD) (Orsati & Causton-Theoharis,
2013; Hyman & Levy, 2013)
have certain specific syndromes, for example Cri du Chat syndrome, Rett
syndrome or Prader Willi syndrome
have a sensory impairment
have a severe physical impairment
have severe problems in speech, language and communication (Sigafoos,
O’Reilly & Lancioni, 2009)
have poor social skills
have sleeping disorders
have psychiatric disorders.
7.4 BASIC BEHAVIOURAL PRINCIPLES
As previously stated, the strength-based approach and the importance of
focusing on abilities rather than disabilities runs like a golden thread
throughout this book. Problems should not be viewed as something within
the child, but a broader perspective should be taken that looks at how the
environment impacts on the problem. Likewise, when looking at
challenging behaviour, one should focus on similarities between children
who display it and those who do not, and not on the differences. This might
sound like a tall order – is it possible?
Behaviours can be divided into respondent and operant behaviour.
Respondent behaviour is elicited by prior specific stimuli and usually
involves the central nervous system, for example eye-blink and heart rate.
In other words if the child experiences something that makes him feel
scared, his heart rate might increase and he might start sweating. Operant
behaviour, on the other hand, refers to learned behaviour, for example what
is expected of learners when the bell rings to indicate that a period is
finished. Learning takes place when the child realises that all behaviours
have consequences. Some behaviours are reinforced when the teacher reacts
positively (e.g. when the child starts packing up his books when he hears
the bell, the teacher might smile and praise him), while certain behaviours
decrease if they are punished (e.g. if the child has to work in the school
garden when he talks in class). Operant behaviour is, however, not only
restricted to learners. If a teacher should ask a colleague for help and she
reacts positively, the behaviour will be reinforced and it will be easier for
the teacher to ask for her help again. However, if she is unhelpful and rude,
the teacher will be unlikely to ask again. Most children are able to learn
from these situations, but when a child has an intellectual disability, this
process is hampered (Sigafoos, Arthur & O’Reilly, 2003). These children
have limited opportunities and experiences to learn about the impact of their
behaviour. For example, if a child has a behaviour outburst every time
during a swimming lesson, the teacher might stop taking him to swimming
lessons.
In summary, then, there is a general consensus that all behaviour serves a
function and that behaviour does not occur in isolation but in context. Over
the past 20 years, our understanding of what challenging behaviour is and
why it occurs has changed significantly. We now know that challenging
behaviours are learned and that they are attempts by children to
communicate (e.g. either to indicate that they want something or not and
that they are trying to avoid it) (Kuhn, 2012), therefore a careful and
detailed assessment is necessary.
7.5 ASSESSMENT
Kuhn (2012) asks an interesting question: is it necessary to understand why
challenging behaviour occurs or is it simply necessary to stop it from
occurring? He suggests that the answer to both question is: “Yes!” He
explains this by using the analogy of deciding whether or not to go to the
doctor for a tummy ache – simply taking some pain medication may end the
pain temporarily, but to understand the cause of the pain and to receive
specific treatment (e.g. surgery to remove the appendix) one needs a visit to
the doctor. Regardless of the outcome, the best approach is to treat the
symptom but also to diagnose the cause. Likewise, when working with a
learner with challenging behaviour one should aim to minimise or prevent it
(the symptoms), but also attempt to understand why it is happening so that a
specific intervention can be developed.
In order to successfully address challenging behaviour, a comprehensive
functional assessment is recommended, which includes collecting
information based on direct observation, interacting with the learner by
reviewing his records and conducting detailed interviews (LaVigna et al.,
2005). This includes the following aspects:
7.5.1 Describing the history and background of the behaviour
Information on the child’s behavioural history and background can be
collected by reviewing his records or files, or by interviewing the most
important people in his life. The aim of collecting this information is to try
to determine when the onset of the behaviour occurred (e.g. did it happen
when the child came into a certain teacher’s class, when a special friend
moved away, when a parent died?), as well as what changes occurred during
the course of the problem. In many cases one can see that the current
problem did not start off with the same type of behaviour. For example, in
the beginning the child might have screamed, but now, in addition to the
screaming, the child may also fall to the floor kicking and biting. Typically,
not only will the type of behaviour change if no form of intervention is
made, but the severity of the behaviour will also increase. Challenging
behaviour is the one instance where it is not advisable to simply ignore it,
because this will not make it go away – it will change and become more
intense.
In order to give a clear description of the history of the behaviour, it is
fundamental to gain information from a variety of sources. Ask the parents
how the child reacts at home, or what he does during a different activity
with a certain teacher, or how he reacts on the playground with his peers.
Often the frequency and severity of challenging behaviour will conform to a
predictable and describable pattern, and once that happens this will shed
light on the behaviour and point towards appropriate intervention.
In addition to this, teachers should try to determine in which contexts, with
which people and in which tasks the challenging behaviour is not seen, as
this might provide a good starting point. The best emergency management
of all challenging behaviour is to avoid the activity that led to it in the first
place.
7.5.2 Describing the behaviour
The term challenging behaviour is a descriptive and not a diagnostic term.
Teachers should never see the child as challenging, although the behaviour
may be (Orsati & Causton-Theoharis, 2013). This means that teachers
should aim to describe the behaviour (“Can you tell me exactly what the
child does?”) rather than label or judge the behaviour. A description such
as: “The child screams and falls on the ground when requested to do certain
classroom activities” is more valuable than simply stating: “The child is
aggressive/rude/annoying”, as the latter type of socially constructed,
judgemental label closes the door for a different type of interpretation with
regard to the function of the behaviour.
It is the very things that we know that keep us from learning what
we should know!
A
Second, the teacher should always aim to describe the child’s behaviour
rather than focus on the child personally. Remember that the behaviour
serves a particular function for the child, it does not become him. For
example, rather than saying: “He’s a head banger”, say: “He bangs his head
when he wants attention”. The child is much more than just the behaviour
he displays.
In order to provide a clear description of the behaviour, teachers should aim
to include a description of the type of behaviour (e.g. biting), the severity of
the behaviour (e.g. there is a difference between a slight bite on the hand
and a bite that leads to swelling and bruising of the skin), and when the
behaviour takes place (e.g. every time the bell rings and learners have to
move from one class to another). Finally, the behaviour should be described
in measurable and observable terms, thus “three times an hour” or “once a
day” is preferable over “always” or “never”.
Some teachers (and parents) have found the use of a scatter plot to identify
the times of the day associated with the challenging behaviour invaluable
(Durand, 2011; Kuhn, 2012). Basically a scatter plot is a graphic display of
observable behaviour over successive days to identify those times of the
day that are associated with high rates of challenging behaviour (Durand,
2011). Usually it is done on a grid datasheet (see Table 7.1) in half-hour
intervals across successive days, and the teacher then marks in each block
whether the behaviour occurs or not (by making a cross or leaving the block
empty). Over a number of days the general pattern of when the behaviour
occurs can be seen, and the teacher can start planning the A-B-C chart,
which is described later (Kuhn, 2012).
Table 7.1 Example of a completed scatter plot
Time
Activity
Mon
Tue
Wed
Thurs
Fri
Total
08:00
Arrival
1
08:30
Circle time
5
09:00
Free play
3
09:30
Break
0
10:00
Art
3
= challenging behaviour
7.5.3 Describing what happens before the challenging
behaviour: setting events and antecedents
When looking at behaviour from a functional perspective, and
acknowledging the fact that challenging behaviour is learnt in the same way
all other behaviours are learnt, and that it is shaped through conditioning,
the importance of understanding the child’s specific context can be
appreciated. In other words, determining the communication function or the
message of the behaviour is critically important (Sigafoos et al., 2009). A
construct that is of particular importance is the setting events. These are
complex conditions that occur concurrently with the challenging behaviour,
but that are distant in time. In other words, they do not directly result in
challenging behaviour, but they are conditions, events or sensations that
increase the probability that challenging behaviour will occur. For example,
on some days the learner might feel physically ill and respond to
demanding tasks by banging his head and screaming, while on other days
no problem behaviour might be observed, and the learner might respond
with cheerful compliance (Carr et al., 2002).
Setting events may be grouped into three broad categories:
Environmental events. This refers to the environmental setup (e.g. the
temperature and whether it is too hot or too cold, the lighting in the
environment, the seating arrangements and the noise levels) as well as
the people in the environment (the number of people present and the
space around the child).
Biological/medical/personal events. This refers to illnesses and
biological conditions, for example pain, fatigue, allergies, digestive
problems, oversleeping or lack of sleep, medication or lack of
medication, and hunger.
Social events. This refers to conditions that precede social events, for
example demands that are placed on the learner, learners who have
limited communication skills, newness in either the situation or task or
people in the environment, unexpected changes in routines,
confrontations, clashing interactional styles and the amount of attention
from teacher and peers.
Teachers have to work closely with parents and other caregivers in order to
determine what the setting events are. Teachers may send the type of
checklist shown in Table 7.2 home and ask parents to complete it.
Table 7.2 Setting events checklist
SETTING EVENTS CHECKLIST
In order to help me understand your child’s behaviour so that I can help him/her optimally,
please mark all of the following events that occurred prior to school today. You may also
write a short comment next to the items that are marked.
Environmental events
Appeared to be too hot or too cold
Appeared to be sensitive to noise
Appeared to be sensitive to light
Yes
No
Comments
Environmental events
Yes
No
Comments
Biological/medical/personal events
Yes
No
Comments
Yes
No
Comments
Sleep pattern changed (oversleeping/lack of
sleep)
Medications were changed/missed
Has menstrual period
Appeared/complained of being ill
Appeared excessively tired/lethargic
Eating pattern changed/missed a meal
Social events
Was informed of something unusually
disappointing
Was refused a requested object/activity
Fought, argued, bullied or had other negative
interactions
Was hurried or rushed more than usual
Experienced major changes at home
Learnt about visit/holiday with friends/family
(will or will not occur)
Visitors arrived/failed to arrive
Appeared excessively agitated
Appeared in a bad mood (e.g. angry, anxious)
Source: Adapted from http////www.udel.edu.cds./pbs/downloads/pbs_settingeventlist.doc
Antecedents or triggers are those specific conditions that lead directly to the
occurrence of the behaviour (e.g. the teacher asks the learner to sit on the
carpet for circle time). Teachers thus need to determine what happens just
before the behaviour occurs that sets it off. In order to determine what the
antecedents are, teachers should aim to answer questions such as the
following:
What activities/periods lead to the behaviour (e.g. art, music time, free
play, and maths)?
What time of the day or day of the week is the child more prone to
problem behaviour?
What observable classroom events lead to the behaviour (what did the
teacher and peers say or do)?
In order to help teachers determine the antecedents (triggers), the use of an
A-B-C chart is recommended, which involves writing down the events that
immediately precede the behaviour (A = Antecedents), the challenging
behaviour itself (B = Behaviour) followed by a description of the immediate
consequences (C = Consequences). The most common antecedents are
placing demands on the learner; transition times (e.g. going from one
activity to another, from one room to another, from one person to another);
paying low attention to or diverting it from the learner; and removing a
preferred item from the learner (Kuhn, 2012). A completed A-B-C chart for
Sally is shown in Table 7.3.
Table 7.3 Completed A-B-C chart
Time
Setting
A = Antecedent
B = Behaviour
C = Consequence
09h00
Circle
time
I asked Sally to sit on
the carpet for circle
time (transition).
She screamed.
I ignored her behaviour.
09h10
Circle
time
Sally sat very close to
other children.
She hit other
children.
I looked at her and told
her it was not
acceptable behaviour.
09h20
Circle
time
Sally sat on carpet.
She screamed
and hit other
children.
I took her away and
placed her on the
“naughty chair”.
09h30
Circle
time
Nothing
She kicked the
“naughty chair”
and screamed.
I ignored her behaviour.
When examining the completed A-B-C chart (Table 7.3), a clear pattern
arises of a child who does not want to sit too close to the other children on
the carpet, possibly because it makes her feel insecure. One can also see
how her behaviour is becoming more intense and challenging. In addition, it
is evident that neither the teacher’s traditional punishment of the behaviour
nor her ignoring the behaviour seems to be effective. The A-B-C chart thus
helps when trying to formulate a hypothesis of why this specific behaviour
occurs.
7.5.4 Describing the function of the behaviour
Throughout this chapter, the fact that behaviour serves a specific purpose
for the child is highlighted. In order to understand this, the teacher needs to
put herself in the child’s position and answer this simple question: “What
did I gain by engaging in the challenging behaviour and what did I avoid?”
Answering this question leads directly to the stimulus events (the function
of the behaviour). Stimulus events are those influences that precede the
behaviour and are assumed to directly influence it by being discriminatory
with regard to the specific consequences that follow a particular response
(Durand, 1990). These events are simple, discrete and immediate. In other
words, these events could be seen as the reason for showing the behaviour.
Four main communication functions (stimulus events) have been identified,
namely:
Escape-motivated behaviour. This type of behaviour is seen particularly
when learners try to escape from demands, situations or people, and is
used as a request to terminate, postpone or withdraw from the ongoing
activity or interaction (Matson & Kozlowski, 2012). Challenging
behaviour increases when demands increase, or it may be that the
individual has strong reactions to certain requirements and tasks, which
are often related to how the training task is presented. For example, to
escape from a pen-and-pencil task, Del, a six-year-old boy with autism,
would scream, yell, cry and engage in self-injurious behaviour (Brown,
2004; Brown & Mirenda, 2006). In order to prevent these outbreaks, the
teacher would not require Del to participate in pen-and-pencil activities,
and therefore the type of challenging behaviour that he displayed had the
intended effect – to escape from a task that he did not want to participate
in. Children thus learn that by engaging in challenging behaviour, adults
stop making demands and this behaviour is then negatively reinforced. It
is important to understand that this is not intended as manipulative
behaviour, but that the specific task creates a feeling of panic, as the
individual feels that he has no control of the situation, making the actual
state intolerable, which then results in the challenging behaviour.
Attention-seeking-motivated behaviour. This type of behaviour is seen
when children are ignored or have too little contact with others, and is an
attempt to elicit or request social attention (Durand, 1990; Matson &
Kozlowski, 2012) (see Figure 7.2). Typically developing children do not
seek attention as such, but attention with some kind of meaning, for
example play, comfort, food, and so on. Challenging behaviour may also
be an attempt to request proximity and interaction with another person
(teacher or peer). For example, Sarah engages in silly behaviour,
giggling, repeating people’s names, imitating animal noises, and talking
to imaginary people (description of the behaviour) in the art activity
when she has to work in a small group (trigger). Her teacher becomes
frustrated, which delights Sarah’s peers and they also continue to giggle
(function of the behaviour). This is more likely to occur on a Monday
after having spent a weekend at home (setting event). In this example, we
can thus clearly see that the behaviour gets the child the attention she
wants, and therefore serves a purpose. If the challenging behaviour thus
serves an attention-seeking purpose, it is important for teachers to
withhold attention directly following the challenging behaviour,
otherwise the child will learn that challenging behaviour is an effective
way of getting attention.
Figure 7.2 Attention-seeking behaviour
Tangible consequence-motivated behaviour. This type of behaviour is
seen when children are, firstly, denied access to a preferred object,
activity or edible; secondly, when an item that they obtained or
manipulated inappropriately is removed and they want it back; or thirdly,
when delays occur between asking for the item and being given it
(Matson & Kozlowski, 2012). For example, Karabo was playing with a
piece of string and the teacher felt he was not paying attention to her, so
she took it away from him. This resulted in Karabo banging his head
against his desk. This violent display of behaviour took the teacher
totally by surprise, and she gave Karabo the piece of string back. In this
situation Karabo learnt that if he wanted to get something back that was
taken away from him, he should bang his head on the table. It is
important to remember that, even though most tangible consequencemotivated behaviour is seen when food, toys or other favourite activities
are involved, it might also be seen in cases such as Karabo’s when a
tangible item (the piece of string) has value for the child, but does not
have any real significance or meaning for the adult. If a child with ASD
is busy with a particular routine (e.g. placing all the toys in a line) and the
routine is interrupted, challenging behaviour might be seen (Hyman &
Levy, 2013). Self-injurious behaviour (such as head banging) is often
either a reaction to frustration (hindrance) or a reaction to experiencing a
feeling of powerlessness and injustice.
Sensory feedback-motivated behaviour. Unlike the other behaviours,
which are primarily displayed to avoid certain activities or tasks (e.g.
escape-motivated behaviour) or to obtain certain things (e.g. attention or
tangible consequence-motivated behaviour), behaviour that is displayed
for sensory feedback purposes aims to provide specific sensory
consequences (e.g. auditory, visual or tactile). This is seen in cases where
the environment either provides too much sensory stimulation (e.g. the
child might feel overwhelmed by the noise and lighting levels, and then
engage in sensory feedback-motivated behaviour in an attempt to shut
out the world), or when there is too little stimulation in the environment
(e.g. if the child feels bored, he might engage in sensory feedback
behaviour in order to provide some form of feedback, like banging or
spinning objects). These sensory-motivated behaviour are often
reparative, perseverative and stereotypic (Hyman & Levy, 2013).
Stereotypical body-rocking movements may also be an attempt to
provide some form of kinaesthetic feedback. The easiest way to
determine if behaviour is sensory feedback motivated is to ignore it, as
ignoring has no effect on this type of behaviour.
There is a well-known saying that in order to find anything, you must be
looking for something! Bearing this in mind, and trying to determine what
the function of a specific behaviour is, a behaviour function scale was
developed based on the MAS (Motivation Assessment Scale) work of
Durand (1990). Although the behaviour function scale (see Table 7.4) will
provide an indication of the main functions of the behaviour, it should be
remembered that the majority of children use challenging behaviour for
more than one purpose. In intervention, the general rule of thumb is that the
behaviours that exist with the highest frequency are the ones that should be
addressed first.
7.5.5 A last word on assessment
In the past, the majority of time was spent on trying to resolve what
happens after the behaviour is seen; however, current thinking is that the
majority of time should be spent before the behaviour occurs in an attempt
to prevent it (Beukelman & Mirenda, 2013), therefore in order to
understand the behaviour, the following four issues have to be considered:
i. What does the challenging behaviour look like? The child does …
(description)
ii. What appears to have triggered the challenging behaviour? When …
(trigger)
iii. What function does the behaviour serve? In an attempt to … (function)
iv. What are the setting events for the behaviour? This is most likely to
occur when … (setting events).
7.6 MANAGING THE BEHAVIOUR: POSITIVE
BEHAVIOUR SUPPORT
In the first part of this chapter, challenging behaviour was described from a
functional perspective, highlighting the fact that behaviour serves a
particular function for the individual. In this part of the chapter, positive
behaviour support will be used as a means of managing challenging
behaviour. Positive behaviour support relies on proactive strategies that
seek to prevent the challenging behaviour from occurring and hence
advocates that the majority of time should be spent on addressing the
behaviour before it occurs (Beukelman & Mirenda, 2013). Furthermore,
positive behaviour support is contextually appropriate and aims to use the
least intrusive yet most effective procedures possible. It uses universal
preventative strategies, such as the adoption of consistent expectations,
training learners to understand these expectations, providing feedback and
consistent reinforcement of expected behaviours (Thompson, 2011).
Positive behaviour support differs from more traditional approaches as,
although it focuses on the reduction of the problem behaviour, it is more
concerned with increasing the child’s overall success and associated quality
of life.
Inherent to this is the importance of building a relationship with the learner,
as this is the most effective way to overcome the obstacles, understand his
behaviour and try to support him. This makes the learner feel comfortable
with the teacher and trusting her, making it possible to deal with the
challenging behaviour. In a study with teachers in the US who were dealing
with learners with challenging behaviour, one teacher explained: “Most of
the time I am able to bring him down cause I’ve built a relationship with
him … I think the key thing with these kids is building a relationship with
them” (Orsati & Causton-Theoharis, 2013).
Table 7.4 Behaviour function scale
Function
Escape
Behaviour
Questions
Does the behaviour occur
following a request to perform a
difficult task?
Does the behaviour occur when
any request is made?
Does the child seem to do the
behaviour to upset or annoy you
when you are trying to get him to
do what you ask?
Does the behaviour stop shortly
after you have stopped making
demands/working with the child?
SCORE
Social
attention
Does the behaviour occur when
you talk to others in the room?
Does the behaviour occur when
you stop paying attention to the
child?
Yes
No
Uncertain
Function
Behaviour
Questions
Yes
No
Uncertain
Does the child seem to display
this behaviour to annoy or upset
you when you are not paying
attention to him?
Does the child seem to display
this behaviour in order for you to
spend more time with him?
SCORE
Tangible
consequences
Does the behaviour ever occur to
get a toy/food/activity (or person)
that the child has been told he
cannot have?
Does the behaviour occur when
you take away a favourite
food/toy/activity?
Does the behaviour stop shortly
after you have given the child the
toy/food he has requested?
Does this behaviour occur when
the child has been told that he
cannot do/have something?
SCORE
Sensory
feedback
Does the behaviour occur
continuously if the child is left on
his own?
Does the behaviour occur
repeatedly in the same way when
no one is around?
Does it appear to you that the
child is enjoying it?
When the behaviour occurs, does
the child seem calm or unaware
of his surroundings?
SCORE
Powell et al. (2006) propose a hierarchical support triangle encompassing
four levels for use as a basis for the development of a multilevel behaviour
management plan, which is presented in Figure 7.3. One of the important
results of this model is that there are specific strategies that can be used in
the home context, and there are also specific classroom-based strategies. It
is important to acknowledge from the outset that the home and the school
context cannot be run in the same manner, as we know that behaviour is
context bound. Although this book is written specifically with the
classroom context in mind, the home context will be dealt with briefly in
line with the zoom lens metaphor. In addition to this, each child should be
viewed individually, as one child might use tantrums to gain attention or
avoid work, while another might engage in the same behaviour owing to
illness or sleep deprivation. Hence, one can never take a one-size-fits-all
perspective when dealing with behavioural difficulties.
7.6.1 Level 1: Building emotional intelligence
This level represents the supports that all children (but particularly younger
children and those with developmental delays) need in order to develop
emotionally and socially.
In the home context it is important to explain to parents how emotions
develop (as described earlier in this chapter). Parents need to understand
that emotional regulation is concerned with how the child perceives and
reacts to different events and that, in ordinary situations, children depend on
adults when they are experiencing stress. Younger children will look at
adults in order to decide how they should react in particular situations.
Teenagers, on the other hand, make more use of their peer group to assist
with this. Effective self-regulation contributes to children’s experiences of
coping and their belief in themselves. Another important responsibility that
parents have is to help shape their children’s character, and the following
six universal core values might be helpful: trustworthiness, respect,
responsibility, fairness, caring and citizenship (T R R F C C).
Figure 7.3 Multilevel behaviour management plan
In the school context, learners need to be able to direct attention to
themselves, to others, to objects and to events in the environment to enable
them to learn. Warm, attentive teachers who engage and encourage learners
are effective in creating a sense of belonging and community in classrooms
that motivate children. Furthermore, teachers should deepen their
understanding of all learners in the classroom, find out what they enjoy and
what their strengths are, and also learn to read their individual cues (e.g. if
they become bored and start pushing each other around) (Orsati & CaustonTheoharis, 2013). Teachers should also be aware of how to create mutually
respectful and supportive relationships between themselves and the parents,
as this creates a feeling of security for the learners.
In the book Beautiful child, Torey Hayden (2002) implemented a traffic
light system to help children understand and express their own feelings,
thereby building internal structures of self-control and adaptive coping.
Teachers might find this a valuable tool for helping all children build their
emotional intelligence. Each of the traffic lights represents a zone: the red
zone uses words that describe out-of-control behaviours; the orange zone
uses words that describe when a child is moving out of the green zone
without being totally out of control; and the green zone describes optimal
learning behaviours (Marlowe & Hayden, 2013). Once children are able to
identify the zone they are in, they can use the zone solutions to develop
strategies that will help them to remain in the green zone. Table 7.5 shows
some practical examples.
Table 7.5 Traffic light system to build emotional intelligence
How am I feeling?
Zone
What should I do?
Like punching someone
Like insulting someone
Wild
Like bullying someone
Like kicking someone
Like hurting myself
Out of control
Like not listening
Leave the group and
take a break with my
teacher
use relaxation
techniques
take alone time and
listen to music, walk,
read
(Red)
do some hard work with
my body
run some laps around
the sports field.
Like being a distracter
Like making noises
Like I have ants in my
pants
Like pacing
Off task
Like not looking at the
teacher
Like touching others
Use relaxation techniques.
Clasp my hands together
tightly.
Go for a walk.
Chew some gum.
Get a drink of water.
Tell my teacher that I am
having a hard day – maybe
she can help!
(Orange)
How am I feeling?
Zone
What should I do?
Like giving positive
comments
Encouraging
Nice
Calm
Friendly
Like listening
Like working hard
Like looking at my teacher
Participate in class activity.
Have fun.
Encourage classmates.
Respect the personal
space of others.
Smile.
(Green)
Source: Adapted from Hayden (2012)
Self-management interventions (such as the traffic light system) require
teachers to teach learners how to identify unacceptable behaviours and
replace them with socially acceptable behaviour. Research has shown that
learners who had been trained in self-management techniques performed
better in maths, spelling, written work (such as essays) and homework
completion (Thompson, 2011).
Another strategy that been endorsed as a best practice technique based on
its proven international success with culturally, linguistically and
socioeconomically diverse learners is the Good Behaviour Game (Nolan,
Houlihan, Wanzek & Jenson, 2013). It entails the teacher, together with the
learners, drawing up a list of inappropriate classroom behaviours (e.g. outof-seat behaviour, shouting out, etc.). These behaviours are then monitored,
and if the learners meet a set target (e.g. if no more than five of these
behaviours occur in a given time), the whole class is rewarded (e.g. allowed
a few minutes of free play, few minutes of extra break time, etc.). Teachers
have also adapted this game, for example by dividing the class into two
teams, and awarding a mark to the relevant team if any of these behaviours
are noticed in that team. This Good Behaviour Game has also proven to
have positive effects beyond the original target behaviours, and has also
washed over to other situations beyond the classroom, therefore earning the
description as a behavioural vaccine (Nolan et al., 2013).
7.6.2 Level 2: Prevention practices and positive programming
In real life, everybody has to learn how to cope with concepts such as
“later”, “no” and “good-bye”, as well as dealing with emotions when
experiencing failure, frustration, criticism, being teased or being sick, and
when required to perform non-preferred tasks (LaVigna & Willis, 2005).
Although every possible effort should be made to keep these events to a
minimum, both parents and teachers realise that they should help children
learn how to cope with negative emotions by increasing their social skills.
In the home context, it is important that parents are empowered to discipline
their children effectively. They need to understand that love for their
children (and a good dose of humour at times!) is the discipline guide, and
that they should never discipline when feeling angry or out of control.
Consistency is another important aspect. For example, if it is the child’s
responsibility to make his own bed, this rule should always apply. Apart
from discipline, the home also provides the cornerstone for teaching
children to have empathy for others, for fostering friendships and solving
social dilemmas, and for children to understand their own emotions.
In the classroom context, teachers are encouraged to make use of visual
schedules to make abstract time visible and to organise sequences of events
or steps in a task (see Table 7.6). Visual schedules provide consistent cues
about the daily routine (the timetable), helping the child to anticipate what
will happen next, thereby reducing anxiety between transitions (Bopp,
Brown & Mirenda, 2004). In order to make a visual schedule, the teacher
should write down what activities are planned for the day in chronological
order (see Table 7.7). Next, she should decide on the type of symbol that
will be used to represent each activity, depending on the children’s level of
functioning (De Clercq, 2003). For Grade 1 children, a combination of real
objects and photos or pictures (e.g. from magazines) might be used at the
beginning of the year, while line drawings (e.g. picture communication
symbols) might be appropriate for Grade 2 children, and written words for
those in higher grades.
It is important that the symbol selected should involve the least possible
amount of effort for the individual, so if there is one learner in the class who
is not yet able to read fluently, the visual schedule should also contain line
drawings. The teacher should point to the next item on the schedule in order
to help learners understand the activity that they will be doing, and then
remove it when completed in order to help them understand the progression
between the activities. Table 7.6 shows examples of different classroom
schedules.
Table 7.6 Examples of different classroom schedules using Picture Communication
Symbols™1
Easy 4-option schedule using
soap boxes showing real
objects and graphic symbols
A picture-based schedule
A Velcro-strip
graphic symbol
schedule
A schedule with different
levels of representation made
from lunch boxes
A hand-held (portable)
graphic symbol-based
schedule
A Velcro strip object
symbol and
photograph-based
schedule
Easy 4-option schedule using
soap boxes showing real
objects and graphic symbols
A picture-based schedule
A Velcro-strip
graphic symbol
schedule
1 Picture Communication Symbols (PCS) is a registered trademark of Mayer Johnson, a
Tobii Dynavox Company of Pittsburgh, PA (www.mayer-johnson.com)
Teachers should also remember that they can change the physical
environment, as something in the environment might act as a setting event,
as described earlier. This could include strategies such as changing the
layout of the classroom or the desk arrangement (as described in Chapter 5),
the traffic patterns in classrooms, as well as the materials that are used.
Ensuring a balance between small- and large-group activities and between
structured and unstructured activities is also useful and prevents boredom
and fatigue, both conditions that could lead to escape-motivated behaviour
(Sigafoos et al., 2009). Activities should be varied, creative and planned to
fit the developmental levels of all the learners – teachers could try some of
the differentiated teaching strategies described in the previous chapter. The
importance of providing clear instructions, focusing on what to do rather
than on what not to do, has also been dealt with. Finally, teachers could be
encouraged to ignore minor inappropriate behaviour and to provide ample
positive attention, encouragement and praise when appropriate.
Table 7.7 Designing a visual schedule
Activity
Real objects
Line drawings
Written
words
Circle time
Piece of carpet
Group of children symbol
Circle time
Numeracy
Calculator
Calculator symbol
Numeracy
Break
Lunch box
Lunch food symbol
Break
Literacy
Storybook and pencil
Books symbol
Literacy
Art and
crafts
Paint brush
Pencils and scissors
symbol
Art and crafts
Free play
Miniature cars, dolls and
balls
Toys symbol
Free play
7.6.3 Level 3: Positive behaviour support
In the home context, parents should be supported to set reasonable and
consistent limits, and to give effective instructions. They should aim at
fostering their child’s socio-emotional skills, such as cooperative play and
friendship skills, understanding and expressing emotions, empathy, selfcalming and resolving conflict.
In the classroom, teachers should follow the four-step assessment strategy
discussed earlier, namely describing the behaviour, the trigger(s), the
function(s) and finally the setting events. If the behaviour is not understood,
it cannot be managed and treated!
Choice-making interventions are also effective as they allow children with
more efficient ways to exert control, express preferences, and indicate
wants and needs (Sigafoos et al., 2009). A teacher can thus give two
different table-top activities and allow the children to choose which one
they would like to do first before moving to the next one.
Next, the teacher should try to avoid situations that are emotionally
overwhelming, as prevention is better than cure. However, in cases where
this is not possible, the individual should be helped to identify the activities
and tasks that induce stress, and appropriate strategies for self-regulation
when stressful situations appear should be taught (please refer to Level 1
for a discussion of possible strategies). The predictability and understanding
of the tasks and activities (e.g. using visual schedules) can also be
enhanced.
Another useful strategy is the use of contingency maps, which was alluded
to earlier in this chapter when Del’s case was presented. These maps aim to
provide information about the current (i.e. problem) and the desired
behaviour, and help children understand the unwritten social rules
(Beukelman & Mirenda, 2013). Such a map depicts the antecedent that
typically triggers the challenging behaviour, the challenging behaviour
itself, as well as the natural consequences that will follow it. However, it
also includes the natural consequences that will follow if the desired
behaviour is used. A contingency map is shown in Figure 7.4.
Figure 7.4 Contingency map
Teachers can also attempt to integrate social stories into teaching (Matson
& Kozlowski, 2012). This intervention is becoming increasingly popular
when teaching learners more appropriate social behaviours during existing
daily routines. Social stories are short narratives (stories) specifically
written to describe a behaviour (e.g. hugging) and the anticipated behaviour
associated with each (e.g. who, how and when to hug) (Gray, 2003). Social
stories focus on describing the social situation that is encountered, rather
than on instructing the learner through the whole situation as they provide
social information to teach appropriate (versus inappropriate) social
behaviour by making some of the unwritten and unspoken rules, as well as
non-verbal cues, more obvious (e.g. arms folded across the chest means “I
don’t want a hug”). Social stories can therefore serve the purpose of
introducing and changing behaviour (Rathbone, 2016). There is published
evidence that social stories are effective for individuals with learning
disabilities (Kalyva & Agaliotis, 2009); to decrease disruptive behaviours
of children with ASD (Ali & Frederickson, 2006; Ozdemir, 2008); to teach
children with ASD about sexuality (Tarnai & Wolfe, 2008); and to change
problematic lunchtime behaviour related to independently entering the
eating area (Toplis & Hadwin, 2006). An example of a social story is shown
in Figure 7.5.
Figure 7.5 Example of a social story: “All about hugs”
Source: Rathbone (2016)
7.6.4 Level 4: Functional communication training
In the assessment section, the four main functions of the challenging
behaviour were described, namely:
Escape behaviour. “I don’t want object/activity/person.”
Attention-seeking behaviour. “I want social interaction/Look at me!”
Tangible-consequence behaviour. “I want object/activity.”
Sensory-feedback behaviour. “I’m bored/overstimulated.”
The main aim of intervention is to replace the challenging behaviour with
new, socially acceptable behaviour that serves the same purpose as the
challenging behaviour, only in a more effective manner. Ultimately, this
will enable the child to have better skills and competencies, impacting
positively on learning and quality of life. This type of intervention is called
functional communication training and was developed by Carr and Durand
in 1985.
This means that the first step is to identify a more appropriate message that
will be acceptable to people in the environment, for example: “Will you
please help me?” or “Am I doing good work?” rather than other attentionseeking behaviour such as biting. The important thing to remember is that
most of these children will lack the verbal skills to rely on speech to
communicate this message, hence using a symbol, a gesture or a device
with speech output could be considered (Sigafoos et al., 2009). However,
the new communication alternative should be as effective and as easy to
perform as the challenging behaviour (e.g. teachers should react to the child
using the manual gesture for “help” in the same prompt way as they would
if he engaged in self-injury behaviour). A brief discussion of the four main
challenging behaviours and some of the strategies to facilitate the
acquisition of more socially acceptable behaviours follows, but often
further support from the district-based support team and/or speech-language
therapist will be needed.
In cases where children display escape-motivated behaviour, one should
remember that they either want to stop the activity or that they need help.
Often it works well to provide these children with the sign for “help” or
“give me a break/time out” as this is a more appropriate way of getting out
of the activity (see Figure 7.6).
Figure 7.6 Manual signs used for escapemotivated behaviour
In a classic example, a young man who displayed escape-motivated
behaviour was given a wooden symbol that he was taught to use as “no” as
a replacement for his self-injurious behaviour (LaVigna & Willis, 2005).
The teacher would get him to engage in a variety of activities, but only for
short periods so that they would not provoke the challenging behaviour.
When he held up the symbol, the activity was immediately terminated.
Gradually, the amount of time that he was able to stay on task without
showing challenging behaviour increased.
Similarly, a ten-year old boy with autism was taught to touch a “No thank
you” card to reject non-preferred items (Sigafoos et al., 2009).
When children display attention-seeking behaviour, they want to draw
attention to themselves, and it is appropriate to give them some form of
calling device, for example using a small bell or teaching them to raise an
arm to call for attention. It is important to remember that initially they
might overuse this new skill that they have been taught, but it is important
for the teacher to react promptly every time so that they experience a
positive consequence. With time, this new skill will be integrated into their
existing skill repertoire and used only when appropriate. Good, positive
messages to teach to replace this type of behaviour would be phrases like:
“Am I doing good work?” or “Can I help you?”
Stop and reflect
If you think back, can you remember when a child first learnt to whistle or found out
that he could stand on one leg? Initially he would show off his new skill at every single
opportunity until the novelty wore off. The same will happen when learning to call the
teacher with a bell or a raised arm.
Tangible-consequence behaviour is more difficult to teach, as ultimately
one has to teach the names of all the possible objects or activities the child
might want. However, this is most important as it encourages choice
making, which gives a child a feeling of autonomy and importance,
combating learnt helplessness (Beukelman & Mirenda, 2013; Matson &
Kozlowski, 2012). The word “more” is a very effective generic word to
teach, as the child could indicate “more” and then point to the object or
activity. Likewise, the use of a carrier phrase such as: “I want …” followed
by pointing could be effective (see Figure 7.7).
Figure 7.7 Manual signs used for attentionseeking behaviour
Replacing sensory-feedback behaviour is not easy, and hence it is better to
try to prevent it, either by providing the individual with a meaningful
activity when boredom is noticed or, in cases where the child becomes
overstimulated, some of the external stimulation can be reduced and kept to
a minimum. In extreme cases, teachers could try to replace the sensoryfeedback behaviour with a more appropriate type of activity, for example
placing the child on a rocking horse, in a rocking chair or on a swing.
7.7 CRISIS MANAGEMENT
What could and should a teacher do when challenging behaviour occurs, for
example when the child is pulling her (the teacher’s) hair? How can she get
out of the situation as quickly as possible? The use of an element of
surprise, such as tickling the child, blowing into his face, or gently pushing
her hands into his sides may be effective. This will cause the child to gasp
for breath (inhale), automatically releasing his grip. However, always
remember that this is crisis management and not intervention. Try never to
get into a power struggle, never retaliate and never hit back.
7.8 CONCLUSION
In this chapter, challenging (problem) behaviour was described from a
functional communicative perspective, and it was stressed that all behaviour
serves a particular function. In other words, some children who are not able
to convey messages verbally, for whatever reason, may use their behaviour
to do so. Strategies for assessing challenging behaviour were given in the
form of a four-point plan.
Stop and reflect
… [Child’s name] does … [describe the behaviour] when … [trigger] in an attempt to
… [function]. This is most likely to occur when … [setting events].
Throughout this chapter it was emphasised that the majority of time and
effort should be spent on trying to understand why the behaviour occurs and
how to prevent it, rather than trying to resolve it afterwards. Finally, this
chapter concluded with a multilevel management plan that is ultimately
aimed at increasing personal control, increasing reinforcement of socially
valued behaviour as well as increasing quality of life.
REFERENCES
Ali, S. & Frederickson, N. 2006. Investigating the evidence base of social stories. Educational
Psychology in Practice, 22(4): 355–377.
Beukelman, D.R. & Mirenda, P. 2013. Augmentative and alternative communication. Supporting
children and adults with complex communication needs, 4th ed. Baltimore, MD: Paul H. Brookes.
Bopp, K., Brown, K. & Mirenda, P. 2004. Speech language pathologist’s roles in the delivery of
positive behaviour support for individuals with developmental disabilities. American Journal of
Speech-Language Pathology, 13(1): 5–19.
Bornman, J. 2007. Challenging behaviour: a lesson from a tree. SAALED News, 27(3): 17–20.
Brown, K. 2004. Effectiveness of functional equivalence training plus contingency mapping with a
child with autism. Unpublished Master’s thesis, University of British Columbia, Canada.
Brown, K. & Mirenda, P. 2006. Contingency mapping: use of a novel visual support strategy as an
adjunct to functional equivalence training. Journal of Positive Behaviour Interventions, 8(3): 155–
164.
Carr, E.G., Dunlap, G., Horner, R.H., Koegel, R.L., Turnbull, A.P., Sailor, W., Anderson, J.L., Albin,
R.W., Koegel, L.K. & Fox, L. 2002. Positive behavior support. Evolution of an applied science.
Journal of Positive Behavior Interventions, 4(1): 4–16.
Carr, E.G. & Durand, N.M. 1985. Reducing behaviour problems through functional communication
training. Journal of Applied Behaviour Analysis, 18: 111–126.
De Clercq, H. 2003. Mum, is that a human being or an animal? Bristol: Lucky Duck Publishing.
Durand, V.M. 1990. Severe behaviour problems: a functional communication training approach:
treatment manuals for practitioners. New York: Guilford.
Durand, V.M. 2011. Optimistic parenting: hope and help for you and your challenging child.
Baltimore. MD: Paul H. Brookes.
Emerson, E. & Hatton C. 2014. Health inequalities and people with intellectual disabilities.
Croydon, UK: Cambridge University Press.
Gray, C. 2003. Social stories. Available at: http://www.thegraycenter.org/social-stories/how-to-writesocialstories?tmpl=compone
Hayden, T.L. 2002. Beautiful child. New York: Avon Books.
Hyman, S.L. & Levy, S.E. 2013. Autism Spectrum Disorders. In Batshaw, M.L., Roizen, N.J. &
Lotrecchiano, G.R. (Eds). Children with disabilities, 7th ed. Baltimore, MD: Paul H. Brookes.
Kalyva, E. & Agaliotis, I. 2009. Can social stories enhance the interpersonal conflict resolution skills
of children with learning disabilities? Research in Development Disabilities, (30)1: 192–202.
Kuhn, D.E. 2012. Functional behavioural assessment and functional analysis of self-injury. In
Luiselli, J.K. (Ed.). The handbook of high-risk challenging behaviours in people with intellectual and
developmental disabilities. Baltimore, MD: Paul H. Brookes.
LaVigna, G.W., Christian, L. & Willis, T.J. 2005. Developing behavioural services to meet defined
standards within a national system of specialist education services. Pediatric Rehabilitation, 8(2):
144–155.
LaVigna, G.W. & Willis, T.J. 1995. Challenging behaviour: a model for breaking the barriers to
social and community integration. Positive Practices, 1(1): 8–15.
LaVigna, G.W. & Willis, T.J. 2005. A positive behavioural support model for breaking the barriers to
social and community inclusion. Tizard Learning Disability Review, 10(2): 16–23.
Marlowe, M.J. & Hayden, T.L. 2013. Teaching children who are hard to reach: relationship-driven
classroom practice. Thousand Oaks, CA: Corwin Press.
Matson, J.L. & Kozlowski, A.M. 2012. Environmental determinants of aggressive behaviour. In
Luiselli, J.K. (Ed.). The handbook of high-risk challenging behaviours in people with intellectual and
developmental disabilities. Baltimore, MD: Paul H. Brookes.
Nolan, J.D., Houlihan, D., Wanzek, M. & Jenson, W.R. 2013. The Good Behaviour Game: a
classroom-behaviour intervention effective across cultures. School Psychology International, 1–15.
doi:10.1177/0143034312471473
Orsati, F.T. & Causton-Theoharis, J. 2013. Challenging control: inclusive teachers’ and teaching
assistants’ discourse on students with challenging behaviour. International Journal of Inclusive
Education, 17(5): 507–525.
Ozdemir, S. 2008. The effectiveness of social stories on decreasing disruptive behaviours of children
with autism: three case studies. Journal of Autism and Developmental Disorder, 38: 1689–1696.
Powell, D., Dunlap, G. & Fox, L. 2006. Prevention and intervention for the challenging behaviour of
toddlers and pre-scholars. Infants and Young Children, 19(1): 25–35.
Rathbone, L. 2016. The effect of a sexuality training programme on the knowledge and attitudes of
caregivers working with women with intellectual disabilities who live in residential care facilities: a
social story approach. Unpublished doctoral thesis. University of Pretoria.
Shapiro, B.K. & Batshaw, M.L. 2013. Developmental delay and intellectual disability. In Batshaw,
M.L., Roizen, N.J. & Lotrecchiano, G.R. (Eds). Children with disabilities, 7th ed. Baltimore. MD:
Paul H. Brookes.
Sigafoos, J., Arthur, M. & O’Reilly, M.F. 2003. Challenging behaviour and developmental disability.
London: Whurr.
Sigafoos, J., O’Reilly, M.F. & Lancioni, G.E. 2009. Functional communication training and choicemaking interventions for the treatment of problem behaviour in individuals with autism spectrum
disorder. In Mirenda, P. & Iacono, T. Autism spectrum disorders and AAC. Baltimore, MD: Paul H.
Brookes.
Tarnai, B. & Wolfe, P.S. 2008. Social stories for sexuality education for persons with
autism/pervasive developmental disorder. Sexual Disabilities, 26: 29–36.
Thompson, A.M. 2011. A systematic review of evidence-based interventions for students with
challenging behaviours in school settings. Journal of Evidence-based Social Work, 8: 304–322.
Toplis, R. & Hadwin, J.A. 2006. Using social stories to change problematic lunchtime behaviour in
school. Educational Psychology in Practice, Theory, 22(1): 53–67.
Tyrer, P., Oliver-Africano, P., Ahmed, Z., Bouras, N., Cooray, S., Deb, S., Murphy, D., Hare, M.,
Meade, M., Reece, B., Kramo, K., Bhaumik, S., Harley, S., Regan, A., Thomas, D., Rao, B., North,
B., Eliahoo, J., Karatela, S., Soni, A. & Crawford, M. 2008. Risperidone, haloperidol, and placebo in
the treatment of aggressive challenging behaviour in patients with intellectual disability: a
randomised controlled trial. The Lancet, 371: 57–63.
8
Understanding children with
intellectual disability
8.1 INTRODUCTION
A child may have difficulty learning for a variety of reasons. Other chapters
in this book illustrate how challenging behaviour, communication
difficulties, motor skills, sensory skills and medical conditions may
interfere with normal learning. This chapter will focus on children who
have an intellectual disability, highlighting Down syndrome, fragile X
syndrome and foetal alcohol spectrum disorder (FASD). The next chapter
(Chapter 9) will describe those learners who do not have an intellectual
disability but who fail to learn effectively at school – children who are
known to have a learning disability.
8.2 INTELLECTUAL DISABILITY
Terminology in the disability field has always been, and will continue to be,
a sticky issue. In this book the term “intellectual disability”, which has
gradually replaced the classic medical term “mental retardation”, is used. In
the literature many other terms are still found, for example “cognitive
impairment” and “intellectual impairment”. Furthermore, a person-first
approach is used which means that “children with intellectual disability”
will be used rather than “the intellectually disabled” as it is important to see
beyond the disability and notice the person, not only the disability label.
Intellectual disability is not a physical trait, like having brown eyes or curly
hair or being tall, and neither is it a personality trait like being friendly or
shy.
Rather, it is a disability characterised by significant limitations in both
intellectual functioning and in adaptive behaviour, which covers many
everyday social and practical skills, and originates before the age of 18,
according to the internationally accepted definition of the American
Association on Intellectual and Developmental Disabilities (AAIDD)
(Schalock et al., 2010).
From this definition it is thus clear that intellectual disability is
characterised by a number of specific features, including the following:
The child’s intellectual functioning is significantly sub-average, which
will lead difficulties in the classroom with attention, perception, thought
processing, memory and generalisation.
Limitations related to the intellectual functioning will be seen in at least
one of these three domains (conceptual, practical and socialisation) when
the child is compared to peers of similar age or culture. Conceptual skills
include language, literacy, numeracy, money, time and self-direction
aspects. Practical skills include activities of daily living, healthcare skills,
schedules and routines, safety and using a telephone. Social skills include
interpersonal skills, social responsibility, self-esteem, social problem
solving and the ability to follow rules (Shapiro & Batshaw, 2013).
Inclusive community settings are important (i.e. places where these
children learn, live, work and play together such as schools, churches,
libraries, sport stadiums, etc.). Can you still remember Rachel’s story in
Chapter 1? This implies the right of everyone, including Rachel, to be
socially included in their communities (Westling & Fox, 2009).
The impairment is the result of an injury, disease or abnormality that
manifests before the age of 18, for example a mother taking drugs or
alcohol during her pregnancy, resulting in FASD, chromosomal or
genetic disorders (e.g. Down syndrome or fragile X syndrome), extreme
premature births, birth injuries, illness (e.g. rubella or meningitis) or poor
nutrition (Shapiro & Batshaw, 2013).
What is also striking in this definition is the fact that ability-level (based on
IQ-score) classifications (mild, moderate, severe, profound) are not used
and that the emphasis is more on the amount of support the child needs. We
know that IQ tests have not always been a true reflection of a child’s
abilities as they may not capture all forms of intelligence, and in many
cases IQ scores have resulted in parents having low expectations of the
child, thereby limiting opportunities for learning. This definition therefore
points to a move away from the medical classifications (where the emphasis
was on the child and the “problem”) to a more functional classification
where the emphasis is placed on the effect of the impairment and the role of
the environment. This is in line with the World Health Organization’s
International Classification of Functioning, Disability and Health and
Functioning – Children and Youth Version (ICF-CY) (World Health
Organization, 2007) that looks at the opportunities and barriers children
face in participating effectively in their particular environments.
This functional classification marks a philosophical shift from focusing on
the degree of impairment to the amount of support required by these
children in more than one major life activity (e.g. mobility, communication,
self-care and learning) in order to participate optimally in inclusive
environments. One tool that is used is the Supports Intensity Scale –
Children’s Version (SIS-C) (Thompson et al., 2004). The SIS-C measures
the child’s support needs in personal, school-related and social activities in
an attempt to identify and describe the types and intensity of the support he
requires. The School Learning category, for example, contains nine items
and measures activities associated with acquiring knowledge and/or skills
while attending school (e.g. learning academic skills, learning how to
problem solve). Each item is then rated regarding the type of support and
how often it is needed, as well as how much total daily time is needed in
order to provide it (Shogren et al., 2016).
As children with intellectual disability are slow to achieve their
developmental milestones, they remain dependent on support for longer
than their typically developing peers. Moreover, they require support that is
ongoing in nature, which implies that they will need lifelong help to lead
meaningful and happy lives. However, the nature of the support will change
and vary as new skills are mastered and as they move to a new
developmental level (Westling & Fox, 2009). Very often it is seen that as
the child moves from one major life phase to another, more support is
needed, for example when starting pre-school for the first time, or when
moving from pre-school to Grade 1, or from the Foundation to the
Intermediate Phase, and so forth. We should also acknowledge that the
support required by these children is extensive, which implies a great deal
of assistance to cope with learning. In summary, this type of functional
classification acknowledges that support can have a successful impact on
the child’s ability to live, work, learn and participate in leisure activities.
Although children with intellectual disability learn more slowly than their
typically developing peers, they are still able to learn, irrespective of the
degree of impairment.
What specific learning characteristics can a teacher expect from children
with intellectual disability? Remember that not all children will display all
of these characteristics, but these are some of the features of which teachers
should be mindful:
These learners may have difficulty focusing on a particular important
aspect, as they may get distracted by the detail and other features of the
learning material It is therefore important for the teacher to be explicit
about the most important aspects, for example: “The most important fact
in this lesson about mammals is that they don’t lay eggs but their babies
are born live, and the mothers suckle their young”. It is obvious that this
type of teaching practice will not only help the children with intellectual
disability, but all children will benefit, therefore summarising the facts is
good teaching practice.
They may have limited opportunities to learn in the natural environment
due to their problems with paying attention. This aspect is covered in
detail later in the chapter.
They may have difficulty remembering facts as their memory is affected.
Remembering previously learnt skills, behaviours and facts is difficult
because of limited practice opportunities, exposure and generalisation
(Kaiser & Roberts, 2013).
They may have problems synthesising skills and facts. Often these
children learn skills as separate entities and do not integrate them, and
therefore it is important that teachers draw their attention to the overlap
and synthesis of skills. Providing practical learning opportunities assists
with this. For example, rather than simply counting, the same principles
could be taught by counting money, sweets, and so on. The teacher
should draw the inferences for the learners, for example: “Yesterday we
counted the sweets. Can you remember that? Today we are going to count
pencils in the same way”.
They may have difficulty generalising facts; in other words applying their
learnt skills in real-life contexts. It is for this reason that a naturalistic
teaching approach is recommended (e.g. teaching by using real-life
situations) (Kaiser & Roberts, 2013).
They may have problems with self-regulation (difficulty in monitoring
and managing their own behaviour). In Chapter 7 we discussed the use of
the traffic light system, which can assist with this.
Next we will explore the possible personal-social characteristics:
Friendship and personal relationships might be compromised in cases
where there are limited opportunities for interaction with peers
(Bornman, 2006). One important prerequisite for true inclusion is that
typically developing peers must know about the disability and its
implications for the child’s development of skills and abilities within
various domains, and at the same time children with disabilities should,
to some degree, also be encouraged to be actively involved (by using
different forms of communication to show interest, dislike, fascination or
appreciation, and asking questions, and not simply being a passive
outsider and onlooker (Downing & Falvey, 2015). If children do not have
the opportunity to interact with peers with disabilities, they might tend to
exaggerate the helplessness or pitifulness of these children, and feel sorry
for them. Research shows that the attitudes of typically developing
children become more positive as a result of inclusion (Dessemontet &
Bless, 2013). The Pathways story at the end of Chapter 2 highlights the
positive effects of inclusion on the attitudes of peers.
The sexuality of individuals with intellectual disability is often
misunderstood. At the one end of the continuum they are regarded as
sexually innocent – perpetual children. This belief implies that these
individuals have little or no understanding of their bodies, making them
prime targets for sex offenders (Bornman, 2015). At the end of the
continuum, it is mistakenly believed that individuals with intellectual
disability have a heightened, uncontrolled sex drive, stemming from their
behaviour that differs from the norm, such as public masturbation. The
real reasons might be the lack of information that these individuals have
about acceptable and unacceptable behaviours, their difficulty in making
sense out of images portrayed in the media, such as music videos,
television and magazines, and their limited self-regulation skills. A recent
international meta-analysis, studying 18 374 children with disabilities
(Jones et al., 2012), reported that up to a quarter of children with
disabilities will experience violence (including sexual violence) in their
lifetime. Children with intellectual disability have an even higher risk of
experiencing violence than children with other forms of disability. The
offenders are often known to the victims, and as they pick up on the
vulnerability of these children, the crimes are often of a repeated nature
(Bornman, 2015), Research has shown that the longer the period of the
child’s exposure to abuse, the more traumatic it becomes (Spies, 2012). It
is therefore critical that children with disability receive appropriate
training to empower them and reduce their victimisation.
A higher incidence of challenging behaviour exists in children with
intellectual disability compared to their typically developing peers
(Beukelman & Mirenda (2013). In Chapter 7 it was highlighted that
challenging behaviour should be interpreted as attempts to communicate,
for example escape-motivated behaviour (e.g. to get away from a difficult
task); attention seeking-motivated behaviour (e.g. to attract the teacher’s
attention); tangible consequence-motivated behaviour (e.g. wanting a
specific toy); or sensory-feedback-motivated behaviour (e.g. in the event
of sensory deficits). A lack of preferred and functional places to go,
people to be with and things to do (activities) in addition to these
communication difficulties may be further reasons for challenging
behaviour to occur (Beukelman & Mirenda, 2013).
In many cases, the causes of the intellectual disability are unknown, and
even if they were, this would not make the condition curable, nor would it
impact on the type of intervention provided. However, in cases where the
origins are chromosomal or genetic, genetic counselling is advisable, as
these inherited conditions carry an increased risk of recurrence. Parents
want to know why their child has an intellectual disability and this
knowledge could foster acceptance. Some parents feel that it provides them
with a clearer idea of how to help their child – for example, they are able to
search on the internet and read more about the condition. Unfortunately,
though, the intellectual disability label often conveys the mistaken idea that
this child cannot learn certain things while in fact the only way to know
what a child can and cannot learn is to involve that child in an active,
exciting learning process.
The term intellectual disability is really an umbrella term that encompasses
a large range of syndromes (e.g. Down syndrome, fragile X syndrome,
FASD, Rett syndrome, Angelman syndrome). As is true for cerebral palsy,
intellectual disability can also co-occur with hearing, vision, motor and
communication disorders, as well as with epilepsy (Shapiro & Batshaw,
2013). Three specific high-incidence syndromes that teachers might
experience in the classroom associated with intellectual disability, namely
Down syndrome, fragile X syndrome and FASD (which is totally
preventable), will be described in a little more depth. However, knowing
that a learner has an intellectual disability, or knowing the medical
diagnosis, may never be used to devalue or marginalise the child, for
example: “He has Down syndrome and all learners with Down syndrome
cannot do x or they always act like y”. This type of stereotyping is grossly
inaccurate and stigmatising.
8.2.1 What is Down syndrome?
Down syndrome is a chromosomal disorder and was the first syndrome
associated with intellectual disability. Archaeological excavations from the
7th century BC found a skull that displays the physical features of a person
with Down syndrome, and paintings from the 1500s show children with
Down syndrome-like features (Roizen, 2013). The most common type of
Down syndrome results from the presence of a third chromosome, number
21, in all the cells of the body (normal cells have two copies, one from each
parent), therefore another name for Down syndrome is Trisomy 21, which
means three copies of chromosome number 21 (Batshaw, Gropman &
Lanpher, 2013). Children with Down syndrome have a variety of features,
such as an intellectual disability and distinctive facial features (see Figure
8.1).
Heart defects at birth occur in 40 to 50 per cent of people with Down
syndrome (South African Inherited Disorders Association, n.d.). Surgical
intervention may be successful, but many of these children live with some
kind of cardiac (heart) problem. Fatigue is an important side effect to take
note of in cases where heart defects are present, as this may seriously
hamper the activities of daily life, impacting on life experiences. Hearing
may be partially affected in up to two-thirds of people with Down
syndrome, and is frequently associated with conductive hearing loss,
therefore regular hearing tests are advisable (Tharpe, 2009; Roizen, 2013).
Epicanthal folds (small skin folds on the inner corners of the eyes), muscle
weakness and susceptibility to infection are also common characteristics.
Often, gross generalisations are made about people with Down syndrome,
for example: “All people with Down syndrome love to be hugged and
cuddled”. Traits such as these are not attributable to Down syndrome per se,
but rather to the individual’s personality.
Figure 8.1 Example of the facial
features of a child with Down
syndrome
8.2.2 What is fragile X syndrome?
Fragile X syndrome is a family of genetic conditions that are related in that
they are all caused by gene changes in the FMR1 gene on the X
chromosome (Bagni, Tassone, Neri & Hagerman, 2012). If one looks at the
X chromosome under a microscope, it appears fragile due to a constriction
caused the FMR1 gene, giving this syndrome its name. Fragile X syndrome
(first described by Martin and Bell in 1943 and thus also known as MartinBell syndrome) is the most common cause of inherited intellectual
disability, and the individual support needs vary markedly.
As males contribute a Y chromosome and not an X chromosome to their
sons, they cannot transmit fragile X syndrome to them. However, if they
carry the fragile X, they will transmit it to all of their daughters, as males
contribute their X chromosome to their daughters. On the other hand,
females carrying one copy of the fragile X can transmit it to either their
sons or daughters; in this case each child has a 50 per cent chance of
inheriting the fragile X. In general, the transmission of fragile X often
increases with each passing generation.
Not everyone with fragile X syndrome has the same signs and symptoms,
even if the affected people are in the same family. The most prominent
characteristics fall into five categories:
Intelligence and learning. Most girls who have fragile X syndrome may
appear to have normal intellect or may have a mild form of intellectual
disability, because of their second X chromosome, although learning
difficulties and emotional problems are common (Bagni et al., 2012).
Approximately 80 per cent of boys with fragile X syndrome have
intellectual disability, mostly in the moderate-to-severe range
(Estigarribia, Martin & Roberts, 2012). They also experience weaknesses
in working memory and attention span.
Physical appearance. Prominent characteristics include a long and
narrow face, large or protruding ears, and low muscle tone, which makes
them often appear clumsy (see Figure 8.2).
Figure 8.2 Example of the
features of a child with fragile X
syndrome
Social and emotional skills. Challenging behaviour is often seen, and
behavioural characteristics may include stereotypic movements such as
hand flapping. Social development is also atypical, and shyness and
limited eye contact is particularly noticeable. Earlier research estimated
that approximately 10 per cent of boys with autism have fragile X
syndrome (Batshaw & Perret, 1992), but with more careful clinical
diagnosis, it has transpired that although many individuals with fragile X
syndrome may have symptoms of ASD (e.g. poor eye contact,
perseverative behaviour), they do not meet the strict criteria for an ASD
diagnosis and hence newer statistics report that up to 2 per cent of boys
with fragile X syndrome are reported to have ASD (Hyman & Levy,
2013).
Speech and language skills. Although many girls with fragile X
syndrome have adequate language skills, virtually all boys with this
syndrome have delayed language ability, with their expressive language
being more affected than their receptive language (McDuffie, Kover,
Hagerman & Abbeduto, 2013). This varies with the degree of intellectual
disability, but their conversational speech is often unintelligible, and
sounds cluttered, echolalic and dysfluent, and they tend to perseverate on
certain words and sounds (Hersh & Saul, 2011).
Sensory skills. Middle-ear infections, often with an early onset in life, are
seen in 60 to 80 per cent of cases, and recurrent middle-ear infections are
present in 23 per cent of boys with fragile X syndrome (Hersh & Saul,
2011). Visual difficulties (specifically strabismus and refractive errors)
are seen in 25 to 50 per cent of children with fragile X syndrome. It is
therefore imperative that teachers ensure that these children have regular
hearing and visual tests.
While there is no current cure for fragile X syndrome, more widespread
screening for this disorder, as well as more targeted treatments, is the order
of the day. In addition to current advances in medical treatment,
multidisciplinary team involvement, including speech and language therapy,
occupational therapy, physical therapy, special education (including good
teaching practices such as differentiated teaching), behavioural
interventions, and genetic counselling should also be considered (Hagerman
et al., 2009; Hersh & Saul, 2011).
8.2.3 What is foetal alcohol spectrum disorder (FASD)?
Foetal alcohol spectrum disorder (FASD) is the largest preventable cause of
permanent intellectual disability, and occurs when an expectant mother
drinks alcohol during her pregnancy. Some authors also refer to this as
alcohol-related neurodevelopmental disorder (Paulson, 2013). At present it
is still unknown whether the amount of alcohol, the frequency of drinking
(e.g. binge pattern where no drinking takes place during the week and
excessive drinking takes place over the weekend) or timing of drinking
during pregnancy (as the brain develops throughout all three trimesters of
pregnancy) causes a difference in degree of damage done to the unborn
baby. In an attempt to raise awareness about the syndrome, Dr Smith, who
described it in 1973, decided not to name the syndrome after himself, but
rather after the cause (i.e. the effect of alcohol on a foetus). He reasoned
that if people knew that alcohol consumption in pregnant women caused the
syndrome, they would refrain from drinking, resulting in prevention.
However, this did not happen. At present, South Africa has the highest
incidence of FASD globally. The latest research figures reported a
prevalence of just under 10 per cent in Witzenberg and just over 12 per cent
in De Aar in the Western Cape, the highest rate reported worldwide (Kelly
& Mian, 2016). This is alarmingly high when compared to First World
countries, which have an incidence figure of between 0,1 and 0,3 per cent,
and which regard prevalence rates of 1 per cent as high (Kelly & Mian,
2016).
The main effect of FASD is permanent, irreversible, lifelong brain damage,
which creates an array of primary intellectual and functional disabilities
(including lack of critical thinking, poor memory and judgement; short
attention span; language deficits and poor communication skills; and
challenging behaviour, as well as secondary disabilities such as mental
health problems and drug addiction) (Mukherjee, Hollins & Turk, 2006;
Phung, Wallace, Alexander & Phung, 2011).
FASD is typically diagnosed by a multidisciplinary team that works
together to assess each of the four key features needed to make the
diagnosis. Generally, a trained medical doctor will determine growth
deficiency and FASD facial features (the first two features listed below)
(see also Figure 8.3), while a psychologist, speech-language pathologist or
occupational therapist will evaluate the central nervous system damage.
Finally, a psychologist, social worker or medical doctor will evaluate the
fourth feature, namely alcohol exposure during pregnancy (May et al.,
2013).
Figure 8.3 Examples of the facial features
of a child with FASD
Four features must be present in order to make an FASD diagnosis
(Chudley et al., 2005; May et al., 2013; Mukherjee et al., 2006; Stratton,
Howe & Battaglia, 1996):
i. Growth deficiency. The pre- or postnatal height or weight (or both)
should be at or below the tenth percentile, after making adjustments for
parental height, gestational age in the case of premature babies, and
other conditions such as poor nutrition.
ii. All three facial features associated with FASD should be present. These
include
– a smooth philtrum (the groove between the nose and upper lip is flat)
– a thin upper lip
– increased width between the eyes.
iii. Central nervous system damage. This can be assessed in three areas,
namely structural, neurological or functional impairments. Each will be
described briefly.
