Pancreatitis: Causes, Symptoms & Treatment - Patient Education
advertisement

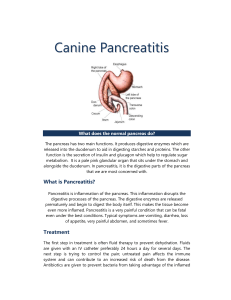
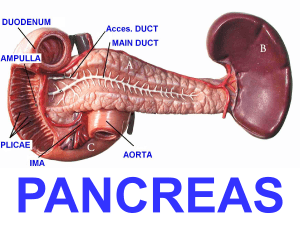
Primary medical problem: PANCREATITIS Rigas Allie PATHO PT EDU-- INFLAMMATION OF THE PANCREAS that Triggers premature release of pancreatic enzymes: o L/T AUTO-DIGESTION Where is it? A gland located behind the stomach. What does it do? Produces digestive enzymes/hormones that aid in digestion and regulation of blood sugar levels. Your pancreas is a gland located behind your stomach that makes digestive juices to help break down things you consume and helps maintain your blood sugar level. Blood sugar is needed by all the cells in your body for energy and to do their job properly. ACUTE PANCREATITIS: Digestive enzymes (Cytokines and Chemokines) produced by the pancreas are activated prematurely and begin to digest the pancreas itself. L/T inflammation and damage to pancreatic tissue. CB many possible factors: o Gallstones o Alcohol abuse o High levels of triglycerides in the blood o Infections o Certain medications. Inflammatory response = L/T edema and ischemia Immune cells: neutrophils, monocytes, and macrophages Release more pro-inflammatory mediators L/T ^^^ permeability of blood vessels o L/T exacerbating inflamm response Edema Ischemia Necrosis o = further tissue damage Degree of injury is correlated with the severity of the disease. Inflammation can spread to nearby organs, triggering: Systemic response L/T multi-organ dysfunction and failure o More severe without prompt Tx CHRONIC PANCREATITIS: Chronic inflammation of the pancreas. Often caused by chronic alcohol abuse. Pancreatitis is inflammation or swelling of the pancreas happens as a response reaction, just like when you catch a cold your body triggers various response reactions like a fever, coughing, or fatigue to help fight off the infection. Our bodies always want to return us to something called homeostasis, or a happy healthy zone that is optimal for everything to work how it’s supposed to. Pancreatitis is when the pancreas becomes swollen, causing symptoms such as: o Severe abdominal pain o Nausea o Vomiting o Fever There are two types of pancreatitis: Acute pancreatitis (sudden onset) Chronic pancreatitis (prolonged) Early diagnosis and management is important to: o Prevent further damage to the pancreas and systemic complications Treatment typically involves hospitalization, supportive care, pain management, and The constant inflammation L/T: Fibrosis and scarring of the pancreas-o Impairs its function- L/T— Chronic pain Malabsorption Eventually diabetes Body System(s) addressing the underlying causes of the condition. How is each system impacted 1. Digestive system 1. Pancreas produces enzymes that help break down food in the small intestine. Inflammation can L/T digestive problems: a. Nausea b. Vomiting c. Diarrhea. 