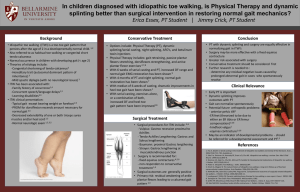
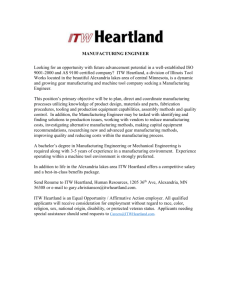
| Idiopathic Toe-Walking in Children and Adolescents Diagnosis, Natural History, and Treatment Options Abstract » Idiopathic toe-walking is a diagnosis of exclusion. Halle D. Freiman, MS, MD Curtis Mensah, MS » The natural history of idiopathic toe-walking has not been studied in many children; we identified only 1 prospective study. Of children without equinus contractures who were toe-walking before the age of 5.5 years, 59% had spontaneous resolution of toe-walking by 5.5 years of age, and 79%, by the age of 10 years. Jason Codrington, BS Steven L. Frick, MD Investigation performed at the Stanford University School of Medicine, Palo Alto, California » Adverse consequences of toe-walking into adulthood have not been reported, but may exist, and further research is needed to define and clarify. » If parents desire treatment to resolve their child’s toe-walking, surgical lengthening of the Achilles tendon is the treatment with the highest chance of success and lowest relapse rate, and thus far, no complications have been reported in any surgical series. I diopathic toe-walking (ITW) is an abnormal gait pattern whereby the child walks on the balls of their feet, skipping the heel strike during the initial stance phase that occurs in a normal gait. ITW can be associated with contracture of the Achilles tendon, resulting in limited range of motion of the ankle; however, many children with ITW have no contracture1,2. Toe-walking commonly presents in children ,2 years of age as they are developing walking abilities. Children who always walk on their toes and cannot ever get their heels to touch the floor when standing typically have Achilles tendon contracture and may have a condition referred to as hereditary Achilles tendon contracture3. The term congenital “short tendo calcaneus” was first associated with toe-walking by Hall et al. in 1967, and children with contractures should be distinguished from children with ITW, where substantial contractures are unusual4. The child’s gait pattern matures over the first COPYRIGHT © 2022 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED JBJS REVIEWS 2022;10(2) :e21.00193 few years of walking, with adult kinematics usually reached by the age of 3 years, and during this time, toe-walking may spontaneously resolve5. Persistent toe-walking after the age of 2 years can be an early identifier of an underlying neuromuscular etiology, and an evaluation to consider cerebral palsy or muscular dystrophy is warranted6. ITW is diagnosed when no underlying pathology can be identified for a patient who has initial contact on the forefoot, with little to no heel strike, and has no associated muscle weakness or decreased reflexes or sensation7. Furrer and Deonna analyzed “persistent toe-walking” in 28 children, and failure to explain this abnormal gait pattern with known disease processes was diagnosed as “habitual toewalking.”8 Today, the literature most commonly uses the term “idiopathic toe walking,” with continued questions about its etiology, natural history, and appropriate treatment9. Some studies report a higher incidence of ITW in children with autism Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSREV/A803). · http://dx.doi.org/10.2106/JBJS.RVW.21.00193 1 | I d i o p a t h i c To e - Wa l k i n g i n C h i l d r e n a n d A d o l e s c e n t s spectrum disorder, and thus far, the pathophysiology of this association is unexplained6,10. Normal Anatomy, Gait, and Ankle Range of Motion Most children diagnosed with ITW have completely normal anatomy, with a normal neurological examination and no muscle weakness or contractures. The important muscles to examine for contracture are the gastrocnemius and soleus. The distal fusion of these 2 muscles gives rise to the Achilles tendon and together form the triceps surae muscle-tendon complex that is responsible, primarily, for ankle plantar flexion and secondarily, knee extension when the foot is planted (ankle plantar flexionknee extension couple)1. Normal gait consists of a heel-toe pattern with 3 ankle motion rockers (or phases) present during the stance phase of the gait cycle. The first rocker is initiated with a heel strike and the ankle dorsiflexed, and is abnormal in children with ITW. Normal ankle range of motion for typically developing children during the gait cycle is reported to be from 25° of dorsiflexion to 15° to 20° of plantar flexion5. Stiffness or contractures that limit this range of motion can cause an abnormal gait. Etiology Normal walking is a coordinated function of the central nervous system (CNS), with unconscious neurological processes controlling multiple muscle contractions and relaxations across many joints, while also monitoring joint and body positions to maintain balance and forward momentum. It is best described as a “controlled fall,” with most muscles contracting