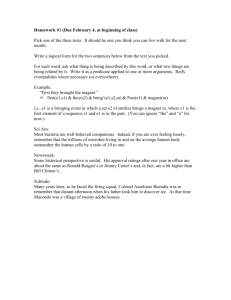
HHS Public Access Author manuscript Author Manuscript Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Published in final edited form as: Policy Polit Nurs Pract. 2021 November ; 22(4): 245–252. doi:10.1177/15271544211053854. The Association of Hospital Magnet® Status and Pay-forPerformance Penalties Andrew M. Dierkes, PhD, RN1, Kathryn Riman, PhD, RN2, Marguerite Daus, PhD, RN3, Hayley D. Germack, PhD, MHS, RN1, Karen B. Lasater, PhD, RN, FAAN4 1Department of Acute and Tertiary Care, University of Pittsburgh School of Nursing, Pittsburgh, PA, USA Author Manuscript 2Department of Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA 3Denver-Seattle Center of Innovation for Veteran-Centered and Value-Driven Care (COIN), Eastern Colorado Health Care System, Aurora, CO, USA 4Center for Health Outcomes and Policy Research, University of Pennsylvania School of Nursing, Philadelphia, PA, USA Abstract Author Manuscript Author Manuscript The Centers for Medicare and Medicaid Services’ Pay-for-Performance (P4P) programs aim to improve hospital care through financial incentives for care quality and patient outcomes. Magnet® recognition—a potential pathway for improving nurse work environments—is associated with better patient outcomes and P4P program scores, but whether these indicators of higher quality are substantial enough to avoid penalties and thereby impact hospital reimbursements is unknown. This cross-sectional study used a national sample of 2,860 hospitals to examine the relationship between hospital Magnet® status and P4P penalties under P4P programs: Hospital Readmission Reduction Program, Hospital-Acquired Conditions (HAC) Reduction Program, Hospital ValueBased Purchasing (VBP) Program. Magnet® hospitals were matched 1:1 with non-Magnet hospitals accounting for 13 organizational characteristics including hospital size and location. Post-match logistic regression models were used to compute a hospital’s odds of penalties. In a national sample of hospitals, 77% of hospitals experienced P4P penalties. Magnet® hospitals were less likely to be penalized in the VBP program compared to their matched non-Magnet counterparts (40% vs. 48%). Magnet® status was associated with 30% lower odds of VBP penalties relative to non-Magnet hospitals. Lower P4P program penalties is one benefit associated with achieving Magnet® status or otherwise maintaining high-quality nurse work environments. Corresponding Author: Andrew M. Dierkes, Department of Acute and Tertiary Care, University of Pittsburgh School of Nursing, 3500 Victoria Street, Pittsburgh, PA 15261, USA. amd323@pitt.edu. Declaration of Conflicting Interests The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Supplemental Material Supplemental material for this article is available online. Dierkes et al. Page 2 Author Manuscript Keywords reimbursement; incentive; value-based purchasing; medicare; quality of health care; crosssectional studies; hospitals Author Manuscript The Centers for Medicare and Medicaid Services’ (CMS) Pay-for-Performance (P4P) programs aim to improve health care through financial incentives to hospitals for care quality and patient outcomes. Three P4P programs, in particular, have hospitals compete on various performance metrics with up to 6% of total hospital CMS reimbursement at stake: (a) Hospital Readmission Reduction Program (HRRP), (b) Hospital-Acquired Conditions (HAC) Reduction Program, and (c) Hospital Value-Based Purchasing (VBP) Program (Centers for Medicare & Medicaid Services, 2020a, 2020b, 2020c). These programs are mandated for hospitals paid under the inpatient prospective payment system. Depending on their performance relative to peer institutions, hospitals may receive financial penalties. The VBP program differs from the HRRP and HAC Reduction Program in that it also extends upside potential to hospitals. High performing hospitals may receive more than the amount withheld under VBP, in effect awarding a financial bonus. Existing research documents that hospitals with better nursing resources, such as better patient-to-nurse staffing ratios, better nurse work environments, and Magnet® recognition perform better on P4P program quality metrics (Lasater et al., 2016). Patients in hospitals with these superior nursing resources are less likely to experience readmissions (Lasater & McHugh, 2016; McHugh et al., 2013; McHugh & Ma, 2013) and hospital-acquired conditions (Barnes et al., 2016; Shin et al., 2019), and are more likely to be satisfied with their care (Martsolf et al., 2016; Stimpfel et al., 2016). Author Manuscript The nurse work environment reflects a healthcare organization’s capacity to support nurses’ professional practice, improve job satisfaction, and champion patient safety (Lake, 2002). One established pathway to improve a hospital’s nurse work environment is achieving Magnet® status (Aiken et al., 2008; Ulrich et al., 2007). Although the existing evidence has linked better nursing resources with superior performance (i.e., higher scores) on P4P program quality metrics, little is known about whether these better P4P program scores affect financial outcomes. P4P Programs Author Manuscript CMS is the largest funder of health care and a portion of CMS hospital reimbursement is contingent upon performance in the areas assessed by P4P programs, including