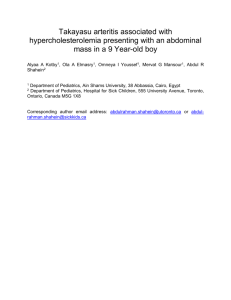
JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 81, NO. 2, 2023 ª 2023 THE AUTHORS. PUBLISHED BY ELSEVIER ON BEHALF OF THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION. THIS IS AN OPEN ACCESS ARTICLE UNDER THE CC BY-NC-ND LICENSE (http://creativecommons.org/licenses/by-nc-nd/4.0/). JACC FOCUS SEMINAR: TROPICAL MEDICINE JACC FOCUS SEMINAR Takayasu Arteritis JACC Focus Seminar 3/4 George Joseph, DM,a Ruchika Goel, DM,b Viji S. Thomson, DM,a Elizabeth Joseph, DNB,c Debashish Danda, DMb ABSTRACT Takayasu arteritis is a rare idiopathic large-vessel vasculitis that typically affects young women. An early "prepulseless" stage is often missed, associated with nonspecific constitutional symptoms (fever, malaise, and weight loss) and elevated inflammatory markers. Unchecked disease progression leads to the "pulseless" stage, manifest clinically by missing pulses, vascular tenderness, and ischemic symptoms (limb claudication, dizziness, angina, and renovascular hypertension), and is characterized pathologically by arterial wall thickening and stenotic/occlusive lesions or aneurysm formation. Vascular complications (stroke, blindness, heart failure, and aneurysm rupture) could follow unless disease progression is halted by immunosuppressive therapy and critical lesions are palliated by timely endovascular therapy or open surgery. Early diagnosis, effective therapy, and lifelong surveillance for disease activity relapses and vascular disease progression are critical to successful long-term outcomes. The outlook for patients has improved significantly in recent years with the establishment of diagnostic and classification criteria, better investigational modalities, and more effective medical and invasive therapy. (J Am Coll Cardiol 2023;81:172–186) © 2023 The Authors. Published by Elsevier on behalf of the American College of Cardiology Foundation. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). T akayasu arteritis (TAK) is a chronic idiopathic been made in managing TAK, and the outlook for pa- granulomatous large-vessel vasculitis that tients with TAK has improved significantly. The aim affects the aorta, its main branches, and pul- of the present review was to provide a synopsis of monary arteries. It typically affects young women and the current status of TAK and its management. is often not diagnosed until late in the disease because of its rarity, often indolent course, nonspe- HISTORICAL PERSPECTIVE cific early symptoms, and lack of specific diagnostic Listen to this manuscript’s markers. Uncontrolled disease progression leads to TAK is eponymous with Mikito Takayasu, professor of the formation of obstructive and aneurysmal vascular ophthalmology at Kanazawa University, Japan, who lesions, which can result in crippling morbidities such described wreath-like anastomoses in the retinal as stroke, blindness, refractory hypertension, heart vasculature of a 21-year-old woman at the Annual failure, and death. Chronicity of the disease and Meeting of the Japanese Ophthalmology Society in frequent need for long-term immunosuppressive 1905. At the same meeting, 2 other ophthalmologists, therapy create the challenges of lifelong surveillance, Katsutomo Onishi and Tsurukichi Kagoshima, pre- medication side effects, poor quality of life, and the sented cases with similar eye findings and noted burdens of loss of productivity and recurring medical missing radial pulses as well. 1 In 1940, Kunio Ohta expenses. Nevertheless, much recent progress has confirmed that TAK is a panarteritis and that the audio summary by Editor-in-Chief Dr Valentin Fuster on www.jacc.org/journal/jacc. From the aDepartment of Cardiology, Christian Medical College, Vellore, India; bDepartment of Clinical Rheumatology, Christian Medical College, Vellore, India; and the cDepartment of Radiology, Christian Medical College, Vellore, India. The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the Author Center. Manuscript received August 19, 2022; revised manuscript received September 6, 2022, accepted September 21, 2022. ISSN 0735-1097 https://doi.org/10.1016/j.jacc.2022.09.051 JACC VOL. 81, NO. 2, 2023 Joseph et al JANUARY 17, 2023:172–186 Takayasu Arteritis EPIDEMIOLOGY HIGHLIGHTS ABBREVIATIONS AND ACRONYMS Early Takayasu arteritis often goes undiagnosed because clinical features are nonspecific, but progression is associated with obstructive or aneurysmal lesions. Immunosuppressive medication is needed to arrest progression of disease, and invasive therapy may be needed to palliate critical vascular lesions. Early diagnosis, effective therapy, and continued surveillance are essential to successful long-term outcomes. TAK has a worldwide, but heterogeneous, distribution, generally more common among Asian populations. 3,4 A recent systematic re- CTA = computed tomography angiography cases per million and an annual incidence of DMARD = disease-modifying 0.4 to 2.6 cases per million.4 Female preponderance is characteristic of TAK, but antirheumatic drug ET = endovascular therapy female-to-male ratios vary from 12:1 in Turkey EULAR = European League to 3:1 in China and India.3,5 Patients experi- Against Rheumatism ence onset of disease with TAK usually be- HLA = human leukocyte tween 20 and 30 years of age, but onset after antigen the age of 40 years is not uncommon, varying IL = interleukin 3 MRA = magnetic resonance angiography characteristic optic fundal finding resulted from ischemia due to obstructed cervical arteries. The AECA = antiendothelial cell antibody view found a global prevalence of 3.2 to 40.0 from 9% to 32%. TAK = Takayasu arteritis PATHOLOGY name “Takayasu arteritis” for this disease was accepted at the 2012 revised International Chapel Hill TAK is a panarteritis, but the initial site of inflam- Consensus Conference on the nomenclature of mation is around the vasa vasorum and at the medio- vasculitides.2 adventitial junction. 6 In the early phase, the active F I G U R E 1 Proposed Immunopathogenesis of Takayasu Arteritis Putative antigen triggers Exogenous: Mycobacterium tuberculosis Endogenous: Heat-shock protein-60 Dendritic cell stimulation Y ↑Toll-like receptor expression ↓ Programmed cell death ligand-1 expression Macrophage Monocyte JAK PD1 Immune cell infiltration Abnormal adventitial dendritic cell Vasa vasorum Macrophages and other cells Y Interleukin-6, -12, -18, -23, -1β T cell activation T cell B cell survival factors Interleukin-6, -18 PDGF, VEGF B cell CD8+ Anti-endothelial cell antibody Perforin, Granzymes mTOR pathway 173 Th1 Th17 Interleukin-6, -17, -22, -23 NK cell Interferon-γ Matrix metalloproteinase2, -3, -9 Tumor necrosis factor-α Granuloma formation Endothelin-1 Endothelial cell activation Intimal proliferation Neo-angiogenesis Vascular smooth muscle cell proliferation and fibrosis Activation by unknown antigens of inherently abnormal adventitial dendritic cells causes cytokine release that drives T-cell differentiation into cytotoxic CD8þ T cells, T helper 1 (Th1) cells, and T helper 17 (Th17) cells. Cytotoxic cells release the cytotoxic proteins perforin and granzymes. The Th cells are vasculitogenic, rich in programmed cell death protein-1 (PD1), with increased Janus kinase (JAK)-signal transducer and activator of transcription proinflammatory signaling. The resultant immune cell infiltration leads to endothelial cell activation, intimal and vascular smooth muscle cell proliferation, and fibrosis. Interferon-g released by natural killer (NK) cells contributes to granuloma formation. Matrix metalloproteinases released by inflammatory macrophages also contribute to granuloma formation and cause digestion and leakiness of the endothelial barrier. B cells promote endothelial cell activation by secreting antiendothelial cell antibodies. mTOR ¼ mammalian target of rapamycin; PDGF ¼ platelet-derived growth factor; VEGF ¼ vascular endothelial growth factor. 