– Structural impairments. Owing to the high costs involved in brain
imaging, this is usually not done. One of the structural impairments
that can, however, be seen with the naked eye is microcephaly (small
head size). When structural impairments are not observable or do not
exist, neurological impairments are assessed.
– Neurological impairments. These are expressed as either hard signs
(diagnosable disorders such as epilepsy, cerebral palsy, and hearing
or visual impairments) or as soft signs. Soft signs are broad, nonspecific impairments which are determined through clinical
judgement, and include aspects such as impaired fine motor skills,
poor gait, clumsiness, poor eye–hand coordination or sensoryintegration problems.
– Functional impairments. These do not as yet have a specific pattern
but teachers should expect learning disabilities; impaired academic
achievement; behavioural problems (as a result of a lack of impulse
control, impaired judgement, poor personal boundaries, poor anger
management, stubbornness, intrusive behaviour); hyperactivity, and
problems with paying attention and concentration; high
distractibility; poor short-term memory; communication and
language problems (including both receptive and expressive
language disorders, marked lack of understanding of metaphors,
idioms or sarcasm); problems with abstract thinking and with maths;
poor cause-and-effect reasoning; poor motor skills (both fine and
gross motor skills might be delayed, which will manifest, among
other things, as poor handwriting in the classroom); and finally
sensory problems (sensory integration might be problematic and
tactile defensiveness is prominent) (May et al., 2013; Phung et al.,
2011). Teachers should also be on the lookout for hearing problems,
as research has shown that as many as 83 per cent of children with
FASD had conductive hearing loss and that 28 per cent had a
sensorineural hearing loss (Muralidharan, Sarmah, Zhou & Marrs,
2013).
iv. Confirmed prenatal alcohol exposure. This is determined by
interviewing the mother or other family members about the mother’s
alcohol use during the pregnancy (if available), through prenatal health
records or birth records (if available), or through court records (if
applicable). Reporting alcohol use during pregnancy can be
stigmatising to mothers, especially if alcohol use is ongoing (Clarren,
2005). However, in a recent South African study, between 89,1 per cent
and 96,8 per cent of the mothers of children with FASD reported
drinking an average of 13 drinks per week during pregnancy, with
specific binge-drinking patterns (May et al., 2013). A diagnosis of
FASD is still possible with an unknown level of prenatal alcohol
exposure if the other three key features of the syndrome are present.
Although there is no cure for FASD, research has shown that early
intervention focused on behaviour and education therapy, and parent
training can improve the child’s prognosis (Phung et al., 2011). Malbin
(2002) identified areas of interests and talents that act as resilience factors
and that should be used, like any strength, in planning a management
programme for such children. This includes the use of music, playing
musical instruments, composing, singing, art, computers, mechanics,
woodworking, skilled vocations (welding, electrician, etc.), writing and
poetry. She recommends that the focus should be on trying differently rather
than trying harder. The idea to try differently refers to trying different
perspectives and options based on the child’s specific profile. For example,
if the child has behaviour problems, some of the guidelines in Chapter 7
could be used; if motor skills are delayed, adaptations are recommended
(e.g. using slip-on shoes or shoes with Velcro instead of shoelaces); and if
short-term memory is impaired, strategies such as visual schedules or
timing devices can be used. This approach also encourages more strengthsbased interventions, which allows the child to develop positive outcomes by
promoting success linked to strengths and interests rather than trying harder,
which means that teachers continue to implement the same programmes
that have consistently failed over time.
There is a well-known saying that prevention is better than cure, and this is
particularly true for FASD as there is no cure. Prevention is possible if
women simply avoid drinking alcohol during pregnancy.
8.3 GENERAL APPROACH TO TEACHING CHILDREN
WITH INTELLECTUAL DISABILITY
Over the past two decades, the acceptance of inclusion as the best practice
in schools has helped to change the general public’s perceptions and
expectations of individuals who face different barriers (Constitution of the
Republic of South Africa, 1996; Donohue & Bornman, 2014; McConkey,
Kelly, Craig & Shevlin, 2015). The United Nations Convention on the
Rights of Persons with Disability (UN, 2007) and the earlier Convention on
the Rights of the Child (UN, 1989) has added momentum to inclusions on a
worldwide scale. Individuals with intellectual disability are now able to be
integrated into society, attend mainstream schools, go to shops and use
public transport, therefore all of them should be offered optimal
programmes adapted to their specific profile that allow them the
opportunity to climb the developmental ladder (Downing & Ryndak, 2015).
This type of dynamic approach will focus on functional instruction in the
natural environment. In other words, not only should the classroom
represent the community, but the community should also become a potential
classroom. Training should be age appropriate and take place in everyday
classroom routines by using the cues and corrections that are naturally
available. This type of approach is characterised by the following:
Knowing such children well, which involves gathering information about
the various home, community and other environments in which they
spend their time, and also investigating the time spent on each activity,
which helps when selecting appropriate teaching activities. If one knows
that a child has a specific interest or skill, it should be capitalised on. For
example, John really loves calculators and in the maths exercises he has a
competition with some of the other children in his group to see who can
complete the worksheet first – John with the calculator or the others
without the calculator.
Using naturally occurring examples to teach specific concepts. For
example, when teaching children about the various materials that can be
used to build houses, take them for a walk through the neighbourhood
and point them out. One of the children in the group could be asked to be
the scribe and write down the names of the various building materials
that they see, while the child with the intellectual disability can be asked
to point them out.
Providing logical responses (e.g. when requesting a pencil he receives a
pencil) and naturally occurring, real consequences. This means that the
behaviour affects the environment, which in turn responds in accordance
with the intention of that behaviour.
Putting the onus on the teacher to identify potential learning
opportunities and to implement a range of specific strategies when these
opportunities arise. It is well known that these children have less
naturally occurring learning opportunities, hence the need to plan
deliberately for them.
Mixing the type of teaching techniques used in the classroom, for
example problem-solving strategies, investigative learning, direct
instruction, hands-on learning and teaching, multimedia and technology,
as this gives all learners the opportunity to demonstrate their strengths. If
something does not work, try something else, and do not be afraid to ask
the children. They sometimes come up with the most interesting and
innovative ideas!
Ensuring that there are extramural opportunities available for children
with intellectual disability to participate in organised sport as well
encouraging them to actively participate in other physical activities, as
research has shown a positive correlation between sports participation
and motor skills in children with intellectual disability (Westendorp,
Houwen, Hartman & Visscher, 2011). Furthermore, research has also
reported that well-developed gross motor skills facilitate children’s
cognitive development (Piek, Dawson, Smith & Gasson, 2008).
In Chapter 5, strategies for differentiating the curriculum were described,
and these are also relevant for children with intellectual disability. However,
there are some additional strategies that might work particularly well with
them.
8.4 SPECIFIC STRATEGIES TO ACCOMMODATE
LEARNERS WITH INTELLECTUAL DISABILITY
8.4.1 Get to know the child: make observations
This short poem beautifully describes what is necessary for learning to
occur:
My five basic needs
I need to be seen
I need to be heard
I need to be appreciated
I need to be safe
I need to belong
When all of my needs are met then
I am ready to learn
Anonymous
The term intellectual disability might bring to mind the image of a child
who does not have the skills to interact meaningfully with others, or who is
unable to behave in a purposeful way, which will influence learning
negatively. These assumptions are unwarranted, and teachers should put
aside some time to observe such learners carefully and get an idea of their
unique strengths and vulnerabilities (Beukelman & Mirenda, 2013). It is
always wise to make a note of what they are able to do. Observe whether
such a child can follow instructions, how he responds to his name being
called and to other sounds in the classroom, and whether he can find things
that are hidden (perceptual skills). Try to determine what the child’s specific
learning style is (see Figure 8.4). Some children have stronger language and
communication skills but weaker motor and perceptual skills, while others
have opposite strengths. Some children may be oversensitive to touch and
sound, while others appear not to be bothered. With so many variations, it is
imperative that all learners need to be carefully observed and described in
great detail according to the things they can and cannot do, and according to
the way they seem to process information (learning style).
Figure 8.4 Incorporating different learning styles in the classroom
Teachers should then begin their work by focusing on the learner’s
strengths, areas of interest and learning style, and build from there: if Dan is
good at finding things and has a good sense of direction (strong visual–
spatial skills), the teacher should use a lot of visual images, such as
pictures, to facilitate optimal learning. However, if his spoken language
skills are the strongest, use that strength. He might be one of many children
who do best with multisensory input, which implies auditory (teacher talks),
visual (teacher points to pictures while she is talking) and movement
instruction, all at the same time.
Once the teacher really knows the child well, the specific learning
objectives can be prioritised. It is important to ensure that these priorities
ultimately enable children to learn new skills, which will give them more
confidence and increase their independence. By involving them in everyday
classroom routines, and showing them where materials are kept and how
things in the class are organised, they will become more self-confident and
feel a sense of belonging to the group.
8.4.2 Collaborating with families
In order to understand a child well, it is imperative to communicate with the
family (Mastropieri & Scruggs, 2010; Phung et al., 2011). Parents are
important partners in teaching children with intellectual disability (Fey,
Yoder, Warren & Bredin-Oja, 2013; Kaiser & Roberts, 2013). In fact,
literature shows that parents of children with intellectual disability have to
invest extraordinary levels of time, energy and resources to get their
children to mainstream schools and to support their progress once they are
included in these schools (De Graaf, Van Hove & Haveman, 2014). Having
a positive relationship in which both the teacher and the parents share the
same vision for the child is one of the cornerstones of school achievement.
Furthermore, if the programmes are to be successful with long-term
benefits, all team members (including the parents) must be comfortable
with the goals set for the child. Consensus may not be achieved at the
beginning of the school year and many differences in opinion can occur.
Very often, consensus building may also entail some training or information
sharing between teachers and family members.
When a problem is put on the table and everybody gives an opinion, the
pros and cons can be considered, and nobody feels left out or disregarded.
Mr Paul Mumba, a turn-around teacher from Zambia, maintains that parents
do not care what happens in class – they care about the outcomes they see
in their children. If parents do not see progress and development in their
children, they regard teachers as incompetent. Teachers are continually
challenged to think of creative ways to ensure progress, and one way of
doing this is through collaborative learning (Mumba, 2006).
8.4.3 Collaborative learning and activity-based lessons
Collaborative learning makes sense in inclusive classrooms as it takes
advantage of the naturally occurring learning opportunities that are
provided when children are grouped together in heterogeneous groups, and
the fact that it formalises and encourages support and connection (SaponShevin, 2010). Despite the critical role of literacy in the curriculum,
improving the literacy skills of children with significant intellectual
disability has remained elusive. This is due, among other things, to limited
opportunities for literacy acquisition (typically as a result of poor-quality or
absent literacy instruction) combined with teachers’ low expectations
regarding literacy for this population (Coyne, Pisha, Dalton, Zeph & Cook
Smith, 2012), therefore, this section of the text will focus on literacy-based
lessons. In collaborative learning, the classroom is divided into smaller
groups within which children’s abilities may differ considerably. Learning
takes place as information is exchanged within each group when they tackle
the tasks presented by the teacher. Working together on such a project can
increase the mutual acceptance of all members of the group and therefore
all children will benefit. It also triggers the contribution of creative
solutions by all members of the group. Although the group as a whole is
responsible for achieving the goal, each member is also responsible for
doing his own part in helping the group achieve the larger goal. In order to
accomplish this, the teacher will need to plan the task given to the learners
carefully.
Stop and reflect
In a literacy activity, the teacher asked the group to write an “I like …” book. Some of
the children who had good language skills wrote the narrative, those who were artistic
drew pictures and another group looked through magazines and cut out pictures.
Then another child in the group read the book to the rest of the class. This example
shows how everybody was able to participate.
For older children, a literacy task could include the following adaptations:
Some learners can be asked to rewrite the lesson at a lower readability
level (i.e. using shorter sentences). This new lesson can be used for
children who need an adapted curriculum (Hanreddy, 2015).
Some learners can be asked to read and retell, while others can be asked
to listen and retell the facts.
Some learners can be asked to add pictures or symbols to the text.
Some learners may be provided with a number of sentences related to the
story and be asked to place them in the correct sequence.
Some learners can be asked to mark all the difficult words in the text with
a highlighter, while others have the task of finding definitions for these
words.
Some learners may have the option of reading the text at home at night to
help with preparation.
Some learners might have the option of using electronic books, for
example the WiggleWorks e-books, which provide multimodal learning
opportunities. Including technology to provide scaffolds directly within
digital texts to support reading, is one of the most promising and growing
current literacy instruction approaches to teaching children with
significant intellectual disability (Coyne et al., 2012).
See Figure 8.5 for an example of a worksheet that can be used if the learner
is unable to write the whole word and where he only has to write the first
letter. The typically developing children in the class are expected to write
out the whole word.
Figure 8.5 Differentiated teaching worksheet for a
literacy activity
Likewise, if the child cannot learn all the words in a spelling test, he can be
expected to spell some words, and others can be given in a dotted form for
him to trace, while some words can be presented in multiple-choice format,
allowing him to circle the correct word (see Figure 8.6).
Figure 8.6 Differentiated teaching worksheet for a
spelling test
In a maths class, the teacher was explaining about comparing greater than
(>) and smaller than (<). She divided the classroom in half, and asked three
children from each group to volunteer. One child then presented the
hundreds column, another the tens column, and the last one the ones
column. The teacher then asked the child with the intellectual disability to
hand out a card from a deck of cards to each of the six children (three
children in each group). The groups then had the opportunity to arrange the
hundreds, tens and ones columns in such a way to form the highest possible
number, and the two groups then competed to see who won (i.e. which
group had the highest number). This game was repeated a few times. Later
the teacher also made it more difficult by adding a thousands column and
she could also make it easier by removing the hundreds column (see Figure
8.7).
Figure 8.7 Interactive game: teaching greater than (>) and smaller than (<)
These examples also demonstrate the principle of activity-based lessons; in
other words lessons that are designed to provide instruction within a handson activity. Teachers need to plan activities that encourage active
participation and interaction (Hanreddy, 2015). This is exactly the opposite
of using more passive strategies such as lectures and worksheets that are
aimed at teaching an isolated skill – the so-called chalk and talk lessons.
This means that, in the above example, rather than completing a worksheet
with greater than and smaller than symbols, learners had the opportunity to
be physically involved – a strategy that is particularly beneficial to learners
who learn optimally with kinaesthetic, tactile or visual input.
Apart from the activity-based lessons, other strategies that can be used in a
maths activity include the following:
Allow the use of a calculator and make use of a reference flip book
(shown in Figure 8.10).
Work out real problems that will have motivational value for the learners,
for example how many hotdogs they should sell to enable the whole class
to go to the movies.
Provide self-instructional training. For example, teach the learners to say
the steps to themselves as they work out the maths problem, such as the
BODMAS rule, which is used to determine the order of mathematical
operations.
Stop and reflect
What is the BODMAS rule? Take a calculation like 7 + (6 × 52 + 3).
Where do you start? Should one go from left to right? Or from right to left? We all
know that if you calculate them in the wrong order, you will get the wrong answer! So
mathematicians agreed on the BODMAS rule, which means:
Do things in brackets first. For example:
7 + (6 × 52 + 3) = 7 + (6 × 25 + 3)
7 + (150 + 3) = 7 + 153
= 160
Order of exponents (roots, powers) should be done before multiply, divide, add or
subtract. For example:
6 × 52 + 3 = 6 × 25 + 3
Divide or multiply, before you add or subtract. For example:
2 + 5 × 3 = 2 + 15 = 17
NOT 2 + 5 × 3 = 7 × 3 = 21 (wrong)
How do I remember the order of operations?
BODMAS!
B
Brackets first
O
Order (i.e. powers and square roots, etc.)
DM Division and multiplication (left to right)
AS Addition and subtraction (left to right)
Furthermore, teachers should not only think about how to adapt the material
(e.g. by reducing the reading, writing or language requirements of
worksheets) but they should also consider how instructions can be adapted
(e.g. by the use of clear, organised presentations, meaningful examples and
activities, and encouraging independent thinking (Mastropieri & Scruggs,
2010), as well as how assessments can be adapted. Assessment
accommodations are generally grouped into the following categories:
Presentation (e.g. repeat the instructions; read the test aloud; use large
print; use Braille)
Equipment and material (e.g. allow the use of a calculator; use
amplification equipment; provide manipulatives, such as counters)
Response (e.g. allow child to mark answers in book; provide a scribe to
record the response; allow child to point to the correct answer)
Setting (e.g. allow child to write in a separate room, such as the library)
Timing/scheduling (e.g. allow extended time, provide frequent breaks,
etc.) (National Centre on Educational Outcomes, 2014)
An example of a maths worksheet is given in Figure 8.8. In this worksheet
the teacher simplified the task by deleting some of the problems (i.e. the
child had fewer to do) and focused the child’s attention by circling the
mathematical symbol (addition or subtraction), thereby increasing the
child’s chances of success.
Figure 8.8 Differentiated teaching worksheet for a
maths test
Teachers might sometimes hear the comment: “It’s not fair that Patricia can
just draw a picture but I have to write out the words.” In these cases,
teachers can explain to the classroom what Socrates emphasised many years
ago: fairness does not mean that everybody should get the same, but rather
that everyone should get what they need.
8.4.4 Visual schedules
When we described challenging behaviour, mention was made of the use of
visual schedules (timetables), which is also a highly effective strategy for
children of all ages with intellectual disability. These can be of particular
value for providing learners with information about their classroom
timetable in a format that is comprehensible to them (e.g. “It is circle time”)
and to orientate them towards their current activity, as well as activities that
will follow. Let us look at how Lesedi’s teacher, Mrs Ledwaba, is
implementing the schedule. Mrs Ledwaba starts by dividing her daily
classroom programme into specific sections, which are each represented by
a picture with a written word and displayed on a wall chart (see Figure 8.9).
At the beginning of each activity, she takes Lesedi to the schedule and
prompts her by asking, “What are we going to do now?” She waits for
Lesedi to point to the picture and say the word, and then confirms by
saying, “Yes, you are going to do art now.” After completing the art activity,
Mrs Ledwaba explains that the activity is “finished”, and Lesedi is then
expected to turn the picture on the wall chart around (right side down) to
indicate that it has been completed. This gives Lesedi a feeling of
satisfaction, as the number of right-side-down pictures gives her a sense of
how many tasks she has already completed. Mrs Ledwaba then orientates
Lesedi towards the next activity, “Tell me what you have to do now”, and
the process starts all over again.
Figure 8.9 Classroom schedule for Lesedi
8.4.5 Explicit requesting and the use of an attention-getting
signal
Some children with intellectual disability will not have the skills to draw
the teacher’s attention in an appropriate way and will just be happy to sit
passively in the classroom. Others might experience frustration at this
inability and then engage in challenging behaviour. Without a means of
drawing the teacher’s attention prior to making a request, spontaneous
requesting will not occur. It is therefore important to teach attention-getting
responses with the requesting behaviour (Beukelman & Mirenda, 2013).
Explicit requesting consists of teaching the individual a single strategy (e.g.
putting up his hand), which can be used in all situations. The teacher then
responds by saying, “Can I help you?” or “Do you need me?”
8.4.6 Reference flip books
These reference flip books that are placed on the learner’s desk provide a
helpful study aid to review and reinforce the most important facts every
learner has to know (see Figure 8.10). These books can have a writeon/wipe-off surface, or different pages that can be torn out at a later stage
and placed inside the child’s flip file. If the write-on/wipe-off surface is
used, learners can use a wipe-off marker to trace letters, draw clock hands,
check off words or numbers they know, and much more. In order to assist
with maths, a short definition can be added next to the mathematical
symbol. For example, + means to add; – means to subtract; < means smaller
than; > means greater than.
Figure 8.10 Reference flip book that can
be used in maths
8.4.7 Augmentative and alternative communication strategies
Some form of communication between the teacher and all the learners in
the classroom is an important prerequisite for learning. Some children with
intellectual disability, however, have limited speech abilities, and might use
a variety of augmentative and alternative communication (AAC) strategies.
This could involve the use of graphic symbols (pictures, line drawings or
written words), manual signs (e.g. signs from South African Sign
Language) or speech-generating devices (also known as voice output
devices) (see Table 8.1). Voice output devices very often provide the
impetus for a child with an intellectual disability to learn language and
speech because of their high motivational value.
Table 8.1 Example of different augmentative and alternative communication devices
Low-technology communication book
with PCS™1
Lightwriter SLP 40™2
Gigabyte with E-triloquist software™3
Tobii S32™4
1 Picture Communication Symbols (PCS) is a registered trademark of Mayer Johnson, a
Tobii Dynavox Company of Pittsburgh, PA (www.mayer-johnson.com).
2 The Lightwriter SLP 40 is a product of Toby Churchill Limited of Over Cambridge,
United Kingdom (www.toby-churhill.com).
3 E-triloquist is a product of E-triloquist (www.etriloquist.com).
4 Tobii S32 is a product of Tobii Dynavox Company of Pittsburgh, PA
(www.tobiidynavox.com).
8.5 CONCLUSION
In this chapter we looked at a functional definition of intellectual disability
and highlighted three of the most prominent syndromes associated with it.
Then, with practical examples we demonstrated how careful preparation
can enhance the successful inclusion of learners with intellectual disability.
Aspects such as creating an open, accepting classroom where all learners
feel equally welcome and important were discussed. Implementing dynamic
functional programmes based on each learner’s unique learning style and
specific strengths was explored, and specific examples of this for different
curriculum activities were given.
Recipe for success
Bite off more than you can chew,
then chew it
Plan more than you can do,
then do it
Point your arrow at a star,
take your aim, and there you are
Arrange more time than you can spare,
then spare it
Take on more than you can bear,
then bear it
Plan your castle in the air,
then build a ship to take you there
Anonymous
REFERENCES
Bagni, C., Tassone, F., Neri, G. & Hagerman, R. 2012. Fragile X syndrome: causes, diagnosis,
mechanisms, and therapeutics. The Journal of Clinical Investigation, 122(120): 4314–4322.
Batshaw, M.L., Gropman, A. & Lanpher, B. 2013. Genetics and developmental disabilities. In
Batshaw, M.L., Roizen, N.J. & Lotrecchiano, G.R. (Eds). Children with disabilities, 7th ed.
Baltimore, MD: Paul H. Brookes.
Batshaw, M.L. & Perret Y.M. (Eds). 1992. Children with disabilities: a medical primer, 3rd ed.
Baltimore, MD: Paul H. Brookes.
Beukelman, D.R. & Mirenda, P. 2013. Augmentative and alternative communication. Supporting
children & adults with complex communication needs, 4th ed. Baltimore, MD: Paul H. Brookes.
Bornman, J. 2006. Using a narrative and drawing approach to investigate Grade 1 children’s
depictions of disability. Social Work Practitioner-Researcher, 18(2): 144–164.
Bornman, J. 2015. Accessing justice via key role players: a view from South Africa. In Bryen, D.N.
& Bornman, J. (Eds). Stop violence against people with disabilities! An international resource.
Pretoria University Law Press: Pretoria.
Chudley, A., Conry, J., Cook, J., Loock, C., Rosales, T. & LeBlanc, N. 2005. Fetal alcohol spectrum
disorder: Canadian guidelines for diagnosis. Canadian Medical Association Journal 172(5 suppl).
Available at: http://www.ecmaj.ca/cgi/reprint/172/5_suppl/S1 (accessed on 19 January 2004).
Clarren, S.K. 2005. A thirty-year journey from tragedy to hope. Foreword to Buxton, B. (Ed.).
Damaged angels: an adoptive mother discovers the tragic toll of alcohol in pregnancy. New York:
Carroll & Graf.
Coyne, P., Pisha, B., Dalton, B., Zeph, L.A. & Cook Smith, N. 2012. Literacy by design: a universal
design for learning approach for students with significant intellectual disabilities. Remedial and
Special Education, 33(3): 162–172.
De Graaf, G., Van Hove, G. & Haveman, M. 2014. A qualitative assessment of educational
integration of students with Down syndrome in the Netherlands. Journal of Intellectual Disability
Research, 58(7): 625–636.
Dessemontet, R. & Bless, G. 2013. The impact of including children with intellectual disability in
general education classrooms on the academic achievement of their low-, average-, and highachieving peers. Journal of Intellectual and Developmental Disability, 38(1): 23–30.
Donohue, D.K. & Bornman, J. 2014. The challenges of realizing inclusive education in South Africa.
South African Journal of Education, 34(2): 1–14.
Downing, J.E. & Falvey, M.A. 2015. The importance of teaching communication skills. In Downing,
J.E., Hanreddy, A. & Peckham-Hardin, K.D. Teaching communication skills to students with severe
disabilities, 3rd ed. Baltimore, MD: Paul H. Brookes.
Downing, J.E. & Ryndak, D.L. 2015. Integrated team expertise to support communication. In
Downing, J.E., Hanreddy, A. & Peckham-Hardin, K.D. Teaching communication skills to students
with severe disabilities, 3rd ed. Baltimore, MD: Paul H. Brookes.
Estigarribia, B., Martin, G.E. & Roberts, J.E. 2012. Cognitive, environmental, and linguistic
predictors of syntax in fragile X syndrome and Down syndrome. Journal of Speech, Language, and
Hearing Research (JSLHR), 55(6): 1600–1612. Available at: http://doi.org/10.1044/10924388(2012/10-0153)
Fey, M.E., Yoder, P.J., Warren, S.F. & Bredin-Oja, S.L. 2013. Is more better? Milieu communication
teaching in toddlers with intellectual disabilities. Journal of Speech Language Hearing Research,
5692: 679–693.
Hagerman, R.J., Berry-Kravis, E., Kaufmann, W.E., Ono, M.Y., Tartaglia, N. & Lachiewicz, A. 2009.
Advances in the treatment of fragile X syndrome. Pediatrics, 123(1): 378–390.
Hanreddy, A. 2015. The relationship between communication and literacy. In Downing, J.E.,
Hanreddy, A. & Peckham-Hardin, K.D. Teaching communication skills to students with severe
disabilities, 3rd ed. Baltimore, MD: Paul H. Brookes.
Hersh, J.H. & Saul, R.A. 2011. Health supervision for children with fragile X syndrome. Paediatrics,
127(5): 994–1006.
Hyman, S.L. & Levy, S.E. 2013. Autism spectrum disorders. In Batshaw, M.L., Roizen, N.J. &
Lotrecchiano, G.R. (Eds). Children with disabilities, 7th ed. Baltimore, MD: Paul H. Brookes.
Jones, L., Bellis, M.A., Wood, S., Hughes, K., McCoy, E., Eckley, L., Bates, G., Mikton, C.,
Shakespear, T. & Officer, A. 2012. Prevalence and risk of violence against children with disabilities:
a systematic review and meta-analysis of observational studies. The Lancet. Available at:
http://dx.doi.org/10.1016/s0140-6736(12)60692-8
Kaiser, A.P. & Roberts, M.Y. 2013. Parent implemented enhanced milieu teaching with preschool
children with intellectual disabilities. Journal of Speech, Language, Hearing Research, 56(1): 295–
309.
Kelly, S. & Mian, N. 2016. High levels of foetal alcohol syndrome found in Saldanha Bay.
GroundUp News. 4 April 2016. Available at: http://www.groundup.org.za/
Malbin, D. 2002. Fetal alcohol spectrum disorders: trying differently rather than harder. Portland,
OR: FASCETS.
Mastropieri, M.A. & Scruggs, T.E. 2010. The inclusive classroom: strategies for effective instruction,
4th ed. Upper Saddle River, NJ: Prentice Hall.
May, P.A., Blankenship, J., Marais, A-S., Gossage, J.P., Kalberg, W.O., Barnard, R. et al. 2013.
Approaching the prevalence of the full spectrum of fetal alcohol spectrum disorders in a South
African population-based study. Alcoholism, Clinical and Experimental Research, 37(5): 818–830.
http://doi.org/10.1111/acer.12033
McConkey, R., Kelly, C., Craig, S. & Shevlin, M. 2015. A decade of change in mainstream education
for children with intellectual disabilities in the Republic of Ireland. European Journal of Special
Needs Education, 31(1): 96–110.
McDuffie, A., Kover, S.T., Hagerman, R. & Abbeduto, L. 2013. Investigating word learning in
fragile X syndrome: a fast-mapping study. Journal of Autism and Developmental Disorders, 43(7):
1676–1691. Available at: http://doi.org/10.1007/s10803-012-1717-3
Mukherjee, R.A.S., Hollins, S. & Turk, J. 2006. Fetal alcohol spectrum disorder: an overview.
Journal of the Royal Society of Medicine, 99(6): 298–302.
Mumba, P. 2006. “Be a star”: an innovation in a rural primary classroom of Zambia. Paper
presented at the From Inclusion to Belonging Conference, Nedbank Sandton Auditorium, Sandton.
Muralidharan, P., Sarmah, S., Zhou, F.C. & Marrs, J.A. 2013. Fetal alcohol spectrum disorder
(FASD) associated neural defects: complex mechanisms and potential therapeutic targets. Brain
Science, 3: 964–99. doi:10.3390/brainsci3020964
National Centre on Educational Outcomes. 2014. Accommodations for students with disabilities.
Available at: http://www.cehd.umn.edu/NCEO/TopicAreas/Accommodations/StatesAccomm.htm
Paulson, J. 2013. Environmental toxicants and neurocognitive development. In Batshaw, M.L.,
Roizen, N.J. & Lotrecchiano, G.R. (Eds). Children with Disabilities, 7th ed. Baltimore, MD: Paul H.
Brookes.
Phung, M.H., Wallace, L., Alexander, J. & Phung, J. 2011. Parenting children with fetal alcohol
syndrome disorder (FASD). Public Health, 2(3): WMC001745.
Piek, J.P., Dawson, L., Smith, L.M. & Gasson, N. 2008. The role of early fine and gross motor
development on later motor and cognitive ability. Human movement science, 27(5): 668–681.
Roizen, N.J. 2013. Down syndrome (Trisomy 21). In Batshaw, M.L., Roizen, N.J. & Lotrecchiano,
G.R. (Eds). Children with disabilities, 7th edition. Baltimore, MD: Paul H. Brookes.
Sapon-Shevin, M. 2010. Because we can change the world. A practical guide to building
cooperative, inclusive classroom communities, 2nd ed. Thousand Oaks, CA: Corwin.
Schalock, R.L., Borthwick-Duffy, S.A., Bradley, V.J., Buntinx, W.H., Coulter, D.L., Craig, E.M., &
Shogren, K.A. 2010. Intellectual disability: definition, classification, and systems of supports.
Washington: American Association on Intellectual and Developmental Disabilities, Washington, DC.
Shapiro, B.K. 1992. Normal and abnormal development: mental retardation. In Batshaw, M.L. &
Perret, Y.M. (Eds). Children with disabilities: a medical primer, 3rd ed. Baltimore, MD: Paul H.
Brookes.
Shapiro, B.K. & Batshaw, M.L. 2013. Developmental delay and intellectual disability. In Batshaw,
M.L. Roizen, N.J. & Lotrecchiano, G.R. (Eds). Children with disabilities, 7th ed. Baltimore, MD:
Paul H. Brookes.
Shogren, K.A., Wehmeyer, M.L, Seo, H., Thompson, J.R., Schalock, R.L., Hughes, C. et al. 2016.
Examining the reliability and validity of the supports intensity scale–children’s version in children
with autism and intellectual disability. Focus on autism and other developmental disabilities. First
published on 8 January 2016. doi:10.1177/1088357615625060
South Africa. 1996. The Constitution of the Republic of South Africa, 1996. Pretoria, South Africa:
Government Printer.
South African Inherited Disorders Association. n.d. http://www.saida.org.za/ (accessed on 19 January
2009).
Spies, G.M. 2012. The effect of sexual abuse on a child. In Spies, G.M. (Ed.). Sexual abuse.
Dynamics, assessment and healing. Pretoria: Van Schaik.
Stratton, K.R., Howe, C.J. & Battaglia, F.C. 1996. Fetal alcohol syndrome: diagnosis, epidemiology,
prevention, and treatment. Washington, DC: National Academy Press.
Tharpe, A.M. 2009. Individuals with multiple disabilities. In Katz, J., Medwetsky, L., Burkard, R. &
Hood, L. (Eds). Handbook of Clinical Audiology, 6th ed. Philadelphia: Thieme Medical Publishers.
Thompson, J.R., Bryant, B.R., Campbell, E.M., Craig, E.P.M., Hughes, C.M. et al. 2004. Supports
intensity scale. Washington, DC: American Association on Intellectual and Developmental
Disabilities.
UN General Assembly, Convention on the Rights of the Child, 20 November 1989. United Nations
Treaty Series, 1577: 3. Available at: http://www.refworld.org/docid/3ae6b38f0.html (accessed on 22
April 2016).
UN General Assembly, 24 January 2007. Convention on the Rights of Persons with Disabilities.
Resolution adopted by the General Assembly, A/RES/61/106. Available at:
http://www.refworld.org/docid/45f973632.html (accessed on 22 April 2016).
Westendorp, M., Hartman, E., Houwen, S., Smith, J. & Visscher, C. 2011. The relationship between
gross motor skills and academic achievement in children with learning disabilities. Research in
developmental disabilities, 32(6): 2773–2779.
Westling, D.L. & Fox, L. 2009. Teaching students with severe disabilities, 4th ed. Upper Saddle
River, NJ: Pearson.
World Health Organization. 2007. ICF-CY, International Classification of Functioning, Disability,
and Health: Children & Youth version. Geneva: World Health Organization.
9
Understanding children with
learning disabilities
9.1 INTRODUCTION
Learning disability is one of those areas where the Pinocchio principle is
often followed; in other words the problem is allowed to get bigger and
bigger. Many teachers (and parents) might have a feeling that there is a
problem early on, yet they decide to wait before seeking help. Later, when
they realise that time is of the essence in developing skills, they regret the
lost months or years. Teachers are often the first to make a referral for
assessment for learning disabilities, because the structured school
environment and the nature of learning activities required at school points
to difficulties that may have been overlooked at home. If teachers (or
parents) suspect a learning problem, they should be encouraged to get help
immediately and start addressing it. Learning difficulties do not disappear
spontaneously, therefore waiting to see if the child will outgrow a learning
disability is never an option.
In the previous chapter, children who experience problems with learning
and thinking as a result of intellectual disability were described, but in this
chapter the broader term learning disability is explored. This refers to
difficulties in one or more of the basic processes involved in understanding
spoken or written language. It may present as a problem in listening,
thinking, speaking, reading, writing, spelling or in maths, despite average or
above-average intelligence (Chu & Flores, 2011). Learning disability is thus
not a specific term, but rather a category that contains many specific
disabilities, all of which make learning difficult. However, it does not
include learning problems resulting from visual, hearing, physical or
intellectual impairment; emotional disturbance; or environmental, cultural
or economic disadvantages. However, some self-advocacy groups are not in
favour of this term as they maintain that it suggests the inability to do
something and hence they prefer learning difficulties, which they suggest
implies that the individual wants to learn and can be taught (Maestri-Banks,
2013). As this terminology is still evolving, the term learning disability will
be used in this chapter.
Some of the most frequently seen forms of learning disability are attention
deficit hyperactivity disorder (ADHD), dyslexia (reading disability),
dyscalculia (maths disability), dysgraphia (writing disability) and dyspraxia
(planning disability) (see Figure 9.1). In this chapter, all of these types of
learning disability will briefly be described, but the emphasis is on
strategies that can be implemented in the classroom to accommodate these
learners optimally. If teachers are not intentional about including these
learners in their classrooms, they are in actual fact excluding them.
Figure 9.1 Types of learning disability briefly
covered in this chapter
9.2 TYPES OF LEARNING DISABILITY
The following types of learning disability are described:
9.2.1 Attention deficit hyperactivity disorder
ADD is the abbreviation for attention deficit disorder, and ADHD for
attention deficit hyperactivity disorder. The current international trend,
however, is that the ADD label has become redundant and that ADHD is
the preferred referential term, incorporating ADD.
9.2.1.1 What is ADHD?
The Diagnostic and statistical manual of mental disorders – 5 (DSM-5)
(APA, 2013) defines ADHD as a persistent pattern of inattention and/or
hyperactivity-impulsivity that interferes with functioning or development,
has symptoms presenting in two or more settings (e.g. at home, at school,
with friends or with family), and negatively impacts on social or academic
functioning. Several symptoms must have been present before the age of 12
years. There are three types of ADHD, as shown in Table 9.1.
Table 9.1 Three types of ADHD presentation
Type
Characteristics
Predominantly
inattentive
type
Diagnosed if six or more symptoms of inattention (but less than six
symptoms of hyperactivity/impulsivity) have persisted for six months or
more.
Nine inattention symptoms:
Makes careless mistakes in schoolwork, or in other activities (e.g.
overlooks or misses details, work is inaccurate).
Has difficulty in sustaining attention in tasks (e.g. has difficulty in
focusing during lessons or reading long passages).
Does not seem to listen when spoken to directly (e.g. day dreams,
mind seems elsewhere).
Has difficulty in following through on instructions and finishing school
work (e.g. starts tasks but easily side-tracked).
Has difficulty in organising tasks (e.g. disorganised work; has poor
time management; fails to meet deadlines).
Avoids tasks that require sustained mental effort (e.g. schoolwork or
homework).
Loses things necessary for tasks or activities (e.g. pencils, books,
tools, wallets, keys, paperwork).
Is distracted by external stimuli.
Is forgetful in daily activities.
Type
Characteristics
Predominantly
hyperactiveimpulsive type
Diagnosed if six or more symptoms of hyperactivity/impulsivity (but less
than six or more symptoms of inattention) have been present for six
months or more.
Nine hyperactivity-impulsivity symptoms
Fidgets with fingers, taps hands or squirms in seat.
Gets up when expected to remain seated.
Runs around or climbs in situations where this is inappropriate.
Is unable to play or participate quietly in leisure activities.
Appears “on the go” or as if charged by a battery (e.g. experienced by
others as restless or difficult to keep up with).
Talks excessively.
Calls out answers before questions have been completed.
Has difficulty waiting for a turn (e.g. while in a queue).
Interrupts others (e.g. in conversations, games or activities).
Combined
type
All three core features are present. ADHD is diagnosed when six or
more symptoms of hyperactivity/impulsivity, and six or more symptoms
of inattention have been observed for six months or more. This is the
most common type.
From Table 9.1 it is thus clear that ADHD describes children or adolescents
who have difficulty focusing and maintaining attention in academic and/or
social situations. As such, this impacts on academic performance and leads
to social skills difficulties as well as strained parent–child interactions
(Harpin, 2005). A child is sometimes labelled as having ADHD if he has
high energy levels and tends to be disruptive in the classroom, or
conversely, if he sits quietly at his desk staring out the window or doodling.
A child who is chronically disorganised; who brings the wrong books home
or takes the wrong books to school; who has difficulty in remembering (e.g.
sometimes forgets to complete assignments while at other times works hard
on an assignment and then forgets to take it to school on the due date); who
constantly loses things; who works too quickly on assignments (leading to
simple mistakes that bring down his marks); and who waits until the last
minute to complete homework, might have ADHD.
In a South African study that focused on teachers’ perceptions regarding the
inclusion of learners with ADHD in this age cohort, it was found that
teachers who had taught more learners with special needs had a more
positive attitude toward the classroom interaction of learners with ADHD
because they had a greater understanding for the needs of such learners
(Bornman & Donohue, 2013).
Older learners with ADHD often have difficulty with time management, for
example knowing how to break down a long assignment into smaller steps
or how to study for a test that covers multiple units of instruction. One often
finds, therefore, that these learners do not have sufficient time to complete
tests or exams. Adolescents are also often unwilling to accept that they need
help to perform scholastically and therefore immerse themselves in social
activities or computer gaming, or may even use drugs or alcohol to avoid
facing their educational difficulties (Brown, 2016).
It is also important that while many individuals find that their ADHD
impairments becomes less problematic as they age (due to brain maturation
or changing environmental demands), there are many for whom this
impairment persists into the adult years (Brown, 2013; Walker, Venter, Van
der Walt & Esterhuysen, 2011).
Although the prevalence rate of ADHD has not yet been determined
officially in South Africa, it is estimated that 10 per cent of South African
schoolchildren experience ADHD symptoms (Perold, Louw & Kleynhans,
2010). This means that in a class of 30 learners, the teacher can expect three
with ADHD.
9.2.1.2 What causes ADHD?
Parents may ask the teacher, “What went wrong? What did I do?” While no
one really knows what causes ADHD, professionals in the medical and
scientific fields generally agree that there is no single cause of ADHD, but
that it is influenced by multiple genes, non-inherited factors and their
interplay (Thapar, Cooper, Jefferies & Stergiakouli, 2012). However,
exposure to a risk factor does not necessarily result in ADHD. Current
research into the causes of ADHD is investigating the role of the following:
Genes. Studies of twins show that ADHD often runs in families, and
researchers are trying to find out whether there are specific genes that put
children at higher risk of developing ADHD (Khan & Faraone, 2005).
Environmental factors. Studies suggest a potential link between cigarette
smoking, alcohol and drug use during pregnancy and ADHD in children
(Mick, Biederman, Faraone, Sayer & Kleinman, 2002; Thapar et al.,
2012). Nutrition, anxiety and stress during pregnancy as well as
infections may also play a role (Thapar et al., 2012). Research has also
shown that there is a link between extreme prematurity, very low birth
weight and ADHD (Thapar et al., 2012). Furthermore, new research is
showing that pre-schoolers who are exposed to high levels of lead (which
can sometimes be found in the plumbing systems or paint in old
buildings), may be at a higher risk (Braun, Kahn, Froehlich, Auinger &
Lanphear, 2006).
Artificial colourants and preservatives. Recent research indicates a
possible link between food containing artificial colourants or
preservatives, and an increase in ADHD (McCann et al., 2007).
Refined sugar. Despite research evidence that proves the contrary, there is
still a popular belief that refined sugar causes ADHD or makes symptoms
worse. In one study, for example, researchers gave one group of children
foods containing sugar and another group sugar substitutes. No
differences were reported between the two groups (Wolraich, Milich,
Stumbo & Schultz, 1985).
9.2.1.3 Characteristics of ADHD
In order to make the correct diagnosis, a consultation with a medical doctor
and appropriate therapist(s) is recommended. This will rule out other
problems that may cause similar behaviours, such as
allergies and asthma (breathing difficulties can interrupt concentration)
diabetes (the quantity of sugar in the blood can cause changes in
concentration and activity levels)
hearing or visual problems (these sensory problems can lead to
behavioural outbursts, difficulties with school, disturbing of classmates
and hyperactivity)
iron deficiency (which can lead to attention and impulsivity problems)
lead intoxication (which could be associated with hyperactivity)
emotional difficulties (which could be, for example, due to a divorce,
death in the family or an accident that could manifest with hyperactivity
symptoms).
An ADHD diagnosis is not an “all-or-nothing” diagnosis – like being
pregnant – which has no in-between (Brown, 2016). One of the puzzling
features of ADHD is how the symptoms vary in certain situations. Most
persons with ADHD can focus their attention very well on a few activities
that have strong personal preference or if they want to prevent an
unpleasant outcome, which is why the common myth exists that it is related
to willpower (Brown, 2013; 2016). If an ADHD diagnosis is made, it will
ensure that the child can be supported and treated appropriately. A
diagnosis will usually only be made from the age of five to seven years,
although some of the symptoms usually appear earlier. It is important that
the symptoms are present for a period of more than six months in all
contexts before a diagnosis is made.
Children with ADHD face a difficult but not impossible future. In order to
achieve their full potential, they should receive help, guidance and
understanding from parents, teachers and peers. Research has shown that
the most effective treatment for ADHD is a combination of an appropriate
diet, medication, remedial education, therapy and/or counselling to learn
coping skills and adaptive behaviours, as well as classroom
accommodations (Reid, 2005). Dr Brown (2013), a leading researcher in
ADHD, explains that medication for ADHD is not a cure – it does not work
like an antibiotic that can cure an infection. Rather, it is like wearing
glasses, which cannot fix problems with vision because when they are
removed, the eye problem is still present, but the person’s functioning may
improve and even normalise when the glasses are worn (Brown, 2013).
Likewise, medication is powerful, and works for between two and 12 hours.
However, each child is different, and each family will have to work out,
very often through trial and error, what works best for them and their child.
9.2.1.4 Strengths: resilience factors
An ADHD diagnosis is not a life sentence as there are many positive
aspects to managing this condition. When properly treated, people with
ADHD can lead fulfilling, happy lives. People with ADHD are often
imaginative, talented, creative, lateral thinkers, and have boundless energy!
9.2.2 Dyslexia
9.2.2.1 What is dyslexia?
The word dyslexia is a combination of two word parts: dys (meaning “not”
or “difficult”) and lexia (meaning “words”, “reading” or “language”, so
quite literally, dyslexia means difficulty with words (Hudson, High &
Otaiba, 2007). Dyslexia is a term that has been loosely applied to people
across the intellectual ability range who have a learning difficulty that
primarily affects the skills involved in accurate and fluent reading and
spelling, despite exposure to adequate instruction (Rose, 2009; Shaywitz,
2005). The definition preferred by the International Dyslexia Association
(n.d.) reads as follows:
Dyslexia is a neurologically-based, often familial, disorder, which
interferes with the acquisition and processing of language.
Varying in degrees of severity, it is manifested by difficulties in
receptive and expressive language, including phonological
processing in reading, writing, spelling, handwriting, and
sometimes in math. Dyslexia is not the result of lack of
motivation, sensory impairment, inadequate instructional or
environmental opportunities, or other limiting conditions, but may
occur together with these conditions. Although dyslexia is
lifelong, individuals with dyslexia frequently respond
successfully to timely and appropriate intervention.
This is quite a mouthful, but if a teacher were required to explain to parents
what dyslexia is in simple terms, she could say something like: “Dyslexia
may run in families because there are genetic, environmental and other
factors involved. Dyslexia makes it extremely difficult to read, write, and
spell in your first language – despite having at least average intelligence.”
The term dyslexia comes from the ophthalmology field, and was first
described in Germany by Dr Rudolf Berlin in the 1800s. He described a
young boy who had a severe difficulty in learning to read and write in spite
of showing typical intellectual and physical abilities (International Dyslexia
Association, n.d.). This was followed in Great Britain by the work of Dr
James Hinshelwood, who published a series of papers in medical journals
describing similar cases, which culminated in his landmark book
Congenital word blindness. He described letter reversals and difficulties
with spelling and reading comprehension, which he attributed to impaired
visual memory for words and letters (Hinshelwood, 1917). Thereafter, the
dyslexia field revolved around theories that believed that the condition was
caused by the failure to establish dominance in either the left or the right
hemisphere in the brain (Orton, 1928). Dr Orton then started working with
psychologist and teacher Anna Gillingham to develop an educational
intervention plan, which became the first multisensory integration
programme, also known as the Orton–Gillingham approach. This approach
is still widely used and forms the basis of many current reading intervention
programmes (Ritchey & Goeke, 2006).
In the 1970s, a new hypothesis, based in part on Orton’s theories, stated that
dyslexia was the result of difficulty in recognising that spoken words are
formed by discrete phonemes (e.g. the word “cat” comes from the sounds
{k}, {æ} and {t}). Persons with dyslexia have difficulty associating these
sounds with the visual letters that make up written words. Hence studies
reported that phonological awareness is the strongest predictor of reading
success in school-age children, and phonological awareness instruction can
improve decoding skills for children with reading difficulties (Alexander,
Anderson, Heilman, Voeller & Torgesen, 1991).
Currently, researchers are trying to find a link between the neurological and
genetic findings on the one hand and the reading disorder on the other.
There are many theories surrounding the causes of dyslexia, but the one that
has the most support from research is that, whatever the biological cause,
dyslexia is a matter of reduced phonological awareness, and a lack of ability
to analyse and link the units of spoken and written language (Lyytinen,
Erskine, Aro & Richardson, 2007).
9.2.2.2 What causes dyslexia?
This is a question that has generated much discussion (and clashes) between
researchers in this field. However, there seem to be signs of a genetic basis,
with chromosomes 6 and 15 being implicated, as dyslexia tends to run in
families (Siegel, 2006), but one should remember that families share genes
as well as environments, making it difficult to disentangle the genetic and
environmental contributions towards dyslexia (Rose, 2009). The following
competing theories have emerged, aimed at identifying the underlying
causes. It is beyond the scope of this book to describe them in depth, but as
it is important for teachers to understand them in case parents ask them
what they think caused their child’s problem, they are mentioned briefly:
THE PHONOLOGICAL DEFICIT HYPOTHESIS
This has been the most influential theory over the past 30 years and refers
to a child’s lack of ability to process phonemes (sounds within words) at the
cognitive level, despite normal hearing (Mortimore & Dupree, 2008).
Children with normal hearing may therefore experience difficulty when
required to identify, sequence or reproduce sounds within a word, which
affects learning to read by phonic methods. It has been suggested that
phonological difficulties emerge from abnormalities in the language area of
the brain.
THE MAGNOCELLULAR THEORY
Research carried out in the 1980s and early 1990s seems to indicate that
visual impairments might play a role in dyslexia, as there might be a
sensory deficit in the large nerve cells in the eye, which are known as the
magnocells (Mortimore & Dupree, 2008). These cells occur in the pathways
between the retina (in the eye) and the visual cortex (in the brain), and are
responsible for carrying information about rapid movement or changes in
the environment. Any impairment in this function will cause images to be
unstable (which makes it difficult to decipher letters or symbols), and text
to be blurred when scanning from left to right, as well as eyestrain,
headaches and a reduced ability to concentrate on printed material.
Stop and reflect
If you were on a speeding train, for example, you would be able to see a sign with a
station name written on it, but you would be unable to read the text on the sign
because the signals from magnocells to the visual cortex would be distorted in other
words the text will not be slowed down enough for you to be able to see it.
The magnocellular theory states that the magnocellular dysfunction is not
restricted to the visual pathways, but is generalised to all modalities (visual
and auditory, as well as tactile). Although this theory highlighted the need
for including visual processing skills in addition to phonological skills in
reading support programmes, it did not challenge the phonological deficit
theory significantly (Franck et al., 2003).
CEREBELLAR THEORY
Another view is represented by the automaticity/cerebellar theory of
dyslexia. The cerebellum is situated at the back of the brain and is
responsible for three main functions: balance; motor control, which
includes speech articulation; and automaticity (mastering a skill at such a
level that one does not have to think about it, e.g. driving a car, typing and
reading). A weak capacity to automatise would affect, among other things,
the learning of grapheme-to-phoneme correspondences (Franck et al.,
2003). Support for this theory comes from evidence that people with
dyslexia perform poorly in a large number of motor tasks, which includes
their difficulty in making skills automatic.
OTHER THEORIES
There are also a number of other, less frequently used hypotheses, which
are mostly variations of the main theories. These include the following:
Rapid auditory processing hypothesis. This is similar to the phonological
deficit hypothesis, and states that the primary deficit lies in the
perception of short sounds.
Visual hypothesis. This is based on the magnocellular hypothesis, and
states that a visual impairment is the reason why difficulties with the
processing of letters and words on a page of text exist.
Perceptual visual-noise exclusion hypothesis. This is an emerging
hypothesis, which postulates that dyslexic symptoms arise because of a
person’s impaired ability to filter out visual and auditory distractions, and
to distinguish between important and irrelevant sensory data (Sperling,
Lu, Manis & Seidenberg, 2005).
The double deficit hypothesis. The first deficit has to do with
phonological impairments and the second with naming speed in other
words how quickly you are able to name certain concepts.
So then which theory is correct? Maybe it will serve us well to remember
the Hindu story about an elephant and four blindfolded people. After
feeling parts of the elephant, the one blindfolded man touched the
elephant’s tail and described it as a stringy rope, the one touched its side
and described it as a high wall, and the one at the trunk thought it was a
hose. Another one put his arms around one leg of the elephant and
described it as a tree trunk. Each man was right about the part he touched,
but also wrong because he did not see the whole picture. Only when the
blindfolds were removed did they discover the truth (Keith, 2001). At this
point, it would probably be safe to say that the causes of dyslexia are not
yet clearly understood and that some or all of these theories hold part of the
truth.
9.2.2.3 Characteristics of dyslexia
Dyslexia can be seen as a pattern of differences in learning and is reflected
in all learners, although individual profiles will be unique (Mortimore &
Dupree, 2008). Learners will thus not necessarily display all of these
characteristics, but any combination of characteristics is possible.
Furthermore, the signs of dyslexia will vary, depending on the child’s
developmental age. However, it is often unexpected in relation to the child’s
other cognitive abilities (Handler & Fierson, 2011). In the pre-school years,
teachers might be aware of delayed or problematic speech and language,
poor rhyming skills and little interest or difficulty in learning letters. In the
early school years, poor letter–sound knowledge, poor phoneme awareness,
poor word-attack skills, problems with copying letters or words, and
idiosyncratic spelling is typical (Rose, 2009). In the intermediate phase,
slow reading, poor decoding skills when faced with new words as well as
poor spelling are seen. In the senior phase, dyslexia typically presents with
poor reading fluency, slow writing speed, and poor organisation and
expression in written work. All of the characteristics listed below will
impact negatively on learning in the classroom.
LITERACY SKILLS: READING AND SPELLING
Difficulty in learning the letters of the alphabet
Difficulty with spelling. Words are often misspelt, or vowels are left out,
due to difficulty in learning letter–sound correspondences (phonemic
awareness). Difficulty in mapping sounds (phonemes) onto letter
symbols (graphemes) exist, which results in many spelling errors.
Learners with dyslexia will have difficulty in doing the following tasks:
– Phoneme segmentation. What sounds do you hear in the word “hat”?
What is the last sound in the word “nap”?
– Phoneme deletion. What word would be left if the [f] sound were taken
away from “fat”?
– Phoneme matching. Do “pen” and “pipe” start with the same sound?
– Phoneme counting. How many sounds do you hear in the word
“lake”?
– Phoneme substitution. What word would you have if you changed the
[h] in “hot” to [p]?
– Blending. What word would you have if you put these sounds together?
[s] [a] [t]
– Rhyming. Tell me as many words as you can that rhyme with the word
“eat”.
Difficulty with taking notes
Losing their place when reading
Difficulty in learning everyday sequences, for example the days of the
week, months of the year and multiplication tables
Reversing the letter order, especially when the final incorrect word looks
similar to the intended word (e.g. spelling “cicurs” instead of “circus”, or
“was” instead of “saw”)
Spelling words in a highly phonetic form, for example “qwikli” for
“quickly”
Difficulty in distinguishing among homophones, for example “to”, “too”
and “two”
Restricted written vocabulary, even if they have a large oral vocabulary
Poor literacy skills in subjects such as maths, and possible difficulty with
story sums (e.g. descriptive mathematics, technology or natural science
problems that rely on written text rather than numbers or formulas)
BEHAVIOUR
Poor attention span and high distractibility
Embarrassed by apparent difficulties, which could lead to some children
becoming shy and withdrawn from their peers or some becoming bullies
because of their inability to understand the social cues in their
environment (Peer, 2009)
Denying difficulties and therefore rejecting help
Appearing depressed
Showing signs of frustration and feeling ashamed, which might lead to
lower motivation as they see how their peers seem to master reading
skills without much effort (Handler & Fierson, 2011)
Acting like the class clown
Becoming uncharacteristically aggressive and angry
Complaining of headaches and itchy eyes when reading
Difficulty with the concept of time and keeping time, and needing extra
time to complete tasks
Difficulty in doing more than one thing at a time (multitasking)
Developing a school phobia and trying to avoid going (Siegel, 2006)
SPEECH, HEARING AND LISTENING
Speech delays may be an early warning sign of dyslexia.
Many individuals with dyslexia also have problems with speaking
clearly. They can mix up sounds in multisyllabic words (e.g. “aminal” for
animal, “bisghetti” for spaghetti, “hekalopter” for helicopter,
“vegtabumble” for vegetable, “hangaberg” for hamburger).
They may also have problems speaking in full sentences, and might have
immature speech (Wilcox, n.d.).
They may have difficulty with word retrieval or naming problems, as
well as a confusion with before/after, right/left, and so on.
There may be difficulty in associating words with their correct meanings.
Auditory discrimination problems (e.g. difficulty distinguishing different
sounds in words may occur.
There may be auditory processing problems, for example difficulty in
sounding out letters, identifying or generating rhyming words, or
counting syllables in words (phonological awareness). In some cases, this
might be attributed to chronic otitis media (middle-ear infection).
ORGANISATIONAL AND MOTOR SKILLS (INCLUDING WRITING)
Working too fast or too slowly
Untidy and illegible writing with poorly formed, reversed or incorrectly
sized letters or words
Difficulty in keeping within the lines when writing or colouring
Difficulty in structuring written work (e.g. knowing where to start, what
follows next)
Difficulty in copying from the board or textbook
Losing track of the aim and/or purpose of the task
Little idea of time or the structure of the daily timetable
Difficulty in following instructions/directions, which results in frequently
getting lost or being late
Difficulty with gross/fine motor tasks, which may result in clumsiness
and poor coordination
It is a misconception that children with dyslexia reverse letters or words
when they write reversals. Reversing letters or words and mirror writing
typically occur in early writers (Handler & Fierson, 2011).
MEMORY
Difficulty in remembering sets of instructions
Difficulty in remembering sequences
Difficulty in remembering rules and patterns
Constantly forgetting pens, pencils, sports clothes, letters that have to be
taken home, arrangements, and so on (this might also be attributable to
lack of organisational skills)
Short-term memory difficulties
Difficulty with any type of rote learning
Difficulty with remembering mathematical facts, such as multiplication
tables, learning the sequence of steps when performing calculations such
as long division, and other mathematics that involves remembering the
order in which numbers appear
9.2.2.4 Strengths: resilience factors
People with dyslexia often have significant strengths in areas controlled by
the right side of the brain. It is important to recognise these strengths and to
boost the individual’s self-esteem. They may include a natural flair for one
or more of the arts such as music, dance, drawing or acting; athletic talent; a
knack for mechanics; 3-D visualisation ability; creative problem-solving
skills; and intuitive people skills. In order to compensate for their
difficulties, children with dyslexia may also have very well-developed
observation skills (looking for cues in pictures or illustrations), listening
skills (paying attention to what the teacher says or what other children are
reading out loud) and memory skills (remembering details of what they
hear) (Shaywitz, 2005).
A study has found that entrepreneurs are five times more likely to have
dyslexia than average citizens (Cass Business School, 2004). Researchers
theorise that such entrepreneurs attain success by delegating responsibilities
and excelling at verbal communication (Bowers, 2007).
Furthermore, high-quality intervention, strong oral language skills, the
ability to maintain attention as well as good family support have been
shown to be protective influences that ultimately lead to better outcomes for
such children (Rose, 2009).
Children might identify with the following role models who had dyslexia:
Albert Einstein, Napoleon, Julius Caesar, Leonardo da Vinci, Walt Disney,
Whoopi Goldberg, Pablo Picasso, Tom Cruise, Mark Twain, Vincent van
Gogh, Robin Williams, Winston Churchill, Michelangelo, Franklin D.
Roosevelt and Richard Branson to name but a few.
Stop and reflect
This is Richard Branson’s story. Richard didn’t breeze through school. It wasn’t
just a challenge for him; it was a nightmare. His dyslexia embarrassed him as he had
to memorise and recite word for word in public. He was sure he did terribly on the
standard IQ tests. These are tests that measure abilities where he is weak. In the
end, it was the tests that failed. They totally missed his ability and passion for sports.
They had no means to identify ambition, the fire inside that drives people to find a
path to success that zigzags around the maze of standard doors that won’t open.
They never identified the most important talent of all: the ability to connect with
people, mind to mind, soul to soul. It’s that rare power to energise the ambitions of
others so that they, too, rise to the level of their dreams.
Source: Retrieved from http://www.johnshepler.com
9.2.3 Dyscalculia
9.2.3.1 What is dyscalculia?
The word dyscalculia comes from Greek and Latin and means “counting
badly”. A distinction should be made between primary dyscalculia (which
is the focus of this chapter) and secondary dyscalculia. Primary dyscalculia
refers to mathematical problems that stem from an impaired ability to
acquire mathematical skills (Price & Ansari, 2013). In contrast, secondary
dyscalculia (pseudo dyscalculia) stems from factors such as poor teaching,
low socioeconomic status, and other developmental disorders – all aspects
that have a known impact on mathematical ability.
Primary dyscalculia describes the essence of the impairment, namely a
neurological condition that affects the ability to acquire mathematical skills.
In other words, it is like dyslexia for numbers. It is not uncommon for
children with dyslexia to also experience difficulties with numbers (Rose,
2009). Learners with dyscalculia may have difficulty in understanding
simple number concepts or calculation symbols (i.e. addition, subtraction,
division and multiplication symbols), confuse similar-looking numbers (e.g.
6 and 9; 3 and 8), lack an intuitive grasp of numbers, and have problems
learning number facts and mathematical procedures (Henderson, Came &
Brough, 2003). Particular difficulties are seen when they have to read
numbers that contain more than one digit, and numbers that contain a zero
(e.g. 1 007 or 1 087), or when they have to write “one thousand and three”,
the zero is lost and they write 103 (Prinsloo, 2008). Furthermore, they
might be confused when reading some numbers (e.g. 12 becomes 21),
although at times they might experience no difficulty with this. They have
problems with copying numbers, recalling numbers, calculating numbers
and writing mathematical symbols (i.e. they find it difficult to remember
how to write a + sign). Even if they are able to produce a correct answer or
use a correct method, they may do so mechanically and without confidence.
In addition, learners with dyscalculia will experience problems with
understanding the concepts of weight, space, direction and time, as all of
these use numbers (Prinsloo, 2008). Reading maps, tables or other diagrams
is extremely confusing. Problems can also arise when understanding the
relationship between units of measurement (e.g. changing centimetres to
metres, or kilograms to grams), as well as arranging numbers by size (e.g.
16 comes before 17, 74 is five more than 69).
9.2.3.2 What causes dyscalculia?
Dyscalculia is caused by the dysfunction of mathematical processes and
areas in the brain. Studies are showing brain impairment in areas of the
brain known to process mathematics (specific parts of the parietal lobes)
(Landerl, Bevan & Butterworth, 2004). However, the functioning and
structure of the brain reflect not only one’s genes, but also one’s
environment, and the interaction between the two. Children with a very low
birth weight, and born of mothers who consumed excessive amounts of
alcohol during pregnancy are also at higher risk for dyscalculia (Grafman &
Romero, 2001). Although it would thus appear as if dyscalculia has
multifactorial causes, it is important to realise that research establishing this
is still in its infancy.
9.2.3.3 Characteristics of dyscalculia
Our understanding of dyscalculia is way behind that of dyslexia. As yet
there are no standardised tests available, but some initial screening tests
have been published. As was the case with dyslexia 20 to 30 years ago,
teachers still have to work on a principle of exclusion, which means that if a
learner has an average or above-average cognitive ability without problems
with literacy or other general subjects, and all other reasons for failure to
achieve in the classroom are excluded, but he is unable to understand the
maths that his peers cope with easily, he might have dyscalculia.
Many other reasons apart from dyscalculia could lead to problems with
maths and therefore care must be taken before this diagnosis is made. The
main difference between learners with dyscalculia and those who have
difficulty as a result of other factors is their lack of any intuitive grasp of
number and numerical relationships.
Some of the most common symptoms of dyscalculia include difficulty in
the following:
Counting, which may be delayed (Rousselle & Noel, 2007)
Classifying mathematical signs (addition, minus, multiplication and
division)
Reading an analogue clock and telling the time (Orfano, 2012)
Calculating basic amounts, such as adding up a bill
Learning multiplication tables (Orfano, 2012)
Using a calculator
Reading a personal schedule (Orfano, 2012)
Learning and remembering mathematical rules and formulas (Rousselle
& Noel, 2007)
Keeping records
Playing games that involve numbers
Number sense – there may be a fundamental difficulty in understanding
quantity (Rousselle & Noel, 2007)
9.2.3.4 Strengths: resilience factors
Like people with dyslexia, people with dyscalculia may be gifted in many
other spheres. This is possibly due to the fact that they have developed
talents in areas other than mathematics. It is almost as if their brains
“rewire” themselves to cope with the missing part. It could be that they
solve problems a little differently and think outside the box. Many wellknown people have dyscalculia, like the singer, Cher, and Sir David
Attenborough, the famous environmentalist.