eccentrically during normal walking11. When discussing toe-walking with concerned parents, the senior author tells parents that children “walk with their brains and spinal cord, not with their feet.” Explaining it this way can help parents understand that their child is not doing it consciously, and thus constant reminders for the child to put their feet on the floor during walking, and 2 instructions to “walk normal,” are not going to change the unconscious CNS abnormality. Why the CNS instructs some children to toe-walk is unknown; however, persistent toe-walking over time may result in limited ankle dorsiflexion2. There is also a potential genetic component to ITW; Pomarino et al. reported that 42% of 836 children with ITW had a family history of toewalking, with a possible autosomaldominant inheritance pattern, but further investigation is needed12. Diagnosis ITW is a diagnosis of exclusion, and therefore, several components of the patient history and physical examination are needed to rule out an underlying cause of toe-walking; in rare instances, further diagnostic studies (magnetic resonance imaging [MRI] of the CNS, nerve conduction tests, and computerized gait analysis) may also be needed. Patient History The history of a patient presenting with toe-walking should highlight the main concerns of the patient’s family, and whether the child has issues with pain, shoe-wear, running, tripping, keeping up with peers, and/or cosmetic concerns. Parents often have concerns about their child’s future function, possible pain, and potential impact on other joints. A detailed account of gestation, birth, and developmental milestones (both motor and communication skills) are key aspects of the history. Toewalking may be a sign of cerebral palsy, and it can also be an early sign of muscular dystrophy, where prompt diagnosis may allow for genetic analysis and family counseling and is thus important. An increased prevalence of toe-walking has been noted in autism spectrum disorder, and delayed motor and speech milestones may assist in making this diagnosis6,10. Family history should note any family member with a history of toe-walking and/or gait abnormalities or any neuromuscular conditions. Gait history should include the age at which the patient began to walk and include details about the onset of toe-walking and frequency (always, most of the time, occasionally). It is important to confirm whether the patient can achieve a flatfoot position during walking. Physical Examination Physical examination of the patient should include a full neurological and musculoskeletal examination. Observational gait analysis should assess for foot position during the swing phase and at initial contact, foot position throughout the stance phase, and evaluation for symmetrical arm swinging. The extremities should be assessed for any abnormalities, such as limited range of motion, strength deficits, limb-length discrepancies, or thigh/calf asymmetry. Assessment for contractures of the ankle has been used to differentiate habitual or dynamic toe-walking from a fixed deformity caused by Achilles contracture. If limited ankle dorsiflexion is noted, the Silfverskiöld test can distinguish between isolated gastrocnemius contracture and triceps surae contracture (comparing ankle dorsiflexion measured with the knee flexed to 90° and the measurement in knee extension). Assessing the plantar callus pattern of the feet provides information about whether or not the heel is in contact with the ground frequently during walking; in a child who walks with a normal first ankle rocker, the heel will have thick, glabrous skin over the heel similar in color, thickness, and roughness to the skin beneath the metatarsal heads. In contrast, a patient who walks only with the forefoot touching the ground will have a widened forefoot compared with the heel, with thickened callus beneath the metatarsal heads and soft, paler skin over the heel as the body adapts to concentration of pressure under the forefoot (Figs. 1-A and 1-B). Knee and ankle range of motion should be assessed. Assessing the patient’s ability to squat can provide information on the functional range of ankle dorsiflexion. Specific evaluations for spasticity include assessments for hyperreflexia, clonus, and the ability to accommodate rapid stretching FEBRUARY 2022 · VOLUME 10, ISSUE 2 · e 21.00193 I d i o p a t h i c To e - Wa l k i n g i n C h i l d r e n a n d A d o l e s c e n t s Fig. 1-A | Fig. 1-B Figs. 1-A and 1-B Plantar surface of the foot of an 11-year-old girl with ITW. Morphological changes in the feet of toe-walking children include thickened callus under the metatarsal heads, a widened forefoot, and a narrow heel. The standing plantar-pressure view shows pressure under the forefoot bilaterally. as in the Duncan-Ely test for spasticity of the rectus femoris13. Another physical examination finding that can highlight CNS abnormalities is