but not limited to the three programs evaluated in this study (Centers for Medicare & Medicaid Services, 2020a, 2020b, 2020c). The HRRP program monitors unplanned readmissions for selected patients and hospitals with excess readmissions can lose up to 3% of CMS reimbursement (Centers for Medicare & Medicaid Services, 2020a). The HAC program tracks five health care-associated infections; poor performance could cost hospitals an additional 1% in forgone reimbursements (Centers for Medicare & Medicaid Services, 2020b). VBP includes four quality domains (Clinical Care, Person and Community Engagement, Safety, and Efficiency and Cost Reduction) and is comprised, in part, of the eight dimensions of the Hospital Consumer Assessment of Healthcare Providers Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 3 Author Manuscript and Systems patient experience survey (communication with nurses, communication with doctors, the responsiveness of hospital staff, communication about medicines, cleanliness and quietness of the hospital environment, discharge information, overall rating of the hospital, and care transition) (Centers for Medicare & Medicaid Services, 2020c). The VBP program withholds 2% of reimbursements and redistributes those funds based on performance (Centers for Medicare & Medicaid Services, 2020c). Magnet® Recognition and P4P Outcomes Author Manuscript The American Nurses Credentialing Center (ANCC) established the Magnet® Recognition Program in 1994 to accredit hospitals that demonstrate nursing excellence and favorable patient outcomes (American Nurses Credentialing Center, n.d.-a). Magnet® status is not just a recognition of nursing excellence and quality of care but a process to improve hospital nurse work environments and patient outcomes (Kutney-Lee et al., 2015). A longitudinal analysis of 136 hospitals between 1999 and 2007 found that achieving Magnet® status is associated with improvements in hospital work environments and lower odds of 30-day mortality and failure-to-rescue among surgical patients (Kutney-Lee et al., 2015). As of July 2021, 561 hospitals were Magnet® recognized—roughly 9% of all hospitals in the United States (American Nurses Credentialing Center, n.d.-a, n.d.-b). Author Manuscript Although many studies have evaluated the association of nursing resources such as Magnet® status and the work environment on the patient outcomes included in Medicare’s P4P programs, little is known about associated financial implications in terms of whether these performance improvements translate to penalties avoided. McHugh et al. (2013) found that hospitals with better nurse staffing had 25% lower odds of penalties under HRRP compared to those with poorer staffing levels. Lasater et al. (2016) documented that Magnet® status predicted higher scores on Total Performance (an indicator of VBP performance) and two VBP domains ([a] Clinical Processes and [b] Patient Experience). Whether nursing resources are associated with penalties under the HAC program is unknown. Likewise, the association of nursing resources with overall P4P performance—the overall financial effect across the three programs—has not been empirically evaluated. A perceived barrier to achieving Magnet® status is the cost of meeting and maintaining accreditation standards (Pinkerton, 2005). Whether Magnet® status is associated with hospitals avoiding penalties is an important, but missing, piece of information for administrators weighing the value and feasibility of investing in hospital nursing. This study evaluated whether a hospital’s Magnet® status is associated with individual P4P program penalties and overall effect accounting for financial penalties and bonuses across three programs. Author Manuscript Methods Data Sources and Sample This was a cross-sectional analysis of a national sample of hospitals using data sets from 2015 to 2017, including (a) the American Hospital Association (AHA) annual survey, (b) CMS data made publicly available by Advisory Board (National P4P Map), (c) CMS Final Rule Impact File, and (d) data on hospital Magnet® status obtained from the ANCC website. The AHA Annual Survey provided information on nurse staffing and hospital organizational Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 4 Author Manuscript characteristics. Data from CMS provided information on penalties and additional hospital organizational characteristics such as case mix index (CMI), disproportionate share, and wage index. ANCC data provided information on hospital Magnet® status. The final sample included 2,860 hospitals (2,529 non-Magnet hospitals and 331 Magnet® hospitals). Measures Author Manuscript Our explanatory variable was Magnet® status. Achieving Magnet® recognition is a multiyear application and approval process and improvements in nursing quality and associated outcomes may be seen before the status is formally awarded, so we considered hospitals to be Magnet® if they received recognition as of 2017. Our outcome of interest was the hospital P4P program and overall penalties. The financial impact within each of three CMS P4P programs—VBP, HRRP, HAC Reduction Program—and the overall impact (sum of the financial penalties and/or bonuses) across all programs is referenced as overall P4P. We dichotomized overall P4P to indicate a positive or negative financial outcome (0 = ≥$0.00, 1 = <$0.00). Penalities are assessed at the individual program level. In order to arrive at an overall penalty indicator for overall P4P, we used the value of dollars summed by hospital across programs. Hospitals that received greater than the 2% originally withheld under VBP were coded as 0 (not a penalty). However, the dollar value of any VBP bonus counted against penalties accrued under other programs in the analysis of overall P4P penalty outcomes. If the VBP bonus meets or exceeds the absolute value of any penalties under both HAC and HRRP combined, overall P4P is coded 0 (not a penalty). Author Manuscript We included hospital characteristics in both our matching approach and regression analyses, similar to prior work in this area (Lasater et al., 2016; McHugh et al., 2013) and consistent with guidance on including variables in propensity score models (Stuart, 2010) and as covariates when modeling treatment effects (Nguyen et al., 2017). Continuous variables included hospital size (number of beds), Herfindahl–Hirschman Index (a measure of market competition calculated as the sum of the squares of the market share of each hospital competing), CMI (a measure of patient acuity represented by the average relative diagnosisrelated group weight of a hospital’s inpatient discharges), disproportionate share (a measure of payments intended to offset costs incurred by hospitals treating a large or disproportionate number of indigent patients), percent Medicare patients, percent Medicaid patients, wage index (a ratio of the area’s average hourly wage to the national average hourly wage), the ratio of medical residents to beds, and nurse staffing (registered nurse hours per adjusted patient day). Dichotomous and categorical variables included technology status (capacity to perform organ transplantation or open-heart surgery), ownership (for-profit versus nonprofit institution), core-based statistical area (a measure of population concentration), and region (geographic areas of the United States as defined by the U.S. Census Bureau). Author Manuscript Analysis We conducted analyses using matched and unmatched samples. Magnet® hospitals were matched 1:1 with non-Magnet® hospitals using nearest neighbor propensity score matching without replacement to identify non-Magnet® hospitals that otherwise had the observable characteristics associated with Magnet® institutions. These variables were presented in our discussion of measures and are listed in Supplementary Table 1. A logistic regression Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 5 Author Manuscript model produced propensity scores representing the probability of Magnet® status based on these variables. Each Magnet® hospital was paired with the “nearest” available non-Magnet hospital, where the distance between hospitals is the difference in propensity scores. This approach approximates a randomized controlled trial in that the matched pairs of hospitals are similar on all observable characteristics except for the treatment (in this case, Magnet® recognition). This allows us to attribute an observed effect of the treatment with greater confidence than a regression analysis of unmatched cross-sectional data (Silber et al., 2001). Matching improves the homogeneity of all other observable characteristics across Magnet® and non-Magnet hospitals and helps account for selection bias—that these characteristics might be associated with a hospital’s decision to pursue Magnet® recognition and therefore result in systematic differences mirroring Magnet® status. Author Manuscript The balance of covariate distribution between Magnet® and non-Magnet hospitals signals the quality of the match. Standardized mean differences (SMDs) are the difference in means between groups (Magnet® vs. all non-Magnet hospitals in the prematch analysis and Magnet® vs. non-Magnet controls in the postmatch analysis) divided by the standard deviation (SD) of each covariate for Magnet® hospitals. Incorporating the SD into the calculation normalizes the scale across covariates to aid in comparison. The closer the resulting SMDs are to zero, the better the match. Consistent with prior research employing propensity score matching to pair Magnet® and non-Magnet hospitals, we adopted 0.2 as the threshold for an adequate match (Lasater et al., 2016). Statistical models employed logistic regression to estimate the odds of penalties associated with Magnet® status. These models, when adjusted, included as controls the same variables used in the matching approach for a doubly robust analysis to account for residual imbalance (Nguyen et al., 2017). Author Manuscript Results Author Manuscript Table 1 presents the descriptive characteristics of the national sample of hospitals, before and after propensity score matching. Seventy-seven percent of hospitals received overall P4P penalties, with rates differing by the individual program. Twenty-three percent of hospitals received penalties under HAC, 46% under VBP, and 84% under HRRP. As indicated by the “pre-match” SMDs greater in absolute value than 0.2, the 331 Magnet® hospitals as a group differed from the 2,529 non-Magnet hospitals across all hospital characteristics. After narrowing the non-Magnet group to 331 matched controls, these differences were greatly diminished—represented by “post-match” SMDs that were in all cases <0.2 in