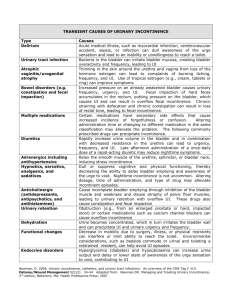
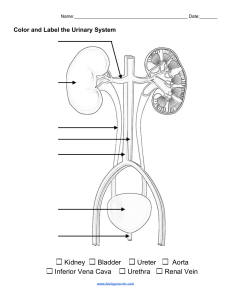
Urinary incontinence Dr. Mohammed Bassil OBJECTIVES 1. Identify and name the major anatomic and histologic features of the bladder and urethra in the male and female 2. Define incontinence 3. List the symptoms and signs of the various types of incontinence; stress, urge, overflow and mixed 4. Describe the epidemiological features of incontinence 5. Describe the natural history and progression of incontinence 6. List the risk factors for incontinence 7. List the important components of the history when interviewing a patient with incontinence 8. List the important components of the physical exam of a patient with incontinence 9. Summarize the laboratory, radiologic, or urodynamic tests, if any, that should be ordered in a patient with incontinence 10. List the indications for treatment of incontinence 11. List the nonsurgical treatment options for stress and urge incontinence, describe their side effects, and outline the mechanisms by which they work. 12. Briefly describe the surgical treatment options for stress and urge incontinence Definition Involuntary loss of urine that is a social or hygienic problem and is objectively demonstrable.” Urinary incontinence (UI) is a failure to store urine usually due to either abnormal bladder smooth muscle or a deficient urethral sphincter. Urine loss may also be extraurethral, secondary to anatomical abnormalities such as ectopic ureter or vesicovaginal fistula. Prevalence UI has been reported to affect 12–43% of adult women and 3–11% of adult men. Severe incontinence has a low prevalence in young women, but rapidly increases at ages 70 through 80. Incontinence in men also increases with age, but severe incontinence in 70- to 80-year-old men is about half that in women. Classification Stress urinary incontinence (SUI) :is involuntary urinary leakage during effort, exertion, sneezing, or coughing, due to hypermobility of the bladder base, pelvic floor,and/or intrinsic urethral sphincter deficiencies. In females SUI is usually associated with multiparity. In males, SUI is most commonly the result of prostatectomy Classification Urgency urinary incontinence (UUI):is involuntary urine leakage accompanied or immediately preceded by a sudden, strong desire to void (urgency). Mixed urinary incontinence:is urine leakage that has characteristics of both SUI and UUI. Overflow incontinence :is leakage of urine when the bladder is abnormally distended with large post-void residual volumes. Typically, men present with chronic urinary retention and dribbling incontinence. This can lead to hydronephrosis and renal failure in 30% of patients. Classification Nocturnal enuresis:describes any involuntary loss of urine during sleep. The prevalence in adults is 0.5%. Approximately 750,000 children over age 7 years will regularly wet the bed. Childhood enuresis can be further classified into primary (never been dry for longer than a 6-month period) or secondary (re-emergence of bed wetting after a period of being dry for at least 6–12 months). Risk factors Predisposing factors • Gender (female > males) • Race (Caucasian > African American/Asian) • Genetic predisposition • Neurological disorders (spinal cord injury, stroke, MS, Parkinson disease) • Anatomical disorders (vesicovaginal fistula, ectopic ureter, urethral diverticulum) • Childbirth • Anomalies in collagen subtype • Prostate or pelvic surgery (radical prostatectomy; radical hysterectomy; TURP) leading to pelvic muscle and nerve injury • Pelvic radiotherapy Risk factors Promoting factors • Smoking (associated with chronic cough and raised intraabdominal pressure) • Obesity • UTI • Increased fluid intake • Medications • Poor nutrition • Aging • Cognitive deficits • Poor mobility Pathophysiology Bladder abnormalities Detrusor overactivity is a urodynamic observation characterized by involuntary bladder muscle (detrusor) contractions during the filling phase of the bladder, which may be spontaneous or provoked, and can consequently cause urinary incontinence. The underlying cause may be neurogenic, where there is a relevant neurological condition, or idiopathic, where there is no defined cause Pathophysiology Low bladder compliance is characterized by a decreased volume-topressure relationship during a cystometrogram and is often associated with upper tract damage. High bladder pressures occur during filling because of alterations in the viscoelastic properties of the bladder wall, or changes in bladder muscle tone (secondary to myelodysplasia, spinal cord injury, radical hysterectomy, interstitial or radiation cystitis). Pathophysiology Sphincter abnormalities Urethral hypermobility is due to a weakness of pelvic floor support causing a rotational descent of the bladder neck and proximal urethra during increases in intra-abdominal pressure. If the urethra opens concomitantly, there will be urinary leaking. Intrinsic sphincter deficiency (ISD) describes an intrinsic malfunction of the sphincter, regardless of its anatomical