174 Joseph et al JACC VOL. 81, NO. 2, 2023 Takayasu Arteritis JANUARY 17, 2023:172–186 genome-wide level of significance (P < 5 10–8 ) were T A B L E 1 American College of Rheumatology 1990 Classification Criteria for found in the HLA region and elsewhere. 9 Two non- Takayasu Arteritis HLA genetic loci, IL12B encoding for the common Definition Age at disease onset <40 y Development of symptoms or findings related to Takayasu arteritis at age <40 y Claudication of extremities Development and worsening of fatigue and discomfort in muscles of 1 or more extremities while in use, especially the upper extremities Decreased brachial artery pulse Decreased pulsation of 1 or both brachial arteries Blood pressure difference >10 mm Hg Difference of >10 mm Hg in systolic blood pressure between the arms Bruit over subclavian arteries or aorta Bruit audible on auscultation over 1 or both subclavian arteries or abdominal aorta Arteriogram abnormality Arteriographic narrowing or occlusion anywhere in the aorta, its primary branches, or large arteries in the proximal upper or lower extremities, not due to arteriosclerosis, fibromuscular dysplasia, or similar causes; changes usually focal or segmental p40 subunit of interleukin (IL)-12 and IL-23, and MLX, have synergistic effects with the allele HLA-B*52:01, increasing TAK susceptibility.10 Similarly, IL6, encoding the pro-inflammatory cytokine IL-6, has been identified as a genetic susceptibility locus for TAK surpassing genome-wide level of significance.8 PATHOGENESIS Large-sized and medium-sized arteries are largely immune-privileged sites. Vascular dendritic cells in the proximity of the vasa vasorum act as gatekeepers, limiting the access of lymphoid cells and blunting immune-inflammatory responses (Figure 1).11 Im- A patient is said to have Takayasu arteritis if at least 3 of these 6 criteria are present. Adapted with permission from Arend et al.17 mune tolerance is breached by activation of inherently abnormal dendritic cells, which have lower expression of regulatory receptors such as pro- inflammatory component and necrotizing character are conspicuous. 7 Mononuclear cell infiltration (lymphocytes, histiocytes, and plasma cells) and edema are seen.6,7 Fragmentation of elastic fibers is prominent, and giant cell granulomatous reaction and laminar medial necrosis may occur. 6 Later, there is reactive fibrosis and increased ground substance in the intima, with overlying mural thrombus and a band of neovascularization at the intimal medial junction. Rapid or more severe inflammation leads to loss of smooth muscle cells, medial weakening, vascular dilatation, and aneurysm formation. In the healed phase, the adventitial fibrosis and scarring along with laminar medial necrosis are more impressive, although lymphoplasmacytic inflammation and multinucleated giant cells also persist.7 The adventitial and periadventitial fibrosis observed in TAK exceeds that seen in any other inflammatory disorder of the aorta.6 grammed cell death ligand-1 and overexpression of surface Toll-like receptors. Exposure to yet unknown stimuli results in the maturation of dendritic cells leading to the release of cytokines, including IL-12, IL-23, and IL-1 b, and an influx of activated vasculitogenic T cells into the adventitia and media. The vascular topography of TAK may be linked to differential expression of Toll-like receptors along the arterial tree; binding of ligands to different Toll-like receptors activates arterial wall–integrated dendritic cells to initiate and promote T effector cell accumulation and distinct types of vasculitis.12 The cellular infiltrate contains macrophages, T helper 1 and T helper 17 cells, CD8 þ T cells, gd T cells, natural killer cells, and neutrophils. 13 Release of growth factors leads to wall edema, extracellular matrix deposition, and the proliferation of myofibroblasts that invade the intima, ultimately leading to arterial stenosis. Arterial dilatation can also occur, caused by excessive local release of toxic reactive oxygen species and GENETICS matrix metalloproteinases by macrophages, resulting in degeneration and thinning of the tunica media, The etiology of TAK involves a complex genetic death of vascular smooth muscle cells, and disruption contribution, which includes genes encoding human of elastin.11 leukocyte antigen (HLA) class I and class II specificities, immune response regulators, and Molecular mimicry between a host and a microbial proin- heat shock protein (hsp60 and hsp65, respectively) flammatory cytokines, all of which relate to known may drive immune responses in TAK; it is hypothe- processes involved in TAK pathogenesis; the most sized that an unknown stimulus triggers heat shock robust genetic signal comes from HLA-B*52, which protein and major histocompatibility complex class I has been confirmed in several ethnicities.8 A recent chain-related A expression in aortic tissue; the latter meta-analysis of patients with TAK from 5 different is recognized by specific gd T cells and natural killer populations provides data suggesting additional ef- cells, leading to their releasing perforins, granzymes, fects beyond HLA-B*52 in TAK; multiple genetic loci and pro-inflammatory cytokines, resulting in acute with independent association with the disease and vascular inflammation. 13 JACC VOL. 81, NO. 2, 2023 Joseph et al JANUARY 17, 2023:172–186 Takayasu Arteritis T A B L E 2 Modified Ishikawa Criteria for Diagnosis of Takayasu Arteritis Brief Description Major criteria 1. Left mid-subclavian artery lesion Most severe obstruction between points 1 cm proximal and 3 cm distal to the left vertebral artery ostium 2. Right mid-subclavian artery lesion Most severe obstruction between the right vertebral artery ostium and a point 3 cm distal to it 3. Characteristic signs and symptoms of at least 1 mo duration Limb claudication, pulselessness or pulse differences in limbs, unobtainable BP or systolic BP difference >10 mm Hg in limb, fever, neck pain, transient amaurosis, blurred vision, syncope, dyspnea, or palpitations Minor criteria 1. High ESR Unexplained ESR >20 mm/h at diagnosis or evidence in patient’s history 2. Carotid artery tenderness Unilateral or bilateral common carotid artery tenderness 3. Hypertension Persistent BP >140/90 mm Hg brachial/>160/90 popliteal 4. Aortic regurgitation or annulo-aortic ectasia By auscultation, Doppler/2-dimensional echocardiography, or angiography 5. Pulmonary artery lesion Lobar or segmental arterial occlusion on angiography or perfusion scintigraphy, or presence of stenosis, aneurysm, luminal irregularity on angiography 6. Left mid-common carotid lesion Most severe obstruction in the 5-cm length from a point 2 cm distal to its ostium 7. Brachiocephalic trunk lesion Most severe obstruction in the distal third 8. Descending thoracic aorta lesion Narrowing, dilation or aneurysm, luminal irregularity; tortuosity alone is unacceptable 9. Abdominal aorta lesion Narrowing, dilation or aneurysm, luminal irregularity 10. Coronary artery lesion Documented before age 30 y, absence of risk factors such as hyperlipidemia or diabetes mellitus The presence of 2 major or 1 major and 2 minor or 4 minor criteria suggests a high probability of Takayasu arteritis. Adapted from Sharma et al.18 BP ¼ blood pressure; ESR ¼ erythrocyte sedimentation rate. F I G U R E 2 Computed Tomography Angiography in a 26-Year-Old Woman With Takayasu Arteritis Sagittal (A) and coronal (B) images show markedly irregular descending aortic luminal outline, calcification (yellow arrows), and wall thickening (blue arrows). Early (C) and delayed (D) acquisition of corresponding axial images shows a mural double ring in the latter, consisting of an inner poorly enhancing (dark) rim representing hyperplastic intima, and an outer late-enhancing (bright) rim (red arrow) representing vasa vasorum neoangiogenesis in the media and adventitia. 