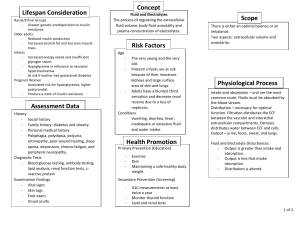
Fluid and Electrolytes ● Electrolytes: what your body craves! ● Both are important for homeostasis ○ differences in age can affect electrolyte balance ■ Men typically have more water content ■ the older you get, the less water content you have ● older adults are at higher risk for dehydration ○ sometimes due to decreased thirst reflex ● Fluid Compartments ○ Intracellular has most of the body’s water ● Electrolytes ○ Sodium, potassium, magnesium, calcium, and chloride are the most important ● Fluids ○ fluid shifts can cause edema ■ hydrostatic pressure forces fluid into tissue ○ Fluid spacing ■ 1st: fluid in vessels ■ 2nd: edema starts ■ 3rd: Fluid retained in areas that don’t easily xchng with circulation ○ Regulation ■ pituitary ● excretes ADH ■ heart releases BNP which tell kidneys to remove more fluid ■ GI: vomit and diarrhea can cause dehydration ■ Renin angiotensin cycle ■ ■ ○ Elderly have reduced kidney function, cannot maintain fluid balance as effectively ■ Burns can cause fluid loss ■ CHF can cause fluid issues Hypovolemia: Dehydration ■ bleeding, changes due to aging, etc can decrease fluid levels ■ assessments ● cardiac: ○ tachy ○ low bp ○ flat veins ● resp ○ increased r rate ● skit ○ tenting ○ chapped lips, sticky tongue ● neuto ○ confused ○ restless ● renal ○ decreased output ● LABS ○ ■ hematocrit is elevated ■ more RBC per volume serum osmolarity is inc protein, BUN, and creatinine may be inc ○ ○ Interventions ● Fluids ○ IV ○ PO ■ ● ○ do not do too much, can cause problems Monitor ○ MAP: (diastolicx2)/systolic ■ http://www.cvphysiology.com/Blood%20Pressure/B P006.htm ■ not on exam ○ BP ○ CVP: fluid returning to rt side of heart ■ not on exam ○ Lab tests ■ electrolytes, BUN, etc Hypervolemia: fluid overload ■ kidney failure, CHF (HF) can be causes ■ Assessment ● cardiac: ○ elevated BP ○ distended veins ○ edema ○ bounding pulses ● Resp ○ crackles ○ coughs ● GU ○ possibly urinary output ● Etc ○ Weight gain ■ Interventions ● daily weight ● dietary changes ○ salt restrictions ■ Treatments ● diuretics ○ lasix: loop diuretic ■ blocks absorption of Na in loop of Henle ■ Watch K+ levels. Does not spare K+ ○ ○ ○ ○ ■ Assess BP before administration Bumex ■ Loop diuretic ■ more potent than Lasix ● used more in emergency situation, prior to Lasix ■ assess the same as Lasix ■ administer IV Mannitol ■ Osmotic diuretic ■ usually given to reduce CSF pressure ■ Use a filter Albumin ■ protein found in plasma, controls osmotic pressure ■ pulls fluid from tissue into vessels so you can pee it out ■ losing favor in practice ■ is considered a blood product, even though it is synthetic Electrolytes ■ Na+, K+, Ca+, Mg+ ■ Sodium ● 135-145 mEq/L ● Uses ○ nerve impulses ○ muscle contraction ● Hypo ○ caused by diuretics, NG suctioning, burns, vomit, excessive water gain. Also caused by inadequate intake r/t anorexia or alcoholism ○ problems: ■ disturbed neuro function ● confusion ● irritability ● confusion ● convulsions ○ Interventions ■ I&Os ■ iso/hypertonic infusions ■ restrict PO fluid intake ■ increase sodium intake ● careful of pt with HF ■ Notify MD if level is <130 ● ● ■ that’s where neuro stuff gets bad Hyper ○ >145 mEq/L ○ causes: ■ too much salt intake, hypertonic infusions (TPN sometimes) ■ Water loss: diarrhea, vomit, diuretics ○ signs ■ confusion, dec LOC, seizure, coma ■ muscle twitching ■ increased BP ○ Interventions ■ Weight ■ I&Os ■ hypotonic infusions ● D5 .45NS ■ reduce salt intake ■ monitor labs Potassium ● 3.5-5.0 mEq/L ● Functions: ○ action potentials ○ protein synth ● regulations ○ excreted through kidney ● Hypo ○ <3.5mEQ/L ○ causes: ■ anorexia, burns, diuretics ○ signs ■ Resp ● low RR, shallow breathing ■ MS ● cramps, weakness ■ CV ● dec BP, ST depression, inverted T wave ● always have pt on a monitor ■ Neuro ● lethargy, coma ○ Interventions ■ reduce any meds that might be causing it ■ do not infuse K >100 mEQ/L ● faster can cause hyperkalemia ■ ● ■ Digoxin + K+ can cause all kinds of interactions ● monitor for neuro changes and muscle weakness Hyperkalemia ○ >5 mEq/L ○ causes ■ excessive intake, renal failure, bowel obstruct, potassium sparing diuretics, addison's disease, burns, trauma ○ Signs ■ CV: ● dec HR and BP, EKG changes ■ CNS ● irritability, confusion, tingling ■ MS ● muscle weakness ○ Interventions ■ Kayexalate ● oral or rectal ■ insulin or glucose can temporarily help ■ diuretics Calcium ● 9.0-10.5 mg/dL ● uses: ○ bones and teeth ○ neuromuscular conduction ○ blood clotting ○ cardiac contraction ● total calcium ○ all calcium, not readily available ● ionized calcium ○ what calcium the body can use at that time ● high Ca usually means low phos level ● Hypocalcemia ○ <9 mg/dl ○ causes ■ blood transfusion, inadequate intake, vampirism, pancreatitis, thyroid/parathyroid issues ○ signs ■ MS ● trousseau’s and chvostek’s signs, muscle cramps, fracture ■ CNS ● ■ CV ● bleeding, cardiac arrest, ecchymosis interventions ■ Ca gluconate ■ watch labs ■ fall risk and seizure precautions ● Hypercalcemia ○ >10.5 mg/dL ○ causes ■ immobilization ■ increase of intake ○ signs ■ decr deep tendon reflexes, CNS issues ○ interventions ■ diuretics, citrate, phosphorus ■ avoid Ca supplements ■ prevent falls ■ ambulation Phosphorus ● 3.0-4.5 mg/dL ● Uses ○ bones, teeth ○ activates vitamins ○ cell growth and metabolism ● Hypophosphatemia ○ <3 ○ causes ■ dec intake, starvation, antacid use, renal failure ○ signs ■ dec HR and BP ■ Irritability - most common ■ CNS symptoms most common ○ interventions ■ stop antacid and diuretic use, adjust diet ■ seizure precautions ■ cardiac monitor ● Hyper ○ >4.5 ○ causes ■ inc intake, renal issues ○ signs ■ looks like hypocalcemia ○ ■ confusion ○ ■ ○ interventions ■ Ca gluconate, seizure and fall prevention Magnesium ● 1.3-2.1 mg/dL ● aides in absorption of potassium, levels go hand in hand ● uses ○ muscle contraction ○ ATP formation ○ vasodilation in periph arteries ● regulation ○ filtered thru kidneys ● Hypomagnesemia ○ <1.3 mg/dL ○ causes ■ malnutrition, impaired absorption ○ signs ■ confusion, memory loss ■ Cardiac Torsades ○ interventions ■ Mg via IV ■ inc Mg intake ■ seizure precautions ■ avoid use of diuretics and laxative ● Hypermagnesemia ○ causes ■ excessive intake, laxatives, renal failure ○ signs ■ decreased membrane excitability ■ lethargy, coma ○ interventions ■ prevent intake of magnesium ■ fall precautions ■ monitor pt ■ Chloride ● 98-106 mEq/L ● uses ○ acid base balance ○ form gastric acid ○ too much can send pt into acidotic state IV fluids ■ isotonic ● stays in vessels ■ hyper ■ ■ ● ● hypo ● Types ● ● pulls water from cells into vessels more likely to cause phlebitis or burning, especially Na+ pulls water from vessels into tissue crystalloid ○ NS, dextrose, LR colloids ○ albumin, dextran, hetastarch, mannitol