absolute value, and in most cases <0.1. The change in these SMDs and the difference between using all data versus matched data is visually apparent in Figure 1. The penalty rates between Magnet® and non-Magnet hospitals in this matched cohort varied by program. The percent of Magnet® and non-Magnet hospitals penalized under overall P4P and HAC were similar (overall P4P, 76% vs. 78%; HAC, 30% vs. 28%, respectively). More Magnet® than non-Magnet hospitals were penalized under HRRP (85% vs. 80%). The opposite was true of VBP in Magnet® versus non-Magnet hospitals (40% vs. 49%). Table 2 presents the results of the logistic regression analyses evaluating the odds of penalties associated with Magnet® status after adjusting for hospital characteristics in both the unmatched and matched samples. Magnet® status was associated with lower odds of Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 6 Author Manuscript penalties for VBP across all models. Within the fully adjusted models, overall P4P crossed our threshold for statistical significance in the unmatched data only (odds ratio [OR]: 0.66, 95% confidence interval [CI]: 0.48–0.91, p < .05). In the matched data, while the direction of effect for both overall P4P and VBP was unchanged from the unmatched analysis, these associations were statistically significant for VBP penalties only (OR: 0.66, 95% CI: 0.48– 0.92, p < .05). In the final matched, adjusted models, HRRP is notable for its large effect size (OR: 1.40) in contrast to HAC (OR: 1.02), although neither result was statistically significant. Sensitivity Analysis Author Manuscript Magnet® status is a signal for good nurse work environments; however, hospitals can have excellent nurse work environments without holding Magnet® recognition. Therefore, we conducted a sensitivity analysis using a subset of hospitals in four states (California, Florida, Pennsylvania, and New Jersey) for which we had detailed data about nurse work environments to evaluate the robustness of our main findings. Supplementary Table 1 presents a comparison of the primary and sensitivity analyses. Using data from the 2016 RN4CAST-U.S. survey of nurses, we created hospital-level measures of the nurse work environments derived from frontline nurse informants’ reports using the Practice Environment Scale of the Nursing Work Index (PES-NWI). (Lake, 2002). Additional details of the survey methodology are provided elsewhere (Lasater et al., 2019). Author Manuscript Author Manuscript The propensity score method of matching hospitals on Magnet® status, a binary indicator, cannot be used to match continuous measures, such as PES-NWI. Nonbipartite matching is designed for matching on nonbinary measures (Lu et al., 2011). We employed nonbipartite matching to mirror our primary analysis of Magnet® hospitals by pairing hospitals with higher- and lower-quality work environments, generating two equal groups of hospitals that were similar on all other observed characteristics. The approach involved several steps. First, the “treatment” of interest—hospital-level nurse work environment score—was categorized by quartile in order to differentiate levels of work environment quality. Next, an ordinal logit model including all hospital covariates produced maximum likelihood estimates representing the distance between hospitals, much like the propensity scores in our primary matching method. Finally, these were used to balance covariate distributions across groups. This approach accomplished two aims: to pair hospitals across groups such that (a) the distribution of observed covariates was balanced and (b) the difference in exposure to a better work environment was maximized across all pairs. Within each pair, the hospital with the higher quality work environment was labeled “high PES-NWI” and the hospital with the lower quality work environment was labeled “low PES-NWI.” This sensitivity analysis examined 482 hospitals: 241 in lower quality work environments and 241 in higher quality work environments. This process was accomplished using the R package “nbpMatching” developed by Lu et al. (2011). Supplementary Table 2 presents the descriptive characteristics of the four-state data set and the results of nonbipartite matching. Although the 482 hospitals in the four-state data had a higher overall rate of P4P penalization than the national sample (83% vs. 77%), the penalty rate by program mirrored that of the national sample presented in our primary analysis, Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 7 Author Manuscript ranging from HAC (28%) to HRRP (85%) (23%–84% in the national sample). The greatest difference in penalty rates by program within the four-state data between hospitals with “low” and “high” work environment scores was observed for VBP (15 percentage points). Differences were statistically significant at the p <.05 level for VBP and overall P4P only. Hospitals with better work environments had substantially lower rates of penalties across all individual programs and for overall P4P. As in the primary analysis, the low SMDs (<0.01 in all cases) signal adequate matching results. Author Manuscript Author Manuscript Supplementary Table 3 presents the results from logistic regression models that are identical in structure to those in the primary analysis except for the independent variable, where this sensitivity