175 176 Joseph et al JACC VOL. 81, NO. 2, 2023 Takayasu Arteritis JANUARY 17, 2023:172–186 F I G U R E 3 Numano Angiographic Classification System for Takayasu Arteritis Shaded areas represent regions of arterial involvement by the disease process. Adapted from Hata et al.20 antibodies (Table 1) to help create homogeneous groups for (AECAs) have been documented in TAK, indicating a Antiaorta and antiendothelial cell research studies, which limits its applicability to role for B cell–mediated autoimmunity. 13 The target clinical practice; age <40 years at onset was 1 of 6 autoantigens of AECAs have recently been identified criteria proposed. Both sets of criteria have been using a complementary DNA–based expression clon- criticized for their age restriction and low sensitivity ing system.14 Endothelial protein C receptor and in TAK patients with predominant aortic involve- scavenger receptor class B type 1 were identified as ment.18 In 1995, modifications (Table 2) to the Ishi- endothelial antigens targeted by AECAs; these anti- kawa diagnostic criteria were proposed, including gens act as negative regulators of endothelial activa- removing the age criterion, which increased the tion, but when AECAs block their function, a sensitivity proinflammatory phenotype results. respectively. and specificity to 92.5% and 95%, Accelerated atherosclerosis may occur in TAK due to a combination of direct vascular and systemic IMAGING AND ANGIOGRAPHIC CLASSIFICATION inflammation, traditional risk factors, and treatment effects and may contribute to cardiovascular adverse events. 15 Initial vascular imaging in TAK is usually performed by using computed tomography angiography (CTA), which, in addition to being widely available and less DIAGNOSIS expensive, provides better image resolution than magnetic resonance angiography (MRA). CTA reveals Ishikawa16 proposed the first diagnostic criteria for luminal narrowing and dilatation and changes in the TAK in 1988, with age <40 years at diagnosis or onset vessel wall such as wall thickening, calcification, of characteristic symptoms/signs as an obligatory and contrast enhancement 19 (Figure 2). The site criterion. In 1990, the American College of Rheuma- and extent of arterial involvement in TAK are highly tology proposed classification criteria for TAK 17 variable, making angiographic classification JACC VOL. 81, NO. 2, 2023 Joseph et al JANUARY 17, 2023:172–186 Takayasu Arteritis desirable. The most widely used angiographic classification scheme for TAK is the Numano system 177 T A B L E 3 Clinical Manifestations of Takayasu Arteritis According to Vascular Region Affected (Figure 3), which defines 6 types of TAK based on the Symptoms and Signs topography of arterial lesions; coronary and pulmonary artery involvement are separately designated Cþ and Pþ, respectively.20 The Numano classification system has improved reporting standards of TAK and has helped reveal ethnic differences in arterial lesion distribution; however, its formulation was empirical General Constitutional symptoms Fatigue, low-grade fever, night sweats, weight loss >2 kg Other symptoms of active disease Myalgia, arthralgia, arthritis, abdominal pain Vascular involvement Weak or missing pulses, vascular bruit, vascular tenderness Specific and not evidence based. Carotid arteries Dizziness, amaurosis fugax, vision loss, transient ischemic attacks, stroke CLINICAL FEATURES Subclavian arteries Arm claudication, inter-arm blood pressure difference >10 mm Hg. Proximal subclavian obstruction can cause subclavian steal Clinical manifestations of TAK vary depending on the Vertebral arteries Stenosis/occlusion can cause vertigo or contribute to cerebral ischemic symptoms when multiple arch branches are obstructed Ascending and arch of aorta Aortic regurgitation due to aortic dilatation, aneurysm, rarely aorta stenosis Descending aorta Systemic hypertension, dyspnea, and heart failure due to aorta stenosis, aneurysm stage of the disease and the vascular region involved (Table 3). Clinical features progress through 2 stages, although not all patients conform to this pattern: Stage I is the “prepulseless” phase, characterized by constitutional symptoms, which are seen in <50% of Abdominal aorta Systemic hypertension, lower limb claudication, aneurysm patients.21 Stage II is the “pulseless” phase marked by Renal arteries Systemic hypertension, renal failure symptoms and signs of vascular inflammation and Mesenteric arteries Postprandial abdominal pain, weight loss, sitophobia, gastrointestinal hemorrhage ischemia. A “fibrotic” third stage has been described,11,22 which is burnt-out disease void of inflammation and presents with complications Iliac and femoral arteries Lower limb claudication or fatigue Coronary arteries Angina, heart failure, myocardial infarction Pulmonary arteries Dyspnea, cough, chest pain, pulmonary hypertension resulting from vascular damage. Very few patients present in the third stage, and progression through all 3 stages (triphasic pattern) is observed in only 19% of Adapted with permission from Kim ESH, Beckman J. Takayasu arteritis: challenges in diagnosis and management. Heart. 2018;104:558-565. patients.22 Clinical features seen in different ethnic groups are presented in Table 4. White and East Asian At our center, relapse within 5 years was 34%, whereas patients tend to have more arch branch involvement a persistent complete response to treatment (no re- and higher age at presentation. South Asian patients lapses at any time) was obtained in 46%; 6% of patients tend to present earlier, with a lower female propor- were refractory to therapy, with persistently active tion and more abdominal aorta involvement. Mexican and progressive disease.25 Disease activity states patients also present early and have the most type V defined by the European League Against Rheumatism disease. (EULAR) 26 are presented in Table 5. NATURAL HISTORY DISEASE ACTIVITY ASSESSMENT The natural history of TAK is highly variable. In 1996, Assessment of disease activity is essential in diag- Ishikawa23 described 4 patterns of clinical symptoms nosis, prognostication, tailoring of immunosuppres- from their onset to the point where the diagnosis was sive first made: A, plateau; B, decrescendo; C, decrescendo- assessment is therefore required repeatedly in the plateau-crescendo; and D, plateau-crescendo. Subse- management of patients with TAK. Disease activity quent 12-year survival was 91% with patterns A and B, determined by clinical assessment and acute-phase and 70% with patterns C and D. With the widespread reactant levels correlates poorly with activity seen use of immunosuppressive therapy in the past few in biopsy specimens; also, the appearance of new decades, most available data on the natural history of arterial lesions was observed in 61% of patients the disease are in treated patients. Kerr et al 21 found thought to be inactive. 