the ability of the patient to selectively control active dorsiflexion and plantar flexion of the toes14; the inability to actively dorsiflex and plantar flex the toes on command should prompt an evaluation for a neurological cause of toe-walking. The gait examination should include asking the patient to heel-walk only, to assess for active ankle dorsiflexion range of motion and strength. Asking the patient to run allows assessment of the ability to change the pace of gait and the ability to swing both arms. An inability to symmetrically swing the arms with upper-extremity posturing during running can be a sign of hemiplegic cerebral palsy2. All patients ,5 years of age with a presenting concern of toe-walking should be asked to sit and rise from the floor to assess for subtle proximal muscle weakness often seen in muscular dystrophies. A positive Gower sign is noted if the patient has difficulty rising, and uses the FEBRUARY 2022 upper extremities to push on the thighs to extend the hips or uses them to “climb up the legs” to gain an erect posture15. Diagnostic Testing Laboratory and imaging studies can identify pathological causes of toewalking. Assessment of creatine phosphokinase (CPK) is a simple screening test for myopathies, and genetic testing or muscle biopsy may be warranted if muscular dystrophy is suspected. In the setting of rigid equinus deformity, radiographs of the foot and ankle can rule out skeletal malformations or congenital fusions. Computerized video gait analysis and electromyography studies have been reported to help differentiate ITW from other neuromuscular causes16. If a CNS abnormality is suspected, MRI of the brain and/or spinal cord can assist in ruling out brain malformations or neoplasms, Chiari malformation, syrinx, and a tethered spinal cord as possible etiologies17. · VOLUME 10, ISSUE 2 · e21.00193 Natural History The natural history of ITW has not been extensively studied. Hirsch and Wagner observed 16 nonoperatively treated patients until at least 13 years of age. Two were excluded as they eventually had an Achilles lengthening. All patients received passive stretching exercises aimed at increasing the length of the triceps surae, and 5 were treated with below-knee plaster casts for 2 to 4 weeks. Three of the 5 were administered night splints after cast removal. At the time of follow-up, 11 of the patients were assessed in the clinic. The remaining 3 patients completed a survey and noted no recurrence of toe-walking. Of the 11 patients seen in person, 3 did toe-walk but had the ability to walk with a normal gait, and 8 walked with an initial heelstrike pattern. None had improved ankle dorsiflexion. The authors concluded that nonoperative treatment did not have a long-lasting effect, and indicated that the natural history of ITW was incomplete resolution of toewalking into adulthood 18 . 3 | I d i o p a t h i c To e - Wa l k i n g i n C h i l d r e n a n d A d o l e s c e n t s A large, population-based cohort study of ITW was reported by Engström and Tedroff in 2018. Among 1,401 children with no known motor or neurodevelopmental conditions, 63 (4.5%) walked on their toes or had been toewalkers at any time up to the age of 5.5 years. Twenty-six of the 1,401 children were still toe-walkers at the age of 5.5 years. At 10 years of age, 8 of the 1,401 were still toe-walkers, while 5 had undergone surgical lengthening of the Achilles tendon between 5.5 and 10 years of age. Thus, 50 (79%) of 63 children who were toe-walkers at any point prior to the age of 5.5 years had spontaneously ceased toe-walking by 10 years of age. In this large cohort study of ITW, no patient developed an Achilles contracture2. The further natural history of the 8 patients for whom ITW did not spontaneously resolve is unknown. A critique of this study by Reinker raised further questions regarding the natural history of ITW, as the population studied included only 63 patients, and a gap was noted in our understanding of spontaneous ITW resolution during adolescence19. Articles and book chapters on ITW state that toe-walking resolves in many/most cases with increased age, and that in patients in Fig. 2 The same 11-year-old girl with ITW as in Figs. 1-A and 1-B. The patient has limited ankle dorsiflexion in knee flexion, confirming the development of an Achilles tendon contracture. 