analysis substituted work environment quality for Magnet® status. The unmatched models regressed on an ordinal variable derived from the continuous PES-NWI score by dividing hospitals into work environment quality groups based on quartile: poor (bottom quartile), mixed (middle two quartiles), and best (top quartile). A unit increase in work environment quality represents a change from “poor” to “mixed” (or from “mixed” to “best”) work environments. This is consistent with existing approaches to modeling PES-NWI in nursing health services research (Lake et al., 2019). The matched models represent the change in odds of penalties between hospitals with relatively higher versus lower PES-NWI scores. The results of the sensitivity analysis paralleled the primary analysis with two key differences. As with Magnet® in the primary analysis, we found an inverse relationship between the quality of the work environment and VBP, while the HRRP and HAC programs did not cross our threshold for statistical significance. However, the direction of effect for HRRP in the final matched, adjusted model was opposite that of the primary analysis, making it more consistent with the other programs and our hypothesis that better nurse work environments are associated with lower odds of penalties. In contrast to the primary analysis, overall P4P in this sensitivity analysis, as with VBP, was significant across all models at the p < .01 or p < .001 level. Discussion Author Manuscript Our analysis is the first to document that Magnet® hospitals are less likely to be penalized under the VBP P4P program. We found no significant differences in odds of HRRP and HAC program penalties or overall P4P penalties between Magnet® and non-Magnet hospitals in our fully adjusted models using matched data. In a sensitivity analysis, we found large effects for VBP as an individual program associated with better hospital nurse work environments. Together, the primary and sensitivity analyses may reveal the work environment as an underlying factor by which Magnet® hospitals might avoid P4P program penalties. Magnet® is just one strategy for improving nurse work environments. Although Magnet® hospitals are known for the quality of their work environments, not all hospitals with higher quality work environments are Magnet®-recognized (McHugh et al., 2016). For hospital administrators, this may be actionable evidence to improve the quality of care and reduce P4P penalties by investing to improve hospital nurse work environments. The only study to document an association between nursing organizational factors and penalties under a P4P program found that hospitals with better nurse staffing were less likely to receive HRRP penalties (McHugh et al., 2013). Our study provides a more complete Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 8 Author Manuscript Author Manuscript picture by documenting the odds of penalties for each program separately and the overall effect across three P4P programs. This is important because avoiding penalties under one program does not guarantee avoidance in another program. Furthermore, under VBP, the amount a hospital receives may be less than (a penalty, in this study), equal to, or greater than (in effect, a bonus) the amount withheld by CMS. As a result, a hospital may incur a penalty in one of the individual programs that is counteracted by a VBP bonus. Both Magnet® recognition and better work environments were associated with lower odds of VBP program penalties across all models. The effects of Magnet status and better work environments on HRRP and HAC penalties were statistically insignificant across all adjusted models. Importantly, HRRP and HAC are distinct from VBP in that they specifically focus on clinical outcomes and aspects of care. It is possible that Magnet® recognition and work environments have less of a direct impact on specific causes of readmission and infection rates and more to do with a summative effect. Although we do not have evidence that penalties under HRRP and HAC were different between Magnet® and non-Magnet hospitals or between hospitals with relatively high- and low-quality work environments, it is possible that hospitals with higher quality work environments, such as Magnet® hospitals, are more likely to receive a bonus under VBP. The combination of significance in VBP and overall P4P and insignificance in HRRP and HAC in the sensitivity analysis suggest that the impact of better work environments on VBP may be great enough to counteract the financial impact of any penalties in these other programs. Author Manuscript P4P penalties represent financial losses for hospitals. They are different from but related to performance scores. Although Lasater et al. (2016) have shown that Magnet® status is associated with better scores on VBP, because performance is evaluated relative to other hospitals in the program, better P4P program scores do not always equate to avoided penalties. Comparable changes in scores across all hospitals may yield the same cohorts of hospitals penalized under each program. By examining penalties directly instead of the underlying change in P4P program scores, this study bridges this gap by providing evidence for Magnet® status associated with penalties avoided. This bolsters the case for Magnet® by demonstrating evidence of favorable financial