21 Nowadays, imaging infor- that 20% of patients had a monophasic self-limiting mation is combined with clinical and laboratory data disease and did not require immunosuppressive to improve disease activity assessment. In 1994, treatment; in the remainder who did, remission could Kerr 21 defined active disease with a 4-category system not be induced in one-quarter, and about one-half of that has been widely used (Table 6). The advantages those who achieved remission later relapsed. Comar- of this system are its simplicity, composite nature, mond et al24 found that 41% of patients in remission and inclusion of angiographic information; however, experience a relapse of disease activity within 5 years. it has not been validated, and cut-off levels of therapy, and timing of invasive therapy; 178 Joseph et al JACC VOL. 81, NO. 2, 2023 Takayasu Arteritis JANUARY 17, 2023:172–186 MEDICAL THERAPY T A B L E 4 Clinical Features of Takayasu Arteritis in Various Geographic Regions Country Advances in medical therapy for TAK have contrib- United States Japan India Mexico uted significantly to the marked decline in mortality Schmidt et al43 Watanabea Danda et al5 Sotob and improved quality of life in patients with TAK over 1984-2009 2001-2011 1998-2017 1976-2003 the last 2 decades. These advances include up-front 126 1,372 602 110 82.5% White East Asian South Asian Mestizo Age at onset, y, median (IQR) or mean SD 29 (15) 35 (35) 26 (12) 26 9 Proportion with age at onset >40 y 25 43 10 9 91 84 77 85 I 20 28 19 19 treat-to-target approach in TAK. Judicious use of IIa 6 16 5c 3 invasive therapy after controlling disease activity has IIb 7 17 -c 4 also improved outcomes. III 5 7 5 4 IV 5 6 16 2 EMPHASIS ON LOWER DOSES OF CORTICOSTEROID. V 57 26 49 69 Fatigue/malaise 54 14 32 30 Fever 29 35 19 20 remission rates as high as 60%.21 However, the asso- Neck pain 15 10 6 21 ciated side effects and frequent progression of dis- Headache 45 8 21 70 ease or relapse while on glucocorticoid monotherapy Dizziness/light-headedness 49 9 6 55 have prompted efforts to reduce dependence on Upper limb claudication 40 66 52d NA 18 10 -d glucocorticoids. An effective Lower limb claudication NA Author Period of study N Ethnicity of patients Female proportion Numano angiographic types 20 Chest pain 6 2 12 32 Systemic hypertension 38 39 53 53 use of synthetic disease-modifying antirheumatic drugs (DMARD) during the initial induction regimen, better DMARDs, and lower doses of steroids. In addition, the formulation of disease activity scoring systems such as the activity version of the Indian Takayasu Clinical Activity Score has enabled a Glucocorticoid monotherapy has been the cornerstone of medical therapy in TAK in the past, achieving strategy has been combining lower initial and cumulative glucocorticoid doses with DMARDs. Renal impairment NA 11 8 28 DMARDs Aortic regurgitation NA 33 7 41 DMARDs are currently available (Table 7). DMARDs Cerebrovascular accidents 11 5 8 9 are classified as synthetic or biologic. Synthetic a Values are % unless otherwise specified. Watanabe Y, Miyata T, Tanemoto K. Current clinical features of new patients with Takayasu arteritis observed from cross-country research in Japan: age and sex specificity. Circulation. 2015;132:1701-1709. bSoto ME, Espinola N, Flores-Suarez LF, Reyes PA. Takayasu arteritis: clinical features in 110 Mexican Mestizo patients and cardiovascular impact on survival and prognosis. Clin Exp Rheumatol. 2008;26(3 suppl 49):S9-S15. cNumano angiographic types IIa and IIb combined is 5% (separate data is not available). dUpper and lower limb claudication combined is 52% (separate data is not available). NA ¼ data not available. AND THEIR EFFECTS. Several effective DMARDs can be conventional (eg, methotrexate, azathioprine, mycophenolate, leflunomide, cyclophosphamide) or targeted (eg, the novel Janus kinase inhibitor tofacitinib, which blocks proinflammatory cytokine signaling). Biologic DMARDs target IL-driven pathways (eg, tocilizumab, an anti–IL-6 receptor individual items are not specified. The Indian antibody) or inhibit tumor necrosis factor-alpha (eg, Takayasu Clinical Activity Score and its activity infliximab, etanercept, adalimumab). Biologic are also composite scores to assess disease DMARDs are usually reserved for refractory cases or activity that additionally allow grading of disease when rapid control of disease activity is required. A version 27 activity and incorporate cardiovascular weighting. recent extensive meta-analysis29 summarized the ef- However, it does not include imaging data; it is fects of DMARDs (Table 8). Biologic DMARDs are more widely used during follow-up of patients with TAK. effective than conventional synthetic DMARDs in F-fluorodeoxyglucose positron emission tomogra- inducing remission, stabilizing vascular disease, and phy co-registered with computed tomography imag- reducing inflammation; however, they are associated 18 ing identifies enhanced metabolic activity in the with more relapses, adverse events, and infections. arterial wall and may improve diagnostic accuracy CURRENT IMMUNOSUPPRESSIVE DRUG STRATEGIES and influence therapeutic decisions. However, the IN TAK. The 2018 EULAR guidelines26 for pharmaco- role of this modality during follow-up is limited logic treatment of TAK recommend a 2-phase strategy, because cumulative radiation exposure is a concern, with and sensitivity and specificity in low-grade activity DMARD combination in phase I, and a biologic DMARD glucocorticoid and conventional synthetic are poor.19 Also, uptake that is confined to arterial in phase II if relapse occurs (Figure 4). The 2021 graft sites in patients with TAK does not correlate American College of Rheumatology guidelines 30 also with clinically relevant disease activity and may recommend combination therapy of glucocorticoids reflect a foreign body reaction. 28 with DMARDs but differ in recommending tumor JACC VOL. 81, NO. 2, 2023 Joseph et al JANUARY 17, 2023:172–186 Takayasu Arteritis necrosis factor inhibitors as an option in initial therapy; tocilizumab is recommended in refractory dis- 179 T A B L E 5 EULAR Consensus Definitions for Disease Activity States in Large-Vessel Vasculitis ease, an indication for which this drug has seen EULAR Consensus Definition widespread use. OTHER MEDICATIONS. Recently, Kwon et al 31 showed Active disease 1. Presence of typical signs and symptoms of active LVV 2. At least 1 of the following: a. Current activity on imaging or biopsy b. Ischemic complications attributed to LVV c. Persistently elevated inflammatory markers (after other causes have been excluded) Major relapse Recurrence of active disease with either of the following: that patients with TAK receiving concomitant statin and immunosuppressive therapy experienced significantly fewer disease relapses than those not receiving statins; proportions of patients with hypercholester- 1. Clinical features of ischemia 2. Evidence of active aortic inflammation resulting in progressive aortic or large-vessel dilatation, stenosis, or dissection olemia and levels of total cholesterol did not differ between the 2 groups, suggesting that pleiotropic effects of statins, rather than cholesterol-lowering ef- Minor relapse fects, may play a role. Antiplatelet therapy is Refractory Inability to induce