position, which is responsible for type III SUI. Causes include inadequate urethral compression (previous urethral surgery; aging; menopause; radical pelvic surgery) or deficient urethral support (pelvic floor weakness; childbirth; pelvic surgery ; menopause). Evaluation History Inquire about LUTS (storage or voiding symptoms), triggers for incontinence (cough, sneezing, exercise, position, urgency), and frequency and severity of symptoms. Establish risk factors (abdominal/pelvic surgery; neurological diseases; obstetric and gynecological history; medications). A validated patient-completed questionnaire may be helpful Evaluation Physical examination Women Perform a pelvic examination in the supine and standing position with a speculum while the patient has a full bladder. Ask the patient to cough or strain, and inspect for vaginal wall prolapse (cystocele, rectocele, enterocele),uterine or perineal descent, and urinary leakage (stress test). Eighty percent of SUI patients will leak with a brief squirt during cough in the supine position, while another 20% will leak only in an inclined or standing position. Urethral hypermobility is assessed with the Q-tip test. A lubricated cottontipped applicator is introduced through the urethra to bladder neck level. Hypermobility is defined as a resting or straining angle of >30* from horizontal. The Bonney test is used to assess continence with manual repositioning of the urethra and vesicle neck. Using one or two fingers to elevate the anterior vaginal wall laterally without compressing the urethra, relief of incontinence during cough suggests that surgical correction will be successful. Evaluation Both sexes Examine the abdomen for a palpable bladder (indicating urinary retention). A neurological examination should include assessment of anal tone and reflex, perineal sensation, and lower limb function. Inspect the underwear for the status of urinary collection pads; for men, a standing or squatting “cough test” gives a good indicator of the presence and severity of stress incontinence. Investigation Bladder diaries Record the frequency and volume of urine voided, incontinent episodes, pad usage, fluid intake, and degree of urgency. Alternatively, pads can be weighed to estimate urine loss (pad testing). Urinalysis can exclude UTIs. Blood tests, X-ray imaging, cystoscopy These are indicated for persistent or severe symptoms, bladder pain, and voiding difficulties. Cystoscopy is useful for evaluating men who have had prostatectomy—it will show the presence of clips, stones, and strictures that may develop after surgery that might need to be addressed concomitantly with anti-incontinence surgery Investigation Urodynamic investigations Valsalva leak point pressure (VLPP) measures the abdominal pressure at which a half-full bladder leaks during straining—normal individuals should not leak. VLPP readings <60 cm H2O suggest ISD; VLPP readings >100 cm H2O suggest hypermobility, while readings of 60– 100 cm are indeterminant. Detrusor leak point pressure (DLPP) measures the bladder pressure at which leakage occurs without valsalva—DLPP >40 cm H2O puts the upper tract at risk. Videourodynamics can visualize movement of the proximal urethra and bladder neck, and establish the precise anatomical etiology of UI. Investigation urodynamics Uroflowmetry testing measures the ability of the bladder to empty; a minimum bladder volume of 150 cc is desired. A low flow rate indicates bladder outflow obstruction or reduced bladder contractility. The volume of urine remaining in the bladder after voiding (post-void residual) is also important(<50 mL is normal; >200 mL is abnormal; 50–200 mL requires clinical correlation). Investigation Sphincter electromyography (EMG) EMG measures electrical activity from striated muscles of the urethra or perineal floor and provides information on synchronization between bladder muscle (detrusor) and external sphincter. Treatment Treatment for urinary incontinence depends on the type of incontinence, its severity and the underlying cause. A combination of treatments may be needed. Behavioral techniques Bladder training, to delay urination after you get the urge to go. You may start by trying to hold off for 10 minutes every time you feel an urge to urinate. The goal is to lengthen the time between trips to the toilet until you're urinating only every two to four hours. Double voiding, to help you learn to empty your bladder more completely to avoid overflow incontinence. Double voiding means urinating, then waiting a few minutes and trying again. Treatment Time voiding, to urinate every two to four hours rather than waiting for the need to go. Fluid and diet management, to regain control of your bladder. You may need to cut back on or avoid alcohol, caffeine or acidic foods. Reducing liquid consumption, losing weight or increasing physical activity also can ease the problem. Pelvic floor muscle exercises It is recommend that you do these exercises frequently to strengthen the muscles that help control urination. Also known as Kegel