4 whom it does not resolve spontaneously, either nonoperative or operative interventions can be beneficial2,20. In addition to the infrequently studied and poorly defined natural history, the indications for treatment are unclear, as the consequences of prolonged or permanent toe-walking gait have not been fully documented. Dietz and Khunsree considered toe-walking a cosmetic deformity that should be treated only if the gait pattern troubles the family, and noted a quote from a 2006 article by Eiff et al. that remains true today: “There is no convincing evidence that any treatment is necessary for toe-walking”21,22. The risks and benefits of operative and nonoperative treatment are also unclear22. Consequences of Continued ITW Literature on the long-term consequences of toe-walking in adolescence and adulthood is scarce. The senior author often hears parental concerns about future foot, knee, hip, and back function or disability. We were unable to find studies with long-term follow-up into adulthood in which these concerns were confirmed or denied. Dietz and Khunsree noted that their adult foot and ankle colleagues did not see adults with foot concerns related to childhood toewalking22. Sobel et al. examined 60 patients who toe-walked, ranging in age from 1 to 15 years20. Patient complaints included falling, in-toeing, pain, fatigue, flatfoot, limping, poor balance, and bunions. In their study, Sobel et al. noted that 46% of patients with ITW had ,0° of passive ankle dorsiflexion, and they found decreased dorsiflexion as age increased. They concluded that ankle equinus contractures may develop as a consequence of prolonged toewalking8,20 (Fig. 2). From our review of the literature, rocker-bottom foot deformity (RBFD) has not been reported among patients with a history of ITW but has been reported among patients with cerebral palsy, clubfoot, peroneal spasticity, flatfoot, and Charcot arthropathy23-25. No report of a patient with ITW describes the development of RBFD or any of its consequences, or adverse effects on knee, hip, or back function. The treating surgeon thus may be well advised to not tell parents that there are long-term adverse consequences of continued toe-walking, such as foot arthritis, ankle arthritis, knee arthritis, or hip arthritis, as there is no evidence yet to support these concerns22. Recent studies note that the abnormal walking pattern has the potential to change foot morphology, with an abnormal shape of the talus, a widened forefoot, and a small and narrow hindfoot26,27. This can be quantified by the forefoot splay index measurement described by Davids et al.: forefoot width divided by hindfoot width28, with an increase in this ratio in children with ITW compared with the normal population27. This change in skeletal development can affect shoewear choice for the patient, and the more concentrated pressure distribution on the forefoot may lead to metatarsalgia in patients with ITW who develop contractures, as DiGiovanni et al. reported forefoot pain in 56% of adults with gastrocnemius contractures29. Compensation for toe-walking can lead to out-toeing to assist foot clearance, and the development of increased external rotation has been reported28,30. After a tendo Achilles lengthening, this may become more obvious and may even require a corrective osteotomy28,31. The potential long-term consequences of persistent toe-walking require more investigation. Treatment Options Nonsurgical treatment options reported for ITW include bracing, botulinum toxin (Botox; Allergan) injections, serial casting, and physiotherapy (PT). The results reported for nonoperative therapy are mixed. While gait improvement is reported for each of these treatment modalities, it seems to be minimal, and in many cases, patients revert to toe-walking after short-term improvement32,33. There is a lack of welldesigned or controlled studies of bracing alone to treat ITW. Bracing is often used FEBRUARY 2022 · VOLUME 10, ISSUE 2 · e 21.00193 I d i o p a t h i c To e - Wa l k i n g i n C h i l d r e n a n d A d o l e s c e n t s as an adjunct with other treatment options such as Botox, PT, or surgery. Bartoletta et al. performed a retrospective review of nonoperative treatment methods, and 103 of the 204 children were given ankle foot orthoses (AFOs). They found that AFO treatment was the only method associated with improvement. At the last follow-up, 55 children had successful outcomes and all had used AFOs at some point in their treatment34. Botox injections into the gastrocnemius for the treatment of ITW have been studied, with successful resolution of toe-walking noted by Sätilä et al. and Brunt et al.32,35, but a randomized controlled trial by Engström et al., which included a group of 15 children between 5 and 13 years of age, found that Botox alone was not an effective treatment. Eleven of the 15 patients completed follow-up at 12 months, and only 3 of the 11 completely ceased toewalking. Four children decreased their toe-walking from 100% to 50%, 100% to 75%, 75% to 50%, and 75% to 25%, respectively36. A follow-up study by Engström et al. combined the use of Botox injections with serial casting. The authors found no significant difference between the Botox and control groups at any time period and concluded that adding Botox injections prior to cast treatment did not improve the outcome33. These studies cast doubt on any utility for botulinum toxin in ITW treatment. There is not a published standardized casting protocol for ITW, but most articles