9.2.4 Dysgraphia
9.2.4.1 What is dysgraphia?
The term dysgraphia comes from the Greek words dys (which means “not”
or “impaired”) and graphia (meaning “making letters by hand”). The DSM5 does not use the term dysgraphia but rather refers to it as an impairment in
written expression (APA, 2013). This is a disorder that expresses itself
primarily during writing or typing. However, in some cases it may also
affect eye–hand coordination and is noticeable when the child is trying to
perform activities that require specific sequences, such as tying knots or
carrying out a repetitive task. Dysgraphia is different from dyspraxia in that
the child may have the word to be written or the proper order of steps
clearly in mind, but carries the sequence out in the wrong order.
9.2.4.2 What causes dysgraphia?
Not much research has been done in the field of dysgraphia. Its cause is
unknown in children, but scientists believe that there are multiple
contributing factors. A genetic component might be possible, as there seems
to be a tendency for more than one person per family to be affected. When
it occurs in an adult, it is usually caused by brain damage due to head
injury, stroke or other neurological condition.
9.2.4.3 Characteristics of dysgraphia
The symptoms of dysgraphia fall into six categories: visual-spatial, fine
motor, language processing, spelling/handwriting, grammar, and
organisation of language (Martins et al., 2013; Rostami, Allahverdi &
Mousavi, 2014). If a child’s writing skills are behind that of his peers, and
some of these symptoms occur, dysgraphia may be present.
VISUAL-SPATIAL DIFFICULTIES
Difficulty with shape discrimination and letter spacing
Difficulty organising words on the page from left to right
Writing letters that go in all directions, and letters and words that run
together on the page
Difficulty in writing on a line and staying inside the margins
Difficulty reading maps, drawing or reproducing a shape
Difficulty in copying text – this task is slow or laboured
FINE MOTOR DIFFICULTIES
Difficulty in holding a pencil correctly, tracing, cutting food, tying shoes,
doing puzzles, working on a computer keyboard
Difficulty in using scissors and colouring inside the lines
Holding wrist, arm, body or paper in an awkward position when writing
as well as a cramped hand or unusual grip, which may lead to complaints
of a sore hand
LANGUAGE-PROCESSING DIFFICULTIES
Difficulty in writing ideas down on paper quickly
Difficulty in understanding the rules of games
Difficulty in following directions
SPELLING ISSUES/HANDWRITING ISSUES
Difficulty understanding spelling rules
Difficulty in telling if a word is misspelled
Making spelling errors in writing but not orally
Spelling words incorrectly and in many different ways
Difficulty using spell-check because of an inability to recognise the
correct word
Showing inconsistencies when writing, for example mixing printing and
cursive writing, mixing upper and lower case, or writing with irregular
sizes, shapes or slant of letters
Difficulty in reading own writing
Avoiding writing
Getting a tired or cramped handed when writing
Erasing a lot
GRAMMAR AND USAGE PROBLEMS
Does not know how to use punctuation, so either uses no punctuation, or
random punctuation, despite appropriate instruction and sufficient time
Overuses commas and mixes up verb tenses
Does not start sentences with a capital letter
Writes in list format – not complete sentences – or writes extremely long
sentences
ORGANISATION OF WRITTEN LANGUAGE
Shows great difficulty when having to think and write at the same time,
for example when taking notes or in creative writing
Has difficulty in telling a story and may start in the middle
Leaves out important facts and details, or provides too much information
Assumes others know what he is talking about
Uses vague descriptions and writes jumbled sentences
Never gets to the point, or makes the same one over and over
Is better at conveying ideas when speaking
9.2.4.4 Strengths: resilience factors
In recent years, technological advances have transformed the written
landscape. Learners no longer have to rely only on handwriting to produce
written output, but can make use of computers and other aids that can assist
with organising information and checking spelling.
9.2.5 Dyspraxia
9.2.5.1 What is dyspraxia?
The term dyspraxia comes from the words dys (which means “no” or
“impaired”) and praxis (which means “doing something”). The DSM-5
prefers to use the term developmental coordination disorder (DCD). It is
also a neurological condition (like dyscalculia) and affects the planning of
what to do and how to do it. It is associated with problems with perception,
language, short-term memory and organisation, and hence interferes
significantly with academic achievement or activities of daily living (Dixon
& Addy, 2004). Furthermore, these learners have a marked difficulty in
carrying out routine tasks involving balance, fine-motor control and
kinaesthetic coordination, and their movement is often slow or tentative
because they have to rely more on visual information than on
proprioceptive information. These learners tend to fail to anticipate, and to
utilise perceptual information or to benefit from cues. For example, when
catching a ball, one sees it coming and has to open one’s arms wide enough
to accommodate its size.
9.2.5.2 What causes dyspraxia?
Very little is known about dyspraxia and for the majority of children who
are diagnosed with it the cause is unknown. However, current research
seems to suggest that it might be a result of an immaturity of the
development of motor neurones in the brain (the nerve cells that control
muscles) rather than brain damage. In other words, if these motor neurons
fail to develop adequate connections, it means that the brain takes longer to
process information (Dyspraxia Foundation, 2009). There also seem to be
some genetic factors involved, and preterm birth and stressful birth
circumstances are also linked to dyspraxia.
9.2.5.3 Characteristics of dyspraxia
Dyspraxia changes as children grow older, but the school-age child with
dyspraxia will
probably show the same difficulties experienced by pre-schoolers with
dyspraxia. This will include aspects such as late milestones (motor and
speech); difficulty with motor activities such as running, hopping,
jumping and kicking; difficulty in walking up and down stairs; difficulty
in dressing; being slow and hesitant in most actions; clumsiness; having
poor pencil grip; the inability to do puzzles or shape-sorting games;
immature artwork; and anxiety and high distractibility
avoid physical exercise and motor games
perform badly in class but significantly better on a one-to-one basis
react to all stimuli (cannot differentiate between important and
unimportant ones)
have a poor attention span
perform poorly in maths and writing structured stories
experience great difficulty in copying from the blackboard
write laboriously and immaturely
be unable to remember and/or follow instructions
be poorly organised.
9.2.5.4 Strengths: resilience factors
Children with dyspraxia do not form a homogeneous group, and therefore
their strengths (and needs) will change as they develop and grow. Each
child’s unique strengths should be identified and then used as the basis on
which to start teaching new skills. These learners respond well in the
classroom with support, for example in the form of a lifeline (knowing that
there is someone to whom they could turn for help) or a study buddy
(Dixon & Addy, 2004).
9.3 MANAGING A CHILD WITH A LEARNING DISABILITY
IN THE CLASSROOM CONTEXT
The secret of education lies in respecting the pupil.
R
W
E
(1803–1882,
)
Learning is a lifelong, dynamic process that involves exploration, practice,
mastery, application and evaluation (Reid, 2005). Children must be actively
engaged in the learning process, and it is not something that is done to or
for them. All people have the capacity to learn and there are many different
ways in which learning takes place. For example, some children learn from
being read to and then memorising the facts, some learn from facts shown
on the back of cereal boxes, some from games instructions, some from
signs found in the community. Some children even teach themselves letter
sounds, while others find it easier to read the whole word (sight
vocabulary). Research has shown that average readers require 4–14
exposures to a word before it becomes a sight word, whereas learners with
learning disabilities may need up to 40 exposures (Handler & Fierson,
2011). Whatever else they learn, reading is probably the single most
important skill children acquire at school. Unfortunately, learners who
cannot read well tend to read less, which means they have fewer
opportunities to develop reading skills – and so a vicious circle starts.
In order to help children with learning disabilities to learn optimally,
teachers should first get rid of all the ants! Ants? Automatic Negative
Thoughts. If you think and believe that you cannot do something, you are
probably right. However, if you think that you can, you are probably right
too, therefore teachers should explain to all learners that no ants are allowed
in the classroom. If somebody spots an ant – deal with it immediately!
Stop and reflect
There is a saying that for the first three years at school children learn to read, and for
the next nine to 14 years they read to learn! How can we help them achieve this?
9.3.1 Developing learning skills
Teachers should always be encouraged to teach to the learners’ strengths,
also known as learning styles (e.g. visual, oral, tactile, etc.). In a classroom
this would ultimately mean that a multimodal teaching approach is
followed, as children will have varying strengths.
Learners must become aware of their own learning styles and strengths so
that they can actively become involved in learning. In order to teach this in
the classroom, teachers should help children explore their own prior
knowledge and understanding of a topic by asking: “What do I already
know?” This helps them integrate new knowledge with existing knowledge,
which ultimately impacts positively on memory (Reid, 2005). The
questions: “How did I acquire that knowledge?” and “How am I going to
learn new things?” then become important.
After thinking about learning styles, the teacher should address the structure
of the lesson: “We are going to watch a video about ‘economy’ and then
we’ll discuss the video. Then you need to find pictures, and in your small
groups design a poster that describes the world economy.” At this point, the
teacher should point to the sequence of learning; in other words: “Where
am I heading?” The learners should understand how this lesson about the
world economy and the next lesson (e.g. about the South African economy)
are linked, and ultimately how this will teach them about becoming
entrepreneurs, therefore all the pieces of the bigger picture should be
explained. Finally, teachers will need to reward and reinforce the learning
by showing learners what is in it for them (e.g. “You’ll do an entrepreneurs’
project, giving you the opportunity to sell your products and earn a few
rand!”).
9.3.2 Reciprocal teaching
Another strategy that is particularly useful in the classroom context is
reciprocal teaching (Green, 2006; Palincsar & Brown, 1984). This method
requires the teacher to place children into flexible groups (also known as
small multiskill-level groups). Research is showing that small groups of
three learners are optimal (McLeskey & Waldron, 2011). The teacher
provides a brief, focused introduction on the topic and hands out a written
worksheet. Where appropriate, attempts should be made to link the text to
other content areas, as this gives added purpose to the children’s learning.
The teacher then introduces the four specific strategies (clarifying,
questioning, summarising and predicting – see Figure 9.2) by handing out a
prompt card to each group that displays the different strategies in order to
remind the learners what is expected of them.
Figure 9.2 Example of a prompt
card used in reciprocal teaching
9.3.2.1 Clarifying
After reading the text the learners are encouraged to clarify concepts by
alerting the other members of the group to unfamiliar vocabulary, new or
difficult concepts, text that is unclear, or aspects they do not understand. If
this were to happen, they can come to grips with the content by rereading,
defining the context of the text or by using a dictionary to check meaning
(in social sciences, a road map or atlas can also be used). It may be
necessary to reread the whole section in order to understand the subject
matter.
9.3.2.2 Questioning
This strategy requires the learners to explore the text in depth, and provides
them with the opportunity to ask questions before, during and after reading.
When suitable questions have been asked, possible solutions can be offered,
and learners can be taught how to find relevant information to answer
questions. They can also be taught to monitor their own understanding by
asking questions, and they can help other learners answer questions –
particularly if they have the same questions. It is important that children are
made aware of the fact that questioning is a means of self-checking and that
they become much more involved in the reading activity when they are
posing and answering questions themselves and not only depending on the
teacher.
9.3.2.3 Summarising
When summarising, learners have to identify the most important facts in the
text and integrate the meaning with their own prior knowledge in order to
fully understand it. Summarising thus teaches the learners to identify and
integrate important information that is presented in the text.
9.3.2.4 Predicting
This encourages learners to predict what will happen next in the text based
on prior knowledge, and on the structure and content of the text. After
having read the new text, they need to accept or reject their hypothesis
(what they predicted would happen).
While the groups are discussing and using these four strategies, the teacher
should listen to the conversations in the flexible groups, and monitor how
effectively they are being used. This information will help teachers increase
the levels of participation and therefore learning in the classroom.
9.3.3 Cognitive organisers
Another useful classroom strategy that will enable learners to remember
and follow procedures and strategies is cognitive organisers. They often
make use of mnemonic devices to help with memory recall. One cognitive
organiser that can be useful to cue children with reading comprehension is
the mnemonic TRAVEL (Kowarski, 2008):
T = Topic. Write down the topic.
R = Read. Read the paragraph.
A = Ask. Ask what the main idea is, as well as three details and write
them down.
V = Verify. Verify the main idea and linking details.
E = Examine. Examine the next paragraph and verify again.
L = Link. When finished, link all the main ideas.
Another mnemonic that is effective for teachers is SCREAM (Mastropieri
& Scruggs, 2012), which was alluded to in Chapter 4:
S = Structure. Teachers should explain how the components of the
lesson are organised: “The first thing that we’ll do is … and then
we’ll …”
C = Clarity. Explain the objectives of the lesson one by one, using clear
language and providing concrete examples.
R = Redundancy. Emphasise and reinforce the most important aspects as
this provides more learning opportunities.
E = Enthusiasm. Enthusiastic teachers enhance learning, thereby
creating more learner engagement and participation in the classroom.
A = Appropriate rate. Generally, a brisk rate keeps lessons interesting
and motivating.
M = Maximised engagement. Use instructional materials and
presentation styles that encourage participation such as praise,
feedback, questioning.
Stop and reflect
A Grade 6 teacher decides to use the mnemonic POWER to assist her learners in
planning how to write an essay:
P = Plan your essay.
O = Organise your thoughts and ideas.
W = Write your draft essay.
E = Edit your work.
R = Revise your work and produce the final essay.
9.3.4 Taking notes in class: teaching this skill
Taking notes in class is difficult for all children due to the multiple steps
involved – and it is particularly difficult for children with learning
disabilities. Teachers often speak quickly, providing lots of information.
Children who belong to the “I-must-write-down-everything” club hear
names, dates and facts, and then struggle to capture everything on paper in
the form of full sentences. Teachers should teach learners to use the
following tricks when taking notes in class (adapted from Levy, 2007):
Use symbols. Teach the use of well-known symbols such as question (?),
percentage (%), money ($), at (@), but also encourage them to design
their own symbols for words such as “equal” and “circle”. Then dictate
mock sentences and help them use symbols, for example: “John has a
question: Is number 1 equal to number 2?” The learner might then write
“John has? 1 = 2?”
Use abbreviations and contractions. Encourage the use of abbreviations
that are used when sending text messages (SMSs) for example Tue
(Tuesday), wth (with), gr8 (great), I’ll (I will), cu (see you), and so on.
Dictate some sentences in class and encourage children to use these
strategies.
The notes. Once learners are able to use symbols, abbreviations and
contractions, they should be taught how to organise them all on paper. It
is important to get some idea of the child’s learning style. Some children
with learning disabilities might prefer a linear style (the analytic
thinkers), while other learners are more visually orientated (the holistic
thinkers) (Mortimore & Dupree, 2008). Analytic thinkers are good with
detail, like lists and sequences, have a strong sense of order and welldeveloped step-by-step logic. However, they might have difficulty in
planning the bigger picture and might fail to make connections. Holistic
thinkers, on the other hand, deal easily with structure, and enjoy using
mind maps and plans (Buzan, 2010). They need to see the big picture and
are good at making connections and seeing creative links. These learners
may, however, lose the detail and often fail to follow logical steps.
Analytic learners will benefit from column-style notes (see Table 9.2).
Divide the page into two columns and label the left column “Main ideas”
and the right column “Notes”. (The right column should be broader than
the left.) In class the learners should then take class notes only in the
right-hand column and, when at home, they should reread the notes and
group different sections of the lesson into main ideas. They can then
move through all their notes in that manner, categorising the main ideas.
Table 9.2 Example of a column-style note page
Main ideas
Notes
Causes of World War II
League of Nations (only four winners)
Punished Germany
Germany retaliated under Hitler
Divided world
– for Germany
– against Germany
Battles of World War II
Barbarossa (Russia used weather)
Blitzkrieg (“lightning” war: six countries/six weeks)
D-Day (sea invasion & from behind dunes)
Pearl Harbour (Japan & “neutral” America)
Column-style notes encourage learners to reread their own notes. If there
are gaps in the notes, the learner can ask a study buddy or the teacher or
consult the textbook. The more they practise this strategy, the better they
will become. Other types of organisation that are effective for more analytic
learners include grids, lists and boxes with one key word per box.
Holistic thinkers will benefit from webbing. This is an effective strategy
for visually orientated learners who tend to see things more holistically.
They should be encouraged to draw a circle in the middle of their page
containing the heading and then branch the different ideas out from that
circle (mind maps). Learners should also be encouraged to combine
graphic images (pictures) and words on their mind maps, and use
different coloured pens and highlighters (Buzan, 2010).
9.3.5 Homework strategies
Homework is a reality for all school-going children, and one of the greatest
gifts teachers can give to their learners is an appreciation of and an ability
to use strategies that make learning easier. These strategies can build on
strengths while at the same time compensate for difficulties. As all children
differ, not all strategies will help all children equally, and therefore teachers
should try to match the strategies to the learning style of the child. Some
useful strategies include the following (Richards, 2008):
Organisation. Use different-coloured folders for specific subjects, have a
special place for letters/papers that have to be taken home or taken to
school, and help the child understand the logic behind the organisation.
Ensure understanding. Always review the task to ensure that it has been
understood – this will help the learner to achieve a high success rate in
terms of completing the task in the required manner (McLeskey &
Waldron, 2011).
Fatigue issues. Some learners might use fatigue as an excuse to escape
from too-difficult or too-easy tasks (see Chapter 7). For children with
learning difficulties, teachers and parents can agree to a maximum time
to spend on homework. Parents should then keep a “time log” and sign
the end of the homework page showing the amount of time spent on the
assignment. If the learner spends excessive amounts of time with
homework, alternatives can be explored.
Use encouragement. Learning requires positive feedback (Reid, 2005).
Encouragement will build the child’s self-esteem and also reduce
frustration, for example: “I know this is difficult, but I’m sure you could
do it with a little help”. Another type of encouragement that helps is to
prioritise the important areas, for example: “Let’s first do this, and then
that.”
Use learning contracts. This was described at length in Chapter 5.
Monitor time on task. A timer is useful for determining time spent on a
task, and helps the learner to see visually how time passes (makes time
concrete).
Reduce homework load and accept dictated homework. Allow learners
with learning difficulties to dictate answers, as they can do this much
more easily and quickly than they can write them down. Their parents or
a sibling can then be allowed to act as a scribe when they do their
homework.
Learn from mistakes. Many children are afraid of making mistakes and
might therefore not even attempt to complete a task or try an activity.
Teach children that learning from their mistakes is a critical component
of learning, and that mistakes are not only accepted, but also expected
(Reid, 2005).
9.4 MOST COMMONLY USED CLASSROOM
ACCOMMODATIONS
There is no quick fix that can cure learning disabilities. However, there are
many classroom adaptation strategies that teachers can easily implement to
assist these learners, of which the best strategy remains to anticipate and
avoid failure! Overlearning – that is, the systematic use of repetition to
ensure that newly acquired skills become automatic and consolidated in
memory so that they can be easily applied or recalled when needed – seems
to be the one key strategy all teachers in this field agree upon (Rose, 2009).
If this is not possible, adaptation strategies can make it easier for these
learners to demonstrate their knowledge, even if they are not yet reading,
writing or spelling at the appropriate level for their specific grade.
9.4.1 Teach problem solving
Many subjects (e.g. maths and natural science) require problem solving in a
systematic stepwise manner. Some learners try to do everything at once,
using the first strategy that comes to mind without considering alternatives.
Teachers should help learners pace themselves (e.g. by using a timer) and
reward them when appropriate for working slowly and carefully. Give them
proofreading exercises where they have the opportunity to find errors in the
work of others. Encourage them to talk their way through the problem, step
by step, and then get them to explain the steps once the activity has been
completed (Levine, 2002).
9.4.2 Teach reading comprehension strategies
Teachers should assist learners to increase their understanding of what they
read. This is a skill that will only improve if teachers directly target it. This
can be achieved by using many different strategies, for example
encouraging them to reread the work, even if they are reluctant to do so.
Teach children to highlight key words (and unfamiliar ones) by using a
highlighter pen. Discuss unfamiliar phrases and content, and encourage
them to look up unfamiliar words in the dictionary. They might then be
taught how to keep a dictionary of new vocabulary.
Ask questions throughout the reading activity and pitch these questions at
various levels (as described in Chapter 4). Questions that are asked at the
inferential level (understanding facts not directly stated in the text) where
learners have to synthesise the literal meaning of the text by using their
intuition, personal knowledge and imagination are particularly difficult for
learners with learning difficulties. Teachers should therefore try to avoid
questions such as: “How would you …? What might happen if …? What do
you think might have happened before/after …? What kind of person was
…?”, unless they provide learners with the necessary scaffolding strategies
to deal with them. Teach learners how to summarise or paraphrase what
they have just read, or even draw a picture of it.
Some learners find it very useful to use visualisation strategies. For
example, when discussing the photosynthesis of plants, they must imagine
how the leaves suck up carbon dioxide and breathe out oxygen. In cases
where they have to learn facts that follow a particular sequence of events,
they might be encouraged to keep a log of these events or even a mind map
(Green, 2006). Finally, reciprocal reading can also be explored, which
means that the teacher and learner take turns in reading – the teacher may
ask questions and the learner should ask for clarification if he does not
understand. At the end of the paragraph, the teacher and learner then
summarise the text and make predictions.
9.4.3 Do not force oral reading
Learning is more effective in non-threatening environments (Reid, 2005).
Teachers should never force learners with dyslexia to read aloud in front of
the class. If for some reason this is absolutely necessary, warn such learners
in advance and show them exactly which paragraph they will have to read
so that they can practise ahead of time. Some children will enjoy listening
to taped stories as these will continue to stimulate their thinking without the
pressure of reading (Peer, 2009; Siegel, 2006.). In order to assist with
learning, new advances in computers such as screen readers are also helpful
as they allow the learner to listen to the work, thereby benefiting from the
auditory modality (Siegel, 2006).
9.4.4 Introduce a personal dictionary of key terms
Encourage learners to make use of a personal dictionary in which they can
write down key elements associated with words. All learners will benefit
from a study guide containing key terms and concepts that are relevant to
the particular subject. Writing down mathematical terms such as “multiply”
or “subtract” is particularly helpful for children with dyscalculia (Levine,
2006). Subject glossaries should also be made available to all learners.
9.4.5 Reduce copying tasks
It takes children with dyslexia longer to copy information from the board,
and if they also have dysgraphia they may not be able to read their notes.
For these learners, teachers can provide class notes or discreetly assign a
buddy to act as a scribe using copy carbon paper (when someone writes on
the top sheet of paper, the coating automatically makes a copy appear on the
lower sheet). When class is over, the scribe just tears off the lower sheet and
gives it to the learner with dyslexia (see Figure 9.3).
Figure 9.3 Using a buddy to make a carbon copy
9.4.6 Accept calculators
Studies have shown that the use of calculators in maths teaches learners
better problem-solving strategies and also fosters a more positive attitude
towards maths (Ellington, 2003). Do calculators not just give learners all
the answers? Not if the teachers get it right! Calculators can help learners
explore mathematical concepts. For example, in the younger grades learners
can use them for counting (using the constantly repeating +1) as well as
number relations (e.g. greater than (>) and smaller than (<)). It can also
assist learners with learning disabilities with calculations, as they can then
focus their attention on higher-level maths concepts rather than on
performing difficult computations. Finally, calculators also provide a
scaffold for effective learning, as learners with learning disabilities are able
to experience success in problem-solving activities that would otherwise be
too difficult (see Figure 9.4).
Figure 9.4 Allow the use of calculators
9.4.7 Adapt assessment procedures
Learners with learning difficulties do not perform well under pressure of
time. It also takes them longer to read the questions, formulate the answers
in their head and get them down on paper. It is therefore suggested that
within reason their tests have no time limit.
Teachers should offer alternative ways to show mastery of material other
than long written papers. This will ensure that the teacher gets a fair and
accurate picture of what the learner knows (Mastropieri & Scruggs, 2012).
Alternatives include match-up questions, fill-in-the-blank or short-answer
formats (see Figure 9.5). The vocabulary words for fill-in-the-blank
sections can be listed at the top of the test. Multiple-choice questions are
also difficult for learners with dyslexia due to the volume of reading
required to answer them correctly (see Chapter 3 for more examples).
Figure 9.5 Adapting test procedures
Spelling tests form a central part of literacy instruction in the Foundation
Phase. However, teachers rarely test spelling words in the same way or
order as they are listed in the homework book, which might confuse
learners with learning difficulties. Many teachers will accept a spelling test
given in a one-on-one session as a replacement for the classroom test, or
only request a spelling test on a small number of predetermined words (i.e.
give children with learning difficulties only half of the number of words
that their peers need to complete).
Another test alternative is oral testing; in other words, the tests are read to
the learners, and learners are allowed to answer orally. Teachers can also
prerecord the test as an audio file, for example by using a smartphone or
Dictaphone to record it, and the learners can then listen to it on a computer
using headphones, and also record their answers orally. Other alternatives to
written tests include doing oral or video presentations, enacting a play,
compiling a collage, creating a poster, completing a timeline, building a
model, designing a flow chart, compiling a quiz, drawing a comic
storyboard, or holding a radio/TV interview where the topic is debated
(Mortimore, 2008).
9.4.8 Grade on content, not spelling or handwriting
Some teachers take spelling and handwriting into consideration when
assigning a grade. For learners with learning difficulties, this is not
appropriate. Teachers should be asked to grade only on the content of an
assignment. Try to provide positive comments, for example: “Well done for
writing more than 50 words!”; “Well done for putting in full stops!”; “Well
done for trying to use capital letters!”; even if the spelling is atrocious.
These comments will not only boost the learners’ self-esteem, but will also
encourage them to keep on trying, as this is much more rewarding that
seeing the whole essay being rewritten in red pen. Teachers should be
encouraged to remember that less is more (in terms of their comments when
marking work) and that two positive comments increase the possibility of
the learners’ future success (Mortimore & Dupree, 2008).
9.5 ASK LEARNERS HOW THEY LEARN BEST
Often, learners with learning difficulties know which strategies and
techniques assist them. Teachers are encouraged to explain the different
dimensions or characteristics of learning to children. One such a creative
tool is the effective lifelong learning inventory (ELLI) (Hutchings, 2008).
To make it easy for the children to remember, an animal is used to depict
each of these dimensions, and both the positive and negative aspects
associated with it are described. Children of all ages are then asked to say
which of these aspects are “very much like me” and which aspects are “not
like me at all”. The key elements of the ELLI are shown in Table 9.3.
Table 9.3 What makes a good learner?
Animal examples
Positive
learning
aspect
Changing
and learning
Negative
learning
aspect
Being stuck
and static
Examples
I see learning as something I
can get better at.
I tend to take ownership of my
own learning and like to be
responsible for what I am
learning and how I go about it.
Critical
curiosity
Passivity
I like to get below the surface of
things and see what is really
going on.
I like to work things out for
myself and ask my own
questions.
I enjoy learning and have a good
deal of energy for learning tasks
and situations.
I value getting at a truth.
Animal examples
Positive
learning
aspect
Making
sense
Negative
learning
aspect
Data
accumulation
Examples
I tend to look for patterns,
connections and coherence
when I am learning.
I seek links between new
information and what I already
know.
I like to make sense out of new
things in terms of my own
experience, and I like learning
what matters to me.
Unicorn
Creativity
Rigidity
I like new situations, and
sometimes create novelty “just to
see what happens”.
I like playing with possibilities
and imagining how situations
could be otherwise.
I sometimes get my best ideas
when I just let my mind float
freely.
I often use my imagination when
I am learning.
Resilience
(hard shell
of the
tortoise
provides a
barrier)
Fragility and
dependence
I tend to stick at things for a
while, even when they are
difficult. I do not give up easily.
I enjoy grappling with things that
are not easy.
I can handle the feelings that
crop up during learning, such as
frustration, confusion, etc.
I am not easily upset or
embarrassed when I cannot
immediately figure something
out.
I do not immediately look for
somebody to help me out when I
find things difficult or when I get
stuck.
Animal examples
Positive
learning
aspect
Strategic
awareness
Negative
learning
aspect
Robotic
Examples
I tend to think about my learning
and how I go about it.
I usually have a fair idea of how
long something is going to take
me, what resources I will need
and my chances of being
successful.
I am able to talk about the
process of learning – how I go
about things, and how I go about
myself as a learner – what my
habits, preferences, aspirations,
strengths and weaknesses are.
Positive
learning
relationships
Isolation
I like working on problems with
other people, especially my
peers.
I have no problems in sharing
thoughts and ideas with others –
I find it useful.
I have important people around
me and in my community who
help me with my learning.
The teacher can either present the children with the various animals, or she
can ask them to choose an animal that represents one of the learning
aspects. Learners are then asked to discuss which learning aspects are
important when completing a task, and then they can rate themselves on a
visual scale by stating whether they are or are not like the particular aspect,
for example:
Like me –––––––––––––––––– Not like me
“I think I was a lot like a bee this morning when we did our social studies activity,
because we worked well together and remained focused on the questions. We listened
to each other and didn’t argue once.”
It is clear that this type of strategy will help children to understand that
being a good learner is made up of many different aspects. Children need to
be taught how to reflect on and think about their learning style and to
identify the aspects that they are good at, as well as those that need
improvement.
9.6 CONCLUSION
In this chapter we discussed the importance of taking things one step at a
time. We looked at the children and at the classrooms in which they have to
function, and suggested some adaptations in order to make the classrooms
dyslexia friendly, as this will benefit all children with learning disabilities.
We all know the saying: “Nothing succeeds like success”, but is that the
whole story? Obviously not. We also have to explore the teacher
characteristics that make it easier for children with learning disabilities
(Giorcelli, 2006):
Teachers who are excited about their subject and who work in creative
ways to get learners to share their enthusiasm
Teachers who are flexible and who work creatively with these learners
instead of sticking to the rules rigidly
Teachers who encourage learners who experience learning difficulties
rather than being critical all the time
Teachers who are organised and clear about what is required in their
subject and class
Teachers who are fun and interesting, and who seem to enjoy teaching
REFERENCES
Alexander, A., Anderson, H., Heilman, P., Voeller, K. & Torgesen, J. 1991. Phonological awareness
training and the remediation of analytic decoding deficits in a group of severe dyslexics. Annals of
Dyslexia, 41: 193–206.
American Psychiatric Association (APA). 2013. Diagnostic and statistical manual of mental
disorders (DSM-5), 5th ed. Washington, DC: American Psychiatric Publishing.
Bornman, J. & Donohue, D. 2013. South African teachers’ attitudes toward learners with barriers to
learning: attention-deficit and hyperactivity disorder and little or no functional speech. International
Journal of Disability, Development and Education, 60(2): 85–104. Available at:
http://dx.doi.org/10.1080/1034912X.2013.786554
Bowers, B. 2007. Tracing business acumen to dyslexia. New York Times. Available at:
http://www.dannykessler.com/images/
ARTICLES/NYT%20Tracing%20Business%20Acumen%20to%20Dyslexia%20%20New%20York%20Times.pdf (accessed on 8 January 2009).
Braun, J., Kahn, R.S., Froehlich, T., Auinger, P. & Lanphear, B.P. 2006. Exposures to environmental
toxicants and attention-deficit/hyperactivity disorder in US children. Environmental Health
Perspectives, 114(12): 1904–1909.
Brown, T.E. 2013. A new understanding of ADHD in children and adults: executive function
impairments. New York: Taylor & Francis.
Brown, T.E. 2016. Growing up with ADHD: clinical care issues. Psychiatric Times. Available at:
http://www.psychiatrictimes.com
Buzan, T. 2010. The mind map book. Unlock your creativity, boost your memory, change your life.
London: BBC Active.
Cass Business School. 2004. Entrepreneurs five times more likely to suffer from dyslexia. Available
at: http://www.cass.city.ac.uk/media/stories/story_8_45816_44300.html (accessed on 8 January
2009).
Chu, S. & Flores, S. 2011. Assessment of English language learners with learning disabilities. The
Clearing House, 84: 244–248 doi: 10.1080?00098655.2011.590550
Dixon, G. & Addy, L.M. 2004. Making inclusion work for children with dyspraxia: practical
strategies for teachers. London: Taylor & Francis.
Dyspraxia Foundation. 2009. Available at: http://www.dyspraxiafoundation.org.uk (accessed on 6
March 2009).
Ellington, A.J. 2003. A meta-analysis of the effects of calculators on students’ achievement and
attitude levels in pre-college mathematical classes. Journal for Research in Mathematics Education,
34(5): 433–463.
Franck, R., Rosen, S., Dakin, S.C., Day, D.L., Castellote, J.M., White, S. & Frith, U. 2003. Theories
of developmental dyslexia: insights from a multiple case study of dyslexic adults. Brain, 126(4):
841–865.
Giorcelli, L. 2006. Best practice in inclusive schools: practical strategies for working effectively with
students with ADD/ADHD. Paper presented at the SAALED From Inclusion to Belonging
Conference, Nedbank Sandton Auditorium, Sandton.
Grafman, J. & Romero, S. 2001. Appearances may not be deceiving: calculation deficits due to a
brain structure abnormality in neurologically normal children. Brain, 124(9): 1681 – 1682. doi:
http://dx.doi.org/10.1093/brain/124.9.1681
Green, S. 2006. Dyslexia: extending strategies for classroom practice. Paper presented at the
SAALED From Inclusion to Belonging Conference, Nedbank Sandton Auditorium, Sandton.
Handler, S.M. & Fierson, W.M. 2011. Learning disabilities, dyslexia, and vision. Pediatrics, 127(3).
Harpin, V.A. 2005. The effect of ADHD on the life of the individual, their family, and their
community from preschool to adult life. Archives of Disease in Childhood, 90: i2 – i7. doi:
10.1136/adc.2004.059006
Henderson, A., Came, F. & Brough, M. 2003. Working with dyscalculia: recognising dyscalculia and
overcoming barriers to learning in maths. Wiltshire, UK: Learning Works International.
Hinshelwood, J. 1917. Congenital word-blindness. London: HK Lewis & Co.
Hudson, R.F., High, L. & Otaiba, S. 2007. Dyslexia and the brain: what does current research tell us?
The Reading Teacher, 60(6): 506–515.
Hutchings, M. 2008. Using the extended lifelong learning inventory (ELLI) to develop a language for
supporting and acknowledging diversity in the classroom. Paper presented at the SAALED From
Inclusion to Belonging Conference, Nedbank Sandton Auditorium, Sandton.
International Dyslexia Association. n.d. Available at: http://www.interdys.org/FAQ.htm (accessed on
8 January 2009).
Keith, K.M. 2001. Anyway: the paradoxical commandments. London: Inner Ocean Publishing Inc.
Khan, S.A. & Faraone, S.V. 2005. The genetics of attention-deficit/hyperactivity disorder: a literature
review of 2005. Current Psychiatry Reports, 8: 393–397.
Kowarski, M. 2008. Dyslexia and reading comprehension. SAALED NEWS, 28(3): 19–22.
Landerl, K., Bevan, A. & Butterworth, B. 2004. Developmental dyscalculia and basic numerical
capacities: a study of 8–9-year-old students. Cognition, 93(2): 99–125.
Levine, M. 2002. A mind at a time. New York: Simon & Schuster.
Levine, M. 2006. Schools in which all kinds of minds can grow in all kinds of good ways. All Kinds
of Minds newsletter. Available at: http://www.readingrockets.org/article/10729 (accessed on 12
January 2009).
Levy, E. 2007. Teaching students to take class notes. SAALED NEWS, 27(1): 11–13.
Lyytinen, H., Erskine, J., Aro, M. & Richardson, U. 2007. Reading and reading disorders. In Hoff, E.
& Shatz, M. (Eds). Blackwell handbook of language development. Malden, MA: Blackwell.
Maestri-Banks, A. 2013. Learning disability, education and empowerment: learning from individuals
who live with a learning disability. The Higher Education Academy, 29(1).
doi:10.11120/hsce.2013.00022
Martins, M.R.I., Bastos, J.A., Cecato, A.T., Araujo, M.L.S., Magro, R.R. & Alaminos, V. 2013.
Screening for motor dysgraphia in public schools. Jornal de Pediatria, 89(1): 70–74. Available at:
https://dx.doi.org/10.1016/j.jped.2013.02.011
Mastropieri, M.A. & Scruggs, T.E. 2012. The inclusive classroom: strategies for effective instruction,
4th ed. New Jersey: Merrill Prentice Hall.
McCann, D., Barrett, A., Cooper, A., Crumpler, D., Dalen, L. & Grimshaw, K. 2007. Food additives
and hyperactive behaviour in 3-year-old and 8/9-year-old children in the community: a randomised,
double-blinded, placebo-controlled trial. The Lancet, 370(9598): 1560–1567.
McLeskey, J. & Waldron, N.L. 2011. Educational programs for elementary students with learning
disabilities: can they be both effective and inclusive? Learning Disabilities Research and Practice,
26(1): 48–57.
Mick, E., Biederman, J., Faraone, S.V., Sayer, J. & Kleinman, S. 2002. Case-control study of
attention-deficit hyperactivity disorder and maternal smoking, alcohol use, and drug use during
pregnancy. Journal of the American Academy of Child and Adolescent Psychiatry, 41(4): 378– 385.
Mortimore, T. 2008. Dyslexia-friendly classrooms. Paper presented at the SAALED From Inclusion
to Belonging Conference, Nedbank Sandton Auditorium, Sandton.
Mortimore, T. & Dupree, J. 2008. Dyslexia-friendly practice in the secondary classroom. Exeter:
Learning Matters.
Orfano, F. 2012. Guide to identifying dyscalculia. Bright Hub Education. Available at:
http://www.brighthubeducation.com/special-ed-learning-disorders/62694-dyscalculia-characteristicsand-symptoms-in-children/
Orton, S.T. 1928. Specific reading disability: strephosymbolia. Journal of the American Medical
Association, 90(14): 1095–1099.
Palincsar, A.S. & Brown, A.L. 1984. Reciprocal teaching of comprehension-fostering and
comprehension-monitoring activities. Cognition and Instruction, 1(2): 117–175.
Peer, L. 2009. Dyslexia: research and remediation. SAALED workshop, Johannesburg.
Perold, M., Louw, C. & Kleynhans, S. 2010. Primary school teachers’ knowledge and misperceptions
of attention deficit hyperactivity disorder (ADHD). South African Journal of Education, 20(3): 457–
473.
Price, G.R. & Ansari, D. 2013. Dyscalculia: characteristics, causes and treatments. Numeracy
Advances in Quantitative Literacy, 6(1). doi:http://dx.doi.org?10.5038/1936-4660.6.1.2
Prinsloo, N. 2008. Dyscalculia: difficulties in performing mathematical calculation of certain type.
SAALED NEWS, 28(5): 4–6.
Reid, G. 2005. Dyslexia and inclusion: classroom approaches for assessment, teaching and learning.
London: David Fulton.
Richards, R.G. 2008. Being an efficient homework helper: turning a chore into a challenge. SAALED
NEWS, 28(5): 9–14.
Ritchey, K.D. & Goeke, J. 2006. Orton–Gillingham and Orton–Gillingham-based reading instruction:
a review of the literature. Journal of Special Education, 40(3): 171–183.
Rose, J. 2009. Identifying and teaching children and young people with dyslexia and literacy
difficulties. An independent report from Sir Jim Rose to the Secretary of State for Children, Schools
and Families, London.
Rostami, A., Allahverdi, F. & Mousavi, F. 2014. Dysgraphia: the causes and solutions. International
Journal of Academic Research in Business and Social Sciences, 4(2). doi:10.6007/IJARBSS/v4i2/582
Rousselle, L. & Noel, M.P. 2007. Basic numerical skills in children with mathematics learning
disabilities: A comparison of symbolic vs non-symbolic number magnitude processing. Cognition,
102: 361–395.
Shaywitz, S. 2005. Overcoming dyslexia: a new and complete science-based program for reading
problems at any level. New York: Vintage Books.
Siegel, L.S. 2006. Perspectives on dyslexia. Paediatrics & Child Health, 11(9): 581–587.
Sperling, A.J., Lu, Z.L., Manis, F.R. & Seidenberg, M.S. 2005. Deficits in perceptual noise exclusion
in developmental dyslexia. Nature Neuroscience, 8: 862–863.
Thapar, A., Cooper, M., Jefferies, R. & Stergiakouli, E., 2012. What causes attention deficit
hyperactivity disorder? Archives of Diseases in Childhood, 97: 260–265. doi:10.1136/archdischild2011-300482
Walker, S., Venter, A., Van der Walt, A. & Esterhuysen, K.G.F. 2011. Prevalence of attention deficit
hyperactivity disorder (ADHD) symptomatology and psychiatric comorbidity among adolescents
diagnosed with ADHD in childhood. South African Journal of Psychiatry, 17(1): 24–28.
doi:http://dx.doi.org/10.7196/sajp.261
Wilcox, S. n.d. Dyslexia questionnaire. Available at: http://www.wilcoxdyslexia.co.uk/questionnaire.asp (accessed on 7 March 2009).
Wolraich, M., Milich, R., Stumbo, P. & Schultz, F. 1985. The effects of sucrose ingestion on the
behaviour of hyperactive boys. Paediatrics, 106(4): 657–682.
10
Understanding children with
physical disabilities
It was in January 2009 when I was a new student at Mitchell House College in
Polokwane, Limpopo. I was very anxious as a new learner trying to adjust to a new
school. I found myself seated right next to a disabled learner by the name of Lesedi
Makgato. I was surprised and confused because from my past experiences I was
taught that the disabled have their very own designated classrooms. I soon realised
that Lesedi wasn’t the only learner with a disability around but there were six more in
other classes. I questioned myself every day but still had no answers to my
questions, so I decided to give up. Discomfort and irritation were my key feelings
whenever Lesedi drove into the classroom with his automated wheelchair as he
bumped into everything without any remorse. Learners didn’t seem to care, so I
decided to join them. Lesson after lesson, day after day it was the same. Five months
down the line I became seriously irritated and approached Lesedi. Politely. We spoke
for about two hours. I was trying to really understand why he had so much
confidence to just drive into a classroom bumping into everything and just continue
with lessons as if nothing had happened. Lesedi had serious physical challenges. His
motor coordination was seriously affected. He was used to being looked and frowned
at so he learned to live with it. He had such a high sense of humour. He was talkative
and adorable. I soon discovered that he was just a normal teenager who joked and
laughed with girls. He was also intelligent. He knew and understood difficult subjects
like maths whilst some of us were struggling. I became very close to Lesedi. He was
my best friend.
Neo Manamela, April 2016
10.1 INTRODUCTION
The story of Neo and Lesedi’s friendship is full of discovery and warmth. It
is a wonderful example of cutting through layers of preconceived ideas and
prejudices. It is a story of two youngsters living and learning together in an
inclusive school and becoming best friends. It is the lens through which to
read this chapter.
Children with disabilities face daily challenges associated with motor or
movement skills (activity limitations) and participation in regular activities
at home, at school and in the community (participation restrictions). These
concepts are defined in the ICF-CY (WHO, 2007) as follows:
Activity limitations: difficulties in executing activities
Participation restrictions: problems in involvement in life situations
Motor skills can typically be divided into two categories:
Gross motor skills. These refer to the control of posture and movement
(e.g. rolling, sitting, crawling, standing, walking and skipping).
Fine motor skills. These refer to control of the upper limbs with the
emphasis on hand function (e.g. writing, drawing, fastening shoelaces,
knitting, putting on make-up and doing woodwork). Oral control is also
considered a fine motor skill, and is essential for sucking, swallowing,
chewing and, most importantly for the development of speech.
Disturbances of gross and/or fine motor control will always impact an
individual’s ability to interact with people and cope with activities of daily
living (e.g. playing, dressing, feeding, learning and socialising).
At some time in their growing years, all children will experience significant
challenges. For some these will be short term but for others they may
persist into adulthood. Intellectual and physical disabilities, which
frequently occur together, may be exacerbated by other factors such as
poverty, abuse, and medical conditions such as HIV/AIDS and TB.
Because physical disabilities are usually obvious, these children frequently
experience cautious or negative attitudes from others. Changing these
attitudes needs to be a conscious process for parents, teachers and
communities. Learning about disabilities is only a start. The process has to
become relational – that is, there has to be meaningful interaction between
individuals. No matter what specific challenges a child may face, the core
values of education remain the same.
All children can learn and succeed, but not necessarily on the same day
or in the same way.
Skill begets skill or, put another way, successful learning promotes even
more successful learning (Heckman, 2006).
As highlighted in Figure 10.1, the focus of this chapter will be on cerebral
palsy, spina bifida and muscular dystrophy, but there are many other
conditions that also cause physical disabilities such as spinal cord injury,
bone cancer, polio, fractures, club feet, scoliosis, juvenile rheumatoid
arthritis and burns.
Figure 10.1 Physical disabilities
What becomes evident is that in spite of the diversity of physical
disabilities, the principles underlying the provision of supports for optimal
learning are the same. A thorough knowledge of normal development is
essential when planning and implementing strategies that will enable full
participation. In this chapter the broad principles will be discussed.
10.2 NORMAL DEVELOPMENT
An understanding of typical development and participation patterns of
typically developing children underlies the planning of programmes in
which all children can flourish. Children gather information from people,
things and events in their environment. They organise this information in
their minds, and code it in ways that is meaningful to them, allowing them
to retrieve it when needed. They match new information with what they
have learnt before, noticing similarities and differences.
Crawling, walking, babbling, talking and following instructions are all
examples of developmental milestones. Sensory-motor development is the
pivot of early learning and may be described as hands-on or experiential.
New phrases such as “eyes-on” and “ears-on” can be coined. Consider the
experiences of not only babies and children but also of adults as they feel
and touch the world they move in and see and hear all that is about them.
These abilities form the developmental building blocks for thinking and
learning, and it follows that if one or more of them develop slowly or
atypically, learning will be compromised. Children’s development usually
follows a broadly predictable pattern. Developmental milestones refer to the
acquisition of skills (learning, communicating, moving, hearing, seeing and
interacting).
In the first part of this chapter, cerebral palsy, spina bifida and muscular
dystrophy will be discussed so as to highlight salient features that may
impact on participation patterns. Although the clinical features of each
condition differ markedly, from a classroom perspective they have a great
deal in common. The second part of the chapter will describe the effects of
physical disabilities in the classroom, and the kinds of support necessary to
create an environment in which these children can flourish. Frequently,
children with physical disabilities have associated cognitive,
communication, language, sensory and social challenges. Although problem
areas must be identified and addressed, it is important to once again
emphasise that the focus must remain on what the child can do and the
support needed to facilitate ongoing learning success.
10.3 SPECIFIC CONDITIONS
10.3.1 Cerebral palsy
10.3.1.1 What is cerebral palsy?
Cerebral palsy (or CP) is the most common physical disability (Mastropieri
& Scruggs, 2014). It is a condition resulting from injury to the developing
brain, and may occur before, during or after birth. The whole brain is not
damaged, only parts of it. Because cerebral palsy has so many different
forms, the terminology can be quite confusing. Think of it this way:
cerebral means concerning the brain, and palsy refers to movement
difficulties. In high-income countries, the incidence is approximately two in
1 000 live births, with little variation between countries (Hoon & Tolley,
2013). However, it is generally accepted that the incidence is higher in lowand middle-income countries, although the prevalence figure has not yet
been established (Beukelman & Mirenda, 2013).
Despite increases in neonatal intensive care practices during the past two
decades, the incidence figures have not significantly changed in highincome countries, resulting in the conclusion that most cases of cerebral
palsy in those countries are not due to complications of labour and delivery
(Cooper, 2015; Hoon & Tolley, 2013). In South Africa, however, the picture
is different. While accurate figures regarding the causes of cerebral palsy
are not known, the number of infants surviving complications at birth or
slightly thereafter, such as birth asphyxia with resulting neurological
damage, is likely to be substantially higher than that of high-income
countries (Cooper, 2015). Measures to ensure that effective healthcare of
mothers and babies are critical in order to address the high number of
children with cerebral palsy in South Africa as a result of complications
during labour and delivery.
Cerebral palsy is a group of disorders of the development of movement and
posture, causing activity limitation due to non-progressive disturbances that
occurred in the developing foetal or infant brain. The motor disorders are
often accompanied by disturbances of sensation, cognition, communication
and behaviour, by epilepsy, and by secondary musculoskeletal problems
(Rosenbaum, Paneth, Leviton, Goldstein & Bax, 2007).
10.3.1.2 How does it happen?
Often the cause of cerebral palsy is unknown but risk factors include
prematurity, low birth weight, exposure of the mother to infections such as
German measles (Hinchcliffe, 2007), part of the baby’s brain not
developing in utero, a blood clot (stroke), complications during labour
(Cooper, 2015), infections such as meningitis and encephalitis,
chromosomal abnormalities, head injuries, high fevers, near drowning, and
many more.
10.3.1.3 Is there a cure?
There is no cure. Although the brain damage is permanent, cerebral palsy is
not progressive, which means that the condition itself does not improve but
it also does not get worse. However, the clinical manifestations change with
time and therefore the impairments such as spasticity may increase and lead
to more severe functional limitations (Dambi, Jelsma & Mlambo, 2015). As
the child develops, the impact of the cerebral palsy may change – that is,
the spasticity (increased muscle tension/tone) may increase as more effort is
required in daily life, and contractures may form if the child does not
receive appropriate intervention. This may impact not only on motor skills
but also on the development of other skill areas. Managing the learning
environment by providing appropriate accommodations and supports will
enable the child to develop his unique potential.
10.3.1.4 What does it look like?
Children with cerebral palsy will not all be affected in the same way. Each
child will have unique characteristics related to the area and the extent of
the brain damage. To varying degrees, development of the cognitive,
language/communication, motor, sensory and social skills may be affected.
Many children with cerebral palsy experience significant activity
limitations and participation restrictions. Developmental milestones may be
delayed, and in severe cases never attained, for example a child with spastic
quadriplegia who never learns to walk.
DIFFERENT TYPES OF CEREBRAL PALSY
Teachers will be well aware that no two children with cerebral palsy are
alike. There are four main categories, which are described below:
In spastic cerebral palsy, children have high muscle tone and experience
stiffness, making movements slow, awkward and difficult, often resulting
in permanent joint contractures. With effort, the muscles become more
spastic, which can make activities of daily life all the more challenging
(Hinchcliffe, 2007). Because the muscle tone is high, the term hypertonic
is also frequently used. This makes up 60 per cent of the children with
cerebral palsy (Westling & Fox, 2009).
In dyskinetic cerebral palsy, children make involuntary movements, and
there can be changing patterns of muscle tone across the day (spasticity is
often more noticeable when they are awake or when they attempt a
specific movement, and decreased or normal when they are asleep)
(Beukelman & Mirenda, 2013). The involuntary movements can be
– slow and writhing, appearing to flow into each other – this is referred to
as athetosis or athetoid cerebral palsy
– rapid, random and jerky, in which case the movements are referred to
as chorea
– repetitive and twisting with a distorted posture, in which case they are
referred to as dystonia or dystonic cerebral palsy (Hoon & Tolley,
2013). Sometimes the muscle tone is low or hypotonic, which makes
up approximately 20 per cent of the cerebral palsy spectrum (Westling
& Fox, 2009).
In ataxic cerebral palsy, children have poor balance and make
uncoordinated, jerky movements, which is more noticeable when they
attempt to perform voluntary actions (Hoon & Tolley, 2013). They
experience great difficulty in controlling their hands and arms during
reaching or pointing – frequently overreaching and missing the target.
For children who can walk, their gait (walking pattern) is wide based and
unsteady. Muscle tone may be increased or decreased. This is a rare
condition and only accounts for approximately 1 per cent of children
diagnosed with cerebral palsy (Westling & Fox, 2009).
In mixed cerebral palsy, children have combinations of the above motor
patterns, without a dominant one, for example athetosis with spasticity
(Hoon & Tolley, 2013).
THE PARTS OF THE BODY AFFECTED
Hemiplegia. This term describes the physical involvement of the arm or
leg on one side of the body.
Diplegia. This term describes the physical involvement of both legs only.
Quadriplegia. This term describes involvement of both legs and both
arms.
All three of these body-part involvement patterns are shown in Figure 10.2.
Figure 10.2 Different parts of the body affected
WHAT SKILL AREAS ARE INVOLVED?
Cognitive skills. Cognitive impairments may be mild, moderate or severe.
Approximately one half of children with cerebral palsy present with
intellectual disabilities, and many with typical intelligence have some
degree of learning disability (Hoon & Tolley, 2013).
Communication skills. A high percentage of children with cerebral palsy
have complex communication needs related to oral control and/or the
development of speech and language.
Visual skills. Visual impairments are common and diverse in children
with cerebral palsy and include, among other things, strabismus (“lazy
eye” or squint), critical visual impairments and nystagmus (Hoon &
Tolley, 2013).
Hearing skills. Early identification is critical, as 30 per cent of children
with cerebral palsy have hearing problems (Hoon & Tolley, 2013).
Hearing loss will range from mild to profound, and is typically sensorineural (Tharpe, 2009)
Social skills. One of the cornerstones of school readiness is the young
child’s ability to interact socially. Children with cerebral palsy are no
different. The importance of social interaction is often overlooked as
other seemingly more important challenges are addressed. This often
results in the child either becoming withdrawn or exhibiting challenging
behaviours.
10.3.1.5 What are the challenges?
Stigma and social exclusion of children with cerebral palsy creates and
strengthens barriers against inclusion, participation and the uptake of
rehabilitative services (Mactaggart & Murthy, 2013).
Children with cerebral palsy frequently have multiple disabilities. There can
be primary sensory impairments, either to the somato-sensory system
(touch, pain, temperature and proprioception), the vestibular system
(balance and equilibrium), or vision and hearing. Even if there is no
primary damage to these systems, the motor impairment may affect daily
function; for example, poor head control will have a negative effect on the
development of visual tracking, constant fisting of the hand will impact on
the tactile development of the hand, and a paucity of movement and lack of
exploration will affect perception and learning.
ASSOCIATED IMPAIRMENTS
Approximately 40 per cent of children with cerebral palsy develop seizures
(Hoon & Tolley, 2013) and thus require medication. They are also
susceptible to respiratory infections. Feeding problems related to oral motor
and/or oral sensory problems may result in poor nutrition and failure to
thrive. These impairments may result frequent absenteeism.
LEARNED HELPLESSNESS
Lack of motivation or passivity is often a very real challenge for children
with cerebral palsy. This is partly due to the energy and effort required to
participate in living and learning, and partly because those around do too
much for them instead of with them (Beukelman & Mirenda, 2013). This
learned helplessness has a significant impact on levels of participation and
the development of independence.
PAIN
Many children with cerebral palsy experience pain every day, which may
affect their attention to and participation in schoolwork due to a variety of
reasons, for example musculoskeletal and gastrointestinal pain which is
associated with spasticity, and the inability to change from one position to
another. Sometimes, due to the communication difficulties of children with
cerebral palsy they cannot tell their teachers that they are in pain (Johnson,
Nilsson & Adolfsson, 2015). Teachers should therefore be on the lookout
for any possible signs of pain, for example by observing these children’s
body language, becoming aware of any behavioural changes, and being
sensitive towards any non-verbal and/or verbal messages. Teachers should
also be aware of the fact that if children do not complain about their pain,
this may not be because they are not experiencing it, but because they are
reluctant to try to communicate about something that had previously been
ignored (Johnson et al., 2015).
CHALLENGING BEHAVIOUR
Behavioural difficulties are common in children with cerebral palsy and
may in part be due to frustration because of limited functional abilities that
may adversely impact family and school life (Brossard-Racine et al., 2012).
Family and societal attitudes have a significant influence on behaviour, for
example overprotection, rejection, limited or unrealistic expectations,
isolation, and belief in witchcraft and other evil spirits.
Stop and reflect
“I took her to a traditional healer … after examining the child the healer told us that
she was encountered by a bad spirit. The healer came to our house many times. He
told us, if you sacrifice two pigeons, then your child will be fine. After I gave her the
pigeons, the healer applied witchcraft and gave her a talisman. But she did not
recover at the treatment of the healer. After that I took her to almost 20 to 30 healers.
All of them gave similar treatments, and it did not cure her.”
Parent, Bangladesh (Mactaggart & Murthy, 2013)
Children with cerebral palsy may have multiple disabilities for example
spastic quadriplegia, cognitive delays, and visual impairment, as well as
epilepsy, and consequently it is associated with multiple limitations and
restrictions in terms of participating in activities. This would necessitate a
wide range of accommodations and supports in order to provide
opportunities similar to those of their typically developing peers. Although
such children may be a source of joy to their parents, their special needs
may affect the physical, social and emotional health of the caregivers, their
wellbeing, as well as their employment and financial status (Dambi et al.,
2015). Such children may need wheelchairs and other adaptive technology
such as a communication devices and computers. This has implications for
teachers and parents in terms of developing their own knowledge and skill.
Teachers should also be able to pace the amount of energy certain activities
require, as children with cerebral palsy often tire more easily. In addition to
the educational needs of these children, they will often be receiving some
form of therapy, such as physio-, speech or occupational therapy, and in
such cases teachers should collaborate with these team members (Palisano,
Snider & Orlin, 2004). Classroom challenges pertaining to physical
disability will be discussed in the second half of this chapter.
10.3.2 Spina bifida
10.3.2.1 What is spina bifida?
Spina (spine) bifida (split) is an opening in the spine (vertebral column)
through which the spinal cord and its membranes may protrude. It comes
from the Latin words spina, which means thorn or spine, and bifida which
means split. The nerves coming out of the spine may be damaged, causing
loss of movement and sensation (feeling). The lower spine is more
commonly affected and the severity might range from very mild with no
neurological abnormalities to severe, in which cases the nerve supply to the
muscles of the legs, bowel and bladder are impaired in varying degrees
(Rodda, 2008). Typically, children with spina bifida present with
ambulation difficulties (walking and running) but with strengths in
language and social skills (Fletcher & Brei, 2010). The incidence of spina
bifida is five per 10 000 births worldwide. In Wales and Ireland, it is three
to four times higher, while the prevalence in Africa is much lower (Liptak,
2013).
10.3.2.2 How does it happen?
Spina bifida is a congenital disorder; in other words, a condition with which
the baby is born. The causes remain uncertain, but both environmental (e.g.
iodine or folic acid deficiency) and genetic factors play a role. The defect
happens within the first six weeks of pregnancy. As medical practitioners
have become increasingly aware of the importance of adequate folic acid
intake in pregnancy, this is one condition where there has been a dramatic
decrease in recent years (Liptak, 2013).
10.3.2.3 Is there a cure?
There is no cure but good antenatal care (an adequate folic acid
supplement) may reduce the risk of spina bifida. Hydrocephalus occurs in
60–95 per cent of children with spina bifida, and is caused by a build-up of
fluid around the brain (Liptak, 2013), which, if left untreated, will result in
brain damage (see Figure 10.3). To prevent this, a shunt is inserted in the
ventricle (the section of the brain that produces the fluid) to drain this
excess fluid into the abdominal cavity. This controls the build-up of
pressure that could cause further brain damage. Almost all shunts are
inserted in the first few weeks after birth – children who do not need a shunt
by the time they are five months old will probably never need one (Dias,
2016). Teachers should be on the lookout for any signs of an infected or
blocked shunt, as this could be life threatening. Warning signs include
vomiting, fever, headache, lethargy, irritability, drowsiness, inability to look
up, difficulty with handwriting and social withdrawal (Yaun, Keating &
Gropman, 2013). Teachers must alert the parents immediately if any of
these signs are noted.
Figure 10.3 Example of
the features of a child
with hydrocephalus
10.3.2.4 What does it look like?
The damage to the spine and spinal cord is present in one of three ways:
Spina bifida occulta. The opening on the infant’s back is usually covered
by muscle, skin and sometimes a tuft of hair but the spinal cord is in its
normal position so the child is unaffected by the condition (Rodda,
2008). Individuals with spina bifida occulta thus do not have
abnormalities visible on their back, a protruding spinal cord or any
symptoms (Liptak, 2013), therefore this condition is not included when
prevalence figures for spina bifida are calculated.
Spina bifida meningocele. This occurs when the meninges (the
membranes that cover the brain and spinal cord) push through the split
vertebra. The spinal cord is normal and other than surgery to ensure that
there is no further damage, the individual usually has no problems.
Spina bifida myelomeningocele. The baby is born with a fluid-filled sac
protruding from its spine, containing nerves and part of the spinal cord.
This is the most common and most severe form, occurring in 80–90 per
cent of all spina bifida births (Fletcher & Brei, 2010). These are the
children who need a great deal of support. An operation to push the
spinal cord back through the opening is necessary within the first couple
of days after birth to prevent further damage.
Figure 10.4 Example of a baby with spina
bifida myelomeningocele before
corrective surgery
There are a number of associated difficulties and medical complications
associated with spina bifida that may to some degree impact on a child’s
learning. The most noticeable is mobility impairment with some children
needing wheelchairs while others may manage with braces, crutches or
walkers. Owing to the lack of movement and weight bearing, some children
develop osteoporosis, making them prone to fractures. Muscle weakness
and/or paralysis, loss of sensation (the ability to feel pressure or
temperature) and obesity further increase their vulnerability. These children
are also susceptible to skin injury and pressure sores. They often have
impaired bladder and/or bowel control, resulting in incontinence, which
means that their ability to go to the toilet is affected and so they need a great
deal of support. These children will need to learn the skills to manage their
toileting routines because soiling, wetness and odour are socially and
emotionally very stressful. Intellectual disability and/or seizures (in
approximately 15 per cent of cases) as well as visual impairments may also
be a consequence of spina bifida (Liptak, 2013).
10.3.2.5 What are the challenges?
There are some challenges related specifically to spina bifida, and teachers
need to be aware of how to support these learners:
Managing bowel and bladder function. Most children with spina bifida
can be taught to use a catheter independently (clean intermittent
catheterisation), and teachers should plan classroom breaks to
accommodate such learners’ specialised toileting needs (Mastropieri &
Scruggs, 2014).
Ensuring that the child does not injure himself because of a lack of
sensation (or feeling). This is particularly true when the children are
outside in the playground.
Managing the varying levels of mobility. Some children with spina bifida
require mobility aids such as walkers, crutches and braces, while others
are wheelchair users, which means that the classroom space should be
arranged to ensure clear, wide, open walkways. Classroom challenges
applicable to children with physical disabilities will be discussed later in
the chapter.
Providing academic instruction at the appropriate level to match the
child’s intellectual development. Approximately three-quarters of
children with spina bifida have intellectual functioning within the typical
range (Liptak, 2013), but some have severe intellectual disabilities,
typically as a complication of an infected shunt. Despite their typical
intellectual development, they may have impairments in perceptual skills,
attention span, memory and organisational abilities.
Being aware of potential seizures (which is also a sign of a shunt that is
not functioning well). Such cases need to be referred.
Ensuring that the vision of a child with spina bifida is checked regularly.
Strabismus (“lazy eye”) is present in about 20 per cent of this population
and may require surgical correction (Liptak, 2013).
10.3.3 Muscular dystrophy
10.3.3.1 What is muscular dystrophy?
Muscular dystrophy (MD) is a genetic condition that affects the muscles
throughout the body. It is a progressive disease in which the muscles get
weaker and weaker over months and years. This weakness affects not only
gross and fine-motor function but also the heart and lung functions that
depend on healthy muscles to function normally. There are more than 30
types of MD that affect adults as well as children. In children the most
common form is Duchenne MD (Kang, 2013).
10.3.3.2 How does it happen?
Duchenne MD is a progressive skeletal muscle inherited disorder that rarely
affects girls (Kang, 2013). The gene (which is recessive) is carried by the
mother but she herself does not have the disorder. It is usually observed in
early childhood, and delayed walking and frequent falling are some of the
first symptoms.
10.3.3.3 Is there a cure?
There is no cure but the child should be kept active and independent for as
long as possible. Playing and learning with other children and being
included in family and community activities are vital. Early diagnosis is
essential to ensure better quality medical care, earlier genetic counselling
and improved rehabilitation, which all impact on quality of life and life
expectancy of children with Duchenne MD (Van Ruiten, Straub, Bushby &
Guglieri, 2014).