impacts associated with such recognition. Author Manuscript The effectiveness of pursuing Magnet® recognition or otherwise improving hospital nurse work environments to improve patient outcomes is well-documented in the literature. There is evidence to suggest that this association may be causal, including Magnet® status (Kutney-Lee et al., 2015) and the work environment (Lake et al., 2020; Sloane et al., 2018). The association of Magnet® status and the quality of hospital work environments with P4P programs is an important consideration of interest to administrators seeking to justify greater investments in nursing. Reductions in financial penalties may offset the expense of pursuing Magnet® recognition or other improvements in the nurse work environment. This study contributes to this body of literature by recognizing both Magnet® recognition and improvements in the work environment as innovative management interventions that leverage the nursing workforce to improve outcomes and lower costs of care. Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 9 Limitations Author Manuscript Author Manuscript This study is not without limitations. However, we have taken steps to mitigate these weaknesses. For example, cross-sectional data ordinarily limits the interpretation of results to associations. Our matching approach, which adjusts for potential selection bias of Magnet® hospitals and associated systematic differences between Magnet® and nonMagnet hospitals, addresses this limitation by significantly improving the comparability of the groups regarding observed characteristics such that the effect may be attributed to the “treatment.” In both our primary and sensitivity analyses, this was achieved by balancing the probability of receiving the “treatment” (i.e., Magnet® recognition or a better work environment) across the treatment and control groups. It is important to note that these matching approaches cannot account for unobserved factors, such as quality improvement initiatives conducted in an organization. These limitations emphasize the need for longitudinal and interventional studies evaluating the outcomes advantages of Magnet® hospitals. Conclusions This study examined the impact of Magnet® recognition and, in a sensitivity analysis, higher quality work environments, on the odds of P4P program penalties. We found that Magnet® hospitals and those with better nurse work environments were less likely to lose a portion of their CMS reimbursement as a result of poor performance in P4P programs. The findings provide evidence that investments to improve hospital nursing through the Magnet® journey or other interventions to improve the hospital work environment may be offset by subsequent savings in reduced P4P program penalties. Author Manuscript Supplementary Material Refer to Web version on PubMed Central for supplementary material. Acknowledgments The findings of this study are solely the responsibility of the authors. The authors would like to thank Duy Do and Morgan Peele for analytic support, Kyle Campbell for assistance in interpreting Advisory Board data and guidance in choosing covariates, and Malia Meyer for assistance in organizing our response to peer reviewers. Funding The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Institute of Nursing Research (grant numbers: T32NR007104, R01NR014855, LH Aiken, PI, T32HL007820, Kahn, PI). Author Manuscript Biographies Andrew M. Dierkes is a registered nurse and a health services and policy researcher studying the nursing workforce at the intersection of cost, quality, and outcomes. He is an assistant professor at the University of Pittsburgh School of Nursing, Department of Acute and Tertiary Care. Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 10 Author Manuscript Kathryn Riman is a practicing staff nurse and health services and policy researcher interested in critical care nursing, critical care organization and management, and quality improvement. She is a postdoctoral scholar in the Department of Critical Care Medicine at the University of Pittsburgh School of Medicine and Treasurer of the AcademyHealth Interdisciplinary Research Group on Nursing Issues. Marguerite Daus research is focused on the optimization of healthcare transitions, specifically from hospital to home, for high-risk patients with social needs with the goal of improving patient outcomes. She is an advanced HSR&D fellow at the Denver/Seattle Center of Innovation VA Eastern Colorado Health Care System. Author Manuscript Hayley D. Germack is a nurse and health services and policy researcher with a focus on improving health outcomes for people with mental health disorders and optimizing the role of the nursing workforce in the delivery of mental health care. She is an assistant professor at the University of Pittsburgh School of Nursing and chair of the AcademyHealth Interdisciplinary Research Group on Nursing Issues. Karen B. Lasater program of research focuses on the impact of nursing on patient outcomes and measuring the value—in terms of outcomes and costs—of improving hospital nurse resources. She is an assistant professor at the University of Pennsylvania School of Nursing in the Center for Health Outcomes and Policy Research and a fellow of the American Academy of Nursing. References Author Manuscript Author Manuscript Aiken LH, Buchan J, Ball J, & Rafferty AM (2008). Transformative impact of magnet designation: England case study. Journal of Clinical Nursing, 17(24), 3330–3337. 