and book chapters recommend bilateral below-the-knee serial walking casts set in slight dorsiflexion, changed at 2 to 4-week intervals. Following casting, there is often a time period with intensified PT and night splints; however, these techniques have led to mixed results. Katz and Mubarak examined 7 toe-walkers with an average age of 7 years. Five underwent serial cast treatment that included bilateral belowthe-knee, dorsiflexion cut-out walking casts for 7 weeks. Two of the 7 continued to toe-walk, and 5 improved. Two years FEBRUARY 2022 after treatment, maximal ankle dorsiflexion increased 6° from the values measured at the termination of the primary treatment3. A 2004 study by Stott et al. included 13 patients who had been treated as children for ITW and underwent gait analysis and calf-muscle strength testing for follow-up after intervention. Six had serial casting only, and 7 had surgery. The patients who received cast treatment had bilateral below-the-knee serial walking casting for 6 weeks, followed by home passive stretching exercises. The 6 patients with cast treatment reported improvement in toe-walking, and all but 1 had visually normal gait, although no child had normalized gait kinematics30. Eastwood et al. found that, despite parental perception of improvement being reported for 51% of patients treated with cast use, physician observation showed that only 22% of patients had a normal heel-totoe gait37. Fox et al. reported that 29 of 44 patients with cast treatment had completely resolved toe-walking at a mean follow-up of 14 months, with 15 continuing toe-walking after bilateral serial casting for 5.7 weeks38. In another cohort of 13 patients with serial walkingcast treatment, 40% continued to toewalk according to the parental report39. Although serial casting has yielded some reported improvements, a high percentage of patients treated with use of casting continue to toe-walk, and the rate of relapse increases over time. The role of PT for ITW is not fully understood, as there are minimal data on PT employed without the incorporation of other treatment modalities. Clark et al. reported that 5 patients had improvement and 1 child had an increase in heel-strike frequency. The parents reported minimal gait change40. Of 14 patients examined by Hirsch and Wagner, 9 were treated with PT that included passive stretching exercises of the calf as well as home exercises to improve active dorsiflexion. Eight of the patients showed complete resolution of toe-walking as noted by physician observation and parental reporting at a mean follow-up of 14 years18. · VOLUME 10, ISSUE 2 · e21.00193 | Surgical treatment of ITW includes gastrocnemius lengthening (zone I), gastrocnemius lengthening with the soleus fascia also lengthened (zone II), or percutaneous or open tendo Achilles lengthening (TAL) (zone III). In toe-walkers, the triceps surae complex is in a shortened length throughout the gait cycle, and lengthening it should promote heel contact during gait. In addition, TAL may weaken plantar flexion temporarily, making toe-walking difficult or impossible for a few months after surgery. Breaking the pattern of continuous toe-walking may allow reprogramming of the CNS to then allow for a normal heel-toe gait pattern to become permanent. In the 1 prospective study that we identified evaluating the natural history of ITW, 8% of patients underwent surgery prior to 10 years of age, although the indications for surgery and the outcomes were not reported2. TAL surgical procedures are simple and effective with minimal complications, with many surgical methods reported to lengthen the triceps surae complex. Stricker and Angulo compared treatment among 3 groups who had undergone observation, casting/AFO use only, and surgery, respectively. The surgical group included 15 patients: 11 with bilateral Achilles Z-plasty lengthening and 4 with bilateral gastrocnemius recession. Among the 3 groups, the surgical group had a 20° improvement (from 210° to 10°) in ankle dorsiflexion, and only 1 patient continued to toewalk41. Hemo et al. retrospectively analyzed 15 patients with ITW, 12 of whom experienced failure of nonoperative measures (serial casting, AFO use, PT). The outcome measurements included passive range of motion, plantar flexion strength, and gait analysis preoperatively and 1 year after surgery. Twelve patients underwent open TAL and 3 underwent percutaneous TAL, and 12 of 15 had complete resolution of toe-walking, whereas 3 had normal gait most of the time but still occasionally walked on their toes42. Similarly, McMulkin et al. retrospectively reviewed 14 patients who had 5 | I d i o p a t h i c To e - Wa l k i n g i n C h i l d r e n a n d A d o l e s c e n t s undergone surgical treatment for ITW (7 TAL: 6 percutaneous and 1 open Z-lengthening, and 7 gastrocnemius lengthenings). Peak knee flexion was normalized in the TAL group, and dorsiflexion was significantly