10.3.3.4 What does it look like?
Children (mostly boys) with Duchenne MD only begin to show signs of the
disease between two and six years of age. The first signs may be poor
balance, clumsiness and frequent falls. It may be difficult to get up off the
ground because of weakness of the thigh muscles. Muscle weakness first
affects the feet, thighs, trunk (body), shoulders and elbows, and later the
hands, face and neck muscles (Kang, 2013). (See Figure 10.5.)
Figure 10.5
Example of a
boy with
muscular
dystrophy
In Duchenne MD, the muscles in the arms, legs and hips become weaker
and weaker until walking is no longer possible. Usually between 10 and 12
years of age, they start losing their ability to walk independently, making a
wheelchair necessary (Kang, 2013). Kyphoscoliosis, an abnormal curve of
the spine and trunk, is common, which not only causes postural deformity,
but also pain, and increases the possibility for breathing and other
respiratory problems (Kang, 2013). Weakening muscles also cause severe
cardiac (heart) problems. Most children with Duchenne MD have average
intelligence, although intellectual disability is seen in about 30 per cent of
boys (Clark, 2008; Metwally, 2009). However, it should be noted that the
intellectual disability is not correlated with the severity of MD weakness.
Speech and language delays as well as challenging behaviour have also
been reported for this population (Van Ruiten et al., 2014).
In the past many of these boys did not survive to their late twenties, but
since the introduction of steroid treatment, ventilation practices and cardiac
support in the past decade, life expectancy has significantly improved (Van
Ruiten et al., 2014).
To summarise, Van Ruiten et al.’s (2014) acronym MUSCLE, suggested for
doctors, was adapted to help teachers remember the key characteristics:
M Motor milestone delay
U Unusual gait
S Speech delay
C Challenging behaviour
L Leads to
E Early diagnosis – with a more successful outcome
10.3.3.5 What are the challenges?
The main challenge for these children and their families is that Duchenne
MD leads to a loss of functional independence, and deterioration in the
individual’s and the family’s quality of life. Traditionally, intervention has
focused on medical management of the heart and lung function as well as
physical management by physio- and occupational therapists. They helped
parents and teachers manage the ever-changing condition by keeping
muscles as strong as possible for as long as possible, keeping tendons (e.g.
the Achilles tendon) from tightening (developing a contracture) by
stretching and/or using special splints or braces, doing regular but not
strenuous exercise, and doing breathing exercises.
Currently, it is considered best practice to focus on participation in activities
of personal care, mobility, social relationships, education, recreation and
leisure, spirituality, and community life (Bendixen, Senesac, Lott &
Vandenborne, 2012). It is important for self-esteem and independence to
encourage these learners to do everything for themselves for as long as
possible. Owing to the progressive nature of the disease, it is important that
the teacher, together with the parents and therapists, anticipates and plans
the type of support the learner may require during the course of the year
(Mastropieri & Scruggs, 2014). For example, these children may tire more
easily than their peers, and may require rest breaks throughout the day.
10.4 SUPPORTING CHILDREN WITH PHYSICAL
CHALLENGES IN THE CLASSROOM
10.4.1 Classroom ethos
As discussed in Chapter 1, teachers are role models and as such will set the
tone for the way others, especially children, interact with one another.
Although the following tips for teachers focus on interaction with children
in wheelchairs, they are powerful examples of core teaching values:
Freedom. Do not assume that a child in a wheelchair or one who uses
crutches or a walking frame cannot do things because of these mobility
aids. In actual fact they give the child freedom – they are enablers, not
disablers.
Intelligence. Do not assume that an individual in a wheelchair has an
intellectual disability. Speak to him as you would to any other child.
Providing assistance. Be sensitive to the amount of help provided.
Always ask a child if he would like assistance. How and when help is
needed should be in the child’s control.
Conversations and discussion. Speak to the child directly. Get down to
his eye level. Resist the temptation to talk over the child to another
person, for example someone pushing the child, his parents or facilitator.
Clear paths. Make sure that there is always space to manoeuvre a
wheelchair or walker.
Do not be patronising. There is no need to pat a child on the head or
shoulder when walking past or talking to him. Wheelchair users
frequently perceive the wheelchair as an integral part of themselves, so
avoid leaning or hanging on the chair.
Compliments. Be ready to compliment the child with a ready smile for a
trendy haircut, a new school bag, and so on. Of course, for it to be sincere
the reverse is also applicable and a reprimand would be appropriate in
certain circumstances, for example rudeness, not taking care of
belongings, being mean, etc.
Independence. Children may need assistance with some activities such as
opening a door, getting on and off a bus, toileting activities, etc. Ensure
this is done in a dignified manner. As far as possible let the child be an
active participant in the process. Being in charge is a vital component of
developing independence. Be careful not to burden the child with things
that he may not be able to do himself.
Planning. Anticipate the requirements of the child in a wheelchair and if
necessary change the plan. The true story below illustrates what can
happen when a teacher knows what she wants.
Stop and reflect
Mrs Brown was planning an outing to a farm for her Grade 6 class. She made the
arrangements and then mentioned that one of her students, Zodwa, was in a
wheelchair.
“I’m sorry,” said the farm manager “She won’t manage the terrain in the farmyard but
she can come along and sit under the shade of our lovely oak tree and wait for her
classmates.” “In that case,” said Mrs Brown, “we won’t be coming. I’ll take the
children somewhere else.” There was a hushed silence at the other end of the phone
as the kindly manager thought about what Mrs Brown had said. “Wait a moment,” he
said. “Let me think about this. Mmm, yes, I know what we can do. We have a tractor
and a sturdy trailer. If the children bring cushions to sit on we can take them around in
the trailer. There are some strong men on the farm who will help lift your young lady
on and off the trailer.”
Mrs Brown smiled to herself and said: “Thank you very much. ALL the children will
enjoy that. See you next Friday.”
10.4.2 Seating and positioning
Initially, the most critical factor in the classroom management of children
with physical disabilities is to ensure correct seating and positioning so that
they can concentrate and focus on learning. Head control, stability of the
trunk (body) and hand function are intricately linked. For all children with
physical disabilities, proper seating and positioning have many benefits,
such as increasing the child’s stability, control and range of movement. This
also helps to prevent pressure sores, increases comfort and decreases fatigue
(Hoon & Tolley, 2013). The responsibility for positioning often becomes
that of the teacher and the parent. In well-resourced schools there may well
be physio- and occupational therapists involved but even then the teacher is
in the best position to inform decisions regarding classroom seating and
positioning.
Stop and reflect
The most useful hands-on resource for positioning is the book Disabled village
children by David Werner (2009). It is freely available online, and Chapter 65 is a
comprehensive and well-illustrated guide. The practical advice is equally relevant for
children in urban, rural, well- or under-resourced settings.
Positioning has two equally important components:
How the child is positioned, for example seated in a corner seat on the
floor or in a wheelchair with an insert, or standing in a standing frame
Where the child is positioned in the classroom and during other activities
so that he is always an active participant
10.4.2.1 Seating and other adaptive equipment
Children must be well seated so that they have a stable base from which to
function, for example looking at the blackboard, drawing, writing and using
technology. Furthermore, if a child is placed in the correct position, the
effects of abnormal muscle tone can be minimised, for example to reduce
tone where there is spasticity or hypertonia, and to increase tone where
there is hypotonia or low tone (Hinchcliffe, 2007). Often all this requires is
that the table and chairs are at the correct height and size for each child.
Children with severe physical disabilities frequently require additional
support. However, the basic principles of seating as shown in Figure 10.6
are the same for all children:
A well-supported upright position facilitates upper-extremity functioning
for fine motor tasks as well as for reaching and accessing high- and low-
tech devices (Stavness, 2006). It also reduces the amount of physical
energy required to engage in a task.
The angles of the hips, knees and feet must be 90 degrees. The seat
should be firm so as to provide support for the thighs and a symmetrical
posture. Ensuring the correct size chair or wheelchair is a priority.
A lap strap can be used if necessary to keep the hips at 90 degrees. This
will also give the child a sense of stability and security.
The feet must be flat on the floor or on the footplates of a wheelchair.
Sometimes it is necessary to secure the feet or ankles with a strap to
maintain the symmetrical posture.
The elbows and forearms must rest comfortably on the desk, table or lap
tray (a cut-out working surface) without having to hunch the shoulders.
The head should be upright with the chin tucked in. With children with
severe physical disabilities, this often necessitates some form of headrest
or support.
Figure 10.6 Example of a comfortable, functional position for the classroom
Sitting balance can only be considered functional if the child has head
control and can use his hands freely for activities such as joining in the
actions of a song, painting, writing, using a computer or communication
device, and so on. If special seating is needed, ensure that it is child friendly
and attractive. This can make a big difference to how the child and his
family accept and make use of it. For a child with poor sitting balance, the
use of a lap strap angled snugly across the hips may be all that is needed
(see Figure 10.7).
Figure 10.7 Example of a lap
strap that provides sitting
balance
Should more support be needed, an H-strap may work well. This looks like
a bib with one set of straps keeping the hips in position as before and the
other two going over the shoulders for additional support. This is much
better than tying a strap around the child’s waist/chest. In addition, it may
be necessary to provide head support by either lengthening the back of the
chair or using a headrest. Strategies such as tilting the whole chair
backwards ± five degrees may be appropriate.
A surface on which a learner can work or play is very important. For
children who are in a wheelchair most of the time, a lap tray is essential
(see Figure 10.8). This not only contributes to postural stability as
discussed, but can also be used for functional activities throughout the day.
A lip or edge around the tray will prevent things such as toys and pencils
from rolling off.
Figure 10.8 Example of a lap tray
that provides a working surface
The degree of support will depend on the demands of a specific activity.
When engaged in academic activity, the child should be given maximum
support so that his attention is fully focused on the learning task. There may
be other times such as in the playground or maybe during story time when
the amount of support is decreased and the child can practise sitting balance
and so develop his postural control. It is important that the child does not sit
in one position all day. Changing position will provide opportunities for
developing motor control and at the same time decrease the possibility of
contractures (stiffening of joints) (Palisano et al., 2004). Sitting, standing,
lying, and so on, may be beneficial, but many children will need assistance
in moving from one position to another.
10.4.2.2 Where the child is seated or positioned
The principles for seating a child are universal. All children should be able
to see, hear and move. Some guiding questions:
What positions do typically developing peers use when engaging in a
similar activity? For example, if young children sit on the floor when the
teacher reads stories during circle time, the child with the physical
disability should also be on the floor in a supported position rather than
in a wheelchair (Downing & Demchak, 2008).
Do the planned positions allow for interactions with peers? For example,
a child in a standing frame is at a disadvantage during circle time if all
the other children are on the floor.
Is the child able to get in and out of the classroom easily? For example, a
child in a wheelchair is usually best positioned near the door of the
classroom.
Is the positioning of a child with an assistant or facilitator such that they
do not distract other learners?
10.4.3 Lifting
Very often, children with severe physical disabilities need help to move
from, for example, a wheelchair to a regular chair or the toilet. This requires
planning and skill. Werner (2009) cautions that a child who needs to be
lifted is not a sack of potatoes (see Figure 10.9). The inference is that
children are often handled that way – bundled around and tied (often with
the best of intentions) to chairs or other adaptive equipment.
Figure 10.9 A child
should not be handled
like a sack of potatoes
The old saying that prevention is better than cure is particularly relevant in
this context. Teachers, parents and indeed all those who share lives with
children with physical disabilities should learn to lift correctly so as not to
injure them or hurt their own backs. Children should never be left in one
position for the whole day. Independent or aided movement is an integral
part of learning and wellbeing.
The following golden rules for lifting children have been compiled from
Westling and Fox (2009) and Orelove, Sobsey and Silberman (2004), and
are shown in Figure 10.10:
The child must always feel secure and respected.
Care should be taken not to hurt the child.
The child should help as much as he can in the process of moving from
one place to another (transferring). The adult should communicate the
plan of action clearly and work at the child’s pace. Initially, the teacher
may have to plan the moves but can work towards saying: “How are you
planning to get from A (e.g. the wheelchair) to B (e.g. the floor)?”
If the child is heavy or has uncontrolled movements, it is always better to
have two people lifting. The movement must be planned and coordinated,
for example: “One, two, three … LIFT!”
The “lifter” must have a stable support base, with feet placed flat on the
floor and wide apart.
The strength of the legs must be used by bending and straightening the
hips and knees while keeping a straight, slightly arched back.
If possible, the child should be held close to the lifter’s body so as to
bring the child’s weight towards the lifter’s centre of gravity. Lifting
should never be done with a twisting movement, as the uneven weight is
likely to cause back strain.
Figure 10.10 Examples of correct and incorrect lifting patterns
10.4.4 Accommodations
Supporting children with physical disabilities requires knowledge, skill and
creativity not only from the teacher but also from the collaborative team.
Chapter 3 highlights some of the assessment accommodations that are
appropriate for children with physical disabilities. Bearing in mind that the
processes of assessment and learning, as described in the participation and
learning model in Chapter 2, are seamless, it follows that many of the
accommodations used in assessment will also be appropriate in classroom
settings, and vice versa. Some of these strategies are particularly relevant
for children with physical disabilities, for example:
Presentation. Position learning materials where the child can see and
reach them; paper and books may be held in place by a clipboard, nonslip mat, Prestik, Velcro, and so on.
Response. Physical difficulties may necessitate that a child uses a
multiple-choice format; a scribe may record verbal responses, or record
the responses the child may make by pointing, eye gaze or technology
Setting. It may be necessary for bigger classrooms to be assigned to
groups in which there are children who have difficulty moving around,
for example those using wheelchairs and walkers, or those with visual
impairments.
Timing or scheduling. Physical challenges may require extra time to
complete tasks and/or frequent breaks.
As an individual learns and grows, some of the accommodations may no
longer be necessary, while new ones may be introduced to facilitate
ongoing participation in the learning process.
10.4.5 Assistive technology
The term assistive technology (AT) describes any technology that enables
individuals to perform tasks that are difficult or impossible because of
disabilities; in other words any aid which facilitates functional capabilities
(Bornman, 2011). Children with physical disabilities very often need a
range of assistive devices, including both low-tech ones (adapted equipment
such as built-up grips for writing implements, communication boards and
adapted books) and high-tech ones such as switches, communication
devices, powered wheelchairs and environmental controls (Copley &
Ziviani, 2004). Technology needs to be carefully matched to the needs and
capabilities of a specific child. Teachers, therapists, parents and learners
must all be involved, not only in the process of selecting appropriate
technology but also in determining when and where it will be used.
Important considerations are, first, to match the abilities of the learner to the
demands of the technology; second, to ensure that the skills can be used in
different contexts, for example an adapted computer keyboard that could be
used with a communication device or a computer; thirdly, to obtain some
measure of immediate success; and, finally, to minimise the demands on
both gross and fine motor systems. If a learner has to consciously think
about maintaining balance or holding a pencil, he will be distracted from
the more important task of learning.
Stop and reflect
As a result of a serious car accident, Mr Botha’s ten-year-old son, Danie, has lost the
ability to walk and talk, and his fine motor coordination has been impaired. Mr Botha
has taken his son to the Centre for Augmentative and Alternative Communication
(CAAC). After a thorough assessment, the CAAC team recommends a
communication device that will help young Danie. This device consists of an adapted
keyboard on which he can type what he wants to say and the device will “speak” for
him. There is only one problem – the device is programmed to speak with an
American accent. Mr Botha listens while his son test drives the device and then blurts
out: “I will never have an American accent in my house!”
It is then back to the drawing board for Danie, his dad and the team as they look for
an acceptable alternative.
It cannot be emphasised strongly enough that when selecting assistive
technology, buy-in is required from the individual, his family and their
support systems. Learning to use technology is like learning to play a
musical instrument. The more you practise the better you become. If you do
not practise, the assistive device may well land up on the scrapheap.
However, the benefits of using technology far outweigh the effort involved.
Two comprehensive studies about the use of assistive technology in the
classroom found that it facilitates independence, which includes the
development of autonomy and self-determination. This again impacts
positively on making choices and taking control of one’s own care. Other
outcomes reported in these studies include enhanced social interaction, and
increased motivation and self-esteem (Copley & Ziviani, 2004).
Consider how many times a typically developing toddler will practise a skill
before it is mastered. Children with physical disabilities need ongoing
support in mastering technology (Almqvist, Uys & Sandberg, 2007). Much
of what children learn is from watching others (incidental learning). So, for
example, if the child is learning to use a communication board by pointing
at the pictures or text, this will not become a functional skill unless the
communication partners (parents, teachers and peers) model its use – that is,
use the same means to communicate. Think about it – this is how toddlers
learn to speak. Even when their words are indistinct, they carry meaning.
Similarly, the speech of children with physical disabilities does not have to
be clear in order to be understood. The same principle applies to the use of
sign language or gestural systems. The motor signs do not have to be
perfect for the meaning to be understood.
10.4.6 Literacy and low technology
Teachers need no persuading about the importance of developing literacy
skills for typically developing children. However, there are still some
commonly held beliefs that children with severe intellectual and/or physical
challenges will never learn to read and write, or that only computers will
solve the problem. Pre-literacy opportunities such as being read to and
manipulating writing implements, for example drawing and scribbling, are
critical. It is not unusual for a child with a significant disability to go to
school having had few, if any, experiences of engaging actively with the
tools of literacy, and the expectation is that the teacher will do it all.
Low-tech adaptive equipment can be very effective. For example, books
can be adapted in order to make them more accessible for children with
physical disabilities, as shown in Table 10.1. For example, books with
thicker pages can be used, and turning the pages of a book can be made
easier by sticking a piece of foam onto the corners of the pages, or by using
concrete pictures and/or real objects as well as detachable Velcro symbols.
Table 10.1 Easy book adaptations
Thicker pages with pegs and ice-cream
sticks to facilitate easier paging
Enhance understanding by using concrete
pictures and real objects
Use detachable symbols with Velcro
attachments
Tactile book with Braille and detachable
symbols
Being able to scribble, draw and write may require adapting writing
implements, for example splints with pencil attachments, modified pencil
holders, fat pencils or pens, and differently shaped pencils. Figure 10.11
shows a variety of possible adaptations.
Figure 10.11 Example of
adaptations that can be used
with pens and pencils
10.4.7 Literacy and high technology
A wide variety of adaptations that enable children with physical disabilities
to operate computers and/or communication devices is available. Examples
include switches, standard keyboards with enlarged keys, key guards, largemembrane keyboards, touch screens, head-controlled access devices,
predictive texting, and software that supports spelling, content and grammar
as well as voice recognition.
Modified digital texts are also now available, such as e-books or slide
presentations (e.g. using PowerPoint) as laptops and tablets are becoming
more freely available in classrooms (Hanreddy, 2015). For example, if a
book is set up as a slide show, a child with a severe physical disability can
use a single switch to move to the next page – providing a sense of
independence in this literacy activity. Teachers should, however, be careful
to select the visual images carefully so that they are meaningful to the child
(e.g. some cartoonlike images are too abstract), or some pages might
become visually overwhelming (e.g. if children have difficulty in
differentiating between the foreground and the background).
Although high-tech interventions are very powerful, there is a growing
recognition, even in high-income countries, that low-tech options are
equally important (Bornman, 2011). For example, a child with physical
disabilities may enjoy playing cards on the computer but when he is out
with friends he may need a card holder, as shown in Figure 10.12. The
game may also be adapted by pairing the child with a typically developing
peer. Peer support strategies form an integral part of the inclusion process.
Figure 10.12 Example of a card holder
10.4.8 Play
The presence of a physical disability limits a child’s potential for play – and
play has often been described as the work of the child (Almqvist et al.,
2007). These children often also do not know how to play, because there is
little modelling in terms of how to play with adapted toys (e.g. rather than
playing ten-pin bowling in the traditional way, it can be played by using
suspended toys, as shown in Table 10.2). Sometimes parents and teachers
also have expectations that are either too high (and therefore children never
experience success) or too low (and therefore they are not challenged to
perform). Children with physical disabilities may also have difficulty in
exploring toys and activities as well as interacting with the play material
and eventually mastering the skills. There might also be limited
opportunities to play with peers, and therefore teachers need to deliberately
create opportunities for interaction (Downing, Hanreddy & PeckhamHardin, 2015).
A number of additional ideas to create adapted toys suitable for children
with physical disabilities are shown in Table 10.2. The most important
consideration should be that play remains playful and that toys do not
simply become vehicles for work, particularly for younger children
(Beukelman & Mirenda, 2013).
Table 10.2 Adapting toys for children with physical disabilities
Brightly coloured toys
and noise-makers can
be suspended from a
clothes dryer.
Enlarge the surface of the knobs
on a form board by using pegs to
facilitate easier grip.
Suspend the toy with a
spring to ensure that the
toy can move but remains
within reach.
Use battery-operated
toys with large
switches.
Use a universal cuff with a
magnet attached to the tip, and a
metal thumbnail inserted into the
wooden puzzle pieces.
Use a baking sheet with
magnetic toys as raised
edges help children with
poor motor functioning.
10.4.9 Peers
For children with physical disabilities, access to the general curriculum
provides many opportunities for peer interaction. It makes peer instruction
mutually beneficial, for example a learner with disabilities tutoring a
typically developing peer, or vice versa (Beukelman & Mirenda, 2013).
Westling and Fox (2009) suggest two distinct roles for peer involvement:
peer tutoring and peer interaction. Peer tutors volunteer to help with
academic work, whereas peer interaction volunteers interact in fun and
leisure activities. The ultimate role of a peer without a disability is to be a
true friend to the learner with the disability (Downing & Eichinger, 2008).
Fostering peer relationships for learners with multiple disabilities is a
cornerstone of inclusive education. Initially these programmes have to be
carefully structured but if successful will, as the learners develop
meaningful relationships, gather a momentum of their own. The peer
support network can make a huge contribution in terms of brainstorming
how to include learners with disabilities, as they are the ones in touch with
what’s in and what’s out at their stage. Strategies for facilitating peer
interaction include the following:
Information and friendship programmes. Although friendships cannot be
specifically taught, they can be encouraged by ongoing getting-to-knowyou sessions to familiarise classmates with the learner with the disability,
his abilities and how to interact with him, as well as the areas in which he
needs support, for example ensuring that items or choices are within
reach (Downing & Eichinger, 2008). The process could, for example,
also include learning a gestural system or becoming familiar with the
features and functional use of high- and low-tech equipment. Interactive
exchanges are encouraged using games, toys and interactive computer
games.
Introduction of a buddy system or special friends programme. In such a
programme, a classmate is assigned specific “helping” activities in and
around the classroom and the school. The long-term aim is to develop
mutually rewarding long-term relationships beyond the confines of the
school.
Academic support. Typically developing peers could, for example, make
carbon copies or photocopy notes, or help set up a computer.
Provision of opportunities for interaction. The teacher identifies and
encourages activities that foster joint activities, for example card games,
computer games and selling cold drinks at a sports match.
Teacher mediation. The teacher models the patterns of interaction and
teaches classmates how to interact with and respond to the learner with
disabilities. She can introduce strategies that the learner with disabilities
can use to engage his classmates. For example, a learner in a wheelchair
who has difficulty speaking can always have a joke card on his lap tray:
face up the card may say: “What did the shark have for supper?” The flip
side gives the answer: “Fish and ships.”
Peer-mediated intervention. Short training sessions can provide
classmates with knowledge and skills to build relationships. For instance,
the peer buddy may want to include a group of friends in a game that
involves two sides. When picking the team he ensures that the learner,
even if he is not very good at the game, is not chosen last and so builds
his self-esteem.
Peer support networks are a central aspect of all children’s lives. The
development of hierarchal relationships – that is, where the typically
developing peer is always the leader – should be avoided. Children with
disabilities should be given equal opportunities to help others, for example
assisting with computer work or teaching a new game.
Peer support networks can definitely lighten the teacher’s load. There are
times, however, when a learner may need more assistance and then the help
of a dedicated classroom assistant should be considered.
10.4.10 Classroom assistants or facilitators
Inclusive education requires innovative strategies to ensure its success. One
such strategy is the use of classroom assistants or facilitators for individual
children who are unable to manage at school, even with the support of
teachers and peers (Beukelman & Mirenda, 2013). Their job description
will depend on the needs of the learner and may include one or more of the
following:
Providing physical assistance, for example helping a child move around
the school buildings, sports facilities and playgrounds
Helping the child understand the lesson by working on adapted
programmes with him
Setting up technology
Helping the child to use the technology
Encouraging the formation of peer relationships
There will always be times when the facilitator must withdraw and let the
child do a manageable task on his own. At times like this the teacher can
get the facilitator to help another child or do some other jobs around the
classroom. This process needs to be very carefully managed by the teacher.
If the facilitator does everything for the child, she will encourage learned
helplessness (Beukelman & Mirenda, 2013). If she does not do enough, the
child may well not reap the benefits of being included.
Sometimes teachers feel very uncomfortable or threatened by the presence
of a facilitator in the classroom. It could be that the facilitator is critical of
the teacher or has difficulty working under authority. The line of authority
has to be firmly established. The teacher is in charge.
Funding a facilitator is still a contentious issue. Facilitators are usually
employed by parents, and this may also cause some tension if the parents
and teachers are not in agreement about how best to support the child. In
South Africa most facilitators hold no formal qualifications. This is partly
because of the cost of employing a qualified person, for example a teacher
or therapist, and partly because it is really a very new field of work. The
lack of qualifications or experience may mean that the teacher often finds
herself having to train the facilitator.
10.5 CONCLUSION
This chapter discussed the most significant issues pertaining to children
with physical disabilities and the support they may require in inclusive
settings. The focus throughout was on treating the learner with respect, and
facilitating full participation. The critical role of peer interaction was
explored and the basics of positioning and lifting, and the role of assistive
technology was discussed. It is clear that although the teacher should be
knowledgeable about specific conditions, the focus should remain firmly on
the provision of appropriate accommodations and support to enable
meaningful participation. It is only partly about muscle tone and movement,
positioning and lifting, accommodations and support. More importantly, it
is about enabling children to experience the joy of friendships and the
excitement of learning, and giving them wings to fly.
REFERENCES
Almqvist, L., Uys, C.J.E. & Sandberg, A. 2007. The concepts of participation, engagement and flow:
a matter of creating optimal play experiences. South African Journal of Occupational Therapy,
37(3): 8–13.
Bendixen, R.M., Senesac, C., Lott, D.L. & Vandenborne, K. 2012. Participation and quality of life in
children with Duchenne muscular dystrophy using the International Classification of Functioning,
Disability, and Health. Health and Quality of Life Outcomes, 10(1)). doi: 10.1186/1477-7525-10-43
Beukelman, D.R. & Mirenda, P. 2013. Augmentative and alternative communication. Supporting
children & adults with complex communication needs, 4th ed. Baltimore, MD: Paul H. Brookes.
Bornman, J. 2011. Low technology. In Wendt, O., Quist, R.W. & Lloyd, L.L. (Eds). Assistive
technology. Principles and applications for communication disorders and special education. Bingley,
UK: Emerald Press.
Brossard-Racine, M., Hall, N., Majnemer, A., Shevell, M.I., Law, M., Poulin, C. & Rosenbaum, P.
2012. Behavioural problems in school-age children with cerebral palsy. European Journal of
Paediatric Neurology (EJPN): Official Journal of the European Paediatric Neurology Society,
16(1): 35–41.
Clark, A. 2008. Muscular dystrophy. Available at:
http://kidshealth.org/parent/medical/bones/muscular_dystrophy.html (accessed on 17 February 2009).
Cooper, P. 2015. Cerebral palsy in SA: perinatal factors and later neurological handicap in infants
born at or near term. South African Journal of Child Health, 9(4): 107.
Copley, J. & Ziviani, J. 2004. Barriers to the use of assistive technology for children with multiple
disabilities. Occupational Therapy International, 11(4): 229–243.
Dambi, J.M., Jelsma, J. & Mlambo, T. 2015. Caring for a child with cerebral palsy: the experience of
Zimbabwean mothers. African Journal of Disability, 4(1), Art. 168, 10 pages. Available at:
http://dx.doi.org/10.4102/ajod.v4i1.168
Dias, M.S. 2016. Hydrocephalus and shunts. Spina Bifida Association National Resource Center.
Available at: http://spinabifidaassociation.org/wp-content/uploads/2015/07/Hydrocephalus-andShunts1.pdf
Downing, J.E. & Demchak, M.A. 2008. First steps: determining individual abilities and how best to
support students. In Downing, J.E. (Ed.). Including students with severe and multiple disabilities in
typical classrooms: practical strategies for teachers, 3rd ed. Baltimore, MD: Paul H. Brookes.
Downing, J.E. & Eichinger, J. 2008. The important role of peers in the inclusion process. In
Downing, J.E. (Ed.). Including students with severe and multiple disabilities in typical classrooms:
practical strategies for teachers, 3rd ed. Baltimore, MD: Paul H. Brookes.
Downing, J.E., Hanreddy, A. & Peckham-Hardin, K.D. 2015. The general education classroom: a
rich communicative environment. In Downing, J.E., Hanreddy, A. & Peckham-Hardin, K.D.
Teaching communication skills to students with severe disabilities, 3rd ed. Baltimore, MD: Paul H.
Brookes.
Fletcher, J.M., & Brei, T.J. 2010. Introduction: spina bifida – a multidisciplinary perspective.
Developmental Disabilities Research Reviews, 16(1): 1–5. Available at:
http://doi.org/10.1002/ddrr.101
Hanreddy, A. 2015. The relationship between communication and literacy. In Downing, J.E.,
Hanreddy, A. & Peckham-Hardin, K.D. Teaching communication skills to students with severe
disabilities, 3rd ed. Baltimore, MD: Paul H. Brookes.
Heckman, J. 2006. Skill formation and the economics of investing in disadvantaged children.
American Association for the Advancement of Science, 1900–1902.
Heckman, J.J., Stixrud, J. & Urzua, S. 2006. The effects of cognitive and noncognitive abilities on
labor market outcomes and social behavior. Journal of Labor Economics, 24(3): 411–482.
Hinchcliffe, A. 2007. Children with cerebral palsy: a manual for therapists, parents and community
workers, 2nd ed. New Delhi: SAGE.
Hoon, A.J. & Tolley, F. 2013. Cerebral palsy. In Batshaw, M.L., Roizen, N.J. & Lotrecchiano, G.R.
(Eds). Children with disabilities, 7th ed. Baltimore, MD: Paul H. Brookes.
Johnson, E., Nilsson, S. & Adolfsson, M. 2015. Eina! Ouch! Eish! Professionals’ perceptions of how
children with cerebral palsy communicate about pain in South African school settings: implications
for the use of AAC. Augmentative and Alternative Communication, 31(4): 325–335 Available at:
http://dx.doi.org/10.3109/07434618.2015.1084042
Kang, P.B. 2013. Muscles, bones and nerves. In Batshaw, M.L., Roizen, N.J. & Lotrecchiano, G.R.
(Eds). Children with disabilities, 7th ed. Baltimore, MD: Paul H. Brookes.
Liptak, G.S. 2013. Neutral tube defects. In Batshaw, M.L., Roizen, N.J. & Lotrecchiano, G.R. (Eds).
Children with disabilities, 7th ed. Baltimore, MD: Paul H. Brookes.
Mactaggart, I. & Murthy, G. 2013. The Key Informant Child Disability Project in Bangladesh and
Pakistan: Main Report 2013. International Centre for Evidence in Disability, London School of
Hygiene and Tropical Medicine.
Mastropieri, M.A. & Scruggs, T.E. 2014. The inclusive classroom: strategies for effective instruction,
5th ed. New Jersey: Merrill Prentice Hall.
Metwally, Y. 2009. Duchenne muscular dystrophy. Eneurology. Available at:
http://yassermetwally.com/blog/?p=64
Muscular Dystrophy Foundation of South Africa. n.d. Available at: http://www.mdsa.org.za
(accessed 25 February 2009).
Orelove, F.P., Sobsey, D. & Silberman, R.K. (Eds). 2004. Educating children with multiple
disabilities: a collaborative approach, 4th ed. Baltimore, MD: Paul H. Brookes.
Palisano, R.J., Snider, L.M. & Orlin, M.N. 2004. Recent advances in physical and occupational
therapy for children with cerebral palsy. Seminars in Paediatric Neurology, 11(1): 66–77.
Rodda, J. 2008. Aspects of spina bifida. Presentation at the SAALED Congress: From Inclusion to
Belonging: Widening the Classroom Circle, Bryanston, Johannesburg.
Rosenbaum, P., Paneth, N., Leviton, A., Goldstein, M. & Bax, M. 2007. A report: the definition and
classification of cerebral palsy, April 2006. Developmental Medicine and Child Neurology, 49(2): 8–
14.
Stavness, C. 2006. The effect of positioning for children with cerebral palsy on upper-extremity
function: a review of the evidence. Physical & Occupational Therapy in Paediatrics, 26(3): 39–53.
Tharpe, A.M. 2009. Individuals with multiple disabilities. In Katz, J., Medwetsky, L., Burkard, R. &
Hood, L. (Eds). Handbook of clinical audiology, 6th ed. Philadelphia: Wolters Kluwer – Health.
Van Ruiten, H.J.A., Straub, V., Bushby, K. & Guglieri, M. 2014. Improving recognition of Duchenne
muscular dystrophy: a retrospective case note review. Archives of Disease in Childhood, 99(12): 1–4.
doi:10.1136/archdischild-2014-306366
Werner, D. 2009. Disabled village children: a guide for community health workers, rehabilitation
workers and families, 2nd ed. Palo Alto, CA: Hesperian Foundation.
Westling, D.L. & Fox, L. 2009. Teaching students with severe disabilities, 4th ed. Columbus, OH:
Merrill Prentice Hall.
World Health Organization (WHO). 2001. International Classification of Functioning, Disability
and Health (ICF). Available at: http://www.who.int/classifications/icf/en/
Yaun, A., Keating, R. & Gropman, A. 2013. The brain and nervous system. In Batshaw, M.L.,
Roizen, N.J. & Lotrecchiano, G.R. (Eds). Children with disabilities, 7th edition. Baltimore, MD: Paul
H. Brookes.
11
Understanding children with
sensory disabilities
11.1 INTRODUCTION
Children rely on all their senses to explore and learn about the world.
Traditionally, the focus was on the five primary senses described by
Aristotle, (namely hearing (the auditory system), seeing (the visual system),
touching (the tactile system), smelling (the olfactory system) and tasting
(the gustatory system)), but during the past decade this has shifted to
sensory integration. Sensory integration refers to the brain receiving,
interpreting and organising input from all of the active senses and from the
environment, and making it possible to use the body effectively within the
environment. One should therefore include the vestibular system and the
proprioception system, and focus on all seven senses.
The vestibular system provides information about the body in relation to
gravity, movement and balance. It measures acceleration, g-force, body
movements and head position (Proske & Gandevia, 2012). Being aware that
we are moving when in an elevator, knowing whether we are lying down or
sitting up, and being able to walk on a balance beam are all examples of the
vestibular system at work.
Proprioception is the sense of the relative position of adjacent parts of the
body (in other words where and how we are positioned without looking at
our body parts) and the amount of effort needed to plan and execute
movements (Proske & Gandevia, 2012). For example, being able to clap
our hands with our eyes closed, write with a pencil and apply the correct
pressure, and navigate through a narrow space are examples of our
proprioceptive system at work.
However, the focus of this chapter is on the two distance senses (i.e. seeing
and hearing) that enable individuals to monitor what occurs in the world
around them; however, this does not negate the vital role the other senses
play in daily life. Consider the experience of touch and touching: the child
being held (touched) by his mother or feeling (touching) different textures
such as the softness of a blanket or the roughness of sandpaper. Consider
too the significance of the sense of smell: the danger of fire approaching,
the inviting aroma of bread baking and the sweet scent of a flowering tree.
Experience tastes that explode in the mouth: the sweetness of honey, the
sourness of lemons, the burning of chillies and the bitterness of unripe fruit.
These images conjure up the rich tapestries of our lives.
Figure 11.1 Sensory systems
There are three sections in this chapter. The first will deal with children
with a hearing disability, the second with children with a visual disability
(low vision), and the third with children who have a dual sensory
impairment (deafblindness). From the outset it must be stressed that both
senses are not equally affected in deafblindness and these learners might
have greater deafness than blindness, or vice versa. For teachers the
challenge is to harness all the abilities and use them to make participation at
home, school and in the community as meaningful as possible.
11.2 HEARING IMPAIRMENT
We live in a sound-oriented world. Hearing uniquely allows reception from
all directions simultaneously, helping children to orientate and make sense
of their world Hearing helps children to develop speech and language, to
grow and develop academically, to develop personal-social skills and also
to develop emotionally (Dawes et al., 2015). Children with hearing
impairments miss out, to some extent or another, on the experience of being
immersed in a world of spoken language. Familiar environmental sounds
such as traffic noises, barking dogs, birds chirping and the wind rustling in
the trees go unnoticed.
11.2.1 What is a hearing impairment?
A hearing impairment may be described in terms of, first, the degree of
loss, and second, the structures (conductive, sensory-neural and central
nervous system) involved.
11.2.1.1 Degree of hearing loss
The degree of hearing loss is measured in decibels (dB), across different
pitches (frequencies), which are measured in hertz (Hz). Table 11.1
provides a description of the degree of hearing loss and the effect on
communication. Although the literature differs with regard to what dB
value constitutes profound hearing loss, a loss of 90 dB or more is generally
accepted as the boundary between hearing and deafness (Schlauch &
Nelson, 2009).
Table 11.1 Degree of hearing loss and the effect on communication
Hearing
Level of hearing
Effect on communication
Normal
hearing
0–15 dB
None.
Slight
hearing
loss
16–25 dB
Can hear vowels but cannot hear voiceless consonants
– this can lead to abnormal auditory perception of
speech sounds.
Mild
hearing
loss
26–40 dB
Can cope with one-to-one communication and mainly
hear the louder voiced sounds, but experience difficulty
in a group and with faint or distant speech. These
children often have a slight delay in language
development.
Moderate
hearing
loss
41–55 dB
Cannot hear faint speech, and experience difficulty at
conversational levels, especially in noisy environments.
This results in speech, language and learning
difficulties as well as poor auditory attention.
Moderately
severe
hearing
loss
56–70 dB
Difficulty understanding speech even with hearing aids.
Typically develop speech, language, learning problems
as well as poor auditory attention if not fitted with
hearing aids before their first birthday.
Severe
hearing
loss
71–90 dB
Cannot hear conversational speech and experience
difficulty with loud speech. They are able to hear loud
environmental sounds. If a hearing aid is fitted only
after the first year of life, it is common for children in
this category to have speech, language and learning
deficiencies. They also typically have poor auditory
attention.
Profound
hearing
loss
91+ dB
Little or no ability to hear speech even with hearing
aids. May benefit from cochlear implant.
Sources: Adapted from Schlauch & Nelson (2009); Storbeck (2016)
11.2.1.2 Structures involved
The ear consists of three parts: the outer ear, the middle ear and the inner
ear:
The outer ear consists of the visible part (pinna) and the auditory canal.
The middle ear is a cavity containing the tympanic membrane (eardrum)
and three small bones: the malleus (hammer), incus (anvil) and stapes
(stirrup). These bones vibrate in response to sound, thereby conducting
the sound to the inner ear (Keefe & Feeney, 2009).
The inner ear is made up of the cochlea and the auditory nerve.
A hearing impairment occurs when there is damage to any one or more of
these parts. The outer ear channels the sound down the auditory canal where
it causes the eardrum to vibrate. The vibrations of the eardrum create
electrical impulses that travel along the auditory nerve to the cochlea and
eventually to the brain.
The type of hearing loss refers to which structure of the ear is mostly
affected.
CONDUCTIVE HEARING LOSS
Conductive hearing loss refers to a blockage in the outer or middle ear and,
as a result, sound waves have difficulty passing through these structures to
the inner ear. Sounds may be distorted or muffled. Causes include the
presence of foreign bodies, wax accumulation, otitis media (middle-ear
infection) and structural abnormalities. This type of hearing loss is usually
temporary and can be treated with medication or surgery. Children with this
type of hearing loss may be late talkers and have indistinct speech; may
have poor listening skills; may often seem insecure or confused; and may
speak loudly.
Figure 11.2 Anatomy of the ear
SENSORY NEURAL HEARING LOSS
Sensory neural hearing loss is caused by damage to the inner ear structures
including the cochlea and/or auditory (hearing) nerve. Causes include
infections, exposure to noise, genetic conditions and ototoxic medication
(medication that is harmful to hearing). This type of deafness may affect
one or both ears, and is usually permanent. Children with such an
impairment may have difficulty hearing certain frequencies of sound as well
as understanding language.
MIXED HEARING LOSS
Mixed hearing loss occurs when a child has both conductive and sensory
neural impairment. An example would be a child with Down syndrome who
has been born with a sensory neural hearing loss as well as a conductive
hearing loss due to recurring ear infection.
(CENTRAL) AUDITORY PROCESSING PROBLEMS
Although there is a lack of consensus regarding the definition of the
disorder, (central) auditory processing problems refer to problems with the
way sound is interpreted and processed by the brain (ASHA, 2005). Such
problems may result from damage to the brain (e.g. head injury) and can
also co-occur with a hearing loss (e.g. repeated ear infections may cause a
temporary conductive hearing loss resulting in auditory processing skills
not developing properly). However, most children with (central) auditory
processing problems have normal hearing, and no brain damage is
detectable on a scan. Children with such problems would typically present
with poor listening skills, difficulties in determining where a sound comes
from (poor auditory localisation), difficulties listening with background
noise and difficulties discriminating between similar-sounding words (e.g.
“bin” and “pin”) (Keith, 2007). Auditory processing problems often have a
negative effect on the learning of literacy skills.
11.2.2 What causes hearing impairments?
Some children are born deaf (congenital deafness) while others develop
deafness at a later stage. Children at risk of hearing impairments include
those with parents or grandparents with hearing loss, autism, cerebral palsy,
intellectual impairment, cleft palate, Down syndrome, jaundice, HIV/AIDS,
meningitis, maternal rubella (German measles), untreated maternal syphilis,
birth complications and/or premature birth (Castillo & Roland, 2007).
11.2.3 Characteristics of hearing impairments
What are the behaviours that would alert a teacher to the possibility of
hearing loss? Some children may cry a lot and/or show signs of irritability;
they may have a discharge from the ears or frequent wax build-up; they
may be mouth breathers or complain of ringing in the ears (tinnitus). In
addition they may show signs of
delayed language development
poor articulation or indistinct speech
speech that is too loud or too soft
poor social skills and social interaction due to communication difficulties
difficulty in following spoken instructions
regularly requesting a repetition of what has been said
dislike of sudden or loud noises
leaning towards the source of the sound
hyperactivity
aggressive or withdrawn behaviour
a predisposition to visual distractions
disruptive behaviour because their disability makes it difficult to focus on
academic tasks.
If hearing loss is suspected, the child must immediately be referred for
assessment by an audiologist. This assessment will identify the degree and
the type of hearing loss. From an educational perspective it is important to
know if the child’s hearing loss is prelingual (congenital) or postlingual
(acquired). This is because a child with prelingual deafness would have
little or no experience of language (isiZulu, Sesotho, English, etc.) whereas
a child with postlingual hearing loss would already have developed some
degree of language exposure and competence, which greatly influences
further language and speech development.
11.2.4 Strengths: resilience factors
Having a hearing impairment does not limit a person from learning and
living a fulfilling life. Over the years there have been well-known deaf
people, like Ludwig von Beethoven, the famous composer. From the age of
28 he gradually lost his hearing and by the age of 48 he was completely
deaf; however, he continued to compose music. Thomas Edison who
invented the light bulb went deaf when he was a boy (Woolley, 1998).
Terrence Parker, a deaf swimmer from South Africa won a silver medal at
the Sydney 2000 Summer Olympic games.
11.2.5 Classroom management
11.2.5.1 Deaf education
In education circles there is a vigorous debate as to the most desirable
approach to teach learners with hearing impairments. On the one hand,
there is the Deaf-World (made up by individuals whose primary language is
sign language and who identify themselves as members of the Deaf
culture), and on the other hand there are individuals who do not identify
themselves as members of the Deaf-World or use its language (sign
language), participate in its organisations or profess its values, but who
rather consider themselves as hearing people with a disability (Lane, 2005).
To acknowledge this contrast, this chapter uses the scholarly convention of
“Deaf” when referring to the former group versus “deaf” when referring to
the latter group. A detailed discussion of the debates and choices around
communication, intervention, amplification and education is beyond the
scope of this book, but teachers should be aware of the issues and further
develop their knowledge and skills base if they are required to teach
children who are deaf. At one end of the spectrum is the oral approach and
at the other the sign language approach. The term “total communication”
embraces both these approaches.
ORAL APPROACH (ORALISM)
The primary goal of this approach is the “normalisation” of children who
are deaf (Storbeck, 2016), and the onus rests on them to “fit into the hearing
world”. With the recent advancements in hearing aids and cochlear
implants, oralism is increasingly gaining popularity (Lederberg, Schick &
Spencer, 2012). Two current oral approaches used frequently are the
auditory-oral and the auditory-verbal approaches. In the auditory-oral
communication approach, the teacher emphasises maximum use of residual
hearing, typically through the use of hearing aids or cochlear implants, and
focuses on speech, auditory training to maximise hearing skills, lip-reading
and natural gestures (e.g. waving) while sign language or the use of
extensive manual gestures is actively prohibited (Reed, 2009).
In the auditory-verbal approach, the emphasis is placed on maximising
listening skills, and signing is also not supported and/or encouraged. The
broad aim of both oral approaches is to get children who are deaf to use
their residual hearing, to learn to lip-read and to speak the language of the
hearing majority (Reed, 2009). Manualists (people who support the sign
language approach) feel that this is an illustration of the outdated medical
model, which focuses on the child’s disability, rather than the more
progressive social model, which suggests that society must change and
become inclusive. The effort to make children who are deaf speak
“normally” is laborious and, according to manualists, could disadvantage
their educational development and psychological health because of the
constant belief that they are “not good enough” and thus not fully
acceptable as they are (Storbeck, 2016). On the other hand, the fact that
teachers and parents do not need to learn a new language (South African
Sign Language or SASL) and can reply in their spoken language (English,
isiXhosa) is seen as a benefit. Children who have been taught with this
approach also appear to fit into the hearing world more easily due to the
fact that they can lip-read and use spoken language (Storbeck, 2016).
Stop and reflect
Look in a mirror and say the sounds “v” and “f”. They look very similar, don’t they?
Now try the sounds “m” and “b” and “p”. You can see how easy it is to make mistakes
when lip-reading!
SIGN LANGUAGE APPROACH
In the 1960s, sign language was recognised as a real language used by
people who are deaf (Moores, 2010). Sign language is a visual, gestural
language that has its own grammatical structure that differs from spoken
language (e.g. English) and that cannot be written (Reed, 2009). There is no
relationship whatsoever between sign languages and spoken languages.
Sign languages have their own vocabulary and rules of semantics, syntax
and pragmatics, which in no way follow the rules of spoken languages.
There is no “universal sign language”. For example, in South Africa SASL
is used (which is an official South African language); in America, American
Sign Language (ASL); and in Britain, British Sign Language (BSL). It
should, however, be noted that there are many SASL variations.
Stop and reflect
The Dictionary of Southern African Signs (Penn, 1992) is a compilation of 3 000
photographs of signs, which was commissioned by the Human Sciences Research
Council and the South African National Council for the Deaf (now DEAFSA) in the
late 1980s. The aim of this dictionary was to document a standardised SASL, which
would also note the many variations of SASL (Aarons & Akach, 2002).
It is important to note that sign languages do not have a written form. The
educational significance of this is that children who use sign language as a
means of communication will need to read and write in a second language –
the language of the speaking majority. This fact gave rise to the use of
educational sign systems such as Signing Exact English (SEE), a sign
system that was created in the early 1970s by Gerilee Gustason, a deaf
university professor and researcher, and Esther Zawolkow, a child of deaf
adults (Stryker, Nielsen & Luetke, 2015).
Unfortunately, most Deaf adults who use sign language have poor literacy
skills. In fact, in South Africa it is estimated that as few as one in three Deaf
adults is functionally literate (Glaser & Van Pletzen, 2012), which has a
negative impact across their lifespan and, in particular, on employment
opportunities. One of the contributing factors related to this fact is that only
14 per cent of South African teachers have well-developed SASL skills
(Glaser & Van Pletzen, 2012), and hence children emerge from various
schools with unconsolidated language skills.
Using the sign language approach in education is based on the premise that
sign language should be the first language of the Deaf. The child would
develop proficiency in a sign language that would, in every sense, be his
mother tongue. An important component of this approach is the presence of
numerous Deaf adults and children in the child’s environment, such as
having Deaf parents and appropriately trained SASL interpreters (Lederberg
et al., 2012). Language used for reading and writing would be the child’s
second language, for example the language of the hearing majority such as
isiXhosa, Afrikaans or Sepedi. Research shows that second language
learning is dependent on strong first language development (Lederberg et
al., 2012).
This would mean that not only teachers but also parents would need to be
fluent users of the specific sign language. It is difficult for parents and
teachers to become proficient sign language users unless they themselves
are deaf (Joseph & Alant, 2000). The disadvantage for a child using a sign
language is that he will only be able to communicate with other sign
language users, which has huge implications for meaningful participation
across environments – that is, fitting into both the “Deaf world” and the
“hearing world”.
It is clear that the issues surrounding language and learning are very
complex and that there are strong arguments to support the different
approaches. The critical issue is that first language proficiency is the core of
language development and the scaffold for the development of a second
language. The Deaf community advocates strongly that the locally used
sign language (i.e. SASL) is the only means through which Deaf individuals
will become proficient language users, which will enable them to be
educated in a second language (e.g. English).
In addition to sign language, these learners should also use fingerspelling.
Fingerspelling is a manual alphabet of 26 distinct hand positions used to
represent each letter of the English alphabet. Fingerspelling is used
particularly in the event of spelling unfamiliar words, such as own names.
TOTAL COMMUNICATION
This approach is a combination of the oral and sign language approaches,
and was the favoured approach in the 1970s (Moores, 2010). Total
Communication is not seen as a language (e.g. like SASL) because it
encodes the structure and grammar of an already existing language, e.g.,
English. The underlying philosophy is to use every channel available for
communication and education, for example stimulating residual hearing by
wearing hearing aids, speaking, using sign language and signing
simultaneously with speech (Reed, 2009). However, speaking and signing
simultaneously is challenging, because the duration of signs is longer than
that of spoken words (Glaser & Van Pletzen, 2012; Lederberg et al., 2012).
The argument against this approach is that children are exposed to different
language forms and therefore never develop a strong first language.
Educational sign systems, such as Signing Exact English (SEE) mentioned
earlier, use signs that follow the structure of the spoken language. This
presents significant difficulties because the grammatical structure of sign
language does not follow the spoken language. Language skills are
compromised, negatively impacting communication and learning. However,
this approach has been instrumental in fostering a mind shift that sign
language is as important as spoken and written languages, and should thus
be seen as a breakthrough in Deaf education (Storbeck, 2016).
Fingerspelling is another strategy that may be incorporated in total
communication, and can be either one-handed (Figure 11.3) or two-handed.
Fingerspelling is a skill hearing people may be prepared to learn and use
when communicating with someone who is deaf.
Figure 11.3 One-handed alphabet
Stop and reflect
Although the debate rages on about the best methods for educating children who are
deaf, there is consensus on one critical issue: children should have early and
extensive good language models no matter what the modality, including sign
language, developing residual hearing and lip-reading.
11.2.5.2 Management
Learners with hearing impairments can benefit from inclusion if
adaptations, which can take many different forms, are made. These
adaptations greatly depend on the degree of hearing impairment. High-tech
options include hearing aids (amplification), a cochlear implant or
installation of a frequency modulation (FM) system in the classroom. Lowtech options include alerting devices such as flashing lights triggered by an
alarm system or doorbell, and other classroom adaptations.
HEARING AIDS
Hearing aids are used to amplify (increase) sound, thereby maximising
whatever residual hearing the child may have. Amplification is a major
contributor to the development, participation and independence of
individuals with hearing impairment (Stelmachowicz & Hoover, 2009). If
the learner has a hearing aid, the teacher and parents must ensure that it is
worn and that it is in good working order. For example, it is particularly
important to ensure that the batteries are not flat. For younger learners,
hearing aids should be checked by the teacher at the beginning of each
school day and at least once a term by an audiologist. Teachers should also
establish good contacts and procedures to assist if the aids malfunction
(Luckner et al., 2012).
COCHLEAR IMPLANTS
Cochlear implants are considered as the 20th century’s most significant
technological advance in the treatment of deafness (Zwolan, 2009). A
cochlear implant is an electronic device that can provide a person who is
deaf with a sense of sound. It consists of an external part that is worn
behind the ear and against the head (the external speech processor that
captures sound and converts it into digital signals); an internal receiver that
is implanted just under the skin of the skull (the processor which send the
digital signals to the implant); and an array of electrodes that are implanted
into the cochlea (inner ear) to stimulate the auditory nerve, bypassing all the
damaged hair cells in the cochlea, so that the brain perceives signals and the
child hears sound.. A cochlear implant does not restore normal hearing, but
allows many children with profound hearing loss access to spoken language
(Lederberg, Schick & Spencer, 2012).
Therapeutic intervention is necessary to teach a person with a cochlear
implant how to process the stimulation received via the implant (Zwolan,
2009). The extent to which a person benefits from the implant depends on
many factors such as age of the individual at the time of the implant, the
number of electrodes successfully inserted into the cochlea, the cognitive
abilities of the person and the amount of support and intervention after the
implant (Spencer & Marschark, 2003). Current research shows that cochlear
implants are less effective for children with multiple disabilities (Lederberg
et al., 2012).
FM SYSTEMS
FM systems are used to relay sound from the teacher to the learner. The
teacher’s voice is transmitted (via a wireless microphone) to a body-worn
receiver, which is plugged into either the hearing aid or headphones worn
by the learner. During a group discussion activity, the teacher should pass
the microphone around to all speakers (Luckner et al., 2012).
BILINGUAL LANGUAGE LEARNING
The challenges of bilingualism are well understood by teachers in South
Africa but most hearing children have developed language skills (in their
first language) before they get to school. Consider the scenario of an isiZulu
child in an English-medium school. The teacher will teach in English but
will often (if she is fluent in isiZulu) give explanations in the child’s first
language. For a child who is deaf it is essential for bilingual support to be
given from the very earliest stages, both at home and at school (Lederberg
et al., 2012; Moores, 2010). When the local sign language is chosen as the
means of communication, the family members and the teacher become not
only the child’s primary communication partners but also interpreters of
what the child is saying to others and what others are saying to the child.
Pointing to objects, photographs, line drawings and print while
communicating in sign language is a core component of the early stages of
bilingual teaching and learning. For example, using a regular library book,
the teacher can “read” it using sign language while pointing to the pictures.
Incidental learning takes place as the child sees the text and, over time,
realises it has meaning of its own. Of course this has its own challenges:
first, the learner who is deaf must be able to see the teacher and the book,
and second, the teacher must sign and point. Creative strategies such as
using a sibling or peer to point to the pictures works well – in no time the
deaf learner will be able to do the pointing himself. The fact that children
like being read favourite stories over and over again provides a wonderful
platform for language learning (Bornman, 2006).
11.2.5.3 Classroom strategies
In addition to these guidelines, teachers can also consider the following
classroom strategies:
Adapt the physical environment by ensuring that these learners are seated
at the front and side of the class so that they can be near the teacher and
see her without any obstruction in their line of sight (which assists with
lip-reading) and see the whole class group (Guardino & Antia, 2012). If
the group is rearranged, for example for circle or story time, these
learners should always sit as close to the speaker (usually the teacher) as
possible.
Reduce loud or irritating background noise like lawnmowers and loud
conversations in the corridors, as hearing aids are ultra-sensitive to
sound. Learners should sit as far away from unavoidable background
noise (e.g. passing traffic) as possible.
Ensure good lighting so that the learner can see the teacher’s face clearly.
In addition, the teacher should stop talking when, for example, she turns
away from the learner to write on the whiteboard. When positioning a
learner, the teacher should also be aware that too much light creates a
dazzling effect on a whiteboard or on learners’ desks, which becomes a
visual distraction (Guardino & Antia, 2012).
The teacher should make sure that she gets the learner’s full attention
before starting a conversation or giving an instruction, for example by
moving closer or touching him (briefly on the shoulder or hand) before
beginning to speak. Specific routine attention-getting strategies can be
taught, for example flicking the lights, counting down from ten (Luckner
et al., 2012).
When speaking, language should be kept simple – single words, short
phrases and sentences using natural rhythm, pitch and intonation.
Supplement speech with facial expressions and body language (Westling
& Fox, 2009).
Try to speak clearly and at the normal volume at close range rather than
shouting from a distance, as shouting distorts the mouth, making lipreading difficult (Woolley, 1998).
Keep good eye contact, bending down to the child’s level if necessary.
Eye contact provides valuable visual information to help understand what
is being said.
When a classmate puts up a hand to say something or answer a question,
the teacher might point to the child who is talking, thereby giving the
learner with a hearing impairment a clue about the direction in which he
must look.
The teacher and learner could develop a “secret sign” that the learner
could use when he misses out and needs the teacher to repeat or explain
something in a different way. Teachers have reported a “listen – then look
– then listen” sequence to be effective in instruction (Mastropieri &
Scruggs, 2011). The learner should focus on the teacher’s face, and then
on other important aspects of the lesson, and then on the teacher’s face
again. For example, when doing an experiment in natural science about
starch and sugar, the teacher can say: “Now I am going to pour the iodine
onto the potato” (listen); then pour the iodine (look) then say: “I poured
the iodine onto the potato. Who can tell me what happened?” (listen).
Select the most important vocabulary related to the lesson and then help
to build vocabulary, as learners who are deaf often have large gaps in
their vocabularies because they are not immersed in language in the same
way as their hearing peers (Luckner, Slike & Johnson, 2012). Teachers,
with the support of parents, need to ensure that learners who are deaf are
prepared in advance for lessons in which new words or concepts will be
introduced. It needs to be a concerted effort – children who are deaf will
not just pick up new words. Teachers can also be encouraged to make use
of visuals such as illustrations graphic symbols and language cards that
contain pictures and definitions of new vocabulary items that are
introduced (Mastropieri & Scruggs, 2011).
Develop reading comprehension as it is strongly related to language
proficiency that is pivotal to all educational activities, for example
reading textbooks, completing worksheets, following instructions, and so
forth. Link new concepts and words to existing concepts and experiences,
and show how they are related in order to strengthen and expand
vocabulary (Luckner et al., 2012).
Provide a wide variety of sensory (seeing, hearing, touching, tasting and
smelling) experiences, as this will facilitate communication and language
development.
Use technology in the classroom, for example overhead projectors,
PowerPoint presentations, videos and Smart boards (an interactive
whiteboard that works in the same way as a touchscreen computer) to
supplement the spoken message with a visual image (Luckner et al.,
2012).
Enhance story reading by initially reading facing the child, thereby
enabling him to look alternately at the teacher and the book. The teacher
should also point to the pictures and to the text while reading.
Ensure that the learner is able to follow the aims, structures and intended
outcomes of instructions. Both visual information and gestures can be
used effectively.
For older learners, teachers can start a blog about the specific study topic
(e.g. “Global warming, myth or fact?”) and have the learners expand it
through group discussions (Luckner et al., 2012).
Teach learners to “RAP” during reading activities (Luckner et al., 2012).
R Read a paragraph.
A Ask yourself: “What are the main ideas and detail in this piece?”
P Put the main idea and detail into your own words.
Stop and reflect
Mrs Nthuli has planned her lesson well: “Today we are going to learn about fruit
farming (aim). We will get into our groups and open our textbooks at Chapter 10,
which is about the fruit grown in different areas. Each group will be given a map of
South Africa and you must indicate where the different fruits are grown (structure).
We will find out what grows in our area and then plant a fruit tree in the school
grounds (outcome).”
Vocabulary related to fruit and farming could be prepared ahead (homework).
Peers could also be given signs to learn (homework) ahead of time. The whole group
could decide how to organise a tree-planting ceremony. Visual strategies could
include asking children to bring fruit, pointing to a wall map of South Africa and then
to graphic symbols of planting, watering and fertilising. These visual prompts can be
used less frequently as the learner develops.
11.2.5.4 Peer supports
Social relationships add quality to a person’s life, contribute to thinking and
learning and are critical for succeeding in life (Antia, Jones, Luckner,
Kreimeyer & Reed, 2011). Children with a hearing impairment are at risk
for not developing social relationships due to problems with peer
communication and interaction. The importance of creating opportunities
for the social inclusion of children with hearing impairments therefore
cannot be emphasised enough. A good starting point is to give hearing peers
information about hearing impairment and get them to experience it by, for
example, wearing earplugs. Peers could also be taught signs and maybe
even the basics of SASL (if that is the language of the child who is deaf).
This can be a group activity in which the child with a hearing impairment
can join in – as participant and as “teacher”. Children enjoy sporting
activities, crafts and playing board games together. Games such as draughts
and chess, which do not require speech, put children on an equal footing,
but it is important to adapt other games such as Snap, which could require
that children put their hand on the cards rather than calling out “snap”.
Adaptations do not have to be costly or complex. All the children could be
challenged to come up with ideas on how to level the playing fields.
Appropriate classroom participation can influence the attitudes of peers
(and other teachers) towards the child with the hearing impairment, thereby
affecting relationships in and outside the classroom – a testimony to the
critical role of the child’s classroom teacher (Antia et al., 2011).
These are just some of the strategies that can be used when teaching
learners who are deaf. The story that follows is a true story written by the
mother of two children who are deaf. It illustrates many of the complexities
that have been discussed.
Where does my daughter’s story start? Maybe with her older brother’s story…
So I guess our story starts when we discovered, at the tender age of two, that our
son was deaf (90 dB at the low frequencies, and 120 dB at the middle frequencies).
We took him to see a famous professor at Tygerberg Hospital who started a centre
where they teach deaf children to talk. This was noticeably different from the schools
for the Deaf that we knew and that were close to us. We went there every three
months for two weeks at a time, and I was trained in what to do with my son and how
to talk to him – the fact that I am also a teacher helped. When he turned three, we
moved to Cape Town and stayed there until he was six years old, as the constant up
and down travelling became too much. Our main mission at that point was to teach
him speech, and he progressed really well. I think personality plays a big part when
teaching a deaf child to speak – he should have the will to learn to talk. I also believe
that it requires a lot of attention from the parents (I didn’t work at the time). I was
reminded that my son’s prognosis wasn’t good because he was diagnosed late, but
despite this, he proved us wrong. When he was six years old we moved back to
Limpopo where my husband was called to (he is in the church ministry). We decided
that our son should attend a crèche twice a week to increase his socialisation skills,
while I home-schooled him for the rest of the time. I had to make him aware of all the
small parts of language, e.g. the article “the” as he couldn’t hear it, and therefore
missed its presence in a sentence. Every activity was seen as an opportunity to
teach him language and when he entered Grade 1 his language skills were actually
ahead of those of his peer group, despite the fact that he couldn’t say the two highfrequency sounds “k” and “s”. Fortunately it was a small school and there were only
22 children in his class.
When my son was three-and-a-half years old, we had another son with normal
hearing.
Then, when our first-born turned eight years old, our daughter was born. I was very
mindful of her hearing and looked for every sign to see if she could hear or not.
Initially everything seemed to be fine, but when she was about seven months old, I
started worrying. Before this time she reacted to sounds in the environment and to
my voice when I was whispering, but suddenly this did not happen anymore. I took
her to an audiologist who put me down as a neurotic mother. She said that just
because our son was deaf didn’t mean that we would have another deaf child. As I
trusted the audiologist at Tygerberg Hospital who had assisted us with our son, we
decided to take her there for a second opinion. When she was ten months old they
confirmed with a brainstem test that she was, indeed, deaf. We had genetic
counselling and were informed that either my husband or I have a recessive gene
that could lead to deafness. This meant that we had a one in four chance in every
pregnancy of having a deaf child. Neither of my children have a dominant gene that
could lead to deafness, so they both have the possibility of having normal hearing
children one day. And so the whole process started all over again.