remission despite the use of standard care therapy Remission Absence of all clinical signs and symptoms attributable to active LVV and normalization of ESR and CRP Sustained remission 1. Remission for at least 6 mo 2. Achievement of the individual target glucocorticoid dose Glucocorticoid-free remission 1. Sustained remission 2. Discontinued glucocorticoid therapy (but could still be receiving other immunosuppressive therapy) associated with a lower frequency of ischemic events in patients with TAK. 32 Antiplatelet therapy is recom- Recurrence of active disease, not fulfilling the criteria for a major relapse mended in critical cerebrovascular disease in TAK 30 but not routinely.26 FOLLOW-UP OF PATIENTS Clinical follow-up with inflammatory marker level monitoring is prudent every 1 to 3 months for a year Adapted with permission from Hellmich et al.26 CRP ¼ C-reactive protein; ESR ¼ erythrocyte sedimentation rate; EULAR ¼ European League Against Rheumatism; LVV ¼ large-vessel vasculitis. after initiation of immunosuppressive therapy and every 3 to 6 months afterward.26 Response to therapy is typically monitored every 6 to 12 months for the first 2 years using CTA or MRA. 11 MRA has the advantage of not involving radiation or iodinated contrast; acquisition time can be reduced if the study is limited to assessing the arterial lumen, which allows accurate assessment of disease extent. 11 Once disease control has been achieved, annual clinical and depends on the mix of cases and locally available expertise.33 Invasive therapy is best conducted at centers specializing in TAK management, with a multidisciplinary team involving surgeons, in- terventionists, and rheumatologists. 26 Invasive therapy is best avoided in active disease. It is prudent to delay such procedures until disease activity is controlled with immunosuppressive therapy; active evaluation and imaging using MRA are required, disease is associated with more frequent complica- although duplex ultrasound evaluation may suffice in tions such as anastomotic aneurysm formation and some situations. Surveillance should be lifelong, mortality after open surgery and restenosis after given the possibility of relapse after a period of ET. 26,34 If invasive therapy is unavoidable in active remission. disease, high-dose oral glucocorticoids are recom- INVASIVE THERAPY Vascular lesions in TAK are responsible for most of the morbidity and mortality associated with the disease, and efforts to palliate them by invasive therapy form an essential component of disease management. Open surgery was the only modality available for decades; today, endovascular therapy (ET) plays an mended in the perioperative setting.30 STRATEGIES IN INVASIVE THERAPY. In most studies, the primary treatment modality used in ET has been balloon angioplasty, with stenting reserved for suboptimal angioplasty results. Restenosis was higher with adjunctive stenting than stand-alone balloon angioplasty, 35 probably because this strategy channels lesions prone to restenosis toward stenting. increasingly important role. Current guidelines favor restricting invasive therapy in TAK to life- or organ- T A B L E 6 Criteria for Active Disease in Patients With Takayasu Arteritis threatening situations, refractory hypertension, or 1. Systemic features, such as fever, musculoskeletal pain (no other cause identified) when patient activities are significantly affected. 30 2. Elevated erythrocyte sedimentation rate (C-reactive protein added later) The rationale for this guarded stance includes lack of good quality data, improvement of ischemic 3. Features of vascular ischemia or inflammation, such as claudication, diminished or absent pulse, bruit, vascular pain (carotidynia), asymmetric blood pressure in either upper or lower limbs (or both) symptoms with medical therapy and spontaneous 4. Typical angiographic features collateral formation (Figure 5), and the risks associated with open surgery. The proportion of patients requiring invasive therapy varies widely (17%-70%) New onset or worsening of 2 or more features indicates "active disease." They are also referred to as the National Institutes of Health criteria or NIH score. Adapted with permission from Kerr et al21. 180 Joseph et al JACC VOL. 81, NO. 2, 2023 Takayasu Arteritis JANUARY 17, 2023:172–186 T A B L E 7 Prospective Studies of DMARDs in Takayasu Arteritis Drug (Type) Author/Study/ Year Study Type Patients Patient Selection/ Study Details Follow-Up Duration Dose (Standard or Mean) Patients refractory to GC alone 2.8 y 17.1 mg/wk Remission in 13 (81%), sustained in 8 (50%). Disease progression despite treatment in 3 (19%). 1y 2 mg/kg/d Remission in all 15 with no significant angiographic changes compared with baseline. AZA well tolerated. 23.3 mo 2 g/d Clinical remission, decrease in ESR and CRP levels, significant steroid dose reduction attained in 9 (90%). Outcome Methotrexate (CS) Hoffman et al,a 1994 Open-label 18 (2 exited) Azathioprine (CS) Valsakumar et al,b 2003 Open-label 15 Newly diagnosed with active disease Mycophenolate (CS) Shinjo et al,c Open-label 2007 10 Active disease despite GC Leflunomide (CS) Cui et al,d 2020 56 Active disease. LEF for induction, 41 CYC resistant, 15 12 mo 16.8 mg/d Complete remission in 55.4%, partial response in 14.3%; 85.7% continued LEF treatment at 14 mo (mean) with good tolerance. Tofacitinib (TS) Kong et al,e Open-label 2022 comparative Active disease Rapid GC taper during 0-6 mo and slow taper during 6-12 mo 12 mo TOF 5 mg twice daily MTX 10-15 mg/wk Comparing the TOF and MTX groups, respectively: Complete remission at 12 mo was 88% and 56% (P ¼ 0.02); Median relapse-free duration was 11.6 and 10.5 mo (P ¼ 0.03); Mean GC dose at 3, 6, and 12 mo was less in TOF group (P < 0.05). Tocilizumab (B) Nakaoka et al,f TAKT study 2018 162 mg/wk In the intention-to-treat analysis, the primary efficacy endpoint (time to relapse while oral GC was tapered in both groups) had a hazard ratio of 0.41 (P ¼ 0.059). Open-label Phase 3 doubleblind RCT 27 TOF 26 MTX 18 drug 18 placebo Patients with recent 19/12 wk relapse, remission drug/placebog induced with oral GC Continued on the next page Restenosis is a significant problem after ET for obstructive lesions in TAK and occurs PREGNANCY AND TAK more frequently than occlusion of surgical bypass grafts Women with TAK are at increased risk of adverse (43% vs 17% in a large meta-analysis). 