10.1111/ j.1365-2702.2008.02640.x [PubMed: 19146592] American Nurses Credentialing Center. (n.d.-a). About magnet. Retrieved December 16, 2020, from https://www.nursingworld.org/organizational-programs/magnet/about-magnet/ American Nurses Credentialing Center. (n.d.-b). Find a magnet organization. American Nurse Credentialing Center. Barnes H, Rearden J, & McHugh MD (2016). Magnet® hospital recognition linked to lower central line-associated bloodstream infection rates. Research in Nursing & Health, 39(2), 96–104. 10.1002/ nur.21709 [PubMed: 26809115] Centers for Medicare & Medicaid Services. (2020a, January 6). Hospital readmissions reduction program (HRRP). Centers for Medicare & Medicaid Services. https://www.cms.gov/Medicare/ Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program Centers for Medicare & Medicaid Services. (2020b, January 6). Hospital-Acquired condition (HAC) reduction program. Centers for Medicare & Medicaid Services. https://www.cms.gov/Medicare/ Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/HAC-Reduction-Program Centers for Medicare & Medicaid Services. (2020c, January 6). The hospital value-based purchasing (VBP) program. Centers for Medicare & Medicaid Services. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/ValueBased-Programs/HVBP/Hospital-Value-Based-Purchasing Kutney-Lee A, Stimpfel AW, Sloane DM, Cimiotti JP, Quinn LW, & Aiken LH (2015). Changes in patient and nurse outcomes associated with magnet hospital recognition. Medical Care, 53(6), 550. 10.1097/MLR.0000000000000355 [PubMed: 25906016] Lake ET (2002). Development of the practice environment scale of the nursing work index. Research in Nursing & Health, 25(3), 176–188. 10.1002/nur.10032 [PubMed: 12015780] Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 11 Author Manuscript Author Manuscript Author Manuscript Author Manuscript Lake ET, Riman KA, & Sloane DM (2020). Improved work environments and staffing lead to less missed nursing care: A panel study. Journal of Nursing Management, 28(8), 2157–2165. 10.1111/ jonm.12970 [PubMed: 32017302] Lake ET, Sanders J, Duan R, Riman KA, Schoenauer KM, & Chen Y (2019). A meta-analysis of the associations between the nurse work environment in hospitals and 4 sets of outcomes. Medical Care, 57(5), 353–361. 10.1097/MLR.0000000000001109 [PubMed: 30908381] Lasater KB, Germack HD, Small DS,& McHugh MD(2016). Hospitals known for nursing excellence perform better on value based purchasing measures. Policy, Politics, & Nursing Practice, 17(4), 177–186. 10.1177/1527154417698144 Lasater KB, Jarrín OF, Aiken LH, McHugh MD, Sloane DM, & Smith HL (2019). A methodology for studying organizational performance: A multistate survey of front-line providers. Medical Care, 57(9), 742. 10.1097/MLR.0000000000001167 [PubMed: 31274782] Lasater KB, & Mchugh MD (2016). Nurse staffing and the work environment linked to readmissions among older adults following elective total hip and knee replacement. International Journal for Quality in Health Care, 28(2), 253–258. 10.1093/intqhc/mzw007 [PubMed: 26843548] Lu B, Greevy R, Xu X, & Beck C (2011). Optimal nonbipartite matching and its statistical applications. The American Statistician, 65(1), 21–30. 10.1198/tast.2011.08294 [PubMed: 23175567] Martsolf GR, Gibson TB, Benevent R, Jiang HJ, Stocks C, Ehrlich ED, Kandrack R, & Auerbach DI (2016). An examination of hospital nurse staffing and patient experience with care: Differences between cross-sectional and longitudinal estimates. Health Services Research, 51(6), 2221–2241. 10.1111/1475-6773.12462 [PubMed: 26898946] McHugh MD, Aiken LH, Eckenhoff ME, & Burns LR (2016). Achieving kaiser permanente quality. Health Care Management Review, 41(3), 178. 10.1097/HMR.0000000000000070 [PubMed: 26131607] McHugh MD, Berez J, & Small DS (2013). Hospitals with higher nurse staffing had lower odds of readmissions penalties than hospitals with lower staffing. Health Affairs, 32(10), 1740–1747. 10.1377/hlthaff.2013.0613 [PubMed: 24101063] McHugh MD, & Ma C (2013). Hospital nursing and 30-day readmissions among medicare patients with heart failure, acute myocardial infarction, and pneumonia. The Journal of Nursing Administration, 43(10 Suppl), S11. 10.1097/MLR.0b013e3182763284 [PubMed: 24022077] Nguyen T-L, Collins GS, Spence J, Daurès J-P, Devereaux P, Landais P, & Le Manach Y (2017). Double-adjustment in propensity score matching analysis: Choosing a threshold for considering residual imbalance. BMC Medical Research Methodology, 17(1), 1–8. 10.1186/ s12874-016-0277-1 [PubMed: 28056835] Pinkerton SE (2005). The financial return on magnet recognition. The Journal of Continuing Education in Nursing, 36(2), 51–52. 10.3928/0022-0124-20050301-01 [PubMed: 15835576] Shin S, Park J, & Bae S (2019). Nurse staffing and hospital-acquired conditions: A systematic review. Journal of Clinical Nursing, 28(23–24), 4264–4275. 10.1111/jocn.15046 [PubMed: 31464017] Silber JH, Rosenbaum PR, Trudeau ME, Even-Shoshan O, Chen W, Zhang X, & Mosher RE (2001). Multivariate matching and bias reduction in the surgical outcomes study. Medical Care, 39(10), 1048–1064. 