We decided to follow the same programme with our daughter, as we were familiar
with it and we had seen how successful it was with our son. My mother, who is also a
teacher, was a great support to me and she worked just as hard as I did. I again
home-schooled my daughter, and when she was four years old, I sent her to crèche
once a week, as socialisation was easier for her than for her brother – not because of
the degree of hearing loss, but because of a difference in personality. We had to
make many sacrifices and experienced many frustrations – but one has to learn to
cope with that. Primary school was difficult for my daughter, as it wasn’t easy for her
to socialise in a group and she felt excluded at times. We also experienced a few
heart-breaking moments as a family. Having two deaf children asks of us to
constantly adapt, e.g. when we watch TV we frequently hear the question: “What’s
happening? What now?” Everything has to be repeated!
Our son really excelled at high school and was readily accepted. Eventually he
completed matric with six distinctions and is currently studying industrial engineering
at the University of Pretoria! He decided to have a cochlear implant when he was 22
years old, and is doing well.
Our daughter, on the other hand, feels that she is not ready for an intrusive operation
such as the cochlear implant and prefers to wear bilateral hearing aids (two aids),
and also asks the teacher to wear an FM system in the class. Initially, the high school
we selected was sceptical and objected to accepting our daughter as the principal felt
that she would cope better at a school for children who are hard of hearing. After a
serious (and heated) discussion between my husband and the principal, it was
agreed that she could attend. Initially she attended the boarding school (for 1½
years). When our son was at boarding school, we had to send him a weekly fax as a
way of communication, due to the fact that he couldn’t use a telephone and
cellphones were not freely available. Nowadays, cellphone technology and text
messaging make communication over a distance much easier. Our daughter is now
back at home, still in the same high school, and doing extremely well. She has won
gold medals at the science expo, as well as at the Afrikaans Eisteddfod! I think the
fact that she is a very keen reader helps with her good language and spelling skills
(she won prizes for poetry writing at school) and broad general knowledge. However,
at times we had to discourage her from reading constantly at primary school, as she
used this as a way of escaping from difficult social situations – she would prefer the
library to the playground. When we went to restaurants and she knew that it might be
difficult, she also preferred to take a book along. As radio and television are not
always accessible to her, she also likes to read newspapers to inform her about world
events. On the down side, she finds it difficult to understand jokes, due to the
abstract concepts that are used, and although she does well at maths, she has to
work hard at it, as maths contains a lot of abstract concepts.
If I had to choose between a school for deaf children or hard-of-hearing children and
an inclusive school again, I would make the same choice, despite the many hours of
hard work. When one has a deaf child, you have to be there for them and give 110
per cent all the time. An inclusive school has given both my children the opportunity
to lead a normal life, to participate in typical activities and to learn everyday skills. It
has equipped them to live in a hearing society, unlike the Deaf culture that is
separate. By putting them in an inclusive school they were exposed to normal speech
and language models, which had a very positive influence on their speech and
language development. I also felt that inclusion gave them self-confidence and guts
to conquer their worlds. For me, as their mother, it fills me with gratitude if I see them
do well, and I realise that my faith and the grace I received helped carry me through
many crises.
The girl’s Grade 9 Afrikaans teacher (see box above), a teacher with 30
years of teaching experience, was asked what guidelines she could give to
other teachers if they had to include a learner with a hearing impairment in
the class. This is what she said:
What strategies help the teacher in the class when teaching learners who are
deaf?
Knowing the child very well, and also knowing her family and background, for
example I knew that she had a very large vocabulary because of the fact that she
liked reading and that she was academically strong. I also knew that she was a
popular girl who got along easily with her peers and that she did not want to be
pitied.
The short training session given by her mom at the beginning of every year helped
all the teachers to know what to expect and what to do, and helped them
understand the child better.
Experiencing cooperation from both the child and the family and a feeling that the
parents supported me. I felt as if we worked together as a team.
The child’s personality – she is enthusiastic and not afraid to ask for a repetition or
clarification if she does not understand. She is always well prepared for lessons
and will read additional books about the topics that are discussed in class. She
also carries the responsibility of giving the FM system to me and asking me to
wear it – hence the FM system does not become an additional burden on me.
The child sits in the front of the class so that she can see me well. The lighting in
the classroom must be good.
The child sits next to a buddy who ensures she understands instructions.
I don’t walk around while presenting the lesson and I don’t turn my back to the
child while I am still talking or giving instructions, for example talking while writing
on the board.
All children, irrespective of their abilities and the possible barriers they face,
basically want the same three things: they want to be noticed, they want to be
acknowledged for what they do and they want to know where the boundaries are
in terms of what they may and may not do. I make sure I give that to all my
learners.
11.3 VISUAL IMPAIRMENT
No other sense can stimulate curiosity, combine information and
invite exploration as efficiently as vision.
A
F
B
( . .)
11.3.1 What is visual impairment?
According to the International Statistical Classification of Diseases and
Related Health Problems 10th Revision (ICD-10, World Health
Organization, 2010), there are four levels of visual function, or which levels
2–4 represent visual impairment:
1. Normal vision
2. Moderate visual impairment
low
3. Severe visual impairment
vision
4. Blindness
Moderate visual impairment (level 2) combined with severe visual
impairment (level 3) are grouped under the term low vision. The term visual
impairment is defined as a limitation of one or more functions of the visual
system, and affects visual acuity (the sharpness or clarity of vision), visual
field (the area a person can see without turning one’s head) and colour
(Royal Institute for Deaf and Blind Children). Considering that as much as
80 to 90 per cent of early learning is based on visual input (Bornman,
2006), children with low vision are at high risk of missing out on many of
the learning experiences available to their sighted peers. A child’s early
sensory motor experiences are limited by the challenges he has in exploring
a world he has difficulty seeing. Incidental learning is severely restricted as
the child is unable to pick up much of what is happening in his
environment. In order to describe a learner’s visual abilities, teachers should
know that the visual system consists of three components, namely sight,
transmission of an image along the optic nerve, and interpretation of the
image in the visual cortex of the brain (Beukelman & Mirenda, 2013).
Children with low vision can and do succeed, but often at different rates and
in different sequences from their sighted peers.
11.3.2 What causes visual impairments?
Visual impairments can be present at birth or acquired later in life. Globally,
the most common causes include uncorrected refraction errors (43%) and
congenital cataracts (clouding of the lens) (33%) (Pascolini & Mariotti,
2010). Other causes include optic nerve atrophy (degeneration of the optic
nerve), retinopathy of prematurity (damage caused by excessive
concentrations of oxygen used to treat prematurely born infants), diabetic
retinopathy (lack of blood to the retina), retinal detachment, glaucoma
(excessive pressure on the eyeball), coloboma (parts of the retina
improperly formed) and retinitis pigmentosa (degeneration of the retina)
(Landsberg, 2016; Mastropieri & Scruggs, 2011). Visual impairment can
also be related to other conditions and syndromes, for example cerebral
palsy, HIV/AIDS, FASD, diabetes mellitus, maternal rubella and pre- and
postnatal drug exposure. Cortical visual impairment, a condition in which
the visual systems of the brain do not consistently understand or interpret
what the brain sees, may be related to brain injury, which may be caused by,
for example, head injury, hydrocephalus, developmental issues and
infections such as meningitis and encephalitis.
Albinism can also lead to reduced visual acuity, increased light sensitivity
(photosensitivity) as a result of a lack of melanin in the eye, astigmatism,
nystagmus (rapid back and forth eye movement or in a circular motion) and
strabismus (squint) (Kivi & Solan, 2015). There are two main categories of
albinism (Kamaraj & Purohit, 2014), and both have visual implications:
Oculocutaneous albinism (stemming from Latin and meaning eye-andskin albinism). In this condition, pigment is lacking in the eyes, skin and
hair, which can range from having no pigment to having nearly normal
levels.
Ocular albinism. In this condition, only the eyes are affected. These
individuals typically have normal skin and hair colour, and many even
have a normal eye colouring, but they have no colour in the retina (the
back of the eye). Ocular albinism is the result of a gene mutation on the
X chromosome, and occurs almost exclusively in males.
It is encouraging to note that data over the last 20 years show that visual
impairment has decreased worldwide since the estimates in the early 1990s,
despite an ageing global population (World Health Organization, 2014).
This decrease is attributed to a reduction in visual impairment from
infectious diseases (as 80 per cent of all visual impairment can be prevented
or cured) through focused health initiatives, increased availability of eye
care services and increased public awareness about possible interventions
(e.g. surgery, glasses and contact lenses).
11.3.3 Characteristics of visual impairments
As explained earlier, there are degrees of low vision, and in this chapter the
definition proposed by Corn and Lusk (2010: 4) is used:
… a person who has measurable vision but who has difficulty
accomplishing (or cannot accomplish) visual tasks even with
prescribed corrective lenses but who can enhance his or her
ability to accomplish these tasks with the use of compensatory
visual strategies, low vision devices and environmental
modifications.
In this section, the most commonly used criteria for assessment are
discussed.
11.3.3.1 Visual acuity
Visual acuity refers to the size and distance of objects that the learner can
see. Normal vision is referred to as 6/6 vision. A child with 6/21 vision (low
vision) would be able to see at six metres what a child with normal vision
will see at 21 metres. In the past, normal vision was referred to as 20/20
vision, low vision as 20/70 vision and legally blind as 20/200. This was due
to the fact that the metric system (metres) was not used, and that the
distances were measured in feet. As this is a South African text, the metric
system is preferred. The impact of loss of acuity is illustrated in Figure
11.4.
Figure 11.4 Impact of visual acuity loss
Source: Adapted from Beukelman & Mirenda
(2013)
11.3.3.2 Visual field
Visual field assessment provides information regarding an individual’s use
of his central, peripheral, superior and inferior visual fields (Erin & Topor,
2010). Looking straight ahead without moving the eyes sideways, a child
with normal vision can see 150 degrees in the horizontal field and 120
degrees in the vertical field. This information is important for teachers in
determining the best positions for placing activities in order to allow for
optimal vision (both near and far activities).
Figure 11.5 Visual field
Table 11.2 Impact of visual acuity and visual field on visual skills
Classification
Normal
Description
Visual acuity 6/6
Visual field 150
degrees horizontal
Effect
Intervention
No effect on vision
(neither on visual
acuity nor on visual
field)
No intervention
required
Visual field 120
degrees vertical
Low vision
Visual acuity 20/70 to
20/160 in better eye
with best possible
correction
Visual field loss
Legally blind
Visual acuity 6/60
Adjustments often
needed in viewing
objects
Moderate or
severe visual
impairment
Severe visual
impairment
Can benefit from
low-vision devices
(optical or
electronic)
Cannot benefit from
low-vision devices
Total loss of vision
11.3.3.3 Visual motility
Visual motility refers to a learner’s ability to localise, fixate, follow and
track visually. These skills are important for a number of activities required
of learners in the classroom, like following a teacher who walks around
while speaking. Disturbances of muscle tone in eye muscles and nystagmus
(rapid eye movements) can cause difficulty with focusing, looking for and
scanning objects, and following moving objects. The vision of most people
with nystagmus is usually well below what is considered to be shortsightedness. These people are mostly classified as partially sighted.
Strabismus (squint) may cause double vision.
11.3.3.4 Light sensitivity
It is important to remember that the needs of learners with visual
impairments vary according to the person, the aetiology of the visual
condition and the environment. Individuals with albinism frequently have
heightened light sensitivity and hence teachers should identify strategies
that increase visual acuity and reduce visual fatigue. Illumination, which
refers to the amount of light received on the surface, is one of the most
important factors to be considered in the enhancement of visual efficiency
(Wilkinson, 2010). Teachers should take note of the amount, type and
position of the light. Although natural light is adequate for most low-vision
children (if they sit with their backs to the window), artificial light allows
better control of illumination (Vasconcelos & Fernandes, 2015). Fluorescent
light is a cooler light source that yields higher levels of illumination but can
produce visual fatigue due to the potential strobe-like effect (Wilkinson,
2010).
Amount of illumination. A white wall, a tiled floor, a concrete sidewalk
and a green chalkboard all reflect different amounts of light, and teachers
should observe the effect of such diverse levels of illumination on a
learner’s performance in near and distance activities. Matte surfaces for
paper, boards and walls prevent light reflection and glare. Illumination
should always seek to enhance contrast and reduce glare.
Type of illumination. Artificial lights such as fluorescent lights are
commonly found in classrooms and although they produce a higher level
and a cooler type of lighting, they also cause the most visual fatigue. The
sun provides natural light, and teachers should be aware of the effect of
windows, open doors and skylights on learners’ performance at various
times throughout the day.
Position of illumination. Teachers will need to look at each learner’s
individual characteristics and try to find the most optimal position of
light, for example over the shoulder of the dominant hand. Light boxes or
high-intensity desk lamps can also be considered.
11.3.3.5 Visual stability
For some children, particularly those with a cortical visual impairment, the
degree of visual impairment may fluctuate, sometimes as often as daily,
depending on his physical status or environmental factors (Beukelman &
Mirenda, 2013). In addition, some eye conditions will deteriorate, with both
the rate of deterioration and the final outcome being unpredictable.
11.3.3.6 Visual perception
Visual perception is the ability of the brain to organise and interpret what
the eyes see, for example visual discrimination, visual analysis and
synthesis, visual sequencing and visual memory.
Although all of the above functions can be assessed and measured, they do
not necessarily accurately reflect the way in which a child functions – that
is, a child classified as partially sighted may have severe visual difficulties
and need extensive support. Similarly, a child classified as blind may
unexpectedly retain some visual skills. This means that even with the same
diagnosis, children will have different abilities and needs. Once again, for
educational purposes, the focus should be on the level of support needed.
It is therefore important that teachers are able to conduct a functional vision
assessment. This requires them to observe systematically how learners use
vision to complete daily activities with a variety of materials. They should
also determine the degree to which the visual impairment interferes with
learning, and identify ways to increase the efficiency of visual functioning
(Huebner, 2000). This information can be used as a basis for selecting
appropriate learning and literacy media for learners who are blind or
visually impaired.
11.3.4 Warning signs of visual impairment
Significant visual impairments will usually be identified before a child gets
to school. However, it can happen that these children slip through the
system, and the following behaviours may alert the teacher to possible
visual impairments (Westling & Fox, 2009; Vision Council, n.d.):
Squinting, closing or covering one eye
Clumsy movements, shuffling walk, bumping into objects
Holding the head in unusual positions and “peering”
Holding materials close to the face or putting the head close to the desk
Relying on sound cues such as environmental noises to help locate
objects
Choosing to sit at the front of the class or where they see best
Not making good eye contact with others
Avoiding visually demanding tasks
Finger flicking or waving in front of eyes
Pressing, poking or rubbing eyes
Redness or tearing of eyes
Over- or under-reaching for objects
Many children with low vision have enough residual vision for reading,
writing and other classroom activities. Systematic instruction in the use of
visual skills will maximise the use of residual vision (Westling & Fox,
2009). In schools, the provision of appropriate supports will enable these
learners to participate in learning activities as well as extracurricular ones.
11.3.5 Strengths: resilience factors
It is not true that people who are blind have more sensitive hearing or other
senses; it is rather a case of having learnt to use hearing, touch and smell to
substitute for some functions that vision normally serves (Silberman, Bruce
& Nelson, 2004). Tactile and auditory skills should be taught in specific
training sessions and then be generalised to use in other functional
activities. Likewise, the sense of smell can be developed through a series of
discrimination activities.
11.3.6 Classroom management
In the classroom, two educational approaches should be blended to ensure
curriculum access for children with low vision: on the one hand, children
should be taught access skills (in other words, how to use technology aids,
such as screen readers) and on the other hand, teachers should provide
materials to optimise access (e.g. by providing large print material)
(Douglas et al., 2011). Furthermore, teachers will find that they can make a
number of physical adaptations to make the classroom more inclusive, such
as ensuring clear, open walkways, teaching learners about certain familiar
landmarks (in and outside the classroom), replacing all visual cues (which
these learners cannot see) with physical cues and notifying them when any
changes are made (Mastropieri & Scruggs, 2011). For these learners,
language also has increased significance as it acts as a substitute for the
missing visual input, and therefore teachers should always use precise
language with clear verbal descriptions and explanations (Morris, 2016). In
addition, teachers should
encourage independence (Wilkinson, 2010)
get to know all learners well and capitalise on their individual strengths
teach by including multiple modalities (e.g. touch, sound and smell) and
use concrete objects during lessons that they can feel and manipulate
use descriptive language and narrate what is happening in the classroom.
Avoid vague phrases such as “over here”, “almost”, “this” and “that”,
and rather use specific language such as “above your head”, “on your
right” and “the ruler in my hand”.
For learners with a visual impairment who can learn to read or write, a
range of specialised reading techniques are available – it depends only on
the degree of visual impairment. For learners with less severe visual
problems, regular print with high contrast and of good quality should be
adequate. For those with more severe visual impairments, augmented
reading can be facilitated with large print or Braille. Various high- and lowtech vision devices are now also becoming available at affordable prices,
for example hand-held magnifiers, monoculars, talking low-vision watches,
talking low-vision calculators, magnifying lamps, etc. These devices can
help the learner to cope in the classroom and other functional settings.
Various speech reading systems (aural reading/auding) which can augment
reading are commercially available, for example Jaws or the Kurzweil 3000
(Mastropieri & Scruggs, 2011).
Learners with visual impairments also have a variety of options for writing,
which includes machine- or hand-embossed Braille, computerised Braille,
typesetting and handwriting. Functional handwriting should also be
considered for blind learners, as it aids independence. For example, blind
people are often required to sign their names on various documents
(Beukelman & Mirenda, 2013). Aids such as special writing paper with
raised bold lines, varying contrast lines, enlarged line spacing as well as
special pens such as broad- and fine-tip markers or pens and pencils in
various colours, which provide tactile and visual feedback during writing,
are valuable options.
11.3.6.1 Curriculum: classroom challenges and support strategies
The curriculum needs of children with visual disabilities have two
components. The first is to provide access to the general curriculum using
available adaptations and supports. The second is to address disabilityspecific issues that are unique to children with visual impairments.
ACCESS TO THE GENERAL CURRICULUM
Some of the critical questions are: What exactly can the child see? What
size/colour should the objects, symbols or writing be? How close to the
child should the objects/pictures/print be and exactly where should they be
positioned? What colour should the background be? What adjustments
should be made to lighting? What strategies would take into account a
deteriorating condition?
Learners should have access to reading and writing supports, which include
class notes in audio recorded, Braille or electronic formats adaptive lap
equipment (e.g. talking thermometers, calculators, light probes, etc.);
computers with optical character readers, speech output, Braille screen
display and printer output; readers, homework and test scribes, and in-class
note takers. Braille may be used as an alternative symbol set to traditional
orthography (see Figure 11.6). This is a unique reading and writing mode of
communication for children who are unable to see text (and children can
learn to read and write Braille at the same time as their peers are learning
more traditional literacy skills, but systematic and regular instruction is
essential (Landsberg, 2016)). Research is also showing that computer
technology is making access to Braille easier, faster and cheaper. The role
of Braille in the personal, social and economic independence of people who
are blind is so important that it is vital that teachers and other rehabilitation
professionals recognise their roles in facilitating literacy development
through Braille (Tobin & Hill, 2015).
Figure 11.6 Braille alphabet
Print can also be made more visible (and hence legible) by following these
guidelines:
Increase the contrast. The highest possible contrast should be used.
White or light yellow text on a dark background may be more legible
than the regular dark letters on a white background. High-contrast line
markers might also be useful for certain learners, for example those with
albinism (Wilkinson, 2010).
Increase the font size. When using computers, font size should be at least
16 to 18 point, although this may vary with different typefaces. An
example is shown in Table 11.3. If font sizes cannot be enlarged on the
computer, learners can also be given magnifiers to use in class (Spungin
& Ferrell, 2007). The optimal print size should, however, be established
on an individual basis (Douglas et al., 2011).
Table 11.3 Increase font size to enhance visibility
10 point font
example
16 point font
example
20 point font
example
Increase line spacing. Increasing the spacing between the lines of text
makes it easier for the child to find the next line.
Justify text. Unjustified text makes it more difficult to move to the next
line
Change font type. Avoid complicated or decorative fonts. Times New
Roman and sans serif fonts are usually the fonts of choice.
Increase letter spacing. Close letter spacing may present difficulties.
Where possible, spacing should be wide.
Paper finish. Where possible, paper with a glossy finish, for example
laminated paper, should be avoided as the glare factor impacts negatively
on legibility.
Binding. Spiral binding of books can be helpful as it keeps the surface
flat, which makes it easier to use low-vision devices such as magnifying
glasses.
Good lighting. Good-quality lighting is essential, for example a personal
lamp on the desk, adjusting the light intensity on a computer screen, and
so on. Background light should not be too intense because of the resultant
glare, and teachers should not stand in front of the window or a light
source when speaking (Wilkinson, 2010).
Photosensitivity. Lighting conditions have to be controlled to ensure
optimal classroom performance for learners such as those with albinism.
In addition, they can be encouraged to wear tinted lenses, sunglasses or
wide-brimmed hats or caps (Vasconcelos & Fernandes, 2015)
Appropriate work surfaces. The learner should be able to rest his elbows
comfortably on the surface, thereby freeing his hands to explore available
materials. The surfaces should be uncluttered and, for younger children
especially, it may be helpful to have a lip around the edge to prevent
things falling off. Reflective or shiny surfaces should be avoided.
CURRICULUM: DISABILITY-SPECIFIC ISSUES
Westling and Fox (2009) identify disability-specific issues as visual
efficiency skills, communication skills, orientation and mobility skills,
social interaction skills, independent living skills, recreation and leisure
skills, use of assistive technology and workplace preparation. Orientation
and mobility skills are prerequisites for safe and purposeful movement
across environments. The child learns skills of moving around in familiar
and unfamiliar environments with a sighted guide. Children need to be
trained by a team specialising in orientation and mobility training, as this
becomes the foundation for developing independence.
Furthermore, these learners should be taught how to discriminate between
objects and activities on a tactile level. Initially identifying objects by touch
assists children in being independent (e.g. in dressing) and at school they
will build on this skill when they learn to use Braille. For this they will not
only need a good memory, but also sensitive fingertips to distinguish
between the various Braille dot combinations (Spungin & Ferrell, 2007).
Using different toys, activities and games, as shown in Table 11.4, may
stimulate such sensitivity.
For certain subjects, for example maths, specific adaptations are required.
Children with low vision often have difficulty with maths, as maths skills
emerge as a visual skill and develop into advanced graphical and spatial
relationships. Specific instruction and adaptations are thus needed,
including the abacus, talking calculator, concrete materials and tactile
graphics (Spungin & Ferrell, 2007).
11.3.6.2 Peer support strategies
Peers with normal or corrected vision can be taught to come alongside a
classmate with low vision. The teacher should continuously monitor these
strategies. Examples of support strategies are as follows:
Peers must announce their own name when approaching, for example:
“Hello Sipho. This is Bob here. Do you want to go with me to the
playground?”
Peers can offer their arm to guide a classmate. The classmate will walk a
step behind and must be warned of approaching obstacles, for example
steps, other people and animals.
Peers can be careful about keeping the environment free of obstacles, for
example closing cupboard doors, pushing chairs under desks, and
keeping classroom equipment neat and in the same place.
Peers can scan the environment and then provide choices, such as where
to sit in the library, the school playground or hall.
Table 11.4 Tactile differentiation activities
Feely hand shapes
Real things as
dominoes
Feely wiggly worm
Friendly
rattlesnake
Feely hand shapes
Real things as
dominoes
Feely wiggly worm
Friendly
rattlesnake
Sorting hand
shapes into pairs is
a good introductory
game. Shapes are
large, so there is
plenty of surface to
feel.
Textures replace the
normal dots, and
they can be made
large enough to
handle with ease.
Use real objects
such as hinges,
buttons, doorknobs,
corks, keys, etc. to
make your own
domino pieces.
The worm consists
of series of little
cushions joined with
Velcro. The texture
of the back half of
one cushion
matches the texture
of the front half of
the next cushion.
Unlike real
rattlesnakes, these
friendly reptiles do
not only use their
tails to make noise.
Different
noisemakers are
distributed
throughout the
snake’s long body
(to enhance
listening skills) and
each segment of the
snake’s body is
made of different
fabric (to enhance
tactile
discrimination).
Children shake
different parts of the
snake and try to
guess what
produces the
particular sound.
Stop and reflect
Did you know that the South African Reserve Bank ensures that the money we use
has features tailored for people with low vision?
A coin has six features by which a person with low vision can identify it: size,
thickness, shape (not all are entirely circular), pattern of grooves around the edge,
the sound it makes when dropped and the raised picture on the face.
One, two, three, four or five raised diamond shapes in the middle of the bottom
half of South African bank notes enable blind people to identify them as R10, R20,
R50, R100 and R200 respectively. The notes also have different widths.
For the benefit of the partially sighted there are geometric shapes on the front of
the bank notes: a diamond on the R10 note, a square on the R20 note, a circle on
the R50 note, a flat hexagon on the R100 note and a honeycomb hexagon on the
R200 note (South African National Council for the Blind, n.d.).
11.4 DEAFBLINDNESS OR DUAL SENSORY
IMPAIRMENT
The most important issues pertaining to hearing and visual impairments
were highlighted in the first sections of this chapter. However, there are
some individuals who have a dual sensory impairment, which means that
both their hearing and vision are impaired. These children, their parents and
teachers face unique challenges.
11.4.1 What is deafblindness?
Deafblindness is a unique disability as it impacts on the two main distance
senses (hearing and vision). These two senses play a critical role in
communicating and learning, moving around with confidence, and
interacting effectively with others. Losing one of the distance senses can
usually be compensated for by the other one. For example, people who are
deaf rely heavily on their vision (e.g. lip-reading), while people who are
blind make extensive use of their hearing.
Being deafblind means having both a hearing and a vision loss that are
present at the same time, affecting communication, mobility and access to
information and the environment (Deafblind International, n.d.). Typically,
these individuals have some degree of sight or hearing. People who are born
deafblind learn and develop independence differently from those who
acquired their disability later in life. The more experience a person had
prior to losing his vision or hearing (or both), the more resources he has to
draw upon and the better the prognosis for learning and communicating.
Frequently these learners are overprotected, which can lead to learned
helplessness (Beukelman & Mirenda, 2013). Challenging behaviour may
occur, especially when there is little functional engagement in activities of
daily living.
11.4.2 What causes deafblindness?
There are over 70 known causes of deafblindness. Causes can be
categorised into two main groups: congenital (when the child is born with
the vision and hearing impairment) or it may be acquired (it occurs later on
in life).
Some of the common causes in children include illness (e.g. meningitis and
asphyxia (when the body is deprived of oxygen)), prenatal infections (e.g.
maternal rubella and herpes), accidents, complications of premature birth
and genetic disorders (e.g. CHARGE syndrome and Usher syndrome)
(Tharpe, 2009). Usher syndrome is a genetic condition of people born deaf
or hard of hearing who gradually start to lose their sight due to retinitis
pigmentosa in late childhood. This condition accounts for more than 50 per
cent of individuals who are both deaf and blind (Millán et al., 2011). Early
symptoms include night blindness and loss of peripheral vision. Many
children who are deafblind also have additional disabilities, such as
physical disabilities, cognitive impairments (in more than 60 per cent of
cases) and challenging behaviour (Tharpe, 2009).
There is no cure for deafblindness, but the use of hearing aids and
spectacles may significantly improve hearing and vision. For some,
cochlear implants may restore functional hearing. Communication
interventions could include specialised communication systems or
technology (high and low tech), sign language instruction, and tactile input
– that is, touch in the palm of the hand. Strategies that help individuals to
become more independent include getting to know the structure of the
physical environment, using a white stick to feel their way forward (and let
others know they have low vision) and the use of a guide dog. Most
effective is holding the arm of a sighted guide who provides information
about the way ahead.
11.4.3 Characteristics of deafblindness
Individuals with deafblindness vary in terms of age, language skills,
abilities, interests and experiences. However, they share some common
challenges such as feelings of isolation (Hersh, 2013) and they may appear
to be disconnected from those around them. They also experience difficulty
in learning (through the visual or auditory mode, or both). They may also
have difficulty in attending to table-top activities, and struggle to master
reading and writing. In order to learn, they have to be actively involved in
the learning process and are dependent on tactile cues, objects, parts of
objects and clear models of behaviour in addition to speech. These learners
provide a real challenge to teachers as they require more time to examine
objects of interest and need opportunities to perform meaningful tasks
(Hersh, 2013). Furthermore, other people may be unsure about how to
interact with them and so avoid them, only making matters worse.
Deafblind individuals use a variety of communication methods, including
(but not limited to), the following:
Spoken languages (e.g. English, Afrikaans, Sepedi, isiXhosa)
Sign languages (e.g. SASL or ASL)
Tactile sign languages: the deafblind person holds the other person’s
wrists and feels their movements as they sign (Hersh, 2013).
Deafblind manual alphabets or tactile signing: the speaker signs the letter
onto the listener’s flat palm; the listener puts his hand over the speaker’s
vertical hand and feels the movements of the fingers to feel the shape,
movement and location of the signs (see Figure 11.7). People can use
one-handed or two-handed alphabets.
Tadoma: the deafblind person puts one hand on the other person’s chin,
lips, or throat to feel their movements as they speak (Hersh, 2013).
The deafblind block alphabet (Spartan): the person communicating with
the deafblind child draws large block capital letters on the child’s palm.
Each letter is written in the same location on the child’s palm. This is
frequently a way for deafblind children to communicate with unfamiliar
people.
Finger Braille, which entails typing onto six fingers as a Braille keyboard
Usually, blind or visually impaired people who lose their hearing later, or
deaf or hard-of-hearing people who depend on their lip-reading skills and
who have never learnt to sign, prefer tactile fingerspelling as sign
language can be difficult to learn.
Figure 11.7 Two-handed manual alphabet used by deafblind
individuals
Interpreting services such as sign language interpreters or communication
aides
Communication devices such as Tellatouch and its computerised version
known as TeleBraille (http://www.abledata.com)
Multisensory methods (e.g. Tacpac) that can be taught to very young
children with developmental delays (to help with pre-intentional
communication) and young children with learning difficulties
(http://www.tacpac.co.uk)
Braille alphabet cards that could be used by the partner by placing the
finger of the deafblind child on the Braille letter and so building the
message. Similarly, the deafblind child can touch the letters and the
partner can read the message.
Braille hand speech, which is similar to print on palm but requires that
both child and partner are able to position their fingers to represent the
configurations of the Braille letters.
One of our organization’s biggest challenges is to actually find
people who are deafblind. We are aware that there are thousands
of children who are deafblind and suffer in total isolation
(particularly in rural areas) because they do not know that help is
available. Once we have identified the person’s needs we provide
assistance. Training methods and modern technology enables
even those who are profoundly deaf and/or blind to communicate
and have access to information.
B
T
,
DBSA
KZN (S
C
A
N
B
, . .)
11.4.4 Classroom management strategies
It would be very difficult to accommodate all children with profound
deafblindness in inclusive settings, and research has shown that the majority
of these children require one-to-one support with communication, accessing
information and/or mobility (Hersh, 2013). Most people learn through their
visual and auditory modes. Whenever these are non-existent or limited,
learning is severely affected. However, there are some children who have
enough sight and hearing to benefit from inclusion. Challenges include
developing the language, communication and social skills that underpin
learning and living. Social isolation, loss of independence (often as a result
of overprotection) and feelings of reduced self-confidence and security, as
well as other people’s negative attitudes, are also frequently experienced by
this population, (Hersh, 2013).
Developing functional communication, which is the basis of learning, is the
biggest challenge for children with deafblindness and teachers alike. As
mentioned earlier, these learners often lack social skills because they have
no idea of the way friendships work or how to develop social closeness. It is
therefore not surprising that they may retreat into themselves and engage in
some challenging behaviour (as described in Chapter 7). There are some
effective strategies that can be used to facilitate communication
development, but they take a great deal of motivation and perseverance.
Remember that these children may have some residual hearing and use
hearing aids, or might have a cochlear implant and thus will benefit from
the strategies described earlier for children who have hearing impairment,
such as enhancing auditory input and careful positioning in the classroom.
They may also have some residual visual skills and will thus benefit from
strategies described earlier for children with low vision, such as enlarging
pictures and reducing glare.
Another critical aspect of teaching learners with deafblindness is providing
them with frequent repetition and routines (Hersh, 2013). Naturalistic
teaching strategies as well as the use of routines, manual signs and gestures,
and the extensive use of tactile cues (e.g. objects) for specific tasks as well
as schedules are critical. For example, objects could be used to represent the
school timetable, such as a songbook to represent school assembly, a ruler
to represent a maths class and a lunch box to represent break time. Of
course, once the child makes sense of the real object, parts of objects can be
used, for example a piece of chain to represent a swing. The critical feature
is that the input remains tactile.
The importance of functional instruction for children with deafblindness is
critical, as they learn most effectively when instruction occurs within
familiar routines, activities, and environments. The use of real items that
have a useful purpose rather than artificial ones (e.g. a real apple rather than
a plastic one) is needed for teaching new concepts and language
development.
11.5 CONCLUSION
In this chapter we described hearing, vision and dual sensory impairments
by looking at the characteristics of these impairments as well as the possible
causes. The emphasis, however, was on evaluating the most effective
approaches to teaching these learners and by exploring some of the
classroom adaptations that teachers have found fruitful.
Irrespective of the severity of a disability or the specific challenges learner
face, teachers have the ability to make or break learning.
I’ve come to the frightening conclusion that I am the decisive
element in the classroom. It’s my personal approach that creates
the climate. It’s my daily mood that makes the weather. As a
teacher, I possess a tremendous power to make a child’s life
miserable or joyous. I can be a tool of torture or an instrument of
inspiration. I can humiliate or humour, hurt or heal. In all
situations, it is my response that decides whether a crisis will be
escalated or de-escalated and a child humanised or dehumanised.
D H
G
,
, 2003
REFERENCES
Aarons, D. & Akach, P. 2002. South African Sign Language: one language or many? In Mesthrie, R.
(Ed.). Language in South Africa. Cambridge: Cambridge University Press.
American Foundation for the Blind (AFB). 2005. Educating students with visual impairments for
inclusion in society. A paper on the inclusion of students with visual impairments. Available at:
http://www.afb.org/Section.asp?SectionID=44&TopicID=189&DocumentID=1344&Mode=Print
(accessed on 23 February 2009).
American Foundation for the Blind (AFB). n.d. Available at: http://www.afb.org/ (accessed on 23
February 2009).
American Speech-Language-Hearing Association (ASHA). 2005. (Central) auditory processing
disorders [Technical Report]. Available at: http://www.asha.org/policy (accessed on 25 February
2009).
Antia, S.D., Jones, P., Luckner, J., Kreimeyer, K.H. & Reed, S. 2011. Social outcomes of students
who are deaf and hard of hearing in general education classrooms. Exceptional Children, 77(4): 489–
504.
Beukelman, D.R. & Mirenda, P. 2013. Augmentative and alternative communication. Supporting
children & adults with complex communication needs, 4th ed. Baltimore, MD: Paul H. Brookes.
Bornman, J. 2006. How to adapt books for children with visual impairment. Free State Libraries
Newsletter – Libraries: Learning better, Living better. October–December 2006.
Castillo, M.P. & Roland, P.S. 2007. Disorders of the auditory system. In Roeser, R.J., Valente, M. &
Hosford-Dunn, H. (Eds). Audiology: diagnosis, 2nd ed. New York: Thieme Medical Publishers.
Corn, A.L. & Lusk, K.E. 2010. Perspectives on low vision. In Corn, A.L. & Erin, J.N. (Eds).
Foundations of low vision: clinical and functional perspectives, 2nd ed. New York: American
Foundation for the Blind Press.
Dawes, P., Emsley, R., Cruickshanks, K.J., Moore, D.R., Fortnum, H., Edmondson-Jones, M. &
Munro, K.J. 2015. Hearing loss and cognition: the role of hearing aids, social isolation and
depression. PLoS ONE, 10(3): e0119616. Available at: http://doi.org/10.1371/journal.pone.0119616
Deafblind International (DbI). n.d. Available at: http://www.deafblind international.org/ (accessed on
23 February 2009).
Douglas, G., McLinden, M., McCall, S., Pavey, S., Ware, J. & Farrell, A.M. 2011. Access to print
literacy for children and young people with visual impairment: findings from a review of literature.
European Journal of Special Needs Education, 26(1): 25–38.
Erin, J.N. & Topor, I. 2010. Functional vision assessment of children with low vision including those
with multiple disabilities. In Corn, A.L. & Erin, J.N. (Eds). Foundations of low vision: clinical and
functional perspectives, 2nd ed. New York: American Foundation for the Blind Press.
Ginott, H. 2003. Between parent and child: the bestselling classic that revolutionized parent-child
communication (Revised and Updated). New York: Three Rivers Press. ISBN 0-609-80988-1.
Available at https://www.goodreads.com/work/quotes/248119-between-parent-and-child (accessed on
12 September 2016).
Glaser, M. & Van Pletzen, E. 2012. Inclusive education for deaf students: literacy practices and South
African Sign Language. Southern African Linguistics and Applied Language Studies, 30(1): 25–37.
Guardino, C. & Antia, S.D. 2012. Modifying the classroom environment to increase engagement and
decrease disruption with students who are deaf or hard of hearing. Journal of Deaf Studies and Deaf
Education, 17(4): 518–533. doi:10.1093/deafed/ens026
Hersh, M. 2013. Deafblind people, communication, independence, and isolation. Journal of Deaf
Studies and Deaf Education. doi:10.1093/deafed/ent022
Huebner, K.M. 2000. In Koenig, A.J. & Holbrook, M.C. (Eds). Foundations of education, volume I:
history and theory of teaching children and youths with visual impairments, 2nd ed. Sewickley, PA:
AFB Press.
Joseph, L. & Alant, E. 2000. Strangers in the house? Communication between mothers and their
hearing impaired children who sign. South African Journal of Communication Disorders, 47: 15–24.
Kamaraj, B. & Purohit, R. 2014. Mutational analysis of oculocutaneous albinism: a compact review.
BioMed Research International, 2014, Article ID 905472, 10 pages. doi:10.1155/2014/905472
Keith, R.W. 2007. Diagnosing (central) auditory processing disorders in children. In Roeser, R.J.,
Valente, M. & Hosford-Dunn, H. (Eds). Audiology: diagnosis, 2nd ed. New York: Thieme Medical
Publishers.
Keefe, D.H. & Feeney, M.P. 2009. Individuals with multiple disabilities. In Katz, J., Medwetsky, L.,
Burkard, R. & Hood, L. (Eds). Handbook of clinical audiology, 6th edition. Philadelphia: Wolters
Kluwer – Health.
Kivi, R. & Solan, M. 2015. Albinism. Healthline. Medically reviewed by Mark R. Laflamme, MD, on
23 November 2015. Available at: http://www.healthline.com/health/albinism
Landsberg, E. 2016. Visual impairment. In Landsberg, E., Krüger, D. & Nel, N. (Eds). Addressing
barriers to learning: a South African perspective, 3rd ed. Pretoria: Van Schaik.
Lane, H. 2005. Ethnicity, ethics, and the Deaf-world. Journal of Deaf Studies and Deaf Education,
10(3): 291–310. doi:10.1093/deafed/eni030
Lederberg, A.R., Schick, B. & Spencer, P.E. 2012. Language and literacy development in deaf and
hard of hearing children: success and challenges. Developmental Psychology. doi:10/1037/a0029558
Luckner, J.L., Slike, S.B. & Johnson, H. 2012. Helping students who are deaf or hard of hearing.
TEACHING Exceptional Children, 44(4): 59–67.
Mastropieri, M.A. & Scruggs, T.E. 2011. The inclusive classroom: strategies for effective
differentiated instruction, 4th ed. New Jersey: Merrill Prentice Hall.
Millán, J.M., Aller, E., Jaijo, T., Blanco-Kelly, F., Gimenez-Pardo, A. & Ayuso, C. 2011. An update
on the genetics of Usher syndrome. Journal of Ophthalmology, Article ID 417217, 8 pages.
doi:10.1155/2011/417217
Moores, D.F. 2010. The history of language and communication issues in deaf education. In
Marshark, M. & Spencer, P.E. (Eds). The Oxford handbook of Deaf studies, language and education,
2: 17–30). New York, NY: Oxford University Press.
Morris, C. 2016. Making sense of education: sensory ethnography and visual impairment.
Ethnography and Education. Early Online. doi:10.1080/17457823.2015.1130639
Pascolini, D. & Mariotti, S.P. 2010. Global estimates of visual impairment – 2010. Chronic Disease
and Health Promotion Department, Prevention of Blindness and Deafness, Geneva, Switzerland:
World Health Organization. Available at: http://www.who.int/blindness/VI_BJO_text.pdf (accessed
on 4 June 2016).
Penn, C. 1992. Dictionary of southern African signs for communication with the deaf. Pretoria:
Human Sciences Research Council.
Proske, U. & Gandevia, S.C. 2012. The proprioceptive senses: their roles in signalling body shape,
body position and movement, and muscle force. Physiological Reviews, 92(4): 1651–1697.
doi:10.1152/physrev.00048.2011
Reed, C.M. 2009. ASL, total communication and oralism: identifying shared characteristics of
school-based writing intervention programs for deaf and hard of hearing students, K-6. Seton Hall
University Dissertations and Theses (ETDs), Paper 246. Available at:
http://scholarship.shu.edu/dissertations (accessed on 4 June 2016).
Schlauch, R.S. & Nelson, P. 2009. Individuals with multiple disabilities. In Katz, J., Medwetsky, L.,
Burkard, R. & Hood, L. (Eds). Handbook of clinical audiology, 6th ed. Philadelphia: Wolters Kluwer
– Health.
Silberman, R.K., Bruce, S.M. & Nelson, K. 2004. Children with sensory impairments. In Orelove,
F.P., Sobsey, D. & Silberman, R.K. (Eds). Educating children with multiple disabilities: a
collaborative approach, 4th edition. Baltimore, MD: Paul H. Brookes.
South African National Council for the Blind (SANCB). n.d. Available at:
http://www.sancb.org.za/press.asp (accessed on 23 February 2009).
Spencer, P.E. & Marschark, M. 2003. Cochlear implants: issues and implications. In Marschark, M.
& Spencer, P.E. (Eds). Oxford handbook of Deaf studies, language and education. Oxford: Oxford
University Press.
Spungin, S.J. & Ferrell, K.A. 2007. The role and function of the teacher of students with visual
impairments. A position paper of the division on visual impairments. Council of Exceptional
Children. Available at: http://community.cec.sped.org/dvi/resourcesportal/ (accessed on 10 June
2016).
Stelmachowicz, P. & Hoover, B. 2009. Hearing instrument fitting and verification for children. In
Katz, J., Medwetsky, L., Burkhard, R. & Hood, L. (Eds). Handbook of clinical audiology, 6th ed.
Baltimore, MD: Lippincott Williams & Wilkins.
Storbeck, C. 2016. Educating the deaf and hard-of-hearing learner. In Landsberg, E., Krüger, D. &
Nel, N. (Eds). Addressing barriers to learning: a South African perspective, 3rd ed. Pretoria: Van
Schaik.
Stryker, D., Nielsen, D. & Luetke, B. 2015. Signing Exact English: Providing a Complete Model of
English for Literacy Growth. NERA Conference Proceedings 2015. Paper 2. Available at
http://digitalcommons.uconn.edu/nera-2015/2 (accessed on 6 September 2016).
Tharpe, A.M. 2009. Individuals with multiple disabilities. In Katz, J., Medwetsky, L., Burkard, R. &
Hood, L. (Eds). Handbook of clinical audiology, 6th ed. Philadelphia: Wolters Kluwer – Health.
Tobin, M.J. & Hill, E.W. 2015. Is literacy for blind people under threat? Does Braille have a future?
British Journal of Visual Impairment, 33(3): 239–250. doi:10.1177/0264619615591866
Vasconcelos, G. & Fernandes, C.L. 2015. Low-vision aids. American Academy of Ophthalmology.
Available at http://www.aao.org/pediatric-center-detail/low-vision-aids (accessed on 12 September
2016).
Vision Council. n.d. Available at: http://www.visioncouncil.org (accessed on 23 February 2009).
Westling, D.L. & Fox, L. 2009. Teaching students with severe disabilities, 4th ed. Upper Saddle
River, NJ: Pearson.
Wilkinson, M.E. 2010. Clinical low vision services. In Corn, A.L. & Erin, J.N. (Eds). Foundations of
low vision: clinical and functional perspectives, 2nd ed. New York: American Foundation for the
Blind Press.
Woolley, M. 1998. Think about being deaf. London: Belitha Press.
World Health Organization (WHO). 2010. International Statistical Classification of Diseases and
Related Health Problem, 10th revision (ICD 10). Available at
http://www.who.int/classifications/icd/ICD10Volume2_en_2010.pdf (accessed on 9 September
2016).
World Health Organization (WHO). 2014. Visual impairment and blindness. Fact sheet no. 282.
Geneva: World Health Organization.
Zwolan, T.A. 2009. Cochlear implants. In Katz, J., Medwetsky, L., Burkhard, R. & Hood, L. (Eds).
Handbook of clinical audiology, 6th ed. Baltimore, MD: Lippincott Williams & Wilkins.
12
Understanding children with
autism spectrum disorder
12.1 INTRODUCTION
Education is the key to a better and more fulfilling future for children, but
some face many barriers that make education a difficult goal tRecently,
researchers have published a huge
amount of work to prove that the measleso achieve. Too often the barriers
that are in the way of a proper education are imposed by others (their
knowledge, skills and attitudes), rather than by the abilities of the child. A
group that often faces these opportunity barriers is children with autism
spectrum disorder (ASD) (Strock, 2008).
ASD stretches over the lifespan and has many different faces, hence the
idea of a spectrum disorder. However, ASD is characterised by social
reciprocity impairment (resulting in difficulties with building relationships),
atypical communication (e.g. responding inappropriately in conversations
and misreading non-verbal interactions) and repetitive, stereotypic
behaviour (Hyman & Levy, 2013). Until 2013 the DSM-IV (Diagnostic and
statistical manual of mental disorders) included four separate categories:
autistic disorder, Asperger’s disorder, childhood disintegrative disorder, and
the “all other” diagnosis of pervasive developmental disorder not otherwise
specified (PDD-NOS). Two rare conditions, namely Rett syndrome and
childhood disintegrative disorder, were both listed as a PDD-NOS (Hyman
& Levy, 2013). However, researchers found that these separate diagnoses
were not consistently applied across different contexts, and in the DSM-5
(APA, 2013) they are no longer identified or described as separate
disorders.
Although the DSM does not address intervention strategies, determining an
accurate diagnosis is the first step in service delivery. The new classification
in the DMS-5 is intended to improve the diagnosis of ASD without limiting
the sensitivity of the criteria or substantially changing the number of
children being diagnosed (APA, 2013). Another change in the DSM-5 is
that it encourages earlier diagnosis of ASD by acknowledging that
individuals with ASD must show symptoms from early childhood even if
they only become recognisable once social demands start exceeding the
capacity of such individuals. This is an important change from DSM-IV
criteria, which were geared toward identifying school-aged children with
ASD (APA, 2013).
12.2 WHAT IS ASD?
ASD includes two main domains, and in order for a person to be diagnosed
with ASD, both have to be present. The first domain refers to social
communication and interaction across multiple contexts, while the second
focuses on restricted and repetitive patterns of behaviour, interests and
activities.
Figure 12.1 Two domains affected by ASD
These individuals therefore display difficulties across these two domains,
which range in terms of severity (the DSM-5 suggests three different levels
of severity) that will now be discussed. It is also important to underscore
that although learners with autism share the same core characteristics from
these two domains, ASD affects each individual differently, and it is the
combination of the communication and social interaction and the restricted
and repetitive behavioural patterns that cause them to behave in unusual
ways (Koudstaal, 2016).
12.2.1 Domain 1: Social communication and social interaction
across multiple contexts
Deficits in social-emotional reciprocity range from abnormal social
approach and failure of normal back-and-forth conversation; to reduced
sharing of interests, emotions or affect; to failure to initiate or respond to
social interactions (APA, 2013). Children with ASD may not make
appropriate eye contact, for example either by not looking at the
communication partner, by looking too briefly or by staring. Those who
do not know the child or who do not understand ASD may misunderstand
the child’s behaviour and view it as naughty, difficult or lazy, when in
fact, the child does not understand the situation or task, or has not read
the adult’s intentions or mood correctly. After having an onlooker stare
and comment on her child’s behaviour, a despondent mother of a young
boy with ASD said: “A damn good hiding would not help my son, since it
is not possible to beat someone’s disability out of them” (Cooper, 2001:
28).
Deficits in non-verbal communication skills range from poorly integrated
spoken and non-verbal communication to abnormalities in eye contact
and body language, to a total lack of facial expressions and non-verbal
communication (APA, 2013). Children with ASD not only have difficulty
in understanding the language and communication of others (receptive
language skills), but also in developing their own language and
communication skills (expressive language). This is true for speech as
well as for non-verbal means of communication. Many children with
ASD learn to speak late and some never develop speech at all. However,
even those who have speech find it difficult to use it to communicate
effectively. It is likely that they will need to be taught what the purpose
of communication is (such as requesting information), a means to
communicate (using pictures, photos, natural gestures, manual signs,
spoken or written words) as well as the pragmatic rules of
communication (who, what, where, when and how).
Deficits in developing, maintaining, and understanding relationships
range from difficulties in adjusting behaviour to suit various social
contexts, to difficulties in sharing imaginative play or in making friends,
and to the absence of interest in peers (APA, 2013). Children with ASD
are very literal thinkers and interpreters of language, often failing to
understand its social context (De Clercq, 2003), therefore they find it
hard to play and communicate effectively with peers, who may be
confused by their behaviour and may avoid or tease them.
12.2.2 Domain 2: Restricted, repetitive patterns of behaviour,
interests or activities
According to the DSM-5 (APA, 2013), at least two of the following
behaviour patterns should be present:
Stereotyped or repetitive motor movements, use of objects or speech (e.g.
simple motor stereotypes, lining up toys or flipping objects, echolalia,
idiosyncratic phrases) (APA, 2013). Children with ASD will not play
with toys in a conventional way, but instead spin or flap objects, or watch
moving parts of toys or machinery for long periods and with intense
concentration.
Insistence on sameness, inflexible adherence to routines, ritualised
patterns of verbal or non-verbal behaviour (e.g. extreme distress at small
changes, difficulties with transitions, rigid thinking patterns, greeting
rituals, the need to take same route or eat the same food every day) (APA,
2013). The fact that children with ASD have difficulty in thinking and
behaving in a flexible manner is shown in their restricted, obsessional or
repetitive imagination and play activities and, as they become older,
restricted interests. They will also have difficulty in adapting to new
situations, and prefer routine to change.
Highly restricted, fixated interests that are abnormal in intensity or focus
(e.g. strong attachment to or preoccupation with unusual objects,
excessively circumscribed or perseverative interest) (APA, 2013). Some
children develop a special interest in a topic or activity (e.g. dinosaurs or
string), which may be followed to extremes. All new skills tend to be tied
to the situation, which means that children with ASD will need specific
help to generalise skills.
Hyper- or hypo-reactivity to sensory input or unusual interest in the
sensory aspects of the environment (e.g. apparent indifference to
pain/temperature, adverse response to specific sounds or textures,
excessive smelling or touching of objects, visual fascination with lights
or movement) (APA, 2013; Sandin et al., 2012). This has implications for
the child’s home and school environment, and may explain their response
to changing clothes or food and to noise. Atypical eating (e.g. only eating
food of the same colour or not allowing different foods to touch on the
plate) is also common (Filipek et al., 1999).
12.2.3 Severity
ASD can vary in severity, with some learners displaying only mild
symptoms while in others they are more serious. The ASD severity is based
on the individual’s level of functioning in the two domains (APA, 2013).
These levels are described below:
Level 1: Requiring support
– Noticeable deficits in social communication
– Difficulty initiating interactions, and atypical or unsuccessful response
to others
– Limited interest in social interactions (e.g. can speak in full sentences,
but communication and attempts to make friends are odd and mostly
unsuccessful)
– Inflexibility of behaviour, interfering with functioning in one or more
contexts
– Difficulty in switching between activities
– Problems with organisation and planning, which impacts negatively on
independence
Level 2: Requiring substantial support
– Marked deficits in both spoken and non-verbal communication
– Noticeable social impairments, even with support
– Limited initiation of social interactions
– Reduced or abnormal responses to communication attempts from others
(e.g. can speak with simple sentences, but interaction is limited to
narrow special interests, and non-verbal communication is markedly
odd)
– Inflexible behaviour, making it difficult to cope with change
– Restricted/repetitive behaviours that appear frequently enough to be
obvious to the casual observer and interfere with functioning in a
variety of contexts
– Distress and/or difficulty changing focus or action
Level 3: Requiring very substantial support
– Severe deficits in both verbal and non-verbal communication
– Very limited, if any, initiation of social interaction, with minimal
response to communication attempts from others with few intelligible
words
– Inflexible behaviour
– Extreme difficulty in coping with change
– Restricted/repetitive behaviours that interfere significantly with
functioning in all spheres
– Great distress/difficulty changing focus or action
12.3 WHAT CAUSES ASD?
It appears that there is no single cause, although current research evidence
is pointing to a genetic predisposition with environmental interactions
(Hyman & Levy, 2013).
12.3.1 Genetic predisposition
Children who have a family member with ASD are at a higher risk (Sandin
et al., 2014). In fact, children with an affected sibling have a ten times
greater autism rate than the general population, while those with an affected
cousin have double this rate (Hyman & Levy, 2013).
ASD is also linked to other genetic disorders that have a known genetic
etiology, for example Rett syndrome, Angelman syndrome, Prader-Willi
syndrome, fragile X syndrome and tuberous sclerosis (Hyman & Levy,
2013; Landrigan, 2010).
ASD thus clearly does have a genetic component to it – researchers have
found that 20 out of 23 chromosomes have regions that may be important
for ASD, for example chromosome 2 (the second largest chromosome),
chromosome 7 (where genes for other language disorders exist) and
chromosome 15 (where genes for other developmental disorders have
already been identified (Hyman & Levy, 2013). Family studies which
compared the DNA of children with ASD with their parents found huge
DNA differences, which implies that one cause of ASD is DNA mutations;
in other words, large pieces of DNA go missing or are duplicated (Chaste &
Leboyer, 2012). The fact that so many genes are involved makes research
aimed at finding a single autism-linked gene very costly. However, if
identifying a specific gene is successful, this may have a significant impact
on how ASD is treated in future.
12.3.2 Environmental factors
Recently, researchers have published a huge amount of work to prove that
the measles, mumps and rubella (MMR) vaccine is not associated with
ASD (see Hyman & Levy (2013) for more details). Teachers should
reassure families that it is safe to have the MMR vaccine as there is no
scientific evidence to prove the contrary. However, if a pregnant woman is
infected with rubella (German measles), there is an increased risk of having
a baby with ASD, depending on the timing of the infection (Hyman &
Levy, 2013). Also, young children who have severe meningitis or
encephalitis (infection of the brain) may also develop symptoms of ASD
(Hyman & Levy, 2013). Research is also showing that some medication
taken during the first trimester of pregnancy (especially that which is used
to control epilepsy) increases the risk for ASD in the unborn child eightfold (Chaste & Leboyer, 2012). Recent research is also pointing to an
association between ASD and airborne mercury in certain locations, but this
needs to be further explored (Landrigan, 2010).
12.3.3 Other impairments often associated with ASD
A number of other impairments have been noted in the literature to cooccur with ASD. These include the following:
Intellectual disabilities. Older studies estimated that up to 75 per cent of
children with ASD also have intellectual disabilities (Hyman & Levy,
2013), while more recent work estimates this figure to be around 50 per
cent (Landrigan, 2010).
Epilepsy. Overall, epilepsy is reported in around 25 to 30 per cent of
individuals with ASD (Hyman & Levy, 2013; Landrigan, 2010; White,
Oswald, Ollendick & Scahill, 2009).
Sleep disorders. Sleep disorders are reported in 50 to 70 per cent of
children with ASD (Hyman & Levy, 2013). The most commonly
reported problems include difficulty in falling asleep, waking up
frequently during the night and early morning awakening (Richdale &
Schreck, 2009). It has also been reported that children with ASD may be
happy and contented with only a few hours of sleep per night (Koudstaal,
2016).
Psychiatric disorders. Children with ASD have an increased risk for
depression, mood disorders, anxiety and ADHD (Hyman & Levy, 2013).
Anxiety, stress and panic in the school context can lead to an inability to
focus on instruction, to understand basic social interaction and to
participate in classroom activities (Hoffman, 2013). Parents have also
cited anxiety as one of the most distressing symptoms (Dawson &
Burner, 2011).
12.4 CLASSROOM STRATEGIES FOR MANAGING
CHILDREN WITH ASD
There is no single treatment for ASD (McPartland & Klin, 2006), but there
is general consensus among all who work in the field that the earlier
intervention (including appropriate education) starts, the better the longterm outcomes. These children should be included in positive, childdirected programmes, which also incorporate parents and peers as
facilitators (Ferraioli & Harris, 2011). In other words, children should be
viewed through a zoom lens! These early intervention programmes should
focus on basic communication development such as turn taking, joint
attention to a task, as well as the role of other people in their environment
as communication facilitators. There is scientific evidence to show that
targeted early intervention can result in significant gains in language and
cognitive abilities, increase social skills, and decrease anxiety and
challenging behaviour in children with ASD (Dawson & Burner, 2011).
Based on multidisciplinary assessment, intervention and education
combined with cognitive, behavioural, environmental, sensory, visual and
structural strategies and then tailored to the needs of each individual child
are most effective (Hoffman, 2013). Most individuals will improve over
time, but difficulties with communication, social adjustment and
independent living continue into adulthood (Woodbury-Smith & Volkmar,
2009). Accommodating these learners in the classroom requires teachers to
take the following issues into account:
Their possible difficulty in engaging in the classroom due to challenges
related to filtering unnecessary information, selective attention and
difficulty attending to meaningful aspects of the learning activity,
especially when they are not explicitly stated (Denning & Moody, 2013)
Their difficulty in generalising learning (every situation appears different
to the child) due to detailed thinking (explained later in this chapter
where aided communication is discussed) (Peeters & Gillberg, 2003). For
example, typically developing children use the word “car” to refer to all
types of vehicles, and only later do they differentiate between cars, taxis,
buses, trucks, and so forth. Children with ASD fail to see the larger
category (“cars”) and focus on the detail that distinguishes each of the
vehicles.
Their difficulty with incidental learning (everything needs to be taught in
a directive manner) and with learning new material in the classroom
(Denning & Moody, 2013)
Their literal understanding of language and of the world in general (they
have difficulty with metaphors, sarcasm, making inferences, etc.)
Their difficulty in becoming involved in group activities including play
and games as a result of the problems they experience with socialisation
Their possible reaction to overstimulation (which manifests as “odd
behaviour”)
Their lack of motivation, which may result in challenging behaviour.
These behaviours (e.g. crying, running away) might look like simple
naughtiness or non-compliance, but might really be their only way of
indicating the need for help or attention, to escape from stressful
situations (task avoidance), to obtain desired objects, or to protest against
unwanted events (see Chapter 7).
12.4.1 Classroom arrangement for optimal learning
Classroom furniture (e.g. bookshelves, room dividers, filing cabinets,
carpets) should be arranged in such a way that it provides clear, visual
boundaries. Teachers can even consider using different coloured insulation
tape or masking tape to mark designated areas on the floor. Children with
ASD do not automatically segment their environments like typically
developing children do, and therefore large open areas can be difficult for
them to cope with.
Likewise, teachers should also aim to use natural lighting as optimally as
possible, as fluorescent lights can be difficult for children with ASD as they
are negatively affected by the constant flickering and buzzing of these lights
(Jackson, 2002). Children with ASD can be encouraged to wear a cap with
a visor to minimise the effect of the light. Blinds and curtains can be used to
control the amount of light in the classroom in order to create a warm and
calm classroom environment. In order to minimise auditory distractions,
carpets can be used, and special rubber caps can be placed under all chairs
and tables so that they do not make a noise when children move about.
It is for this same reason that children with ASD should not be seated on the
carpet during circle time, but should remain on their chairs, as this provides
them with an additional sense of physical boundaries and hence security.
12.4.2 Predictable routines and visual schedules
All individuals with ASD thrive on predictable routines; in other words, the
activities that learners perform without prompting or supervision (Denning
& Moody, 2013). When something unexpected happens, these children
have difficulty coping, and some stereotypical behaviour such as rocking
and repeating the same word or phrase might occur. These behaviours have
a calming effect on such children, and efforts should be made to teach them
gently how to cope with changes in a routine (Jackson, 2002). The best way
to prevent these behaviours from occurring and helping children to cope
with change is to provide them with a very clear structure and a set daily
routine (including for play).
Visual schedules thus aid children with ASD because they do the following:
Help with the organisation of time and the sequence in which activities
will take place (sequential memory), as these schedules use the so-called
“first–then” strategy – that is, “first you do ___, then you do ___”, rather
than an “if–then” approach (i.e. “if you do ___, then you can do___”).
The child learns that if he has completed the first expectation (e.g. his
written worksheet), then he can move on to his next visually scheduled
task or activity (e.g. playing on the computer) (Koyama & Wang, 2011)
(see Figure 12.2).
Figure 12.2 Example of a “first-then” page
Help the children to prepare for the activity and also organise and predict
daily and weekly events as they provide a specific structure. Visual
schedules clarify the fact that activities happen within a specific time
period (e.g. understanding that computer time is coming, but only after
work time), and also point out that changes might occur. This helps to
reduce the children’s levels of anxiety and therefore also reduces
challenging behaviour.
Help the children move between activities and environments
independently (transitioning) by telling them where they are to go next
(Wendt, 2009). Transitions are particularly difficult for children with
ASD. Those who are very distractible might need to take the item (card
or object) off the visual schedule and carry this with them to the next
activity in order to make the transition easier.
Help to increase the children’s motivation to complete activities that they
do not enjoy by strategically alternating these activities with highly
motivating ones.
Help children with receptive language problems (understanding) to know
what is expected of them.
Help learners to attend to and focus on the material through priming.
Priming is related to providing learners with access to material and
letting them know in advance what will happen during an activity. This is
beneficial to learners with ASD as it helps them to create connections
with new class content and thereby increases their likelihood of attention,
work completion and appropriate responses (Denning & Moody, 2013).
Visual schedules should be taught directly and used consistently. They are
not something that is put up in the classroom to act as an incidental teaching
tool. A visual schedule will assist teachers at the start of each day by
ensuring that all children are familiar with the day’s programme, and she
can refer to it frequently throughout the day (Ferraioli & Harris, 2011). For
example, a visual schedule lays out the day’s activities, as explained in
Chapter 7. Having a schedule taped to the learners’ desks may also be
helpful, as they can look at it themselves and know what is coming next. It
can also be added to a keyring, which can be attached to their school bags.
They can move the activity picture or symbol to the finished section on the
board before moving on to the next activity. Sometimes there is a fear that
this type of visual schedule will make children with ASD even more rigid,
thereby causing even more difficulty in coping with change. However, the
exact opposite is true. Visual schedules are especially helpful when the
schedule changes as one can show the child with ASD visually that the
activity that was planned could not happen for one reason or another, or that
something else has come up that was not planned. In these cases teachers
can use a “wild card” (i.e. something that the child is taught represents
unplanned activities).
Visual schedules should not be considered a strategy from which learners
with ASD should be gradually weaned. Instead, they should be viewed as a
strategy that has the potential to increase independent functioning
throughout their lives (Dawson & Burner, 2011).