36 Repeat ET pregnancy outcomes. A French study 39 of 98 preg- procedures (usually balloon angioplasty) can effec- nancies in 52 patients with diagnosed TAK reported tively treat restenotic lesions, yielding high assisted obstetric complications in 40% and maternal com- patency rates.37 In the coronary arteries, which are plications in 39% (mainly new-onset or worsening involved in 18% of patients with TAK 5 by both hypertension); active disease was an independent vasculitis and premature atherosclerosis, 33 coronary risk factor for both. Conception should, therefore, artery bypass grafting is the preferred treatment op- only be planned after remission is achieved and if tion in patients remaining symptomatic despite contraindications to pregnancy do not exist.40 Medi- medical therapy, as percutaneous coronary inter- cations safe in pregnancy should be used to control vention is associated with a significantly higher hypertension (labetalol, hydralazine, and alpha- restenosis rate. 38 Open surgery has been the standard methyldopa) and for immunosuppression (steroids of care for treating aortic aneurysms in TAK, but the and azathioprine); disease flare-ups can be treated less repair with tumor necrosis factor inhibitors. Most patients (Figure 6), is steadily making inroads into this field. can have a vaginal delivery, although the second Invasive strategies in specific lesions and arteries are stage of labor may have to be expedited to limit detailed in Table 9. surges in blood pressure; Cesarean section is usually invasive alternative, endovascular JACC VOL. 81, NO. 2, 2023 Joseph et al JANUARY 17, 2023:172–186 Takayasu Arteritis 181 T A B L E 7 Continued Drug (Type) Author/Study/ Year Study Type Patients Patient Selection/ Study Details Follow-Up Duration Dose (Standard or Mean) Outcome Tocilizumab (B) Nakaoka et al,h TAKT study 2020 Open-label 36 (28 got TOC for 96 wk) Patients completing the double-blind period of TAKT study 96 wk 162 mg/wk GC dose reduced to <0.1 mg/kg/d in 46% of patients. Imaging evaluations: improved in 18%, stable in 68%. Physical and mental wellbeing scores improved. Tumor necrosis factor inhibitorj (B) Park et al,i 2018 Open-label 12 (1 excluded) Active disease. FDGPET performed at baseline and 30 wk 54 wk 5 mg/kg at wk 0, 2, 6, then q8wk until wk 46 Primary efficacy endpoint (at 30 wk): complete remission in 3 (27%) and partial remission in 6 (55%). Significant improvements were seen in ITAS-2010 and ITAS-A scores, ESR, CRP, and FDG-PET parameters. a Hoffman GS, Leavitt RY, Kerr GS, Rottem M, Sneller MC, Fauci AS. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994;37:578-582. bValsakumar AK, Valappil UC, Jorapur V, Garg N, Nityanand S, Sinha N. Role of immunosuppressive therapy on clinical, immunological, and angiographic outcome in active Takayasu’s arteritis. J Rheumatol. 2003;30:17931798. cShinjo SK, Pereira RM, Tizziani VA, Radu AS, Levy-Neto M. Mycophenolate mofetil reduces disease activity and steroid dosage in Takayasu arteritis. Clin Rheumatol. 2007;26:1871-1875. dCui X, Dai X, Ma L, et al. Efficacy and safety of leflunomide treatment in Takayasu arteritis: case series from the East China cohort. Semin Arthritis Rheum. 2020;50:59-65. eKong X, Sun Y, Dai X, et al. Treatment efficacy and safety of tofacitinib versus methotrexate in Takayasu arteritis: a prospective observational study. Ann Rheum Dis. 2022;81:117-123. fNakaoka Y, Isobe M, Takei S, et al. Efficacy and safety of tocilizumab in patients with refractory Takayasu arteritis: results from a randomised, double-blind, placebo-controlled, phase 3 trial in Japan (the TAKT study). Ann Rheum Dis. 2018;77:348-354. gMedian treatment duration. hNakaoka Y, Isobe M, Tanaka Y, et al. Long-term efficacy and safety of tocilizumab in refractory Takayasu arteritis: final results of the randomized controlled phase 3 TAKT study. Rheumatology (Oxford). 2020;59:2427-2434. iPark EH, Lee EY, Lee YJ, et al. Infliximab biosimilar CT-P13 therapy in patients with Takayasu arteritis with low dose of glucocorticoids: a prospective single-arm study. Rheumatol Int. 2018;38:2233-2242. jInfliximab biosimilar CT-P13. AZA ¼ azathioprine; B ¼ biologic disease-modifying antirheumatic drug; CS ¼ conventional synthetic disease-modifying antirheumatic drug; CYC ¼ cyclophosphamide; DMARD ¼ disease-modifying antirheumatic drug; FDG-PET ¼ 18F-fluorodeoxyglucose positron emission tomography co-registered with computed tomography; GC ¼ glucocorticoid; ITAS-2010 ¼ Indian Takayasu Clinical Activity Score; ITAS-A ¼ activity version of the Indian Takayasu Clinical Activity Score; LEF ¼ leflunomide; MTX ¼ methotrexate; q8wk ¼ every 8 weeks; RCT ¼ randomized controlled trial; TAKT ¼ Takayasu arteritis treated with tocilizumab; TOC ¼ tocilizumab; TOF ¼ tofacitinib; TS ¼ targeted synthetic disease-modifying antirheumatic drug; other abbreviations as in Table 5. reserved for severe hypertension, severe aortic with that of the general population (standardized regurgitation, and obstetric indications. mortality ratio 3.0). Ishikawa and Maetani 44 reported OCULAR INVOLVEMENT enced by vascular complications, progressive clinical in 1994 that survival in TAK was negatively influcourse of disease (crescendo pattern), and elevated The common forms of ocular involvement in TAK are erythrocyte Takayasu retinopathy (15%), ocular ischemic syn- Comarmond drome (7%), hypertensive retinopathy (16%), and complication-free survival in TAK as 70% and 54%, steroid-induced cataract (23%); retinopathy and ocular ischemic syndrome are only seen in patients sedimentation et al24 rate. reported More 5- recently, and 10-year respectively; progressive clinical course (<1 year from symptom onset to diagnosis), thoracic aorta with aortic arch involvement and were associated with low or nonrecordable upper limb blood pres- T A B L E 8 Effects of DMARDs in Takayasu Arteritis sure. 41 A recent systematic review of the treatment of Type of DMARD ocular ischemia in 66 patients with TAK found that carotid revascularization by open surgery or ET All Biologic Conventional Synthetic 64 effectively improved both acute and chronic vision At least partial clinical remission attained 78 84 loss; the visual prognosis was better in patients with Angiographic stabilization 85 86 81 less severe retinopathy and better visual acuity at Improvement of PET-CT parameters 69 69 ND baseline.42 Normalization of inflammatory markers 90 92 80 Relapses 22 26 15 Adverse events 18 21 13 Infections 6 8 2 Median reduction in prednisolone dose 81 81 ND Mean reduction in prednisolone dose 65 70 63 PROGNOSIS The prognosis of patients with TAK has improved in this millennium, which is attributable to several factors (Central Illustration). The overall survival was Values are %. Extracted with permission from Misra et al.29 97% at 10 years and 86% at 15 years in a North DMARD ¼ disease-modifying antirheumatic drug; PET-CT ¼ positron emission tomography co-registered with computed tomography; ND ¼ no data. 43 American study ; mortality was increased compared 182 Joseph et al JACC VOL. 81, NO. 2, 2023 Takayasu Arteritis JANUARY 17, 2023:172–186 F I G U R E 4 The 2018 EULAR Algorithm for Pharmacologic Treatment of Takayasu Arteritis Phase I Diagnosis of Takayasu arteritisa Start glucocorticoid (GC) 40-60 mg/day + Start csDMARDb Taper GC to 15-20 mg/day within 2-3 months and then to ≤10 mg/day after 1 year Continue taper Yes Targetc achieved? No Phase II Consider tocilizumab or TNF-inhibitor Major relapse Minor relapse Increase GC to 40-60 mg/day Increase GC to last effective dose Taper GC Taper tocilizumab or TNF-inhibitor Yes Targetc achieved? No Consult expert center Proposed 2-phase treatment protocol involving glucocorticoids (GC) and conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) in phase I, and biologic DMARD if relapse occurs (phase II). aThe clinical diagnosis of Takayasu arteritis should be confirmed by imaging. bCyclophosphamide should be used only if all other csDMARDs are ineffective. cThe treatment target is sustained remission plus the ability to taper GCs to the specified target without relapse. TNF ¼ tumor necrosis factor. Adapted with permission from Hellmich et al.26 involvement, and retinopathy were identified as risk robust, gold standard criteria for diagnosing TAK and factors for vascular complications. The prognosis in determining disease activity are 2 critical lacunae. patients with pulmonary artery involvement is worse Reliable biomarkers are required to distinguish sub- in those with pulmonary hypertension than those sets of large-vessel vasculitis, assess disease activity, without