2. Endocrine system 2. Pancreas also produces hormones: Insulin and glucagon Help regulate BG levels Inflammation can cause problems with BG control L/T: Hyper/Hypoglycemia 3. Cardiovascular system 4. Respiratory system 3. Severe cases of pancreatitis: a. Inflammation can spread to other organs, including: i. Heart and blood vessels b. L/T complications: i. HYPOtension ii. Dysrhythmias iii. HF 4. Severe cases of pancreatitis, inflammation affect the lungs L/T: o Respiratory distress o Pneumonia o Acute respiratory distress syndrome (ARDS) 5. Nervous system 5. Rare that o o o cases, severe pancreatitis can L/T complications affect the nervous system: Seizures AMS/confusion Coma Tx— ABDO PAIN RELIEF IVF TO REPLENISH FLUID/LYTES NPO WITH NG TUBE & SXN, and DECREASE GI MOTILITY TX OR PROPHYLAXIS O’ INFECTION ID UNDERLYING CAUSE & TX: AXBX, ANTICHOLINERGICS, PANCREATIC ENZYMES (LIPASE, TRYPSIN, AMYLASE) WITH MEALS (CHRONIC PANCREATITIS); SX IF D/T BILIARY DISEASE Priority assessments What are the expected abnormal findings? 1. MONITOR FOR VS ALTERATIONS INDICATORS FOR LIFETHREATENING (SHOCK) 1. Shock d/t hemorrhage/perforation, excessive FV shifting, or abdo sepsis from pancreatic enzyme damage: a. HYPOtension b. Tachycardia c. Fever 2. ASSESS LOC/ALTERATION 2. LOC alterations d/t drop in BP = poor cerebral perfusion 3. ABDOMINAL 3. Abdo pain that may radiate to back: Sudden onset Severe, deep, stabbing, continuous or steady Abdo tenderness with guarding Rigid, board-like appearance HYPO-active or absent bowel sounds Anorexia N/V Ascites 4. SKIN 5. F/E STATUS: I/O’s 6. BG levels 4. Jaundice: yellowing of skin/sclera Cullen’s sign: blueish periumbilical color Grey Turner’s sign: bluish flank color 7. CARDIOVASCULAR 5. ^RF dehydration, hypovolemia 8. RESPIRATORY 6. Hyperglycemia may result d/t chronic pancreatitis tetany 9. NUTRITIONAL STATUS 7. Dysrhythmias 10. PAIN 8. Tachypnea may result d/t diaphragm elevated, pain, pulmonary infiltrates, effusion and atelectasis 9. Malnourished d/t inadequate dietary intake, impaired pancreatic secretions, and increased nutritional needs 10. d/t pancreatic inflammation, abdo/back pain Abnormal labs 1. WBC How affected (high or low) 1. Leukocytosis (H) > 10,000 2. Ca 2. HYPOcalcemia (L) < 9 How does the abnormal lab affect physical assessment findings? 1. Fever, overall malaise/fatigue 2. Tetany: muscle spasms (laryngospasm/bronchospasm = dyspnea); muscle cramps; V; seizure; impaired cardiac function (dysrhythmias) 3. Pancreatic Enzymes 3. Amylase (H) WNL: 30-110 (^ 2-3x) 3. Severe abdo or back pain; T; N/V; anorexia Lipase stays elevated longer than amylase. Lipase (H) WNL: 10-150 4. BG 4. HYPERglycemia (H) 5. K 5. HYPOkalemia (L) < 3.5 4. Urgency or frequency Thirsty Blurred vision Weak/fatigue 5. Weak, fatigue, dizzy Muscle cramps/spasms C Arrhythmias Medication Mechanism of Action Expected outcome 1. Albumin 1. Plasma volume expander 1. Replace fluid volume Prevent renal failure 2. Lactated Ringers 2. Correct F&E imbalances 2. Replenish blood volume and return lytes to WNL. 3. PPI a. Omeprazole (Prilosec) 3. Decrease hydrochloric (HCl) acid secretions (HCl secretions stimulate pancreas) 3. Decrease triggering factors of inflammation response. 4. AxBx 4. Eliminate growth of pathogens causing infection 5. Analgesics 4. Tx and prophylaxis of infection d/t necrotic tissue. 5. Pain relief 6. Anticholinergics 7. Pancreatic enzyme replacement therapy (PERT) 6. Inhibits pancreatic enzyme secretions (Acute) 5. Pt will report tolerable pain level. 6. Reduce tissue damage CB pancreatic enzymes 7. Proteases digest protein; amylases digest carbs; lipase digests fat. (chronic) 7. Pt has improved digestion and absorption of food