improved in both groups43. McMulkin et al. later studied 8 patients who had surgical lengthening of the gastrocnemius/ soleus. Five years after surgery, gait analysis demonstrated improvements in pelvic tilt and ankle dorsiflexion during stance and swing phases. Ankle plantarflexion power peak values significantly improved from before surgery to the 1-year follow-up (from 0.83 to 1.10 Nm/kg)44. Further improvement was noted at 5-year follow-up, from 1.10 to 1.31 Nm/kg. Overall kinematic improvements were maintained 5 years postsurgery in all 8 patients44. Kogan and Smith’s analysis of 10 surgically treated patients with ITW found that percutaneous TAL is extremely effective, with a predictable outcome, smaller scars, and less time spent in casts as compared to traditional open TAL. None of the patients had any recurrence of toewalking, regardless of the age at initial treatment45. Westberry et al. concluded that those with severe ITW treated initially with a zone-III lengthening have more successful outcomes, no increased risk of overlengthening, no need for additional interventions, and a decreased rate of recurrence. Zone-III procedures were a mix of open Zlengthening, percutaneous Hoke TAL, and open Hoke lengthening. After an average of 3.6 years, no zone-III patients needed additional treatments, operative or nonoperative28. The main concerns with surgical lengthening of the Achilles tendon are overlengthening and permanent weakening, with loss of the ankle plantar flexion-knee extension couple, possible inability for the patient to walk on their toes, or the development of crouch gait. Multiple authors have specifically looked for overlengthening after TAL for ITW, and it has not been found28,39. It is also important to consider the possible risks associated with any lower-extremity surgical procedure, TABLE I Literature on Surgical Treatment of ITW* Study Stricker and Angulo41 (1998) No. of Participants Mean Who Underwent Age at Surgery Surgery (yr) 15 3.9 Type of Intervention TAL (bilateral Z-plasty), 11 Gastrocnemius recession, 4 Followed by cast and AFO for 2-6 months Kogan and Smith45 (2001) Stott et al.30 (2004) 10 7 Not available 10.5 Percutaneous TAL 15 9 TAL (bilateral), 5 TAL (bilateral): percutaneous, 3 and open, 12 Followed by below-the-knee casting and AFO use McMulkin et al.43 (2006) 14 9.3 McMulkin et al.44 (2016) 8 9 14 with complete resolution and 1 continued to toe-walk but showed improvement 3 10 with complete resolution 3.4 6 with complete resolution and 1 occasionally walked on toes when not being observed 10.8 12 with complete resolution and 3 with normal gait most of the time but occasionally walked on toes 2.9 Followed by below-the-knee walking casts for 4 weeks Gastrocnemius lengthening, 2 Hemo et al.42 (2006) Results of Surgical Intervention Mean Time to Follow-up for Surgically Treated Patients (yr) TAL: percutaneous, 6 and open, 1 14 with improvement in all gait parameters Gastrocnemius lengthening, 7 11 TAL, 4 8 with improvement in all gait parameters 5 21 extremities with complete resolution after zone-III lengthenings (100%) 3.6 Gastrocnemius lengthening, 4 Followed by casting for 4 weeks Westberry et al.28 (2021) 26 9.9 Zone-II and zone-III TAL 25 extremities with complete resolution after zone-II lengthenings (88%) *All patients in the published surgical series demonstrated notable improvement, and there were no reported surgical complications. Specifically, no wound-healing problems, Achilles tendon rupture, plantar flexion weakness, or crouch gait were reported. 6 FEBRUARY 2022 · VOLUME 10, ISSUE 2 · e 21.00193 I d i o p a t h i c To e - Wa l k i n g i n C h i l d r e n a n d A d o l e s c e n t s such as venous thromboembolic disease, poor wound-healing, or damage to nearby nerves or vascular structures46. To our knowledge, none of these concerns or complications have been reported after TAL for ITW. Relapse rates after surgery are low, but there are limited surgical series reporting relapse rates with mid to long-term follow-up (Table I). Conclusions ITW is a diagnosis of exclusion with an unknown cause. It is common for children ,2 years of age to walk on their toes, but if this abnormal gait continues after reaching 2 years of age, evaluation for a possible neuromuscular cause is warranted. Most children who toe-walk spontaneously develop a heel-toe gait pattern, but the natural history of toewalking is poorly understood; adverse functional consequences of prolonged toe-walking have not been reported, but further research is needed to define and clarify. Toe-walking is a cosmetic and social concern in childhood, but recent literature shows morphological changes of the foot and the development of equinus contractures in patients with ITW that, as is seen with other orthopaedic conditions, may have an adverse effect on long-term foot function20,26. There is currently no widely accepted protocol for the treatment