it.45 and predict response to specific therapies.11 Safe imaging techniques with high sensitivity and specificity DIRECTIONS FOR FUTURE RESEARCH in detecting areas of vascular inflammation are another area of need. A deeper understanding of the Several lacunae exist in the management of TAK that pathogenesis of TAK may unravel new targets for could be the focus of future research. The lack of effective drug development. More clarity is required JACC VOL. 81, NO. 2, 2023 Joseph et al JANUARY 17, 2023:172–186 Takayasu Arteritis F I G U R E 5 Middle Aortic Syndrome in a 38-Year-Old Woman With Takayasu Arteritis (A) Reconstructed computed tomography angiography image showing severe stenosis of the descending thoracic and abdominal aorta with multiple bridging collaterals, including bilateral Winslow pathway collaterals (yellow arrows). Baseline descending thoracic (B) and abdominal aortic (C) conventional angiograms and corresponding 1-year follow-up angiograms (D, E) after successful endovascular therapy using an endograft (blue arrow in D) and a braided self-expanding bare stent (red arrow in E). in managing advanced vascular disease, and ran- CONCLUSIONS domized trials may be required to settle issues that have eluded resolution. A global registry to capture The outlook for patients with TAK has improved the heterogeneity in TAK worldwide would be ideal. significantly in recent years with the establishment of 183 184 Joseph et al JACC VOL. 81, NO. 2, 2023 Takayasu Arteritis JANUARY 17, 2023:172–186 F I G U R E 6 Aneurysms in a 27-Year-Old Woman With Takayasu Arteritis Reconstructed computed tomography angiography images are shown. (A) Descending thoracic aorta and left subclavian artery (yellow arrow) aneurysms. (B) Six-year follow-up after successful endovascular therapy of both aneurysms. The celiac artery received a covered stent (white arrow) to treat ostial stenosis. T A B L E 9 Invasive Strategies for Specific Lesions and Arteries Strategy Comment Aortic/mitral regurgitation Valve replacement surgery Hospital mortality 4.8% with aortic valve replacement, late dilatation of ascending aorta 11.1%a Coronary artery occlusion/stenosis Coronary artery bypass surgery if refractory to medical treatment PCI is associated with 39% restenosis compared with 9% with bypass surgeryb Carotid artery occlusion/stenosis Balloon angioplasty adjunctive stenting, or bypass surgery High incidence of brain hyperperfusion after carotid artery bypass surgeryc Subclavian artery occlusion/stenosis Balloon angioplasty adjunctive stenting in short lesions (<8 cm); conservative Rx in long lesions High restenosis rates in long lesions Distal anastomosis to small arteries may impact bypass surgery resultsd Descending thoracic stenosis Endovascular therapy/bypass surgery Long endografts enable safe high-pressure lesion dilatation (Figure 5) Visceral aorta occlusion or stenosis Endovascular therapy/bypass surgery Access to aortic side branches is possible via braided selfexpanding stent strutse Infra-renal aorta and iliac occlusion/ stenosis Endovascular therapy/aorto-bi-iliac or -femoral bypass surgery Covered stents are preferred in occlusions to avoid rupture and bare stents for stenosis Mesenteric/renal aorto-ostial occlusion/stenosis Balloon angioplasty adjunctive stenting or elective covered stentd Bypass surgery/renal autotransplant if endovascular therapy is not feasible Pulmonary artery occlusion/stenosis Balloon angioplasty adjunctive stenting; staged revascularization Angioplasty improves survival in patients with pulmonary hypertensionf Aortic aneurysms Open surgery/Bentall procedure/endovascular therapy (Figure 6) Hospital mortality 7.4% with Bentall procedurea 93% 5 y survival in a recent hybrid series of thoracic aortic aneurysmsg a Matsuura K, Ogino H, Kobayashi J, et al. Surgical treatment of aortic regurgitation due to Takayasu arteritis: long-term morbidity and mortality. Circulation. 2005;112:3707-3712. bHuang et al.38 cLuo XY, Wu QH, Zhang FX. Open and endovascular management of severe cerebral ischemia in Takayasu’s arteritis. Ann Vasc Surg. 2017;42:101-110. dPorter and Mason.33 eJoseph G, George PV, Pati PK, Chandy ST. Feasibility of angioplasty and stenting for abdominal aortic lesions adjacent to previously stented visceral artery lesions in patients with Takayasu arteritis. Cardiovasc Intervent Radiol. 2007;30:293-296. f Zhou YP, Wei YP, Yang YJ, et al. Percutaneous pulmonary angioplasty for patients with Takayasu arteritis and pulmonary hypertension. J Am Coll Cardiol. 2022;79:1477-1488. gOishi K, Mizuno T, Fujiwara T, et al. Surgical strategy for inflammatory thoracic aortic aneurysms in the endovascular surgery era. J Vasc Surg. 2022;75:74-80.e2. PCI ¼ percutaneous coronary intervention; Rx ¼ treatment. JACC VOL. 81, NO. 2, 2023 Joseph et al JANUARY 17, 2023:172–186 Takayasu Arteritis C ENTR AL I LL U STRA T I O N Components of Patient Care in Takayasu Arteritis Early diagnosis • An initial "prepulseless" phase often goes undiagnosed, characterized by: • nonspecific constitutional symptoms (fever, malaise, weight loss) • raised acute phase reactants (ESR, CRP) • 18FDG uptake in inflamed arterial walls revealed by PET-CT • Immunosuppressive therapy relieves symptoms and prevents vascular damage Vascular damage assessment • CT and MR angiography are the commonly used imaging modalities • Involved arteries typically show wall thickening, obstructive lesions, ectasia, or aneurysm formation Optimal long-term patient outcome Life-long surveillance • Disease activity and vascular damage need life-long periodic assessment given the persistent potential for relapse • Modalities include clinical assessment, acute phase reactant levels, MR or CT angiography, and duplex-ultrasonography Immunosuppressive therapy • Halts progressive vascular damage • Corticosteroids and DMARDs (synthetic or biologic) are often used in combination • Dose and duration are tailored to suppress disease activity that is assessed periodically using clinical and imaging parameters Invasive therapy • Performed to palliate critical obstructive or aneurysmal vascular lesions • Open surgery and endovascular therapy play complementary roles Joseph G, et al. J Am Coll Cardiol. 2023;81(2):172–186. Five vital contributing arms of management that together lead to optimal long-term patient outcomes are depicted. 18 FDG ¼ 18 fluoro-deoxy-glucose; CRP ¼ C-reactive protein; CT ¼ computed tomography; DMARD ¼ disease-modifying antirheumatic drug; ESR ¼ erythrocyte sedimentation rate; MR ¼ magnetic resonance; PET-CT ¼ positron emission tomography co-registered with computed tomography. diagnostic and classification criteria, better investi- FUNDING SUPPORT AND AUTHOR DISCLOSURES gational modalities, and more effective medical and invasive therapy. However, the understanding of disease pathogenesis remains poor, diagnosis of TAK The authors have reported that they have no relationships relevant to the contents of this paper to disclose. tends to be delayed, and advanced vascular injury at presentation is common. Dependence on corticosteroid therapy, although reduced, is still too high. ADDRESS Monitoring of disease activity and vascular disease Joseph, Department of Cardiology, Christian Medical FOR CORRESPONDENCE: progression remains suboptimal. Much work remains College, Vellore-632004, India. E-mail: joseph59@ to be done more than a century after the initial gmail.com OR josephg@cmcvellore.ac.in. Twitter: description of this disease. @GeorgeJoseph59. Dr George 185 186 Joseph et al JACC VOL. 81, NO. 2, 2023 Takayasu Arteritis JANUARY 17, 2023:172–186 REFERENCES 1. Numano F. The story of Takayasu arteritis. Rheumatol Oxf Engl. 2002;41:103–106. for the classification of Takayasu arteritis. Arthritis Rheum. 