12.4.3 Avoid change – be consistent
Children with ASD are easily overwhelmed by minimal change, are highly
sensitive to environmental stressors, and sometimes engage in challenging
behaviour rituals when they become stressed or tired, or experience sensory
overload. Furthermore, they are anxious and tend to worry obsessively
when they do not know what to expect (e.g. in one teacher’s class, learners
must wait for an instruction before sitting down, while another teacher
wants them to sit at their desks without an instruction).
Stop and reflect
What are the important rules in your classroom? How do you react when learners do
not stick to them? How are they different or similar to those of your colleagues? Could
different rules possibly confuse the learners?
What can a teacher do to make life easier in the classroom? First, by
providing a safe and predictable environment with a consistent daily
routine, for example by using visual schedules as described above. Second,
by minimising transitions – for children with hyperactivity, providing more
transitional activities helps them to stay on task, but for children with ASD
this has exactly the opposite effect – frequent transitions take away their
security and thereby induce stress. If, on the other hand, the child with ASD
knows what to expect, he will be able to concentrate on the task at hand.
Finally, surprises should be avoided: prepare the child thoroughly and in
advance for special activities such as a birthday or Christmas, altered
schedules, or any other change in routine, regardless of how minimal this
might appear to the teacher (Bornman, 2003).
12.4.4 Communication skills in the classroom
Seeing that one of the characteristics of children with ASD is their lack of
motivation to communicate intentionally, one must be careful not to push
them too hard or too soon to learn new forms of communication. However,
research is showing that children with ASD are often provided with very
few communication opportunities – often as little as one per day (Koegel,
Matos-Fredeen, Lang & Koegel, 2011). When providing communication
opportunities, it is important to do so when the child is motivated – for
example if the child really wants to work on the computer, the mouse can be
placed out of the child’s reach, “forcing” him to ask the teacher to help.
Children’s own vocalisations and natural gestures should be used to expand
naturally occurring situations. The initial goal should be the development of
natural speech and language. When working with children with ASD, it
seems clear that the multimodal approach (using speech, natural gestures,
manual signs and graphic symbols) is the most beneficial for
communication training (Bornman & Alant, 1999). As we know that visual
learning is one of their main skills, and we use a strengths-based approach
throughout this book, augmentative and alternative communication (AAC)
strategies are particularly useful for these children. The various
interventions for the unaided and aided communication modes follow.
UNAIDED COMMUNICATION
The use of manual signs combined with speech is the most commonly used
method for training communication skills in children with ASD. When
speech is used in combination with signs (the key elements of the message
are also signed simultaneously), this is known as multi-modal
communication. However, not every single word is signed, only the most
important concepts, hence keyword signing. In South Africa, signs from
SASL or Makaton are typically used. The advantages of unaided
communication is the fact that learners do not have to carry anything with
them but only have to rely on their own body, making it particularly
suitable for ambulatory individuals, such as the majority of these children.
Because manual signs require no external equipment (unlike graphic
symbols or devices), this would imply that children cannot lose them, leave
them behind or break them (Wendt, 2009). However, this brings to mind
questions such as: “Which gestures should I teach first? Where do I start?”
A few factors, together with functionality (i.e. what the child can do with
the particular word) are important for the selection of initial vocabulary:
Iconicity. This refers to the ease by which the meaning of a sign is
guessed by people who do not know it. Highly iconic signs (transparent
signs) (e.g. “eat” and “drink”) are learnt more easily than less-iconic
signs (e.g. “want”). The strong resemblance between the manual sign and
the object or action it represents may help children with ASD to learn
manual signs quite quickly (Wendt, 2009). Spoken language is not iconic,
except for a few words that imitate the sound, such as “click” or “beep”
(see Figure 12.3).
Figure 12.3 Iconicity of SASL signs
Motor complexity. Four motor elements make it easier to learn certain
signs: those signs that require contact between both hands, for example
“work”; those signs where both hands make the same movement
(symmetrical), for example “ball”; those signs that are produced within
the visual field of the user, for example “red”; as well as those signs that
require a single simple handshape, for example “drink”. These signs are
all shown in Figure 12.4.
Figure 12.4 Motor complexity of SASL signs
Handshape. Signs that require that the same simple handshape be
repeated (e.g. “play” or “belt”) are easier to learn (see Figure 12.5).
Figure 12.5 Repeated handshapes of SASL signs
Signs that are similar in shape and meaning should not be taught at the
same time as this may be confusing, for example “play” and “want”. The
signs selected should also be of high motivational value to the child and
meaningful to use.
Manual signing is more effective when taught to children who have already
acquired the skill of imitation. The training method consists of various
levels of prompting, starting with modelling, physical guidance (hand-overhand) if necessary and verbal prompts, which are systematically faded.
Instruction should always be conducted within naturally occurring events
with strategies such as milieu teaching approaches. The use of speech and
signing is incorporated in natural language teaching.
Very often, however, manual signs may be difficult to understand by
untrained individuals and thus this limits the number of interaction partners.
The possibility of such situations occurring should be anticipated.
Nonetheless, unaided systems (including natural gestures and manual signs)
can play a significant role as one of the components of a multimodal
communication system for this population.
AIDED COMMUNICATION
Unfortunately not everyone in the community understands manual signs
and therefore the child with ASD might have to rely on graphic symbols
(e.g. Picture Communication Symbols or Rebus) or objects. These symbols
can be either displayed on low-technology displays, for example object
boards, communication boards, bags or E-Tran (symbols attached to a
frame), or on high technology, for example speech-generating devices such
as the GoTalk or DynaVox Xpress. If the individual can read and spell,
various keyboard-based devices can be considered, such as a tablet with
Proloque2Go. The different low-technology systems are shown in Table
12.1.
Table 12.1 Different low-technology-aided systems
Object board
Communication board showing PCS™1
Object board
Communication board showing PCS™1
Communication bag in E-Tran format
showing PCS™1
E-Tran showing PCS™1
1 Picture Communication Symbols (PCS) is a registered trademark of Mayer Johnson, a
Tobii Dynavox Company of Pittsburgh, PA (www.mayer-johnson.com)
One strategy that is often very helpful is the use of objects to represent
spoken communication, for example using a bag to represent shopping. The
advantages of using 3D objects (tangible objects) are that they offer
concrete representations of abstract concepts and are visible and stable (one
can see them for an extended period, whereas words “disappear” the
moment they are spoken) (De Clercq, 2003). By doing so, one focuses on
the strengths of individuals with ASD and not the weaknesses. These
symbols are also excellent for use in visual schedules. Individuals with
ASD often experience challenging behaviour when they face changes in
their routines and are unable to predict the sequence of events. Visual
representations (e.g. by using objects) facilitate this prediction process
(Koyama & Wang, 2011). However, emphasis was also placed on what
Peeters and Gillberg (2003) call detail thinking. This means that care has to
be taken when selecting a symbol as individuals with ASD frequently see
detail in objects of which others are not even always aware. For example,
where one would see different types of bicycle as a collection of bicycles,
children with ASD may see them as very distinct, for example in one they
would focus on the pedals, in another on the frame, or maybe on the seat.
Hilde de Clercq (2003), the mother of a young man with ASD, explained
how traumatic a shopping experience was when her husband accidentally
took the bag that represented “swimming” when they went “shopping”. It is
therefore always best to teach children with ASD in the actual settings
where they will use these skills.
12.4.5 Picture Exchange Communication System (PECS)
After having alluded to the value of using visual symbols for these learners,
one specific naturalistic instructional technique that has proved to be
effective with children with ASD will be described, namely the Picture
Exchange Communication System (PECS). It is an effective tool for
helping children to communicate without relying on spoken words, which
means that children with ASD who have little or no speech will benefit
particularly from using it. In addition, it also allows the child to make
choices (e.g. “Do you want the blue pencil or the red one?”) and
communicate needs, and when that happens, challenging behaviours can
often be reduced and the child becomes happier. PECS is typically
introduced using pictures of desired objects (such as food or toys). When
the child wants one of these items, he gives the picture to a communication
partner such as a parent, therapist, caregiver or another child. The
communication partner then hands the child the food or toy, thus
reinforcing communication. For example, Debbie gives the symbol for
“glue” to her teacher and in turn receives the real glue, enabling her to
participate in a cutting and pasting activity in the classroom. Ultimately, the
pictures can be replaced with words and sentence strips (e.g. “I want the
glue, please.”) (see Figure 12.6).
Figure 12.6 Example of a PECS suitcase showing
PCS™1
1 Picture Communication Symbols (PCS) is a
registered trademark of Mayer Johnson, a Tobii
Dynavox Company of Pittsburgh, PA (www.mayerjohnson.com)
The PECS protocol is divided into six different training phases (Bondy &
Frost, 2009):
(i) Teaching the communication exchange: the child is taught to request, for
example to hand over a graphic symbol to request a particular object
(e.g. “I want nail polish”).
(ii) Teaching persistence: the child is taught to seek out the communication
partner (e.g. the teacher) wherever she may be in the classroom and then
hand over the graphic symbol. In this phase children are also taught to
make eye contact with the teacher when requested to do so (e.g. “Look
at me”).
(iii) Discriminate training: the child is taught that different graphic symbols
represent different objects, and he is provided with different cards, as is
shown in the suitcase example (Figure 12.6).
(iv) Teaching the “I want” sequence: the child is taught to use a sentence
strip and to combine two graphic symbols, namely the “I want” symbol,
with the desired object.
(v) Teaching a response to “What do you want?”: the child is taught that he
can use his “I want + desired item/activity” to respond to simple
questions.
(vi) Teaching the use of additional sentence starters: the child is taught that
he can also initiate sentences with: “I see…; “I have…: I hear…”, and
so forth.
Many people believe that PECS can also be used to create visual schedules
(calendar systems) for children, but this is incorrect. This confusion
probably stems from the fact that the same graphic symbols that are used
for PECS are frequently used for creating visual schedules, but this is not
PECS – it is simply using graphic symbols to create a visual schedule.
PECS does not refer to the individual graphic symbols, but is the exchange
of the graphic symbol as a form of communication, not the symbol itself.
The introduction of PECS can be a long and drawn-out process taking
months to complete. For a family facing a lifetime with a child who has
little or no functional speech, PECS can definitely be one of the modes that
addresses the lack of communication. There is also research evidence
showing that PECS increases spoken communication in children with ASD
(Koegel et al., 2011).
12.4.6 TEACCH
TEACCH (Treatment and Education of Autistic and related
Communication-handicapped Children) is one of the educational
approaches that is implemented worldwide (including South Africa) for this
population (Koudstaal, 2016). It is based on the notion that people with
ASD process visual information more easily than verbal information, and
consists of the following four components:
Physical structure: the way in which the physical environment is set up
and organised; in other words how the classroom is arranged, as
described earlier
Daily schedules: which include both classroom timetable and individual
schedules (see the discussion on visual schedules in section 12.4.2)
Work systems: the systematic and organised presentation of tasks or
materials in order for children to learn to work independently without
constant directions from the teacher. Each work system should address
the following four questions:
– What is the work (nature of the task) that I have to do?
– How much work (how many tasks) should I do in a specific time?
– How will I know that I am progressing and when I will be finished?
– What happens next? (What happens after the work is completed?)
Visual structure and information: incorporating concrete visual cues into
the task or activity itself so that the child will not have to rely on the
teacher’s directions and/or prompts in order to understand what to do.
Hence these visual cues increase the learner’s ability to work successfully
and independently.
TEACCH also highlights fun with others for developing social skills. The
goal is thus to acquire social skills and experience positive feelings with
other people to improve social reciprocity. In a randomised control study in
Japan, the researchers reported that children with high-functioning ASD
were able to develop social skills and reciprocity using TEACCH, and their
mothers’ stress was reduced (Ichikawa et al., 2013).
Children with ASD often have intense fixations on narrow topics of interest
and tend to lecture on them, ask repetitive questions about them, and have
difficulty in letting go of ideas. Sometimes they refuse to learn about
anything outside their limited field of interest.
Stop and reflect
One young boy with ASD with whom I had the privilege of working had a fixation on
electrical wires and cords. After an outing to the greengrocer, which focused on
healthy eating habits and vegetables, all children were asked to draw something that
related to the outing. Can you guess what this little boy drew? The cash register –
complete with every single electrical wire and cord that you could possibly imagine!
So if he were in your class, how would you go about managing him? First,
he should not be allowed to constantly discuss or ask questions about his
isolated interests. However, as it is difficult to avoid this completely, one
could consider putting aside a specific time during the day when the child
could talk about his particular interest. Second, positive reinforcement
could be used to shape a desired behaviour – that is, praising the child for
simple, positive social behaviour that is taken for granted in other children.
Children with ASD respond well to compliments (e.g. in the case of a child
who asks too many questions, the teacher might consistently praise him as
soon as he pauses and congratulate him for allowing others to speak)
(Williams, 1995). Third, a child might not want to do assignments outside
his area of interest, and teachers must then set firm expectations for
completion of class work. It must be made very clear to the child that he is
not in control and that he must follow specific instructions. At the same
time, however, meet the child halfway by providing him with opportunities
to pursue his own interests (e.g. in a drawing activity he can be allowed to
draw anything that he likes).
Fourth, in some cases the child’s fixation can be used as a way to broaden
his repertoire of interests (Williams, 1995). For instance, during a unit on
the different habitats of elephants, and in particular the Knysna Forest, the
child who is fixated on elephants can be led not only to study the forest
animals but also to study the forest itself, as this is the animals’ home. He is
then motivated to learn about the local people who are forced to chop down
the animals’ natural habitat in order to survive. At first it might be
necessary to incorporate the child’s special interest into all his assignments
before gradually introducing other topics (e.g. offer grammar sentences,
story sums, and reading and spelling tasks about elephants).
12.4.7 Sensory integration therapy (SIT)
Sensory integration therapy (SIT) is among the most common interventions
for learners with ASD (Lang et al., 2012; Pfeiffer, Koenig, Kinnealey,
Sheppard & Henderson, 2011). It typically involves some combination of
the child wearing a weighted vest, being brushed or rubbed with various
instruments, riding a scooter board, wringing, sitting on a bouncing ball,
being squeezed between exercise pads or pillows, and other similar
activities (Lang et al., 2012). There seemed to be positive research evidence
that SIT was effective in reducing self-injury challenging behaviour
(Thompson, 2011) and increasing functional behaviour such as social
interaction and play (Pfeiffer et al., 2012). However, after a large-scale
systematic review involving 25 published research studies, Lang et al.
(2012) concluded that there is at present a lack of scientific evidence to
prove that SIT is effective or even valuable. In fact, these authors argue that
there might even be evidence to show that SIT may increase challenging
behaviour as it provides access to enjoyable activities, attention from
therapists and breaks from work when challenging behaviour erupts.
Further research in this area is therefore needed.
12.4.8 Addressing poor concentration
In the section on the arrangement of the classroom, it was noted that
children with ASD are easily distracted (either visually or auditorily), which
leads them to be distracted, disorganised and unfocused (not necessarily
because of a short attention span, but because they focus on detail and
stimuli that are not relevant as a result of their detailed thinking patterns). In
addition, it might also appear as if they are daydreaming.
How should a teacher address this? First, by attempting to break
assignments into smaller, manageable units, with frequent feedback and
encouragement to stay focused. Children with ASD often have difficulty in
estimating how long a piece of work will take, and then cannot make the
deadline, or they might spend all their free time on the task at hand because
they feel it must be perfect and they are unable to tell when it is good
enough to count as finished (Sainsburg, 2003). Teachers should therefore
give learners an estimate of how long a task should take.
Second, teachers can time the work sessions as this usually helps children
with ASD to organise themselves (Williams, 1995). Classwork that is not
completed within the time limit (or that is done carelessly) must be made up
during the child’s free time (i.e. during break time or during the time used
for pursuit of special interests). Children with ASD need firm expectations
and a structured programme that teaches them that compliance with rules
leads to positive reinforcement (rewards) while these are withheld for
challenging behaviour (Koegel et al., 2011) Providing learners with ASD
with opportunities to make choices regarding the order in which they want
to complete a task (e.g. first colouring in and then cutting out, or vice versa)
and the use of stimulus materials (e.g. painting versus colouring) improved
their accuracy, productivity and mood, and also reduced challenging
behaviour. These findings support the use of providing choices as a
teaching strategy to improve the academic performance of children with
ASD during curricular activities.
Third, a teacher might find it necessary to decrease the child’s homework or
classwork. Teachers might also find that it helps to place children with ASD
at the front of the class and to direct frequent questions at them (starting
with their names to help them attend to the lesson by addressing them
directly, e.g. “Pretty, can you tell me who Dingaan was?”). Apart from
calling the child’s name, a non-verbal signal can also be used (e.g. a gentle
pat on the shoulder), or if a buddy system is used, the buddy can be trained
to remind the child with ASD to concentrate on the task or listen to the
teacher. Children with ASD need to be encouraged constantly to leave their
inner thoughts behind and to focus on the real world (Williams, 1995).
12.4.9 Addressing academic difficulties
Owing to the fact that autism is a spectrum disorder, intelligence includes
the whole range: from below average to above average, but high-level
thinking and comprehension skills are usually lacking. These children tend
to be literal thinkers, so teachers should avoid slang or idiomatic speech.
They may also have difficulty interpreting tone of voice and facial
expressions, so a sarcastic comment: “Oh, that was great!” may be
perceived as a positive statement and may consequently reinforce negative
behaviour. Moreover, teachers should not rely on these children’s
understanding of meaningful looks (also known as an if-looks-could-kill
look) that the other children in the classroom can easily identify. Nita
Jackson (2002: 20), a young adult with high-functioning autism, explains:
“I discovered that I couldn’t comprehend people’s facial expressions … I
used to laugh when somebody cried because I thought the person was
laughing.” Sometimes children with ASD have pedantic speaking styles
and impressive vocabularies, which give the false impression that they
understand what they are talking about when in reality they are merely
parroting what they have heard or read (Sainsburg, 2003). Problem-solving
skills are also poor, and they do not realise that they may ask a teacher or a
peer for help.
Certain things that teachers can do in the classroom will make life a lot
easier. Teachers should never assume that children with ASD understand
something just because they repeat word for word what they have heard –
there is a huge difference between this type of parrot speech and
understanding. The same applies to reading – they are often able to read
fluently, but their reading comprehension might be weak, so teachers should
not assume that because they are fluent readers they understand the text.
Remember the “RAP” strategy described in Chapter 11? First, learners
Read the paragraph, then they Ask themselves about the main idea and two
details, and finally they Paraphrase the paragraph by putting it into their
own words (Denning & Moody, 2013; Luckner, Slike & Johnson, 2012).
Repeat instructions at least twice and also give them in writing (Jackson,
2002). Some learners will benefit from the use of audio-recorded lessons,
particularly if they find it difficult to take notes. In such cases, lessons can
be recorded and the learner can play them back at any time. Abstract
concepts will require more explanation and simplification – often tapping
all a teacher’s creativity. For assessment activities, teachers should allow
multiple means of expression to allow learners with ASD to effectively
demonstrate their knowledge, for example through the use of photo essays,
poetry, and movies (Denning & Moody, 2013). Teachers should remember
that these children typically do not generalise from specific contexts to
overall principles. For example, they will not understand that “stay away
from the swimming pool” also forbids playing in fish ponds, dams,
manholes and quarries (Sainsburg, 2003).
12.4.10 Addressing emotional vulnerability and developing
social competence
Children with ASD often do not have the emotional resources to cope with
the demands of the classroom and of the social context. This means that
they not only have to have been taught the curriculum, but also the hidden
curriculum (those rules that are not taught, but that teachers assume all
children know, for example knowing how to line up to go outside)
(Mercado, 2007). These children are easily stressed because of their
inflexibility and low self-esteem (Sainsburg, 2003). When they become
adolescents, they may be prone to depression (Jackson, 2002). To
complicate matters more, these individuals do not understand the complex
rules of social interaction; are naïve (typically developing peers often try to
manipulate children with ASD into breaking a school rule); are extremely
egocentric; may not like physical contact; talk at people instead of to them;
do not understand jokes, irony or metaphors; use inappropriate gaze and
body language; seem to be insensitive and lack tact; misinterpret social
cues; have well-developed speech but poor communication; and are easily
taken advantage of (as they do not perceive that others sometimes lie or
trick them). No wonder that Claire Sainsburg (2003) describes ASD as an
“Oops-Wrong-Planet” feeling, leaving her feeling like a woman from Mars
on the playground. Interacting with people and coping with the ordinary
demands of everyday life is a huge burden.
Teachers have a significant role to play in helping children function
optimally in the classroom. They should teach the children how to wait their
turn and share materials, and know when they should be quiet and when
they can talk. Moreover, teachers should teach them coping strategies to
prevent outbursts when stress overwhelms them, for example by using the
traffic light system described in Chapter 7 (Table 7.5). Be aware that
adolescents are prone to depression, and teachers should therefore be on the
lookout for any early signs. Because children with ASD are often not in
touch with their feelings and cannot seek comfort from others, it is critical
that depression be diagnosed quickly (Williams, 1995). Always address
children with ASD in a calm, predictable and matter-of-fact way, while at
the same time showing compassion and patience.
In order to foster social relationships and friendships and to prevent
bullying and teasing, teachers should attempt to educate peers about the
child with the disability by describing the condition and its effect. Stories in
which the hero is a child with a particular disability work well for younger
children (Bornman, Collins & Maines, 2004), while older children prefer
class discussions. This may prevent them from always being misunderstood
and at the same time it promotes empathy and tolerance in the other
children (Jackson, 2002; Sainsburg, 2003). Another strategy is to highlight
the child with ASD’s proficient academic skills during cooperative learning
situations (i.e. good reading skills, extensive vocabulary, good memory,
etc.) so that the peers view him as an asset, and the child is more likely to
be accepted into the group (Ferraioli & Harris, 2011).
Most children with ASD want friends but they simply do not know how to
interact. They should be taught how to react to social cues and be given
specific responses that they can use in social situations. Teach them what to
say and how to say it, and then role play it. Although these children have
difficulty in understanding other people’s emotions, they can learn the
correct way to respond. One technique that is being used more and more to
improve social behaviour is social stories (Gray, 2000). A social story is
written to provide individuals with ASD with the social information needed
to cope in a specific situation, (e.g. how to wait their turn) (O’Connor,
2009). Social stories use simple sentences and pictures to demonstrate the
social behaviour and the feelings and reactions, for example: “When I wait
my turn, the other kids in my group are happy.” It is important that these
stories are written in a manner that is easily understood by the child. The
permanence of the text and the illustrations provide an opportunity to revisit
the story, thereby allowing the concepts in the story to become consolidated
(O’Connor, 2009). More recently, social stories have also been presented on
iPads (Vandermeer, Beamish, Milford & Lang, 2013). See Figure 12.7 for
an example of a social skill story written in symbol format.
Figure 12.7 Example of a social skills story
Source of symbols: Detheridge, Whittle & Detheridge (2002)
Story: Author’s own
Teachers have frequently reported satisfaction implementing social stories
to change behaviour and state that it is easy to develop, implement and
acquire limited resources (Foster, 2015). Research has shown that social
stories combined with visual and behaviour strategies have brought change
and success in intervention with children with ASD (Hoffman, 2013;
Vandermeer et al., 2013).
12.5 A TALE OF TWO MOTHERS
Following is a true story of a mother whose pre-school son has ASD.
My son is six years old, and currently in Grade R at a mainstream school. We have
not yet decided if we would like him to repeat Grade R, or take him out of school, or
home school him, or whether we will consider an alternative placement. As parents
we want to build on his strong points and make a decision that will be right for him –
we don’t want him to suffer.
He is really good at drawing; he only started about eight months ago and we can’t
believe the progress he’s made! He also has an intuitive feel for the computer. He
enjoys playing on it at home and figuring things out – all by copying other people. He
has never received any formal computer training. His language still is not the same
as his peers, but he has a special way of making his needs and wants known. For
example, if he doesn’t know the name of an object, he will describe it and ask:
“Waar’s hom sny?” (“Where’s the cut?”) to get a pair of scissors. His behaviour can
also be a challenge at times, because he uses it to show what he wants. In the
beginning he also had difficulty with group activities, but he is starting to participate
more and more because he knows what he wants and what is expected of him during
group time. We also took him for tennis lessons because we want to encourage him
to be more active. Initially his lessons were done on an individual basis, but due to
his good progress he now participates in the group.
Some things really make it easier for parents, like it really helps if the teacher tells us
beforehand what the theme of the week is, because then we can prepare our son. He
feels a lot more secure when he can anticipate what will happen, and then he acts
accordingly. It is really difficult for me as a mom if I receive negative feedback from
the school every day saying that my child had a difficult day – as his mother I know
what he can’t do, I know what he has problems with, I can see all those things. I don’t
need somebody else to tell me. I would prefer it if the teacher rather told me what he
had achieved, what he had mastered and what he had enjoyed. I think it is so
important for a teacher to spend time with my child so that she really gets to know
him and to understand him. She needs to see what makes him tick. I also think it is
important if a teacher can sometimes admit that she doesn’t know what to do in a
certain situation. I want my son’s teacher to see me as her partner – we are all on the
same side in trying to make it better for him. I think it is natural for a teacher to ask for
help, but this help should be achievable, in other words a teacher shouldn’t only ask
for financial help such as a facilitator or class aid, as most parents cannot afford that.
I know that we still face huge challenges with our son’s education, for example with
discipline and how to manage his behaviour, but this is our journey in life. All I ask of
the teacher is a chance. A chance for us as a family, but also a chance for my son …
by giving him a chance and by giving him time, he will have the opportunity to
become who he was meant to be.
This little boy has had a facilitator, who is privately paid by the parents, who has for
the past three years been helping to implement his home programme. She went with
him to school for the first two weeks in both his Grade RR year and his Grade R year.
This is how she described her journey:
I think being there for the first two weeks with him in his new classroom gave him a
sense of security because he felt comfortable with me as he has known me for a
while. I think it also comforted his parents because they knew I was there to
intervene if any problems might arise. But I think for the teacher it was more difficult
because in the beginning of the year she has to get to know all the children and
establish a classroom routine, and having another adult in the classroom if one is not
used to it is difficult. I think it would have worked better if all of us (myself, the teacher
and the parents) could have met before school started to discuss our expectations
and to sort out practical issues, such as the times I was expected to be there. I felt
that it worked best for all if I arrived early in the morning with him, assisted in the
classroom and then if I left when it was time for outside play. I quickly learnt that if I
was around on the playground, he would stay with me and not socialise with his
peers. The other children were also quick to ask, “Why does he need an extra
teacher?” because that was the way they saw me. I then realised that I had to
change my way of working from focusing only on one child to becoming more of a
general class aid who assisted the teacher in any way I could. This helped to take the
focus away from him alone. I think this also made it easier for the teacher, because it
is important for the teacher to be the head of the class and to have authority in the
class – therefore I couldn’t give my own instructions, I could only repeat hers. But I
guess this is a very personalised account, because everything has a positive as well
as a negative side to it … and it is also largely dependent on all the individuals who
are involved.
Following is a true story of a mother who has a son in Grade 2 with highfunctioning autism who attends a mainstream school.
When my son, who has Asperger syndrome, had to go to school, we approached the
same school that his older brother attended. As I knew that he would need more
support than the average Grade R child, we said that we would pay for a facilitator to
go to school with him. Although we were willing to pay for the facilitator ourselves and
had said that the facilitator could act as a general classroom assistant and help the
teacher with other children in class, the school was adamant that they would not
accept learners with special needs. One of our friends suggested the school that he
attends now, and they welcomed him – and his older brother – with open arms.
In his Grade R year, he learnt many things, also around socialisation. For example,
the little girls did not want to allow him to play inside the dollhouse, claiming it to be
“girls’ territory”. He is very aware of what is right and what is wrong, and really tries
his best to fit in with his peer group. He was frequently invited to birthday parties,
which he enjoyed. However, in Grade 1 he was not invited all that often and in Grade
2 he was only invited twice, which is difficult for him, because he knows that the other
children are invited. I think that many of the children accept him for who he is, but
their parents are not always as accepting and accommodating. I believe that one day
he will get a special friend on whom he can depend, and that will be a friendship for
life.
At the end of his Grade R year, we decided to hold him back, as we felt that he
wasn’t yet ready for Grade 1. I am glad we did, because he is now progressing
satisfactorily in Grade 2, although he works slowly and usually only finishes about
half of the work. His teacher asks one of the little girls who works quickly to sit next to
him, and when her work is done, she helps him to finish his work. At the moment he
enjoys maths in particular – and although he is only able to finish about half of the
work, he gets all of them correct! His teacher feels that he will be promoted to Grade
3, but feels that he will continuously battle to complete work on time.
If I think back now, my husband said that he realised that something was wrong with
our son when he was born. I, on the other hand thought that it was just a case of
children developing differently, but maybe it was also my way of coping then? When
he was a year old we started taking him to paediatricians, neurologists, genetic
screenings … but nobody could explain what was going on with our son, or maybe
they were just being extra cautious. I had the feeling that they would rather say
nothing than make the wrong diagnosis. Despite this, the doctors made all kinds of
negative comments about him possibly never talking or never being independent and
never attending school. When he turned two and a half, a friend casually gave me a
book while we were drinking tea, in which a boy with Asperger syndrome was
described and said that she wanted me to read a specific page. Reluctantly I did, and
while doing so recognised more and more of our son’s traits. Although I then had a
“diagnosis”, it was only confirmed when he was five years old, and then I had to hear
even more negative comments.
For a child with special needs, the family is very important. When he turned two, God
gave me inner peace and acceptance for our whole family, which helped us to know
how to handle the situation. I think this is very important, or else our whole family
could easily have disintegrated. I am glad that he is my middle child, because he has
an older brother who will always defend him, and if children ask questions about
strange behaviour, his brother will explain. His older brother is also a good role
model, and he learns a lot of new skills from him, and he even assists with
homework. He also enjoys playing rough and tumble games with his older brother …
On the other hand, I see that he really enjoys playing with his sister (who is three
years younger than him) as they are on the same level in terms of play development,
and nobody thinks it is strange when siblings play together.
At this stage I feel that we made the correct choice to put him into an inclusive
classroom. I feel that it is unfair to create a ceiling for any person; one should rather
open up a door for them, create opportunities, and then everything that they achieve
is wonderful. In the inclusive classroom he is exposed to a normal language model,
and he speaks well. In the special school I visited when we had to decide on where
to place him, the children were not really interacting with each other, spoke little and
used gestures that I couldn’t understand. I didn’t feel that it was in my son’s best
interest to take him there. He really loves every day at school and is keen to go to
school. It is so rewarding to see how proud and happy he is over everything that he
accomplishes. He really works hard at school – but what’s even better is the fact that
he does this with zest! However, I am also not blind – and if things should change
and he is no longer happy or keen to go to school, we might have to revisit the
alternatives.
WHAT MAKES IT EASIER FOR ME AS A MOM?
I know that there is no one single recipe that can work for all children all of the time,
but certain things have made it easier for me:
Teachers who have a lot of patience – not only with my child, but also with me!
Teachers who give information about both the positive and the negative aspects of
my son’s day (I speak to his teacher every single day after school to hear how it
went). This is very important, as he can’t tell me if he had a wonderful day or a
terrible day; the teacher has to provide that contextual information. It is sometimes
painful to hear that he just sat on the stoep for two whole weeks and didn’t want to
play on the playground … but I want to hear that too.
Teachers who take trouble to get to know my child and who can share both his
strengths in the classroom as well as his weaknesses.
Teachers who know about the condition, as more knowledge creates a better
understanding. At the beginning of this year, I asked “Daantjie Dinamiet” (a role
model with high-functioning autism) to give a talk to the teachers. The teachers
said that this was very helpful, and I think it made a great impact because it was
not a mother giving advice, but an adult with the same condition who had
succeeded in life.
He has a study buddy who sits next to him in class and who helps him complete
his work.
What do these stories tell you? What do these mothers share? Are you the
type of teacher that makes it easier for families? Are you a turn-around
teacher?
12.6 CONCLUSION
Teachers can play a vital role in helping children with ASD learn to
negotiate the world around them by providing the external structure,
organisation and stability that they need. Using creative teaching strategies
is critical, not only to facilitate academic success, but also to help them feel
less alienated from other people and less overwhelmed by the ordinary
demands of everyday life.
REFERENCES
American Psychiatric Association (APA). 2013. Diagnostic and statistical manual of mental
disorders: text revision (DSM), 5th ed. Washington, DC: American Psychiatric Publishing.
Bondy, A. & Frost, L. 2009. The Picture Exchange Communication System. In Mirenda, P. & Iacono,
T. Autism spectrum disorders and AAC. Baltimore, MD: Paul H. Brookes.
Bornman, J. 2003. Christmas: a time for surprises? CAAC newsletter, November.
Bornman, J. & Alant, E. 1999. Training teachers to facilitate classroom interaction with autistic
children using digital voice output devices. Suid-Afrikaanse Tydskrif vir Opvoedkunde, 19(4): 364–
373.
Bornman, J., Collins, M. & Maines, B. 2004. Just the same on the inside: understanding diversity
and supporting inclusion in circle time. London: Lucky Duck.
Chaste, P. & Leboyer, M. 2012. Autism risk factors: genes, environment, and gene-environment
interactions. Dialogues in Clinical Neuroscience, 14(3): 281–292.
Cooper, R. 2001. Hidden tears and happy smiles: living with Andrew and other special children.
London: The Book Factory.
Dawson, G. & Burner, K., 2011. Behavioural interventions in children and adolescents with autism
spectrum disorder: a review of recent findings. Current Opinions in Pediatrics, 23: 616–620.
De Clercq, H. 2003. Mum, is that a human being or an animal? A book on autism. Bristol: Lucky
Duck.
Denning, C.B. & Moody, A.K. 2013. Supporting students with autism spectrum disorders in inclusive
settings: rethinking instruction and design. Electronic Journal for Inclusive Education, 3(1).
Detheridge, T., Whittle, H. & Detheridge, C. 2002. Widgit Rebus Symbol Collection. Cambridge:
Widgit Software Ltd.
Ferraioli, S. & Harris, S.L. 2011. Effective educational inclusion of students on the autism spectrum.
Journal of Contemporary Psychotherapy, 41: 19–28.
Filipek, P.A., Accardo, P.J., Baranek, G.T., Cook Jr, E.H., Dawson, G., Gordon, B. et al. 1999. The
screening and diagnosis of autistic spectrum disorders. Journal of Autism and Developmental
Disorders, 29(6): 439–484.
Foster, J. 2015. A review of the effectiveness of social stories among children and adolescents with
autism spectrum disorders. Master’s thesis, SUNY Plattsburgh. Available at:
http://digitalcommons.plattsburgh.edu/cgi/viewcontent.cgi?article
Gray, C. 2000. The new social story book. Arlington, Texas: Future Horizons.
Hoffman, J. 2013. Evidence-based classroom strategies for reducing anxiety in primary aged children
with high-functioning autism. New Zealand Journal of Teachers’ Work, 10(1): 25–43.
Hyman, S.L. & Levy, S.E. 2013. Autism spectrum disorders. In Batshaw, M.L., Roizen, N.J. &
Lotrecchiano, G.R. (Eds). Children with disabilities, 7th ed. Baltimore, MD: Paul H. Brookes.
Ichikawa, K., Takahashi, Y., Ando, M., Anme, T., Ishizaki, T., Yamaguchi, H. & Nakayama, T. 2013.
TEACCH-based group social skills training for children with high-functioning autism: a pilot
randomized controlled trial. BioPsychoSocial Medicine, 7(14). doi:10.1186/1751-0759-7-14
Jackson, N. 2002. Standing down: falling up. Bristol: Lucky Duck.
Koegel, L., Matos-Fredeen, R., Lang, R. & Koegel, R. 2011. Interventions for children with autism
spectrum disorders in inclusive school settings. Cognitive and Behavioural Practice.
doi:10.1016/j.cbpra.2010.11.003
Koudstaal, C. 2016. Autism spectrum disorder. In Landsberg, E., Kruger, D. & Nel, N. (Eds).
Addressing barriers to learning: a South African perspective, 3rd ed. Pretoria: Van Schaik.
Koyama, T. & Wang, H. 2011. Use of activity schedule to promote independent performance of
individuals with autism and other intellectual disabilities: a review. Research in Developmental
Disabilities, 32: 2235–2242.
Landrigan, P.J. 2010. What causes autism? Exploring the environmental contribution. Current
Opinion in Pediatrics, 22: 219–225.
Lang R., O’Reilly, M., Healy, O., Rispoli, M., Lydon, H., Streusand, W., Davis, T., Kang, S.,
Sigafoos, J., Lancioni, G., Didden, R. & Giesbers, S. 2012. Sensory integration therapy for autism
spectrum disorders: a systematic review. Research in Autism Spectrum Disorders, 6: 1004–1018.
Luckner, J.L., Slike, S.B. & Johnson, H. 2012. Helping students who are deaf or hard of hearing.
TEACHING Exceptional Children, 44(4): 59–67.
Mayer-Johnson, R. 1992. The picture communication symbols. Solana Beach, CA: Mayer-Johnson
Co.
McPartland, J. & Klin, A. 2006. Asperger’s syndrome. Adolescent Medicine Clinics, 17(3): 771–788.
Mercado, C. 2007. Accommodating learners with Asperger syndrome in the classroom. SAALED
News, 27(4): 5–7.
O’Connor, R.E. 2009. The use of Social Story DVDs to reduce anxiety levels: a case study of a child
with autism and learning disabilities. Support for Learning, 24: 133–136. doi:10.1111/j.14679604.2009.01413.x
Peeters, T. & Gillberg, C. 2003. Autism. Medical and educational aspects, 2nd ed. London: Whurr.
Pfeiffer, B.A., Koenig, K., Kinnealey, M., Sheppard, M. & Henderson, L. 2011. Effectiveness of
sensory integration interventions in children with autism spectrum disorders: a pilot study. American
Journal of Occupational Therapy, 65(1): 76–85.
Richdale, AL. & Schreck, K.A. 2009. Sleep problems in autism spectrum disorders: prevalence,
nature, & possible biopsychosocial aetiologies. Sleep Medicine Review, 13(6): 403–411.
Sainsburg, C. 2003. Martian in the playground: understanding the schoolchild with Asperger
syndrome. Bristol: Lucky Duck.
Sandin, S., Lichtenstein, P., Kuja-Halkola, R., Larsson, H., Hultman, C.M. & Reichenberg, A. 2012.
The familial risk of autism. Journal of the American Medical Association (JAMA), 311(17): 1770–
1777.
Strock, M. 2008. National Institute of Mental Health: autism spectrum disorders (pervasive
developmental disorders). Available at:
http://nimh.nih.gov/health/publications/autism/nimhautismspectrum.pdf (accessed on 15 January
2009).
Thompson, C.J. 2011. Multisensory observational research. International Journal of Special
Education, 26: 202–214.
Vandermeer, J., Beamish, W., Milford, T. & Lang, W. 2013. iPad-presented social stories for young
children with autism. Developmental Neurohabilitation, Early Online, 1–7.
Wendt, O. 2009. Research on the use of manual signs and graphic symbols in autism spectrum
disorders. A systematic review. In Mirenda, P. & Iacono, T. Autism spectrum disorders and AAC.
Baltimore, MD: Paul H. Brookes.
White, S.W., Oswald, D., Ollendick, T. & Scahill, L. 2009. Anxiety in children and adolescents with
autism spectrum disorders. Clinical Psychology Review, 29(3): 216–229.
Williams, K. 1995. Understanding the student with Asperger syndrome: guidelines for teachers.
Focus on Autistic Behavior, 10(2): 9–16.
Woodbury-Smith, M.R. & Volkmar, F.R. 2009. Asperger syndrome. European Child & Adolescent
Psychiatry, 18(1): 2–11.
13
Understanding children with
chronic medical conditions
13.1 INTRODUCTION
Teachers have a unique opportunity to assist in the identification of a
potential medical problem due to the extended period of times and sustained
interaction they have with learners (Valletutti, 2004). This is often an
important precursor to medical diagnosis and treatment, and therefore
teachers need a framework to help understand the causes, impact and
challenges they may face when teaching, supporting and accommodating
children with chronic (long-term) medical conditions.
Teachers should be concerned about medical conditions that may affect
learning or behaviour. This chapter does not deal with common childhood
diseases like measles and chicken pox (although teachers also need to be
aware of them) but rather with more severe chronic medical problems, for
example HIV/AIDS, epilepsy, tuberculosis (TB), diabetes, and asthma, as
well as conditions that may go undetected, such as the early stages of, for
example, malaria and Duchenne’s muscular dystrophy. This chapter will
highlight just a few of these conditions and discuss the accommodations
and supports needed to facilitate the participation of children with these
diseases (see Figure 13.1). In line with the social model of disability, a child
must never be defined by his medical condition. The focus should be on
creating an environment in which the child can participate on an equal
footing with his peers. It will become evident that although the conditions
vary widely, children will benefit from many common supports and
accommodations.
Figure 13.1 Chronic medical conditions seen
most frequently in the classroom
13.2 MEDICAL CONDITIONS SEEN MOST FREQUENTLY
IN THE CLASSROOM
In order to make finding a particular condition easier, they are described in
alphabetical order and not in order of frequency of occurrence.
13.2.1 Asthma
13.2.1.1 What is asthma?
The word asthma stems from the Greek word meaning “short of breath” or
“panting”, which implies that breathlessness is a key feature of asthma
(Holgate, 2010). Asthma is one of the most common chronic diseases in
children and affects approximately 5 per cent of children (Shouldice, 2004).
Over the past decade, the prevalence has increased without a sound
explanation as to why this is happening (Van Aalderen, 2012). It affects the
respiratory system and is characterised by recurrent episodes of airway
obstruction, resulting in wheezing, difficulty in breathing and tightness of
the chest. Two factors contribute to asthma symptoms: first, a narrowing of
the airways, which results in a tightening of the muscles surrounding the
airway tubes in a response to certain triggers and, second, inflammation of
the airways, which causes swelling of the lining of the airway tubes (Van
Aalderen, 2012). Some of the most typical asthma triggers include
allergens (e.g. indoor and outdoor agents, such as tobacco smoke, animal
hair, dust, pollens, perfumes, foods such as peanuts, milk, preservatives
or colourants)
environmental factors such as cold air
emotional distress
physical exertion or exercise
viral infections (e.g. influenza/flu).
Asthma has implications for learning in that these children may lose several
days of school when they are ill. In addition, poor quality of sleep is
frequently seen in children with asthma, and sleep disruption influences
daily activities such as school attendance and performance, and may even
lead to challenging behaviour (Van Aalderen, 2012).
13.2.1.2 What are the characteristics of asthma?
Although asthma is a serious disease, often few signs of the disease are
exhibited between acute episodes (often referred to as asthma attacks).
Children with asthma who are exposed to specific triggers may exhibit
specific symptoms such as shortness of breath, wheezing, coughing or
tightness of the chest. A severe asthma attack can result in a child
experiencing severe chest pain, turning blue from lack of oxygen, or even
losing consciousness.
13.2.1.3 Is there a cure for asthma?
There is no cure for asthma, although some children will outgrow the
disease. Asthma therapy has improved considerably over the last decade
and can be managed very effectively, hence children can lead full and
normal lives. It is usually treated with two forms of medication, namely
controllers and relievers (Kim & Mazza, 2011):
Bronchodilator medication. These reliever/rescue inhalers act
immediately by relaxing the muscles around the airway tubes and
providing short-term relief. Bronchodilators are typically administered
with an inhaler, and the child (and teacher) should have access to one in
case of an emergency.
Long-term inhaled corticosteroids. This is long-term, chronic medication
taken on a daily basis to prevent or decrease airway inflammation, even
when the child shows no asthma symptoms. When used regularly, it
controls the asthma effectively and prevents daily symptoms. This
medication will typically only be taken at home.
Research has shown that the relative high incidence of death in asthmatic
teenagers may be ascribed to non-compliance with medication (i.e. they do
not take their medication regularly) (Kunneke & Orr, 2016).
13.2.1.4 Classroom management
Considering the large number of children with asthma and the extended
time they spend at school, it is important that teachers be trained to manage
an asthma attack. Many teachers feel that their knowledge of asthma is
limited and that the procedures for giving anti-asthmatic drugs
(bronchodilators) are generally unsatisfactory, causing unnecessary
disruption to the child’s participation in classroom activities (Hawkins,
Painter & Richter, 2011). However, the single most important part of
classroom management is that teachers should, together with the child, be
knowledgeable about the possible contributing triggers. This includes
identifying situations that are likely to cause an asthma attack, so that
(where possible) these allergens can be avoided (Kim & Mazza, 2011). For
example, allergic triggers such as dust, grass and animals may influence a
bring-your-pet-to-school day or a school outing to a farm (Levin, 2008).
Children who have asthma that is under control (i.e. they are not exhibiting
asthma symptoms) should not be excluded from playing sport, although
teachers should guard against outdoor sport activities in the cold, as the cold
air might act as a trigger. However, if children have breathing difficulties as
a result of exercise, their asthma may not be under control and they should
be encouraged to see a doctor for appropriate medical treatment in order to
resume normal sporting activities (Holgate, 2010; Van Aalderen, 2012).
Cycling, swimming and walking build lung capacity, and are appropriate
sports for children with asthma.
All children with asthma should have an asthma action plan, which should
be shared with the teacher via the parents (Van Aalderen, 2012). Children
with asthma may minimise their symptoms in order to avoid negative peer
response and avoid taking necessary medications (typically an inhaler) in
front of their classmates for fear of being teased or rejected (Hawkins et al.,
2011). When a child is experiencing breathing difficulties (e.g. during an
acute asthma attack), teachers should follow these steps:
i. Ensure that the child is sitting comfortably. Be calm and reassuring.
ii. Give four puffs of an inhaler.
– Use one puff at a time and ask the child to take four breaths from the
spacer after each puff.
– Use the child’s own inhaler if possible. If not, use the first-aid kit
inhaler.
iii. Wait four minutes. If there is no improvement, give another four puffs.
iv. If there is little or no improvement, call an ambulance and the parents,
and state that the child is having an asthma attack. Keep giving four
puffs every four minutes until the ambulance arrives (National Asthma
Council Australia, 2008).
13.2.2 Childhood cancers
13.2.2.1 What are childhood cancers?
All cancers have the same disease process – cells grow out of control,
develop abnormal sizes and shapes, destroy their neighbouring cells, and
ultimately spread (or metastasise) to other organs and tissues (Miller, 2007).
As the cancer cells grow, they demand more and more of the body’s
nutrition, draining the child’s strength, destroying organs and bones, and
finally weakening the body’s immune system. There are many different
kinds of cancers which affect children, although the most common are
blood cancers (leukaemia), lymphomas (tumours of the lymph glands and
lymph nodes), brain and other central nervous system tumours, and, as
children enter their teen years, osteosarcoma (bone cancer) (Ward,
DeSantis, Robbins, Kohler & Jemal, 2014).
13.2.2.2 What are the characteristics of childhood cancers?
Some of the early symptoms include fever, swollen glands, frequent
infections, anaemia and bruises. However, these symptoms are also
associated with other infections or conditions other than that are not cancer,
and therefore it is not uncommon for doctors and parents to suspect other
illnesses when the cancer symptoms first appear. Later, symptoms will
differ depending on the type of cancer but may include general malaise,
weight loss, fatigue (exhaustion) and pain. Children will have an increased
susceptibility to infection, which may be life threatening. Parents and
teachers should establish open lines of communication to ensure that there
is a common understanding of the issues and the treatment options.
13.2.2.3 Is there a cure for childhood cancers?
Research has shown that curing childhood cancer is one of the great success
stories of modern medicine in which diseases previously considered as
untreatable are now treated effectively (Ward et al., 2014). Three cancer
treatment options are typically considered:
Chemotherapy (the use of medical drugs to kill cancer cells, which can
be given daily, weekly or monthly, depending on the specific treatment
regime)
Radiation (the use of radiant energy to kill cancer cells)
Surgery (to remove cancerous cells or tumours, or bone-marrow
transplants to allow new, healthy cells to grow)
All of these options are usually debilitating and painful, at least in the short
term.
13.2.2.4 Classroom management
Teachers play a critical role in reducing the child’s social isolation and
helping with the reintegration of the learners into the classroom after having
received treatment. In other words, teachers often act as the bridge between
the hospital setting and the school. Spinelli (2004) writes about a mother
who commented that she never realised how important school and its
routines were for her child until they were faced with her son’s cancer. His
first question after being told about his illness and treatment was: “Will I
still be able to graduate from high school with my class?” followed by:
“Will I die?”
So as to ensure a smooth transition back into the classroom, the teacher
should be knowledgeable about the child and the illness, for example the
type of cancer that the child has, its symptoms, the prognosis, the treatments
and their side effects (e.g. low energy and chronic fatigue when receiving
chemotherapy), as well as the parents’ (and the child’s) wishes regarding
what they want peers to know about the cancer.
The following box gives a true story of a Grade 3 boy who had a brain
tumour, as told by his teacher.
I have been a teacher for more than 20 years, and in my career I have taught
children with various disabilities and different learning needs: children with Down
syndrome and Asperger syndrome, children who have had cochlear implants,
children with severe learning disabilities, and developmental delays … I think it was
all this experience that helped me cope last year when I had to deal with a nine-yearold boy with a brain tumour. It came as a total surprise when his mother phoned me
to say that doctors had discovered that the pain and fevers he was complaining of
were actually caused by a brain tumour. After this telephone call, he did not come
back to class, which gave me the opportunity to prepare the other children in the
class, as I knew they would have many questions.
I asked his mother if I could be honest and explain to the class what was happening,
or whether she only wanted me to say that he was very ill. After checking with him,
his mom said that we should explain about cancer and chemotherapy. I was taken
totally by surprise when I told the children, and they started retelling their own
“cancer stories”. One little girl said that her mommy had died of cancer, another little
boy said so had his grandfather … I then realised how important it was to be totally
honest with the children and explain that some people do die from cancer, many heal
totally, and some get better for a while and then the cancer comes back. The children
wanted to pray for him, which we diligently did on a daily basis. They also wanted to
do something practical for their friend.
They decided to all donate a small amount of money, which we used to buy him new
pyjamas for his long hospital stay. I also organised a PlayStation® for his hospital
room, and the children brought games and videos and DVDs for him to watch while
in hospital – I think this was very valuable, as it made them all feel part of the process
of caring for their friend. I also paired the children up into groups of two, and made a
roster for when each pair could send him a text message on the cellphone – this
ensured that he would have at least two messages daily from his friends in the class!
They also made cards and wrote get-well messages, and when we had computer
days, we sent him e-mail messages. All of this made it a lot easier to help him return
to class, as he never started feeling like an outsider.
The whole class was overjoyed when he eventually was healed and could return. I
prepared them by explaining that he would look a little different (due to the fact that
he had no hair and a huge scar on his head), and that he would tire more easily, but
that nothing else would change. He would still be their same friend that went to
hospital a few months earlier. However, I did mention that they should be a bit more
careful when playing and that he couldn’t participate in rough and tumble and tackling
games due to the shunt that was inserted in his head. He also started swimming
again, and received a great deal of admiration from his friends for that! When he
initially came back we also allowed him to come a little later than usual, and to leave
a little earlier for the first couple of weeks … and then I ensured that I taught the
really important subjects like maths when he was there, and the less critical ones
when he was gone.
If I reflect back on this process, I think there are three really important things that can
help a teacher to handle this kind of situation:
Experience. It is so much easier to handle things outside of the ordinary if one
feels secure in your teaching knowledge.
Personality. I care deeply about each learner that I teach, and I think the learners
know that … I continuously asked myself, “What would I do if it was my own
child?” I also don’t get flustered easily, and this helped me to remain level headed.
Good communication between the parents and teacher. I spoke to his mother
almost on a daily basis, and this helped me understand the whole process,
knowing what to expect, what the parents felt I could do to make it easier for them,
how to prepare the other children, and understanding what information the family
felt I could convey.
Teachers also need to know how the cancer and treatments affect skills
needed for learning, such as concentration, memory, non-verbal skills,
language skills and motor skills, without neglecting the psychological
effects, such as anxiety, depression, behaviour problems, emotional
difficulties, peer relationship difficulties and frustration related to school
difficulties (Marcus, Yasamy, Van Ommeren, Chisholm, Saxena, 2012).
Teachers should receive a schedule of upcoming medical appointments so
that they can help the child prepare ahead for absences (Leigh & Miles,
2002). Teachers should play a part in helping children to keep up with work
and to catch up when work is missed. Buddies can also be appointed to
assist with this, as it creates a sense of belonging for all the children in the
classroom.
A group of 67 children between the ages of eight and 15 who had different
types of cancer (excluding brain tumours) and were receiving chemotherapy
were compared to healthy classroom peers (Noll et al., 1999). Teachers
perceived children with cancer as being more sociable than their peers.
Teachers and peers also perceived children with cancer as being less
aggressive, leading the researchers to conclude that childhood cancer has a
protective effect resulting from side effects of chemotherapy, namely
fatigue or general malaise. Peers also reported that children with cancer had
greater social acceptance skills, which could possibly be attributed to the
fact that the experience with cancer, the painful procedures the children
were subjected to, the side effects from chemotherapy, and the possibility of
death may increase the sensitivity of children with cancer to the needs of
others, resulting in better social functioning.
Results thus highlight the importance for teachers to ensure social
belonging by focusing on aspects that influence health in a positive way,
such as hope, positive coping and social support (Haase, 2004; Noll et al.,
1999). Ultimately, this will build resilience in these learners, in their
families and in the other learners in the classroom.
While children are undergoing cancer treatment, they may be tired and
nauseous, and may not have much energy. Teachers should consider this
when physical education is on the agenda. Furthermore, while undergoing
chemotherapy, these children’s immunity is extremely weak, and infectious
diseases would be exceptionally problematic (National Cancer Institute,
n.d.). Teachers should therefore enforce school rules and guidelines for
parents to keep their sick children at home. The loss of hair, which
accompanies some cancer treatments, can be very traumatic for some
children and is a very visible sign of their illness. Teachers should be
sensitive and allow children to wear a hat or scarf even when this is not in
line with usual uniform guidelines.
Children with cancer may exhibit psychological distress and may need
pastoral care. In particular, children may develop a fear of death, separation
anxiety and mood swings. If a child dies, the teacher will also need to
support the parents and other learners through the grieving process.
13.2.3 Epilepsy
13.2.3.1 What is epilepsy?
Epilepsy stems from the Greek word meaning “to take hold” or “to seize”.
It is a neurological disease (not a disorder, according to the ILAE) resulting
from brief electrical-chemical disturbances in the brain – a single episode of
such a disturbance is called a seizure or a fit (Fisher et al., 2014; Hedge,
2008). It is not surprising, therefore, that epilepsy should be seen as the
disease while the seizures are the symptoms of the disorder. Currently,
epilepsy affects 50 million people worldwide, and 80 per cent of them live
in the developing world (Bhesania, Rehman, Saleh Savul & Zehra, 2014;
Ekeh & Ekrikpo, 2015). It is a common disease in school-age children, and
can affect people of all ages, backgrounds and intelligence (Haslam, 2004).
Children with developmental disorders have a significantly higher risk for
epilepsy (Zelleke, Depositario-Cabacar & Gaillard, 2013). Seizure patterns
and the after-effects differ from person to person.
Unfortunately, epilepsy carries a strong social stigma, and the social attitude
leading to stigma and discrimination against individuals with epilepsy is
often more distressing than the disease itself (Bhesania et al., 2014).
Misconceptions are rife, and arise due to myths and beliefs that are passed
down through generations. In sub-Saharan Africa, this stigmatisation stems
from the fact that the traditional African belief views epilepsy as a spiritual
disease (Ekeh & Ekrikpo, 2015).
Epilepsy is not a mental illness or a psychiatric condition, it is not
infectious or contagious, and it cannot be spread by urine, saliva, blood or
faeces (Epilepsy South Africa, 2008; Ekeh & Ekrikpo, 2015). Epilepsy also
does not cause intellectual disability (Bhesania et al., 2014).
However, epilepsy is often associated with injuries to the brain, as seen in
conditions such as cerebral palsy and head injury. In addition, infections
(e.g. meningitis and encephalitis), metabolic disturbances (e.g.
hypoglycaemia as a result of diabetes), toxins (e.g. pesticides), trauma or
other acute illness may provoke seizures (Zelleke et al., 2013). Other causes
include high fever, severe dehydration, hereditary factors, brain tumours
and cerebral malaria. In 70 per cent of cases, no specific cause can be
identified (Orelove, Sobsey & Silberman, 2004).
13.2.3.2 What are the characteristics of epilepsy?
Recent changes have been made to epilepsy terminology, and the
International League against Epilepsy (ILAE) has adopted a new seizure
classification system. According to this system, seizures are broadly
grouped into two categories: first, partial seizures (formerly known as focal
or local seizures), which implies seizure activity that starts in one area of
the brain, and second, generalised seizures, which involve the whole brain.
These two main types and their sub-classes are shown in Figure 13.2.
Figure 13.2 Seizure classification
13.2.3.3 Is there a cure for epilepsy?
There is no medical cure for epilepsy, although some children outgrow it.
Epilepsy is considered to be resolved for individuals who have not had any
seizures for ten years and who have been without anti-seizure medication
for at least five years, and also for individuals who had an age-dependent
epilepsy syndrome but who are now older than the applicable age. Antiepileptic drugs are the first line of treatment, and seizures can usually be
successfully controlled if the medication is taken regularly (Zelleke et al.,
2013). Westling and Fox (2009) suggest the following criteria for the
selection of medicine(s):
Effective (preventing seizures)
Safe (having few side effects); for example, some medication makes
learners drowsy, creating the impression that they are lazy or
unintelligent, while others may lead to restlessness, irritability or
agitation
Affordable (as they may have to be taken for years)
Easy to take (long acting, few doses a day). New medication is only
taken at night and early morning, avoiding the embarrassment of taking
pills at school and the additional burden this may place on teachers.
Easy to obtain (from local hospitals, clinics and doctors)
Recently, other treatment options have also become popular for children
who failed to respond to antiepileptic drugs, for example the ketogenic diet
(high fat, low carbohydrate and low protein), surgery (which involves the
removal of the damaged part of the brain) as well as treatments with
vitamins, minerals and other alternative medicines (Zelleke et al., 2013).
The sociocultural belief around the causes of epilepsy influences healthseeking behaviour and subsequent management. In many African cultures
there is a perception that epilepsy is caused by spirit possession, witchcraft
or poisoning, and in such cases parents may be more likely to turn to
traditional healers than seek medical advice (Birbeck, Chomba,
Atadzhanov, Mbewe & Haworth, 2006; Ekeh & Ekrikpo, 2015).
13.2.3.4 Classroom management
To achieve optimal classroom management for children with epilepsy,
teachers must feel confident in handling seizures, which would include
knowledge of epilepsy, adequate support for teachers and effective lines of
communication between teachers, parents and the medical professionals
(doctors and nurses) (Dumeier et al., 2015). Teachers’ attitudes towards
epilepsy, based on their knowledge and beliefs, play a significant role in
reducing epilepsy-associated stigma, and therefore teacher training
programmes should include both an educational and a social component in
which teachers are exposed to a learner with epilepsy (Bhesania et al.,
2014; Birbeck et al., 2006).
Going to school can be stressful for children with epilepsy, as they may
worry about having a seizure in class and how classmates will react. Parents
are also anxious, and worry that their child’s teacher may not know how to
handle a seizure, or that their child may be treated unfairly because of
epilepsy (Spiegel, Cutler & Yetter, 1996). These fears may not be totally
unrealistic, as some teachers may never have seen a seizure before and may
not know anything about the condition. The best way to prevent
misunderstandings about epilepsy at school is to take proactive steps. At the
beginning of the year, parents should talk to their child’s teacher and other
involved parties (e.g. the soccer coach) about epilepsy. They should explain
what epilepsy is and how it affects their child. Getting the right information
to the right people at school early on can make a big difference to every
learner’s school experience. Children with epilepsy are not strange or
different. Parents, teachers, clinic sisters and others can help educate the
community about the condition so as to dispel negative attitudes, which
often have their origins in myth, for example witchcraft or madness.
Educating the community would include enabling them to recognise a
seizure and know how to handle it. “For most people with epilepsy the
biggest problem they have to face is other people’s attitude to epilepsy”
(Epilepsy South Africa, 2008).
Teachers should also educate the classroom peers about epilepsy without
necessarily identifying the specific child (Zelleke et al., 2013). They should
be encouraged to treat the learner with epilepsy in the same way as all the
other learners. Classroom discipline should not be lessened for this learner
for fear of triggering a seizure. Many schools use a buddy system, which
means that unnecessary attention is not put on the child. Likewise, children
with epilepsy should be encouraged to participate in sport activities,
although some sports should be avoided, such as scuba diving, rock
climbing, unsupervised swimming and parachuting (Zelleke et al., 2013).
Teachers are irreplaceable members of the multidisciplinary team involved
in the care of children with epilepsy, and should therefore learn to recognise
and report side effects, for example fatigue, drowsiness, headaches, slurred
speech, as well as irritability and aggression (Zelleke et al., 2013). In
addition, an accurate description of the seizure will help doctors prescribe
the correct medication. Children should be encouraged to take
responsibility for remembering to take their medication, but it should be
given by parents or the teacher. Where seizures are well controlled by
medication, children should be able to lead completely normal lives. When
seizures are not controlled it may be desirable to consider some protective
measures, for example close supervision of physical activities such as
swimming, cycling and climbing; or the use of a thick cap or helmet (only
in extreme cases) to prevent the child hurting himself when he falls.
However, a word of warning: restricting and overprotecting the child may
do more harm than taking the risk that he may hurt himself. Management of
daily activities will be unique for each child, but the principle of
participation should always be uppermost in the minds of parents and
teachers who make the decisions. Where there are dangers, such as open
fires, candles and gas cookers, children should be strictly supervised.
Knowing how to cope with a seizure will eliminate a teacher’s fear and
embarrassment. Her calm handling of the seizure will also affect the other
learners’ attitudes and experiences. In the event of a learner having a
generalised seizure, the teacher should
lower the learner on to the floor, if he has not yet fallen
position the learner on his side with his head slightly tilted back and a
little lower than his body so that he will not choke.
The teacher should not
put anything in his mouth even although he may bite his tongue
give him anything to eat or drink while the seizure is in progress.
Orelove et al. (2004) state that medical attention (e.g. calling an ambulance)
is only necessary if breathing stops (start mouth-to-mouth resuscitation), if
there are repeated seizures without regaining consciousness, if the learner
has been hurt in the fall, or if the seizure lasts more than five minutes.
13.2.4 Diabetes mellitus
13.2.4.1 What is diabetes?
Type 1 diabetes is usually diagnosed during the school years and was
previously known as juvenile-onset or insulin-dependent diabetes. It is a
common chronic disorder of childhood – second in prevalence to asthma
(Daneman & Frank, 2004). In type 1 diabetes, the body does not produce
insulin, which is a hormone that is needed to convert sugar (glucose),
starches and other food into the energy needed for daily life.
Type 2 diabetes, previously called adult-onset or non-insulin-dependent
diabetes, is the most common form, and is associated with a strong family
history of diabetes and a tendency to obesity. In type 2 diabetes, either the
body does not produce enough insulin or the cells ignore it. When eating,
the body breaks down all the sugars and starches into glucose, which is the
basic fuel for the cells in the body. Insulin takes the sugar from the blood
into the cells. When glucose builds up in the blood instead of going into
cells, it causes cells to become starved of energy in the short term, and over
time high blood glucose levels may damage the eyes, kidneys, nerves or
heart (American Diabetes Association, 2011).
The World Health Organization (WHO) estimates that more than 346
million people worldwide have diabetes and that this number may double
by 2030 without intervention. Almost 80 per cent of deaths from diabetes
occur in low- and middle-income countries (Shrivastava, Shrivastava &
Ramasamy, 2013).
13.2.4.2 What are the characteristics of diabetes?
Without insulin, people are unable to use the glucose from the food they eat
as a source of energy. Instead, the unused sugar builds up in the blood and
is disposed of in the urine, together with large amounts of water (Maggiore,
2013), hence increased urination (day and night) as well as enuresis (bed
wetting) are often among the first signs of diabetes. This increased urination
in turn creates increased thirst. In addition, the glucose loss in urine
represents energy loss, resulting in associated hunger (or decreased
appetite), weight loss and increased fatigue or lethargy. Blurred vision may
also occur, with potential loss of vision as a long-term complication
(American Diabetes Association, 2011).