for ITW, with possible interventions including bracing, PT, use of botulinum toxin, serial casting, and tendon/muscle lengthening surgery. While nonoperative treatments avoid surgical and anesthetic risks, their effectiveness in published studies is poor, and the longevity of a normal gait following these treatments is not well documented. Surgical lengthening of the Achilles tendon, however, results in the most consistent and successful outcomes, and thus far, no surgical complications have been reported. Literature reports of surgically treated patients show complete resolution of, or notable improvement in, toe-walking. The excellent results with no morbidity reported for zone-III lengthenings, and the simplicity and effectiveness of per- FEBRUARY 2022 cutaneous TAL, have made this the preferred treatment option for some authors28,45. This treatment is offered to parents of toe-walking children $5 years of age when the family finds the gait pattern troubling and they desire an effective treatment. More research is needed focusing on the population of adolescent toe-walkers with no spontaneous resolution and assessing whether morphological changes and the development of contractures noted in toewalking adolescents have functional consequences. Larger cohorts and longer follow-up periods are essential to developing an evidence-based approach to the treatment of ITW. Source of Funding No funding was received for this manuscript. Halle D. Freiman, MS, MD1, Curtis Mensah, MS2, Jason Codrington, BS3, Steven L. Frick, MD1 1Stanford University School of Medicine, Palo Alto, California 2Meharry Medical College, Nashville, Tennessee 3University of Miami Miller School of Medicine, Miami, Florida Email for corresponding author: sfrick01@stanford.edu References 1. Oetgen ME, Peden S. Idiopathic toe walking. J Am Acad Orthop Surg. 2012 May;20(5):292-300. 2. Engström P, Tedroff K. Idiopathic ToeWalking: Prevalence and Natural History from Birth to Ten Years of Age. J Bone Joint Surg Am. 2018 Apr 18;100(8):640-7. 3. Katz MM, Mubarak SJ. Hereditary tendo Achillis contractures. J Pediatr Orthop. 1984 Nov;4(6):711-4. 4. Hall JE, Salter RB, Bhalla SK. Congenital short tendo calcaneus. J Bone Joint Surg Br. 1967 Nov; 49(4):695-7. 5. Sutherland DH. Gait Disorders in Childhood and Adolescence. Williams & Wilkins; 1984. Walking: Etiology, Prevalence, Classification, and Treatment. Foot Ankle Spec. 2017 Aug; 10(4):337-42. 8. Furrer F, Deonna T. Persistent toe-walking in children. A comprehensive clinical study of 28 cases. Helv Paediatr Acta. 1982 Sep;37(4): 301-16. 9. Williams CM, Tinley P, Curtin M. Idiopathic toe walking and sensory processing dysfunction. J Foot Ankle Res. 2010 Aug 16;3(1):16. 10. Leyden J, Fung L, Frick S. Autism and toewalking: are they related? Trends and treatment patterns between 2005 and 2016. J Child Orthop. 2019 Aug 1;13(4):340-5. 11. O’Connor SM, Kuo AD. Directiondependent control of balance during walking and standing. J Neurophysiol. 2009 Sep;102(3): 1411-9. 12. Pomarino D, Ramı́rez Llamas J, Pomarino A. Idiopathic Toe Walking: Family Predisposition and Gender Distribution. Foot Ankle Spec. 2016 Oct;9(5):417-22. 13. Lee SY, Sung KH, Chung CY, Lee KM, Kwon SS, Kim TG, Lee SH, Lee IH, Park MS. Reliability and validity of the Duncan-Ely test for assessing rectus femoris spasticity in patients with cerebral palsy. Dev Med Child Neurol. 2015 Oct; 57(10):963-8. 14. Pomarino D, Ramı́rez Llamas J, Pomarino A. Idiopathic Toe Walking: Tests and Family Predisposition. Foot Ankle Spec. 2016 Aug;9(4): 301-6. 15. Chang RF, Mubarak SJ. Pathomechanics of Gowers’ sign: a video analysis of a spectrum of Gowers’ maneuvers. Clin Orthop Relat Res. 2012 Jul;470(7):1987-91. 16. Griffin PP, Wheelhouse WW, Shiavi R, Bass W. Habitual toe-walkers. A clinical and electromyographic gait analysis. J Bone Joint Surg Am. 1977 Jan;59(1):97-101. 17. Morozova OM, Chang TF, Brown ME. Toe Walking: When Do We Need to Worry? Curr Probl Pediatr Adolesc Health Care. 2017 Jul; 47(7):156-60. 18. Hirsch G, Wagner B. The natural history of idiopathic toe-walking: a long-term follow-up of fourteen conservatively treated children. Acta Paediatr. 2004 Feb;93(2):196-9. 19. Reinker KA. Does Idiopathic Toe-Walking Spontaneously Correct?: Commentary on an article by Pähr Engström, MD, PhD, and Kristina Tedroff, MD, PhD: “Idiopathic Toe-Walking: Prevalence and Natural History from Birth to Ten Years of Age”. J Bone Joint Surg Am. 2018 Apr 18;100(8):e53. 20. Sobel E, Caselli MA, Velez Z. Effect of persistent toe walking on ankle equinus. Analysis of 60 idiopathic toe walkers. J Am Podiatr Med Assoc. 1997 Jan;87(1):17-22. 21. Eiff MP, Steiner E, Judkins DZ, Winkler-Prins V. Clinical inquiries. What is the appropriate evaluation and treatment of children who are “toe walkers”? J Fam Pract. 2006 May;55(5): 447-50: 450. 22. Dietz F, Khunsree S. Idiopathic toe walking: to treat or not to treat, that is the question. Iowa Orthop J. 2012;32:184-8. 