10.1097/00005650-200110000-00003 [PubMed: 11567168] Sloane DM, Smith HL, McHugh MD, & Aiken LH (2018). Effect of changes in hospital nursing resources on improvements in patient safety and quality of care: A panel study. Medical Care, 56(12), 1001. 10.1097/MLR.0000000000001002 [PubMed: 30363019] Stimpfel AW, Sloane DM, McHugh MD, & Aiken LH (2016). Hospitals known for nursing excellence associated with better hospital experience for patients. Health Services Research, 51(3), 1120– 1134. 10.1111/1475-6773.12357 [PubMed: 26369862] Stuart EA (2010). Matching methods for causal inference: A review and a look forward. Statistical Science: A Review Journal of the Institute of Mathematical Statistics, 25(1), 1. 10.1214/09STS313 [PubMed: 20871802] Ulrich BT, Buerhaus PI, Donelan K, Norman L, & Dittus R (2007). Magnet status and registered nurse views of the work environment and nursing as a career. JONA: The Journal of Nursing Administration, 37(5), 212–220. 10.1097/01.NNA.0000269745.24889.c6 Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Dierkes et al. Page 12 Author Manuscript Author Manuscript Figure 1. Standardized bias plot summarizing matching performance across all covariates, highlighting the change in standardized mean differences between using all data and matched data. Author Manuscript Author Manuscript Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Author Manuscript Author Manuscript 258 (78) 252 (76) 755 (1,482) 249 (75) HHI, mean (SD) High-tech, N (%) Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. 0.27 (0.12) 1.79 (0.29) 8.33 (2.32) Disproportionate share, mean (SD) Case mix index, mean (SD) Nurse staffing, mean (SD) 100 (30) 99 (30) 49 (15) Midwest South West 52 (16) 104 (31) 100 (30) 75 (23) 8.12 (2.63) 1.76 (0.28) 0.27 (0.14) 1.05 (0.21) 49 (12) 19 (9.8) 0 (0.0) 7(2.1) 324 (98) 240 (73) 726 (1,170) 6 (1.8) 0.16 (0.30) 392 (322) 514 (20) 1,057 (42) 582 (231) 376 (15) 6.79 (2.64) 1.52 (0.28) 0.31 (0.17) 0.98 (0.21) 52 (14) 21 (13) 212 (8.4) 498 (20) 1,819 (72) 923 (37) 874 (1,598) 587 (23) 0.06 (0.17) 205 (191) 1,937 (77) 549 (22) 1,174 (46) 2,132 (84) 0.090 Non-Magnet hospitals (N = 2,529) Notes: Nurse staffing is registered nurse hours per patient day. Wage index is for fiscal year 2017. 83 (25) Northeast Region, N (%) 1.04 (0.19) Wage index, mean (SD) 19 (9) 50 (11) 1 (0.3) Rural % Medicaid pts., mean (SD) 10 (3.0) Micro % Medicare pts., mean (SD) 320 (97) Metro Core-based statistical area, N (%) 11 (3.0) 0.19 (0.37) Residents per bed, mean (SD) For-profit, N (%) 440 (297) Total hospital beds, mean (SD) Overall P4P 92 (28) 98 (30) HAC 163 (49) 134 (40) VBP 264 (80) 0.287 280 (85) 0.314 Matched controls (N = 331) HRRP Penalties, N (%) Propensity score Magnet® hospitals (N = 331) 563 (20) 1,156 (40) 682 (24) 459 (16) 6.97 (2.65) 1.55 (0.30) 0.31 (0.17) 0.99 (0.21) 52 (13) 21 (12) 213 (7.5) 508 (18) 2,139 (75) 1,172 (41) 860 (1,585) 598 (21) 0.07 (0.21) 232 (219) 2,189 (77) 647 (23) 1,308 (46) 2,412 (84) n/a All hospitals (N = 2,860) −0.16 −0.26 0.17 0.24 0.66 0.93 −0.32 0.33 −0.21 −0.21 −1.47 −0.97 1.38 −0.90 −0.08 −1.11 0.36 0.79 1.04 Prematch n/a −0.03 −0.03 <0.01 0.06 0.09 0.11 0.05 −0.01 −0.01 0.06 0.06 −0.05 −0.07 −0.07 0.02 0.08 0.09 0.16 0.12 Postmatch Standardized mean differences Author Manuscript Hospital Characteristics and Performance on P4P Programs, Before and After Matching. Author Manuscript Table 1. Dierkes et al. Page 13 Author Manuscript Author Manuscript Author Manuscript Author Manuscript Standardized mean differences approach zero as the quality of the match improves. SD = standard deviation; HHI = Herfindahl-Hirschman Index; P4P = Pay for Performance; HRRP = Hospital Readmissions Reduction Program; VBP = Value- Based Purchasing; HAC = Hospital-Acquired Conditions Reduction Program; n/a, not applicable; pts., patients. Dierkes et al. Page 14 Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22. Author Manuscript Author Manuscript Author Manuscript 0.70* (0.52–0.95) 1.09 (0.78–1.53) 0.79* (0.62–0.99) 1.52** (1.18–1.96) 0.97 (0.74–1.28) HAC Overall P4P 1.02 (0.71–1.46) 0.75 (0.50–1.11) 0.66* (0.48–0.91) 0.66* (0.48–0.92) 1.40 (0.89–2.19) 1:1 Matched (N = 662) 0.81 (0.60–1.10) 0.58*** (0.44–0.76) 1.18 (0.81–1.70) Unmatched (N = 2,860) Adjusted p < .001. *** p < .01 p < .05 ** * Notes: Coefficients represent the change in odds of a penalty under each individual program (HRRP, VBP, and HAC) and in aggregate across all three programs (overall P4P) associated with Magnet versus non-Magnet hospitals. Hospital covariates include technology status, percent Medicare/Medicaid patients, core-based statistical area, hospital ownership, Herfindahl–Hirschman Index, residents per bed, total hospital beds, case mix index, disproportionate share, wage index, registered nurse hours per adjusted patient day, and U.S. census region. P4P = Pay for Performance; HRRP = Hospital Readmissions Reduction Program; VBP = Value-Based Purchasing; HAC = Hospital-Acquired Conditions Reduction Program. 0.90 (0.63–1.30) 1.40 (0.93–2.08) 1.02 (0.74–1.40) VBP 1:1 Matched (N = 662) HRRP Unmatched (N = 2,860) Unadjusted Unadjusted and Adjusted Logistic Regression Models, Before and After Matching of the Association Between Magnet® Status and P4P Program Penalties. Author Manuscript Table 2. Dierkes et al. Page 15 Policy Polit Nurs Pract. Author manuscript; available in PMC 2022 August 22.
 0
0
advertisement
Related documents




Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users