Teachers may notice that a learner leaves the classroom frequently to go to
the toilet, appears to have little energy and generally appears unwell. In an
Italian study it was reported that when teachers were made aware of the
early signs of diabetes, they were able to facilitate an early diagnosis
through referral (Vanelli et al., 1999). All learners with diabetes should
wear visible identification, such as a MedicAlert bracelet, which indicates
that they have diabetes.
13.2.4.3 Is there a cure for diabetes?
Type 1 diabetes cannot be cured. However, learners with well-controlled
diabetes can expect to enjoy healthy school years, participating in the same
kinds of activities as their peers (Maggiore, 2013). Diabetes may be
controlled with medication in the form of pills or by self-administration of
insulin injections, and some children will have insulin pumps. There are
seven essential self-care behaviours in individuals with diabetes which
predict good outcomes, namely healthy eating, being physically active,
monitoring blood sugar levels, compliance with medication, good problemsolving skills, healthy coping skills and risk-reduction behaviours
(Shrivastava et al., 2013). Clearly this type of management will impact on
school life. Regular medical check-ups are also necessary. In most cases,
medication is not necessary for type 2 diabetes, although insulin may
become necessary if the disease is not well controlled.
13.2.4.4 Classroom management
Diabetes self-management is a critical element of care for all learners with
diabetes (Haas et al., 2012). The general health of a learner with diabetes is
a family responsibility, and teachers should not be expected or required to
perform blood sugar checks or inject insulin. However, teachers and school
nurses play an important supportive role in the management of diabetes and
should understand enough about the procedures to allow the learner privacy
to do injections and blood glucose testing, and supply any necessary
supervision.
Teachers also play an important role in ensuring that learners with diabetes
are safe in the classroom, on the playground and during school outings, as
they are often the sole monitor of these learners during school hours
(Schwartz, Denham, Heh, Wapner & Shubrook, 2010). They are also
critical in alleviating parental anxiety. For example, many parents find it
difficult to transition from parent to self-orientated care, fearing that their
children might not inject themselves with the insulin at the required times
(Daneman & Frank, 2004). The expectations of and demands placed on
teachers to participate in the medical care will vary, depending on the
child’s age, parental expectations and specific treatment.
It is important that teachers are knowledgeable about diabetes when having
such learners in their class in order to reduce their own anxiety and also
help these children manage their own diabetes with minimum disruption of
the classroom. Unfortunately, many children with diabetes and their parents
feel that dealing with diabetes in school is among the worst experiences
they have faced while growing up (Schwartz et al., 2010). To avert potential
problems, the teacher should encourage the parents to come to school and to
discuss their child’s specific needs and characteristics (e.g. the child
requires regular small meals that do not necessarily fall into the regular
routine of school breaks and may need to go to the toilet more frequently
than his peers). Teachers have to acknowledge parental expertise with
regard to their child’s condition, but unfortunately research shows that
communication between parents and teachers is often poor regarding
diabetes management (Nabors et al., 2005). Small-group training focused
on a specific learner might be a more appropriate way of increasing
knowledge than traditional mass training of teachers when they do not have
a learner with diabetes in their classroom. A study conducted by Schwartz
et al. (2010) indicated that teachers felt inadequately trained to manage
diabetes and to handle diabetic emergencies such as hypoglycaemia or
hyperglycaemia (discussed in Table 13.1).
Teachers of younger learners need to be especially observant during
physical exercise periods, and remind the child with diabetes to eat a snack.
Teachers should also understand that meal planning is an important element
of managing diabetes, and that it is difficult for such children to participate
in birthday parties and other celebrations as they have to be very particular
as to what food they eat. Teachers should inform parents of these events in
advance so that the insulin dose can be planned and adjusted accordingly.
Furthermore, when school activities revolve around food, for example
cooking lessons or arranging a picnic, the teacher must ensure that the
child’s dietary needs are accommodated in as unobtrusive a manner as
possible.
Children with diabetes should participate in school outings with their peers,
but careful forward planning is essential. If the outing involves more
physical activities than usual, extra food should be packed in their lunch
box, including some fast-acting carbohydrate snacks (juice and dried fruit),
as well as complex carbohydrate snacks (breakfast bars, wholewheat
sandwiches with peanut butter). Overnight trips or special events require
even more planning.
Often adolescents with diabetes do not receive the support they need in high
school to manage their diabetes during or after school. Research has shown
that adolescents need more support at school and that they should be
encouraged to communicate more frequently about what they need to
manage well in school (Nabors et al., 2005). One teacher in this study
commented: “Parents, let alone the teen, are not communicating with
teachers or health staff directly.”
Table 13.1 Understanding hypo- and hyperglycaemia
Hypoglycaemia (insulin shock/insulin reaction)
(low blood sugar levels)
Caused by too much insulin, too little food owing to a
delayed or missed meal, too much unplanned vigorous
activity. Relatively common (at least once a week).
Hyperglycaemia (diabetic
coma)
(high blood sugar levels)
Caused by too little insulin,
missed dose of insulin, too
much food or simple sugar,
infection, illness, surgery and
emotional stress.
Hypoglycaemia (insulin shock/insulin reaction)
(low blood sugar levels)
Hyperglycaemia (diabetic
coma)
(high blood sugar levels)
Develops within minutes with early warning symptoms
such as shakiness, jitteriness, extreme hunger,
coldness, sweaty skin, tiredness, blurred vision,
anxiety, headache, abdominal pain or nausea,
extreme paleness. Later symptoms include increasing
confusion and aggression, lack of coordination, rapid
and shallow breathing, eventually progressing to
coma.
Develops slowly and shows
symptoms such as drowsiness,
confusion, deep and fast
breathing, blurred vision,
confusion and drowsiness, a
strange sweet or fruity smell on
the breath, nausea and
vomiting, and coma.
Give some concentrated glucose like a sugary drink, a
glass of fruit juice or a sweet. Call parents and an
ambulance, if necessary. Do not leave the learner
unsupervised until fully recovered.
Call an ambulance (rapid
transport to a hospital is
necessary) as well as the
learner’s parents. Keep the
learner awake.
Sources: Adapted from Kunneke & Orr (2016); Maggiore (2013)
One of the critical aspects that teachers should be well aware of is the
ability to recognise and treat minor hypoglycaemic attacks to prevent them
from escalating into more severe ones. The school should have a plan of
action in place in case the child has either a hypoglycaemic attack (low
blood sugar levels) or a hyperglycaemic attack (high blood sugar levels)
(see Table 13.1).
13.2.5 Heart defects
13.2.5.1 What are heart defects?
Many children (25–50%) are diagnosed with a harmless heart murmur
(using a stethoscope a medical doctor can hear the blood rushing through
the heart). These murmurs have no underlying heart conditions, have no
symptoms and hence require no treatment (Shouldice, 2004). Children with
detectable heart defects may have underlying heart valve abnormalities,
abnormal holes between the heart chambers, abnormalities in the blood
vessels entering or leaving the heart, or irregularities of the heart rhythm
(Russell & Fazari, 2010; Votroubek & Tabacco, 2010).
Children can either be born with heart defects (congenital) or can acquire
them in childhood. Some causes could be genetic (run in families), maternal
rubella (the mother having German measles while pregnant), diabetes or the
mother taking certain drugs during pregnancy (Neill, Clark & Clark, 2001).
Some are associated with other conditions such as Down syndrome.
Congenital heart defects are usually diagnosed before a child is enrolled at
school.
13.2.5.2 What are the characteristics of heart defects?
Because there are many conditions that affect the heart, it would be difficult
to give a comprehensive list of symptoms, but examples would include
cyanosis (a blueness of the lips and nail beds caused by reduced oxygen in
the blood, which may increase with exercise but the learner may not be
aware of it), increased breathing rate, poor appetite, profuse sweating,
failure to thrive, tiredness, decreased energy levels, and exercise intolerance
(Fazari & Russell, 2007). Learners with heart defects may also be shorter or
lighter than their classmates and in some instances have difficulty gaining
weight. These learners may also be more likely to get common chest
infections such as bronchitis and pneumonia (Russell & Fazari, 2010).
There may be some developmental difficulties related to prolonged periods
of recovery from surgery or procedures that could limit early learning
experiences. Parents and teachers should establish open lines of
communication to ensure that there is a common understanding of the
issues and the treatment plan for the individual learner.
In a study of 109 children with complex congenital heart disease who
underwent cardiac surgery as newborns, a significant proportion were at
risk for inattention and hyperactivity, and nearly half needed remedial
school services (Shillingford et al., 2008). Ongoing neurodevelopmental
follow-up and screening are therefore recommended for this vulnerable
population.
13.2.5.3 Is there a cure for heart defects?
A high number of children who are born with heart problems have surgery
before they reach school age with no residual effects (Shouldice, 2004). In
some instances, medication may be effective and in others there are viable
surgical options. Many children with heart defects or heart disease will have
effective treatment, but in some cases the condition could become chronic.
Abnormalities of heart rhythm can be treated with a pacemaker, in which
case the child will be prevented from doing any contact sport (Kunneke &
Orr, 2016).
13.2.5.4 Classroom management
A sharing team approach between parents, teachers and medical staff avoids
anxious speculation, and equips teachers with the knowledge to answer
questions in an appropriate way including the frank questions that other
children in the classroom might ask (Neill et al., 2001). Teachers therefore
require insight into the exact nature of the child’s medical condition in order
to ensure optimal classroom management. Most children with simple heart
defects do not require any special care when they attend school. In cases
where the condition is more severe, children may need to attend numerous
doctors’ appointments and are likely to have significant periods of absence
from school. Teachers should play a part in helping such children keep up
with work and to catch up when work is missed. In some cases, learners
may need surgery. To help the child before surgery, the teacher should talk
to the parents and discuss the date of surgery, the reason for it, the estimated
length of hospitalisation, and time needed to recover before returning to
school (Fazari & Russell, 2007). The teacher should also determine if it is
appropriate to discuss the surgery with the classmates. A child in hospital
can benefit from contact with classmates, which can be in the form of getwell cards, text messages on a cellphone or visits. A gradual return to
school and other normal activities is usually recommended, for example
only attending classes for half days for the first few days back at school.
Typically, the level of activity permitted for learners with heart defects will
be different. For example, if there are only five minutes between classes but
a child with a heart condition needs ten minutes to get from one class to
another, arrangements should be made to give the child the extra time and
not penalise him for being slow (Russell & Fazari, 2010). Although some
children with a heart condition may need to limit the amount or type of
exercise, many can participate in normal or near-normal activity, while
others are allowed to exercise but are not allowed to participate in races,
organised games or team sports. Teachers should be aware of any medical
restrictions and should seek input from parents.
Finally, some children with serious heart problems may be overprotected by
their parents (due to the seriousness of the medical condition). In the long
term, this could lead to these children feeling isolated and stigmatised,
which may do more harm than a heart defect itself (Dowshen, 2007).
Teachers should therefore attempt to take all possible measures to ensure
that such children lead as normal a life as possible. In some cases, they may
also exhibit psychological distress and need pastoral care, as they may
develop a fear of death, separation anxiety and mood swings. In these
instances, teachers could think of referring the family to a support group or
for counselling.
13.2.6 HIV/AIDS
13.2.6.1 What is HIV/AIDS?
The human immunodeficiency virus (HIV) causes acquired immune
deficiency syndrome (AIDS), a condition in which the immune system is
destroyed as a result of opportunistic viral infections (Sharp & Hahn, 2011).
Children with HIV can lead active, normal lives and initially there may be
no obvious physical signs that they are infected. Healthy eating, exercise
and attention to basic hygiene are all important factors in slowing the
disease’s progression. HIV is not very contagious and does not penetrate
intact skin. It is not transmitted by
sharing a classroom or a home with an HIV-infected or HIV-affected peer
sharing cooking or eating utensils
sharing bathroom or toilet facilities
kissing (unless there is an open sore in the person’s mouth)
contact with tears, sweat, vomit, faeces and urine
fleas, mosquitoes or other insects.
There are a number of ways that people can contract HIV, for example
mother-to-child transmission; blood transfusions; sharing needles or
syringes with an HIV-infected person and unprotected sexual intercourse
(either vaginal, anal or, in some instances, oral) with a person infected by
HIV (Shete, 2013). This could also include rape or sexual abuse.
Unfortunately, high-risk behaviour is common among adolescents (some
authors even refer to “risk-seeking behaviour” in this population), and
unprotected sex as well as experimentation with drugs (often involving
needle procedures) increases their vulnerability to HIV infection (Naswa &
Marfatia, 2010). Childhood sexual abuse also leads to increased adolescent
sexual vulnerability.
AIDS takes a severe human toll – in 2000, 40 per cent of child deaths in
South Africa were directly related to HIV/AIDS, while many other deaths
reported from other causes could also have had HIV/AIDS as an underlying
cause (Kvalsvig, Taylor, Kauchali & Chhagan, 2013).
13.2.6.2 What are the characteristics of HIV/AIDS?
Three different groups of learners with different characteristics exist:
Children infected by HIV (who are at risk for developmental delays,
cognitive difficulties and neurological problems, and who may or may
not be receiving antiretrovirals (ARVs)). These children could also have
co-occurring risks such as malnutrition, TB and recurrent chronic illness
(Kvalsvig et al., 2013). HIV infection is particularly aggressive in
children – without access to ARVs, more than half of HIV-infected
infants die before the age of two years (Rose, Hall & Martinez-Alier,
2013).
Children exposed to or affected by HIV (they are not infected
themselves, but they may need to care for a chronically ill, HIV-positive
parent or have been orphaned as a result of the disease). The emotional
impact results in higher levels of anxiety, depression, withdrawal from
others, feelings of hopelessness and anger (Busman, Page, Oka, Giordani
& Boivin, 2013).
Children living in a society disrupted by the HIV/AIDS pandemic.
Research in KwaZulu-Natal involving three- to six-year-old children
showed that about half of these children knew that they had to be helpful
when people were ill, many were sympathetic and some understood the
need for emotional support (Kvalsvig et al., 2013).
13.2.6.3 Is there a cure for HIV/AIDS?
Several strategies are in place to protect children: treating both parents and
children with ARVs, preventing new mother-to-child infections, as well as
better health, education and social welfare services. Unfortunately, none of
these strategies is currently fully effective (Kvalsvig et al., 2013).
13.2.6.4 Classroom management
In many African countries, teachers have been given a major role in
promoting HIV awareness and behavioural change among children (Sarma
& Oliveras, 2013). The rationale behind this is that these teachers
can be found in rural parts of the country where no other staff (e.g.
nurses) are available
can be given sufficient knowledge about HIV/AIDS, which they in turn
can disseminate further
are credible in the community.
Schools should thus play a role in the worldwide effort to control and
eventually eradicate this disease (Sarma & Oliveras, 2013). Furthermore,
many teachers believe that they play an important role in talking to learners,
hence on paper the education of teachers to promote HIV awareness sounds
like a master plan. Why then is it not foolproof? Research has shown that
teachers themselves have not escaped the HIV/AIDS pandemic, as an HIV
prevalence of 12,7 per cent was found among teachers and approximately 4
000 had died in 2004 of AIDS-related complications (Shisana, Peltzer,
Zungu-Dirwayi & Louw, 2005). In cases where teachers are infected, high
rates of absenteeism may exist, leading to lower teaching quality, extensive
disruption of school activities and a negative influence on the morale of
colleagues. Even where educators are present, they may be sick and
ineffective, or poorly qualified, as schools are likely to make use of
whoever is available (Louw, Shisana, Peltzer & Zungu, 2009).
One of the major contributing factors to this pandemic is the fact that there
is often a stigma associated with HIV, and both children infected and
affected may experience discrimination, gossip and teasing from peers and
the community at large (Kvalsvig et al., 2013). Teachers should respect the
fact that learners have the right to keep their status confidential, and
disclosure of information can therefore be done only with consent from the
learner and his family. Where a teacher suspects that a child might be HIV
infected, she should ensure that any enquiries are made with discretion, and
that she does not inadvertently disclose a child’s status.
It is important that teachers provide accurate information to learners about
HIV/AIDS and that they are aware of how children infected or affected by
HIV are treated by their peers. Children may suffer from this stigma even if
they are not infected by HIV themselves, but where a member of their
family is known to have HIV/AIDS (Busman et al., 2013). Teachers should
ensure that they are familiar with the National Policy on HIV/AIDS for
Learners and Educators (South African Department of Education, 1999).
This is a comprehensive document dealing with non-discrimination and
equality; school attendance; HIV/AIDS testing and the admission of
learners to a school; disclosure of HIV/AIDS-related information and
confidentiality; a safe school environment (e.g. teachers should ensure that
they do not handle blood and that children are aware of the dangers of
touching blood); prevention of HIV transmission during play or sport;
education on HIV/AIDS; duties and responsibilities of learners, teachers
and parents; and finally, responsibility for implementation at school and
national level.
Many schools provide some form of HIV/AIDS education, but research has
shown that teachers are doing so with the sole objective of imparting
knowledge and not helping children understand the implications of this
pandemic (Sarma & Oliveras, 2013). This might be due to the fact that
many teachers feel uncomfortable when teaching about HIV/AIDS as it
deals with sensitive issues such as discussing sexuality. Effective awareness
programmes not only involve good resources and materials, but also good
teaching approaches and a positive attitude, and while many teachers still
feel that they lack knowledge this type of prevention programme will not be
optimal. For younger children, materials have been made available in the
form of children’s books that explain what HIV/AIDS is, for example
Brenda has a dragon in her blood, which is available in all of the 11 official
South African languages (Vink, 2005), and The little hare/Umvundlana
(Bloch, 2003), which is available in English and isiXhosa, and highlights
issues related to being chronically or terminally ill. Cotlands has also
developed a series of colouring-in books that contain drawings and activity
pages for children aged four to nine, designed to give children fun while
conveying an educational message concerning HIV/AIDS (Smit, Teitge &
Kleingeld, 2002; Smit, 2004).
As the disease progresses, children will become more susceptible to
infection and are likely to be absent from school for longer and longer
periods when they are unwell. HIV/AIDS sufferers have periods when their
immune systems are weak, and infectious diseases are exceptionally
problematic. Teachers should therefore enforce the school rules and make
sure that parents keep any infectious children at home. Teachers can support
children by giving homework and also by helping them to catch up when
they are back at school.
In many instances children with HIV/AIDS will have some family members
with the disease and who may have died from it. Families are losing many
of their productive members, leaving children and elderly members without
a means of support. This places a huge burden on children, and teachers
need to be aware of any particular issues. Children’s books, such as
Remembering Mommy, have been produced by UNICEF to help teachers
discuss grieving with younger children (Bloch, Mgcina, Patel, Seleti &
Sithole, 2006). They also provide guidelines such as encouraging children
to explore their lives through play, maintaining their routines and talking to
them about their feelings, and so forth. Ebersöhn, Ferreira and Mnguni
(2008) have examined the use of making memory boxes with older children
as a means of providing psychosocial support for children confronting
bereavement issues. They define memory-box making as a facilitated
means of reminiscing by collecting and storing valued belongings of loved
ones in order to remember that person’s life. In the classroom this would
mean that teachers can engage with children who are faced with
bereavement issues by helping them to collect and store items that they
value because of the memories they associate with a parent or close family
member who has passed away. This study reported that teachers found
memory boxes to be useful, because
they create space for children to reflect on and discuss their memories
they provide children with the opportunity to reflect on their loss and
think about the past and the future
children’s memories fade fast in the absence of concrete intervention
strategies, and maintaining those childhood memories will engender a
clear idea of roots and identity
they facilitate basic counselling processes
they enable teachers to become more familiar with the children and their
circumstances.
The enormity of the HIV/AIDS pandemic means that most teachers in
South Africa have to support families affected or infected by the disease.
Katlego’s story, as told by his teacher, highlights the pastoral role of the
teacher with the child and his family.
Katlego was in my class for two years. His mother enrolled him and a few months
later, aged 25, she died. His granny Elizabeth felt strongly about his education and
decided to keep him at our school despite the hardship of getting him to school and
paying the fees.
Katlego was a very capable child, although he was shy and seldom talked. He fitted
in very well and knew exactly what was expected of him. There was always an aura
of great sadness around him. He was greatly loved by Elizabeth, who had no
surviving children. Her youngest daughter was killed in a taxi accident when she was
six years old and now her last daughter had also died. Elizabeth saw Katlego as her
last child and someone to call her “mommy”.
After a while Katlego began to get frequent chest infections. He used to cough and
cough to the extent that he would be ill. He was a proud little boy who never
complained and did not accept help easily. During the second half of the year of that
first year I began to suspect that he was depressed. He did not want to play with the
other children. The lively little boy I’d known just sat under a tree and watched the
other children. I subsequently discovered that chronic fatigue in children is often
mistaken for depression – I had no idea he might have HIV/AIDS until near the end of
his life.
Elizabeth phoned me at the beginning of the following school year to say Katlego
was very ill with diarrhoea. I began to suspect he had AIDS and with great sadness
suggested to Elizabeth that she have him tested, all the while assuring her that my
feelings towards her and Katlego would not change, whatever the result. She phoned
a few days later to give me the news I already knew in my heart. She never
discussed the fact with me again. It was heartbreaking for her to have to face the fact
that her daughter had also died from an AIDS-related illness, not just from
pneumonia.
It is difficult to convey the great shame that is associated with HIV/AIDS.
Katlego got weaker and weaker until he was admitted to Baragwanath Hospital
where he died. On the day of his burial I gave him a final kiss and made a short
speech at the funeral. In his eulogy it read that he had died after a short illness. Very
suddenly I wanted to scream out to everybody that our people are dying as a result of
this horrible disease. What would it take to break the silence?
A few weeks later I went with Elizabeth to put flowers on his grave. After this she
served me a cup of tea and told me she had wonderful news. She handed me
Katlego’s death certificate, which gave bronchial pneumonia as the cause of death.
“See,” she said, “it wasn’t AIDS. It wasn’t AIDS!”
The silence around this disease is deafening despite the billboards advocating
condoms and abstinence. Children are orphaned, and forced to become the main
breadwinner at a young age. Katlego’s granny is one of millions like her and her
sadness is seen in the faces all around us.
Source: Sue Askew (personal account, December 2006)
13.2.7 Malaria
13.2.7.1 What is malaria?
Malaria is a disease with a substantially negative impact on school
attendance, achievement and learning. It is estimated that in sub-Saharan
Africa, where 90 per cent of the world’s malaria occurs, about 500 million
cases are recorded annually with hundreds of thousands of child deaths
(Udonwa, Gyuse & Etokidem, 2010). In South Africa the picture looks
different as malaria has been controlled since the 1940s. Through these
interventions, South Africa has successfully reduced malaria and is now
targeting malaria elimination (zero local malaria cases) by the year 2018
(Morris et al., 2013).
Malaria is an infectious disease caused by the malaria parasite (Plasmodium
falciparum, Plasmodium vivax, Plasmodium oval or Plasmodium malaria)
that is transmitted by female anopheles mosquitoes. Only these mosquitoes
can transmit malaria, and only if they have been infected by a previous
blood meal taken from an infected person. When the anopheles mosquito
bites, it injects the parasite into the individual’s body. Although school-age
children are less likely to die from malaria than pre-schoolers, malaria
accounts for 5 to 8 per cent of school absenteeism in Africa (Brooker,
Clarke, Snow & Bundy, 2008).
13.2.7.2 What are the characteristics of malaria?
The symptoms of malaria are similar to flu symptoms: high fever, shaking
chills, profuse sweating, feeling unwell, severe headaches, muscle/joint
pains, anaemia, nausea, vomiting and diarrhoea (Magnussen, Ndawi,
Sheshe, Byskov & Mbwana, 2001). These symptoms often occur in one- to
three-day cycles. In the study conducted by Magnussen et al. (2001), it was
noted that with little training but regular support from the health sector, it
was feasible for teachers to make a presumptive diagnosis of malaria,
usually based on the “feeling feverish” symptom. Cerebral malaria can lead
to long-term intellectual impairment and even death if not treated early
(Kunneke & Orr, 2016).
Malaria is responsible for school absenteeism, poor performance in school,
examination failures, school dropouts and even death (Udonwa et al.,
2010).
13.2.7.3 Is there a cure for malaria?
In most cases malaria can be quickly and effectively treated with a course
of inexpensive oral medication. On 29 January 2016, the World Health
Organization released a position paper on RTS,S, the world’s first malaria
vaccine. It is currently being considered as a complementary malaria
control tool in Africa that could potentially be added to the core package of
proven malaria preventive, diagnostic and treatment interventions (WHO,
2016a). After the extensive clinical trial in predetermined pilot sites, a
further position statement will be put out. Furthermore, many effective
interventions to reduce malaria in Africa exist, for example prevention
through using long-lasting insecticidal mosquito nets; indoor residual
spraying with insecticides; seasonal malaria prevention in specific settings;
prompt diagnostic testing; and the treatment of confirmed cases with
effective antimalarial medicines (Malaria Policy Advisory Committee,
2016).
13.2.7.4 Classroom management
Many teachers are stretched to the limits of their resources, including
having the time and the ability to cope with an increasingly difficult
environment. Why then should teachers also be expected to teach their
learners about malaria? Because any chance of reducing the incidence of
malaria (e.g. by increasing knowledge about this condition) will contribute
to furthering the health and prosperity of everyone in Africa and may also
improve the general attendance of learners in the classroom, which in turn
will impact positively on participation and learning. Experience with
malaria has shown that prevention is better and cheaper than cure; however,
prevention is related to the knowledge and belief of people (Udonwa et al.,
2010). Correct knowledge of a health problem (e.g. regarding the causes of
malaria and how it is spread) combined with the right attitude can result in
healthy behaviour and practice. School support is focused on prevention
and prompt identification of the disease, as deaths are often a result of a
delay in seeking medical care. In Malawi, Save the Children introduced
Pupil Treatment Kits to provide immediate in-school treatment for malaria
(Kalengamaliro & Roschnik, 2008). In Tanzania, research has shown that
teachers can play a major role in school health programmes and are willing
to be involved in health matters as long as they are supported by health and
educational authorities (Magnussen et al., 2001).
Schools can become models for malaria control efforts in the community at
large, and this is particularly important if these schools are in malarial areas.
School-based malaria prevention programmes would include
providing knowledge about the causes of malaria. In a study done with
400 adolescents in Nigeria, only 41 per cent knew that it was spread by
female anopheles mosquitoes (Udonwa et al., 2010).
identifying early symptoms with prompt referral to clinics, hospitals or
doctors – learners should be made more aware of the dangers of malaria
in the rainy season
efforts to reduce pools of water that act as mosquito breeding spots on the
school grounds, for example stagnant puddles of water in potholes
using ceiling fans and air conditioners
reducing the chances of being bitten by mosquitoes by using insect
repellents (aerosol insecticides, mosquito coils or citronella candles) and
suitable clothing (long sleeves, long pants, socks) when going out at
night (Morris et al., 2013)
facilitating the distribution of treated mosquito nets (see Figure 13.3) and
fostering the correct attitudes towards the treated nets. Some individuals
wrongly believe that the chemicals used in treating the nets are very
poisonous (Udonwa et al., 2010).
using window and door screens to keep mosquitoes out
remaining indoors between dusk and dawn when mosquitoes are most
active (Morris et al., 2013)
taking all reasonable precautions when school trips are planned to
malaria areas.
Figure 13.3 Malaria-prevention techniques
13.2.8 Malnutrition
13.2.8.1 What is malnutrition?
Malnutrition literally means “bad nutrition” and therefore includes undernutrition (hunger) and over-nutrition (overweight and obesity). The World
Food Programme (WFP, 2000) defines malnutrition as a state in which
individuals’ physical functions are impaired to such an extent that they
cannot maintain adequate bodily processes such as growth (referred to as
stunting), pregnancy, lactation, physical work, and resisting and recovering
from disease. It has a cumulative effect and is not the result of a single day’s
food intake (or lack thereof); in other words, it does not refer to individuals
who “went to bed hungry today”. Children are particularly vulnerable as
they need energy for growth and their immune systems are immature
(Kvalsvig et al., 2013). The actual causes of malnutrition are varied and
complex, but include aspects such as lack of agricultural productivity and
over-cultivation; overgrazing and impoverished soil combined with
increases in population; the effects of natural disasters, conflict and war; the
effect of the HIV/AIDS pandemic; the consequence of other health issues;
poor education regarding proper nutrition; and, most importantly,
unemployment and the resultant impact on family income (Mamadou &
Duebel, 2006). Overpopulation, commonly seen in low- and middle-income
countries, can also reduce food security, which results in inadequate food
intake or intake of foods of poor nutritional quality and quantity.
According to the World Food Programme approximately 795 million people
in the world still suffer from hunger – that is about one in nine people on
earth (WFP, 2016). A total of 66 million primary school-age children in low
and middle income countries go to school hungry, with 23 million in Africa
alone. Sub-Saharan Africa is the region with the highest prevalence of
hunger (WFP, 2016). In a 2013 study based on a large 2001 data set, it was
calculated that malnutrition was associated with 54 per cent of deaths in
children in developing countries (Bain et al., 2013). The study also
associated poverty, illiteracy, ignorance, big family size, climate change,
government policies regarding feeding programmes and corruption with
malnutrition.
However, rapid changes in diet and physical activity patterns have resulted
in an increasing prevalence of overweight and obesity (the so-called
overweight/obesity transition) in school-aged children in low- and middleincome countries, such as South Africa (Kimani-Murage et al., 2015).
Overweight/obesity is classified as the fifth leading cause of global
mortality and an important predictor of various non-communicable
diseases, and hence this increasing trend is worrying. More and more low-
and middle-income countries (including South Africa) are thus facing a
double burden of malnutrition – that is, the persistence of under-nutrition,
along with a rapid rise of over-nutrition, and the associated noncommunicable diseases such as diabetes, hypertension and heart disease
(Kimani-Murage et al., 2015). The recent South African National Health
and Nutrition Examination Survey found that 25 per cent of young children
(two to four years of age) were either overweight or obese (Shisana.et al.,
2013).
13.2.8.2 What are the characteristics (consequences) of malnutrition?
Malnourishment has many faces: increased susceptibility to disease,
shortfalls in nutritional status, loss of energy, disability, and death resulting
from starvation or infectious diseases as a result of weakened general
health. Hence, these children grow up with worse health and lower
educational achievements than peers who are well nourished. In cases of
malnourishment, the lack of sufficient nutrients weakens the immune
system, increasing the risk of infectious disease. For example, it is also
associated with TB, diarrhoea, malaria and anaemia, and by compromising
digestive functioning many of these diseases can intensify malnutrition,
prolong the duration of hospital stays and even result in death among
affected children (Bain et al., 2013). When access to safe drinking water is
lacking, additional health risks present a critical problem. Malnourished
learners also have lower energy levels and impaired brain function, putting
them further at risk as they are less able to participate in classroom
activities.
13.2.8.3 Is there a cure for malnutrition?
Hunger can only be addressed successfully if there is interaction between
economic development, technology, policy, culture, ecological factors and
the availability of natural resources. All of these factors influence
communities in terms of food availability, basic education and knowledge,
caring capacity for children and the general health environment. A shortfall
in any of these areas can lead to a vicious cycle of insufficient dietary
intake, weight loss, a weakened immune system, and infections
accompanied by loss of appetite and energy-consuming fever. This impacts
negatively on learning, therefore, government-level interventions to
improve healthcare infrastructure and assure food security are important
steps in the prevention of malnutrition in children (Rose et al., 2013).
13.2.8.4 Classroom management
Children’s nutritional status is particularly important because
malnourishment puts them at high risk of physical and/or intellectual
impairment and mortality. Teachers should therefore have a background of
each child’s nutritional needs, and they should be aware of malnutrition
(either under- or over-nutrition) problems that may arise (Amari, 2012).
School feeding programmes, where learners are given meals or snacks at
school, are intended to alleviate short-term hunger and improve nutrition so
that the children are better able to concentrate, understand and participate in
the classroom (Jomaa, McDonnell & Probart, 2011). These authors also
report a positive effect on school enrolment and attendance. School meals
have also been linked to the fight against HIV/AIDS (Rose et al., 2013). In
some instances, school feeding programmes have an additional purpose,
namely to transfer income to families, for example by assisting them to
grow vegetables and then selling them. Programmes that benefit the
community at large are more effective than those that benefit just a few.
As childhood obesity is becoming an increasing challenge, teachers should
be equipped with relevant knowledge in health education, not only to
address under-nutrition but to also improve children’s knowledge about
healthy foods, fitness and physical activity in order to impact on overnutrition (Amari, 2012).
13.2.9 Tuberculosis
13.2.9.1 What is tuberculosis?
Tuberculosis (abbreviated to TB for tubercle bacillus) is a common and
often deadly infectious disease that usually attacks the lungs (75%), but can
also affect the central nervous system, the lymphatic system, the
gastrointestinal system, the bones, the joints and even the skin.
It is a top infectious disease killer worldwide and every day, more than 200
children globally younger than 15 years of age die needlessly from TB – a
disease that is preventable and curable (Marais & Graham, 2016).
13.2.9.2 What are the characteristics of tuberculosis?
In children, TB is typically characterised by weight loss, a chronic cough
(lasting more than three weeks), chronic ill health and failure to thrive. In
older children and adults, TB is characterised by a chronic cough with
blood-tinged sputum, fever, night sweats, loss of appetite, weight loss and a
tendency to tire easily (Jahromi & Sharifi-Mood, 2014). Infections of other
organs cause a wide range of symptoms. The diagnosis is usually made with
a chest X-ray and sputum smears, as well as with blood tests.
TB is infectious and is spread through the air when people who have the
disease cough, sneeze, spit or laugh (Jahromi & Sharifi-Mood, 2014). The
World Health Organization reported that in 2014, 9,6 million people fell ill
with TB of whom 1,5 million died from it (95% of TB deaths occurred in
low and middle-income countries) (World Health Organization, 2016b).
Research has shown that there are one million estimated cases of TB in
children worldwide, of which the majority are younger than 15 years of age
and living in Africa or Southeast-Asia (Swaminathan & Rekha, 2010).
Furthermore, in countries with a high prevalence of HIV infection, there has
been a marked increase in the incidence of TB. A rising number of people
in developing countries are contracting it because their immune systems are
compromised by HIV/AIDS (Getahun, Sculier, Sismanidis, Grzemska &
Raviglione, 2012). TB is a leading killer of HIV-positive persons and the
World Health Organization reported that in 2015, one in every three HIV
deaths was due to TB (WHO, 2016b). HIV weakens the immune system,
and these children are much more likely to become sick with TB when in
contact with another person with the disease. TB is a leading cause of death
among people who are also infected by HIV (WHO, 2016b). Individuals
with diabetes mellitus are also at increased risk of contracting TB and they
have a poorer response to treatment (Restrepo, 2007). In low- and middleincome countries such as South Africa, childhood TB is also closely
associated with poverty, overcrowding and malnutrition, resulting in higher
death and lower treatment success rates (Jaganath & Mupere, 2012; Marais
& Graham, 2016; Swaminathan & Rekha, 2010).
13.2.9.3 Is there a cure for tuberculosis?
South Africa is the country with the highest prevalence of TB, and the BCG
vaccination is given to all children under the age of three (WHO/UNICEF,
2006). All South African children of school-going age should thus have
received their BCG vaccination, and hence, theoretically, teachers should
not have children with TB in class. However, the reality is different. TB
treatment is difficult and requires long courses of multiple antibiotics
(usually about 6–12 months). One of the most common treatment protocols
in South Africa is referred to as DOTS (Directly Observed Treatment,
Short-course), which has been implemented in virtually all countries, and
has been identified by the World Bank as one of the most cost-effective
global health strategies available in the fight against TB (Getahun et al.,
2012). This initiative has been extremely effective and since 2000 the TB
incidence has fallen by an average of 1.5 per cent per year and is now 18
per cent lower than the 2000 level. Furthermore, the TB death rate has
dropped 47 per cent between 1990 and 2015 (WHO, 2016b).
The DOTS strategy combines appropriate TB diagnosis and registration of
each new case, followed by standardised multidrug treatment, which
includes a secure supply of high-quality anti-TB medication, individual
monitoring to ensure adherence, and evaluation of the whole group to
determine overall programme performance (TB Alert, 2005). Unfortunately,
antibiotic resistance is a growing problem, as seen in drug-resistant TB.
This is caused by inconsistent or partial treatment when individuals do not
take all their medicines regularly for the required period because they start
to feel better, or because the wrong treatment regimens are prescribed, or
because the drug supply is unreliable. A particularly dangerous form of
drug-resistant TB is multidrug-resistant TB, which is treated with toxic
drugs that have very unpleasant side effects. TB prevention, diagnosis and
treatment interventions are low cost and have a high impact (Getahun et al.,
2012) and should thus receive high priority.
13.2.9.4 Classroom management
Before admitting any learner, all schools should ensure that his BCG
immunisation has been done (usually done soon after birth). If teachers are
unsure about a learner’s health, they should refer him for a medical checkup at the local clinic or doctor. In disadvantaged schools, teachers should
refer children to the school’s nutrition programme. Teachers should also
educate learners about the importance of good hygiene, such as not spitting
and placing tissues in dustbins (Kunneke & Orr, 2016).
13.3 STAKEHOLDERS IN THE MANAGEMENT OF
CHILDREN WITH MEDICAL CONDITIONS IN
SCHOOLS
There are a number of critical stakeholders in the support of children with
medical conditions. This should not detract from the fact that parents and
primary caregivers bear the primary responsibility for the management of
the child’s medical condition; however, it is recognised that learners will
need support from teachers, schools, hospitals and other community
organisations in order to facilitate participation across home, school and
community environments.
Teachers play a key role in ensuring that children with medical conditions
are included in all facets of school life, and that their medical conditions are
recognised so that basic first aid or other necessary interventions are readily
available.
To support teachers, schools should have a framework for accommodating
and supporting children with medical conditions. This framework should
include the following aspects, and is shown in Figure 13.4.
Figure 13.4 Roles of key stakeholders in managing children with chronic medical
conditions in schools
13.3.1 Records of children with medical conditions
Confidentiality permitting, schools should ask parents to give them the
information necessary to help teachers manage children with specific
medical conditions. If teachers are unaware of a specific medical condition,
their course of action in an emergency may not be effective. Schools should
have information on a child’s medical doctor and details of any specialists
or instructions from hospitals or clinics as to how to deal with an
emergency.
It is important for schools to encourage dialogue between teachers and
parents so that children with medical conditions can be identified and
appropriately supported. As each child is an individual, teachers should
discuss their specific condition and needs with a parent to ensure an optimal
outcome. The parent engagement model in Figure 13.5 outlines the key
issues that should be discussed once a child has been identified as living
with a medical condition.
Figure 13.5 Parent engagement model
13.3.2 First aid training for staff
First aid training should be provided for all teaching and administration
staff as well as sports coaches, and should include an overview of
approaches to dealing with emergencies that may arise as a result of
common medical conditions.
13.3.3 Ability to administer emergency or essential medication
Schools should have access to some key medication and equipment for
first-aid treatment. This should include plasters, bandages, gloves,
disinfectant liquid, antiseptic cream, and so forth.
13.3.4 Support framework where teachers identify need
Schools should ensure that there is a process to follow when teachers have
concerns about the physical wellbeing of their learners. This could include
referral agreements to school guidance counsellors, social services, local
hospitals, local community workers and other organisations.
13.4 OVERVIEW OF CHALLENGES RELATED TO
ACCOMMODATION AND SUPPORT
Once a child has been identified as having a medical condition, it is likely
that teachers will have to accommodate and support him in a classroom
setting.
Teachers who identify the need for additional support for a particular child
should approach the National Department of Education. Their National
Strategy on Screening, Identification, Assessment and Support (SIAS)
School Pack (2008) provides the documentation for the Requesting and
Provisioning of Additional Support and focuses on
monitoring and providing wellness intervention for the learner
assisting with the administration of personal healthcare
developing, implementing and monitoring a health and wellness
programme
administering special healthcare procedures that require specific training,
for example the administration of medication and the management of
seizures
supporting and guiding learners’ self-administration of procedures (e.g.
self-catheterisation, which was discussed in Chapter 10 as a procedure
for learners with spina bifida, and the monitoring and administration of
insulin for children with diabetes discussed earlier in this chapter).
The task may appear daunting, and so it would be without the involvement
of the institution-level support teams (ILSTs) and the district-based support
teams (DBSTs). Once the assessment is complete, the appropriate supports
will ensure that the learner’s specific needs are accommodated within the
school setting.
Table 13.2 gives examples of accommodations that may have to be made by
a teacher or school in order to support a learner. The exact accommodations
will differ depending on the actual medical condition, but there are common
issues that should be considered.
Table 13.2 Types of accommodation or support
Type of
accommodation
or support
Features of this accommodation
or support
Constraints and
approaches to dealing with
them
Increased parent
engagement
In order to manage a child’s medical
condition, teachers and parents will
need to communicate. Where
parents are not forthcoming, teachers
should engage with them and
reassure them that the school is
looking to actively support the
learner.
Parents may be withdrawn
about engaging with
teachers and should be
assured of their
confidentiality (where
appropriate). Teachers
should also reassure parents
that discussion of medical
conditions will not result in
discrimination against the
learner.
Changes to
physical
environment
In some instances, children with
medical conditions will require some
changes to their physical
environment. These changes could
include
Teachers or parents may be
able to make the appropriate
adjustments to ensure that
learners with physical
constraints are able to
participate in classroombased learning or other
school activities, but there
may be resource constraints
that a school is unable to
overcome. These can be
referred to the DBST.
access to classrooms (e.g. using a
downstairs classroom for a learner
with a severe cardiac condition)
positioning desks and other
equipment away from draughts
removal of known allergens.
Type of
accommodation
or support
Features of this accommodation
or support
Constraints and
approaches to dealing with
them
Allowances for
limitations to
involvement in
physical activity
In many cases, although not all,
chronic medical conditions may limit
a learner’s ability to participate in all
activities. While this should be
recognised, teachers should
encourage partial participation where
possible, and should discuss with
parents what medical advice
regarding physical exertion has been
given. Teachers should be mindful
that intervention may be needed for
any child who experiences significant
physical discomfort when exercising,
and who is tired or upset, even if
there is no identified medical
condition.
In many instances, a
modified form of the activity
may be the only requirement.
In some instances children
with specific medical
conditions may not be able
to participate in physical
activity. In all instances
where teachers are aware
that a condition may be
exacerbated by exercise, but
can be controlled with
medication, teachers should
ensure that they have
access to these medications.
Specialised first
aid needs
Some medical conditions will require
specific first aid knowledge, and
specific medication may accompany
acute attacks. Teachers should
ensure that they are confident of their
ability to act in the case of an
emergency (e.g. learners with
epilepsy, asthma or severe allergies).
Formal specialised training
may not always be possible,
and teachers should request
that parents pass on
information they receive
about handling emergencies
from the relevant hospital or
clinic.
Absenteeism
Children with long-term medical
conditions may have higher rates of
absenteeism. This could arise as a
result of
Teachers should ensure that
they provide parents with
resources to help learners
catch up if they miss long
periods of school. Teachers
should also spend some
extra time with learners to
help them catch up.
illness
medical treatment.
Type of
accommodation
or support
Features of this accommodation
or support
Constraints and
approaches to dealing with
them
Dealing with
discrimination or
stigma
In many cases there will be a stigma
associated with a particular medical
condition. This can result in children
being discriminated against, with the
other children either excluding them
or subjecting them to physical or
verbal abuse. This should be
considered a serious issue and
teachers should educate the class (in
an age-appropriate manner) to
understand that they are not at risk of
contracting the condition and that all
people should be treated with
respect. Continued incidents should
be reported to school management.
Schools are part of broader
communities and there are
issues regarding stigma and
discrimination in many parts
of society. Teachers can
influence attitudes and be
part of the process of
growing knowledge and skills
alongside other stakeholders
in the community.
Type of
accommodation
or support
Features of this accommodation or
support
Constraints and approaches
to dealing with them
Psychological
support
Many children with medical
conditions will be under significant
psychological distress. Distress may
be exhibited by
Teachers should provide a
supportive environment that
allows learners to discuss
their negative emotions. As
teachers are not trained as
psychologists, they may face
constraints if the school does
not employ a psychologist or
there are no services
available at the local clinic or
hospital. There are, however,
some creative approaches
available to teachers that
may be useful in helping
children process their
feelings.
withdrawal and passivity
behaviour problems
depression.
Where teachers consider this is the
case, they should discuss it with the
parent and offer support where it is
available.
13.5 CONCLUSION
This chapter explored the roles of key stakeholders in creating educational
environments in which all children can thrive, even when they have specific
medical conditions. The responsibilities of parents, teachers, school
communities as well as the Department of Education have been considered
in relation to the provisioning of appropriate accommodations and supports
to facilitate participation. Once again, the notion that all children can and
will learn in a nurturing environment has been highlighted. Only in these
inclusive environments can the freedom, equality and dignity of all children
be protected.
REFERENCES
Amari, H.A. 2012. Perception of teachers on health education & nutrition for kindergarten students in
Kuwait. College Student Journal. Available at: https://www.questia.com/read/1G1302464018/perception-of-teachers-on-health-education-nutrition
American Diabetes Association. 2011. Diagnosis and classification of diabetes mellitus. Diabetes
Care, 34 (Supplement 1): S62 – S69. doi: 10.2337/dc11-S062
Bain, L.E, Awah, P.K., Geraldine, N., Kindong, N.P., Sigal, Y., Bernard, N. & Tanjeko, A.T. 2013.
Malnutrition in sub-Saharan Africa: burden, causes and prospects. The Pan African Medical Journal,
15(120). doi:10.11604/pamj.2013.15.120.2535
Bhesania, H.N., Rehman, A., Saleh Savul, I. & Zehra, N. 2014. Knowledge, attitude and practices of
school teachers towards epileptic school children in Karachi, Pakistan. Pakistan Journal of Medical
Sciences, 30(1): 220–224. Available at: http://doi.org/10.12669/pjms.301.4307
Birbeck, G.L., Chomba, E., Atadzhanov, M., Mbewe, E. & Haworth, A. 2006. Zambian teachers:
what do they know about epilepsy and how can we work with them to decrease stigma? Epilepsy and
Behaviour, 9(2): 377–385.
Bloch, C. 2003. The little hare/Umvundlana. Glosderry: UNICEF & New Africa Books.
Bloch, C., Mgcina, B.B., Patel, R., Seleti, J. & Sithole, E. 2006. Remembering Mommy. Glosderry:
UNICEF & New Africa Books.
Brooker, S., Clarke, S., Snow, R.W. & Bundy, D.A. 2008. Malaria in African schoolchildren: options
for control. Transactions of the Royal Society of Tropical Medicine and Hygiene, 102: 304–305.
Busman, R.A., Page, C., Oka, E., Giordani, B. & Boivin, M.J. 2013. Factors contributing to the preschool adjustment of Ugandan pre-school children with HIV/AIDS. In Boivin, M.J. & Giordani, B.
(Eds). Neuropsychology in children in Africa. Perspectives on risk and resilience. New York:
Springer.
Daneman, D. & Frank, M. 2004. Chronic illness in children. In Haslam, R.H.A. & Valletutti, P.J.
(Eds). Medical problems in the classroom: the teacher’s role in diagnosis and management. Austin,
Texas: Pro-Ed.
Department of Education. 1999. National Education Policy Act, 1996 (No. 27 of 1996). National
Policy on HIV/AIDS, for Learners and Educators in Public Schools, and Students and Educators in
Further Education and Training Institutions, Notice 1926 of 1999. Government Gazette, 410, no.
20372. Available at: http://www.doh.gov.za/docs/notices/1999/not99-1926.html (accessed on 11
March 2009).
Dowshen, S. 2007. If your child has a heart defect. Available at:
http://kidshealth.org/PageManager.jsp?dn=wellercenter&article_set=21474&lic=127&cat_id=172
(accessed on 9 March 2009).
Dumeier, H.K., Neininger, M.P., Bernhard, M.K., Syrbe, S., Merkenschlager, A., Zabel, J., Kiess, W.,
Bertsche, T. & Bertsche, A. 2015. Knowledge and attitudes of school teachers, preschool teachers
and students in teacher training about epilepsy and emergency management of seizures. Archives of
Disease in Childhood, 100: 851-855. doi:10.1136/archdischild-2015-308306
Ebersöhn, L., Ferreira, R. & Mnguni, M. 2008. Teachers’ use of memory-box-making to provide
psychosocial support in their pastoral role. Journal of Psychology in Africa, 18(3): 305–316.
Ekeh, B.C. & Ekrikpo, U.E. 2015. The knowledge, attitude, and perception towards epilepsy amongst
medical students in Uyo, southern Nigeria. Advances in Medicine, 2015, Article ID 876135, 6 pages.
doi:10.1155/2015/876135
Epilepsy South Africa. 2008. Epinews Winter Edition. Available at:
http://www.epilepsy.org.za/facts/index.php (accessed on 13 March 2009).
Fazari, L. & Russell, R.N.J. 2007. Congenital heart defects: information for teachers. Available at:
http://www.aboutkidshealth.ca/HeartConditions/Congenital-Heart-Defects-Information-ForTeachers.aspx?articleID=6544&categoryID=HC-nh4-06d (accessed on 10 March 2009).
Fisher, R.S., Acevedo, C., Arzimanoglou, A., Bogacz, A., Cross, J.H., Elger, C.E., Engel, J.,
Forsgren, L., French, J.A., Glynn, M., Hesdorffer, D.C., Lee, B.I., Mathern, G.W., Mosh, S.L.,
Perucca, E., Scheffer, I.E., Tomson, T., Watanabe, M. & Wiebe, S. 2014. A practical clinical
definition of epilepsy. An official ILAE report. Epilepsia, 55(4): 475–482. doi:10.1111/epi.12550
Getahun, H., Sculier, D., Sismanidis, C., Grzemska, M. & Raviglione, M. 2012. Prevention,
diagnosis, and treatment of tuberculosis in children and mothers: evidence for action for maternal,
neonatal, and child health services. Journal of Infectious Diseases. doi:10.1093/infdis/jis009
Gold, R. 2004. What every teacher should know about infectious diseases. In Haslam, R.H.A. &
Valletutti, P.J. (Eds). Medical problems in the classroom: the teacher’s role in diagnosis and
management. Austin, TX: Pro-Ed.
Haas, L., Maryniuk, M., Beck, J., Cox, C.E., Duker, P., Edwards, L., Fisher, E.B., Hanson, L., Kent,
D., Kolb, L., McLaughlin, S., Orzeck, E., Piette, J.D., Rhinehart, A.S., Rothman, R., Sklaroff, S.,
Tomky, D. & Youssef, G. 2012. National standards for diabetes self-management education and
support. Diabetes Care, 35(11): 2393-2401. doi:10.2337/dc12-1707
Haase, J.E. 2004. The adolescent resilience model as a guide to interventions. Journal of Pediatric
Oncology Nursing, 21(5): 289–299.
Haslam, R.H.A. 2004. Common neurological disorders in children. In Haslam, R.H.A. & Valletutti,
P.J. (Eds). Medical problems in the classroom: the teacher’s role in diagnosis and management.
Austin, TX: Pro-Ed.
Hawkins, A., Painter, L. & Richter, S. 2011. Managing childhood asthma in the school environment.
Perspectives in Learning: A Journal of the College of Education & Health Professions Columbus
State University, 12(1): 33–39.
Hedge, M.N. 2008. Hedge’s pocket guide to communication disorders. New York: Delmar Learning.
Holgate, S.T. 2010. A brief history of asthma and its mechanisms to modern concepts of disease
pathogenesis. Allergy, Asthma & Immunology Research, 2(3): 165–171. Available at:
http://doi.org/10.4168/aair.2010.2.3.165
Jahromi, M.K. & Sharifi-Mood, B. 2014. Pulmonary tuberculosis in children. International Journal
of Infection, 1(3): e21116, DOI: 10.17795/iji-21116
Jaganath, D. & Mupere, E. 2012. Childhood tuberculosis and malnutrition. Journal of Infectious
Diseases. doi:10.1093/infdis/jis608
Jomaa, L.H., McDonnell, E. & Probart, C. 2011. School feeding programs in developing countries:
impacts on children’s health and educational outcomes. Nutrition Reviews, 69(2): 83-98.
doi:10.1111/j.1753-4887.2010.00369.x
Kalengamaliro, H. & Roschnik, N. 2008. Presumptive malaria treatment in schools: successes and
lessons learned from Mangochi District, Malawi. Available at: http://www.savethechildren.org
(accessed on 13 March 2009).
Kim, H. & Mazza, J. 2011. Asthma. Allergy, Asthma & Clinical Immunology, 20117(Suppl 1): S2.
doi:10.1186/1710-1492-7-S1-S2
Kimani-Murage, E.W., Muthuri, S.K., Oti, S.O., Mutua, M.K., Van de Vijver, S. & Kyobutungi, C.
2015. Evidence of a double burden of malnutrition in urban poor settings in Nairobi, Kenya. PLoS
ONE, 10(6): e0129943. doi:10.1371/journal.pone.0129943
Kunneke, M. & Orr, J. 2016. Health impairments and conditions in children. In Landsberg, E.,
Kruger, D. & Nel, N. Addressing barriers to learning: a South African perspective, 3rd ed. Pretoria:
Van Schaik.
Kvalsvig, J.D., Taylor, M., Kauchali, S. & Chhagan, M. 2013. Acknowledging methodological
complexity in assessing children in HIV-affected communities in KwaZulu-Natal province, South
Africa. In Boivin, M.J. & Giordani, B. (Eds). Neuropsychology in children in Africa. Perspectives on
risk and resilience. New York: Springer.
Leigh, L.D. & Miles, M.A. 2002. Educational issues for children with cancer. In Pizzo, P.A. &
Poplack, D.G. Principles and practice of pediatric oncology, 4th ed. Philadelphia: Lippicott Williams
& Wilkins, 1463–1476.
Levin, M. 2008. Allergy and asthma. Available at:
http://www.asthma.co.za/Downloadable_content/Allergy%20and%20Asthma1.pdf (accessed on 12
March 2009).
Louw, J., Shisana, O., Peltzer, K. & Zungu, N. 2009. Examining the impact of HIV & AIDS on South
African educators. South African Journal of Education, 29(2): 205–217.
Maggiore, W.A. 2013. Recognizing & treating hypoglycaemia, hyperglycaemia and other diabetesrelated health problems. JEMS (Journal of Emergency Medical Services), 38(12). Available at:
http://www.jems.com/articles/print/volume-38/issue-12/patient-care/recognizing-treatinghypoglycemia-hyperg.html
Magnussen, P., Ndawi, B., Sheshe, A.K., Byskov, J. & Mbwana, K. 2001. Malaria diagnosis and
treatment administered by teachers in primary schools in Tanzania. Tropical Medicine and
International Health, 6(4): 273–279.
Malaria Policy Advisory Committee. 2016. Immunization, vaccines and biologicals. Geneva: World
Health Organization. Available at:
http://www.who.int/immunization/research/development/malaria_vaccine_qa/en/
Mamadou, B. & Duebel, T.F. 2006. Persistent hunger: perspectives on vulnerability, famine, and food
security in sub-Saharan Africa. Annual Anthropological Review, 35: 521–538.
Marais, B.J. & Graham, S.M. 2016. Childhood tuberculosis: a roadmap towards zero deaths. Journal
of Paediatrics and Child Health, 52: 258–261. doi:10.1111/jpc.12647
Marcus, M., Yasamy, M.T., Van Ommeren, M., Chisholm, D. & Saxena, S. 2012. Depression: a
global public health concern. WHO Department of Mental Health and Substance Abuse, 1: 6–8.
Miller, R.E. 2007. Childhood cancer. Available at:
http://kidshealth.org/parent/medical/cancer/cancer.html (accessed on 12 March 2009).
Morris, N., Frean, J., Baker, L., Ukpe, I., Barnes, K., Kruger, P., Mabuza, A., Raswiswi, E., Maharaj,
R., Blumberg, L. & Moonasar, D. 2013. Re-defining the extent of malaria transmission in South
Africa: implications for chemoprophylaxis. South African Medical Journal, 103(11): 861–864.
doi:10.7196/SAMJ.7533
Nabors, L., Troillett, A., Nash, T. & Masiulis, B. 2005. School nurse perceptions of barriers and
supports for children with diabetes. Journal of School Health, 75(4): 119–124.
Naswa, S. & Marfatia, Y.S. 2010. Adolescent HIV/AIDS: issues and challenges. Indian Journal of
Sexually Transmitted Diseases, 31(1): 1–10. http://doi.org/10.4103/0253-7184.68993
National Asthma Council Australia. 2008. Available at: http://www.nation
alasthma.org.au/html/emergency/index.asp (accessed on 10 March 2009).
National Cancer Institute. n.d. Childhood cancers: questions and answers. Available at:
http://www.cancer.gov/cancertopics/factsheet/Sites-types/childhood (accessed on 11 March 2009).
National Department of Education. 2008. National Strategy on Screening, Identification and Support:
school pack 2008. Available at:
http://curriculum.pgwc.gov.za/resource_files/20101953_SIAS_School_Pack_25_March_08.pdf
(accessed on 12 January 2009).
Neill, C.A., Clark, E.B. & Clark, C. 2001. The heart of a child. What families need to know about
heart disorders in children, 2nd ed. Baltimore, MD: Johns Hopkins University Press.
Nicas, M., Nazaroff, W.W. & Hubbard, A. 2005. Toward understanding the risk of secondary
airborne infection: emission of respirable pathogens. Journal of Occupational and Environmental
Hygiene, 2(3): 143–154.
Noll, R.B., Gartstein, M.A., Vannatta, K., Correll, J., Bukowski, W.M. & Davies, W.H. 1999. Social,
emotional, and behavioral functioning of children with cancer. Pediatrics, 103(1): 71–78.
Orelove, F.P., Sobsey, D. & Silberman, R.K. 2004. Educating children with multiple disabilities: a
collaborative approach, 4th ed. Baltimore, MD: Paul H. Brookes.
Restrepo, B.I. 2007. Convergence of the tuberculosis and diabetes epidemics: renewal of old
acquaintances. Clinical Infectious Diseases, 45: 436–438.
Rose, A.M., Hall, C.S. & Martinez-Alier, N. 2013. Aetiology and management of malnutrition in
HIV-positive children. Archives of Disease in Childhood. doi:10.1136/archdischild-2012-303348
Russell, J. & Fazari, L. 2010. Congenital heart defects: information for teachers about kids’ health.
Available at:
http://www.aboutkidshealth.ca/en/resourcecentres/congenitalheartconditions/athome/learningandeduc
ation/pages/congenital-heart-defects-information-for-teachers.aspx
Sarma, H. & Oliveras, E. 2013. Implementing HIV/AIDS education: impact of teachers’ training on
HIV/AIDS education in Bangladesh. Journal of Health, Population, and Nutrition, 31(1): 20–27.
Schwartz, F.L., Denham, S., Heh, V., Wapner, A. & Shubrook, J. 2010. Experiences of children and
adolescents with type 1 diabetes in school: survey of children, parents, and schools. Diabetes
Spectrum. 23(1): 47–55. doi:10.2337/diaspect.23.1.47
Sharp, P.M. & Hahn, B.H. 2011. Origins of HIV and the AIDS pandemic. Cold Spring Harbor
Perspectives in Medicine, 1(1): a006841. Available at: http://doi.org/10.1101/cshperspect.a006841
Shete, A. 2013. Current trends in HIV/AIDS. Journal of HIV/AIDS Infectious Diseases, 1: 1–2.
Shillingford, A.J., Glanzman, M.M., Ittenbach, R.R.F., Clancy, R.R., Gaynor, J.W. & Wernovsky, G.
2008. Inattention, hyperactivity, and school performance in a population of school-age children with
complex congenital heart disease. Pediatrics, 121(4).
Shisana, O., Labadarios, D., Rehle, T., Simbayi, L., Zuma, K., Dhansay, A., Reddy, P., Parker, W.,
Hoosain, E., Naidoo, P., Hongoro, C., Mchiza, Z., Steyn, N.P., Dwane, N., Makoae, M., Maluleke, T.,
Ramlagan S., Zungu, N., Evans, M.G., Jacobs, L., Faber, M. & SANHANES-1 Team. 2013. South
African National Health and Nutrition Examination Survey (SANHANES-1). Cape Town, HSRC
Press.
Shisana, O., Peltzer, K., Zungu-Dirwayi, N. & Louw, J. 2005. The health of our educators: a focus
on HIV/AIDS in South African schools. Cape Town: HSRC Press.
Shouldice, M. 2004. Chronic illness in children. In Haslam, R.H.A. & Valletutti, P.J. (Eds). Medical
problems in the classroom: the teacher’s role in diagnosis and management. Austin, TX: Pro-Ed.
Shrivastava, S.R., Shrivastava, P.S. & Ramasamy, J. 2013. Role of self-care in management of
diabetes mellitus. Journal of Diabetes & Metabolic Disorders, 12(14), 5 pages. Available at:
http://www.jdmdonline.com/content/12/1/14
Smit, C. 2004. Learning about life, death and my feelings. Somerset West: Bevan Printing.
Smit, C., Teitge, M.A. & Kleingeld, C. 2002. Learning about HIV/AIDS. Somerset West: Bevan
Printing.
South African Department of Education. 1999. National policy on HIV and AIDS for learners and
educators in public schools and students and educators in further education and training institutions.
Available at: http://wced.wcape.gov.za/branchIDC/special_ed/hiv_aids/National_policy_on_HIVAIDS.pdf (accessed on 11 March 2009).
Spiegel, G.L., Cutler, S.K. & Yetter, C.E. 1996. What every teacher should know about epilepsy.
Intervention in School and Clinic, 32(1): 34–38.
Spinelli, C.G. 2004. Dealing with cancer in the classroom. Teaching Exceptional Children, 36(4):
14–21.
Swaminathan, S. & Rekha, B. 2010. Pediatric tuberculosis: global overview and challenges. Clinical
Infectious Diseases, 50 (Supplement 3): S184-S194. doi:10.1086/651490
TB Alert. 2005. DOTS. Available at: http://www.tbalert.org/
Udonwa, N., Gyuse, A. & Etokidem, A. 2010. Malaria: knowledge and prevention practices among
school adolescents in a coastal community in Calabar, Nigeria. African Journal of Primary Health
Care & Family Medicine, 2(1), 4 pages. doi:10.4102/phcfm.v2i1.103
Valletutti, P.J. 2004. The crucial role of the teacher. In Haslam, R.H.A. & Valletutti, P.J. (Eds).
Medical problems in the classroom: the teacher’s role in diagnosis and management. Austin, TX:
Pro-Ed.
Van Aalderen, W.M. 2012. Childhood asthma: diagnosis and treatment. Scientifica, 2012, Article ID
674204, 18 pages. doi:10.6064/2012/674204
Vanelli, M., Chiari, G., Ghizzoni, L., Costi, G., Giacalone, T. & Chiarelli, F. 1999. Effectiveness of a
prevention programme for diabetic ketoacidosis in children: an 8-year study in schools and private
practices. Diabetes Care, 22(1): 7–9.
Vink, H. 2005. Brenda has a dragon in her blood. Cape Town: Tandym Print.
Votroubek, W. & Tabacco, A. 2010. Care of the child with altered cardiac function. In Votroubek,
W.L. & Tabacco, A. Pediatric home care for nurses: a family-centered approach, 3rd ed. Boston,
MA: Jones & Bartlett.
Ward, E., DeSantis, C., Robbins, A., Kohler, B. & Jemal, A. 2014. Childhood and adolescent cancer
statistics, 2014. CA: A Cancer Journal for Clinicians, 64(2): 83–103.
Westling, D.L. & Fox, L. 2009. Teaching students with severe disabilities, 4th ed. New Jersey:
Merrill Prentice Hall.
World Food Programme (WFP). 2000. Food and nutrition handbook. Rome: World Food
Programme.
World Food Programme (WFP). 2016. Available at: http://www.wfp.org/hunger/stats (accessed on 12
September 2016).