1990;33:1129–1134. 2. Jennette JC, Falk RJ, Bacon PA, et al. 2012 Revised International Chapel Hill Consensus Con- 18. Sharma BK, Jain S, Suri S, Numano F. Diagnostic criteria for Takayasu arteritis. Int J Cardiol. 1996;54(Suppl):S141–S147. ference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65:1–11. 3. Onen F, Akkoc N. Epidemiology of Takayasu arteritis. Presse Medicale Paris Fr 1983. 2017;46: e197–e203. 4. Sun Y, Yin M-M, Ma L-L, et al. Epidemiology of Takayasu arteritis in Shanghai: a hospital-based study and systematic review. Int J Rheum Dis. 2021;24:1247–1256. 5. Danda D, Goel R, Joseph G, et al. Clinical course of 602 patients with Takayasu’s arteritis: comparison between childhood-onset versus adultonset disease. Rheumatol Oxf Engl. 2021;60: 2246–2255. 19. Tombetti E, Mason JC. Application of imaging techniques for Takayasu arteritis. Presse Medicale Paris Fr 1983. 2017;46:e215–e223. 20. Hata A, Noda M, Moriwaki R, Numano F. Angiographic findings of Takayasu arteritis: new classification. Int J Cardiol. 1996;54(suppl):S155– S163. 21. Kerr GS, Hallahan CW, Giordano J, et al. Takayasu arteritis. Ann Intern Med. 1994;120:919– 929. 22. Quinn KA, Gribbons KB, Carette S, et al. Patterns of clinical presentation in Takayasu’s arteritis. Semin Arthritis Rheum. 2020;50:576–581. 6. Vaideeswar P, Deshpande JR. Pathology of Takayasu arteritis: a brief review. Ann Pediatr Cardiol. 2013;6:52–58. 23. Ishikawa K. Patterns of symptoms and prognosis in occlusive thromboaortopathy (Takayasu’s disease). J Am Coll Cardiol. 1986;8:1041–1046. 7. Miller DV, Maleszewski JJ. The pathology of large-vessel vasculitides. Clin Exp Rheumatol. 2011;29:S92–S98. 24. Comarmond C, Biard L, Lambert M, et al, Takayasu French Network. Long-term outcomes 8. Renauer P, Sawalha AH. The genetics of Takayasu arteritis. Presse Medicale Paris Fr 1983. 2017;46:e179–e187. 9. Ortiz-Fernández L, Saruhan-Direskeneli G, Alibaz-Oner F, et al. Identification of susceptibility loci for Takayasu arteritis through a large multiancestral genome-wide association study. Am J Hum Genet. 2021;108:84–99. 10. Terao C, Yoshifuji H, Kimura A, et al. Two susceptibility loci to Takayasu arteritis reveal a synergistic role of the IL12B and HLA-B regions in a Japanese population. Am J Hum Genet. 2013;93: 289–297. 11. Tombetti E, Mason JC. Takayasu arteritis: advanced understanding is leading to new horizons. Rheumatology. 2019;58:206–219. 12. Deng J, Ma-Krupa W, Gewirtz AT, Younge BR, Goronzy JJ, Weyand CM. Toll-like receptors 4 and 5 induce distinct types of vasculitis. Circ Res. 2009;104:488–495. 13. Arnaud L, Haroche J, Mathian A, Gorochov G, Amoura Z. Pathogenesis of Takayasu’s arteritis: a 2011 update. Autoimmun Rev. 2011;11:61–67. 14. Mutoh T, Shirai T, Ishii T, Shirota Y, et al. Identification of two major autoantigens negatively regulating endothelial activation in Takayasu arteritis. Nat Commun. 2020;11:1253. 15. Clifford AH, Cohen Tervaert JW. Cardiovascular events and the role of accelerated atherosclerosis in systemic vasculitis. Atherosclerosis. 2021;325:8– 15. 16. Ishikawa K. Diagnostic approach and proposed criteria for the clinical diagnosis of Takayasu’s arteriopathy. J Am Coll Cardiol. 1988;12:964–972. 17. Arend WP, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria and prognostic factors of complications in Takayasu arteritis: a multicenter study of 318 patients. Circulation. 2017;136:1114–1122. 25. Goel R, Danda D, Joseph G, et al. Long-term outcome of 251 patients with Takayasu arteritis on combination immunosuppressant therapy: singlecenter experience from a large tertiary care teaching hospital in Southern India. Semin Arthritis Rheum. 2018;47:718–726. 26. Hellmich B, Agueda A, Monti S, et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. 2020;79:19–30. 27. Misra R, Danda D, Rajappa SM, et al. Indian Rheumatology Vasculitis (IRAVAS) group. Development and initial validation of the Indian Takayasu Clinical Activity Score (ITAS2010). Rheumatol Oxf Engl. 2013;52:1795–1801. 28. Youngstein T, Tombetti E, Mukherjee J, et al. FDG uptake by prosthetic arterial grafts in large vessel vasculitis is not specific for active disease. J Am Coll Cardiol Img. 2017;10:1042–1052. 29. Misra DP, Rathore U, Patro P, Agarwal V, Sharma A. Disease-modifying anti-rheumatic drugs for the management of Takayasu arteritis— a systematic review and meta-analysis. Clin Rheumatol. 2021;40:4391–4416. 30. Maz M, Chung SA, Abril A, et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Giant Cell Arteritis and Takayasu Arteritis. Arthritis Rheumatol Hoboken NJ. 2021;73:1349–1365. 31. Kwon OC, Oh JS, Park M-C, et al. Statins reduce relapse rate in Takayasu arteritis. Int J Cardiol. 2019;287:111–115. 32. de Souza AWS, Machado NP, Pereira VM, et al. Antiplatelet therapy for the prevention of arterial ischemic events in Takayasu arteritis. Circ J. 2010;74:1236–1241. 33. Porter A, Mason JC. Intervention in Takayasu aortitis: when, where, and how? Hearts. 2020;1: 62–74. 34. Saadoun D, Lambert Retrospective analysis of vascular intervention in multicenter experience. 813–819. M, Mirault T, et al. surgery versus endoTakayasu arteritis: a Circulation. 2012;125: 35. Peng M, Ji W, Jiang X, et al. Selective stent placement versus balloon angioplasty for renovascular hypertension caused by Takayasu arteritis: two-year results. Int J Cardiol. 2016;205:117– 123. 36. Jung JH, Lee YH, Song GG, Jeong HS, Kim J-H, Choi SJ. Endovascular versus open surgical intervention in patients with Takayasu’s arteritis: a meta-analysis. Eur J Vasc Endovasc Surg. 2018;55: 888–899. 37. Gülcü A, Gezer NS, Akar S, Akkoç N, Önen F, Göktay AY. Long-term follow-up of endovascular repair in the management of arterial stenosis caused by Takayasu’s arteritis. Ann Vasc Surg. 2017;42:93–100. 38. Huang Z, Zhang H, Wang M, Yang W, Qiao S, Hu F. Revascularization versus medical therapy in Takayasu’s arteritis patients with coronary artery involvement. Rheumatol Ther. 2021;8:119–133. 39. Comarmond C, Mirault T, Biard L, et al, Takayasu French Network. Takayasu arteritis and pregnancy. Arthritis Rheumatol. 2015;67:3262– 3269. 40. Padiyar S, Manikuppam P, Kabeerdoss J, Rathore S, Danda D. Update on pregnancy in Takayasu arteritis—a narrative review. Int J Rheum Dis. 2021;24:758–765. 41. Peter J, David S, Danda D, Peter JV, Horo S, Joseph G. Ocular manifestations of Takayasu arteritis: a cross-sectional study. Retina. 2011;31: 1170–1178. 42. Zeng Y, Duan J, Ge G, Zhang M. Therapeutic management of ocular ischemia in Takayasu’s arteritis: a case-based systematic review. Front Immunol. 2022;12:791278. 43. Schmidt J, Kermani TA, Bacani AK, et al. Diagnostic features, treatment, and outcomes of Takayasu arteritis in a US cohort of 126 patients. Mayo Clin Proc. 2013;88:822–830. 44. Ishikawa K, Maetani S. Long-term outcome for 120 Japanese patients with Takayasu’s disease. Clinical and statistical analyses of related prognostic factors. Circulation. 1994;90:1855– 1860. 45. Huang Z, Gao D, Liu Z, Liu X, Liang Y. Longterm outcomes and prognostic predictors of patients with Takayasu’s arteritis along with pulmonary artery involvement. Clin Exp Rheumatol. 2022;40:765–771. KEY WORDS antirheumatic agents, endovascular procedures, immunosuppression, invasive procedures, vasculitis