6. Williams CM, Tinley P, Curtin M, Wakefield S, Nielsen S. Is idiopathic toe walking really idiopathic? The motor skills and sensory processing abilities associated with idiopathic toe walking gait. J Child Neurol. 2014 Jan;29(1): 71-8. 23. Hoover GH, Frost HM. Dynamic correction of spastic rocker-bottom foot. Peroneal to anterior tibial tendon transfer and heel-cord lengthening. Clin Orthop Relat Res. 1969 JulAug;65(65):175-82. 7. Pomarino D, Ramı́rez Llamas J, Martin S, Pomarino A. Literature Review of Idiopathic Toe 24. Koureas G, Rampal V, Mascard E, Seringe R, Wicart P. The incidence and treatment of rocker · VOLUME 10, ISSUE 2 · e21.00193 | 7 | I d i o p a t h i c To e - Wa l k i n g i n C h i l d r e n a n d A d o l e s c e n t s bottom deformity as a complication of the conservative treatment of idiopathic congenital clubfoot. J Bone Joint Surg Br. 2008 Jan;90(1):57-60. 25. Persky JD, Langan T, Smith CN, Burns PR. Plantar Approach for Midfoot Wedge Resection to Reconstruct the Rocker Bottom Foot. J Foot Ankle Surg. 2019 Sep;58(5):1030-5. 26. Sinclair MR, Lind AA, Knowlton JQ. The effect of persistent toe walking on the skeletal development of the pediatric foot and ankle. J Pediatr Orthop B. 2018 Jan;27(1):77-81. 27. Davids J, Kephart D, Phan J, Calafi A, Brown S, Laing S, Bagley A, Kulkarni V. Quantitative assessment of forefoot splay in children with persistent idiopathic toe walking. Poster presented at: AACPDM 73rd Annual Meeting; September 18, 2019; Anaheim, CA. 28. Westberry DE, Carpenter AM, Brandt A, Barre A, Hilton SB, Saraswat P, Davids JR. Surgical Outcomes for Severe Idiopathic Toe Walkers. J Pediatr Orthop. 2021 Feb 1;41(2): e116-24. 29. DiGiovanni CW, Kuo R, Tejwani N, Price R, Hansen ST Jr, Cziernecki J, Sangeorzan BJ. Isolated gastrocnemius tightness. J Bone Joint Surg Am. 2002 Jun;84(6):962-70. 30. Stott NS, Walt SE, Lobb GA, Reynolds N, Nicol RO. Treatment for idiopathic toe-walking: results at skeletal maturity. J Pediatr Orthop. 2004 Jan-Feb;24(1):63-9. 31. Schoenecker P, Rich M. Chapter 28: Idiopathic Toe-Walking. In: Eastwood DM, editor. Lovell and Winter’s Pediatric 8 Orthopaedics. 6th ed. Lippincott, Williams & Wilkins; 2006. p 1204-11. 32. Sätilä H, Beilmann A, Olsén P, Helander H, Eskelinen M, Huhtala H. Does Botulinum Toxin A Treatment Enhance the Walking Pattern in Idiopathic Toe-Walking? Neuropediatrics. 2016 Jun;47(3):162-8. 33. Engström P, Bartonek Å, Tedroff K, Orefelt C, Haglund-Åkerlind Y, Gutierrez-Farewik EM. Botulinum toxin A does not improve the results of cast treatment for idiopathic toe-walking: a randomized controlled trial. J Bone Joint Surg Am. 2013 Mar 6;95(5):400-7. 34. Bartoletta J, Tsao E, Bouchard M. A Retrospective Analysis of Nonoperative Treatment Techniques for Idiopathic Toe Walking in Children: Outcomes and Predictors of Success. PM R. 2021 Oct;13(10):1127-35. 39. Eastwood DM, Menelaus MB, Dickens DR, Broughton NS, Cole WG. Idiopathic toe-walking: does treatment alter the natural history? J Pediatr Orthop B. 2000 Jan;9(1):47-9. 40. Clark E, Sweeney JK, Yocum A, McCoy SW. Effects of motor control intervention for children with idiopathic toe walking: a 5-case series. Pediatr Phys Ther. 2010 Winter;22(4):417-26. 41. Stricker SJ, Angulo JC. Idiopathic toe walking: a comparison of treatment methods. J Pediatr Orthop. 1998 May-Jun;18(3):289-93. 42. Hemo Y, Macdessi SJ, Pierce RA, Aiona MD, Sussman MD. Outcome of patients after Achilles tendon lengthening for treatment of idiopathic toe walking. J Pediatr Orthop. 2006 May-Jun;26(3):336-40. 35. Brunt D, Woo R, Kim HD, Ko MS, Senesac C, Li S. Effect of botulinum toxin type A on gait of children who are idiopathic toe-walkers. J Surg Orthop Adv. 2004 Fall;13(3):149-55. 43. McMulkin ML, Baird GO, Caskey PM, Ferguson RL. Comprehensive outcomes of surgically treated idiopathic toe walkers. J Pediatr Orthop. 2006 Sep-Oct;26(5):606-11. 36. Engström P, Gutierrez-Farewik EM, Bartonek A, Tedroff K, Orefelt C, HaglundÅkerlind Y. Does botulinum toxin A improve the walking pattern in children with idiopathic toewalking? J Child Orthop. 2010 Aug;4(4):301-8. 44. McMulkin ML, Gordon AB, Tompkins BJ, Caskey PM, Baird GO. Long term gait outcomes of surgically treated idiopathic toe walkers. Gait Posture. 2016 Feb;44: 216-20. 37. Eastwood DM, Dennett X, Shield LK, Dickens DR. Muscle abnormalities in idiopathic toe-walkers. J Pediatr Orthop B. 1997 Jul;6(3): 215-8. 45. Kogan M, Smith J. Simplified approach to idiopathic toe-walking. J Pediatr Orthop. 2001 Nov-Dec;21(6):790-1. 38. Fox A, Deakin S, Pettigrew G, Paton R. Serial casting in the treatment of idiopathic toewalkers and review of the literature. Acta Orthop Belg. 2006 Dec;72(6):722-30. 46. Mosca VS. Principles and Management of Pediatric Foot and Ankle Deformities and Malformations. 1st edition. Lippincott Williams and Wilkins; 2014. FEBRUARY 2022 · VOLUME 10, ISSUE 2 · e 21.00193