World Health Organization (WHO). 2016a. Malaria vaccine. WHO position paper. Weekly
Epidemiological Record, 91(4): 33–52.
World Health Organization (WHO). 2016b. Tuberculosis Fact sheet No.104. Reviewed March 2016.
Available on http://www.who.int/mediacentre/factsheets/fs104/en/ (accessed on 14 September 2016).
World Health Organization (WHO)/UNICEF. 2006. WHO/UNICEF: Review of National
Immunization Coverage 1980–2005. August, South Africa. Available at:
http://web.archive.org/web/20070630073246/http://www.who.int/immunization_monitoring/data/sou
th_africa.pdf (accessed on 12 March 2009).
Zelleke, T.G., Depositario-Cabacar, D.F.T. & Gaillard, W.D. 2013. Epilepsy. In Batshaw, M.L.,
Roizen, N.J. & Lotrecchiano, G.R. Children with disabilities, 7th ed. Baltimore, MD: Paul H.
Brookes.
PART
III
Functional approach to integrating
disability and support
This book explores what inclusion means from a number of different
perspectives and disciplines, thereby providing an opportunity to open up
dialogue about inclusion. In this final part of the book, a number of trends
in the body of knowledge with regard to inclusion are highlighted, such as a
zoom lens metaphor that uses a strengths-based approach, collaboration and
teamwork, as well as the use of narratives in training.
Throughout the book, a zoom lens metaphor of a camera that zooms in and
out is used as a scaffold to guide the move away from the historical special
education perspective to that of inclusive education. Despite the growing
conviction about the importance of participation of all learners for optimum
learning, the knowledge and skills of teachers have remained limited in
certain contexts. Teachers are in the process of redefining their roles in an
inclusive classroom and rediscovering the true meaning of the Latin word
educo, which means “bringing up” and “leading forth”. As inclusion
becomes more of a reality with more policies being implemented, teachers
will increasingly be exposed to diverse classrooms. They will therefore
need a variety of tools in their “teaching toolbox” to meaningfully involve
all learners.
Inclusion also emphasises the role of closer collaboration among different
members of the team, and teachers need to develop and build specific skills
in negotiation, joint decision making and problem solving. All of these are
skills can be developed, but they are often sadly lacking in training
programmes, of which the focus is too often on building specific content
knowledge. For example, teachers will be trained in how to deal with a
learner who has an epileptic seizure without addressing attitudinal issues
around epilepsy or seeing classroom management as a small part of the total
service delivery to this learner. Teachers should therefore realise that they
contribute valuable knowledge to the rest of the team due to their particular
training, expertise and function.
Throughout this book, a different approach to training is used, namely the
use of personal narratives. This enables teachers to extend and improve
their knowledge base (particularly with regard to disabilities and learning)
through listening to the stories of those who struggle with the same issues
they face on a daily basis. In this way, teachers are provided with
appropriate teaching strategies to equip them for the unique problems they
might face in their work. As it is expected of teachers to work
independently after any type of training (e.g. after a workshop on
differentiated teaching), the value of this approach is evident.
14
Integrating disability and
support
May He who has chosen to limit some of His children, be merciful
enough to guide the hands of us, entrusted with their care (and
education).
R. W
M
14.1 INTRODUCTION
This book is about thinking and believing. It is about teachers who bring
their knowledge, skills, attitudes and dispositions into the classroom,
ultimately impacting on the outcome of each of the hundreds of learners
who passes through their hands. It is about equipping teachers to teach in
classrooms that in all likelihood do not resemble the classrooms they
attended when they were growing up. It is about implementing feasible and
realistic teaching strategies in large classrooms with limited resources. It is
about accepting and embracing diversity and collaborating with others.
Education must become more multifaceted and dynamic if it is to work for
everyone (Schwarz, 2006).
The goal of this chapter is to integrate the first two parts of the book and to
provide a picture of “real inclusion” in South African classrooms. It will
start by critically evaluating where inclusive practices are at present, by
providing some reasons for optimism. The relevance of Education White
Paper 6 as a policy document aimed at building an inclusive education
system is highlighted. Finally, some suggestions for the way forward are
made based on a critique of the areas of concern.
14.2 INCLUSION IN SOUTH AFRICA: CURRENT POLICY
AND PRACTICE
Focusing on the strengths and positive educational outcomes achieved by
means of inclusion and looking at effective current practices seems to be the
logical starting point for a discussion on ways to expand inclusive
education; in other words, to look at what is working, then do more of it.
However, it would be foolish not to take note of the areas of concern and
then address them in a constructive manner, because if something does not
work, it should be done differently. One of the biggest challenges facing
teachers today is to engage the hearts and minds of all learners.
14.2.1 Reasons for optimism
Motivation is the fuel that generates and directs energy and efforts, hence a
teacher’s motivation is the best predictor of ultimately success. In addition,
focusing on positive aspects is one of the most effective strategies for
ensuring motivation. Table 14.1 highlights some of the strengths and
positive factors that give reasons for optimism.
Table 14.1 Reasons for optimism
1
Schools welcome all learners, and peer support is encouraged. In 2012
approximately 120 000 learners with disabilities were included in mainstream schools
(Martin, 2014).
2
The general education curriculum is used as the basis for teaching with an emphasis
on support regardless of the type or severity of the disability.
3
Alternative assessment possibilities exist.
4
Collaboration and partnerships between families and professionals are encouraged.
5
Challenging behaviour is seen as an attempt to communicate: positive behavioural
support can be in place.
6
Diversity is valued.
7
Zoom lens perspective in a support-based framework is advocated.
14.2.1.1 Inclusion: a strategy for change or attempting the impossible?
This book began by asking what inclusion is; however, 13 chapters later
there is no one definition that encapsulates inclusion in its truest sense. The
main reason for this is that inclusion means different things to different
people, and therefore a simple (yet not oversimplified) definition might
possibly not add anything to the inclusion rhetoric. Some authors have also
started actively advocating for de-sloganising inclusion and abandoning the
inclusion bandwagon (Pather, 2008). However, there seems to be consensus
on some of the factors, such as the fact that true inclusion is about attitudes
and belonging – the attitude that all learners belong everywhere with
everyone else in the school (Schwarz, 2006).
Inclusion is also about achieving quality and appropriate education, and
arguably the best strategy for this is through supports such as collaborative
teaming, innovative learning approaches, differentiated teaching,
curriculum adaptation and the use of a study buddy system. Classrooms
need to be exciting, inspiring, thought-provoking and enlightening
environments for all learners. The notion of “all learners” refers to children
with diverse characteristics (e.g. race, gender, ability and socioeconomic
status) as well as those who for any reason experience difficulties in
becoming part of the classroom’s learning community (Snell & Brown,
2011).
The face of education has changed dramatically in South Africa since the
implementation of White Paper 6 as the preferred education policy for a
single, undivided education system for all learners (no special and
mainstream schools), using a curriculum that is more flexible and suited to
the needs of all children, and developing district-based support teams to
provide support to teachers (National Department of Education, 2001).
White Paper 6 facilitates the paradigm shift from the deficit-based medical
model to the acceptance of the biopsychosocial model and the notion that
inclusion is part of the human rights discourse. However, 15 years later,
most children are still in special schools and there is no consensus about
what should and should not be classified as a disability in South Africa
(Heap, Lorenzo & Thomas, 2009). Unfortunately some individuals still do
not see disability as relating to functional aspects (in other words, how the
learner’s life is affected, or how he copes with the difficulties brought on by
the impairment in his daily life). When referring to these learners, they have
simply replaced the term learners with special needs with learners with
barriers (Howell & Lazarus, 2008). This means that the concept of special
needs has merely been replaced by barriers without a conceptual shift in
understanding that disability does not lie at an individual level but that it
lies outside the individual. If the environment is changed in such a manner
that it provides sufficient support, the individual might not experience any
barriers to learning.
Another critical element of White Paper 6 is that it is essentially about the
importance of the role of the teacher in making the curriculum accessible to
all learners, and contemporary South African teacher training focuses on
how to accommodate diverse learners in a single classroom (Oswald &
Swart, 2011). This is in line with the Minimum Requirements for Teacher
Education Qualifications (Department of Higher Education and Training,
2011) which emphasises that all teachers need to understand how to
implement inclusive education. This is different from earlier views that
specialised staff (mostly therapists) were more important than teachers in
providing education for these learners. Teachers have embraced the role of
ensuring that all learners have the right to learn and participate in the
classroom, as this aligns with their core purpose of teaching and learning.
Research has also shown that teachers with more education and inclusive
training tend to hold more positive attitudes towards learners with
disabilities (Forlin, Loreman, Sharma & Earle, 2009).
Furthermore, White Paper 6 is committed to a community-based approach,
which suggests that the main resources for providing support in teaching
and learning are drawn from the school, from the parents and from the local
community within which the school is located (Howell & Lazarus, 2008).
Community-based support focuses on building the capacity of those in and
around the school to understand their own needs, but the real issue is a more
complex one of exploring how to train teachers and parents using resources
in the most economical way to ensuring long-term sustainability. Much has
been written about community-based intervention and building community
supports to sustain intervention efforts (Hartley, Nganwa & Kisanji, 2002).
Although the merit of this approach is largely self-evident, it often imposes
additional challenges on teachers and already tired and poorly resourced
community members (McConkey & Alant, 2005).
14.2.1.2 Access to the general curriculum: including differentiated teaching
For many children in South Africa and other developing countries, good
education is a basic human right as well as a reality, but many others are not
so fortunate. For children with disabilities, the focus of inclusive education
is often more on caring, loving and socialising than on learning (Donohue
& Bornman, 2015). This is apparent in the general attitude towards these
children based on the assumption that only care and love are needed, as
teachers have low expectations in terms of their potential for learning
(Bornman, Alant & Uys, 2008).
Fortunately, with the implementation of White Paper 6, curriculum options
for these learners have been expanded and they are now better aligned to
the general curriculum. Differentiated teaching (multilevel instruction) is
viewed as an effective strategy in diverse classrooms, as each learner has
individualised learning outcomes that may be at different levels (below, at
or above grade level) within the same curriculum area (Snell & Brown,
2011). In this book, aspects such as knowing each learner’s individual
characteristics and learning style are emphasised as hallmarks of good
teaching practice.
A critical aspect of good teaching practice is maintaining instruction with a
just right challenge – in other words, work that is neither too easy nor too
difficult. A number of aspects impact on this – first, the amount of new
information that is taught, which is linked to, among other things, a child’s
age. For example, a Grade 1 learner can typically manage three new chunks
of information, whereas a Grade 10 learner might manage seven (Snell &
Brown, 2011). Second, the demands of the task have an impact. For
example, for comprehension tasks learners need to know 93 to 97 per cent
of the material in order to be in their optimal zone for learning. This implies
that only 3 to 6 per cent of the material should be new. However, if it is not
a comprehension task but one that requires drill and practice, 70 to 85 per
cent of the material should be known with only 15 to 30 per cent new
material (Gravois & Gickling, 2002).
South Africa’s current basic education policy, the Curriculum and
Assessment Policy Statement (CAPS, 2011) is built on the following
principles (Department of Education, 2011):
Social transformation: redressing educational imbalances of the past and
ensuring equal educational opportunities for all learners
Active and critical learning: encouraging active and critical learning
High knowledge and high skills: setting high minimum standards of
knowledge and skills at each grade and in all subjects
Progression: progressing from simple to complex content in each grade;
English home language Grades R–3 CAPS 5
Human rights, inclusivity, environmental and social justice: sensitising
the curriculum to issues around poverty, inequality, race, gender,
language, age and disability
Valuing indigenous knowledge systems: acknowledging South Africa’s
rich history and heritage to nurture the values contained in the
Constitution
Credibility, quality and efficiency: providing a basic education that is
comparable to those of other countries
From the above principles it is clear that inclusion should be at the centre of
each school’s organisation, management, planning and teaching. This can
happen only if all teachers understand how to recognise and address barriers
to learning, and how to plan for diversity. For example, it is more
straightforward to try to remove intrinsic learner barriers (e.g. some
physical barriers can be removed by providing ramps while some sensory
barriers can be removed by providing batteries for hearing aids), than trying
to remove some of the extrinsic barriers the learners face (e.g. poverty or
being orphaned due to HIV/AIDS) (Donohue & Bornman, 2014).
14.2.1.3 Alternative assessment opportunities
Assessment in an inclusive classroom requires teachers to make a huge
paradigm shift in their thinking. Assessment can no longer be viewed as a
process of gathering scores for grading or comparing learners, but rather as
part of the learning process – in other words, how a learner thinks about and
learns what is being taught (Nel, 2015). Assessment should be seen as an
attempt to determine what a learner can do and not about what he cannot.
For example, if a learner is able to read Grade 2 material, but is assessed on
Grade 3 material, the teacher will only see what he cannot do rather than his
actual skills in decoding and understanding the text. Spending most of the
time in his area of weakness will improve his skills, perhaps to a level of
average, but it will never produce excellence. Furthermore, by focusing on
what the learner cannot do, his motivation, which leads to participation, will
plumment. The purpose of assessment should never be to create fear or
discomfort for the learner, but to discover what he knows and what he can
do.
Along with curricular changes to CAPS, assessment practices were also
adjusted. CAPS describes assessment as a continuous planned process of
identifying, gathering and interpreting information about learners’
performance through the use of various forms of assessment (Department of
Education, 2011). The form of assessment selected is dependent upon the
subject – for example, debates may not be the most appropriate method of
assessing maths skills, but are ideally suited to assess language skill. The
form of the assessment also depends on the age of the learners, for example
writing an essay is not appropriate for young learners with limited writing
skills. Other forms of assessment that can be explored include pen-andpaper tests and exams, role plays, simulations, making a collage, building
structures, designing posters, conducting research, reading and analysing
literature, case studies, questionnaires, portfolios, projects and presentations
(Nel, 2015).
An effective assessment would give the teacher an understanding of the
following (Doerries, 2004):
What the learner knows. Prior knowledge is the foundation of learning,
and linking new knowledge to prior knowledge is one of the best
practices for effective knowledge retention.
What the learner does. The assessment task must provide an appropriate
challenge and be linked to prior knowledge. If the task is too difficult, or
if the learner does not understand the instructions, he will be unable to be
successful and show what he can do.
How the learner thinks. Teachers can ask learners to think aloud and
explain how they came to their answer, as this will assist them to know
where the learners have knowledge gaps.
How the learner approaches tasks he is unsure of. During challenging
tasks, teachers should evaluate persistence and frustration tolerance, and
at which point the learner asks for help or just gives up.
14.2.1.4 Collaboration and partnerships
When parents and teachers work together, the impact on the child’s
development and learning multiplies. An effective partnership between
teachers and parents is pivotal to ensuring long-term and sustained effects
(Bornman et al., 2008). The mindset of us versus them, school versus home
has to stop. Parents are not the enemy! All should work together as a
cooperative, collaborative team to educate every learner effectively. Parents
should be seen for the experts they are – they look after their child for the
18 hours of the day when he is not at school. When everyone in the team is
committed to making inclusion work, the efforts are successful. Parents and
teachers should act as a support network for each other, and opportunities
for them to meet and to share ideas and experiences, and to help solve each
other’s problems should be a high priority (Atkins-Burnett & Allen-Meares,
2000).
14.2.1.5 Positive behavioural support
Looking at challenging behaviour as a means to communicate specific
intentions (e.g. requesting attention or desired items, or trying to avoid
difficult tasks) has been one of the most exciting developments in the
disability field over the past two decades. Challenging behaviour has been a
major obstacle to independent living, and to educational and employment
opportunities (Snell & Brown, 2011). In the past, challenging behaviour
was seen as part of the disability and it was assumed that acceptable
behaviour was a prerequisite for being allowed to participate in social
contexts. The current trend, however, is to see all behaviours as learned,
including challenging behaviour, and to teach more acceptable forms of
behaviour in real-life contexts. The strategies associated with the
management of challenging behaviour focused on identifying specific
situations that trigger the behaviour, and then avoiding those situations. In
cases where it is not possible to avoid triggers, strategies are taught to
manage the situation, for example through the use of visual schedules that
assist with predicting a series of events.
14.2.1.6 Valuing diversity
In science, a diverse ecosystem is generally accepted as being a stronger,
healthier and more enduring system (biodiversity). Similarly, differences
(the more the better) are seen as the building blocks of a robust living
community (Schwarz, 2006). The world is becoming increasingly
heterogeneous, not only in terms of race, ethnicity and language, but also in
terms of the participation of persons with disabilities who are no longer
institutionalised and locked away from society as was done in the past
(Kreps, 2000). One of the factors that either facilitates or hinders inclusion
is the attitude of peers. It is never too early (or too late) to teach children
about diversity and the potential positive effects of inclusion on both
children with disabilities and their non-disabled peers have been well
documented (Von Tetzchner, Brekke, Sjøthun & Grindheim, 2005).
14.2.1.7 Strengths-based approach
A strengths-based approach works on the premise that all people have the
strengths and resources needed for their own empowerment. Individuals
gain more when they build on their strengths than when they make
comparable efforts to improve their areas of weakness (Clifton & Harter,
2003).
Historically, teaching and other intervention models took the deficit-based
approaches for granted, ignoring the strengths and experiences of learners.
In a strengths-based approach, the focus is on the child and on strengths and
assets. It does not, however, negate problems, but rather shifts the frame of
reference to defining the issues. By focusing on what works well, informed
successful strategies support the adaptive growth of organisations and
individuals.
Stop and reflect
What are strengths?
Talent + Knowledge + Skills = Strengths
By focusing on what is working well, the development and learning of
individuals are supported. As far as individual strengths are concerned,
small movements in any individual in the system creates movements in
others in the system (Ebersöhn & Eloff, 2006), thus if any person makes the
slightest change in behaviour (e.g. the teacher places the child with highfunctioning autism next to a buddy who can encourage him to continue with
his work), it will also lead to changes in others (e.g. the buddy has increased
self-esteem because he knows that he is making an important contribution,
and the child with high-functioning autism is satisfied because he receives
positive feedback from the teacher). In using a strengths-based approach,
teachers are encouraged to see strengths and assets rather than only needs.
No school is too hopeless to implement inclusive education because it may
be under-resourced, and neither is any individual too disabled to benefit
from some form of education. Learned helplessness is, without a doubt, the
worst disability of all, therefore the best gift teachers can give learners is
the ability to participate by nurturing their inherent strengths and building a
platform for the development of independence.
14.2.2 Areas of continuing concern
It would be foolish and irresponsible not to discuss the areas of current
concern in the educational field. In popular media and education circles,
certain issues frequently come to the fore. The 2015 matric results were
disconcerting as there was a 5,1 per cent drop in the pass rate from the 2014
figures to 70,7 per cent (Quintal, 2016). In effect this means that 30 per cent
(three of ten) learners failed.
Second, literacy education has come increasingly under the spotlight
following South Africa’s poor performance in the 2006 international
Progress in International Reading Literacy (PIRLS) study conducted with a
sample of Grade 4 and Grade 5 learners. Results from PIRLS 2006 showed
that only 13 per cent of the Grade 4 learners and 22 per cent of the Grade 5
learners reached the Low International Benchmark while 94 per cent of
learners in half of all the other participating countries reached this
benchmark. Not reaching this benchmark is considered as a serious risk
factor for not learning how to read (Howie et al., 2008) Furthermore, the
South African learners achieved the lowest score of the 45 countries that
participated, including other middle-income countries such as Morocco,
Iran, Trinidad and Indonesia (Howie et al., 2008). In 2011, South Africa
participated in the PIRLS study again, with the majority of Grade 4 learners
completing the pre-PIRLS assessment which is a shorter, easier test at a
lower level of cognitive demand. Unfortunately, the South African Grade 4
learners still performed at a low level overall on this easier assessment in
comparison to their international counterparts (Zimmerman & Smit, 2014).
Third, the language of learning and teaching (LOLT) used in schools has
been a much-debated topic, and many South African children do not speak
the language used in schools (mostly English). Recognising and responding
to diversity is a key principle of inclusive education, yet the important role
of language in our multicultural context is often overlooked. There is
growing evidence that first-language-based multilingual education is the
most appropriate approach for children who do not use the language of
instruction at home (Pinnock, 2008). This approach states that children need
good-quality education in their first language (also referred to as home
language or mother tongue), and that the second or third languages should
be gradually introduced, transferring to second-language instruction, if
needed, only after at least six years of first-language instruction (Alidou et
al., 2006). First-language instruction has also been linked to greater
motivation to attend school, doing better at learning and improved language
skills (Pinnock, 2008). This is in line with the recommendation of the
Department of Basic Education’s Overview report (2010) which strongly
recommends that learners’ first language should be used for learning and,
particularly in the Foundation Phase when children learn to read and write
and that teaching and learning material should be made available in all
languages. When learners have to make a transition from their home
language to an additional language, careful planning is necessary.
Fourth, much has been written about the importance of leadership in
schools. A recent systematic review showed that school leadership and
management skills are developing but it also flagged some ongoing
challenges, including poor learner outcomes, conflict with teacher unions,
uneasy relationships between principals and school-governing bodies and
leadership that remains focused on administration rather than on teaching
and learning (Bush & Glover, 2016).
Although these issues are important, they are not the focus of this book.
Only issues more closely related to inclusive practices will be described in
detail. This is not done in an attempt to suggest that inclusion is failing in
South Africa, but rather as an attempt to address and fix some of these
issues (see Table 14.2).
Table 14.2 Areas of concern
1
Uneven and inconsistent access to inclusive classrooms
2
Questionable quality of instruction
3
Challenging working conditions for teachers
4
Limited resources
5
Limited pre- and post-school opportunities
Source: Adapted from Snell & Brown (2011)
14.2.2.1 Uneven and inconsistent access to inclusive classrooms
South Africa has a national disability prevalence rate of 7,5 per cent
(Statistics South Africa, 2014), with the highest proportion of people with
disabilities in the Free State and Northern Cape provinces (11 per cent
each), followed by North West (10 per cent) and the Eastern Cape (9,6 per
cent), and with the lowest percentages in the Western Cape and Gauteng (5
per cent each). It is estimated that 8 per cent of children with disabilities
between the ages of seven and 15 years were out of school, and this figure
for 16–18-year-olds is 24 per cent (Martin, 2014). The Department of Basic
Education estimates that in 2010/2011, approximately 400 000–480 000
children with disabilities were out of school (Martin, 2014) This is an area
of concern as the value of early childhood intervention is widely recognised
(Shonkoff & Garner, 2012). This includes aspects such as the prevention of
developmental delays in young children, the identification of at-risk
children and families to provide sufficient support to prevent further
difficulties, and the minimisation of the impact of a disability on the further
development of a child. All of these aspects contribute to building a strong
foundation for educational achievement, economic productivity, responsible
citizenship, and lifelong health that will ultimately impact on the quality of
life of the children and their families, as well as on the broader community.
The enormous distances in some parts of the country where a single rural
special school is required to act as a resource centre for the whole area is
resulting in extreme challenges (Martin, 2014). In some provinces, such as
the Eastern Cape, schools in rural areas still lack running water and toilet
facilities.
14.2.2.2 Questionable quality of instruction
The quality of instruction continues to be a serious and ongoing issue, as
teachers increasingly discover that inclusion is more than a one-size-fits-all
programme. As alluded to earlier in the book, being physically present in a
classroom with peers who do not have disabilities is not enough to be
included. When a child is simply fitted into the routine of the school, this is
mere integration – inclusion only happens once a school changes to fit the
needs of the child. In many schools, the idea of inclusion still tends to be
more about the child simply fitting in.
Inclusion requires that supports be put in place to allow optimal
participation of all learners in their different contexts (e.g. home, school and
community) without any form of discrimination, which can work only if the
school and teachers are willing to try. Half-hearted attempts and lip-service
will only make things worse.
However, inclusion should not take away teachers’ ability to offer specialist
services. For example, all teachers can be taught how to make certain
classroom adaptations to accommodate diverse learners, but not all teachers
will have the skills to teach children who are blind to read by means of
Braille. In some instances, therefore, specialist services will always remain
a high priority.
Based on global trends, teachers should also become more skilled in using
computer software and websites in their classrooms as this makes learning
more enjoyable and memorable, and is more effective in accommodating
different learning styles (Nompula, 2012). Electronic media and the internet
are widely recognised as the vehicle through which local, regional and
global institutional contemporary activities and effective transformation
take place (Delacruz, 2009). Supplementing web-based learning with a
variety of other instructional strategies, such as graphic organisers of
content, concept maps and salient navigation cues to help slower learners, is
generally considered as best classroom practice.
What would be the most effective way to equip teachers to offer effective
instruction in diverse classrooms? Possibly a two-tiered approach, which
would include the following:
The need to train new teachers more effectively in teaching all learners.
There is a need for both well-trained general teachers who have deep
knowledge about subject areas and specialist teachers who have expertise
in effective instruction for learners with disabilities (e.g. Braille and
SASL).
The need to redesign teacher education programmes. There is a common
core of knowledge that all teachers should have in order to work
effectively in inclusive schools. Universities and other teacher training
institutions need to be more intentional in redesigning their teacher
education programmes to provide novice teachers with this common
knowledge base and set of experiences.
14.2.2.3 Challenging working conditions for teachers
South Africa faces a chronic shortage of qualified teachers with too few
entering the teaching profession, too many leaving the profession, and too
many inappropriately deployed (Centre for Education Policy Development
et al., 2005). This shortage is a result of many factors, including the exodus
of teachers to other countries such as Britain, the HIV/AIDS pandemic, low
salaries and challenging working conditions (Crouch & Perry, 2003). In
2005, there were 8 144 South African teachers in Britain and in 2015 17
752 South African teachers were working abroad (Magubane, 2016). The
main reason given for this is the promise of a higher salary and better
benefits such as housing and medical aid (Magubane, 2016; Miller, Ochs &
Mulvaney, 2008). This matter is further complicated by the fact that a large
proportion of South African teachers are older than 50 years of age
(Armstrong, 2009), and hence reorientation of these teachers (who would
all have approximately 30 years of experience or more) to new ways of
teaching remains a significant challenge. Older South African teachers tend
to hold more negative attitudes toward inclusion than their younger
counterparts (Bornman & Donohue, 2013). Furthermore, when teachers are
promoted to the positions of principal or deputy principal, they become
administrators, and in this way competent teachers are lost to the school.
However, the role of the school principal as a role model, enabler,
champion and a visionary for inclusive education should never be
underestimated.
When asking teachers themselves about the factors that hinder inclusion,
they cite lack of specialised knowledge, overcrowded classrooms, lack of
support personnel such as classroom assistants, the demands of the
curriculum and lack of educational materials (Walton, 2011; Walton &
Lloyd, 2011).
14.2.2.4 Limited resources
The question is no longer about whether to include all children, but how to
do it effectively. Teachers regard quality education as being difficult to
achieve (Nelson Mandela Foundation, 2005). The most important problems
teachers cite are a lack of teaching aids (71%), a lack of cooperation from
parents (60%), poor infrastructure (59%) and teacher shortages (48%). In a
survey of 25 156 mainstream schools, it was found that 97,1 per cent did
not have accessible toilets for children with disabilities, and that 97,8 per
cent had no ramps (Martin, 2014). Regarding inclusion, one of the greatest
challenges that face many schools today is that the resources to
accommodate children with disabilities are not in place, and often the
schools are used as a place to “dump and run”, leaving the teachers to cope
on their own. If the supports are not in place, including teaching assistants,
smaller class sizes, special equipment, test accommodations for learners and
flexible teaching schedules, then the school is simply not an inclusive
school (Donohue & Bornman, 2015). In these instances, the children do not
flourish in the school. They continuously fail and as a result become deschooled after a few months. In some instances, the door to education
literally closes for them, leaving them at home where they often become
victims of crime, abuse or neglect.
In many ways the current education system is not conducive to what might
be considered as ideal in the education of diverse learners. Inclusion is
needed, not placement, and to make this a reality, more resources and by
default more training are needed. Special schools as well as full-service
schools are receiving assistive devices and technology from the Department
of Basic Education in order to mediate the impact of disability. These
include spectacles, hearing aids, cochlear implants, wheelchairs, white
boards, Perkins Braillers, white canes, bookmakers, augmentative and
alternative communication devices (AAC), etc. (Department of Basic
Education, 2013).
Stop and reflect
It will have little to no effect if learners who are unable to speak are simply provided
with speech-generating devices, but teachers are not effectively trained to use them.
AAC devices have a certain “magical quality” as they provide opportunities to express
basic needs in a manner understandable to most people, thereby facilitating
inclusion. Frustration is reduced as communication needs are being met due to the
fact that children are given a means to express themselves. Furthermore, the
provision of an AAC device raises expectations (teachers start to expect more from
these learners, which impacts positively on learning), and it also allows children who
do not speak to become more independent.
Although devices might thus solve many problems, merely providing them will not
solve all of them – and hence they are not really magic. They do not operate by
themselves, and teachers (and learners and parents) have to be trained in how to use
them. One single device will also never meet all of a learner’s communication needs.
Devices are relatively expensive (i.e. the device itself, cost of training, cost of
maintenance and cost of repair) and some are not portable. However, devices have
opened up communication opportunities for non-speaking learners to participate more
effectively in interaction, which positively impacts on education.
Sceptics may therefore argue that the provision of assistive technology by
the Department of Basic Education is at risk of failing because teachers are
not receiving appropriate training in using these devices. The opposite is,
however, also true. Well-equipped resource centres do not guarantee
successful inclusion. Sometimes low-tech options such as large-print books,
adapted positioning and seating, behaviour management programmes or
modified desks may be sufficient.
For inclusion to work effectively, more resources should go into resourcebased schools and to forming a closer relationship between these schools
and full-service schools, with more use of specialist expertise (e.g. provided
by DBST) (Donohue & Bornman, 2014; 2015). Inclusion, if implemented
properly, is expensive, but the old special schools model was also expensive
(Wilce, 2006). What evidence there is, is that if children with disabilities
mix with peers without disabilities, this helps to make people in society
more accepting of difference (Von Tetzchner et al., 2005).
14.2.2.5 Limited pre- and post-school opportunities
The school years are characterised by three major transitions, namely from
pre-school to primary school, and then from primary school to high school,
and finally from high school to adulthood, which is seen as a rite of passage
for most learners. Some leave for further studies at university or universities
of technology, others begin jobs and some start families. For most this it is
seen as an exciting time with the promise of increased independence and
participation in communities (Leinert, Jones, Sheppard-Jones, Harp &
Harrison, 2012). Unfortunately, this is not true for the majority of learners
with disabilities. It is estimated that there are 3,2 million youth between the
ages of 16 and 24 classified as NEET youth (not in education, employment
or training) (Department of Women, Children and People with Disabilities,
2013). The availability of further education and training (FET) colleges for
children with disabilities is a neglected area and of grave concern. The fact
that there is no national policy that covers education and training for
persons with disabilities at post-school FET level contributes to this
(Martin, 2014). Recent research has shown that as many as 68 per cent of
working-age South Africans with disabilities have never attempted to seek
employment (Pitso & Magubane, 2014). This is attributable to a variety of
reasons. For example, learners do not master certain prerequisite skills; low
expectations of individuals with disabilities as they may be viewed as
unemployable; and limited work opportunities. While sheltered workshops
and other day-care facilities may be well intended, they are inconsistent
with the core values of inclusive education.
Teachers hold a precious responsibility, and too many learners are saying:
“School failed me. I am unemployed” (Schwarz, 2006). Employers look for
a number of essential skills in their employees: the ability to collaborate, to
solve problems, to access information, to apply technology, to be innovative
and to use their imagination – all skills which can easily be taught in
inclusive classrooms if teachers are made aware of their value.
Another important transition time is from pre-school to primary school. The
early childhood development years have been prioritised by government as
this is seen as the period in which children grow and thrive physically,
mentally, emotionally, spiritually, morally and socially, as discussed in
Chapter 6 (Biersteker, 2001). Since 1994, various policies and documents
have been developed to address the needs of children, and these have been
implemented across different government departments (primarily the
Departments of Social Development, Education and Health, and the Office
of the Rights of the Child in the Presidency). The provision of services to
pre-schoolers has therefore been fragmented and uncoordinated, which has
resulted in ineffective service delivery (UNICEF, 2005). White Paper 5 on
Early Childhood Education (Department of Education, 2001b) is currently
being implemented and, as discussed in Chapter 6, 95 per cent of children
enrolled in Grade 1 in 2015 had been in Grade R the previous year.
Teachers therefore has a big responsibility to ensure the school readiness of
young learners. The training of Grade R teachers has become a core
concern as most do not hold appropriate qualifications. From 2019 the
minimum qualification for Grade R teachers will be the Diploma in Grade
R (NQF 6 Level). Together with policies such as the National Integrated
Early Childhood Development Policy (South Africa, 2015) and the National
Development Plan (2030), there is hope for building strong educational
foundations for all children (South Africa, 2012). ECD programmes have
the potential for producing positive and lasting effects on children, and in
order to turn this vision into a reality, partnerships between all the different
role players are needed.
14.3 SHAPING THE FUTURE: WHAT WILL INFLUENCE
EDUCATIONAL OUTCOMES?
Better understanding and appreciation of the role teachers can play should
lead to better inclusive practices. Inclusion may not always be the easier
option, but it is always the better one. We look forward to a future in which
seemingly diverse role players work together in an integrated manner in
order to optimise educational outcomes. Figure 14.1 shows three
intersecting circles that represent the critical role players, namely the
teachers, parents and learners. These circles are of equal size to indicate that
they all play an equally important role in the educational process. It is also
important to realise that each of these role players brings their own beliefs,
attitudes and values to the situation, and that they all need to feel safe in
order to explore, share, challenge and rethink some of them (Donohue &
Bornman, 2014). If the role players understand where the others are coming
from, it will be easier to plan how to work together. The various role
players also interact differently with each other – that is, the teacher–parent
collaboration is one of respectful adult-to-adult interaction, while a positive
teacher–child collaboration will result in effective learning. The main
purpose of the parent–child collaboration is to build a strong nurturing
relationship. It is also important to remember that at certain points in time,
other team members can become part of the collaboration process for a
certain period of time. For example, if a learner develops visual problems
and requires spectacles, the optometrist may become part of the team for a
while.
Figure 14.1 Basic beliefs, assumptions and attitudes that influence the
educational outcomes
In summary, collaboration requires all involved to listen to each other, to
respect each other’s rights, to create safe learning environments where
teachers strive to support learners and where parents support teachers, and
finally, to strive to help and assist each other (Idol, 2002).
14.4 CONCLUSION
What is the most important job in life? Teaching! Professor Jonathan
Jansen, former rector of the University of the Free State (2009) wrote a
moving personal story about his Grade 1 teacher and concludes: “Because
of you, I became a teacher, and, whenever I meet people I tell them, ‘If you
wish to honour me, call me teacher’.” Teaching is a noble profession as it
not only educates everyone from all walks of life, but it also has an
incredible responsibility. Teachers have the ability to shape and mould the
lives of those learners who pass through their classes, with the proverbial
power to make or break them.
REFERENCES
Alidou, H., Boly, A., Brock-Utne, B., Satina Diallo, Y., Heugh, K. & Ekkehard Wolff, H. 2006.
Optimizing learning and education in Africa – the language factor: a stock-taking research on
mother tongue and bilingual education in sub-Saharan Africa – Working draft. Pretoria: HSRC Press.
Armstrong, P. 2009. Teacher pay in South Africa: how attractive is the teaching profession?
Stellenbosch Economic Working Papers 04/09. Available at:
http://ideas.repec.org/p/sza/wpaper/wpapers76.html
Atkins-Burnett, S. & Allen-Meares, P. 2000. Infants and toddlers with disabilities: relationship-based
approaches. Social Work, 45(4): 371–380.
Biersteker, L. 2001. Early childhood development: a review of public policy and funding. Cape
Town: Children’s Budget Unit, IDASA.
Bornman, J., Alant, E. & Uys, C.J.E. 2008. From caring to education for children with severe
disabilities in a rural context. In Waddell, A.T. & McBride, R.M. (Eds). New research on early
childhood education. Hauppauge, NY: Nova Science.
Bornman, J. & Donohue, D.K. 2013. South African teachers’ attitudes towards learners with barriers
to learning: attention-deficit disorder and little or no functional speech. International Journal of
Disability, Development & Education, 60: 85–104.
Bush, T. & Glover, D. 2016. School leadership and management in South Africa: Findings from a
systematic literature review. International Journal of Educational Management, 30(2): 211-231.
doi://dx.doi.org/10.1108/IJEM-07-2014-0101
Centre for Education Policy Development (CEPD), Centre for Evaluation and Assessment (CEA)
University of Pretoria, Human Sciences Research Council (HSRC), South African Institute for
Distance Education (SAIDE). 2005. Teacher education in South Africa: proposal for a research and
development programme. Available at: http://www.cepd.org.za/files/TESAProposal.pdf (accessed 18
March 2009).
Clifton, D.O. & Harter, J.K. 2003. Strengths investment. In Cameron, K.S., Dutton, J.E. & Quinn,
R.E. (Eds). Positive organizational scholarship. San Francisco: Berrett-Koehler.
Crouch, L. & Perry, H. 2003. Educators. In HSRC Human Resources Development Review 2003:
education, employment and skills in South Africa. Available at:
http://media.hsrcpress.co.za.dedi423.nur4.host-h.net/downloadpdf.php?
pdffile=files%2FPDF%2F1981%2F1981_21_Human_Resources_Development_Review_2003%7E1
0112004011104PM.pdf&downloadfilename=Human%20Resources%20Development%20Review%2
02003%20-%20Chapter%2021%20Educators (accessed on 18 March 2009).
Delacruz, E.M. 2009. Art education aims in the age of new media: Moving toward global civil
society. Art Education, 62(5): 13–18.
Department of Basic Education. 2010. The Status of the Language of Learning and Teaching (LOLT)
in South African Public Schools: A Quantitative Overview. Pretoria: Department of Basic Education.
Available at http://www.education.gov.za/Portals/0/Documents/Reports/Status%20of%20LOLT.pdf?
ver=2011-03-30-231358-000 (retrieved on 16 September 2016).
Department of Basic Education. 2013. Challenges faced by deaf learners regarding facilities and
equipment. PowerPoint presentation to the Portfolio Committee on Public Service and
Administration.
Department of Education. 2001a. Report on the national ECD Pilot Project. Pretoria: ECD
Directorate.
Department of Education. 2001b. White Paper 5: Early Childhood Development. Pretoria:
Department of Education.
Department of Education. 2003. Revised National Curriculum Statement Grades R to 9 (Schools).
Pretoria: Department of Education.
Department of Education. 2009. Education statistics in South Africa 2007. Available at:
http://www.education.gov.za/emis/emisweb/07stats/Education%20Statistics%20in%20South%20Afri
ca%202007.pdf (accessed on 15 March 2009).
Department of Education. 2011. National Curriculum Statements (NCS) Grades R–12. Available at:
http://www.education.gov.za/Curriculum/CurriculumAssessmentPolicyStatements/tabid/419/Default.
aspx
Department of Health. 1997. White Paper for the transformation of the health system in South Africa.
Government Gazette, 382, no. 17910. Pretoria: Government Printer.
Department of Higher Education and Training. 2011. National Skills Development Strategy III.
Available at: http://www.dhet.gov.za/Booklets/NSDS%20III%20Progress%20Report%20%207%20October%202013%20-%20V11.pdf
Department of Women, Children and People with Disabilities. 2013. South Africa Baseline Country
Report. UN Convention on the Rights of Persons with Disabilities.
Doerries, D. 2004. KIDTAP: a strengths-based approach to curriculum-based assessment. Training
and Technical Assistance Centre, William and Mary School of Education. Available at:
https://education.wm.edu/centers/ttac/index.php
http://www.naptosa.org.za/users/specialEd_detail.php?pubID=322 (accessed on 15 March 2009).
Donohue, D.K. & Bornman, J. 2014. The challenges of realising inclusive education in South Africa.
SA Journal of Education, 34(2): 1–13.
Donohue, D.K. & Bornman, J. 2015. South African teachers’ attitudes towards the inclusion of
learners with different abilities in mainstream classes. International Journal of Disability,
Development and Inclusion, 62(1): 42–95.
Ebersöhn, L. & Eloff, I. 2006. Life skills & assets, 2nd ed. Pretoria: Van Schaik.
Heap, M., Lorenzo, T. & Thomas, J. 2009. “We’ve moved away from disability as a health issue, it’s
a human rights issue”: reflecting on 10 years of the right to equality in South Africa. Disability &
Society, 24(7): 857–868.
Forlin, C., Loreman, T., Sharma, U. & Earle, C. 2009. Demographic differences in changing preservice’ teachers’ attitudes, sentiments and concerns about inclusive education. International Journal
of Inclusive Education, 13: 195–209.
Gravois, T. & Gickling, E. 2002. Best practices in curriculum-based assessment. In Thomas, A. &
Grimes, J. (Eds). Best practices in school psychology. Washington, DC: National Association of
School Psychologists.
Hartley, S., Nganwa, A. & Kisanji, J. 2002. Professionals’ participation in CBR programmes. In
Hartley, S. (Ed.). CBR: a participatory strategy in Africa. London: Centre for International Child
Health.
Howell, C. & Lazarus, S. 2008. Education White Paper 6: a framework for change or limiting new
possibilities? In Muthukrishna, A. (Ed.). Educating for social justice and inclusion in an African
context: pathways and transitions. Hauppauge, NY: Nova Science.
Howie, S., Venter, E., Van Staden, S., Zimmerman, L., Long, C., Du Toit, C., Scherman, V. & Archer,
E. 2008. PIRLS 2006 Summary report: South African children’s reading literacy achievement.
Pretoria: Centre for Evaluation and Assessment. Available at
https://web.up.ac.za/sitefiles/file/43/314/SA%20PIRLS%202006%20SUMMARY%20REPORT.pdf.
Accessed 14 September 2016.
Idol, L. 2002. Creating collaborative and inclusive schools. Austin, TX: Pro-Ed.
Integrated National Disability Strategy (INDS). 1997. White Paper. Available at:
http://www.info.gov.za/whitepapers/1997/disability.htm (accessed on 9 February 2009).
Jansen, J. 2009. Call me teacher. SAALED News, 29(1): 4.
Kleinert, H.L., Jones, MM., Sheppard-Jones, K., Harp, B. & Harrison, E.M. 2012. Students with
intellectual disabilities going to college? Absolutely! Teaching Exceptional Children, 44(5): 26–35.
Kreps, G.L. 2000. Disability and culture: effects on multicultural relations in modern organisations.
In Braithwaite, D.O. & Thompson, T.L. (Eds). Handbook of communication and people with
disabilities. Mahwah, NJ: Lawrence Erlbaum.
Magubane, K. 2016. The exodus of teachers from SA is not slowing down. Business Day Live.
Available at: http://www.bdlive.co.za/national/education/2016/03/23/the-exodus-of-teachers-from-sais-not-slowing-down (accessed on 3 April 2016).
Martin, P. 2014. Children’s right to basic education: a review of South Africa’s laws and policies. In
Proudlock, P. (Ed.). South Africa’s progress in realising children’s rights: a law review. Cape Town:
Children’s Institute, University of Cape Town & Save the Children South Africa.
McConkey, R. & Alant, E. 2005. Promoting leadership and advocacy. In Alant, E. & Lloyd, L.L.
(Eds). Augmentative and alternative communication: beyond poverty. London: Whurr.
Miller, P.W., Ochs, K. & Mulvaney, G. 2008. International teacher migration and the Commonwealth
Teacher Recruitment Protocol: assessing its impact and the implementation process in the United
Kingdom. European Education, 40(3): 89–101.
National Department of Education. 2001. Education White Paper 6. Special needs education:
building an inclusive education and training system. Pretoria: National Department of Education.
National Programme of Action (NPA). 1999. National programme of action for children in South
Africa: 2000 and beyond. Pretoria, South Africa: The Presidency.
Nel, M. 2015. Understanding classroom assessment within an inclusive framework. In Dunbar-Krige,
H. (Ed). Guidelines for assessment adaptation. Pretoria: Van Schaik.
Nelson Mandela Foundation. 2005. Emerging voices: a report on education in South African rural
communities. Pretoria: HSRC Press.
Nompula, Y. 2012. An investigation of strategies for integrated learning experiences and instruction
in the teaching of creative art subjects. South African Journal of Education, 32(3): 293–306.
Oswald, M. & Swart, E 2011. Addressing South African pre-service teachers’ sentiments, attitudes
and concerns regarding inclusive education. International Journal of Disability, Development and
Education, 58(4): 389–403. doi:10.1080/1034912X.2011.626665
Pather, S. 2008. Demystifying the notion of “inclusion” in the context of a rural school and its
communities in South Africa. In Muthukrishna, A. (Ed.). Educating for social justice and inclusion
in an African Context: pathways and transitions. Hauppauge, NY: Nova Science.
Pinnock, H. 2008. Mother-tongue-based multilingual education: how can we move ahead? Available
at:
http://www.seameo.org/_ld2008/doucments/Presentation_document/Helen_Pinnock_mle_how_do_w
e_move_ahead.pdf (accessed on 19 March 2009).
Pitso, R. & Magubane, K. 2014. South Africa failing the disabled. Business Day Live. Available at:
http://www.bdlive.co.za/national/2014/06/12/south-africa-failing-the-disabled (accessed on 4 April
2016).
Quintal, G. 2016. Matric results 2015: Pass rate drops to 70.7%. Mail and Guardian. Available at
http://mg.co.za/article/2016-01-05-matric-pass-rate-drops-to-707 (accessed on 15 September 2016).
Schwarz, P. 2006. From disability to possibility: the power of inclusive classrooms. Portsmouth, NH:
Heinemann.
Shonkoff, J.P. & Garner, A.S. 2012. The lifelong effects of early childhood adversity and toxic stress.
2012. Paediatrics, 129(1): e232–246. doi:10.1542/peds.2011-2663
Snell, M.E. & Brown, F. 2011. Instruction of students with severe disabilities, 7th ed. Upper Saddle
River, NJ: Pearson.
South Africa. 2012. National Development Plan 2030 (NDP). Pretoria: Government Printer.
South Africa. 2015. National Integrated Early Childhood Development Policy. Pretoria: Government
Printer.
Statistics South Africa. 2014. Census 2011. Profile of persons with disability in South Africa. Report
no. 03-01-59. Pretoria: Government Printer. Available at:
http://www.statssa.gov.za/publications/Report-03-01-59/Report-03-01-592011.pdf
UNICEF. 2005. National integrated plan for early childhood development in South Africa 2005–
2010. Available at: http://www.unicef.org/southafrica/SAF_resources_nip.pdf (accessed on 16 March
2009).
Von Tetzchner, S., Brekke, K.M., Sjøthun, B. & Grindheim, E. 2005. Constructing pre-school
communities of learners that afford alternative language development. Augmentative and Alternative
Communication, 21(2): 82–100.
Walton, E. 2011. Getting inclusion right in South Africa. Intervention in School and Clinic, 46: 240.
Available at: http://www.sagepublications.com
Walton, E. & Lloyd, G. 2011. An analysis of metaphors used for inclusive education in South Africa.
Acta Academica, 43(3). Available at: http://www.ufs.ac.za/ActaAcademica
Wilce, H. 2006. Special-needs education: does mainstream inclusion work? The Independent.
Available at: http://www.independent.co.uk/news/education/education-news/specialneeds-educationdoes-mainstream-inclusion-work-470960.html (accessed on 19 March 2009).
Zimmerman, L. & Smit, B. 2014. Profiling classroom reading comprehension development practices
from the PIRLS 2006 in South Africa. South African Journal of Education, 34(3), 1–9.
USEFUL CONTACTS
This is not an exhaustive list. It is intended to act as a contact point with the specific
organisations.
ACCESSIBILITY
Assistive devices: products and information
http://www.mobilityone.co.za/
Boksburg
Tel: 082 558 4640
National Accessibility Portal
www.meraka.org.za/nap.htm/
CSIR, Pretoria
Tel: 012 841 2000
ADHD
Attention Deficit and Hyperactivity Support Group of Southern Africa
http://www.adhasa.co.za/
Delta Park School, Blairgowrie, Randburg
Tel: 011 888 7655
Attention Deficit Disorder Resources
http://addresources.net/
Seattle, Washington State, United States
AUGMENTATIVE AND ALTERNATIVE COMMUNICATION
Centre for Augmentative and Alternative Communication
http://www.caac.up.ac.za/
Pretoria, South Africa
Tel: 012 420 2001
Edit microsystems
http://editmicro.co.za/
Sea Point, Cape Town (National head office)
Tel: 086 111 3973
Inclusive Solutions
http://www.inclusivesolutions.co.za
Bedfordview, Johannesburg
Tel: 086 888 121
Interface KZN
http://www.interface-kzn.co.za/
Pinetown, Durban
Tel: 031 708 4237
International Society for Augmentative and Alternative Communication (ISAAC)
http://www.isaac-online.org/
Toronto, Canada
AUTISM
Autism Research Institute (ARI)
http://www.autism.com/
San Diego, California, United States
Autism South Africa (ASA)
http://www.autismsouthafrica.org/
Johannesburg
Tel: 011 484 9909
BLINDNESS
National Federation of the Blind
http://www.nfb.org/
Baltimore, Maryland, USA
National Institute for the Blind
http://www.kaleidoscopesa.org/
Worcester
Tel: 023 347 274
South African National Council for the Blind
http://www.sancb.org.za/
Muckleneuk, Pretoria
Tel: 012 452 3811
CEREBRAL PALSY
National Association for Persons with Cerebral Palsy
http://www.napcp.org.za/
Edenvale
Tel: 011 609 3252
DEAFNESS
Deafblind South Africa
http://www.deafblindsa.co.za/
Worcester
Tel: 023 342 5555/6
Deaf.com
http://www.deaf.com/
New York, United States
Deaf Federation of South Africa
http://www.deafsa.co.za/
Westhoven, South Africa
Tel: 011 482 1610
National Institute for the Deaf
http://www.deafnet.co.za/
Worcester
Tel: 023 342 5555
DISABILITY ORGANISATIONS
Association for Persons with Disabilities: Western Cape
http://www.wcapd.org.za/
Milnerton, Cape Town
Tel: 021 555 2881
Centre for Disability and Health Policy
http://www.westernu.edu/
Pomona, California, United States
Disability Lifestyle Magazine
http://www.rollinginspiration.co.za/
Northcliff, Johannesburg
Tel: 011 782 1070
Disability Rights Education and Defense Fund (DREDF)
http://www.dredf.org/
Main office: California, United States
Government affairs: Washington, DC, United States
Disability Solutions
http://www.disabilitysolutions.co.za/
Western Cape & Gauteng
Tel: 021 872 1101
Disabled Children’s Action Group (DICAG)
http//www.dicag.co.za/
Wynberg, Cape Town
Tel: 021 797 5977
Disabled Peoples’ International
http://www.dpi.org/
Mount Pearl, Newfoundland, United States
Disabled People South Africa (DPSA)
http://www.dpsa.org.za/
Cape Town
Tel: 021 422 0357
SADA: South African Disability Alliance
https://www.facebook.com/SADA-South-African-Disability-Alliance-1400539236884527/
DOWN SYNDROME
Down Syndrome South Africa
http://www.downsyndrome.org.za/
Bedfordview
Tel: 0861 DOWNSA (0861 369672)
Tel: 011 615 9401
Down Syndrome International (DSI)
http://www.ds-int.org/
Middlesex, United Kingdom
DYSCALCULIA
Dyscalculia.org – Math Learning Disability Resource
http://www.dyscalculia.org/
Dearborn, Michigan, United States
DYSLEXIA
The International Dyslexia Association
http://www.interdys.org/
Baltimore, Maryland, United States
EARLY CHILDHOOD DEVELOPMENT
http://www.ecdtraining.co.za/
Groenkloof, Pretoria
Tel: 012 460 2617
Cotlands
http://www.cotlands.org.za/
Turffontein (Head office)
Tel: 011 683 7201
HiHopes
http://www.hihopes.co.za/
Johannesburg (Head office)
Tel: 011 717 3750
Ntataise
http://www.ntataise.co.za/
Viljoenskroon
Tel: 056 343 0034
Pebbles
http://www.pebblesproject.co.za/contact-us/
Koelenhof, Stellenbosch
Tel: 021 865 1018
Save the Children South Africa
http://www.savethechildren.org.za/
Hatfield, Pretoria
Tel: 012 430 7775
Training and Resources in Early Education (TREE)
http://www.tree-ecd.co.za/
Durban
Tel: 031 579 4711
EPILEPSY
Epilepsy.com
http://www.epilepsy.com/
Landover, Maryland, United States
Epilepsy South Africa
http://www.epilepsy.org.za/home/
Observatory, Cape Town
Tel: 021 595 4900
FOETAL ALCOHOL SYNDROME
Fetal Alcohol Disorders Society Research, Information, Research, Support and
Communications
http://www.faslink.org/index.htm/
Ontario, Canada
Foetal Alcohol Syndrome Facts
http://www.fasfacts.org.za/
Worcester, Western Cape
Tel: 023 342 7000
National Organization on Fetal Alcohol Syndrome
http://www.nofas.org/
Washington, DC, United States
FRAGILE X SYNDROME
Fragile X Research Foundation
http://www.fraxa.org/
Newburyport, Massachusetts, United States
The National Fragile X Foundation
http://www.fragilex.org/html/home.shtml/
Washington, DC, United States
HIV/AIDS
AIDS Foundation South Africa
http://www.aids.org.za/hiv.htm/
Durban
Tel: 031 277 2701
International HIV/AIDS Alliance
http://www.aidsalliance.org/sw1280.asp/
Hove, United Kingdom
The Body – The Complete HIV/AIDS Resource
http://www.thebody.com/
New York, United States
INCLUSION
Inclusive Education South Africa
http://www.included.org.za/
Wynberg, Cape Town
Tel: 021 762 6664
INTELLECTUAL AND DEVELOPMENTAL DISABILITY
American Association on Intellectual and Developmental Disabilities (AAIDD)
http://www.aamr.org/
Washington, DC, United States
LEARNING AND EDUCATIONAL DIFFICULTIES
Learning Disabilities Association of America
http://www.ldanatl.org/
Pittsburgh, Pennsylvania, United States
The National Center for Learning Disabilities
http://www.ncld.org/
New York, United States
The Southern African Association for Learning and Educational Difficulties (SAALED)
http://www.saaled.org.za/
Johannesburg
Tel: 011 648 5779
PARENT ORGANISATIONS
DICAG
http://www.dicag.co.za/
Wynberg, Cape Town
Tel: 021 797 5977
PACSEN
E-mail: pacsengauteng@absamail.co.za
Pretoria
Tel: 012 333 0149
PHYSICAL DISABILITY
APD: Association for Physical Disability
http://www.apd.org.za/contacts-us/
Johannesburg
Tel: 011 646 8331/2/3/4
National Council for Persons with Physical Disabilities
http://www.ncppdsa.org.za/
Edenvale
Tel: 011 452 2774
QUADPARA Association of South Africa
http://www.qasa.co.za/
Durban
Tel: 031 767 0348
SPINAL CORD
South African Spinal Cord Association
http://www.sasca.org.za/
Monument Park, Pretoria
South African Spine Society
http://www.saspine.org/
Constantia, Cape Town
Tel: 021 404 5387
TUBERCULOSIS
South African National Tuberculosis Foundation
http://www.santa.org.za/
Edenvale
Tel: 011 454 0260
Stop TB Partnership
http://www.stoptb.org/
Geneva, Switzerland
INDEX
A
access 299
accommodation 54
environmental accommodation 57
marking and progress reporting accommodation 57
presentational accommodation 56
response accommodation 56
setting accommodation 56
timing and scheduling accommodation 56
Acts
Bill of Rights 28
Children’s Act 38 of 2005 114
Curriculum and Assessment Policy Statement (CAPS) 43
Education White Paper 6 5
Employment Equity Act 29
National Curriculum Framework (2012) for children from birth to four 115
National Development Plan (2030) 114
National Integrated Early Childhood Development Policy (2015) 115
National Protocol for Assessment Grades R–12 43
Norms and Standards for Educators 12
Policy on Screening, Identification, Assessment and Support (SIAS) 7
South African Constitution 23, 28, 113
South African Schools Act 28, 114
United Nations Sustainable Development Goals (2015) 115
White Paper 5 on Early Childhood Education 114
White Paper 6 Inclusive Education 114
White Paper on an Integrated National Disability Strategy (INDS) 29
White Paper on the Rights of Persons with Disabilities 29
aided communication 253
aided language stimulation 96
Angelman syndrome 248
assessment 44
accommodation 54
alternative assessment approach 53
alternative assessment opportunity 300
alternative form 99
assessment model 46
assessment procedure 188
curriculum modification 48
curriculum-based assessment (CBA) 47
formal assessment 45
formats and achievement standards 49
informal assessment 45
personal mapping 49
purpose 45
asset-based approach 10
assistive device 8
assistive technology 210
asthma 267
characteristics 268
classroom management 268
cure 268
definition 267
attention deficit hyperactivity disorder 170
characteristics 172
definition 170
strengths 172
attitude 9
augmentative and alternative communication 165
autism spectrum disorder (ASD) 245
cause 248
definition 245
severity 247
B
barrier 6
access barrier 6
opportunity 6
barriers to learning 33
attitudinal barriers 34
environmental (extrinsic) barrier 33
knowledge and skills barrier 34
personal (intrinsic) barrier 33, 36
physical barrier 36
policy barrier 33
practice barrier 33
belonging 298
bio-ecological model 9
chronosystem 9
exosystem 9
macrosystem 9
mesosystem 9
microsystem 9
C
cerebral palsy 197
ataxic cerebral palsy 198
cause 197
challenge 200
characteristics 198
cure 198
definition 197
diplegia 199
dyskinetic cerebral palsy 198
hemiplegia 199
quadriplegia 199
spastic cerebral palsy 198
type 198
challenging behaviour 127
A-B-C chart 132
adaptive coping 138
assessment 130, 136
attention-seeking-motivated behaviour 134
contingency map 142
crisis management 145
definition 129
description 131
escape-motivated behaviour 134
form 129
function 134, 144
managing 136
positive behaviour support 136
prevention practice 140
principle 130
problem behaviour 127
self-management 139
sensory feedback-motivated behviour 135
setting event 132
stimulus event 134
tangible consequence-motivated behaviour 135
visual schedule 142
vulnerability 129
childhood cancer 269
characteristics 269
classroom management 270
cure 269
definition 269
classroom 63
classroom ethos 63, 204
rules 66
strategy 69
classroom accommodation 185
classroom assistant 214
classroom management 234, 239
classroom strategy 249
COACH 49
cochlear implant 225
collaboration 301
Convention on the Rights of the Child 43
co-teaching 8
alternative teaching 8
one teach, one assist 8
parallel teaching 8
station teaching 8
team teaching 8
curriculum 28
D
deaf education 221
deafblindness 237
decision-making 66
diabetes mellitus 275
characteristics 275
classroom management 276
cure 276
definition 275
differentiated learning 8
differentiated teaching 7, 85
compacting 90
complex instruction 89
content 85
cubing 91
process 93
product 99
district-based support teams (DBST) 7, 25
diversity 6, 297, 301
Down syndrome 152
dual sensory impairment 237
cause 238
characteristics 239
definition 238
dyscalculia 177
characteristics 178
primary dyscalculia 177
secondary dyscalculia 177
strengths 179
dysgraphia 179
cause 179
characteristics 179
strengths 180
dyslexia 172
cause 173
characteristics 175
definition 173
strengths 177
dyspraxia 180
cause 181
characteristics 181
cognitive organisers 183
learning skills 182
management 181
reciprocal teaching 182
strengths 181
taking notes 184
E
early childhood development (ECD) 110
core concept 111
definition 113
ECD practitioner 113
participation 116
role and responsibility 115
transition 112
early childhood education (ECE) 111
ecosystemic perspective 9
empowerment 301
environment 9
epilepsy 272
characteristics 272
classroom management 274
cure 273
definition 272
F
facilitator 214
first aid training 287
foetal alcohol spectrum disorder (FASD) 154
fragile X syndrome 153, 248
functional communication 241
G
group
collaborative 93
pair 93
performance-based 93
small group 92
group work 92
H
hearing impairment 218
auditory processing problems (central) 220
bilingual language learning 225
cause 220
characteristics 220
classroom strategy 225
cochlear implant 225
conductive hearing loss 218
definition 218
degree 218
FM system 225
hearing aid 223
mixed hearing loss 220
sensory neural hearing loss 220
strengths 221
heart defect 277
characteristics 278
classroom management 278
definition 277
high technology 211
HIV/AIDS 279
characteristics 279
classroom management 280
cure 280
definition 279
homework 100, 185
I
inclusion 5, 9
attitude 30
environment 32
knowledge 31
policy 28
practices 29
skills 31
independence 234
individual support plan (ISP) 27, 47
institution-level support team (ILST) 25
intellectual disability 149
accommodation strategy 158
adaptation 160
collaborative learning 159
definition 149
features 150
stereotyping 152
strategy 161
teaching approach 157
terminology 149
intelligence 64
bodily-kinaesthetic 65
interpersonal 65
intrapersonal 65
logical-mathematical 64
musical 65
naturalistic 65
verbal-linguistic 64
visual-spatial 65
International Classification of Functioning, Disability and Health – Children and Youth (ICF-CY) 25
L
labelling 24
learned helplessness 200
learning disability 169
cause 171
classroom accommodation 185
type 169
literacy 211
low technology 211
M
malaria 282
characteristics 283
classroom management 283
cure 283
definition 282
malnutrition 284, 285
characteristics 285
classroom management 285
cure 285
definition 284
MAPS 49
medical condition 267
chronic 267
multiskilling 12
muscular dystrophy 203
cause 203
challenges 204
characteristics 203
cure 203
definition 203
N
narrative approach 8
non-governmental organisation (NGO) 9
P
parent 14
advocate 15
belief 15
communication 15
culture 16
dream 16
guideline 16
opportunity 15
responsibility 17
role 14
support 15
support group 17
participation 6, 22
activity limitation 195
facilitate 28
participation and learning model (PLM) 26
Participation Model 6
participation restriction 195
partnership 301
peer 213
peer support 227
physical disability 196
accommodation 209
adaptive equipment 206
fine motor skills 196
gross motor skills 196
lifting 208
normal development 196
Picture Exchange Communication System (PECS) 254
play 212
positioning 205
positive behaviour support 301
Prader-Willi syndrome 248
problem solving 186
proprioception 217
R
reading comprehension 186
resilience 118
Rett syndrome 248
S
scaffolding 93
school governing body (SGB) 9
seating 205
self-discipline 67
sensory integration 217
proprioception system 217
vestibular system 217
sensory integration therapy (SIT) 255
sensory system
auditory system 217
gustatory system 217
olfactory system 217
tactile system 217
visual system 217
sign language 222
social competence 258
social transformation 299
spina bifida 201
cause 201
challenges 202
characteristics 202
cure 201
definition 201
strengths 297
strengths-based approach 301
stress 119
manageable stress 119
tolerable stress 119
toxic stress 119
T
teacher 12
administrator 12
administrator role 14
assessor 12
collaborative role 13
designer 12
leader 12
leadership role 14
learning mediator 12
lifelong learner 12
lifelong learner role 14
manager 12
pastoral role 13
pastoral role player 12
researcher 12
researcher role 14
responsibility 306
role model 68
scholar 12
scholar role 14
school manager role 14
specialist 12
turn-around teacher 12
TEACCH 255
teaching strategy 70
academic engagement 70
managing time 71
presentation 72
self-reflection 80
unhelpful strategy 82
team
approach 25
challenge 25
collaborative teaming 25
district-based support teams (DBST) 25
function 7
institution-level support team (ILST) 25
role 7
total communication 223
transition 306
tuberculosis 286
characteristics 286
classroom management 287
cure 286
definition 286
tuberous sclerosis 248
U
unaided communication 252
V
visual impairment 230
Braille 235
cause 231
characteristics 231
definition 230
light sensitivity 233
strengths 234
visual acuity 232
visual field 232
visual motility 232
visual perception 233
visual stability 233
visual schedule 250
Z
zoom lens
close-up lens 14
regular lens 11
wide-angle lens 10
zoom lens metaphor 10