exercises, these techniques are especially effective for stress incontinence but may also help urge incontinence. Treatment Medications Anticholinergics. These medications can calm an overactive bladder and may be helpful for urge incontinence. Mirabegron . Used to treat urge incontinence, this medication relaxes the bladder muscle and can increase the amount of urine your bladder can hold. It may also increase the amount you are able to urinate at one time, helping to empty your bladder more completely. Alpha blockers. In men with urge or overflow incontinence due to BPE , these medications relax bladder neck muscles and muscle fibers in the prostate Topical estrogen. Treatment Interventional therapies •Bulking material injections. A synthetic material is injected into tissue surrounding the urethra. •Botulinum toxin type A (Botox). Injections of Botox into the bladder muscle may benefit people who have an overactive bladder. Botox is generally prescribed to people only if other first line medications haven't been successful. •Nerve stimulators. A device resembling a pacemaker is implanted under your skin to deliver painless electrical pulses to the nerves involved in bladder control (sacral nerves). Stimulating the sacral nerves can control urge incontinence if other therapies haven't worked. The device may be implanted under the skin in your buttock and connected directly to the sacral nerves or may deliver pulses to the sacral nerve via a nerve in the ankle. Treatment Treatment of sphincter weakness incontinence: injection therapy The injection of bulking materials into the bladder neck and periurethral muscles is used to increase outlet resistance. Indications These include stress incontinence secondary to demonstrable intrinsic sphincter deficiency (ISD), with normal bladder muscle function. Injection therapy is used in adults and children. Treatment Treatment of sphincter weakness incontinence: retropubic suspension Retropubic suspension procedures are used to treat female stress incontinence caused by urethral hypermobility. The aim of surgery is to elevate and fix the bladder neck and proximal urethra in a retropubic position, to support the bladder neck, and to regain continence. It is contraindicated in the presence of significant intrinsic sphincter deficiency (ISD). Treatment Marshall–Marchetti–Krantz (MMK) procedure Sutures are placed either side of the urethra around the level of the bladder neck and then tied to the hyaline cartilage of the pubic symphysis. Burch colposuspension This requires good vaginal mobility, to allow the vaginal wall to be elevated and attached to the lateral pelvic wall where the formation of adhesions over time secures its position. The paravaginal fascia is exposed and approximated to the iliopectineal (Cooper) ligament of the superior pubic rami. Vagino-obturator shelf/paravaginal repair Sutures are placed by the vaginal wall and paravaginal fascia and then passed through the obturator fascia to attach to part of the parietal pelvic fascia below the tendinous arch (arcus tendoneus fascia). Cure rates are up to 85%. Treatment Treatment of sphincter weakness incontinence: pubovaginal slings Indications Sling procedures were developed mainly for female stress incontinence associated with poor urethral function (type III or ISD) or when previous surgical procedures have failed. The success of sling procedures, however, has resulted in expanded applications in women with hypermobility. Types of sling • Autologous—rectus fascia, fascia lata (from the thigh), vaginal wall slings • Nonautologous—allograft fascia lata from donated cadaveric tissue • Synthetic—monofilament “macropore” polypropylene mesh (via transobturator, transabdominal, or transvaginal needles) Treatment of sphincter weakness incontinence the artificial urinary sphincter Indications include incontinence secondary to urethral sphincter deficiency in patients with normal bladder capacity and compliance. In men, it is used almost always for sphincter damage due to prostatectomy (radical prostatectomy for prostate cancer or TURP). In women it can be used for neuropathic sphincter weakness (e.g., spinal cord injury, spina bifida) if the incontinence is not due to bladder overactivity. causes of transient incontinence 1) 2) 3) 4) 5) 6) 7) Drug side effects Delirium or hypoxia Impaired mobility Urinary tract infection Atrophic vaginitis psychological problems Excessive fluid intake REFERENCES 1-Oxford Handbook of Urology • 2-Smith’s General Urology • 3-CAMPBELL-WALSH Urology • THE END THANK YOU QUIZZZZZ TRUE OR FALSE (Genuine stress incontinence)? A. The bladder neck and proximal urethra is poorly supported by musculofascial ligamentous structures B. which is responsible for type III SUI. C. Pubovaginal sling procedure is the method of choice for correction of this condition D. A large proportion will resolve on its own E. It is relatively uncommon TRUE OR FALSE • Promoting factors for incontinence a)Obesity b) UTI c)Increased fluid intake d) Childbirth e) Anomalies in collagen subtype